-
7/30/2019 Neuro Anaphy
1/27
B. PATHOPHYSIOLOGY
1.) Anatomy and Physiology
FUNDAMENTALS OF NERVOUS SYSTEM CONDUCTION
Within the brain and nervous system are specialized cells, known
as neurons. The
neurons are responsible for delivering chemical messages to
other cells to achieve some
response. This is the basis of how our nervous system works.
Within the brain, there are
approximately 100 billion neurons. Neurons are typically
classified by the direction that they
send information. Sensory, or afferent, neurons send impulses
from sensory receptors in the
periphery or some organ to the central nervous system. Motor, or
efferent, neurons send impulses
away from the central nervous system to muscles or glands.
Neurons have specialized extensions called dendrites and axons.
Dendrites bring
information to the cell body (soma) and axons take information
away from the cell body. Some
neuronal axons are myelinated (have a fatty substance coating
them that speeds impulse
transmission) and some are not. Nodes of Ranvier are short
unmyelinated segments of an axon.
-
7/30/2019 Neuro Anaphy
2/27
Neurotransmitters then cross the synapse where they may be
accepted by the next
neurons receptor site. The action that follows activation of a
receptor site may be either
depolarization (excitatory in nature) or hyperpolarization
(inhibitory in nature). If the neuron is
depolarized, its response is excitatory. If the neuron is
hyperpolarized, the response is inhibitory.
There are three major categories of substances that act as
neurotransmitters. They are
amino acids, peptides, and monoamines, plus acetylcholine. The
major neurotransmitters of the
brain are glutamic acid and GABA. The peripheral nervous system
has only two
neurotransmitters. They are acetylcholine and norepinephrine.
Neurotransmitters vary greatly in
the response they enact upon particular cells or receptor sites.
Acetylcholine, for example, can be
excitatory or inhibitory depending upon which receptor site it
binds to. The following is a list of
several known and well-studied neurotransmitters.
Neurotransmitter Function
Acetylcholine Mostly excitatory
Dopamine Excitatory and inhibitory
Epinephrine Excitatory
Norepinephrine Excitatory
Serotonin Excitatory
Glutamate Excitatory
Glycine Mostly inhibitory
g-Aminobutiric acid (GABA) Inhibitory
-
7/30/2019 Neuro Anaphy
3/27
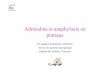
The meninges cover the brain and spinal cord and protect them as
well. There are three
meningeal layers. They are the dura mater, arachnoid mater, and
pia mater.
Courtesy of the National Cancer Institute,2004www.nci.gov
Dura Mater
The dura mater is the outer, tough layer of the meninges. It
lines the inside of the skull.
The dura mater also separates specific portions of the brain.
The falx cerebri is a portion of the
dura mater that separates the right and left hemispheres of the
brain. The tentorium cerebelli is a
portion of the dura mater that separates the cerebrum from the
cerebellum (AACN, 1998).
Arachnoid Mater
The arachnoid mater is the middle layer of meninges.It is a
web-like structure that allows the passage of blood vessels and
through it. Between the
arachnoid mater and the pia mater, is the subarachnoid space.
Cerebral spinal fluid (CSF) flows
http://www.nci.gov/http://www.nci.gov/
-
7/30/2019 Neuro Anaphy
4/27
subarachnoid space, as discussed earlier is the space below the
arachnoid, between the arachnoid
and the pia mater (AACN, 1998).
THE BRAIN
The brain in an adult is one of the bodys largest organs. It
weighs about three pounds
and is divided into four major parts: the cerebrum,
diencephalon, brain stem, and cerebellum
(Tortora, 1989).
Cerebrum
The cerebrum is the largest portion of the brain. It covers the
diencephalon. The surface
of the cerebrum is composed of gray matter and is known as the
cerebral cortex. During
embryonic development the gray matter grows in increased
proportion to the underlying white
matter. This increased growth rate causes the gray matter to
fold into itself and create
convolutions known as gyri.
