-
Neuroendocrine TumorsRocío García CarboneroHospital 12 de
Octubre, Madrid
-
Outline1. Epidemiology and prognosis
2. Singularities of NETs
3. Therapeutic aims in advanced disease (G1-G2 tumors)
4. Available treatment options (G1-G2 tumors)
Targeting somatostatin receptors
Targeting angiogenesis
Targeting mTOR
5. Therapeutic algorythms & clinical guidelines
-
Epidemiology of GEP-NENs
Incidence of NETs continues to grow: 6.98/105h/year(SEER
2012)
64,971 patients diagnosed with NETs from 1973 to 2012 (USA)
Age-adjusted incidence by site
Lung
Pancreas
Small IntestineRectum
Dasari et al, JAMA Oncol 2017
-
Prognosis by stage, grade and primary tumor site
Median OS for all patients: 112 months Local stage: from >
360 m for appendix to 168 m for small intestine Regional stage:
from > 360 m for appendix to 33 m for unknown primary Distant
stage: from 70 m for small intestine to 4 m for colon
Dasari et al, JAMA Oncol 2017
RectumAppendixStomachColonSmall
intestineLungCecumPancreasLiver
A: Survival by stage B: Survival by grade C: Survival by tumor
site
-
• Overall survival has improved over time, particularly for NETs
ofpancreatic or GI origin with advanced disease
Dasari et al, JAMA Oncol 2017
2005-2008
2000-2004
2009-2012
Year of Dx
Prognosis by year of diagnosis
-
Prevalence of GEP-NETs
2x more prevalent than pancreatic cancer
1. National Cancer Institute. SEER Cancer Statistics Review,
1975–2004. http://seer.cancer.gov/csr/1975–2004
2. Modlin IM, Lye KD, Kidd M. Cancer. 2003;97:934–959.
1,200,000
1,100,000
100,000
0Colorectal1 GEP-NET2 Stomach1 Pancreas1 Oesophagus1
Hepatobiliary1
Prevalence in SEER Database
-
TAXONOMY OF NENs
1. Oberndorfer (1907)
- Carcinoid vs Carcinoma
2. William & Sandler (1963)
- Embriologic origin: foregut, midgut, hindgut
3. WHO classification (2000/2010/2015)
4. TNM staging- ENETS 2006/2007- AJCC 2007
-
William & Sandler (1963)
FOREGUT
MIDGUT
HINDGUT
-
Tumor GradeKi67/MIB-1
-
WELL DIFFERENTIATED
NEUROENDOCRINE TUMOR
POORLY DIFFERENTIATED
NEUROENDOCRINE CARCINOMA
-
Clinical Presentation• Median age: 55-60 years• Primary tumor
site: 25% lung 50% GI (small intestine, rectum) 6-7% pancreatic
10-15% UK primary
• Tumor grade: ≈ 40% G1 / 20% G3• 30-50% Stage IV at diagnosis
(> for pancreatic or G3)• 20-25% Hormonal syndrome• 20%
Incidental diagnosis• 5% MEN syndrome
-
Tumor Hormone SymtomsCarcinoid
Insulinoma
Gastrinoma
Glucagonoma
VIPoma
Somatostatinoma
Serotonin
Insulin
Gastrin
Glucagon
Vasoactive Int. Peptide
Somatostatina
Flushes, diarrea. bronchospasm, carcinoid right heart
disease
Hypoglicemia: dizziness, fatigue, confusion, sweats, tremor
Zollinger-Ellison Sd: severe pepticulcer, diarrea
Diabetes, necrolytic migratoryerithema, glositis, thromboembolic
disease
Verner-Morrison Sd (WDHA) : watery diarrea, hipokalemia,
achloridria
Diabetes, esteatorrea, colelitiasis
Hormone Syndromes of Functional NETs
-
Localized disease: Surgery
Endoscopic resection (small rectal or gastricNETs)
Advanced disease: Hormonal syndrome control (G1-2 NETs)
Control of tumor proliferation
o G1-2: focus of this presentation
o G3: treat like SCLC
-
Antiproliferative Therapeutic Options
G1-G2 NETs - Available evidence from RCT:
Somatostatin analogues: “cold” (Octreotide, Lanreotide); “hot”
(PRRT)
Targeted therapies: Sunitinib, Everolimus
Chemotherapy: STZ, 5FU, ADR, other..
