Embed Size (px)
Citation preview

NEUROSURGICALOPERATIVE ATLAS
Volume 8
The American Association of Neurological Surgeons
AANS Publications Committee
Editors
SETTI S. RENGACHARYROBERT H. WILKINS

© 1999For copies of this Cumulative Index contact:
The American Association of Neurological Surgeons22 South Washington St.Park Ridge, Illinois 60068-4287
email: [email protected]: 847-692-9500fax: 847-692-6770

C o n t e n t sVolume I
Optic Gliomas. Edgar M. Housepian / 1-13F i b rous Dysplasia Involving the Craniofacial Skeleton.
James T. Goodrich, Craig D. Hall / 14-22D e p ressed Skull Fracture in Adults. F red H. Geisler / 23-33
Cervical Hemilaminectomy for Excision of a Herniated Disc. Robert H. Wilkins, Sarah J. Gaskill / 34-38
Lateral Sphenoid Wing Meningioma. Joseph Ransohoff / 39-45Selective Micro s u rgical Vestibular Nerve Section for Intractable Ménière’s Syndro m e .
E d w a rd Tarlov / 46-53Chiari Malformations and Syringohydromyelia in Children. W. Jerry Oakes / 54-60
C a rotid Body Tumors. F redric B. Meyer, Thoralf M. Sundt, Jr. / 61-69Olfactory Groove Meningiomas. Joshua B. Bederson, Charles B. Wilson / 70-78
C e rebral Aneurysms at the Bifurcation of the Internal Carotid Artery.Eugene S. Flamm / 79-88
Treatment of Unilateral or Bilateral Coronal Synostosis. John A. Persing, John A. Jane / 89-98Convexity Meningioma. Sarah J. Gaskill, Robert H. Wilkins / 99-105
Occipital Lobectomy. Milam E. Leavens / 106-112Spinal Meningiomas. Michael N. Bucci, Julian T. Hoff / 113-116
P e rcutaneous Trigeminal Glycerol Rhizotomy. Ronald F. Young / 117-123Lumbar Hemilaminectomy for Excision of a Herniated Disc.
Patrick W. Hitchon, Vincent C. Traynelis / 124-129Transoral Surgery for Craniovertebral Junction Anomalies. A rnold H. Menezes / 130-135
A n t e rolateral Cervical Approach to the Craniovertebral Junction. Dennis E. McDonnell / 136-153
C o r rection of Malposition of the Orbits. John A. Persing / 154-163Removal of Cervical Ossified Posterior Longitudinal Ligament at Single and Multiple Levels.
Ralph B. Cloward / 164-170Technique of Ventriculostomy. Joseph H. Piatt, Jr., Kim J. Burchiel / 171-175
C e rebellar Medulloblastoma. Arthur E. Marlin, Sarah J. Gaskill / 176-183Shunting of a Posttraumatic Syrinx. David J. Gower / 184-190
D i rect Surgical Treatment of Vein of Galen Malformations. H a rold J. Hoffman / 191-200Spinal Nerve Schwannoma. Phyo Kim, Burton M. Onofrio / 201-206Combined Craniofacial Resection for Anterior Skull Base Tumors.
Ehud Arbit, Jatin Shah / 207-217Diagnostic Open Brain and Meningeal Biopsy.
R i c h a rd P. Anderson, Howard H. Kaufman, Sydney S. Schochet / 218-222Ventriculoperitoneal Shunting. David C. McCullough / 223-230
Ventriculoatrial Shunting. Paul J. Camarata, Stephen J. Haines / 231-239Excision of Acoustic Neuromas by the Middle Fossa Approach. Derald E. Brackmann / 240-248
Upper Thoracic Sympathectomy by a Posterior Midline Approach. P rem K. Pillay, Issam A. Awad, Donald F. Dohn / 249-255
C a rotid Endarterectomy. Daniel L. Barrow, Christopher E. Clare / 256-266Transsphenoidal Excision of Macroadenomas of the Pituitary Gland.

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
G e o rge T. Tindall, Eric J. Wo o d a rd, Daniel L. Barrow / 267-278C o m p u t e r-D i rected Stereotactic Resection of Brain Tumors. Patrick J. Kelly / 279-293
Sagittal Synostosis. A. Leland Albright / 294-300Glossopharyngeal Rhizotomy. Burton M. Onofrio / 301-304
Occipitocervical and High Cervical Stabilization. Volker K.H. Sonntag, Curtis A. Dickman / 305-315
P e t roclival Meningiomas. Ossama Al-Mefty, Michael P. Schenk, Robert R. Smith / 316-326Facial Reanimation without the Facial Nerve. Mark May, Steven M. Sobol / 327-336
Omental and Musculocutaneous Free Flaps for Coverage of Complicated Neuro s u rg i c a lWounds. Daniel L. Barrow, Foad Nahai / 337-348
Repair of “Growing” Skull Fracture. Tadanori Tomita / 349-354Occipital Encephaloceles. William O. Bell / 355-362
Foramen Magnum Meningiomas and Schwannomas: Posterior Approach. Chad D. Abernathey, Burton M. Onofrio / 363-371
Penetrating Wounds of the Spine. E d w a rd C. Benzel / 372-378P e rcutaneous Radiofrequency Rhizolysis for Trigeminal Neuralgia.
James Fick, John M. Tew, Jr. / 379-390Extended Costotransversectomy. Eddy Garrido / 391-396
S u rgical Resection of Posterior Fossa Epidermoid and Dermoid Cysts. Lee Kesterson / 397-406Luque Rod Segmental Spinal Instrumentation. E d w a rd C. Benzel, / 407-412
En Bloc Anterior Temporal Lobectomy for Te m p o rolimbic Epilepsy. Michel F. Levesque / 413-422
Cingulotomy for Intractable Pain Using Stereotaxis Guided by Magnetic Resonance Imaging.Samuel J. Hassenbusch, Prem K. Pillay / 423-432
C e rebellar Astrocytomas. A. Leland Albright / 433-439E x t reme Lateral Lumbar Disc Herniation. Robert S. Hood / 440-444
Tentorial Meningiomas. Laligam N. Sekhar, Atul Goel / 445-455
Volume II
S u rgical Repair of Trigonocephaly. Ken R. Winston, Michael J. Burke / 1-8Dorsal Root Entry Zone (DREZ) Lesioning. Blaine S. Nashold, Jr., Amr O. Ei-Naggar / 9-24
Ophthalmic Segment Aneurysms. Arthur L. Day / 25-41C h ronic Subdural Hematoma. James E. Wi l b e rg e r, Jr. / 42-48
Ta i l o red Temporal Lobectomy Using Subdural Electrode Grids. Issam A. Awad, Joseph F. Hahn / 49-55
Gunshot Wounds of the Brain. Suzie C. Tindall, Ali Krisht / 56-59Tr a n s t o rcular Occlusion of Vein of Galen Malformations. J. Parker Mickle, Ronald G. Quisling, Keith Peters / 60-66
Detection of an Epileptic Focus and Cortical Mapping Using a Subdural Grid.Sumio Uematsu / 67-78
A n t e romesial Temporal Lobectomy for Epilepsy. Issam A. Awad, Prem K. Pillay / 79-87Anastomosis of the Facial Nerve After Resection of an Acoustic Neuroma.
Charles M. Luetje / 88-90An Extended Subfrontal Approach to the Skull Base.
Chandranath Sen, Laligam N. Sekhar / 91-100

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
Pansynostosis: Surgical Management of Multiple Pre m a t u re Suture Closure. James T. Goodrich, Craig D. Hall / 101-112
Distal Anterior Cerebral Artery Aneurysms. H. Hunt Batjer, Duke Samson / 113-126Te t h e red Spinal Cord, Intramedullary Spinal Lipoma, and Lipomyelomeningocele.
W. Jerry Oakes / 127-135Interstitial Brachytherapy. J e ff rey D. McDonald, Philip H. Gutin / 136-144
Lateral Extracavitary Approach to the Thoracic and Lumbar Spine. Dennis J. Maiman, Sanford J. Larson / 145-153
An Extreme Lateral Transcondylar Approach to the Foramen Magnum and Cervical Spine.Chandranath Sen, Laligam N. Sekhar / 154-162
R e t rolabyrinthine Presigmoid Approach for Sectioning of the Vestibular Nerve for Ménière ’ sDisease. Charles M. Luetje / 163-166
S t e reotactic Surgical Ablation for Pain Relief. Ronald F. Young / 167-177Anterior Screw Fixation of Odontoid Fractures. Ronald I. Apfelbaum / 178-188
Carpal Tunnel Syndrome. Setti S. Rengachary / 189-199Transantral Ethmoidal Orbital Decompression For Graves’ Ophthalmopathy.
L a w rence W. DeSanto / 200-206Middle Fossa Approaches for Invasive Tumors Involving the Skull Base.
Laligam N. Sekhar, Atul Goel, Chandranath Sen / 207-218Transthoracic Excision of a Spinal Metastasis with Vertebral Body Reconstruction.
G regory J. Bennett / 219-228Anterior Cervical Discectomy and Fusion-the Cloward Technique. Ralph B. Cloward / 229-240
Cubital Tunnel Syndrome. Setti S. Rengachary / 241-245Caspar Plating of the Cervical Spine.
H. Louis Harkey, Wo l f h a rd Caspar, Yaghoub Tarassoli / 246-256S u rgical Management of Anterior Communicating Artery Aneurysms.
Timothy C. Ryken, Chistopher M. Loftus / 257-265Basilar Bifurcation Aneurysm: Pterional (Transsylvian) Approach.
H. Hunt Batjer, Duke S. Samson / 266-281Thalamotomy for Tre m o r. Roy A. E. Bakay, Jerrold L. Vitek, Mahlon R. Delong / 282-295
Endovascular Treatment of Carotid Cavernous Fistulas. Arvind Ahuja, Lee R. Guterman, Kimberly Livingston, Leo N. Hopkins / 296-304
Combined Transsylvian and Middle Fossa Approach to Interpeduncular Fossa Lesions.Chandranath Sen, Laligam N. Sekhar / 305-311
Aneurysms of the Ophthalmic Segment of the Internal Carotid Artery. Daniel L. Barrow / 312-322
L u m b a r-Peritoneal Shunting. Setti S. Rengachary / 323-333S u rgery of the Cavernous Sinus.
Harry van Loveren, Magdy El-Kalliny, Jeff rey Keller, John M. Tew, Jr. / 334-344Encephaloceles of the Anterior Cranial Base. Alan R. Cohen / 345-353
C o t re l-Dubousset Instrumentation: Internal Fixation for Thoracolumbar Fractures and Tumors. Bruce E. van Dam / 354-358
P o s t e r i o r-Lateral Lumbar Spinal Fusion. E d w a rd S. Connolly / 359-366C o r rection of Exorbitism.
Constance M. Barone, Ravelo V. Argamaso, David F. Jimenez, James T. Goodrich / 367-372Meralgia Paresthetica. Setti S. Rengachary / 373-379
D e p ressed Skull Fracture in Infants. Lyn C. Wright, Marion L. Walker / 380-383Combined Pre s i g m o i d-Transtransversarium Intradural Approach to the Entire Clivus and

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
Anterior Craniospinal Region. Mario Ammirati, Melvin Cheatham / 384-395Partial Median Corpectomy with Fibular Grafting for Cervical Spondylotic Myelopathy.
Setti S. Rengachary / 396-409C o r rection of Orbital Hypertelorism and Orbital Dystopia.
Constance M. Barone, David F. Jimenez, Ravelo V. Argamaso, James T. Goodrich / 410-416P e rcutaneous Radiofrequency Rhizotomy for the Treatment of Paraplegic Spasms.
Sumio Uematsu / 417-427E n d o c r i n e-Inactive Pituitary Adenomas. Charles B. Wilson / 428-437
Posterior Decompression and Fusion for Cervical Spondylotic Myelopathy. Paul Kurt Maure r, Charles Nussbaum / 438-447
S u rgical Correction of Swan Neck Deformity. Peter M. Klara, Kevin T. Foley / 448-461
Volume III
Tu b e rculum Sellae Meningiomas. Ossama Al-Mefty / 1-11Craniofacial Techniques Used in Resection of Anterior Skull Base Tumors.
James T. Goodrich, Ravelo V. Argamaso / 12-20Occipital Transtentorial Approach to Pineal Region Neoplasms.
James I. Ausman, Balaji Sadasivan / 21-26Meningioma of the Lateral Ventricle. E d w a rd Tarlov / 27-30
P re a u r i c u l a r-Infratemporal Fossa Approach to Tumors that Involve the Lateral Cranial Base.Robert L. Grubb, Peter G. Smith / 31-37
Repair of the Myelomeningocele. David G. McLone / 38-44Anterior Clinoidal Meningiomas. Franco DeMonte, Ossama Al-Mefty / 45-57
D a n d y - Walker Malformation. Arthur E. Marlin, Sarah J. Gaskill / 58-65Acoustic Neuromas: Surgical Anatomy of the Suboccipital Approach.
Martin B. Camins, Jeff rey S. Oppenheim / 66-75E x p o s u re of the Skull Base via the Midface.
James T. Goodrich, Sidney Eisig, George J. Cisneros, Allen B. Kantrowitz / 76-83E x p o s u re of the Skull Base by Transoral, Translabial, and Transmandibular Routes.
James T. Goodrich, Sidney Eisig, Joseph G. Feghali, Allen B. Kantrowitz / 84-93S u rgical Management of Chiari I Malformations and Syringomyelia.
R i c h a rd B. Morawetz / 94-102Open-Door Maxillotomy Approach for Lesions of the Clivus.
H. Louis Harkey, Vinod K. Anand, H. Alan Cro c k a rd, Michael P. Schenk / 103-112Peripheral Nerve Repair. Allan J. Belzberg, James N. Campbell / 113-128
S u rgical Management of Split Cord Malformations. Dachling Pang / 129-143Te t h e red Cord Syndrome Secondary to Previous Repair of a Myelomeningocele.
Timothy A. Strait / 144-150Craniofacial Techniques for Managing Orbital Trauma.
James T. Goodrich, Simeon A. Lauer, Ravelo V. A rgamaso / 151-158Tr a n s o r a l - Transclival Approach to Basilar Artery Aneurysms.
R. A. de los Reyes, Paul W. Detwiler / 159-166F rontal Lobectomy. Setti S. Rengachary / 167-175
Thoracic Outlet Syndrome: Supraclavicular First Rib Resection and Brachial PlexusD e c o m p ression. Susan E. Mackinnon, G. A. Patterson / 176-182
Transfacial Approaches to the Clivus and Upper Cervical Spine. Ivo P. Janecka / 183-192S u rgical Management of Prolactinomas. A n d rew D. Parent / 193-202

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
Sectioning of the Filum Te rminale. F rederick A. Boop, William M. Chadduck / 203-209Repair of Diastematomyelia. F rederick A. Boop, William M. Chadduck / 210-214
Repair of a Lipomyelomeningocele. F rederick A. Boop, William M. Chadduck / 215-219Untethering of the Spinal Cord After a Previous Myelomeningocele Repair.
F rederick A. Boop, William M. Chadduck / 220-224Secondary Carpal Tunnel Syndrome. Susan E. Mackinnon / 225-234
Spheno-Orbital Craniotomy for Meningioma. Joseph C. Maroon, John S. Kennerdell, Danko V. Vidovich / 235-243
S u rgical Treatment of Anterior Sacral Meningocele. K. Stuart Lee / 244-251Acrylic Cranioplasty. Setti S. Rengachary / 252-259
P reauricular Transzygomatic Infratemporal Craniotomy for Skull Base Tumors. Stephen L. Ondra, Michael G. Donovan / 260-269
Medial Sphenoid Ridge Meningiomas. Vallo Benjamin, Jules M. Nazzaro / 270-282S u rgical Treatment of Arteriovenous Malformations of the Cerebral Convexity.
Wink S. Fisher III / 283-291Lumbar Microdiscectomy. Peter M. Klara, Kevin T. Foley / 292-301
M i c rovascular Decompression of the Facial Nerve. Robert H. Wilkins / 302-311Craniofacial Resection of Neoplasms of the Anterior Skull Base.
Vincent C. Traynelis, Timothy M. McCulloch, Henry T. Hoffman / 312-323Postlaminectomy Instability: Posterior Pro c e d u res.
Seth M. Zeidman, Thomas B. Ducker / 324-336Vertebral Artery and Posterior Inferior Cerebellar Artery Aneurysms: Surgical Management.
F e rnando G. Diaz, Richard D. Fessler / 337-343Anterior Cervical Discectomy and Fusion: Smith-Robinson Technique.
Philip R. Weinstein / 344-358Management of Basilar and Posterior Cerebral Artery Aneurysms by
Subtemporal Approaches. Robert M. Crowell, Christopher S. Ogilvy / 359-374Subcutaneous Transposition of the Ulnar Nerve for Ta rdy Ulnar Palsy.
Melvin L. Cheatham, Fredric L. Edelman, Martin Holland / 375-381Image-Guided Neuro s u rgery: Frame-Based and Frameless Approaches.
Lucia Zamorano, Lutz Nolte, Charlie Jiang, Majeed Kadi / 482-401Anterior Stabilization of the Cervical Spine Using a Locking Plate System.
Setti S. Rengachary / 402-413Endoscopic Neuro s u rg e r y . Alan R. Cohen / 414-426
S u rgical Management of Brain Abscess. Timothy C. Ryken, Christopher M. Loftus / 427-435Submuscular Transposition of the Ulnar Nerve at the Elbow: Musculofascial Lengthening
Technique. A. Lee Dellon / 436-443S u p e rficial Temporal Artery to Middle Cerebral Artery Bypass Grafting.
Issam A. Awad / 444-456
Volume IV
Spinal Vascular Malformations. E d w a rd H. Oldfield / 1-18Posterior C1-2 Screw Fixation for Atlantoaxial Instability. Ronald I. Apfelbaum / 19-28
S u p r a c e rebellar Infratentorial Approaches to the Pineal Region. Michael L. Levy, Michael L. J. Apuzzo / 29-36
T h i rd-Ventricle Exposure by the Interhemispheric Corridor. Peter Gruen, Michael L. J. Apuzzo / 37-42

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
Arteriovenous Malformations of the Basal Ganglia, Thalamus, and Adjacent Ventricles. Ghaus M. Malik, Fady T. Charbel / 43-58
Selective Denervation for Spasmodic Torticollis. Antonio A. F. DeSalles / 59-66Unilateral Coronal Synostosis. James T. Goodrich, Ravelo Argamaso / 67-74
N e u ro s u rgical Approaches to the Orbit. Part 1: Orbital Anatomy and Lateral Orbitotomy.Johnny B. Delashaw, Jr. / 75-84
N e u ro s u rgical Aproaches to the Orbit. Part 2: Craniotomy for Surgical Exposure of the Orbit.Johnny B. Delashaw, Jr. / 85-94
Fourth Ventricular Ependymoma. J. Gordon McComb, John H. Schneider / 95-106Sectioning of the Corpus Callosum for Epilepsy. Issam A. Awad / 107-116
S u rgical Treatment of Intracranial Glomus Tumors. Vinod K. Anand, Michael P. Schenk, John P. Leonetti, Ossama Al-Mefty / 117-130
Technique of Temporal Lobectomy. Allen R. Wyler / 131-138Treatment of Moyamoya Syndrome in Children with Pial Synangiosis.
R i c h a rd G. Ellenbogen, R. Michael Scott / 139-146Isthmic Spondylolysis and Spondylolisthesis: Treatment by Reduction, Interbody Fusion,
and Lateral Stabilization. Timothy C. Wirt / 147-158Translabyrinthine Removal of Acoustic Neuromas. John T. McElveen, Jr. / 159-164
Transsphenoidal Surgical Treatment of Cushing’s Disease. William F. Chandler / 165-172Upper Thoracic Spinal Exposure Through a Lateral Parascapular Extrapleural Appro a c h .
R i c h a rd G. Fessler, Donald Dietze, David Peace / 173-182Selective Dorsal Rhizotomy for the Spasticity of Cerebral Palsy. T. S. Park / 183-190
S u rgical Treatment of the Subclavian Steal Syndrome. G e o rge E. Pierce / 191-198S u rgery for Tumors Affecting the Cavernous Sinus.
Franco DeMonte, Vinod K. Anand, Ossama Al-Mefty / 199-208Lambdoidal Synostosis.
David F. Jimenez, Constance M. Barone, Ravelo V. Argamaso, James T. Goodrich / 209-214Gamma Knife Radiosurgery of Intracranial Lesions. Robert J. Coffey / 215-224
Submuscular Transposition of the Ulnar Nerve at the Elbow. Susan E. Mackinnon / 225-234Ulnar Nerve Entrapment at the Wrist. V. Leroy Young, Jill M. Young / 235-249
Volume V
Endoscopic Pituitary Surgery. H a e-Dong Jho, Ricardo L. Carrau, Yong Ko / 1-12To rcular and Peritorcular Meningiomas. G r i ffith R. Harsh IV / 13-22
S u rgical Resection of Lower Clivus-Anterior Foramen Magnum Meningioma.Vallo Benjamin, Ramesh P. Babu / 23-32
Basilar Bifurcation Aneurysms: Transsylvian Transclinoidal Tr a n s c a v e rnous Appro a c h .Murali Guthikonda, Fernando G. Diaz / 33-42
S u rgical Management of Posterior Plagiocephaly. R i c h a rd G. Ellenbogen, Michael H. Mayer / 43-56
Acute Subdural Hematoma. F red H. Geisler / 57-64Intracranial Pre s s u re Monitoring. A n d rew D. Firlik, Donald W. Marion / 65-74
Temporal Lobectomy Under General Anesthesia. Diana L. Abson Kraemer, Dennis D. Spencer / 75-84
F a r-Lateral Disc Herniation Treated by Microscopic Fragment Excision. Bruce V. Darden II, J. Robinson Hicks / 85-90
Stabilization of the Cervical Spine (C3-7) with Articular Mass (Lateral Mass) Plate and

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
S c re w s . T. Glenn Pait, Luis A. B. Borba / 91-100Stabilization of the Cervical Spine with the Orion Anterior Cervical Plate System.
Gary L. Lowery / 101-108Texas Scottish Rite Hospital System for Internal Stabilization of Thoracolumbar Fracture s .
B r a d f o rd M. Mullin, Gary L. Rea / 109-120Application of Frameless Stereotaxy in the Management of Intracranial Lesions.
Dennis A. Tu rn e r, Paul B. Johnson / 121-128A Modified Transfacial Approach to the Clivus.
B rooke Swearingen, Michael P. Joseph, Matthew Cheney, Robert G. Ojemann / 129-134Management of the Vertebral Artery During Excision of Extradural Tumors of the Cervical
Spine. Chandranath Sen, Mark Eisenberg / 135-142P o s t e roventral Pallidotomy for Patients with Parkinson’s Disease.
Robert P. Iacono, Shokei Yamada / 143-154Functional Hemispherectomy. Joseph R. Smith, Mark R. Lee / 155-164
M i c ro s u rgical Decompresson of the Root Entry Zone for Trigeminal Neuralgia.Chandranath Sen / 165-170
The Anterior Cervical Approach to the Cervicothoracic Junction. Julian K. Wu / 171-176Management of Extradural Non-Neoplastic Lesions of the Craniovertebral Junction via theTranscondylar Appro a c h . Luis A. B. Borba, Ossama Al-Mefty, T. Glenn Pait, Ronald Tribell /
1 7 7 - 1 8 4Far Lateral Lumbar Disc Herniation. Nancy E. Epstein, Joseph A. Epstein / 185-198
Repair and Reconstruction of Scalp and Calvarial Defects. Wa r ren Schubert, Jeff rey Aldridge / 199-218
Sagittal Synostosis. Larry A. Sargent, Timothy A. Strait / 219-226M i c ro s u rgical Lumbar Decompression Using Pro g ressive Local Anesthesia.
Stephen D. Kuslich / 227-232Banked Fibula, the Locking Anterior Cervical Plate, and Allogeneic Bone Matrix in Anterior
Cervical Fusions Following Cervical Discectomy. Scott Shapiro / 233-240Endoscopic Third Ventriculostomy for Obstructive Hydrocephalus.
Jonathan J. Baskin, Kim H. Manwaring / 241-246
Volume VI
Treatment of Caro t i d-C a v e rnous Sinus Fistulas Using a Superior Ophthalmic Vein Appro a c h .Neil R. Miller, Lee H. Monsein, Rafael J. Ta m a rgo / 1-4
The Separation of Craniopagus Twins. H a rold J. Hoffman, James T. Rutka / 5-12P o s t e roventral Pallidotomy for Parkinson’s Disease Patients.
Kim J. Burchiel, Jamal M. Taha, Jacques Favre / 13-26M i c ro e l e c t ro d e-Guided Pallidotomy. A n d res M. Lozano, William D. Hutchison / 27-34
A n t e rolateral Transforaminal Approach for a Large Dumbbell-Shaped Cervical Neurinoma.Isao Yamamoto / 35-42
Bridge Bypass Coaptation for Cervical Nerve Root Avulsion. Shokei Yamada, Russell R. Lonser, Robert P. Iacono / 43-50
Sinus Skeletonization Technique: A Treatment for Dural Arteriovenous Malformations atthe Tentorial Apex. E v a n d ro De Oliveira, Helder Tedeschi / 51-56
M i c ro s u rgical Carotid Endarterectomy. Julian E. Bailes, Patrick P. Flannagan / 57-64Endoscopic Approaches to the Ventricular System. David F. Jimenez / 65-74
S u rgical Management of Cranial Dural Arteriovenous Fistulas. Lokesh S. Tantuwaya, Julian E. Bailes / 75-84

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
Intraventricular Endoscopy: Diagnostic Ventriculoscopy, Tissue Biopsy, Cyst Fenestration,and Shunting. Jonathan J. Baskin, Kim H. Manwaring / 85-98
Endoscopic Carpal Tunnel Release Through a Monoportal Approach. Jay Menon / 99-108Endoscopic Excision of Colloid Cysts. Jonathan J. Baskin, Kim H. Manwaring / 109-114
S u rgical Anatomy of the Temporal Lobe. Steven N. Roper / 115-124Multiple Subpial Transection. Walter W. Whisler / 125-130
S t e reotactic Depth Electrode Implantation in the Evaluation of Candidates for AblativeEpilepsy Surgery. Joseph R. Smith, Mark R. Lee / 131-146
Tr a n s-Sulcal Approach to Mesiotemporal Lesions. Isabelle M. Germano / 147-156Anterior Cervical Spine Stabilization with the Codman Locking Plate System.
R. John Hurlbert, Volker K. H. Sonntag / 157-166Posterior Cervical Fusion with Tension Band Wiring. Thomas J. Lovely / 167-172
Primary Anterior Treatment of Thoracolumbar Burst Fractures. David W. Polly, Jr., Richard G. Ellenbogen / 173-182
Technique for Reduction of Spondylolisthesis Using Custom Texas Scottish Rite HospitalF o rceps. Gary L. Lowery, David A. Fernandez, Atul L. Bhat, A. Eugene Pennisi / 183-192
S u rgical Management of Infected Ventriculoperitoneal Shunt. Timothy M. George, Sohaib A. Kureshi / 193-200
Combined Fro n t o-Orbital and Occipital Advancement for Total Calvarial Reconstruction. Ian F. Pollack, H. Wolfgang Losken / 201-212
Repair of Meningoceles. Timothy M. George, Eric M. Gabriel / 213-220Installation of a Dorsal Column Stimulator for Pain Relief. John P. Gorecki / 221-236
Implantation of Drug Infusion Pumps. John P. Gorecki / 237-250S t e reotactic Micro s u rgical Craniotomy for the Treatment of Third Ventricular Colloid Cysts.
Kyle L. Cabbell, Donald A. Ross / 251-256H e m i s p h e rectomy. Benjamin S. Carson, Aaron L. Zuckerberg / 257-264
Volume VII
Posterior Lumbar Interbody Fusion Augmented With the Ray Threaded Fusion Cage.Peter Klara, Berkley Rish, Charles D. Ray / 1-10
Total Sacre c t o m y . Ziya L. Gokaslan, Marvin M. Romsdahl, Stephen S. Kroll, T h e resa A. Gillis, David W. Wildrick, Milam E. Leavens / 11-20
Treatment of Fractures at the Thoracolumbar Junction with Kaneda Anterior SpinalInstrumentation System. Seth M. Zeidman, Randy F. Davis / 21-28
Cannulated Screws for Odontoid and Atlantoaxial Transarticular Screw Fixation.Curtis A. Dickman, R. John Hurlbert / 29-42
Anterior Microforaminotomy for Cervical Radiculopathy: Disc Preservation Te c h n i q u e .Hae-Dong Jho / 43-52
Pedical Subtraction and Lumbar Extension Osteotomy for Iatrogenic “Flatback.”Gary L. Lowery, Atul L. Bhat, A. Eugene Pennisi / 53-58
The Surgical Treatment of Dolichoectactic and Fusiform Aneurysms. Michael T. Lawton, John A. Anson, Robert F. Spetzler / 59-68
P e t rosal Approach for Resection of Petroclival Meningiomas. William T. Couldwell / 69-82S u rgical Resection of Esthesioneuro b l a s t o m a . Scott L. Henson, John A. Jane, Sr. / 83-92
S t e reotactic Radiosurgery of the Trigeminal Nerve Root for Treatment of Trigeminal Neuralgia. Ronald F. Young / 93-98
Techniques of Peripheral Neurectomy for Control of Trigeminal Neuralgia. Raj Murali / 99-106

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
P e rcutaneous Balloon Compression for the Treatment of Trigeminal Neuralgia.
J e ff rey A. Brown, Jan J. Gouda / 107-116M i c rovascular Decompression for Hemifacial Spasm. Thomas J. Lovely / 117-124
Thalamic Deep Brain Stimulation for the Control of Tre m o r. A n d res Lozano / 125-134Magnetic Resonance Image-Guided Stereotactic Cingulotomy for Intractable Psychiatric
D i s e a s e . Osama S. Abdelaziz, G. Rees Cosgrove / 135-140Magnetic Resonance Image-Guided Pallidotomy. Antonio A.F. De Salles, Marwan Hariz / 141-148
Endoscopic Carpal Tunnel Release via a Biportal Appro a c h . David F. Jimenez / 149-156Thoracic Sympathectomy. J. Patrick Johnson, Samuel S. Ahn / 157-162
Blood Flow-Monitored Transthoracic Endoscopic Sympathectomy.R i c a rdo Segal, Peter M. Ferson, Edwin Nemoto, Sidney K. Wolfson Jr. / 163-172S u rgical Management of Craniopharyngiomas. H a rold J. Hoffman / 173-182
S u rgical Resection of Craniopharyngiomas. Ali F. Krisht, Ugur Türe / 183-190Optic Nerve Sheath Fenestration in the Management of Pseudotumor Cere b r i .
Eric L. Berman, Jonathan D. Wirschafter / 191-200S u rgical Correction of Unilateral and Bilateral Coronal Synostosis.
Ann Marie Flannery, Jack C. Yu / 201-210Te t h e red Cord Syndrome: Management of Myelomeningocele, Diastematomyelia, and
H y p e r t rophied Filum Te rm i n a l e . Robert F. Keating, James Tait Goodrich / 211-218Te t h e red Cord Syndrome: Management of Lipomyelomeningoceles.
James Tait Goodrich / 219-226Excision of Colloid Cyst via the Transcallosal Appro a c h . Deepak Awasthi, John J. Kruse /
2 2 7 - 2 3 4L a p a roscopy Assisted Lumboperitoneal Shunt Placement in the Management of
P s e u d o t u m o r C e re b r i . F l o rence C. Barnett, Dennis E. McConnell / 235-240The Transparaspinal Approach to Dumbbell-Shaped Spinal Tumors.
Stephen T. Onesti, Ely Ashkenazi, W. Jost Michelsen / 241-248Posterior Occipito-axial Fusion for Atlantoaxial Dislocation Associated with
Occipitalized Atlas. Vijendra K. Jain, Sanjay Behari / 249-256Evaluation and Management of Severe Facial Nerve Injury Resulting From
Temporal Bone Tr a u m a . Aijaz Alvi / 257-260
Volume VIII
S u rgical Management of Paraclinoid Carotid Aneurysms.Murali Guthikonda, Fernando G. Diaz / 1-12
S u rgical Management of Middle Cerebral Artery Aneurysms.Philip E. Stieg, Robert M. Friedlander / 13-22
S u rgical Removal of Tentorial and Posterior Fossa Dural Arteriovenous Malform a t i o n s .Adam I. Lewis, John M. Tew Jr. / 23-34
S u rgical Resection of the Arteriovenous Malformations of the Posterior Fossa.Thomas Kopitnik, Duke Samson, Michael Horowitz / 35-46
S u rgical Treatment of Arteriovenous Malformations of the Ventricular Tr i g o n e .Daniel L. Barrow, Roger H. Frankel / 47-56
Dural Arteriovenous Malformations of the Transverse and Sigmoid Sinuses. Todd A. Kuether, Gary M. Nesbit, Stanley L. Barnwell / 57-68

NEUROSURGICAL OPERATIVE ATLAS: TABLE OF CONTENTS
Operative Management of Anterior Fossa, Superior Sagittal Sinus, and Convexity DuralArteriovenous Malform a t i o n s . Aman B. Patel, Wesley A. King, Neil A. Martin / 69-78
Use of the Operating Arm System in Skull Base Surg e r y .J e ff rey J. Larson, Ronald E. Warwick, John M. Tew Jr. / 79-86
The Orbitocranial Zygomatic Approach to Aneurysms of the Upper Basilar Trunk. T. C. Origitano / 87-94
Extradural Approaches for Resection of Trigeminal Neurinomas. J. Diaz Day / 95-106S u rgical Management of Trigeminal Schwannomas.
Madjid Samii, Ramesh Pitti Babu, Marcos Tatagiba / 107-120S u rgical Management of Cholesterol Granulomas of the Petrous Apex.
Mark B. Eisenberg, Ossama Al-Mefty / 121-126S u rgical Management of Angiographically Occult Vascular
M a l f o rmations of the Brainstem, Thalamus, and Basal Ganglia.Gary K. Steinberg, Steven D. Chang / 127-134
Management of Jugular Foramen Tu m o r s . J e ff rey Bruce, Ian Storper / 135-142S u rgical Management of Esthesioblastomas. Ramesh Pitti Babu, Mark S. Persky / 143-152
S u rgical Treatment of Brainstem Gliomas. Mark R. Lee, Michael Cowan / 153-160Brainstem Gliomas. Harold J. Hoffman / 161-170
The Contralateral Transcallosal Approach to Lesions In or Adjacent to the Lateral Ve n t r i c l e .Michael T. Lawton, Robert F. Spetzler / 171-178
Posterior Fossa Decompression Without Dural Opening for the Treatment of Chiari I Malform a t i o n . Jonathan Sherman, Jeff rey J. Larson, Kerry R. Crone / 179-184Computed Tomography-Assisted Pre f o rmed Prosthesis for Repair of Cranial Defects.
Manuel Dujovny, Celso Agner, Fady T. Charbel, Lewis L. Sadler, Raymond Evenhouse, D i e rd re McConathy / 185-194
C h ronic Subthalamic Nucleus Stimulation for Parkinson’s Disease. Ali R. Rezai, William Hutchison, Andres M. Lozano / 195-208
A r t h roscopic Microlumbar Discectomy.Kenneth F. Casey, Parviz Kambin, Marc Chang / 209-216
Excision of Herniated Thoracic Disc Via the Transthoracic Appro a c h .Mary Louise Hlavin, Russell W. Hardy / 217-224
S u rgical Management of Advanced Degenerative Disease of the Lumbar Spine withM u l t i p l a n a r D e f o rm i t y . Michael F. O’Brien, Gary L. Lowery, A. Eugene Pennisi / 225-234
The Retropleural Approach to the Thoracic and Thoracolumbar Spine.T h e o d o re H. Schwartz, Paul C. McCormick / 235-242
S u rgical Treatment of Lateral Lumbar Herniated Discs.Giuseppe Lanzino, Christopher I. Shaff rey, John A. Jane, Sr. / 243-252
“ Trap Door” Exposure of the Cervicothoracic Junction.Ziya L. Gokaslan, Garrett L. Walsh / 253-260
Peripheral Nerve Suture Te c h n i q u e s .Rajiv Midha, Margot Mackay / 261-269

A
B
C
D
E
F
G
H
I
J
K
L
M
N
O
P
Q
R
S
T
U
V
W
X
Y
Z
AAblative epilepsy surgery, 6:131-146Acoustic neuromas, 4:159-164Acrylic cranioplasty, 5:214-215Acute subdural hematoma, 5:57-63Allogeneic bone matrix, 5:233-239Aneurysms
basilar bifurcation, 5:33-42broad-based siphon, 8:3-4; 8:10-11carotid cave, 8:3-4carotid ophthalmic, 8:2-3; 8:10-11carotid-superior hypophyseal, 8:3-4dolichoectatic, 7:59-67fusiform, 7:59-67middle cerebral artery, 8:13-22paraclinoid carotid artery, 8:1-12superior hypophyseal, 8:1-2; 8:10-11upper basilar trunk, 8:87-94ventral paraclinoid, 8:3-4; 8:10-11
Angiographically occult vascular malformations, 8:127-133
Angioma, cavernous, 4:13-18Anterior cervical spine
discectomy, 5:233-239implant systems, 5:101-108stabilization, 6:157-166
Anterior foramen magnum meningioma,5:23-32
Anterior fossa dural AVMs, 8:69-78Anterior microforaminotomy, 7:43-52Apert syndrome, 7:201Arteriovenous fistulas (AVFs)
cranial dural, 6:75-84dural, 4:3-7; 6:51-56intradural, 4:11-16perimedullary, 4:11-13
Arteriovenous malformations (AVMs)anterior fossa, 8:69-78basal ganglia, 4:43-58cerebellar hemisphere, 8:36; 8:40-42cerebellar tonsil, 8:36; 8:43-44cerebellar vermis, 8:35-36, 8:38-40deep parenchymal, 8:36dural, 8:23-34; 8:69-79glomus, 4:9-10juvenile, 4:8-10posterior fossa, 8:23-46spinal cord, 4:7-10
superior sagittal sinus dural, 8:69-78tentorial dural, 8:23-34thalamic, 4:43-58upper basilar trunk, 8:87ventral paraclinoid, 8:3-4; 8:10-11ventricular trigone, 8:47-56
Astrocytomasbrainstem, 8:162; 8:164; 8:165-169craniocervical, 8:169-170
Atlantoaxial dislocation with occipitalizedatlas, 7:249-256
Atlantoaxial instability, C1-2 screw fixation,4:19-28
Atlantoaxial transarticular screw fixation,7:29-41
BBanked fibula, 5:233-239Basal ganglia AVMs, 4:43-58Basilar bifurcation aneurysms, 5:33-42Bilateral coronal synostosis, 7:201-210Birth defects, 5:219-225Bone graft harvesting
fractures, 7:24-25atlantoaxial dislocation, 7:251-254calvarial defects, 5:199-217; 6:201-211posterior lumbar interbody fusion,
7:6-10Bone-wiring procedures, 5:91-100Brainstem
AVMs, 8:36; 8:43; 8:45-46craniocervical astrocytomas, 8:169-170dorsally exophytic gliomas, 8:161-163diffuse intrinsic astrocytomas, 8:162;
8:164focal intrinsic astrocytomas, 8:165-169gliomas, 8:153-159
Bridge bypass coaptation, 6: 43-50Broad-based siphon aneurysms, 8:3-4;
8:10-11Burst fractures, 5:110; 6:173-182
CCallostomy, 7:227-233Calvarial defects, 5:199-217Calvarial reconstruction, 6:201-211Cannulated screws, 7:29-41

Carotid cave aneurysms, 8:3-4Carotid endarterectomy, 6:57-64Carotid-cavernous sinus fistulas, 6:1-4Carotid ophthalmic aneurysms, 8:2-3;
8:10-11Carotid-superior hypophyseal aneurysms,
8:3-4Carpal tunnel syndrome, 6:99-108;
7:149-156Cavernous angiomas, 4:13-18Cavernous sinus tumors, 4:199-207Cerebellar hemisphere AVMs, 8:36; 8:40-42Cerebellar tonsil AVMs, 8:36; 8:43-44Cerebellar vermis AVMs, 8:35-36; 8:38-40Cerebral palsy, 4:183-190Cervical fusion, 5:233-239; 6:167-171Cervical nerve root avulsion, 6:43-50Cervical neurinoma, 6:35-41Cervical radiculopathy, 7:43-52Cervical spine
C1-2 screw fixation, 4:19-28degenerative disc disease, 7:43-52discectomy, 5:233-239extradural tumors, 5:135-141implant systems, 5:101-108stabilization, 6:157-166stabilization (articular mass), 5:91-100stabilization (Orion system), 5:101-108
Chiari I malformation, 8:179-183Children
cerebral palsy, 4:183-190moyamoya syndrome, 4:139-146
Cholesterol granulomas of petrous apex,8:121-125
Chondrosarcoma, 5:129Cingulotomy for psychiatric disease,
7:135-140Clivus, 5:129-133Codman locking plate system, 6:157-166Colloid cyst, 6:109-114; 6:251-256;
7:227-233Complex spinal schwannomas, 7:241-242 Convexity dural AVMs, 8:69-78Coronal synostosis, 4:67-73; 6:201-211;
7:201-210Corpus callosum sectioning, 4:38-39;
4:107-116Cranial defects, 8:185-194Cranial dural arteriovenous fistulas,
6:75-84Craniocervical brainstem astrocytomas,
8:169-170Craniopagus twins, 6:5-11Craniopharyngiomas, 7:173-181; 7:183-190Craniovertebral junction lesions,
5:177-184Crouzonís syndrome, 7:201Cubital tunnel syndrome, 4:235-249Cushingís disease, 4:165-172Cyst
colloid, 6:109-114; 6:251-256; 7:227-233fenestration, 6:85-98
DDecompressive corpectomy, 5:101Deep brain stimulation
control of tremor, 7:125-134subthalamic nucleus, 8:169-197;
8:200-201; 8:205-206Deep parenchymal AVMs, 8:36Degenerative disc disease, 7:43-52;
8:225-233Denervation for spasmodic torticollis,
4:59-65Diastematomyelia, 7:219-226Direct end-to-end repair of peripheral
nerves, 8:263-269Disc herniation
far lateral, 5:85-89far lateral lumbar, 5:185-197lateral, 8:243-251thoracic, 8:217-224
Disc preservation, 7:43-52Discectomy, cervical, 5:233-239Dolichoectatic aneurysms, 7:59-67Dorsal column stimulation, 6:221-235Dorsal lipomyelomeningocele, 7:221-225Dorsal rhizotomy, 4:183-190Drug infusion pumps, 6:237-250Dumbbell-shaped cervical neurinoma,
6:35-41Dumbbell-shaped spinal tumor, 7:241-248Dural AVFs, 4:3-7; 6:51-56; 6:75-84Dural AVMs
anterior fossa, 8:69-78convexity, 8:69-78inferior petrosal sinus, 8:29-32

petrous apex, 8:24-27posterior fossa, 8:23-46superior sagittal sinus, 8:69-78tentorial, 8:23-34
EElbow, ulnar nerve transposition,
4:225-233Electrode implantation, 6:131-146Endarterectomy, carotid, 6:57-64Endoscopy
approaches to the ventricular system,6:65-74
carpal tunnel release, 6:99-107;7:149-156
colloid cysts, 6:109-114fenestration of the third ventriculosto-
my, 5:241-246intraventricular, 6:85-98pituitary surgery, 5:1-12thoracoscopic sympathectomy,
7:157-162; 7:163-171Ependymoma, fourth ventricular, 4:95-106Epilepsy
ablative surgery, 6:131-146corpus callosum sectioning, 4:107-116medial temporal onset, 5:75-83
Esthesioblastomas, 7:83-91; 8:143-151Exophytic gliomas, 8:161-163Extradural non-neoplastic lesions,
5:177-184Extradural cervical spine tumors,
5:135-141
FFacial nerve injury, 7:257-260Facial pain, 5:227-232Far lateral disc herniation, 5:85-89;
5:185-197Fascicular peripheral nerves repair, 8:267Fields of Forel, 8:200Fistulas
carotid-cavernous sinus, 6:1-4dural arteriovenous, 4:3-7; 6:51-56; 6:75-
84intradural, 4:11-16
Flat-back syndrome, 7:53-58
Focal intrinsic brainstem astrocytomas,8:165-169
Foramen magnum, 5:23-32Fourth ventricular ependymoma, 4:95-106Frameless stereotaxy, intracranial lesions,
5:121-128Full facetectomy, 5:190-191Full thickness calvarial bone graft,
5:215-217Functional hemispherectomy, 5:155-164Fusiform aneurysms, 7:59-67Fusion tension band wiring, 6:167-171
GGalen, vein of, 8:32-34Gamma Knife radiosurgery, intracranial
lesions, 4:215-224Gliomas, brainstem, 8:153-159Glomus AVM, 4:9-10Glomus tumors, intracranial, 4:117-130Grafts, 5:233-239; 8:267-269
bone, 5:199-217; 7:6-10; 7:24-25;7:251-254
Granulomas, petrous apex cholesterol,8:121-125
HHematoma, acute subdural, 5:57-63Hemicorticectomy, 5:155Hemifacial spasm, 7:117-124Hemispherectomy, 5:155-164; 6:257-264Herniation
far lateral disc, 5:85-89far lateral lumbar disc, 5:185-197thoracic disc, 8:217-224
Horner’s syndromeand anterior microforaminotomy, 7:51complication of thoracoscopic
sympthectomy, 7:162Hydrocephalus, 5:241-246; 6:65; 6:76; 6:98;
6:261-264Hyperhidrosis, 7:158Hypertrophied filum terminale, 7:219-226
IIdiopathic intracranial hypertension,

7:191-200Implantation of drug infusion pumps,
6:237-250Infection of ventriculoperitoneal shunt,
6:193-200Inferior dental neurectomy, 7:103-104Inferior petrosal sinus dural AVMs, 8:29-32Infraorbital neurectomy, 7:101-103Interbody fusion, 4:147-157Intercostal neuralgia, 7:162Interhemispheric corridor and third-
ventricle exposure, 4:37-42Internal stabilization, 5:109-119; 5:233-239Intervertebral disc damage, 7:51-52Intracranial glomus tumors, 4:117-130Intracranial hypertension, 7:191-200Intracranial lesions, 4:75-83; 4:85-93;
4:215-224; 5:121-128Intracranial pressure monitoring, 5:65-74Intradural arteriovenous fistulas, 4:11-16Intraventricular endoscopy, 6:85-98Intraventricular shunt, 6:85-98Isthmic spondylolysis/spondylolisthesis,
4:147-157
JJugular foramen tumors, 8:135-142Juvenile AVMs, 4:8-10
KKambin instrumentation for microlumbar
discectomy, 8:211Kaneda anterior spinal instrumentation
system, 7:21-27
LLabbé, vein of, 8:58-60Lambdoidal synostosis, 4:44-45; 4:209-214Lateral disc herniation, 8:243-251Lateral mass plate and screws, 5:91-100Lateral orbitotomy, 4:81-83Lateral ventricles, 5:67-69Lipomyelomeningoceles, 7:219-226Lobectomy, temporal, 4:131-137; 5:75-83Locking anterior cervical plate, 5:233-239
Locking plate system, 6:157-166Low back pain, 5:227-232Lower clivus-anterior foramen magnum
meningioma, 5:23-32Lumbar decompression, 5:227-232Lumbar disc herniation, far-lateral, 5:185-
197Lumbar extension osteotomy for flat-back
syndrome, 7:53-58Lumbar spine
arthroscopic microlumbar, 8:209-216degenerative disease, 8:225-233far lateral disc herniation, 5:85-89far lateral lumbar disc herniation,
5:185-197foraminal stenosis, 8:227thoracolumbar fractures, 5:109-119
Lumboperitoneal shunt placement forpseudotumor cerebri, 7:235-240
MMeningioma
anterior foramen magnum, 5:23-32lower clivus, 5:23-32petroclival, 7:69-81torcular/peritorcular, 5:13-21
Meningoceles, 6:213-219Mental neurectomy, 7:103-106Mesiotemporal lesions, 6:147-156Microelectrode-guided pallidotomy,
6:27-33Microforaminotomy, anterior, 7:43-52Microsurgery
carotid endarterectomy, 6:57-64craniotomy for colloid cysts, 6:251-256lumbar decompression, 5:227-232root entry zone decompression,
5:165-170Microvascular decompression for
hemifacial spasm, 7:117-124Middle cerebral artery aneurysms, 8:13-22Moyamoya syndrome, 4:139-146MRI-guided pallidotomy, 7:141-148MRI-guided stereotactic cingulotomy,
7:135-140Multiple subpial transection, 6:125-129Myelomeningocele, 7:219-226

NNerve root avulsion, 6: 43-50Nerve root injury, 7:51Neurectomy for trigeminal neuralgia,
7:99-106Neurinoma, 6:35-41; 8:95-105Neuroblastomas, olfactory, 7:83-91; 8:
143-151Neuroma, acoustic, 4:159-164Non-neoplastic lesions of the cranioverte-
bral junction, 5:177-184
OObstructive hydrocephalus, 5:241-246Occipitalized atlas, 7:249-254Occipitoaxial fusion, 7:249-254Odontoid transarticular screw fixation,
7:29-41Olfactory neuroblastomas, 7:83-91;
8:143-151Operating Arm System, 8:79-85; 8:133Optic nerve injury, 8:12Optic nerve sheath fenestration, 7:191-200Orbit
anatomy, 4:75-81craniotomy, 4:85-93lateral orbitotomy, 4:81-83
Orbitotomy, 4:81-83Orion anterior cervical plate system,
5:101-108
PPain
facial, 5:227-232low back, 5:227-232relief, 6:221-235trigeminal neuralgia, 5:165-170
Pallidotomymicroelectrode-guided, 6:27-33MRI-guided, 7:141-148posteroventral, 5:143-153; 6:13-26subthalamic nucleus, 8:196-197;
8:200-201; 8:205-206Paraclinoid carotid artery aneurysms,
8:1-12
Parkinsonís diseasedeep brain stimulation for control of
tremor, 7:125-134MRI-guided pallidotomy, 7:141-148posteroventral pallidotomy, 5:143-153;
6:13-26subthalamic nucleus, 8:196-197;
8:200-201; 8:205-206Pedical screw, 5:112-113; 5:116-117Pedicle subtraction for flat-back syndrome,
7:53-58Percutaneous balloon compression for
trigeminal neuralgia, 7:107-116Perimedullary AVFs, 4:11-13Peripheral nerve suture techniques,
8:261-269Peripheral neurectomy for trigeminal
neuralgia, 7:99-106Peritorcular meningiomas, 5:13-21Petroclival meningiomas, 7:69-81Petrous apex
cholesterol granulomas, 8:121-125dural AVMs, 8:24-27
Pfeifferís syndrome, 7:201Pial synangiosis, 4: 139-146Pineal region masses, 4:29-36Pituitary
Cushing’s disease, 4:165-172surgery, 5:1-12
Plagiocephaly, posterior, 5: 43-55Pneumothorax, postoperative, 7:162Posterior C1-2 screw fixation, 4:19-28Posterior cervical fusion with tension band
wiring, 6:167-171Posterior fossa dural AVMs, 8:23-46Posterior lumbar interbody fusion, 7:1-10Posterior occipitoaxial fusion for
atlantoaxial dislocation, 7:249-254Posterior plagiocephaly, 5: 43-55Posterior stabilization, 5:91-100Posterolateral tentorium dural AVMs,
8:25-29Posteroventral pallidotomy, 5:143-153;
6:13-26Pseudotumor cerebri
lumboperitoneal shunt placement,7:235-240

optic nerve sheath fenestration,7:191-200
Psychiatric disease, surgery for, 7:135Pulse generator for subthalamic nucleus
stimulation, 8:205-206
RRadiosurgery of intracranial lesions,
4:215-224Radiosurgical dose planning, 7:94-96Radiosurgical localization, 7:94-96Ray Threaded Fusion Cage, 7:1-10Raynaud’s syndrome, 7:158Revascularization and
dolichoectatic/fusiform aneurysms,7:61-65
Rhizotomydorsal, 4:183-190spasmodic torticollis, 4:59-65
Rod placement and thoracolumbar junction fractures, 7:24-27
Root entry zone decompression,5:165-170
SSacrectomy, 7:11-20Sacrum tumors, 7:11-20Sagittal synostosis, 5:219-225Sathre-Chotzen syndrome, 7:201Scalp reconstruction, 5:199-217Schwannomas
complex spinal, 7:241-242trigeminal, 8:107-120
Screw fixationatlantoaxial instability, 4:19-28atlantoaxial transarticular, 7:29-41odontoid transarticular, 7:29-41
Seizuresablative epilepsy surgery, 6:131-146corpus callosum sectioning, 4:38-39;
4:107-116temporal lobectomy, 4:131-137
Shuntintraventricular, 6:85-98ventriculoperitoneal, 6:193-200
Sinus fistulas, carotid-cavernous, 6:1-4Sinus skeletonization technique, 6:51-56
Sinus, sagittal, 8:74-77Sinus, transverse-sigmoid, 8:57-68Spasmodic torticollis, 4:59-65Spasticity, 4:183-190Spina bifida, 7:219-226Spinal cord AVMs, 4:7-10Spinal exposure, upper thoracic, 4:173-182Spinal instrumentation, 7:21-27Spinal plate/screw placement, 7:23-25Spinal stabilization
cervical spine, 6:157-166cervical spine with articular plates and
screws, 5:91-100cervical spine with the Orion system,
5:101-108posterior, 5:91-100thoracolumbar fractures, 5:109-119
Spinal tumor, dumbell-shaped, 7:241-248Spinal vascular malformations, 4:1-18Spondylolisthesis, 4:147-157; 6:183-191Spondylolysis, 4:147-157Stabilization
cervical, 6:157-166lateral, 4:147-157posterior, 5:91-100thoracolumbar fractures, 5:109-119
Stereolithography for cranial repair, 8:188Stereotactic cingulotomy for psychiatric
disease, 7:135-140Stereotactic depth electrode implantation,
6:131-146 Stereotactic imaging and deep brain
stimulation for control of tremor,7:127-128; 7:141
Stereotactic microsurgical craniotomy,6: 251-256
Stereotactic radiosurgery of trigeminalnerve root, 7:93-97
Stereotaxy, frameless, 5:121-128Subclavian steal syndrome, 4:191-198Subdural hematoma, 5:57-63Substantia nigra pars reticulata/pars
compacta, 8:201Subthalamic nucleus, 8:196-197; 8:200-201;
8:205-206Superior hypophyseal aneurysm, 8:1-2;
8:10-11Superior sagittal sinus dural AVMs, 8:69-78Supraorbital, supratrochlear neurectomy,

7:99-101Sympathectomy, 7:157-162Synostosis
coronal, 4:67-73; 6:201-211; 7:201-210lambdoidal, 4:44-45; 4:209-214sagittal, 4:219-225
TTemporal bone trauma, 7:257-260Temporal lobe, 4:131-137; 5:75-83;
6:115-124Tension band wiring, 6:167-171Tentorial apex, 6:51-56Tentorial dural AVMs, 8:23-34Tethered cord syndrome, 7:219-226Texas Scottish Rite Hospital
forceps, 6:183-191system, 5:109-119
Thalamic AVMs, 4:43-58Thalamic mapping for control of tremor,
7:125-134Third ventricular colloid cysts, 6:251-256Third ventriculostomy for obstructive
hydrocephalus, 5:241-246Third-ventricle exposure, 4:37-42Thoracic disc herniation, 8:217-224Thoracic spine exposure, 4:173-182Thoracolumbar spine
burst fractures, 6:173-182fractures, 5:109-119junction fractures, 7:21-27
Thoracoscopic sympathectomy, 7:157-162Thrombectomy, 7:61-62Torcular/peritorcular meningiomas,
5:13-21Transthoracic endoscopic sympathectomy,
7:163-171Transverse-sigmoid sinus, 8:57-68Tremor, 7:125-134Trigeminal neuralgia
percutaneous balloon compression,7:107-116
peripheral neurectomy, 7:99-106microvascular decompression of root
entry zone, 5:165-170stereotactic radiosurgery of the trigemi-
nal nerve root, 7:93-97Trigeminal schwannomas, 8:107-120
Tumorscavernous sinus, 4:199-207dumbell-shaped spinal, 7:241-248ependymomas, 4:95-106extradural cervical spine, 5:135-141intracranial glomus, 4:117-130jugular foramen, 8:135-142orbital region, 4:87-90pineal region, 4:36sacrum, 7:11-20
Twins, craniopagus, 6:5-11
UUlnar nerve
entrapment, 4:235-249submuscular transposition, 4:225-233
Unilateral coronal synostosis, 4:67-73;7:201-210
Upper basilar trunkaneurysms, 8:87-94AVMS, 8:87
Upper clivus dural AVMs, 8:24-27
VVascular malformations
angiographically occult, 8:127-133spinal, 4:1-18
Vein of Galen, 8:32-34Vein of Labbé, 8:58-60Ventral intermediate thalamotomy, 7:125;
7:134Ventral paraclinoid
aneurysms, 8:3-4, 8:10-11AVMs, 8:3-4; 8:10-11
Ventricular AVMs, 8:52-58Ventricular system, 6:65-74Ventricular trigone AVMs, 8:47-56Ventriculoperitoneal shunt, 6:193-200Vertebral artery, 5:135-141
WWrist, ulnar nerve entrapment, 4:235-249
ZZona incerta, 8:200

INTRODUCTIONThe paraclinoid segment of the internal carotid artery(ICA) extends from the proximal dural ring up to theorigin of the posterior communicating artery. Aneu-rysms arising from this segment of the ICA accountfor 5% to 10% of all intracranial aneurysms. The sur-gical management of these aneurysms has techni-cally challenged most neuro s u rgeons because of thecomplex anatomy of this region and, most impor-tantly, the difficulty in obtaining proximal caro t i dc o n t rol prior to aneurysm clipping. A clear under-standing of the anatomy of this ICA segment and itsadjacent osseous, vascular, and neural structure swill optimize chances for successful surgical tre a t-ment of aneurysms of the paraclinoid segment.
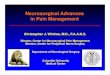
ANATOMYOf the many nomenclatures proposed to designatethe segments of the ICA, we have used the modifiedFischer classification proposed by the University ofCincinnati group as it describes the segments of theICA in an anterograde sequence (Figure 1).
The ICA traverses anteriorly through the cav-e rnous sinus as the C4 segment and bends twice asit exits the sinus: medially and superiorly at first andsubsequently posteriorly and superiorly, thus form-
SURGICAL MANAGEMENT OF PARACLINOID CAROTID ANEURY S M S
MURALI GUTHIKONDA, M.D., F.A.C.S. FERNANDO G. DIAZ, M.D., PH.D.
1
ing a loop and reversing its course by 180 d e g re e s .This so-called anterior loop is oriented appro x i m a t e l y4 5 d e g rees to the base of the skull. As the oculomo-tor nerve crosses this anterior loop coursing towardthe superior orbital fissure, its membranous epineu-rium blends with the adventitia of the ICA and ex-tends across to fuse with the periosteum of the sphe-noid bone. As it encircles the ICA, this layer ist e rmed the proximal dural ring; the tissue betweenthe oculomotor nerve and the ICA is called the ca-rotid-oculomotor membrane. After the ICA completesthe second bend, it emerges either from the roof orf rom the cavernous sinus, under the anterior clinoidp rocess and continues intracranially as the C6 seg-ment. The dura encircling the ICA as it exits the cav-e rnous sinus forms the distal dural ring. The seg-ment of the ICA between the proximal and distaldural rings is extracavernous, but not intradural,and is termed the C5 segment. The C5 and C6 seg-ments of the ICA together constitute the paraclinoidsegment.
The proximal C6 segment of the ICA remains hid-den under the anterior clinoid process beyond thedistal dural ring. Two branches arise from this seg-ment of the ICA: the ophthalmic artery and the supe-rior hypophyseal artery. The ophthalmic artery arisesdistal to the distal dural ring on the superior surf a c eof the ICA, bends forward, and travels through theoptic foramen lying inferior and lateral to the opticnerve. At times, the ophthalmic artery is adherent tothe dura of the optic canal floor and hence is insepa-© 1999 The American Association of Neurological Surg e o n s

rable. The superior hypophyseal artery, which can besingle or multiple, arises from the medial surface ofthe ICA as it emerges from the distal dural ring andc rosses over the diaphragma sellae.
CLASSIFICATIONBased on the site of origin and direction of pro j e c-
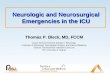
tion as it relates to the C5 and C6 segments, theaneurysms in this location can be classified into fourvariants, types I through IV (Figure 2). Any of the fourvariants of the aneurysms described below can en-l a rge, making classification difficult and impractical.
Types I(a) and I(b): Type I aneurysms are alsocalled carotid-ophthalmic aneurysms. The type I(a)
aneurysm variant is the most common paraclinoidaneurysm; it arises from the dorsal surface of the C6segment close to the ophthalmic artery. These aneu-rysms project superiorly into the subarachnoidspace, displacing the optic nerve upward and medi-ally. Presenting symptoms are either visual or due tor u p t u re with subarachnoid hemorrhage (SAH). Theseaneurysms can at times erode the anterior clinoidp rocess to a thin shell. The type I(b) aneurysm vari-ant re p resents a small subset of aneurysms thatarise from the superior surface of the C6 segment ofthe ICA, often a few millimeters from the ophthalmicartery origin. They are typically broad-based, sessile,and thin-walled.
NEUROSURGICAL OPERATIVE ATLAS. VOL. 82
F i g u re 1. Depiction of the segments of the ICA in an anterograde sequence. The paraclinoid seg-ment consists of C5and C6segments (University of Cincinnati modification of the Fischer classifica-tion). ACA = anterior cerebral artery; PCoA = posterior communicating artery. (Reproduced fro mBouthillier A, van Loveren HR, Keller JT: Segments of the internal carotid artery: a new classifica-tion. N e u ro s u rgery 38:425-433, 1996, with perm i s s i o n )
ACA
MCA
PCoA

GUTHIKONDA AND DIAZ : PARACLINOID CAROTID ANEURYSMS 3
F i g u re 2. Illustration showing the four variants of aneurysms. Type I(a) and I(b) variants arise from the dorsal surface of theC6 segment; the type I(a) aneurysm is closely related to the ophthalmic artery (OA) origin and the type I(b) aneurysm has nobranch relation and is often sessile. The type II variant arises from the ventral surface of the C6 segment without branchrelation. Insets A and B show variants in types III and IV. Type III(a) and III(b) aneurysms (supra- and infradiaphragmaticvariants), closely related to the superior hypophyseal artery (SHA) origin, arise on the medial surface of C6 and C5 seg-ments. The type IV variant is a large broad-based aneurysm extending from the distal C4 segment to the proximal C6 seg-ment, widening the distal dural ring. DS = diaphragma sellae.
B
type IV
OA
type II
type I(b)
type I(a)
OA
type III
A
DS
SHAtype III(a)
OA
type III(b)

NEUROSURGICAL OPERATIVE ATLAS. VOL. 84
Type II: Type II aneurysms, also called ventralparaclinoid aneurysms, arise from the ventral sur-faces of the C6 segment of the ICA. They have a broad base and the dome projects toward the ro o fof the cavernous sinus. The dome may extend intothe cavernous sinus in larger aneurysms. Theseaneurysms often present with third cranial nervepalsy and rarely with SAH.
Types III(a) and III(b): Type III aneurysms (alsocalled carotid-superior hypophyseal aneurysms) areclosely related to the origin of the superior hypophy-seal artery. Type III(a) aneurysms arise from themedial surface of the proximal C6 segment, pro j e c tabove the diaphragma sellae, and can present withSAH. This variant is the so-called carotid cave an-eurysm. The type III(b) variant arises from the medials u rface of the C5 segment and projects below the di-aphragma sellae and can be mistaken for a sellarmass on computed tomography (CT). Both variantscan enlarge to the extent of presenting both aboveand below the diaphragma sellae.
Type IV: Type IV aneurysms (also called bro a d -based siphon aneurysms) are often large or giant,and span from distal C4 to proximal C6 segments. Atleast one half of the circ u m f e rence of the vessel wallf o rms the broad base of the aneurysm. The baseexpands into the cavernous sinus and into the sub-arachnoid space. The dome often elevates the roof ofthe cavernous sinus and, at times, enlarges thep roximal and distal dural rings, thus projecting out-side the cavernous sinus under the anterior clinoidp ro c e s s .
PRESENTING SYMPTOMSBased on the type of paraclinoid-carotid aneurysm,p resenting symptoms can include SAH, ocular symp-toms of decreased visual acuity, visual field impair-ment, and diplopia; at times, re t ro-orbital pain is alsoa presenting symptom. Visual symptoms are usuallyipsilateral but can be bilateral, with contralateralcentral scotoma because of the involvement of theknee fibers of von Wi l l e b r a n d .
INITIAL MANAGEMENTPatients presenting with symptoms of SAH are admit-ted to the intensive care unit. Their clinical conditionis classified according to the Hunt and Hess gradingsystem. Respiratory support is provided for patientswith impaired sensorium. Indwelling catheters areused to monitor systemic arterial pre s s u re, centralvenous pre s s u re, and pulmonary arterial and wedgep re s s u res. Cardiac output, cardiac index, and sys-temic vascular resistance are optimized for each pa-tient. All patients receive intravenous phenytoin, andtherapeutic levels are maintained. Nimodipine is ad-m i n i s t e red in doses of 60 mg every 4 hours orally orvia a nasal gastric tube.
All patients diagnosed with paraclinoid-caro t i daneurysms undergo a detailed preoperative neuro -ophthalmological evaluation. Patients pre s e n t i n gwithout SAH undergo detailed visual field evaluation,and those presenting with SAH undergo bedsideevaluation by confrontation methods.
PREOPERATIVE RADIOLOGICAL EVALUATION
Computed To m o g r a p h yPatients presenting with SAH undergo cranial CT;the extent of hemorrhage is graded according to theFischer classification. The presence or absence ofh y d rocephalus is noted. A ventriculostomy is notp e rf o rmed unless the patient has impaired con-sciousness in association with CT evidence of hydro-cephalus. All patients above 50 years of age underg othin-section CT of the clinoidal region with bone win-dows to determine whether calcification is pre s e n twithin the aneurysm wall and the ICA. Any evidenceof erosion of the clinoid process is noted. If the ante-rior clinoid process has been eroded by theaneurysm and if the erosion is not detected, theaneurysm can be inadvertently torn while drillingthe clinoid pro c e s s .
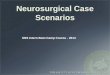
C e rebral AngiographySelective internal carotid angiography is perf o rm e don all patients via transfemoral selective catheteriza-tion. The direction of projection allows classificationof an aneurysm into one of the four types: types I(a),I(b), II, and IV are best visualized on the lateral pro-jection; type III is best seen in anteroposterior andsubmento-vertical projections (Figure 3).
Balloon Test Occlusion and Single Photon Emission CTIn patients with large or giant aneurysms, especiallya type IV variant or an aneurysm with extensive cal-cification, balloon test occlusion (BTO) with systemichypotension and single photon emission CT (SPECT)a re used to evaluate the patient’s tolerance for ca-rotid occlusion as a definitive therapy and to assessthe need for a bypass pro c e d u re. If a patient toler-ates the test occlusion clinically and SPECT does notreveal perfusion defects, permanent balloon occlu-sion of the ICA and trapping of the aneurysm areo ff e red as definitive therapy.
A vascular bypass is carried out in patients whodo not tolerate the BTO or who have significant per-fusion defects on SPECT. If the superficial temporalartery (STA) is greater than 1.5 mm in diameter, anS TA to M2 segment of the middle cerebral artery(MCA) bypass is carried out; if the STA is less than1.5 mm, a vein bypass graft is used from the cervicalICA to the M2 segment of the MCA.

GUTHIKONDA AND DIAZ : PARACLINOID CAROTID ANEURYSMS 5
F i g u re 3. The four variants of aneurysms seen by angiography. Types I (A), II (B), and IV (D) a re best visualized on lateralangiography and type III (C) on anteroposterior projection.
A B
C D

NEUROSURGICAL OPERATIVE ATLAS. VOL. 86
Magnetic Resonance Imaging and MR AngiographyThe exact dimensions of an aneurysm filled with at h rombus are better determined by a magnetic re s o-nance imaging (MRI) study. Coronal MRI of the sellara rea may preoperatively identify types III(a) andIII(b), the supra- and infradiaphragmatic variants ofthe paraclinoid aneurysm. This knowledge will helpin planning the extent of diaphragmatic divisionneeded to provide adequate exposure of the aneu-rysm. The infradiaphragmatic variant is visualizedonly after the diaphragma sellae is divided aro u n dthe superior surface of the dome of the aneurysm.Small and asymptomatic infradiaphragmatic vari-ants may not re q u i re surgical intervention if diag-nosed preoperatively.
SURGICAL TECHNIQUE
Timing of Surg e r yPatients who are classified in Hunt and Hess GradesI-IV undergo surgery within 24 hours after admis-sion. Surgery is delayed for patients classified in a Hunt and Hess Grade V or with multiple systemicp roblems (e.g., sepsis or aspiration pneumonia)until their clinical grade or general condition im-p roves.
Anesthetic Te c h n i q u eIntra-arterial and Swan-Ganz catheters are insertedto monitor blood pre s s u re and pulmonary arterialand wedge pre s s u res. The anesthetic agents used in-clude propofol (2.5 mg/kg), sufentanil (1-2 mcg/kg),v e c u ronium (0.1 mg/kg), lidocaine (1.5 mg/kg), and100% oxygen. Anesthesia is maintained with a per-centage concentration of Forane at subminimal alveo-lar concentration (i.e., the amount re q u i red to pre v e n tmovement with skin incision), continuous infusion ofp ropofol (25-75 mcg/kg/min), and sufentanil (0.5-1.0mcg/kg/min). Mean arterial pre s s u re is maintainedat 70 to 80 mm Hg. Mannitol is administered as a0.5-gm/kg bolus prior to craniotomy. If a temporaryclip cannot be applied or if the aneurysm rupture sduring dissection, the mean arterial pre s s u re is low-e red to 40 to 60 mm Hg by increasing the concentra-tion of Forane, a nitroprusside infusion, or both.
Patient PositioningThe patient is positioned supine with the head andthorax elevated by 15 degrees; the neck is neutral sothat the projected plane of the orbital roof is perpen-dicular to the ground. The head is rotated 15 degre e sto the contralateral direction. A motorized operativetable permits most changes in positioning durings u rgery. A full-length silicone gel pillow is placed onthe table.
The neck is included in the sterile operative field.The angle of the mandible and the anterior margin ofthe sternocleidomastoid muscle are marked afterp repping so that the carotid artery can either bec o m p ressed digitally or exposed for proximal contro l ,trapping, or a vein bypass pro c e d u re.
OPERATIVE PROCEDUREThe skin incision starts 1 cm anterior to the pre a u r i c-ular area just above the zygomatic arch, continuest o w a rd the midline, and curves forward toward thef o rehead, ending at the hairline in the opposite mid-pupillary line (Figure 4). If the anterior branch of theS TA is larger than the posterior branch, the scalpincision starts posterior to the main trunk, thuskeeping the main trunk with the scalp flap. If the pos-terior branch is larg e r, the incision is made anterior tothe STA trunk. The temporalis muscle is incisedalong with the scalp and retracted forward toward theorbital ridge. The supraorbital ridge and the fro n t o-zygomatic suture are exposed. The supraorbital nerveand vessel are retracted with the scalp flap; anosteotome is used to isolate the bony margins aro u n dthe neurovascular bundle, if enclosed in an osseousforamen, thus allowing the bundle to be mobilizedalong with the scalp. The orbital periosteum is sepa-rated superiorly and laterally from within the orbit.P recautions are taken to avoid perforation of the peri-orbital fascia, which could cause herniation of theperiorbital fat. If the subperiosteal plane is main-tained around the orbital ridge, the chance of disrup-tion of the orbital periosteum is lessened.
Craniotomy and Orbital Osteotomy F i g u re 5 shows frontal and oblique views of the cra-niotomy and oblique osteotomy. Three burr holes areplaced using a 7-mm Acra-Cut perf o r a t o r. The firstburr hole is made 1 cm above and lateral to thenasion. If the hole fails to penetrate both the innerand outer tables because of a large frontal sinus, theinner table is drilled separately to expose the dura. Asecond burr hole is made 5 cm posterior to the firstone and 1 cm from the midline, midway between thec o ronal suture and orbital ridge. A third burr hole ismade in the squamous temporal bone above themidzygomatic arch. The three burr holes are con-nected parallel to the midline and posteriorly. Forleft-sided aneurysms, the craniotomy is made asclose to the midline as possible.
A keyhole opening is made at the level of theorbital roof, posterior to the frontozygomatic suture ,using an acorn-shaped dissecting burr; this openingexposes the floor of the anterior cranial fossa superi-orly and the orbit inferiorly. Once the dura materand orbital periosteum are separated from eitherside of the orbital roof, its lateral-most part is nib-bled using a needle-nose Leksell ro n g e u r.

GUTHIKONDA AND DIAZ : PARACLINOID CAROTID ANEURYSMS 7
F i g u re 4. Scalp incision preserving the STA trunk and the frontalis innervation.
F i g u re 5. F rontal (A) and posterior oblique (B) views outlining the frontotemporal craniotomy with supraorbital ridgeosteotomy, elevated as a single flap. Note the keyhole burr hole with orbit inferiorly and frontal dura superiorly, and that thepterion is drilled down.
A B
facial nerve
STA

NEUROSURGICAL OPERATIVE ATLAS. VOL. 88
An osteotomy extends across the orbital ridgef rom the supraorbital burr hole into the orbital ro o fusing a C1 dissecting tool. A second osteotomy isp e rf o rmed across the frontozygomatic suture andthe lateral wall of the orbit. The pterional area isdrilled down and thinned. At this point, the cranialbone flap with the supraorbital ridge is lifted fro mthe dura and rotated forward and down. As a re s u l t ,the orbital roof will fracture, connecting the keyholeopening to the supraorbital osteotomy across theorbital roof. The bone flap is removed in one piecewith the orbital rim.
A self-retaining retractor system is attached to theMayfield clamp. The dura is elevated from the ante-rior cranial fossa and the tip of the middle fossa. Thepterion and greater wing of the sphenoid are drilledflat until the entire shiny inner cortical bone is seenand the lateral edge of the superior orbital fissure isvisualized. The posterior part of the orbital roof andthe lateral part of the lesser wing are removed usinga fine ro n g e u r.
The frontal sinus is often entered and the entiremucosa and posterior wall are removed, thus cra-nializing the sinus. The frontonasal duct is obliter-ated by a small piece of temporalis muscle graft.
Dural Opening and Arachnoidal Dissection The dura is opened in a T-shaped fashion. Its stemcontinues along the sylvian fissure: one limb extendsmedially across the orbital ridge toward the midlineand the other limb extends laterally toward the tem-poral pole and the floor of the middle fossa, thusleaving the dural flaps to protect the brain surf a c e .Under microscopic magnification, the sylvian fissureis opened widely, usually from its lateral to medialend. The entire MCA complex is exposed. The sylvianveins are preserved and are left attached to the tem-poral lobe. The frontal lobe is elevated from the opticnerve and optic chiasm; all arachnoid strands aresharply divided. The lamina terminalis is exposedand opened to allow drainage of cere b rospinal fluidf rom the ventricles. The cisterns around the opticnerve and the ICA are opened widely. In type I an-eurysms that project superiorly, the dome of theaneurysm may be adherent to the frontal lobe. Ele-vation and traction of the frontal lobe must be donegently, dividing all arachnoid strands until the entirea rea is exposed.
Resection of the Anterior Clinoid Process Once the frontal lobe is elevated, the retractor bladesa re adjusted. The tips of the blade are inclinedt o w a rd the tip of the anterior clinoid process to cre a t ea conical exposure (wide near the surface and narro wat the depth near the anterior clinoid process), thusminimizing the retraction pre s s u re that is on the
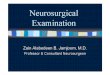
basal surface of the frontal lobe. The dura over theanterior clinoid process and the optic canal is coagu-lated, incised, and elevated medially as a flap in ord e rto expose the roof of the optic canal and the anteriorclinoid process (Figure 6A). Using a diamond-tippeddissecting tool, the entire optic canal is unroofed in ap o s t e roanterior direction under continuous irriga-tion. Next, the anterior clinoid process is drilled fro mits tip to the base, keeping in mind that the contentsof the superior orbital fissure are on its infero l a t e r a laspect, the anterior loop of the ICA is directly under-neath, and the optic nerve is medial (Figure 6B).Once the anterior clinoid process is resected, theoptic strut is further isolated by the elevation of thedura from the floor of the optic canal superiorly andthe second deflection of the anterior loop of the ICAd o w n w a rd. Using a fine diamond-tipped burr, theoptic strut is drilled further. Curettes and ro n g e u r sa re not used, as they are not as precise and atrau-matic as the drill.
P roximal Control (C4 and C5 Segments)To attain proximal control, the ICA can be exposed int h ree are a s :
Cervical carotid artery (C1). If the aneurysm isl a rge and encroaches on the entire cavernous sinus,the cervical carotid artery is exposed for pro x i m a lc o n t rol.
C a v e rnous carotid segment (C4). The temporallobe is retracted laterally to expose the oculomotornerve as it enters the roof of the cavernous sinus. Asickle-shaped knife is used to incise the dural sleeveon the medial margin of the oculomotor nerve fro mthe point of its entrance into the roof of the cav-e rnous sinus to the superior orbital fissure. Thisallows the entire contents of the superior orbital fis-s u re to be retracted away from the anterior loop ofthe ICA. The cavernous sinus is opened by incisingits roof, extending from the distal dural ring to theposterior clinoid process. Bleeding encountered fro mthe cavernous sinus, both medial and lateral to thec a v e rnous carotid artery, is controlled by gentlepacking with small pieces of Gelfoam. Dissection ofthe lateral aspect of the ICA must remain close to theartery to prevent injury of the sixth cranial nerve.The cavernous carotid artery is isolated (Figure 6C),thus enabling placement of a temporary clip forp roximal control.
C5 segment. The distal dural ring is divided cir-c u m f e rentially around the ICA across the floor of theoptic canal (after the ophthalmic artery is dissectedf ree) and across the roof of the cavernous sinust o w a rd the diaphragma sellae. The C5 segment isdissected from the inferior surface of the optic strut,enabling temporary clip placement for proximal c o n t rol.

GUTHIKONDA AND DIAZ : PARACLINOID CAROTID ANEURYSMS 9
F i g u re 6. A, dural incision outlined over the anterior clinoid process and the optic canal; B, the optic canal is unroofed and anterior clinoid process drilled away; note the oculomotornerve seen through the membranous layer after clinoidectomy. C , c a rotidoculomotor mem-brane is incised medial to the third nerve and the nerve is retracted laterally. The cavern o u ssinus roof is opened and the C4 and C5 segments of the ICA are exposed for proximal con-t rol. II and III indicate cranial nerves.
A
anteriorclinoidprocess
optic canal
II
III
B
C
II
optic strut
III
C5
C6
C4
C5
C6
III
Gelfoam
II
proximal dural ring
distal dural ring
ophthalmicartery
superior hypophyseal
artery

ISOLATION AND CLIPPING OF THE ANEURYSM The four variants of aneurysms are shown with idealplacement of clips in Figure 7.
Type I(a) (Carotid-Ophthalmic Aneurysm) In type I(a) aneurysms, the optic canal sheath is in-cised longitudinally to allow gentle retraction of theoptic nerve. The arachnoid strands, which lie be-tween the optic nerve and the ICA and the aneu-rysm, are sharply divided. The ophthalmic artery isidentified. The carotid artery is displaced laterally.With large aneurysms, proximal control is achievedby exposing the C4 or C5 segments of the ICA. Mostaneurysms projecting superiorly can be clipped byusing a 45-degree angled clip, placing the bladesparallel to the long axis of the carotid artery.
At times, a carotid segment can be so ectatic thatthe aneurysm neck may be located medial to theoptic nerve. In these instances, the tuberculum sellais drilled medial to the optic nerve. The optic nerve isretracted laterally and the clip is applied from itsmedial aspect.
Type I(b) (Carotid-Ophthalmic Aneurysm)Type I(b) aneurysms are difficult to obliterate be-cause they are broad-based and sessile. Wide mobi-lization of the carotid artery with circ u m f e re n t i a ldivision of the distal dural ring followed by pro x i m a land distal temporary clipping make the segment ofthe ICA become slack, thus allowing satisfactory clipplacement with the blades parallel to the caro t i dartery. At times, a portion of the parent vessel mayneed to be included in the clip blades, as the base isvery thin and fragile and may tear with appro x i m a-tion of the clip blades.
Type II (Ventral Paraclinoid Aneurysm) The optic nerve sheath is incised longitudinally tofacilitate gentle medial retraction of type II aneu-rysms. The distal dural ring along the floor of theoptic canal is incised and the C5 segment is mobi-lized laterally for proximal control. A right-angledfenestrated clip is placed, with the blades on theu n d e r s u rface of the ICA parallel to its long axis andthe parent vessel passing through the fenestration.At times, a second fenestrated clip may need to beplaced parallel to the first one so as to totally obliter-ate and occlude the neck of the aneurysm. If theaneurysm projects significantly into the cavern o u ssinus, the rigid dura of the roof of the cavern o u ssinus that encircles the aneurysm does not allow theclip blades to approximate. Dura forming the roof ofthe cavernous sinus can be incised circ u m f e re n t i a l l ya round the waist of the aneurysm, allowing the clipblades to approximate and occlude the neck of theaneurysm. The tips of the clip blades must be
inspected for inadvertent encroachment of the C5segment.
Type III (Superior Hypophyseal Aneurysm)P reoperative studies do not always clarify whether atype III aneurysm is projecting above or below thediaphragma sellae. Definitive assessment of the loca-tion can only be made by exploration. Proximal con-t rol is achieved in large aneurysms by exposing thec a v e rnous carotid artery (C4 segment). The opticnerve sheath is incised and the optic nerve is gentlyretracted medially to bring the supradiaphragmaticvariant into view. After isolating the ophthalmicartery, the dura along the floor of the optic canal isincised and the C5 segment is mobilized laterally. Thesupradiaphragmatic variant aneurysm can be visual-ized and a 90-degree angled fenestrated clip is ap-plied from a lateral direction. In the infradiaphrag-matic variant, the aneurysm is hidden under thediaphragm and not visible when the C6 segment isdisplaced laterally. When faced with this variant, thedistal dural ring is incised circ u m f e rentially aro u n dthe carotid artery, and extending medially across thediaphragma sellae, leaving a cuff of the dura attachedto the periphery of the aneurysm. The roof of the cav-e rnous sinus is opened during this process, andbleeding is controlled by packing with Gelfoam. Thepituitary gland is identified medial to the aneurysm.A 90-degree curved fenestrated clip (placed encirc l i n gthe ICA) will obliterate the aneurysm.
Type IV (Broad-Based Siphon Aneurysm)When clipping a type IV aneurysm, the optic nervesheath is incised and the nerve is gently re t r a c t e dmedially. The ophthalmic artery is identified. Thedura is incised along the roof of the cavernous sinusmedial to the oculomotor nerve, and the nerve is retracted laterally. The distal dural ring is oftenwidened or made incompetent by the large aneu-rysm. This dural ring, along with the dura on theroof of the cavernous sinus, is incised around theaneurysm. The dura on the floor of the optic canalunder the ophthalmic artery is incised, thus en-abling the mobilization of the C5 and C6 segments. Atemporary clip is placed on the C4 and C6 segments,and the aneurysm is trapped. A right-angled fenes-trated clip is applied encircling the carotid artery; theclip blades are placed on the inner curvature of theartery along the neck of the aneurysm. Often, multi-ple serial clips are needed to obliterate the entirelength of the aneurysm neck. If the clip slides towardthe carotid artery and compromises the lumen, asecond clip is placed tangentially; the aneurysm iscollapsed with a 25-gauge needle and the first clip is removed. After restoration of the patency of the ca-rotid artery and obliteration the aneurysm, the tem-porary clips are re m o v e d .
NEUROSURGICAL OPERATIVE ATLAS. VOL. 810

GUTHIKONDA AND DIAZ : PARACLINOID CAROTID ANEURYSMS 11
F i g u re 7. Illustrations depicting the four variants of aneurysms with ideal clip placement.
ophthalmic artery
MCA
ACAtype I type II
type III type IV

NEUROSURGICAL OPERATIVE ATLAS. VOL. 812
P i t f a l l sType IV aneurysms and, less frequently, variants ofparaclinoid aneurysms may contain significant calci-fication in the vessel wall. Attempts to clip a heavilycalcified aneurysm may be dangerous because of therisks of avulsion of the aneurysm, embolic phenom-ena with ischemic complications, or the inability toobliterate the aneurysm. Obliteration of a markedlycalcified aneurysm is difficult in elderly patients.P reoperative CT scans may alert the surgeon to thepossibility of calcification. If a calcified aneurysm ise n c o u n t e red and if the presenting symptoms are notdue to SAH, the pro c e d u re may be terminated or abypass pro c e d u re perf o rmed, followed by endovas-cular balloon occlusion of the ICA.
C l o s u reThe anterior clinoid process and optic strut may bepneumatized and must be recognized while drilling.This sinus communication must be obliterated priorto closure. A small fat graft obtained from deep tem-poral fat or from the abdomen is secured in placewith fibrin glue.
Wound closure is done in the usual fashion toachieve a watertight dural closure. The frontal sinusis obliterated with fat or muscle and secured in placewith cryoprecipitate. A small local periosteal flap isrotated from the scalp over the sinus and sutured tothe adjacent dura. The fronto-orbital bone flap isreplaced and secured with plates and screws. A sub-galeal suction drain is left in place for 24 hours.
COMPLICATIONS
Optic Nerve Injury and BlindnessThis is the most frequently encountered postopera-tive complication in the management of paraclinoid-c a rotid aneurysms. Although the optic nerve can bei n j u red while unroofing the optic canal, the chancesfor injury can be decreased by following the princi-ples of drilling: “Hold tight and stroke gently.” Thedura covering the optic nerve must not be disruptedby the drill. The field is continuously irrigated withcool saline to decrease the chance of thermal injuryto the nerve. The pial vessels of the optic nerve mustnot be disrupted while incising the dural sleeve.Retraction must be minimal and brief. Completee x p o s u re of the anterior loop and extensive mobiliza-tion is pre f e r red, thus allowing the artery to beretracted laterally rather than retracting the nerve
medially. The ophthalmic artery must be identifiedb e f o re incising the dura on the floor of the optic canaland the distal dural ring to avoid inadvertent injury.
C e re b rospinal Fluid Rhinorrh e aThe frontal sinus entry must be identified and pro p-erly managed. The sphenoid sinus and the posteriorethmoid sinuses may have opened during clinoidec-tomy and be recognized and obliterated.
Role of Intraoperative AngiographyPatency of the carotid artery is easily evaluated usingm i c roDoppler ultrasound after aneurysm oblitera-tion. In large and complex aneurysms, a radiolucentheadholder is used in preparation for angiographyand the patient’s neck is included in the sterile oper-ative field. The ICA is punctured percutaneously orby an open method, and the angiography is com-pleted.
S u rgical Experience Using the above classification, 99 (95%) of 115patients who had aneurysms near the paraclinoidsegment underwent successful clipping of theaneurysm. Four patients underwent a bypass pro c e-d u re to the M2 segment of the MCA, using a saphe-nous vein bypass in two patients and an STA in theother two. Postoperative endovascular trapping ofthe aneurysm was completed following the confirm a-tion of the patency of the bypass. The re m a i n i n gpatients underwent trapping without a bypass.
CONCLUSIONSPatients with ICA aneurysms of the paraclinoid seg-ment who are considered for surgical interventionshould be evaluated thoroughly using selectiveangiography. In patients with complex and larg eaneurysms, CT and MRI studies can provide infor-mation re g a rding their size, relation to the adjacents t r u c t u res, and presence of calcification. Identifica-tion of the aneurysms into one of four types facili-tates operative planning, thus allowing successfulclipping. As optic nerve dysfunction is the most fre-quent complication, very little retraction should beapplied to the optic nerve, and the micro v a s c u l a t u reof the optic nerve should not be disturbed. A clearunderstanding of the paraclinoid segment of the ICAanatomy is important to ensure successful tre a t-ment of aneurysms presenting in this are a .