The deep grooves between the folds are known as fissures. The
shallow grooves between
the fold are known as sulci. The most noticeable fissure is the
one that nearly separates the right
and left hemispheres of the brain the longitudinal fissure. The
hemispheres remain connected
by the corpus collosum, a transverse bundle of nerve fibers.
Additionally, between the
hemispheres is an extension of the dura mater known as the falx
cerebri.
Each cerebral hemisphere is subdivided into lobes. The central
sulcus separates the
frontal from the parietal lobe The frontal and the temporal
lobes are separated by the lateral
-
7/30/2019 Neuro Anaphy
5/27
The precentral gyrus, is located immediately anterior to the
central sulcus and is the
major motor area of the brain. The post central gyrus is located
immediately posterior to the
central sulcus and is the major motor area of the brain.
White Matter -The white matter that is underneath the cerebral
cortex and consists of
three different types of nerve fibers. Association fibers
transmit impulses between gyri in
the same hemisphere. Commisural fibers transmit nerve impulses
from gyri on one
hemisphere with the corresponding gyri in the opposite
hemisphere. Finally, protection
fibers transport nerve impulses from parts of the cerebrum to
other parts of the brain and
spinal cord (Tortora, 1989).
Limbic System - The limbic (border) system is composed of
certain components of the
cerebrum and the diencephalons. The components of this system
are the limbic lobe, the
hippocampus, amygdaloid nucleus, the mamillary bodies of the
hypothalamus, and the
anterior nucleus of the thalamus. Basically, the limbic system
encircles the brainstem and
functions in the emotional aspects of behavior that are
essential to our survival. It also
plays a role in memory, although the exact mechanism is not
understood fully. The limbic
system is also thought to play some part in how we sense
pleasure, pain, anger, rage, fear,
sadness and sexual feelings. Because of its role in these core
emotions, it is also known as
the visceral or emotional brain (Tortora, 1989).
-
7/30/2019 Neuro Anaphy
6/27
Parietal Lobe - The parietal lobe is located behind the central
sulcus. It is concerned with
perception of stimuli related to touch, pressure, temperature,
and pain. The parietal lobescan be divided into two functional
regions, involving sensation and perception. The
overall role of the parietal lobe is to integrate sensory
information to form a single
perception (cognition) (Kandel, Schwartz and Jessel, 1991).
Temporal Lobe - The temporal lobe is located below the lateral
fissure. It is concerned
with sensory perception and recognition of auditory stimuli
(hearing) and memory
(hippocampus) (Read, 1981; Tortora, 1989). Individuals with
temporal lobes lesions have
difficulty placing words or pictures into categories. The
temporal lobes are highly
associated with memory skills and language. Temporal lobe damage
may result in
impaired memory, difficulty recognizing words or speaking, and
recall of non-verbal
stimuli such as music or drawings (Tortora, 1989).
Occipital Lobe - The occipital lobe is located at the back of
the brain, behind the parietal
lobe and temporal lobe. It is concerned with many aspects of
vision. Lesions or damage
to the occipital lobe typically results in visual changes, even
producing visual
hallucinations.
-
7/30/2019 Neuro Anaphy
7/27
system. The hypothalamus is also known as the master gland of
the endocrine system,
for this reason. It produces and releases hormones that
stimulate the pituitary gland. This
connection or relationship with the pituitary gland is referred
to as the hypothalamic-
pituitary axis. The three major hormones that stimulate the
hypothalamus are growth
hormone releasing hormone (GRH), thyrotropic releasing hormone
(TRH), and
corticotropin releasing hormone (CRH) (AACN, 1998). These
hormones travel to the
pituitary via the hypothalamic pituitary stalk. Once in the
pituitary, they act to produce or
release other hormones from the pituitary gland. The
hypothalamus is also responsible for
the mind over body phenomenon. When strong emotions are produced
by the cerebral
cortex, nerve impulses travel down through the hypothalamus to
the body. Likewise,
continued psychological stress traveling upward through the
hypothalamus may produce
long-term, very, real, systemic illnesses. The hypothalamus also
plays a role in feelings
such as rage and aggression and regulates body temperature,
hunger, thirst, sleep and
wake cycles.
