Embed Size (px)
Citation preview

NEURORADIOLOGY IN MS DIAGNOSIS AND TREATMENT
MONITORING
This report is from a Biogen organised and funded meeting that occurred at the Royal Society of Medicine, London, 5th October 2017

2
Magnetic resonance imaging (MRI) aids the diagnosis and follow up of people with multiple sclerosis (MS). For instance, MRI can help exclude differential diagnoses, assess the efficacy of disease modifying therapies (DMTs) and screen for potentially serious complications. However, there is a lack of consistency in MRI protocols across the UK, which hinders clinicians’ ability to compare images and potentially delays treatment.
In 2017, a group of neurologists, neuroradiologists and other healthcare professionals attended a meeting organised and funded by Biogen at the Royal Society of Medicine, chaired by Dr Klaus Schmierer from the Royal London Hospital, to discuss the state of the art of imaging in MS. The meeting discussed some clinical conundrums, reviewed the place of imaging in MS management, debated the benefits of automated registration and introduced new imaging technologies. The meeting also took the first steps toward developing UK guidelines. This newsletter summarises some of the meeting’s highlights.

3
HOW WELL DO MRI-DETECTED FEATURES OF MS MAP ONTO ITS PATHOLOGY? THE CHALLENGE OF DIAGNOSING MS EARLY AND ACCURATELY
Dr Klaus Schmierer, Reader in Clinical Neurology and Consultant Neurologist, Royal London Hospital
MS is a chronic progressive disease associated with slightly reduced life expectancy,1 increased rates of suicide,2 divorce3 and unemployment 4 as well as poor cognition.5
Inflammatory demyelination is an important determinant of axonal loss throughout the course of MS. So, reducing the immune reaction that drives inflammation is the cornerstone of management.
The efficacy of current MS immunotherapies reflects the extent to which the drug contains immune effector cells in the peripheral bloodstream and, in turn, depletes memory B cells in the CNS.6, 7
A new understanding of MS pathophysiology underscores the importance of early diagnosis and rapidly starting effective treatment to maximise brain health.
SU
MM
ARY
MS is a chronic progressive disease that is driven by inflammation throughout its natural history. “Inflammation can cause the loss of thousands of axons and the capacity to repair the damage declines over time,” Dr Schmierer said. “Spontaneous repair [remyelination] occurs, but usually the condition of the person with MS deteriorates, particularly when left untreated.”
MS is associated with numerous adverse outcomes, including a reduction in life expectancy,1 in part because the suicide rate is higher in people with MS than among the general population.2 The divorce and unemployment rates are also higher in people with MS compared to the general population.3, 4
The loss of CNS axons undermines cognition. Indeed, the decline in cognitive performance can emerge early in the natural history of MS and, Dr Schmierer added, may affect work capacity and contribute to unemployment. Feuillet et al, for example, compared the cognitive performance of 40 people with clinically isolated syndrome
(CIS) and 30 matched healthy controls. 57% of the people with CIS and 7% of the healthy controls showed impaired cognition.5 “This study illustrated that in people with MS, deficits in memory, speed of information processing, attention and executive functioning can occur even without significant physical disability,” Dr Schmierer said.
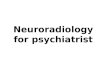
The loss of brain tissue and volume (atrophy), which is typical of MS and is visible on MRI, reflects neuronal loss. “Brain atrophy occurs at all stages, even CIS,” Dr Schmierer remarked (figure 1).8 “There is a misconception that inflammation ceases in the later stages of MS. But we now know that inflammatory demyelination makes an important contribution to axonal loss at all stages of MS.”

4
Approximately 60% of people with MS eventually show axonal loss in the spinal cord, which is visible on histology. “The loss is apparent throughout all levels of the spinal cord,” Dr Schmierer commented. “Spinal cord demyelination especially affects the grey matter, but the white matter is also affected.” In fact, the loss in axonal density below a spinal lesion (42%) is similar to that in the plaque (48%) suggesting anterograde (Wallerian) degeneration.9
Against this background, treatment with the aim of ‘No Evidence of Disease Activity’ (NEDA) - in other words, no relapses, no sustained disability progression and no MRI activity - aims to suppress the inflammation so that there is no axonal loss. This requires active monitoring with a re-baselining MRI after the DMT has had time to work. Patients should also receive at least one MRI scan annually to monitor for subclinical relapses.10
Attaining NEDA depends on reducing the immune reaction that drives the inflammation, although imaging techniques do not capture the subtleties of the immune reaction. In particular, current effective MS immunotherapies deplete memory B lymphocytes.6 Indeed, the efficacy of MS treatments reflects the extent to which the drug contains immune effector cells in the peripheral bloodstream and, in turn, depletes memory B cells in the CNS. Conversely, drugs that enrich B cell populations in the CNS – such as atacicept and infliximab – are associated with an increased risk of demyelination and relapses in people with MS.6, 7
Dr Schmierer added that infection with Epstein-Barr virus (EBV) is a risk factor for MS. Memory B cells are a reservoir for latent EBV infection.6
Therefore, depleting memory B cells removes the EBV reservoir as well as being anti-inflammatory.
Further evidence supporting the role of B cells in MS has emerged from studies investigating the pathology of white matter lesions, which are associated with demyelination, perivascular inflammation and activated microglia cells. The disruption to the blood brain barrier (BBB) results in perivascular inflammation – the so-called central vein sign (CVS), discussed later in this newsletter. The BBB disruption, in turn, facilitates clustering of B and T cells in brains affected by MS. Indeed, the chronic inflammation generates ectopic lymphoid tissue with a germinal centre – the area where B cells proliferate and develop.11 “The germinal centres are probably important in driving MS pathology,” Dr Schmierer said. “In the future, measuring memory B lymphocyte populations may offer a biomarker that could reduce the need for MRI monitoring.”
Once inflammation subsides, the brain’s repair mechanisms lead to remyelination, although this is difficult to detect with current imaging techniques. The magnetisation transfer ratio (MTR; discussed later in this newsletter) may offer one approach.12, 13
“MS is progressive from day one,” Dr Schmierer concluded. “Immune-mediated demyelination is a key determinant of the progressive axonal loss, even in the later stages of MS. In particular, memory B cells link clinical observations, immune phenotyping and the biology of MS. This new understanding of MS pathophysiology underscores the importance of early diagnosis and rapidly starting treatment to maximise brain health.”
Figure 1: Brain atrophy is present at all stages of MS8
Adapted from De Stefano N, et al Neurology 2010;74:1868-76
PB
VC /
yea
r co
rrec
ted
for
base
line
NB
V 0.4 CISn = 157
RRMSn = 579
SPMSn = 139
PPMSn = 88
0.2
0.0
-0.2
-0.4
-0.6
-0.8
-1.0
-1.2
-1.4 n = 963 pwMS