INTRODUCTIONThe middle cerebral artery (MCA) is the second
most common site of aneurysm formation; in Ya s a r-gil’s 1984 series it re p resented 20% of all aneurysms.In addition, aneurysms in this region are the thirdmost common site associated with subarachnoidh e m o r rhage (SAH). Typically, the aneurysms occur atthe bifurcation of the M1 segment of the MCA; how-e v e r, they may occur proximal or distal to this point.Aneurysms in this location are particularly challeng-ing to the microvascular surgeon for several re a s o n s ,including the following: 1) they are frequently associ-ated with hematomas that may be adherent to andd i fficult to dissect from the fundus of the aneurysm;2) the anatomical variability of the M1 segment andthe associated medial and lateral lenticulostriate ves-sels re q u i re meticulous technique; and 3) the overallanatomic complexity of the sylvian fissure demandspatient micro s u rgical dissection. In addition, MCAaneurysms are frequently broad-based and include aportion of the distal M2 segment, thereby re q u i r i n gunusual or multiple clip configurations.
In 1944, Dandy provided the first report on surg i-cal treatment of MCA aneurysms. Each case re s u l t e din a fatality. Successful treatment of an aneurysm in this region was first reported by Dott. Curre n t l y ,
SURGICAL MANAGEMENT OF MIDDLE CEREBRAL ART E RY
A N E U RY S M SPHILIP E. STIEG, PH.D., M.D.
ROBERT M. FRIEDLANDER, M.D.
13
t h e re are three surgical approaches to MCA aneu-rysms: 1) proximal to distal, exposing the intern a lc a rotid artery within the basal cistern and dissectingalong the path of the sylvian fissure; 2) a transtem-poral approach through the superior temporal gyrus;and 3) the transsylvian approach with direct splittingof the sylvian fissure.
This chapter reviews the anatomy of the sylvianf i s s u re as well as the preoperative assessment andmanagement of aneurysms associated with the MCA.M o re specifically, the various surgical techniques fort reatment of these lesions and the complicationsassociated with their management are discussed.
SURGICAL ANATOMYThe internal carotid artery bifurcates lateral to the
optic chiasm, at the junction of the carotid and syl-vian cisterns, into the MCA and the anterior cere b r a lartery (Figure 1). In approximately 70% of cases, theMCA is the larger branch. The first segment (M1) ofthe MCA courses laterally 1 cm posterior to the sphe-noid wing and enters the deep sylvian fissure run-ning horizontally in its sphenoidal portion. The meanlength of the M1 segment is 14 to 17 mm. Several im-portant and variable vessels arise from the M1 seg-ment, which can be classified in the inferior medial( p e rforating) or superior lateral (temporal) groups. Itis of paramount importance to understand the nor-mal neurovascular course as well as the commonvariants of the MCA branches in order to adequatelyi n t e r p ret angiographic anatomy and effectively dealwith surgical lesions.© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 814
F i g u re 1. Schematic view of the sylvian fissure after micro s u rgical opening. The origin of the MCA from the internal caro t i dartery and its proximal branches are demonstrated. M2: branches of the main MCA (M1) segment.
temporal lobe
posterior communicating artery
anterior clinoid artery
optic nerve
A1 segment of theanterior cerebral
artery
artery of Heubner
lenticulostriate vessels
M1 segment of the MCA
frontal lobe
superior trunk of the M2 segment
inferior trunkof the M2 segment
sylvian fissure
anterior temporal artery
oculomotor nerve
anterior choroidal artery

STIEG AND FRIEDLANDER : SURGICAL MANAGEMENT OF MIDDLE CEREBRAL ARTERY ANEURYSMS 15
The inferior medial group (lenticulostriate perf o r a-t o r s ) originates on the inferior medial surface of theM1 segment, demonstrating significant variations insize and number (range two to 29). They may arise asindividual branches directly from the M1 segment oras larger feeders that branch into multiple smallerarteries. Ya s a rgil notes that in 40% of cases, a singlel a rge vessel originates from the M1 segment andthen divides into smaller perforators. Two additionalp a t t e rns are described, one (30%) where there aretwo main branches that thereafter divide and theother (30%) where the small lenticulostriate vesselsd i rectly arise from the M1 segment. Lenticulostriatevessels may also arise from the proximal portion ofone of the two M2 segments. The lenticulostriate ves-sels course medially into the lateral aspect of the an-terior perforated substance, supplying a portion ofthe nuclei of the basal ganglia, the superior half ofthe internal capsule, and the lateral segment of theanterior commissure .
The superior lateral group of vessels includes theuncal artery, the polar temporal artery, and the ante-rior temporal artery. The anterior temporal branchcourses anteriorly and turns above the superficial as-pect of the sylvian fissure en route to the anteriortemporal lobe surface. The uncal artery arises 30% ofthe time as a lateral M1 branch and 70% as a dire c tbranch from the internal carotid artery. On occasion,the polar temporal artery is hypoplastic and the ante-rior temporal artery is re c i p rocally larg e r. In this case,the anterior temporal artery supplies the distributionof both vessels. The surgeon must also be careful inthis situation not to confuse the anterior temporalartery take-off with the true M1 bifurcation. An alter-nate variant in which both the polar temporal arteryand the anterior temporal artery are hypoplastic hasbeen described. In this situation, a large branch orig-inating from the inferior M2 segment usually suppliesthe respective territories.
The MCA bifurcation is located just medial to thehigh point of the limen insulae at the junction of thesphenoidal and operc u l a r-insular subdivisions of thesylvian cistern. Because the sylvian cistern is sur-rounded by brain, MCA bifurcation aneurysms areoften embedded in the parenchyma. There f o re, rup-t u red lesions commonly present with intrapare n c h y-mal hemorrhage in addition to SAH. The junction ofthe temporal and frontal operculas can be used ass u p e rficial cortical landmarks to commence explo-ration of the bifurcation of M1 and M2. The M1-M2junction is usually located 1.5-2 cm posterior to theanterior aspect of the insular portion of the sylvianf i s s u re and 2-2.5 cm deep to the superior temporalsulcus. Two M2 branches arise from the bifurc a t i o n ,the superior and inferior segments. The M2 segmentsthen turn superior-posterior reaching the insulars u rface. The two segments separate initially at the
b i f u rcation and then come into close proximity in theo p e rc u l a r-insular portion of the sylvian fissure. Oftendistal to the true bifurcation, large M3 branchesmight arise, creating the impression of a trifurc a t i o nas well as causing confusion as to the location of thetrue bifurcation. On the other hand, a true trifurc a-tion or greater number of branching vessels is foundin up to 22% of cases. In true M1 bifurcations, theinferior trunk is larger in 41% of cases, the superiortrunk in 36%, and they are of equal size in 23%. Theterritory supplied by the superior trunk includes theinferior frontal cortex, the frontal opercular cortex,and the parietal and central sulcus territories. Theterritory supplied by the inferior trunk includes themiddle temporal cortex, the posterior temporal cor-tex, and the angular and posterior parietal re g i o n s .
VASCULAR ABNORMALITIES ASSOCIATEDWITH THE MIDDLE CEREBRAL ARTERYIt is important to be aware of the more common vas-cular abnormalities present in the MCA. McCorm i c knoted in his landmark autopsy study of 1000 con-secutive brains that the MCA was the least likelymajor intracranial vessel to harbor an anatomicala b n o rmality. Albeit uncommon, aneurysms appearm o re frequently in patients with anatomical neuro-vascular abnormalities. Fenestrations are re p o r t e din the proximal portion of the M1 in 2% of cases anda re often associated with aneurysms, which formsecondary to intimal deficiencies at the proximal bi-f u rcation. An accessory MCA may also be pre s e n tand originate from the junction of A1 and A2, pro x i-mal A1, or the distal internal carotid artery.
PATIENT SELECTIONWe recommend that the patient presenting in goodn e u rological status (Grades I-III on the Hunt-Hessscale) after an SAH be treated urgently as the risk forre h e m o r rhage is significant. However, each casemust be individualized and surgical decisions shouldbe based on age, grade of patient, aneurysm size andcomplexity, medical issues, and operating room per-sonnel. The patient in a poor neurological status(Grades IV-V on the Hunt-Hess scale) may impro v efollowing a ventriculostomy and become a good can-didate for surgery. Aneurysms in this region are fre-quently associated with large hematomas and masse ffect causing a worsened neurological picture. Inthis case, emergent surgery may also be indicatedbased on mass eff e c t .
The management of incidental aneurysms in thisregion is controversial because of conflicting data ontheir natural history. Recent data suggest that size isthe critical issue in deciding to operate. All aneu-rysms greater than 10 mm are treated unless therea re medical contraindications. For lesions less than10 mm in size, the surgeon must perf o rm a re l a t i v e

risk analysis between the surgical morbidity/mortal-ity rate and the risk for aneurysm rupture which,after a rupture occurs, has a mortality rate of up to60%. Again, surgical decision making is multifactor-ial and each case must be treated individually.
SURGICAL TECHNIQUEP o s i t i o nThe patient is placed supine on the operating tablewith a roll under the ipsilateral shoulder. The skull isimmobilized with the Mayfield headholder, elevatedabove the heart, and rotated 45 degrees contralateralto the incision; the neck is flexed slightly to the con-tralateral shoulder to flatten the orbital roof and thevertex is lowered slightly. These maneuvers facilitateopening of the sylvian fissure with minimal tractionon the frontal and temporal lobes. Care is taken toavoid venous outflow obstruction in the neck, eithert h rough positioning or methods used to secure theendotracheal tube. This position allows the surg e o nto pursue any of the three surgical appro a c h e s .
Incision and CraniotomyA standard frontotemporal or pterional incision,made completely behind the hairline, is ro u t i n e l yused (Figure 2). The incision is started no more than1 cm anterior to the tragus of the ear at the root ofthe zygoma and extends behind the hairline up tothe midline. Placing the incision in this location pre-vents injury to the frontalis branch of the seventhcranial nerve. The skin is dissected separately andreflected inferiorly over a rolled sponge with fishhookretractors. It is important to stay deep to the fat-padin the keyhole region to avoid injury to the fro n t a l i sbranch of the seventh nerve. The temporalis muscleis then incised along the superior temporal line andthe posterior margin of the incision. The muscle isreflected inferiorly with the skin flap to provide ade-quate bony exposure. Leaving the superior tuft ofmuscle allows for a better cosmetic closure uponcompletion of the case. Three burr holes are placedindividually in the pterion or keyhole region, thetemporal squamous bone slightly above the root ofthe zygoma, and at the posterior margin of the inci-sion at the height of the temporalis muscle. A stan-d a rd pterional bone flap is elevated with cuts be-tween the burr holes, as demonstrated in Figure 2.The temporal squamous bone is removed with ro n-geurs and the lateral roof of the orbit and lesser wingof the sphenoid bone are drilled down until the orb-ital meningeal artery is visualized. This bony re m o v a lp rovides better exposure of the proximal sylvian fis-s u re and allows gentle traction on the temporal lobe.After Surgicel and narrow cottonoid patties areplaced around the margins of the craniotomy, thedura is opened in a crescent moon-shaped fashionc e n t e red over the sylvian fissure. This minimizes ve-
nous run-in. In addition, all bony margins are waxedto prevent air emboli. Subsequently, the dura isplaced on stretch with sutures and covered withmoist patties to facilitate dural closure upon comple-tion of the case.
SURGICAL APPROACHESTranstemporal Appro a c hThe transtemporal approach utilizes the skin inci-sion and bony removal described above with slightlyless removal of the lateral orbital roof and lesserwing of the sphenoid bone. A 3-4 cm cortisectomy ismade in the superior temporal gyrus and centere da p p roximately 2 cm posterior to the anterior- m o s taspect of the sylvian fissure. A subpial resection ofthe superior temporal gyrus is utilized to enter thehorizontal portion of the sylvian fissure, enabling thes u rgeon to identify the M2 segments of the MCA.Dissection is then taken from distal to pro x i m a lwithin the sylvian fissure to identify the M1 segment,t h e reby providing proximal and distal control of theaneurysm. The lenticulostriate vessels, branchingpoints of the M1 segment of the MCA, the aneurysmneck, and the fundus are also identified. Thisa p p roach was initially advocated and popularized forpatients who presented with large temporal lobehematomas.
A transtemporal approach is advantageous in thatit re q u i res a smaller craniotomy and provides a di-rect approach to the essential anatomy with goodvisualization of the inferior M2 trunk. In addition,t h e re is less brain retraction and less manipulationof the M1 segment. The disadvantages of this ap-p roach include minimal release of cere b ro s p i n a lfluid (CSF) resulting in manipulation and re t r a c t i o nof a firm, stiff brain parenchyma. There is also moretissue resection than re q u i red by the othera p p roaches. This may subject the patient to ani n c reased risk for seizures. Finally, the aneurysmfundus is often exposed first with no proximal con-t ro l .
S u b f rontal/Pterional Appro a c hThe subfrontal/pterional approach utilizes the posi-tioning, craniotomy, and dural opening describede a r l i e r. Adequate bone removal of the orbital roof andlesser wing of the sphenoid down to the orbital men-ingeal artery is re q u i red to provide proximal expo-s u re to the sylvian fissure. In addition, a temporalcraniectomy is re q u i red to allow retraction of thetemporal lobe. A retractor blade is advanced sub-f rontally and secured under microscopic visualiza-tion to provide exposure of the olfactory tract andoptic and carotid cisterns. These cisterns are openedsharply with an arachnoid knife, thereby allowingthe egression of spinal fluid and subsequent soften-ing of the brain parenchyma. The exposure is then
NEUROSURGICAL OPERATIVE ATLAS. VOL. 816

STIEG AND FRIEDLANDER : SURGICAL MANAGEMENT OF MIDDLE CEREBRAL ARTERY ANEURYSMS 17
zygoma
ronguered bone
facial nerve
temporalis muscle
temporalis muscle incision
skin incision
craniotomy
temporalis muscle
craniotomy
facial nerve
F i g u re 2. Schematic views of the head position,skin and muscle incisions, placement of burrholes, and location of the craniotomy. A , n o t ethe location of the skin and muscle incisionwithin 1 cm of the tragus to avoid injury to thef rontalis division of the facial nerve. The tempo-ralis muscle is incised within its superior attach-ment to facilitate closure and provide bettercosmesis. Note the position of temporal squa-mous bone, removed with rongeurs. This allowsgentle traction on the temporal lobe. B , the skinflap is reflected individually, elevating the facialnerve with it. Subsequently the temporalis mus-cle is elevated, leaving the superior tuft of mus-cle; both the skin and muscle are isolated withfishhook retractors. The craniotomy is centere dover the sylvian fissure .
A
B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 818
taken distally along the internal carotid artery to itsb i f u rcation and into the proximal sylvian fissure ,again using sharp dissection. The entire M1 segmentis exposed within the horizontal portion and into theo p e rc u l a r-insular region of the sylvian fissure, pro-viding exposure of the bifurcation of the M1 segmentinto the M2 segments, as well as the neck of theaneurysm. With this exposure, the surgeon can alsovisualize the medial lenticulostriate vessels, whichextend along the frontal surface of the anterior cere-bral artery, and the M1 and M2 segments of theMCA. This dissection provides an excellent view ofthe anatomy of the sylvian fissure. Because of thiswide opening, retraction is re q u i red of both thef rontal and the temporal lobes.
This approach offers several advantages, includ-ing early release of CSF and proximal control of theaneurysm. Concerns re g a rding a wide opening of thesylvian fissure include prolonged frontal lobe re t r a c-tion and extensive manipulation of the entire M1 andM2 segments, which may induce spasm in these vessels.
Transsylvian Appro a c hThe transsylvian approach is the one that we mostcommonly use and it has recently been described bymany other authors. The positioning, incision, andcraniotomy described above facilitate the applicationof sharp microdissection techniques to enter theo p e rc u l a r-insular segment of the sylvian fissure forthe initial exposure. The atmosphere of the operatingsuite is calm and quiet with the surgeon in a seatedposition. The self-retaining retractor system, micro-scope, surgical assistant, surgical technician, con-t rolled suction devices, and bipolar cautery are alle rgonomically positioned to maintain economy ofmotion and ease of access. The sylvian fissure isopened 3 cm distal to the anterior lip of the inferiorf rontal surface. Initially, this is a superficial expo-s u re and non-bayoneted, short, straight instrumentsa re utilized. The venous drainage typically runs par-allel to the sylvian fissure and is associated with thetemporal surface. Small cortical veins within the syl-vian fissure can be sacrificed without great concern ;h o w e v e r, their preservation is always ideal. The su-p e rficial and thickened arachnoid over the sylvianf i s s u re is opened from the point of entry anteriorly,p roviding wide exposure. Subsequently, an M3 seg-ment of the MCA is identified and followed pro x i-mally, using sharp dissection. Blood is removed fro mthe sylvian fissure during dissection and the thinwisps of arachnoid can be identified and cut sharply.Commonly, the fissure will open with gentle re t r a c-tion on both the frontal and temporal lobes. This isnot the case when there is a thick dense hematomathat re q u i res sharp dissection and suctioning. Dis-section is taken along the M2 segment of the MCA,
sequentially providing exposure of the lateral lentic-ulostriate vessels, as well as the limen insula, theneck of the aneurysm, and finally the M1 segment.Arteries within the sylvian fissure either run fro n t a l l yor temporally and can be reflected in their re s p e c t i v ed i rections.
Disadvantages of this approach include late pro x-imal control in addition to frontal and temporal re-traction to provide complete exposure of the aneu-rysm neck and branches of the MCA. Advantages ofthis technique include early CSF release and brainsoftening, minimal brain dissection, removal of sub-arachnoid blood, and wide exposure of the MCA bi-f u rcation. Once dissection is complete, the objectiveis to occlude the aneurysm with a clip while pre s e r v-ing the normal anatomy without any stenosis, ast h e re is minimal collateral flow in this distal region ofthe arterial tre e .
CLIP APPLICATIONSaccular narrow-necked aneurysms are the leastcommon form found in this region (Figure 3). An an-eurysm clip is selected after the anatomy is com-pletely displayed. Ideally, we try to place a clip paral-lel to the M1 and M2 segments; however, on occasiona clip can be placed perpendicular to the pro x i m a land distal vessels, as demonstrated. Lesions of thissize rarely re q u i re temporary occlusion for placementof the permanent clip. After the aneurysm has beenobliterated, it is punctured with a 26-gauge spinalneedle to ensure occlusion.
B road-based aneurysms, which include in theirneck either a portion of the proximal M1 or distal M2vessel wall, are more commonly seen in this location( F i g u re 4). In addition, a trifurcation instead of bifur-cation is a common anatomical variant. This shouldbe visualized on the preoperative angiogram; how-e v e r, vessel spasm may diminish the surgeon’s abilityto visualize all vessels preoperatively. Thus, completedissection of the neck and fundus of the aneurysm aswell as the surrounding vessels in this region is es-sential to avoid postoperative complications.
One must be pre p a red for temporary occlusion atall times but particularly under conditions of un-timely aneurysm rupture or for complete dissectionof the aneurysm. In many cases, a proximal tempo-rary clip on the M1 segment may be all that isneeded to soften the neck of the aneurysm and facil-itate clip placement. However, as demonstrated inF i g u re 4, temporary trapping may be needed forsharp dissection of the aneurysm fundus from a dis-tal branch. There are several guidelines to followduring temporary clip application. The proximal clipshould be placed first and none of the clips shouldlimit the surgeon’s view, the preservation of flowwithin the lenticulostriate vessels should be maxi-mized, and finally the clips should not be placed in a

STIEG AND FRIEDLANDER : SURGICAL MANAGEMENT OF MIDDLE CEREBRAL ARTERY ANEURYSMS 19
M1 segment
inferior trunk ofthe M2 segment
superior trunk ofthe M2 segment
M1 segment
inferior trunk ofthe M2 segment
superior trunk ofthe M2 segment
A B
B
A
C
F i g u re 4. high-magnification views of the MCA trifurcation. A , the associa-tion between the M1, three M2 trunks, and a broad-based aneurysmincluding a segment of the inferior M2 trunk in its neck is demonstrated. B ,temporary clips have been placed across the M1 and M2 segments. Theclips are placed to allow maximum exposure for the surgeon and maintainflow through the lenticulostriate vessels. Sharp dissection techniques areutilized to create a plane between the fundus of the aneurysm and the par-ent vessel. Preservation of all distal arteries is essential. C , clip applicationis parallel to the parent vessels and occludes the portion of the aneurysmneck that extends into the M2 trunk. All three distal M2 branches havebeen preserved and the aneurysm is punctured to ensure complete occlu-sion. Larger aneurysms with hematoma may be opened widely for evacua-tion of the mass. The fundus of the aneurysm is left intact. The distal tem-porary clips are removed first and the proximal M1 temporary clip is thenre m o v e d .
F i g u re 3. A, high-magnification view of the MCA bifurcation demonstrating the M1 and M2 segments with lenticulostriatevessels on the M1 segment. A narrow-necked aneurysm between the superior and inferior M2 trunks is demonstrated. B , ap e rmanent clip has been placed across the neck of the aneurysm perpendicular to the axis of the parent vessel. In addition,the fundus of the aneurysm has been punctured and aspirated to ensure complete occlusion and removal of any masse ff e c t .

NEUROSURGICAL OPERATIVE ATLAS. VOL. 820
region of atheroma which could result in an emboliccomplication. In addition to facilitating dissection be-tween the aneurysm fundus and the parent vessels,temporary trapping allows the surgeon to perf o rm ana n e u r y s m o r rhaphy. Indications for opening the an-eurysm widely include a large thrombus within theaneurysm or calcium in the fundus, both of whichlimit closure of the clip. The thrombus can be re-moved with an ultrasonic aspirator, micro p i t u i t a r i e s ,or sharp dissection. Calcified plaque in the wall ofthe aneurysm can be either surgically removed orcrushed with a hemostat, thereby enabling the clipto approximate the walls of the aneurysm. The sur-geon must remember to open the aneurysm distalenough on the fundus to allow closure of the an-eurysm with a clip. More o v e r, dissecting the hema-toma or atheroma too proximally may result in thec reation of an intimal flap in the parent vessel.Should an intimal flap occur, dissection and occlu-sion may result once flow is re s t o red in the pare n tvessels.
C e re b ro p rotective maneuvers are used in order tominimize the effects of induced cerebral ischemiaduring temporary occlusion. The mechanisms ofaction for the protective measures are poorly under-stood but focus on decreasing cerebral oxygen re-q u i rements (general anesthesia, cooling to 33°C andplacing the patient in burst suppression with etomi-date or barbiturates), increasing collateral flow (ele-vating systolic blood pre s s u re 20% to 30%) and fre eradical scavenging (0.5 gm mannitol/kg bodyweight). Intermittent 10-minute periods of temporaryocclusion with reconstitution of flow between theperiods can be used in specific circumstances whenthe aneurysm has not been opened. Five minutes oftemporary occlusion is usually well tolerated. Be-yond 15 minutes, the risk of ischemic injury risessharply. Hypothermic circulatory arrest is consid-e red only in the most extreme cases.
Multiple clip configurations have been designed toenable the surgeon to apply them parallel to the par-ent vessels. The clips should also be placed to mini-mize torque on the M1 and M2 segments, whichcould result in vessel stenosis and ischemia. Fenes-trated clips including one of the M2 branches havealso been used. After the aneurysm has beens e c u red, we recommend puncture with a 26-gaugespinal needle to rule out residual filling. Under con-ditions of temporary trapping, aneurysmorrh a p h y ,and clipping, the distal M2 temporary clips areremoved first. At that time, the surgeon may notebleeding from the aneurysm which would re q u i replacement of a tandem clip or adjustment of the pri-mary permanent clip. After removal of the distal tem-porary clips, the proximal temporary clip is removed.
F u s i f o rm aneurysms of the MCA bifurcation alsop resent significant challenges (Figure 5). These an-eurysms, which include a portion of the parent ves-
sel, cannot be excluded from the circulation bys t r a i g h t f o r w a rd clip applications. The aneurysm mayinclude the entire trifurcation, as demonstrated, ormay involve one of the M2 branches. In either situa-tion, reconstitution of flow in the distal M2 vessels isoften needed and can be provided by bypass pro c e-d u res. The surgeon must anticipate the need for by-pass on the basis of the preoperative angiogram.Prior to making the skin incision, the superf i c i a ltemporal artery (STA) is mapped out on the scalpusing Doppler ultrasound. Infiltration of the scalpwith lidocaine is avoided. The STA and its adventitiaa re isolated along its full length for use later in thecase. As demonstrated, the aneurysm has beentrapped by permanent clips on the M1 and M2 seg-ments and subsequently opened for debulking of thehematoma within the aneurysm. In addition, anS TA-to-MCA bypass in an end-to-end fashion is per-f o rmed. One or two branches of the STA are isolatedfor use in the pro c e d u re. A proximal temporary clipis placed on this vessel and the distal ends are tran-sected at the appropriate length. The adventitia isdissected away from the distal end. The vessel is irri-gated with heparinized saline and anastomosed tothe M2 branch with running 10-0 Prolene sutures. As u t u re is placed at each pole of the anastomoseswith one run along the frontal surface and the otheralong the temporal surface of the anastomosis. Arubber dam is placed under the recipient vessels tofacilitate visualization of the suture. Again, the distal(M2) temporary clips are removed first to assess theanastomosis; finally, the temporary clip on the STAis removed. Intraoperative angiography is used toevaluate the bypass before closure of the craniotomy.C a re must be taken to closely oppose the galea dur-ing the closure to avoid leakage of CSF from thewound, as the dura cannot be closed tightly in thissituation. Also, adequate bone removal will ensurepatency of the STA as it enters the sylvian fissure .When only one M2 branch is involved in a fusiformaneurysm, an end-to-side anastomosis between theinvolved M2 segment and the normal M2 segment,respectively, is perf o rmed. Cerebral protection isused during perf o rmance of the bypass pro c e d u re.
MANAGEMENT AND AVOIDANCE OF COMPLICATIONSWe will discuss general and location-specific man-agement issues as well as strategies to avoid compli-cations in patients with MCA aneurysms.
P reoperative ManagementFor All PatientsAdequate angiograms need to be obtained and care-fully studied prior to surgery in order to thoro u g h l yunderstand the variable MCA anatomy for the indi-vidual patient. A general medical evaluation needs to

STIEG AND FRIEDLANDER : SURGICAL MANAGEMENT OF MIDDLE CEREBRAL ARTERY ANEURYSMS 21
inferior trunk of the M2 segment
M1 segment
A1 segment
superior trunk of the M2 segment
STA
recipient M2 distal branches
A
B
F i g u re 5. A, schematic of a fusiform aneurysm involving a distal portion of the M1 segment as well asp roximal portions of both M2 trunks. Frequently, the lenticulostriate vessels are adherent to the surface ofl a rge aneurysms in the region and must be meticulously dissected free prior to placing the perm a n e n tclips as demonstrated. The clips are placed as close to the aneurysm as possible. B , demonstrations of p e rmanent clip application across the M1 segment and two distal M2 segments, placed as close to theaneurysm as possible, can maintain flow to the lenticulostriates. In addition, an end-to-end STA - t o - M C Aanastomosis is demonstrated. The aneurysm is opened and the hematoma evacuated as needed. Branchesof the STA are anastomosed to the M2 trunks in an end-to-end fashion to maintain distal flow.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 822
be perf o rmed to optimize the preoperative conditionof the patient.
For Patients with Ruptured Aneurysm Patients with ruptured MCA aneurysms may pre s e n tin extremis, secondary to a large intrapare n c h y m a lhematoma. Because of the urgency in such situa-tions, conventional angiography may not be per-f o rmed. Computed tomography (CT) angiographyp rovides invaluable information prior to pro c e e d i n gwith aneurysm clipping following hematoma evacua-tion. Avoidance of aneurysmal re h e m o r rhage can beachieved by early and aggressive blood pre s s u re con-t rol as well as proceeding with early surg e r y .S e i z u res can be avoided by using antiepileptic med-ications at the time of admission. When the patientp resents with early symptomatic hydrocephalus, wep re f e r, if possible, to delay placement of a ventriculardrain until surgery because of the associated in-c reased risk of re h e m o r rhage. However, if the patientre q u i res immediate CSF drainage, placement of aventriculostomy with gradual lowering of the intra-cranial pre s s u re is the goal.
Intraoperative ManagementIntraoperative rupture can be prevented by avoidinghypertension as well as careful micro s u rgical tech-nique. A specific challenge of MCA bifurcation an-eurysms is the inadvertent occlusion of an M2 or M3branch during clipping of the aneurysm. This com-plication can be avoided by thorough pre o p e r a t i v eevaluation of the angiogram and circ u m f e re n t i a levaluation of the aneurysm neck either during tem-porary occlusion or following clipping. If one cannotc o n f i rm either complete obliteration of the aneurysmor patency of all the distal branches, intraoperativeor early postoperative angiography should be per-
f o rmed. In order to avoid a stroke following tempo-rary vessel occlusion, ischemic time must be kept ata minimum. Cere b ro p rotective aids employed toavoid ischemic complications after temporary occlu-sion include moderate hypothermia (33°-34°C), in-duced hypertension (160-170 mm Hg), mannitol (0.5gm/kg body weight), and etomidate or barbiturate-induced burst suppre s s i o n .
Postoperative ManagementIf subacute neurological deterioration (several hourspostoperatively) occurs and is not related to seizure s ,h e m o r rhage, or persistent brain edema, one shouldconsider an M2 occlusion or stenosis due to clip ro-tation. This has been described after closure or post-operative swelling of the sylvian fissure. An urg e n tCT scan will rule out a hemorrhagic complicationand expeditious angiography will confirm vesselpatency. Delayed hydrocephalus and vasospasmshould be treated in the standard fashion.
CONCLUSIONSMCA aneurysms are common and often very chal-lenging for the microvascular neuro s u rgeon. Surg i c a lresults have improved immeasurably over the pastseveral decades with the advancements in micro-s u rgical technique, cerebral protection, and the ag-g ressive management of vasospasm. The surg e o nmust be pre p a red for using any of the three describeda p p roaches for aneurysms in this region, as well asthe need for possible bypass pro c e d u res. We feel mostcomfortable with the transsylvian approach; however,occasionally we open the proximal sylvian fissure .This latter technique is utilized when we have con-c e rn re g a rding the stability of the aneurysm fundus,p rojection of the aneurysm, or the complexity of theaneurysm neck. A methodical approach to theseaneurysms with a thorough understanding of theanatomy, as well as patient, meticulous dissectiontechniques, should result in a good surgical outcome.

I N T R O D U C T I O NOur understanding of the anatomy and pathophysi-ology of dural arteriovenous malformations (DAV M s )has evolved rapidly with advancements in the field ofinterventional neuroradiology. DAVMs arise from ab-n o rmal arteriovenous shunts, yet venous hyperten-sion from arterialized veins is responsible for theirclinical presentation. The arterialized veins dilate,elongate, and rupture to cause subarachnoid or in-t r a p a renchymal hemorrhage. Ischemia may developin the surrounding brain from stagnant venousdrainage and poor perfusion. Communicating hydro-cephalus occurs because venous hypertension im-pedes cere b rospinal fluid (CSF) absorption, and ob-structive hydrocephalus occurs when large venousaneurysms obstruct CSF pathways.
Many intracranial and spinal DAVMs can bec u red by ligating the draining vein or occluding anassociated dural venous sinus. Unlike pare n c h y m a larteriovenous malformations (AVMs), the arterialsupply does not have to be eliminated before thevenous drainage because the leaves of the dura pro-tect the nidus from bleeding. Venous occlusion issafe when the primary drainage is antegrade thro u g ha dural venous sinus or when a single draining vein
SURGICAL REMOVAL OF TENTORIALAND POSTERIOR FOSSA DURAL
A RTERIOVENOUS MALFORMAT I O N SADAM I. LEWIS, M.D.
JOHN M. TEW, JR., M.D.
23
can be identified as it exits the dura. When a DAV Mis not associated with a venous sinus and corticalvenous drainage is present, ligating multiple drain-ing veins may be catastrophic. Ligation may worsenthe venous hypertension, produce a venous infarc-tion, or cause hemorrhage by diverting flow intononarterialized veins.
Tentorial and posterior fossa DAVMs are a uniquesubset of intracranial DAVMs that do not have anassociated venous sinus and frequently have multipledraining veins that are tortuous and aneurysmal.The common presentation is subarachnoid hemor-rhage (SAH) caused by a ruptured venous aneurysm.T h e re f o re, treatment is directed to the arterial side,an approach that is similar to that for pare n c h y m a lAVMs. The therapeutic strategy for deep-seatedD AVMs includes transarterial embolization followedby either stereotactic radiation or surgical excision.Transarterial embolization is perf o rmed to reduce theblood flow to the DAVM and decrease the venoushypertension. Because some dural arteries are toosmall to cannulate, endovascular techniques arer a re l y curative. Instead, embolization is followed bys t e reotactic radiation or surgical excision of thenidus. DAVMs with no cortical venous drainage canbe partially treated; however, tentorial and posteriorfossa DAVMs re q u i re complete obliteration to pre v e n tre c u r rent hemorrh a g e .
In the past, micro s u rgery for deep-seated DAV M swas associated with high morbidity from postopera-© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 824
tive hemorrhage if draining veins were occluded pre-m a t u rely and residual DAVM was present. Limitede x p o s u re with conventional craniotomies and larg evenous aneurysms accompanying the dural nidusalso discouraged the use of micro s u rgery. Combiningskull base approaches with conventional craniot-omies has been an important addition in the man-agement of patients with deep-seated DAVMs. Theskull base approach expands the field of view, widensthe angle of exposure, improves maneuverability thatis needed to coagulate, clip, and excise the duralleaflet, and minimizes retraction of the brain. Foura p p roaches are illustrated as the applicable tech-nique for the surgical management of tentorial andposterior fossa DAV M s .
PATIENT SELECTIONPatients with tentorial and posterior fossa DAV M sa re commonly men between 50 and 70 years of agewho have suff e red an SAH. Less frequently, they suf-fer pro g ressive neurological deterioration or symp-toms related to hydrocephalus. Because DAVMs withcortical venous drainage have an aggressive naturalhistory, the goal of treatment is complete angio-graphic obliteration.
If patients improve neurologically after emboliza-tion and do not have a venous aneurysm, stere o t a c-tic radiation is a reasonable option. Direct surg i c a lexcision of the dural nidus is indicated if the rup-t u red venous aneurysm is not eliminated by em-bolization or if the feeding arteries are too small toembolize. Surgery is also recommended if the symp-toms fail to resolve or new symptoms arise after em-bolization. Some authors recommend open craniot-omy with direct transvenous embolization or ligationof the draining veins. This approach is safe in asmall subset of patients who have had transarterialembolization and a single fistula (e.g., petrous apexD AV M s ) .
SURGICAL PLANNINGThe first imaging study obtained is usually computedtomography (CT), which frequently shows SAH orobstructive hydrocephalus from a large dilated ve-nous aneurysm. Magnetic resonance (MR) imagingand MR angiography are useful for identifying thes o u rce of hemorrhage (usually a ruptured venousaneurysm), determining the degree of venous hyper-tension, establishing the ventricular size, and plan-ning the operative approach based on the re l a-tionship of the nidus to the surrounding brains t r u c t u res. MR imaging and MR angiography alsoserve as screening studies for DAVM thrombosis afters t e reotactic radiation.
The findings of the initial cerebral angiogram maybe negative if only the internal carotid arteries andv e r t e b robasilar circulation are injected in search of a
r u p t u red saccular aneurysm. Selection of the exter-nal carotid arteries is important because a majorityof the arterial supply may arise from branches of themiddle meningeal artery, superficial temporal artery,and occipital artery. To identify venous aneurysmsand to determine the extent of venous congestionand stagnant flow, the late venous phase should beimaged as well. Bone windows on the angiogram,which establish the location of the nidus in re l a t i o nto the skull base, are particularly helpful to deter-mine if a skull base exposure is re q u i red in additionto a conventional craniotomy.
After the imaging studies are complete, tre a t m e n tbegins with transarterial embolization of the feedingarteries through the external carotid artery. Larg ebranches from the meningohypophyseal trunk mayalso be embolized. Decreasing arterial flow re d u c e sthe vascularity to the DAVM and the effect of venoushypertension. Occluded vessels that have been em-bolized preoperatively also provide a good road mapintraoperatively for understanding the surg i c a la n a t o m y .
Intraoperative angiography with imaging of thei n t e rnal and external carotid arteries and the verte-b robasilar system documents obliteration of theD AVM. Postoperative angiography provides betterresolution, selective arterial injections can be safelyp e rf o rmed, and a variety of projections can be per-f o rmed to expand the findings of intraoperative an-g i o g r a p h y .
SURGICAL APPROACHESThe best approach to deep-seated DAVMs includes ascalp incision, craniotomy, and dural opening thatremoves a significant portion of arterial supply fro mthe external carotid artery. Removal of the petro u sbone eliminates the transosseous supply and ex-poses dura around the entire DAVM nidus. The duraa round the nidus is resected to eliminate the re-maining dural supply. After removal of the duralcomponent, the remaining arterial supply from thei n t e rnal carotid artery is coagulated and incised.
The following are descriptions of the surgical ap-p roaches that provide access to most tentorial andposterior fossa DAVMs, including those located atthe petrous apex, the posterolateral tentorium, thefalx-tentorial junction, the inferior petrosal sinus,the lower clivus, and the foramen magnum.
D AVMs of the Petrous Apex and Upper ClivusAt the petrous apex, the most common surgical find-ing is the tentorial artery from the meningohypophy-seal trunk feeding a tentorial nidus with a singledraining petrosal, mesencephalic, or pontine vein( F i g u re 1A). A subtemporal craniotomy with zygo-matic osteotomy or suboccipital craniotomy is per-f o rmed to provide access to the fistula. An anterior

LEWIS AND TEW : SURGICAL REMOVAL OF TENTORIAL AND POSTERIOR FOSSA DAVMS 25
p e t rosectomy in combination with a subtemporala p p roach is necessary when there is transosseousarterial supply through the petrous bone or whenthe nidus is located along the upper one half of theclivus (Figure 1B). An anterior petrosectomy re q u i re sremoval of bone between the petrous portion of thei n t e rnal carotid artery, the third division of the tri-geminal nerve, and the internal auditory canal. Thisa p p roach provides access to the upper half of theclivus and anterior aspect of the posterior fossadown to the inferior petrosal sinus. Exposure belowthe internal auditory canal re q u i res a posterior pet-rosectomy and suboccipital appro a c h .
After induction of general endotracheal anesthe-sia, a lumbar catheter placed to drain CSF impro v e se x p o s u re and prevents postoperative CSF leakage.The patient’s head is placed in a radiolucent Mayfieldh e a d rest to permit intraoperative angiography. Posi-tioning for a subtemporal approach is supine with agelatin roll under the right shoulder, and the thoraxis elevated 15 degrees. The head is rotated so thatthe sagittal sinus is parallel to the floor and thentilted downward 10 degrees so that the zygoma is thehighest point in the surgical field (Figure 1C). Thisposition brings the skull base into view and dimin-ishes the need for retraction of the temporal lobe.
A frontotemporal, or inverted question-mark, inci-sion provides exposure from the cavernous sinus tothe arcuate eminence of the petrous bone. The scalpis reflected inferiorly with the frontalis fat pad toavoid injury to the facial nerve. A zygomatic osteot-omy may be perf o rmed to permit reflection of thetemporalis muscle below the floor of the middle fossaand minimize temporal lobe retraction. The zygomaremains attached to the masseter muscle to impro v ehealing after closure. The temporalis muscle and fas-cia are reflected inferiorly, leaving a superior cuff offascia for closure .
A high-speed drill is used to perf o rm the subtem-poral craniotomy and additional bone is re m o v e dwith a burr to make the craniotomy flush with thefloor of the middle fossa. When an anterior petro s e c-tomy is re q u i red, the microscope is used to dissectthe temporal fossa dura away from the petrous bone.Removal of approximately 30 ml of CSF aids in re-traction of the temporal fossa dura. The middle men-ingeal artery is sacrificed at the foramen spinosum.Removal of bone around the foramen ovale allowsmobilization of the trigeminal root and improved re-traction of the temporal fossa dura medially. Self-retaining retractors are placed at the edge of thep e t rous ridge before drilling the petrous bone.
The greater superficial petrosal nerve, identifiedwith a facial nerve stimulator, is sectioned near thefacial hiatus to prevent injury to the geniculate gan-glion. The petrous carotid artery, which lies underthe greater superficial petrosal nerve, is exposed
using a high-speed diamond-tipped drill. The poste-rior loop of the internal carotid artery is not exposed,thus avoiding injury to the geniculate ganglion andcochlea. The superior semicircular canal, which pro-vides the posterior border of the anterior petro s e c-tomy, is located beneath the hard white bone of thea rcuate eminence at a 120-degree angle to theg reater superficial petrosal nerve (Figure 1D). Drillingbegins anterior to the arcuate eminence in the softbone of the meatal plane to expose the dural sleeve ofthe internal auditory canal (Figure 1E). To avoidinjury to hearing or the facial nerve, the geniculateganglion, falciform crest, and cochlea are not ex-posed. The remaining bone between the third divisionof the trigeminal nerve, petrous carotid artery, andi n t e rnal auditory canal (i.e., Kawase’s triangle) isremoved inferiorly along the posterior fossa dura tothe inferior petrosal sinus (Figure 1F).
The dura is opened along the inferior temporallobe and the tentorium is split from the superior pet-rosal sinus toward a point posterior to the tro c h l e a rnerve. Clips are placed on the superior petrosal si-nus and the sinus is divided. Frequently, the sinus ist h rombosed. The dural incision is then extended in-f e rolateral to the inferior petrosal sinus to expose theupper posterior fossa (Figure 1G).
After opening the dura, numerous feeding arteriesin the tentorium are usually visualized and coagu-lated using bipolar electrocautery. The tentorium isincised with scissors and coagulated using bipolare l e c t rocautery. The electrocautery causes the tentor-ial dura to shrink and retract, thus exposing the ten-torial artery. The tentorial artery from the meningo-hypophyseal trunk can be seen communicating witharterialized vein(s). Occlusion of the feeding arteryleads to collapse of the venous aneurysm. Similar toligating spinal DAVMs, the veins and venous aneu-rysms of intracranial DAVMs need not be removed.
Intraoperative angiography is perf o rmed to docu-ment complete obliteration of the petrous apexD AVM. To avoid postoperative CSF leakage, exposedmastoid air cells are closed with bone wax. Pericra-nium and fibrin glue (i.e., combination of thro m b i nand cryoprecipitate) are placed along the defect inthe temporal lobe dura, and a pericranial fat graft ispacked. A lumbar catheter is connected to a closeddrainage system for 24 to 72 hours, with the level setat the external auditory canal. Drainage of CSFshould not exceed 10 mL per hour to avoid pneumo-c e p h a l u s .
D AVMs of the Posterolateral Te n t o r i u mP o s t e rolateral tentorial DAVMs are usually the larg e s tand most complex deep-seated DAVMs (Figure 2A).The arterial supply is generally bilateral with contri-butions from the anterior circulation, posterior circ u-lation, and external carotid system to form a plexi-

f o rm nidus with multiple draining veins. A subtempo-ral craniotomy with removal of the posterior petro u sbone and mastoid minimizes retraction of the tempo-ral lobe, removes the transosseous arterial supply,enables the surgeon to excise a large area of the ten-torium, and provides access to draining veins andvenous aneurysms below the tentorium (Figure 2B).
The addition of a posterior petrosectomy pro v i d e sa presigmoid approach with sectioning of the supe-rior petrosal sinus to mobilize the junction of thetransverse-sigmoid sinus and protect the vein ofLabbé when the temporal lobe is retracted. This pre-sigmoid approach gives access to the upper twot h i rds of the clivus, anterior cerebellum, and brain-stem. The fifth through the 10th cranial nerves canbe visualized. The addition of a suboccipital craniot-omy provides a re t rosigmoid approach with access tothe lower clivus and foramen magnum. Sectioning ofthe transverse-sigmoid sinus and a labyrinthectomyis not re q u i red for most posterolateral DAVMs. Fur-ther exposure may be obtained with sacrifice of con-duction hearing by total petrosectomy and sealingthe semicircular canals. In our experience, occlusionof the dominant transverse-sigmoid sinus worsensvenous hypertension and may cause a hemorrh a g i cvenous infarction or postoperative hydro c e p h a l u s .
A lumbar catheter inserted to drain CSF willi m p rove exposure and prevent postoperative CSFleakage. The patient’s head is placed in a radiolucent
Mayfield headrest. The femoral arterial catheter usedfor intraoperative angiography is placed prior to posi-tioning the patient in the right lateral decubitus posi-tion. An axillary roll is used and the thorax is ele-vated 15 degrees. The head is rotated until thesagittal sinus is parallel to the floor and is tilted 10d e g rees downward so that the zygoma is the highestpoint in the surgical field (Figure 2C).
To gain additional exposure of the petrous bone,mastoid tip, and deep venous structures, a J- s h a p e dincision extends vertically from the root of the zy-goma crosses the superior temporal line, and de-scends 3 cm posterior to the ear. The incision term i-nates at the insertion of the neck musculature to theskull. The temporal skin flap is reflected inferiorlyand the temporalis muscle is reflected separately,leaving a superior fascial cuff .
Burr holes are made at the anterior mastoid pointand asterion, which are above and below the trans-verse-sigmoid junction, respectively. Bone overlyingthe sinus between the burr holes is removed with adrill. A pneumatic craniotome is used to perf o rm thetemporal craniotomy (Figure 2D). Under the micro-scope, the bone overlying the transverse sinus isremoved with a high-speed drill. The mastoid aircells are removed. The middle fossa and meatal boneplates are dissected until the antrum is identified( F i g u re 2E). The bone of the sinodural angle isremoved with a diamond-tipped drill to expose the
NEUROSURGICAL OPERATIVE ATLAS. VOL. 826
F i g u re 1. T h rombosis of the superior petrosal sinus is frequently seen in petrous apex dural arteriovenous malform a t i o n s .A , schematic drawing of the petrous apex DAVM with arterial supply from the tentorial artery and drainage into a petro s a lvein with an associated bilobed venous aneurysm. The vein drains into the contralateral superior petrosal sinus. B , h a t c h e da re a re p resents boundaries of subtemporal craniotomy (1) and anterior petrosectomy (2). The area in re d re p resents thelocation of the DAVM nidus. C , positioning for the subtemporal approach. An inverted question-mark incision (hatched line)is outlined over the temporal squama. Solid lines re p resent bony removal including the suboccipital craniotomy and zygo-matic osteotomy. D , the temporal lobe dura is retracted to visualize the floor of the middle cranial fossa and petrous bone.Kawase’s triangle is bounded by the mandibular division of the trigeminal nerve, petrous internal carotid artery, and the sev-enth and eighth cranial nerve complex. Removal of the bone within this anatomical triangle re p resents the anterior petro s e c-tomy. GSPN = greater superficial petrosal nerve. E , under the microscope, the bone overlying the petrous internal caro t i dartery (ICA) and internal auditory canal (IAC) is removed to define the borders of the anterior petrosectomy. The cortical boneof the superior semicircular canal forms a 50-degree angle with the IAC. F, after removal of the bone in the meatal plane, aline drawn from the tip of transverse crest to the intersection of the carotid artery with the trigeminal nerve (Miller’s line)a p p roximates the basal turn of the cochlea. G , the dural reflection of the temporal lobe, posterior fossa, and tentorium form sthe superior petrosal sinus. After the dura is opened, the contents of the upper posterior fossa are exposed. (Figure Areprinted with permission from the Mayfield Clinic; B reprinted from Tew JM Jr, van Loveren HR, Keller JT: Atlas of Opera -tive Micro n e u ro s u rgery, Vol II. Philadelphia: WB Saunders (in press); C-G reprinted from Tew JM Jr, van Loveren HR: Atlas ofOperative Micro n e u ro s u rgery, Vol I. Philadelphia: WB Saunders, 1994, pp 40-43)

LEWIS AND TEW : SURGICAL REMOVAL OF TENTORIAL AND POSTERIOR FOSSA DAVMS 27
A
B
C
D
E
F G
Figure 1.
CN V
ICA IAC
GSPN
CN VIII
superiorpetrosalsinus
transversecrest
geniculateganglion
cochleaMiller’s line
Kawase’striangle
CN IV

NEUROSURGICAL OPERATIVE ATLAS. VOL. 828
anterior border of the sigmoid sinus and the poste-rior semicircular canal. The mastoid air cells of themastoid tip are then removed to expose the posteriorfossa dura and digastric ridge, which serves as alandmark to the stylomastoid foramen, the begin-ning of the fallopian canal, and the location of thefacial nerve (Figure 2F).
Thirty milliliters of CSF are removed and a duralincision is made from the posterior fossa (inferior tothe superior petrosal sinus), to the middle fossa, andup to the petrous apex. The superior petrosal sinus isdivided with clips. Under the microscope, the tento-rium is divided toward the incisura directed posteriorto the trochlear nerve (Figure 2G). The leaves of thetentorium are coagulated with bipolar electro c a u t e r yto obtain hemostasis and to shrink and retract thedura. Feeding arteries entering the tentorium arecoagulated with bipolar electrocautery and cut withm i c roscissors. Frameless stereotaxis may be usefulto guide the approach and corroborate location of theD AVM in the tentorium. After excising the dura leaf-let, the draining veins are coagulated and divided.
In addition to documenting obliteration of theD AVM, intraoperative angiography reveals re s i d u a lD AVMs, which cannot be visualized because they areconcealed by cavernous and tentorial dura. Placing ametal clip at the operative site provides inform a t i o non the intraoperative angiogram re g a rding the re l a-tive position of the remaining nidus to the skull base.
A free abdominal fat graft used to close the defectin the mastoid and temporalis muscle is split tocover the mastoid defect. The bone flap and zygo-
matic bone are secured with titanium plates. Thetemporalis and cervical muscles are reattached totheir respective fascial cuffs. The lumbar catheter isconnected to a closed drainage system for 24 to 72hours with the level set at the external auditorycanal. CSF drainage should not exceed 10 mL perh o u r. A compression dressing is applied.
D AVMs of the Inferior Petrosal SinusD AVMs of the inferior petrosal sinus are often sup-plied by the ascending pharyngeal artery, occipitalartery, posterior meningeal artery, and muscularbranches of the vertebral artery (Figure 3). The pos-terior auricular artery and meningohypophysealtrunk may contribute to the arterial supply. Thearteriovenous connection commonly occurs at theend of the inferior petrosal sinus near the jugularbulb. Venous drainage is antegrade through the in-t e rnal jugular vein or spinal medullary veins andmay also occur re t rograde through cortical veins intothe transverse-sigmoid or cavernous sinuses (Figure4A and B).
Lower clivus and foramen magnum DAVMs gainsupply from the posterior meningeal, meningojugu-l a r, occipital, and anterior spinal arteries, as well asthe muscular branches of the vertebral artery.Drainage is into either the spinal medullary veins orthe mesencephalic veins that drain toward the veinof Galen and straight sinus.
A right far lateral suboccipital craniotomy isre q u i red to isolate the transverse-sigmoid sinus and jugular bulb, visualize the ventral brainstem
F i g u re 2. D AVM of the posterolateral tentorium. A , arterial supply from the intracavernous carotid artery branches ande x t e rnal carotid artery supply. Venous drainage flows into mesencephalic and cerebellar veins. B , hatched are a re p re s e n t sboundaries of the subtemporal, suboccipital, and posterior petrosectomy. The dotted are a re p resents sigmoid and transversesinuses exposed but not sacrificed. The area in re d re p resents the location of the DAVM nidus. C, positioning for the poste-rior petrosectomy. D , the temporalis muscle is reflected anteroinferiorly, leaving a superior fascial cuff. Burr holes placed oneither side of the transverse sinus reduce the risk of injury to the sinus. The bone between the burr holes is removed with ab u r r. A pneumatic craniotome is used to per f o rm the craniotomy. E , the spine of Henle is a landmark to the antrum. Theantrum floor is the cortical bone of the lateral semicircular canal, which serves as a guide to deeper structures. The mastoidair cells are removed, and the middle fossa and meatal bone plates are dissected until the antrum is identified. F, the bone ofthe sinodural angle is removed with a diamond-tipped drill. The sigmoid sinus and posterior semicircular canal are exposed.The posterior semicircular canal is identified by following the lateral semicircular canal until it bisects the posterior semicir-cular canal. The mastoid air cells of the mastoid tip are then removed to expose the digastric ridge, which serves as a land-mark to the stylomastoid foramen and the beginning of the fallopian canal. Removal of the sigmoid plate exposes the supe-rior petrosal sinus. G , the superior petrosal sinus is divided and the tentorium is incised ventrally toward the incisura in acourse toward the trochlear nerve. The feeding arteries and dural nidus are encountered along the path to the incisura. (Fig-u re A reprinted with permission from the Mayfield Clinic; B reprinted from Tew JM Jr, van Loveren HR, Keller JT: Atlas ofOperative Micro n e u ro s u rgery, Vol II. Philadelphia: WB Saunders (in press); C-G reprinted from Tew JM Jr, van Loveren HR:Atlas of Operative Micro n e u ro s u rgery, Vol I. Philadelphia: WB Saunders, 1994, pp 40, 45, 47-49, 51)

LEWIS AND TEW : SURGICAL REMOVAL OF TENTORIAL AND POSTERIOR FOSSA DAVMS 29
A
B
C
D
E
F
G
CN IV
lateral semicircularcanal
spine of Henle
tentorium
superiorpetrosalsinus
fallopian canal
sigmoid sinus
transverse-sigmoidjunction
Figure 2.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 830
F i g u re 3. T h rombosis or stenosis of a major sinus may cause re t rograde flow into cortical veins. A , right anteriorposterior vertebral artery angiogram demonstrating a DAVM of the inferior petrosal sinus with stenosis of the righti n t e rnal jugular vein and venous drainage through the contralateral transverse-sigmoid sinus into the left intern a ljugular vein. B , lateral vertebral angiogram demonstrating re t rograde venous drainage into the superior sagittalsinus and vein of Galen via the straight sinus. (Reprinted with permission from Lewis AI, Rosenblatt SS, Tew JMJr: Surgical management of deep-seated dural arteriovenous malform a t i o n s . J Neuro s u rg 87:198-206, 1997)
A B
F i g u re 4. D AVM of the inferior petrosal sinus. A , the inferior petrosal sinus DAVM is fed by both posterior meningeal arteriesand muscular branches from both vertebral arteries. The occipital artery is causing the constriction of the right internal jugu-lar vein. The jugular bulb is dilated and a r ro w s within the lumen of the dural sinuses show that venous drainage is re t ro-grade. B , hatched are a re p resents boundaries of the far lateral suboccipital approach. The area in re d re p resents the locationof the DAVM nidus. C , a lateral hemisphere incision is outlined over the suboccipital bone and cervical spine. The h a t c h e dl i n e re p resents the scalp incision. The solid line re p resents the bony removal including the suboccipital craniotomy, openingthe foramen magnum, laminectomy of the posterior arch of C1, and partial resection of the posteromedial condyle. D , m a s t o i demissary veins and the epidural venous plexus may be arterialized. Hemostasis of these veins is best achieved with bipolare l e c t rocautery or compression with Oxycel or other hemostatic agent. E, the posterolateral one third of the occipital condyle isremoved with a high-speed diamond-tipped drill. F, after removal of the posterior arch of C1, the extradural horizontal seg-ment of the vertebral artery is mobilized out of the vertebral groove on C1 to obtain proximal control of the primary arterialsupply to the DAVM. G , the posterior fossa and spinal dura are reflected laterally with dural retention sutures. An incisionbegins in the spinal arachnoid and proceeds through the cisterna magna while cere b rospinal fluid is aspirated. (Figure Areprinted with permission from the Mayfield Clinic; B, D-F reprinted from Tew JM Jr, van Loveren HR, Keller JT: Atlas ofOperative Micro n e u ro s u rgery, Vol II. Philadelphia: WB Saunders (in press); C and G reprinted from Tew JM Jr, van Lovere nH R: Atlas of Operative Micro n e u ro s u rgery, Vol I. Philadelphia: WB Saunders, 1994, pp 69 and 72)

LEWIS AND TEW : SURGICAL REMOVAL OF TENTORIAL AND POSTERIOR FOSSA DAVMS 31
A
B
C
D
E
F
G
occipitalcondyle
vertebralartery
cisternamagna
vertebralartery mobilized
foramen transversarium
C2 nerve root
vertebralvenousplexus
Figure 4.

and lower clivus, and resect the involved dural seg-ment. The far lateral exposure isolates the vertebralartery, which is the primary arterial supply to mostposterior fossa DAVMs. This exposure provides ac a u d a l - t o - rostral and lateral-to-medial field of viewfor DAVMs of the inferior petrosal sinus and lowerc l i v u s .
After induction of general endotracheal anesthe-sia, the patient’s head is placed in a radiolucent May-field headrest for intraoperative angiography. A lum-bar catheter is optional. The femoral arterial sheathfor intraoperative angiography is inserted before thepatient is placed in the lateral oblique position. Anaxillary roll is placed and the thorax is elevated 15d e g rees. The head is rotated 45 degrees from parallelt o w a rd the floor and flexed until the posterior neckmuscles are stretched but not tight. The mastoidp rocess is the highest point.
A midline suboccipital incision is perf o rmed fro mthe spinous process of C2 toward the superior tem-poral line and inferior to the mastoid tip (Figure 4C).This incision allows dissection of the extracranialvertebral artery and exposes the suboccipital bone,mastoid region, and deep venous structures. Theskin flap is reflected inferiorly, leaving a superior fas-cial cuff. A cuff of nuchal fascia and splenius capitismuscle is preserved to re a p p roximate the cervicalm u s c u l a t u re during closure. The suboccipital boneis removed in one piece with the fascial cuffs at-tached using a pneumatic drill. Additional bone isremoved in the mastoid region with a burr. A subpe-riosteal dissection of the lamina of C1 and C2 is per-f o rmed 2 cm lateral to the midline. Sharp dissectionof the soft tissues between the foramen magnum andthe arch of C1 identifies the vertebral artery as itp i e rces the dura. Dissection continues from medialto lateral until the foramen transversarium is identi-fied. The surrounding venous plexus and vertebralmuscular branches are coagulated and divided usingbipolar electrocautery (Figure 4D). The arch of C1 isremoved with a rongeur or drill. The lateral portion ofthe foramen magnum and the posteromedial third ofthe occipital condyle are removed with a diamond-tipped drill (Figure 4E). An occipitocervical fusion isnot necessary if only one third of the condyle hasbeen removed. Bone overlying the foramen transver-sarium is removed with a diamond-tipped drill tomobilize the vertebral artery (Figure 4F).
The dura is opened in the midline at C1 and ex-tended laterally up to the transverse-sigmoid sinus( F i g u re 4G). The intracranial vertebral artery is iden-tified and followed to the nidus, which is antero m e-dial to the jugular bulb. The feeding branches to thenidus are coagulated and the dural leaflet is excised.Bovine pericardium, fascia lata, or other dural sub-stitutes are used to close the dural defect. The boneflap is replaced with plates and a standard closure
with re a p p roximation of the nuchal fascia is per-f o rm e d .
D AVMs of the Vein of GalenThe arterial supply of midline DAVMs is often bi-lateral from the tentorial, middle meningeal, ands u p e rficial temporal arteries. Venous drainage is viac e rebellar and vermian veins. The straight sinus isf requently thrombosed and a vein of Galen aneurysmis present. Venous aneurysms are very common and,in most cases, are responsible for hemorrhage orobstructive hydrocephalus (Figure 5).
Because DAVMs of the vein of Galen and falx-ten-torial junction are midline, an interhemispheric ap-p roach is used (Figure 6A and B). The trajectory isposterior to the splenium of the corpus callosum.T h e re are four major steps in the operation. First, thescalp incision, craniotomy, and dural opening assistwith the elimination of the arterial supply over theconvexity. Second, the remaining dural arterial sup-ply is eliminated by excising the falx and tentoriums u r rounding the nidus. Third, arterial branches fro mthe meningohypophyseal trunk and posterior cere-bral arteries are coagulated and cut as they enter thevein of Galen aneurysm. Division of the feeding arter-ies as they enter the DAVM is important to avoidoccluding vessels of passage. Fourth, the thro m b u swithin the venous aneurysm is removed to decom-p ress the mesencephalon. The wall of the aneurysmremains in situ to avoid injury to the brainstem.
A femoral arterial sheath is inserted before posi-tioning the patient in a left lateral oblique position;for a right occipital approach, the head is placed inneutral position. The vertex becomes the highestpoint in the operative field (Figure 6C). The head isplaced in a radiolucent Mayfield headrest to perm i tintraoperative angiography; the right hemisphere isd e p e n d e n t .
A right posterior parasagittal craniotomy is per-f o rmed for midline DAVMs (Figure 6D); bilaterala p p roaches can be achieved by sectioning the falxand retracting the contralateral hemisphere. Theskin flap is reflected toward the transverse sinus andthe dura is opened in cruciate fashion (Figure 6E).The interhemispheric trajectory places the neuro s u r-geon at the falx-tentorial junction, behind the sple-nium of the corpus callosum and above the intern a lc e rebral veins and the vein of Galen.
Arterial supply from branches of the superf i c i a ltemporal artery are coagulated during the openingand approach to the vein of Galen DAVM (Figure 6F).The tentorial and falx dura are coagulated and cut toeliminate the remaining meningeal arterial supply.The arachnoid is opened and the tentorial arteriesf rom both meningohypophyseal trunks are coagu-lated and divided.
The resected tentorium and falx dura overlying
NEUROSURGICAL OPERATIVE ATLAS. VOL. 832

LEWIS AND TEW : SURGICAL REMOVAL OF TENTORIAL AND POSTERIOR FOSSA DAVMS 33
the vein of Galen aneurysm is removed with scissors.T h rombus within the aneurysm is removed with anultrasonic aspirator to decompress the mesen-cephalon. The capsule is left in situ to prevent injuryto the brain stem from excessive manipulation.
OUTCOME AND COMPLICATIONSS u rgical obliteration of a DAVM re q u i res coagulationof the dura followed by excision of the dural leaflet top revent the fistula from re d i recting into anotherlocation or diverting flow into nonarterialized veins.Patients may develop transient, delayed neuro l o g i c a lworsening. The presumed cause of the delayed post-operative deterioration is the exacerbation of pre o p-erative venous hypertension. Patients may also re-q u i re postoperative ventriculoperitoneal shunting for
communicating hydrocephalus after SAH or pre o p e r-ative shunting for obstructive hydrocephalus causedby giant venous aneurysms.
Ligating the draining veins prior to obliterating thearterial supply may lead to devastating hemorrh a g i cvenous infarction. In addition, clipping or re m o v i n gthe venous aneurysm is unnecessary because it willcollapse and thrombose when the DAVM nidus isobliterated. Thrombus within the venous aneurysmcan be removed to decrease mass effect; however, theaneurysm wall should be left in situ to avoid injury tothe surrounding brain (e.g., vein of Galen DAV M s ) .
Intraoperative angiography is useful to identify aresidual DAVM. However, postoperative angiographywith selective injection of the external carotid arteryand venous phase images should be perf o rmed toc o n f i rm complete DAVM obliteration.
F i g u re 5. MR imaging and MR angiography are perf o rmed to identify the source of hemorrhage, follow theventricular size, identify thrombus within the venous aneurysm, and plan the operative approach basedon the relationship of the nidus to the surrounding brain structures. A , T1-weighted axial MR imageshowing a partially thrombosed vein of Galen aneurysm with edema in the right subcortical nuclei due tovenous hypertension. B , T1-weighted sagittal MR image showing the DAVM posterior and inferior to thesplenium of the corpus callosum. An interhemispheric approach with a parieto-occipital trajectory avoidedsectioning the corpus callosum. (Reprinted with permission from Lewis AI, Rosenblatt SS, Tew JM Jr: Sur-gical management of deep-seated dural arteriovenous malform a t i o n s . J Neuro s u rg 87:198-206, 1997)
A B

F i g u re 6. Schematic drawing of the falx-tentorial DAVM with bilateral arterial supply from the meningohypophyseal trunk,s u p e rficial temporal artery, and superficial temporal artery. A , the venous drainage is into a partially thrombosed vein ofGalen aneurysm and the right basal vein of Rosenthal. B , the area in re d re p resents the location of the DAVM nidus alongthe tentorium and falx. C , the affected side is positioned down to allow the hemisphere to retract with the aid of gravity. Thisposition is more comfortable than the sitting position because it allows the surgeon to use both hands side-by-side. Also,the risk of air embolism is significantly reduced compared with the sitting position. D , the site of the bone flap is shown.T h e re are a paucity of bridging veins to the sagittal sinus in this location. E , a cruciate incision is perf o rmed to retract thedura toward the sagittal sinus. F, in the dependent position, minimal retraction of the occipital lobe is re q u i red to exposethe falx-tentorial junction. Coagulation of the feeding arteries is perf o rmed as they enter the vein of Galen DAVM. (Figure Areprinted with permission from the Mayfield Clinic; Figures B-F reprinted with permission from Tew JM Jr, van Loveren HR,Keller JT: Atlas of Operative Micro n e u ro s u rgery, Vol II. Philadelphia: WB Saunders (in pre s s ) )
NEUROSURGICAL OPERATIVE ATLAS. VOL. 834
A
B
C
D
E
F
occludedstraightsinus
vein of Galenaneurysm
feeding arteries

INTRODUCTIONA p p roximately 20% of all arteriovenous malform a-tions (AVMs) of the brain occur in the posterior fossa.They are more likely to become symptomatic thansupratentorial AVMs because of the concentration ofvital neurological structures within the limited con-fines of the posterior fossa. Infratentorial AVMs com-monly present with hemorrhage, but may also pre-sent with pro g ressive neurological deterioration orcranial neuropathy. Mixed intraparenchymal, sub-arachnoid, and intraventricular hemorrhage are themost common presenting findings of patients newlydiagnosed with posterior fossa AVMs. The naturalhistory of these lesions left untreated is poor becauseof the high incidence of hemorrhage and the neuro-logical deterioration associated with AVMs of the pos-terior fossa. For this reason, most patients newly di-agnosed with an AVM of the cerebellum or brainstembenefit from surgical treatment directed at eliminat-ing the lesion and preventing future hemorrh a g e .
AVM CLASSIFICATIONAccurate classification of an AVM in the posteriorfossa is necessary to guide preoperative planning andthe optimal surgical treatment. Attempts at classify-ing cerebral hemispheric AVMs has met with limitedacceptance, due in part to the variability of most
SURGICAL RESECTION OF A RTERIOVENOUS MALFORMATIONS
OF THE POSTERIOR FOSSATHOMAS KOPITNIK, M.D.
DUKE SAMSON, M.D.MICHAEL HOROWITZ, M.D.
35
supratentorial lesions and the complexities of thep roposed classification systems. We classify AVMs ofthe posterior fossa into five groups relative to the in-volved brain tissue and blood supply. These fiveg roups lend predictability to the anticipated vascularsupply, venous drainage, and the ease or difficulty of surgical resection. We subdivide posterior fossaAVMs into lesions involving the following: 1) the cere-bellar vermis, 2) the cerebellar hemisphere, 3) thec e rebellar tonsil, 4) the pial surface of the brainstem,and 5) the deep parenchyma of the brainstem. Thisclassification system accurately predicts the vascularsupply to the lesion, aids in preoperative planning in-cluding the optimal surgical approach, and aids ind e t e rmining the necessity of adjunctive pre o p e r a t i v eembolization. Because 95% of posterior fossa AV M sa re confined to the cerebellum and only 5% are truebrainstem lesions, we will focus on AVMs involvingthe cerebellum. Despite the complexity of the poste-rior fossa, it is extremely rare for AVMs to simultane-ously involve both the cerebellum and the brainstem.L a rge AVMs of the cerebellum may appear to involvethe entire contents of the posterior fossa, but invari-ably the lesion is confined to the cerebellar tissue orthe brainstem tissue, not both.
AVMs of the cerebellar vermis are some of themost common vascular malformations found in theposterior fossa. The primary arterial supply to ver-mian AVMs is usually via the superior cere b e l l a rarteries (SCAs) and the posterior inferior cere b e l l a r© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 836
arteries (PICAs) bilaterally (see Figure 2C). The domi-nant arterial feeding supply of either the SCA or thePICA distribution depends upon the anatomical loca-tion of the vascular malformation within the verm i srelative to the horizontal fissure. AVMs occurringsuperior to the horizontal fissure and involving thefolium, declive, culmen, central lobule, and lingulausually have significant arterial input from the ver-mian branches of the SCA and lesser input from thePICAs. AVMs below the horizontal fissure within thet u b e r, pyramid, uvula, and nodulus typically derivethe dominant arterial supply from the PICA bilater-ally and the SCA to a much lesser extent. Althoughthe SCA and PICA provide the majority of arterialinput to vermian AVMs, the anterior inferior cere b e l-lar artery (AICA) often provides deep lateral feeding tol a rger and deeper vermian AVMs through branchesof the AICA. These deep branches of the AICA enterthe foramen of Luschka and supply the lateral roof ofthe fourth ventricle and middle cerebellar peduncle.Ve rmian AVMs usually drain superiorly into thegalenic system through the precentral cerebellar veinor through superior vermian veins bridging into thet e n t o r i u m .
The cerebellar hemisphere also re p resents a com-mon location of cerebellar AVMs due to the re l a t i v e l yl a rge anatomical region re p resented by the cere b e l l a rh e m i s p h e re. The arterial supply to AVMs of the cere-bellar hemisphere is unilateral and typically involvesall three vascular territories (SCA, AICA, and PICA),with the dominant supply depending largely on thespecific hemispheric location of the lesion (see Figure5C). The closer the AVM is located to the cere b e l l o-pontine angle (CPA) cistern, the more prominent thesupply from the AICA. Similarly, the more superiorthe malformation is located within the cere b e l l a rh e m i s p h e re, the more arterial input from the SCAcan be anticipated. If angiography demonstratesp rominence and significant feeding from the deepbranches of the AICA, the AVM usually involves thelateral aspect of the ventricular wall and middle cere-bellar peduncle. AVMs within the cerebellar hemi-s p h e re usually have venous drainage superiorly andlaterally into the petrosal system or superiorly intothe galenic system.
C e rebellar AVMs confined to the cerebellar tonsiloccur less frequently and are limited in size by then a t u re of their location. The arterial feeding to tonsil-lar AVMs is usually via a unilaterally dilated PICAwith occasionally some secondary feeding from distalinferior branches of the AICA if the lesion extendsinto the cerebellar hemisphere (see Figure 6B). Ve-nous drainage can be lateral into the sigmoid sinusbut is more common into the midline inferior ver-mian veins.
Brainstem AVMs are rare lesions that pose uniquechallenges to treatment and should be classified as
separate and distinct entities from cerebellar AV M s .Although AVMs of the cerebellar hemisphere maypartially involve the middle cerebellar peduncle,AVMs of the cerebellum are usually sharply demar-cated and distinct from AVMs of the brainstem.Brainstem AVMs are usually small and should befurther subgrouped into superficial lesions confinedto the pia or the deep parenchyma. The superf i c i a lpial lesions are usually supplied by dilated branchesof the SCA or AICA and drain into the prepontine orp e t rosal venous system. Pial AVMs of the brainstemdo not usually present on the ventricular surf a c eand have superficial re p resentation of both arterialsupply and venous drainage. Conversely, deep pa-renchymal AVMs of the brainstem are rarely seenominous lesions with arterial supply usually thro u g hdeep vertebrobasilar perforator vessels into the ven-tral aspect of the malformation. Ventricular involve-ment is common and venous drainage is via peri-ependymal venous channels that ultimately connectinto the galenic system.
PATIENT SELECTION AND TIMING OF INTERVENTIONBecause of the natural history of untreated AV M sand the limited tolerance of the posterior fossa con-tents to hemorrhage, most patients with cere b e l l a rAVMs should undergo treatment aimed at eliminatingthe vascular malformation. As potential tre a t m e n toptions are contemplated, the estimated risk of fu-t u re hemorrhage, the patient’s age, life expectancy,general medical condition, and neurological statusa re considered together. Aneurysms commonly occuron the major feeding vessels associated with posteriorfossa AVMs and are often the source of both intra-p a renchymal and subarachnoid hemorrhage. Theseaneurysms usually occur distally along the majorfeeding vessels to the AVM nidus. Small pre - a n e u r y s-mal dilatations on the intracranial vertebral or basi-lar artery are frequently found in association withl a rge cerebellar AVMs and do not usually re q u i ret reatment. On the other hand, proximal saccular an-eurysms associated with an AVM should be tre a t e dprior to or in conjunction with treatment of the AV M .F a i l u re to treat a proximal aneurysm may result inc a t a s t rophic subarachnoid hemorrhage after an AV Mis removed distal to an aneurysm. Surgical re s e c t i o nof the AVM without treatment of a proximal saccularaneurysm markedly increases the risk of aneurysmr u p t u re due to an abrupt increase in arterial pre s-s u re within the feeding vessel as surgical resection ofthe AVM is perf o rmed.
Unlike ruptured cerebral aneurysms pre s e n t i n gwith subarachnoid hemorrhage, AVMs of the cere b e l-lum typically present with mixed intrapare n c h y m a l ,subarachnoid, and intraventricular hemorrh a g e ,with a majority of the hemorrhage usually within the

KOPITNIK ET AL : SURGICAL RESECTION OF AVMS OF THE POSTERIOR FOSSA 37
c e rebellar parenchyma, and some degree of obstruc-tive hydrocephalus. The volume of subarachnoidblood is usually underestimated on computed to-mography (CT) due to the bony confines of the poste-rior fossa and the poor parenchymal re s o l u t i o nobtained with routine CT techniques. When an acuteposterior fossa hemorrhage occurs from a suspectedc e rebellar AVM, one of the first considerations mustbe whether external ventricular drainage is immedi-ately necessary. Patients with posterior fossa andintraventricular hemorrhage may rapidly deterioratedue to acute obstructive hydrocephalus and shouldeither be treated with external ventricular drainageor undergo close neurological observation to detectearly deterioration from acute hydrocephalus.
If hydrocephalus has been adequately treated oris not present, the next consideration is whether anassociated hematoma is producing significant masse ffect within the posterior fossa and whether emer-gency clot evacuation is re q u i red. If the patient isn e u rologically stable, operative intervention is bestdelayed for 4-6 weeks until a portion of the intra-p a renchymal clot has liquefied and the peak time forp a renchymal edema has passed. Patients often toler-ate large hematomas of 5-6 cm without significantn e u rological sequelae if hydrocephalus is adequatelyt reated. This delay in operative intervention allowsfor liquefication of the clot, potential improvement ofthe patient’s preoperative neurological status, andtime for extensive radiological investigation of thevascular lesion.
If the patient’s neurological condition has deterio-rated to such an extent as to warrant emergency pos-terior fossa exploration and clot evacuation, severalfactors must be considered. If an arteriogram hasbeen obtained in the presence of a large intra-p a renchymal hematoma, the hematoma may com-p ress and partially obscure a significant portion ofthe AVM during angiography. The surgeon mustt h e re f o re be pre p a red to potentially encounter anAVM significantly larger than the lesion visualized onan arteriogram obtained shortly after the initial hem-o r rhage. An adequate bone flap should be fashionedto accommodate cerebellar swelling and possibleh e m o r rhaging from the malformation during re s e c-tion. If surgery is re q u i red acutely following AV Mh e m o r rhage, clot evacuation without AVM re s e c t i o nshould be perf o rmed if possible and, if necessary, ac-companied by large bony craniectomy and dura-plasty. Occasionally, due to the location of the clot,complete hemostasis unfortunately cannot be ob-tained until the AVM has been resected. Anticipationof this possible eventuality should be factored intothe decision-making process when emergency clotevacuation is considered. We prefer to defer definitiveAVM resection for 4-6 weeks following a significantposterior fossa hemorrhage if the patient’s neuro l o g i-
cal condition remains stable. Once a hematoma cav-ity begins to resolve and liquefy, the surgical re s e c-tion is greatly facilitated. Repeat arteriography priorto the delayed surgical pro c e d u re often reveals por-tions of the AVM that were not apparent on the initialarteriogram. We reserve acute emergency surgical intervention only for patients with a potentially re-coverable posterior fossa hemorrhage who are eithermoribund despite external ventricular drainage ordeteriorate neurologically during a period of obser-v a t i o n .
PREOPERATIVE PREPARATION AND RADIOLOGICAL EVALUATIONT h e re are few other lesions in vascular neuro s u rg e r yw h e re the surgeon’s conceptualization of the norm a land pathological anatomy is as critical as in the sur-gical management of posterior fossa AVMs. Completeangiographic evaluation combined with high-qualitymultiplanar magnetic resonance (MR) imaging iscrucial to preoperative planning. CT is useful ford e t e rmining the size and configuration of an initialh e m o r rhage, if present, and for sequential follow-upstudy of hemorrhage resolution. Diagnostic cere b r a langiography, which includes injection of both inter-nal carotid and both vertebral arteries, is the defini-tive diagnostic test. For complete evaluation of poste-rior fossa AVMs, both vertebral arteries must bestudied individually. Despite a lesion lateralized toone cerebellar hemisphere, angiographic opacifica-tion of the contralateral vertebral artery will yieldvaluable information re g a rding feeding to the lesionthat is often obscured during ipsilateral vertebralangiography due to overlap and prominence of anindividual feeding pedicle. Potential adjunctive pre-operative embolization can be planned only aftercompletion and careful review of the diagnostic arte-riogram. Following cerebral angiography, MR imag-ing provides information to aid in determining theanatomical limits of the AVM, the subtle involvementof adjacent structures, and the limits of a plannedresection margin. MR imaging will demonstrate thed e g ree to which AVMs of the cerebellar vermis mayinvolve the superior medullary velum or whetherl a rge hemispheric and tonsillar AVMs involve themiddle and inferior cerebellar peduncles, re s p e c-tively. At the present time, there is limited indicationfor CT angiography (spiral CT) or MR angiography inthe management of a posterior fossa AVM. The infor-mation obtained from these computer re n d e r i n g sdoes not replace high-quality angiography or multi-planar MR imaging. Spiral CT shows great potentialfor future study of complex vascular lesions due tothe relatively quick acquisition times and thre e -dimensional spacial reconstruction capability.
P reoperative embolization of selected feeding ves-sels can be of significant benefit prior to a surg i c a l

NEUROSURGICAL OPERATIVE ATLAS. VOL. 838
p ro c e d u re to resect a posterior fossa AVM. Emboliza-tion is not without inherent risk and an estimated5% morbidity to overall patient management risk isi n t roduced with each embolization pro c e d u re. Em-bolization should be directed primarily at deep arter-ial feeding to the AVM, which is not easily accessibleearly in an operative resection of the lesion. Pre o p e r-ative embolization of deep AICA feeding arteries tol a rge vermian or cerebellar hemispheric AVMs cansignificantly lessen the difficulty with intraoperativebleeding from along the roof of the fourth ventricle.Feeders such as these are difficult to access early inthe pro c e d u re and can be a significant source ofh e m o r rhage deep in the resection bed late in the op-erative pro c e d u re. On the other hand, although thePICA may be easily accessed with an embolizationc a t h e t e r, it is also the most surgically accessible ves-sel within the posterior fossa and can almost alwaysbe surgically transected immediately adjacent to theAVM nidus, much closer to the nidus than can beroutinely achieve with an embolization catheter.
A g g ressive embolization of SCA feeders distal tothe dorsal aspect of the brainstem can be very help-ful prior to a planned surgical resection of superiorlylocated cerebellar AVMs, which typically have signifi-cant SCA supply. Because large cerebellar AVMs andsmall AVMs superior to the horizontal fissure typi-cally have venous drainage directed superiorly intothe galenic system, preoperative SCA embolizationaids the surgical resection and re q u i res less initialdissection over the tentorial surface of the cere b e l-lum early in the pro c e d u re. This avoids initial dissec-tion around fragile arterialized venous structure sprior to surgical transection of other more accessiblefeeding vessels early in the pro c e d u re. Although em-
bolization of the SCA territory does not eliminate thenecessity for dissection over the cerebellar tentorials u rface, with preoperative embolization of the SCAterritory, this dissection can be done late in the oper-ative pro c e d u re when a portion of the arterial pre s-s u re has been eliminated from the venous structure sand exposure of the superior aspect of the cere b e l-lum has been maximized.
Patients with brainstem AVMs are not ideal candi-dates for adjunctive embolization. We embolized ninebrainstem AVMs prior to the attempted surg i c a lresection of 23 such lesions and found an unaccept-ably high morbidity rate with preoperative emboliza-tion of these dangerous lesions. The vascular supplyto these extremely rare lesions is best accessed sur-gically as close to the malformation as possible, toavoid iatrogenic ischemia to exceptionally vulnerabletissue such as the brainstem.
SURGICAL TECHNIQUEAVMs of the Cerebellar Ve rm i sAVMs of the cerebellar vermis are midline lesionsand are best approached via a midline exposure. Wep refer the pro n e - c o n c o rd position for patients under-going resection of vermian AVMs, re g a rdless of thelocation of the lesion within the vermis. The patientsa re positioned prone on chest rolls with the neckflexed. The operating room table is placed in extre m ereverse Tre n d e l e n b u rg position to bring the patient’snuchal region horizontal with respect to the floor,and the patient’s lower extremities and knees arepadded and flexed against table support to pre v e n tcaudal movement (Figure 1A). The patient’s head isthen laterally canted toward the shoulder contralat-eral to the side of the operating table where the sur-geon will stand. The table is rotated so the patient’shead is aligned to the surgeon’s pre f e rence with re-g a rd to operating room orientation (Figure 1B).
Ve rmian AVMs can be resected via a large midlineincision extending from above the inion to the C3-4region. A large craniotomy bone flap is elevated suchthat the superior, inferior, and lateral margins of theAVM can be easily visualized, with no portion of theAVM concealed beneath bone. This axiom usually re-q u i res a customized removal of bone to include theforamen magnum for caudal lesions and exposure ofthe transverse sinus and torcula for superiorly lo-cated vermian lesions. A wide stellate durotomy isp e rf o rmed in a fashion to optimize posterior fossae x p o s u re (Figure 2A). Prior to initiating resection ofthe AVM, the superficial margins of the malform a t i o na re inspected to ensure that the bony removal anddural opening have been adequate and that subse-quent AVM resection can proceed unhindered. Ob-scuring a margin of the AVM by poor bony exposurecan limit the ability to control hemorrhage duringthe pro c e d u re .
F i g u re 1. P ro n e - c o n c o rd position used for midline exposureof a posterior fossa AVM, lateral ( A ) and superior ( B ) v i e w s .
floor

KOPITNIK ET AL : SURGICAL RESECTION OF AVMS OF THE POSTERIOR FOSSA 39
C
A
B
F i g u re 2. AVM of the cerebellar verm i s . A , e x p o s u re. B , schematic re p resentation of the arterial supply andvenous drainage. C , clip ligation of the PICA bilaterally adjacent to the nidus.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 840
The initial microdissection of a vermian AVM isd i rected at accessing both PICAs within the sub-arachnoid space at the midline and dissecting thevessels to their entrance into the inferior aspect ofthe malformation (Figure 2C). The distal PICA arter-ial supply to the AVM is divided as close to the nidusas possible to minimize iatrogenic infarction of adja-cent but uninvolved cerebellar tissue. After PICAfeeding has been eliminated, circ u m f e rential dissec-tion of the superficial pial margin of the AVM from aninferior to superior direction is perf o rmed on eachlateral margin. This will eliminate possible superf i-cial AICA feeding to the malformation, which is usu-ally minimal in all but large vermian AVMs. Superf i-cial dissection along the superior margin is thenp e rf o rmed with caution so as not to jeopardize ro s-tral venous outflow from the AVM, which is typicallyt h rough the superior vermian venous system. Afters u p e rficial feeding has been eliminated, continuedfeeding to the AVM is usually present through deepSCA and deep lateral AICA feeders within the supe-rior medullary velum and lateral roof of the fourthventricle. It is advisable to protect the floor of thefourth ventricle with a soft cotton strip so that ifbleeding occurs during later, deeper stages of the re-section from small but often numerous periepen-dymal feeders, the lesion can be expediently re m o v e dwithout inadvertently injuring the floor of the fourthventricle. Venous drainage of vermian AVMs is usu-ally directed superiorly through the dilated superiorv e rmian or precentral cerebellar venous system (Fig-u re 2B). The venous outflow is transected only after
the AVM resection has been completed and the le-sion is ready to be delivered from the operative field.
AVMs of the Cerebellar HemisphereThe optimal surgical approach and operative patientpositioning for AVMs involving the cerebellar hemi-s p h e re is greatly dependent upon the size of the mal-f o rmation, the location of the lesion within the hemi-s p h e re, the necessity for exposure of the CPA cistern ,and surgeon pre f e rence. We prefer the lateral posi-tion for most operative pro c e d u res involving AVMs ofthe cerebellar hemisphere. The patient can usuallybe positioned supine with a blanket-roll under theipsilateral shoulder and hip and the head positionedlateral and horizontal with respect to the floor (Fig-u re 3A). If the patient is very large or has limitedrange of motion of the cervical spine, the patient isbest placed in the park-bench lateral position (Figure3B). The disadvantage of the park-bench lateral posi-tion is that the ipsilateral shoulder can decrease theworking room of the operative field, especially in al a rge patient.
To resect cerebellar hemispheric AVMs, we gener-ally use a large C-shaped incision centered on themastoid process and elevate a large subgaleal-sub-cutaneous skin flap (Figure 4A). The majority of theposterior cervical muscles are detached from theocciput and reflected posteriorly and inferiorly (Fig-u re 4B). Most lateral cerebellar hemispheric AV M shave significant blood supply from the AICA, andaccess to the CPA cistern is imperative to surg i c a l l yc o n t rol this blood supply to the AVM. In order to
F i g u re 3. AVM of the cerebellar hemisphere . Vertex view of the patient for the lateral ( A ) and park-bench lateral (B) p o s i t i o n s .

