Embed Size (px)
Citation preview

Neonatal Haematology
DR. AGELEBE.E Bowen University Teach
Hosp Ogbomoso

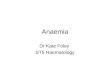
Fetal circulation
O2 blood from placenta
Umbilical vein(50%) Hepatic circulation
Bypassesliver
Ductus venosus
IVC
RA (ovale)
SVC LA
TV
RV
Lungs (10%)PA
LV
PDA
DescendingAorta
Umbilical arteries
Blood from lower part of body
Ascending aorta
Upper part of body
Lower partOf body
SPO2 45%

Globin Synthesis in Embryo, Fetus and Adult


Regulation of Erythropoiesis
Retic count is 3 -7%
Fetal haemoglobin increases with gestational age, at
about 28 weeks, fetal Hb is about 45%.

Normal Hemoglobin and MCV Values in Term
Infant
Hb MCV
(g/dL) (fl)
Day 1 19.0±2.2 119 ±9.4

Anatomy /PhysiologyIn-utero fetal blood volume is 115ml/kg(75ml baby & 40ml placenta)
• At birth : 80 – 90ml/kg.
• After birth, SPO2 rises to 95%
• Newborn - 90 days
• Preterm - 75 days
• Adult - 120 days
• Hb nadir occurs at 8 – 12 weeks in term
• 12 weeks PCV= 11.3 ±0.9 MCV= 88 ±7.9
• HbA /HbF starts to increase
• 2,3 –DPG increases
• Oxygen delivery to tissue increases

Haematological Indices
HAEMATOLOGICAL INDICES
1. Haemoglobin (g/dl)
Term 14 – 20
Preterm 14 at 28 weeks of gestation. (It is 1 -2g/dl less.)
2. Haematocrit 45 – 65%, (lower in preterm)
3. White blood cells (Varies with post-natal age)
Day 1 6,000 – 35,000/µL
Week 1 8,000 – 16,000/µL
First month 6,000 – 14,000

FBC Differentials Neutrophils %
Day 1 50 – 80 (Neutrophil predominance)
Day 4 35 – 60 (Approx % of lymphocytes)
Day 7 35 – 45 (Is falling)
3 months – 7 years 25 – 45 ( typical childhood lymphoctes predominance
Lymphocte
%
Day 1 31
Day 7 41
Day 14 48
Retic count%
Day 1 2 – 8Day 7 0.51 month 0 .2– 0.5

Neonatal anaemia
• The most common haematological disoder
• Reduced haemoglobin below normal for gestational and post-natal age.
• Different classification

Aetilogical Classification of Anaemia(1)
A. Blood loss fetal to fetal, feto-maternal, traumatic delivery
B. Excessive blood destruction
1. Intrinsic factors
a. Enzymatic defect: G6PD deficiency, pyruvate kinase
b. Defects of membrane: spherocytosis, elliptocytosis
c. Defects of hemoglobin
Synthesis anomaly: thalassemia

Aetilogical Classification of Anaemia(1)
2. Extrinsic factors
a. Immune mechanisms: Rh, ABO incompatibility, autoimmune hemolytic anemia
b. non-immune mechanisms: infections
C. Decreased production
1. Deficiency of substrates: iron, folic acid
a. Primary: aplastic anemia

Classification Based on Onset Time
• Early-onset Anaemia
• Late-onset Anaemia

EARLY-ONSET ANAEMIA
• Occurs in first few days after birth
• Most frequently due to haemolytic disease or haemorrhage
Causes Haemolytic disease
• Rhesus haemolytic disease
• ABO haemolytic disease
• G6PD deficiency – is common here, 20 – 25% of male population
• Infections – causes suppression of bone marrow and excessive haemolysis

EARLY-ONSET ANAEMIA
Causes
• Neonatal haemorrhage –
Birth trauma -
– Cephal haematoma
– Sugaleal haematoma
– Ruptured Liver or spleen etc
– Intra-abdominal haemorrhage
– Fracture of femur