5
* Subsequent to this meeting, further revisions of the McDonald
criteria have been published.
Please see Thompson et al.,
Lancet Neurol 2018;7:162–73
for further information.
A BRIEF HISTORY OF DIAGNOSTIC CRITERIA FOR MS
Dr Klaus Schmierer, Reader in Clinical Neurology and Consultant Neurologist, Royal London Hospital
Since Jean-Martin Charcot described his eponymous neurologic triad in 1868, various groups have developed diagnostic criteria for MS. Over the years, the criteria evolved to reflect neurologists’ greater understanding of MS and advances in imaging.14
Dissemination in time (DIT) and dissemination in space (DIS) as well as the exclusion of differential diagnoses are consistently important diagnostic principles.
Recently updated criteria did not distinguish between symptomatic and asymptomatic MRI lesions in terms of DIS and DIT.* 15
Future guidelines will probably include the central vein sign (CVS).
SU
MM
ARY
In 1868, Jean-Martin Charcot described his eponymous neurologic triad of nystagmus, intention tremor and scanning speech that he apparently observed in his housemaid. While these are some of the typical clinical signs of MS, the housemaid turned out to have Friedreich’s ataxia. Charcot’s neurologic triad represents features that are characteristic of MS rather than formal pathognomonic criteria that allow diagnosis.
In 1931, Sydney Allison segregated people with disseminated sclerosis – the term then used for MS in the UK – into four groups:
Typical cases of disseminated sclerosis. Early cases in which disseminated sclerosis is the probable diagnosis.
Deceased or untraceable patients: diagnosed based on clinical history.
Doubtful cases: people with inconclusive symptoms and signs.
John Millar proposed the first ‘proper’ diagnostic criteria in 1954, which differentiated three groups:
Early: Patients with a history of symptoms that are commonly associated with MS.
Probable: Patients who show some physical disability. The symptoms usually show a remitting quality. The physical signs are explicable only based on MS.
Possible: Patients show symptoms that suggest MS.
The Millar criteria indicated that DIT was a diagnostic consideration. DIS, however, “was only hinted at,” Dr Schmierer said. Moreover, the authors stated that the criteria were suitable for use by experienced neurologists only and were inappropriate for epidemiological surveys performed by less experienced staff.

6
During the 1960s, Charles Poser aimed to determine the accuracy of MS diagnoses in epidemiological surveys using clinical vignettes based on: MS confirmed on autopsy; MS and another CNS disease; and patients who did not have MS. Poser asked neurologists to classify each case as probable, possible or unlikely, without specifying the criteria. Poser received responses from 108 neurologists in 33 countries. Depending on the vignette, between 2.8% and 98.2% of neurologists correctly identified the confirmed cases as probable MS. However, between 1.9% and 14.8% incorrectly identified the non-MS cases as probable MS and 13.9% incorrectly identified a case of lung cancer without metastases as probable MS.16 The study underscored the need for robust diagnostic criteria.
Meanwhile, Tore Broman outlined the principles that formed the basis for subsequent diagnostic criteria. Broman’s 1965 criteria, published in the Annals of the New York Academy of Sciences, suggested that neurologists should consider age of onset, the number of lesions and exacerbations, and any family history of MS. The criteria stressed the empiric significance of symptoms for an MS diagnosis, introduced antibodies in the cerebrospinal fluid (CSF) and exclusion of alternatives into the criteria and articulated the diagnostic importance of DIT and DIS clearly for the first time.
In the same issue of the Annals of the New York Academy of Sciences, a group led by George Adam Schumacher defined the criteria for ‘clinically definite MS’. These stipulated that the patient must show objective signs of CNS dysfunction. Symptoms alone were not an acceptable basis for MS diagnosis. The criteria also included DIS – evidence of damage to at least two sites – and DIT (eg at least two episodes of at least 24 hours separated by at least 6 months). In addition, the Schumacher criteria stressed that to diagnose MS the signs should not be explicable by any other disease.17
The next major revision followed in 1983.18 “The Poser criteria made the diagnosis of MS much clearer,” Dr Schmierer said. Moreover, the Poser criteria included paraclinical criteria, such as evoked potentials and imaging:18
MRI had been introduced in 1981.14 The scheme stratified patients into:
Clinically definite MS. Laboratory supported definite MS. Clinically probable MS. Laboratory supported probable MS.
An exacerbation could consist of symptoms alone, but had to last at least 24 hours. Remission had to last at least 1 month. The new laboratory supported category specifically referred to evidence of oligoclonal bands, increased IgG in the CSF (and not in serum) or both. The Poser criteria raised the “acceptable age of onset” from 50 years in Schumacher’s version to 59 years.18
In addition, the Poser criteria strongly recommended that a neurologist should establish the diagnosis and stressed the importance of excluding differentials. Dr Schmierer, however, pointed out a major weakness: the criteria did not incorporate primary progressive MS, which accounts for 10-15% of MS cases.18
In 2001, Ian McDonald lead a group that developed criteria that stressed the importance of DIS, DIT and excluding other causes.19 The McDonald criteria were revised in 2010 and included primary progressive MS. This iteration also simplified the imaging needed to demonstrate DIS and DIT. To meet the DIS criteria, for example, at least one T2 lesion had to be present in at least two of the four CNS areas: periventricular, juxtacortical, infratentorial and spinal cord. Gadolinium enhancement is not required to demonstrate DIS.20
In 2016, Magnetic Resonance Imaging in Multiple Sclerosis (MAGNIMS), a European research network, published criteria that importantly did not distinguish between symptomatic and asymptomatic MRI lesions in terms of DIS (defined as at least two of five areas of the CNS) and time (table 1). Brainstem or spinal cord syndrome and optic neuritis, contribute to lesion count. In addition, the guidelines noted the need to exclude other causes of MRI white matter lesions, which include ageing and cerebrovascular disease.* 15
* Subsequent to this meeting, further revisions of the McDonald
criteria have been published.
Please see Thompson et al.,
Lancet Neurol 2018;7:162–73
for further information.

7
Dr Schmierer speculated that future guidelines could include the CVS: a blood vessel visible on MRI inside a white matter lesion. The CVS seems to be a biomarker for inflammatory demyelination in the brain.21 FLAIR* images the CVS by combining T2-weighted fluid-attenuated inversion recovery (FLAIR) contrast, which images white matter lesions, and T2*-weighted contrast, which reveals parenchymal veins, on a single image.22
Since Jean-Martin Charcot described his eponymous triad in 1868, diagnostic criteria have evolved to reflect advances in the understanding of MS and imaging.14 Indeed, on-going advances mean that the guidelines are likely to be revised further.
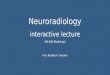
Table 1: Proposed MAGNIMS criteria suggest that involvement of at least two of the CNS shown demonstrates DIS
Adapted from Filippi M, et al Lancet Neurol 2016;15:292–303.
≥ 3 periventricular lesions
≥ 1 infratentorial lesion
≥ 1 spinal cord lesion
≥ 1 optic nerve lesion
≥ 1 cortical/juxtacortical lesion (involvement of the white matter next to the cortex, involvement of the cortex or both)