KOPITNIK ET AL : SURGICAL RESECTION OF AVMS OF THE POSTERIOR FOSSA 41
maximize exposure of the CPA cistern, we extend thelateral extent of the bony craniotomy to the level ofthe sigmoid sinus laterally. The superior, inferior,and posteromedial extents of the bony resection de-pend on the size and location of the AVM, but suff i-cient bone must be removed so that exposure is ade-quate and dissection unhindered (Figure 4C).
After the dura has been widely opened and them a l f o rmation inspected to confirm the location of themajor arterial feeders and the venous drainage, theprimary initial task is to microdissect and transectthe arterial feeders as close to the nidus as possible( F i g u re 5A). The PICA can be identified caudally inp roximity to the cerebellar tonsil and followed to itspoint of entry into the malformation, where it is tran-sected. Similarly, the AICA is identified in the CPAc i s t e rn and dissected to its entry into the AVM whereit is ligated and divided. Often, the deep supply fro mthe SCA to cerebellar hemispheric AVMs is partiallyo b s c u red by the superiorly and laterally drainingvenous outflow of the malformation. By working
a round the venous structures and undercutting thec e rebellar tissue under the venous drainage, themajor feeding from the hemispheric SCA branchescan be transected close to the malformation withoutc o m p romising the venous drainage (Figure 5C). Oc-casionally, large cerebellar hemispheric AVMs havedeep arterial supply from deep branches of the AICAalong the lateral aspect of the roof of the fourth ven-tricle and superior medullary velum (Figure 5B). Onreview of a preoperative MR image, if the AVM pre-sents or is immediately adjacent to the fourth ventri-cle, or partially involves the middle cerebellar pedun-cle, there is a high likelihood of AICA feeding alongthe deep margin of the AVM. If troublesome bleedingoccurs during resection from deep periependymalfeeding vessels, expedient entry into the fourth ven-tricle allows the surgeon to access the periependymalfeeding from the AICA supply proximally as the ves-sels enter the foramen of Luschka.
F i g u re 4. S u rgical resection of AVMs of the lateral cerebellar hemisphere. A, skin incision. B, scalp and muscle reflected. C, bone removal (shaded are a ) .

NEUROSURGICAL OPERATIVE ATLAS. VOL. 842
A
B
C
F i g u re 5. AVM of the cerebellar hemisphere . A , e x p o s u re. B , schematic re p resentation of the arterialsupply and venous drainage. C , transection of SCA feeding to an AVM close to superiorly locatedvenous drainage.

KOPITNIK ET AL : SURGICAL RESECTION OF AVMS OF THE POSTERIOR FOSSA 43
AVMs of the Cerebellar To n s i lBecause of the somewhat small size of the cere b e l l a rtonsil, AVMs confined to the tonsil are relatively rarebut easy to resect. These patients can be positionedp ro n e - c o n c o rd or lateral, and adequate bony expo-s u re should be perf o rmed in the caudal direction toinclude wide opening of the foramen magnum. Occa-sionally, the posterior arch of C1 must be removed tocompletely expose the caudal extent of tonsillarAVMs (Figure 6A). These lesions usually derive theirblood supply solely from the PICA (Figure 6C), whichcan be easily accessed in the subarachnoid space atits lateral and posterior medullary segments. Afterthe PICA feeding has been transected close to theAVM, it is usually simple and expedient to perf o rm alimited tonsillar resection in order to remove theAVM. The venous drainage of AVMs involving thec e rebellar tonsil is either lateral into the sigmoidsinus or, more commonly, into the inferior verm i a nvenous system (Figure 6B).
AVMs of the BrainstemBrainstem AVMs include those lesions with pare n c h y-mal re p resentation in the mesencephalon, tectalplate, pons, medulla, floor of the fourth ventricle, andC PA cistern. These malformations are extremely rareand can present with intraparenchymal or subarach-noid hemorrhage or a variety of fluctuating neuro l o g i-cal symptoms. AVMs of the brainstem are best dividedinto two distinct groups: superficial or pial AVMs anddeep parenchymal AVMs. Although AVMs from bothg roups may present with similar clinical signs andsymptoms, the indications for surgical treatment andoutcomes from the two groups are markedly diff e rent.
S u p e rficial AVMs of the brainstem primarily in-volve the pial-arachnoid layers, and minimally in-volve the underlying parenchyma. They often occuron the anterior or lateral surface of the brainstem inthe CPA, and the arterial supply of these lesions isusually via dilated branches of the AICA with occa-sional supply from the SCA (Figure 7). Superf i c i a lbrainstem AVMs that involve the anterior surface ofthe brainstem usually have no deep perforator feed-ing, with the venous drainage through lateral pontineveins into the petrosal system (Figure 8). We havefound preoperative embolization of superficial brain-stem AVMs to be extremely hazardous and of littlevalue as an adjunct to their re s e c t i o n .
Brainstem AVMs in the CPA are usually ap-p roached with the patient in a lateral position with ane x t reme lateral bony exposure in order to maximizeaccess to the CPA cistern (Figure 9). Bone is re m o v e dlaterally to the sigmoid sinus, superiorly to the tento-rium, and inferiorly to include the foramen magnum.The cistern of the CPA is opened widely from the cis-t e rna magna to the tentorium, and cere b ro s p i n a lfluid is allowed to egress to provide relaxation of the
c e rebellum. Under high-power magnification, thefeeding vessels to the malformation are identified andsequentially transected. The complexity of pial AV M sof the lateral brainstem in conjunction with the lim-ited space available in the CPA usually pre c l u d e scomplete circ u m f e rential dissection during the initialphases of AVM resection. Following the initial dissec-tion of the AVM, it is often necessary to gently elevatethe nidus away from the brainstem within a shallowplane of pial dissection beginning postero l a t e r a l l yand continuing anteromedially along the ventral sur-face of the brainstem (Figure 10). With sequentialocclusion of the smaller feeding vessels entering them a l f o rmation, the malformation can be completelyu n d e rcut from the pial surface, and the re m a i n i n gfeeding vessels and draining veins cauterized, di-vided, and delivered from the operative field.
Deep parenchymal AVMs of the brainstem posean entirely diff e rent surgical risk than superf i c i a l l ylocated lesions. The feeding vessels to deep brain-stem AVMs are usually vertebrobasilar perf o r a t o rarteries originating ventrally and coursing thro u g hn o rmal brainstem tissue prior to penetrating thedeep margins of the malformation (Figure 11). Deepp a renchymal brainstem AVMs often involve the floorof the fourth ventricle, and venous drainage is usu-ally through dilated periependymal veins into thegalenic venous system. These malformations are in-timately associated with normal brainstem pare n-chyma, and the arterial supply to these malform a-tions cannot be accessed beyond the margins of theAVM without significant risk of iatrogenic ischemiaand infarction of adjacent normal brainstem pare n-chyma. The small size of the feeding vessels alongwith their irrigation of adjacent normal tissue makesadjunctive embolization difficult and minimally suc-cessful. In a similar fashion, surgical resection ofdeep parenchymal AVMs of the brainstem carries ex-t remely high morbidity and mortality rates. Occa-sionally, when the lesion is small and associatedwith an intraparenchymal hematoma, surgical re s e c-tion can be accomplished by working within the re-solving hematoma cavity without significant disrup-tion of normal brainstem tissue. The approach top a renchymal AVMs of the brainstem should traversethe minimum amount of normal tissue re q u i red toaccess the lesion. The margins of the malform a t i o na re identified and the lesion is circ u m f e rentially dis-sected until the small feeding vessels at the depths ofthe resection bed are reached. The surgical re s e c t i o nof these lesions is usually associated with consider-able and persistent deep arterial bleeding that canonly be managed by cautery and careful, persistentm i c rodissection. In general, patients with deep pa-renchymal brainstem AVMs are poor candidates form i c ro s u rgical resection because of the multitude ofp roblems mentioned above.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 844
A
B
C
F i g u re 6. AVM of the cerebellar tonsil. A , e x p o s u re. B , schematic re p resentation of the arterial supplyand venous drainage. C , e l e c t rocautery of PICA feeding vessel.

KOPITNIK ET AL : SURGICAL RESECTION OF AVMS OF THE POSTERIOR FOSSA 45
SUMMARYAVMs of the posterior fossa frequently present withclinically significant hemorrhage within the sub-stance of the cerebellum or brainstem, within thesubarachnoid space, or both. It is common to findaneurysms on proximal feeding arteries of posteriorfossa AVMs that are the source of subarachnoid ori n t r a p a renchymal hemorrhage. AVMs of the poste-rior fossa are best subdivided by location into cere-bellar vermian AVMs, cerebellar hemispheric AV M s ,c e rebellar tonsillar AVMs, superficial brainstem pials u rface AVMs, and deep parenchymal brainstemAVMs. Classification into one of the above locationshelps anticipate the suspected arterial supply andlikely venous drainage.
AVMs of the posterior fossa re q u i re full radiologi-cal evaluation prior to treatment, including four- v e s-
sel angiography and high-quality MR imaging. Em-bolization as an adjunct to surgical resection is use-ful to decrease the blood flow to cerebellar AVMs pri-marily through embolization of the deep feedingvessels, which are not easily accessed initially duringan operative resection. Feeding arteries that are eas-ily accessed micro s u rgically should not undergo un-necessary embolization due to the risk of iatro g e n i ctissue infarction. Embolization of brainstem AV M scarries a high risk and is of little benefit as an ad-junct to surgical resection. The surgical resection ofposterior fossa AVMs is best delayed until partial re s-olution of any hematoma, dependent upon the pa-tient’s neurological condition. The natural history ofposterior fossa AVMs suggests that surgical tre a t-ment to eliminate these aggressive lesions is indi-cated in the majority of circ u m s t a n c e s .
F i g u re 7. MR image ( A ) and antero p o s t e r i o r angiogram ( B ) of a superficial AVM of the brainstem.
A B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 846
F i g u re 9. Illustration depicting the initial lateral exposure ofa superficial pontine AVM presenting to the CPA cistern .
F i g u re 10. Illustration depicting ligation of feeding arteries and elevation of a superficial pontine AV M .
F i g u re 11. Illustration depicting a deep parenchymal AVM ofthe brainstem with deep perforators feeding from the basilara r t e r y .
F i g u re 8. Illustration depicting an AVM of the superf i c i a lC PA surface of the pons.

INTRODUCTIONArteriovenous malformations (AVMs) in the region ofthe ventricular trigone present unique challenges tothe neuro s u rgeon. These lesions are invariably lo-cated in eloquent or functionally important brain andhave a complex arterial supply and deep venousdrainage. Involvement of the choroid plexus with theAVM may add to the overall size of the lesion. Toexpose and resect these complex lesions, a number oftangential approaches have been utilized rather thanthe more conventional perpendicular appro a c h e sused for AVMs on the cerebral convexity.
PATIENT SELECTIONAs with other AVMs, lesions in the region of the ven-tricular trigone most commonly come to clinicalattention during the third or fourth decades of life.These deep-seated lesions most frequently pro d u c esymptoms after an intraventricular and/or intra-c e rebral hemorrhage. Infrequently, these malform a-tions present with seizures or a visual field deficit inthe absence of hemorrhage. Since the incidence ofAVM rebleeding is very low immediately after the ini-tial hemorrhage and cerebral vasospasm is exceed-
SURGICAL TREATMENT OF A RTERIOVENOUS MALFORMATIONS
OF THE VENTRICULAR TRIGONEDANIEL L. BARROW, M.D. ROGER H. FRANKEL, M.D.
47
ingly rare, immediate surgery is usually not indi-cated for the patient presenting with a hemorrh a g e .S u rgical intervention is typically delayed for 2 or 3 weeks to allow for recovery from the hemorrh a g e .Occasionally, a patient presenting with a large he-matoma and associated mass effect may re q u i reu rgent evacuation of the hematoma. In this situa-tion, the emergency operation is usually perf o rm e dto remove the hematoma, with the actual resection ofthe AVM reserved for a later date. Once the patienthas stabilized, the intricate neurovascular operationcan be carried out more electively.
After the AVM has been localized and defined bya p p ropriate imaging studies, the various therapeuticoptions are reviewed with the patient and family.Treatment recommendations are then tailored to theindividual patient and lesion. In addition to no tre a t-ment, options include embolization, surgical re s e c-tion, and stereotactic radiosurgery. The decision ismade after careful consideration of a variety of factorsrelated to both the patient and the malformation. Thepatient’s age, health, neurological condition, occupa-tion, and psychological reaction to the knowledgethat he or she harbors a potentially dangerous lesionmust all be taken into consideration. Factors re l a t e dto the AVM that are of importance in decision-makinginclude the precise location, size, arterial supply,venous drainage, and relationship of the malform a-tion to associated hematomas. Because of the poornatural history of untreated AVMs, most of these© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 848
lesions re q u i re some form of therapy. Embolizationalone rarely cures an AVM in the region of the ven-tricular trigone and is there f o re not often of benefit asa sole treatment. It is, however, a very useful adjunctto surgery. Stereotactic radiosurgery is a re a s o n a b l eoption for treating small AVMs in this region, but thesignificant time interval re q u i red for the radiation tohave its beneficial effects as well as the risk of radia-tion injury re p resent significant detractors to thistherapeutic modality. In the majority of trigonalAVMs, the risk of surgical removal with an immediatec u re is significantly less than the risk of the naturalhistory of the untreated malform a t i o n .
PREOPERATIVE PREPARATIONPatients presenting with an intracerebral and/or in-traventricular hemorrhage are managed aggre s s i v e l yto control intracranial hypertension and may re q u i rea ventriculostomy for control of hydrocephalus, ifp resent. Blood pre s s u re control using oral or par-enteral medications is also commonly necessary inthe acute period. Since all operative approaches toAVMs in the region of the ventricular trigone re q u i reviolation of the cortex, patients are placed on pro p h y-lactic anticonvulsants.
After initial stabilization of the patient, diagnosticimaging studies are carried out to define the anatom-ical features of the lesion. Noncontrasted computedtomography is the initial diagnostic study perf o rm e dacutely in the patient presenting with a hemorrh a g e .This allows determination of the extent and locationof the hemorrhage and the diagnosis of hydro c e p h-alus. Invasive cerebral angiography is essential todefine the angioarc h i t e c t u re of the AVM. The poste-rior cerebral artery usually feeds these lesions, withthe posterior choroidal and posterior temporal arter-ies being predominant. Other arteries that occasion-ally contribute include the anterior choroidal, middlec e rebral, pericallosal, and thalamoperforating arter-ies. Venous drainage is typically deep into the galenicsystem. Occasionally, a small amount of superf i c i a lcortical venous drainage is there as well. In rareinstances, the vein of Labbé is involved or the lesionhas purely superficial venous drainage.
Magnetic resonance imaging (MRI) provides ana-tomical information that complements the angio-gram and is extremely useful in planning the mosta p p ropriate operative approach. MRI demonstratesthe precise relationship of the vascular malform a t i o nand associated hematoma to the trigone, indicatesthe proximity to adjacent anatomical structures, andreveals the cortical surface closest to the AV M .
We have found preoperative embolization to be animportant adjunct to the surgical resection of AV M sin this region. The surgical approaches to these mal-f o rmations often expose the deep arterial supply at alater stage of the pro c e d u re. Reduction or elimination
of the deep arterial supply by embolization re d u c e sthe critical blood supply and diminishes surgical dif-ficulty and risk. Furtherm o re, preoperative emboliza-tion allows for a more gradual redistribution of arter-ial blood flow to the surrounding normal brain andt h e o retically reduces the risk of postoperative re p e r-fusion complications.
ANESTHETIC TECHNIQUEThe advantages of general anesthesia to achieve arelaxed brain and to control blood pre s s u re provide am o re optimal environment for successful operationson these lesions. Prior to the induction of generalanesthesia, patients are given anticonvulsants, sys-temic corticosteroids, and prophylactic antibiotics.An invasive arterial line is placed to provide accessfor arterial blood gas determinations and to allow forcontinuous monitoring of the arterial pre s s u re. It isour pre f e rence to operate on AVMs under norm a lblood pre s s u re and to prevent hypotension. Sincea u t o regulation is often impaired in the brain adjacentto an AVM, profound hypotension or excessive re-traction to the adjacent brain may result in ischemici n j u r y .
If the patient’s head is elevated above the heart toany significant degree, a pre c o rdial Doppler ultra-sound and an atrial catheter are placed pre o p e r a-tively to optimally monitor for and manage potentialair emboli. A Foley catheter is used for urinarydrainage and measure m e n t .
SURGICAL TREATMENTWe have utilized three basic approaches in the surg i-cal management of AVMs in the region of the ventric-ular trigone. They include: 1) a lateral temporala p p roach through the inferior or middle temporalgyrus; 2) a parieto-occipital transcortical appro a c h ;and 3) an occipital interhemispheric approach. Thelatter can be ipsilateral and parafalcine or contralat-eral and transfalcine. Selection of the appro a c hshould be based upon the presence of pre o p e r a t i v en e u rological deficits, the presence of an intracere b r a lh e m o r rhage, and the relationship of the AVM to thetrigone based on angiographic and MRI localization( F i g u re 1).
The transtemporal approach is used for AV M slocated along the lateral, anterior, or inferior wall ofthe trigone (Figure 1A). This approach is particularlyuseful for AVMs associated with a hematoma extend-ing into the temporal lobe. The interh e m i s p h e r i ca p p roach is reserved for selected AVMs situatedalong the medial aspect of the trigone that may alsoinvolve the splenium of the corpus callosum (Figure1B). The parieto-occipital approach, as described byH e ros, is used for AVMs involving the superior andmedial walls of the trigone (Figure 1C).

BARROW AND FRANKEL : ARTERIOVENOUS MALFORMATIONS OF THE VENTRICULAR TRIGONE 49
Temporal Appro a c hAfter induction of anesthesia, the patient is placed ina supine position with the ipsilateral shoulder ele-vated and the head parallel to the floor with the ver-tex angled slightly downward. The head is held inposition by a radiolucent headholder. A horseshoe-shaped incision is made around the auricle of the earf rom the zygomatic arch to the re t romastoid re g i o n .A temporal craniotomy is extended to the floor of the middle cranial fossa (Figure 2). Dural tack-ups u t u res are placed and the dura is opened. The AV Mis localized along with any associated hematoma uti-lizing intraoperative ultrasound. The vein of Labbé isidentified and a 1- to 2-cm incision is created in theinferior temporal gyrus. The middle temporal gyrusmay be traversed in the nondominant hemisphere .The cortisectomy should be planned in order to pro-vide the most direct access to the AVM while pro t e c t-ing the vein of Labbé. A small horizontal cortical inci-sion parallel to the optic radiations will minimize the
risk of visual field deficits (Figure 3 upper). The oper-ating microscope is used to assist in guiding the dis-section slightly posteriorly and superiorly toward thetrigone with suction and bipolar cautery (Figure 4).S e l f - retaining retractors are used to maintain expo-s u re (Figure 3 lower). To minimize injury to the elo-quent cortex, minimal force should be used in plac-ing the retractors. If a hematoma is present, it isevacuated to provide more relaxation and exposure .Once the trigone is entered, the brain relaxes signifi-cantly due to the drainage of cere b rospinal fluid andminimal retraction is necessary to maintain ade-quate exposure. Utilizing this approach, the surg e o nusually encounters the nidus of the AVM prior to thefeeding arteries. Dissection must be carried circ u m-f e rentially around the nidus to the feeders that aresequentially coagulated and/or clipped and divided( F i g u re 5). The deep venous drainage is usually onthe medial aspect of the AVM and is preserved untilthe AVM is completely devascularized.
F i g u re 1. Various relationships of trigonal AVMs to the ventricu-lar trigone. A = AVM along the lateral, anterior, or inferior wall ofthe trigone. B = AVM on the medial aspect of the trigone. C = AV Minvolving the superior wall of the trigone.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 850
F i g u re 4. Temporal approach. Illustration of the direction of the operativea p p roach through the inferior or middle temporal gyrus to the ventriculart r i g o n e .
F i g u re 2. Skin incision (solid line) and temporal craniotomy (hatched line)for the temporal approach to AVMs of the ventricular trigone.

BARROW AND FRANKEL : ARTERIOVENOUS MALFORMATIONS OF THE VENTRICULAR TRIGONE 51
F i g u re 3. Temporal approach. Illustrations demonstrating thehorizontal cortical incision parallel to the optic radiations( u p p e r ) and use of self-retaining retractor to maintain expo-s u re ( l o w e r ) .
F i g u re 5. Temporal approach. Illustration of coronal section of thebrain demonstrating the relationship of the AVM to the ventriculartrigone and the operative approach through the inferior temporalg y r u s .

Parieto-Occipital Appro a c hThe patient is placed in a semi-sitting “slouch” orlounging position, with the head slightly flexed (Fig-u re 6). The external landmark for the cortical inci-sion is a point approximately 9 cm cephalad to theinion and 1.5 to 2.0 cm lateral to the midline (Figure7A). A horseshoe-shaped skin incision is centere dover this point, extending to the midline and basedinferiorly. Burr holes are placed and a parieto-occipi-tal craniotomy is created that is centered on theabove landmark (Figure 7A). Once the dura is ex-posed, it can be opened with the flap based on thesagittal sinus. After opening the dura, the exact loca-tion of the cortical incision should be made byd i rectly measuring 7.0 cm above the occipital poleand 2.0 cm lateral to the midline (Figure 7A). A later-ally oriented cortical incision is then cre a t e d ,a p p roximately 2.0 cm in length, and the approach tothe trigone is aimed toward the ipsilateral pupil (Fig-
u re 7B). Again, intraoperative ultrasound or animage-guided stereotactic navigational system maybe used to increase the precision of the approach. Aswith the transtemporal approach, the surgeon usu-ally initially encounters the nidus of the AVM; cir-c u m f e rential dissection around the superior, medial,or lateral surface of the nidus exposes the feedingarteries (Figure 8). The surgeon has a direct view tothe trigone from a superior angle using thisa p p roach. This is opposed to the oblique tangentialview given to the superior portion of the trigoneobtained from a parasagittal approach. In addition,t h e re is less retraction re q u i red than for theparasagittal approach in order to reach this superiorregion of the trigone, and prolonged retraction ofparasagittal veins is avoided. Since placement of thecortical incision is between the parietal sensoryassociation fibers and the occipital visual associationfibers, the risk of neurological injury is minimized.
NEUROSURGICAL OPERATIVE ATLAS. VOL. 852
F i g u re 6. Parieto-occipital transcortical approach. Patient is in a semi-sitting“slouch” or lounging position with the head slightly flexed. A r ro w = dire c t i o nof approach to the ventricular trigone.

BARROW AND FRANKEL : ARTERIOVENOUS MALFORMATIONS OF THE VENTRICULAR TRIGONE 53
F i g u re 7. Parieto-occipital transcortical approach. Posterior (A) and lateral (B) views of external and internal landmarksfor approach to the ventricular trigone. Solid line = skin incision; hatched line = craniotomy.
A B
Figure 8. Parieto-occipital transcortical approach. Illustrationof laterally oriented cortical incision with exposure maintainedby self-retaining retractors. The AVM is encountered on thesuperior surface of the ventricular trigone and extends intothe ventricular system.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 854
Parasagittal Interhemispheric Appro a c hThe patient is positioned in the lateral position withthe ipsilateral shoulder on a roll and the head paral-lel to the floor with the AVM side down, so that grav-ity assists in retraction of the occipital lobe (Figure9). A horseshoe-shaped incision is made in the occip-ital region based laterally. An occipital craniotomy isc reated with the medial burr holes placed over thesuperior sagittal sinus (Figure 10). The dural open-ing is based medially on the superior sagittal sinus.The occipital lobe can then be retracted from the falxsince there are usually no veins draining from thisa rea of the cortex to the superior sagittal sinus.Retraction is minimized by the positioning of thepatient, which allows the side with the lesion to fallaway from the falx. The calcarine or parieto-occipitalsulci are opened to expose the most medial aspect ofthe AVM (Figure 11). One disadvantage of this ap-p roach is that the surgeon often exposes the venous
Figure 9. Parasagittal interhemispheric approach. Patient is positioned with theside of the craniotomy dependent to allow gravity to assist with occipital lobe retrac-tion. Solid line = skin incision; hatched line = craniotomy.
drainage before the arterial supply. The former mustbe protected until the AVM is devascularized. Feed-ing vessels are then coagulated and divided with lar-ger arteries requiring clips. Venous drainage is thencoagulated and/or clip ligated and divided.
A variation of this approach involves parafalcinedissection contralateral to the side of the AVM ino rder to approach the AVM from a more perpendicu-lar trajectory. The patient can be positioned in a semi-sitting slouch position. The horseshoe-shaped inci-sion is made across the midline with the base of theflap on the side contralateral to the lesion. The cra-niotomy crosses the midline instead of basing itselfon the superior sagittal sinus and is mainly contralat-eral to the AVM. The dura is opened contralateral tothe AVM and the flap is based on the superior sagittalsinus. The falx is split, allowing access to the hemi-s p h e re ipsilateral to the lesion, and is appro a c h e dtranscortically as described above.

BARROW AND FRANKEL : ARTERIOVENOUS MALFORMATIONS OF THE VENTRICULAR TRIGONE 55
F i g u re 11. Parasagittal interhemispheric approach. The calcarine fissurehas been opened and the AVM is approached beneath the surface of theoccipital lobe. Circ u m f e rential dissection around the AVM is utilized todevascularize the lesion.
F i g u re 10. Parasagittal interhemispheric approach. Illustration of an AV Mon the medial surface of the ventricular trigone. The craniotomy is cen-t e red over the occipital lobe extending to the occipital tip, and the AVM isexposed via an interhemispheric approach. A r row points to location ofAVM and relationship to the ventricular trigone on insert.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 856
INTRAOPERATIVE ANGIOGRAPHYOnce the AVM has been surgically removed, we ro u-tinely per f o rm intraoperative angiography to docu-ment complete obliteration of the malformation. Ifd i s c o v e red postoperatively, incompletely re s e c t e dAVMs are associated with a significant risk of hemor-rhage and re q u i re reoperation. If any portion of theAVM is identified on intraoperative angiography, theresection bed is re - e x p l o red and residual malform a-tion re s e c t e d .
HEMOSTASIS AND CLOSUREOnce complete removal of the malformation is docu-mented by intraoperative angiography, the re s e c t i o nbed is carefully inspected under the operating micro-scope to be certain that there is absolute hemostasis.Under constant irrigation, the surgeon examines theresection bed with a piece of cotton or cottonoid pattyand suction. Any bleeding points are carefully coagu-lated with bipolar cautery because one should notrely on hemostatic agents to arrest bleeding in theresection bed. During this stage of inspection, the pa-tient’s blood pre s s u re is maintained at a normal orslightly elevated level. Once excellent hemostasis isobtained, the resection bed is lined with a single layerof Surgicel. The Surgicel layer should turn bro w nwhen adequate hemostasis has been achieved. Anya reas of red indicate inadequate hemostasis andre q u i re removal of the Surgicel and complete contro lof the bleeding site. Gelfoam or Avitene packing mayo b s c u re underlying bleeding and are avoided. Oncep roper hemostasis is achieved, the anesthesiologist isasked to perf o rm a Valsalva maneuver on the patientto ensure that there are no venous bleeders. Theresection cavity is filled with saline, and the dura isclosed in a watertight fashion. The bone flap is re-placed with sutures or miniplates, and the wound isclosed in layers.
COMPLICATIONSThe surgical management of intracranial AVMs pre-sents some of the most complex decision-makingand technical challenges in neuro s u rgery. Complica-tions and misadventures may occur at any point inthe diagnostic or therapeutic process in the manage-ment of trigonal AV M s .
P reoperatively, the patient must undergo appro-priate risk stratification with re g a rd to other medicalconditions that may affect the intraoperative andpostoperative hospital course. Multimodal imagingobtained during the preoperative work-up is impor-tant for providing the surgeon with spatial conceptu-alization of the lesion with respect to the re g i o n a lanatomy. All risks that apply to craniotomy in gen-eral and AVM surgery specifically exist in the surg i-cal management of trigonal AVMs. Some potentialcomplications are unique to these lesions due totheir anatomical relationships to the optic radia-tions, language cortex, and thalamus.
Intraoperatively, most complications can beavoided by using meticulous technique. Since theseAVMs are in eloquent or functionally important cor-tex, the margin of resection must not be too wide.Dissection must closely follow the nidus as there mayor may not be a clear gliotic plane to follow. Choosingthe correct approach to expose the AVM will avoidretraction injury to the surrounding normal cortexand minimize the risk of damage to the optic radia-tions. Arteries en passage that supply the AVM butextend beyond to perfuse normal brain must be iden-tified. Only pedicles devoted to the AVM are coagu-lated or clipped. As with other AVMs, care must betaken to protect the venous drainage until the malfor-mation has been devascularized to avoid congestionand bleeding from the nidus. Postoperative hemor-rhage may occur due to rebleeding from the re t a i n e dAVM, poor intraoperative hemostasis, or normal per-fusion pre s s u re bre a k t h ro u g h .
AVMs in the region of the ventricular trigone arenot common. Their surgical treatment is confoundedby the lack of cortical re p resentation, involvement ofthe choroid plexus, deep arterial feeders and venousdrainage, and location in functionally important cor-tex. These technical challenges have resulted in thedevelopment of the surgical approaches describedabove. Selective angiography and MRI assist in deter-mining which approach is optimal for the individualAVM. The judicious use of preoperative embolizationto devascularize the lesion and intraoperative angiog-raphy to document achievement of the surgical goalsa re additional adjuncts that enhance the safety ande fficacy of surgical treatment of these lesions.

I N T R O D U C T I O NDural arteriovenous malformations of the transverseand sigmoid sinuses are abnormal direct shunts be-tween the dural arterial supply and the dural venoussystem. They re p resent 10% of all intracranial vas-cular malformations. The lesions are acquired in lifeand are more appropriately re f e r red to as fistulasrather than malformations. The management of du-ral arteriovenous fistulas (DAVFs) re q u i res a clearunderstanding of the angioarc h i t e c t u re of the lesion.This chapter describes the treatment appro a c h ,which uses the combined neuro s u rgical and neu-rointerventional services with specific emphasis ons u rgical treatment. A case is also presented to illus-trate the concepts presented in this chapter. Theselesions can be extremely complex and re q u i re an un-derstanding of the arterial supply, nidus location,venous drainage, and location of the vein of Labbé.
The arterial supply to these lesions can originatef rom any of the arteries that supply the dura. Thesearteries include transcranial perforating vessels fro mthe occipital, posterior auricular, middle meningeal,and ascending pharyngeal branches of the extern a lc a rotid artery. Supply can also come from the dural
DURAL ARTERIOVENOUS M A L F O R M ATIONS OF THE
TRANSVERSE AND SIGMOID SINUSESTODD A. KUETHER, M.D.G A RY M. NESBIT, M . D .
S TANLEY L. BARNWELL, M.D., PH. D .
57
branches that arise from the anterior, middle, andposterior cerebral arteries, in addition to petrous andc a v e rnous branches of the internal carotid arteryand the posterior meningeal branch of the vertebralartery. Infrequently, there can also be branches fro mthe subclavian artery. This vast number of potentialsupplying arteries is the basis for treatment failurewhen only supplying arteries are embolized or surg i-cally ligated. Occluding any portion of the arterialsupply often leads to hypertrophy of the re m a i n i n gsupplying vessels. For this reason, the arterial sup-ply to DAVFs does not strongly guide the therapy.
The nidus of the DAVF is located in the wall of thesinus, is usually small and can be spread over severalcentimeters of the sinus. The nidus can generally bedefined on the early phase of the angiogram, andtherapy is directed at this portion of the sinus. Hyper-t rophied arteries and veins supplying the fistula cangive the appearance that the bone, brain, or convexitydura is involved in the lesion, although the true nidusis located within the dura and around the sinus.
The crucial aspect of these lesions is the venousdrainage. Venous drainage is the most importantfactor in assessing the risk of stroke as well asd i recting treatment of the lesion. A distinction mustbe made between the normal venous drainage pat-t e rn of the brain into cortical veins and duralsinuses and the drainage of the DAV F, which mayalso fill dural sinuses and cortical veins in a re t ro-grade dire c t i o n .
© 1999 The American Association of Neurological Surg e o n s

PATIENT SELECTIONPatients with DAVFs can present with a number ofd i ff e rent clinical symptoms. These symptoms dependon the location, flow, and venous drainage of theD AV F. Most commonly, the patient will develop ap u l s e - s y n c h ronous bruit. This bruit may be bare l yaudible to the patient or, in rare instances, so loud itcan be heard by others in the room. The character ofthe bruit can change as flow dynamics within the fis-tula change.
Many patients present with a new headache pat-t e rn that may relate to pre s s u re changes within thesinus. These headaches are often more prominent onthe side of the fistula and can change in characterwith the fistula.
Venous hypertension without hemorrhage canalso result in neurological deficits as a result of cere-bral edema and infarction. Memory or visual impair-ment may be noted by the patient. Symptoms re l a t e dto raised intracranial pre s s u re may also occur as aresult of impaired cere b rospinal fluid absorption.D AVFs with cortical drainage can also result ins e i z u re s .
D AVFs may present with epidural, subdural, sub-arachnoid, or intracerebral hemorrhage. Patientswith spontaneous brain hemorrhages must be fullyevaluated for a possible DAV F.
ANGIOARCHITECTUREThe angioarc h i t e c t u re of DAVFs involving the trans-verse and sigmoid sinuses can be divided into fivecategories based on the patterns of venous drainageof the fistulas. These categories are not rigid andsome lesions may not fit exactly within a single cate-gory. It is equally important to understand and char-acterize the venous drainage of the brain with specificattention to the vein of Labbé. This chapter empha-sizes these aspects of the DAV F. These categories aregraphically illustrated in Figure 1.
N o rmal Antegrade FlowD AVFs with normal antegrade flow drain into the in-volved sinus and down the ipsilateral jugular vein( F i g u re 1A). The arterial supply to the fistula is usu-ally small and the sinus pre s s u re is not suff i c i e n t l yelevated to cause re t rograde flow toward the torc u l a .The direction of flow is not only dependent on theflow rate but also the presence of any stenosis in theipsilateral sigmoid sinus or jugular vein. The sagittaland straight sinuses may drain to the right and/orleft transverse sinus.
Antegrade and Retrograde Flow Through the Transverse-Sigmoid SinusD AVFs with antegrade and re t rograde flow are usu-ally larger and the sinus pre s s u re is sufficient tocause antegrade flow to the ipsilateral jugular veinas well as re t rograde flow toward the torcula (Figure
1B). The sagittal and straight sinuses drain via thet o rcula and contralateral transverse sinus and jugu-lar vein. Any stenosis in the ipsilateral sigmoid sinusor jugular vein may increase the re t rograde flow. Inthe presence of jugular venous outflow re s t r i c t i o n ,even small DAVFs may have some re t rograde flow.
R e t rograde Flow to the To rc u l aSome fistulas appear to drain entirely toward the
t o rcula, contralateral transverse sinus, and jugularvein. This pattern occurs when the ipsilateral sig-moid sinus, jugular bulb, or jugular vein is occluded( F i g u re 1C). The flow may also appear angiographi-cally to be entirely re t rograde in cases of severestenosis. Only when a microcatheter is advancedt h rough the stenosis can a determination of patencybe made.
Antegrade and Retrograde Flow Through the Transverse-Sigmoid Sinus with Cortical Venous Drainage
This category applies to fistulas that, in additionto drainage through the involved dural sinuses, havedrainage into cortical veins (Figure 1D). The vein ofLabbé is commonly involved with cortical venousdrainage. This group would also include those fistu-las that drain re t rograde into the straight sinus,rather than across the torcula to the contralateraltransverse sinus. The critical finding in this group iscortical venous drainage. This pattern has a muchhigher risk for hemorrhage. Cortical venous drainagemay result from large fistulas with high flow ratesand/or venous outflow restriction in the dural si-nuses or jugular vein. Both states result in highp re s s u res in the transverse and sigmoid sinuses.The result is reflux of blood into the cortical veins.
Flow into Cortical Veins OnlyA variety of fistulas may drain entirely into corticalveins and not the adjacent dural sinuses (Figure 1E).This may occur angiographically if the associatedsinus is thrombosed. Rarely, the fistula may draine n t i rely into cortical veins even if the underlying si-nus is completely normal. The connection betweenthe fistula and the sinus has either thrombosed orwas never present. These fistulas have the highestrisk of hemorrhage because of the high venous pre s-s u re. They are similar to the DAVFs of the anteriorcranial fossa/ethmoidal groove that virtually alwaysdrain to cortical veins and present with hemorrh a g e .
The Vein of LabbéThe vein of Labbé provides venous drainage from theparietal and posterior temporal lobes. Usually, it isnot a single vein but several veins that enter thesinus at the junction of the transverse and sigmoidsinuses. This vein may be very small and inconse-quential or large and provide a significant and cru-
NEUROSURGICAL OPERATIVE ATLAS. VOL. 858

KUETHER ET AL : DURAL ARTERIOVENOUS MALFORMATIONS OF THE TRANSVERSE AND SIGMOID SINUSES 59
F i g u re 1. The angioarc h i t e c t u re of a right DAVF of thetransverse-sigmoid sinus supplied by the right occipitalartery. A , n o rmal antegrade flow down the right jugularvein. B, antegrade and re t rograde flow toward the torc u l awith right sigmoid sinus stenosis. C , re t rograde flow tothe torcula with right sigmoid sinus occlusion. D , a n t e-grade and re t rograde flow with cortical venous drainageinto the right vein of Labbé. E , flow into cortical veinsonly. Flow in the sinus is normal with no connection tothe fistula located in the wall of the sinus. All drainage ist h rough the sinus wall into the right vein of Labbé.
A
B C
D E

NEUROSURGICAL OPERATIVE ATLAS. VOL. 860
cial pathway of venous drainage from the brain. Thevein is seen on late phases of an internal caro t i dangiogram on lateral and frontal projections. DAV F sof the transverse and sigmoid sinus may alter drain-age of the vein of Labbé. The pre s s u re in a norm a ldural sinus is less than 10 mm Hg. Usually, the veinof Labbé drains the posterior temporal lobe into thetransverse-sigmoid sinus junction. Direct arterial tosinus shunts increase the pre s s u re in the sinus.Depending on the size of the shunt and the pre s e n c eof venous outflow restriction in the sigmoid sinus orjugular vein, pre s s u re rises within the sinus. As thep re s s u re in the sinus rises, flow in the vein of Labbéceases; if the pre s s u re is sufficiently high, flow willreverse direction. This is what is re f e r red to as corti-cal venous drainage. The vein of Labbé may not beseen on the delayed phase of the internal caro t i dangiogram if there is re t rograde flow that is dif f i c u l tto distinguish from a small or absent vein.
INDICATIONS FOR TREATMENTThe decision to surgically treat an individual must bebased on knowledge of the patient’s symptoms, an-giographic anatomy, risk factors for hemorrhage orn e u rological deficits, and an understanding of therisks of surgical tre a t m e n t .
A common indication for treatment is patientintolerance of the bruit. In many cases, the patient isable to cope very well with a loud bruit and no tre a t-ment is indicated. However, appropriate treatment iso ff e red to those who cannot tolerate the bruit.
Risk factors for hemorrhage and stroke includecortical venous drainage and re t rograde flow into thet o rcula and straight sinus. These conditions lead tovenous hypertension, which can also result in cere-bral edema and associated neurological deficits.Nearly all DAVFs associated with hemorrhage, raisedintracranial pre s s u re, or neurological deficits haveone of these risk factors. Every effort should be madeto cure these high-risk lesions. Subtotal occlusionmay not protect the patient from further episodes ofbleeding; there f o re, the goal of treatment is completeo c c l u s i o n .
TREATMENTOnce the indications for treatment and the angioar-c h i t e c t u re of the fistula have been determined, tre a t-ment plans can proceed. The risks and benefits ofeach treatment must be weighed against the risk ofs t roke from the fistula. Patients with hemorrhage, in-f a rction, or cerebral edema with associated neuro l o g-ical deficits are considered at high risk and shouldhave definitive treatment that results in complete ob-literation of the fistula. Subtotal treatment may notp rovide patients with protection from further hemor-rhage, since the fistula may re t u rn with hypertro p h yof residual arterial feeders. However, in patients whohave low-risk fistulas, the options for treatment are
m o re broad. Low-risk fistulas may not re q u i re surg i-cal treatment if the patient can tolerate the symp-toms. If the fistula is treated, palliative therapy maybe more appropriate for the initial treatment. If thefistula recurs, the fistula may eventually need moredefinitive treatment for cure. The following is a re v i e wof the diff e rent treatment options. These therapiesa re primarily based on fistula angioarc h i t e c t u re .
CONSERVATIVE TREATMENTThe spontaneous remission of DAVFs has been re-ported in rare instances. Although the incidence ofspontaneous closure is not known, it needs to bec o n s i d e red when discussing the natural history ofthese lesions. Low- or high-risk DAVFs may closewithout tre a t m e n t .
COMPRESSION THERAPYIn many instances, DAVFs of the transverse and sig-moid sinuses have arterial supply from the occipitalartery. Before being evaluated in a clinic, many pa-tients have already noticed that they can stop theirbruit by compressing this artery. Compression ther-apy is an appropriate option for the compliantpatient with a low-risk fistula. Compression of thec a rotid artery may also lead to thrombosis of the fis-tula. The arteries are compressed in an incre a s i n gfashion over several days to a maximum of 30 sec-onds 3 times per hour. This treatment is continuedfor 3 weeks before follow-up. However, patients withhigh-risk fistulas, such as those with cortical venousdrainage, hemorrhage, or infarction, should not per-f o rm compressive therapy and if possible should un-d e rgo more definitive treatment. Compressive ther-apy has a relatively low chance of resulting in fistulat h rombosis, with most patients eventually underg o-ing additional tre a t m e n t .
EMBOLIZATIONM o re definitive treatment of DAVFs of the transverseand sigmoid sinuses re q u i res one or a combination ofthe following: transarterial embolization, transvenousembolization, or intraoperative transvenous emboliza-tion with surgical re s e c t i o n .
Transarterial EmbolizationTransarterial embolization may be used as either de-finitive treatment of a DAVF or as a preoperative ad-junct. Microcatheters are navigated into as manyarteries supplying the fistula as possible which arethen occluded with an embolic agent. General classesof embolic agents include particles (Gelfoam orpolyvinyl alcohol (PVA)), platinum microcoils, liquidadhesives, or sclerosing agents (glucose, alcohol, orS o t r a d e c o l ) .
A thorough understanding of possible collateralconnections between branches is imperative toreduce the risk of neurological deficit resulting fro m

KUETHER ET AL : DURAL ARTERIOVENOUS MALFORMATIONS OF THE TRANSVERSE AND SIGMOID SINUSES 61
arterial embolization. Virtually all external caro t i dartery branches relevant to a DAVF of the transverseand sigmoid sinuses also have anastomoses witheither the internal carotid artery or the vertebralartery. Knowledge of the arterial supply to the cra-nial nerves is also important to avoid complications.P rovocative testing of an artery can easily be per-f o rmed by neurological testing during selective intra-arterial lidocaine injection. If neurological deficits re-sult, it is probably not safe to embolize that arterywith small particles or liquid adhesives.
Although arterial embolization can be perf o rm e dwith little risk if particles or coils are used, the mainc o n c e rn is a low cure rate with isolated arterial em-bolization. Even if the arterial supply to the DAVF isalmost completely closed, a high rate of re c u r re n c eremains. This re c u r rence is due to the large numberof arterial feeders that supply a fistula. It is usuallynot possible to embolize every arterial pedicle, andthe remaining arteries will hypertrophy and re - e s t a b-lish the fistula. However, transarterial embolizationis usually effective in eliminating or reducing thebruit for some time. This may alleviate the patient’ssymptoms to a degree that can be tolerated. The fis-tula may also pro g ress to complete thro m b o s i s .
Transvenous EmbolizationTranvenous embolization can be perf o rmed eitherp e rcutaneously, via the femoral vein, or intraopera-tively with direct exposure of the sinus. This ap-p roach is safe but carries increased risk in the pre s-ence of cortical venous drainage. In those casesembolization may divert flow into the cortical veins,i n c reasing the risk of hemorrhage. Without corticalvenous drainage, embolization is safe due to the lowchance of hemorrhage from dural sinuses. Emboliza-tion of cortical veins is generally not safe secondaryto their thin walls, which increase the risk of per-f o r a t i o n .
In the presence of cortical venous drainage, aD AVF may still be embolized safely if the sinus is sur-gically exposed. The sinus is exposed via a pro c e s sdescribed later in this chapter. After exposing thecortex around the sinus, the arterialized veins drain-ing re t rograde from the sinus are divided. Any nor-mal draining vein is preserved. The sinus can then bep u n c t u red and coils placed in the sinus along thee n t i re length involved in the DAV F. This operativee x p o s u re allows for occlusion of these fragile re t ro-grade draining veins prior to sinus embolization, pre-venting a catastrophic hemorrh a g e .
The placement of coils transvenously must be pre-cise, whether perf o rmed percutaneously or dire c t l yafter operative exposure. The coils are placed acro s sthe entire length of involved sinus. If the entire in-volved portion is not occluded, any residual will con-tinue to allow flow through the fistula and will en-l a rge with time. Care must be taken to avoid sinus
occlusion where normal veins, especially the vein ofLabbé, drain antegrade into the sinus. There is usu-ally enough separation between a normal vein ofLabbé and the fistula to allow placement of coilsa c ross the fistula while preserving the vein. In casesof close proximity, operative exposure and intraoper-ative coil placement allow for more precise placementof the coils.
S u rgical ResectionT h e re are relatively few instances in which it is nec-essary to resect the involved sinus. When the sinusis thrombosed and venous drainage of the DAVF isonly into cortical veins, surgery is the best appro a c hto occlude the veins draining the fistula. Resection ofthe sinus is not needed. An example of when surg i c a lresection may be re q u i red is the case of a fistula withunderlying transverse and sigmoid sinus thro m b o s i sthat drains into the superior petrosal sinus. Thissinus may be more difficult to embolize due to itssmall size and deep location. Surgical resection ofthe involved sinus is technically superior and morelikely to result in cure of the DAV F.
S u rgical resection of lesions affecting the trans-verse and sigmoid sinuses has been well describedp reviously but is reviewed in this chapter.
CLINICAL APPROACH TO DURAL ARTERIOVENOUS FISTULAS OF THETRANSVERSE AND SIGMOID SINUSESThe approach to treating DAVFs of the transverseand sigmoid sinuses depends largely on the angioar-c h i t e c t u re of the fistula. As mentioned pre v i o u s l y ,this is based on the five patterns of venous drainagef rom the fistula, which include the following.
• N o rmal antegrade flow through the transverse-sigmoid sinus to the jugular vein
• Antegrade and re t rograde flow through the transverse-sigmoid sinus
• R e t rograde flow to the torc u l a• Antegrade and/or re t rograde flow through the
sinus with cortical venous drainage• Flow into cortical veins only
N o rmal Antegrade Flow Through the Transverse-Sigmoid Sinus to the Jugular Ve i nIn this type of malformation, the clinical pro b l e mrelates to a bruit or to headaches. The risk of hemor-rhage or stroke is low since the fistula flows ante-grade through the sinuses. Treatment is off e red onlywhen there is intolerance of these symptoms. Manypatients are surprisingly tolerant of the bruit, espe-cially when re a s s u red that the risk of stroke is small.H o w e v e r, other patients experience serious interrup-tions of sleep, normal daily activities, and work.
Arterial embolization is an effective approach toeliminating or reducing the intensity of the bruit,although the effect may be short-lived. Catheter

NEUROSURGICAL OPERATIVE ATLAS. VOL. 862
i m p rovements have allowed for more complete arter-ial occlusion, but it is important to understand thelimitations of this approach and to avoid multiplelengthy arterial embolization pro c e d u res in those pa-tients with re c u r rent DAVF after a similar pro c e d u re .A curative approach is taken in those patients withsymptomatic re c u r rence after one or two arterialembolization pro c e d u res if the contralateral trans-verse and sigmoid sinuses can provide venous drain-age from the brain. Prior to occluding the sinustransvenously, it must be confirmed that flow in thesuperior sagittal sinus can enter the opposite trans-verse sinus; flow in the vein of Labbé must also bep reserved during the embolization. If flow in the veinof Labbé cannot be preserved, or the opposite trans-verse sinus is small, transvenous embolizationshould not be perf o rm e d .
Antegrade and Retrograde Flow Through the Transverse-Sigmoid SinusThe presence of re t rograde flow in the transversesinus, directed toward the torcula, indicates that theinvolved sinus can be safely occluded perc u t a-neously without causing a venous occlusive stro k e .The contralateral transverse and sigmoid sinuseswill provide sufficient venous outflow from the brain.The venous phase of an angiogram of the ipsilaterali n t e rnal carotid artery generally shows venous drain-age to the opposite transverse sinus or anteriorly tothe cavernous sinus.
Once again, the important factor is the vein ofLabbé. If transvenous embolization is perf o rmed, thevein must not be occluded. Generally, the fistula islocated closer to the sigmoid sinus, allowing for thecoils in the sinus to occlude the fistula without com-p romising flow in the vein of Labbé. After tre a t m e n t ,the vein drains into the transverse sinus that flowsre t rograde to the torcula and contralateral trans-verse sinus. If the vein of Labbé is located at thesame portion of sinus that contains the fistula, thefistula cannot be safely occluded. In this instance,transarterial embolization may be all that can beo ff e red since surgical resection is likely to also re s u l tin occlusion of the vein of Labbé.
The first step in treating these lesions is trans-arterial embolization to reduce the flow into theD AV F. Transvenous embolization is then perf o rm e dduring the same pro c e d u re to occlude venousdrainage from the fistula. Coils are placed in theinvolved section of sinus, maintaining flow in thevein of Labbé. Often the coils are packed down to thejugular bulb.
R e t rograde Flow to the To rc u l aA DAVF that drains entirely toward the torcula isusually a high-flow lesion associated with severevenous outflow restriction or occlusion of the ipsilat-
eral sigmoid sinus. Although the sigmoid sinus mayappear occluded, a microcatheter can sometimes benavigated through the apparent occlusion. The veinof Labbé usually does not fill because it is either oc-cluded or blood from the posterior temporal lobedrains anteriorly toward the cavernous sinus. Thehigh pre s s u re in the sinus prevents normal drainagef rom the vein of Labbé into the transverse sinus. Am o re extreme situation arises when the pre s s u re iselevated enough to result in re t rograde flow in thevein of Labbé from the fistula and cortical venousd r a i n a g e .
The treatment of these lesions is similar to thatdescribed above. First, transarterial embolization isp e rf o rmed to reduce flow through the fistula. Tr a n s-venous embolization is re q u i red to cure this lesion.Coils are placed in the involved segment of sinusdraining the fistula. To place the coils, the cathetermust either be navigated through the occluded sinusor through the opposite transverse sinus and acro s sthe torcula. If the vein of Labbé does not fill, it can bes a c r i f i c e d .
Antegrade and/or Retrograde Flow Thro u g hthe Sinus with Cortical Venous DrainageThe presence of cortical venous drainage definesthese lesions as high risk for causing stroke, so ther-apy is directed at curing these lesions. Incompletetherapy may provide a risk reduction if the corticalvenous drainage is occluded. Transarterial emboliza-tion is first perf o rmed to reduce flow through theD AV F. Occlusion of the venous drainage is then per-f o rmed, which re q u i res surgical resection or surg i c a le x p o s u re with intraoperative embolization.
Flow Into Cortical Veins OnlyThe fistula present when the involved sinus is thro m-bosed and the venous drainage of the DAVF is en-t i rely through the cortical veins is perhaps the fistulawith the highest risk. This case may re p resent a pro-g ression of the above lesions as the sinus thro m b o s i sp ro g resses to occlusion. Surgery is the definitive ther-apy for these lesions. Preoperative transarterial em-bolization may be useful to reduce flow through thefistula and reduce surgical blood loss. However, it isthe surgical interruption of the draining veins thatp rovides the cure. Intraoperative angiography is par-ticularly helpful to ensure that all draining veins areoccluded. A portable digital subtraction angiographicmachine can be used in conjunction with a radio-lucent headholder. After the patient is placed undergeneral anesthesia, a sheath can be placed with acontinuous infusion of heparin. This sheath is thenkept sterile; when an intraoperative angiogram is re-q u i red, the selective angiogram can be perf o rmed ra-pidly through this sheath. The surgical exposure isd e t e rmined by whether the veins drain supra- or in-

KUETHER ET AL : DURAL ARTERIOVENOUS MALFORMATIONS OF THE TRANSVERSE AND SIGMOID SINUSES 63
fratentorially, or both. It is not necessary to re m o v ethe sinus since it is already occluded. These lesionscannot be treated percutaneously since the drainingveins are too tortuous and thin to safely catheterizeand embolize. The authors have encountered a pa-tient who spontaneously thrombosed before surg e r y .
R a rely, a fistula will be identified that drains en-t i rely into cortical veins only, with a normal patenttransverse sinus. These DAVFs are treated the sameway as above with the exception that the underlyingsinus must not be damaged since it is carrying nor-mal venous blood. The vein of Labbé may drain in an o rmal fashion into the sinus and must be pre s e r v e dwhen this is encountered.
SURGICAL EXPOSURE WITH INTRAOPERATIVE EMBOLIZATIONAs with any surgery around the dural sinuses, thea p p ropriate anesthetic precautions must be taken tot reat possible air embolism. Initially, the high pre s-s u re in the sinus prevents air from entering thesinus. As the fistula is closed, pre s s u re in the sinus
d rops and air embolism may occur. The sitting posi-tion increases the risk of air embolism.
Positioning the PatientThe patient can be positioned in a park bench thre e -quarter prone position or in a supine position withthe shoulder elevated and the head turned sharply ina headholder. The region that must be accessible ex-tends from the mastoid to the inion. Either of thesepositions allows for intraoperative angiography if asheath has been placed in the femoral artery prior top o s i t i o n i n g .
Scalp FlapThe incision is generally shaped like a hockey stick,which allows for scalp retraction and access from themastoid to the inion (Figure 2). Bleeding from thescalp edges can be significant secondary to hypertro-phy of either the occipital, superficial temporal, orposterior auricular artery. These arteries should al-ways be embolized preoperatively if they supply the
A
B
C
F i g u re 2. Head position for surgical exposure of a DAVF of the right transverse-sigmoid sinus. Skin incision ( A ), craniotomy ( B ), and dural incisions ( C ) a reshown. The patient is positioned three quarters prone on the operating table.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 864
fistula. Care is taken to avoid any incision that mayresult in an ischemic flap. Raney clips are applied tothe scalp edges, and the flap is reflected to its base,exposing the mastoid tip. Some of the deep cervicalfascia and musculature are separated from theoccipital bone with a Bovie. Occasionally, large feed-ing or draining vessels are encountered that can becoagulated and divided. Venous bone bleeding is eas-ily controlled with bone wax. Fishhooks are thenused to retract the flap for adequate exposure .
C r a n i o t o m yThe craniotomy must be carefully planned to includethe necessary portion of the sinus as well as to avoidany catastrophic bleeding. If the patient has hadtransarterial embolization, flow through the fistulashould be significantly lower. Once the extent of ex-p o s u re has been determined, two sets of burr holesa re drilled; one burr hole set is located above thesinus and one set below the sinus (Figure 2). Thesesets of burr holes are placed at the medial and lateralextents of the craniotomy. A #3 Penfield dissector canthen be used to separate the dura and sinus from theoverlying bone. The drill can also be used to re m o v ethe bone directly over the sinus until it can be visual-ized through a very thin layer of bone. Once the sinushas been safely crossed, a craniotome can be used tocomplete the removal of the bone flap. It cannot beemphasized enough that great care must be takenwhen using the craniotome to avoid laceration of thesinus. The dura should be bluntly dissected off thebone before cutting the bone with the craniotome. Ab u r red bit can be used to remove the bone overlyingany area of concern .
Pieces of Gelfoam are pre p a red to be placed overany bleeding site in the dura or laceration in thesinus. The bone flap is then carefully elevated whileseparated from the underlying dura. Once the flap iselevated, Gelfoam is quickly placed on the dura andsinus and pre s s u re is manually applied. Beginningat the edges, bleeding is controlled as quickly as pos-sible with bipolar coagulation. Gelfoam is then sys-tematically elevated while coagulating using bipolarcautery. This is continued until hemostasis is ob-tained. During this process, attention must be di-rected to the patient’s monitors for signs of venousair embolism. Pre s s u re in the sinus is generally ele-vated enough as a result of the fistula in addition tothe recumbent position to prevent air embolism.
Cortical Vein LigationAfter hemostasis has been achieved, the margins ofthe dura are tacked up to the bone edges with multi-ple interrupted sutures. These sutures are placed 2 cm apart and serve to provide hemostasis of epi-dural bleeding and prevent a postoperative epiduralh e m a t o m a .
The dura 1-2 cm above and below the transversesinus is opened parallel to the transverse sinus. Thisexposes the occipital lobe and cerebellum. Corticalveins draining the fistula are coagulated using bipo-lar cautery, clipped with Weck clips, and cut. Usuallythe vein of Labbé is one of the veins draining re t ro-grade and can be safely occluded, decreasing thevenous hypertension in the brain. The sinus is thenp u n c t u red with a catheter, and coils are placed in thesinus over the involved segment. Intraoperativeangiography is necessary to ensure that the coils aredeposited in the proper area. A large Weck clip, or lig-a t u re, is then placed across the transverse sinusbetween the portion of the sinus involved by the fis-tula and the torcula. This ensures that there is nore t rograde flow from the fistula to the torcula. Pre o p-eratively, it is important to verify that there is nodrainage through the superior petrosal sinus be-cause, if left open, it may allow the fistula to continueto drain toward the cavernous sinus.
Operative exposure prior to embolization is safestbecause of the risk of diverting flow to the corticalveins if a purely percutaneous approach is used. Asthe coils are placed in the sinus during a perc u t a-neous pro c e d u re, there is a risk that the outflow ofthe fistula through the sinus may then be diverted tothe cortical veins. These cortical veins are too thin tocatheterize and embolize. This excessive flow in theveins could cause catastrophic hemorrh a g e .
SURGICAL RESECTIONP reoperative transarterial embolization is very eff e c-tive at reducing blood loss during sinus exposureand may prevent massive hemorrhage. Reports havew a rned that blood transfusions should be startedprior to elevating the bone flap. Blood loss could ap-p roach 300 ml/min in some cases. With routine pre-operative embolization, the need for transfusion hasbeen significantly reduced and is usually not re-q u i red. Preoperative embolization is usually per-f o rmed within 48 hours prior to surg e r y .
The positioning, incision, and craniotomy shouldbe perf o rmed in a manner similar to that describedfor surgical exposure with intraoperative emboli-z a t i o n .
Sinus LigationAfter the dura has been opened parallel to the trans-verse sinus both above and below the sinus, any re t-rograde-filling cortical veins that are identified canbe coagulated, clipped, and divided.
Hemostats are then placed across the sinus andthe sinus is cut between the hemostats, leavingenough cuff of sinus to close with a running suture .The cuff is closed with a running suture and thehemostat removed.

KUETHER ET AL : DURAL ARTERIOVENOUS MALFORMATIONS OF THE TRANSVERSE AND SIGMOID SINUSES 65
Fistula ResectionOnce the sinus has been divided, the next step is tobegin dividing the tentorium toward the petro u sbone. The hemostat may be used to begin elevatingthe lateral portion of the sinus from the wound, ex-posing the tentorium. The tentorium is then slowlyincised, controlling any dural bleeding with cauteryor Weck clips. As the fistula is encountered, the sur-geon must be pre p a red to control brisk hemorrh a g e .The fistula is most commonly located near the sig-moid-transverse sinus junction. This is the point atwhich preoperative transarterial embolization canplay a very beneficial role. As resection is carried fur-ther anteriorly, the petrous bone and superior pet-rosal sinus are ultimately encountered and may con-tain many vascular channels feeding the fistula.Bleeding from these channels can be controlled withcautery, bone wax, or Surgicel, or by drilling the bonewith a diamond-tipped burr. The superior petro s a lsinus is cut and the dura is reflected off the floor ofthe middle fossa laterally to the transverse-sigmoidsinus junction.
When the fistula has been resected, the re s i d u a lsigmoid sinus can simply be packed with Surg i c e land sutured, taking care to avoid any air embolism.It is usually not necessary to resect the sigmoidsinus since the fistula most commonly involves thesinus at the junction with the transverse sinus.
As mentioned previously, when initially openingthe dura, the arterialized veins draining the sinuscan be sacrificed since the brain is not dependent onvenous drainage from these sites. However, norm a l -appearing veins, particularly the vein of Labbé if flowis antegrade, must be preserved as well as that por-tion of the sinus to avoid venous infarction. If thevein of Labbé appears to be draining antegrade intothe sinus, the sinus must be subtotally re s e c t e dallowing the vein of Labbé to drain through the supe-rior petrosal sinus or the distal sigmoid sinus. Thedural vascular supply is interrupted, preserving flowt h rough the sinus.
Prior to closure, an intraoperative angiogram canbe easily perf o rmed to verify complete closure of thefistula. If an intraoperative angiogram is planned, afemoral artery introducer can be placed prior to posi-tioning the patient.
C l o s u reThe dura is closed using an allograft dural substitutein a watertight fashion. The bone flap is re p l a c e dwith titanium microplates and the scalp is closed ina layered fashion.
DAVFS INVOLVING THE TORCULAD AVFs involving the torcula are mentioned sincethey are almost always associated with cortical ve-nous drainage and hemorrhage. Surgery is the besta p p roach and may be preceded by pre o p e r a t i v etransarterial embolization to reduce blood flow in thefistula. First, cortical venous drainage from the fis-tula is occluded as described above. If the fistuladrains entirely to the cortical veins and not into thet o rcula, it must be preserved. If the fistula drainsinto the torcula, the torcula can be sacrificed only ifall venous drainage from the brain is directed awayf rom the torcula toward the cavernous sinus.
POSTOPERATIVE CAREPatients are monitored closely in a neuro i n t e n s i v ec a re unit following surgery. Their neurological statusis closely observed for any signs that may indicatec e rebral edema, hemorrhage, or venous infarc t i o n .Depending on the treatment, anticoagulation of anytype is avoided to improve the likelihood of fistulat h ro m b o s i s .
A postoperative angiogram can be perf o rm e deither prior to discharge or on an outpatient basis.Repeat angiography is perf o rmed to document thestatus of the fistula if there is any change in thecharacteristics of the patient’s symptoms.
ILLUSTRATIVE CASEAs an example of the above treatment discussion, wep resent the case of a 75-year-old woman who pre-sented with a loud bruit, headaches, ataxia, and cog-
F i g u re 3. Angiogram of the left common carotid artery, lat-eral projection, demonstrating a markedly enlarged leftoccipital artery (a r ro w) and multiple external carotid andsmall cavernous carotid artery branches (a r ro w h e a d) sup-plying the left transverse-sigmoid sinus DAV F.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 866
nitive changes. An angiogram was perf o rmed (Figure3) which demonstrated a large high-flow left trans-verse-sigmoid sinus DAVF with supply from the leftvertebral artery and both right and left internal ande x t e rnal carotid arteries. The sigmoid sinus appeare dt h rombosed, with the predominant venous drainagere t rograde toward the torcula. There also was somereflux into cortical veins. No vein of Labbé was iden-t i f i e d .
Transarterial embolization was perf o rmed to re-duce flow through the fistula. The left occipital, acces-sory meningeal, middle meningeal, internal maxillary,and posterior auricular arteries were selectively cathe-terized, studied angiographically, tested with lido-c a i n e , and embolized with PVA particles (500-1000 µ).Post-embolization angiography (Figure 4) demon-strated marked devascularization of the DAV F, al-though supply remained from the internal carotid ar-tery and a branch of the occipital artery. As discussedabove, transarterial embolization may result in im-p rovement of symptoms but will not cure these lesionsdue to hypertrophy of remaining arterial feeders.
The patient re t u rned 2 months later for transve-
nous embolization. No cortical venous drainage wasidentified at this time. An attempt was made tocatheterize the left sigmoid sinus, but it could not beaccessed either through the left internal jugularvein, due to occluding thrombus, or across the tor-cula from the right transverse sinus, due to multiplet o rcular septations. Also noted during this pro c e d u rewas some reflux into the straight sinus, which maybe an indication that this re p resented a lesion athigher risk for stroke or hemorrhage. Definitive tre a t-ment of this lesion with occlusion of the venousdrainage was necessary. This would re q u i re surg i c a le x p o s u re of the sinus.
The patient underwent surgical exposure of theleft transverse-sigmoid sinus as previously described.The left sigmoid sinus was embolized by placing anangiocatheter into the left transverse sinus thro u g hwhich a microcatheter was positioned at the fistulasite near the sigmoid sinus (Figure 5). The sinus wasthen occluded with multiple fiber platinum coils (Fig-u re 6). An intraoperative angiogram was obtainedthat confirmed sinus occlusion and no residual f i s t u l a .
F i g u re 4. Angiograms of the left common carotid artery following arterial embolization. A , lateral pro j e c t i o n .Reduction of flow to the fistula with residual arterial supply from the left occipital artery, ascending pharyngealartery, and intracavernous branches of the internal carotid artery. B , a n t e roposterior projection. Left transverse-sigmoid DAVF seen with re t rograde venous drainage toward the torcula and contralateral sigmoid sinus (a r ro w) .
A B

KUETHER ET AL : DURAL ARTERIOVENOUS MALFORMATIONS OF THE TRANSVERSE AND SIGMOID SINUSES 67
F i g u re 6. Intraoperative fluoroscopy image with an angiocatheter (a r ro w) beingused to guide a microcatheter for coil embolization of the left transverse-sigmoidsinus (a r ro w h e a d) .
F i g u re 5. A , intraoperative photograph showing expo-s u re of the transverse and sigmoid sinuses and angio-catheter positioned in the transverse sinus dire c t e dt o w a rd the sigmoid sinus. B , line diagram of photo-graph depicting anatomic structures of the transversesinus, the left occipital cortex, and the cere b e l l u m .
retentionsutures
retentionsuture
retention suture
left transversesinus
left occipitallobe
MEDIAL
LATERAL
left cerebellum
angiocatheter
B
A

NEUROSURGICAL OPERATIVE ATLAS. VOL. 868
The patient re t u rned 6 months later with completeresolution of her symptoms, and a follow-up angio-gram (Figure 7) demonstrated no residual fistula.
CONCLUSIONSDural arteriovenous fistulas of the transverse-sig-moid sinus can be very complex to treat and re q u i re a clear understanding of the arterial supply, nidus lo-cation, venous drainage, and location of the vein ofLabbé. These lesions can present with a wide varietyof symptoms and may pose a significant risk to thepatient. The venous drainage is the most importantfactor in assessing the risk of stroke and hemor-
rhage. Depending on the angioarc h i t e c t u re of theD A V F ,a treatment regimen can be developed which may in-clude conservative therapy, transarterial emboliza-tion, transvenous embolization, surgical resection, ora combination of the above. These lesions can only bec u red by occlusion of the venous drainage. Based onthe fistula characteristics, this can be successfullyachieved by transvenous embolization, either perc u-taneously or after operative exposure, or surgical re-section. This approach to DAVFs re q u i res a combinede ffort from both the neuro s u rgical and neuro i n t e r-ventional services to provide each patient with thebest treatment possible.
F i g u re 7. Postoperative angiogram, lateral projection, ofthe left common carotid artery injection with no evidenceof residual DAV F.

INTRODUCTIONDural arteriovenous malformations (DAVMs) of theanterior fossa are a rare subgroup of malform a t i o n sthat have been only sporadically reported. They ac-count for only 10% of all DAVMs and are distin-guished by their high incidence of hemorrhage andunusual anatomy. Lesions associated with the duralconvexity and superior sagittal sinus are also un-usual, comprising approximately 5% to 10% ofD AVMs. Nevertheless, these DAVMs are quite inter-esting in that they are distinguished by their high in-cidence of hemorrhage, which is in contrast to theindolent symptomatology associated with the morecommon lesions involving the cavernous, transverse,and sigmoid sinuses. The pertinent micro s u rg i c a lanatomy and operative treatment of anterior fossaand superior sagittal sinus DAVMs are reviewed inthis chapter.
NORMAL ANATOMYThe anterior fossa dura receives its blood supply fro mboth the internal and the external carotid arteries. Inmost cases, the internal carotid artery supplies theanterior fossa dura through branches of the oph-thalmic artery. The ophthalmic artery usually arisesf rom the supraclinoid portion of the internal caro t i d
O P E R ATIVE MANAGEMENT OF ANTERIOR FOSSA,
SUPERIOR SAGITTAL SINUS, AND CONVEXITY DURAL
A RTERIOVENOUS MALFORMAT I O N SAMAN B. PATEL, M.D.WESLEY A. KING, M.D.NEIL A. MARTIN, M.D.
69
siphon and passes through the optic canal inferior tothe optic nerve. After entering the orbit, it gives off asmall branch, the re c u r rent meningeal artery, whichruns back into the middle fossa through the lateralpart of the superior orbital fissure and may anasto-mose with branches from the middle meningealartery. The intraorbital ophthalmic artery also giveso ff anterior and posterior ethmoidal arteries in theregion of the ethmoidal air cells. The posterior eth-moidal artery, the smaller of the two branches, sup-plies the basal dura in the region of the planum sphe-noidale, while the anterior ethmoidal artery serves asthe principal branch to the dura of the antero m e d i a lanterior fossa floor. The anterior ethmoidal arteryalso gives rise to the anterior falx branch that sup-plies the falx cerebri. After the anterior falx branch,the anterior ethmoidal artery perforates the cribri-f o rm plate, and its branches course along the ante-rior cranial fossa floor and ascend in the falx cere b r i .In some cases, the anterior meningeal branches ofthe anterior ethmoidal artery supply a large portion ofthe dura of the frontal convexity as well (Figure 1).
The principal external carotid arterial supply tothe anterior fossa dura comes from the middle men-ingeal branches, which is also the predominant sup-ply to the frontal convexity dura. These branchesmay then anastomose with meningeal branches ofthe ophthalmic artery. Four sites of anastomosis ex-ist between the ophthalmic artery and meningealbranches of the external carotid artery: 1) thro u g hthe re c u r rent meningeal branch; 2) through men-ingeal branches of the posterior ethmoidal artery; 3)© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 870
t h rough the anterior falx branch of the anterior eth-moidal artery; and 4) through meningeal branches ofthe anterior ethmoidal artery. These collateral ro u t e scan become prominent in pathological conditionssuch as meningiomas, DAVMs, and internal caro t i dartery occlusion. In addition, the external caro t i dartery can contribute blood supply through transcal-varial branches of the superficial temporal artery andt h rough branches of the internal maxillary artery( F i g u re 1).
Arterial supply to the dura of the superior sagittalsinus and convexity is primarily from branches ofthe external carotid artery. The most pro m i n e n tbranches that supply this site are the middle men-ingeal, superficial temporal, internal maxillary, andoccipital arteries. The latter three supply the duravia transosseous perforations. Less commonly, thereis supply from the anterior falcine branch of the oph-thalmic artery or the posterior meningeal branch ofthe vertebral artery.
Radiographic Feature sIn most cases, an intracranial hemorrhage can beseen on computed tomography (CT). Bleeding iseither intraparenchymal, subarachnoid, or a combi-nation of the two. In this way, the behavior of aD AVM mimics that of a pure pial AVM. Most fre-quently, intraparenchymal bleeding is massive andlocated in the anteromedial aspect of the frontal lobe.Subarachnoid hemorrhage is most often seen in thei n t e rhemispheric fissure. Enlarged veins or varicesmay be demonstrated on contrast-enhanced CT. Inaddition to demonstrating acute or subacute intrapa-renchymal or subarachnoid hemorrhage, magneticresonance imaging (MRI) without contrast enhance-ment may reveal the draining vein at the floor of theanterior cranial fossa as a flow void, especially in thec o ronal projection. The presence of venous ectasia orvarices may be confirmed.
Anterior fossa DAVMs almost universally involvethe dura in the region of the cribriform plate and the
F i g u re 1. N o rmal anatomy of the blood supply to the anterior fossa dura. Thefour sites of anastomosis between the ophthalmic artery and meningeal branchesof the external carotid are depicted. 1 = Middle meningeal artery to re c u r re n tmeningeal artery; 2 = middle meningeal artery to meningeal branch of the poste-rior ethmoidal artery; 3 = middle meningeal artery to anterior falx branch of theanterior ethmoidal artery; 4 = middle meningeal artery to meningeal branch ofanterior ethmoidal artery.
mid. meningeal branches
ant. falx branch ant. ethmoidal a.
ant. meningeal branchesant. ethmoidal a.
ant. ethmoidal a.
post. ethmoidal a.
recurrent meningeal a.
ophthalmic a.
maxillary a.int. carotid a.
ext. carotid a.
1
2
3 4

PATEL ET AL : ANTERIOR FOSSA, SUPERIOR SAGITTAL SINUS, AND CONVEXITY DAVMS 71
anterior falx. Usually, a hypertrophied anterior eth-moidal artery supplies the lesion (Figure 2). The an-terior ethmoidal supply is bilateral in about one halfof cases. Additional blood supply can be obtainedf rom the posterior ethmoidal artery or the anteriorfalx artery. The external carotid artery may con-tribute additional feeders, supplying the DAV Mt h rough frontal branches of the superficial temporalartery (transosseous) and the anterior branches ofthe middle meningeal artery. Additionally, there maybe supply from the internal maxillary artery.
Anterior fossa DAVMs usually drain exclusivelyinto pial veins of the anterior frontal lobe, fro mwhich they empty into the superior sagittal sinus or,in rare cases, subfrontally into the cavernous sinus.In patients with hemorrhage from anterior cranialfossa DAVMs, cerebral angiography consistentlydemonstrates focal aneurysmal dilatation of thevenous channel (venous aneurysm or varix) near thesite of the dural-to-pial anastomosis. Such a varix
has been described in approximately 90% of cases ofanterior fossa DAVM and appears to be the source ofh e m o r rhage. When an aneurysm is not present, thelesion more frequently causes insidious nonhemor-rhagic symptoms or is an incidental finding.
D AVMs of the superior sagittal sinus are mostoften located in the middle and posterior thirds of thesinus and are supplied by hypertrophied branches ofthe external carotid artery. Enlarged middle menin-geal arteries and veins may lead to prominent duralg rooves on plain skull radiography. In patients with along history of hyperemia, thickening and sclerosis ofthe overlying bone may be found. CT may also showassociated bony thickening, sclerosis, and enlarg e ddural grooves. However, CT is most useful for detect-ing hemorrhagic complications (e.g., intrapare n c h y-mal, intraventricular, or subarachnoid) and associ-ated hydrocephalus from prior hemorrhage ori n c reased intracranial pre s s u re (ICP). Contrast en-hancement is useful to demonstrate the enlarg e d
F i g u re 2. Anterior fossa DAVM is demonstrated in the region of the cribriformplate and the anterior falx. The lesion shows a hypertrophied anterior ethmoidalartery with a fistulous connection to leptomeningeal veins. This connection isdilated into a varix, which is usually the source of hemorrhage. The goal of opera-tive treatment is to divide this fistulous connection.
falx
AVM
ethmoidal branches
ophthalmic a.

draining vein and varices. In cases of thrombosis ofthe superior sagittal sinus, contrast enhancementmay demonstrate the so-called “empty delta sign,” inwhich a triangular area of non-enhancement is seenwithin the sinus, corresponding to clot. MRI willdemonstrate acute and subacute intrapare n c h y m a l ,subarachnoid, and subdural hemorrhage, as well asthe flow voids of the enlarged draining veins. Associ-ated superior sagittal sinus venous thrombosis mayalso be detected. Contrast enhancement may demon-strate the nidus within the leaves of the sinus, con-f i rm sinus thrombosis, and further enhance the pialvenous drainage.
C e rebral angiography reveals that the primarypedicles supplying superior sagittal sinus and con-vexity DAVMs are the middle meningeal arteries. Ad-ditionally, other branches of the external caro t i dartery, namely the superficial temporal and occipitalarteries, may supply these lesions through trans-osseous perforations. It is important to carefully eval-uate both external carotid arteries, since DAVMs inthis location not uncommonly have bilateral symmet-ric blood supply. Less commonly, there is supplyf rom the anterior falcine branch of the ophthalmicartery or the posterior meningeal branch of the verte-bral artery. The most posterior DAVMs may derivesome blood from the meningohypophyseal trunkt h rough the arteries of Bernasconi and Casaneri. Pialcortical contributions from branches of the anteriorc e rebral, middle cerebral, or posterior cerebral arter-ies may also supply the DAVM.
D AVMs may drain directly into the superior sagit-tal sinus, in which case hemorrhage is rare. Pialveins that normally connect with a dural sinus in-volved by a DAVM may also be recruited for venousdrainage. In these, due to shunting or to sinus occlu-sion, the high dural sinus pre s s u re causes re t ro-grade flow in the pial veins that normally drain intothe sinus. Dementia may be present if pre s s u rewithin the sinus is elevated in such a way as to pre-vent normal pial cerebral venous drainage. It is notuncommon to find DAVMs a distance away from thesuperior sagittal sinus because of drainage into cor-tical veins which may travel a variable path beforereconnecting with the superior sagittal sinus. Again,with DAVMs in this location, venous ectasias (or an-eurysms) may be seen; these are notoriously associ-ated with intracerebral hemorrh a g e .
INDICATIONS FOR TREATMENTOne of the most serious and urgent indications for
t reatment is the presence of a single cortical drainingvein that could rupture. This is especially true if itdrains a sinus that has a major obstruction, particu-larly if it is a sinus cut off from its normal drainagechannel. If there is dilatation of the draining vein (ve-nous aneurysm or varix), intervention becomes even
m o re urgent. Intracranial hemorrhage is serious andquite possibly is an indication for emergency tre a t-ment. Other indications for surgical treatment in-clude severe papilledema that threatens visual func-tion and local cortical dysfunction that may incre a s ewithout treatment. For example, a large accumula-tion of cortical veins over a silent area such as thef rontal lobe might in time cause serious functionali m p a i rment without giving adequate warning. Head-ache and bruit are symptoms that re q u i re individualjudgment re g a rding the circumstances of the partic-ular case. A serious headache may indicate an ele-vated ICP, or the headache itself may be intolerable( D AVMs cause more prominent headaches than cor-tical malformations). In addition, a continuous bruitcan be quite intolerable and may be an indication fors u rgical tre a t m e n t .
PREOPERATIVE PREPARATIONPatients presenting with intraparenchymal hemor-rhage should be given an anticonvulsant agent. Weuse Dilantin as the first drug of choice, with an intra-venous loading dose of 15 mg/kg, followed by amaintenance dose of 300 mg at bedtime. All patientsa re also given 10 mg Decadron on arrival to the oper-ating room, which is continued every 6 hours duringthe course of the operation. Intravenous antibiotics(1 gm Ancef and 80 mg gentamicin) are given on ar-rival and throughout the pro c e d u re and are contin-ued for 24 hours postoperatively. After the inductionof anesthesia and insertion of a catheter into theb l a d d e r, 100 gm of mannitol is given intravenously;10 to 20 mg furo s e m i d e can be given if additionalbrain relaxation is re q u i re d .
Anesthetic Te c h n i q u eIn most patients, there is a decrease in intravascularvolume immediately prior to intracranial surg e r y .T h e re f o re, the replacement of intravascular volumeby the intravenous administration of crystalloid orcolloid solution is indicated before the induction ofanesthesia. Minimal preoperative medication with abenzodiazepine eliminates the risk of narc o t i c - i n-duced obtundation, hypoventilation, and re s u l t a n tC O2 retention. Patients with altered levels of con-sciousness should not receive premedication. Moni-toring includes direct arterial pre s s u re, centralvenous pre s s u re, cardiac rate and rhythm by electro-c a rdiography, temperature, end-tidal CO2 and bloodoxygen saturation, urinary output, and interm i t t e n tm e a s u rement of arterial blood gases, hematocrit, se-rum electrolytes, and osmolality. A peripheral nervestimulator is used to measure the degree of musclerelaxation. Venous air embolism is detected by achange in the pre c o rdial ultrasonic Doppler signaland the presence of increased end-tidal nitrogen ord e c reased end-tidal CO2.
NEUROSURGICAL OPERATIVE ATLAS. VOL. 872

