Embed Size (px)
DESCRIPTION
Neurological System Chapter 38. White Christensen Kockrow Adam Leslie Lehmkuhl, RN 2008. Affect Agnosia AneurysmAphasia Areflexia Apraxia Ataxia Aura Automatism Autonomic nervous system. Bradykinesia Stroke Central nervous system Diplopia. Key Terms. Cephalgia - PowerPoint PPT Presentation
Citation preview

Neurological SystemChapter 38
White
Christensen
Kockrow
AdamLeslie Lehmkuhl, RN 2008

Key Terms
• Affect• Agnosia• AneurysmAphasia• Areflexia• Apraxia• Ataxia• Aura• Automatism• Autonomic nervous
system
• Bradykinesia• Stroke• Central nervous
system • Diplopia

Terms
• Cephalgia • Chorea • Copralalia• Dysarthria• Dysphagia• Emotional lability• Encephalitis
• Decorticate posturing: of arms and legs rigid plantar flexion
• Decerebrate: rigid extension of arms and legs with wrists turned outward


Terms
• Fasciculation• Flaccid • Glascow coma scale• Global cognitive
dysfunction• Graphesthesia• Hemanopia• Hemiplegia
• Hemiparesis• Hyperreflexia• Meningitis • Mentation• Nystagmus• Neuralgia• Neurogenic shock• Orientation • Paraplegia


Terms
• Postictal period• Proprioception• Quadrspelegia• Sclerotic• Spastic
• Spinal shock• Status epilepticus• Sterognosis • Unilateral neglect
• Vertigo

Introduction• The nervous system is
the body’s communication network.
• It coordinates and organizes the functions of all other body systems.
• A highly complex and coordinates and controls all motor, sensory and autonomic functions.
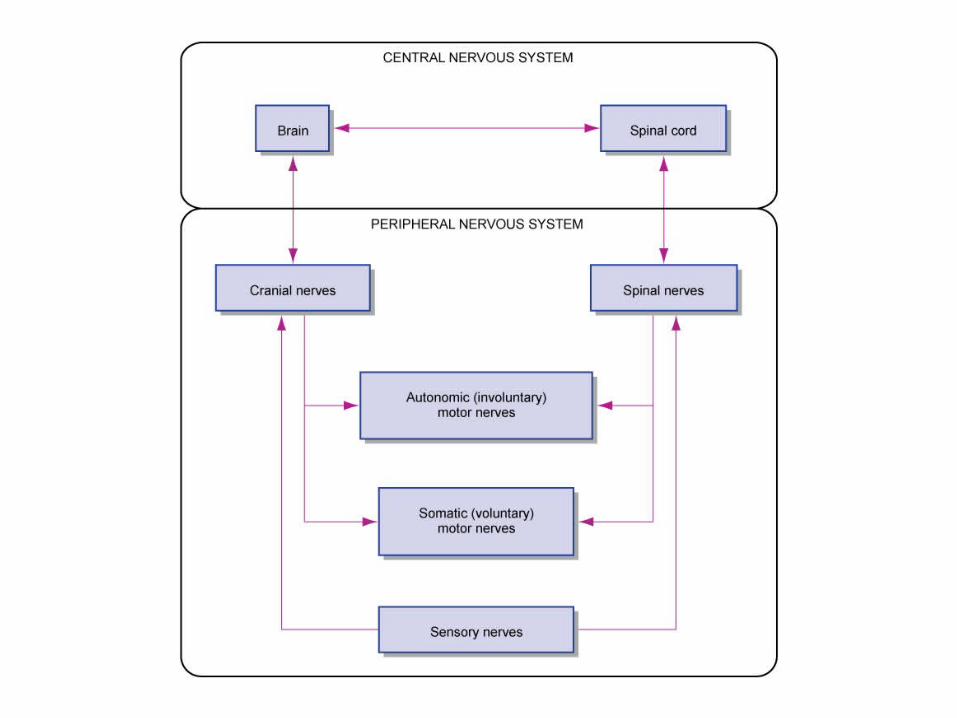
• This intricate network has 2 main divisions:– Central Nervous System– Peripheral Nervous System

