Embed Size (px)
Citation preview

M 919, ~~. S - -.
Neurogenic Switching: A Hypothesis for aMechanism for Shifting the Site of Inflammationin Allergy and Chemical SensitivityWilliam J. MeggsDepartment of Emergency Medicine, East Carolina University School of Medicine,Greenville, NC 27858 USA and New York City Poison Center, New York, NY 10016 USA
Neurogenic switching s p*ows4d::'kA"hwothcsis for a m~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~....... ... ... ....aahypothesis for a mecaisi' wFI:.stimulus at one site can..lead.t. .....m.tion at a distant site. Neo ition occurs when substance Pni o.th..e.r :neuropeptides released m s .e.rons produce an inflammatory response,whereas unogeic inflammat o.n.resultsfrom the binding of antgen to an rleukocyte receptors. There is acr.ossoer:mechanism between ..:es ..;.tw .....
inflammation. Neuon s ispr-posed to result when aso imuse fm.a site ofacvation is rerot.. .. ..t....cenervous system to a distant l o pro-*duce neurgenic inflammation::a d.es.e. olocation. Neurogenic svc ..g..apsbexplanation for systemic aphyla.`is,:iniwhich inoculation of the skin .or gt withantge produXces sytemi syp1m inving. the respiratory and cut. se,and an experimental model of . isconsistent with this hypothesis. od-lgy-iducing asthma, urticaria,ar:thritsd.d..fibromyhga are other poss ealo:esrogc switng. N n wprovides a mechanism to e h
...... .........................................................-gens -infectious agents, irtns adpsibly em.otional stress can ea c,odi-tons such as migaine, asthma, n artritis. Because neurogenic Sinam.atio..o.:sknown to be triggered by emi. po-surm, it may play a role in the sickbsyndrome and dhe multiple chcal sensi-ivity syndrome. Thus _.rgnc tchingwould explain how the p irtory irrita_a..n.lead to smptoms at othersies i tsorders. Key words: allergy, l-arthritis, asthma,ceia estvt,foaler, in t, miginfation, substa P.:P:
103:54-56 (1995)
There are two grand, interrelated systemsby which foreign materials can produceinflammation in a tissue. Immunogenicinflammation arises when an antigen bindsto an antibody or leukocyte receptor totrigger an inflammatory cascade. Prior sen-sitization is required, and the inflammato-ry response can take several forms includ-ing immediate and cell-mediated hyper-sensitivity. Neurogenic inflammationoccurs when a chemical combines with thechemical irritant receptors on sensorynerves, leading to the release of substanceP and other inflammatory neuropeptides(1). Neurogenic inflammation can alsoarise when a nerve impulse travels down an
axon to release substance P at the terminus(2,3). There is an interplay betweenimmunogenic and neurogenic inflamma-tion, in that substance P can degranulatemast cells and histamine can activate sen-sory nerves (4), as depicted in Figure 1.This figure is a simplification, in that ahost of other cells and mediators areinvolved in inflammation. However, thecells and mediators depicted in the figuredominate the type I immediate hypersensi-tivity response to allergens and sensitivityto chemicals. Clinically, the two formsmay lead to the same end result. For exam-ple, asthma can be initiated by allergens(immunogenic inflammation) or chemicalirritants (neurogenic inflammation).
One puzzling feature of the inflamma-tory response is that a stimulus in one tis-sue can sometimes lead to inflammation atanother site. Food allergy provides anexample. Ingestion of a food allergen canproduce gastrointestinal symptoms, withdiarrhea, abdominal pain, bloating, andemesis arising from the direct degranula-tion of gut mast cells with local mediatorrelease. A small percentage of patients withfood allergy develop symptoms at othersites, manifesting as asthma (5), rhinitis(6), or urticaria ('). Food hypersensitivitycan also manifest as arthritis (8,9) andmigraine (10,11). Histamine from gutmast cells could bind to sensory nerves toproduce an afferent signal, which could bererouted via the central nervous system toanother site, as depicted in Figure 1. Thisneurogenic switching could then explainthe diverse manifestations of food allergy.
Systemic anaphylaxis may be a mani-festation of neurogenic switching.Cutaneous inoculation with an antigen,such as a bee sting, or gut inoculation, asin the ingestion of a food or drug, canaffect multiple organ systems immediately.Respiratory involvement with bron-chospasm, bronchorrhea, and laryngealedema, gastrointestinal symptoms, skininvolvement away from the site of inocula-tion with diffuse flushing or urticaria, andcardiovascular symptoms with hypotensionfrom vasodilation can all arise. A role forthe nervous system in systemic anaphylaxishas been demonstrated in experimentalmodels. It is known that vagotomy pro-tects rats from lethal anaphylaxis withoutchanging the production of antibody or
histamine release (12). Experimentallesions of the anterior hypothalamuslessens the anaphylactic reaction in aguinea pig model (13). Neurogenic switch-ing may be the mechanism for thisobserved modulation of anaphylaxis by thenervous system, though other mechanismssuch as a generalized decrease in parasym-pathetic tone should be considered.