Brain Stem
The brain stem consists of the medulla oblongata, pons, and
mid-brain, or
mesencephalon.
-
7/30/2019 Neuro Anaphy
8/27
Pons - Pons means bridge. The pons is the bridge that connects
the spinal cord with the
brain and certain parts of the brain with each other. These
connections occur via fibersthat run in two major directions. The
transverse fibers connect with the cerebellum. The
longitudinal fibers connect the spinal cord or medulla with the
upper parts of the brain
stem.
Mid-Brain - The mid-brain, or mesencephalon, extends from the
pons to the lower
portion of the diencephalons. The cerebral aqueducts travels
through the mid-brain and
connects the third and fourth ventricles. Within the midbrain,
there are nerve fibers that
convey nerve impulses from the cerebral cortex to the pons and
spinal cord. The mid-
brain also has some reflex centers that control eye, head, and
neck movements. The mid-
brain is also the origin of cranial nerves II and IV (Tortora,
1989).
The Reticular Activating System - The reticular activating
system is so named because it
resembles the reticular system of a leaf. It is a network of
neurons located in the central
core of the brainstem that serves to monitor the state of the
body in functions such as
arousal, sleep, and muscle tone. The reticular activating system
is the attention center in
the brain. The reticular activating system is connected at its
base to the spinal cord where
it receives information projected directly from the ascending
sensory tracts. The brain
stem reticular formation runs all the way up to the midbrain. As
a result, the reticular
activating system serves as a point of union for signals from
the outside world to our
-
7/30/2019 Neuro Anaphy
9/27
Cerebrospinal Fluid
The cerebral spinal fluid, or CSF, protects and cushions the
brain from injury. The CSF
acts as a shock absorber from injuries that would normally send
the brain crashing up against the
inside of the skull. By nature of its circulatory abilities, it
also delivers nutrients filtered from the
blood to the brain and spinal cord and removes wastes and toxic
substances produced by the
brain and spinal cord (Tortora, 1989).
It circulates in the subarachnoid space, around the brain, the
spinal cord and the ventricles
of the brain. The ventricles, like the hearts ventricles are
spaces. In the brain, there are two
lateral ventricles located in each hemisphere of the brain, just
under the corpus collosum. There
is a third ventricle just in between and below the thalamus.
Finally, there is a fourth ventricle,
just below the brain stem and beside the cerebellum. All four
ventricles may circulate CSF
between them by way of foramen (narrow oval openings), aqueducts
(canal-like passages), and
apertures (openings) (Tortora, 1989).
-
7/30/2019 Neuro Anaphy
10/27
unites the anterior and posterior blood supply to the brain.
This is a unique mechanism of
cerebral circulation that allows the brain to have a backup
system if one source of blood is
interrupted.
The cerebral arteries arise from the Circle of Willis and supply
specific areas of the brain.
The posterior cerebral artery (PCA) supplies blood to the
occipital lobe, midbrain, thalamus, and
part of the temporal lobes.
The middle cerebral artery (MCA) supplies blood to parts of the
frontal, parietal and
temporal lobes. The anterior cerebral artery (ACA) supplies
blood to different areas of the
frontal parietal and temporal lobes (AACN 1998)
-
7/30/2019 Neuro Anaphy
11/27
components of cranial nerves transmit nerve impulses from the
brain to target tissue outside of
the brain. Sensory components transmit nerve impulses from
sensory organs to the brain.
A summary of the functions of the cranial nerves is listed in
the table below.