8
STANDARDISING MRI PROTOCOLS FOR MS DIAGNOSIS AND FOLLOW-UP ACROSS THE UK – WHAT IS THE RIGHT STANDARD?
Dr Audrey Sinclair, Consultant Neuroradiologist, St George’s Hospital, London
MRI is the most sensitive tool currently available for monitoring inflammation in MS. However, there is a need for a standardised MRI protocol in the UK.
Accurately assessing whether a person with MS has developed new lesions depends on comparing good-quality MRIs with similar parameters and orientation. Comparing non-standardised MRI examinations that use different sequences is difficult. The lack of standardisation can delay treatment decisions.
Dr Sinclair proposed developing new guidelines based on existing guidelines from other countries as basis, but tailored to the UK.
The proposed UK guidelines should cover diagnosis, re-baselining, cord imaging and follow up as well as recommendations for requisition information and reporting.
SU
MM
ARY
MRI remains the most sensitive tool to monitor inflammation in MS. As such, MRI is the cornerstone of diagnosis in people with CIS or radiologically isolated syndrome (RIS). MRI is also invaluable for the follow up of people with confirmed MS to assess new or enlarging lesions, determine brain volume and screen for certain complications associated with DMT.
“Accurate assessment for new lesions depends on having good-quality MRIs with similar parameters and orientation that allow comparison,” Dr Sinclair said. “In practice, however, we often need to compare non-standardised MRI examinations, which is difficult.” Indeed, recent American guidelines stress the importance of using a standardised MRI protocol with similar orientation and other parameters to detect new lesions reliably.23 Dr Sinclair suggested that there is a need for guidelines outlining standardised MRI protocols tailored to the UK.
Numerous protocols for brain and spinal cord imaging are currently used in the UK (table 2) to facilitate diagnosis by, for instance, showing DIS and DIT, and revealing lesion characteristics. Typical MS lesions are ovoid or flame shaped and perivenular, which gives rise to the CVS on 1.5T MRI. Lesions are typically perpendicular to the ependyma and show an irregular, “nibbled” appearance on the inferior surface of corpus callosum. Anecdotally, Dr Sinclair commented, lesions form around the temporal horn.

9
Table 2: Protocols for brain and spinal cord imaging
Conventional Quantitative
Spin echo/gradient echo T1, T2, short T2
Axial/ sagittal /coronal T2/T1/ FLAIR Magnetisation transfer
2D/3D Diffusion (tractography)
Diffusion Quantitative susceptibility
Susceptibility weighted imaging (SWI)
MRI also aids differential diagnosis. Dr Sinclair, for example, summarised the case of a 36-year-old patient who presented with a three-month history of headache, confusion, slurred speech and abnormal facial movements that emerged after visiting Jamaica. The MRI revealed neurosarcoidosis. In another case, MRI helped diagnose cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) in a 47-year-old person presenting with episodes of blurred vision.
Nevertheless, Dr Sinclair highlighted the need for standardisation of MRI protocols in the UK. “MRI is the most sensitive tool currently available for monitoring inflammatory disease activity in MS,” she said. “Clinical assessments underestimate disease activity and burden compared with MRI. However, accurately assessing whether a person has developed new lesions depends on having good-quality MRIs with similar parameters and orientation for comparison. Comparing non-standardised MRI examinations that use different sequences is difficult. In some cases, the lack of standardisation delays treatment decisions.”

10
Table 3: Recommendations for MRI sequences23, 24
Consortium of MS Centers Task Force
Core sequences Optional sequences
Anatomic 3D inversion recovery (IR) T1 gradient echo Axial proton attenuation
Gadolinium single dose (0.1 mmol/kg for 30 seconds)Pre- or post-gadolinium axial T1 spin-echo (for chronic black holes)
3D sagittal T2 weighted image (WI) FLAIR SWI for identification of CVS within T2 lesions
3D T2WI b
2D axial diffusion weighted imaging (DWI) (5-mm sections, no gap)
3D FLASH (non-IR prep) post-gadolinium
3D series (eg 1.0-1.5mm thickness); typically reconstructed to 3mm for display and comparison of lesion counts
Swedish Multiple Sclerosis Association and the Swedish Neuroradiological Society
Diagnostic protocol Follow-up protocol
3D T1 (Pre-contrast) Gadolinium-based contrast agents
Haemorrhage sensitive sequence (SWI, gradient recalled echo or fast field echo)
Axial T2
DWI 3D T2 FLAIR
Gadolinium-based contrast agents 3D post-gadolinium T1
Axial T2
3D T2-FLAIR
3D T1 (post-gadolinium)
Against this background, Dr Sinclair proposed developing UK guidelines that include a standardised protocol for MRI in MS. She noted that NICE guidelines do not offer detailed advice on specific MRI protocols for diagnosis or monitoring after switching DMT. However, numerous other guidelines - including those published by the Consortium of MS Centers Task Force (CMSC)23 and Swedish Multiple Sclerosis Association and the Swedish Neuroradiological Society24 (table 3) - could form the basis of the UK guidelines.
The CMSC guidelines, for example, stress the importance of taking a good-quality scan (3T or 1.5T) with adequate signal-to-noise ratio and resolution (in pixel ≤1 x 1mm). MRI images should be taken in the subcallosal plane, using ≤ 3mm slice thickness with no gap. This facilitates 2D acquisition or 3D reconstruction.23
Gadolinium-enhancement identifies emerging lesions and helps exclude alternative diagnoses, such as tumours (persistent enhancement) or leptomeningeal diseases, including neurosarcoidosis or infection. The CMSC guidelines recommend waiting for at least five minutes before obtaining a post-gadolinium T1. Imaging for progressive multifocal leukoencephalopathy (PML) surveillance should use 2D or 3D FLAIR and diffusion-weighted imaging (DWI).23 Dr Sinclair noted that post-contrast T1 adds little diagnostic value to PML surveillance. Indeed less than 50% of early PML lesions show gadolinium enhancement.25

11
The CMSC guidelines clarify the role of brain and spinal cord imaging. For example, in people with CIS, suspected MS or both, the guidelines recommend a gadolinium-enhanced brain MRI at baseline. Spinal cord imaging should be considered if:
The MRI shows transverse myelitis. There are insufficient features on brain MRI to support diagnosis.
The patient is older than 40 years of age and shows nonspecific brain MRI findings.
Performing cervical cord MRI simultaneously with brain imaging would reduce the number of people recalled. The guidelines suggest considering orbital MRI in people with severe optic neuritis that show poor recovery.23
The CMSC guidelines recommend follow-up brain MRI after 6 to 12 months for high-risk CIS (eg ≥2 ovoid lesions on first MRI). The interval can be 12 to 24 months for people presenting with low-risk
CIS (ie normal brain MRI) and those with uncertain clinical syndrome with suspicious brain MRI features (eg RIS).23
In established MS, the guidelines suggest considering gadolinium-enhanced MRI when there is no recent image, such as when people transfer to a new clinic. Gadolinium-enhanced MRI should be considered before starting or switching DMT and to establish a new baseline postpartum and about 6 months after switching DMT. Gadolinium-enhanced MRI should be repeated every 1-2 years while taking DMTs to assess subclinical MS activity.23
Against this background, Dr Sinclair suggested elements that could be included in a UK protocol. “We should use the existing guidelines as basis,” she commented. “There’s no need to reinvent the wheel.” Nevertheless, the protocol should be tailored to the UK. For example, many hospitals in the UK do not have a 3T scanner. Therefore, the protocol should be based on 1.5T scanners.
Figure 2: Suggested protocol for diagnosis and re-baselining
Figure 3: Suggested protocol for follow up in MS or CIS
Brain imaging Spinal cord
3D T1 Sagittal T2
3D FLAIRSagittal short tau inversion recovery
Give gadoliniumThick axial T2 through
whole cord (no interslice gap)
Axial T2Sagittal
post-gadolinium T1
Axial DWIAxial post-gadolinium
T1 through any lesions
Axial SWI
3D post-gadolinium T1(5-minute delay)
Brain Spinal cord
Axial T2 Sagittal T2
Axial DWISagittal short tau inversion recovery
Axial SWI Axial T2
3D FLAIR (axial reconstruction
3D T1
Optional: Double inversion recovery, 3D,
axial spin-echo T1
Dr Sinclair proposed that the UK guidelines should include protocols for diagnosis, re-baselining, cord imaging and follow up (figures 2 and 3). She suggested cord imaging only if the person experienced symptoms that could arise from a spinal cord lesion.
Gadolinium enhancement is not generally required for follow up as imaging aims to detect only new lesions. The guidelines could also mention future developments, such as automated lesion counting and automated brain volume measurement.