Gustatory rhinitis is another phenome-non in which neurogenic switching mayplay a role. In this syndrome, rhinorrhea,nasal congestion, and facial sweating devel-op after the ingestion of spicy foods.Ingested irritants such as capsaicin, theactive ingredient in chili peppers, interactwith branches of the trigeminal nerveinnervating the oral cavity. The efferentsignal is switched to the nose and face(14).
Sick building syndrome (15), in whichdiverse symptoms such as headache anddifficulty with concentration accompanymucosal irritation in occupants of poorlyventilated buildings, may involve neuro-genic switching. The site of inflammationcould be switched from the airway to thebrain, causing vasodilation and edema. Analternative hypothesis is that lymphocytesat the site of stimulation release mediatorswhich circulate to the brain and causesymptoms (16). Interleukin-I and inter-leukin-2 are known to affect cerebral func-tion in animal models (17,18). This typeof switching might be termed "immuno-genic switching."
Neurogenic switching may play a rolein multiple chemical sensitivity syndrome(19-21), which is thought to be mediatedby neurogenic inflammation (22). In thissyndrome, exposure to respiratory irritantstriggers symptoms in more than one organsystem. An individual patient with chemi-cal sensitivities often has recurrent sites ofsymptomatology and inflammation whichreoccur with a well-defined pattern.Myalgias in the nape of the neck, inflam-mation of a particular set of joints, or gas-trointestinal symptoms might occur overand over again in a single patient. Theestablishment of a neuronal pathway sothat stimulation of irritant receptors in theairway, for example, leads to inflammationin a given tissue may be the mechanism forinvolvement of secondary organ systems.
Neurogenic inflammation is thoughtto play a role in rheumatoid arthritis (23),migraine headache (24,25), and fibromyal-gia (26). The basis of these conditions may
Address correspondence to W.J. Meggs, Room4W54, Brody Building, Department of Emer-gency Medicine, East Carolina University,Greenville, NC 27858 USA.Received 1 July 1994; accepted 14 September1994.
Environmental Health Perspectives54

L- a h Ia.,- I=
-p
FBI~~ 4m0
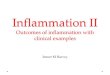
Figure 1. Interplay between neurogenic and immunogenic inflammation, with neurogenic switching of theinflammation site. (A) Chemical irritants (Ch) bind sensory neurons to release neuropeptides includingsubstance P (Sp). An afferent signal travels to the central nervous system (CNS). (B) Antigen (Ag) bindsIgE molecules on mast cells to release mast cell mediators including histamine (H). Histamine binds toreceptors on sensory neurons, and substance P binds to receptors on mast cells. (C) Both histamine andsubstance P can bind effector cells, such as endothelial cells, mucus-secreting cells, and bronchialsmooth muscle cells to produce inflammation. (D) Neurogenic switching occurs when an efferent signalfrom the CNS causes release of neuropeptides at another site, producing inflammation at the second sitewithout local stimulation.
be an acquired neuronal pathway thatshunts inflammatory stimuli to the joints,cerebral vasculature, or muscles, respective-ly. Then, inflammatory stimuli arisingfrom allergens, chemical irritants, or infec-tious agents could lead to a flare in inflam-mation at the diseased site. Emotionalstress might also lead to neuronal signalsthat could result in inflammation at sus-ceptible sites.
To summarize, it has been pointed outthat the multiple organ system involve-ment that has been so problematic inunderstanding chemical sensitivity alsooccurs in allergy. A single mechanism mayunderlie this switching of the site of in-flammation in both allergy and chemical
sensitivity. It is hypothesized that neuro-genic switching is one possible mechanismby which stimulation of inflammation atone site can lead to inflammation at anoth-er (Fig. 1). An exposure to either an aller-gen or chemical irritant at one site leads toa sensory nerve impulse. For allergens,mast cell degranulation leads to the releaseof histamine and other mediators, and hist-amine binds receptors on sensory nerves.For chemical irritants, receptors on periph-eral nerves are directly triggered. When theimpulse reaches the central nervous system,it is redirected to another peripheral loca-tion, leading to the release of substance Pand other neuropeptides, producing in-flammation at the second site.
An alternative hypothesis is thatimmunogenic switching occurs, with therelease of cytokines which act on distantcells. There are several differences expectedbetween neurogenic switching andimmunogenic switching. The time requiredfor the onset of neurogenic switchingdepends on nerve conduction velocity,while immunogenic switching depends oncirculation time and diffusion times in tis-sues. Neurogenic switching would directlytarget a particular organ in a repetitive pat-tern, while immunogenic switching mighthave a more diffuse effect. The mechanismby which the site of inflammation is shiftedin both allergy and chemical sensitivity canbe determined experimentally, both in con-trolled challenges in human subjects andexperimental models. Such a programcould further our understanding of theseconditions while leading to improvementsin diagnosis and treatment.