EARLY-ONSET ANAEMIA
• Maternal infections e.g parvo-virus
• Others
– Spherocytosis
– α-thalassemias
– Fetal haemorrhage
- Abruptio placentae
- Vasa praevia
– Fetomaternal transfusion
– Twin-twin transfusion
– Congenital hypoplastic anaemia

Clinical Presentation
History • Antepartum haemorrhage
• Multiple delivery
• Instrumental delivery
• Poor feeding
• Breathlessness
Physical examination
• Colour
• Bruises – scalp, shoulder
• Cephal haematoma – is limited at suture line
• Rigid abdomen
• Small pulse volume
• Tachycardia
• Hypotension
• Tachypnoea
• Fever /Hypothermia –suggesting infections

Management
Investigation
• PCV
• WBC - pancytopaenia is a feature of aplastic anaemia
• Blood film – may show spherocytosis
Treatment
• Asymptomatic – leave the child
• If in shock (and the child is term) i.e BP < 25mmHg, PCV < 30%, pH < 7.1 Immediate transfusion with 15 – 20ml/kg of whole blood over 5 – 10minutes ( if it is due to haemorrhage)

Management Treatment
• If not in shock, but anemia is severe
• Transfuse 20ml/kg over 2 – 3hours with IV frusemide, 2mg/kg
• or
• 10 – 15ml/kg (2 -3 mls/kg/hour) partially packed
• Note : 2ml/kg of packed cells raises haemoglobin by 0.5 – 1g/dl or PCV of 10%.
• Very severe anaemia Hb < 8g/dl or the child is in congestive cardiac failure
• Single volume EBT with packed cells
• The procedure involves – calculating the total volume
– Taking of blood in aliquots (10mls for each round)

LATE ONSET ANAEMIA
This appears later in the neonatal period
• Causes– Mild haemorrhagic disease of the newborn
– Haemolytic disease of the newborn – ABO incompatibility (Note Rhesus isommunization often presents as early-onset anaemia
– Chronic blood loss e.g GI bleeding (Merkel’s diverticulum)
– Infection – causing DIC by the toxins which damage to the endothelium, stimulating consumption coagulopathy. It also depresses bone marrow.
– Chronic infections e.g. rubella, parvovirus
– G6PD deficiency
– Spherocytosis
– α – thalassemia
– Congenital hypolplastic aplasia
– Repeated venipuncture

Management
• If it is severe, do exchange blood transfusion
•
• Transfuse with straight forward transfusion if
moderate
• If mild would need haematinics

ANAEMIA OF PREMATURITY• An exaggeration of physiological anaemia
• Common in preterm because of lower RBC life span and higher tendency to be sick.
• Reasons For Higher Incidence Rate in Preterm
• Minimum value of PCV is reached earlier in preterm than in term babies which is
about 6 weeks (1- 3 months)
• Their RBCs have reduced life span
• Iatrogenic – samples for investigation.
• Because of relative more rapid somatic growth rate.
• Due to Vitamin E deficiency – from relative fat absorption
• Preterm infants start to produce erythropoietin when Hb falls to 7 – 9g/dl in contrast to
10 – 11g/dl in term infants because their tissues require lower oxygen requirement.

Clinical Presentation
• May be asymptomatic
• Pallor
• Apnoea
• Poor weight gain
• Tachypnoea
• Tachycardia
• Re-opening of Patent ductus arteriousus

Management
• If symptomatic – give blood transfusion slowly with
10ml/kg of packed cells over 1 – 3 hours. Note,
haematinics are not used because it takes longer time
to act if moderate to severe.)