12
In addition, Dr Sinclair suggested that the guidelines should include recommended requisition information, such as:
The indication (suspected or known MS, CIS or RIS).
Any DMT. The reason for MRI (eg diagnosis, routine follow up, clinical relapse).
The guidelines should outline reporting recommendations (table 4).
Table 4: Suggested reporting recommendations
Diagnosis or 1st MRI
Parts examined, was gadolinium used, sequences
DIS: Location of lesions
Lesion load (eg 0, 1-9, 10-20, ≥20)
Characteristics typical or atypical of demyelination
Radiologically viable alternative diagnosis
DIT: number and location of enhancing lesions
McDonald criteria satisfied or not
Follow up
Disease activity; no evident disease activity or number and location of new lesions
Complications of DMT
Dr Sinclair noted that implementation is the “most difficult part” of guideline development. Translating the guidelines into protocols would also help by offering “clarity, expedience and ease of implementation”. Dr Sinclair proposed involving professional bodies in guideline development supported by local, regional and national engagement and education to aid dissemination and implementation. Finally, she remarked that multidisciplinary team meetings should include radiology.

13
Table 5: Differentiating MS and SVD
Adapted from Barkhof F, et al Radiology Assistant Available at: www.radiologyassistant.nl/en/p4556dea65db62/multiple-sclerosis.html Accessed March 2018
Involvement MS SVD
Corpus callosum Typical Rare
U-fibre Often Rare
Infratentorial Always Late
Temporal lobe Often Never (except CADASIL)
Gadolinium-enhancement Common Never
Asymmetrical Never Possible
Black holes Typical Rare
Cystic lesions Never Lacunes
Spinal cord Frequent Never
MRI TO MONITOR MS: DEBATING WHETHER NEURORADIOLOGIST INSPECTION OR AUTOMATED REGISTRATION IS KEY?
Before the debate, most delegates agreed that inspection of MRI scans by a neuroradiologist was key. However, after a lively debate, most delegates switched their opinion and agreed that automated registration is key. Nevertheless, automated registration cannot always replace an expert eye.
Frederik Barkhof, Professor of Neuroradiology at VU University Medical Centre Amsterdam and University College London, opened the debate by commenting that evaluation by a neuroradiologist was important to establish an early and correct diagnosis using the McDonald criteria. “Making the diagnosis can be difficult,” he said. “For example, ascertaining DIS can be problematic in the spinal cord.”
Evaluation by a neuroradiologist can also differentiate MS from other conditions such as age-related small vessel disease (SVD), vasculitis, infections, metabolic disease and neuromyelitis optica. “To make the diagnosis of MS there needs to be no better explanation,” Professor Barkhof said. “So it is especially important to exclude vascular pathology, such as SVD and macrovascular disease. Almost everyone over the age of 55 years has 1 or 2 bright spots due to SVD, which can complicate the diagnosis.” Professor Barkhof made some suggestions that may help discriminate MS and SVD (table 5), although certain people have both conditions.

14
In addition, acute disseminated encephalomyelitis can show deep grey matter involvement. Sarcoid can exhibit periventricular lesions and meningeal enhancement. Such clinical presentations can complicate diagnosis. “So much depends on the correct diagnosis that a referral to an expert neuroradiologist is important,” Professor Barkhof said.
In addition, neuroradiologist evaluation can monitor treatment efficacy based on new lesions, safety and neurodegeneration. “The protocol is important,” Professor Barkhof said. “Lesions are easy to miss if the protocol is not the same.” In addition, frequent MRI detects preclinical PML, which is associated with better outcomes than late detection. Detecting PML depends, however, on the neuroradiologist’s expertise in detecting subtle MRI findings in, for example, the motor cortex, punctate lesions and enhancement.
“Neurodegeneration is the next target in treatment,” Professor Barkhof said. “But measuring neurodegeneration in MS is challenging.” Normalised brain volume can depend on the patient’s age and other characteristics, for instance. In addition, quantification of brain volume is associated with various absolute scaling errors and the neuroradiologist needs to look for variations in magnets, gradients, coils, distortion correction, all of which may influence the image, as well as changes that affect tissue contrast, such as inconsistent pulse-sequences and imperfect radio frequency tuning. “The technical variability in measurements of brain volume is substantial. Each of these factors can outweigh the atrophy caused by MS,” Professor Barkhof remarked. “Some of these factors induce changes of 1-2%. MS typically induces changes of 0.5% a year.”
Wim Van Hecke, co-founder and CEO of icometrix, countered that automated registration improves the consistency and reliability of MRI reporting. He noted, for example, that in one study the number of MS lesions counted by 84 healthcare professionals varied from 5 to 85 with a median of 16.
Another study asked an expert neuroradiologist and three clinicians to evaluate MRI scans from 85 patients. Agreement on lesion counts was highest for gadolinium-enhancing lesions, intermediate for new T2 lesions and poor for enlarging T2 lesions. MRI activity was classified differently by the clinicians in 18% to 25% of the cases compared with the neuroradiologist or computer program.26 Unpublished data also shows variations in lesion counts when the same MRI is evaluated at different times by the same person.
Dr Van Hecke claims that software is reliable. Lesion load and the count of new and enlarging lesions correlate strongly with the expert evaluation. Moreover, the software reduces reading time between 2 and 10 fold. In one case, both radiologists asked to evaluate a clinical case changed their conclusion when they had software support. Both radiologists felt more confident when supported by the software, which added numbers to the report. The radiologists felt that the reports were more accurate and consistent. The reading time declined from about 15 to 5 minutes.
“Software reduces observer-dependency and measurement error. The standardisation improves patient monitoring and offers better treatment decisions, which improves outcomes for patients,” Dr Van Hecke said. “These benefits are especially important outside of expert centres. Software, however, supports but does not replace the expert eye.”