Nervous System DivisionCentral nervous system (CNS)
• Brain and spinal cord (body’s control center)
Peripheral nervous system(PNS) • Contains cranial and spinal nerves that
connect to CNS to remote body parts which relay and transmit messages
• Somatic nervous system– Sends messages from the CNS
to the skeletal muscles; voluntary
• Autonomic nervous system– Sends messages from the CNS
to the smooth muscle, cardiac muscle and certain glands; involuntary. Includes the sympathetic and parasympathetic
*note: a & i are vowels

CNS
• Brain is composed of gray and white matter.
• Gray matter is the outside which contains billions of neurons.
• The white matter make up the inner structure of the brain contains pathways that transmit nerve impulses to different areas of the brain.
• The brain and spinal cord are protected by the bony skull and vertebre, CSF and three membranes:– Dura mater– Pia mater– Arachnoid mater

Dura mater,Pia mater, Arachnoid mater
• Dura mater – a tough fibrous, leatherlike tissue composed of two layers.
• Inner lining/ layer of the skull
• Thick layer which covers the brain and provides support and protection
• Pia mater- connective tissue that covers and contours the spinal tissue and brain.
• Arachnoid mater- thin, fibrous membrane that hugs the brain and spinal cord, though not as preciously as the pia mater.

The Spaces Between
• Between the dura mater and arachnoid membrane is the subdural space
• Between the pia matter and the arachnoid membrane is the subarachnoid space.
• Within the subarachnoid space and the brain’s four ventricles is CSF, a liquid composed of water, and traces of organic material (protein, glucose, and minerals.
• The fluid protects the brain and special tissue from jolts and blows

CNS
• Cells of the nervous system– Neuron (fundamental
unit of the nervous system)
– Delicate threadlike nerve fibers called axons and dendrites that extend from the cell body

CELLS OF THE NERVOUS SYSTEM
• Neurons (Nerve Cell)– Consist of three main
parts—dendrites; cell body of neuron; and axon
• Dendrites conduct impulses to cell body of neuron
• Axons conduct impulses away from cell body of neuron
• Most neurons have multiple dendrites but only one axon.
• Gap between each neuron is a synapse and neurotransmitters conduct impulses through the gap
• Neurotransmitters: acetycholine, norepinephrine, dopamine, serotonin

Nerve Cell

Myelin and Nerve Structure

Brain Hemispheres
• The cerebrum is divided into right and left hemispheres
• The right side controls the left side of the body
• The left side controls the right side of the body
“Right Controls the Left, and the Left Controls the Right”

Brain Hemispheres
• Right Hemisphere-
perception, physical environment, art, music, spiritual, non-verbal communication
• Left Hemisphere-
Analysis, interpretation,
calculation, problem solving, writing, and reading

Spinal Cord
• 17 to 18 inches long is a 2 way conductor pathway between the brain and peripheral nervous system.
• Spinal cord conducts impulses to and from the brain, serves as a center for reflex action
• 31 pairs of spinal nerves originate from the spinal cord to the body
• The spinal cord has an H shaped appearance called horns. (gray mater)
• These horns contain the cell bodies of neurons needed for voluntary reflex action

Gray mater cell bodies

CSF
• 500 milliliters are produced daily
• CSF absorbs shock and bathes the brain
• The nutrients (protein, glucose, Na+urea) are delivered to the CNS cells
• Toxic and waste products are removed.


NERVES AND TRACTS
• Nerve—bundle of peripheral axons– Tract—bundle of central
axons– White matter—tissue
composed primarily of myelinated axons (nerves or tracts). Transmits nerve impulses to different areas of the brain.
– Gray matter—tissue composed primarily of cell bodies and unmyelinated fibers
• Nerve coverings—fibrous connective tissue– Endoneurium—surrounds
individual fibers within a nerve
– Perineurium—surrounds a group (fascicle) of nerve fibers
– Epineurium—surrounds the entire nervea


CENTRAL NERVOUS SYSTEM
• Divisions of the brain Brainstem
• Consists of three parts of brain; named in ascending order: the medulla oblongata, pons, and midbrain
• Structure—white matter with bits of gray matter scattered through it
• Function—gray matter in the brainstem functions as reflex centers (e.g., for heartbeat, respirations, and blood vessel diameter)
– Sensory tracts in the brainstem conduct impulses to the higher parts of the brain
– Motor tracts conduct from the higher parts of the brain to the spinal cord