Cranial Nerve Major Functions
Cranial Nerve I: Olfactory Sensory Smell
Cranial Nerve II: Optic Sensory Vision
Cranial Nerve III: Oculomotor Sensory and Motor
Primarily Motor
Eyelid and eyeball
movementCranial Nerve IV: Trochlear Sensory and Motor
Primarily Motor
Innervates superior
oblique
Turns eye downwardand laterally
Cranial Nerve V: Trigeminal Sensory and Motor ChewingFace and
mouth touch
and pain
Cranial Nerve VI: Abducens Sensory and Motor Primarily Motor
Turns eye laterallyProprioception
Cranial Nerve VII: Facial Sensory and Motor Controls most
facialexpressions
Secretion of tears and
saliva and Taste
Cranial Nerve VIII: Vestibulocochlear
(auditory)
Sensory Hearing
Equilibrium sensationCranial Nerve IX: Glossopharyngeal Sensory
and Motor Taste
Senses carotid blood
pressure
-
7/30/2019 Neuro Anaphy
12/27
proprioception
Spinal Cord
The spinal cord is the primary structure that connects the brain
and peripheral nervous
system. It is protected by the vertebrae of the spinal column.
The spinal cord is located in the
vertebral foramen and is made up of 31 segments: 8 cervical, 12
thoracic, 5 lumbar, 5 sacral and
1 coccygeal vertebrae. While a pair of the spinal nerves exit
from each segment of the spinal
cord, the spinal cord itself extends down to only the last of
the thoracic vertebrae. The spinalnerves that branch from the
spinal cord from the lumbar and sacral levels must run in the
vertebral canal for a distance before they exit the vertebral
column. This collection of nerves in
the vertebral canal is called the cauda equina (horses
tail).
-
7/30/2019 Neuro Anaphy
13/27
Reflexes are rapid, involuntary responses to stimuli which are
mediated over simple
nerve pathways called reflex arcs. Involuntary reflexes are very
fast, traveling in milliseconds.
The fastest impulses can reach 320 miles per hour (Sherwood,
1997). Reflexes can be
categorized as either autonomic or somatic. Autonomic reflexes
are not subject to conscious
control, are mediated by the autonomic division of the nervous
system, and usually involve the
activation of smooth muscle, cardiac muscle, and glands. Somatic
reflexes involve stimulation of
skeletal muscles by the somatic division of the nervous
system.
When peripheral reflexes are intact, a sensory stimulus travels
to the spinal cord. That
stimulus is then converted to a motor stimulus within the spinal
cord. The motor stimulus travels
back to the site of sensory input and usually causes muscle
contraction. An example is the knee-
jerk reflex or placing your hand on a hot stove. The sensory
stimulus does not need to travel all
the way to the brain to be interpreted and then back to the site
of potential injury (Sherwood
-
7/30/2019 Neuro Anaphy
14/27
PERIPHERAL NERVOUS SYSTEM
The peripheral nervous system is subdivided into the somatic
nervous system and the
autonomic nervous system. The somatic nervous system consists of
the twelve pairs of cranial
nerves and thirty-one pairs of spinal nerves.
Somatic Nervous System
The somatic nervous system is typically under voluntary control.
The somatic nervous
system includes all nerves controlling the muscular system and
external sensory receptors. The
somatic nervous system has both motor and sensory divisions.
Motor fibers are efferent fibers
which innervate skeletal muscle. They are present in spinal
nerves and cranial nerves III, IV, VI
and XII and terminate at the skeletal muscles. Sensory fibers
are afferent fibers that relay
sensations such as touch, pain and temperature from the skeletal
muscles via peripheral, spinal,
and cranial nerves V, VII, IX and X to the central nervous
system (Tortora, 1989).
Autonomic Nervous System
In contrast, the autonomic nervous system is not voluntary. It
is also a good thing it is
not. If it was voluntary, we would have to think about every
heart beat we had, the amount of
blood we delivered to specific tissues, the dilation of our
pupils, and how much digestive
motility our gastrointestinal tract needed. In other words, the
autonomic nervous system
regulates the activities of the internal organs (Sherwood,
1997).