15
GADOLINIUM DEPOSITION IN THE BRAIN
Dr Tom Campion, Senior Radiology Registrar, Barts Health London
Gadolinium-based contrast agents (GBCAs) enhance diagnostic precision, such as by excluding other pathologies, and facilitate monitoring of safety and disease activity.
While multiple doses of GBCAs are associated with gadolinium accumulation, this has not yet been associated with clinical harm to patients.
Several approaches could reduce reliance on GBCAs in the future.
According to a recent consensus document, GBCAs should be avoided when not necessary. However, GBCAs should not be withheld when clinically indicated.27
The European Medicines Agency (EMA) and the Food and Drug Administration (FDA) recently reviewed the safety of GBCAs. While acknowledging the risk of deposition, the authorities concluded that the benefits outweighed the risks in MS.
SU
MM
ARY
In suspected and confirmed MS, GBCAs enhance diagnostic precision, such as by excluding other pathologies, and facilitate monitoring of safety and disease activity. However, GBCA administration leads to dose-dependent gadolinium deposition in the brain. While gadolinium deposition associated with GBCAs has not yet been associated with clinical harm to patients, Dr Campion stressed the importance of continuing vigilance.
Gadolinium is a rare earth metal with paramagnetic properties at room temperature.
As such, gadolinium selectively shortens T1 relaxation times in tissues. This enhances the intensity of the T1 signal.28 GBCAs cross into the CNS only when the BBB is damaged.29
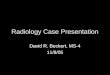
Elemental gadolinium can displace calcium from enzymes and other biological systems, which may be associated with toxicity.30 As a result, GBCAs use a chelated form of gadolinium,29 with either a linear or macrocyclic structure (figure 4).30 Macrocyclic GBCAs show higher kinetic and thermodynamic stability, which reduces the likelihood of dissociation, compared to linear agents.
Figure 4: Examples of linear and macrocyclic gadolinium-based contrast agents
Linear (Gd-DTPA) Macrocyclic (Gadoteric Acid)

16
Nevertheless, a risk of dissociation or transmetallation (where chemical groups transfer between different metals) persists even with macrocyclic GBCAs, although the likelihood of adverse events appears to be relatively low. For example, the linear GBCA gadodiamide entered radiological practice in 1993. The first indication of harm from nephrogenic systemic fibrosis was identified in a subset of patients with end-stage renal disease in a paper published in 2006.31 “Since then, there have been very few cases of toxicity associated with retention of gadolinium and almost none with macrocyclic GBCAs,”
Dr Campion told the meeting.
Despite these reassuring findings, increasing evidence confirms that multiple doses of GBCAs are associated with gadolinium accumulation. McDonald et al, for example, used plasma mass spectrometry, electron and light microscopy to assess gadolinium deposition on autopsy in 13 patients who received GBCAs, mainly for CNS tumours, and 10 controls, most of whom had stroke, dementia or lymphoma. The controls showed undetectable levels of gadolinium. The GBCA group, however, showed dose-dependent accumulation of gadolinium in the dentate nucleus and globus pallidus (compared to the pons and thalamus respectively), capillary endothelium and neural interstitium. The accumulation appeared to be independent of renal and hepatic function.32
A retrospective study compared changes in the signal intensity in the dentate nucleus and globus pallidus to those of other structures on unenhanced T1-weighted MRI in patients who received a linear (gadopentetate dimeglumine) or macrocyclic (gadoterate meglumine) GBCA. The study excluded patients with impaired renal function. The authors reported increased signal intensity in the dentate nucleus and globus pallidus in patients who received the linear GBCA, but not those who received the macrocyclic agent.33 In general, studies using other macrocyclic GBCAs replicate these findings.34
Stojanov et al, however, reported cumulative increases in signal intensity in the dentate nucleus and globus pallidus among people who received multiple doses of the macrocyclic GBCA gadobutrol.35
Against this background, the EMA and the FDA recently reviewed the safety of GBCAs. While acknowledging the risk of deposition, the authorities concluded that the benefits outweighed the risks in MS. Similarly, in a consensus statement, The International Society for Magnetic Resonance in Medicine noted that, in line with standard practice, “use of GBCAs should be avoided when not necessary”. The statement notes, however, that “GBCAs should not be withheld from patients with a clinical indication for gadolinium-enhanced MRI. The physician responsible for the administration of a contrast agent should understand the benefits and risks of the agent.” 27 Dr Campion advocated considering the specific risks associated with the GBCA used in each department and, in particular, considering the merits of a macrocyclic compared to a linear agent.
Further studies, Dr Campion noted, should evaluate long-term outcomes and determine the mechanism underlying gadolinium deposition. Such insights could allow the rational design of newer agents. In addition, surveillance protocols could be rationalised and alternative strategies assessed, such as using DWI and FLAIR to screen for PML. In addition, non-contrast techniques, such as quantitative susceptibility mapping and diffusion tensor-imaging-derived fractional anisotropy, might identify active lesions.36
“More work is needed, but these are potential avenues if there is harm associated with gadolinium,” Dr Campion concluded. “We always need to make a risk/benefit analysis. But we also need to remember that GBCAs offer significant benefits in suspected and confirmed MS.”

17
THE ROLE OF IMAGING IN MS TREATMENT SAFETY MONITORING
Professor Mike Wattjes, Head of Imaging in Neuroinflammation and Neuroinfection, Hannover Medical School, Germany
Pharmacovigilance has three main components: measuring treatment efficacy; predicting treatment responses; and monitoring safety, including detecting comorbidities, opportunistic infections and paradoxical reactions.
Patients with vascular comorbidity at diagnosis reach ambulatory disability significantly earlier than those without.38
Ultrasensitive quantitative real-time polymerase chain reaction (PCR) can detect DNA from John Cunningham Virus (JCV) in the CSF of people with PML.39 CSF PCR can confirm suspected PML, but a negative result cannot be used to rule out PML.
Several MRI protocols aid pharmacovigilance. FLAIR offers the highest sensitivity in the detection of PML. T2-weighted MRI detects PML’s typical ‘punctate pattern’. T1 weighted gadolinium-enhanced MRI can visualise demyelination and inflammation. DWI can detect acute and active infections.40, 41
Patients and physicians should be alert for opportunistic infections associated with DMTs, which can include Nocardia,42 varicella-zoster virus encephalitis and vasculopathy43 and haemorrhagic encephalitis.44
Patients and physicians should continue monitoring and remain alert for any new signs or symptoms that may suggest PML for approximately 6 months following natalizumab discontinuation.
SU
MM
ARY
Pharmacovigilance has three main components. Firstly, pharmacovigilance measures treatment efficacy based on inflammation and neurodegeneration. Secondly, pharmacovigilance can predict treatment responses and allow stratification into responders and non-responders. Finally, pharmacovigilance monitors safety, including detecting comorbidities, opportunistic infections (such as PML and varicella zoster virus) and paradoxical reactions. “Patients are heterogeneous, with different treatments, co-morbidities and adverse events,” Dr Wattjes said. “Safety monitoring is, therefore, essential.”
Clinically, PML, for example, usually manifests as subacute neurologic deficits that progress over days to weeks. The deficits include:39, 45
Altered mental status and cognitive changes. Limb and gait ataxia. Motor deficits (hemiparesis or monoparesis). Visual symptoms (hemianopia or diplopia).
Outcomes are generally better when PML is detected early, which further underscores the importance of safety monitoring.