Peripheral Nervous System
Somatic Nervous
System
• Connects CNS to skin and skeletal muscles
• Conscious activities (walking, exercise)
Autonomic Nervous
System• Connects CNS to
visceral organs (e.g. heart, stomach, GI, and other viseral organs)
• Unconscious activities (breathing)


ANS
• Sympathetic System • Parasympathetic System
See pg 1064Table 38-2

ANS
• Sympathetic nervous system increases heart rate, blood pressure, dry mouth
• Fight or flight system
• Parasympathetic slows the system for normal function
• Decreases heart rate, decreases blood pressure..
NEUROLOGICAL ASSESSMENT
• History
• Cerebral function
• Cranial nerve function
• Motor function
• Sensory function
• Reflexes

Nursing assessment
• History of incident or accident headaches, changes of vision, seizure activity,numbness or tingling in an extremity, mood changes, personality changes, fatigue,
• pupil size and reaction, level of consciousness, perception, speech, lethargy, motor coordination, proprioception

Cerebral Function Assessment
Level of consciousness (responsiveness and orientation), most important indicator of change in LOC..
1. Call pt by name2. If no response… touch
pt gently or shaking shoulder
3. If no response…. use strong stimulation (e.g. nail bed pressure)
• To document use Glasgow Coma Scale or document pts state of arousal
• Alert• Disorientation• Lethargic• Obtunded• Stuporous• Semiconcious• Comatose

Glasgow Coma Scale• Scale of responses to eye
opening, motor response and verbal response with a number for each
• Eyes open: 4- spontaneous 3- to speech 2- to pain 1- none
• Best verbal response: 5- obeys commands 4- confused 3- inappropriate 2- incomprehensible
• 1- none• Best motor response: 5-
obeys commands 4- localizes pain 3- flexion to pain 2- extension to pain 1- none
• Total 3 to 15
• <7 is considered a comatose state
• It is important to monitor any downward trend in the patients score. If this happens, the nurse must act quickly, call MD and assist with measures to prevent or reduce ICP and prevent further brain damage..

Cerebral Function Assessment
Mental status (e.g., Mood, behavior, facial expressions, gestures)
Intellectual function (e.g., concentration and recall)
• repeating numbers-recall • adding small numbers -
calculation• last meal eaten
• Short term memory=repeating 3 numbers stating what was eaten for last meal
• Long term memory=school attended time served in the military
• concentration• general knowledge
repeating recent news information

Cerebral Function AssessmentEmotional status
(affect).
Pupillary reaction (size and equality)
Cerebral Function Assessment
PERRLA:• Pupils• Equal• Round• Reactive
– Brisk– Sluggish– Non-reactive– consensual
• Accommodation normal findings– Distance= dilation– Close up=
constriction
Cerebral Function Assessment
Oral and written communication.
Vocabulary used-Aphasia: no speechSensory aphasia:
Receptive aphasia inability to comprehend the spoken or written word
Motor aphasica: Expressive aphasia inability to use words or symbols
Global aphasia: inability to understand the written word or to speak
Anomia: inability to name objects
Dysarthria: difficult speech

Cranial Nerve Function Assessment
• a reflection of brain stem activity, is usually assessed by a physician or advanced practice nurse.
• See “Understanding Cranial Nerves” handout provided.


Motor Function Assessment
• Muscle size and symmetry– Compare bilaterally
• Muscle tone– Normal, flaccid
(hypotonic), rigid (constant stae of spacicity), spastic (rigid, may have tremors)
• Muscle strength– 0 to 5 (see next slide)– Push against resistance
• Coordination– Cerebellum functioning– finger to nose (38-6) – run heel of foot down
opposite shin (38-7)– Ataxia is the inability to
perform voluntary muscle function

Muscle Strength
• 5/5 strong
• 4/5 fair to moderate strength
• 3/5 just able to overcome gravity
• 2/5 can move but not overcome gravity
• 1/5 minimal power strength
• 0/5 no movement

Finger to nose with eyes closed

Coordination using heel slide

Motor Function Assessment• Balance
– Romberg test
1. Eyes closed
2. Feet together
3. Arms extended in front
Slight swaying is normal use safety precautions (stand in front of pt)and prevent falls
• Posturing
– Decorticate posturing: of arms and legs rigid plantar flexion
– Decerebrate: rigid extension of arms and legs with wrists turned outward
– Flaccid weak, lack muscle tone
– Spastic sudden involuntary movement