G3 P-NECs - Available evidence from case series &
non-controlled or retrospective studies:
Chemotherapy: CDDP/CBDCA-VP16, TEM-CAP, OX-FP, IRI-FP,
IRI-Platinum,…
-
Singularities of NETs: SSTR• 80-90% of well diff. NETs express
Somatostatin Receptors
relevant diagnostic and therapeutic implications
• Their natural ligand is Somatostatin, a physiological
neuropeptide involved in the regulation of neurotransmission, GI
motility, nutrient and ion
absorption, exocrine and endocrine secretion.
• Somatostatin analogs were developed with a longer half-life to
enable clinical use
Modlin et al, Aliment Pharmacol Ther 2010; 31:169
-
Inhibition of angiogenesis
Modulation of immune system
SMS Mechanism of Action
Antisecretory action Antiproliferative action
Guillermet-Guibert et al, Best Pract Res Clin Gastroenterol
2005.
-
OCTREOSCAN
• Scintigraphy with radiolabeled somatostatin analogs (SRS)
111In-DTPA-D-Phe1-octreotide (In-111 Pentreotide)
• Imaging technique to detect tumors expressing STS-R
Limitations of Octreoscan
Evaluation of organs with high physiological uptake (liver and
gut)
Poor spatial resolution (partially improved with the addition
of
SPECT/CT to SRS planar views)
Not all NETs express STS-R (i.e. Insulinomas 50-60%)
Time consuming / irradiation
-
Benefits of 68Ga-based NET tracers over OctreoScan
Decreased radiation dose (shorter half-life)
Improved image quality (PET vs SPECT)
Decreased biliary excretion
Improved lesion detection
Improved patient convenience
Availability of quantitation
-
Based on the ITT analysis
67% reduction in the risk of tumour progression HR=0.33; 95% CI:
0.19–0.55; P=0.000017
Time (months)
0
0.25
0.5
0.75
1
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90
Prop
ortio
n w
ithou
t pro
gres
sion
Time (months)
Octreotide LAR: 42 pts / 27 eventsMedian 15.6 months [95% CI:
11.0–29.4]
Placebo: 43 patients / 41 eventsMedian 5.9 months [95% CI:
5.5–9.1]
Rinke A et al. J Clin Oncol 2009;27:4656
PROMIDOctreotide LAR vs Placebo in G1 Midgut NETs
Antiproliferative Effect of “cold” SSA in GEP-NETs
CLARINETLanreotide Autogel vs Placebo in GEP-NETs (ki67
-
22
Pasireotide LAREverolimusPasireotide LAR and everolimus
0.7
1.0
0.9
0.8
0.6
0.2
0.4
KM P
roba
bilit
y of E
vent
0.5
0.3
0.0
0.1
Time (months)6 12 1590 3
No. of patients still at riskPasireotide
LAREverolimusCombination
221927
574
000
161725
414241
293030
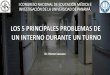
LUNA TRIAL: PROGRESSION-FREE SURVIVAL
124 pts with advanced WD typical and atypical carcinoids of the
LUNG or THYMUS
%PFS at 9 monthsPASIREOTIDE + EVE: 79.2%EVEROLIMUS:
56.9%PASIREOTIDE: 49.6%
-
Median PFS • 177-Lu: NOT REACHED• Control: 8.4 months
HR=0.21P
-
In mean, during the study, DIARRHOEA: LUTATHERA: 39% improved /
19% worsened Octreotide LAR: 23% improved / 23% worsened
QOL: Global Health Status/DiarrheaPercentage of patients with at
least 10 point changes compared to baseline
In mean, during the study, GLOBAL HEALTH STATUS : LUTATHERA: 28%
improved / 18% worsened Octreotide LAR: 15% improved / 26%
worsened
EORTC QLQ-G.I.NET21 questionnaire
-
Other Targeted Agents
Approved by FDA (2017) for use with SSA in patients with
carcinoid syndrome diarrhea not controlled by SSA:
TELOTRISTAT
Approved by FDA/EMA (2016) in GI and Lung NETs:
EVEROLIMUS
Approved by FDA/EMA (2011) for the treatment of PNETs:
SUNITINIB
EVEROLIMUS
-
Telotristat Etiprate A Tryptophan Hydroxylase (TPH)
Inhibitor
• Telotristat etiprate is a novel oral inhibitor of TPH, the
rate-limiting enzyme in serotonin biosynthesis1
• Two early-stage clinical studies of telotristat etiprate
demonstrated a favorable safety profile and evidence of clinical
activity in carcinoid syndrome2,3
• Both preclinical and clinical studies suggested that
telotristat etiprate is associated with minimal CNS activity1-3
• Granted Fast Track Status and Orphan Drug Designation4
31
5-HT secretion
Tryptophan
5-HTP
5-HT
5-HT in blood
5-HIAA
5-HIAA filtered by kidney
5-HIAA in urine
Monoamine oxidaseAldehyde dehydrogenase
TPH TelotristatEtiprate
5-HIAA, 5-hydroxyindoleacetic acid; 5-HT, serotonin; 5-HTP,
hydroxytryptophan; CNS, central nervous system; TPH, tryptophan
hydroxylase.1. Liu Q, Yang Q, Sun W, et al. J Pharmacol Exp Ther
2008; 325:47–55. 2. Kulke MH, O'Dorisio T, Phan A, et al. Endocr
Relat Cancer2014;21:705–714. 3. Pavel M, Horsch D, Caplin M, et al.
