-
8/3/2019 Nephritic Syndrome
1/24
Nephritic SyndromeDr. Muhamed Al Rohani, MD
-
8/3/2019 Nephritic Syndrome
2/24
-
8/3/2019 Nephritic Syndrome
3/24
-
8/3/2019 Nephritic Syndrome
4/24
-
8/3/2019 Nephritic Syndrome
5/24
-
8/3/2019 Nephritic Syndrome
6/24
Nephrotic Syndrome Proteinuria (>3.0 g/day)
Hypoalbuminemia (
-
8/3/2019 Nephritic Syndrome
7/24
Humoral Antibody-Mediated InjuryThe major mechanisms of antibody
deposition within the glomerulus are:
1. Immune complexes of circulating antibodies with extrinsic
antigens that have beentrapped, or planted, within the glomerulus,
as occurs in postinfectious
glomerulonephritis;
2. Reactivity of circulating autoantibodies with intrinsic
autoantigens that are
components of normal glomerular parenchyma, as occurs in
anti-GBM disease
(Goodpastures syndrome)
3. Intraglomerular trapping of immune complexes that have formed
in the systemic
circulation:
1. Cryoglobulinemia-associated glomerulonephritis.
2. Circulating autoantibodies against neutrophil cytoplasmic
antigens (antineutrophil
cytoplasmic antibodies, ANCA)
3. Endothelial antigens (antiendothelial cell antibodies,
AECA).
-
8/3/2019 Nephritic Syndrome
8/24
Factors affecting the pathogenesis of glomerular disease:
1. The capacity of the reticuloendothelial system to clear
immune complexes
from the circulation,
2. The capacity of the glomerulus itself to remove deposited
complexes. this is
thought to be a function of the glomerular mesangium.
Small complexes, formed in antigen excess, localize on the
capillary basement
membrane.
Larger complexes tend to localize in the mesangium and cause
much less
glomerular injury.
-
8/3/2019 Nephritic Syndrome
9/24
Cellular Antibody-Independent Glomerular Injury
The cell-mediated injury is less well defined than antibody
mediated glomerular injury.
T cells have also been implicated as independent mediators of
glomerular injury and as modulators of theproduction of
nephritogenic antibodies.
T cells interact, through their cell-surface T cell receptor/CD3
complex, with antigens presented in theglomerular endothelial,
mesangial, and epithelial cells, a process that is facilitated by
cell-cell adhesionand costimulatory molecules. activated T cells
produce cytokines and other mediators which are potentstimuli for
further leukocyte recruitment, cytotoxicity, and fibrogenesis.
Cell Proliferation and Accumulation of Extracellular Matrix:
Initially, this hypercellularity is due predominantly to
infiltration of the glomerular tuft by leukocytes.Subsequently,
resident glomerular cells proliferate in response to growth factors
released into the local
inflammatory milieu. The proliferating cells are typically
mesangial in mesangioproliferativeglomerulonephritis and both
endothelial and mesangial cells in diffuse proliferative
glomerulonephritis.
Factors affecting the pathogenesis of glomerular disease:
1. The capacity of the reticuloendothelial system to clear
immune complexes from the circulation,
2. The capacity of the glomerulus itself to remove deposited
complexes. this is thought to be a function ofthe glomerular
mesangium.
Small complexes, formed in antigen excess, localize on the
capillary basement membrane.
Larger complexes tend to localize in the mesangium and cause
much less glomerular injury.
-
8/3/2019 Nephritic Syndrome
10/24
-
8/3/2019 Nephritic Syndrome
11/24
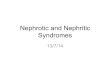
Glomerular Diseases by Age and Presentation
Age (yr) Nephritic Syndrome Nephrotic Syndrome Mixed Nephritic
and Nephrotic
Syndrome
< 15 Mild PIGN
IgA nephropathy
Thin basement membrane disease
Hereditary nephritis
Henoch-Schnlein purpuraLupus nephritis
Minimal change disease
Focal and segmental glomerulosclerosis
Lupus (membranous nephropathy)
Lupus nephritis
Membranoproliferative GN
1540 IgA nephropathy
Thin basement membrane disease
Lupus nephritis
Hereditary nephritis
Mesangial proliferative GN
RPGN
PIGN
Focal and segmental glomerulosclerosis
Minimal change disease
Membranous nephropathy
Diabetic nephropathy
Preeclampsia
Late PIGN
IgA nephropathy
Membranoproliferative GN
Fibrillary and immunotactoid GN*
IgA nephropathy
> 40 IgA nephropathy
RPGN
Vasculitides
PIGN
Focal and segmental glomerulosclerosis
Membranous nephropathy
Diabetic nephropathy
Minimal change disease
IgA nephropathy
Amyloidosis (primary)
Light chain deposition diseaseBenign nephrosclerosis
Late PIGN
IgA nephropathy
Fibrillary and immunotactoid GN*
*More commonly manifests as nephrotic syndrome.