PATEL ET AL : ANTERIOR FOSSA, SUPERIOR SAGITTAL SINUS, AND CONVEXITY DAVMS 73
Anesthesia is induced with the intravenous ad-ministration of propofol or thiopental. Fentanyl (3 to6 µg/kg) or sufentanil (0.5 to 1 µg/kg) and vecuro-nium (0.1 mg/kg) or atracurium (0.5 mg/kg) areadded after controlled hyperventilation with 100%oxygen has been instituted. The larynx is intubatedafter intravenous lidocaine (1.5 mg/kg) and addi-tional thiopental (2 mg/kg) have been administere dto prevent systemic and intracranial hypertensionduring intubation. Anesthesia is maintained with thecontinuous administration of oxygen, nitrous oxideor air, low concentrations of isoflurane, and interm i t-tent doses or infusion of narcotic, muscle re l a x a n t ,and barbiturate or propofol. Ventilation is contro l l e dto keep the arterial pCO2 between 35 and 40 mm Hgb e f o re the skull is opened and between 25 and 30mm Hg after.
TREATMENT OF ANTERIOR FOSSA DAVMSGeneral ConsiderationsA number of therapeutic options are available fort reating DAVMs. These include conservative manage-ment, endovascular therapy, and surgical oblitera-tion. A complete review of the patient’s medical his-tory and careful examination of the angiographicrelationships are critical before initiating therapeuticintervention. In some cases symptomatic treatment isindicated, while in others palliation without completeobliteration of the DAVM is acceptable. Since anteriorfossa DAVMs have an extraordinarily high risk ofh e m o r rhage, conservative management is rarely indi-cated and complete obliteration should be the goal inmost patients. In cases of anterior fossa DAVM thathave supply from the external carotid branches, par-tial embolization may be feasible. However, the mainblood supply to anterior fossa DAVMs is from thei n t e rnal carotid artery through the ophthalmic arterybranches. Because of the difficulty of catheterizingthe ophthalmic artery and the significant risk ofvisual deficit from occlusion of this vessel or its re t i-nal branches, complete endovascular obliteration ofanterior fossa DAVMs seems impractical at the pre-sent time. The open surgical management of fistulasin this location is normally successful, and endovas-cular therapy probably has no role because of thehigh risk of occluding the central retinal artery.D i rect surgical intervention has been advocated foranterior fossa DAVMs and has been associated withexcellent results in experienced hands.
Operative Te c h n i q u eA unilateral low frontal craniotomy approach allowse x p o s u re to the region of dural pathology and is usu-ally undertaken from the side of maximal leptomen-ingeal venous drainage or from the nondominanth e m i s p h e re. A unilateral exposure allows transfal-
cine access for interruption of ipsilateral and contra-lateral leptomeningeal venous drainage. This is pre-f e r red over a bifrontal approach because it avoidsu n roofing of a potentially arterialized superior sagit-tal sinus. In addition, when approached via a lowf rontal craniotomy, minimal brain retraction is re-q u i red.
The patient is placed in the supine position withc a reful attention to padding of all pre s s u re points.The head is elevated, slightly extended, and held inthe vertical position with the skeletal-fixation head-rest. The extension of the head will facilitate re t r a c-tion of the frontal lobe. A radiolucent headrest maybe used if there may be a need for intraoperativea n g i o g r a p h y .
A skin incision is made just above the zygomaticp rocess behind the hairline and extending medially,ending at or just beyond the midline at the hairline( F i g u re 3). If the incision is too far forward or extendsbelow the zygomatic process, the frontal branch ofthe facial nerve may be injured. The skin, underlying
Figure 3. The skin incision, craniotomy, and dural open-ing for the operative approach to anterior fossa DAVMs.This is a unilateral low frontal craniotomy approach. Thepatient is placed in the supine position with the headmaintained in a vertical position and slightly extended.The skin incision is just behind the hairline and extendspast the midline to allow exposure farther anteriorly. Thecraniotomy is performed unilaterally to the superior sagit-tal sinus.
dural incision
osteotomy
incision

NEUROSURGICAL OPERATIVE ATLAS. VOL. 874
temporalis muscle, and the pericranial tissue aret u rned together, exposing the anterior and lateralinferior frontal and anterior temporal bone. A burrhole is placed just below the anterior end of thesuperior temporal line, which allows exposure of thefloor of the anterior fossa. Two additional burr holesmay be placed, one in the posterior frontal re g i o nand the other in the temporal region. A free bone flapis then turned. The bone flap should extend just offthe midline. The lateral portion of the sphenoid wingis removed using the drill. After drill holes are madea round the craniotomy opening, dural sutures areplaced to control epidural bleeding. The dura is thenopened over the inferior frontal and anterior tempo-ral regions. The frontal lobe is protected with Instatand is carefully elevated over the orbital roof withs e l f - retaining re t r a c t o r s .
If a large intracerebral hematoma is present, itshould be evacuated initially to allow safe re t r a c t i o nof the frontal pole. In most situations, the vascularm a l f o rmation consists of simple fistulous connec-tions between the dura and the pial veins without asignificant dural nidus (Figure 2). The most impor-tant step in surgery is occlusion of the vascular con-nection between the dura of the cribriform plate are aand the pial vessels. If the falx or the anterior fossadura is extensively involved by a nidus, which isr a re, it should be excised since residual DAVM cane n l a rge, recruit pial veins, and thus increase thechance of future hemorrhage. It is probably not nec-essary to excise the venous aneurysm from the cere-bral parenchyma because once the varix is discon-nected from the dura it will thrombose and involute.
C o m p l i c a t i o n sThe major potential complications include worseningof mental function due to frontal lobe retraction oranterior cerebral artery injury, cere b rospinal fluid(CSF) leak, anosmia, infection, and postoperatives e i z u re. Unilateral or bilateral anosmia is an expectedcomplication of this operation. If the frontal sinuswas entered on turning the bone flap it must be cra-nialized, the mucosa removed, packed with muscle orGelfoam, and sealed with a pericranial flap. If this isnot done, the patient will be at risk for the develop-ment of an intracranial infection. Any potential site ofCSF leakage, especially in the region of the cribriformplate, must be sealed. We use pericranium and mus-cle in addition to fibrin glue to seal potential sites ofCSF leakage.
TREATMENT OF SUPERIOR SAGITTALSINUS AND CONVEXITY DAVMSGeneral ConsiderationsD AVMs that involve the superior sagittal sinus or thedural convexity are associated with a variety ofanatomical configurations. There f o re, treatment op-
tions must be carefully considered and planned. Inaddition to the anatomical characteristics of theD AVM, the clinical status of the patient must betaken into account. In cases where the DAVM hasr u p t u red, operative treatment with or without pre o p-erative embolization must be considered. However,when the DAVM is discovered incidentally or sec-ondary to symptoms not related to hemorrhage, as t rong case can be made for palliative treatment top revent the possibility of hemorrhage. Palliative tre a t-ment can also be considered for medically unstablepatients or to prevent further bleeding in patientswho have hemorrhaged and who are not able to toler-ate an open surgical pro c e d u re. Embolization of theD AVM is generally the best option for palliation.
Operative Te c h n i q u eSuperior sagittal sinus DAVMs may be treated by acombination of embolization and surgery for com-plete extirpation. Preparatory embolization may min-imize the risk of scalp and dural bleeding duringoperative treatment of these DAVMs. The surg i c a lt reatment of superior sagittal sinus DAVMs is basedupon the venous flow pattern determined on pre o p-erative or intraoperative angiography.
To minimize venous congestion and edema, thehead is positioned so that the DAVM is uppermost inthe operative field and is held in skeletal fixation.With DAVMs of the convexity that can be visualizedon MRI or CT, the use of a frameless stereotactic sys-tem may aid in the positioning, minimal skin inci-sion, and subsequent craniotomy. The planned skinincision must allow for full exposure of the DAV M ,adequate removal of the dura surrounding the AV M ,and adequate access to any potential bleeding. Awide area of the head should be prepped and drapedso that the opening can be enlarged if necessary.Blood supply to the scalp flap must be adequate, anda wide enough base left to provide sufficient vascu-larization. The cosmetic result of the scar and boneflap should also be considere d .
For superior sagittal sinus DAVMs located anteriorto the coronal suture (anterior third of the superiorsagittal sinus), the patient is placed supine with thehead slightly extended (Figure 4). A bicoronal skinincision is used. The incision should be placed wellbehind the posterior limit of the DAVM. The tempo-ralis muscle can be left attached to the superior tem-poral line on both sides of the head. The pericraniumshould be left intact to serve as a dural substitute atthe end of the operation. For lesions in the middlet h i rd of the sagittal sinus, the patient is placed in asupine or semilateral position with the head elevatedso that the scalp over the center of the DAVM isu p p e rmost (Figure 5). A horseshoe-shaped incision,with the base broader than the apex, is made. Theapex of the flap must extend sufficiently far acro s s

PATEL ET AL : ANTERIOR FOSSA, SUPERIOR SAGITTAL SINUS, AND CONVEXITY DAVMS 75
F i g u re 4. Patient positioning, skin incision, andcraniotomy for DAVMs of the anterior third ofthe superior sagittal sinus. The patient is placedsupine with the head slightly extended. A bi-c o ronal skin incision is used.
F i g u re 5. Patient positioning, skin incision, andcraniotomy for DAVMs of the middle third of the superior sagittal sinus. The patient is placedsupine with the head elevated so that the scalpover the center of the DAVM is uppermost. Ahorseshoe-shaped incision is used.
AVM
incision
sup. sagittal sinus
incision
osteotomy
AVM

NEUROSURGICAL OPERATIVE ATLAS. VOL. 876
the midline to allow adequate bone removal on bothsides of the sagittal sinus. For DAVMs located in theposterior third of the sagittal sinus, the patient isplaced in the lateral position (Figure 6). The head iselevated and turned at least 45 degrees toward thefloor to bring the center of the DAVM to the highestpoint. The skin incision is horseshoe shaped, extendsabout 2 cm across the midline, and is based in the
posterior temporal-inferior occipital re g i o n .A free bone flap is raised and a sufficient number
of burr holes on either side of the sinus are made toallow easy stripping of the dura. A craniotome isused after the dura has been stripped. The duralstripping and bone cuts over the sinus are madelast, after all other burr holes have been connected( F i g u re 7). If the dura is densely adherent over the
F i g u re 7. Superior sagittal sinus DAVM following the craniotomy. Thisshows a malformation at the middle third of the superior sagittal sinus,with a nidus located over the sinus. The DAVM depicted here re c e i v e sblood supply from bilateral middle meningeal arteries.
F i g u re 6. Patient positioning, skin incision, and craniotomyfor DAVMs of the posterior third of the superior sagittalsinus. The patient is placed in the lateral position and thehead is well elevated and turned 45 degrees toward the floorto bring the center of the DAVM to the highest point. Theskin incision is horseshoe shaped.
osteotomy
incision
osteotomy
AVM
AVM
incision
sup. sagittal sinus

PATEL ET AL : ANTERIOR FOSSA, SUPERIOR SAGITTAL SINUS, AND CONVEXITY DAVMS 77
sinus, a free flap should be raised unilateral to thesinus, the dura should be stripped over the sinusunder direct vision, and a second free bone flapshould be raised across the midline. As the bone flapis elevated, Gelfoam and cottonoids are placed di-rectly over the sagittal sinus. Bleeding from the boneis controlled with bone wax, and dural bleeding isc o n t rolled with cautery, Gelfoam, and Surgicel. Thedura is then tacked up in the periphery by holesdrilled into the bone.
Paramedian lesions, which are occasionally asso-ciated with an occluded dural sinus and variceal oraneurysmal leptomeningeal venous structures, canbe treated by coagulation of the pathological duralleaflet and interruption of leptomeningeal arterial-ized venous drainage (Figure 8). If a fistula is locatedin the wall of the sinus and drains exclusivelyt h rough cortical veins, one should divide the attach-ment of the fistulous vein to the sinus. It is possibleto do this with impunity since cortical blood flow hasa l ready found collateral pathways. The wall of thesinus can thus be coagulated without entering thesinus lumen. If the nidus drains directly into thesinus, it is sufficient to interrupt the arterial supply
to the DAVM by coagulating and interrupting thefeeding vessels. This will decrease the venous hyper-tension within the superior sagittal sinus, which isthe main source of symptoms. If the sinus is notused as a primary outlet for the brain venousdrainage, it may be possible to excise the sinus andnot cause significant parenchymal venous hyperten-sion. This is most frequently encountered in the an-terior third of the sinus.
C o m p l i c a t i o n sPostoperative complications include venous air em-bolus, hemorrhage, increased neurological deficit,and wound infection. If an air embolus is detected bya reduction in end-tidal CO2 or if air is heard on thep re c o rdial Doppler, the patient’s head can be low-e red. Once the opening is covered and the vital signsa re stable, the patient can be re t u rned to the originalposition. CT visualizes the presence of a hematomaor increased cerebral edema. Increased cere b r a ledema can be treated with an increase in the stero i ddose and a prolonged steroid taper. As in anteriorfossa DAVMs, openings in the frontal sinus need to
F i g u re 8. Drawing showing the arterial supply to the superior sagittal sinusD AVM interrupted following coagulation. This opening of the dura and coagula-tion of vessels is done lateral to the sinus. In the figure depicted here, this wouldneed to be accomplished bilaterally secondary to the bilateral arterial supply.This is usually sufficient treatment for DAVMs that drain exclusively into thesinus, since the high-pre s s u re arterial flow into the superior sagittal sinus willbe interrupted. Leptomeningeal venous drainage, if present, can be interruptedwhen the dura is opened.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 878
be dealt with as described in the previous section.
GENERAL WOUND CLOSURE The dura can be closed primarily or by taking a pieceof pericranium and sewing it into the dural defect.For anterior fossa DAVMs, closure of the dura in theregion of the cribriform plate may be difficult. Thisa rea can be packed with muscle or pericranium andsubsequently sealed with fibrin glue. Central tack-upsites are drilled into the bone flap and tack-ups u t u res are placed partial thickness through thedura. The bone flap is replaced and held in placeusing miniplates, and mesh or burr-hole covers canbe used to cover large defects. The temporalis muscleis re a p p roximated using 3-0 Vicryl sutures in a sim-ple interrupted fashion. The galea is then closedusing 3-0 Vicryl sutures in an inverted interruptedfashion. The skin is closed using skin staples or 3-0nylon in a running interlocking pattern. The woundis then covered with a sterile dressing, and a pre s-s u re head wrap is placed.
IMMEDIATE POSTOPERATIVE MANAGEMENTAs the patient awakens from anesthesia, intravenousagents are used to control blood pre s s u re tightly. Aportable monitor is used to follow blood pre s s u re andheart rate as the patient is transported to the re c o v-ery room or intensive care unit (ICU). Close observa-tion in the ICU setting is indicated for at least the firstpostoperative night. Steroid doses are usually ta-p e red over 5 to 10 days, depending on the patient’sn e u rological status and the extent of cerebral edema.Antibiotics are continued for 24 hours. The length oftime for anticonvulsant medication has not beenestablished. If there is no history of seizures, anticon-vulsant medication can likely be stopped within 2 to3 months. If a seizure disorder has been pre s e n t ,anticonvulsants are continued for 6 months to a year,and further treatment is planned depending on elec-t roencephalographic findings. Prior to discharge fro mthe hospital, the patient should undergo cerebral an-giography to confirm the absence of residual DAV M .

INTRODUCTIONThe surgical treatment of skull base lesions is fre-quently limited because of extension of the tumorinto the bony, neural, and vascular structure sa round the skull base as well as by the presence ofcritical neurovascular structures surrounding orinvested by the lesion. These limitations have in partbeen overcome by the use of frameless stere o t a c t i csystems, such as the Operating Arm System (OAS)(Radionics, Inc., Burlington, MA). The OAS aids inthe preoperative planning of surgical approaches byallowing the surgeon to visualize the operative trajec-tory to a skull base lesion on the computer graphicworkstation. During surgery, the OAS allows then e u ro s u rgeon to visualize the anatomy along the tra-jectory to the lesion and delineate lesion boundaries,achieving a more complete resection, with potentiallyd e c reased morbidity.
BACKGROUNDThe OAS is an advanced neuro s u rgical instrumentused in the operating room for interactive, image-guided surgery. It provides precise, real-time local-ization of patient anatomy by displaying a point inthe surgical field on a preoperative image set, whichis viewed on a computer workstation in the operating
USE OF THE O P E R ATING ARM SYSTEM IN SKULL BASE SURGERY
JEFFREY J. LARSON, M.D.RONALD E. WARNICK, M.D.
JOHN M. TEW, JR., M.D.
79
room. Frameless stereotactic systems such as theOAS are powerful new tools for preoperative surg i c a lplanning and for interactive, frameless stere o t a c t i cnavigation.
The OAS includes an ergonomic digitized arm thatsenses the position of its probe tip and an integratedcomputer graphic workstation that stores andmanipulates imaging data. The system facilitatesplanning of the optimal surgical approach and, indoing so, plans the craniotomy trajectory. Durings u rgery, the OAS aids in navigating around criticalneural and vascular structures. This improved surg i-cal technique increases the safety, accuracy, ande fficiency of skull base surgery, reduces operatingtime, and may reduce complications from the oper-a t i o n .
PATIENT SELECTION The OAS is effective for cortical and subcorticallesions, skull base lesions, and deep-seated vascularlesions. The accuracy of the OAS ranges from 1 to 4mm, which suffices for most neuro s u rgical pro c e-d u res. However, target shifts resulting from intraop-erative tumor swelling, lesion debulking, re t r a c t i o n ,or cere b rospinal fluid (CSF) drainage can incre a s ethe erro r, limiting the usefulness of the OAS in defin-ing the margins of some intra-axial lesions. The OASis well suited for skull base lesions because targ e tshifts are usually not encountered when a lesion isa ffixed to the skull base.© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 880
F i g u re 1. A and B , f rontal (A) and lateral (B) views of the placement of four re f e rence fiducials on rigid areas of thef o rehead and one fiducial in the mastoid region respectively. C, the correct attachment of the Operating Arm Sys-tem to the Mayfield headholder and the optimum placement of the arm so as not to interf e re with access to thes u rgical target. The articulating operating arm should be tested for proper positioning before calibration to ensurep roper reach and probe trajectory. Dashed line indicates skin incision. (Reproduced with permission from theMayfield Clinic)
A
B
C

LARSON ET AL : THE OPERATING ARM SYSTEM IN SKULL BASE SURGERY 81
IMAGE SELECTIONComputed tomography (CT) or magnetic re s o n a n c eimaging (MRI) can be used for frameless stere o t a c t i cs u rgery. MRI is pre f e r red for skull base lesions whensuperior resolution of soft tissue is re q u i red. CT bonewindows are useful for visualizing skull base ap-p roaches that re q u i re extensive drilling in the tempo-ral bone, occipital condyles, or clivus, such as duringanterior or posterior petrosal approaches, far lateraltranscondylar approaches, and transoral, transmax-illary, or transsphenoidal appro a c h e s .
Application of Fiducial MarkersFiducial markers (Radionics, Inc.) are placed on thepatient’s head prior to imaging. For optimal perf o r-mance, four re f e rence fiducials are applied to rigida reas of the head (i.e., forehead and mastoids) wherescalp elasticity is minimal (Figure 1A and B). Thisapplication scheme forms a plane passing thro u g hthe target structure. It is not necessary to tailor thefiducial placement to account for location of the skinincision since stereotactic registration of the OAS isp e rf o rmed before surgery. The fiducials can be out-lined with a permanent marking pen to ensure accu-rate replacement in the event that a marker is inad-vertently removed, such as when the stere o t a c t i cimaging study is perf o rmed on an outpatient basisprior to hospital admission.
Skull Fixation and Operating Arm PlacementFrameless stereotaxy with the OAS re q u i res thre e -point skull fixation, as well as fixation of the operat-ing arm to the head holder. Care is taken duringskull fixation to minimize scalp and fiducial move-ment that would increase error during stere o t a c t i cregistration. The articulating operating arm shouldbe tested for reach and probe trajectory before re g i s-tration. The articulating arm must have freedom ofmovement to allow the probe tip to reach all fiducialsand also provide the desired trajectory to the lesion( F i g u re 1C).
S t e reotactic RegistrationS t e reotactic registration is obtained following fixationof the operating arm and skull. Imaging data andregistration are perf o rmed in the operating room andtake approximately 15 minutes. Following re g i s t r a-tion, the computer workstation calculates and dis-plays the registration erro r. Error of less than 3 mmis generally acceptable for skull base lesions. Thefiducials can be removed after registration so thatthey will not interf e re with the sterile preparation orskin incision.
PRESURGICAL PLANNINGThe OAS facilitates planning the surgical appro a c hto a skull base lesion by allowing the surgeon tovisualize trajectories to the boundaries of the lesionand directing the optimal surgical pathway. Thehand-held depth probe is a retractable calibratedp robe that allows the surgeon to “scan” into thedepths of a patient’s anatomy before making an inci-sion and compare various approaches to a lesion( F i g u re 2).
OPERATIVE PROCEDUREThe OAS can be used at all stages of surgery, includ-ing skin incision, craniotomy, intraoperative naviga-tion and localization, and lesion re s e c t i o n .
Skin IncisionSkin incisions are minimized with the OAS becausethe incision is placed precisely over the desired cra-niotomy site. Smaller skin incisions are cosmeticallym o re appealing and, when the scalp and muscle dissection is minimized, can result in less postopera-tive pain.
C r a n i o t o m yUsing the OAS, the craniotomy is customized to pro-vide a corridor to the skull base lesion. The OASdepth probe is indispensable in showing the lesion in relation to a proposed craniotomy. Additionally,
F i g u re 2. The Operating Arm System depth probe shown fully expanded ( A ) and fully contracted ( B ).
A B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 882
underlying critical structures and landmarks areidentified with the depth probe (rather than withtopographical landmarks, which can be inconsistent)during placement of the burr holes and craniotomy.For example, when basing a craniotomy on the sig-moid sinus-transverse sinus junction for a suboccip-ital or posterior petrosal exposure, the depth pro b eidentifies the exact position of the sinuses, allowingfor the safe and accurate positioning of the burrholes and craniotomy and eliminating the search foraccurate topographical landmarks (Figure 3).
During anterior approaches to the skull base, theOAS shows the corridor to a clival or upper cervicallesion. This allows for maximum exposure through a transoral, transmaxillary, or transsphenoidal ap-p roach. The lesion is surveyed with the depth pro b eb e f o re soft-tissue dissection. This interactive pre s u r-gical planning helps determine the extent of the
opening re q u i red (i.e., inclusion of a transmandibularor transpalatal approach) and maximizes exposure tothis region (Figure 4).
During transsphenoidal surgery, the OAS helpsidentify the midline of the sella and the medial extentof the internal carotid artery in the cavernous sinus( F i g u re 5). The sella opening is configured to the spe-cific anatomy of the lesion.
Intraoperative Navigation and Lesion ResectionThe boundaries of a skull base lesion are easilydetected using the OAS. This is especially helpfulwhen anatomical landmarks are not clearly visible orwhen the lesion is invested in critical structures. Forexample, tumor extensions are difficult to identifyintraoperatively because they frequently involve theforamina, fissures, and dural folds of the skull base
F i g u re 3. Illustration of the depth probe identifying the transverse and sigmoid sinusesb e f o re craniotomy (dashed line). (Reproduced with permission from the Mayfield Clinic)
sigmoid sinus
asterion
transversesinus

LARSON ET AL : THE OPERATING ARM SYSTEM IN SKULL BASE SURGERY 83
F i g u re 4. Operating room setup for usingthe Le Fort approach to a clival chord o m a .A , depth probe passing through the pre-sumed transoral opening. B , c o m p u t e rs c reen of the Operating Arm System show-ing the location of the tip of the depthp robe ( g reen circ l e ) in relation to the targ e t .
F i g u re 5. Computer screen of the OperatingA rm System used to identify the location of thei n t e rnal carotid artery in a patient with a clivalgiant cell tumor. G reen circ l e indicates locationof the probe tip.
A
B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 884
( F i g u re 6A). Using the operating arm probe, the neu-ro s u rgeon can more completely resect a tumor byidentifying extensions of skull base tumor intraoper-atively (Figure 6B and C).
Brainstem lesions are visualized with the OAS be-f o re opening the surface of the brainstem (Figure 7).This technique minimizes morbidity to cranial nervenuclei often related to resecting brainstem lesionsthat do not extend to the surface of the brainstem.
The OAS can be used to stereotactically guide sur-gical instruments, such as endoscopes, into ventri-cles or cysts, making the OAS an important navi-gational tool in the operating room for re a l - t i m einteractive surg e r y .
CAUTIONSAs with any frameless stereotactic system, errors canoccur while using the OAS during image acquisition,s t e reotactic registration, and intraoperative naviga-tion. The accuracy of the operating arm is 1 to 4 mm.
E r rors during image acquisition are due to patientmovement. Thin-slice, fast-acquisition images mini-mize the error associated with patient movement and
i m p rove the resolution. Errors during stere o t a c t i cregistration occur when diff e rent parts of a fiduciala re selected on the computer workstation and thescalp. Fiducials that have recognizable parts on boththe fiducial itself and the image of the fiducial on the computer workstation decrease selection erro r.Scalp elasticity increases error by displacing thefiducials. Care must be taken to avoid scalp move-ment when placing the head in three-point fixation.E r ror during intraoperative navigation results fro mt a rget shifts during surgery. Ta rget shifts are re-duced by avoiding hyperventilation, osmotic diure-sis, CSF, and brain retraction. Ta rget shifts are lessof a problem for skull base lesions because the le-sions are often fixed to the skull base.
CONCLUSIONThe OAS is a useful adjunct to skull base surgery. Al-though frameless stereotactic technology has not ob-viated the need for high-level surgical skills and com-p rehension of the complex anatomy of the skull base,it does provide useful information that can be incor-porated when perf o rming a skull base pro c e d u re .
F i g u re 6. Patient with a tentorial meningioma with dural tail. A , p reoperative MRI. B , p o s t o p-erative MRI demonstrating complete resection. C , intraoperative view of the computer scre e nfor the Operating Arm System showing the dural tail ( g reen circ l e ).
A B

LARSON ET AL : THE OPERATING ARM SYSTEM IN SKULL BASE SURGERY 85
C
F i g u re 7. Illustration indicating placement of the depth probe to identify the brainstemlesion and location of the cranial nerve nuclei before opening the floor of the fourth ventri-cle. (Reproduced with permission from the Mayfield Clinic)
F i g u re 6C.
motor nucleus Vnucleus VI
nucleus VII
obex


INTRODUCTIONThe orbitocranial zygomatic approach re p resents amodification of the classical pterional approach to thep re-pontine cistern that allows maximal exposure ofthe region of interest. This approach takes advantageof removal and/or relocation of soft tissue and boneto maximize the viewing and working area while min-imizing the overall working distance. While the over-all dimensions of the pre-pontine space (upper basi-lar trunk) are fixed by the inherent spatial anatomy,the overall surface area of exposure is enhanced uti-lizing this cranial base approach (Figure 1).
PATIENT POSITIONINGAll surgical approaches begin with patient fixationand positioning. Lesions of the pre-pontine cistern s ,being deep and constrained, re q u i re three-point pinfixation of the head for maximum stability. Thre e -point pin fixation is carried out in such a fashion as to place all pins behind the ears. This allows for maximum soft-tissue mobilization and minimal
THE ORBITOCRANIAL Z Y G O M ATIC APPROACH TO
A N E U RYSMS OF THE UPPER BASILAR TRUNK
T.C. ORIGITANO, M.D., PH.D., F.A.C.S.
87
© 1999 The American Association of Neurological Surg e o n s
The orbitocranial zygomatic approach con-sists of the following sequential steps:1 . Skin incision, which preserves the temporalis
fascia and pericranium.2 . Intra- or transfacial management of the tempo-
ralis fascia to preserve the frontalis branch ofthe facial nerve.
3 . A tailored zygomatic osteotomy.4 . The rotational removal of the temporalis
muscle out of the temporal fossa.5 . A pterional-based craniotomy.6 . A tailored supraorbital osteotomy.7 . A tailored orbital osteotomy.8 . A tailored extradural removal of portions of the
g reater and lesser wings of the sphenoid,exposing the superior orbital fissure .
9 . A low, wide-perimeter dural opening withdural pleating.
1 0 . Mandatory micro s u rgical dissection of the sylvian fissure .
1 1 . Optional extradural removal of the anterior clinoid pro c e s s .
1 2 . Optional intradural removal of the posteriorclinoid pro c e s s .
1 3 . Optional extradural entry into the posteriorfossa through Kawase’s triangle.
1 4 . Optional mobilization of the third nerve bytentorial re l e a s e .
1 5 . Optional tentorial splitting.

i n t e rf e rence of pin(s) to the operator’s hands; in ad-dition, the transition of instruments between sur-geon and nurse and, when necessary, assistant’s aidis facilitated. Treatment with a pentobarbital bolusprior to pin placement will diminish the patient’sphysiological response to pin placement. Head posi-tioning re q u i res three degrees of freedom of move-ment: rotation, approximately 30 degrees from theneutral position, and extension 15 to 20 degrees withneutral head tilt. The ability to rotate the table side-to-side during the operative pro c e d u re greatly en-hances the surgeon’s operative flexibility. Prior to pinfixation, a lumbar spinal drain is placed to be uti-lized if necessary. Care should be taken not to sub-stitute spinal drainage for microdissection to gainoperating space. Spinal drainage should re m a i nclosed during the extradural drilling so that the cere-b rospinal fluid (CSF) can act as a buffer for the brainagainst inadvertent dural contact. Also, overd r a i n a g eof CSF collapses the cisterns, making their dissec-tion more diff i c u l t .
ELEVATION OF SCALP FLAPThe skin incision is marked out behind the hairline,starting in front of the tragus of the ear, running alongthe hairline to the contralateral temporal line. First,lidocaine with epinephrine is injected. The initial inci-sion is made down to, but not including, the tempo-ralis fascia or pericranium. Scissors are utilized top rotect the underlying soft tissue. Skin clips areapplied for additional hemostasis. Attempts should bemade to preserve, in continuity, the frontal branch ofthe superficial temporal artery. Anterior and posteriorskin flaps are raised. The anterior flap is raised to thelevel of the keyhole. At this point, a curvilinear cut inthe temporalis fascia is made through both the super-ficial and the deep temporalis fascia. A cut is startedjust behind the keyhole down to the muscle. Scissorsa re placed over the muscle, and the fascia is cut to theroot of the zygomatic process of the temporal bone.Two veins are encountered during the transaction,which should be anticipated and controlled with bipo-lar cautery. The temporalis fascia, both superf i c i a land deep with the fat pad in between, is elevated offthe muscle to the level of the zygoma. At the zygomathe fascia splits, with the superficial fascia and fatpad going superficial to the bone and the re m a i n i n gfascia deep to it. Splitting the fascia is accomplishedby gentle dissection with a periosteal elevator startingat the root(s) of the zygomatic process of both the tem-poral bone and the frontal bone and moving to thezygoma. Once accomplished, the frontal branch of thefacial nerve is safely protected and the re s u l t i n gmaneuver exposes the bone from the root of the zygo-matic process of the frontal bone to the zygomaticp rocess of the temporal bone.
The pericranial flap is now harvested by re a c h i n g
4 to 6 cm behind the posterior flap and cutting fro mthe temporal line to the temporal line with a unipolarcautery. The flap is now elevated with further cuttingalong both temporal lines. Care should be taken notto tear the tissue, especially where it is most adher-ent at the coronal suture. As the flap is elevated tothe level of the supraorbital rims, care is taken tofind and preserve the supraorbital neuro v a s c u l a rbundle. It may be in a notch or a true foramen. Aforamen can be converted to a notch by utilizing a 1-to 2-mm Kerrison to open the foramen or by drillingc i rc u m f e rentially around the foramen. The neuro-vascular bundle is then brought forward with thepericranial sheet graft. Further forward mobilizationof all planes of the soft tissue anterior flap occurs byreleasing the periorbitum from the superior and lat-eral orbital walls, utilizing a combination of #1 and#4 Penfield dissectors. At this point, the anterior flapis well away and below the bone. These maneuversflatten the exposure, thereby beginning the pro c e s sof bringing the surgeon closer to the target (Figure 2).
ELEVATION OF BONE FLAPThe zygomatic osteotomies are now made. These cutsa re oriented to maximize the area for temporal mus-cle displacement. The first osteotomy is made parallelto the zygomatic process of the frontal bone using theposterior bony rim as a cutting guide. A brain spatulashould be passed under the zygoma to protect themuscle. The second osteotomy at the temporal ro o tmust be made diagonally to reflect the arc h i t e c t u re ofthe bony attachment. Again, the muscle below is pro-tected by a brain spatula. The zygoma itself can beleft attached to the muscle on its underside.
At this point, the temporalis muscle is takendown. A variety of techniques can be used dependingon how reattachment along the temporal line isplanned. Generally, a cut is made 1 cm below andparallel to the temporal line to the coronal suture .This will leave a cuff of tissue for re a p p ro x i m a t i n gduring reconstruction. A second cut is made perpen-dicular to the temporal line from behind the pterionto the base of the zygoma. The anterior border of thetemporalis muscle is not attached to the bone. Mobi-lization of the inferior border of the temporalis musclenow occurs. A large diploic vein is encountered in theregion of the keyhole. This must be controlled withbone wax packing. The temporal muscle is folded in-feriorly over the cut zygoma. Bleeding on the backwall of the muscle should be controlled with pre c i s ebipolar cautery. Dissection is taken down to justbelow the original level of the zygoma. Great caremust be taken to obtain and maintain hemostasis toavoid postoperative discoloration down into the neck.Remember that the only remaining blood supply tothe temporalis muscle at this point is from its deeparterial supply. Reckless use of cautery can result in
NEUROSURGICAL OPERATIVE ATLAS. VOL. 888

ORIGITANO : ORBITOCRANIAL ZYGOMATIC APPROACH TO UPPER BASILAR TRUNK ANEURYSMS 89
F i g u re 1. I n c reased viewand working space aff o rd e dby orbitocranial zygomatica p p roach. The surface are aviewed is enhanced and theworking distance shortenedwith multiple operative corri-dors (purple = classical pteri-onal approach; blue = orbito-cranial zygomatic appro a c h ) .
F i g u re 2. Initial soft tissue transfers and bonework begin the process of widening and flatten-ing the operative approach. Care is taken to pre-serve the neurovascular bundle of the pericranialflap and mobilization of the temporalis fascia top reserve the facial nerve.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 890
a dead temporalis muscle. Mobilization of the tempo-ralis muscle in this fashion again leads to a flatteroperative site. Bony exposure places the surgeon inf ront of and below the temporal lobe.
C r a n i o t o m yA pterional craniotomy is now perf o rmed (Figure 3).Burr holes are placed: 1) at the base of the zygomaticp rocess of the temporal bone, providing access to thefloor of the middle temporal fossa; 2) behind the pte-rion; 3) at the keyhole (giving access to the anteriorcranial fossa and orbit); and 4) just behind theorbital ridge medial to the temporal line. The dura isstripped off the bone with a #3 Penfield dissector.The burr holes are connected with a craniotome,raising a free bone flap. Dural bleeding is contro l l e dwith bipolar cautery. The frontal and temporal lobedura are now elevated off their respective bones. Arongeur is utilized to remove the bone from aro u n dthe temporal tip, exposing the dura over the tempo-ral lobe superolaterally from temporal pole to root ofthe zygoma. Elevation of the temporal dura anteri-orly would allow exposure of the V2 and V3 ro o t s .Gentle dissection of the periorbitum from the supe-rior and lateral orbital walls is now undertaken. Uti-lizing a fine cutting blade or re c i p rocating saw, theorbital osteotomies are perf o rmed, protecting thedura and periorbitum with soft, malleable re t r a c t o r sunder direct visualization. The extent of the supraor-bital osteotomy is tailored to the size of the lesion.Often only a superolateral, supraorbital osteotomy isnecessary, sparing entry into the frontal sinus. Like-wise, the extent of the lateral orbital cut can be mod-ified. With removal of the supra- and lateral orbitalridges, the periorbitum is further dissected free ofthe superior and lateral orbital walls, which can thenbe removed as a single piece with a drill or piecemealwith microdissection back to the base of the anteriorclinoid process. Occasionally, a robust anterior cli-noid process can project into and limit the oculo-c a rotid triangle. With prepontine lesions, the clinoidp rocess can be safely removed extradurally. A sec-ond benefit to removing the anterior clinoid pro c e s sand opening the optic canal is the ability to intradu-rally mobilize both the ipsilateral optic nerve and thec a rotid artery, increasing their mobility and thusopening both the opticocarotid and the oculocaro t i dcorridors to the basilar tip. At this point, great caremust be taken to ensure hemostasis of all dural andbony surfaces to avoid continued bleeding during theintradural dissection, which can be a nuisance.
Opening of the DuraThe dura is now opened. To protect the brain duringbone work, the spinal drain has not been opened tothis point. The drain remains closed to keep the cis-t e rns and sylvian fissure expanded during the initial
m i c ro s u rgical dissection.The dural opening starts low across the fro n t a l
lobe, approximately 1 cm above the floor of the ante-rior fossa, and proceeds down into the sylvian fis-s u re. This maneuver allows the frontal lobe dura tobe pleated back on itself and tacked to the pericra-nium, compressing the orbit. Tacking the dura flati n c reases the flatness of the approach while decre a s-ing the necessity for retraction and CSF diversion.The dura is then cut around the front and side of thetemporal lobe, again tenting over the adjacent softtissue covered by Oxycel, further flattening the ap-p roach and improving hemostasis. A final cut up thesylvian fissure completes the dural opening. At thispoint, the entire temporal lobe from tip to the root ofthe zygoma is exposed, with visualization of the su-p e r i o r, middle, and inferior temporal gyri (Figure 4A).
THE ORBITAL ZYGOMATIC APPROACHThe microscope is now brought onto the field; underm i c roscopic magnification and illumination, the syl-vian fissure is opened. Again, it is important to notopen the CSF drain at this point. This keeps the fis-s u re and cisterns expanded with CSF and easier todissect. Following Ya s a rgil’s technique, the fissure isdissected by opening the arachnoid and dissectingdown to the artery; using the gentle opening pre s s u reof the bipolar cautery to dissect, the arachnoid isopened deep to superficial. Sharp dissection withscissors is used for the most superficial arachnoid, ifnecessary. Furtherm o re, it is suggested that no re-tractors be placed at this time. While use of re t r a c t o r smay be tempting, they tend to immobilize the brainand limit the freedom and visualization of dissection.T h e re is also great potential risk of over- re t r a c t i o nleading to brain injury in a still tethered brain.M i c rodissection is carried down to the carotid cistern ,which is opened. The optic nerve is freed from thef rontal lobe, and the A1 segment is untethered. Dis-section is now directed toward releasing the uncusand opening the space lateral to the carotid artery.The posterior communicating artery is freed and thet h i rd nerve is identified and freed as it enters the ten-torial edge. At this point, the temporal lobe has beenreleased circ u m f e rentially. If necessary for maximalworking space, the veins entering the sphenoparietalsinus are bipolar coagulated and cut. The temporallobe can now be mobilized up and out of the middlecranial fossa and held by a small amount of tractionvia a brain blade. The diff e rence between traction andretraction is not a matter of mere semantics. I defineretraction as the application of a pulling force againstthe brain. Traction, on the other hand, simply con-tours an object in place without significant pullingf o rce. With complete microdissection of the sylvianf i s s u re, the brain blade can be placed to position thee n t i re temporal lobe in space. The blade is brought in

ORIGITANO : ORBITOCRANIAL ZYGOMATIC APPROACH TO UPPER BASILAR TRUNK ANEURYSMS 91
F i g u re 3. Bone work. A , p t e r i o n a lcraniotomy, tailored orbital osteot-omy, and tailored zygomatic os-teotomy. B , removal of the superiorand lateral orbital walls perm i t t i n gan unobstructed view to the tentor-ial edge.
F i g u re 4. A , with soft tissue transfer and bony removal, a wide view of the temporal lobe and fro n t a l / s u b-f rontal region is possible. The dura is opened as demonstrated by the dotted lineand tented back against thesoft tissue with some compression of the periorbitum. B , the view down the orbitocranial zygomatica p p roach with its fullest exposure. The temporal lobe being freed from the middle cranial fossa is positionedup and out. The third nerve is the pathway to the brainstem and the basilar artery. Mobilization of thec a rotid artery and optic nerve can enhance the operative space.
B
A
B
A

anteriorly to the temporal tip and slightly medially.The untethered temporal lobe will assume a positionallowing a corridor for visualization and work of ap-p roximately 4 to 5 cm (Figure 4B).
The head and microscope are now positioned tobring the third nerve into the middle of the field. Uti-lizing micro s u rgical dissection, the arachnoid alongthe nerve is cut and the nerve is followed back to thebrainstem. The third nerve acts as an approach vec-tor to the basilar artery. The basilar, superior cere b e l-l a r, and posterior cerebral arteries can all be identi-fied. The posterior communicating artery is followedalong its entire course with great care to preserve allof its perforators. The posterior clinoid process isidentified just medial to the third nerve. At this point,one has proximal control of the basilar artery. Dissec-tion is carried along the posterior cerebral artery tothe basilar junction (and aneurysm). By rotating thetable, a more subtemporal view is obtained and dis-section of the back wall and perforators is perf o rm e d .Rotation of the scope allows a view through the optic-o c a rotid and oculocarotid triangles for visualization
of the contralateral posterior cerebral artery. The ap-p roach thus maximizes the viewing angles and opera-tive corridors, minimizing the limitations of the tradi-tional approaches (Figure 5).
ADJUNCTS TO THE APPROACHA number of adjuncts can be applied to cope withvariations in aneurysm size, geometry, and positionalong the clivus. At times, the perforators off the pos-terior communicating artery, in combination with af o reshortened length, can hinder advancement of theclip. Injury of a posterior communicating artery per-forator should not be taken lightly as it can lead toh e m i p a resis. Transection of the posterior communi-cating artery at its most proximal perforator (as re-lated to the carotid artery) will allow the entire com-plex to be rotated back out of harm’s way. Thisp e rmits further mobilization of a now laterally un-t e t h e red carotid artery, expanding the oculocaro t i dt r i a n g l e .
At times, with a low-riding basilar artery, the pos-
NEUROSURGICAL OPERATIVE ATLAS. VOL. 892
F i g u re 5. Operative view through the orbitocranial zygomatic approach to the upper basilar trunk and bifurc a t i o n .

ORIGITANO : ORBITOCRANIAL ZYGOMATIC APPROACH TO UPPER BASILAR TRUNK ANEURYSMS 93
terior clinoid artery can become an obstacle, espe-cially with re g a rd to clip trajectory. With the middlecranial fossa empty, drilling of the posterior clinoidbecomes less onerous as it allows for the use ofshorter drills as the hand is brought closer to thet a rget. The dura over the posterosuperior aspect isbipolarly cut and gently dissected forward, exposingseveral millimeters of the bone, which can then bedrilled. Overzealous takedown of the bone or duracan lead to cavernous sinus bleeding, which can berobust. Bleeding is generally controlled by packingwith a hemostatic agent, which can lead to a gre a t e robstruction than the primary anatomy. Generally, nom o re than 3 to 5 mm of bone needs to be exposedand drilled. Great care must be taken not to injurethe third nerve during the drilling pro c e s s .
For low-lying aneurysms or large aneurysms thatre q u i re lower basilar artery control, the third nervecan be mobilized and the tentorium split. The thirdnerve is visualized entering the tentorium. With theaid of a scythe blade or a #11 bladed knife, the duraover the course of the third nerve is opened for ap-p roximately 1 cm. Care is taken to stay directly overthe nerve while transecting the dura. Again, entryinto the cavernous sinus can occur and should bec o n t rolled with minimal packing with a hemostaticagent and pre s s u re with a cottonoid patty. The thirdnerve may now be mobilized forward or back. Thetentorium is then split behind the third nerve, takingc a re not to injure the fourth nerve which is situatedbehind it. To avoid injury, the fourth nerve must beidentified prior to this maneuver and its trajectoryp rojected. The tentorial edges can then be tentedback with 6-0 retention sutures to give a V- s h a p e dcorridor to the basilar artery.
A more sophisticated adjunct to expose the basi-lar trunk is the anterior petrosectomy, or the Kawasea p p roach. This extradural approach relies on theidentification of key temporal bone anatomy and re-q u i res an intimate knowledge of the temporal boneanatomy; it is not for the uninitiated. Complicationsf rom this approach can include carotid artery injury,deafness, and facial paralysis. The reader is re f e r re dto the works of Kawase for a detailed description. Afull description is beyond the scope of this chapterand is mentioned here for completeness.
Radiological adjuncts to basilar artery surg e r yinclude intraoperative balloon proximal control andangiography and preoperative computed tomography(CT) angiography. Preoperative CT angiography isp e rf o rmed utilizing spiral CT with venous injection.Data collection takes approximately 60 seconds withre f o rmat times of 5 to 10 minutes. Studies can bere f o rmatted in: 1) simultaneous axial, coronal, andsagittal planes with point-to-point tracking; 2) multi-planar volume rendering; and 3) thre e - d i m e n s i o n a l
rendering. The vessels of interest can be followedwith a cursor along their route and cro s s - re f e re n c e din all three planes. The precise anatomical re l a t i o n-ship of the aneurysm geometry and spatial orienta-tion to its osseous environment are well visualized.Calcification of the neck can be readily identified.Most importantly, aneurysm neck geometry can bere n d e red from multiple views including inside of thea n e u r y s m .
Intraoperative angiography may be critical forl a rge and giant basilar apex aneurysms to assuremajor vessel patency (particularly contralateral pos-terior cerebral and superior cerebellar arteries) andaneurysm obliteration. Remember that perf o r a t o rvessel integrity is beyond angiographic resolution andmust be assured by careful postclipping inspection.To assure intraoperative angiography when needed,we place the catheter in the parent artery of intere s tp reoperatively with a slow heparin drip through thec a t h e t e r. In our series of 100 intraoperative angio-grams, constituting 425 injections, we have experi-enced one embolic event utilizing this protocol. Key toassuring obliteration is to take multiple views, re p ro-ducing those views that best demonstrate the lesionp reoperatively.
Intraoperative balloon proximal control can alsobe of help in dealing with large and giant basilarapex lesions. This maneuver avoids placement of ap roximal clip, which can obscure visualization ofcritical structures. Retrograde suction can collapseor at least soften the aneurysm, allowing for finaldissection and clip application. Even with pro x i m a lendovascular control, the surgeon is encouraged, ifpossible, to pre p a re for proximal clip control shouldthe balloon fail. Retrograde suction can lead to larg evolumes of blood loss if the collateral anterior circ u-lation is robust. Utilization of a cell-saver to re c o n s t i-tute the blood volume should be considered.
This approach and adjuncts can be utilized toreach aneurysms of the basilar apex, P1 and P2 seg-ments of the posterior cerebral artery, and the supe-rior cerebellar artery. Aneurysms below the upperone third (midbasilar) of the basilar artery are bettera p p roached petrosally. Occasionally, a very low-lyingshort basilar artery exists with an apex aneurysmwhose dome is at or below the posterior clinoid ar-tery. These lie anatomically in the midbasilar re g i o nand should be approached petro s a l l y .
Manipulation of the third nerve will lead to palsy,with the patient generally recovering over 4 to 6weeks. The surgeon should be pre p a red for the pre s-ence of a unilateral dilated pupil in the re c o v e r yroom. Generally, this can be determined clinically.CT can confirm if there is any doubt. Intraoperativeangiography usually relieves the surgeon of a vascu-lar catastrophe in these cases.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 894
WOUND CLOSURE AND COMPLICATIONSWound closure begins with opening the lamina term i-nalis. This may aid in reducing the incidence of post-operative hydrocephalus in a patient with subar-achnoid hemorrhage. The brain blade is re m o v e d .Generally, the view without the blade is adequate( F i g u re 5). It should be stressed that the blade needonly be placed for the moments before and duringclipping when a static field is re q u i red. Generally, Ip e rf o rm a duraplasty with a generous piece of peri-cranium to provide nonconstricting dural closure .Just prior to closure, the intradural space is filledwith warm saline to check for a watertight closureand to evacuate air. If the frontal sinus was entere d ,the mucosa is cauterized and the sinus packed withan antibiotic-soaked hemostatic agent. A small pieceof temporalis muscle is then packed into the openinginto the sinus. Epidural tenting sutures are placedc i rc u m f e rentially over the hemostatic agent alongwith a central tenting suture. The pericranial flap isthen pulled over the sinus opening packed with mus-cle and sutured to the dura. A sheet of bacteriostatichemostatic agent is cut and placed over the superiorand lateral orbital bone defect prior to tacking downthe pericranium. If the sinus is not entered, the peri-cranium is laid back down in its anatomical position.The supraorbital bone is now re a p p roximated to thepterional free flap by a microplate and screws on theunderside. This construct is re a p p roximated to thecranium with microplates and screws. It is possibleto plate with all plates hidden by the temporalis mus-cle. If further cosmesis is re q u i red, hydro x y a p a t i t ebone cement can be used to fill the bone cuts, burrholes, and temporal craniectomy site. If used, onemust have the strictest hemostasis, leave the are awell drained, and allow the material to set before con-tinuing the closure (20 to 40 minutes). The tempo-ralis muscle is now brought back into its anatomicallocation. Care should be taken to secure it high abovethe keyhole to avoid a cosmetic defect. A wire - p a s s e rdrill hole at the junction of the zygomatic process ofthe frontal bone and supraorbital ridge can facilitatethis maneuver. If possible, the temporalis fasciashould be re a p p roximated anatomically. The zygomais now reattached with a microplate and screws. Wi t h
reattachment, care should be taken not to constrictthe base of the temporalis muscle; this now re p re-sents the primary blood supply of the muscle. Post-operative swelling against a constricting zygoma canlead to loss of the temporalis muscle.
Critical inspection of the skin flaps is now under-taken with a goal of maximum hemostasis. A drain isplaced under the posterior skin flap, using gre n a d esuction, not as a substitute for hemostasis but to en-courage obliteration of the large subgaleal deadspace. A galeal closure of inverted suture is placed,followed by skin staples. Blood loss for this exposure(excluding re t rograde suction or aneurysm rupture )is estimated to be approximately 100 to 150 cc. Thespinal drain is removed prior to extubation, and thesubgaleal drain is removed in 24 to 48 hours. If thereis no facial nerve function, re t u rn is generally seen in1 to 6 weeks; however, it may be hard to determ i n eimmediately postoperatively. Any forehead and scalpnumbness noted by the patient should resolve and isa result of manipulating the supraorbital neuro v a s-cular bundle. Eye swelling and ecchymosis are rare ifthe periorbitum has not been violated. It either oc-curs, an ice bag to the eye appears to control anddiminish the consequences.
Because of the lower, wider, flatter operative field,the surgeon will find that long-bayoneted instru-ments are cumbersome and no longer necessary. Am i x t u re of short-bayoneted and straight bipolars ofvariable lengths can now accommodate the dissec-tion. With experience, the additional osteotomies willadd approximately 20 minutes to the approach andc l o s u re times.
CONCLUSIONIt is always asked, “Is all of this necessary? Ya s a rg i lnever did this. Drake never did this. Sugita never didthis.” Which one of us is a Ya s a rgil, Drake, or Sugita?
The concepts and techniques in this chapter arenot my own but ones that have been learned from themaster surgeons willing to share with their students.I humbly acknowledge and am grateful to Drs. GaziYa s a rgil, Ossama Al-Mefty, and Evandro DeOliveirafor sharing their experience and wisdom.

INTRODUCTIONNeurinomas arising from the trigeminal nerve arer a re tumors that occupy the cavernous sinus andparasellar regions. These tumors typically cause avariable degree of trigeminal dysfunction and some-times diplopia. This condition necessitates surg i c a lintervention. No benefit has been demonstrated byother therapies, including radiosurg e r y .
These tumors are divided into four types andclassification is by their location. The first two typesa re not addressed in this chapter. The first type in-cludes tumors arising from the trigeminal nerveroot, contained within the posterior fossa. These arebest approached via a re t rosigmoid approach. A sec-ond type of tumor, the “dumbbell” type, spans theposterior and middle fossas. These masses involveboth the nerve root and the ganglion, and, whenvery large, may extend peripherally. This tumor re-q u i res a combined petrosal type of strategy and isnot addressed here .
This chapter is concerned with the surgical tre a t-ment of the ganglion and peripheral types of neuri-nomas of the trigeminal nerve. The large majority ofganglion-type tumors may be approached via an
EXTRADURAL APPROACHES FOR RESECTION OF
TRIGEMINAL NEURINOMASJ. DIAZ DAY, M.D.
95
e n t i rely extradural temporopolar approach. Gangliontumors located laterally may also be approached viaan extradural subtemporal transpetrosal appro a c h .Peripheral neurinomas are handled by one of theseextradural strategies or by a variation. The key con-cept is that these two types of neurinomas are lo-cated extradurally and that a contemporary cranialbase strategy can result in total resection with lowm o r b i d i t y .
An important consideration in the surgical ap-p roach to these tumors is determining an appro p r i-ate surgical strategy for extradural bone re m o v a l .The preoperative imaging studies must be care f u l l yreviewed to determine the exact location of the mass.The necessary degree and locations of extraduralbone removal are then determined for the individualpatient. In the case of a ganglion tumor, for example,a lateral location will not necessitate removal of theanterior clinoid process and decompression of theoptic canal (Figure 1A-C). Also, laterally located tu-mors approached via an extradural subtemporalt r a n s p e t rosal approach may not re q u i re full petro u sapex removal for adequate exposure (Figure 1D-H).This is mainly determined by the size of the tumorand the presence of any inferior extension of tumore roding the petrous bone or involving the caro t i dcanal. Anterior and medially located tumors may notre q u i re unroofing of the foramen ovale or ro t u n d u mfor adequate exposure of the tumor (Figure 1I). Thesetumors may be approached adequately by unro o f i n g© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 896
F i g u re 1. A, illustration of an anterolaterally located ganglion tumor. B, axial MRI of a small ganglion tumor that would not re q u i re opticcanal unroofing and anterior clinoid resection. C, c o ronal view of thesame neurinoma. D, illustration of a laterally positioned neurinoma ap-p roached via an extradural subtemporal approach. E, axial MRI of asmall lateral trigeminal neurinoma.
A B
C D
E

DAY : EXTRADURAL APPROACHES FOR RESECTION OF TRIGEMINAL NEURINOMAS 97
H
GF
F i g u re 1. F, intraoperative photograph of an exposed pigmented neurinoma located between V2 andV3. (Photo courtesy of T. Fukushima, M.D.) G, e x p o s u re following removal of a well-encapsulatedt u m o r. H, pigmented trigeminal neurinoma. I, anterior and medially located tumor not re q u i r i n gu n roofing of foramen rotundum or ovale. J, extensive tumor requiring global exposure of the cav-e rnous sinus.
J
I

NEUROSURGICAL OPERATIVE ATLAS. VOL. 898
the optic canal, the superior orbital fissure, and thea n t e romedial triangle via removal of the anterior cli-noid process. Large tumors involving the entire cav-e rnous sinus region will re q u i re a global strategy ino rder to optimize extradural bone removal (Figure1J). This process of strategy development is impor-tant so as to limit potential morbidity to the pericav-e rnous structure s .
PREOPERATIVE PREPARATIONThe patient’s medical history is obtained and adetailed neurological examination completed. In par-t i c u l a r, trigeminal nerve function is carefully testedand documented. All sensory modalities are testedand the intensity of sensation as compared to a nor-mal area is graded using a 10-point scale. This isimportant in terms of determining postoperativei m p rovement in sensory function. The corneal re-flexes are tested with a cotton wisp. Patients withany sign of keratitis are re f e r red to an ophthalmolo-gist for consultation.
The majority of patients will be re f e r red with adiagnostic imaging study, typically magnetic re s o-nance imaging (MRI). Patients in whom the anteriort r a n s p e t rosal approach is indicated will underg oimaging work-up supplemented by a fine-cut bonewindow computed tomography scan. Particular at-tention is directed toward the relationship betweenthe cochlea, the internal auditory canal, and thec a rotid canal in interpreting this study. Measure-ments may be taken from the images to provide thes u rgeon with an accurate concept of the operativewindow that will be created through petrous apexremoval. This study is also important in cases whereframeless stereotaxis will be used as an adjunct.
Patients undergo the usual preoperative labora-tory blood work, electro c a rdiogram, and chest x-ray.Medical clearance is obtained when warranted byany chronic medical conditions such as diabetes orhypertension. Patients are administered anticonvul-sant medication in the operating room, typicallydiphenylhydantoin at a dose of 10 mg/kg. For ashort period, the patient receives a maintenancedose of 3-5 mg/kg/day. In the majority of casesinvolving an entirely extradural surgery, anticonvul-sant prophylaxis is stopped on the seventh to 10thpostoperative day if the patient has not had anys e i z u res. All patients are given antibiotics periopera-tively. A broad-spectrum cephalosporin is used inthe majority of cases. Vancomycin is given to pa-tients who have exhibited an allergy to penicillin andits derivatives.
ANESTHETIC TECHNIQUEPatients are administered general anesthesia viainhalation agents. All patients have a radial arterialline placed to monitor blood pre s s u re. In addition
to two larg e - b o re intravenous lines, some patients re-q u i re central venous access. Preferably, this is placedin the subclavian vein.
Several maneuvers are important in terms of man-aging the intracranial pre s s u re during the pro c e d u re .Selected patients undergoing an anterior transpet-rosal approach have a lumbar drain inserted fordrainage of cere b rospinal fluid during retraction ofthe temporal lobe. This is especially important in theolder patient who may not tolerate any degree of tem-poral lobe retraction. In the younger patient in whomt h e re is usually an adequate degree of cerebral com-pliance, I do not insert a drain. The end-tidal CO2 i sm o n i t o red and maintained between 25 and 30 mmHg. Furosemide, 10-20 mg, and mannitol, 25 gm/kg,a re also administered intravenously at the time ofcutting the cranial bone flap to initiate a diure s i s .These maneuvers are directed at providing a compli-ant brain, although it will be retracted only sparinglyand under the protection of the overlying dura.
When perf o rming the anterior transpetrosal ap-p roach, facial nerve monitoring is a useful adjunct.The nerve monitor is utilized to assist with identifyingthe geniculate ganglion when located deep to thebone. Otherwise, no specific neurophysiological mon-itoring modality is of particular benefit in these cases.
THE EXTRADURAL FRONTOTEMPORALTEMPOROPOLAR APPROACHOperative PositioningThe patient is placed supine on the operating tableand the table is “couched,” elevating the back and theknees. All bony prominences are well padded withfoam. Sequential compression boots are placed onthe patient’s legs and the device is activated. Thehead is placed in the Mayfield three-pin headre s twith the two-pin side on the side of the appro a c h ,which is the dependent side. The single pin arm isplaced in the area of the midpupillary line on the con-tralateral side, within the hairline. The head is turn e da p p roximately 45 degrees toward the opposite shoul-d e r. The vertex is placed in the neutral position.D ropping the vertex of the head in these pro c e d u re sis not suggested, as this is an operation where thes u rgeon is looking down onto the middle fossa andc a v e rnous sinus areas. The head is draped in theusual fashion for a frontotemporal craniotomy.
P ro c e d u reThe scalp incision is made beginning just anterior tothe tragus of the ear, over the root of the zygomaticp rocess. The incision continues superiorly, within thehairline, gently curving to end at the midline (Figure2). Scalp clips are applied to the margins of the scalp,incorporating galea, for hemostasis. The galeocuta-neous flap is then elevated, utilizing an interf a s c i a l

DAY : EXTRADURAL APPROACHES FOR RESECTION OF TRIGEMINAL NEURINOMAS 99
dissection over the temporalis muscle. This will re s u l tin rotating the temporalis muscle and fascia inferiorlyand posteriorly, clearing out the frontozygomatic re-cess and providing a wide, flat access to the middlefossa. The galea is separated from the pericraniummedial to the superior temporal line, taking care top reserve the supraorbital nerves with the galeal layer.At the superior temporal line, the fascia innominata(loose connective tissue between the temporalis fasciaand the galea) is incised from its connection to themedial pericranium. This fascia is then elevated withthe galeal layer, leaving bare temporalis fascia. Thismaneuver places the surgeon in the correct plane toseparate the superficial and deep components of thetemporal fat pad. The superficial fat pad layer con-tains the frontalis branches of the facial nerve, whicha re protected when this maneuver is properly per-f o rmed. Scalp elevation proceeds until the supra-orbital and lateral orbital rims are exposed, covere dby the periosteum. Inferiorly, the periosteum over thezygomatic arch is exposed. The scalp is held withl a rge blunt scalp hooks and rubber bands.
A vascularized pericranial flap is preserved, incis-ing along the margin of the scalp incision and thesuperior temporal line. The flap is then raised viasubperiosteal dissection and wrapped in moist gauze.The pericranial flap is held anterior with the scalp flapusing large blunt scalp hooks. This may be used laterfor dural repair or coverage of an opened air sinus.
The temporalis fascia is separated at the superiortemporal line using a sharp instrument. Periosteum
over the lateral orbital rim and zygomatic arch isincised next, such as to leave a cuff of tissue for laterreattachment. The periosteum is then elevated to-w a rd the temporalis muscle, freeing the fascia of itsanterior and inferior attachment. The temporalismuscle is then elevated from the fro n t o z y g o m a t i crecess and the temporal squama via subperiostealdissection. This is done “cold” in order to avoid dam-age to the neural or vascular supply to the muscle;the result will be superior cosmetic outcome withoutloss of muscle bulk and tone. The muscle is held in-feriorly and posteriorly using large blunt hooks.
The frontotemporal craniotomy is then cut usinga high-speed drill. Burr holes are placed over thepterion and in the low temporal region. The cra-niotomy is roughly centered one third above and twot h i rds below the superior temporal line. The boneflap typically measures roughly 6 × 4 cm. After re-moval of the flap, hemostasis is secured and theposterior dural margins are tacked up to the bonem a rgin with fine suture. The dura is elevated awayat the anterior temporal margin with a dissector,and any remaining bone overhanging the middlefossa is ro n g e u red away.
Extradural removal of bone at the anterior andtemporal base is the next step in the pro c e d u re, andis perf o rmed with a high-speed drill. The dura is ele-vated away from the sphenoid ridge, and self-re t a i n-ing retractor blades are placed to hold it away (Figure3). The sphenoid ridge is reduced until a smooth con-tour of the superior and lateral orbit is created. The
F i g u re 2. The extradural frontotemporal temporopolar approach. The patient is positioned withthe head turned approximately 45 degrees (A). The scalp incision and craniotomy are similar tothat of a routine pterional-type appro a c h ( B ) .
A B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8100
F i g u re 4. The defining maneuver of theextradural approach for neurinomas is separation of the lateral wall of the cavern o u ss i n u s .
F i g u re 5. Tumor is exposed and resected uti-lizing the various entry corridors to the cav-e rnous sinus.
F i g u re 3. Elevation of the dura exposes theneural foramina at the middle fossa base and the superior orbital fissure .

DAY : EXTRADURAL APPROACHES FOR RESECTION OF TRIGEMINAL NEURINOMAS 101
bone of the middle fossa is shaved down toward theperiosteum forming the roof of the infratemporalfossa, leaving the outer cortical table intact wherepossible. The dura is further elevated toward the tem-poral base to expose the superior orbital fissure, fora-men rotundum, and foramen ovale. From this pointof the pro c e d u re, the structures exposed via boneremoval are tailored specifically to what is re q u i re dby the anatomy of the individual lesion being tre a t e d(as outlined above in the Introduction). At a mini-mum, bone must be removed over the superior orbi-tal fissure, foramen rotundum, and foramen ovale. Inselected cases, the anterior clinoid process will be re-moved and the optic canal unro o f e d .
Beginning at the superior orbital fissure, the cleav-age plane between the temporal dura propria andperiorbital fascia is separated using sharp dissectiontechnique. A retractor blade is placed over the tempo-ral pole and pre s s u re is directed in the posterior di-rection. This cleavage plane is developed and openedover V2, V3, and the ganglion. At this point of dissec-tion, the tumor becomes readily evident. Usually,trigeminal nerve fibers are spread and flattened overthe capsule of the tumor. Separation of the dura pro-pria from the connective tissue covering of the nerve(i.e., the outer cavernous membrane) continues to-w a rd the incisural edge. This is the defining man-euver of the extradural approach to these tumors( F i g u re 4). The tumor and the cavernous sinus areexposed without opening the dura and exposing theunderlying temporal lobe (Figure 5). Additionally, thetemporal tip bridging veins are left undisturbed.
Resection of the tumor now proceeds utilizing thevarious triangular entry corridors to the cavern o u ssinus. The routes accessible by this approach are thea n t e romedial, anterolateral, far lateral, postero l a t-eral, lateral, superior, and medial. Typically, the an-t e rolateral, far lateral, and lateral triangles will be themost frequently employed for ganglion tumors. Stan-d a rd principles of tumor resection are used in thesep ro c e d u res. The tumor capsule is identified andopened, usually exposed via the anterolateral or farlateral triangle. Sometimes, fibers of the trigeminalnerve are separated to expose the capsule. Afteropening the capsule, generous internal debulking isp e rf o rmed. This can be adequately perf o rmed withsharp dissection techniques and the use of micro -ring curettes. After internal debulking, the planebetween the trigeminal nerve and tumor capsule isdeveloped with sharp microdissectors, first workingwithin one triangular corridor. This same maneuveris then perf o rmed in the various triangular entry cor-ridors used, pushing tumor and capsule toward theprimary entry corridor with soft cottonoid patties.Any cavernous bleeding is controlled with Surg i c e lpacking. Usually, cavernous sinus bleeding is notparticularly problematic in these cases.
Wound ClosureAfter tumor resection, the wound is closed. The pri-mary goal of closure in this approach is re c o n s t r u c-tion of the skull base. Any openings made in thedura must be reconstructed in watertight fashion.Usually, adipose and fascial grafts are not necessary.H o w e v e r, pro c e d u res in which an air sinus has beenopened through the course of extradural bone re-moval will re q u i re adipose and fascial grafting foradequate closure. Any opened air sinus must be ex-enterated of its mucosa and packed with fat or mus-cle to prevent infection and mucocele formation. Thebone flap is then re a p p roximated with stainless steelw i re or titanium microplates for best cosmesis.
THE EXTRADURAL SUBTEMPORALTRANSPETROSAL APPROACHOperative PositioningThe patient is positioned with the head in a lateralorientation (Figure 6). The head is placed in the May-field three-pin headrest with the two-pin side strad-dling the subocciput. The single pin arm is placedwithin the hairline, near the midline. Prior to turn i n gthe head, the mobility of the patient’s neck shouldhave been tested to determine the degree of re s i s-tance to turning the head 90 degrees. If significantresistance is encountered, a roll is placed under theshoulder to reduce strain on the neck and minimizethe chances of vertebral artery occlusion. In somecases, especially an elderly patient, the lateral posi-tion is re q u i red so that no strain is placed upon thecervical spine.
Monitoring of the facial nerve is employed ro u-tinely in this pro c e d u re because of the risk to thefacial nerve during dural elevation, through possibletraction on the greater superficial petrosal nerve(GSPN). The monitor is useful in locating the positionof the geniculate ganglion and confirming the in-tegrity of the GSPN on the floor of the middle fossa.
P ro c e d u rePrior to scalp incision, external landmarks are iden-tified. The root of the zygomatic process is palpated,and the tragus of the ear located. The third impor-tant surface landmark for planning is the superiortemporal line. Two diff e rent incisions may be utilizedfor this approach. The choice depends upon the nec-essary size of the craniotomy. For most small lesionsof the ganglion or V3 peripheral branch, a straightincision with a small anterior curve is adequate. Theincision begins just anterior to the tragus of the earat the inferior margin of the zygomatic root. Thescalp is incised straight superiorly, curving slightlyanteriorly as the superior temporal line is neare d .Scalp clips are applied to the wound edges for hemo-stasis. The temporalis fascia and muscle are then in-cised with unipolar cautery along the line of the

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8102
scalp incision. The muscle is cleared away from theroot of the zygoma and pulled anteriorly. The tempo-ralis muscle is held anterior and posterior with bluntscalp hooks.
When a larger craniotomy is necessary, a questionmark-shaped incision is made (Figure 6). The inci-sion extends superiorly to the level of the superiortemporal line. After applying scalp clips to the galeo-cutaneous margins, the scalp is elevated from thetemporalis fascia. This re q u i res an interfascial dis-section, splitting the superficial and deep compo-nents of the temporal fat pad in order to protect thef rontalis branches of the facial nerve. The key to thisdissection is identification of the loose areolar layerof connective tissue, called the fascia innominata,between the galea and the temporalis fascia. The fas-cia innominata is elevated with the galea, openingthe appropriate dissection plane to split the compo-nents of the fat pad. The temporalis fascia and mus-cle are then incised in the line of the scalp incisionwith unipolar cautery. The muscle is then elevatedvia subperiosteal dissection from the temporalsquama and elevated anteriorly, held by blunt scalphooks. Again, it is important to free the muscle fro mthe zygomatic root and pull it anteriorly to maximizee x p o s u re .
A temporal craniotomy is then cut, centered twot h i rds anterior and one third posterior to the exter-nal auditory canal. The craniotomy needs to mea-s u re no more than approximately 4 × 4 cm. A high-speed drill is then used to reduce any re m a i n i n g
bony overhang of the middle fossa floor. A flat view-ing angle across the floor is necessary in terms oflimiting temporal lobe retraction.
The dura is elevated from the middle fossa floorwith a fine dissector, beginning over the petro u sridge (Figure 7). Initiating dural elevation posteriorlyis important in terms of avoiding traction on theGSPN, which may lead to postoperative facial nervedysfunction. The dura is elevated medially until thelateral margin of the trigeminal impression isexposed. Elevation in the anterior direction sepa-rates the dura propria from the periosteum coveringthe GSPN, lying in the major petrosal groove. Eleva-tion continues anteriorly until the middle meningealartery is exposed at the foramen spinosum. Theartery is coagulated and divided. The dura is furtherelevated to expose the foramen ovale and V3. Tw ot a p e red self-retaining retractor blades are thenplaced on the dura over the temporal lobe.
The cleavage plane between the temporal durap ropria and the connective tissue sheath over V3 isnext identified and developed sharply. The dura pro-pria is separated from V3 and the lateral portion ofthe gasserian ganglion, similar to the temporo p o l a ra p p roach (Figure 8). This maneuver exposes the tri-geminal fibers stretched over the tumor mass. Insome cases, removal of bone at the petrous apex maybe necessary for full exposure and removal of thet u m o r.
To safely remove the bone of the petrous apex viathe extradural route, sequential dissection of the
A B
F i g u re 6. The extradural subtemporal transpetrosal approach. The patient’s head ispositioned laterally ( A ) . The incision and craniotomy are shown ( B ) .

DAY : EXTRADURAL APPROACHES FOR RESECTION OF TRIGEMINAL NEURINOMAS 103
F i g u re 7. Elevation of the middle fossadura exposes key landmarks of the mid-dle fossa floor.
F i g u re 8. Separation of the dura pro p r i af rom the outer cavernous membrane pro-vides exposure of the posterolateral cav-e rnous sinus. The exposure is now ade-quate for petrous apex removal, if indicated.
F i g u re 9. P e t rous apex removal in-c reases exposure into the posterior cav-e rnous sinus, down to the clivus andentrance of the sixth cranial nerve intoD o rello’s canal.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8104
middle fossa floor is critical (Figure 9). It is helpful toconsider the key landmarks of the middle fossa flooras a guide to bone removal. Four landmarks outlinethe rhomboid-shaped volume of bone which maythen be removed and which is devoid of neural orvascular structures. These landmarks are: 1) theGSPN-V3 junction, 2) the porus trigeminus, 3) thea rcuate eminence-petrous ridge junction, and 4) thejunction of the axes of the GSPN and the arcuate emi-nence. Obliquely projecting this rh o m b o i d - s h a p e dcomplex through the bone toward the clivus delimitsthe volume of bone removed to the level of the inferiorp e t rosal sinus. Radical petrous apex removal is sel-dom re q u i red in these patients, and the appro a c hmust be tailored for the individual patient.
To begin, the intrapetrous carotid artery is ex-posed by unroofing the carotid canal in Glasscock’striangle. This triangle is defined by the foramenovale, the cochlea, and the V3 origin. It is easiest tobegin drilling near V3, just anterior to the GSPN. Theartery is followed laterally until the crossing point ofthe tensor tympani muscle is identified. This marksthe genu of the petrous carotid artery. Next, the in-t e rnal auditory canal is unroofed. This is done byfirst drilling near the petrous ridge over the bisectionaxis of the angle between the GSPN and the arc u a t eeminence. This axis is roughly 60 degrees fro meither the GSPN or the superior semicircular canal.With the internal auditory canal and the petro u sc a rotid exposed, the bone between these two struc-t u res may then be quickly removed with the drill.The majority of this bone is vascular cancellous bonethat can be easily drilled away. The bone under thegasserian ganglion may also be removed by thinningwith the drill followed by removal using a dissector.
The tumor is then resected by utilizing the lateraltriangular entry corridors to the cavernous sinus.Most typical via this approach are the far lateral,p o s t e rolateral, and posteromedial triangles. Thesame principles apply as for the temporopolar ap-p roach, outlined above.
This approach is typically perf o rmed without anydural disruption. In some cases, the posterior fossasubarachnoid space will come into communicationwith the extradural space as a consequence of tumorresection near the trigeminal root in Meckel’s cave.This circumstance re q u i res exclusion of the sub-arachnoid space from communication with the mid-dle fossa. Two methods for closure are possible. Myp re f e r red method is placement of a pedicled tempo-ralis muscle flap into the defect. This flap is takenf rom the posterior to the middle section of the tem-poralis muscle. This tends to heal very well due tothe vascularized nature of the flap. An altern a t i v emethod is to place a free adipose graft in the defect.Typically, this is harvested from the abdomen. Thebone flap is then replaced and the wound closed.
COMPLICATIONSCertain complications are common after resection oftrigeminal neurinomas. Certainly, deficits of the fifthcranial nerve may be expected in the early postopera-tive period. Most patients present with some dysfunc-tion of the trigeminal nerve, whether it be hypesthe-sia or pain. Many patients will have some re s o l u t i o nor a diminution of their hypesthesia. Patients withpain as a presenting complaint are typically re l i e v e d .A large number of patients suffer trigeminal motordysfunction after resection. This is less common inpatients with small, medially situated ganglion tu-mors and those with peripheral lesions of V1 and V2.Because of the high risk of motor dysfunction, ther a re patient with bilateral tumors is treated only onthe side producing the bulk of symptoms. The oppo-site side must be managed expectantly and may onlybe treatable by radiation therapy.
P robably the most troublesome complication fro mremoval of these tumors is keratitis suff e red as aconsequence of a diminished corneal reflex. How-e v e r, most patients will present with a diminishedc o rneal reflex. There f o re, eye care is extremely im-portant beginning at the time of pre s e n t a t i o n .
Diplopia is also a frequent presenting complaintthat may or may not be helped by surgery. Certainly,any operation in or around the cavernous sinus hasthe potential to injure the ocular motor nerves.Diplopia may be a consequence of surgical re s e c t i o n ,although this is uncommon. Careful dissection of thetumor capsule while limiting manipulation of thesenerves is the key to reducing the chances of thisc o m p l i c a t i o n .
When utilizing the extradural subtemporal trans-p e t rosal approach, the seventh and eighth cranialnerves are especially at risk. The seventh nerve inparticular may be damaged via traction on theGSPN, which translates to the geniculate ganglion,damaging the nerve. Elevating the dura posteriorly toanteriorly will reduce the chance of this complica-tion. Also, the seventh and eighth nerves are at riskduring unroofing of the internal auditory canal. Thecochlea may also be damaged during this drilling.Avoidance of this structure is achieved by observingthe anatomical relationship of the cochlea to thelandmark structures. The cochlea resides in the vol-ume of bone located under the geniculate ganglion,between the internal auditory canal and the genu of the petrous carotid artery. This may also be de-scribed by the “premeatal” triangle, defined by thec a rotid genu, the geniculate ganglion, and the mediallip of the porus acusticus. Of course, practice in thecadaver laboratory and clinical experience are keyfactors in avoiding the cochlea during drilling.
Other structures at risk from the high-speed drilla re the optic nerve, the carotid artery, the oculomo-tor nerve, and the trigeminal peripheral branches.

DAY : EXTRADURAL APPROACHES FOR RESECTION OF TRIGEMINAL NEURINOMAS 105
All structures are at risk both from direct damage bythe burr and from the heat generated by using a dia-mond-tipped burr. Such complex bone removal mustbe done carefully after sufficient training in thecadaver laboratory to reduce complications. Also, alldrilling is perf o rmed with strict attention to main-taining a cool local environment with continuousi r r i g a t i o n .
CONCLUSIONSTrigeminal neurinomas are rare tumors treated pri-
marily with surgical resection. In the vast majority ofcases, tumors classified as ganglion or peripheraltypes may be treated through an entirely extradurala p p roach. The two main extradural approaches forthese tumors have been presented. It should be keptin mind that each approach is tailored according tothe individual anatomy of the tumor in terms of thenecessary extradural bone removal. When success-fully employed, these approaches result in a highrate of success with re g a rd to tumor resection andresolution of symptoms.