18
The recommended monitoring MRI sequences are FLAIR, DWI, T1, and T2.41 Approximately half the PML cases associated with natalizumab show gadolinium enhancement.39 In addition, pharmacovigilance using MRI can help exclude co-morbidities that may complicate PML evaluation. For example, reversible leukoencephalopathy syndrome in patients taking natalizumab can mimic PML.46 MRI can also aid the evaluation of paradoxical reactions, such as tumefactive demyelinating lesions, seen occasionally with some treatments.37
Moreover, patients with at least one vascular comorbidity at diagnosis reach ambulatory disability significantly earlier than those without. In a study that enrolled 8983 people with MS, for example, the median time between diagnosis and the need for ambulatory assistance was 18.8 and 12.8 years in patients without and with vascular comorbidities respectively.38 FLAIR* can rule out vascular comorbidity.47 “Vascular comorbidities in MS are very important, and are much more frequent and severe in people with MS.”
Biomarker studies can also help pharmacovigilance, Dr Wattjes explained. PCR, for example, can detect DNA from JCV in the CSF of people with PML.39 JCV, first described in 1971, is a neurotropic polyomavirus that infects oligodendrocytes and astrocytes, but spares the optic nerves and spinal cord.
The natural history of JCV shows three stages:
A primary, typically clinically silent, infection, usually during childhood.
A latent infection in the urinary tract or bone marrow.
Reactivation.
Dr Wattjes noted that JCV reactivation occurs almost exclusively in immunocompromised patients. As a result, about 80% of PML cases occur in people with HIV. The remainder occur in several other settings including recipients of bone marrow transplantation, chemotherapy, malignancies, rituximab (used for rheumatoid arthritis) and natalizumab.
Against this background, quantitative real-time PCR (ultrasensitive assay with a level of detection of at least 10 copies/mL) performed by a reference laboratory can confirm suspected PML,48 but a negative result cannot be used to rule out PML. In the early stages of PML associated with natalizumab, the CSF can be negative for JCV DNA despite clinical and radiographic findings supporting the diagnosis. If a suspicion of natalizumab-associated PML persists despite repeated testing for JCV in the CSF using quantitative PCR, neurologists could consider a brain biopsy.39

19
The American Academy of Neurology developed diagnostic criteria for PML that encompasses imaging and JCV CSF testing (table 6).49 Several MRI protocols might aid diagnosis and screening, each of which offers a different perspective. FLAIR offers the highest sensitivity in the detection of PML. T2-weighted MRI detects the vacuoles and microcysts responsible for the ‘punctate pattern’ typical of PML, which may arise from enlarged perivascular spaces, inflammation or both.
Table 6: American Academy of Neurology diagnostic criteria for PML49
Adapted from Berger JR, et al Neurology. 2013;80:1430-1438
Certainty of PML diagnosis
Compatible clinical features
Compatible imaging findings
CSF PCR for JC virus
Definite + + +Probable + - +
- + +Possible + + -/ND
- - +Not PML - - -
+ - -- + -
T1-weighted gadolinium-enhanced MRI can visualise the degree of demyelination and inflammation, while DWI can detect acute and active infections.40, 41 Dr Wattjes added that T1-weighted gadolinium-enhanced MRI is not required for screening.

20
Patients and physicians should continue the monitoring protocol and remain alert for any new signs or symptoms that may suggest PML for approximately 6 months after natalizumab discontinuation. This covers the development of lesion(s) that were visible before natalizumab discontinuation as well as missed lesions and misinterpreted lesions (eg MS disease activity). “When you switch treatments, the risk of PML doesn’t drop to zero,” Dr Wattjes said. “It’s important to re-baseline after switching.”
Finally, patients and physicians should be alert for opportunistic infections associated with DMT treatments, which can include Nocardia,42 varicella-zoster virus encephalitis and vasculopathy43 and haemorrhagic encephalitis.44
Table 7: MRI pattern of asymptomatic PML51
Adapted from Wattjes MP, et al J Neurol Neurosurg Psychiatry 2015;86:793-798.
Table 8: Lesion differentiation in asymptomatic PML52
Adapted from Wattjes MP, et al Journal of Neurology, Neurosurgery & Psychiatry 2016;87:1138-1145
*The model is corrected for age and treatment duration and the lesion characteristics are listed in order of stepwise entering in the model, †OR>1 is associated with PML lesions, OR<1 is associated with new MS lesions; ‡compared with “non-focal appearance” (i.e., rated as: diffuse, confluent irregular, or infiltrative appearance); §defined as punctiform T2/FLAIR hyperintense lesions in the vicinity of the main PML lesions recently described as “milky way appearance” and/or punctiform T2/FLAIR hyperintense lesions with a perivascular spread (<5 mm in diameter). OR = odds ratio; CI = confidence interval.
Image Characteristics Patients, n (%)
Location
Frontal lobe 14 (77.8%)
Parietal lobe 4 (22.2%)
Occipital lobe 1 (5.6%)
Temporal lobe 1 (5.6%)
Basal ganglia 1 (5.6%)
Infratentorial 1 (5.6%)
Involvement of the brain tissue
WM only 2 (11.1%)
Cortical GM only 2 (11.1%)
Mixed cortical GM/WM 13 (72.2%)
Deep GM 1 (5.6%)
Predictive Lesion Characteristics*
OR for PML† 95% CI
P value
Focal lesion appearance‡ 0.009
0.0008 - 0.12
<0.001
Periventricular white matter location
0.00060.00003 - 0.0121
<0.001
Presence of punctate T2 lesions§ 183.2
11.4 - 2950.7
<0.001
Cortical grey matter involvement
59.88.4
- 427.6<0.001
PML associated with natalizumab can arise in the white matter, cortex or deep grey matter. “Small lesions are associated with a better prognosis,” Dr Wattjes said. Retrospective analysis of MRI scans often reveals an asymptomatic preclinical stage (table 7).50, 51 For example, 6 to 12 months before PML diagnosis, MRI did not show any lesions that evolved into PML. One to 6 months
before diagnosis, small lesions that evolved into PML are observed frequently. Indeed, the lesion characteristics may predict the risk of PML (table 8).52 Lesion volume also correlates with the likelihood that the lesion will test positive on PCR for JCV, ranging from 96% with a lesion volume of 68ml, 80% with 10ml and 55% with 3ml.
“Outcomes are better if safety issues are detected early. Pharmacovigilance is, however, a new field in MS research and is not yet exclusively evidence based,” Dr Wattjes concluded. “Safety monitoring is based on clinical vigilance, MRI monitoring and additional biomarkers, such as JCV in the CSF. A heterogeneous spectrum of adverse events can be detected on MRI and a high neuroradiological expertise is crucial. Therefore, I advise neurologists to follow the guidelines and obtain a second opinion when needed.”