The autonomic nervous system has two main parts, the sympathetic
and the
parasympathetic systems These two opposite systems often operate
in opposition to each
-
7/30/2019 Neuro Anaphy
15/27
muscles (Tortora, 1989). Sympathetic stimulation also dilates
the pupils, dilates the trachea and
bronchi, stimulates the conversion of glycogen into glucose,
inhibits peristalsis in the
gastrointestinal tract, and inhibits contraction of the bladder
and rectum. The overall effect of
sympathetic activation is to increase cardiac output, systemic
vascular resistance (both arteries
and veins), and increase arterial blood pressure. Enhanced
sympathetic activity is particularly
important during exercise, emotional stress, and during
hemorrhagic shock (AACN, 1998;
Sherwood, 1997).
Parasympathetic Nervous System
When the parasympathetic system is activated, it works to
decrease heart rate,
contractility, and conduction velocity of the myocardial tissue
via the vagus nerve, cranial nerve
X. Parasympathetic nerves mainly innervate salivary glands,
gastrointestinal glands, and genital
erectile tissue where they cause vasodilation (Tortora,
1989).
The parasympathetic system returns the body functions to normal
after they have been
altered by sympathetic stimulation. In times of danger, the
sympathetic system prepares the body
for aggressive activity. The parasympathetic system reverses
these changes when the danger is
over. Parasympathetic stimulation causes slowing down of the
heartbeat, lowering of blood
pressure, constriction of the pupils, increased blood flow to
the skin and viscera, and decreased
peristalsis of the gastrointestinal tract (AACN, 1998; Sherwood,
1997).
2 ) Readings
-
7/30/2019 Neuro Anaphy
16/27
injures part of the brain, it leaves a scar, and this scar can
then trigger abnormal electrical activity
that can start a seizure.
Dr. Sacco said that bleeding (hemorrhagic) strokes are more
likely to produce seizures
than ischemic strokes. That accounts for many of the seizures
that hit 26 percent of stroke
survivors in the first 30 days, making seizure risk the greatest
during that period.
Focusing on Treatment
Although research has led to a greater understanding of how to
treat seizures, no cure has
been found. Physicians focus on controlling seizures with
medicine while keeping side effects to
a minimum.
Once a seizure occurs, getting help quickly is essential.
Promptly treating seizures seems
to lower the risk of having more seizures, Dr. Sacco said, and
increases the chance of becoming
seizure-free. Medications may be less successful once seizures
and their consequences become
established.
The longer you go seizure-free on medicine, the lower your risk
and the more
reasonable it may be to take you off medicine.
If you have seizures early in the period of a stroke, yes, you
are still at risk for long-term
seizures. However, suppose that you have them early, get treated
and remain seizure-free. You
may be over the acute period and be able to come off the
drugs
-
7/30/2019 Neuro Anaphy
17/27
disease, stroke, brain tumors and Alzheimers disease. Of these,
stroke is the most frequent
cause.
If you are a stroke survivor and havent had seizures yet, having
another stroke is going
to increase your risk of seizures, Dr. Sacco said. Effective
lifestyle changes to reduce the risk of
seizures are the same as those to reduce the risk of recurrent
stroke. Controlling weight and
blood pressure, increasing physical activity and eating
nutritious food will help.
Out of Control
With most seizures, the effects last only a few seconds or
minutes, and normal physical
and mental functions are restored. But a condition called status
epilepticus, in which a person has
an abnormally long seizure or does not regain consciousness
between seizures, is life-
threatening. A seizure lasting longer than five minutes, for
practical purposes, should be treated
as a status epilepticus condition. Immediate medical help is
necessary.
Status epilepticus has been known to cause further injury (to
the brain), especially if its
occurring around the time of the stroke, Dr. Sacco said. Status
epilepticus in anybody will
increase the risk of mortality.