J Clin Endocrinol Metab 2015;100:1511–1519. 4. FDA Orphan Drug
Designations. Available at:
http://www.accessdata.fda.gov/scripts/opdlisting/oopd/index.
Accessed September 2015. 5. Kronenberg HM, Melmed S, Polonsky KS,
et al. Williams Textbook of Endocrinology, 11th edn.
2008:1823–1824.
Serotonin Synthesis in Carcinoid Tumor Cells
http://www.accessdata.fda.gov/scripts/opdlisting/oopd/index
-
TELESTARPhase 3 Study Design
32
*Including a blinded titration step of one week of 250 mg
TID.
BM, bowel movement; SSA, somatostatin analog; TID, three times
daily.ClinicalTrials.gov. NCT01677910 TELESTAR. Available at:
https://clinicaltrials.gov/ct2/show/NCT01677910. Accessed September
2015.
Telotristat etiprate 500 mg TID* (n=45)
Telotristat etiprate 250 mg TID (n=45)
Placebo TID (n=45)
All patients required to be on SSA at enrollment and continue
SSA therapy throughout study period
1:1:13- to 4-
week run-in (n=135)
R
Telotristat etiprate
500 mg TID
Evaluation of primary endpoint:Reduction in number of daily BMs
from baseline
(averaged over 12-week double-blind treatment phase)
Run in: Evaluation of
bowel movement
(BM) frequency
https://clinicaltrials.gov/ct2/show/NCT01677910
-
33
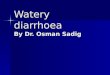
TELESTAR: Reduction in Daily Bowel Movement Frequency Averaged
Over Double-Blind Treatment Phase
BM, bowel movement; SSA, somatostatin analog.
All patients continue SSA therapy throughout study period
Placebo n=45Telotristat etiprate 250 mg n=45Telotristat etiprate
500 mg n=45
• Hodges–Lehmann estimator of treatment differences estimated a
reduction versus placebo of • –0.81 BMs daily for telotristat
etiprate 250 mg dose (P
-
• Wilcoxon rank-sum test showed significant differences for each
telotristat etiprate dose vs. placebo (p
-
VEGF WHO I VEGF WHO III High MVD Low MVD
A rich vascular network is a distinctive feature of NETs
A negative correlation of microvascular density (MVD) and VEGF
expression with tumor progression has been documented
Low MVD is an unfavorable prognostic factor in PNETs
British Journal of Cancer 2005;92:94-101.; Gastroenterology
2003;125:1094-1104.
-
Raymond, NEJM 2011
Sunitinib: 11,5 monthsPlacebo: 5,5 months
HR 0.42P
-
Sunitinib vs Placebo in PNETs 2016 – Final OS analysis 5y after
study closure
Raymond, ASCO GI 2016
69% crossoverΔ 9,5 months
Median OSSunitinib: 38,6 monthsPlacebo: 29,1 months
HR 0.73P=0.094
-
19/06/2017 38
mTOR activation in tumors Occurs in ~ 50% of human cancers
Pathway activation occurs through: Excess of ligand Receptor
overexpression (EGFR, Her2,..) Gain of function mutations (PI3K,
AKT,..) Inactivation of PTEN, TSC1/TSC2, LKB1,.. Other (bcr-abl
traslocation, ras-raf mutations..)
Pathogenesis of NETs: Familial syndromes: NF1, TSC1/TSC2, menin?