Sensory Function Assessment
• Tactile Sensation use cotton ball on arms, hands, feet, legs bilat.
• Pain and temperature transmit on same pathway. Use safety pin dull sharp
• Vibration tuning fork feel vibrations on wrists and ankles
• Proprioception space position in regard sto joints. Passively move pt fingers or extremities and ask direction moved to pt. – Unilateral neglect
individual ignores one side of body
– Hemianopia defect in vision blind in ½ vision field

Vibration

Sensory Function Assessment
• Sterognosia: recognition of objects comb, pen, pencil, coin, keys…. with eyes closed (sensation a function of brain not pathways)
• Graphesthesia: recognize letters drawn on the palm of the hand with eyes closed
• Integration of sensation: two point discrimination touching 2 points on opposite sides of the body at one time with a distance between the points.– Have pt give # of times
touched

Stereognosis
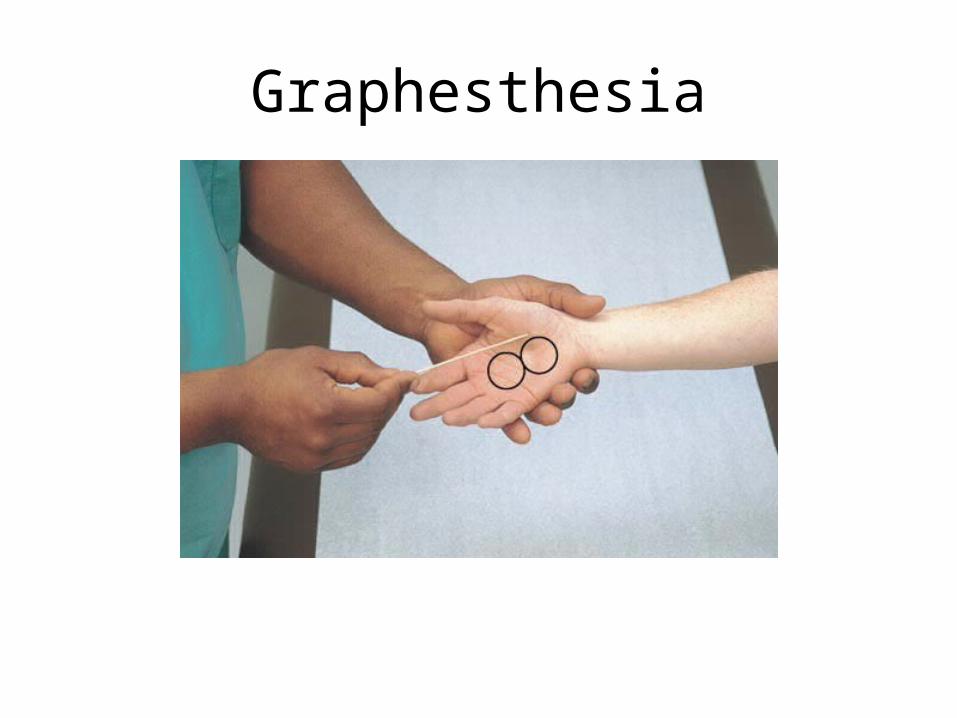
Graphesthesia

Reflex Assessment• Deep tendon reflexes
are usually assessed by a physician or advanced practice nurse.
• Superficial- on the skin as the plantar reflex or Babinski negative in adults can use reflex hammer handle, finger, pen
• Deep tendon reflexes patellar or knee jerk reflex normally intact –stretching near the insertion site of the muscle not present indicates motor or sensory dysfuynction
• The abscemce of DTR’s is considered abnormal

+ Babinski
• A fanning of toes and dorsoflex of big toe
• Indicates a corticospinaldiseaes and is the most important abnormal superficial reflex
•

Babinski Reflex Possible Causes
• Generalized tonic-clonic seizure (there may be a temporary Babinski's reflex for a short time after a seizure)
• Amyotrophic lateral sclerosis
• Brain tumor (if it occurs in the corticospinal tract or the cerebellum)
• Familial periodic paralysis
• Friedreich's ataxia • Head injury
• Hepatic encephalopathy • Meningitis • Multiple sclerosis • Pernicious anemia • Poliomyelitis (some
forms) • Rabies • Spinal cord injury • Spinal cord tumor • Stroke • Syringomyelia • Tuberculosis (when it
affects the spine)