Drug Interaction
Stroke survivors who take blood thinners such as warfarin must
be carefully watched by
their doctors. Warfarin, an anticoagulant, fights the formation
of blood clots, which could cause
another stroke. Because it affects the liver, warfarin magnifies
the detrimental effect that anti-
seizure medicines have on the liver For the same reason Dr Sacco
recommends that alcohol
-
7/30/2019 Neuro Anaphy
18/27
All drugs have risks, and you dont want to use a drug if you
dont need it. Not every
stroke patient has a seizure.
Epilepsy is the commonest neurologic disorder with therapeutic
indications. Prevalence
of epilepsy is 0.5-1%.
Seizure is a clinical manifestation where you have a neuron
which fires excessively, so
there is hyper-excitability of a neuron coupled with hyper
synchronization. Hyper
synchronization means that a hyper-excitable neuron will lead to
excessive excitability of a large
group of surrounding neurons and you end with millions of
neurons in the brain firing
excessively leading to the clinical manifestations of the
seizure.
The phenotype of the seizure depends on the site it occurs at.
If the seizure comes from
the limbic system you will end up with temporal lobe or
emotional disturbances. If it occurs in
the rolandic area you will have motor seizure. If it starts in
both sides of the brain you will end
up with generalized seizure.
Seizure is a sudden time limited involuntary alteration of
behavior with or without loss of
consciousness accompanied by an abnormal electrical discharge.
Epilepsy is a disorder of the
CNS whose symptoms are seizures.
Seizures are a symptom of epilepsy. Seizures ("fits,"
convulsions) are episodes of
disturbed brain function that cause changes in attention or
behavior. They are caused by
abnormally excited electrical signals in the brain.
A single seizure may be related to a temporary medical problem
(such as brain or tumor
-
7/30/2019 Neuro Anaphy
19/27
cases, partial seizures can spread to wide regions of the brain.
They are likely to develop
from specific injuries, but in most cases the exact origins are
unknown (idiopathic ).
Generalized seizures. These seizures typically occur in both
sides of the brain. Many
forms of these seizures are genetically based. There is usually
normal neurologic
function.
PARTIAL SEIZURES (ALSO CALLED FOCAL SEIZURES)
These seizures are subcategorized as "simple" or "complex
partial."
Simple Partial Seizures. A person with a simple partial seizure
(sometimes known as
Jacksonian epilepsy) does not lose consciousness, but may
experience confusion, jerking
movements, tingling, or odd mental and emotional events. Such
events may include deja
vu, mild hallucinations, or extreme responses to smell and
taste. After the seizure, the
patient usually has temporary weakness in certain muscles. These
seizures typically last
about 90 seconds.
Complex Partial Seizures. Slightly over half of seizures in
adults are complex partial
type. About 80% of these seizures originate in the temporal
lobe, the part of the brain
located close to the ear. Disturbances there can result in loss
of judgment, involuntary or
uncontrolled behavior, or even loss of consciousness. Patients
may lose consciousness
briefly and appear to others as motionless with a vacant stare.
Emotions can be
exaggerated; some patients even appear to be drunk. After a few
seconds, a patient may
begin to perform repetitive movements such as chewing or
smacking of lips Episodes
-
7/30/2019 Neuro Anaphy
20/27
Tonic-Clonic (Grand Mal) Seizures. The first stage of a grand
mal seizure is called the
tonic phase, in which the muscles suddenly contract, causing the
patient to fall and lie stiffly for
about 10 - 30 seconds. Some people experience a premonition or
aura before a grand mal seizure.
Most, however, lose consciousness without warning. If the throat
or larynx is affected, there may
be a high-pitched musical sound (stridor) when the patient
inhales. Spasms occur for about 30
seconds to 1 minute. Then the seizure enters the second phase,
called the clonic phase. The
muscles begin to alternate between relaxation and rigidity.