Sporadic PNETs: 15% mutations PI3K-mTOR
pathway (WES) Sporadic Si-NETs: 29% PI3K-mTOR genetic
alterations(amplifications/mutations AKT/mTOR/PI3K)
Altered expression of mTOR pathway componentsassociated with
proliferative index, metastaticpotential and survival
Chan et al, Curr Treat Options Oncol. 2014
-
Yao et al, NEJM 2011
Everolimus (n=191) Placebo (n=189)
Tumor Shrinkage: 64% Tumor Shrinkage: 21%
ORR= 4.8% ORR= 2.0%
RADIANT-3: Everolimus vs Placebo in Pancreatic NETs(N=410)
-
Crossover: 73%
Yao et al, NEJM 2011
-
RADIANT-2 Study DesignInternational, Multicenter, Double-Blind,
Placebo-Controlled, Phase III Trial
Treatment until disease progression
Adult patients with advanced NET and a history of secretory
symptoms (N = 429)
• Advanced low- or intermediate-grade NET
• Radiologic progression in the past 12 months
• History of secretory symptoms (flushing or diarrhea)
• Previous antitumor therapy allowed
• WHO Performance Status d2
1:1
Multi-phasic CT or MRI performed every 12 weeks
Crossover at time of disease progression
Enrollment January 2007 to May 2008.
Everolimus 10 mg/d + Octreotide LAR 30 mg q28d
n = 216
Placebo + Octreotide LAR 30 mg q28d
n = 213
RANDOMIZE
-
PFS by Central Review*
Time, monthsNo. of patients still at riskE + OP + O
216213
202202
167155
129117
120106
10284
8172
6965
6357
5650
5042
4235
3324
2218
1711
119
43
11
10
00
*Independent adjudicated central review committee. The
prespecified boundary for significance was P ≤ 0.0246.E + O =
everolimus + octreotide LAR.P + O = placebo + octreotide LAR.
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38
Perc
enta
ge E
vent
-Fre
e
Kaplan-Meier median PFSEverolimus + octreotide LAR: 16.4
monthsPlacebo + octreotide LAR: 11.3 months
Hazard ratio, 0.77; 95% CI, 0.59-1.00P = 0.026
Total events = 223Censoring timesE + O (n/N = 103/216)P + O (n/N
= 120/213)
-
RADIANT-4 Study Design
*Based on prognostic level, grouped as: Stratum A (better
prognosis) - appendix, caecum, jejunum, ileum, duodenum, and NET of
unknown primary. Stratum B (worse prognosis) - lung, stomach,
rectum, and colon except caecum.Crossover to open label everolimus
after progression in the placebo arm was not allowed prior to the
primary analysis.
Patients with well-differentiated (G1/G2), advanced,
progressive, nonfunctional NET of lung or GI origin (N = 302)•
Absence of active or any history
of carcinoid syndrome• Pathologically confirmed
advanced disease • Enrolled within 6 months from
radiologic progression
Everolimus 10 mg/day N = 205
Treated until PD, intolerable AE, or
consent withdrawal
2:1
Placebo N = 97
RANDOMIZE
Endpoints: • Primary: PFS (central)• Key Secondary: OS•
Secondary: ORR, DCR, safety, HRQoL (FACT-G),
WHO PS, NSE/CgA, PK
Stratified by:• Prior SSA treatment (yes vs. no)• Tumor origin
(stratum A vs. B)*• WHO PS (0 vs. 1)
Yao JC et al. Lancet 2015; Published Online December 15,
2015.
-
Baseline and Disease Characteristics (2/2)
†Organs as per target and non-target lesion locations observed
at baseline by central radiology review.‡Patients were expected to
have disease progression in ≤ 6 months prior to enrolment as per
inclusion criteria. Protocol deviation was reported in 7
patients.
Characteristic EverolimusN = 205PlaceboN = 97
Tumor gradeGrade 1 / grade 2 63% / 37% 67% / 33%
Metastatic extent of disease†Liver 80% 78%Lymph node or
lymphatic system 42% 46%Lung 22% 21%Bone 21% 16%
Median time from initial diagnosis to randomization, months
(range) 29.9 (0.7-258.4) 28.9 (1.1-303.3)
Median time from most recent progression until enrolment, months
(range)‡ 1.68 (0.0-7.8) 1.45 (0.2-11.8)
Prior treatmentsSomatostatin analogues 53% 56%Surgery 59%
72%Chemotherapy 26% 24%Radiotherapy including PRRT 22%
20%Locoregional and ablative therapies 11% 10%
Yao JC et al. Lancet 2015; Published Online December 15,
2015.
-
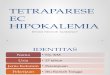
Primary Endpoint: PFS by Central Review
P-value is obtained from the stratified one-sided log-rank test;
Hazard ratio is obtained from stratified Cox model.