PIGN = postinfectious glomerulonephritis; GN =
glomerulonephritis, RPGN = rapidly progressive
glomerulonephritis
Adapted from Rose BD. Pathophysiology of Renal Disease (2nd
edition). New York: McGraw-Hill, 1987, p. 167.
-
8/3/2019 Nephritic Syndrome
12/24
Alport's Syndrome:Hereditary nephritis is a genetically
heterogenous disorder characterized by hematuria, impaired
renal
function, sensorineural deafness, and ocular abnormalities.
Cause is a gene mutation affecting type IV
collagen. Symptoms and signs are those of nephritic syndrome
with sensorineural deafness and, less
commonly, those of ophthalmologic diseases. Diagnosis is by
family history and urinalysis. Treatment is
that of chronic renal failure.
Immunoglobulin A Nephropathy:
IgA nephropathy is deposition of IgA immune complexes in
glomeruli, manifesting as slowly
progressive hematuria, proteinuria, and, often, renal
insufficiency. Diagnosis is based on
urinalysis and renal biopsy. Prognosis is generally good.
Treatment options include ACE inhibitors,
corticosteroids, and -3 polyunsaturated fatty acids.
Rapidly Progressive Glomerulonephritis (RPGN)
(Crescentic Glomerulonephritis)Rapidly progressive GN causes
microscopic glomerular crescent formation with progression to
renal
failure within weeks to months. Diagnosis is based on history,
urinalysis, serologic tests, and renal
biopsy. Treatment is with corticosteroids, with or without
cyclophosphamide, and sometimes
plasmapheresis.
-
8/3/2019 Nephritic Syndrome
13/24
Definition:
Acute Post Sterptococcal Glomerulonephritis is characterized by
the sudden appearanceof hematuria, proteinuria and red blood cell
casts in the urine, edema, andhypertension with or without
oliguria.
History:
This illness was first recognized as a complication of the
convalescence period ofscarlet fever in the 18th century. A link
between hemolytic streptococci and acute
glomerulonephritis was recognized in the 20th century.
Acute Post Sterptococcal Glomerulonephritis
Causes:
Poststreptococcal glomerulonephritis follows infection with only
certain strains ofstreptococci designated as nephritogenic.
The offending organisms are virtually always group A
streptococci. APSGN follows pyodermatitis with streptococci M types
47, 49, 55, 2, 60, and 57 and
throat infection with streptococci M types 1, 2, 4, 3, 25, 49,
and 12.
-
8/3/2019 Nephritic Syndrome
14/24
Epidemiology:
Internationally: APSGN can occur sporadically or epidemically.
Epidemic poststreptococcal glomerulonephritis occurs mainly in
developing countries in areas
such as Africa, the West Indies, and the Middle East. Reasons
for this changing epidemiologyrelate to the nutritional status of
the community, the more liberal use of antibiotic prophylaxis,and,
possibly, the change in the nephritogenic potential of
streptococci. Among epidemic
infections with nephritogenic streptococci, the apparent
clinical attack rate is 10-12%. Mortality/Morbidity:
Early death is extremely rare in children (
-
8/3/2019 Nephritic Syndrome
15/24
Pathology :
Light microscopy The most striking finding is hypercellularity
of the glomeruli. All glomeruli are affected
(diffuse) and usually to an approximately equal degree. The
glomerular tufts are larger thannormal, and the cells are more
numerous.
The cell types typically present include endothelial and
mesangial cells and migrantinflammatory cells, which include
polymorphonuclear leukocytes and monocytes.
Polymorphonuclear leukocytes are present in large numbers, hence
the term exudativeglomerulonephritis.
The tubules are normal in the majority of cases.
The degree of interstitial involvement is variable. The
interstitial areas show edema andinfiltration with
polymorphonuclear leukocytes and mononuclear cells. The arteries
andarterioles are normal.