INTRODUCTIONSchwannomas arising from the trigeminal nerve arequite uncommon and re p resent only 0.2% of allintracranial tumors. Although 50% of intracranial tri-geminal schwannomas arise from the trigeminal gan-glion, schwannomas can arise from any part of thetrigeminal nerve, including its origin in the posteriorfossa, and extend to the extracranial branches on theface. Approximately 20% of trigeminal schwannomasarise from the fifth cranial nerve in the posterior fossaand present as a mass in the cerebellopontine angle,causing dysfunction of the fifth, seventh, and eighthcranial nerves with or without cerebellar dysfunction.It is estimated that 25% of trigeminal schwannomashave an hourglass type of extension above and belowthe tentorium. Symptoms may consist of pare s t h e-sias, numbness, pain, and/or difficulty in chewing onthe side where the tumor is located.
Although some patients experience facial pain,d e c reased sensation is more commonly reported thanpain. Fifteen percent of patients with a middle fossaschwannoma may be asymptomatic. However, as thetumor increases in size, it can grow in a variety ofways depending on which branch is involved; thus,signs and symptoms depend upon the direction oftumor growth. These tumors may appear as masses
SURGICAL MANAGEMENT OF TRIGEMINAL SCHWA N N O M A S
MADJID SAMII, M.D., PH.D.RAMESH PITTI BABU, M.D.MARCOS TATAGIBA, M.D.
107
in the cavernous sinus with third, fourth, and sixthcranial nerve dysfunction, or as para-pharyngealmasses, nasopharyngeal masses, or masses in thepterygopalatine and infratemporal fossae. Among theextracranial branches, the ophthalmic division is themost commonly involved, followed by the maxillaryand mandibular divisions. Schwannomas of the oph-thalmic division present with proptosis. However,lesions arising from the maxillary or mandibular divi-sions can be quiescent for a long time, pro g re s s i v e l ye roding the skull base; they are often accidentallyd i s c o v e red during work-up for sinus conditions orfacial injury.
PATIENT SELECTIONPatients with intracranial lesions presenting with in-c reased intracranial pre s s u re (ICP) and neuro l o g i c a ldeficits are candidates for surgery. However, patientsp resenting with small, incidentally discovere d ,asymptomatic, extracranial lesions at the skull basewithout erosion of the skull base should be periodi-cally followed. Although rare, an increase in size or achange in the character of the lesion should alert thes u rgeon to a possible malignant transform a t i o nrequiring surgery. Patients with extracranial lesionsand erosion of the skull base, or the enlargement ofexit foramen (such as the foramen rotundum orovale) may be candidates for surgery since these tu-mors have a tendency to violate the dura and be-come intracranial. Resection of these tumors maynot be a technical challenge, but significant morbid-ity can result from cere b rospinal fluid (CSF) leakage© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8108
if the floor is not re p a i red well. In elderly patientsp resenting with intracranial lesions, for whom longhours of surgery cannot be undertaken for medicalreasons, intratumoral debulking may be ideal to re-duce the mass. All patients should be advised of thepotential risks of deficits of the fifth cranial nerve fol-lowing surg e r y .
RADIOLOGICAL EVALUATIONThe availability of computed tomography (CT) andmagnetic resonance (MR) imaging has made plain x-rays obsolete. CT with bone windows is an excel-lent diagnostic tool by which to visualize the bonye rosions at the skull base. On CT, schwannomasappear isodense and enhance with contrast medium.On MR imaging, these lesions are hypo-, iso-, orhyperintense on T1-weighted images and signifi-cantly enhance after intravenous contrast. MR angi-ography may be perf o rmed to visualize displacementof the major vessels, particularly in large tumors. Inaddition, conventional cerebral angiography may beundertaken to better delineate the carotid artery andto study the venous anatomy with attention to thevein of Labbé and the sigmoid sinus, particularly intumors with infra- and supratentorial extensions( h o u rglass type). The balloon occlusion test may benecessary in cases where the carotid artery needs tobe sacrificed and a vein bypass graft is contem-plated, or where temporary occlusion of the caro t i dartery is re q u i red during tumor dissection.
PREPARATION AND ANESTHESIAStarting at midnight prior to surgery, the patient isgiven intravenous Solu-Medrol, 250 mg every 6hours. The day prior to surgery, a loading dose of 1gm Dilantin is administered, which is continuedpostoperatively at 100 mg three times a day. Whenp remedication is used, it may be one of the shorter-acting benzodiazepines such as diazepam or midazo-lam, on call to the operating room. Narcotics shouldbe avoided because they tend to produce re s p i r a t o r yd e p ression and/or nausea and vomiting, which canresult in increased ICP. Routine monitoring in theoperating room consists of pulse oximetry, noninva-sive blood pre s s u re measurement, electro c a rd i o g r a-phy, and capnography. Capnography assesses theICP level and is titrated to obtain optimal ICP c o n t rol. An arterial catheter and one or two larg e -b o re intravenous lines are inserted. A short-actingopioid and ultrashort-acting intravenous anesthetic(generally thiopental or propofol) are used for induc-tion, followed by a nondepolarizing muscle re l a x a n tfor intubation. Intravenous lidocaine (1.0-1.5 mg/kgbody weight) may be useful prior to laryngoscopy. A combination of these agents permits a smoothinduction of anesthesia, thus avoiding hypertension,hypoxia, hypercarbia, or coughing, all of which may
i n c rease ICP. The hypertensive response to pin fixation of the
head may be minimized or eliminated by prior ad-ministration of an intravenous anesthetic. Anesthesiais generally maintained with a narcotic by infusion ori n t e rmittent dosage of nitrous oxide and isoflurane.The PaCO2 is maintained in the range of 25 to 30 mmHg. Induced hypotension may be re q u i red durings u rgery to reduce blood loss and the need for transfu-sion. A mean arterial pre s s u re of 50-60 mm Hg isacceptable in a healthy individual, but may not betolerated by a patient with cardiovascular disease orhypertension. In highly vascular tumors, deliberatehypotension may be induced by increasing the levelof isoflurane or by a direct-acting vasodilator, such assodium nitroprusside or nitroglycerine. After intuba-tion, the bladder is catheterized and 20% mannitol isa d m i n i s t e red intravenously (1 gm/kg body weight).
Evoked potential monitoring necessitates somemodification of the anesthetic technique. If just thesensory modalities are monitored, the level of isoflu-rane is maintained at <0.4% and anesthesia is sus-tained primarily with a narcotic infusion and nitro u soxide. If motor evoked potentials and electro m y o g r a-phy are also employed, halogenated anesthetics can-not be used. In this case, propofol and opioid (fen-tanyl or sufentanil) infusions are substituted andonly nitrous oxide is used as an inhalant.
OPERATIVE TECHNIQUEThe surgical approach to a trigeminal schwannomadepends upon the location of the tumor. These tu-mors are classified into four categories: Type A tu-mors are located entirely within the middle cranialfossa, commonly arising from the trigeminal gan-glion. Type B tumors are situated in the posteriorfossa and arise from the root of the fifth cranial nerve,p roximal to the ganglion. Type C tumors occupy thesupra- and infratentorial compartment in an hour-glass manner and grow across the tentorial hiatus.Type D tumors arise from the extracranial branchesof the fifth cranial nerve.
Type A Tumors (The Frontotemporal Appro a c h )Type A tumors are entirely confined to the middlecranial fossa (Figure 1). They arise either from thetrigeminal ganglion or from one of the branches ofthe fifth cranial nerve prior to exiting the intracranialcompartment. These tumors may invade the cav-e rnous sinus or extend into the orbit via the superiororbital fissure, such as in tumors arising from theophthalmic division.
The frontotemporal approach is best suited fortype A tumors situated in the middle cranial fossa( F i g u re 2). Patients are placed in the supine positionw i t h the head fixed in a three-pin Mayfield head-

SAMII ET AL : SURGICAL MANAGEMENT OF TRIGEMINAL SCHWANNOMAS 109
F i g u re 1. MR imaging, axial ( A ) and coronal ( B ) views, of the brain with gadolinium demonstrating tumor of the middle cranial fossa (type A tumor).
A B
F i g u re 2. Supine position used for resection of tumors via the frontotemporal approach. Note thatthe patient is well padded and secured and the head is maintained above the level of the heart.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8110
F i g u re 3. Skin incision. Note that the lower part of theskin incision is within 1 cm of the ear to avoid injury tothe facial nerve.
F i g u re 4. Skin flap has been retracted. After interf a c i a ldissection at the zygomatic process, the temporalismuscle and fascia are incised as a second layer.
F i g u re 6. Tumor has been exposed afterwidely splitting the sylvian fissure. Note therelationship of optic nerve and cerebral vesselsto the tumor.
F i g u re 5. Craniotomy and planneddural incision are shown.
Tumor resection viathe fro n t o t e m p o r a l
a p p roach (type A tumor)
fissure

SAMII ET AL : SURGICAL MANAGEMENT OF TRIGEMINAL SCHWANNOMAS 111
h o l d e r. A shoulder roll is placed under the ipsilaterals h o u l d e r, elevating and turning the upper torso tothe opposite side, minimizing rotation of the head.The head is tilted to the other side by 30 to 35d e g rees and extended by 150 to 120 degrees, makingthe zygomatic eminence the highest point in theoperating field. The head is elevated above the levelof the heart, facilitating the venous drainage. Allp re s s u re points are well padded.
The skin incision is marked starting within 1 cmin front of the external auditory meatus, beginning atthe zygoma and gently curving around the temporalline onto the frontal area, all within the hairline (Fig-u re 3). A single myocutaneous flap is elevated andretracted using fishhooks, exposing the frontal andtemporal bones and centered on the pterion (Figure4). A cuff of fascia along the superior temporal line isleft for later closure. A frontal keyhole and anotherburr hole at the squamous portion of the temporalbone, just above the zygomatic root, are placedb e f o re the craniotome is used. In elderly patients,since the dura is stuck to the bone, it is better toplace two or three burr holes and gently separate thedura from the bone before the craniotomy flap islifted, to expose the dura covering the frontal andtemporal lobes and the sylvian fissure. Extraduraldrilling of the lesser wing of the sphenoid bone isaccomplished, making the base very flat. The dura isthen opened in a semicircular manner based on thefloor; from it, a second T-shaped cut is made verti-cally corresponding to the sylvian fissure (Figure 5).Beginning at this stage, microscopic magnificationand illumination are used. The sylvian fissure is splitf rom medial to lateral, exposing the tumor, caro t i dartery, and the sylvian vessels (Figure 6). Retractionof the frontal and temporal lobes is accomplished bythe Gre e n b e rg retractor system. Initially, the brain isc o v e red with a Penrose drain and cottonoids areplaced over the brain; later, a malleable brain re t r a c-tor is used on the surface of the cottonoids. Thesetumors are extracerebral and subdural. They have awell-defined capsule and often are not vascular. Ini-tially, the surface of the tumor is coagulated and cut,allowing the tumor’s interior to be exposed. An ultra-sonic aspirator is generously used to reduce the sizeof the tumor and thoroughly decompress it so thatthe surrounding structures, such as the caro t i dartery bifurcation and the third and fourth nerves onthe medial aspect of the tumor near the tentorialm a rgin, are well visualized. It also helps to identifythe arachnoid membrane around the tumor, avoid-ing injury to the blood vessels, which are inside thearachnoid toward the pia around the brain. Pro g re s-sive internal decompression helps identify thebranches of the fifth cranial nerve as well. On mostoccasions, the tumor can be removed without caus-ing undue damage to the fifth nerve.
Once the tumor is removed, the gasserian gan-glion and the posterior cavernous sinus are care f u l l yexamined and exposed if necessary, since in massivetumors, remnants of the tumor may lurk that cancause re c u r rence if not removed. Once the tumor isremoved from the cavernous sinus, bleeding thatoriginates from the sinus is readily stopped by pack-ing it with surgical cotton or Avitene. At the conclu-sion of surgical resection, the dura is closed in awatertight fashion and the operation is completed ina routine manner. We use a Jackson Pratt drain inthe submuscular-galeal plane, which is discontin-ued after 48 hours.
Type B Tumors (Retromastoid Appro a c h )Tumors situated in the posterior fossa (Type B) area p p roached via conventional re t romastoid craniec-tomy (Figure 7). These tumors are approached withthe patient in the semi-sitting or lounging position( F i g u re 8). A l t e rnatively, the lateral decubitus posi-tion can be used. If the semi-sitting position is cho-sen, a pre c o rdial Doppler ultrasound is used todetect air embolism and a central venous line with itstip at the junction of the superior vena cava and theright atrium is placed after intubation to aspirate theembolized air. Otherwise, no special anesthetic con-siderations are necessary. Initially, the patient’s headis placed in a three-pin Mayfield headholder and isslowly positioned in the sitting position. The head isslightly turned to the ipsilateral side of the tumor.
A re t romastoid skin incision is made from thesuperior nuchal line up to the base of the occiput( F i g u re 9). The muscles are cut using a knife or Boviecoagulator; however, incision and muscle dissectionat the skull base is carefully done using a knife, lestinjury to the vertebral artery occur. Cere b e l l a rretractors are later applied to retract the musclesthat are supporting the bone. A single burr hole isplaced just below the Frankfurt horizontal plane and4.5-5 cm behind the external auditory canal and isconverted into a 4-5 cm diameter craniectomy expos-ing the edge of the transverse and sigmoid sinusjunction, including the posterior fossa dura (Figure10). During bone removal, the mastoid air cells maybe opened; these are packed with muscle at the endof surgery. Alternatively, in younger patients, a cra-niotomy flap exposing the posterior fossa with addi-tional re q u i red drilling toward the sinuses can beaccomplished. Dural opening is carried out severalmillimeters away from and along the sinuses andthen retracted with tack-up sutures. The cere b e l l u mis then covered with cottonoids and retracted using amalleable brain re t r a c t o r, exposing the cere b e l l o p o n-tine angle. Initially, brain relaxation is achieved bydraining CSF through an opening of the cistern inthe angle (Figure 11). Prior to tumor resection, it isusually not necessary to cut the superior petro s a l

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8112
F i g u re 7. MR imaging, sagittal ( A ) and axial ( B ) views, of the brain with gadolinium demonstratingtumor in the posterior fossa (type B tumor).
F i g u re 8. Semi-sitting position commonly employed for resection of type B tumors. Note theelevation of the legs and ipsilateral turning, with mild flexion, of the head, without causingjugular vein compro m i s e .
A B

SAMII ET AL : SURGICAL MANAGEMENT OF TRIGEMINAL SCHWANNOMAS 113
F i g u re 9. R e t romastoid skin incision.
F i g u re 10. Craniectomy adequate to expose the edge of the trans-verse and sigmoid sinuses. The dura is opened a few millimetersaway from the sinuses.
F i g u re 11. Dura is tightly tacked up tothe nearby soft tissue, maximizing thee x p o s u re. Once the cerebellum is re-tracted, the tumor is exposed in thec e rebellopontine angle. Note the re l a-tion of the superior cerebellar arteryand the seventh and eighth nerve com-plex to the tumor.
Resection of tumors situated in the posterior fossa (type B tumor)

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8114
vein, but sacrificing the vein is not known to causeany deficits. Once the cerebellopontine angle ex-posed, the fifth cranial nerve at the brainstem, aswell as the tumor are observed. Since these tumorsarise from the sensory component, the motor compo-nent is separately identified, pushed to the caudalaspect of the tumor, and preserved. In large tumors,the entire nerve is often splayed on the surface of thetumor; with pro g ressive debulking using the ultra-sonic aspirator, the nerve is visualized after the dis-placed nerve fibers become compact, and can be pre-served completely. To achieve total tumor re s e c t i o n ,it may be necessary to sacrifice a few nerve fiberswithout any major neurological deficit. The extra-arachnoidal dissection and debulking are perf o rm e dby teasing with the help of two tumor-holding for-ceps and an ultrasonic aspirator. Enthusiastic sepa-ration from the brainstem using cottonoids is to beavoided. Constant suction and irrigation help toclear the operative field. The seventh and eighth cra-nial nerve complex (which has been pushed down) is identified, both anatomically as well as physiologi-cally, using electrophysiological monitoring. Oncethe tumor is completely removed, jugular compre s-sion is perf o rmed to test hemostasis, and the dura isclosed in a watertight fashion. The mastoid air cellsa re packed with fibrin glue-soaked muscle to pre v e n tCSF leak. Routine closure of muscle and fascia islater achieved using 0-0 Vicryl sutures. Subcuta-neous closure with interrupted 3-0 Vicryl suture s ,and skin closure with either staples or monofilamentnylon, is perf o rm e d .
Type C Tumors (Combined Pre-sigmoid Supra- and Infratentorial Appro a c h )Patients with type C tumors are operated on using a combined pre-sigmoid supra- and infratentoriala p p roach (Figures 13-18). This approach is donewith the patient either in the semisitting position, inthe supine position with the head turned, or in astrict lateral position. We believe that the sittingposition is ideal for operating on these patients. Asfar as the sitting position is concerned, similar pre-cautions and maneuvers are undertaken as men-tioned in the previous section.
The skin incision is marked as shown in Figure13, in a “7” shape around the ear. The area of skinincision is infiltrated with 1:100,000 lidocaine withepinephrine. The skin is incised and reflected towardthe ear, and the temporal and suboccipital bones areexposed after raising a single musculoperiosteal flap.Initially, by using a high-speed drill, the bone overthe sigmoid sinus and the junction of the transversesinus is drilled. Part of the transverse sinus closer tothe midline is also drilled. Later, two additional burrholes are placed in the temporal area. A helmet-
shaped bone flap is then removed using a cranio-tome, thus exposing the subtemporal and suboccipi-tal dura as well as the transverse and sigmoidsinuses. At this stage, a total mastoidectomy extend-ing to the semicircular canals is accomplished. Thee n t i re dura from the sigmoid sinus to the semicirc u-lar canals is then exposed. The pre-sigmoid dura iscut vertically and the subtemporal dura is incisedhorizontally along the base of the temporal fossa.
B e f o re the tentorium is cut, the superior petro s a lsinus is doubly heated using 2-0 silk ties. It isadvised not to simply coagulate and leave the sinussince it can open during the surgery and cause tro u-blesome bleeding. It is advisable to cut the tentoriumin its posterior portion to prevent injury to thet rochlear nerve. The last cut on the tentorium ismade after identifying and isolating the fourth cra-nial nerve in the subarachnoid space with the assis-tance of a fine nerve hook. Once the tentorium is cut,the tumor is exposed after placing two re t r a c t o r s ,one on the cerebellum and another on the temporallobe. The fourth cranial nerve and the posterior cere-bral artery at the tentorial hiatus are protected whilethe retractors are applied. Pro g ressive intratumorald e c o m p ression with an ultrasonic aspirator is car-ried out, maintaining the integrity of the peritumoralarachnoid. In the posterior fossa, the tumor liesabove the seventh and eighth nerve complex, push-
F i g u re 12. MR imaging, axial view, of the brain withgadolinium demonstrating tumor in both the posteriorand middle fossa (ype C tumor).

SAMII ET AL : SURGICAL MANAGEMENT OF TRIGEMINAL SCHWANNOMAS 115
F i g u re 13. R e t romastoid skin incision is continued as a lowtemporal incision around the ear is used.
F i g u re 14. The mastoidectomy, suboccipital craniectomy,and temporal craniotomy are completed, exposing thedura in the re t rosigmoid, pre-sigmoid, and temporal are a s .
F i g u re 15. Dural incision as marked by the dotted line. Note the relationship of thesuperior petrosal sinus relative to the dotted line. The superior petrosal sinus needs tobe ligated prior to the tentorial incision.
Tumor resection viathe combined
p re-sigmoid supra-and infratentorial
a p p roach (type C tumor)

ing it downward. Intratumoral decompression with-out disturbing the arachnoid will shrink the tumorand separate it from the seventh and eighth nervecomplex. Residual tumor situated near the brain-stem is managed after resecting the tumor from theposterior cerebral and superior cerebellar arteries,the fourth cranial nerve, and the seventh and eighthnerve complex. Large tumors in this area signifi-cantly compress the brainstem. Careless peeling ofthe tumor from the brainstem before adequated e c o m p ression of the tumor should be avoided. Wi t hp ro g ressive decompression, the tumor delivers itselfand becomes separated from the brainstem, sincet h e re is always a layer of arachnoid at the interf a c e .Peritumoral arachnoid separates the tumor from theimportant surrounding neurovascular structure s ,and if the surgeon stays within the tumor and withinthe arachnoid, inadvertent injury to these structure sis avoided.
At the end of the pro c e d u re, the dura is appro x i-mated with an interrupted 4-0 Nurolon suture. Ifwatertight closure cannot be achieved, lyophilizeddura or temporalis fascia is used for duraplasty andfibrin glue is used to re i n f o rce the suture line. Themyocutaneous flap and skin are closed in layers inthe usual fashion. In the case of duraplasty, lumbarspinal drainage is used for a period of 3-5 days untilthe dura seals.
Type D Tumors (Preauricular Subtemporal-Infratemporal Appro a c h )Type D tumors are primarily extracranial tumorswith or without intracranial extension. If the tumorarises in the maxillary division, the tumor lies in thepterygopalatine fossa; if it arises in the mandibulardivision, the tumor occupies the subtemporal andinfratemporal fossa. These tumors cause erosion ofthe foramen ovale or rotundum and extend intracra-nially. Once they extend intracranially, they mayc o m p ress the temporal lobe, often embedded into thedura yet never violating it. In the case of giant-sizedtumors, the petrous bone is eroded and the petro u sc a rotid artery becomes incorporated into the tumor,or at least lies very densely adherent to the tumor. At h o rough understanding of this information acquire dby preoperative neuroimaging is very important forp roper surgical planning.
Type D tumors are resected using the subtempo-ral-infratemporal approach in collaboration with afaciomaxillary surgeon (Figure 19). Patients are oper-ated on while in the supine position (Figure 20). Theskin incision begins in front of the ear, just below thelevel of the zygoma, and extends to the temporala rea, to the top of the superior temporal line, gentlycurving forward (Figure 21). A standard interf a c i a ldissection is carried out at the zygoma, thus pro t e c t-ing the facial nerve branch traveling to the fore h e a d( F i g u re 22). The zygomatic osteotomy, including part
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8116
F i g u re 16. Tumor is exposed after the tentorium is cut. Gentle retraction ofthe temporal lobe and the cerebellum in the presigmoid area exposes thet u m o r, blood vessels, and cranial nerves.

SAMII ET AL : SURGICAL MANAGEMENT OF TRIGEMINAL SCHWANNOMAS 117
F i g u re 17. Intraoperative photograph showing the extent ofcraniectomy and mastoidectomy.
F i g u re 18. Intraoperative photograph axial view, showing the tumor exposed.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8118
of the frontal process, is perf o rmed later (Figure 23).T h e re is no need to perf o rm an orbital osteotomy fortumors located in the pterygopalatine and infratem-poral fossa area. In large tumors, the facial nervemay need to be identified, at the parotid fascia, toavoid injury during tumor dissection. Even if thetumor is not compressing the temporal lobe, it isadvisable to per f o rm a craniectomy and expose thedura to avoid inadvertent dural and temporal lobeinjury. A small low temporal craniotomy and craniec-tomy, including the margins of the foramen ovaleand spinosum, is carried out, identifying the man-dibular division and the middle meningeal artery.
After bipolar cauterizing, the middle meningealartery is carefully sectioned. The tumor borders areidentified and its relation to the temporal duradefined. If there is radiographic evidence of compre s-sion on the temporal lobe, it is advisable to re t r a c tthe temporal dura before the tumor is resected. Ifretraction is difficult, an elective dural-arachnoidalincision is made to allow drainage of some CSF. Ini-tially, the mandibular division is followed from itsextracranial course toward the middle fossa. Oncethe tumor in this area is identified, it is pro g re s s i v e l yd e c o m p ressed and resected. If the tumor capsule isdensely adherent to the dura and is difficult to sepa-
F i g u re 19. MR imaging, coronal view, with gadoliniumdemonstrating extracranial tumor (type D tumor).
F i g u re 20. Supine position used for resection. Note the generous padding of pre s s u re points, aswell as the adequate taping to secure the patient and position the legs above the level of the heart.

SAMII ET AL : SURGICAL MANAGEMENT OF TRIGEMINAL SCHWANNOMAS 119
F i g u re 21. Skin incision. Note that the lower part ofthe skin incision is within 1 cm of the ear as well asbelow the zygomatic arc h .
F i g u re 22. After interfacial dissection to preserve thef rontal branch of the facial nerve, the temporalismuscle has been separated from the zygomatic arc h .
F i g u re 23. Zygomatic osteotomy and temporal cra-niotomy have been perf o rmed and the tumor isexposed. Note the relation of the tumor to the duraand the parotid gland.
Tumor resection viathe preauricular s u b t e m p o r a l -i n f r a t e m p o r a l
a p p roach (type D tumor)

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8120
rate, the involved dura is resected and duraplasty is later perf o rmed. In tumors with a tongue-likeintracranial extension after extracranial tumorresection, the dura is opened, the temporal loberetracted, and the tumor completely excised. Oncethe tumor is resected, osteotomy and craniotomy arereplaced and the wound is closed in layers in a ro u-tine fashion.
If the approach described above does not give ade-quate exposure, particularly in very large tumorse roded into the pterygopalatine fossa, extra space isc reated by dislocation of the mandible of the tem-p o romandibular joint. Sometimes, mobilization ofthe facial nerve (by detaching the pterygoid musclesto the coronoid process of the mandible and sectionof the ramus of the mandible) gives extra room. Intumors arising from the maxillary division, in rarecases, a transfacial-transmaxillary approach is nec-essary. This is more useful in very large and malig-nant tumors and often is not necessary in ro u t i n eschwannomas. In tumors arising from the ophthal-mic division or tumors with intraorbital extension, af rontotemporal craniotomy and orbitozygomaticosteotomy are perf o rmed with removal of the roof ofthe orbit and the superior orbital fissure. The dura inthe superior orbital fissure area is cut and continuedto the periorbita. Intraorbital tumors are very welllocalized and can be removed without causing injuryto the ocular muscles or nerves. The optic nerve,which lies in the area, needs to be identified and pre-served with great attention.
Tumors that extend into the cavernous sinus arelocated primarily in the leaves of the lateral wall andcan be completely removed after opening the lateralwall of the cavernous sinus. After removing thet u m o r, the periorbita is closed with 0-0 Vicryl, andthe craniotomy and osteotomy are closed with 0-0Tevdek stitches. The remainder of the closure is car-ried out as usual.
COMPLICATIONSOther than routine complications of craniotomy,such as infection, hemorrhage, CSF leak, and otherrelated problems, fifth nerve dysfunction is the mostcommon complication associated with these opera-tions. Dysfunction of the ophthalmic division cancause exposure keratitis and corneal ulceration,which need to be recognized and treated pro m p t l y .Gold weights in the upper eyelid and temporary tar-s o r rhaphy are two of the best methods for pro t e c t i n gthe eye. To prevent life-threatening infection, it isessential to recognize the entry into the paranasalsinuses during surgery, and prompt attention mustbe paid to repair it appropriately at that time. Theskull base defects are re p a i red using fat, muscle,and fibrin glue to prevent potential CSF leak; occa-sionally, postoperative lumbar drainage is necessaryfor 3-5 days.
POSTOPERATIVE CARE AND FOLLOW-UPPostoperatively, patients undergoing surgery for tri-geminal schwannomas are given intravenous antibi-otics for a period of 72 hours, tapering doses of intra-venous steroids and anticonvulsants. Except inthose with a spinal drain, patients are mobilized outof bed as soon as possible, to prevent potential com-plications such as deep venous thrombosis. Pneu-matic compression boots are used for patients whilein bed.
After 3 months, follow-up MR imaging with andwithout gadolinium enhancement is perf o rmed. Ift h e re is no residual tumor, MR imaging every year for2 years and then every 5 years is suggested. Patientswith small residual tumors are closely followed withMR imaging since these tumors grow very slowly. Re-operation is not indicated unless there is significantc o m p romise of the neural structures from the re s i d-ual tumor.

INTRODUCTIONC h o l e s t e rol granulomas are benign expansile lesionsmost commonly found in either the middle ear or themastoid region in association with some type of in-flammatory ear disease. Petrous apex cholestero lgranulomas (PACGs), however, have been describedless often and in many cases have been erro n e o u s l yg rouped with epidermoid tumors, which are etiologi-cally and histologically distinct from PACGs.
P e t rous apex cholesterol granulomas are the endresult of chronic obstruction of normal aeration tothe petrous air cells. This obstruction leads to thedevelopment of negative pre s s u res within the aircells, causing mucosal engorgement. The mucosalh e m o r rhage that ensues sets the stage for a cycle ofh e m o r rhage and inflammation ending in the form a-tion and growth of a cholesterol granuloma. Becausethe pro g ression from hemorrhage to granuloma for-mation is an ongoing process, these lesions have var-ied clinical and radiographic characteristics depend-ing upon their stage of formation.
In the past, PACGs have usually been drained byotolaryngologists via either a transtemporal or atranssphenoidal route; placement of a small Silastictube was then inserted to re-establish aeration. Un-fortunately, the re c u r rence rates following the pro c e-d u re using these approaches have been reported inthe literature to be as high as 60%, with some pa-
SURGICAL MANAGEMENT OF CHOLESTEROL GRANULOMAS
OF THE PETROUS APEXMARK B. EISENBERG, M.D.
OSSAMA AL-MEFTY, M.D., F.A.C.S.
121
tients requiring multiple revisions. An alternative ap-p roach is complete excision of the lesion, includingthe mucosal lining, followed by obliteration of thecavity with vascularized tissue.
CLINICAL PRESENTATIONThe presenting signs and symptoms of PACG arel a rgely dependent upon the size and extent of thelesion. Smaller asymptomatic lesions may be discov-e red only during the evaluation of an unrelated com-plaint (e.g., headache or dizziness). As it grows, thePACG has a compressive effect upon the surro u n d-ing neurovascular structures. The trigeminal and ab-ducens nerves are particularly vulnerable because oftheir proximity to the petrous apex. As such, manypatients present either because of diplopia or facialnumbness or pain. With larger lesions, the patientmay present with hearing loss and facial nerve dys-function. While there is no pathognomonic symptomof a PACG, the time course of symptoms often gives aclue as to the diagnosis. The cyclical pattern of hem-o r rhage and inflammation often leads to periodicworsening of symptoms rather than a steady pro-g ression, as in a neoplastic growth.
PATIENT SELECTIONSmall asymptomatic or minimally symptomaticlesions in a compliant patient may be safely followedwith serial magnetic resonance imaging (MRI) stud-ies. In a small subset of these patients, the pro g re s-sive cycle will be arrested and no further tre a t m e n twill be re q u i red. Patients with pro g ressive symptomsor enlarging lesions obviously re q u i re tre a t m e n t .Patients who present with either significant symp-© 1999 The American Association of Neurological Surg e o n s

toms (re g a rdless of lesion size) or large lesions (re-g a rdless of symptoms) will also re q u i re surgical in-tervention. The traditional mode of therapy involves a drainage pro c e d u re via either a transtemporal ortranssphenoidal route. Because the re c u r rence ratefor these types of pro c e d u res is relatively high, wehave approached these lesions via an extended mid-dle fossa approach, which allows complete removal ofthe granuloma and pseudocapsule. This is followedby obliteration of the cavity with vascularized tissuein the form of a pedicled strip of temporalis muscle.
PREOPERATIVE EVALUATIONBecause of frequent involvement of the sixth andeighth cranial nerves, all patients should undergo af o rmal neuro-ophthalmological examination as wellas an audiogram and monitoring of brainstem audi-tory evoked responses. The radiographic evaluationconsists of an MRI with and without contrast en-hancement in order to confirm the diagnosis. Petro u sapex cholesterol granulomas often display a high-signal characteristic on both T1- and T2-weightedimages with only meager peripheral enhancement( F i g u re 1). Depending on the age of the lesion, how-e v e r, this “classic” appearance may not be pre s e n t .MRI also provides information re g a rding the extent ofthe lesion and whether intradural extension is pre s-ent. A computed tomography (CT) scan with bonewindow settings should also be obtained in order toevaluate the extent of erosion of the petrous apexand the temporal bone. Any involvement of the mid-dle ear will also be readily seen on CT.
PREOPERATIVE PREPARATIONThe extended middle fossa approach is an ex-tradural, subtemporal approach to the petrous apex.Although the dissection is entirely extradural, thereis a small risk of postoperative seizures because ofelevation of the temporal lobe. Patients are there f o restarted on an anticonvulsant medication the nightprior to surgery. This is continued for 3 to 6 monthsfollowing surgery. No other special preparations ormedications are re q u i red apart from the routine pre-operative evaluation and preparation for surgery.
THE EXTENDED MIDDLE FOSSAAPPROACHFollowing the induction of general endotrachealanesthesia, a lumbar drain is placed to allow cere-b rospinal fluid (CSF) drainage during the extraduralsubtemporal dissection. The patient is also main-tained in a hypovolemic state and is hyperventilated.These maneuvers are important to maximize brainrelaxation. Electrodes are then placed to allow formonitoring of somatosensory evoked potentials andfacial nerve electromyography (EMG). In addition, anearphone is placed in each external auditory canal
and scalp electrodes are inserted for monitoring ofbrainstem auditory evoked potentials. During thee x p o s u re, excessive traction or manipulation on theg reater superficial petrosal nerve, which runs alongthe floor of the middle fossa, may result in tractioninjury to the facial nerve via the geniculate ganglion.This complication has been minimized by continu-ously monitoring the facial nerve EMG. There f o re ,the patient must not receive muscle relaxants follow-ing induction and intubation.
The patient is positioned supine and the head isfixed in a three-pin head clamp. The head of the bedshould be elevated to bring the patient’s head abovethe level of the heart, thus maximizing venousdrainage and brain relaxation. The head is turned tobring the zygoma nearly horizontal, and a roll isplaced under the ipsilateral shoulder to maintain theneck in a neutral position (Figure 2). Altern a t i v e l y ,the patient may be positioned in the true lateral posi-tion with a subaxillary roll in place. The operatingm i c roscope is then balanced and brought over to thefield to check that it will be in a comfortable operat-ing position prior to draping. The ipsilateral fro n t o-temporal region is then shaved, prepped, and drapedin a standard manner. For cases in which intraduralextension is suspected, the lateral thigh is also ex-posed and pre p a red, should the need for a fascial orfat graft arise.
A preauricular curvilinear incision is made (Fig-u re 2) and the scalp flap is elevated along the sub-galeal plane. Care is taken to preserve the superf i c i a ltemporal artery. At the anterior third of the tempo-ralis muscle, the superficial layer of the deep tempo-ral fascia is incised down to the muscle and re f l e c t e danteriorly with the scalp flap, thus sparing thef rontalis branches of the facial nerve. The zygomatica rch may then be safely dissected in a subperiostealmanner and sectioned at its most anterior and pos-terior ends. This allows downward displacement ofthe arch along with the temporalis muscle. Thismaneuver provides access along the middle fossafloor with <1 cm of temporal lobe elevation. A limitedtemporal craniotomy abutting the floor of the middlefossa is perf o rmed. It is important to drill the edge ofthe craniotomy flush with the middle fossa floor ino rder to avoid unnecessary temporal lobe re t r a c t i o n( F i g u re 3).
At this point, the operating microscope is bro u g h tinto the field and the remainder of the surgery is per-f o rmed under the microscope. The lumbar drain isopened and 30 to 50 cc of CSF is allowed to drain.The temporal lobe is supported extradurally with amalleable re t r a c t o r, and extradural dissection is car-ried medially until the middle meningeal artery isidentified at the foramen spinosum. Small dural ves-sels traversing the middle fossa floor are easily con-t rolled with either direct bipolar coagulation or bone
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8122

EISENBERG AND AL-MEFTY : CHOLESTEROL GRANULOMAS OF THE PETROUS APEX 123
F i g u re 1. Axial T1- ( A ) and T2-weighted ( B ) MRIs. Note the high signal of the right petrous apex cholesterol granuloma.
A B
F i g u re 2. Patient positioning and scalp in-cision for an extended middle fossa appro a c hto the petrous apex.
F i g u re 3. Temporal craniotomy flush with themiddle fossa floor to avoid retraction of the tem-poral lobe. Note osteotomy of zygoma ( a s t e r i s k s ).

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8124
F i g u re 4. S u rgeon’s view following extradural elevation of the temporal lobe and liga-tion of the middle meningeal artery (1). 2 = petrous portion of carotid artery; 3 = V3; 4 = greater and lesser petrosal nerves; 5 = cholesterol granuloma.
F i g u re 5. The emptied petrous apex cavity obliterated using a pedicled strip of temporalis muscle.

EISENBERG AND AL-MEFTY : CHOLESTEROL GRANULOMAS OF THE PETROUS APEX 125
wax. The middle meningeal artery is coagulated andsectioned sharply, and the foramen is packed withbone wax or oxidized cellulose. The foramen ovaleanteriorly and the greater superficial petrosal nerve(GSPN) medially are then identified. The lesser su-p e rficial petrosal nerve may be seen lateral to theGSPN. The GSPN is sharply dissected from its duralattachment and preserved; in some cases, the GSPNmust be divided to avoid traction injury to the facialnerve. Further medially, the petrous portion of thei n t e rnal carotid artery can be seen deep to the pos-t e rolateral border of the third division of the trigemi-nal nerve, and, depending upon the size of thePACG, may be deviated superolaterally (Figure 4).C a re must be taken in exposing this region becausethe bone over the carotid canal is often thin or evendehiscent. Once the PACG is identified and entere d ,the fluid is drained and the soft tissues, includingthe pseudocapsule, are completely excised. This ismost often done with a combination of micro d i s s e c-tors, bipolar forceps, and smooth ring cure t t e s .When using ring curettes, it is important to be surethat they are smooth in order to avoid inadvertentinjury to the carotid artery. Often, a portion of theremaining petrous apex must be removed with ahigh-speed drill in order to gain access to all areas ofthe cavity. If this is necessary, a diamond bit is usedin order to minimize the chance of injuring any sur-rounding structures (e.g., the dura or the intern a lc a rotid artery). Obliterating the resultant cavity withfat fragments makes follow-up MRI arduous becauseof the difficulty in distinguishing the signal intensi-ties of fat versus postoperative fluid collections. Wet h e re f o re fashion a pedicled strip of temporalis mus-cle that can be used to obliterate the PACG cavity( F i g u re 5). This permits easy postoperative MRI fol-low-up, with the muscle flap giving a consistentlyhypointense signal on T1-weighted images. The boneflap is re t u rned and secured with titanium mini-plates and screws, and the remainder of the flap isclosed in standard fashion. No subgaleal drain is uti-lized. The lumbar drain is removed prior to thepatient being reversed from anesthesia unless adural repair was necessary, in which case the drainis usually left in place for 24 to 48 hours.
Patients are reversed from anesthesia in the oper-ating room and observed overnight in either the neu-ro s u rgical intensive care unit or the recovery ro o m .They are maintained on dexamethasone for 1-2 days
followed by tapering doses, and antibiotics are main-tained for 48 hours. All patients receive antiseizuremedication for 3 to 6 months, which is then tapere do ff if the patient remains seizure - f re e .
POSTOPERATIVE COMPLICATIONSBecause this is an extradural approach, primaryn e u rological complications are rare. Maximal brainrelaxation using a combination of hypovolemia, hy-perventilation, and CSF drainage has nearly elimi-nated temporal lobe-related problems. Despite this,h o w e v e r, there is a risk of postoperative seizure s ;patients are there f o re maintained on antiseizuremedication for 3 to 6 months. If a dural repair wasnecessary because of intradural extension of thegranuloma, then close postoperative surveillance fora CSF leak is crucial. The use of either a fat or a fas-cial graft, combined with the vascularized temporalisflap and postoperative lumbar drainage, helps mini-mize the risk of a CSF leak in patients requiring are p a i r. If it should occur, efforts to stop the leakmust be taken, including re-exploration. As men-tioned above, postoperative facial weakness is re-lated to traction injury via the superficial petro s a lnerve. This is prevented with careful intraoperativemonitoring of facial nerve EMG.
CONCLUSIONS1 . C h o l e s t e rol granulomas of the petrous apex are
distinct lesions resulting from blockage of the nor-mal aeration of the petrous apex air cells, which in turn leads to a repeating cycle of mucosale n g o rgement, hemorrhage, and granuloma for-mation.
2 . The extended middle fossa approach provides asafe, shallow, extradural exposure of the petro u sapex. It enables the surgeon to radically re m o v ethe granuloma and obliterate the cavity with vas-cularized tissue.
3 . Complications related to temporal lobe re t r a c t i o na re minimized by combining a zygomatic osteot-omy and drilling the temporal squama flush withthe middle fossa floor; adequate brain re l a x a t i o nis obtained using hyperventilation, hypovolemia,and CSF drainage.
4 . Ipsilateral facial nerve function is protected byattending to the greater superficial petrosal nerveand intraoperative EMG monitoring.
The authors thank Ron Tribell for his expert creation of the illustrations in this article.


INTRODUCTIONResection of angiographically occult vascular malfor-mations (AOVMs) of the brainstem, thalamus, andbasal ganglia has only recently been possible; thishas come about largely as a result of impro v e m e n t sin micro s u rgery and radiographic imaging. Prior tothe advent of magnetic resonance (MR) imaging, itwas extremely difficult to diagnose the presence ofAOVMs in these regions. Many patients suff e r i n gepisodic clinical deterioration secondary to hemor-rhage from an AOVM were diagnosed as having mul-tiple sclerosis or cerebral infarctions. The use of mi-c roinstrumentation and the neuro m i c roscope alongwith the aid of stereotaxis and electro p h y s i o l o g i c a lmonitoring have enabled neuro s u rgeons to safelyresect many of these lesions, most of which were be-lieved to be “unre s e c t a b l e . ”
The natural history of untreated AOVMs in thebrainstem, thalamus, and basal ganglia is variableand incompletely described, with bleed rates rangingf rom 0.25% to 43% per year. Data suggest thatbrainstem AOVMs presenting with clinical hemor-rhage may rebleed at a higher rate of 4.5% to 21.5%per year. The neurological morbidity and mortalityassociated with clinical bleeding from AOVMs inthese regions can be significant, due to the criticaln a t u re of structures affected by a single or re c u r re n th e m o r rh a g e .
SURGICAL MANAGEMENT OF A N G I O G R A P H I C A L LY OCCULT
VASCULAR MALFORMATIONS OF THEBRAINSTEM, THALAMUS,
AND BASAL GANGLIAGARY K. STEINBERG, M.D., PH.D.
STEVEN D. CHANG, M.D.
127
CLINICAL PRESENTATIONAngiographically occult vascular malformations typi-cally become symptomatic following a hemorrh a g e .The volume of the hemorrhage, as well as the partic-ular location, determine the type and severity of then e u rological symptoms. Given the critical functionsof the brainstem, thalamus, and basal ganglia, mosth e m o r rhages in these regions are symptomatic.Acute hemorrhages usually yield new deficits, whileother neurological deficits may result from edema orgliosis surrounding the AOVM. Seizures (supratento-rial AOVMs) and cranial nerve deficits (brainstemAOVMs) as well as generalized symptoms such asheadache and nausea may be noted.
RADIOGRAPHIC APPEARANCEThe radiographic appearance of AOVMs is quite char-acteristic. These lesions usually appear as well-de-m a rcated areas of heterogenous signal intensity onboth T1- and T2-weighted images, surrounded by aperipheral rim of hypointensity that is more easilyseen on the T2-weighted images. The high-attenua-tion areas on T1- and T2-weighted images re p re s e n tsubacute blood (extracellular methemoglobin), whilethe peripheral rim of hypointensity re p resents hemo-siderin and ferritin (chronic hemorrhage). SmallAOVMs may appear as a punctate region of low at-tenuation. Occasionally, a large subacute hemor-rhage will dominate the MR appearance, obscuringthe characteristic mixed attenuation appearance.
PATIENT SELECTIONC u r rent indications for surgery include multiple, clin-ically symptomatic hemorrhages or a single larg e© 1999 The American Association of Neurological Surg e o n s

h e m o r rhage associated with significant neuro l o g i c a ldeficit. It is also important to consider the location ofthe AOVM in relation to a ventricular or pial surf a c e ,since operative exposure through intact brainstem,thalamic, or basal ganglia structures usually re s u l t sin unacceptable neurological consequences. An ex-ception to this is the presence of deep lesions in thethalamus that can be stereotactically appro a c h e dt h rough the pulvinar region and micro s u rgically re-sected with good clinical results. The T1-weighted MRimage is best for assessing proximity to such anependymal or pial surface. If the AOVM or its hemo-siderin ring is immediately adjacent to such a surf a c e ,the AOVM can be approached safely. T2-weightedimages, including first echo or second echo, causesome “blooming” in the hemosiderin ring and a falsesense of proximity to the pial or ventricular surf a c e .
Patients in the following categories are poor anes-thetic risks and are excluded from surgical consider-ation: elderly patients, those severely and chro n i c a l l ydebilitated by neurological deficits, or those withassociated severe medical problems. Patients withAOVMs located within the posterior limb of the inter-nal capsule are also not good surgical candidates,because of fear of producing permanent contralat-eral hemiplegia. However, large AOVMs located inthe basal ganglia or thalamus and adjacent to theposterior limb of the internal capsule can be suc-cessfully removed with good clinical outcomes.
PREOPERATIVE PREPARATIONThe timing of surgery following the last clinical hem-o r rhage is important. A 4-week delay from the mostrecent significant clinical hemorrhage allows for sta-bilization and possible improvement of the clinicalcondition. This also provides time for acute hemor-rhagic components to soften or liquefy, facilitatingeasier dissection. Another advantage of operating inthe subacute period is that the hematoma has al-ready perf o rmed some of the dissection and, afterdrainage or removal of this blood, one can workt h rough the clot cavity without entering norm a lp a renchyma. Removal of subacute hematoma mayalso immediately improve the patient’s neuro l o g i c a lcondition by relieving pre s s u re on normal neuralpathways. Over several months’ time, the hematomawill organize, fibrose, and become surrounded byglial scarring, obscuring the well-demarcated dissec-tion planes and making surgical removal more diff i-cult. Thus, resection more than several months afterthe last hemorrhage may be more difficult than pro-c e d u res perf o rmed in the subacute phase. Prior tos u rgery, hypertension is controlled with oral anti-hypertensive medications.
Anesthetic Te c h n i q u eThe patient is given general anesthesia with judicious
c o n t rol of blood pre s s u re. Patients undergo surg e r ywhile under normotensive conditions. Mild brainh y p o t h e rmia is used, dropping the core body andbrain temperature to 33°-34°C by applying a coolingblanket. This degree of mild brain hypothermia hasbeen shown to provide excellent protection againstexperimental ischemic and traumatic cerebral injury.Under operative conditions of AOVM resection, thish y p o t h e rmic technique is safe, feasible, and econom-ical with excellent overall clinical outcomes. Spinalc e re b rospinal fluid (CSF) drainage is not ro u t i n e l yutilized. Adequate relaxation is achieved thoro u g hthe use of ventricular or subarachnoid CSF drainage.
Upon completion of the pro c e d u re and duringe m e rgence from anesthesia, the patient’s blood pre s-s u re should be controlled to avoid any hypertensiveepisodes, particularly during extubation.
Operative Positioning and ExposureThe surgical approach is chosen according to the sitew h e re the AOVM presents at the pial or ependymals u rface. For AOVMs in the midline medulla or ponsthat present to the fourth ventricular surface, a mid-line suboccipital approach is utilized, with the patientpositioned prone (Figure 1A). If the medullary or pon-tine AOVM is located laterally or anteriorly and pre-sents to one of these pial surfaces, but not to thefourth ventricular surface, the far lateral suboccipitala p p roach is employed. The patient is positioned later-ally or supine with the head turned (Figure 1B). Mid-brain or pontomesencephalic AOVMs are exposed viaa subtemporal or a subtemporal, transpetrosal ap-p roach if they present to the lateral or anterior sur-face of these structures. The patient is positionedsupine with a shoulder roll and the head is turned oroperated in the lateral position. Some of the midlinepontomesencephalic AOVMs can also be appro a c h e dvia a midline suboccipital exposure if they present tothe fourth ventricle or the cerebral aqueduct. If mes-encephalic AOVMs are located in the tectal plate re-gion, a supracere b e l l a r, infratentorial exposure is uti-lized. We prefer the patient to be in a sitting positionto allow easier positioning of the microscope (Figure1C). Others have used the supracere b e l l a r, infra-tentorial approach with the patient in the Concord ep o s i t i o n .
AOVMs of the thalamus are exposed via a midlineposterior parietal interhemispheric approach, usu-ally transcallosal to the lateral ventricle, but some-times inferior to the splenium of the corpus callo-sum. The patient is positioned laterally with theinvolved side down to allow gravity relaxation of the ipsilateral parietal-occipital mesial cortex (Figure1B). AOVMs of the basal ganglia are exposed, eithertranscallosal transventricular as the thalamic le-sions, or transsylvian, depending on their pre c i s esize and location.
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8128

STEINBERG AND CHANG : AOVMS OF THE BRAINSTEM, THALAMUS, AND BASAL GANGLIA 129
OPERATIVE PROCEDUREAfter general anesthesia is induced and the patientpositioned, a sterile surgical scrub is perf o rmed andthe incision site draped. The skin incision is madeusing a No. 10 blade, and bipolar coagulating forc e p sa re used to cauterize any bleeding scalp vessels. Dis-section is carried through the subcutaneous tissue,galea, and/or muscle using a No. 15 blade or electro-cautery, and the bone is exposed. A perforator andcraniotome are used to perf o rm the craniotomy.Bone wax is used to control bleeding along the boneedges, and dural tack-up sutures are placed. Thedura is opened using dural forceps and a No. 15blade. For AOVMs in the midline medulla or ponsthat present to the fourth ventricular surface, a sub-
occipital craniotomy (removing the foramen magnumbut not the posterior arch of C1) is used. The cere-bellar tonsils are retracted and the inferior midlinev e rmis is sectioned to facilitate exposure to the floorof the fourth ventricle (Figure 2). A region of blue dis-coloration (hemorrhage) or hemosiderin indicates thelocation of the AOVM (Figure 3).
M i c ro s u rgical resection is done under high-powermagnification with very fine bipolar irrigating coagu-lation forceps and using low coagulation power. It iscritical to perf o rm the dissection on the edge of theAOVM, leaving the hemosiderin-stained pare n c h y m aintact (Figure 4). Hemostasis is achieved with smallpieces of Surgicel, Gelfoam, or cotton. Dissection ofthe AOVM is done using extreme caution to avoid
F i g u re 1. A, for AOVMs in the midline medulla or ponsthat present to the fourth ventricular surface, the patient isplaced in the prone position. B, for lateral medullary orpontine AOVMs, the patient is placed in the lateral positionwith head turned. C , for tectal plate or posterior mesen-cephalic AOVMs, the patient is positioned in the sittingp o s i t i o n .
A
B
C

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8130
F i g u re 2. The prone position as viewed through microscope withs u rgeon at the top of the patient’s head. A , the floor of the fourthventricle is exposed for medial medullary or pontine AOVMs, and amidline suboccipital approach is utilized. B , once the AOVM is lo-calized, a gently placed small retractor blade may aid in exposure.
A
B
F i g u re 3. Intraoperative low-power photo-graph showing hemorrhagic discolorationw h e re the AOVM presents to the ependymals u rface of the fourth ventricle ( a r ro w ).
F i g u re 4. Intraoperative high-power photo-graph showing circ u m f e rential dissectiona round the AOVM, taking care to stay on theAOVM margin, thereby avoiding injury tos u r rounding brainstem pare n c h y m a .

STEINBERG AND CHANG : AOVMS OF THE BRAINSTEM, THALAMUS, AND BASAL GANGLIA 131
excessive coagulation with spread of current to sur-rounding brain tissue. Occasionally, the smallestsized tapered retractor blade applied gently to theedge of the brainstem is used for exposure (Figure2B). It is important to employ piecemeal removal ofthe AOVM if the parenchymal opening is smaller thanthe AOVM in order to avoid excessive retraction ofn o rmal parenchyma; however, it is essential to re s e c tthe entire AOVM, since any residual has a highchance of re c u r rence with rebleeding and enlarg e-ment. It is also critically important to preserve anydevelopmental venous anomaly (venous angioma)that is associated with the AOVM to avoid a venousi n f a rction with subsequent neurological injury.
For AOVMs located in the lateral or anteriormedulla or pons, a far-lateral suboccipital appro a c his used. Meticulous drilling of bone up to the trans-verse and sigmoid sinuses maximizes exposure .Once the craniotomy is complete, the dura is openedwhile carefully preserving the transverse and sig-moid sinuses. Retractor blades are used to gentlyretract the cerebellum to expose the brainstem. Dis-coloration of the normal tissue indicates the AOVMlocation, and micro s u rgical resection proceeds asabove. Cranial nerves and vascular branches of thebasilar and vertebral artery are carefully avoided( F i g u re 5).
AOVMs in the tectal plate or posterior mesen-cephalon are approached via a suboccipital craniot-omy, and a supracere b e l l a r, infratentorial exposure ismost frequently used (Figure 6). This approach re-q u i res dissection (using bipolar electrocautery andsmall bore suction) of the superior cerebellar verm i sand superior medullary velum. The precentral cere-bellar vein may be sacrificed to improve exposure .E x p o s u re is maximized using retractor blades toretract the cerebellar hemispheres. Care must betaken to avoid injury to the vein of Galen, the twodraining veins of Rosenthal, and the straight sinus.Hemostasis is maintained at all times to reduce bloodclots within the fourth ventricle in order to minimizepostoperative hydrocephalus. Once the AOVM loca-tion is identified, micro s u rgical resection proceeds asdescribed pre v i o u s l y .
Following the craniotomy, AOVMs of the thalamusa re approached via a midline posterior interh e m i-spheric transcallosal approach if the malformation ismedial (Figure 7A). Retractor blades placed on theipsilateral cortical hemisphere improve exposure (thedura maintains retraction of the contralateral hemi-s p h e re if the involved side faces down). The corpuscallosum is identified, and a callosotomy perf o rm e dusing bipolar electrocautery forceps and small boresuction to achieve exposure to the third ventricle( F i g u re 7B). Hemostasis must be maintained at alltimes to ensure visibility while working in the ventri-cle. The AOVM is identified on the surface of the pos-
terior thalamus or, if not directly visible, located withthe aid of stereotaxis. Micro s u rgical resection can besafely perf o rmed within the pulvinar nucleus with-out any significant neurological deficit. Occasionally,the smallest sized tapered retractor blade appliedgently to the edge of the thalamus is used to incre a s ee x p o s u re. Care must be taken to avoid significantamounts of intraventricular blood to minimize therisk of postoperative hydrocephalus. Postero i n f e r i o rthalamic AOVMs may be difficult to reach via theabove exposure, and are optimally appro a c h e dt h rough a transcallosal interhemispheric appro a c hinferior to the splenium.
Basal ganglia AOVMs are exposed via a transcal-losal transventricular approach if they are mediallylocated. For these lesions, the case proceeds as de-scribed above for the thalamic AOVMs. Lateral basalganglia AOVMs are generally exposed via a transsyl-vian approach (Figure 8). Following completion of atemporal craniotomy, the dura is reflected and thesylvian fissure opened under the microscope to ex-pose the insular cortex. Stereotaxis is useful in thea p p roach to these lateral lesions, which generally donot come to a pial surface. Once the AOVM location isidentified, bipolar electrocautery is used to dissectt h rough a small portion of the insular surface dire c t l yoverlying the AOVM. Small retractor blades may begently placed to maximize exposure. Micro d i s s e c t i o nis perf o rmed similarly to thalamic lesions, using bi-polar electrocautery forceps and gentle small boresuction. Perforating arteries from the middle cere b r a lartery traverse the insula and the basal ganglia, andshould be avoided if they do not directly feed theA O V M .
CLOSURE TECHNIQUESMeticulous hemostasis is obtained in the re s e c t i o nbed of the AOVM, and a final inspection is perf o rm e dto ensure that the entire AOVM has been completelyremoved. Transient induced hypertension can beused to test hemostasis. The resection bed is thenlined with Surgicel. The dura is closed in the stan-d a rd fashion using 4-0 nylon suture, and the bonereplaced to complete the craniotomy. A subgalealdrain is attached to light suction for 12-24 hours.The scalp incision is closed in two layers, with ap-p roximation of galeal layer using 3-0 Dexon suture sand the skin with staples. A sterile head dressing isa p p l i e d .
MONITORINGE l e c t rophysiological monitoring and mapping ofbrainstem motor nuclei are extremely valuable aidsfor the resection of AOVMs of the brainstem, thala-mus, and basal ganglia, and will improve clinicalresults. Monitoring routinely consists of bilateral so-matosensory evoked potentials, bilateral brainstem

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8132
F i g u re 5. The far-lateral suboccipital approach to the antero-lateral medulla or pons. Cranial nerves V (short arro w ), VII/VIII (long arro w ), and IX, X, XI complex ( a r ro w h e a d ) a re wellv i s u a l i z e d .
F i g u re 7. Thalamic and mesial basal ganglia AOVMs are approached via a midline interhemispheric approach ( A ) and acallosotomy is perf o rmed providing access to the lateral ventricle and thalamus or basal ganglia ( B ). A r ro w indicates cor-pus callosum.
F i g u re 8. Lateral basal ganglia AOVMs are ex-posed via a transsylvian approach with gentle re-traction of the frontal (A) and temporal (B) lobes.
F i g u re 6. The infratentorial supracerebellar approach to tectal plate or posterior mesencephalic AOVMs. Gentleretraction on the cerebellum can sometimes facilitate ex-p o s u re .
A B
A B

STEINBERG AND CHANG : AOVMS OF THE BRAINSTEM, THALAMUS, AND BASAL GANGLIA 133
auditory evoked potentials, and, if appropriate, bilat-eral fifth, seventh, 11th, and 12th nerve motor func-tion for brainstem surgery. Bilateral upper and lowersomatosensory evoked potentials are used duringresection of thalamic and basal ganglia AOVMs. Con-tinuous monitoring of these sensory pathways andmotor nuclei has allowed early detection of excessiveretraction or manipulation of critical structure s .E l e c t rophysiological mapping of the brainstem fifth,seventh, and 12th nerve motor nuclei function, usingtiny stimulating electrodes to localize these functions,has allowed more precise planning of safe trajectoriest h rough the floor of the fourth ventricle to appro a c hAOVMs. A midline approach to the floor of the fourthventricle should be avoided, if possible, since thisrisks causing bilateral internuclear ophthalmoplegia.Special precautions should also be taken to avoid thesixth/seventh cranial nerve complex.
STEREOTAXISIntraoperative stereotaxis helps localize portions ofthe deep AOVMs not presenting directly to the ven-tricular or pial surface. The CRW (Cosman-Roberts-Wells) frame was previously used, but was found tobe somewhat cumbersome. The Radionics framelessOperating Arm System (OAS) was easier to use, al-though we now routinely employ the new RadionicsOptical Tracking System (OTS) or the Elekta Vi e w-scope, which obviate the need for any articulatinga rm system and maintain a precision of a few milli-meters. This stereotactic approach has allowed betterplanning for the initial incision into the brainstem,thalamus, or basal ganglia, and also has helped con-f i rm complete resection of all components of thel a rger AOVMs that may have irregular configurations.
POSTOPERATIVE CAREThe patient is monitored for 24 hours in an intensivec a re setting. Careful control of blood pre s s u ret h rough the judicious use of antihypertensive med-ication minimizes hemorrhage at the AOVM re s e c t i o nsite. The subgaleal drain is removed on the first post-operative day. Antibiotics are routinely used only
while the subgaleal drain is in place. Postoperativeanticonvulsants are utilized on a routine basis only ifthe patient presented with preoperative seizure s .
COMPLICATIONSThe most devastating complication is perioperativere c u r rent hemorrhage which, fortunately, is ex-t remely rare. This can be due either to lack of ade-quate hemostasis or failure to completely resect theAOVM and emphasizes the importance of re m o v i n gthe entire malformation, including any irregular ex-tensions. MR scanning 3-6 months following surg e r yis generally reliable in confirming complete re s e c t i o nof the malformation, although hemosiderin stainingwill persist forever in the resection bed. There shouldbe no evidence of persistent subacute hemorrhage inthe form of methemoglobin.
Other areas of postoperative morbidity can be re-lated to manipulation, retraction, and edema of criti-cal brain parenchyma surrounding these deepAOVMs. Transient internuclear ophthalmoplegia iscommon after a midline fourth ventricular appro a c h ,but usually resolves. Transient worsening of hemi-p a resis is associated with resection of some thalamicand basal ganglia AOVMs. Worsening of facial nervefunction, sixth nerve paresis, appendicular ataxia, orgait is sometimes noted following resection of certainbrainstem AOVMs. “Ondine’s curse” is a risk in pa-tients with large medullary AOVMs. The far- l a t e r a la p p roach can sometimes be accompanied by tran-sient lower cranial nerve palsies.
Postoperative hydrocephalus is a known compli-cation in patients with significant intraventricularblood, but this can be avoided with meticuloushemostasis throughout the pro c e d u re. A watertightdural closure minimizes the risk of CSF leaks andpseudomeningoceles. As with other craniotomies,postoperative meningitis and wound infections arer a re, but well-described, events. Better clinical re-sults are achieved in patients who are in good pre o p-erative condition; however, patients in poor pre o p e r-ative condition have been found to make re m a r k a b l ere c o v e r i e s .


INTRODUCTIONThe anatomical complexity and functional impor-tance of jugular foramen structures present a form i-dable challenge to the surgical removal of tumors in that region. Optimal therapeutic outcomes are de-pendent upon the cooperation of a multidisciplinaryteam consisting of neuro s u rgeons, otologists, head-neck surgeons, and neuro r a d i o l o g i s t s .
A thorough understanding of the jugular foramenand its adjacent anatomy is essential for a success-ful surgical outcome. The jugular foramen containsthe jugular bulb, re p resenting the continuation ofthe sigmoid sinus and pro g ressing to the intern a ljugular vein. Additional venous drainage enters thejugular bulb via the inferior petrosal sinus. The lowercranial nerves (the glossopharyngeal, the vagus, andthe spinal accessory nerves) also traverse the fora-men. Additional adjacent anatomical structure se n c o u n t e red during jugular foramen surgery includethe facial nerve, carotid artery, hypoglossal nerve,s e m i c i rcular canals, middle ear, and the temporalcomponents for hearing function.
MANAGEMENT OF JUGULAR FORAMEN TUMORS
JEFFREY BRUCE, M.D.IAN STORPER, M.D.
135
PATIENT SELECTIONThe most common tumors of the jugular forameninclude neuromas of the lower cranial nerves andglomus jugulare tumors. Glomus jugulare tumorsre q u i re a much greater operative exposure than neu-romas due to their highly vascular and locally inva-sive characteristics. Neuromas are less of a surg i c a lchallenge since they are noninvasive and are gener-ally localized to one nerve fascicle, making them eas-ily separable from the surrounding cranial nerves.Less commonly presenting tumors include chord o-mas, epidermoids, and a variety of carcinomas.
A detailed radiological workup is necessary forestablishing the diagnosis and determining the ana-tomic extent of the tumor. Magnetic resonance imag-ing (MRI) with and without gadolinium enhancementis best for demonstrating the tumor and its re l a t i o n-ship to adjacent structures (Figures 1 and 2). High-resolution computed tomography (CT), with andwithout bone windows, delineates the destructionand erosion of the temporal bone and its re l a t i o n s h i pto the carotid artery, hypoglossal canal, temporalbone structures, and arteries (Figure 3). Angiographyis useful for establishing the diagnosis of a glomustumor; in addition, it is necessary for determ i n i n gthe degree of vascularity, the location of feeding ves-sels, and routes of venous drainage (Figure 4A). Thediagnosis of a glomus tumor should be anticipatedprior to angiography so that simultaneous emboliza-tion may be perf o rmed if indicated (Figure 4B). When© 1999 The American Association of Neurological Surg e o n s

a p p ropriate, a carotid occlusion test may also be per-f o rmed if the tumor involves the carotid artery andpotential damage to the artery during surgery exists.
In addition to the radiographic workup, an en-docrine evaluation including a 24-hour urine collec-tion to measure for catecholamines should be per-f o rmed. Approximately 4% of glomus tumors secre t ecatecholamines; if not recognized, the presence ofcatecholamines can lead to postoperative complica-tions. Complete hearing and swallowing evaluationsand otoscopic examinations are also indicated.
Nearly all symptomatic patients with jugular fora-
men tumors are candidates for surgical re s e c t i o n .Since many tumors grow slowly, however, considera-tion must be given to the patient’s age and anyunderlying medical conditions that might contraindi-cate surgery. There is no simple formula for deter-mining the risk-benefit ratios of surgery other thanon an individual basis. These operations are rare l ye m e rgencies and adequate time for complete diag-nostic workups and thoughtful preparations can bemade. More controversial are asymptomatic tumors,which must also be evaluated within the context ofthe patient’s age and medical condition. Conserva-
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8136
F i g u re 1. Contrast-enhanced axial MRI demonstratingenhancing mass in the jugular foramen.
F i g u re 2. Contrast-enhanced coronal MRI demonstratingan enhancing mass in the jugular foramen and extendinginto the jugular vein.
F i g u re 3. Axial CT showing glomus tumor eroding thejugular foramen.

BRUCE AND STORPER : MANAGEMENT OF JUGULAR FORAMEN TUMORS 137
tive management is often desirable under these cir-c u m s t a n c e s .
The selection of alternatives to surgery is alsoc o n t roversial. Embolization alone is thought to re-duce the rate of growth of these tumors; however, itis generally used in conjunction with surgery ratherthan as a primary, single therapeutic option. The ef-fectiveness of radiation therapy on a long-term basisis disputed. Most of the literature addressing alter-natives to surgery is distorted by the lack of scientificmethodology. Similarly, even less is known about thel o n g - t e rm effects of radiosurgery. The decision toradiate has important implications. If radiation failsand surgery is ultimately necessary, there is signifi-cantly greater difficulty and morbidity associatedwith surgery.
The patient must be well pre p a red for the exten-sive surgery that is re q u i red. Significant risks tohearing, swallowing, facial functions, and speechmust be anticipated. In certain instances wheret h e re is extensive tumor, functions such as hearingmay need to be deliberately sacrificed as part of theresection. Patients must be pre p a red for the possibil-ity of either a temporary or permanent tracheostomy.In most instances, cranial nerve impairment is tem-porary. Patients must also be aware that because of
the labor-intensive surgery involving the jugularforamen, it may be necessary to stage the operationinto two parts.
PREOPERATIVE PREPARATION All patients with glomus tumors should undergo pre-operative embolization (Figure 4). The timing of thisis controversial but generally should be done within24 to 72 hours of surgery. Extensive tumors mayre q u i re two separate embolizations. Tr a c h e o s t o m y ,p e rf o rmed prophylactically, may be preferable torisking postoperative aspiration pneumonia. The tra-cheostomy can be removed if the swallowing functionis intact.
Anesthetic Te c h n i q u eT h e re are no special general anesthesia consid-erations. Electrophysiological monitoring is re c o m-mended, consisting of brain stem auditory evokedresponses as well as monitoring of the lower cranialnerves and facial nerve. Routine bro a d - s p e c t r u mantibiotics are used. Since a spinal drain is usuallynecessary to reduce postoperative cere b ro s p i n a lfluid (CSF) leakage, it is best placed pre o p e r a t i v e l y ,unless intradural exploration is not likely to be per-
F i g u re 4. A, angiogram showing prominent vascularity of the glomus tumor. B , angiogram following embolizationdemonstrating marked reduction in vascularity.
A B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8138
f o rm e d .
Operative PositioningFor optimal positioning, the patient is placed supinewith the head turned 90 d e g rees in the contralaterald i rection (Figure 5). A sandbag is placed undern e a t hthe ipsilateral shoulder, facilitating head turning. Ifan individual is particularly large and of limitedmobility, a lateral position may be needed. A thre e -point head fixation device may be used to maintainthe head position, although a simple cere b e l l a rh e a d rest is often preferable so that the head positionmay be moved as desired.
Skin IncisionA wide operative exposure of the petrous bone andneck is necessary for safe removal of jugular foramentumors. It is important to have control of the vesselsp roximally and distally as well as to identify the cra-nial nerves proximally and distally where the anat-omy has not been disturbed by tumor (Figure 6).Inadequate exposure adds to the difficulty of theoperation and may result in failure to completelyremove the tumor. Smaller glomus tumors and non-invasive tumors such as neuromas generally re q u i rea less extensive exposure. As the surgeon’s experi-ence increases, the size of the operative field may bereduced; however, this is not of major concern .
A C-shaped posterior auricular incision is madeextending anteriorly into the temporalis muscle anddown along the anterior border of the stern o c l e i d o-mastoid muscle. This will provide the exposure nec-essary to the lower cranial nerves, the carotid artery,and the jugular vein in the neck, as well as to be ableto mobilize the temporomandibular joint and per-f o rm temporal bone dissection.
OPERATIVE PROCEDUREThe scalp flap is retracted anteriorly, leaving thetemporalis muscle and fascia intact. The ear canal istransected at the bony-cartilaginous junction and isthen oversewn. Inferiorly, a flap is raised off theperiosteum of the skull continuous with the stern o-cleidomastoid muscle. Subplatysmal flaps are ele-vated in the neck until the parotid gland is visual-ized, with the flap remaining continuous with thefascia of the parotid gland. The stern o c l e i d o m a s t o i dmuscle is retracted laterally and the internal jugularvein is identified and dissected from an inferior tosuperior direction. The vagus nerve is identified andfollowed along its path between the carotid arteryand the internal jugular vein. The jugular vein andcommon carotid arteries are both tagged with a ves-sel loop. The internal carotid artery is dissected upt o w a rd the base of the skull after elevating the sub-mandibular gland. The spinal accessory and hypo-
glossal nerves are identified and dissected above theb i f u rcation of the carotid artery. The spinal acces-sory nerve is followed through the stern o c l e i d o m a s-toid muscle and up to the jugular foramen. Thep a rotid gland is sharply dissected off the tympanicand mastoid bones to the level of the posterior bellyof the digastric muscle. The facial nerve is care f u l l ydissected adjacent to the styloid process and peeledo ff the parotid gland up to where it branches. Thefacial nerve is dissected from an inferior to superiord i rection until it is completely freed from the paro t i dgland. The parotid gland can then be removed in itse n t i rety. At this point, the neck dissection is com-pleted, with exposure and control of the intern a ljugular vein, the carotid arteries, and the nintht h rough 12th cranial nerves up to the jugular fora-men. The facial nerve is also dissected free from thep a rotid gland.
The next phase is temporal bone dissection (Fig-u re 7). This can be perf o rmed using either loupesand a strong headlight or the operating micro s c o p e .A high-speed drill with copious irrigation is used tobegin the mastoidectomy. The bone over the middlecranial fossa (tegmen) and the sigmoid sinus is ex-posed. The posterior external auditory canal wall isthen ground to Koerner’s septum. The septum is re-moved and the incus can be seen. As dissection pro-ceeds anteriorly into the zygomatic route, the de-scending segment of the facial nerve is visualized.This is followed down to the stylomastoid foramen.The facial nerve is dissected and drilled away fro mits bony canal up to the level of the external genu( F i g u re 8). The bony external auditory canal is drilledaway circ u m f e rentially to the area of the facialrecess. The incudostapedial joint and incus are re-moved from the middle ear. Dissection proceeds untilthe external auditory canal itself is removed. Thetympanic membrane, the tympanic malleus, and theannulus are removed. The temporal bone posteriorto the facial nerve is drilled away down to the level ofthe jugular bulb. The tumor can often be seen bythis point. Dissection continues until the facial nerveis completely mobilized distal to the lateral genu.
At this point, a decision can be made as towhether or not the petrous carotid artery needs to bemobilized. To accomplish this, the temporo m a n d i b u-lar joint must be drilled away on all sides, takingc a re to avoid the carotid artery lying just medial to it.The zygoma is then divided, enabling the mandible tobe mobilized anteriorly.
Drilling continues into the posterior cranial fossato the re t rosigmoid region. Enough bone is re m o v e dto be able to mobilize the sigmoid sinus. At anypoint, the sigmoid sinus can be opened and packedwith Surgicel or other suitable hemostatic agent. Thee n t i re sigmoid sinus is drilled away down to thejugular foramen as well as down to the occipital

BRUCE AND STORPER : MANAGEMENT OF JUGULAR FORAMEN TUMORS 139
F i g u re 5. Photograph showing patient positioned supine with the head turned appro x i-mately 90d e g rees. A C-shaped posterior auricular incision provides the exposure neces-sary to expose the temporal bone and lower cranial nerves in the neck.
F i g u re 6. Drawing demonstrating a postauricular incision. Smaller tumors can beremoved with a smaller incision and less exposure. (Drawing courtesy of George Card )

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8140
F i g u re 7. Drawing of the tumor in the jugular foramen after temporal bone drilling.(Drawing courtesy of George Card )
F i g u re 8. Operative photograph demonstrating facial nerve e x p o s u re after temporal bone drilling.
facial nerve
facial nerve
external auditory canal
tumor withinjugular bulb
jugular bulb
sigmoid sinus
sigmoid sinus

BRUCE AND STORPER : MANAGEMENT OF JUGULAR FORAMEN TUMORS 141
F i g u re 9. Drawing showing the jugular foramen anatomy following tumor re m o v a l .(Drawing courtesy of George Card )
F i g u re 10. Operative photograph demonstrating closure with free fat graft overlyingvascularized temporalis muscle flap that has been rotated into temporal bone defect.
facial nerve
glossopharyngealnerve
carotid artery
vagus nerve
jugular vein
accessory nerve
sigmoid sinus(opened)

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8142
condyle and hypoglossal canal. Drilling continuesuntil the endolymphatic sac and semicircular canalsa re drilled away. A complete labyrinthectomy is oftenneeded. The facial nerve can be followed up to thegeniculate ganglion and to the cere b e l l o p o n t i n eangle. Throughout drilling, it is important to leavethe capsule of the tumor intact to reduce bleeding inthe operative field. Once the cochlea is drilled away,the middle fossa dura is easily freed up. Dissection iscontinued anteriorly into the clivus and the boneoverlying the Eustachian tube is removed. Thep e t rous carotid artery can be identified and safelydissected away, but enough exposure must be main-tained to have control of the artery should a tearo c c u r. The middle meningeal artery can also be li-gated at this point.
Following the extensive exposure, removal of thetumor begins. If there is a significant intradural com-ponent, the dura may be opened adjacent to thei n t e rnal auditory canal. En bloc removal of thetumor is pre f e r red; however, piecemeal removal maybe necessary depending on the size of the tumor. Theouter capsule is generally vascular, even with embo-lization. Cautery may be used to reduce the capsule;because of the adjacent cranial nerves, this must bedone with great care. Generally, it is preferable toallow minor bleeding to continue rather than to riskcranial nerve damage from cautery. The tumor canbe internally debulked, and hemostatic materialsuch as Avitene placed into the tumor will contro lmost bleeding. The cranial nerves can be identifiedp roximally as they go into the jugular foramen, al-though is often difficult to follow the nerves as theyenter the canal. It is generally best to mobilize thesigmoid sinus and resect it down to the jugular fora-men (Figure 9). The internal jugular vein will alre a d yhave been ligated distally and following the jugularbulb through the foramen and down to the dividedjugular vein is straightforward. Venous back bleed-ing from the inferior petrosal sinus can be contro l l e dwith Avitene. Tumor attachments to the caro t i dartery as well as the surrounding nerves may re q u i resharp dissection. This puts the carotid artery atsome risk and, there f o re, it is important to havecomplete control of the vessel. Once the tumor hasbeen completely removed, complete hemostasis is
easier to obtain.
CLOSUREFollowing tumor removal, the defect in the dura mustbe closed. Watertight closure is accomplished by mo-bilizing a vascularized portion of the temporalis mus-cle and fascia and sewing it to the dural defect with arunning suture. Fascia lata may be used if necessary;h o w e v e r, vascularized tissue is pre f e r red. Non-autolo-gous materials should be avoided as they provide lesscapacity for watertight closure and carry a higher riskof infection. Fibrin glue may be used to re i n f o rce thisc l o s u re, although its benefit is questionable. Fat har-vested from the thigh can be used to fill any openspace from the temporal bone dissection (Figure 10).
The eustachian tube is sealed using a piece oftemporalis muscle. The temporomandibular joint isre a p p roximated with microplates. The stern o c l e i d o-mastoid muscle is re a p p roximated at its site of originwith interrupted sutures. A subfascial drain is oftenhelpful for at least the first 48 hours. The scalp flapis re a p p roximated with subgaleal sutures, followedby staples for the skin.
A spinal drain is left in place for approximately 5days. Continuous drainage is best avoided in favor ofi n t e rmittent drainage of 12 to 15 cc of CSF every 2hours. The drain is clamped in between draining toavoid overdrainage.
COMPLICATIONSMajor complications include facial nerve and lowercranial nerve palsies, most of which are transient. Ift h e re is obvious damage to the facial nerve durings u rgery, an interposition graft with the greater auric-ular nerve or a direct re-anastomosis may be per-f o rmed. If there is significant vagus nerve palsy, amedialization pro c e d u re or Teflon injection may benecessary. Following a labyrinthectomy, the patientno longer has the capacity for hearing.
CSF leakage can be a problem and is best pre-vented by the meticulous use of layered closure anda spinal drain. Because of the length of the pro c e-d u re and the potential for open space around thetemporal bone, infection is common. Althoughunusual, there is always risk of catastrophic injuryto the carotid artery which could result in a stroke.

INTRODUCTIONE s t h e s i o n e u roblastomas, or olfactory neuro b l a s t o-mas, are uncommon tumors constituting 3% of allintracranial neoplasms. They are derived from then e u roepithelial sensory cells of the olfactory mucosa.They usually arise in the nasal vault, presenting asnasal masses. These tumors are locally aggre s s i v eand invade the paranasal sinuses, nasopharynx,palate, orbit, or the basicranium. In 20% to 25% ofcases, they produce neurological symptoms due tointracranial invasion. When present in the nasal cav-ity, the common findings are nasal obstruction andepistaxis. However, the intracranial masses pre s e n twith anosmia and signs and symptoms of raisedintracranial pre s s u re (ICP) or proptosis and visualdefects once they invade the orbit. The disease mayalso begin with the signs of a brain tumor or menin-gitis. Esthesioneuroblastomas are often slow-gro w-ing tumors and have a tendency to metastasize toregional lymph nodes and the lung. Regional cervicalmetastases are known to occur in 10%-40% of cases,even after a silent period lasting years; distant me-tastases in the lung, bone, liver, mediastinum, andspleen occur in 8% of cases.
No definite correlation between the histologicalgrading of these tumors and the biological behavior
SURGICAL MANAGEMENT OFE S T H E S I O B L A S T O M A S
RAMESH PITTI BABU, M.D.MARK S. PERSKY, M.D.
143
is known; rather it is the location and extent of thetumor at the time of the diagnosis that appear tobear a direct relation to the pro g n o s i s .
Management of these tumors is primarily surg i-cal. Although they have a certain degree of radiosen-sitivity, esthesioneuroblastomas tend to recur afterradiotherapy. The role of chemotherapy in the man-agement, either as primary treatment or as an adju-vant, remains to be evaluated.
RADIOLOGICAL EVALUATIONComputed tomography (CT) and magnetic re s o n a n c eimaging (MRI) are the two most valuable diagnostictools in evaluating this disease. CT with bone algo-rithms shows the extent of bone destruction (Figure1), and MRI, with and without gadolinium en-hancement, serves to detail the location and extentof submucosal spread of the tumor and define duralinvolvement (Figure 2). In large tumors, CT of theparanasal sinuses demonstrates the entire extent ofthe disease process, the obstruction of paranasalsinus outlets, and the destruction to the bone (Fig-u re 3). A three-dimensional CT with bone windowswould show the defect in the skull base; the studyhelps plan reconstruction of the skull base. In MRI,these tumors are hypointense on T1-weightedimages and enhance with contrast. The diff e re n t i a ldiagnoses include hemangiopericytoma and olfactoryg roove meningioma. Tumors with intracranial exten-sion associated with cysts in the peritumoral are aa re often diagnostic of esthesioblastomas. In larg etumors, magnetic resonance angiography and/or© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8144
conventional cerebral angiography are necessary tod e t e rmine the vascularity of the tumor and the dis-placement of the major intracranial vasculature. Inselective cases, the work-up should include a com-plete skeletal survey complemented with a bone scanto detect the metastatic spread to the skeleton.
PREOPERATIVE CONSIDERATIONSP resentation, Clinical Evaluation, and Patient SelectionE s t h e s i o n e u roblastoma most frequently occurs inpatients 40-60 years of age. However, a second peakis noted in persons aged 10-20 years. Caucasians arem o re commonly affected than Blacks. These tumors
F i g u re 1. C o ronal section of CT with bone algorithm demonstrating the extent of bonedestruction caused by the esthesioneuro b l a s t o m a .
F i g u re 2. MRI with gadolinium enhancement in sagittal ( A ) and coronal ( B ) views verifies the location and submucosal spread of the tumor.
A B

BABU AND PERSKY : SURGICAL MANAGEMENT OF ESTHESIOBLASTOMAS 145
a re slow growing and remain asymptomatic for along time, except for a few episodes of epistaxis andnasal obstruction, as long as they are confined to thenasal cavity. Although between 19% and 47% ofpatients have neurological complications associatedwith the disease, only 7% have primary symptoma-tology referable to the nervous system; 70% have rh i-nological complaints, hence, the initial evaluation isoften done by an otolaryngologist. Radiological stud-ies are warranted in patients with the above symp-toms and clinical evidence of nasal polypoid masses(especially unilateral). At times, either a direct endo-scopic or open biopsy is necessary for the diagnosisprior to definitive surgery. A thorough examination ofthe neck to rule out cervical lymphadenopathy or awork-up for distant metastases, possibly in thelungs, is undertaken along with a routine generalmedical preoperative evaluation.
Treatment ChoiceT h e re is an ongoing debate as to the optimal methodof treatment. When large series are critically evalu-ated, surgery and radiation seem to offer a similarbenefit, particularly in small intranasal tumors. Inl a rger tumors, radiation alone or radiation prior tos u rgery appears to yield less favorable results than
combined craniofacial surgery and postoperativeradiation. Currently, the approach is multidiscipli-nary and multimodality based.
For optimal treatment planning, the tumor shouldbe staged based on the classification proposed byKaddish and coworkers (Figure 4):
Stage A: Tumor confined to the nasal cavity.Stage B: Tumor in the nasal cavity with extension to
one or more paranasal sinuses.Stage C: Tumor extending beyond the nasal cavity
into the orbit and/or the intracranial cavity, cervi-cal lymph nodes, or distant structure s .
In Stages A and B craniofacial resection with post-operative radiation has been found to give the bestt u m o r- f ree survival time; however, it is a matter ofdebate whether radiotherapy prior to surgery orpostoperatively (even in the absence of re s i d u a ltumor) is useful. Some oncologists favor using radio-therapy as the sole treatment. However, for Stage Ct u m o r, the consensus is to perf o rm a craniofacialresection with the addition of radiotherapy andchemotherapy (cyclophosphamide and vincristine)for distant metastases, although all tumors re s p o n dto radiation. Since local re c u r rence is as high as 60%in patients treated with radiotherapy followed byextracranial surgery, we feel that in all stages (A, B,and C) craniofacial resection is necessary, as there isonly a 12% re c u r rence. The term “cure” in these pa-tients is to be used with caution because 50% of thepatients who are survivors eventually succumb tore c u r rent or metastatic disease.
Radical tumor dissection or any of its modifica-tions followed by postoperative radiation is war-ranted for clinically evident neck metastases.
The Role of BiopsyA correct preoperative diagnosis is crucial in lesionsconfined to the nasal cavity with either minimal or no intracranial extension. Hemangiopericytoma, lym-phoma, plasmacytoma, undiff e rentiated squamouscell carcinoma, oat cell carcinoma, melanoma, em-bryonal rh a b d o m y o s a rcoma, and aggressive invertingpapilloma are some of the tumors considered in thed i ff e rential diagnosis.
Transnasal biopsy with the patient under localanesthesia is easily perf o rmed. The results of the bi-opsy help in planning for definitive treatment. Al-though routine hematoxylin-eosin staining is helpfulin diagnosis, further clarification is obtained by elec-t ron microscopy and immunohistochemical studies.
OPERATIVE TECHNIQUEE s t h e s i o n e u roblastomas presenting at the anteriorskull base pose a surgical challenge; they are man-aged via a combined craniofacial or rh i n o - n e u ro s u r-gical approach. Some surgeons advocate a form of
F i g u re 3. C o ronal section of CT with contrast en-hancement showing the full extent of the diseasep rocess as well as obstruction of the paranasal sinuso u t l e t s .

transfacial exposures such as lateral rhinotomy, eth-moidectomy, and medial maxillectomy for tumorsthat do not extend intracranially or do not involvethe cribriform plate. However, a combined transfacialand transcranial approach is necessary becauset h e re is microscopic infiltration of the cribriformplate and olfactory bulbs, even in small tumors.
P reoperative Preparation and Anesthetic ConsiderationsStarting at midnight prior to surgery, the patients aregiven 250 mg intravenous Solu-Medrol every 6 hours.The day prior to surgery, patients are given a loadingdose of 1 gm Dilantin, which is continued after sur-gery at 100 mg three times a day. If sedation is de-s i red, one of the shorter-acting benzodiazepines suchas diazepam or midazolam is administered on call tothe operating room. Narcotics should be avoided be-cause of their tendency to produce respiratory de-p ression and/or nausea and vomiting, which in turncan result in increased ICP. Routine monitoring inthe operating room consists of pulse oximetry, con-
tinuous blood pre s s u re measurement, electro c a rd i o-graphy, and capnography. Capnography assesses thelevel of hyperventilation and is titrated to obtain opti-mal ICP control. An arterial catheter and one or twol a rg e - b o re intravenous lines are inserted. A short-act-ing opioid and ultrashort-acting intravenous anes-thetic (generally thiopental or propofol) are used forinduction, followed by a nondepolarizing muscle re-laxant for intubation. Intravenous lidocaine, 1.0-1.5mg/kg body weight, may be useful prior to laryn-goscopy. A combination of these agents permits asmooth induction of anesthesia, thus avoiding hyper-tension, hypoxia, hypercarbia, and coughing, all ofwhich may increase ICP. The hypertensive re s p o n s eto pin fixation of the head may be minimized or elimi-nated by the prior administration of an intravenousanesthetic.
Anesthesia is generally maintained with a nar-cotic by infusion or by nitrous oxide and isoflurane.The PaCO2 is maintained in the range of 25 to 30mm Hg. Controlled hypotension may be desired dur-ing surgery to reduce blood loss and the need for
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8146
F i g u re 4. The Kaddish tumor staging process, frontal ( l e f t ) and lateral ( r i g h t ) views, assessing the extent of tumor. Appro p r i-ate treatment planning follows staging. A = tumor confined to the nasal cavity; B = tumor in the nasal cavity extending toone or more paranasal sinuses; C = tumor extension beyond the nasal cavity into the intracranial compartment.