Prevention
• Adminstration of folic acid 5mg weekly to babies < 2kg from 2 weeks of age.
• Adminstration of α – tocopherol acetate (Vit E) daily to babies < 1.5kg from 2 weeks of age
• Administration of Ferous sulphate, 50 mg/day or elemental iron 6mg/kg/day from 2kg or 2 weeks of age.
• Use of recombinant human erythropoietin, 100 -22iu/kg, given 5d /week, 400u/kg/d, 3d/week + iron + vit. E. This is forcing baby to start erythropoieis, after which iron can be given in this case.

Polycythaemia
• Definition
• Is venous PCV > 65% ( the more the PCV above 65%, the low the oxygen carrying capacity due to increase in viscosity.
• Aetiology
• Placenta insufficiency – due to placental infarcts e.g in diabetes mellitus
• Maternal –fetal transfusion – due to delayed cord clamping
• Twin-twin transfusion e.g monozygotic twins
• Infants of diabetic mothers (IDM) - due to hypoxia caused by vascular problems
• Dehydration
• Others– Congenital adrenal hyperplasia
– Trisomy 13, 18, 21
– Neontal thyrotoxicosis
– Becwith-Weidmann syndrome
– Maternal drugs e.g propanolol
•

Clinical Presentation
General
• Plethora
• Jaundice
• Cyanosis (≥ 5g/dl of deoxygenated blood) -may be a cause or effect.
• Prolonged capillary refill
Respiration
• Tachypnoea
• Dyspnoea
GIT
• Feeding problems
• Necrotizing enterocolitis
CNS – Mostly undesirable
• Irritability
• Jitteriness
• Lethargy
• Seizures

Investigation Complications
• Thromboembolism
• Pulmonary haemorrhage
• Congestive cardiac failure
• Brain damage
•Bilirubin -
hyperbilirubinaemia
•Blood sugar –
hypoglycaemia
•Serum calcium –
hypocalcaemia
•Chest X-ray – shows
prominent pulmonary
vascular markings

Management
• If PC < 70% and the child is asymptomatic
• Admit and observe
• Ensure no dehydration
•
• If < 70% and symptomatic
• - Do erythropoiesis ( note, not plasmapharesis)
•
• If > 70% and asymptomatic
• Treat

Management Con’t
Calculation
Vol(ml) = bld vol x (observed-desired pcv)
actual pcv
• Blood Volume = 80 – 90ml X Weight
The following can be used– plasma
– Fresh frozen plasma
– Normal saline
– Haemacel

Management Con’tPrecaution
• At any time, don’t take > 25% of blood
volume.

Bleeding Disorders
Tests of coagulation:
• PT ; Extrinsic system
• Dependent on factors II VII, IX, X (1972) measures vit K def.
• Normal range is 13 – 20s
• PTT; Measures intrinsic pathway factors XII, XI, VII, X, V, II, I
• Prolonged in DIC, heparin therapy, haemophylia and severe vit k def
• In Vitamin k deficiency, both PT & PTTK are done abnormal

Bleeding Disorders
Tests of coagulation:
PT ratio ( Test/Control )INR
• Normal range = 0.9 – 1.2.
• Fibrinogen – Normal range is 150 – 300mg/dl
Bleeding time
• Platelet function

HAEMORRHAGIC DISEASE OF THE NEWBORN
HDNIt is due to deficiency of vitamin K in newborn.
• Normally, the gut of babies are sterile and breast milk is not rich in vitamin K.
• It takes about a week for the baby to acquire gut flora.
• Vitamin K received from the mother disappears after few days, 2 – 7days, leading to the inactivation of vitamin K dependent factors, thus prone to HDN.
• It may result into provoked or unprovoked bleeding.
• The common sites of haemorrhage are :
– GIT
– Nose
– Cord
– Intracranial
– Circumcision
– Trauma

HDN• Early HDN
- Occurs < 24 hours of age. Here, you should exclude other possible causes
•
• Late HDN
• Occurs > 1 week
•
• Predisposing Factors to Early or Late HDN
• Birth Asphyxia
• Maternal drug ingestion e.g. phenobarbitone, aspirin, anticoagulant (Coumadin) – leading to vitamin K deficiency in the mother
• Exclusive breastfeeding – since breast milk is not rich in vitamin K
• Broad spectrum antibiotics – reduce the normal flora in the gut
• Total parenteral nutrition – delays the acquire of normal gut flora through oral feeding.