-
8/3/2019 Nephritic Syndrome
16/24
Immunofluorescence In biopsy samples taken in the first 2-3
weeks of illness, deposits of
immunoglobulin G and C3 in a diffuse granular pattern are
present along the
glomerular capillary wall and mesangium. Immunoglobulin M may be
present in small amounts. Significant amounts of
IgA suggest an alternative diagnosis.
3 different patterns of immunofluorescence called the garland
pattern, the
starry sky pattern, and the mesangial pattern.
-
8/3/2019 Nephritic Syndrome
17/24
Electron microscopy Many of the ultrastructural changes confirm
the findings from light microscopy
evaluations.
The number of endothelial, mesangial, and infiltrating
inflammatory cells isincreased.
The glomerular basement membrane is usually normal in thickness
and
contour, although occasionally patchy thickening may be
noted.
Presence of glomerular subepithelial electron-dense immune-type
deposits. The
deposits are discrete and are commonly found on the part of the
glomerularbasement membrane overlying the mesangium
-
8/3/2019 Nephritic Syndrome
18/24
CLINICAL FINDINGS
History: A history suggestive of preceding streptococcal
infection may
include a preceding infective episode such as pharyngitis,
tonsillitis, orpyoderma.
Latent period: In general, the latent period is 1-2 weeks after
a throat infection and 3-6 weeks
after a skin infection.
The onset of signs and symptoms at the same time as pharyngitis
(also calledsynpharyngitic nephritis) is more likely to be
immunoglobulin A (IgA)nephropathy rather than APSGN.
Dark urine (brown-, tea-, or cola-colored) This is often the
first clinical symptom.
Dark urine is caused by hemolysis of red blood cells that have
penetrated theglomerular basement membrane and have passed into the
tubular system.
Nonspecific symptoms These can include general malaise,
weakness, and anorexia and are present in
50% of patients.
Approximately 15% of patients complain of nausea and
vomiting.
-
8/3/2019 Nephritic Syndrome
19/24
Physical:
Acute nephritic syndrome Acute nephritic syndrome presenting as
edema, hematuria, and hypertension with or without oliguria
is the most frequent presentation of APSGN.
Approximately 95% of clinical cases have at least 2
manifestations, and 40% have the full-blownacute nephritic
syndrome.
Edema and Periorbital edema Edema is present in 80-90% of cases,
and it is the presenting complaint in 60% of cases.
The onset of puffiness of the face or eyelids is sudden. It is
usually prominent upon awakening and, ifthe patient is active,
tends to subside at the end of the day.
In some cases, generalized edema and other features of
circulatory congestion, such as dyspnea, maybe present.
Edema is a result of a defect in renal excretion of salt and
water.
The severity of edema is often disproportionate to the degree of
renal impairment.
Hypertension Hypertension occurs in 60-80% of cases and is more
common among elderly individuals.
In 50% of cases, the hypertension can be severe; however, more
often it is transient, withnormalization of BP upon therapy
If hypertension persists, it is more indicative of the
progression to a more chronic stage.
Plasma renin activity is usually low due to fluid overload.
Left ventricular dysfunction
Oliguria and anuria This is present in 10-50% of cases, and, in
15%, urine output is less than 200 mL. Oliguria is indicative of
the severe crescentic form of the disease.
It is often transient, with diuresis occurring within 1-2
weeks.
Hematuria This is present universally.
In 30% of cases, gross hematuria is present.
-
8/3/2019 Nephritic Syndrome
20/24
Complications:
Complications in the acute phase include the following:
Congestive heart failure
Azotemia
Early death secondary to congestive heart failure and
azotemia
Complications in the chronic phase include the following:
Nephrotic-range proteinuria
Chronic renal insufficiency and end-stage renal disease
Prognosis:
In children, the immediate prognosis is excellent.
In elderly patients who have congestive heart failure or
azotemia in the early phase, earlymortality rates can be as high as
25%.
The long-term prognosis is debatable. Fewer than 1% of children
have elevated serum creatinine values after 10-15 years of
follow-
up.
Adults who develop massive proteinuria often have the
garlandlike pattern of immunedeposits. Their prognosis is worse;
approximately 25% progress to chronic renal failure.
-
8/3/2019 Nephritic Syndrome
21/24
Lab Studies:
Evidence of preceding streptococcal infection
Antibody titers to extracellular products of streptococci are
positive in more than 95% of patients with pharyngitisand 80% of
patients with skin infections.
The antistreptolysin (ASO), antinicotinamide adenine
dinucleotidase (anti-NAD), antihyaluronidase (AHase), and
antiDNAse B are commonly positive after pharyngitis, and
antiDNAse B and AHase titers are more oftenpositive following skin
infections.