BABU AND PERSKY : SURGICAL MANAGEMENT OF ESTHESIOBLASTOMAS 147
transfusion. A mean arterial pre s s u re of 50 to 60mm Hg is acceptable in a healthy individual, butmay not be tolerated by a patient with card i o v a s c u-lar disease or hypertension. In highly vasculartumors, deliberate hypotension may be induced byi n c reasing the level of isoflurane or by a dire c t - a c t i n gv a s o d i l a t o r, such as sodium nitroprusside or nitro-glycerine. After intubation, the bladder is catheter-ized, the table padded, and 20% mannitol is givenintravenously (1 gm/kg body weight).
Patient PositioningPrior to positioning the patient, a tunneled lumbardrain is placed; cere b rospinal fluid (CSF) is notdrained unless necessary for brain retraction durings u rgery. Venodyne pneumatic compression boots areapplied with their use continued into the postopera-tive period. The patient is then placed in the supineposition. All pre s s u re points are well padded. Thehead is slightly extended and fixed to the bed aftersecuring it in a three-pin Mayfield headholder, with-out any side-to-side tilt. The entire head and face up
to the upper lip is thoroughly prepped with Betadinescrub and solution and draped. Prior to the Betadinep rep, a temporary tarsorrhaphy using 6-0 nylon isundertaken. The right quadrant of the abdomen isalso prepped and draped for harvesting the fat graftat a later stage.
Skin IncisionA high bicoronal skin incision within the hairline atleast 13 cm from the root of the nose and a separatelateral rhinotomy incision are marked as shown inF i g u re 5. This long skin flap is necessary to obtainan adequate pericranial graft. In the case of a larg et u m o r, it is safer to deal with the intracranial portioninitially, defining the tumor and protecting the brain;otherwise, any brain herniation through the skullbase might cause injury to the brain pare n c h y m aduring the rhinological portion of surgery. The pro-posed line of incision is infiltrated with 1% lidocainewith epinephrine. The skin is incised and the bleed-ing skin edges are controlled with Raney clips. Theposterior edge of the cut skin is lifted with hooks,and subcutaneous dissection is carried out 2 to 3inches behind the line of the incision. Using a #11blade, the pericranium is cut right to the bone. Thusobtained (at least 2 to 3 inches longer than the skinflap), the pericranium is later used to cover the ante-rior cranial fossa during the re p a i r. The pericranium,along with the thin layer of fascia on the temporalismuscle (which is located superficial to the temporalisfascia), is stripped and reflected along with the skinup to the nasion, exposing both of the supraorbitalridges and held retracted until the end of surgery.
Craniotomy and Supraorbital OsteotomyInitially, a low frontal craniotomy is perf o rmed usingthe Midas Rex drill. It is necessary to raise a lowf rontal bone flap but not a large one. Two burr holesa re placed just above the supraorbital ridges on thelateral aspect (“keyholes”) and another burr hole isplaced exactly in the midline just anterior to thec o ronal suture. Special attention is paid while theburr hole is drilled near the frontal sinus. When theburr hole is made, the surgeon may decide to stopafter penetrating the outer wall of the frontal sinusand use the Midas Rex drill to cut the bone. Thistechnique could cause a tear of the dura and/or thesuperior sagittal sinus. Instead, it is better to drillthe inner wall of the frontal sinus as well, separatethe dura and sagittal sinus from the overlying bone,and use the side-cutting Midas Rex drill to completethe craniotomy. The frontal sinuses entered in thesee x p o s u res are obliterated and re p a i red at the end ofthe surgery to prevent potential CSF leak or the for-mation of mucoceles. One can also raise the boneflap in two pieces. The first piece comes up almost tothe midline, then the superior sagittal sinus is sepa-
F i g u re 5. The skin incisions (dotted lines) for resection ofe s t h e s i o n e u roblastomas, including a high bicoronal incisionbehind the hairline (which is at least 13 cm from the root ofthe nose) as well as a separate lateral rhinotomy incision.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8148
rated from the bone; later the second piece isremoved from the other side. This would avoid injuryto the superior sagittal sinus and provide excellentcosmetic results. After the frontal bone is re m o v e d ,the addition of a supraorbital osteotomy, at least onone side, will minimize the need for brain re t r a c t i o n ,especially in large tumors (Figure 6). In giant tumors,which occupy the anterior cranial fossa aboutequally from the midline, bilateral supraorbital os-teotomies are necessary. Prior to the osteotomy, thesupraorbital nerve is released from the notch using aCottle elevator. If the notch is converted into a fora-men, the rim of the foramen on either side is bro k e nwith a small osteotome and the nerve is re l e a s e d
t o w a rd the orbit along with the periorbita which, int u rn, is sharply separated from the inner surface ofthe orbit.
Resection of Tu m o rTwo horizontal incisions are made in the dura alongthe floor of the anterior cranial fossa up to the mid-line, and two rubber dam cottonoid patties are ap-plied on the surface of the brain next to the midlineand retracted posteriorly. This exposes the falx andu n d e r s u rface of the superior sagittal sinus. Thesinus is divided between two 2-0 silk ligatures. Thef rontal lobes are retracted back, exposing the cribri-f o rm plate and the olfactory bulbs (Figure 7).
F i g u re 6. After the craniotomy, a supraorbital osteotomy is perf o rmed. This is particularlynecessary with large tumors.
line of pericranialincision
craniotomy
supraorbitalosteotomy
skin reflected

BABU AND PERSKY : SURGICAL MANAGEMENT OF ESTHESIOBLASTOMAS 149
In extracranial tumors or tumors with minor intra-cranial extension, the olfactory nerve filamentsshould be microdissected and excised at the time ofremoval of the intranasal component of tumor. Thisshould be done even in the absence of CT evidence ofintracranial involvement, to prevent re c u r rence of thet u m o r, because of its origin from olfactory epithelium.After resection, a routine closure is undertaken.
In medium-sized tumors, resection is carried outpiecemeal. Pro g ressive intratumoral decompre s s i o nand shrinkage of the tumor with bipolar coagulationunder constant irrigation would separate the tumorf rom surrounding compressed brain and open thesubarachnoid space. Once partial decompression isaccomplished, the base of the tumor at the cribri-f o rm plate is managed. The ethmoidal feeding arter-ies are generally found in this area. They are cauter-ized and cut, and the intranasal part of the tumor isre m o v e d .
In giant tumors, the dura is attached to the sur-face of the tumor; in order to obtain a satisfactoryresult, the dura (along with the tumor) is re s e c t e d .Giant tumors could extend posteriorly and pre s supon the optic nerves and anterior cerebral arterycomplex. Pro g ressive extra-arachnoidal debulking ofthe tumor would create a peritumoral space, avoid-
ing injury to the arachnoid toward the brain side.After tumor resection, it is important to resect theolfactory nerve filaments and bulbs.
Resection of the Cribriform Plate and PlanumIf the tumor has extensively penetrated the skull base,then en bloc resection of the cribriform plate, the eth-moid sinuses, and a portion of the planum sphe-noidale including both the olfactory bulbs with theirfilaments is attempted. En bloc resection can beachieved either by drilling at the tumor margins ort h rough saw cuts. If saw cuts are pre f e r red, cut at theglabella parallel to the anterior cranial fossa. A secondcut just behind the cribriform plate approximately 2.5cm from the root of the nose and two lateral cuts oneither side of the cribriform plate will surround thetumor and avoid injury to the optic nerves. Occasion-ally, in patients with extensive tumors presenting withpoor vision, unroofing the optic nerves from the chi-asm to the orbital apex, either unilaterally or bilater-ally with the resection of the entire planum betweenthe nerves, is undertaken. The cut margins are exam-ined to ensure that they are tumor free. Orbital exen-teration is necessary only if the tumor extends beyondthe periorbita into the orbit.
We advised earlier to complete the intracranial
F i g u re 7. The cribriform plate and the olfactory bulbs are exposed, while the frontal lobes areretracted back, just prior to tumor resection.
anterior cranialfossa
frontal loberetracted
cranial nerve II
intracranialtumor
eye globe

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8150
portion of resection before the rh i n o s u rgical portion;h o w e v e r, in massive tumors, it is easier and safer tohave the otolaryngologist and the neuro s u rgeon workin concert so that the neuro s u rgeon, after pro t e c t i n gthe frontal lobes with rubber dam cottonoid pattiesand placing retractor blades, should be able to pushthe tumor through the cribriform plate so that theotolaryngologist can remove it from below thro u g hthe nose. Because these tumors are notorious fortheir re c u r rence, total gross surgical resection with-out causing undue complications should be the goal.
Lateral RhinotomyAn incision is made from the inferior medial third ofthe eyebrow along the lateral nasal area and aro u n dthe base of the ala nasi (Figure 5). The soft tissuesa re elevated in a subperiosteal plane to expose thenasal bone, the frontal process of the maxilla, andthe maxillary process of the frontal bone. If wide ex-p o s u re of the anterior superior nasal cavity is neces-sary, a lateral nasal osteotomy extending into thenasal cavity is perf o rmed. The nasal bone is re p l a c e dusing miniplates at the end of the pro c e d u re. Themedial orbit is then dissected in a subperiorbitalfashion to the orbital apex. The medial canthal liga-ment is mobilized without disrupting it. The naso-lacrimal duct is sharply transected and the anteriorand posterior ethmoid arteries are bipolar cauterizedand transected. Identification of the fro n t o - e t h m o i d a ls u t u re indicates the border between the anterior cra-nial fossa above and the ethmoid cavity below. Acomplete anterior and posterior ethmoidectomy andsphenoidectomy are done; the lacrimal bone andlamina papyracea are resected. Adequate tumor ex-p o s u re is now obtained. Large tumors may re q u i re amedial maxillectomy. The medial third of the orbitalfloor can also be resected without need for subse-quent reconstruction. The orbital roof is resected asnecessary; this is safely perf o rmed since the fro n t a llobe has been retracted via an intracranial approach.
RECONSTRUCTION AND REPAIRRepair of Frontal SinusPrior to reconstruction, the frontal sinus is re p a i re d .Initially, it is cranialized and the mucosa is thor-oughly removed. The interior of the sinus is thendevascularized by cauterizing it with a Bovie coagu-lator and is filled with Gelfoam soaked with baci-tracin powder. Later, a piece of muscle that has beenharvested from the temporalis muscle is placed andglued down using fibrin glue. Lastly, the pericranialflap is turned to cover the sinus.
Reconstruction of Anterior Cranial FossaAfter en bloc resection, the floor of the anterior cra-nial fossa is re p a i red. Three layers of grafting areused. The bottom-most layer is the bone graft, the
second layer is the fat graft, and the third layer is thevascularized pericranial flap (Figure 8). The bonydefect in the anterior cranial fossa could be left alone,but we advocate repairing the floor with a split-thick-ness bone graft obtained from the craniotomy flap.This would act as a bridge, preventing herniation ofthe frontal lobes and sagging of the soft tissue layersplaced on the floor. However, some surgeons dorepair it with a methylmethacrylate mold. A primarilywatertight dural closure is not possible; hence, clo-s u re of the dura using either cadaver fascia lata orautologous temporalis fascia should be undertaken.To further achieve a tight seal, a fat graft obtainedf rom the abdominal wall is placed on the floor overthe bone graft. At this stage, the vascularized pericra-nial flap is separated from the skin and laid down onthe floor over the fat graft. This flap is also tackeddown with 4-0 Nurolon to the posterior end of thedura of the anterior cranial fossa. The suture linesand the tissue grafts are routinely sealed by fibringlue. In reoperations or in the absence of a stro n gpericranium, the floor is covered with vascularizedtemporalis muscle; the free rectus abdominus flaphooked to the superficial temporal artery (with thehelp of a plastic surgeon) may be used. Postopera-tively, a lumbar drain is routinely used for 5-7 days.Repair of the cribriform plate from the nose is accom-plished using fat and full-thickness grafts of the skinand subcutaneous tissue placed on a gelatin sponge;keeping the raw surface upward toward the intracra-nial cavity and packing with iodoform gauze impre g-nated with bacitracin ointment gives the best re s u l t sof re p a i r. The nose is then sewn back in position.
POSTOPERATIVE CAREAll patients are maintained on antibiotics, pre f e r a b l y500 mg vancomycin every 6 hours and 80 mg to-bramycin or gentamycin administered intravenouslyevery 8 hours, until the drains and packing are re-moved. Alternatively, Unasyn can be used. If nodrains are placed, antibiotics are given for a period of48 hours. Patients are also continued on 100 mgDilantin three times a day. Bed rest is re q u i red untilthe lumbar drain is removed, and the patient shouldbe carefully monitored for any signs or symptoms ofCSF leak through the nose. This potential problem ishopefully prevented via a lumbar drain for 5-7 days,after all layers of repair are stuck down and wellhealed. CSF, 50 to 60 cc every 8 hours, is drained. Inr a re instances, it is necessary to seal the leak via atransfacial, transsphenoidal approach by packing thesphenoid sinus. After the spinal drain is removed, thepatient is mobilized. While on bed rest, the patient isgiven 5000 U heparin subcutaneously administere devery 8 hours, beginning 72 hours after surgery. Nasal packing is removed on the 7th postopera-tive day.

BABU AND PERSKY : SURGICAL MANAGEMENT OF ESTHESIOBLASTOMAS 151
COMPLICATIONSOperative complications include injury to the ante-rior cerebral artery complex and the optic nerves,especially when the tumors are large. Care is exer-cised during dissection of the posterior aspect of the tumor to avoid these structures. During tumorresection, one should not violate tumor- a r a c h n o i di n t e rface. Bilateral frontal lobe damage, either due toexcessive retraction or to inadvertent injury duringtumor removal, may result in serious cognitive pro b-lems. Supraorbital osteotomy and good anestheticbrain relaxing technique would help to avoid theseknown complications. Other complications includemeningitis secondary to CSF leak and the develop-ment of meningoencephalocele or mucoceles. As
mentioned earlier, all of these complications can beavoided by strict adherence to the re p a i r, re c o n s t r u c-tion principle, and postoperative care .
FOLLOW UP, PROGNOSIS, AND SURVIVALThe 5-year survival rate ranges from 18% to 71%.Survival depends on the size of the tumor, intracra-nial extension, and lymph node involvement. In pa-tients with Stage C disease, the 5-year survival isreported in the range of 60%, while with Stage A it is almost 100%. Postoperatively, these patients arec a refully followed by CT or MRI about every 6months. In suspicious cases, endonasal endoscopy isp e rf o rmed and any re c u r rence is appropriately man-aged by either surgery or adjuvant therapy.
F i g u re 8. Illustration demonstrating complete repair of the anterior cranialfossa, which is carried out after the en bloc resection. The bottom-most layerconsists of the bone graft, the middle layer consists of the fat graft, and the toplayer is the vascularized pericranial flap.
pericranial flap
fat graft
bone graft


INTRODUCTIONBrainstem gliomas re p resent approximately 10% ofpediatric brain tumors, but are rare in adults. As ag roup, these tumors have a poor prognosis and areassociated with a 30% 5-year survival rate. However,it has become clear that brainstem gliomas are ah e t e rogeneous group of tumors in re g a rd to biologi-cal behavior and surgical accessibility. Certainly,some categories of brainstem gliomas possess a low-grade pathology and have a better prognosis. Inaddition, with modern imaging and technicaladvances, many of these tumors re p resent surg i c a lchallenges that can be overc o m e .
A very important tool in the surgical managementof brainstem gliomas is magnetic resonance (MR)imaging. This makes it possible to identify the pre-cise anatomical location of the neoplasm. In con-junction with the clinical picture, MR imaging allowsone to know the pathology of the tumor with somed e g ree of certainty. Thus, therapeutic decisions, in-cluding those re g a rding the surgical management ofbrainstem gliomas, can be made based on character-istic MR images.
PATIENT SELECTIONPatient selection is vital to the successful surg i c a lt reatment of brainstem gliomas. The most re w a rd i n gs u rgical outcomes will be in patients who harbor
SURGICAL TREATMENT OF BRAINSTEM GLIOMAS
MARK R. LEE, M.D., PH.D.MICHAEL COWAN, M.D.
153
low-grade tumors that displace rather than infiltraten o rmal brainstem structures (Figure 1). In addition,patients who are most able to withstand the surg i c a lmanipulation of brainstem structures are those whohave not yet been injured by their tumor; thus,s u rgery early in the disease course is preferable tos u rgery late in the disease course.
T h e re is a subgroup of patients with diffuse brain-stem tumors in whom surgical intervention plays norole. These patients typically present with a veryshort history (a duration of weeks) of pro g ressive cra-nial nerve palsies and gait ataxia. MR imaging re-veals an expanded brainstem throughout, with dif-fuse infiltration by neoplastic cells as evidenced by amarked increase in signal on T2-weighted images ofthe pons and the medulla. Because these tumors dif-fusely infiltrate normal brainstem structures, re s e c-tion of any portion of the tumor also involves re m o v a lof functional brainstem tissue. These tumors behavequite aggressively and the patient’s prognosis is dis-mal. The histology typically is anaplastic astro c y-toma or glioblastoma multiform e .
Focal brainstem tumors, on the other hand, areamenable to surgical resection, especially those withan exophytic component. Because these tumors arevery slow-growing, patients typically present with along history (years) of a mild cranial nerve palsy andoccasionally with long-tract signs. MR imaging re-veals a focal tumor that frequently enhances withgadolinium contrast. As noted above, the tumoroften has a large exophytic component. The gro w t hp a t t e rn of these tumors suggests that they re s p e c tanatomical boundaries and they remain restricted tothe “compartment” of the brainstem from which they© 1999 The American Association of Neurological Surg e o n s

originated (e.g., in the medulla). These tumors be-have in a fairly indolent manner until they reach acritical mass, at which time the clinical course mayaccelerate. The histology typically is low-grade astro-cytoma, juvenile pilocytic astrocytoma, or morer a rely ganglioglioma. Focal or exophytic brainstemgliomas typically displace and compress norm a lbrainstem structures. This characteristic, coupledwith their low-grade pathology and slow growth, canmake these lesions amenable to complete surg i c a lresection and possible cure .
PREOPERATIVE PREPARATIONAll patients should undergo preoperative MR scan-ning with contrast enhancement. Not only does thisp rovide for anatomic localization of the tumor and itsrelationship with normal structures, it also pro v i d e sfor a baseline study in which to judge the efficacy ofthe operation. It is unusual for patients with brain-stem gliomas to suffer from hydrocephalus, andt h e re f o re cere b rospinal fluid (CSF) diversion is rare l yan issue.
Routine laboratory studies including a completeblood count with diff e rential, pro t h rombin time, andpartial thromboplastin time are obtained. The pa-tient is typed and cross-matched for two units ofpacked red blood cells. The patient’s hair is sham-pooed with antiseptic soap the night before surg e r y .
Patients receive 10 to 20 mg of dexamethasoneintravenously every 6 hours starting at midnightb e f o re surgery. In addition, 10 to 20 mg of Pepcid(famotidine) is given intravenously at midnight. Pro-phylactic antibiotics (usually a first-generation ceph-alosporin) are given the morning of surgery, earlyenough to obtain a therapeutic tissue level at thetime of incision.
OPERATIVE TECHNIQUE
A n e s t h e s i aThe patient is induced with intravenous Pentothaland intubated in the supine position. Although notessential, it may be worth a discussion with the anes-thesiologists as to the merits of using an “arm o re d ”
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8154
F i g u re 1. An illustration of a partially exophytic focal medullary tumor. The tumor displaces thelower cranial nerve motor nuclei anterior to the tumor rather than infiltrating normal brainstems t r u c t u re s .

LEE AND COWAN : SURGICAL TREATMENT OF BRAINSTEM GLIOMAS 155
endotracheal tube. We frequently use one to pre v e n tthe collapse of the endotracheal tube that occasion-ally occurs with aggressive flexion of the patient’sneck to obtain optimal suboccipital exposure duringpositioning. Patients are generally maintained withinhalation anesthesia consisting of Forane andn i t rous oxide. Supplemental intravenous fentanyl isalso administere d .
An intra-arterial line is placed to monitor bloodp re s s u re and blood gas levels. There is no need forhyperventilation since early in the course of the pro-c e d u re, the cisterna magna is opened with release ofCSF and resulting relaxation of the posterior fossa.
Patients undergoing brainstem surgery re q u i restrict hemodynamic monitoring. It is not unusual tonote wide fluctuations in blood pre s s u re and heartrate during tumor dissection and removal. Ty p i c a l l y ,the patient will become either hypertensive or brady-c a rdic, and it is essential that the anesthesiologist bep re p a red for pharmacological intervention if neces-sary. If hemodynamic changes are encountere d ,tumor dissection and manipulation should be haltedtemporarily. The hemodynamic instability usuallys e l f - c o r rects, allowing for the pro c e d u re to continue.
Patient PositioningThe patient is placed in a pinned headholder (eitherMayfield or Sugita) and is turned to the prone posi-tion onto two gel chest rolls. The arms are tucked onthe sides under the sheets. The headholder is at-tached to the operating table with the neck moder-ately flexed and the chin pulled posteriorly. Thisgives excellent exposure of the suboccipital re g i o n( F i g u re 2A). The operating table is placed in re v e r s eTre n d e l e n b u rg position until the posterior neck andinion are parallel to the ground. In children underthe age of 3 years, a horseshoe-shaped headholder isused instead of a pinned headholder. In this case,c a re is taken to protect the eyes. Unfortunately, opti-mal exposure of the suboccipital region is diff i c u l twithout a pinned headholder.
An alternative method of positioning patients forthis operation is the sitting position. However, notonly is there a risk for air embolism, but there arealso major concerns re g a rding adequate cere b r a lp e rfusion during times of hemodynamic instabilityb rought on during the tumor surgery. There f o re, wedo not advise the sitting position for brainstemglioma surg e r y .
Incision and OpeningWe typically do not shave the patient’s hair, but planfor the incision in a midline part. If a patient’s hair istoo short to comb, we will shave a small strip. Theincision line is infiltrated with 0.5% lidocaine with1:200,000 epinephrine. After the usual prep anddrape, an incision is made from several centimeters
above the inion to the palpated spinous process ofC2 or C3, and taken down to the pericranium of theocciput and the fascia of the nuchal muscles (Figure2B). The fascia is cut on the midline with Bovie cur-rent and taken down to the cranium, the arch of C1,and the spinous process of C2. Care must be takenwhen cutting down on the midline of the arch of C1since this can be cartilaginous, especially in youngerc h i l d ren. The nuchal muscles are dissected in a sub-periosteal manner utilizing Bovie current on the sub-occipital cranium and a combination of blunt andsharp dissection on the foramen magnum and thea rch of C1. There is no need to perf o rm further mus-cle dissection on C2 unless a laminectomy is re-q u i red for resection of the cervical portion of somebrainstem gliomas.
An oval-shaped burr hole is then created on themidline just below the inion. Typically, an air- p o w-e red drill with an “acorn-shaped” bit is utilized. Itshould be re m e m b e red that a “keel” of bone verycommonly exists on the midline in the posteriorfossa. There f o re, when drilling one must be awarethat the bone thickness will vary widely over thesmall area of the burr hole, and violation of the duracould occur if care is not taken. After exposure of thedura, the burr hole is enlarged with a curette and thedura is widely stripped with a #3 Penfield. Attentionis then turned to the foramen magnum where theperiosteum, which melds into the outer leaf of dura ofthe posterior fossa, is cut widely utilizing a curette. Asmall amount of bleeding may be encountered at thispoint from the marginal sinus, which can be easilyc o n t rolled with Gelfoam soaked in thrombin. Thedura is again widely stripped at the foramen magnumwith a #3 Penfield. A bone flap is then created utiliz-ing a craniotome. Bone cuts are made from the burrhole, bringing them laterally and then inferiorly anddiagonally toward the foramen magnum to make a“heart-shaped” craniotomy (Figure 3). The bone flapis elevated with a #3 Penfield. There is no need to ex-pose the transverse sinus. The lateral edges of theposterior rim of the foramen magnum are re m o v e dusing rongeurs. The posterior arch of C1 is not re-moved except in cases where the brainstem tumorextends into the cervical spinal cord .
After epidural hemostasis is obtained, attention ist u rned to the dural opening. A small dural opening ismade with a #11 blade at one of the upper corners ofthe craniotomy. Using Metzenbaum scissors, thedural opening is continued diagonally to the midlineat the craniocervical junction. Care is taken not toc ross the midline occipital sinus or the usually pre s-ent marginal sinus. This is repeated on the oppositeside. Two Ligaclips are placed across the occipitalsinus, and the sinus is divided at the base of the twodiagonals. If the marginal sinus is significant, twoLigaclips are placed across it on the midline. The

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8156
F i g u re 2. A, patient positioning. The patient is placed in the prone position on two gelchest rolls. The head is fixed with a pinned head clamp and attached to the operating tablewith the neck moderately flexed; the chin is pulled posteriorly to give good exposure of thesuboccipital region. B , a skin incision is made from several centimeters above the inion tothe palpated spinous process of C2 or C3. The hair is not shown for illustrative purposes.
F i g u re 3. A suboccipital craniotomy. A high-speeddrill is utilized to create an oval-shaped burr holeover the midline. One must be aware of the varyingbone thickness because of the midline “keel.” Afterstripping the dura at the foramen magnum, twobone cuts are made, creating a “heart-shaped”craniotomy (dotted lines). Any remaining bone ofthe posterior foramen magnum is removed withrongeurs (also shown with dotted lines) .
F i g u re 4. Dural opening. A “ Y ”-shaped duralopening is created. When cutting across theoccipital and marginal sinus, Ligaclips may needto be placed to control bleeding. After cutting thedura, the superior and lateral flaps are suture dout of the field.
A B

LEE AND COWAN : SURGICAL TREATMENT OF BRAINSTEM GLIOMAS 157
dural opening is then completed, bringing a finallimb inferiorly on the midline in the upper cervicalregion. The dural opening appears as a “Y” ( F i g u re 4).The three corners are sutured and tacked laterallyand superiorly. If not already violated during thedural opening, the cisterna magna should be openedat this time to allow for release of CSF and re l a x a t i o nof the posterior fossa.
The degree and method of magnification duringthe remainder of the operation depend on the individ-ual surgeon. However, we elect to bring in the operat-ing microscope at this time and perf o rm the re m a i n-der of the operation under microscopic illumination.
Tumor ExposureTo provide adequate exposure of the fourth ventricle,the inferior half of the vermis is split. Initially, theretractors from the system of choice (we use eitherthe Sugita or Gre e n b e rg systems) are placed to splitthe tonsils and provide good exposure of the inferiorv e rmis. The bipolar cautery is then utilized to coagu-late the pia and veins on the surface of the verm i s .The coagulated surface is then cut with micro s c i s-sors. The corticectomy is created using bipolar coag-ulation and suction. With completely intrinsic brain-stem tumors, the floor of the fourth ventricle isf requently elevated with partial or complete oblitera-tion of the fourth ventricle. There f o re, care must betaken when removing tissue of the inferior verm i ssince the floor of the fourth ventricle can be inadver-tently violated. To help guard against this, we typi-cally split the vermis from a caudal to a craniald i rection after retracting the cerebellar tonsils. Thisallows direct visualization of the dorsal surface of theupper cervical spinal cord, which can be followed tothe obex, and the floor of the fourth ventricle as thev e rmis is split. With dorsally exophytic brainstemtumors, the tumor is usually encountered first, andthe floor of the fourth ventricle will not be identifieduntil the superior pole of the tumor has beenb re a c h e d .
Tumor ResectionFocal intrinsic brainstem tumors are completelyintra-axial; however, a portion of the tumor will usu-ally have an abnormal-appearing layer of ependymaover it where it broaches the floor of the fourth ventri-cle. This can be readily identified. This area can becoagulated utilizing bipolarity and entered using suc-tion, after which tissue is removed for pathologicalexamination. An ultrasonic aspirator is then used forthe majority of the tumor removal (Figure 5). Thesetumors are typically quite soft and suckable; there-f o re, it is advisable that the aspirator settings of lowamplitude and suction be used. Typically, these le-sions will displace brainstem nuclei either superiorly,laterally, or inferiorly (Figure 6). Although displaced,
the important nuclei will be intimately associatedwith the tumor margins, and, there f o re, it is vitallyimportant that tumor resection proceeds from theinside out (internal resection). Tumor margins arerecognized by a change in the way the tumor tissueresponds to suction. The area where there is littleresidual tumor becomes “floppy,” as if there re m a i n sa fragile capsule. The diff e rence in tissue consistencybetween tumor and brainstem causes tumor tissue topull away from brainstem tissue under light suctionwhen there is little tumor bulk left at a specific mar-gin. When this is encountered, the remainder oftumor removal should be accomplished with lightsuction and bipolar coagulation. Once white matter ise n c o u n t e red, tumor removal is complete at this mar-gin (Figure 7). Significant bleeding is uncommon andis usually easily controlled. One should be loath touse bipolar coagulation in the tumor bed unless aspecific bleeding vessel can be identified, since thiscan easily injure normal brainstem tissue. Usually,hemostasis is obtained with gentle, warm saline irri-gation, and if necessary with application of micro f i b-rillary collagen and thro m b i n .
With dorsally exophytic brainstem tumors, thetumor bulk is outside the brainstem. In fact, whenfirst reviewing imaging studies, it is common tobelieve that one is dealing with a cerebellar tumoruntil invasion of the brainstem via the floor of thefourth ventricle or the inferior and middle cere b e l l a rpeduncles is recognized. After opening the posteriorfossa as described above, we usually perf o rm a cor-ticectomy of the inferior vermis or over the dome ofthe mass of exophytic tumor coming closest to thec e rebellar cortex as defined by intraoperative ultra-sound. Upon encountering the tumor, we take sev-eral specimens for pathological examination andthen proceed with surgically defining the tumor. Lat-eral, inferior, and superior margins of the tumormust be identified and dissected from the surro u n d-ing cerebellar tissue prior to tumor debulking withthe aspirator. Continuously alternating between de-fining tumor borders and removing tumor tissueallows one to safely proceed with tumor re s e c t i o nwithout risking inadvertent entry into the brainstem.Although these tumors can be very large, with ade-quate debulking, the superior pole of the tumor canbe identified and the floor of the fourth ventriclevisualized. At this point, it is prudent to place a cot-tonoid patty over the floor of the upper fourth ventri-cle to guard against injury to the facial colliculi andto block any blood from entering the aqueduct.Working over the dome of the debulked and moremobile tumor, the tumor can begin to be amputatedat the level of the floor of the fourth ventricle, bring-ing this dissection inferiorly until the tumor hasbeen completely mobilized and removed. This allowsremoval of the tumor tissue while maintaining the

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8158
F i g u re 5. Tumor exposure and resection. A corticec-tomy is made with bipolar coagulation and suction, andthe lower half of the vermis is split. Identifying the floorof the fourth ventricle is critical. Intrinsic tumors usu-ally can be readily identified broaching the ventricularf l o o r. After tumor samples are taken for pathology, ani n t e rnal resection is perf o rmed, primarily utilizing theultrasonic aspirator.
F i g u re 6. An illustration of an intrinsic focal pontine tumor displac-ing the facial colliculi (abducens nuclei) inferiorly and laterally.
F i g u re 7. View of the floor of the fourth ventricle aftertumor resection and hemostasis have been achieved.

LEE AND COWAN : SURGICAL TREATMENT OF BRAINSTEM GLIOMAS 159
orientation of the normal brainstem tissue. It ise x t remely important that the small amount of re s i d-ual tumor tissue which may invade the brainstem isnot chased below the level of the floor of the fourthventricle, as this can lead to permanent injury of themotor nuclei of the lower cranial nerves.
C l o s u reAt completion of the tumor resection, the tumor bedis irrigated with warm saline, and hemostasis is as-s u red. The dura is closed with running 4-0 silk su-t u res, and the bone flap is secured with 2-0 silks u t u res. A few 2-0 Vicryl sutures are placed in themuscle to decrease the amount of “dead” space, fol-lowed with interrupted 3-0 Vicryl sutures for the fas-cia and the galea or subcutaneous tissue. The skin isclosed with a running 3-0 nylon suture. No drainsa re placed.
POSTOPERATIVE MANAGEMENTPatients with lesions restricted to the pons are extu-bated in the operating room. They are usually man-aged in the intensive care unit for about 24 hours.This is primarily for close observation and monitor-ing. At this point, they are most often fully re s p o n-sive and able to assist in their own care; they are
then transferred to the regular ward. Physical andoccupational therapy is often begun on the thirdpostoperative day to assist in their recovery. Dexa-methasone is usually tapered over 7-10 days.
Patients with lesions involving the medullaremain intubated for 72 hours. Sedation may be nec-essary to keep them comfortable. Continued intuba-tion and ventilation is a precaution against the lossof respiratory drive suf f e red by some patients 24 to48 hours postoperatively. This is probably related toedema of the medulla and leads to hypoventilation,hypoxia, and hypercarbia. Patients who do well aret r a n s f e r red to the regular ward usually 24 hoursafter extubation. Physical and occupational therapyis begun at this time. If they have an adequate gagreflex, they are fed orally. If not, a nasal feeding tubeis placed temporarily until it is no longer needed.Most patients recover their ability to swallow quicklyand do not re q u i re a percutaneous gastro s t o m ytube. Patients are maintained on high-dose stero i d s(6 to 10 mg dexamethasone every 6 hours dependingon their size) for 3 days, and then tapered over 7-10days. Skin sutures are usually removed 7-10 daysafter surgery, and most patients are discharged atthat time. Some patients may re q u i re inpatient re h a-bilitation and are usually transferred to an appro p r i-ate facility at that time.


INTRODUCTIONBrainstem gliomas have long been re g a rded as inop-erable tumors. In 1939, Bailey et al described thet reatment of brainstem gliomas as “a pessimisticchapter” in the history of neuro s u rgery. Tr a d i t i o n-ally, all tumors involving the brainstem were consid-e red infiltrative with diffuse gliomatous pro l i f e r a t i o n .B e f o re the advent of modern neuroimaging, brain-stem tumors were diagnosed using air and contrastx-ray techniques. Although these studies gave a verypoor view of the brainstem, they allowed neuro s u r-geons to recognize tumors in the brainstem and tooperate on them.
In 1967, Olivecrona described 26 patients withtumors of the medulla; of these, seven survived for 10to 25 years after an operation that comprised eitherpartial removal or biopsy and decompression. Nomention was made on whether these patients re-ceived radiotherapy. In 1968, Poole reported thre ecases of confirmed astrocytoma in the brainstem, inwhich the lesions were intrinsically solid and cystic;these patients survived for long periods. Pooleascribed this long-term survival to treatment includ-ing radiotherapy. In 1971, Lassiter et al described fivepatients with brainstem masses that were larg e l ycystic and contained mural nodules. These patientsw e re treated by uncapping the cyst, biopsy of thenodule, and postoperative radiotherapy. Again, therew e re long-term survivors among these patients. Vi l-
BRAINSTEM GLIOMASHAROLD J. HOFFMAN, M.D., F.R.C.S.(C)
161
lani, in writing about brainstem gliomas in 1975,stated that during the previous 30 years, no pro g re s shad been achieved in this field.
Brainstem gliomas are a relatively common tumorin children. Russell and Rubinstein stated that 77%of brainstem gliomas occur in patients less than 20years of age. Matson stated that 18.7% of posteriorfossa tumors were in the brainstem. Koos and Millerfound that 13% of the posterior fossa tumors theye n c o u n t e red were in the brainstem, and in my owninstitution 29% of posterior fossa tumors were lo-cated in the brainstem. A review of brainstem gliomashas indicated that 20% are dorsally exophytic intothe fourth ventricle, 50% are diffuse intrinsic tumorsthat start in the pons and spread throughout thebrainstem, 20% are focal in the brainstem, and 10%a re located in the craniocervical junction. These fourtypes of brainstem gliomas are discussed below. Mag-netic resonance images (MRIs) and operative pho-tographs are used in describing these tumors.
DORSALLY EXOPHYTIC BRAINSTEM TUMORSIn 1980 at The Hospital For Sick Children, To ro n t o ,we encountered a small but distinct group of eightbrainstem tumors that behaved in a significantly dif-f e rent fashion from the typical infiltrating brainstemglioma. In these patients, symptoms frequently beganearly in childhood and sometimes during infancy. Ininfants, the history tends to be one of intractablevomiting and failure to thrive, whereas in older chil-d ren, signs of raised intracranial pre s s u re, includingpapilledema, are frequently present. A long history ofsymptoms can usually be elicited.
© 1999 The American Association of Neurological Surg e o n s

Dorsally exophytic brainstem tumors pro t r u d einto and largely fill the fourth ventricle (Figures 1and 2). They mushroom down over the dorsal sur-face of the cervical spinal cord and typically enhancebrightly with the administration of a contrast agent.These tumors are typically low-grade astro c y t o m a so r, more rarely, gangliogliomas. Furtherm o re, thevast majority of these tumors are solid and not cys-tic. Subtotal surgical excision has been extre m e l ysuccessful (Figure 3).
DIFFUSE INTRINSIC ASTROCYTOMAS OF THE BRAINSTEMIntrinsic astrocytomas of the brainstem start in thepons and spread up into the midbrain and down intothe medulla; they typically present with cranial nervepalsies and long-tract signs. Initially, the tumorshows no enhancement and enlarges the brainstem.If the patient is treated with radiotherapy, the brain-
stem typically re t u rns to a normal size. For a briefperiod the child responds positively, until MRI re v e a l sthe tumor to be enhancing, with nodular excre s-cences extending from the brainstem (Figure 4).
Patients with these diffuse intrinsic tumors rare l ysurvive for more than 2 years, despite aggre s s i v etherapy. At autopsy, these tumors are revealed to beeither malignant astrocytomas or glioblastoma multi-f o rme (Figure 5). Furtherm o re, at autopsy, extensiveleptomeningeal metastases are frequently pre s e n t( F i g u re 6).
No treatment has been shown to be successful inenhancing the length of survival in children with thistype of tumor. In numerous instances, surgeons haveoperated on these tumors with no effective long-termresults. Adjunctive therapy, including radiotherapyand chemotherapy, provides short-term relief forthese patients, but eventually the tumor re t u rns andsurvival for more than 2 years is rare .
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8162
F i g u re 1. Sagittal T1-weighted MRI showing a dorsally exophytic tumor.

HOFFMAN : BRAINSTEM GLIOMAS 163
F i g u re 3. A, operative view of a dorsally exophytic astrocytoma. B, operative view following resection of tumor.
F i g u re 2. Operative view of a large dorsally exophytic tumor.
A B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8164
F i g u re 4. Sagittal T1-weighted MRI showing a diff u s etumor of the pons extending up into the midbrain anddown into the medulla with nodular excre s c e n c e s . F i g u re 5. Postmortem view of a diffuse tumor in the pons.
F i g u re 6. Leptomeningeal metastases seen in a diffuse tumor in the pons.

HOFFMAN : BRAINSTEM GLIOMAS 165
FOCAL INTRINSIC BRAINSTEM ASTROCYTOMASFocal intrinsic gliomas make up about 20% of brain-stem gliomas. They are most commonly located inthe midbrain, although they have been known tooccur in the medulla; in rare instances, they arelocated in the pons itself. Depending on the location,they can give rise to cranial nerve palsies and tolong-tract signs. They can be solid or cystic. Afterresection, no additional therapy is necessary in 60%of patients, whereas 40% re q u i re adjunctive therapybecause of re c u r rence. Focal tumors can occur inany location within the brainstem. They usually in-volve a portion of the tegmentum of the midbrain( F i g u res 7 to 10).
In my experience, I have found that one can ele-vate the temporal lobe, section the tentorium, andthen expose the side of the midbrain; a horizontalincision is then made in the midbrain exposing thet u m o r, which can then be debulked using an ultra-sonic aspirator or a contact laser. Small tectal tumors
can be very indolent and typically close off the aque-duct, producing hydrocephalus. Hydrocephalus canbe treated with a third ventriculostomy or a ventricu-loperitoneal shunt. There is no need to resect thesesmall indolent tectal gliomas. However, one can re-sect a very large tectal glioma that mimics a pinealt u m o r. These tumors must be explored and debulked( F i g u re 11). Frameless stereotaxis is essential inremoving focal tumors of the brainstem (Figure 12).
Focal tumors in the pons are rare; they area p p roached usually via a midline incision in the floorof the fourth ventricle (Figure 13). Focal tumors inthe medulla are approached via an incision in themidline; if they bulge out laterally, they can bea p p roached from the external surface of the medulla( F i g u re 14). In patients in whom resection is under-taken in the medulla, it is important for the patientto maintain postoperative ventilation in the intensivec a re unit until it can be ascertained that breathing ise ffective and there is no evidence of CO2 re t e n t i o n .
F i g u re 7. A, computed tomography scans in an 8-month-old infant showingan enhancing tumor of the midbrain extending into the thalamus. B, T 1 -weighted MRIs of the patient at 8 years old. Six years later, hemiparesis hasd i s a p p e a red and there is very little tumor.
B
A

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8166
F i g u re 8. A, axial T-1 weighted MRIs showing large enhancingtumor of the midbrain. B, 3 months following resection of thet u m o r, some enhancing tumor is still seen; C, 2.5 years later, noresidual tumor is seen.
A
B
C

HOFFMAN : BRAINSTEM GLIOMAS 167
F i g u re 9. A, MRIs showing focal tumorfilling the left midbrain. B, operative viewof the tumor. C , following resection, littletumor re m a i n s .
F i g u re 10. A and B, MRIs showing focal tumor in the midbrain with acystic component in the fourth ventricle. C, frameless stereotaxy isused in removing the tumor.
B C
A
A
B
C

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8168
F i g u re 11. A, T1-weighted MRIs showing a large tectal tumor. B, operative view showing the left colliculus filled with tumor. C, operative view after resection of the tumor.
F i g u re 12. Frameless stereotaxy is used in resecting a focal tumor.
A
BC

HOFFMAN : BRAINSTEM GLIOMAS 169
CONCLUSIOND i ffuse intrinsic brainstem tumors are malignantand patients do not benefit from surgical interven-tion. Dorsally exophytic tumors, focal intrinsic tu-mors, and craniocervical tumors are usually benignand surgical debulking is beneficial. Some of thesetumors undergo involution, and no adjuvant ther-apy is needed. In patients with small tectal gliomas,only control of the hydrocephalus and observationa re needed. In patients with large tectal gliomas thatcan mimic a pineal tumor, the glioma should bee x p l o red and re s e c t e d .
CRANIOCERVICAL BRAINSTEM ASTROCYTOMASCraniocervical brainstem gliomas arise in the uppercervical cord and extend into the medulla (Figures 15to 17). These patients typically present with long-tractsigns and may have lower cranial nerve signs as well.
Laminotomy is a useful pro c e d u re if the tumorextends down into the spinal cord. A midline lamino-tomy is made, and the tumor is debulked using anultrasonic aspirator. Resection is carried out ro s-trally to the level of the medulla, where resection be-comes more conservative. The use of motor and sen-sory evoked potentials is essential.
F i g u re 14. T1-weighted enhanced MRIs showing a focal tumor in the medulla with a cyst.
F i g u re 13. Axial T1-weighted MRIs showing a focal tumor in the pons.
F i g u re 15. MRIs showing a l a rge enhancing tumor extendingf rom the cervical cord and into the medulla.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8170
F i g u re 16.Operative view of a craniocervical tumor.
F i g u re 17. A, M R I of a craniocervical tumor—the patient underwent bi-opsy and radiation at another institution. B , following resection andfusion of the spine, the child responded to treatment. C , operative view oftumor extending into fourth ventricle.
A B
C

INTRODUCTIONLesions located laterally in or adjacent to the lateralventricle can be difficult to surgically expose. Tr a d i-tional approaches to such lesions are transcortical,t h rough the superior or middle temporal gyrus, thesuperior parietal lobule, or the frontal lobe. The trans-callosal approach is usually perf o rmed via an ipsilat-eral route with the patient supine and the midline ofthe head vertically oriented. Dissection pro c e e d st h rough the ipsilateral interhemispheric fissure andthe ipsilateral ventricle to reach the lesion. The au-thors prefer a contralateral transcallosal approach. Inthis approach, the patient is supine, the midline ofthe head is oriented horizontally with the lesion onthe upside, and dissection proceeds through the con-tralateral interhemispheric fissure and ipsilateralventricle to reach the lesion.
The contralateral transcallosal approach hasmany advantages compared to other routes. The useof this approach avoids a transcortical incision; inaddition, gravity retracts the hemisphere to open thei n t e rhemispheric fissure. A more lateral angle ofa p p roach increases the surgical exposure and mini-mizes retraction of the medial hemisphere. Finally,lesions located in the dominant hemisphere can beresected without an interhemispheric dissection onthat side.
THE CONTRALATERAL TRANSCALLOSAL APPROACH TO
LESIONS IN OR ADJACENT TO THEL ATERAL VENTRICLE
MICHAEL T. LAWTON, M.D.ROBERT F. SPETZLER, M.D.
171
We perf o rmed our first contralateral transcallosala p p roach in 1983 and recently published our re s u l t swith 32 patients. The technique is safe and eff e c t i v eand warrants consideration for appropriate lesions.
PATIENT SELECTIONThe contralateral transcallosal approach can be usedto expose several diff e rent types of lesions located lat-erally in or adjacent to the lateral ventricle, includingc a v e rnous malformations, arteriovenous malform a-tions (AVMs), and tumors. Cavernous malform a t i o n slocated in the caudate nucleus, anteromedial thala-mus, lateral ventricular wall, and posterior thalamusa re well suited to this approach. These lesions re a c han ependymal surface laterally in the ventricular sys-tem. AVMs located in the corpus callosum, choro i dplexus/lateral ventricle, and thalamus are also wellsuited to this approach. Typically, such AVMs are fedby the pericallosal and choroidal arteries, and the ni-dus extends laterally. Likewise, tumors in similarlocations, including gliomas, central neuro c y t o m a s ,intraventricular meningiomas, choroid plexus papil-lomas, and some craniopharyngiomas, can be ex-posed via the contralateral transcallosal appro a c h .
Patient age can be a contraindication to this ap-p roach because the craniotomy flap crosses the su-perior sagittal sinus. In older patients with more ad-h e rent dura, the risks of sinus injury, significantblood loss, sinus occlusion, and air embolism arei n c reased. © 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8172
SURGICAL TECHNIQUEThe patient is placed in the supine position with bol-sters under the shoulder ipsilateral to the lesion (Fig-u re 1). The head is placed in a Mayfield headholderand turned so that the hemisphere contralateral tothe lesion is down, the lesion is up, and the sagittalmidline is parallel to the floor (Figure 2). The head isangled 45° upward (lateral neck flexion) to optimizethe angle of view into the ventricle (Figure 3). A U-shaped skin incision in the frontoparietal region cre-ates a scalp flap that is based laterally on the con-tralateral side and crosses the midline to the otherside. The anterior limb of the incision parallels thehairline, and care is exerted not to incise the skin onthe forehead. A fishhook retraction system, with thehooks pulling inferiorly on this limb of the incision,helps to increase the anteroinferior exposure of thebone flap. The coronal suture is identified, and a cra-niotomy is made with two thirds of the bone flapanterior and one third posterior to the coronal su-t u re, crossing the superior sagittal sinus twice to ex-pose the other side.
G reat care must be exercised in crossing the sa-gittal sinus with the craniotome. Its epidural positionis established visually before the sinus is crossed byaiming a light into the cut of bone and irrigatingenough to see intact dura. If a dural breach is de-tected, the flap is taken in two pieces, with the firstpiece entirely over the down hemisphere and the sec-ond piece crossing the sinus to complete the cra-niotomy. With two pieces, the dura and sagittalsinus can be carefully dissected off the inner table ofskull after the first piece is removed under excellentvisualization. This technique is particularly impor-tant in elderly patients with adherent or thin dura.
The dura is opened contralateral to the lesion witha C-shaped flap based along the superior sagittal si-nus. Important bridging veins must be pro t e c t e d( F i g u re 4A). The dural flap is tented superiorly toopen the interhemispheric fissure, which is thenopened further by removing adhesions between thebrain and falx, working between the veins bridgingto the superior sagittal sinus. Every effort is made top reserve these bridging veins. The arachnoid mem-brane deep to the free edge of the falx is opened toexpose the pericallosal arteries and corpus callosum.
Gravity allows the contralateral (down) hemisphereto separate from the falx, eliminating the need forretraction. A retractor is placed along the inferior fre eedge of the falx to expose the pericallosal arteries andcorpus callosum. The superior falx should not be re-sected aggressively, to avoid stenosis or occlusion ofthe superior sagittal sinus which would thereby pro-mote sinus thrombosis and venous infarction. Thepericallosal arteries are separated, and the corpuscallosum is incised 2 cm to permit entry to the lateralventricle ipsilateral to the lesion. The incision site canbe identified using an intraoperative navigational sys-tem or by retracting the ipsilateral pericallosal arterylaterally and entering the ventricle beneath theartery’s normal location (Figure 4B). Once inside theventricle, normal ventricular anatomy is identified(including the choroid plexus, thalamostriate vein,and septal vein) and the appropriate ventricle is con-f i rmed (Figures 5 and 6). The lesion is then identifiedand treated. Further exposure can be obtained bydeepening the retractor so that its tip is in the ventri-cle retracting the corpus callosum.
At the end of the pro c e d u re, the ventricles are ex-tensively irrigated and filled with saline. If not in-
F i g u re 1. Lateral ( A ) and superior ( B ) views of the patient positioned for a contralateral transcallosala p p roach to a left intraventricular lesion. The head is turned to the right, the left shoulder is bolstere d ,and the skin flap is based on the right.
A B

LAWTON AND SPETZLER : THE CONTRALATERAL TRANSCALLOSAL APPROACH TO LESIONS IN OR ADJACENT TO THE LATERAL VENTRICLE 173
F i g u re 3. Patient position and lesion location f rom the surgeon’s perspective.
lesion in left lateral ventricle
A B
F i g u re 2. A, gravity retracts the contralateral hemisphere, opens the interhemispheric fissure, and pulls the lesion into thes u rgeon’s view. B , the ipsilateral transcallosal approach (line A) re q u i res retraction of the medial hemisphere to reach thelateral aspect of the lesion, whereas the contralateral transcallosal approach (line B) re q u i res no additional retraction.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8174
falx
planned callosotomy
falx
midline corpus callosum (long striae)
cingulategyrus
callosomarginal artery
pericallosal arteries
section of corpus
callosum
pericallosal arteries
superior sagittal
sinus
dura
midline corpus callosum
F i g u re 4. A, the interhemispheric dissection has been completed, and the corpus callosumis in view at the depth of the exposure. The fishhooks pull the scalp forward to incre a s ee x p o s u re for the bone flap while keeping the incision off the forehead. The bone flapc rosses the sagittal sinus twice to expose it completely. This bone work enables the duralflap to be tacked superiorly, permitting a view directly down the falx and the ability to openthe interhemispheric fissure widely. B , the callosotomy is made beneath the pericallosalartery ipsilateral to the lesion in order to enter the appropriate ventricle.
A
B

LAWTON AND SPETZLER : THE CONTRALATERAL TRANSCALLOSAL APPROACH TO LESIONS IN OR ADJACENT TO THE LATERAL VENTRICLE 175
cavernous malformationin caudate nucleus
pericallosal artery
corpus callosum
thalamostriate vein
foramen of Monro
septal vein
septum pellucidum
slit of lateral ventricle
corpus callosum
entire lateralventricle visualized
fornix
choroid plexus of thelateral ventricle
thalamus
F i g u re 5. The relationship between the lateral thalamostriate vein and the medialc h o roid plexus confirms entry into the appropriate ventricle, and the lesion is visual-ized. Note how gravity pulls the lesion down into the corridor of operative exposure .Deepening the tip of the retractor into the ventricle helps visualize the pathology better.
F i g u re 6. Sagittal view illustrating that all regions of the lateral ventriclea re accessible via this exposure, depending upon the angle of approach.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8176
serted preoperatively, a ventriculostomy catheter isleft in the ventricle at the end of the operation to clearresidual blood that could obstruct the flow of cere-b rospinal fluid.
The contralateral transcallosal approach is alsoused for lesions located laterally in the corpus callo-sum and the cingulate gyrus. The corpus callosummay not be traversed, but the advantages of the con-tralateral approach apply as well to these lesions.With the more superficial lesions, the falx often is cutinferiorly after the inferior sagittal sinus has beencoagulated to enable a sharper angle across to theopposite side.
RESULTSThe contralateral transcallosal approach was used inlesions laterally in or adjacent to the lateral ventriclein 32 patients. Three patients had right-sided lesions,and they were positioned with the left side down; theremaining 29 patients had left-sided lesions and werepositioned with the right side down. In four patients,the falx was cut to increase exposure of the contralat-eral medial hemisphere. In two patients with left hy-pothalamic lesions, the foramen of Monro was en-l a rged by opening the choroidal fissure posteriorly togain access to the third ventricle. In one patient witha thalamic AVM, the posterior contralateral transcal-losal approach was used; in the re m a i n d e r, the stan-d a rd anterior contralateral transcallosal appro a c hwas used.
In six patients, cavernous malformations were re-sected completely in a single surgical stage. In fivepatients, AVMs were resected in a single stage, and intwo, a second-stage surgery was re q u i red. Choro i d a land pericallosal AVMs can be resected completely viathis approach; however, thalamic AVMs may re q u i ret reatment with stereotactic radiosurgery to the deepresidual nidus. In four patients, benign tumors (twomeningiomas, one choroid plexus papilloma, and onep rolactinoma) were resected completely via the con-tralateral transcallosal approach. More malignant tu-mors (e.g., astrocytomas, glioblastomas multiform e ,and central neurocytomas) can also be accessedt h rough this approach, but their resection is typicallysubtotal.
Ventriculostomy catheters were often indicatedp reoperatively due to hydrocephalus from intraven-tricular hemorrhage, trapped ventricular horns, orobstruction of the foramen of Monro. When not al-ready present, ventricular catheters were insertedduring the operation and left in place for several days.Only four patients re q u i red ventriculoperitoneals h u n t i n g .
T h e re were no surgical deaths in this series. Tw o(6%) of the 32 patients experienced transient neuro-logical deficits. After resection of a thalamic AV M ,one patient developed a small thalamic infarc t i o n
with right-arm weakness, which resolved completely.After resection of a left atrial meningioma, a secondpatient developed left moderate hemiparesis, whichalso resolved completely. Two patients (6%) experi-enced permanent neurological morbidity. One pa-tient with a central neurocytoma experienced post-operative intraventricular hemorrhage that re q u i re dmultiple ventriculostomies. He subsequently devel-oped a S e r r a t i a ventriculitis. The other patient devel-oped a venous infarction after resection of a leftglioblastoma multiforme, with resultant right hemi-p a resis and expressive aphasia.
At last examination, patient outcome in terms ofthe Glasgow Outcome Scale score (GOS) was deter-mined over a mean follow-up of 1.6 years. Tw e n t y - s i xpatients had a good recovery (GOS 1), four had mod-erate disabilities (GOS 2), and two had severe dis-abilities (GOS 3).
DISCUSSIONThe contralateral transcallosal approach is an excel-lent technique for dealing with laterally placed lesionsin the lateral ventricles, which can be particularly dif-ficult to resect. With this approach, the craniotomyand interhemispheric approach are contralateral tothe lesion and the transventricular approach is ipsi-lateral to the lesion.
We are not the first to report the contralateraltranscallosal approach. Other surgeons, includingLong and Chou, Shucart and Stein, Machado de Al-meida, and Ehni, also have mentioned it. It seems,h o w e v e r, that most neuro s u rgeons use this ap-p roach rarely, if at all. The outcomes in this seriesdemonstrate the utility of the contralateral transcal-losal approach for treating a wide variety of lesionslocated laterally in or adjacent to the ventricle or inthe interhemispheric fissure, including cavern o u sm a l f o rmations, AVMs, and tumors of all types. Themodifications described here make this a safe ande ffective approach, which may warrant more thanoccasional use.
Two other approaches for exposing ventricular le-sions are the transcortical-transventricular appro a c hand the transcallosal-transventricular approach. Thetranscortical approach is more direct with a shortworking distance to the lesion, but it has distinct dis-advantages. First, transcortical approaches traversen o rmal brain tissue, increasing the risk of neuro l o g i-cal deficits. Various trajectories through cortex havebeen described (e.g., through the superior and middletemporal gyri and through the inferior (Van Wa g e n e n )and superior parietal lobules), each associated withn e u rological sequelae. Second, transcortical ap-p roaches are more difficult to perf o rm than the trans-callosal approach. Fewer anatomical landmarks arep resent to guide the surgeon transcortically to the

LAWTON AND SPETZLER : THE CONTRALATERAL TRANSCALLOSAL APPROACH TO LESIONS IN OR ADJACENT TO THE LATERAL VENTRICLE 177
ventricle. This problem, however, has been mitigatedby the advent of intraoperative navigational systems.The approach is particularly difficult when the ventri-cles are not dilated. The exposure tends to be limitedbecause of the inclination to minimize the extent ofcortical incision. Finally, the transcortical appro a c hcan cause postoperative seizure s .
The limitations of the transcortical approach ledDandy, Milhorat and Baldwin, Shucart and Stein,and others to develop the transcallosal approach. Thetranscallosal approach does not traverse cortex butgoes through the interhemispheric fissure and corpuscallosum instead. This route has identifiable an-atomical landmarks to guide the surgeon to the ven-tricle and enlarged ventricles are not a necessity. Thet h i rd ventricle can be exposed simply by enlarging theforamen of Monro, a maneuver not easily accom-plished through a more oblique transcortical ap-p roach. Most importantly, many studies have dem-onstrated that the transcallosal approach is welltolerated and produces no functional neuro l o g i c a ldeficits or postoperative seizure s .
Most neuro s u rgeons position their patients su-pine or sitting with the head and neck in the neutralposition and the sagittal midline oriented vertically.We prefer to rotate the neck laterally to orient themidline horizontally. This horizontal position is eas-ier on the surgeon’s hands, allowing the hands towork in the same plane rather than on top of eacho t h e r. The surgeon can use an instrument in eachhand without obscuring the operative field. Thisposition also permits gravity to retract the downsideh e m i s p h e re and open the interhemispheric fissure
while the falx retracts the upside hemisphere. In-c reasingly, the advantages of this position are beingre c o g n i z e d .
The horizontal position necessitates a decision re-g a rding laterality. In most cases, the head is posi-tioned with the lesion side down (i.e., right-sided le-sions are approached with the right side down andleft-sided lesions with the left side down). This posi-tion works well for lesions located near the midline.H o w e v e r, exposure of laterally placed lesions in oradjacent to the lateral ventricle re q u i res significantretraction of the hemisphere and risks injury to theparafalcine and cingulate gyri.
The contralateral transcallosal approach offers abetter angle of approach that increases lateral ex-p o s u re of the lesion and minimizes the retraction re-q u i red on the medial hemisphere. In addition to open-ing the interhemispheric fissure to facilitate thea p p roach, gravity pulls the upside lesion mediallyinto the surgeon’s view. Without this angle of ap-p roach, the lateral margin of the lesion can bereached only with excessive retraction. The contralat-eral transcallosal approach is ideal for left-sided le-sions. Although added lateral exposure is gained re-g a rdless of the side of approach, the approach to aleft-sided lesion from the right spares the dominanth e m i s p h e re from retraction injury and the potentialsacrifice of bridging veins. Because of this, it is be-lieved to be safer than the approach to a right-sidedlesion from the left. Thus, the contralateral transcal-losal approach from the left can be used judiciouslywhen the need for more lateral exposure offsets theadditional risks of a left interhemispheric dissection.
Illustrations re p roduced with permission from Barrow Neurological Institute.


INTRODUCTIONThe treatment of patients with Chiari I malform a t i o ntraditionally consists of posterior fossa decompre s-sion, with or without cervical laminectomy, com-bined with duraplasty. Posterior fossa decompre s-sion has been developed to relieve impaction cre a t e dby tonsillar herniation and to cause re g ression ofsymptoms. Modifications of this treatment includefourth-ventricle-to-subarachnoid shunting to main-tain free egress of cere b rospinal fluid (CSF), as wellas plugging of the obex to prevent syrinx expansion.H o w e v e r, it is unclear whether the syrinx is in dire c tcommunication with the subarachnoid space.
We have adopted the use of intraoperative ultra-sound to evaluate decompression of the foramenmagnum and the need for duraplasty in childre nwith Chiari I malformation. Our treatment forpatients with Chiari I malformation is based on thetheory that posterior fossa decompression withoutduraplasty is adequate if CSF flow can be estab-l i s h e d .
POSTERIOR FOSSA DECOMPRESSIONWITHOUT DURAL OPENING FOR
THE TREATMENT OF CHIARI I MALFORMATION
JONATHAN SHERMAN, M.D.JEFFREY J. LARSON, M.D.
KERRY R. CRONE, M.D.
179
© 1999 The American Association of Neurological Surg e o n s
PATIENT SELECTIONC h i l d ren with Chiari I malformation are candidatesfor posterior fossa decompression. Contraindicationsto this treatment include the presence of any intra-dural pathology that re q u i res dural opening, such asarachnoid scarring or sequestrations. Ultrasoundmay be perf o rmed in such patients; however, intra-dural exploration is still re q u i red. In patients withmedical conditions that preclude surgery (e.g., bleed-ing disorders or cardiac anomalies), this pro c e d u rewould be contraindicated until treatment is initiated.
PREOPERATIVE EVALUATION AND PREPARATION
Magnetic resonance imaging (MRI) of the cranio-cervical junction is obtained preoperatively to deter-mine the extent of the Chiari I malformation. Sagittaland axial T2-weighted images are important to visu-alize the CSF spaces ventral and dorsal to the cervi-comedullary junction. MRI of the spine is helpful todemonstrate the presence and extent of a syrinx,especially in patients with signs and symptoms sug-gestive of a syrinx. Preoperative evaluation shouldinclude complete blood cell count, electrolyte pro f i l e ,coagulation studies, and blood type and cro s s m a t c h .
Prior to being placed on the operating table, thepatient is intubated, an inhalation anesthetic is ad-

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8180
m i n i s t e red, and intravenous antibiotics are com-pletely infused. Prior to patient positioning, card i a cmonitor leads, intravenous access, pulse oximetry,and an arterial line or a blood pre s s u re cuff arep l a c e d .
SPECIAL EQUIPMENTIn addition to the standard surgical instrumentationneeded for posterior fossa decompression, intraoper-ative ultrasound equipment is necessary. Sagittaland axial imaging of the cervicomedullary junctionis obtained intraoperatively to evaluate the ade-
quacy of decompression. A 7-MHz transducer(actual head size 1.2 × 2.2 cm) is introduced into thes u rgical bed, which has been irrigated with 0.9%NaCl.
SURGICAL SET-UPIn the surgical suite (Figure 1) the patient is posi-tioned prone, with the neck slightly flexed. The headis placed on a Mayfield headrest or in three-point fix-ation. The shoulders are pulled down to expose thesuboccipital region and the posterior cervical spinef rom C1 to C6.
F i g u re 1. Superior view of the operating room layout during posterior fossa decompression. The sur-geon stands at the patient’s left side, while the patient is prone. The assistant and the scrub nursea re on the patient’s right side. The ultrasound equipment is behind the assistant, allowing the sur-geon a clear view of the image while ultrasonography is perf o rm e d .
video monitor
assistant scrub nurse
electrocautery
surgeon
anesthesiologist
x-ray view boxes
video monitor
instrument table

SHERMAN ET AL : POSTERIOR FOSSA DECOMPRESSION WITHOUT DURAL OPENING FOR THE TREATMENT OF CHIARI I MALFORMATION 181
OPERATIVE PROCEDUREA midline skin incision is made from the inion to thelevel of C3. The paraspinous fascia is dissected at theavascular linea albae and is retracted laterally toexpose the occiput and the upper cervical laminae.
Using a high-speed drill, the surgeon thins thesuboccipital bone. Bone rongeurs are used to exposethe posterior fossa and spinal dura. Bony decom-p ression, which is carried laterally to the occipitalcondyles, provides lateral decompression of the cer-vicomedullary junction. An upper cervical laminec-tomy is perf o rmed to accommodate the extent of thedescended cerebellar tonsils. Laminectomy is carriedto the lateral aspect of the canal (Figure 2A).
After completing the bony decompression of thesuboccipital and cervical canal, the surgeon identi-fies a transverse dural band at the level of the cervi-comedullary junction. This dural band, which con-sists of thickened dura and periosteum of the bonyforamen magnum, must be incised to achieved e c o m p ression (Figure 2B). The band is divided witha #15-blade scalpel, being careful that the underly-ing dura is not incised. The thickened band is thenpeeled away from the dura using forceps (Figure 2C).Ultrasound images are obtained to reveal the level oftonsillar herniation. Sufficient decompression hasbeen achieved if CSF can be identified dorsal to thetonsils and cervicomedullary junction by ultrasoundon sagittal and axial views and if tonsillar “pistoning”(i.e., pulsatile rostral-caudal movement of the tonsilswith little anterior–posterior pulsation (Figure 3A)) isa b s e n t .
Ultrasonography is used to determine whethert h e re is adequate CSF dorsal to the cervicomedullaryjunction and tonsils. Movement of the tonsils is alsoassessed. If the CSF spaces are small (i.e., less than2 mm between the tonsils and dura (Figure 3B)) or ift h e re is “pistoning,” then duraplasty is perf o rm e dusing a graft of periosteum or dural substitute (Fig-u re 3C). An incision is made in the dura from the topof the bony decompression to the bottom. The duralopening is made lateral to the midline on one side,above the level of the foramen magnum to avoidopening the occipital sinus. To allow sufficient spaceinside the dura for adequate decompression, a graftis sewn in place using 5-0 Prolene sutures, runninga simple suture to obtain a watertight closure .
Intradural exploration and coagulation of thec e rebellar tonsils elevate the tonsils above the level ofthe foramen magnum. Release of an arachnoid mem-brane, which is frequently found overlying the fourthventricle and foramen of Magendie, is also per-f o rm e d .
After adequate decompression is obtained, a Va l-salva maneuver is perf o rmed to ensure, via ultra-sonography, that foramen magnum obstruction byfurther tonsillar descent does not occur and to verify
that no holes or defects were created in the dura.The paraspinous musculature is re a p p ro x i m a t e dusing widely spaced, simple, interrupted 3-0 Vi c r y ls u t u res. The overlying cervical fascia is tightlyclosed, using simple, interrupted 3-0 Vicryl suture s .The skin is closed in the usual fashion.
POSTOPERATIVE CAREThe patient remains in a high-acuity care setting for24 hours following surgery. Activity is increased pro-g ressively. The patient is discharged when dietaryintake is adequate and he or she is ambulating well.
Follow-up CareA p p roximately 6 weeks after the operation, MRI isp e rf o rmed to evaluate the CSF space around thetonsils and cervicomedullary junction. We have usedcine-MRI to assess CSF flow. If the patient has anassociated syrinx, repeat MRI at the appro p r i a t espinal level is perf o rmed to monitor the size. In ourexperience, a decrease in the size of the syrinx canbe observed by 4 to 6 months postoperatively.
C o m p l i c a t i o n sMost postoperative complications in posterior fossad e c o m p ression are a result of duraplasty. Fre q u e n t l ye n c o u n t e red complications such as CSF leakage,meningitis, hemorrhage, and arachnoiditis can bep revented when duraplasty is avoided. In onepatient, a portion of the cerebellar tonsil hern i a t e dt h rough a small hole that occurred in the dura dur-ing dural thinning. This caused infarction of the her-niated portion of tonsil. After presenting with re c u r-rent, intractable posterior headaches, the patientunderwent duraplasty. Her symptoms resolved fol-lowing this second pro c e d u re. We have subsequentlydiscontinued the practice of dural thinning andrelease the fibrous band only at the level of the fora-men magnum, as described.
CONCLUSIONSWe have found that posterior fossa decompre s s i o nwithout duraplasty can adequately treat patientswith Chiari I malformation. Intraoperative ultra-sound is a useful adjunct to evaluate adequated e c o m p ression by assessing the amount of CSFa round the descended tonsils in the obstructed fora-men magnum. Avoiding duraplasty has decre a s e dthe incidence of postoperative complications.
The use of this pro c e d u re without duraplasty hasbeen limited to the pediatric population, but mayalso prove effective in adults. Further studies areneeded to assess the amount of CSF necessary foradequate decompression, as well as to determine thel o n g - t e rm outcomes in patients in whom decompre s-sion is perf o rmed with and without dural opening.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8182
transverse sinus
occipital sinus
thickened transverse band
vertebralartery
C1 laminectomy
bulging tonsil
marginal sinus
F i g u re 2. A, the posterior fossa and spinal dura areexposed following a suboccipital craniectomy and C1laminectomy. Note the thickened transverse fibro u sband at the level of the foramen magnum, still com-p ressing the dura and underlying tonsils and brain-stem. B , a right-angle dissector is inserted between thef i b rous band and the dura. The fibrous band is thenincised to prevent cutting the dura or marginal sinus.C , the fibrous band is peeled from the dura after inci-sion, thus providing further decompression of the fora-men magnum.
A
B
C

SHERMAN ET AL : POSTERIOR FOSSA DECOMPRESSION WITHOUT DURAL OPENING FOR THE TREATMENT OF CHIARI I MALFORMATION 183
tonsillar pistoning
diastole
2 mm CSF space
systole
C2
dural graft
foramen ofMagendiefourth ventricle
tonsil
confluence
A
B
C
F i g u re 3. A, illustration of tonsillar pis-toning ( a r ro w ) or the ro s t r a l - c a u d a lmovement of the tonsils that occurs inChiari malformation during systole–dias-tole pulsations. Loss of this pistoningmovement, combined with adequate CSFspace between the tonsils and the dura,indicates sufficient decompression of theforamen magnum. B , ultrasonic imagedemonstrating adequate decompre s s i o nof the foramen magnum. Note the 2 mmof CSF space between the cerebellar ton-sils and the dura posteriorly. C , in casesin which adequate decompression can-not be obtained without dural opening, amidline dural incision, placement of a dural graft, and duraplasty are used towiden the foramen magnum.


INTRODUCTIONCranioplasty is among the oldest neuro s u rgical pro-c e d u res. Trauma, infections, tumors, and compre s-sion caused by brain edema are some of the re a s o n sfor removal of cranial bone (Figure 1). Table 1 listscommon causes of bone defects. Many authors sug-gest that cranioplasty may have a therapeutic eff e c tthat broadens previous indications for the pro c e d u re .
DIAGNOSTIC STUDIES1 . skull x-ray2 . diagnostic and three-dimensional (3D) re c o n-
struction computed tomography (CT) 3 . diagnostic and phase-contrast magnetic re s o-
nance imaging (MRI)4 . transcranial cerebral oximetry (TCCO) with ortho-
static challenge (Figure 2A and B)5 . e l e c t roencephalography (EEG)6 . xenon-enhanced CT cerebral blood flow (CBF)
( F i g u re 2C and D)7 . n e u ropsychiatric evaluation (exit interview and
C o g n i s t a t )
COMPUTED TOMOGRAPHY- A S S I S T E DPREFORMED PROSTHESIS FOR R E PAIR OF CRANIAL DEFECTS
MANUEL DUJOVNY, M.D.CELSO AGNER, M.D.
FADY T. CHARBEL, M.D.LEWIS L. SADLER, M.S.
RAYMOND EVENHOUSE, B.S.DEIRDRE MCCONATHY, PH.D.
185
© 1999 The American Association of Neurological Surg e o n s
Table 1Causes of Cranial Defects
TraumaMotor vehicle accidentsOccupational accidentsUrban violenceSports injuriesWar
NeoplasiaMeningioma involving the boneEosinophilic granulomaPosterior fossa tumorsBone metastasis
InfectionOsteomyelitisFungiTuberculosis
MiscellaneousAneurysmsSubdural hematomaCranial decompressionCranial nerve neuralgias

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8186
F i g u re 1. Causes of cranial defects. A , p recranioplasty 3D reconstruction of the skull in a patient with a large cranial defectsecondary to trauma. B , postcranioplasty 3D reconstruction of the skull in the same patient. C , p recranioplasty 3D re c o n-struction of the skull in a patient with a large convexity meningioma. D , postcranioplasty 3D CT reconstruction in the samepatient. E , p recranioplasty plain CT in a patient with frontal sinusitis. F, p recranioplasty 3D CT reconstruction of the samep a t i e n t .
A B
C D
E F

DUJOVNY ET AL : CT-ASSISTED PREFORMED PROSTHESIS FOR REPAIR OF CRANIAL DEFECTS 187
F i g u re 2. Diagnostic tests in cranioplasty. A , p recranioplasty TCCO with orthostatic challenge. B , postcranioplasty TCCOwith orthostatic challenge, showing re t u rn to precranioplasty values in the same patient. C , p recranioplasty anatomical andquantitative Xenon-enhanced CT CBF study of a patient with a large cranial defect. D, postcranioplasty anatomical andquantitative Xe-CT CBF of the same patient, showing generalized improvement of CBF after the surgical pro c e d u re .
D
C
B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8188
SURGICAL RECONSTRUCTIONThe fabrication and surgical fitting of cranial im-plants by traditional methods is dependent on sub-jective skills and pro c e d u res, producing in mostcases a close but imperfect fit that necessitates re v i-sions during the surgical placement of the implant.Results from our experience using computer- a i d e ddesign and computer-aided manufacturing (CAD/CAM) technology indicate that pre s u rgical designand the fabrication of cranial implants using CT dataf rom the patient results in a “near perfect” fit. Ta b l e s2 and 3 list characteristics of a good cranioplastyand of a good implant material.
S t e re o l i t h o g r a p h yRapid prototyping is a term for several manufactur-ing processes that permit the creation of solid, physi-cal objects directly from a digital file or computerdata. The specific rapid prototyping technology usedin our pro c e d u re is stereolithography technologyf rom 3D Systems (Valencia, CA). Stere o l i t h o g r a p h ywas first applied commercially in the automobileindustry by Chrysler Motors in 1989. The first primi-tive demonstration of the technology was in 1984,
but its full development was not realized until a fewyears later. Since its development, stere o l i t h o g r a p h yhas been applied to a wide range of objects, fro ma rchaeology and environmental science to physicaland paleoanthropology. In the medical field, it wasfirst applied for maxillofacial prosthetics in the late1980s and was later used to design cranial implantsin the middle 1990s. Table 4 lists the characteristicsof implant materials used in stereolithography vs.those used in intraoperative molding. Several authorshave claimed to be the first to adopt the technologyfor cranioplasty.
A pro c e d u re for generating CAD/CAM files tom a n u f a c t u re cranial implants to repair interm e d i a t eand large-sized skull defects was developed in 1996by the Department of Neuro s u rgery and re s e a rc h e r sin the Biomedical Visualization Laboratory, School ofBiomedical and Health Information Sciences at theUniversity of Illinois at Chicago in collaboration withc o m m e rcial design and rapid prototyping pro d u c t s .The process involves the following steps: data acqui-sition (image acquisition, data processing, and modelbuilding); implant fabrication; and implantation.
Table 2Characteristics of a Good Cranioplasty
• structural integrity• infection-resistant properties• stability over time• ease of fabrication• precise fit• minimal inflammation and graft-host reaction• radioneutral for visualization• material properties
Table 3Characteristics of a Good Implant Material
• biocompatible• high-impact strength• Food and Drug Administration-approved and
readily available• nonbiodegradable• non-exothermic during surgery• no toxic fumes and/or residues• MRI compatible
Table 4Comparison Between Intraoperative Molding and Stereolithography of Methylmethacrylate
Intraoperative Molding Stereolithography
Exothermic reaction severe noneFume production severe noneTissue reaction severe mildGraft-host reaction severe mildOperating time long shortHospital stay long short

DUJOVNY ET AL : CT-ASSISTED PREFORMED PROSTHESIS FOR REPAIR OF CRANIAL DEFECTS 189
IMPLANT DESIGN AND FABRICATIONData AcquisitionImage AcquisitionA 1-mm slice thickness CT scan is generated using a General Electric high-speed advantage CT scanner(GE Medical Systems, Inc., Milwaukee, WI) andimaged on the viewing console (Figure 3A-D). Thedata are transferred to DAT or magnetic tape, ort r a n s f e r red through the university’s data network toa graphics workstation (Silicon Graphics, Inc., Moun-tain View, CA). The image data protocol allows thedata to be taken directly into software on the work-station for slice and volumetric viewing to verify theintegrity of the database. The data can then be store dfor later processing or imported directly intoCAD/CAM software (Surgicad, Inc., Dallas, TX orMaterialise, Ann Arbor, MI).
Data Pro c e s s i n gTo construct a file suitable for driving the rapid pro-totyping (stereolithography) device, several pro c e s s-ing steps must be completed. Pixel data from the CTslices must undergo segmentation to extract theskull information from the rest of the slice imagedata. Semiautomatic segmentation algorithms in thes o f t w a re initiate the segmentation scheme, but eachslice is manually checked and corrected, as neces-sary, using a drawing tool. The edges of the innerand outer tables of cranium are identified and theircontours converted from a pixel map re p re s e n t a t i o nto a vector map. The pixel-to-vector map conversionestablishes the geometry of each skull outline curvef rom the CT slice. Pixels and their volumetric equiva-lent “voxels” are image re p resentations only and donot explicitly establish the geometry of the objectsthey re p resent. Vector maps, on the other hand, aremathematical curves explicitly defining geometry.The vector maps are then connected to generate as u rface model of the skull. To create an appro p r i a t eoutput file for use in rapid prototyping, the softwarepositions the surface model in the optimal orienta-tion for the “build cycle” in the machine and re s a m-ples the data into appropriate slice thicknesses fors t e reolithography. The “resliced” data now re p re s e n ta tool path to guide the stereolithography machine inc reating the model.
Model BuildingThe computer file is imported into the stere o l i t h o g r a-phy machine, where the tool path information isused to drive a computer-guided laser positionedover a vat of polymer. The liquid polymer is convertedto a solid by the energy of the laser beam. As eachslice from the CAD file is traced by the laser beam, abed or platform in the vat of polymer to which themodel is attached is lowered, flooding the surface ofthe developing model. The polymerization by the
laser beam is repeated, according to this sequence,slice-by-slice. In this way, a solid plastic form isgradually created in the photocurable polymer. Thefinished model is removed from the vat, drained ofexcess polymer, and submitted to a final curing stageusing ultraviolet radiation. The final model is anexact physical re p resentation of the computer modelof the patient’s skull and defect (Figure 3E). To savetime and the cost of additional material and “build-time,” only the portion of the skull immediately sur-rounding the defect is manufacture d .
Implant FabricationThe physical model generated through stere o l i t h o g-raphy (Figure 4A) serves as a template for the manu-f a c t u re of the final implant.
Initial StepsModeling clay is applied to the plastic model of thepatient’s defect. It is smoothed and contoured to re p-resent the inner surface of the pro s t h e s i s / n e u ro t i s-sue boundary. A silicone rubber mold is made of thisa g g regated piece (Figure 4B). Dental stone is poure dinto the Silastic mold to produce a solid base uponwhich the prosthesis is designed.
Design of the ImplantA dental grade wax is applied to the negative spacere p resenting the skull defect. Care is exercised inmaintaining appropriate contour and thickness toa s s u re the best cosmetic appearance following im-plantation of the custom prosthesis.
The MoldWhen the wax model is completed, the second half ofthe mold can be made. “Keys” are placed in the backpiece of the mold so that the final two pieces can bep e rfectly realigned. A separator is applied to all ex-posed surfaces so that the two halves of the finalmold will not bond together. Dental stone is poure donto the surface to an appropriate thickness andallowed to set until thoroughly hardened (Figure 4C).
Casting the ImplantThe mold halves are separated and the wax is re-moved, leaving a negative space to receive the finalimplant material. A medical-grade methylmethacry-late is mixed to form a soft, pliable lump the consis-tency of warm butter. The material is placed into themold and clamped tightly (Figure 4D). The clampedmold is placed in a hot-water bath to slow cure. Fol-lowing a prescribed cure time, the clamps are re-moved and the solid methylmethacrylate implant istaken from the mold (Figure 4E). Additional curing in an oven releases free monomers trapped in theimplant. After trimming and polishing, the finishedimplant is sent to the operating suite for ethyleneoxide gas sterilization.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8190
F i g u re 3. Steps for using stereolithography in cranioplasty.A , plain skull CT slice. B , p recranioplasty 3D soft tissuereconstruction. C , p recranioplasty 3D bone re c o n s t r u c t i o n .D , c o m p u t e r-generated 3D model of the bone defect. E , f i n a lcranial pro s t h e s i s .
A
C
D
E
B

DUJOVNY ET AL : CT-ASSISTED PREFORMED PROSTHESIS FOR REPAIR OF CRANIAL DEFECTS 191
AB
C
D
F i g u re 4. Steps in the prosthesis fabrication. A , s t e reolithographic model of the cranial defect. B , positive clay model.C , wax pattern or stone positive. D , mold in clamp.

F i g u re 5. Implantation of the prosthesis. A , posterior view of the cranial defect. B , lateral view of the cranial defect. C , patient in prone position. D , opening of the skin and dissection of the musculocutaneous flap. E , liberation of adhesions.F, implant in bacitracin solution. G , detail of the screwed titanium plates. H , postoperative posterior view. I , p o s t o p e r a t i v elateral view.
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8192
I m p l a n t a t i o nPatient SelectionAny patient with a large cranial defect (≥9 sq cm) orwho has a cranial defect with a complex shape is acandidate for implantation (Figure 5A and B). Pre-s u rgical tests are important for establishing the intra-cranial hemodynamic environment. The decision top e rf o rm a cranioplasty may be influenced by tests fors e i z u re control, as well as knowledge of the neuro p s y-chiatric status of the patient. Additionally, patientsp resenting with “sinking scalp” syndrome or the“ s y n d rome of the trephined” may benefit from cranio-p l a s t y .
C o n t r a i n d i c a t i o n sContraindictions of cranioplasty include infection ofthe skin or bone, thin skin with compromised bloodsupply after radiotherapy, missing skin, or patientsin poor clinical condition who may not withstandanesthesia and surgery well. Cranioplasty as a sec-ondary pro c e d u re is per f o rmed only after re s o l u t i o nof the basic pathological processes that led to itsavoidance as a primary pro c e d u re. Infection of thes u rgical site, allergic reaction to the implant mater-ial, graft rejection, hematoma formation, and carc i n-ogenic potential are some of the general risks of thep ro c e d u re .
P reoperative Pre p a r a t i o nIn cases where there is concern about an active in-fection of the bone, gallium single photon emissionCT (SPECT) is perf o rmed and an appropriate antimi-c robial chemotherapy initiated. Seizure control, asevidenced by EEG, plasma drug levels, and no clini-cal evidence of seizures, and normal pre o p e r a t i v epsychiatric status need to be established in order toavoid major complications postoperatively.
Anesthesia and MonitoringInduction is perf o rmed with mesethlin and thiopen-tal, and the patient is paralyzed with pancuro n i u m .General anesthesia is administered with isofluraneafter intubation with an endotracheal tube, con-t rolled mechanical ventilation, arterial and venous
lines, and Foley catheter placement. Ventilatory con-t rol is established. Electro c a rdiography, arterialblood gases, pulse oximetry, body temperature, andmean arterial pre s s u re are generally monitored intra-operatively. If necessary, a spinal drain may be intro-duced to control increased postoperative intracranialp re s s u re .
Patient Postioning and DrapingPositioning is predicated on the location of the bonedefect. Accordingly, the patient is positioned in theappropriate supine, prone, or lateral position (Fig-ure 5C).
After shaving and cleansing the surgical site, thepatient is draped in the standard fashion dictated bythe cranial defect.
Skin IncisionTo avoid postoperative healing that might compro-mise the flap, the skin incision replicates that usedin the previous surgery.
Operative Pro c e d u reThe incision site is infiltrated with 1% lidocaine andepinephrine, and the incision made. Raney skin clips(Codman, Inc., Randolph, MA), if needed, are usedfor hemostasis. The flap is undermined and thedural attachments are released (Figure 5D and E).Dissection continues until the edges of the skulldefect are visualized. The surgical site is irrigatedwith bacitracin. The implant is removed from thebacitracin bath in which it was preserved followingthe ethylene oxide sterilization (Figure 5F). Holes aredrilled in the surrounding bone and implant with aMidas Rex high-power drill (Midas Rex, Fort Wo r t h ,TX). The implant is fixed in place and screwed with aminimum of three to four titanium plates and scre w sto effect immobilization of the prosthesis and re s t i t u-tion of the calvarium (Figure 5G). After careful hemo-stasis of the periosteum and musculocutaneous flap,the incision is closed in two layers. The subcuta-neous/galea incision is closed with 0-0 interruptedinverted Dexon, and the skin is closed using staples( F i g u re 5H and I).

DUJOVNY ET AL : CT-ASSISTED PREFORMED PROSTHESIS FOR REPAIR OF CRANIAL DEFECTS 193
A B C
I
F i g u re 5.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8194
COMPLICATIONS AND POSTOPERATIVE COURSEHematoma, infection, seizures, cere b rospinal fluidleak, and skin dehiscence may occur. With the inten-tion of early detection of any acute postoperativecomplication, a 3D reconstruction of the skull ismade from a 1-mm CT slice, within the first 24hours, to assess the fit of the implant. Patients aregenerally sent home 1 day after surgery and re t u rn to the outpatient clinic 1 week later. At that time,xenon-enhanced CT, transcranial cerebral oximetrywith orthostatic challenge, neuropsychiatric analysis,and plasma anti-epileptic drug levels are measure d .
CONCLUSIONC o m p u t e r-aided cranial implant design and fabrica-tion pro c e d u res appear to provide a better qualityp roduct, a “near perfect” custom fit to the individualpatient, thereby decreasing patient risk in the formof reduced operating room time and better implantfit and function. Computer-aided preoperative im-plant manufacture methods yield cost savings as aresult of reduced operating room time and short-ened hospital stays for patients requiring implants u rg e r y .

INTRODUCTIONIn the last several years, there has been a re n a i s-sance in the neuro s u rgical management of patientswith movement disorders. Advances in anatomicaland functional imaging, improvements in physiologi-cal localization techniques, the wide availability ofs t e reotactic systems, and the realization of the limi-tations of medical therapy have all been instrumen-tal in the re s u rgence of surgery for the treatment ofmovement disord e r s .
C u r rently, stereotactic thalamotomy and postero-ventral pallidotomy are the most commonly employedlesioning pro c e d u res for movement disorders. De-spite being effective, lesioning has implicit limita-tions. Lesioning offers a one-time benefit and is notadaptable to clinical changes or disease pro g re s s i o n .Additionally, the irreversible nature of lesioning canresult in significant morbidity, particularly with bi-lateral pro c e d u res. Complications associated withthalamotomy include speech disturbances such asdysarthria, cerebellar signs, gait difficulties, and cog-nitive dysfunction. Complication rates as high as
CHRONIC SUBTHALAMIC NUCLEUS STIMULATION
FOR PARKINSON’S DISEASE ALI R. REZAI, M.D.
WILLIAM HUTCHISON, PH.D.ANDRES M. LOZANO, M.D., PH.D.
195
© 1999 The American Association of Neurological Surg e o n s
60% have been reported with bilateral thalamotomy.In patients undergoing pallidotomy, cognitive, speech,m o t o r, and visual field deficits have been re p o r t e d .
An increasingly utilized alternative mode of ther-apy is chronic electrical stimulation of specific intra-cranial structures, also called deep brain stimulation(DBS). DBS involves the placement of multicontacte l e c t rodes in the thalamus, basal ganglia, or whitematter tracts. The exact mechanism of DBS action isunknown. However, prevailing theories implicate adepolarizing blockade or “jamming” of neurons and/or axonal tracts resulting from high-frequency stimu-lation. This chronic stimulation effectively mimics alesion, but is re v e r s i b l e .
The major advantage of DBS is its adjustable andreversible feature, allowing for maximal efficacy whileminimizing complications. Currently the most com-mon application of DBS is thalamic (ventralis inter-medius (VIM)) stimulation for refractory tremor (es-sential tre m o r, Parkinson’s disease, cerebellar) andpallidal stimulation for rigidity from Parkinson’s dis-ease. The improved patient safety and the strikingbenefits of DBS have expanded the possibilities ofintervention into new targets. One such target area ofi n c reasing attention is the subthalamic nucleus( S T N ) .

