Embed Size (px)
DESCRIPTION
A pdf slideshow which introduces the nephrotic and nephritic syndromes, explains how to remember their presentations, and explains why they present this way. The syndromes are compared and contrasted throughout.
Citation preview

Nephrotic and Nephritic Syndromes
13/7/14

What are they, and why do we care?
• The nephrotic and nephritic syndromes are distinct clusters of symptoms caused by various glomerular diseases.
• For each syndrome, there is a set of possible underlying causes.
• So while the syndromes are not diagnoses, identifying whether your patient is nephrotic or nephritic can narrow down the DDx.
• The syndromes may overlap, and some diseases can cause either.

Silly picture
nephrotic nephritic
glomerular disease:
presentation:
D E F A B C
DDx: A B C D C D E F

Nephritic syndrome
• “-itic” like “-itis” means inflammation, so think of a glomerulus damaged by inflammation.
• Such a glomerulus will be leaking inappropriately, i.e.: 1. Leaking things it shouldn’t be (blood) 2. Not leaking things it should be (↓GFR).
• ↓GFR leads to too much fluid on one side (hypertension) and less than normal on the other side (oliguria).

Pathogenesis of nephritic syndrome underlying cause
glomerular damage with inflammation
(↓GFR but glomerulus becomes very leaky to
other things)

Pathogenesis of nephritic syndrome underlying cause
glomerular damage with inflammation
(↓GFR but glomerulus becomes very leaky to
other things) hematuria with RBC casts
?minor proteinuria
↓GFR

Pathogenesis of nephritic syndrome underlying cause
glomerular damage with inflammation
(↓GFR but glomerulus becomes very leaky to
other things) hematuria with RBC casts
?minor proteinuria
↓GFR
oliguria ↑plasma creatinine and urea (“uremia”)

Pathogenesis of nephritic syndrome underlying cause
glomerular damage with inflammation
(↓GFR but glomerulus becomes very leaky to
other things) hematuria with RBC casts
?minor proteinuria
↓GFR Na+ retention severe ↓GFR activates RAAS system, as it should
oliguria ↑plasma creatinine and urea (“uremia”)

Pathogenesis of nephritic syndrome underlying cause
glomerular damage with inflammation
(↓GFR but glomerulus becomes very leaky to
other things) hematuria with RBC casts
?minor proteinuria
↓GFR Na+ retention severe ↓GFR activates RAAS system, as it should
Na+ retention occurs even if GFR is not significantly reduced. Appears to be due to upregulation of basolateral Na+/K+ ATPase in late DT, but the mechanism by which glomerular damage causes this is unknown.
oliguria ↑plasma creatinine and urea (“uremia”)

Pathogenesis of nephritic syndrome underlying cause
glomerular damage with inflammation
(↓GFR but glomerulus becomes very leaky to
other things) hematuria with RBC casts
?minor proteinuria
↓GFR Na+ retention
water retention
↑plasma volume oliguria ↑plasma creatinine
and urea (“uremia”)
severe ↓GFR activates RAAS system, as it should
Na+ retention occurs even if GFR is not significantly reduced. Appears to be due to upregulation of basolateral Na+/K+ ATPase in late DT, but the mechanism by which glomerular damage causes this is unknown.

Pathogenesis of nephritic syndrome underlying cause
glomerular damage with inflammation
(↓GFR but glomerulus becomes very leaky to
other things) hematuria with RBC casts
?minor proteinuria
↓GFR Na+ retention
water retention
↑plasma volume
hypertension ?edema
↑JVP, cardiomegaly
oliguria ↑plasma creatinine and urea (“uremia”)
severe ↓GFR activates RAAS system, as it should
Na+ retention occurs even if GFR is not significantly reduced. Appears to be due to upregulation of basolateral Na+/K+ ATPase in late DT, but the mechanism by which glomerular damage causes this is unknown.

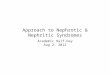
Pathogenesis of nephritic syndrome underlying cause
glomerular damage with inflammation
(↓GFR but glomerulus becomes very leaky to
other things) hematuria with RBC casts
?minor proteinuria
↓GFR Na+ retention
water retention
↑plasma volume
hypertension ?edema
↑JVP, cardiomegaly
oliguria ↑plasma creatinine and urea (“uremia”)
severe ↓GFR activates RAAS system, as it should
Na+ retention occurs even if GFR is not significantly reduced. Appears to be due to upregulation of basolateral Na+/K+ ATPase in late DT, but the mechanism by which glomerular damage causes this is unknown.