ASO titers are frequently used to document streptococcal
infection, but a more sensitive test is the streptozymetest, which
tests antibodies to ASO, antiDNAse B, AHase, and anti-NAD.
Antizymogen titers that are 2 dilutions higher than the mean in
healthy controls are reported to have a sensitivity of88% and a
specificity of 85% in the diagnosis of streptococcal infection in
patients with glomerulonephritis.
The antibody titers are elevated at 1 week, peak at 1 month, and
fall toward preinfection levels after severalmonths.
Elevated BUN and creatinine could be elevated transient
Serologic findings Low serum complement levels universal finding
in the acute phase of APSGN.
Most patients have marked depression of serum hemolytic
component CH50 and serum concentrations of C3.
In some patients, the levels of C2 and C4 may also be
decreased.
In most uncomplicated cases, the complement levels return to
normal in 6-8 weeks.
Occasionally, low complement levels persist for 3 months.
Urinalysis
Hematuria and proteinuria are present in all cases. Urine
sediment has red blood cells and casts, white blood cells, granular
casts, and, rarely, white blood cell casts.
Hematuria usually resolves within 3-6 months but may persist as
long as 18 months.
Approximately 5-10% of patients with APSGN have nephrotic-range
proteinuria.
Proteinuria usually disappears in 6 months. A mild increase in
urinary protein excretion is present in 15% at 3years and 2% at 10
years.
-
8/3/2019 Nephritic Syndrome
22/24
Imaging Studies:
CXR and KUB are normal.
Renal ultrasound images usually reveal normal-sized kidneys
bilaterally.
Atypical features in the early phase that suggest the need for
renal biopsy include thefollowing:
Absence of the latent period between streptococcal infection and
acute glomerulonephritis
Anuria
Rapidly deteriorating renal function
Normal serum complement levels
No rise in antistreptococcal antibodies
Extrarenal manifestations of systemic disease
No improvement or continued decrease in the glomerular
filtration rate at 2 weeks
Persistence of hypertension beyond 2 weeks
Atypical features in the recovery phase that mandate a renal
biopsy include thefollowing:
Failure of glomerular filtration rate to normalize by 4
weeks
Persistent hypocomplementemia beyond 6 weeks Persistent
microscopic hematuria beyond 18 months
Persistent proteinuria beyond 6 months
-
8/3/2019 Nephritic Syndrome
23/24
Management:Symptomatic therapy:
During the acute phase of the disease, restrict salt and water
(Low-salt diet2g/d) Restricting physical activityis appropriate in
the first few days.
Hypertension; If significant edema or hypertension develops,
administer diuretics. Loop diuretics increase urinary output and
consequently improve cardiovascular congestion and
hypertension.
ACEi or CCB. For malignant hypertension, intravenous
nitroprusside.
Dialysis; is indicated if life-threatening hyperkalemia and
clinical manifestations of uremia.
Medications Steroids, immunosuppressive agents, and
plasmapheresis are not generally indicated.
A renal biopsy is indicated for patients with rapidly
progressive renal failure. If the biopsy findings showevidence of
crescentic glomerulonephritis with more than 30% of the glomeruli
involved, a short course ofintravenous pulse steroid therapy is
recommended (500 mg to 1 g/1.73 m2 of methylprednisone qd for
3-5d). However, no controlled clinical trials have evaluated such
therapy.
Specific therapy for streptococcal infection is an important
part of the therapeutic regimen.
Treat patients, family members, and any close personal contacts
who are infected.
Throat cultures should be performed on all these individuals.
Treat with oral penicillin G (250 mg qidfor 7-10 d) or with
erythromycin (250 mg qid for 7-10 d) for patients allergic to
penicillin.
This helps prevent nephritis in carriers and helps prevent the
spread of nephritogenic strains to others.
Patients with skin infections must practice good personal
hygiene. This is essential.
During epidemics, recommend that high-risk individuals,
including close contacts and familymembers, receive empirical
prophylactic treatment.
Surgical Care: Surgical care is not indicated.
-
8/3/2019 Nephritic Syndrome
24/24
A 21 year-old woman presents with tea-colored urine,three weeks
after being evaluated for
a sore throat. Physical examination is notable for a blood
pressure of 170/100 and 3+ pitting
edema. Serum creatinine is 2.1 mg/dl. Urine dipstick
demonstrates 2+ protein, large heme
and large leukocyte esterase.