After this phase, the patient may lose
bowel or urinary control. The seizure usually lasts a total of 2
- 3 minutes, after which the patient
remains unconscious for a while and then awakens to confusion
and extreme fatigue. A severe
throbbing headache similar to migraine may also follow the
tonic-clonic phases.
Absence (Petit Mal) Seizures. Absence or petit mal seizures are
brief losses of
consciousness that occur for 3 - 30 seconds. Physical movement
and loss of attention may stop
for only a moment. Such seizures may pass unnoticed by others.
Young children may simply
appear to be staring or walking distractedly. Petit mal may be
confused with simple or complex
partial seizures, or even with attention deficit disorder. In
petit mal, however, a person may
experience attacks as often as 50 - 100 times a day.
Myoclonic. Myoclonic seizures are a series of brief jerky
contractions of specific muscle
groups, such as the face or trunk.
Atonic (Akinetic) Seizures. A person who has an atonic (or
akinetic) seizure loses muscle
tone Sometimes it may affect only one part of the body so that
for instance the jaw slackens
-
7/30/2019 Neuro Anaphy
21/27
could be tied to the condition. For most people, genes are only
part of the cause, perhaps
by making a person more susceptible to environmental conditions
that trigger seizures.
Head trauma sustained during a car accident or other traumatic
injury can cause
epilepsy.
Medical disorders. Events like strokes or heart attacks that
result in damage to the brain
also can cause epilepsy. Stroke is responsible for up to
one-half of epilepsy cases in those
over age 35.
Dementia is a leading cause of epilepsy among older adults.
Diseases such as meningitis, AIDS and viral encephalitis can
cause epilepsy.
Prenatal injury. Before birth, babies are susceptible to brain
damage caused by an
infection in the mother, poor nutrition or oxygen deficiencies.
This can lead to cerebral
palsy in the child. About 20 percent of seizures in children are
associated with cerebral
palsy or other neurological abnormalities.
Developmental disorders. Epilepsy can sometimes be associated
with other
developmental disorders, such as autism and Down syndrome.
-
7/30/2019 Neuro Anaphy
22/27
Seizures occur whenever there is a scar in the brain, said Ralph
L. Sacco, M.D.,
professor of neurology and epidemiology at Columbia University
Medical Center. When stroke
injures part of the brain it leaves a scar and this scar can
then trigger abnormal electrical activity
-
7/30/2019 Neuro Anaphy
23/27
Seizures are one of the most common complications of stroke.
Overall, 5%-15% of stroke
patients will experience seizure within 2 years of stroke. The
reported risk factors for and
incidence of seizures after stroke vary widely, likely secondary
to differences in study design,
study populations, and use of antiepileptic drugs (AEDs). In
previous studies, the main risk
factors for poststroke seizures include stroke subtype, location
and severity. Poststroke seizures
rates are highest in those with intraparenchymal hemorrhage and
large supratentorial ischemic
strokes, and lowest after transient ischemic attacks, lacunar
infarcts, and brainstem strokes.