21
THE VALUE OF ADVANCED IMAGING TECHNIQUES IN MS
Professor Paul Matthews, Edmond and Lily Safra Chair and Head of the Division of Brain Sciences, and Associate Director, UK Dementia Research Institute at Imperial College London
New imaging methods emphasise that the different clinical classifications of MS share common, progressive disease processes.
The extent of the neurodegeneration shows marked interpatient variation, but correlates with the risk of disability progression.
Changes visible on the high-resolution images provided by optical coherence tomography (OCT) reflect the extent of axonal injury in MS.
Innate immunity seems to make an important contribution to MS pathogenesis and progression. Current drugs for MS, however, do not modulate innate immunity.
Inflammation remains a primary treatment target throughout the course of the disease. Indeed, results of studies using the new imaging methods underscore the importance of early treatment to reduce the likelihood of complications.
SU
MM
ARY
New imaging methods offer unprecedented insights into MS pathogenesis and progression, Professor Matthews told the meeting. Indeed, recent studies employing the new imaging methods emphasise that the different clinical classifications of MS share common, progressive disease processes. “The findings underscore the importance of early treatment,” he said. “The findings also show that inflammation remains a primary target for treatment throughout the course of the disease.”
Quantitative MRI can assess the brain atrophy arising from the loss of myelin and neurones that is characteristic of MS. The extent of the neurodegeneration shows marked interpatient variation, but correlates with disability risk. For example, a person with low Normalised Brain Volume (NBV) is approximately 2.4 times more likely to show 3-month confirmed disability progression during a two-year follow up as those with high NBV (36% and 18% progressed respectively).53
Professor Matthews noted that inflammation and immune changes in the retinal nerves parallel those in the rest of the CNS. OCT provides a rapid, non-invasive quantification of retinal layers by low-coherence near-infrared light. Changes visible on the high-resolution image provided by OCT reflect the extent of axonal injury in MS. For example, OCT shows that the retinal nerve fibres thin with progressive MS. “OCT is a promising tool to detect subclinical changes in the retinal nerve fibre layer even in people who do not show optic neuritis,” 54 he remarked. “OCT seems to be very precise, has the potential to be a valuable biomarker of retinal pathology in MS and should be examined further in longitudinal studies.”

22
Another advanced imaging technique - double inversion recovery (DIR) MRI - highlights the contribution made by meningeal inflammation and dynamic cortical inflammation to MS. DIR uses gadolinium-contrast enhanced T2-FLAIR MRI to visualise the continuing, acute leptomeningeal inflammation and cortical demyelination that occurs in people with MS. Leptomeningeal enhancement correlates with demyelination post-mortem.55
Other techniques – such as measuring myelin-associated water, MTR and myelin-basic protein positron emission tomography (PET) – can image repetitive cycles of demyelination and remyelination in the white matter of people with MS. Myelin water, for instance, has a different T2 relaxation time (15-40ms) to free intra- and extra-cellular water (40-200ms). Myelin water images of the whole cerebrum, derived from T2 relaxation, can be acquired in less than 15 minutes. Measuring myelin-associated water may allow neurologists to follow the processes that underlie recovery after an exacerbation.
Free water shows less hydrogen bonding, less magnetic field inhomogeneity, a longer T2 and a narrower excitation range than water near macromolecules, such as myelin. In MTR, the magnetisation transfer pulse excites bound water selectively. The magnetisation transfers to free water. These ‘pre-excited molecules’ provide a weaker signal on T1 weighted images. Myelin content can also be assessed using [11C] PIB PET, which uses Pittsburgh compound B (PIB) - a radioactive analogue of thioflavin T - to image myelin basic protein.56 Professor Matthews noted that these approaches do not measure myelin directly and have not been compared quantitatively. Nevertheless, the different assessments of myelin show broadly consistent results.
Professor Matthews also described ultra-high field imaging and translocator protein-18 kDa Positron Emission Tomography (TSPO PET). The binding of the ligand to TSPO in the brains of MS patients reflects primarily the number of activated microglia and macrophages. “This technique allows the assessment of the previously ‘hidden’ burden of chronic, innate immune activation,” Professor Matthews said. “Innate immunity is a very active player in MS. Current drugs for MS, however, don’t modulate innate immunity.”
For example, TSPO PET shows diffusely heterogeneous innate immune activation in the white matter of people with secondary progressive MS (SPMS). The heterogeneous inflammation in ‘normal appearing white matter’ shows up as variable TSPO uptake.57 The technique also reveals that activated microglia on the rim of MS lesions can exhibit a destructive, inflammatory phenotype.58 Moreover, greater diffuse white matter activation of the innate immune system imaged with TSPO PET is associated with a greater risk of disease progression in patients with clinically isolated syndrome.59
As a final example of the potential offered by the new imaging methods, Professor Matthews pointed out that quantitative susceptibility mapping using MRI may visualise chronic activation of microglial cells. The number of iron-laden microglial cells detected using this method reflects the population of slowly expanding MS white matter plaques.60
Despite their differing methodologies, the new imaging methods demonstrate that clinically isolated syndrome, relapsing remitting and SPMS share common, progressive disease processes. “Inflammation is present early and persists throughout the disease course,” Professor Matthews concluded. “As we’ve seen with other inflammatory conditions, such as Crohn’s disease, there is a strong argument for treating MS early and hard to avoid complications.”

23
1. Rolak L. Clinical Medicine and Research 2002;1:57-60
2. Sadovnick A et al., Neurology 1991;41:1193-1196
3. Hammond S et al., Journal of Neurology, Neurosurgery, and Psychiatry 1996;61:311-313
4. Morales-Gonzales J et al., Multiple Sclerosis Journal 2004;10:47-54
5. Feuillet L et al., Multiple Sclerosis Journal 2007;13:124-127
6. Baker D et al., EBioMedicine 2017;16:41-50
7. Dooley J et al., Neurology - Neuroimmunology Neuroinflammation 2016;3:1-10
8. De Stefano N et al., Neurology 2010;74:1868-1876
9. Petrova N et al., Brain Pathol 2018;28:334-348
10. Giovannoni G et al., Multiple Sclerosis and Related Disorders 2015;4:329-333
11. Magliozzi R et al., Brain 2007;130:1089-1104
12. Schmierer K at al., Annals of Neurology 2004;56:407-415
13. Barkhof F et al., Nature Reviews Neurology 2009;5:256-266
14. Poser C, Brinar V. Clinical Neurology and Neurosurgery 2004;106(3):147-158
15. Filippi M et al., The Lancet Neurology 2016;15:292-303
16. Poser C. Annals of the New York Academy of Sciences 1965;122:506-519
17. Schumacher G et al., Annals of the New York Academy of Sciences 1965;122:552-568
18. Poser C et al., Annals of Neurology 1983;13:227-231
19. McDonald I et al., Annals of Neurology 2001;50:121-127
20. Polman C et al., Annals of Neurology 2011;69:292-302
21. Mistry N et al., JAMA Neurology 2013;70:623-628
22. Sati P et al., Radiology 2012;265:926-932
23. Traboulsee A et al., American Journal of Neuroradiology 2016;37:394-401
24. Vagberg M et al., Acta Neurologica Scandinavica 2017;135:17-24
25. Yousry T et al., Annals of Neurology 2012;72:779-787
26. Erbayat Altay E et al., JAMA Neurology 2013;70(3):338-344
27. Gulani V et al., The Lancet Neurology 2017;16:564-570
28. Weinmann H J et al., American Journal of Roentgenology 1984;142:619-624
29. Kanal E, Maravilla K, Rowley H A. American Journal of Neuroradiology 2014;35:2215-2226
30. Sherry D, Caravan P, Lenkinski R. Journal of Magnetic Resonance Imaging 2009;30:1240-1248
REFERENCES
31. Marckmann P et al., Journal of the American Society of Nephrology 2006;17:2359-2362
32. McDonald R et al., Radiology 2015;275:772-782
33. Radbruch A et al., Radiology 2015;275:783-791
34. Lee J et al., PLoS ONE 2017;12:DOI:10.1371/journal.pone.0183916
35. Stojanov D et al., European Radiology 2016;26(3):807-815
36. Gupta A et al., American Journal of Neuroradiology 2017;38:1317-1322
37. Visser F et al., Neurology 2012;79:2000-2003
38. Marrie R et al., Neurology 2010;74:1041-1047
39. Kappos L et al., The Lancet Neurology 2011;10:745-758
40. Wattjes M et al., Multiple Sclerosis Journal 2013;19(14):1826-1840
41. Wattjes M, Barkhof F. Current Opinion in Neurology 2014;27(3):260-270
42. Sheikh-Taha M, Corman L. Multiple Sclerosis Journal 2017;23(6):872-874
43. Ratchford J et al., Neurology 2012;79:2002-2004
44. Leypoldt F et al., Neurology 2009;72:1022-1024
45. Tysabri Summary of Product Characteristics (SmPC)
46. Decard B et al., Multiple Sclerosis Journal 2012;19:249-251
47. Kilsdonk I et al., European Radiology 2014;24:841-849
48. Tysabri PID v17
49. Berger J et al., Neurology 2013;80:1430-1438
50. Phan-Ba R et al., Journal of Neurology, Neurosurgery & Psychiatry 2012;83:224-226
51. Wattjes M et al., Journal of Neurology, Neurosurgery & Psychiatry 2015;86:793-798
52. Wijburg M et al., Journal of Neurology, Neurosurgery & Psychiatry 2016;87:1138 1145
53. De Stefano N. ECTRIMS Online Library 2014:63996:
54. Gordon-Lipkin E et al., Neurology 2007;69:1603-1609
55. Absinta M et al., Neurology 2015;85(1):18-28
56. Bodini B et al., Annals of Neurology 2016;79:726-738
57. Rissanen E et al., Journal of Nuclear Medicine 2014; 55:939-944
58. Vogel D et al., Journal of Neuroinflammation 2013;10(35):1-12
59. Giannetti P et al., Brain 2015;138:110-119
60. Harrison D et al., American Journal of Neuroradiology 2016;37:1447-1453