Nephritic syndrome summary
• Defining symptoms: – Hematuria – Hypertension – Oliguria.
• A quick way to remember: – “H2O”.

Nephrotic syndrome
• The glomerulus is damaged but not inflamed, so it leaks things it shouldn’t, but otherwise filters normally.
• The damage is more subtle than nephritic, so proteins can leak, but not usually blood.
• Symptoms are all consequences of this protein loss.

Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration

Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration
proteinuria
hypoalbuminemia
?anemia (loss of transferrin)

Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration
proteinuria
Na+ retention hypoalbuminemia
?anemia (loss of transferrin)
Filtered proteases cleave inactive
ENaC in late DT

Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration
proteinuria
Na+ retention
Glomerular damage may cause Na+ retention by additional mechanisms, but this is poorly understood.
hypoalbuminemia
?anemia (loss of transferrin)
Filtered proteases cleave inactive
ENaC in late DT

Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration
proteinuria
Na+ retention
water retention
↑plasma volume
Glomerular damage may cause Na+ retention by additional mechanisms, but this is poorly understood.
hypoalbuminemia
?anemia (loss of transferrin)
Filtered proteases cleave inactive
ENaC in late DT

Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration
proteinuria
Na+ retention
water retention
↑plasma volume
edema
↓plasma oncotic pressure
Glomerular damage may cause Na+ retention by additional mechanisms, but this is poorly understood.
hypoalbuminemia
?anemia (loss of transferrin)
Filtered proteases cleave inactive
ENaC in late DT

Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration
proteinuria
Na+ retention
water retention
↑plasma volume
edema
↓plasma oncotic pressure
Glomerular damage may cause Na+ retention by additional mechanisms, but this is poorly understood.
hypoalbuminemia
?anemia (loss of transferrin)
Filtered proteases cleave inactive
ENaC in late DT
In the setting of ↓plasma oncotic pressure, extra fluid moves straight into interstitium, so BP is rarely/barely raised.

Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration
proteinuria
Na+ retention
water retention
↑plasma volume
edema
↓plasma oncotic pressure
Liver makes more proteins (not just
albumin)
Glomerular damage may cause Na+ retention by additional mechanisms, but this is poorly understood.
hypoalbuminemia
?anemia (loss of transferrin)
↑plasma LDL (“hyperlipidemia”)
Filtered proteases cleave inactive
ENaC in late DT
In the setting of ↓plasma oncotic pressure, extra fluid moves straight into interstitium, so BP is rarely/barely raised.

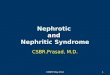
Pathogenesis of nephrotic syndrome underlying cause
glomerular damage without inflammation
(preserves GFR but makes glomerulus leaky to protein) ↑protein filtration
proteinuria
Na+ retention
water retention
↑plasma volume
edema
↓plasma oncotic pressure
Liver makes more proteins (not just
albumin)
Glomerular damage may cause Na+ retention by additional mechanisms, but this is poorly understood.
hypoalbuminemia
?anemia (loss of transferrin)
↑plasma LDL (“hyperlipidemia”)
Filtered proteases cleave inactive
ENaC in late DT
In the setting of ↓plasma oncotic pressure, extra fluid moves straight into interstitium, so BP is rarely/barely raised.

Summary of nephrotic syndrome
• Defining symptoms: – Hypoalbuminemia – Edema – ↑Lipids – Proteinuria ≥3.5g/day (equivalently, protein/
creatinine ratio ≥350mg/mmol) • A quick way to remember:
– “HELP”

Summary and comparison
Nephritic • Inflammatory causes • Hematuria • Hypertension • Oliguria • +Maybe edema and mild
proteinuria
Nephrotic • Non-inflammatory causes
• Hypoalbuminemia • Edema • ↑Lipids • Proteinuria

Potential confusing things
Nephritic • Glomerulus is damaged enough to
let big RBCs through, so you’d think proteins would easily pass through. However proteinuria is not usually seen, and if it is present, it’s mild.
Nephrotic • In nephritic, Na+ and water
retention lead to hypertension. But in nephrotic, which also involves these processes, the BP is usually normal. (This is because the low plasma oncotic pressure allows the extra fluid to go straight into the interstitium, so it doesn’t hang around long enough to raise BP).

In the next episode…
• Explore some of the different types of glomerulonephritis (GN).
• For each type of GN, learn whether it typically presents as nephrotic or nephritic syndrome, and why.