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8196
The STN plays a crucial modulatory role in influ-encing the basal ganglia projections to the motorthalamus and the brainstem. Although a logical tar-get for intervention, the association of the STN withhemiballismus has been worrisome. Recently, how-e v e r, reports from several centers have shown safetyand efficacy of bilateral STN stimulation for Parkin-son’s disease. These studies have demonstrated thatc h ronic high-frequency bilateral STN stimulationresults in improvements in all of the cardinal motormanifestations of Parkinson’s disease (akinesia,bradykinesia, rigidity, and tremor), including themost resistant and disabling axial components ofgait, posture, and balance. The overall results havebeen very encouraging and, at times, dramatic.
ANATOMY AND PHYSIOLOGY OF THE SUBTHALAMIC NUCLEUSThe rationale for targeting the STN lies in its distinctanatomical connections to the basal ganglia and thebrainstem (Figure 1). The STN comprises appro x i-mately 540,000 neurons and measures 10 mm(medial-lateral) × 8 mm (anterior-posterior) × 6 mm(dorsal-ventral). It lies inferior to the thalamus, supe-rior to the substantia nigra, and posteromedial to thepallidum and the internal capsule. The STN re c e i v e sinput from the motor cortex as well as inhibitorygamma-aminobutyric acid (GABA) input from theglobus pallidus externus (GPe) via the “indire c t ”pathway. The STN sends excitatory (glutamate) eff e r-ents to the output nuclei of the basal ganglia (i.e.,the globus pallidus internus (GPi) and the substan-tia nigra pars reticulata (SNr)). Additionally, the STNsends projections to the GPe and striatum as well asto brainstem nuclei such as the pedunculopontinenuclei, a nucleus of importance for axial control andlocomotion.
The currently proposed models of basal gangliafunction are based on work in the 1-methyl-4-p h e n y l - 1 , 2 , 3 , 6 - t e t r a h y d ropyridine (MPTP) primatemodel of parkinsonism and studies in patients withParkinson’s disease. These models have shown thatthe degeneration of the substantia nigra pars com-pacta (SNc) and the resultant dopamine deficientstate lead to an overactivity of the STN and GPi/SNr.The increased STN activity is believed to be sec-ondary to the loss of inhibition from the GPe via thei n d i rect pathway. The overactive STN through its ex-citatory projections to the GPi/SNr causes hyperac-tivity in the basal ganglia output, which has also lostits striatal inhibition via the “direct pathway.”
The overall effect in patients with Parkinson’s dis-ease is overactive GPi/SNr nuclei with corre s p o n d i n gexcessive inhibitory (GABA) eff e rents to the motorthalamus and the brain stem. This hyperactive basalganglia output is implicated in the generation of the
symptomatology of Parkinson’s disease causing ab-n o rmalities of the motor thalamus and its upstre a mp rojections (supplementary motor cortex, pre m o t o rcortex, and primary motor cortex) as well as in thebrainstem regions involved with the control of pos-t u re and gait. Indeed, in MPTP-treated primates, do-pamine agonists, radiofrequency lesioning, or chro n i ch i g h - f requency electrical stimulation of the STN re-sult in the resolution of motor dysfunction.
PATIENT SELECTIONThe indications for treating patients using STN stim-ulation are expanding and evolving. Patients consid-e red for STN DBS must be examined by a movementd i s o rder specialist and meet the clinical criteria forthe diagnosis of idiopathic Parkinson’s disease. Theseinclude tre m o r, rigidity, akinesia/bradykinesia, pos-tural instability, and gait disturbance. It is not knownif patients with secondary parkinsonism and the“Parkinson plus” syndrome are suitable candidatesfor STN stimulation.
At our center, STN DBS candidates typically willhave bilateral, axial manifestations of Parkinson’sdisease and are advanced in their disease, with a sig-nificant disability despite optimization of their med-ication regimen. Many also have dyskinesias ands e v e re on-off fluctuations. Advanced age is not neces-sarily a contraindication for the pro c e d u re, as pa-tients in their 80s have successfully undergone DBS.It should be noted that the selection process shouldbe case specific. A patient with predominantly unilat-eral drug-induced dyskinesias may be a better candi-date for pallidotomy than STN stimulation.
S u rgical candidates should not have a bleedingd i s o rder or contraindications to general anesthesia.Patients must be motivated and have sufficient cog-nitive functions and reserves to undergo an awakes u rgery requiring their active participation. Addition-ally, patients and family must be able to eff e c t i v e l yuse the stimulator and be willing to participate inf requent follow-up visits for detailed evaluation andadjustments of the stimulator. Other important con-siderations include living in close proximity to orhaving ready access to a center with expertise inDBS and having re s o u rces to deal with long-termh a rd w a re/system maintenance and associated com-p l i c a t i o n s .
P reoperative InvestigationsAll patients must be evaluated preoperatively in the“ o ff” phase (approximately 12 hours without medica-tion) as well as in the “on” phase (1 hour after theusual morning dose of medication). This baselineevaluation should consist of objective standard i z e dparkinsonian scales incorporated into the Core As-

REZAI ET AL : CHRONIC SUBTHALAMIC NUCLEUS STIMULATION FOR PARKINSON’S DISEASE 197
sessment Program for Intracerebral Tr a n s p l a n t a t i o n(CAPIT), such as the Unified Parkinson’s DiseaseRating Scale (UPDRS), the Hoehn and Yahr stagingscale, and the Schwab and England disability scale.Additionally, all patients should undergo a form a ln e u ropsychological evaluation.
OPERATIVE TECHNIQUEWhenever possible, the patient should undergo thep ro c e d u re in the “off” state, with all medications with-
held overnight. This accentuates the pathophysiologi-cal findings seen with micro e l e c t rode re c o rding andallows for optimal assessment of the intraoperativeclinical improvements in patients with stimulation.
Frame Application and S t e reotactic ImagingAny one of several commercially available stere o t a c-tic frames can be applied under local anesthesia (1:1m i x t u re of 0.25% bupivacaine and 2% lidocaine).This can be perf o rmed in the operating room or in a
F i g u re 1. Schematic diagram demonstrating the inhibitory (GABA, blue arro w s) and excitatory (glutamate, red arro w s) pro-jections between the striatum, the subthalamic nucleus (STN), basal ganglia, motor thalamus, brainstem locomotion/gaitcenters, and cortical motor areas. Note the excitatory projection of the STN to the output nuclei of the basal ganglia: globuspallidus internus (GPi) and substantia nigra pars reticulata (SNr). These output nuclei, in turn, have inhibitory input to themotor thalamus as well as descending inhibitory input to the pedunculopontine (PPN) and the mesencephalic area (MEA) ofthe brainstem (believed to play an important role in axial control of posture and locomotion). The STN receives inhibitoryinput from the globus pallidus externus (GPe) via the “indirect pathway,” whereas the GPi receives inhibitory pro j e c t i o n sf rom the striatum via the “direct pathway.” Not all projections (including the cholinergic pathways) are demonstrated in thisdiagram. The PPN/MEA also have re c i p rocal ascending input to the Gpe, GPi/SNr, STN, thalamus, and striatum. The sub-stantia nigra pars compacta (SNc) with its dopaminergic projections to the striatum is also not shown. In Parkinson’s dis-ease, degeneration of the SNc results in the loss of dopaminergic input to the striatum. This causes a hyperactivity of theGPi/SNr secondary to loss of inhibition via the direct pathway and hyperactivity of the STN via loss of inhibition through thei n d i rect pathway.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8198
p ro c e d u re room adjacent to the imaging suite. At ourinstitution, we use the Leksell G frame (Elekta, Inc.,Atlanta, GA) which can be attached to the skull withsharp pins or with carbon fiber pins inserted intoholes drilled into the outer table of the skull. Thes u rgeon also has the option of applying ear bars toassist in frame alignment. Most patients, however,find the ear bars to be uncomfortable. The frameshould be applied such that it is parallel to the ante-rior commissure (AC)-posterior commissure (PC)line. As a guideline, an imaginary line from the exter-nal auditory meatus to the lateral canthus cana p p roximate this AC-PC line.
After frame application, the magnetic re s o n a n c eimaging (MRI) or computed tomography (CT) localizer(fiducial box) is attached to the frame and the patientu n d e rgoes either CT or MRI for anatomical localiza-tion. Ventriculography is not used in most centers asthe currently available MRIs with high-re s o l u t i o nvolumetric acquisitions obviate the need for thisinvasive technique. MRI has a higher anatomical re s-olution than CT, but is more prone to distortions inspatial accuracy. Any of the currently availablei m a g e - c o r rection algorithms or MRI-CT image fusions o f t w a re can minimize these distortions.
At the To ronto Hospital, we use a Signa 1.5-teslaMRI magnet (General Electric, Milwaukee, WI). Afterthe initial image acquisition, a midline sagittal sliceis chosen to best identify the AC and the PC. A sub-sequent volumetric scan is perf o rmed along the AC-PC line providing coronal, sagittal, and axial images.The sections are 1 mm thick and non-overlapping.Images are acquired using a gradient echo sequencewith a relaxation time of 43 msec and an excitationtime of 13 msec (flip angle 450, FOV 24 × 24, matrix256 × 2 5 6 ) .
Anatomical Ta rget LocalizationAnatomical localization of the STN can be achievedin two ways: 1) direct targeting; or 2) indirectly usinga standardized anatomical atlas as a function of theAC and PC. For direct targeting, STN can be visual-ized on coronal T2-weighted MRI or various othersequences such as an inversion recovery sequence.On axial MRI, the STN is located anterolateral to thered nucleus and posterior to the cerebral peduncle.
At our institution, we utilize the anatomical brainatlas method for targeting. On MRI and/or axial CTslices, the stereotactic x, y, and z coordinates of theAC and PC are calculated using the MRI/CT consoles o f t w a re program. The calculated AC and PC stere o-tactic coordinates are fed into a computer with ac o m m e rcially available program containing digitizeddiagrams of sagittal brain sections from a standard-ized brain atlas (G Schaltenbrand, W Wa h ren: A t l a sfor Stereotaxy of the Human Brain. 2nd ed, 1977).The program transcribes the patient’s calculated AC-
PC intercommissural line onto the digitized map atthe sagittal laterality of interest. We usually startwith the laterality of 12 mm from the midline thatc o r responds to the plane with the maximum diame-ter of the STN in an anteroposterior direction. To cor-rect for individual variations in the AC-PC distance,this corresponding 12-mm sagittal map is shrunk ors t retched and re f o rmatted to the length of the inter-commissural line for each specific patient. The sub-sequently generated brain map is overlaid onto amillimeter grid ruled in stereotactic coordinates inthe anteroposterior and dorsoventral scales with ac o r responding diagram of the brain nuclei and tractsdepicted in the chosen laterality (Figure 2). Our finalanatomical target is chosen at the center of the STNon this re f o rmatted brain map. Typically, structure se n c o u n t e red in our trajectories include the anteriorthalamic nuclei such as the nucleus reticularis, ven-tralis oralis anterior, ventralis oralis posterior nuclei,zona incerta, H2 fields of Forel, STN, and SNr/SNc inthe midbrain.
S u rgical Pro c e d u reSubsequent to stereotactic CT/MRI image acquisitionand anatomical target localization, the patient istaken to the operating room and placed in a supineposition, with the head elevated approximately 30 de-g rees. Intravenous prophylactic antibiotics are ad-m i n i s t e red. The frontal region is shaved and pre p p e din the standard fashion. The pro c e d u re is perf o rm e dwith the patient under local anesthesia with 2% Xylo-caine. A 5-cm linear or curvilinear incision is made2.5 cm lateral to the midline and centered anterior tothe coronal suture. Raney clips are placed for hemo-stasis, and a self-retaining retractor is applied. Usinga 14-mm diameter drill bit on a power drill, a burrhole is made anterior to the coronal suture. The durais coagulated and incised, in a cruciate fashion. Thepial surface is also coagulated and incised, avoidings u rface vessels. Fibrin glue is applied to minimizec e re b rospinal fluid leaks and entry of air into the cra-nial cavity. When perf o rming simultaneous bilateralSTN pro c e d u res, an identical sequence of steps iscarried out on the opposite side. The stereotactic arcis then applied, and the x, y, and z coordinates for theanatomical STN target are set. A guide tube cannulawith a blunt tip stylet is then introduced into thebrain parenchyma to a point 10 mm proximal to thechosen target. Physiological localization begins at thistime, with the ultimate aim of correlating the anatom-ical and physiological findings.
Physiological Ta rget Localization In our experience, physiological localization is man-datory for definitive target determination. Sole re-liance on anatomical localization can be pro b l e m a t i cbecause of the frequent discrepancy between the

REZAI ET AL : CHRONIC SUBTHALAMIC NUCLEUS STIMULATION FOR PARKINSON’S DISEASE 199
F i g u re 2. A 12-mm sagittal map of the Schaltenbrand and Wa h ren A t l a s re f o rmatted to anactual AC-PC distance of a patient and ruled in stereotactic coordinates for the Leksell frame. A typical trajectory of the micro e l e c t rode through various nuclei is depicted. Each gradation is1 mm. The + in the center of the subthalamic nucleus (STN) re p resents the chosen anatomicalt a rget. This point is annotated as 0 on the trajectory. H2 = fields of Forel, Hpth = hypothala-mus, IC = internal capsule, mcp = midcommissural point, Rt = nucleus reticularis of the thala-mus, SNr = substantia nigra pars reticulata, Vim = ventralis intermedius, Voa = ventralis oralisa n t e r i o r, Vop = ventralis oralis posterior, ZI = zona incerta.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8200
expected location and actual position of the stere o-tactic targets. Physiological corroboration can beachieved with micro e l e c t rode re c o rding and stimula-tion and/or macrostimulation. Macro e l e c t rode stim-ulation is rapid and re q u i res minimal equipment.H o w e v e r, it has low spatial resolution and is not ableto re c o rd neurons and to discriminate between axonsand neurons. Micro e l e c t rodes, however, provide ex-quisite physiological identification of receptive fieldsand neuronal firing patterns via direct measures ofindividual single-unit neuronal activity and are ableto distinguish somatodendritic from axonal activity.We rely exclusively on micro e l e c t rode re c o rding andstimulation for STN localization. Micro e l e c t rodes pro-vide precise mapping information, which guides thes u rgeon in determining the most optimal location forfinal electrode implantation.
The micro e l e c t rodes are made of Parylene-C insu-lated tungsten electrodes plated with gold and plat-inum. Tip lengths range from 15 to 40 µm withimpedance of 0.2 to 0.5 MOhm. The micro e l e c t rode ishoused in its own guide tube, which is the samelength as the larger guide tube described above. Amanual hydraulic microdrive is used to advance them i c ro e l e c t rode in submillimeter steps beyond themost distal aspect of the cannula into the brain pa-renchyma (typically 10 mm superficial to the chosenanatomical STN target (Figure 2)). The electrical sig-nal derived from single- and multi-unit neuronal re-c o rdings is amplified, filtered, displayed on an oscil-loscope, and fed to an audio monitor. A windowdiscriminator is used to determine the discharge fre-quency of the re c o rded units. Thus the relative sizeand shape of the action potential is visualized, audiomonitoring of neuronal activity is achieved, and thefiring frequency of individual neurons determined.
As an adjunct to micro e l e c t rode re c o rding, micro-e l e c t rode stimulation is perf o rmed by passing electri-cal current of 0.1 to 100 µA (1-second train, 300 Hz,and 100-µsec pulse width) through the tips of thee l e c t rode. The re c o rding is typically perf o rmed con-tinuously, whereas stimulation is done every 1-2 mm.The clinical stimulation responses are corre l a t e dwith electrical thresholds to further determine thep roximity to a given location. Usually, the lower thet h reshold of stimulation, the closer the proximity tothe area of intere s t .
In a typical STN case, three or four trajectories( a n t e r i o r, posterior, medial, and lateral) are made forphysiological localization. With simultaneous bilat-eral pro c e d u res, the opposite side usually re q u i re sone or two trajectories because of the brain symme-try. Trajectories are made by removing the guidetube assembly and moving the arc in the desire dd i rection in increments of 2-3 mm.
The ultimate goal of physiological localization is toidentify the STN. In order to accomplish this, struc-
t u res anterior (internal capsule), dorsal (zona in-certa), superior (zona incerta, nucleus re t i c u l a r i s ,and the ventralis oralis anterior and posterior), andventral (SNr) must be localized (Figure 2). The char-acteristic frequencies of cellular activity encountere din each of these structures are shown in Figure 3.
PHYSIOLOGICAL LOCALIZATION OF SPECIFIC STRUCTURESAnterior Thalamic Nuclei: Nucleus Reticularis,Ventralis Oralis Anterior and PosteriorT h e re are two characteristic types of neuro n sobserved in the anterior thalamic nuclei. One type iscalled a “bursting cell,” which has a slow firing rateinterposed by characteristic rapid bursts of activity.These cells usually have a firing rate of 15 to 25spikes/second but the bursts can reach firing ratesup to 300 or 400 spikes/second. These characteris-tic bursting cells have also been described in otherthalamic regions as well as in re c o rdings from labo-ratory animals. The other major cell type is a non-bursting but irregular firing cell. These have firingrates ranging from 15 to 25 spikes/second and maybe cells of the nucleus reticularis, the ventralis oralisa n t e r i o r, or the ventralis oralis posterior.
Zona Incerta and Fields of Forel As the micro e l e c t rode passes ventrally to the anteriorthalamic nuclei, a relatively quiet region is encoun-t e red. This is the thalamic fasciculus (H1 fields ofF o rel), which contains pallidofugal fibers with veryfew cells. The zona incerta is a thin strip of gray mat-ter below this fiber tract with a variable re c o rd i n gp a t t e rn. Occasionally, we have re c o rded larg e - a m p l i-tude re g u l a r-firing or, less frequently, burst-firingn e u rons from this region in the range of 25 to 45spikes/second. Alternatively, the zona incerta can bea relatively quiet region. Ventral to the zona incerta isthe lenticular fasciculus (H2 fields of Forel) contain-ing pallidofugal fibers, which is also a relatively quietregion.
Subthalamic NucleusAs the micro e l e c t rode enters the STN, an increase inb a c k g round noise is detected reflective of a region ofi n c reased cellular density. In Parkinson’s disease pa-tients in the “off’ state, STN neurons have an irre g u-lar firing pattern with a mean rate of 37 Hz (range 25to 45 Hz). The cellular activity in the dorsal portion ofthe STN can be modulated by active and/or passivemovements of limbs. These movement-related re-sponses are clear, re p roducible, and should beactively sought during the re c o rding. The ventralaspect of the STN may also have movement-re l a t e dn e u rons, but in our experience these are more pre v-alent in the dorsal regions.

REZAI ET AL : CHRONIC SUBTHALAMIC NUCLEUS STIMULATION FOR PARKINSON’S DISEASE 201
In the patient with clinically apparent tre m o r,cells with spontaneous discharge rates synchro n o u swith the tremor (i.e., “tremor cells”) can be observed.M i c rostimulation can result in tremor reduction ort remor arrest. In addition to tremor cells, occasionalbursting cells can be encountered in the STN, butwith less prevalence than in the anterior thalamicnuclei. Microstimulation can occasionally result inthe patient experiencing paresthesias, pre s u m a b l yf rom current spread to the medial lemniscus. Inm o re anterior and lateral trajectories, axons of thei n t e rnal capsule are encountered and, with micro-stimulation, contralateral muscle contraction can beo b s e r v e d .
Substantia Nigra Pars Reticulata and Pars Compacta The substantia nigra pars reticulata and pars com-pacta lie ventral and posterior to the STN and arecharacterized by cells with a regular pattern of firingwith higher rates than the STN (mean 71 Hz, range60 to 80 Hz). Occasionally, cells can be found thatrespond to saccades. Microstimulation (particularlyin the medial regions of the SNr) can result in ocular
deviation due to current spread to the oculomotornerve fascicles. Occasionally, paresthesias can bereported, presumably from current spread to the pos-teriorly located medial lemniscus.
The characteristic physiological findings of micro-e l e c t rode re c o rding and stimulation are summarizedin Table 1. The physiological information derived fro mthe corresponding micro e l e c t rode re c o rding (re c e p-tive fields) and micro e l e c t rode stimulation (pro j e c t e dfield) along each tract/trajectory is annotated on the corresponding stereotactic brain maps, allowingsimultaneous visualization and correlation of thephysiological and anatomical findings (Figure 4).This assists in the selection of the optimum locationfor implantation of the DBS electrode.
IMPLANTATION OF THE DBS ELECTRODE General principles guiding the final implantation ofthe electrode involve placement of the electrode at aregion allowing for maximal clinical response whileminimizing the undesired side effects. The ideal loca-tion for the placement of the electrode is in the tra-jectory, which is traversing the midportion of the
F i g u re 3. Graph showing the mean neuronal firing frequencies (spikes/second) of neuro n se n c o u n t e red in trajectories traversing the anterior thalamus, STN, and SNr. The anterior thal-amic nuclei consist of the nucleus reticularis, ventralis oralis anterior, and ventralis oralisp o s t e r i o r. AnTh-B = anterior thalamic cells with bursting characteristics; AnTh-NB = anteriorthalamic cells with no bursting activity.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8202
STN with the most distal lead being placed in themost ventral portion of the STN. This arrangementallows for the contacts/poles to be within the STN,thus providing maximal programming possibilities.
The DBS electrode we currently use is a quadripo-lar electrode (Figure 5) supplied by Medtronic, Inc.(Minneapolis, MN). Each pole/contact is made ofcylindrical platinum/iridium alloy and is 1.5 mm inlength, separated from the other pole by an insulateddistance of 1.5 mm or 0.5 mm, depending on themodel (Figure 5). The diameter of the electrode is1.27 mm, and the entire electrode length can be 28or 40 cm, depending on the model.
To confirm the position and trajectory of theactual DBS electrode, the use of intraoperative x-rayor fluoroscopy is mandatory. This is accomplishedvia a beam orthogonal to the stereotactic frame. At this time, the x, y, and z coordinates of the deter-mined target are set on the frame. A lead holderassembly (Medtronic) is attached to the frame. Thisassembly device stabilizes and secures the DBS elec-t rode and the cannula. A stylet-coupled cannula (1.6mm in diameter) is inserted to the target under fluo-roscopic guidance and verification. Subsequently,the DBS electrode is inserted under fluoro s c o p i c
guidance to the target and the cannula is re m o v e d( F i g u re 6). The mere introduction of the cannula/DBS lead causes the patient to exhibit dyskinesiasand chore i f o rm movements, which is a good pro g-nostic sign that clinically verifies the target.
At this time, intraoperative test stimulation is p e rf o rmed by attaching the proximal portion of theDBS lead to a hand-held pulse generator device( S c reener). The patient is tested at the most pro x i m a land distal pole combinations for therapeutic andadverse effects. If adverse effects (motor contraction,p a resthesias, or ocular deviation) are persistent atlow thresholds (<2 V, ≥120 Hz, 60 msec), the elec-t rode may be repositioned to a more favorable sitea c c o rding to the anatomical/physiological map.Finally, the stylet is removed and the DBS electro d eis anchored to the burr-hole ring (a plastic ring de-signed to fit the 14-mm burr hole) by wedging thee l e c t rode into one of its two grooves. An additionalplastic burr-hole cap further locks the DBS lead intothe burr hole ring. This maneuver is designed to pre-vent lead migration, which was a significant pro b l e min the past. At this time, final fluoroscopic imaging isp e rf o rmed for verification. For simultaneous bilateralSTN electrode implantation, the same pro c e d u re is
Table 1Characteristic Physiological Findings Using Microelectrode Recording and Stimulation
Structure Microelectrode Recording Microelectrode Stimulation
Thalamic nuclei: Bursting cells No clinical effectreticularis, ventral oralis anterior and posterior
Zona incerta Sparse cells (bursting) No clinical effect
Subthalamic nucleus Irregular firing pattern Tremor arrestMean rate (37 Hz) Paresthesias‡ Range (25-45 Hz) Contralateral muscle contraction*Movement responsiveNeuronsTremor cells
Subtantia nigra: Regular firing pattern Ocular deviation†pars reticulata Mean rate (71 Hz) Paresthesias‡pars compacta Range (60-80 Hz)
Saccade and movement responsive Neurons
‡Paresthesias are most likely due to current spread to the medial lemniscus.*Contralateral muscle contraction secondary to current spread to the internal capsule.†Ocular deviation secondary to stimulation of third cranial nerve.

REZAI ET AL : CHRONIC SUBTHALAMIC NUCLEUS STIMULATION FOR PARKINSON’S DISEASE 203
F i g u re 4. M i c ro e l e c t rode re c o rding findings of three trajectories superimposed on the 12-mm lateral sagittal brain map areused for initial anatomical targeting as shown in Figure 2. Each gradation is 1 mm. Black circ l e s re p resent single unit cellu-lar re c o rdings. The corresponding frequencies are shown. Solid bars = quiet regions with sparse neurons; red dots = neu-rons responsive to passive and active movements of areas depicted by red circ l e s; hfd = high frequency discharge >80 Hz;BC = cells with characteristic bursting activity; red P = paresthesias experienced with microstimulation in the distal lowere x t remity, most likely due to current spread to the medial lemniscus; hpth = hypothalamus.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8204
F i g u re 5. The quadripolar DBS electrode. Each pole/contactis made of cylindrical platinum/iridium alloy and is 1.5 mm inlength and 1.27 mm in diameter, separated from the otherpole by an insulated distance of 1.5 mm (Model 3387, l e f t) or0.5 mm (Model 3389, r i g h t). (Courtesy of Medtro n i c )
F i g u re 6. Intraoperative stereotactic radiograph of the DBS electro d eat the target. The electrode is introduced from a pre c o ronal burr holeand directed posteriorly and ventrally. The position of the electrode ism o n i t o red via fluoroscopy. The black circ l e re p resents the targ e t ,which is also the center of the stereotactic ring. Note the appearance ofthe four contacts/poles and the cannula, which has been withdrawnp ro x i m a l l y .

REZAI ET AL : CHRONIC SUBTHALAMIC NUCLEUS STIMULATION FOR PARKINSON’S DISEASE 205
repeated on the opposite side. Alternatively, theopposite side can be implanted at a later time. Weroutinely implant bilateral STN stimulators simulta-n e o u s l y .
After DBS implantation, intraoperative test stimu-lation, and securing of the DBS electrode, one canp roceed directly to the implantation of the pulse gen-e r a t o r. Alternatively, the DBS lead can be connectedto a percutaneous extension for prolonged testingand obtaining imaging studies prior to perm a n e n ti n t e rnalization with the pulse generator.
PULSE GENERATOR IMPLANTATIONThis stage of the pro c e d u re should be carried outwith the patient under general anesthesia as it re-q u i res a tunneling pro c e d u re that can cause signifi-cant discomfort and anxiety. Intravenous pro p h y l a c-tic antibiotics are administered. The patient ispositioned in a similar fashion as for a ventriculoperi-toneal shunt, placed supine with the head turn e dt o w a rd the opposite side, with a shoulder roll on theipsilateral side. A 5-cm horizontal incision is madebelow the clavicle and a subcutaneous pocket ismade for placing the generator. The implantablepulse generator (IPG) device (Itrel II, Medtronic) isp o w e red by a lithium battery and is fully pro g r a m m a-ble via telemetry (Figure 7). The scalp opening is con-nected to the infraclavicular opening using a tunnel-
ing device similar to a shunt passer (provided byM e d t ronic). An electrode extension wire is passed re t-rograde from the infraclavicular opening to the scalp.The distal end of this extension is connected to theIPG device. The pulse generator is sutured to the pec-toralis fascia to prevent migration. Similarly, at thecranial opening, the proximal portion of the extensionw i re is connected to the proximal portion of the DBSlead by tightening the four screws. A plastic cover/sheath is place over the connector and sutured atboth ends to keep fluids out and maintain contactpoint isolation. Finally, a two-layered standardwound closure is perf o rmed (Figure 8). Figure 9 dem-onstrates the final position of the DBS electro d e swith postoperative MRI.
DEEP BRAIN STIMULATION PROGRAMMINGThe goal of DBS programming is to provide the bestclinical response with minimal or no side effects. DBSp rogramming is achieved via a telemetry device capa-ble of adjusting parameters such as the choice ofpoles, mode of stimulation, frequency, pulse width,amplitude, and continuous or cycling stimulation.
The mode of stimulation can be unipolar, bipolar,or multipolar. Each of the four poles/contacts (desig-nated as 0, 1, 2, or 3) can be positive, negative, or off .The direction of current is from cathode (–) to anode
F i g u re 7. The implantable pulse generator (Itrel II) unit is powered by alithium battery and fully programmable via telemetry. The quadripolarDBS electrode is also shown. (Courtesy of Medtro n i c )

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8206
(+) in bipolar stimulation, and the case of the IPGdevice serves as the ground for unipolar stimulation.The amplitude of stimulation can range from 0.1 to10 V (usually 2 to 3.5 V for STN). The fre q u e n c y(number of pulses/second) can go as high as 185 Hzwith the currently available models. Like thalamic(VIM) stimulation for tre m o r, effective STN stimula-tion is best achieved using a high frequency (≥ 1 2 0Hz). The pulse width (duration of pulses) is com-monly 60-90 µsec.
Choosing the optimal stimulation parameters canbe a complex task and can re q u i re hours of pro g r a m-ming. Most stimulation parameter adjustments aremade in the initial 1-3 months after implantation.After this period, stimulation parameters usually re-main stable. The patient also has the capability tot u rn the stimulator off and on with a hand-heldmagnet. The life expectancy of the pulse generatorvaries depending on the parameter and duration ofstimulation. In general, a pulse generator can beexpected to last 3 or 4 years.
The multiple combination of stimulation settingsis particularly advantageous as it allows the bestclinical response to be achieved with the fewest sidee ffects. The determination of the optimal selectionparameters, however, is individualized. Each time asetting is changed, the patient must be assessedobjectively and subjectively in a systematic and con-sistent fashion. This process can consume much
F i g u re 8. Composite photograph showing the overall con-figuration/positioning of the implanted bilateral DBS elec-t rodes, connectors, and pulse generators.
F i g u re 9. Postoperative T1-weighted MRI, axial ( A ) and sagittal ( B ) views, demonstrating the final position of the DBS electro d e s .
A B

REZAI ET AL : CHRONIC SUBTHALAMIC NUCLEUS STIMULATION FOR PARKINSON’S DISEASE 207
time and re s o u rces, particularly with bilateral STNstimulation. Patients with advanced disease andaxial symptomatology re q u i re more frequent adjust-ments and careful clinical evaluation, while thosewith tre m o r-dominant Parkinson’s disease re q u i reless programming. An experienced team with avail-able re s o u rces is re q u i red to achieve these goalsmost efficiently and eff e c t i v e l y .
CLINICAL OUTCOME AND COMPLICATIONSThe reversible and adjustable features of DBS tech-nology have permitted its application to the STN inthe patient with advanced, bilateral, and medicallyrefractory Parkinson’s disease. DBS not only pre-vents undesired side effects, but also can be adapt-able as the symptoms change or the disease pro-g re s s e s .
T h e re have been several recent reports of follow-upwith chronic high-frequency bilateral STN stimula-tion. These studies have documented striking im-p rovements in parkinsonian symptoms. Impro v e-ments in overall “off” state UPDRS motor scores havebeen 60% or greater with the most striking impro v e-ment in tre m o r, followed by akinesia/bradykinesiaand rigidity, as well as significant improvements ingait. There have also been significant impro v e m e n t sin dyskinesias and on/off motor fluctuations, as wellas reduction in the use of drugs by 40%-50%. In ourown series of patients who have undergone chro n i ch i g h - f requency bilateral STN stimulation, we have ob-served total UPDRS motor score improvements in themedication “off” state of 63%, including tremor (82%),akinesia (62%), rigidity (60%), and gait and posturalinstability (51%). In the “on” state, the overall im-p rovement of total UPDRS motor scores was 47% andL-dopa-induced dyskinesias were reduced by 76%with total drug dosage being decreased by 40%.
The complications associated with STN DBS canbe categorized as those related to the surgical pro c e-d u re, stimulation, and technical/equipment. Thecomplications of the surgical pro c e d u re are similarto those seen following other stereotactic DBS orlesioning pro c e d u res. The most serious complicationi n h e rent to any intracranial stereotactic pro c e d u re isthat of intracranial hemorrhage, which occurs on theo rder of 1%-3%. The additional small risk of pneu-mocephalus is minimized by sealing the dural open-ing with fibrin glue. Transient complications such asintraoperative and postoperative confusion and agi-tation have also been seen (up to 2 weeks), but mostcommonly in older individuals. Other complications
have involved neuropsychiatric changes with subtlememory deficits, word finding and concentration dif-ficulties, and personality changes.
The stimulation-induced side effects includeapraxia of eyelid opening, diplopia, paresthesias, andinvoluntary movements such as chorea, all of whichcan be alleviated by adjusting stimulation settings.Transient hemiballism has also been observed withstimulation. The potential hard w a re - related compli-cations are on the order of 1%-3% and include elec-t rode migration, breakage, disconnection, skin ero-sion, and equipment failure. Additionally, there isa p p roximately a 5% chance of infection that is mostoften superf i c i a l .
PRACTICAL CONSIDERATIONSImportant issues to take into consideration in theinitial decision-making process include the cost of abilateral system and the long-term system mainte-nance (including equipment-related complicationsand battery replacement). Another consideration isthe proximity of the patient or ready access to a cen-ter with expertise in the management of DBS. Addi-tionally, programming can re q u i re significant timeand re s o u rce expenditures. A center dedicated tothis endeavor must be carefully planned and haveadequate re s o u rces for the long term. Finally, pa-tients must be willing and have the ability to cooper-ate with the extensive evaluation and prolonged pro-gramming that may be necessary to reach theoptimal settings.
CONCLUSIONThe reversible and adjustable features of DBS tech-nology have allowed its application to the STN. TheSTN is an ideal target in patients with Parkinson’sdisease, because of its overactivity and its pro j e c-tions to the basal ganglia output nuclei (GPi/SNr).Single cell micro e l e c t rode re c o rding technology canp recisely and re p roducibly localize the STN. STNn e u rons have an irregular firing pattern with a firingrate in the range of 25-45 Hz. They can also exhibitm o v e m e n t - related activity and/or activity in syn-c h rony with the tre m o r. Micro e l e c t rode stimulationis less useful for STN localization.
Although complications related to the pro c e d u re ,h a rd w a re, and stimulation can occur, the overallmarked benefits obtained by these disabled patientsoutweigh the adverse effects. In patients with ad-vanced Parkinson’s disease, bilateral STN DBS re-sults in a definitive improvement in all of the card i-nal motor manifestations of Parkinson’s disease.


INTRODUCTIONMinimally incisional spine surgery is undergoing arevolution at the current time. Over the last decade,we have seen advances in anesthetic techniques,coupled with technical advances in the size, diversity,and scope of the instruments available to the sur-geon. With those advances have come radically diff e r-ent attitudes toward the possibilities of minimallyincisional surgery. Orthopedic and neurological sur-geons have had at their disposal a variety of surg i c a ltechniques to approach the lumbar disc since it wasfirst approached in 1934. The evolution of these tech-niques has revolved around the need to remove theo ffending material and reduce the patient’s pain,while preserving neurological function. Althoughfraught with complications, the “open” pro c e d u re isone of the most common techniques for alleviatingpain in this area and remains a pro c e d u re commonlyp e rf o rmed by orthopedic and neurological surg e o n s .The percutaneous approach utilizing the endoscopeextends the knowledge that we have acquired overthe past 50 years. This approach dates to 1951, whenHope described an anterior re t roperitoneal appro a c hto the disc space. In 1975, Hijikata expanded this ap-p roach when he described the percutaneous tech-nique. Kambin has pioneered and extensively devel-
A RTHROSCOPIC MICROLUMBAR DISCECTOMY
KENNETH F. CASEY, M.D.PARVIZ KAMBIN, M.D.MARC CHANG, M.D.
209
oped instruments for targeted posterior fragmentec-tomy, herein called arthroscopic microlumbar discec-tomy. In 1982, Kambin described the technical as-pects of the operation as we shall describe it in thisc h a p t e r. Since that time, the further development ofinstrumentation has made this technique one that,with the appropriate training, can be a part of thea rmamentarium of all spine surg e o n s .
PATIENT SELECTIONPatients are selected for arthroscopic micro l u m b a rdiscectomy as they would be for any discectomy ap-p roach. Patients with a history of lumbar root symp-tomatology of either myotomal loss, dermatomal pain,or/and sensory loss are candidates. Patients usuallyhave not responded to conservative therapy. Conserv-ative therapy persists for a period of not less than 6weeks nor longer than 18 weeks, and consists ofland- or water-based exercises for flexion/extensionof the spine. Patients who present with motor loss orother acute neurological syndromes can certainly beevaluated and treated more promptly as the situationdictates. At the conclusion of the conservative ther-apy phase, patients should undergo imaging studies.At the current time, magnetic resonance imaging(MRI) of the spine aff o rds the most compre h e n s i v eview as to the origin, extent, and contributing factorsof compressive nerve root pathology. Patients with ac l e a r-cut single-level root symptom ideally pre s e n twith MRI evidence for focal disc pathology. In someinstances, disc pathology may be combined with aminimum of anterior bony disease causing a mini-© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8210
mum of lateral recess stenosis. Patients whose imaging studies reveal extensive
lateral recess stenosis, focal bilateral stenosis, or ad-ditional other bony pathology would not be candi-dates for this lateral extracanalicular approach. Inaddition, local instability such as antero- or re t ro l i s-thesis is a relative contraindication to the pro c e d u re .Also not feasible for removal due to limitations withthe equipment is disc material that has migrated theequivalent of one disc space level above or below theindex. At the time of counseling for endoscopic sur-gery, patients are advised of the possibility of conver-sion to an open pro c e d u re should the pathology sodictate. Patients with tumors in the foramen, withinthe canal space, and a combination of bony and epi-dural pathology should be counseled as to the lim-ited nature of biopsy in resection possible thro u g hthe scope. However, that is not the subject of thisre v i e w .
The risks and complications of arthro s c o p i cm i c rolumbar discectomy include those experiencedin the open pro c e d u re: 1) infection (seen in 1% to 3%of patients in the current series); 2) failure to re l i e v esymptomatology (seen in 13% of our patients; symp-tomatology was relieved in 87%); and 3) transientworsening of symptomatology (seen in 2% to 4% ofpatients). This worsening takes the form of dysesthe-sia occurring frequently along the anterior aspect ofthe calf or thigh. Dysesthesia is described as burn i n gin nature, occurs most often on Day 5 following thep ro c e d u re, and has been self-limited in most pa-tients. There have been no neurovascular complica-tions to date.
The preoperative selection of the patients is nei-ther age nor sex limited. However, patients who can-not comfortably be positioned in the prone positiondue to orthopedic or soft-tissue deformity of thelower extremities are not candidates. In addition,patients whose anatomical size would preclude theinstrument use are also not candidates. This can bed e t e rmined by a simple measurement from the lat-eral aspect of the disc space to the skin entry pointdescribed in this article. This is best accomplishedusing computed tomography (CT) at the sympto-matic level.
ANESTHETIC TECHNIQUE AND PREOPERATIVE PREPARATIONThe anesthetic technique used is determined by thes u rgical team. Intravenous conscious sedation utiliz-ing fentanyl and midazolam and/or propofol has en-joyed large acceptance in the institutions in whichwe currently practice this surgery. In some patients,h o w e v e r, the use of spinal anesthetics or generalanesthesia is necessary for the successful comple-tion of the pro c e d u re .
During preoperative counseling, some patients
become obvious candidates for general anesthesiawhen their level of anxiety and/or their previous ex-perience with conscious sedation so dictates to theanesthesiologist. The anesthesia of choice, however, isintravenous conscious sedation. Occasionally, whilerelying predominantly on midazolam or propofol, wehave found intravenous ketamine to be useful, espe-cially if the patient is large and the apparent volumeof distribution makes the administration of conscioussedation more challenging. Despite adequate intra-venous sedation for the initial steps of the pro c e d u redescribed here, the occasional patient complains ofpain at the time of manipulation of the annular fibers.We have found that the topical use of fentanyl appliedvia cottonoid patty to the annular fibers has beenhelpful. In some cases, 50 µg fentanyl injected intothe annular fibers will aff o rd and extend relief.
Antibiotics are also administered as part of thep reoperative preparation, including 1 gm Ancef ad-m i n i s t e red intravenously within 1 hour of incision;some patients presenting with penicillin allergies aregiven 120 mg gentamycin intravenously when re n a lfunction is appropriate. Single preoperative dosesa re employed.
PATIENT POSITIONINGPatient positioning commences with the patient beingrequested to turn prone on a radiolucent operatingframe (Kambin Frame, Northstar Medical, Philadel-phia, PA), which allows for the straightening of lum-bar lordosis and gentle positioning and cushioning ofthe chest and hips (Figure 1). The arms are bro u g h tup alongside the patient’s head and the legs areflexed over two pillows. To avoid the complication ofstrap pre s s u re, adequate padding is re q u i red over thelower extremities. The fibular head can inadvertentlybe trapped under the operating table belt. Bladdercatheterization is not generally employed. Pre o p e r a-tively, we utilize the biplanar fluoroscopic x-ray de-vice (OEC Medical Systems, Salt Lake City, UT) toe n s u re proper positioning and readily readable x-rayimages. The surgeon has the option of standing onthe side of the patient ipsilateral or contralateral tothe pathology. The fluoroscopic arm is best posi-tioned opposite the side that the surgeon stands toallow for ease of use during the operation with a min-imum of movement in the area of the field. The cam-era tower (Stryker Systems, Stryker Instruments,Kalamazoo, MI) and additional arthroscopic materialsincluding the printing device are best positioned atthe foot of the patient in clear view of the surgeon. Weusually allow the camera device to be positioned atthe foot of the patient, the x-ray fluoroscopic televi-sion immediately to the surgeon’s left of the camerat o w e r, and the C- a rm device to the left, completing a9 0 - d e g ree arc from the foot of the patient to the pointopposite the surg e o n .

CASEY ET AL : ARTHROSCOPIC MICROLUMBAR DISCECTOMY 211
OPERATIVE TECHNIQUESkin preparation is accomplished utilizing surf a c eagents (e.g., Betadine or alcohol) supplemented withan Ioban drape (3M Corp., Minneapolis, MN) to coverthe entire operative field, three disc levels above andbelow the target level. Laterally, the drape should ex-tend at least 12 cm off the midline. The pre p a r a t i o nis augmented by a shower curtain-type drape (Ioban2 patient isolation system 6617, 3M Corp.). Thisfacilitates manipulation of the biplanar fluoro s c o p eduring the pro c e d u re. The electrocautery device andsuction are positioned at the head or foot of thepatient to facilitate C- a rm movement and to avoidthe lines crossing the patient during x-ray evalua-tion. The C- a rm is ideally positioned in the antero-posterior (AP) plane at the start of the pro c e d u re ,and the angle of the C- a rm is adjusted so that the
disc space is seen straight ahead after the appro p r i-ate disc level has been selected. A line is drawn onthe skin utilizing a marking pen to indicate the levelselected and identified, for example, “L4-5.” Later-ally, the skin entry point 9 to 11 cm from each mid-line is marked and the entry point is selected (usu-ally 9 cm) and infiltrated at the skin level using 0.5%lidocaine without epinephrine. The muscles are infil-trated as well with lidocaine. The instruments useda re the Smith and Nephew arthroscopic surgical sys-tem and Kambin surgical set (Memphis, TN) (Figure2). The camera equipment is a Dyonics Surgical Sys-tem (Andover, MA). We use a Sony color video printerto re c o rd the pro c e d u re. The pictures are useful forreview and teaching purposes.
A 22-gauge spinal needle measuring 18 cm is in-t roduced at the skin entry point at an angle of 35-45
F i g u re 1. Line drawing of a patient in the prone position.
F i g u re 2. The Kambin arthroscopic microlumbar discectomy instruments.

d e g rees. The preoperative imaging study, whether CTor MRI, may be utilized to determine the exact angleof entry as measured from the triangular workingzone to the point of entry on the skin. The triangularworking zone (Figure 3) is the annular entry portt h rough a posterolateral approach that is form e danteriorly by the descending spinal nerve from thelevel above, inferiorly by the proximal plate of theinferior vertebrae, and posteriorly by the pro x i m a larticular process of the lower lumbar segment.
As the needle is introduced and penetrates thes a c rospinalis, quadratus lumborum, and psoas ma-jor muscles, it is gently rotated to allow the bevel tocarry the needle through a straight line toward thet a rget level. The biplanar fluoroscopic arm can be uti-lized to check the pro g ress of the needle. The needlehas entered the triangular working zone when the tipof the needle seen in the AP projection lies at the lat-eral margin of the bipedicular line formed by the ipsi-lateral outer margin of the pedical above and belowthe disc space selected. In the lateral view, the needlewill lie just at the inferior margin of the disc space at the level selected (Figure 4). Needle geometry isimportant so as to avoid too steep an entry anglewhich would project the surgeon past the disc spaceand into the re t roperitoneal structures or too shallowan angle which would project posteriorly behind thelamina and other spinal structures. Needle geometryis also important so as to avoid too lateral an entry,which carries the potential to traverse the peritonealspace prior to entering the re t roperitoneal muscles.The biplanar fluoroscopic C- a rm images are mosthelpful in avoiding incorrect needle positioning whenseen in true orthogonal relationship. A technical notere g a rding the L5-S1 disc space: This disc space isbest approached by imaging the sharp angle of theendplates in the lateral view and projecting that pointto the skin. It will become apparent that to re m a i nparallel with the endplates, the needle entry pointmay come to lie at the level of the L4-5 disc space asseen in the AP pro j e c t i o n .
P reoperative evaluation of the imaging studies willalso identify the position of the iliac crest relative tothe disc space. A high crest as seen on CT or MRI willf o rce a more cephalad entry point for successful can-nulation of the disc space. Occasionally, the heightof the crest will obstruct the approach. The goal ofthe lateral projection is to maintain the plane of theneedle parallel with one of the endplates in the discspace. This will allow the safe docking and entry ofthe instruments into the disc space. This emphasisdistinguishes the angle normally employed during abiopsy when simple triangulation of the lateral edgeof the disc space is appropriate.
Following successful needle placement, the needlestylet is removed and a small metal wire is placed inthe center barrel of the needle into the disc space,
c o n f i rmed by biplanar fluoroscopy. At this point, a#15 scalpel blade is used to incise the skin and sub-cutaneous fascia. The cannulated obturator is intro-duced over the stylet through the muscle layers untilwithin 1-2 cm of the annulus. The stylet is re m o v e dwhile approaching the annulus to avoid inadver-tently pinning or trapping the nerve root in the trian-gular working zone. The biplanar C- a rm is utilized todemonstrate placement of the cannulated obturatorat the lateral aspect of the bipedicular line and at theposterior margin of the disc space.
The universal access cannula is now intro d u c e dover the end of the obturated cannula. At this point,the edge of the annulus can often be assessed by tap-ping against the obturated cannula and feeling asense of steady pre s s u re, which then springs backagainst the thumb. The operation then proceeds byattaching the suction cap to the access cannula. Thez e ro - d e g ree forward-looking endoscope can be intro-duced through the suction cap. Irrigation is pro v i d e dvia a 1- or 3-L bag of saline positioned at the edge ofthe operative field. Control of flow is accomplished inthe field with the usual stopcocks. The scope allowsfor inspection of the annulus. The pattern of annularfibers and fat can be visualized to distinguish theannulus from the periosteum of the bone above andbelow (Figure 5). The biplanar C- a rm can be utilizedto demonstrate the level of visualization. The annuluscan then be cleaned utilizing a cottonoid patty intro-duced into the universal access cannula and moveda round the end of the cannula with either the back ofthe obturator twirled between the fingertips or asmall grasping forceps to place the patty against theannulus and wipe off some of the fat. At this point,the cottonoid patty can be used to introduce the fen-tanyl at the level of the annulus. We soak the 1-cmcottonoid patty in 50 µg fentanyl and apply it dire c t l yto the annulus, leaving it in place for 1 minute. Afterinspection of the annulus, it is helpful to use a spinalneedle to check each of the four quadrants in the uni-versal access cannula, with the 12 o’clock positionposteriorly or dorsally on the patient, the 3 o’clockcaudally, the 9 o’clock rostrally, and the 6 o’clockventrally as viewed from the end of the access can-nula. This confirms the position of the cannula overthe disc space. Prior to the application of the localanesthetic, We find it helpful to move the scope tovisualize the exiting root, thereby avoiding inadver-tent injury. The annulus can be infiltrated duringthese maneuvers as well with 25 µg fentanyl or 1-2ml 1% lidocaine without epinephrine. Straight tre-phines 3 and 5 mm in diameter are intro d u c e dt h rough the universal access cannula and twisteduntil they penetrate the annulus. Once the 5-mmt rephine has been introduced, the access cannulacan be gently advanced 0.5 cm to allow docking orf i rmly seating it in the annular fibers. This allows for
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8212

CASEY ET AL : ARTHROSCOPIC MICROLUMBAR DISCECTOMY 213
F i g u re 3. Drawing of the triangular working zone, viewed axially (upper) and sagittally ( l o w e r ).
F i g u re 4. Radiographs in anteroposterior ( l e f t ) and lateral ( r i g h t ) p rojections showing the needle position.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8214
stability at the annular fibers as well as at the opera-tor’s hand at the skin level. Alternatively, a smalllocking cap can be placed over the cannula. We findhand stabilization to be superior, especially for theinitial cases. A zero - d e g ree endoscope can be intro-duced for visualization of the intradiscal material( F i g u re 6).
When introducing the scope, it is useful to brieflyirrigate to clear material and occasional blood pro d-ucts in the access cannula; then reduce or turn offthe suction to allow a column of water for visualiza-tion and magnification. Via the arthroscope photo-graphic towers, photos can be taken through theendoscope and the steps of the operation docu-mented as well as providing a teaching file.
Once the presence of disc material has been con-f i rmed through a zero - d e g ree endoscope, it can beremoved utilizing the various forceps in the instru-ment set. Commonly, one starts with the straightf o rceps to evacuate material directly in the path ofthe approach. The deflecting forceps are used tomove more posteriorly in the disc space. Enough discmaterial is removed to enable room to introduce thes h a v e r. The shaver has a forward and reverse footpedal and is provided with constant irrigation via auniversal access cannula. Suction is attached to theshaver head itself. A suction trap is used to collectdisc material as it is removed. Caution should betaken to engage the drive motor for the shaver onlywhen it is fully engaged in the disc space. Tr a v e r s i n gthe edge of the cannula with the shaver engaged cancause neural elements to be drawn toward thes h a v e r. The shaver is utilized in a 270-degree arcwhich excludes the posterior 90 degrees runningroughly between 10 o’clock and 2 o’clock positions inthe clock face previously described (i.e., avoiding themost dorsal portion of the disc space at the level ofthe root). Zero- and 30-degree scopes can be re i n t ro-duced as needed during the shaving process toinspect the posterior-most elements.
When a biportal exposure is utilized, similar stepsa re followed to this point with the introduction of theneedle, stylet, obturated cannula, access cannula,scope, trephines, and disc space evacuation. Duringthis phase, it is possible to introduce a zero- or 30-d e g ree endoscope through one portal and the shavert h rough another portal and observe the function andmotion of the shaver and other grasping instruments( F i g u re 7). Alternatively, through a unilateral ap-p roach, a working scope with a central channel canbe introduced to allow simultaneous visualization ofthe removal of disc material. Another altern a t i v etechnique utilizes the oval cannula with an extern a ldiameter of 9 mm, which allows for simultaneous aswell as metachronous visualization. Disc re m o v a lcontinues posteriorly with the angle-edged instru-ments until elements of the posterior longitudinal
ligament are identified. These fibers are oriented inparallel, as opposed to the amorphous nuclear mate-rial. On many occasions, disc material that has pen-etrated the posterior longitudinal ligament and/orannular fibers can be retrieved, allowing the dura tobe inspected (Figure 8). Once disc removal is judgedto be adequate, the universal access cannula can bedisengaged and moved somewhat more posteriorlyalong the edge of the annulus, allowing for visualiza-tion of the lateral end of the foraminal contents. Thismaneuver enables inspection of the posterior marg i nof the triangular working zone and, on occasion,removal of small bony elements from the vertebralbody that may impinge on the lateral aspect of theforamen. During routine disc removal, this alsoallows for inspection of and removal of fragmentsthat are in a paraforaminal location. Fragments thata re totally extraforaminal, the so-called lateral disc,a re particularly advantageous to remove as the ex-tracanalicular approach of the scope brings the sur-geon down directly on the offending pathology.
After completing the operation, inspection of theannular surface allows for confirmation of the extentof removal of the protruding disc material and sub-sequent decompression of the nerve root visualizedimmediately rostral to the disc space. Bleeding occa-sionally occurs in the venous elements lateral to theannulus and can be controlled with gentle irrigation,the application of Surgicel through the scope appa-ratus, or the utilization of a monopolar coagulationw i re. The monopolar coagulation wire can be appliedwith the working channel scope and perf o rm e dunder direct vision (Ellman Wi re, Surg i t ron Corp.).We have found that the initial inspection of the discspace and the subsequent inspection at the end arebest accomplished with the zero - d e g ree scope whenmoving along the annulus exterior to the disc space.H o w e v e r, within the disc space, the 30-degree and7 0 - d e g ree endoscopes allow for visualization espe-cially along the posterior margin of the disc space atthe level of the expected pathology.
The extent of fragment removal and subsequentdisc removal is obviously determined by the operat-ing surgeon. We have found a useful classificationregimen that identifies disc material in the axial andsagittal planes as visualized on MRI. In the axialplane, disc material can occur in a medial, parame-dial, foraminal, or extraforaminal location movingf rom medial to lateral in any given disc space. In thesagittal view, the material can be interannular, sub-ligamentous, or extraligamentous and, in the lattercategory, the extraligamentous material is at thelevel of the disc space or either above or below thedisc space. Disc fragments that have migrated be-yond the confines of the posterior ligament and/ormigrated within the epidural space are going to pre-sent the greatest challenge in the early phases of

CASEY ET AL : ARTHROSCOPIC MICROLUMBAR DISCECTOMY 215
F i g u re 5. The annulus as seen through an endoscope.
F i g u re 7. Endoscopic view of grasping forc e p s .
F i g u re 6. Disc material viewed through an endoscope.
F i g u re 8. The posterior longitudinal ligament andthe dura are visible at left.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8216
acquiring the skill of arthroscopic micro d i s c e c t o m y .Removal of these disc fragments should not be at-tempted until a surgeon’s learning curve justifiesthat approach. The instruments have limitations asto the degree of posterior reach that they enjoy. Inaddition, exploration through the annulus and pos-terior ligaments into that epidural space incre a s e sthe possibility of inadvertent dural injury and subse-quent cere b rospinal fluid egress. Irrigation is contin-ued throughout the pro c e d u re, often using 3 L ofn o rmal saline. We have not seen any systemicchanges or local nerve root problems using this irri-gation regimen. On occasion, when there is evidenceof mild venous oozing near the root at the end of thep ro c e d u re, a small Hemovac drain can be placedd i rectly through the universal access cannula andremoved in 6-8 hours. In most patients, the accesscannula is removed, a single nonabsorbable sutureis placed at the skin line, and a single SteriStrip ban-dage is placed on the skin; the patient is then takento the recovery ro o m .
POSTOPERATIVE FOLLOW-UPPostoperatively, clinical signs and symptoms dictatethe degree of success. Occasionally, however, pa-tients present with possible residual symptomatology
or symptomatology that can be attributed to otherstructural abnormalities. We evaluated the useful-ness of immediate postoperative imaging in thisseries of patients. We found that MRI and CT exami-nations are both quite sensitive to the removal ofo ffending disc material in the canal space. When thep reoperative studies are compared to the studies ob-tained in the first 12-24 hours after surgery, re s i d u a lair in the previous area of disc protrusion, re s u m p-tion of a more normal canal configuration along theposterior margin of the vertebral body, and removal ofthe laterally placed disc herniation can be clearlyvisualized. We have looked at the percent of canalclearance in these patients and demonstrated a highd e g ree of correlation with successful canal clearanceand subsequent clinical outcome.
In the current series, a successful outcome hasbeen seen in approximately 87% of patients. As withmany pro c e d u res in this region, other factors, in-cluding the presence of workers’ compensation, liti-gation, and re c u r rent disc disease have been associ-ated with reduced incidence of successful outcomes.Although the pro c e d u re has many similarities toopen disc surgery, advantages include a smaller inci-sion, no canalicular dissection, and minimal discspace collapse as indicated by long-term follow-up.

INTRODUCTIONThe use of thoracotomy to treat spinal disease origi-nated with the treatment of spinal tuberculosis orPott’s disease. The abysmal results following lam-inectomy for herniated thoracic disks have led sur-geons to seek novel approaches for this problem, andin 1969, Perot and Munro, and later Ransohoff andcolleagues described the transthoracic removal ofh e rniated discs. This is now a standard and veryuseful pro c e d u re for treating thoracic intervertebraldisc disease, particularly lesions that are large ormidline in location.
Symptomatic thoracic disc herniations are un-usual. It is estimated that 0.25%-0.75 % of clinicallya p p a rent discs will occur in this region and most fre-quently present between T8 and T11. The typicalp resentation involves radicular pain, which caneither be acute or chronic.
Given the risks of this type of surgery, nonsurg i c a loptions such as use of anti-inflammatory drugs ornerve blocks should be considered in patients withpain alone and no neurological deficit. Involvementof the cord can produce paraparesis or sensory dis-turbances that are generally subacute or chronic inn a t u re, although sudden paraplegia can be seen.Myelopathy is an indication for surgery.
EXCISION OF HERNIATED THORACIC DISC VIA THE
TRANSTHORACIC APPROACHMARY LOUISE HLAVIN, M.D.RUSSELL W. HARDY, M.D.
217
PREOPERATIVE IMAGING AND PLANNINGP recise preoperative imaging is key in the surg i c a lplanning for herniated thoracic disc. Magnetic re s o-nance imaging (MRI) (preferably) or computedtomography myelography must clearly define thelevel of the offending disc. Thoracic spine x-rays areuseful to provide identifying landmarks for pro p e rintraoperative localization.
Although a seemingly formidable surgery, withc a reful patient selection morbidity and mortality ratesusing transthoracic discectomy are not unre a s o n a b l yhigh. We have perf o rmed the pro c e d u re in patientsup to 70 years old with underlying coronary disease.H o w e v e r, certain patients, including the elderly, thosewith chronic obstructive pulmonary disease, and per-sons who smoke do re p resent higher risk gro u p s .Generally, however, surgery can be planned on anelective basis to allow thorough evaluation of the pre-operative pulmonary and cardiac status. However,u rgent or emergent surgery is mandatory when thereis rapid loss of lower extremity function. Pulmonaryfunction should be assessed with an arterial bloodgas and spirometry. A satisfactory arterial blood gasvalue includes a pO2 >90 mm Hg, pC O2 <42 mm Hgand O2 saturation >92%. Value ranges of pO2 6 0 - 8 0mm Hg, pCO2 42-45 mm Hg, or O2 saturation 90%-92% would be considered borderline acceptable. Va l-ues out of these ranges place the patient at a muchhigher surgical risk. On spirometry, the followingresults are associated with significantly higher pul-© 1999 The American Association of Neurological Surg e o n s

monary complications: forced vital capacity (FVC)<1.5 liters, FEV1 ( f o rced expiratory volume at 1 sec-ond) less than 1.0 liter, FEV1/FVC <35% or forc e dexpiratory flow of 25%-75% (FEF25%-75%) <1 liter/second. Premorbid cardiac disease, including a his-tory of angina, congestive heart failure, or even dia-betes, carries a much greater risk for perioperativec a rdiovascular complications. Cardiac evaluationshould be directed by the patient’s internist or card i-ologist and may include a treadmill test in asympto-matic individuals between ages 45 and 60 years or a thallium exercise scan in patients aged over 60 or with a history of myocardial infarction, angina, orheart failure. (An intravenous dipyridamole-thalliumscan may be obtained in a patient unable to exerc i s e . )All patients should refrain from smoking for at least 2weeks before surgery and those with underlying lungdisease should have their pulmonary status opti-mized with bronchodilators or treatment of anyc h ronic bronchitis or bronchial edema.
OPERATIVE TECHNIQUEUsing the posterolateral thoracotomy appro a c hdescribed here, the fourth to the 10th thoracic verte-
brae are easily accessible, with excellent visualiza-tion of the anterior and lateral portions of the discspace as well as the spinal canal. To reach the ex-t reme levels of the thoracic spine, specialized tech-niques must be utilized. The uppermost thoracic ver-tebrae can be approached via either a posteriortransthoracic technique elevating and retracting thescapulae or by an anterior route, possibly requiring amedian sternotomy. The thoracolumbar junction iso b s c u red by the diaphragm; there f o re, techniques toexpose the T11, T12, and L1 vertebrae must includemanaging the diaphragm.
S u rgical Appro a c hSelecting the side of the surgical approach for a tho-racotomy is largely a matter of pre f e rence. Some sur-geons prefer using a left-sided thoracotomy to pro v i d eaccess because of greater ease in dealing with theaorta than the venous structures on the right,although at the superior aspect, the arch and gre a tvessels may be of concern. Other surgeons prefer touse a right-sided approach because of concern ofinjuring the artery of Adamkiewicz, which usually en-ters on the left side in the region of the thoracolum-
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8218
F i g u re 1. T1-weighted non-contrasted MRI demonstrating a larg eright-sided, laterally herniated disc at the T10-11 level which re s u l t e din sudden paraplegia. A right-sided thoracotomy was used to re m o v e dthe fragment.

HLAVIN AND HARDY : EXCISION OF HERNIATED THORACIC DISC VIA THE TRANSTHORACIC APPROACH 219
bar junction. On the other hand, when working at thelower portions of the thoracic spine, the liver is mored i fficult to retract, making a left-sided approach moredesirable. Should instrumentation be re q u i red, injuryto the aorta is of concern, and again a right-sided ap-p roach is pre f e r red by some. Clearly, a lateralizingdisc, as shown in Figure 1 (or other pathology), candictate the route of choice. Other considerations in-clude coexistent lung pathology, which might dictateopening a particular side of the chest. In most cases,h o w e v e r, approach from either side can be used.
A n e s t h e s i aS u rgery is carried out with a general anesthetic tech-nique utilizing at least two larg e - b o re intravenousaccess (16 gauge) catheters and arterial blood gasmonitoring. Some patients may re q u i re more inva-sive central venous pre s s u re or Swan-Ganz card i a cmonitoring.
The use of a double lumen-cuffed endotrachealtube (e.g., Carlens tube) permits deflating the ex-posed lung out of the way should additional room forretraction be necessary. Other methods can be usedto separate lung ventilation if necessary, such as a
b ronchial blocker. A urinary catheter is placed.Spinal cord monitoring with somatosensory evokedpotentials may be helpful, although the inform a t i o np rovided is clearly limited and injury to the anteriorspinal cord can occur without significant changes inthe signal. As with other pro c e d u res, perioperativeantibiotics are given. Perioperative steroids may beused in cases with significant cord compre s s i o n .
Patient PostioningAs shown in Figure 2, the patient is placed in a lat-eral position for surgery, rotated slightly forward sothat the chest contents will tend to fall away from thespine with gravity. A beanbag device or sand bagspadded in towels can be used to maintain this posi-tion, as long as the support is radiolucent to allowintraoperative x-ray localization. The chest should bepositioned over the break in the operating table sothat it may be flexed during surgery to open theinterspace and thus improve working room. At com-pletion, the break can be re t u rned to neutral to facil-itate closure. The axilla is supported and pro t e c t e dwith a roll while the legs are cushioned with pillows.The lower leg is bent while the upper leg is kept
F i g u re 2. Patient positioning and incision. The patient is secured in a lateral position with thechest centered over the break in the table to facilitate opening the interspace during surgery. Abeanbag device or padded sand bags (not shown) can support the patient. Care must be taken top rotect the axillary and peroneal areas as well. The course of a typical incision is shown ( d o t t e dl i n e s ). A , s u rgeon’s view from above. B , side view, surgeon facing the patient.
A
B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8220
extended. The upper arm is supported with pillowsand bent at about a 90-degree angle to rotate it outof the field. The patient is secured well to the operat-ing table with 3-inch tape to enable safe ro t a t i o nduring the pro c e d u re. The patient may be tiltedslightly toward the surgeon to allow for a better view.
Operative Pro c e d u reFor a standard thoracotomy, the incision is typicallyc e n t e red over the rib, which potentially may be re-moved. The nipple is a marker for the fourth inter-space. In young patients, intercostal ligaments maybe reasonably supple such that use of a rib spre a d e rwill provide adequate retraction and exposure. Alter-natively, a portion of the rib numbered by the verte-bral body superior to the offending intervertebraldisc can be removed. In the thoracic spine, it isimportant to remember that any particular rib artic-ulates with the posterior/superior margin of the ver-tebral body with which it shares a number. Forexample, as shown in Figure 3, the head of the T9 ribarticulates with the body of T8 and T9 at the postero-lateral aspect of the offending disc space. One accu-rate way to count ribs is to place one’s hand insidethe pleural cavity and count down from the top andthen up from the bottom. The counts should agre eb e f o re a resection is perf o rmed. Alternatively, a plainspine x-ray should be obtained. To obtain optimale x p o s u re and working room, it is best to remove therib numbered by the vertebrae superior to the discspace. (Thus, as shown in Figure 3, the T8 rib isremoved laterally to gain access to the T8-9 space.)This compensates for the angulation of the ribs infe-riorly across the anterior aspect of the vertebral bodyand facilitates working inferiorly rather than superi-orly. As depicted in Figure 2, the incision should fol-low the rib and curve slightly cephalad posteriorly,w h e re it extends to approximately halfway betweenthe spinous process and the medial portion of thescapula. Anteriorly, the incision curves toward thes t e rnum. The skin incision is made initially with ascalpel. There a f t e r, Bovie cautery is used for hemo-stasis and division of the musculofascial layers,which includes the trapezius and rhomboid musclesmedially and the latissimus dorsi and serratus ante-rior muscles deeper and extending anteriorly. Larg evessels should be ligated and divided. The perios-teum of the rib to be resected is incised with theBovie cautery, then stripped from the superf i c i a ls u rface using a Cobb or other periosteal elevator.After clearing off the undersurface of the rib with ac u rette, a “pigtail” rib stripper can be used to dissecto ff the remaining periosteum and elevate the rib outof its bed (Figure 4A). Care should be taken to iden-tify and save the neurovascular bundles that travelalong the inferior border of each rib. (Some surg e o n sp refer ligating the neurovascular bundle with 2-0 or
3-0 silk ties because it is believed to eliminates t retch injury to the nerve that has been implicatedin postoperative pain syndrome.) At this point, therib to be resected may be cut out with a rib cutter,dividing as posteriorly as possible, close to the cos-tovertebral angle. Should an attempt be made to pre-serve the rib, the intercostal muscles may be splitadditionally to enable further separation of the inter-costal space. The pleura is grasped with smooth for-ceps and opened using scissors (Figure 4B). Afterp rotecting the ribs with cotton tape, a self-re t a i n i n g(Finochietto) retractor is placed in the pleural cavityand opened. The lung may be covered with a moistlap pad and retracted out of the way. A wide ribbonretractor or sweetheart retractor may be used to ac-complish this. Judicious placement of the ribbonunder the Finochietto retractor can eliminate theneed for manual re t r a c t i o n .
At this point, the vertebral bodies and otheranatomic structures should be visible through theparietal pleura (Figure 5). The intervertebral discscan be both visualized and palpated as the pro m i-nent bulging areas of the vertebral column while theintervening concavities re p resent the vertebral bod-ies. The bottom of the concavity approximates themid portion of the body. Radiographic confirm a t i o nof the proper disc space before proceeding is crucialat this point. An open-sided rectangular incision isthen made in the parietal pleura, extending from themid portion of the vertebral bodies above and belowthe affected disc space and extending laterally ateither end (Figure 6). The pleura is then dissectedc a refully from the vertebral body and reflected later-ally, thereby exposing the intervertebral vessels aswell as the sympathetic chain. The segmental vesselsshould be identified and ligated using 3-0 silk ties ino rder to provide adequate bony exposure. Runningwith the segmental artery and vein are the inter-costal nerves. The intercostal nerve can be traced tothe neural foramina of interest, which then enablesidentification of the pedicle, an important landmark.It is important to re m e m b e r, however, that the headof the rib overlies the pedicle and occasionally needsto be removed to obtain adequate exposure of thethecal sac (Figure 7). In some instances, althoughnot routinely, it may be necessary to drill off a por-tion of the pedicle as well.
At this point, the operative microscope is bro u g h tinto place. The annulus of the offending disc is in-cised anteriorly and the disc space is grossly evacu-ated using a combination of pituitary ronguers andc u rettes. This initial debulking is crucial prior to anyattempts to remove the extruded fragment compre s s-ing the neural elements, as this provides exposureand working room. It is important to remember towork away from the spinal cord. Flexion of the oper-ating table at this juncture may be used as a maneu-

HLAVIN AND HARDY : EXCISION OF HERNIATED THORACIC DISC VIA THE TRANSTHORACIC APPROACH 221
F i g u re 4. Rib resection and pleural opening. A , the rib to be resected, still lying in its bed, has been cleared off withperiosteal elevators and the underside dissected free to allow insertion of a pigtail rib stripper. B , after bony resection, thenow-exposed rib bed and pleura are grasped with forceps and divided.
F i g u re 3. Anatomic diagram of the rib cage, posteriorview. This picture depicts the articulation of the ribs withtheir respective bodies and interspaces and demonstratesthe bony resection that would be used for a T8-9 hern i-ated disc through a left-sided approach. The head of theT9 rib articulates with the bodies of T8 and T9 at the pos-t e rolateral aspect of the offending disc space. The headhas been removed to gain access to the T8-9 disc space.In addition, the T8 rib has been removed laterally to pro-vide working ro o m .
BA
112
23
3
44
55
66
77
88
9
10
11
12
9
10
11
12

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8222
Figure 6. Pleural incision. The dashedline indicates the window openingthrough the pleura (left-sided approach).
F i g u re 5. Intrathoracic anatomy. A , right-sided view. B , left-sided view.
A
B
lung
diaphragm
trachea
esophagus
azygous vein
greatersplanchnicnerve
sympathetictrunk
lung
esophagus
aorta
diaphragm
CAUDALCEPHALAD
CAUDALCEPHALAD
intercostal arteries, veins, nerves

HLAVIN AND HARDY : EXCISION OF HERNIATED THORACIC DISC VIA THE TRANSTHORACIC APPROACH 223
F i g u re 7. Removal of the rib head. The parietal pleura hasbeen reflected, segmental vessels ligated, and the head ofthe rib drilled off. The dashed line indicates where the ribwas re m o v e d .
A B
C
F i g u re 8. Bony resection and disc re m o v a l . A, the annulus has been incisedand the disc space preliminarily emptied using long pituitary ronguers andc u rettes. Additional bone is being drilled off the superior and inferior end-plates to widen working room. B, l a rge osteophytes or calcified ligament canre q u i re more extensive bony removal of the bodies and pedicle to visualizethe thecal sac and ensure adequate decompression. C, anatomic diagramdemonstrating extent of final bony re m o v a l .

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8224
ver to open the disc space. Alternatively, a disc spaces p reader may be placed into the interspace. Drillingo ff a small portion of both the superior and inferiorendplates as well as the vertebral body enlarges thee x p o s u re and provides access to the herniated frag-ments (Figure 8A). Additional exposure of the duramay be obtained by resecting the head of the ribabutting the intervertebral disc space and re m o v i n gthe superior portion of the pedicle (Figure 8B). Anycalcified posterior longitudinal ligament or fibro t i cannulus should be resected either with Kerrisonronguers or by forcing the material into the inter-space and removing it. At completion, palpation ofthe dura with a No. 4 Penfield should be perf o rm e dto confirm adequate decompression. A typical verte-bral bony resection is shown in transverse section inF i g u re 8C.
WOUND CLOSURER e t u rn of the operating table to a flat position facili-tates wound closure. The parietal pleura is re a p p ro x i-mated using interrupted absorbable sutures of eitherc h romic catgut or 3-0 Vicryl sutures. An apical de-pendent chest tube is externalized through a stabwound and the chest is then closed serially in layers.A rib approximator is used to initially place 0-0N u rolon stitches around the ribs. A running absorb-able stitch is used for the individual muscular layers.The skin can be stapled or closed with an absorbablesubcuticular stitch such as 4-0 Vicryl sutures. The
chest tube is attached to an underwater suctiondrainage. It is subsequently removed when drainagehas subsided and no air leaks are present. An imme-diate postoperative chest film as well as daily chest x-rays should be obtained to confirm resolution of anypneumothorax.
COMPLICATIONS AND AVOIDANCERisks of surgery include death, paraplegia, hemor-rhage, infection, cere b rospinal fluid (CSF)-pleural fis-tula, post-thoracotomy pain, or kyphotic deform i t y .C a reful patient selection and preoperative card i o p u l-monary assessment with judicious perioperativemonitoring will help minimize morbidity and mortal-ity from this pro c e d u re. Clearly, manipulation aro u n dthe spinal cord poses a threat for neurological injury.An ample bony decompression to provide workingroom without retracting the cord as well as alwaysworking away from the cord will help decrease risk ofdamage. An extensive bony removal must be weighedagainst the risk for postoperative kyphotic deform i t yf rom collapse. Should a significant bony defect bep resent, placement of a bone graft can reduce the riskof long-term angulation. Care must be taken to watchfor a CSF leak at the end of the pro c e d u re, withinspection under a Valsalva maneuver. Should therebe suspicion of a rent, this should be sealed with amuscle or fascia graft and fibrin glue and a lumbardrain placed for several days postoperatively to avoida CSF fistula.

INTRODUCTIONIt is not possible to predict the natural history ofu n t reated adult spinal deformity. The deformity mayp resent in many forms, either idiopathic, degenera-tive, or the result of a post-surgical imbalance withinduced deformity either above or below the indexfusion area. In the vast majority of adults with severespinal deformity, degenerative disc disease is thecause. The onset of adult degenerative scoliosis isr a rely seen in patients younger than age 40. Oncebelieved to be stable in comparison to adolescentidiopathic disease, long-term studies have shownthat these deformities pro g ress anywhere from atleast 1° to 3° per year. Followed over 5 to 10 years,these deformities can result in a crippling disability.
As with all spinal disease, the first course of tre a t-ment is conservative. For patients with minimalsymptoms, observation may be sufficient. In those inwhom the symptoms are back pain alone, a course ofn o n s t e roidal anti-inflammatory medications, brac-ing, and aerobic conditioning programs may be ofuse. Unlike adolescent idiopathic scoliosis, bracingp robably has less of a role in the elderly. In patientswho present with symptoms of spinal claudication,an aerobic conditioning program may be of benefit.This, along with epidural steroid injections and nerveroot blocks, may temporize through a period ofsymptom exacerbation or, in some fortunate pa-tients, give sufficient relief to obviate the need to con-
SURGICAL MANAGEMENT OFA D VANCED DEGENERATIVE DISEASE
OF THE LUMBAR SPINE WITH M U LTIPLANAR DEFORMITY
MICHAEL F. O’BRIEN, M.D.GARY L. LOWERY, M.D., PH.D.
A. EUGENE PENNISI, M.A.
225
sider surgery. When all conservative means havefailed and the patient’s symptoms suggest that sur-gery is the most appropriate option, patient selectionand a clear understanding of the structural pathol-ogy are the two most important factors in the suc-cessful surgical treatment of this disease. The surg i-cal treatments are really the sequential applicationof standard anterior and posterior spinal techniques.These include anterior lumbar intradiscal fusion,posterior lumbar intradiscal fusion, pedicle scre wplacement, anterior instrumentation techniques,corpectomies, and osteotomies. Other techniques in-clude derotation for correcting coronal deform i t i e sand restoring lord o s i s .
The appropriate application of these techniquesin a well thought-out manner is necessary for thesuccessful surgical treatment of these patients. Anunderstanding of the peculiarities of each uniquecurve, as well as the underlying pathology, is essen-tial. Without a clear understanding of the uniquesegmental abnormalities in each deformity, it isimpossible to correctly determine the surgical tech-nique most appropriate (whether anterior, posterior,or combined) and the area over which the surgeryneeds to be performed to stabilize the spine in thecorrected coronal and sagittal planes. Failure toachieve a balanced correction, to address each ab-normality at each level, and to anticipate changesin the remaining discs above and below will lead tolong-term failure. Ultimately, success will resultfrom the appropriate realignment of the structuralelements in both the coronal and sagittal projec-tions and through decompression of stenotic levelsto eliminate the effects of nerve root traction andspinal stenosis. © 1999 The American Association of Neurological Surg e o n s

PREOPERATIVE PREPARATIONSThe most important portions of the radiologicalworkup are the plain x-rays. These should includelong-standing anteroposterior and lateral scoliosisfilms. In addition, long-cassette right and left lateralside-bending films in the supine position and push-p rone and extension films over a bolster are neces-sary to assess the structural components of thecurve, including curve segment flexibility and theability of the spine in the potentially uninstrumentedsegments to fall within the stable zone after operativeconnection. Push-prone films are done with thepatient in the prone position, with the pelvis stabi-lized by an assistant and the surgeon pressing onthe deformity to attempt to create a radiographic pic-t u re of the maximum possible correction. Not onlydoes this help assess the flexibility of the main curve,it also approximates the response of the compen-satory curves to this correction. Bolster films areparticularly useful when considering the flexibility ofa kyphotic segment and its ability to be corre c t e d .The patient is placed in the supine position with abolster over the apex of the kyphosis, allowing thetorso to fall backward under the effect of gravity.This will usually give a good indication as to the abil-ity of the kyphosis to be corrected with instrumenta-tion alone.
When a patient presents with neurological deficitssecondary to spinal stenosis and nerve root com-p ression, the level and the extent of the compre s s i v epathology need to be delineated. In mild curves,magnetic resonance imaging (MRI) is useful to ascer-tain the intracanal pathology. In addition, MRI givesvaluable supplemental information about the lowerlumbar discs and the possibility of avoiding fusion tothe sacrum. It is, however, unusual in a populationof aging patients to have MRI “normal discs.”
Computed tomography (CT) myelography may bea more useful study for investigation of intracanalpathology in the severely stenotic and/or severe l yd e f o rmed spine. Because the myelographic dyeclearly and accurately outlines the neural space, ap recise and detailed re p resentation of the extent ofneural element compression can be obtained. In pa-tients who have undergone previous surgery andimplantation of stainless steel instrumentation, thisis often a useful study.
Discography is useful for delineating the optimaloperative levels. It is important that every attemptbe made to spare lower lumbar segments in partic-ular. This helps maintain some degree of flexibilityand provides a stress relief point for the spinal in-strumentation. CT discography is an excellent wayto investigate both the morphology and the clinicalcondition of the disc.
A chief concern in this population of patients isgeneral nutrition. In patients with reduced serum
p rotein, some form of preoperative enteral alimenta-tion or hyperalimentation may be necessary to opti-mize the patient for the surgical challenge. Pre o p e r a-tive laboratory investigations should include totalalbumin, total lymphocyte count, transferrin, andp re-albumin. If there is a possibility of anteriortransthoracic surgery, a full pulmonary and card i a cworkup should be perf o rm e d .
Cosmetic issues are also important. Patients withsignificant upper lumbar and lower thoracic abnor-malities may have unsightly rotational pro m i n e n c e sthat are an integral part of the patient’s dissatisfac-tion. If the patient has a significant and unacceptablelumbar prominence, consideration should to be givento an anterior multilevel discectomy and intradiscalfusion to help decrease this rotational deformity. In asimilar manner, if the thoracic prominence is a cos-metic issue, consideration may be given to a thora-coplasty in combination with the deformity surg e r y .Pulmonary function is decreased for several monthsfollowing thoracoplasty, a factor that should be con-s i d e red preoperatively in patients with pulmonarydysfunction.
ANESTHETIC TECHNIQUEBecause of lengthy surgical time, the possibility ofpoor vascular access, and large fluid shifts, these pa-tients should be monitored with intra-arterial linesand central venous access lines. Although hypoten-sive anesthesia is a possibility, serious complicationscan be associated with this. In the elderly population,s e v e re hypotensive anesthesia can result in myocar-dial infarction, stroke, and multisystem failure in-cluding the renal and hepatic systems. In addition,hypotensive anesthesia, particularly during large cor-rective deformity surgeries, can result in blindness ifd i rect ocular pre s s u re is not applied. Norm o t e n s i v eanesthesia may be more appropriate in these exten-sive pro c e d u res. Blood loss can be offset by pre o p e r a-tively donated autologous blood and the use of a cells a v e r.
OPERATIVE POSITIONINGFor the most part, both an anterior and a posteriora p p roach will be needed for the correction of thesed e f o rmities. Because of the severe nature of thed e f o rmity and the poor fusion rates expected in thispopulation, structural grafting and fixation bothanteriorly and posteriorly are warranted to ensureadequate fusion. However, in some instances thed e f o rmity may be addressed exclusively anteriorly orposteriorly. Many adequate positioning techniqueshave been described. Specific positioning schemesmay depend to a large degree on anticipated intraop-erative repositioning (i.e., closing or opening osteot-omy sites) and maintenance of lumbar lord o s i s .Whichever technique is used, adequate decompre s-
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8226

O’BRIEN ET AL : DEGENERATIVE DISEASE OF THE LUMBAR SPINE WITH MULTIPLANAR DEFORMITY 227
sion of the abdominal contents must be achieved toreduce intraoperative bleeding.
SURGICAL GOALSThe primary dysfunction in patients with this pathol-ogy is the asymmetric collapse of the degeneratinglumbar intervertebral disc. The goal of surgery is tod e c o m p ress where appropriate, re s t o re spinal bal-ance, reconstruct the deficient disc(s), and stabilizethe spine until fusion occurs. The hallmark of thedisease is lateral listheses or “rotatory subluxations.”Early in the course of the disease, this is often identi-fied as a slight asymmetric collapse without obvious
rotation at the involved disc space. This asymmetriccollapse increases until there is near complete loss ofunilateral disc height in the coronal plane. This is fol-lowed by a lateral shift of the superior vertebral bodyon the inferior vertebral body and evidence of ro t a t i o nas identified by using Nash/Moe observations forpedicle position. At this point, the patient fre q u e n t l yp resents with radicular symptoms. These symptomstypically result from either standard foraminal orcentral stenosis due to collapse of the disc spaceanteriorly and overg rowth of the facet joints withredundant ligamentum flavum posteriorly (Figure 1).Characteristically, there is compression on the cauda
Figure 1. Foraminal stenosis due to hypertrophic facets.
©Neill BioMedical Art Co., 1999

equina secondary to the loss of overall central canaldiameter associated with rotatory subluxation (Fig-u re 2). Another unique mechanism for the onset ofradicular symptoms in this pathology is nerve ro o ttraction secondary to the rotatory translation of thepedicles, causing nerve root stretching as the ro o t sexit the neural foramen (Figure 3). The curves rangef rom subtle, tight radius deformities confined to theupper and middle lumbar spine to fairly large curvesinvolving the lower thoracic and upper lumbar spineas the primary curve and fractional or compensatorycurve in the lower lumbar spine which re t u rns thespine to the pelvis (Figure 4). In the vast majority ofcases, the apex of the degenerative scoliosis is at theL3-4 disc level, which typically corresponds to atleast one rotatory subluxation. It is not uncommon atthe level of the rotatory subluxation to also have asagittal plane spondylolisthesis in addition to a lossof lordosis (see Figure 3). While it is most common tohave only one such obvious level of instability, boththe rotatory subluxations and the spondylolisthesescan involve multiple levels.
Contraindications for surgical treatment in thesepatients often center more around the medical con-ditions of the elderly and presence of osteoporosisthan around specific difficulties with the procedure,although correcting large, stiff curves can be a for-midable undertaking.
OPERATIVE PROCEDURE
Posterior Appro a c hThe determination as to whether to proceed anteri-orly, posteriorly, or both needs to be assessed on acase-by-case basis. When the deformity is supple orunstable, consideration should first be given to in-strumentation. This usually implies a posterior ap-p roach with realignment and instrumentation first.The standard posterior approach for spinal cases isused (Figure 5). Realignment in such cases mayoften be achieved via a posterior osteotomy in whichthe lamina and facet are removed. In this technique,the inferior facets of the superior vertebra and thelamina and the superior facets of the inferior verte-bra are removed (Figure 6). The osteotomy is thenclosed and stabilized under compression instrumen-tation (Figure 7). Finally, posterolateral fusion, in-cluding the facets, is perf o rmed to heal the osteot-omy site.
Pedicle screws are an excellent means of segmen-tal fixation in the posterior lumbar spine (Figure 8).Their safe placement is certainly within the realm ofpossibilities for the accomplished spine surgeon, butthe risk of serious neurological injury should not beneglected. Special care must be taken not to injurethe dura and the neural elements secondary to im-pertinent penetration into the canal. For the most
part, concerns associated with the posterior ap-p roach have to do with improperly or poorly placedinstrumentation. Insufficient or suboptimal biome-chanical placement of instrumentation can result inf a i l u re. In the osteoporotic spine, even rigid con-structs may be inadequate due to the poor osseousp u rchase of the metallic implants.
Combined Anterior/Posterior Approach Posterior osteotomies, fusion, and instrumentationf requently re q u i re supplementary intradiscal graftingin order to fully address discal pathology and securea solid fusion. This may be perf o rmed via an anterioror posterior approach. Intradiscal fusion of L5-S1 isoften needed to re s t o re spinal balance and to re c o n-struct a deficient disc that is placed under incre a s e dshear and torsional loads (Figure 9). This may be per-f o rmed re t roperitoneally or via Pfannenstiel’s incision( F i g u re 10). Additionally, if the deformity is rigid, ananterior release of the remaining structures mostresponsible for resisting rotation may be re q u i red ino rder to achieve correction. Once released, the appro-priate posterior osteotomies, operative positioning,and efficient placement of biomechanically corre c tposterior instrumentation can be accomplished. In-strumentation used both anteriorly and posteriorly iscommon to less complicated surgeries and is used inmultiple combinations to achieve the desired corre c-tion in complicated deformities.
Anterior Appro a c hIn certain instances, anterior instrumentation maybe sufficient for reconstruction. Anterior instrumen-tation is particularly helpful in substantially de-c reasing coronal plane deformities and in stabilizingthe spine after corpectomy. The type of anterior ap-p roach used depends on the individual patient’sanatomy that needs to be accessed and the type ofinstrumentation to be used during surgery. Anteriorinstrumentation at multiple levels typically re q u i re sa lateral approach and may be best suited to a pa-tient positioned in the right or left lateral decubitusposition and an extensile flank incision (Figure 11).This allows the development of the re t ro p e r i t o n e a lspace and provides for a straight lateral approach tothe spine.
The major considerations during an anterior ap-p roach are predominantly anatomic and center onthe safe dissection of the vascular structures, espe-cially at L4 and below. At this level, adequate expo-s u re of the anterior spine re q u i res immobilization ofthe great vessels at the aortic bifurcation and safeidentification and ligation of the often prominent andn u m e rous re c u r rent lumbar veins. This safeguard sagainst uncontrolled intraoperative bleeding andavulsion of these vessels from the iliac vein. The seg-mental vessels are more easily located and contro l l e d ;
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8228