Biogen-81140. Date of preparation: November 2020
PRESCRIBING INFORMATION: TYSABRI® (natalizumab) 300mg concentrate for solution for infusion
Please refer to the Summary of Product Characteristics (SmPC) for further information. Indication: Single disease modifying therapy (DMT) in adult patients with highly active relapsing remitting multiple sclerosis (rapidly evolving disease or highly active disease despite a full and adequate course of at least one DMT). Dosage and administration: TYSABRI is administered by IV infusion every 4 weeks at specialist centres with timely access to MRI. Patients should be observed during infusion and for 1 hour afterwards for hypersensitivity reactions. TYSABRI is not recommended for use in patients over 65 years. Contraindications: Hypersensitivity to natalizumab or to any of the excipients; progressive multifocal leukoencephalopathy (PML); patients with increased risk of opportunistic infections, including immunocompromised patients; combination with other DMTs; known active malignancies except for patients with cutaneous basal cell carcinoma. Special warnings and precautions: Traceability; To improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. PML; Use of TYSABRI has been associated with increased risk of PML (opportunistic infection caused by John Cunningham virus (JCV)) which may be fatal or result in severe disability. Patients must be monitored at regular intervals for early signs and symptoms of PML. JCV also causes JCV GCN (granule cell neuronopathy), which is similar to PML (i.e. cerebellar syndrome). PML should be considered as a differential diagnosis in any MS patient taking TYSABRI presenting with neurological symptoms and/or new brain lesions in MRI. If PML or JCV GCN is suspected, further dosing must be suspended until PML has been excluded. Presence of anti-JCV antibodies, treatment duration (especially beyond 2 years) and prior immunosuppressant use are risk factors for PML. Anti-JCV antibody testing provides supportive information for risk stratification of
TYSABRI treatment. Please refer to the SmPC and Physician Information and Management Guidelines for information on quantification and stratification of PML risk; monitoring of anti-JCV antibodies; MRI monitoring and management of suspected PML. Patients and physicians should continue to be alert for signs or symptoms suggestive of PML for approximately 6 months following treatment discontinuation. IRIS; Immune Reconstitution Inflammatory Syndrome occurs in almost all TYSABRI PML patients after TYSABRI removal, which can be fatal. Infections including opportunistic infections; TYSABRI increases the risk of encephalitis and meningitis caused by herpes simplex and varicella zoster viruses. Rare cases of acute retinal necrosis have also been observed and can be potentially blinding. Patients with eye symptoms should be referred for retinal screening. Other opportunistic infections may occur. If suspected, TYSABRI should be suspended until such an infection can be excluded. Educational guidance; Physicians intending to prescribe TYSABRI must be familiar with the Physician Information and Management Guidelines. Physicians must discuss benefits and risks with the patient, counsel on the importance of uninterrupted dosing (particularly in the early months), and provide an Alert Card. Patients and caregivers should be instructed on early signs and symptoms of PML and to inform their physician of any infection. Hypersensitivity reactions have been associated with TYSABRI, including serious systemic reactions. Prior treatment with immunosuppressive DMTs; care should be taken in order to avoid additive immune effects. Immunogenicity; in the case of disease exacerbations or infusion related events, the presence of antibodies should be evaluated. Treatment should be discontinued if persistent antibodies develop. Hepatic events; serious cases of liver injury have been reported. Patients should be monitored for liver impairment and TYSABRI discontinued if serious liver injury occurs. Anaemia; Rare, serious cases of anaemia
and haemolytic anaemia have been reported. Stopping therapy; if therapy is discontinued the physician needs to be aware that TYSABRI has pharmacodynamic effects for approximately 12 weeks. Fertility, pregnancy and lactation: In case of pregnancy, consider discontinuation. A benefit-risk evaluation of the use of TYSABRI during pregnancy should be undertaken. Data from clinical trials, a pregnancy registry, post-marketing and literature do not suggest an effect of TYSABRI on pregnancy outcomes. In case of exposure during the third trimester, newborns should be monitored for potential transient haematological abnormalities which may occur. Patients receiving TYSABRI should not breastfeed. It is unlikely that TYSABRI will affect fertility. Undesirable effects: The most commonly reported side effects are; urinary tract infection, nasopharyngitis, urticaria, headache, dizziness, vomiting, nausea, arthralgia, rigors, pyrexia, fatigue. See special warnings and precautions for serious side effects. See SmPC for full list of side effects. Legal classification: POM. Pack size and price: 1 vial/pack £1130. Package quantities: 300mg/15ml. Marketing Authorisation number: EU/1/06/346/001. Marketing Authorisation Holder: Biogen Netherlands B.V., Prins Mauritslaan 13, 1171 LP Badhoevedorp, The Netherlands. Date of last revision of Prescribing Information: November 2019.
Adverse events should be reported.For Ireland, reporting forms and
information can be found at www.hpra.ie.For the UK, reporting forms and
information can be found at https://yellowcard.mhra.gov.uk/ or via
the Yellow Card app available from the Apple App Store or Google Play Store.Adverse events should also be reported to Biogen Idec on 1800 812 719 in Ireland
and 0800 008 7401 in the UK.