Aging/Prevention of Problems
• Slower reflexes• Tremors that increase
with fatigue• Decreased sense of
touch, fine motor coordination decreases
• Takes longer to learn.. Chronic diseases cause chronic pain and interfers with movement
• Reduce factors as high blood pressure, smoking, obesity, stress, lack of exercise, control heart disease
• History: assess =headaches, loss of function, visual changes, seizure activity, numbness or tingling in extremity, pain, change of personality
Tests
• Arterial blood gas (o2 content Guillain-barre)
• Urinalysis (Diabetes Insipidus)
• Cerebral spinal fluid (infection lower glucose in infection blood)
• CT (with or without contrast takes 20-30 min to an hour person must lie still and have no allergy to iodine invasive procedure and consent required)
• Brain scan (detect brain abnormalities)
• mri• Angiography(Angiogram
for vascular abnormalities dye injected and takes 2-3 hours bedrest for 4-6 hours post test vital signs q 15 min post test and neurological check )

Tests
• Carotid doppler (technology usually of carotid artery to detect carotid blockage)
• Electromylogram( for nerve conduction as in Myasthenia gravis)
• Echoencephlogram (for intracranial brain structure detect intracranial structureshave pt brain-shampoo hair to remove gel
• MRI magnetic resonance imaging (use of a magnetic force)
Mini Neuro Assessment
• Speech, squeeze hands equally, raise forearms against resistance, pupil size and reaction to light, push against nurses hands equally with feet,raise feet against resistance orientation to person, place, time and environment and notate response.
MR F COP

Prevention of Disorders
• Avoid drugs and alcohol, wear seat belts, safe swimming practice, treatment for iv drug abuse to prevent hiv transmission prompt treatment of ear and sinus infection to prevent brain infections

Head Injury
• Scalp injuries bleed profusely to blood vessels in the scalp wound is cleaned and irrigated, object removed if present and scalp is sutured
• Skull Injuries fractures are common
• Open- dura matter is torn
• Closed- dura matter is not torn Symptom of fracture is pain

Head Injury Skull Fx
• TYPES: – Linear a line fracture – Comminuted the bone
is broken into multiple fragments
– Depressed when bone depressed into the tissue or intracranial cavity
– Basilar**Basa the bones at the base of the skull…dura matter may be torn with cerebral spinal fluid leaking from ears or nose. The internal carotid and cranial nerves may also be damaged

Battle's Sign - Behind the Ear Skull fractures are common
in children and result from accidents (the majority are automobile or auto/bike accidents) or abuse. Battle's sign is seen several days following a basilar skull fracture. There may have been bloody drainage from the ear immediately after the fracture occurred.
Basilar fractures are concerning secondary to proximity of the fragile sinus bones and adhesion of the dura mater to this area..