Although frequently encountered in clinical practice, there are
few evidence-based guidelines for
therapy of poststroke seizures. Poststroke seizures are
classified as early or late according to
their temporal proximity to the stroke. Early seizures, also
termed acute symptomatic seizures,
occur within the first week following stroke. These early
seizures are likely provoked by the
metabolic and physiologic derangements associated with acute
infarction or hemorrhage. Late
seizures are thought to result from epileptogenesis, changes in
neurons that result in permanent
hyperexcitability. (Herman, Susan T. MD.2011. Bech Israel
Deaconess Medical Center, Harvard
Medical School. Boston, MA)
The following factors increase your chance of developing some
seizure disorders:
Previous brain injury-seizure disorder usually develops within
one year of injury
Previous brain infection
Brain tumor
-
7/30/2019 Neuro Anaphy
24/27
Chemical abnormalities (decreased or excess blood sodium or
glucose, low blood
calcium)
Liver or Kidney Failure
Severe, untreated High Blood Pressure
Chronic diseases (eg, Systemic Lupus Erythematosus ,
Polyarteritis Nodosa ,
Porphyria , Sickle Cell Anemia , Whipple's Disease )
Syphilis
If you already have a seizure disorder, the following factors
can increase your chance of
having a seizure:
Sleep deprivation
Alcohol
Hormonal changes (such as those that occur at points during the
menstrual cycle)
Stress
Flashing lights, especially strobe lights
Use of certain medicines
Missing doses of anti-epileptic medicines
-
7/30/2019 Neuro Anaphy
25/27
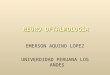
3) Schematic Diagram
NERVOUS SYSTEM
ETIOLOGY PREDISPOSINGFACTORS
- an electrical disturbance - idiopathic(genetic,in the nerve
cells in one developmental
defects)section of the brain, causing - acquired
(hypoxemia,them to emit abnormal, vascular
insufficiency,recurring, uncontrolled, fever (childhood),
head injury,electrical discharges hypertension,
CNS infections,metabolic and toxic
conditions,brain tumor, drug and
alcoholwithdrawal, and
allergies)
CELLULAR/ METABOLIC CHANGES GROSS ANATOMICAL PHYSICAL
CHANGES
PHYSIOLOGIC MANIFESTATION
26
-
7/30/2019 Neuro Anaphy
26/27
- when the integrity of the neuronal cell - involuntary
movements may spread - epigastricsensations, pallor,membrane is
altered, the cell begins firing centrally and involve the entire
limb, including sweating,flushing, goose fleshwith increased
frequency and amplitude. one side of the face and lower
extremities. (piloerection),
pupillary dilation,When the intensity discharges reaches the the
client also may exhibit changes in posture tachycardia,and
tachypnea.threshold, the neuronal firing spreads to or spoken
utterancesadjacent neurons, ultimately resulting toseizure.
Inhibitory neurons in epilepsy haveslow neuronal firing in the
cortex, anteriorthalamus, and basal ganglia. Once theinhibitory
processes develop or theepileptogenic neurons are exhausted,
theseizure stops then later events depress the
CNS activity and impair consciousness
SIGNS AND SYMPTOMS LABORATORY FINDINGSTONIC PHASE:
- fall, loss of consciousness, yell or tonic cry, - MRI may
detect lesions in thebrain, focal abnormalities,extension of arms,
legs, and/or face, fingers and cerebral degenerative changesand jaw
clenched. AUTONOMIC SYMPTOMS - EEG may allow diagnosis of thetype
and location of theinclude increase in blood pressure, heart rate
occurring seizure.and bladder pressure, flushing, sweating, - SPECT
may identify the epileptogeniczone so that the
27
-
7/30/2019 Neuro Anaphy
27/27
increased salivation and bronchial secretion, area in the brain
giving rise toseizures can be removedand apnea surgically.CLONIC
PHASE:
- muscles relax completely, then muscle tonereturns which causes
rhythmic jerking of headand body.POST-ICTAL PHASE:
- biting of the tongue, cheek or lip, andurinary incontinence
are common
SEIZURE
COMPLICATIONS
- Hypoxic brain damage and mental retardation may follow
repeated seizures- Depression and anxiety may develop. Long-term
social isolation may also occur
28


























![Neuro Assessment for Scalp the Non-Neuro Nurse … · Neuro Assessment for the Non-Neuro Nurse Terry M. Foster, RN, ... Microsoft PowerPoint - Neuro Grand Forks ND [Read-Only] Author:](https://img.pdfslide.net/doc/110x75/5b88746b7f8b9a301e8d8c76/neuro-assessment-for-scalp-the-non-neuro-nurse-neuro-assessment-for-the-non-neuro.jpg)