HDN Con’t
Clinical Presentation
• Bleeding – provoked or
unprovoked
• On examination, patient
may look well in the
absence of any other
comorbidity.
•
Investigation
• Packed cell volume
• FBC - normal
• Platelet count – normal
• Prothrombin time -
prolonged
• PTTK – prolonged
• Fibrinogen – normal
• FDP – normal

Treatment of HDN
Non-severe
– Give Intravenous Vitamin K1, 1 – 5mg stat. ( K2 & K3 are
not used if patient is G6PD deficient because they cause
haemolysis.
Severe & Life non-threatening
• Intravenous Vitamin K stat
• Double volume EBT with fresh whole blood - to remove
inactivated clotting factors, called Protein-induced Vitamin K
factors with vitamin K replenishment.
Note
• Single volume EBT – 65%
• Double volume EBT – 83 -85%. It is often used for it maximal
effect.

Prevention
• Rotine intramuscular vitamin K1, 1 mg stat, to every newborn baby. For preterm, the dose is 0.5mg stat.
• For special babies (with any of the conditions listed above e.g total parenteral nutrition), you continue to give 0.5mg / week until the baby starts feeding.

DISSEMINATED INTRAVASCULAR
COAGULOPATHY (DIC)Predisposing Factors
These are causes of generalised vascular damage
• Severe birth asphyxia
• Septicaemia
• Hypothermia
• Hypotension
• Acidosis
• Hypoxia
Pathogenesis
• Due to consumption of clotting factors

DICClinical Presentation
• Provoked bleeding - from puncture sites
• Unprovoked bleeding e.g petechiae, spontaneous massive bleeding form orifices.
• Investigation
As in the bleeding disorders
• Treatment
• Treat the underlying cause
• Specific treatment
• Give Platelet concentrate /Platelet rich plasma + transfusion with fresh frozen plasma using 10 – 15ml/kg
• Give Vitamin K1 intravenously
• If severe do EBT with fresh whole blood – to remove the toxins & FDP which causes haemorrhage

Disease
Clinica
l state
Platele
t
PT PTTK Other tests ( to
confirm)
1. Haemorrhagic
disease of the
newborn
Well Normal ↑ ↑ Fibrinogen/FDP – Normal, because there is no excessive breakdown of clots
2. Idiopathic
thrombocytopaenic
purpura (ITP
Well ↓ Normal Normal Maternal platelet
count – decrease confirms it
3. Large Haemangioma Well ↓ Normal Normal Maternal platelet
count – normal
4. Bone Marrow
Hypoplasia Well ↓ Normal Normal Peripheral blood film –
shows pancytopaenia
5. Haemophilia Well Normal Normal ↑ Factors 8 & 9 Assay 6. Liver disease Sick Normal ↑ ↑ Albumin, Fibrinogen &
LFTs are deranged
7. Intrauterine TORCH
Infection Sick ↓ (may
be) N or ↑ N or ↑ Fibrinogen, Albumin
8. Infections Without
DIC e.g Septicaemia
Sick ↓ Normal Normal FBC, Blood culture
9. Infections + DIC (or in any cause of DIC )
Sick ↓ ↑ ↑ Fibrinogen - ↓
FDP - ↑
PBF – fragmented rbc due
to trapping

a-thalassemia
a-globin Cluster

Hydrops Fetalis Syndrome
– Most Hb- Hb Barts, unable to deliver O2 to tissues
– Tissue hypoxia & anemia
– Massively enlarged placenta
– Heart failure, edema anasarca interferes with organogenesis, congenital malformations
– Extramedullayerythropoiesis

• Thank You