Skull Fracture
• Although the skull is tough, resilient, and provides excellent protection for the brain, a severe impact or blow can result in fracture of the skull and may be accompanied by injury to the brain. Some of the different types of skull fracture include:
Indications of Head Injury
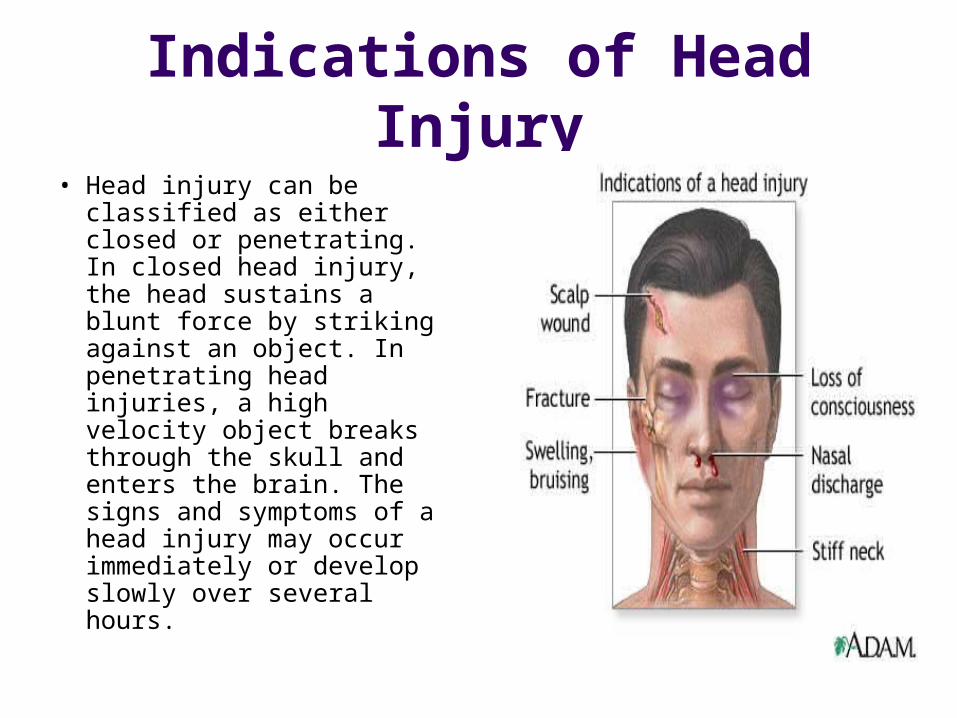
• Head injury can be classified as either closed or penetrating. In closed head injury, the head sustains a blunt force by striking against an object. In penetrating head injuries, a high velocity object breaks through the skull and enters the brain. The signs and symptoms of a head injury may occur immediately or develop slowly over several hours.


Open Brain Injury
• Injury as skull fracture can hemorrhage from the nose, pharynx, ears, or ecchymosis over the mastoid area
• Battle’s sign or blood in conjunctiva cerebral spinal fluid can leak from the nose or ears CT or MRI done to determine extent of injury
•
• Deficits depend on area and extent of injury

Closed Brain Injury
• Caused by blunt force to the head
• Concussion: transient deficits caused by shaking the brain
• Coup: impact of head against an object
• Countercoup: impact of brain against the opposite side of the head
• Contusion: surface bruises of brain often unconscious for longer period than concussion, or drift back and forth from conscious to unconscious Laceration: tearing of cortical tissue manifestations deep coma from time of impact, extension posturing, autonomic dysfunction, nonreactive pupils,.


Concussion
• A concussion may result when the head strikes against an object or is struck by an object. Concussions may produce unconsciousness or bleeding in or around the brain, momentary loss of reflexes, resp arrest for several seconds, amnesia before and after the event
Concussion

Hemorrhage
• Epidural hematoma• Decreased in Neuro
status, HA’s, seizures, hemparesis
• Stop the bleeding and evacuate the clot

Subdural Hematoma
• Bleeding in subdural space
• May be acute, subacute, or chronic
• Manifestations: headache, drowsiness, confusion
• Small hematoma may be absorbed
• Large hematoma needs surgical removal

Subarrachnoid
• Below the arrachnoid• Manifestations: nuchal
rigidity, stiffness, inability to bend neck, blood in subarrachnoid space
• --Increased intracranial pressure
• Intracranial hematoma with contusion in temporal or frontal lobes
• DecreasedLOC, pupil change, VS change

Intracranial Pressure
• Etiology: bleeding trauma
• Causing: increasing pressure and pressure on the brain stem
• Movement of pressure is supratentorial and can result in brain herniation --pressing down on brain stem
• Manifestations: equal pupils are no longer equal one is larger or dilated or blown (fully dilated), decreasing heart rate, widening pulse pressure and dilating pupil/s, decreasing level of consciousness
• Report to MD immediately),