52% reduction in the relative risk of progression or death with
everolimus vs placeboHR = 0.48 (95% CI, 0.35-0.67); P <
0.00001
205 168 145 124 101 81 65 52 26 10 3 0 097 65 39 30 24 21 17 15
11 6 5 1 0Placebo
Everolimus
No.of patients still at risk
0 2 4 6 8 10 12 15 18 21 24 27 30Months
0
10
20
30
40
50
60
70
80
90
100
Prob
abili
ty o
f Pro
gres
sion
-free
Sur
viva
l (%
) Kaplan-Meier mediansEverolimus: 11.0 months (95% CI,
9.23-13.31) Placebo: 3.9 months (95% CI, 3.58-7.43)
Censoring TimesEverolimus (n/N = 113/205)Placebo (n/N =
65/97)
Yao JC et al. Lancet 2015; Published Online December 15,
2015.
-
PFS HR by Primary Tumor Origin –Retrospective Analysis, Central
Review
*One patient with thymus as primary tumor origin was not
included.†Stomach, colon, rectum, appendix, cecum, ileum, duodenum,
and jejunum are grouped under GI.Hazard ratio obtained from
unstratified Cox model.GI, gastrointestinal; NET, neuroendocrine
tumors
Lung
GI†
NET of unknown primary
Hazard Ratio (95% CI)Subgroups*
90
175
36
No.
0.1 0.4 1 10
0.50 (0.28-0.88)
0.56 (0.37-0.84)
0.60 (0.24-1.51)
Everolimus Better Placebo Better
Yao JC et al. Lancet 2015; Published Online December 15,
2015.
-
PFS midgut vs non-midgut
Stomach, colon, rectumDuodenum, jejunum, ileum, caecum,
appendix, small intestine
-
Interim Overall Survival Analysis
*Boundary for significance = 0.0002.P-value is obtained from the
stratified one-sided log-rank test; Hazard ratio is obtained from
stratified Cox model.NS, not significant.
First interim OS analysis performed with 37% of information
fraction favored the everolimus arm
205 195 184 179 172 170 158 143 100 59 31 5 097 94 86 80 75 70
67 61 42 21 13 5 0Placebo
Everolimus
No. of patients still at risk
0 2 4 6 8 10 12 15 18 21 24 27 30Months
0
10
20
30
40
50
60
70
80
90
100
Prob
abili
ty o
f Ove
rall
Surv
ival
(%)
Censoring TimesEverolimus (n/N = 42/205)Placebo (n/N =
28/97)
Everolimus vs PlaceboHR = 0.64 (95% CI, 0.40-1.05); P = 0.037
(NS)*
Next interim analysis is expected in 2016
Yao JC et al. Lancet 2015; Published Online December 15,
2015.
-
Moertel et al, NEJM 1980
STREPTOZOTOCIN
1950’s – 1st isolated 1968 – 1st case report 1982 – FDA approval
for PNETs
Cytotoxic chemotherapy
-
Cytotoxic Chemotherapy: Randomized Trials
N Tx arms RR OS
PANCREATIC NETS
Moertel - ECOG 1972 84 STZ + FU 63%* 26 m(NEJM 1980) STZ 36% 16
m
Moertel - ECOG 1978 105 STZ + DOX 69%* 26 m*
(NEJM 1992) STZ + FU 45% 17 m
Chlorozotocin 30% 18 m
RR includes clinical, biochemical and radiological responses * p
< .05
-
Moertel et al, NEJM 1980 Moertel et al, NEJM 1992
Cytotoxic Chemotherapy: Randomized Trials
• No proper assessment of STZ vs placebo or BSC
• Adding 5FU to STZ improves response rate and survival
• Doxo is better than 5FU in combination with STZ (↑ RR and
OS)
-
Temozolomide-based chemotherapy
Type of study Treatment Regimen # Pts Grade RR PFS OS
All (PNET) PNET
Retrospective1 TMZ 200 mg/m2 d1-5 q4w 36 (12) Any 8% NR NR
Phase II2 TMZ 150 mg/m2 d1-7 q2w 29 (11) WD 45% NR NR
Thalidomide 50-400 mg/d
Retrospective3 Capecitabine 750 mg/m2 bid d1-14 q4w 30 (30) WD
70% NR NR
TMZ 200 mg/m2 d10-14 q4w
Phase II4 Capecitabine 750 mg/m2 bid d1-14 q4w 28 (11) WD 45% NR
NR
TMZ 200 mg/m2 d10-14 q4w
Retrospective5 Capecitabine 750-1000 mg/m2 bid d1-14 q4w 65 (46)
G1-G2 52% 18.4 38.3
TMZ 150-200 mg/m2 d10-14 q4w
Encouraging data from small non-controlled studies or
retrospective series Convenient and well tolerated Role of
MGMT?