REFERENCES
1. Foreman JC. Peptides and neurogenic inflam-mation. Br Med Bull 43:386 (1987).
2. Hinsey JC, Gasser HS. The component of thedorsal root mediating vasodilation and theSherrington contracture. Am J Physiol 92:679(1930).
3. Chahl LA. Antidromic vasodilation and neuro-genic inflammation. Pharmacol Ther 37:275-300 (1988).
4. Cavagnaro J, Lewis RM. Bidirectional regula-tory circuit between the immune and neuroen-docrine systems. Year Immunol 4:241-252(1989).
5. Onorato J, Merland N, Terral C, Michel FB,Bousquet J. Placebo-controlled double-blindfood challenge in asthma. J Allergy ClinImmunol 78:1139-1146 (1986).
6. Bousquet J, Chanez P, Michel F-B. The respi-ratory tract and food hypersensitivity. In: Foodallergy: adverse reactions to foods and foodadditives (Metcalfe DD, Sampson HA, SimonRA, eds). Oxford:Blackwell ScientificPublications, 1991; 139-149.
7. Adkins FM. Food-induced urticaria. In: Foodallergy: adverse reactions to foods and foodadditives (Metcalfe DD, Sampson HA, SimonRA, eds). Oxford:Blackwell ScientificPublications, 1991; 129-138.
8. Parke AL, Hughes GRV. Rheumatoid arthritisand food: a case study. Br Med J 282:2027-2029 (1981).
9. Panush RS, Stroud RM, Webster EM. Foodinduced (allergic) arthritis: clinical and serolog-ical studies. Arthritis Rheum 29:220 (1986).
10. Egger J, Wilson J, Carter CM, Turner MW. Ismigraine food allergy? A double-blind trial ofoligoantigenic diet treatment. Lancet 2:865-869 (1983).
11. Mansfield LE, Vaughan TR, Waller SF,Haverly RW, Ting S. Food allergy and adultmigraine: double blind and mediator confirma-tion of an allergic etiology. Ann Allergy 55:126-129 (1985).
12. Levy RM, Rose JE, Johnson JS. Effect of vago-tomy on anaphylaxis in rat. Clin Exp Immunol24:96-101 (1976).
13. Leslie CA, Mathe AA. Modification of guineapig lung anaphylaxis by central nervous system
Volume 103, Number 1, January 1995 55

e i
(CNS) perturbations. J Allergy Clin Immunol83:94-101(1989).
14. Raphael GD, Baraniuk JN, Kaliner MA. Howand why the nose runs. J Allergy ClinImmunol 87:457-467 (1991).
15. Molhave L. The sick buildings-a subpopula-tion among the problem buildings. In: IndoorAir '87. Proceedings of the IV Internationalconference on indoor air quality and climate,vol 2 (Sefert B, Esdorn H, Fischer M, eds).Berlin:Institute for Water, Soil, and AirHygiene, 1 987.
16. Meggs WJ. Multiple chemical sensitivities andthe immune system. Toxicol Ind Health 8:203-214 (1992).
17. Obal F Jr, Opp M, Cady AB. Interleukin 1alpha and interleukin 1 beta fragments are
somnogenic. Am J Physiol 259:R439-446(1990).
18. DeSarro GB, Masuda Y, Ascioti C, AudinoMG, Nistico G. Behavioral and ECG spectrumchanges induced by intracerebral infusion ofinterferons and interleukin-2 in rats are antago-nized by naloxone. Neuropharmacology 29:167-179 (1990).
19. Randolph TG. Human ecology and suscepti-bility to the chemical environment.Springfield, IL:C. C. Thomas, 1962.
20. Tabershaw IR, Cooper WC. Sequelae of acuteorganic phosphate poisoning. J Occup Med8:5-19 (1966).
21. Cullen MR. The worker with chemical sensi-tivities: an overview. State Art Rev Occup Med2:655-661 (1987).
22. Meggs WJ. Neurogenic inflammation and sen-sitivity to environmental chemicals. EnvironHealth Perspect 101:234-238 (1993).
23. Gronblad M, Konttinen YT, Korkala 0, LiesiP, Hukkanen M, Polak JM. Neuropeptides insynovium of patients with rheumatoid arthritisand osteoarthritis. J Rheum 15:1807-1810(1988).
24. Silberstein SD. Advances in understanding thepathophysiology of headache. Neurology42(suppl 2):6-10 (1992).
25. Buzzi MG, Moskowitz MA. The trigemino-vascular system and migraine. Pathol Biol40:313-317 (1992).
26. Zimmerman M. Pathophysiologic mechanismsof fibromyalgia. Clin J Pain 7(suppl):S8-1 5(1991).
~~~~~~~~~~~r~~~~~~~7r SS< .Xairi~~~~~~~~~i.20iti22ig08X; -..w75X;X. Dim.. ;.t~.........
wlm.~~~~~~~~~I~f IA.|
~~~~~~~~~_ FLLf'-V~~~~~~~~~~,,,St,,Ae<Gl_%g iifX4
56 Environmental Health Perspectives