Abnormal Posturing
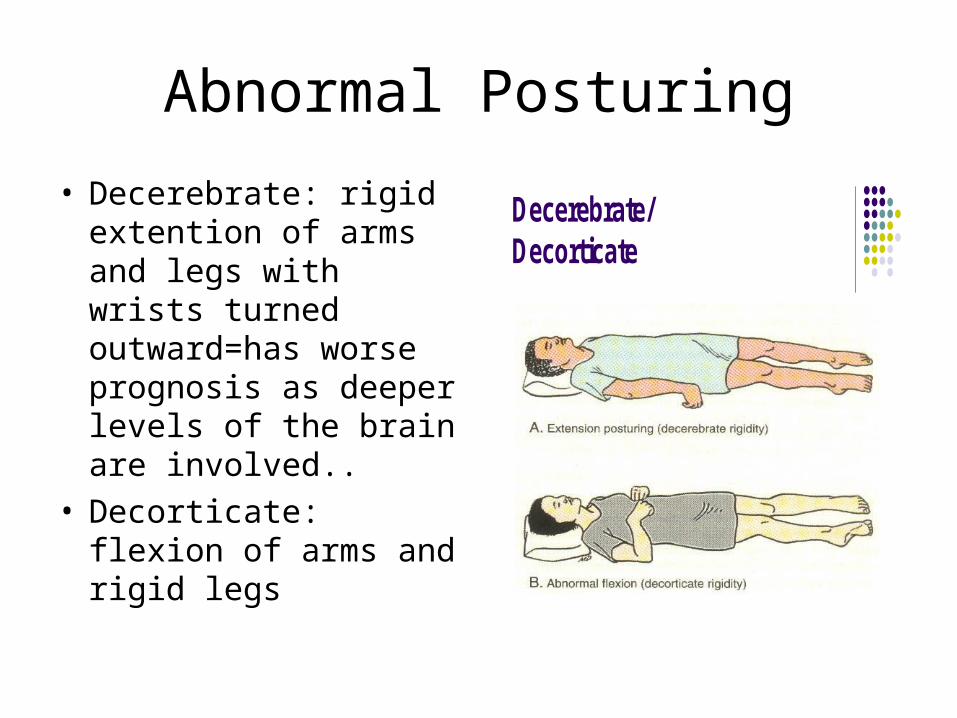
• Decerebrate: rigid extention of arms and legs with wrists turned outward=has worse prognosis as deeper levels of the brain are involved..
• Decorticate: flexion of arms and rigid legs
Decerebrate/Decorticate

Brain Injury
Management: • Reduce intracranial
pressure • Stabilize VS• Keep temperature stable. • Oxygen• IV fluids- osmotic
diuretics (Mannitol) to rapidly reduce fluid in brain tissue
• Corticosteroids (Decadron) to reduce cerebral edema…
• Neuro checks• Foley• Suctioning may be
necessary but is never done in the nose on a head injury because it could possibly be CSF leakage..

Intracranial Pressure Catheter

BRAIN TUMOR
• Space-occupying intracranial lesions, either benign or malignant.
• Symptoms differ according to area of lesion and rate of growth.
• Manifestations are relative to the functions of areas involved (e.g. visual problems resulting from occipital lobe tumors)
• Management is based on tumor type, growth rate, and assessment of client.
• Also radiation, surgery, chemotherapy

CEREBROVASCULAR ACCIDENT (CVA)
• A “brain attack.”• Can be caused by
ischemia from a thrombus, embolus, severe vasospasm, or cerebral hemorrhage.
• Causes neurological deficits of sensation, movement, thought, memory, or speech.
• Loss of function: temporary or permanent.
• Transient ischemic attacks (TIAs) are mini strokes
• Caused by temporary impairment of blood flow to the brain..
• Loss of motor or sensory function may last from a few seconds to minutes to 24 hours..

Stroke


CVA/TIA
Documenting clinical manifestations
• Hemiparesis: weakness of one side of the body
• Dysarthria: difficulty in speaking
• Emotional lability: unstable fluctuating
• Homonymous Hemianopia: defect or blindness in half of the visual field
• Agnosia: total or partial loss of ability to recognize familiar objects or people
• Unilateral neglect: unaware of one side of body
• Teach modification of risk factors
• Have B/P checked annually

CVA/TIA Management
• Airway maintenance and supportive therapy during the first 24 to 48 hours.
• Depending on the location of the CVA and the extent of neurologic deficit, collaboration with physical, occupational, and speech therapists for client to reach the optimal functional level of recovery.
• Ca Channel blockers help to dilate blood vessels and increaese cerbral perfusion
• B/P meds to control • Anticoagulents to
prevent bllod clots• Thrombolytics to
dissolve clots
CVA/TIA Management (cont)
• Fluids may be restricted• IV fluids or tube feedings
given (gag reflex needs to be checked before po foods are given)
• If embolic or thrombolic stroke HOB is kept flat to increase cerebral perfustion
• If hemorrhagic stroke HOB is elevated to decrease cerebral perfusion (reduces swelling)
• Footboard• PROM to affected
side



