1Ekeblad et al, Clin Cancer Res 2007; 2Kulke et al, JCO 2006;
3Strosberg et al, Cancer2011; 4Fine et al, ASCO GI 2014; 5Crespo et
al, Future Oncol 2016
-
19/06/2017 53
Chemotherapy vs Targeted agents
Chemotherapy:
poorer available evidence: few RCT, many small prospective or
retrospective cohorts
limited availability of some agents (STZ)higher tumor response?
less convenient (iv) but cheaper
Targeted agents:
high level of evidence (placebo-controlled trials) no tumor
shrinkage (RR < 10%) improved PFS but no evidence of improved
survival more convenient (oral) but greater cost
-
19/06/2017 54
When would we favor chemotherapy?
High tumor burden
control symptoms related to tumor bulk
neoadjuvant setting: induce tumor shrinkage to facilitate
surgery
High mitotic or proliferative index (ki-67 cut-off?)
Poorly differentiated tumors
Pancreatic primary
Biomarkers? (MGMT deficient -> temozolomide?)
-
Optimal Sequence?
-
PD
Pancreatic NEN: ENETS Guidelines for advanced disease
Pavel M et al, Neuroendocrinology 2016
-
PD
Pancreatic NEN: ENETS Guidelines for advanced disease
Pavel M et al, Neuroendocrinology 2016
-
SI-NEN: ENETS Guidelines for advanced disease
Pavel et al, Neuroendocrinology 2016
-
19/06/2017 59
Conclusions Medical and non-medical therapeutic options are
increasing:
PNETs: Lanreotide, Sunitinib, Everolimus, Chemotherapy GI NETs:
SSA, PRRT, Everolimus Lung NETs: Everolimus
New challenges arise: What to use and when? For how long?
Optimal sequence and combination? Integration with other non
medical therapies?
Pending issues: What is the best option for each individual pt?
– Biomarkers!! Improve safety and efficacy!! Novel targets
Número de diapositiva 1Número de diapositiva 2Epidemiology of
GEP-NENsPrognosis by stage, grade and primary tumor siteNúmero de
diapositiva 5Prevalence of GEP-NETsTAXONOMY OF NENsWilliam &
Sandler (1963)�Número de diapositiva 9Tumor GradeNúmero de
diapositiva 11Clinical PresentationNúmero de diapositiva 13Número
de diapositiva 14Antiproliferative Therapeutic OptionsNúmero de
diapositiva 16SMS Mechanism of ActionNúmero de diapositiva 18Número
de diapositiva 19Número de diapositiva 20PROMID�Octreotide LAR vs
Placebo in G1 Midgut NETsNúmero de diapositiva 22Número de
diapositiva 23Número de diapositiva 24Número de diapositiva
25Número de diapositiva 26Número de diapositiva 27Número de
diapositiva 28Número de diapositiva 29Other Targeted
AgentsTelotristat Etiprate �A Tryptophan Hydroxylase (TPH)
Inhibitor TELESTAR �Phase 3 Study DesignTELESTAR: Reduction in
Daily Bowel Movement Frequency Averaged Over Double-Blind Treatment
PhaseTELESTAR: Mean Absolute Change in Urinary 5-HIAA (mg/24 h)
from Baseline to Week 12Número de diapositiva 35Número de
diapositiva 36Sunitinib vs Placebo in PNETs �2016 – Final OS
analysis 5y after study closuremTOR activation in tumorsNúmero de
diapositiva 39Número de diapositiva 40RADIANT-2 Study DesignPFS by
Central Review*RADIANT-4 Study DesignBaseline and Disease
Characteristics (2/2)Primary Endpoint: PFS by Central Review PFS HR
by Primary Tumor Origin – �Retrospective Analysis, Central Review
PFS midgut vs non-midgutInterim Overall Survival AnalysisNúmero de
diapositiva 49Número de diapositiva 50Número de diapositiva
51Número de diapositiva 52Chemotherapy vs Targeted agentsWhen would
we favor chemotherapy?Número de diapositiva 55Número de diapositiva
56Número de diapositiva 57Número de diapositiva 58Conclusions