O’BRIEN ET AL : DEGENERATIVE DISEASE OF THE LUMBAR SPINE WITH MULTIPLANAR DEFORMITY 229
Figure 2. Loss of overall central canal diameter in rotational deformity.
Figure 3. Lateral view showing spondylolisthesis and loss of lor-dosis. Note the nerve root stretching around the pedicle at L3.
Figure 4. Anteroposterior view showing primaryand fractional curve.
©Neill BioMedical Art Co., 1999

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8230
they also need to be considered when perf o rming cor-pectomies and during placement of transvertebralbody screws with bicortical purchase. Failure to con-sider these vessels during these pro c e d u res canresult in significant bleeding that is difficult to con-t rol since the vessels in question are on the oppositeside of the vertebral body.
Other anatomic structures that need to be care-fully identified and considered include the hypogas-tric plexus, the ure t e r, the ilioinguinal and genito-femoral nerves, the lumbar plexus, and of course thespinal cord and cauda equina. Care must be takento mobilize all structures anterior to the periosteumover the sacral promontory (L5-S1 disc space) usingblunt dissection. Cautery should not be used on thisanterior soft tissue, and sharp dissection should belimited to intradiscal dissection.
The anterior and posterior reconstruction tech-niques used in these complicated pro c e d u res are notsignificantly diff e rent than the techniques used insimpler degenerative pro c e d u res. They merely re p re-sent the sequential application of various techniquesto address the numerous problems in these compli-cated deformities. It is obvious that multiple pro c e-d u res perf o rmed in the same patient increase therisk of infection and other complications. Significantp reoperative planning is necessary to be sure thateach technique is applied in a sound and planned
o rder so as to achieve the goals of surgery with mini-mum blood loss and minimum operative time.
MONITORINGAs with all types of deformity surgery, particularlywhen large changes are anticipated in the overallc o ronal and sagittal alignment, electro p h y s i o l o g i c a lmonitoring is necessary. It is optimal to have bothsomatosensory evoked potential and motor evokedpotential monitoring available. To ensure the gre a t-est safety for the neural elements, the use of moni-t o red pedicle probes and pedicle screw stimulationshould be considered during the placement of pedi-cle screws. For electrophysiological monitoring to betruly effective, there needs to be cooperation betweenthe electrophysiologist and the anesthesiologist. Inaddition, the electrophysiologist needs to be familiarwith sophisticated techniques that involve monitor-ing both nerve roots via EMG and monitoring ofmotor and sensory tracts. Also affecting the useful-ness of the electrophysiological monitoring is thewillingness of the surgeon to cooperate with the elec-t rophysiologist. There must be adequate time formonitoring during dissection techniques using elec-t rocautery and when probing pedicles and placingpedicle screws. In the event that electro p h y s i o l o g i c a lmonitoring is equivocal or suggests an intraoperativec o n c e rn, a wake-up test should be considered as the
Figure 5. Patient positioning for a standard posterior approach.
©Neill BioMedical Art Co., 1999

O’BRIEN ET AL : DEGENERATIVE DISEASE OF THE LUMBAR SPINE WITH MULTIPLANAR DEFORMITY 231
Figure 6. Posterior osteotomy.
F i g u re 7. Stabilization of the lumbar and lumbosacralspine using Texas Scottish Rite Hospital instrumentation.
Figure 8. Pedicle screws placed for fixation in the posterior lumbar spine.
©Neill BioMedical Art Co., 1999

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8232
Figure 9. Total discectomy in preparation for intradis-cal fusion in a combined anterior/posterior approach.
Figure 10. Pfannenstiel’s incision.
©Neill BioMedical Art Co., 1999

O’BRIEN ET AL : DEGENERATIVE DISEASE OF THE LUMBAR SPINE WITH MULTIPLANAR DEFORMITY 233
gold standard for intact neurological functioning,especially for the motor tracts.
SPECIALIZED INSTRUMENTATIONHigh-speed burrs, which provide both high torq u eand high speed, are extremely helpful when perf o rm-ing complicated osteotomies and decompre s s i o n sa round the neural elements. Although a high-speedburr near the dural sac may appear somewhat dan-g e rous, it is probably much less dangerous than dullosteotomes, Kerrisons, and rongeurs which have atendency to slip off hard bone and may not be able tobe applied to the osseous structures in a convenientm a n n e r. In spite of this, great care is necessary whileusing these tools near the neural elements. Thesechallenging cases are certainly not the forum topractice using this instrumentation.
INTRAOPERATIVE RADIOGRAPHYIntraoperative imaging is most important in casesinvolving severe deformities in which large changes inpatient positioning in either the frontal or the sagittalp rojection are anticipated. Intraoperative fluoro s c o p yalso helps to ascertain the coronal alignment of pedi-cle screws since the head of the image machine can
actually be manipulated in such a way as to show the screw in a “bulls eye” position in the pedicle. Nointraoperative imaging techniques, however, can sub-stitute for careful preoperative planning.
COMPLICATIONSAs described above, anatomic or instrumentationp roblems can be avoided by careful pre o p e r a t i v eplanning and meticulous technique. Frequently, com-plications in this group of patients concern the met-abolic consequences of surgery. Large transfusionvolumes may result in disseminated intravascularcoagulation or adult respiratory distress syndro m e .Overzealous manipulation of vascular structures mayresult in intimal injuries leading to either local thro m-bosis or the propagation of thrombi with re s u l t i n gs t roke, myocardial infarction, or pulmonary embol-ism. In addition, large-volume fluid shifts may re s u l tin multisystem failures. To prevent these complica-tions, careful preoperative planning is critical. Intra-operative decisions can be anticipated and altern a t i v esolutions developed, resulting in more safely per-f o rmed complex operations. The optimal surgical goalcannot be achieved in all cases. Other solutions and aworse-case scenario option must be detailed.
Figure 11. Extensile flank incision for an anterior approach.
©Neill BioMedical Art Co., 1999


INTRODUCTIONThe re t ropleural approach provides the shortestd i rect route to the ventral thoracic and thoracolum-bar spine and spinal canal, avoiding entry of thepleural cavity. One advantage of a ventral appro a c hto the spinal cord is the ability to visualize significantventral pathology that extends past the midline ofthe involved vertebral body. Dorsolateral appro a c h e ssuch as the costotransversectomy and the lateral ex-tracavitary provide exposure that barely extends tothe midline; further ventral visualization may re q u i reextensive muscle mobilization and bloody transfo-raminal dissection. These approaches also re q u i resacrifice of the intercostal nerve and risk possible oc-clusion of the radiculomedullary artery.
The re t ropleural approach offers several advan-tages over the alternative transthoracic ventral ap-p roach. Since a shorter segment of the chest cavitymust be traversed to reach the spine through theopening, significant retraction of the unpro t e c t e dlung is avoided. In the re t ropleural approach, the pa-rietal and visceral pleura shield the lung from thef o rces of retraction. Postoperative pulmonary compli-cations are minimized and placement of a chest tubeis usually not re q u i red. While some authors report ahigher incidence of pleural effusion in the re t ro-
THE RETROPLEURAL APPROACH TO THE THORACIC AND
THORACOLUMBAR SPINETHEODORE H. SCHWARTZ, M.D.
PAUL C. McCORMICK, M.D.
235
pleural approach, this has not been the experience ofthe senior author (P.C.M.). In the case of a cere b ro-spinal fluid (CSF) leak, the transthoracic appro a c hre q u i res placement of a spinal drain as well as achest tube on water seal. For the re t ropleural ap-p roach, no treatment is indicated. The re t ro p l e u r a la p p roach also allows a smaller incision and mini-mizes soft tissue dissection, which may lessen post-operative pain and shorten the patient’s hospitalstay. In one large series, post-thoracotomy pain syn-d rome lasting at least 6 months was reported in 9.2%of patients undergoing the transthoracic approach. As h o r t e r, more secure operative field reduces the riskof untoward intraoperative events and facilitatesachievement of the surgical objective.
The re t ropleural approach also uses a less obliqueangle, which aff o rds improved visualization of thespinal canal unobstructed by the rib head, aorta, orvena cava. During the transthoracic approach, thecurved dorsal cortical vertebral body margin maydisorient the surgeon, especially if inadequate bonydissection has been perf o rmed. Finally, bleedingf rom the extensive ventral epidural thoracic venousplexus is easier to control from a less oblique angle.The approach also provides both lateral canal expo-s u re through the resected pedicle bed and adjacentforamen as well as a direct line of vision that is ante-rior to the ventral canal floor. Thus, initial canalidentification and complete canal decompression ism o re easily and confidently achieved. Some authorsfind that pleural adhesions encountered in adultpatients make re t ropleural dissection difficult. In the© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8236
authors’ opinion, however, minor lacerations of thepleura are easily re p a i red. If the pleurae are signifi-cantly compromised, the approach can easily bemodified into a transthoracic appro a c h .
INDICATIONSThe re t ropleural approach is most appropriate forlocalized (two or fewer vertebral segments) pathologyof the ventral thoracic and thoracolumbar spinebetween T3 and L1. Traumatic fractures and post-traumatic kyphoses occur frequently in the thora-columbar spine and are often amenable to surg i c a lc o r rection via the re t ropleural approach. The trau-matic lesion most suitable to the re t ropleural ap-p roach is the burst fracture, in which there is failureof the anterior and middle columns due to compre s-sion loading (Figure 1). Neurologically intact patientswith minimal canal compromise and an intact dorsalcolumn can usually be managed conservatively withbracing, bed rest, and physiotherapy. Likewise, pa-
tients with complete loss of neurological functionbelow the level of injury for more than 48 hours willusually not improve following operative decompre s-sion but may re q u i re surgical stabilization for re h a-bilitation. Fractures with a greater than 40% loss ofbody height, greater than 50% canal compro m i s e ,major kyphotic deformity, or significant neuro l o g i c a ldeficits are generally considered operative lesions. A ventral approach is also useful in posttraumatickyphosis in the setting of increasing deformity, ky-phosis greater than 30 degrees, intractable pain, orpersistent or pro g ressive neurological deficits sincedorsal fusion alone is usually not sufficient. If thereis dorsal stability, neurological improvement and sig-nificant pain relief are achieved in a majority of thesepatients approached ventrally. Adequate re d u c t i o nand fusion, however, usually re q u i re ventral instru-mentation or prolonged postoperative recumbency. Ift h e re is a question of compromised posterior stabil-ity, then dorsal spinal fusion may be re q u i red in
F i g u re 1. A, computed tomography scan demonstrating L2 flexion/compression fracture with re t ropulsion of bonefragment into the spinal canal. B , a n t e roposterior radiograph following re t ropleural corpectomy and re c o n s t r u c t i o ndemonstrating lateral titanium plate and autologous rib/femoral head allograft bone graft. C , lateral radiograph follow-ing re t ropleural corpectomy and reconstruction. (Reproduced from McCormick PC: Retropleural approach to the tho-racic and thoracolumbar spine. N e u ro s u rgery 37:908-914, 1995, with perm i s s i o n )
A B C

SCHWARTZ AND McCORMICK : RETROPLEURAL APPROACH TO THE THORACIC AND THORACOLUMBAR SPINE 237
addition to ventral fusion, and a dorsolateral or sep-arate dorsal and ventral approaches may be morea p p ropriate.
Disc herniations in the thoracic region are alsoeasily decompressed via the re t ropleural appro a c h .The increased exposure is particularly useful for calcified discs, which cannot be adequately re m o v e dvia the transpedicular or costotransversectomy ap-p roach.
Significant ventral compression from primary andmetastatic tumors to the vertebral body or infectionsof the spine can also be appropriately managed viathe re t ropleural approach. Laminectomy alone isoften contraindicated in these situations and carriesa risk of neurological deterioration. Posterolateral ap-p roaches are more appropriate for lesions involvingt h ree-column dysfunction or greater than three seg-ments of involvement.
Indications for the ventral approach include pro-g ressive neurological deficit, lack of tissue diagnosis,instability and kyphosis during or following radiationtherapy, and patients with a known radio-re s i s t a n ttumor such as melanoma or hypern e p h roma orPott’s disease. Anterior decompression and stabiliza-tion also have the long-term benefit of minimizingp ro g ressive deform i t y .
PREOPERATIVE PREPARATIONS ANDANESTHETIC TECHNIQUEFollowing appropriate venous and arterial lineaccess, a lumbar epidural catheter can be placed forperioperative morphine installation, which markedlydiminishes postoperative pain, even at upper tho-
racic levels. Routine induction and intubation arethen accomplished. A double lumen endotrachealtube is requested for lesions above T6. A Foley cath-eter is placed and preoperative antibiotics are ro u-tinely administered. Air- c o m p ression boots are usedto prevent deep vein thro m b o s i s .
Operative PositioningThe side of the approach is determined primarily bythe level and location of the pathology. The patient ist u rned to a lateral position on a beanbag with asmall roll placed under the dependent axilla (Figure2). The upper arm is rested on a pillow. Thoracolum-bar lesions should be centered over the kidney bre a kor flexion joint of the operating table to improve theoperative exposure. The lower leg is flexed at the hipand knee to stabilize the patient. Suction aspirationof the beanbag secures the position. All bony pro m i-nences and subcutaneously coursing peripheralnerves are well padded.
Skin IncisionFor lesions between T5 and T10, a 12-cm skin inci-sion extending from the posterior axillary line to apoint 4 cm lateral to the posterior midline is madeover the rib at the level of the lesion (Figure 2). For aT8-9 disc herniation, for example, a skin incision ismade in line with the T9 rib, which will be re m o v e d .The skin incision must be altered for upper thoracic(T3-4) lesions. While forward flexion of the upper armand shoulder rotates the scapula superolaterally toexpose the T5 and T6 ribs, the T3-4 ribs re m a i nunder its cover. For these lesions, a “hockey-stick”
F i g u re 2. Artist’s drawing depicting patient positioning. Skin incisions for upper thoracic ( A ) ,midthoracic ( B ) , and thoracolumbar (C) levels are shown. (Reproduced from McCormick PC:R e t ropleural approach to the thoracic and thoracolumbar spine. N e u ro s u rgery 37:9 0 8 - 9 1 4 ,1995, with perm i s s i o n )

incision, which parallels the medial and inferiorscapular borders, is per f o rmed (Figure 2). The inci-sion is carried down through the scapular muscleattachments (i.e., the trapezius or rhomboid muscles)to the ribs. The detached scapula is rotated superi-orly to expose the appropriate rib. The approach tothe thoracolumbar junction is discussed separately.
OPERATIVE PROCEDUREAfter confirmation of the correct vertebral level, asubperiosteal detachment of the intercostal musclesover an 8-10 cm rib segment is perf o rmed. This ribsegment is removed (Figure 3A). Note that the mostp roximal 4 cm of rib, which is attached to the trans-verse process and vertebral body, remains in place. Awell-defined tissue layer is identified in the bed of theresected rib segment. This is the endothoracic fascia,which lines the entire thoracic cavity. The parietalpleura maintains its attachment to the inner chestwall through this layer. The potential space betweenthe parietal pleura and the endothoracic fascia maycontain a small amount of loose areolar tissue. Theendothoracic fascia is analogous to the transversalisfascia which lines the abdominal cavity. Both linetheir respective visceral cavities and are re f l e c t e dover the diaphragm as its fascia. The endothoracicfascia is continuous with the inner periosteum of therib and the thoracic vertebral bodies. Occasionally,muscle fibers of the inconstant subcostal musclemay be identified within this fascia in the rib bed.The thoracic sympathetic chain, intercostal vesselsand nerves, thoracic duct, and azygous veins arecontained against the thoracic wall and vertebralbodies within this fascial layer.
The endothoracic fascia is sharply incised in linewith the rib bed (Figure 3B). The parietal pleura isdissected widely off the undersurface of the endotho-racic fascia with Kitner (peanut) clamps, much thesame way in which the peritoneum is freed from thetransversalis fascia of the abdominal wall during are t roperitoneal exposure (Figure 4). The pleura isdissected proximally to expose the vertebral column.Small pleural tears are re p a i red with suture. A table-mounted malleable blade maintains lung re t r a c t i o n .Deflation of the lung with a double-lumen tube is not critical but does facilitate lung retraction at theupper thoracic levels (above T6). A self-re t a i n i n gcrank retractor on the adjacent ribs widens the expo-s u re. The endothoracic fascia is opened over the re-maining proximal rib segment with cautery. The soft-tissue attachments, costotransverse, and stellateligaments are sharply divided and the rib head is dis-articulated from the vertebral body (Figure 4b).
For thoracic disc removal, the endothoracic fasciaover the disc space is incised. This divides the sym-pathetic chain which descends on the vertebral col-umn just anterior to the rib head insertion (Figure5A). The fascia and the vertebral body periosteum
a re elevated in either direction away from the discspace. The intercostal vessels that run transverselyat the midvertebral body level are preserved withinthis reflected tissue. The margins of the pedicle aredefined sharply with curettes and nerve hooks.
The disc space is incised and evacuated withc u rettes and rongeurs (Figure 5B). A high-speed drillremoves the adjacent endplates and extends the dis-section into the adjacent vertebral bodies. The pedicleis also removed with the drill and Kerrison ro n g e u r s( F i g u re 6A). This provides access to the lateral spinalcanal, which is probed with a dissector. The bony ver-tebral body dissection can now be completed posteri-orly with knowledge of the canal’s location. Genero u sbony removal facilitates and assures adequate canald e c o m p ression. The depth of decompression shouldbe 3 to 3.5 cm from the lateral vertebral body marg i n .The corpectomy should extend about 1.5 cm oneither side of the disc space. This opening should bemaintained back to the dorsal cortical margin. Bonebleeding may be intermittently controlled withs m e a red wax at the end of a Kitner clamp.
Once the dorsal cortical margin has been suff i-ciently thinned, a reverse-angled curette sharply di-vides the posterior longitudinal ligament. The adher-ent endplates, annulus, and cortex are pushed downinto the corpectomy defect. This invariably results inepidural venous bleeding so it must be completedquickly. Bipolar cautery forceps may be passed oneither side of the vessels from the lateral canal en-trance for effective coagulation of the ventral epiduralvessels. The thin dorsal layer of the posterior longitu-dinal ligament usually remains. In the author’s expe-rience, the calcified thoracic disc is often suspendedwithin this layer and is not as commonly intraduralas the literature suggests. The ligament is gentlyp robed with a nerve hook for identification and deliv-ery of these fragments away from the spinal cord .Once adequate decompression has been achieved,t roughs are drilled into the adjacent vertebral bodiesand the harvested rib is placed as an interbody strutgraft (Figure 6B).
Vertebral body corpectomy re q u i res removal of anadditional rib head for adequate exposure. For a T7corpectomy, which has been exposed through the T7rib bed, for example, resection of the T8 rib head pro-vides exposure of the T7-8 disc space and adjacentT8 vertebral body and pedicle (Figure 7). The inter-costal artery and vein are divided between suture s ,close to the midline. Proximal ligation of the inter-costal artery can be safely perf o rmed because abun-dant muscular and osseous anastomoses will distallyreconstitute the occluded vessel and maintain spinalc o rd blood flow. Following disc exposure and inter-costal vessel ligation, the periosteum and endo-thoracic fascia are incised and elevated off the verte-bral body. The discs are incised and curetted asp reviously described. The corpectomy is completed
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8238

SCHWARTZ AND McCORMICK : RETROPLEURAL APPROACH TO THE THORACIC AND THORACOLUMBAR SPINE 239
F i g u re 3. A, an 8-10 cm rib segment is removed following subperiosteal dissection. B , the endothoracic fascia is openedin line with the resected rib bed. The pleura has been bluntly freed from its inner surface and remains intact. (Repro-duced from McCormick PC: Retropleural approach to the thoracic and thoracolumbar spine. N e u ro s u rgery 37:9 0 8 - 9 1 4 ,1995, with perm i s s i o n )
A B
F i g u re 4. The pleura is bluntly freed and retracted ( a ) f rom the under-s u rface of the endothoracic fascia to widely expose the posterior tho-racic wall and vertebral bodies. The neurovascular bundle ( b ) has beenpartially mobilized from its underlying fascia to improve visualization.The endothoracic fascia remains densely adherent to the posterior tho-racic wall and vertebral column. Incision and subperiosteal elevation ofthe endothoracic fascia then continue proximally over the rib head ( c ) ,the disc space, and adjacent vertebral bodies. (Reproduced fro mM c C o rmick PC: Retropleural approach to the thoracic and thoracolum-bar spine. N e u ro s u rgery 37:908-914, 1995, with perm i s s i o n )

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8240
F i g u re 5. A, the sympathetic chain is divided and the disc space sharply incised. B , the disc space is evacuated using curettes and ro n g e u r s .
A B
F i g u re 6. A, a high-speed drill is utilized for removal of adjacent endplates and pedicle. B , the harvested rib is placed asan interbody strut graft. (Figure 6A re p roduced from McCormick PC: Retropleural approach to the thoracic and thora-columbar spine. N e u ro s u rgery 37:908-914, 1995, with perm i s s i o n )
A B

SCHWARTZ AND McCORMICK : RETROPLEURAL APPROACH TO THE THORACIC AND THORACOLUMBAR SPINE 241
using rongeurs, curettes, and a high-speed drill.A p p ropriate reconstruction is then perf o rmed. There t ropleural approach must be modified at the thora-columbar junction (T11-L1) because of the dia-phragm and the greater caudal angulation of the ribs.In these cases, the skin incision and rib resection arep e rf o rmed two levels rostral to the pathological seg-ment. In the case of a T12 vertebral body exposure ,for example, a 12-14 cm skin incision is made overthe T10 rib from the posterior axillary line to 4 cm offthe midline (Figure 2). The incision is carried downt h rough the subcutaneous tissue and muscles to theT10 rib with cautery. A 10-cm segment of exposed ribis cleaned circ u m f e rentially and removed. The pleurals u rface of the diaphragm is identified. The endotho-racic fascia is reflected over the diaphragm andtightly applied to its surface. The costophrenic pleu-ral reflection may also be seen. The initial exposure istight because of the diaphragm attachment to theribs. If the lateral endothoracic fascia is present inthe rib bed, it is opened. Caudally, the pleural sur-face of the diaphragm is depressed and detachedf rom the inner surface of the T11 and T12 ribs withsharp periosteal dissectors. This immediately unitesthe re t roperitoneum with the re t ropleural space. Thedetachment is easily continued medially to elevate
the arcuate ligaments off the quadratus and psoasmuscles. The subcostal nerve can be seen runninglaterally beneath the lateral arcuate ligament on thequadratus lumborum surface. Division of the ipsilat-eral crus completes the diaphragm mobilization.Table-mounted malleable blades provide re t r a c t i o n .The proximal 4 cm of the T12 rib, including the ribhead, is removed. Part of the psoas muscle, whichattaches to the T12 vertebral body, may need to beelevated. This completes the exposure of the T12 ver-tebral body, adjacent disc, and T12 pedicle. Disc inci-sion or corpectomy is perf o rmed utilizing the princi-ples previously outlined.
C l o s u reFollowing decompression and stabilization, the arc u-ate ligaments are reattached to the psoas and quad-ratus muscles with suture. The pleura is then care-fully inspected. A chest tube should be placed if anypleural tears are identified. The remainder of thewound is closed in layers. Approximation of the adja-cent ribs with suture reduces the chest wall defor-mity associated with rib resection. Care is taken notto ensnare the intercostal nerves with suture duringc l o s u re. This may substantially increase postopera-tive pain.
F i g u re 7. A, adequate exposure for corpectomy re q u i res the removal of two proximal rib segments, incision and re m o v a lof discs both superior and inferior to the involved body, and proximal ligation of the intercostal vessels (a) at the aff e c t e dlevel. B, reconstruction is perf o rmed following adequate spinal canal decompression. (Figure 7B re p roduced fro mM c C o rmick PC: Retropleural approach to the thoracic and thoracolumbar spine. N e u ro s u rgery 37:908-914, 1995, withp e rm i s s i o n )
A B

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8242
COMPLICATIONS The following are commonly seen complications andsuggestions for avoiding them.
1 ) Pneumothorax can be avoided by repairing anypleural tears with sutures or staples under posi-tive pre s s u re ventilation. In the face of large tears,or if air remains in the intrapleural space at theconclusion of the pro c e d u re, a chest tube shouldbe placed.
2 ) CSF leak is prevented by visualizing the duraearly in the operation. This can be achieved byidentifying and removing the pedicle to expose thelateral canal.
3 ) H o rner’s syndrome can be avoided by pre s e r v i n gthe sympathetic chain in the upper thoracic re g i o nif possible. Do not use this approach above T3.
4 ) Spinal cord infarction can be avoided by not usingcautery in the foramen.
5 ) I n t e rcostal neuralgia is minimized by not suturingthe intercostal nerve during rib appro x i m a t i o n .This may be prevented by passing suture thro u g hholes drilled in the caudal rib. Also, avoid crush-ing the neurovascular bundle against rib withcrank re t r a c t o r s .
6 ) C a refully ligate the intercostal neurovascular bun-dle if perf o rming corpectomy. Preserve the inter-costal neurovascular bundle if only removing disc.
7 ) Pleural effusion can be avoided with selectiveplacement of a chest tube or even a Hemovacdrain in the re t ropleural space in cases wherehemostasis is not totally secure due to persistentoozing from epidural veins or bone to prevent sig-nificant re t ropleural fluid collection.

DEFINITION AND DIAGNOSISLateral disc herniation has been denoted by a varietyof terms, including herniation of the foramen, far lat-eral disc, posterior lateral disc, extreme lateral disc,and extraforaminal disc. Lateral disc herniation is de-fined here as herniated disc material pre d o m i n a n t l ylocated lateral to the midportion of the intervertebralforamen. This is compared to an intracanalicular disch e rniation when the disc lies in the midline (central)or out to the midportion of the intervertebral foramen(paracentral). A further diff e rentiation can be made ofa lateral disc herniation between a foraminal lateraldisc herniation (when the disc material is primarilylocated in the intervertebral foramen) and a far lateralh e rniation (when the herniated disc is mainly situ-ated extraforaminally and the nerve is compressed inits paraspinal course). The surgical approach is sig-nificantly influenced by the location of the disc hern i-ation relative to the intervertebral foramen (foraminalvs. far lateral) and whether any associated intraca-nalicular pathology, such as lateral recess stenosis,is present.
B e f o re the widespread use of computed tomogra-phy (CT) and magnetic resonance imaging (MRI) per-mitted an accurate diagnosis, lateral disc hern i a t i o n sw e re difficult to visualize and were often missed onroutine myelography. In surgical series, the incidence
SURGICAL TREATMENT OF L ATERAL LUMBAR HERNIATED DISCS
GIUSEPPE LANZINO, M.D.CHRISTOPHER I. SHAFFREY, M.D.JOHN A. JANE, SR., M.D., PH.D.
243
of lateral disc herniation ranges from 4% to 12% of allh e rniated lumbar discs. Lateral disc herniations gen-erally occur in older patients and at higher interspacelevels than routine (intracanalicular) hern i a t i o n s .Central and paracentral disc herniations involve theL4-5 or L5-S1 levels in 95% of reported cases. Lateralh e rniation occurs more frequently at higher lumbarspine levels; the L4-5 disc is affected in 40% of casesand the L3-4 level in 37%.
A superolateral migration of disc material occursin most cases of lateral lumbar disc herniation, whichresults in compression of the exiting nerve root at thelevel of the foramen (i.e., an L4-5 disc herniation com-p resses the L4 root). In contrast, with most intra-canalicular disc herniations, the traversing nerve ro o tis much more commonly affected (i.e., an L4-5 disch e rniation compresses the L5 root). Because of theanatomical relationships of the neural foramen, thenerve root and ganglion are displaced cranially and/or dorsally and are compressed against the loweredge of the upper pedicle. Downward migration of afragment is prevented by the lower pedicle. This supe-rior migration has important surgical implications be-cause disc fragment removal is frequently possiblewithout compromising the facet joint, which oftenoverlies the intervertebral disc space.
Since the L3 and L4 nerve roots are commonlyinvolved, patients with a herniated lateral disc oftencomplain of radiating pain and sensory changes inthe medial or anterior thigh. Quadriceps weaknessand reduced or absent patellar reflexes are commonfindings on neurological examination. The straight-leg raising test is usually positive if the L5 nerve ro o t© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8244
is involved, is sometimes present if the compre s s e dnerve root is L4, and is usually absent when the discinvolves the L3 root. The femoral stretch test is usu-ally positive when there is involvement of the L3 andL4 nerve ro o t s .
Optimally, high-resolution CT and MRI will dis-play lateral disc herniation when present. Lateralh e rniation can occur as an isolated condition or inassociation with other forms of spinal degenerativedisease. To avoid overlooking this source of neuralc o m p romise, careful analysis of the intervertebralforamen on the axial and sagittal images is war-ranted despite either the normal appearance of thecentral and paracentral disc or cases with associatedpathology. Signs of lateral disc herniation on MRIand/or CT studies include the presence of disc den-sity or disc signal material at the level of or lateral tothe neural foramen, displacement or obliteration ofperineural fat, and nerve root or ganglion compre s-sion/displacement.
Myelography alone has little value in the identifi-cation of far lateral disc herniation. In fact, this diagnostic test is often negative since the nerve com-p ression usually occurs outside the nerve root sub-arachnoid space. We frequently use CT myelographyas a complementary study for patients with lateraldisc herniation; the addition of high-resolution, thin-cut axial CT improves the diagnostic accuracy byshowing whether the disc fragment is in continuitywith the intervertebral disc and whether it en-c roaches on the nerve root just inside or lateral to theintervertebral foramen. We believe that CT myelogra-phy continues to have a significant role in the diagno-sis and management of lateral herniation because itp e rmits a better evaluation of associated lateral re-cess and spinal stenosis, especially in older patientsin whom lateral disc herniation often occurs. In addi-tion, CT myelography defines the bony anatomy bet-ter than MRI and improves preoperative planning byenhancing visualization of the orientation and loca-tion of the facet joints, and demonstrating the re l a-tionship of the disc herniation to the isthmus lami-nae and transverse pro c e s s.
PATIENT SELECTIONUnless a severe neurological deficit is present, con-servative management is recommended as a first-linet reatment for the patient with a lateral disc hern i a-tion. The early phase of conservative therapy includesp h a rmacological pain relief (generally with nonste-roidal anti-inflammatory agents) and a reduction ofactivities such as heavy lifting, prolonged sitting, ors t renuous exercise for several weeks. Prolonged bedrest is not indicated and is usually counterpro d u c-tive. Frequently, symptoms resolve with time and noadditional therapy is needed. Other treatment modal-ities such as physical therapy and selective perineu-
ral infiltration with steroid solution may be consid-e red in selected patients.
S u rgery is perf o rmed only when the patient’s painis persistent and disabling following a complete 6- to8-week course of conservative treatment. It has beensuggested that patients with a lateral herniated discmay experience lasting, disabling pain more oftenthan patients with an intracanalicular hern i a t i o n ;this may be caused by the involvement of the verysensitive posterior root ganglion.
ANATOMICAL CONSIDERATIONSFamiliarity with the relevant anatomy is of utmostimportance to fully understanding the surgical ap-p roach to lumbar lateral disc herniation. The inter-vertebral foramina are three-dimensional canals bor-d e red anteriorly by the more cephalad vertebral bodyand the intervertebral disc and posteriorly by thepars interarticularis of the vertebral body above (Fig-u res 1 and 2). The cranial vertebral body may consti-tute more of the anterior border of the foramen thanthe intervertebral disc. The superior margin is delim-ited by the inferior aspect of the pedicle of the upper
F i g u re 1. Illustration showing the anatomi-cal relationships of the neural foramen andthe far lateral space at diff e rent levels of thelumbar spine.

LANZINO ET AL : SURGICAL TREATMENT OF LATERAL LUMBAR HERNIATED DISCS 245
F i g u re 3. Transverse section illustrating the neurovascular anatomy and the direction ofthe surgical exposure obtained via an intertransverse route. (Reproduced from O’BrienM F, Peterson D, Cro c k a rd HA: A posterolateral micro s u rgical approach to extre m e - l a t e r a llumbar disc herniation. J Neuro s u rg 83:636-640, 1995, with permission)
F i g u re 2. R e p resentation of the normal anatomy. I n s e t , the ligamentum flavum is openedand a small hemilaminectomy is perf o rmed on the lamina of L3. The lateral and most infe-rior portions of the inferior facet of the superior lamina are removed for an extension out-lined by the dotted line. (Reproduced from Chenelle AG, Shaff rey CI, Lanzino G, et al:Treatment of far lateral discs by an approach lateral to the facet joint. Techn Neuro s u rg2 :249-253, 1996, with perm i s s i o n )
Inset
L4 superior facet
partial facetectomy
posterior primary ramus
ventral nerve root

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8246
vertebra, while the inferior margin is circ u m s c r i b e dby the superior aspect of the pedicle of the lower ver-tebral body. The entrance and exit to the foramena re the medial and lateral margins of adjacent pedi-c l e s .
Lateral to the foramen is the far lateral space. Thisspace is bord e red medially by the foramen, laterallyby the intertransverse ligament, anteriorly by the cra-nial vertebral body and disc covered by the annulusf i b rosus, and posteriorly by the lateral fibers of theligamentum flavum. The nerve root enters the fora-men and far lateral space medially and superiorly,adjacent to the pedicle of the superior vertebra, thenc rosses the disc space extraforaminally, laterally andslightly anterior to the posterolateral margin of thedisc. The dorsal root ganglion is found within theintervertebral foramen just medial to the lateral bor-der of the pars interarticularis. The nerve divides intothe posterior primary ramus and the ventral nerveroot immediately distal to the dorsal root ganglion.The ventral root crosses the disc space obliquely andpasses in close proximity to the lateral aspect of thecaudal pedicle. The posterior primary ramus travelsin a caudal and dorsal direction, passes between thepars interarticularis and the intertransverse muscleand ligaments, and then through a gap between themedial free edge of the intertransverse ligament andthe lateral free edge of the ligamentum flavum (Fig-u res 3 and 8). The lumbar segmental artery travelst h rough the space defined medially by the emerg i n gnerve root and laterally by fibers of the intertrans-verse ligament and divides into five re c o g n i z a b l ebranches. These branches include: 1) a branch to theu n d e r s u rface of the transverse process; 2) a dorsallyd i rected branch in the waist of the pars interarticu-laris; 3) a laterally directed branch that enters thespace between the multifidus and longissimus mus-cles; 4) a branch into the midlateral aspect of thee rector spinae muscles; and 5) a branch accompany-ing the lateral branch of the posterior primary ramus( F i g u res 3 and 8).
F rom a surgical point of view, the operative ap-p roach to the far lateral space is limited dorsally bythe isthmus laminae (defined as the lateral margin ofthe interarticular portion of the lamina); superiorly bythe inferior margin of the cranial pedicle, the trans-verse process, and, when present, by a prominent ac-cessory process; and inferiorly by the apophysealjoint of the articular facet. The relationships amongthese structures vary significantly at diff e rent levelsand the operative exposure to the lateral space be-comes pro g ressively smaller in the lower lumbarspine, especially at L5-S1 (Figure 1).
The lumbar spinal anatomy is a major considera-tion in determining the appropriate approach to a lat-eral disc herniation. Significant compromise of thefacet joint should be avoided when possible. These
anatomical considerations strongly affect the micro-s u rgical approach to an extraforaminal disc hern i a-tion. From L1-2 to L3-4, a midline approach, with lat-eral retraction of the paraspinal muscles past thefacet joints to expose the isthmus of the lamina andthe proximal transverse processes, allows for enoughe x p o s u re of the lateral portion of the intervertebralforamen.
In the upper lumbar spine (L1-2 to L3-4), thepedicles arise vertically from the dorsal aspect of thevertebral bodies; the distance between the inferiorm a rgin of the upper transverse process and the su-perior boundary of the facet joint averages 10 mm.The width of the isthmus lamina is small so that thelateral disc herniation at these levels frequently lieslateral to the isthmus. Because of the usual superiormigration of the lateral disc herniation, a few milli-meters of the isthmus need to be removed to identifythe nerve root, the ganglion, and the disc fragment(following removal of the lateral extension of the liga-mentum flavum, intertransverse muscle, and liga-ment). At these levels the facet joint partially or com-pletely covers the intervertebral disc, but rarely ism o re than a small resection of the superior aspect ofthe facet needed. Often at L4-5 and always at L5-S1,an exposure through a paramedian incision perm i t sa more direct approach and reduces the need for sig-nificant bone resection. However, in cases with sig-nificant spinal or lateral recess stenosis, or when se-v e re facet tropism is present, partial or completefacetectomy is occasionally re q u i red to adequatelyd e c o m p ress the nerve ro o t .
Conversely, at the L4-5 and L5-S1 levels the op-erative exposure decreases in size because the pedi-cles originate more obliquely, the isthmus laminaea re substantially wider, a prominent accessory pro-cess may be present, and the facet joints substan-tially overlie the intervertebral disc space. There isalso a pro g ressive decrease in the cephalocaudal di-mension of the operative window because of dimin-ished distance between the inferior border of thetransverse process of L4, the superior and lateral as-pects of the facet joint and the transverse process atthe L4-5 level, and the superior and lateral aspects ofthe facet joint and of the sacrum at L5-S1. The L4-5and L5-S1 facet joints may overlap the intervertebraldisc space significantly. Frequently, resection of thelateral aspect of the isthmus, the inferior aspect ofthe superior transverse process and accessory pro-cess, the lower one fourth of the superior pedicle, andthe superior one fourth of the facet joint is needed toachieve satisfactory exposure, especially at the L5-S1level.
SURGICAL CONSIDERATIONSLateral disc herniation presents a particular pro b l e ms u rgically because the disc fragment and disc space

LANZINO ET AL : SURGICAL TREATMENT OF LATERAL LUMBAR HERNIATED DISCS 247
a re often hidden either under or lateral to the facetjoint, especially at lower lumbar levels. Several sur-gical approaches to this area have been described: 1) a unilateral facetectomy through a midline inci-sion; 2) a muscle-splitting paraspinal operation withlateral dissection between the transverse pro c e s s e s ;3) a partial hemilaminectomy with partial or completefacetectomy; 4) a re t roperitoneal approach; and 5) ahemilaminectomy with foraminotomy (more re c e n t l y ,a midline approach with a partial resection of theisthmus laminae). This multiplicity of surgical ap-p roaches underscores the difficulty in achieving ade-quate exposure without potentially destabilizing thespine in the course of treating these herniations. An-atomical variations for each patient should be ana-lyzed on both plain radiographs and imaging studiesto help determine the optimal approach. Specific at-tention should be given to the bony structures in theintertransverse process region. Coexisting pathologywithin the canal should be defined and the operativea p p roach tailored to address all significant pathology.Significant coexisting pathology such as severe facetjoint arthritis, significant lateral recess or foraminalstenosis, or synovial cyst formation may re q u i re in-complete or total facetectomy. In cases where the fa-cet joint has been significantly compromised, simul-taneous fusion may be considered. We have graduallymodified our surgical approach, placing greater em-phasis on maintaining the integrity of the facet joint.
The diff e rent approaches described can be dividedin two broad categories: midline hemilaminectomy,and paramedian splitting of the paraspinal muscles.The paramedian muscle-splitting approach allows alateral exposure either through the longissimus-ilio-costalis interval or via a muscle-splitting appro a c ht h rough the iliocostalis muscle. This lateral ap-p roach provides more direct visualization of the discfragment and permits reduced bone excision andmuscle retraction, allowing greater exposure thanthe midline approaches. This approach can be eff e c-tively perf o rmed in cases of extraforaminal lateraldisc herniation at any level and is frequently the pro-c e d u re of choice for cases of foraminal or extraforam-inal disc herniation at the L4-5 or L5-S1 levels. Theanatomy involved, however, is somewhat unfamiliarto most neuro s u rgeons and it is not possible to di-rectly address any intracanalicular pathology.
The midline approach with several modificationsis favored by many surgeons because of the ease ofdissection, familiarity with the operative anatomy,and the ability to address pathology within thespinal canal. We believe that most disc hern i a t i o n swithin the intervertebral foramen at the L2-3 and L3-4 levels can be reached via a hemilaminectomya p p roach (J.A.J.) or by an approach lateral to theisthmus lamina with resection of a portion of theisthmus (C.I.S.). Nevertheless, isolated disc hern i a-
tions truly lateral to the facet joint from L1-2 to L3-4can be very effectively undertaken via a midlinea p p roach lateral to the isthmus lamina withouthemilaminectomy. For far lateral disc hern i a t i o n s ,only a very small portion of the isthmus usuallyneeds to be resected. This technique spares themajority of the facet joint and reaches the disct h rough the interval between the inferior aspect ofthe superior transverse process and the superiorb o rder of the inferior facet joint. If more than 50% ofthe facet joint is removed, the risk of spinal instabil-ity ranges between 1.6% and 2.4% and the incidenceof back pain is substantially higher. Removing eitherthe entire medial or lateral half of the facet jointresults in total facet joint compromise. By pre s e r v i n gthe facet joint, the risk of instability and postopera-tive pain is substantially reduced. If re q u i red, explo-ration of the intraspinal compartment can be per-f o rmed through a partial hemilaminectomy forremoval of any additional disc fragments or tre a t-ment of associated lumbar or lateral recess stenosis( p resent in 20% to 72% of the cases). If a simultane-ous partial hemilaminectomy is planned, care mustbe taken not to make the isthmus overly thin afterresection of the lateral aspect of the isthmus lamina.Consequences include predisposition to fracture asthe patient regains full activity, back pain, andspinal instability.
Midline Approach With or Without H e m i l a m i n e c t o m yAfter the administration of perioperative antibioticsand steroids and infiltration of the skin and para-spinal muscles with 0.25% bupivacaine with 1:200,000 epinephrine, a midline skin incision of 6 to10 cm is made slightly superior to the disc space ofi n t e rest (Figure 4A). Dissection is carried down to thelevel of the thoracolumbar fascia, which is opened ina curvilinear fashion away from the insertion on thespinous process. This flap is retracted past the mid-line. Electrocautery and a periosteal elevator are usedto subperiosteally dissect the paraspinal musclesaway from the spinous processes and lamina. Theparaspinal muscles are retracted just past the lateralb o rder of the facet joint and a self-retaining re t r a c t o ris inserted to maintain retraction (Figure 5). Care istaken to preserve the facet joint capsules during the exposure. The proximal aspect of the transversep rocesses, the isthmus lamina, and the facet jointcapsules are identified. An intraoperative lateral radi-ograph is then taken to confirm the level of the dis-section; a blunt marker placed lateral to the isthmusgives a good indication of position and facilitates ori-e n t a t i o n .
We routinely use an operating microscope for bone resection and disc fragment removal to allow adequate magnification and proper illumination.

A microdrill is used to remove a small portion of theisthmus and, if re q u i red, the inferior aspect of thesuperior transverse process and accessory pro c e s s ,the lower one fourth of the superior pedicle, and thesuperior one fourth of the facet joint. The amount ofbone resection re q u i red is frequently less with upperlumbar levels than with lower levels. This methodusually provides adequate access to remove the disch e rniation. The intertransverse fascia and the lateralextension of the ligamentum flavum are re m o v e donly when drilling and bony resection are completedbecause the dorsal root ganglion is vulnerable tot h e rmal or mechanical trauma. The intertransver-sarii muscles and the intertransverse ligament cannow be sharply removed from the transverse pro c e s sof the superior vertebral body. This exposes the nerveroot of interest, and ruptured disc material is usuallyseen inferior to the nerve root. The herniated lateraldisc can then be removed with little nerve root re t r a c-tion. Brisk bleeding can occur from the lumbar seg-mental artery and its branches if they are inadver-tently compromised. Bipolar coagulation of bleedingvessels should be perf o rmed with good visualizationof the vessel to avoid thermal trauma to the dorsal
root ganglion.At the middle and lower lumbar levels, it can be
d i fficult to enter the intervertebral disc space via thisa p p roach. The amount of aggressive disc re m o v a lf rom within the disc space has been reduced as wehave observed that removal of the free fragment is allthat is re q u i red for symptomatic relief in most cases.
If exposure within the spinal canal is anticipated,the ligamentum flavum is opened more medially anda small hemilaminectomy is perf o rmed laterally onthe superior lamina (Figure 2 inset). A small portionof the lateral section of the superior facet of the infe-rior vertebral body can be removed without compro-mising the facet joint (Figure 2 inset). Care is takento maintain the integrity of the isthmus lamina. Ift h e re is associated intraspinal herniation and/orstenosis, the laminectomy can be enlarged to com-plete the intraspinal portion of the pro c e d u re (Fig-u res 6 and 7A). To ensure complete decompre s s i o nof the nerve root once the discectomy is completed,the foramen can be explored from inside and outsidethe canal using a blunt nerve hook (Figure 7B). Atthe end of the pro c e d u re, fat grafts are placed overthe extraforaminal and intraspinal defects.
Intertransverse Appro a c hThe patient is placed in the prone position on aspinal frame. A spinal needle is inserted in the mid-line in the interspace of interest and an intraopera-tive x-ray is obtained to confirm the correct level. Theskin and the paraspinal muscles are anesthetizedwith 0.25% bupivacaine with 1:200,000 epinephrine.A vertical incision, usually 8 to 10 cm in length, ismade 10 cm from the midline (Figure 4B) thro u g hskin, fat, and then investing deep fascia. The trans-verse process is then palpated and access is gainedin a 30-degree line to the horizontal by longitudinallysplitting fibers of the iliocostalis muscle (Figure 3).The muscle is separated by blunt dissection, andhandheld retractors are placed. A neuro v a s c u l a rband can be felt obliquely crossing the vertical mus-cle fibers and is followed ventromedially to the pedi-cle-transverse process junction (Figure 8A). A self-retaining retractor is inserted to maintain exposure .The operative microscope is then brought into posi-tion and the pedicle-transverse process junction isidentified. When these steps have been followedc a refully, this approach allows for a relatively avas-cular exposure. Adjacent to the intervertebral fora-men is often a “plug” of fat which, when removed, ex-poses the origin of the posterior primary ramus, theganglion, and the ventral root. Careful dissection ofthe tissue planes will separate the neuro v a s c u l a rs t r u c t u res from the disc fragment, which can be re-moved with pituitary micro rongeurs without boneresection (Figure 8B).
Most lateral disc herniations are sequestered frag-
NEUROSURGICAL OPERATIVE ATLAS. VOL. 8248
F i g u re 4. A straight incision is made along themidline for the medial hemilaminectomy ap-p roach (A) or 10 cm from the midline at thelevel of interest for the intertransverse pro c e s sa p p roach ( B ) .
AB

LANZINO ET AL : SURGICAL TREATMENT OF LATERAL LUMBAR HERNIATED DISCS 249
F i g u re 5. After incising the lumbosacral fascia in a curvilinearfashion, the paraspinal muscles are dissected using aperiosteal elevator and retracted laterally. (Reproduced fro mChenelle AG, Shaf f rey CI, Lanzino G, et al: Treatment of farlateral discs by an approach lateral to the facet joint. Te c h nN e u ro s u rg 2:249-253, 1996, with perm i s s i o n )
F i g u re 6. A, the intertransverse muscle is sharply removed and the lateral herniated disc overlying thenerve root is visualized. B , the disc is removed. (Reproduced from Chenelle AG, Shaff rey CI, Lanzino G,et al: Treatment of far lateral discs by an approach lateral to the facet joint. Techn Neuro s u rg 2:2 4 9 - 2 5 3 ,1996, with perm i s s i o n )
A Btraversing nerve root
dural sac

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8250
F i g u re 7. A, if the herniated disc extends medially to the neural foramen, the hemi-laminectomy is extended and the disc removed working on both sides of the foramen.B , a blunt nerve hook is inserted in the neural foramen to verify that no disc frag-ments are left behind. (Reproduced from Chenelle AG, Shaff rey CI, Lanzino G, et al:Treatment of far lateral discs by an approach lateral to the facet joint. Techn Neuro -s u rg 2:249-253, 1996, with perm i s s i o n )
A B
F i g u re 8. A, the microscopic view obtained by the intertransverse route. B , after microdissection, the disc canbe removed, decompressing the nerve root. (Reproduced from O’Brien MF, Peterson D, Cro c k a rd HA: A posterolateral micro s u rgical approach to extreme-lateral lumbar disc hern i a t i o n . J Neuro s u rg 83:6 3 6 - 6 4 0 ,1995, with perm i s s i o n )
A B
medial intertransverse muscle
medial branch of theposterior primary ramus
extreme lateral disc herniation
lateral branch of the posterior primary ramus
terminal branch of thesegmental artery
ventral nerve rootdorsal root ganglion
transverse process
intertransversemuscle
herniated disc
exiting nerveroot

LANZINO ET AL : SURGICAL TREATMENT OF LATERAL LUMBAR HERNIATED DISCS 251
ments. If a diffuse disc bulge is present, the annuluscan be incised and fine rongeurs used to remove thedegenerated disc material. When a more medial ex-p o s u re is re q u i red, the lateral margin of the isthmuslamina or facet joint can be removed without jeopar-dizing facet integrity. After discectomy, the split mus-cle comes together and sutures are confined to thedeep fascia and superficial layers. No drains are nec-essary and the patient is mobilized a few hours afterthe surgical pro c e d u re .
CONCLUSIONSWith the availability and routine use of CT and MRI,intraforaminal and far lateral disc herniations arediagnosed more frequently. Lateral herniated discspose particular surgical problems because the disc iseither behind or lateral to the facet joint and it is diff i-cult to treat using a standard lumbar hemilaminec-tomy without significantly compromising the facetjoint. In cases of L1-2 or L3-4 lateral disc hern i a t i o n s ,
we recommend a midline approach with resection ofa small portion of the isthmus lamina that spares themajority of the facet joint. For some L4-5 and mostL5-S1 far lateral disc herniations, the anatomical re-lationships often make an intertransverse appro a c hm o re convenient. Each technique has its advantagesand disadvantages. The midline approach allows for easy exploration of the intraspinal compartmentt h rough a hemilaminectomy when medial extensionof the lateral disc fragment, foraminal stenosis, lum-bar stenosis, or intracanalicular pathology is pre s e n tat other levels. This technique is easy to learn andthe anatomy involved is familiar to neuro s u rg e o n s .The amount of resection of the isthmus lamina andfacet joint decreases as surgeons’ familiarity with thisa p p roach increases.
The paramedian intertransverse technique is lessfamiliar to many neuro s u rgeons and re q u i res a news u rgical orientation. This technique, however, allowsremoval of the disc with minimal bone resection anddamage to the soft tissues and offers a more dire c tavenue to far lateral disc herniations, especially atthe lower lumbar levels.


INTRODUCTIONPrimary and metastatic tumors may both involve theupper thoracic spine, and occasionally trauma aff e c t sthis region of the spinal column. The standarda n t e rolateral cervical approach combined with a me-dian sternotomy provides satisfactory exposure of thecervicothoracic junction from C7 through the T2-3junction, whereas a high posterolateral thoracotomyallows access to the thoracic spine up to the T3-4disc space. The T3 through T4 region, on the otherhand, is mostly hidden behind the great vessels, andneither of the approaches described above would beoptimal for exposure of this region, which is locatedat the apex of the chest pyramid and offers little ro o mfor maneuvering instruments. The “trap door” expo-s u re described by Nazzaro and coworkers in 1994 isa combination of the anterolateral cervical appro a c h ,median sternotomy, and anterolateral thoracotomyand is the most suitable intervention for gainingaccess not only to the T3 and T4 vertebral bodiesanteriorly, but also to the entire ventral cervicalspinal column, as well as to the mid and upper tho-racic spine. Unlike previously described appro a c h e sto the cervicothoracic junction, it also spares thes t e rnoclavicular junction and does not re q u i re tran-section of the clavicle.
“TRAP DOOR” EXPOSURE OF THE C E RVICOTHORACIC JUNCTION
ZIYA L. GOKASLAN, M.D.GARRETT L. WALSH, M.D.
253
PATIENT SELECTIONThe main indication for this surgical pro c e d u re is ananteriorly located pathology resulting in spinal cordc o m p ression due to re t ropulsed bone or disc frag-ments and/or tumor mass or kyphotic angulation,primarily affecting the T3 and T4 levels. Although the anterior weight-bearing spinal column can bee ffectively reconstructed, either by using polymethyl-methacrylate or a bone graft after the removal of avertebra, the placement of supplemental anteriorinstrumentation is difficult to achieve due to the lackof appropriately designed upper thoracic spinal fixa-tion devices. Whereas anterior cervical plate ands c rew constructs can be used for the fixation of thisregion in the absence of severe kyphotic angulation,additional posterior instrumentation is usually re c-ommended for those who have significant spinal de-f o rm i t y .
In patients who have significant spinal cord com-p romise at the time of presentation, surgical inter-vention is usually per f o rmed within 12 to 24 hoursof diagnosis. In patients with traumatic injuries,h o w e v e r, one may elect to postpone surgery untilother concomitant injuries are dealt with and thepatient is stabilized medically.
W h e reas magnetic resonance imaging (MRI) isp re f e r red for evaluating the cervicothoracic junctionand upper thoracic spine in most patients, computedtomography (CT) can provide important additionaldetails of bony anatomy and is very helpful in deter-© 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8254
mining the nature of compressive pathology (i.e., thep resence of re t ropulsed bone fragment(s) vs. tumormass effect). This is particularly important if one iscontemplating the use of radiation therapy as theprimary mode of tre a t m e n t .
Isolated lesions involving the spine but not thelung can be addressed in patients with marginal pul-monary function. In addition, because the right re-c u r rent laryngeal nerve is at considerable risk duringthe exposure, an appropriate preoperative laryngo-scopic examination is usually needed to rule outvocal cord paralysis, especially in those in whom aleft-sided re c u r rent laryngeal nerve dysfunction isa l ready suspected.
PREOPERATIVE PREPARATIONIn addition to the routine monitoring needed for gen-eral anesthesia, the patient should undergo place-ment of a larg e - b o re intravenous catheter, becausethese surgical pro c e d u res may re q u i re a significantamount of blood volume replacement during the ver-t e b rectomy pro c e d u re. This catheter is placed in afemoral or left subclavian vein, thereby avoiding theright internal jugular and right subclavian veins,which are in the surgical field. The intravascular vol-ume status is monitored with either a central line ora Swan-Ganz catheter, depending upon the patient’sc a rdiopulmonary reserve. Second-generation cepha-losporins are routinely administered pre o p e r a t i v e l yfor pro p h y l a x i s .
ANESTHETIC TECHNIQUEThe use of inhalation anesthetics should be mini-mized in order allow somatosensory evoked potential(SSEP) monitoring for assessment of spinal cordfunction during surg e r y .
OPERATIVE POSITIONINGThe patient is positioned as described in Figure 2A.
OPERATIVE PROCEDUREThe skin incision’s path and the location of criticalcuts through the chest wall that are needed to expose
the important anatomical structures are illustratedin Figure 1 (with inset). This exposure is carried outt h rough the right side. The incision extends along theanterior border of the sternocleidomastoid muscledown to the sternal notch, as shown in the intraoper-ative photograph (Figure 2A). From there the incisionis carried down the midline and over the sternum tothe fourth intercostal space, where it curves laterallyand follows the fourth interspace.
The neck platysma is then incised, and a plane isestablished between the carotid sheath (laterally)and the tracheoesophageal viscera (medially) usingblunt dissection. During this stage of exposure, boththe omohyoid muscle and middle thyroid vesselsmay need to be ligated and transected to gain accessto the lower cervical spine. Subsequently, dissectionis carried further down to the prevertebral fasciae,w h e re the longus colli muscles are visualized bilater-ally, running longitudinally over the anterior cervicalspinal column off the midline. A plane is establishedat this point between the manubrium and the under-lying vascular structure s .
The anesthesiologist is then instructed to selec-tively deflate the right lung, so that the chest cavitycan be entered without injuring the lung under-neath. Next, a sternal saw is used to transect thes t e rnum in the midline down to the fourth inter-costal space (Figure 2B), where this cut is connectedlaterally to the previously made thoracotomy inci-sion. A chest spreader is placed to open the stern u min the midline and to retract the anterior chest walls u p e rolaterally (Figure 2C). At this stage, the mam-mary artery is identified and may need to be ligatedand transected to permit further retraction of thechest wall.
Attention is then directed toward the caro t i dsheath. The sheath is opened and the vagus nerveidentified (Figure 2D). The innominate artery is thenlocated under the sternal notch and is dissected fre elaterally up to the take-off of the right carotid artery.Just distal to that, the right subclavian artery is iden-tified and the vagus nerve is traced down to the take-o ff of the right re c u r rent laryngeal nerve, which loops
F i g u re 1. Artist’s depiction of the “trap door” exposure. Anterolateral chest wall is retracted superolaterally. Retractors inthe upper cervical region and over the sternal angle allow visualization of all important anatomical structures in the midline.The right carotid artery and right vagus nerve are pulled laterally, whereas the right re c u r rent laryngeal nerve (shown exag-gerated to demonstrate its entire course and relationship to the subclavian artery and tracheoesophageal structures) isretracted ventrally and medially. The anterior cervical spinal column is visualized through the space between the caro t i dartery and the tracheoesophageal viscera. In the chest cavity, the aorta, the left common carotid artery (origin), the innomi-nate artery, the right subclavian artery, and the take-off of the right common carotid artery are shown. Also visible are thetransected azygos vein, the superior vena cava, and the left brachiocephalic vein. Rib heads have been removed, and T3 andT4 vertebrectomies have been completed. Through the vertebrectomy defect, the dura and the right T3 nerve root are seen.

GOKASLAN AND WALSH : “TRAP DOOR” EXPOSURE OF THE CERVICOTHORACIC JUNCTION 255
F i g u re 1.
right internal jugular veinsternocleidomastoid muscle
esophagus
azygos
lung
duraright brachio-cephalic vein
T3 nerve root
right commoncarotid artery
cervical spine
right vagusnerve
right atrium
right ventricle
trachea
right recurrent laryngeal nerve
innominate arteryleft brachiocephalic vein
superior vena cava
sternum
aorta
T5

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8256
right recurrentlaryngealnerve
innominateartery
rightphrenicnerve
superiorvena cava
aorta
right brachiocephalic
vein
leftbrachio-cephalicvein
rightvagusnerve
right commoncarotid artery
heartrightlung
A
B
C
D
E
F

GOKASLAN AND WALSH : “TRAP DOOR” EXPOSURE OF THE CERVICOTHORACIC JUNCTION 257
under this vessel. This nerve is then traced moremedially to where it enters the tracheoesophagealg roove, and a vessel loop is placed around it for iden-tification. Similarly, vessel loops are placed aro u n dthe carotid, subclavian, and innominate arteries, aswell as the brachiocephalic vein. Further dissectionat this stage also allows visualization of the thymus.
After the re c u r rent laryngeal nerve has been iden-tified and properly protected, blunt dissection isused to obtain further exposure of the cervicotho-racic junction. This provides exposure of the upperthoracic spine, usually at the T1-T2/3 junction. T3and T4 are mostly hidden from view behind the gre a tvessels. The junction of the mediastinal, apical, andposterior chest wall pleurae covers the anterior anda n t e rolateral surface of the T3 and T4 vertebral bod-ies. The pleura is incised over the spinal column andis dissected off the spine (Figure 2E). The azygos veinusually crosses the T4-5 disc space from a lateral toa medial direction in joining the superior vena cava.This vein is dissected free of the surrounding are o l a rtissue and is ligated, transfixed, and transected.
At this point it is possible to visualize the segmen-tal vessels at the T3 or T4 levels and, if needed, atthe T5 level. These vessels are doubly ligated with 2-0 silk ties, clipped, and transected, allowing them tobe dissected free of the vertebral bodies and to beretracted more laterally. After the thoracic level hasbeen confirmed, either with an intraoperative x-rayor by visual inspection, the vertebrectomy is carriedout using the standard landmarks. Usually, the discspace between the vertebrae above and below is
identified, and then the annulus is incised using a #15 blade. Subsequently, the disc material is re-moved using curettes of various sizes and Leksellrongeurs. A high-speed diamond-tipped burr is typi-cally used to remove the vertebral body down to thelevel of the posterior longitudinal ligament.
In the case of tumor resection, an ultrasonic aspi-rator is often useful for breaking down and aspiratingthe tumor in a piecemeal fashion. Bipolar electro-cautery is used for hemostasis. After the posteriorlongitudinal ligament is exposed, it is opened and re-moved, usually with a small upward-angled cure t t e .Either transaxial illumination with headlights andloupe magnification or an operating microscope canbe used during this part of the pro c e d u re .
R e c o n s t r u c t i o nAfter completion of the vertebrectomy, re c o n s t r u c-tion of the spinal column is perf o rmed. In patientswith tumors, polymethylmethacrylate is used. How-e v e r, in trauma patients, autologous bone from theiliac crest is pre f e r red. A fibular strut graft or a tibialallograft can also be used for reconstruction of theanterior weight-bearing spinal column.
After completion of the reconstruction, the place-ment of anterior instrumentation can usually be car-ried out using a cervical plate and screw construct( F i g u re 2F). The low cervical exposure present at thispoint allows insertion of the screws into the vertebralbodies anteriorly at the T2 level, whereas the loweraspect of the plate can be carried down to T5 or evenf u r t h e r, depending upon the number of levels of ver-
F i g u re 2. Intraoperative photographs of the patient presented as an illustrative case. A , the position of the patient andplanned skin incision prior to draping. The patient’s head is turned to the left and his neck is slightly extended by placing aroll between the scapulae. The arms are tucked in at the sides and padded. The incision follows the anterior border of thes t e rnocleidomastoid muscle down to the sternal notch, from which it is carried to the fourth intercostal space over the ster-num in the midline. The incision is then curved laterally, following the space between the fourth and fifth ribs. Also visible isa double-lumen endotracheal tube that allows selective ventilation of the lungs during surgery. B , the use of a sternal sawfollowing cervical dissection and completion of the anterolateral thoracotomy. C, close-up view, showing the transition fro mthe lower cervical region to the chest cavity. The anterolateral parietal pleura, along with the chest wall, is retracted supero-laterally. Also visualized are the right lung and the right brachiocephalic vein, as well as the pericardium (more medially). D ,all the anatomical structures of importance. The lower cervical dissection has been completed, and the right lung has beenselectively deflated. Visualized structures include the right common carotid artery, right vagus nerve, right innominateartery, right subclavian arteries (origin), right brachiocephalic vein, pericardium, and aorta. Also seen is the right re c u r re n tlaryngeal nerve, which loops around the right subclavian artery and enters the tracheoesophageal groove, crossing the C7-T1 vertebral region. The surgeon’s hand is retracting the tracheoesophageal viscera medially. E , close-up view of the poste-rior chest wall and the upper thoracic spine. The surgeon’s hand is retracting the right lung to show the thoracic spinal col-umn, which is covered by parietal pleura extending from the mediastinum. Parietal pleura has been resected over the spineinferiorly, down to the T5-6 disc space. Also seen are the DeBakey forceps, which have been passed from the lower cervicalregion into the chest cavity through an opening in the apical pleura. The azygos vein, which crosses the field at the T4-5level, has been ligated and transected, allowing further medial retraction of mediastinal pleura. F, close-up view showing thefinal construct. The T2 through T4 vertebrectomy has been completed, and the anterior spinal column has been re c o n-structed with polymethylmethacrylate, which is hidden from view under the plate. Lateral to the plate, decompressed duracan be observed. The cervical plate extends from T1 to T5 and has vertebral body screws located at the T1 and T5 levels.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8258
t e b rectomy perf o rmed during the pro c e d u re. At thispoint, exposure of the lower cervical spine is achievedin a standard fashion by mobilizing the longus collimuscles bilaterally. At no time during this pro c e d u reshould metal retractors be used, as they could poten-tially compress the re c u r rent laryngeal nerve.
C l o s u re Te c h n i q u e sAfter completion of the instrumentation, the rightlung is re-expanded. Following irrigation of the chestcavity, two chest tubes are usually placed, one locatedposteriorly and the other more anteriorly. Both tubesa re brought out through the anterolateral chest wallalong the anterior axillary line at the T8-9 level. Theribs are brought together with a rib appro x i m a t o r, andthe rib cage is closed using 2-0 Vicryl pericostal inter-rupted sutures. The sternum is closed using inter-rupted 5-gauge stainless steel wires. The peristern a lfascia and the subcutaneous layer are closed with 1-0and 2-0 Vicryl sutures, respectively. The neck incisionis closed at the platysmal layer using 3-0 Vicryl run-ning sutures. The subcutaneous layer in the cervicalregion is approximated using 3-0 Vicryl inverted inter-rupted sutures, and the skin is closed using a subcu-ticular 4-0 Vicryl running suture .
Both the sternal incision and the antero l a t e r a lthoracotomy incision can be closed using either sta-ples or a subcuticular running suture. If needed, anadditional drain can be placed in the cervical inci-sion and brought out of the operative field through aseparate stab wound incision.
Specialized InstrumentationT h roughout the pro c e d u re, the important vascularand neural structures are protected and are in viewat all times. A diamond-tipped burr is used exclu-sively for the removal of the vertebral body because itdoes not snag either the dura (during the exposure ofthe thecal sac) or the other soft tissue structure sa round the exposed area. In addition, an ultrasonicaspirator is very helpful for removing tumor tissue.
M o n i t o r i n gDuring the pro c e d u re, SSEP monitoring is ro u t i n e l yused to assess the spinal cord function. Fluid vol-ume replacement is determined by the blood lossobserved during the pro c e d u re, as well as by intra-venous pre s s u re or Swan-Ganz catheter re a d i n g s .
COMPLICATIONSComplications of the “trap-door” exposure of the cer-vicothoracic junction pro c e d u re are those typical ofa n t e rolateral cervical exposure, as well as complica-tions related to the thoracotomy pro c e d u re. The neu-ral structure at highest risk is the re c u r rent laryngealnerve, and great attention should be paid to pre s e r v e
this structure completely, as well as to avoid placingit in traction, especially with metal retractors, duringthe exposure. Other structures at risk include the ca-rotid artery, the subclavian and vertebral arteries (asthey are dissected out), the vagus nerve, and, moremedially, the esophagus and trachea. Blunt dissec-tion allows protection of the tracheoesophageal struc-t u res medially and the carotid artery more laterally.
In the chest cavity, the great vessels, the innomi-nate artery, the subclavian artery, and the brachio-cephalic vein can potentially be injured during thedissection. However, injuries to these structures canbe dealt with more easily if the thoracic surgical ex-p o s u re has already been completed.
Should a dural tear occur during the vertebre c-tomy pro c e d u re, its primary repair is extremely diff i-cult. In this situation, one can usually place a pieceof muscle or fascia lata over the dura along withGelfoam and fibrin glue. If cere b rospinal fluid (CSF)is visualized during surgery, placement of a postop-erative lumbar drain for CSF drainage for 4 to 5 daysfollowing the operation is almost always re q u i re d ,and the patient is kept at bed rest. If the surgeon be-lieves the potential exists for a continuous CSF leak,a vascularized intercostal muscle flap can be used toplug the dural opening. Again, this would re q u i repostoperative lumbar CSF drainage. Unfortunately,the chest tubes that are routinely placed to pre v e n tpostoperative hemo- or pneumothorax would alsocontribute to a CSF leak by creating a negative pre s-s u re. There f o re, in the presence of an intraoperativeCSF leak, one should remove chest tubes as quicklyas possible (i.e., as soon as the thoracic output hasfallen below 150 cc in 24 hours or when there is no significant pneumothorax on the follow-up chest x-ray). A CSF leak occurring postoperatively in spite of these precautions may re q u i re reoperation andrepair of the dural tear, usually with a vascularizedmuscle graft (as described above) and postoperativeCSF drainage.
Esophageal laceration can also occur, either as aresult of sharp dissection or from the sharp teeth ofthe cervical retractors. If the laceration of the esopha-gus is recognized intraoperatively, it should underg oprimary re p a i r. The wound should be drained and thepatient placed on nasogastric drainage for at least 7to 10 days. Subsequently, a barium swallow studyshould be obtained to confirm that the perf o r a t i o nhas sealed. However, in the majority of the cases, in-jury to the esophagus is not recognized at the time ofs u rgery and presents later as a local infection, fistula,generalized sepsis, or mediastinitis. The presence ofc repitus in the neck or of mediastinal air on a chestx-ray should strongly suggest the possibility of anesophageal perforation. The diagnosis can be con-f i rmed with an esophagogram, although this test isnot always positive. Esophagoscopy or CT scanning

GOKASLAN AND WALSH : “TRAP DOOR” EXPOSURE OF THE CERVICOTHORACIC JUNCTION 259
following an esophagogram may also demonstratep e rforation. The treatment of a delayed perf o r a t i o nconsists of nasogastric drainage, antibiotics, and re -exploration of the incision. Once found, a defect canbe re p a i re d .
In order to avoid injury to the esophagus, oneshould minimize the use of sharp dissection belowthe level of the superficial cervical fascia. In addition,the longus colli muscles should be freed enoughboth rostrally and caudally that the sharp teeth ofthe self-retaining retractors can be safely placedunder them without being likely to dislodge duringthe pro c e d u re. Also, attention should be paid tomake sure that the esophagus or the other soft tis-sue structures are not protruding into the fieldbetween the retractors during the use of the powerdrill, because the esophagus can sometimes getcaught in the drill burr, resulting in esophageal per-
f o r a t i o n .Occasionally, a displaced graft can perforate the
esophagus, thereby necessitating re - e x p l o r a t i o n .Either replacement or removal of the graft may beindicated, depending upon the need for the graft inmaintaining spinal stability. The esophageal perf o r a-tion should be re p a i red, if possible, and the patientt reated with antibiotics and nasogastric drainage, asdescribed pre v i o u s l y .
ILLUSTRATIVE CASEA 27-year-old white man with a history of renal cellc a rcinoma presented with a 3-month history of pro-g ressively worsening interscapular pain. His neuro-logical examination was unremarkable. MRI re v e a l e da T3 vertebral body metastasis involving primarilythe left pedicle as well as radiographic spinal cord
F i g u re 3. P reoperative MRI of the patient in Figure 2.The patient had already undergone a transpedicularT3 vertebrectomy for metastatic renal cell cancer, fol-lowed by insertion of posterior instrumentation withtitanium rods, hooks, and Wisconsin wires. Sixmonths later, he presented with re c u r rent tumora round the methylmethacrylate construct that wasplaced during the initial pro c e d u re, resulting inmyelopathy. Epidural tumor extended rostrally andcaudally behind the T2 and T4 vertebral bodies.
F i g u re 4. Postoperative MRI of the patient inF i g u re 2 showing the T2 through T4 vertebre c-tomy, the methylmethacrylate construct ex-tending from T1 to T5, and the cervical lockingp l a t e / s c rew fixation. Artifacts visible posteriorto the thecal sac are the result of pre v i o u s l yplaced cervicothoracic instrumentation con-sisting of hooks, rods, and Wisconsin wire s .

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8260
and nerve root compression. The patient underwenta T3-4 laminectomy, a transpedicular T3 vertebre c-tomy, reconstruction with methylmethacrylate, andhad posterior cervicothoracic instrumentation andfusion (C4-T8). Titanium rods, hooks, and Wi s c o n s i nw i res were used initially for posterior fixation. Thepatient did well following surgery and was placed onchemotherapy. He re t u rned 4 months later with leftT3 radiculopathy. MRI (Figure 3) showed re c u r re n ttumor posterior to the methylmethacrylate con-
struct, extending behind the T2 and T4 vertebralbodies. A neurological examination revealed myelop-athy. At this point, the decision was made to pro c e e dwith a “trap door” surgical exposure and to per f o rma T2-4 vertebrectomy and an anterior re c o n s t r u c t i o nwith instrumentation, as described in this chapterand figures. Postoperatively, the patient’s myelopa-thy resolved (Figures 4 and 5). In this patient,s u rgery was followed by local radiation therapy. At 1-year follow-up review, the patient was fully ambula-tory with no symptoms.
F i g u re 5. Postoperative anteroposterior ( l e f t ) and lateral ( r i g h t ) x-rays of the patient inF i g u re 2 showing that anteriorly, the construct consists of methylmethacrylate (whichreplaces the T2-4 vertebral bodies) and a cervical locking plate (with screws) extendingf rom T1 through T5. Also seen is the initially placed posterior cervicothoracic fixationincluding rods, hooks and Wisconsin wire s .

INTRODUCTIONTo appreciate the suture repair of a peripheral nerve,an understanding of the connective tissue layers aswell as the fascicular anatomy of a nerve is impor-tant. As seen in Figure 1, which contains a diagramof the peripheral nerve arc h i t e c t u re and its compo-nents, an external epineurial sheath surrounds eachperipheral nerve and is composed of connective tis-sue and longitudinal blood vessels. There is an exter-nal epineurium and an internal epineurium. Thei n t e rnal epineurium demarcates fascicles and gro u p sof fascicles within the nerve. Each individual fascicleis surrounded by perineurium. The axons are con-tained within fascicles, in close association withSchwann cells and the basement membrane that sur-rounds Schwann cells, the endoneural basal lamina.The proportion of connective tissue within the nervevaries considerably, from 25% to 85%, thro u g h o u tthe cross section of the nerve. In general, there ism o re connective tissue in the nerve where it cro s s e sthe joint. The connective tissue, particularly the peri-neurium, is the source of the main tensile strength tothe nerve. It is also the layer that can take and hold as u t u re. From a practical viewpoint, the smallest com-ponent of nerve that can be re p a i red is the fascicle.
PERIPHERAL NERVE SUTURE TECHNIQUES
RAJIV MIDHA, M.D., M.SC., F.R.C.S.(C)MARGOT MACKAY, A.N.S.C.A., B.SC.A.A.M.
261
Nerves may be generally divided into four basicp a t t e rns of intraneural arc h i t e c t u re, based on theirfascicular structure (Figure 1). Nerves containingone large fascicle are termed “monofascicular,” whilethose containing a few or a discrete number of fasci-cles are “oligofascicular.” Most nerves contain manyfascicles of varying sizes and are termed polyfascicu-l a r. The polyfascicular pattern exists either with fas-cicles grouped together or with a more diffuse (un-g rouped) arrangement throughout the cross sectionof the nerve. The fascicular nature of a nervechanges as it extends from proximal to distal in thee x t remity. For example, the ulnar nerve is polyfascic-ular as it comes off the brachial plexus and thengenerally becomes organized into four fascicles at thelevel of the elbow. These fascicles are further segre-gated into motor and sensory groupings at the levelof the wrist and, finally, the motor branch in thehand is monofascicular.
Following a nerve injury resulting in axotomy, thedistal axon undergoes Wallerian degeneration. At-tempted regeneration from the proximal axon may ormay not be successful, depending primarily on localand certain systemic factors. In the absence of eff e c-tive spontaneous regeneration, repair of the periph-eral nerve is in ord e r. Methods of peripheral nerverepair fall under two basic categories: direct re p a i r( n e u ro r rhaphy), and bridge pro c e d u res in whichautologous nerve grafts are most commonly utilized.The direct or suture repair may be perf o rmed usingan epineurial, a grouped fascicular, a fascicular, orvarious combinations of these methods. © 1999 The American Association of Neurological Surg e o n s

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8262
It must be stressed at the outset that a peripheralnerve repair is not a type of cellular re p a i r, but isactually a repair done at the level of the connectivetissue to coapt a healthy proximal nerve to a healthydistal nerve stump. The appropriate anatomical envi-ronment is then provided, so that axons from thep roximal stump can regenerate into endoneuraltubes within the distal nerve stump and, hence, beled to end organs to re s t o re function. Note that anerve graft functions as a conduit whose axons aredestined to undergo degeneration as soon as it is
removed from its harvest site. Thus, the graft pro-vides an endoneural tube network available to beexploited by regenerating axons from the pro x i m a lhost nerve stump. It also provides viable Schwanncells, as long as the caliber of the nerve graft is nottoo large. For this reason, small-caliber cutaneousnerves are most commonly used as graft material.The small-caliber nerves, when sutured in a series ofparallel segments, are in close proximity to tissuefluid and are there f o re nourished. They also underg orapid revascularization, and thus remain viable.
FASCICULAR PATTERNS IN PERIPHERAL NERVES
PERIPHERAL NERVE COMPOSITION
F i g u re 1. Schematic diagram of peripheral nerve arc h i t e c t u re and composition. The patterns of fasciculars t r u c t u re of peripheral nerve are illustrated: monofascicular, oligofascicular, and polyfascicular (gro u p e dand ungrouped). The anatomical composition, with emphasis on the connective tissue layers of the nerve(i.e., epineurium (external and internal), perineurium, and endoneurium) are illustrated.
monofasicular
oligofascicular
polyfasicular
grouped
ungrouped (diffuse)
external epineurium
internal epineurium
fascicle
perineuriumendoneuriumnerve fiber

MIDHA AND MACKAY : PERIPHERAL NERVE SUTURE TECHNIQUES 263
GENERAL PRINCIPLES OF NERVE EXPLORATION AND REPAIRA detailed knowledge of the gross anatomy of the ex-t remities and peripheral nerves is imperative beforeundertaking nerve exploration and re p a i r. The sur-geon must be pre p a red to expose the nerve well pro x-imal and distal to the area of injury. Appro p r i a t epositioning of the limb, padding of pre s s u re points,and wide draping are essential. Special attention todraping of the limb or a diff e rent limb for pro c u r i n gnerve grafts is also re q u i red. Since the nerve mayneed to be stimulated intraoperatively to evoke mus-cle contractions, only a short-acting paralyzing agent,given at the induction of anesthesia, should be used.The author prefers the use of general anesthesia anddoes not use tourniquets for these pro c e d u res.
The isolation of the nerve itself should be per-f o rmed using sharp dissection. The surgeon identi-fies normal nerve proximal and distal to the zone ofinjury, and then works toward the area of injury. Inclean lacerating injuries, the area of exposure maybe relatively small. However, most injuries leave thenerve in continuity; since these injuries are alsoe x p l o red weeks to months following trauma, there isconsiderable scar formation and distortion of tissue,necessitating a wide exposure. Using sharp dissec-tion techniques, the area of injured nerve is circ u m-f e rentially exposed. With the aid of an operating mi-c roscope, the gross anatomical details of the injurya re identified. As advocated by Kline, intraoperativenerve action potential studies dictate an extern a ln e u rolysis only if evidence of spontaneous re g e n e r a-tion (the presence of a nerve action potential studies)is found (Figure 2). On the other hand, the lack ofevidence of spontaneous regeneration (the absenceof a nerve action potential studies) dictates re s e c t i o nof the neuroma and appropriate re p a i r.
The placement of lateral stay sutures using 6-0monofilament (as illustrated in Figure 2A and B)helps maintain the topographical alignment of thenerve. Under the operating microscope, the surg e o nthen cuts across the center of the neuroma. Smallsegments of the nerve are sliced in perfect cross sec-tion, using a fresh blade, until a healthy fascicularp a t t e rn is identified both at the proximal and at thedistal stump (Figure 2C and D). This step is critical,as attempting to oppose or graft scarred pro x i m a land distal stumps is a major cause of nerve re p a i rf a i l u re. Healthy fascicular tissue is recognized whenthe epineurium retracts slightly and the endoneu-rium appears to “pout” or mushroom out of the fasci-cles (because of positive endoneural pre s s u re). Thistype of adequate debridement invariably leaves somed e g ree of gap between the proximal and the distalstump. If the gap is short and the two ends can beb rought together without undue tension, a dire c trepair is appropriate. One good way to determine the
d e g ree of tension present at the suture line is tobring the ends together using the stay epineurial su-t u res. If this can be perf o rmed without suture dis-traction, a direct repair is appropriate. However, ifthe ends are under considerable tension and thes u t u re line appears to tear out, a graft repair mustbe perf o rmed.
Several techniques are available to bring the pro x-imal and distal stumps closer together and allow ad i rect repair to be perf o rmed. In all situations, pro x i-mal and distal mobilization of the nerve for consider-able distances should be perf o rmed. Thus, tetheringf o rces to adjacent surrounding fascial and subcuta-neous tissue are removed, allowing short gap lengthsto be overcome. In certain situations, such as theulnar nerve at the elbow, the nerve may be trans-posed, allowing a considerable length to be obtained( F i g u re 3). Nerve repairs perf o rmed with a joint inslight flexion (e.g., the elbow joint for upper extre m i t yand the knee joint for lower extremity) may be appro-priate. In these situations, the extremity will need tobe splinted in this position for 2-3 weeks postopera-tively and then gradually mobilized with physiother-apy. Excessive flexion of joints, however, should beavoided. Indeed, most nerve repairs should be per-f o rmed with the extremity in a state of near- m a x i m a lextension, so that postoperative mobilization occurswithout risk of distraction at the suture line. Onecan there f o re avoid prolonged limb immobilization.Under most circumstances for extremity nerve re-pairs, I place bulky dressings (but not splints)a round the incision area and leave in place for 2weeks as a reminder to the patient to avoid excessivemotion. Brachial plexus repairs are protected with ashoulder immobilizer or sling for 3 weeks. There a f t e r,the patient is allowed gradual and pro g ressive rangeof motion supervised by an appropriately instructedphysiotherapist.
DIRECT REPAIR D i rect end-to-end repair is possible in the majority ofclean lacerating injuries and in cases of delayed re-pair when the two ends can be brought togetherwithout tension. The author uses magnification withthe operating microscope (others may prefer loupes)for all repairs. Indispensable tools include micro i n-struments with fine tips (such as jeweler’s forc e p s )and fine-tipped micro s u t u re needle drivers. Com-monly, 8-0, 9-0, or 10-0 monofilament nylon micro-s u t u res are utilized, determined by the caliber of the nerve undergoing re p a i r. In general, 8-0 andm o re rarely 9-0 sutures are utilized for pro x i m a lrepairs such as brachial plexus elements and 10-0 sutures are utilized for more distal repairs andfascicular coaptations. To control bleeding from thenerve ends, minor oozing is often halted by simple

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8264
F i g u re 2.
B
A
D
C

MIDHA AND MACKAY : PERIPHERAL NERVE SUTURE TECHNIQUES 265
F i g u re 2. A and B: s u rgical management of a neuroma in continuity. A , operative photomicrograph illustrating injury to thep e roneal nerve just proximal to the head of the fibula. The superficial peroneal nerve (in the upper part of photograph, encir-cled with the Penrose drain) conducted a nerve action potential and underwent neurolysis. There was no demonstrable evi-dence of regeneration across the deep peroneal branch (no re t u rn of clinical function and absence of a nerve action potentiala c ross the neuroma). The nerve appears attenuated at the site of the neuroma, with 6-0 stay sutures placed proximal anddistal to the neuroma. B , drawing of a neuroma pre p a red for resection and debridement. Stay or lateral stay sutures arepositioned to orient and topographically align the nerve. The site of the initial nerve section is across the middle of the neu-roma (solid line in center). C and D: sectioning technique used to debride the neuroma in continuity until all scarring hasbeen removed and a fresh fascicular pattern is observed at the nerve stump. C, operative photomicrograph demonstratingsequential sectioning of the neuroma under microscopic magnification to obtain a fascicular pattern. D , schematic diagramdemonstrating pro g ressive sectioning until a grossly normal fascicular pattern is observed. (Figure 2C re p roduced courtesyof Dr. Alan Van Beek)
F i g u re 3. Drawing demonstrating techniques available to gain length to allowd i rect repair of nerve ends without tension. An injury gap of the ulnar nerve justdistal to the elbow is used as an example. In addition to slight flexion of the elbowjoint, the ulnar nerve undergoes anterior transposition. These two maneuversrelax the nerve, overcoming the gap, and permit tension-free direct re p a i r.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8266
p re s s u re with cottonoids. However, more substantialbleeding from small epineurial vessels should bec o n t rolled using small amounts of bipolar curre n td e l i v e red via fine-tipped jeweler’s forceps. The use ofa microirrigator for saline flushes enhances visibilityand further aids the perf o rmance of the nerve re p a i r.
D i rect repair techniques include epineurial,g rouped fascicular, and fascicular repairs. The indi-cations and use of each of these techniques are de-scribed here.
Epineurial Repair Epineurial suture repair has been a traditionalmethod of nerve coaptation. These repairs are mosta p p ropriate for monofascicular (e.g., digital) nervesand diffusely grouped polyfascicular (most pro x i m a llimb and plexus element) nerves. Simplistically, thismethod achieves continuity of the connective tissuef rom the proximal to the distal stumps, without ten-sion and with appropriate rotational alignment ofboth stumps. The goal is to obtain good coaptation ofp roximal and distal fascicular anatomy. Fre s h e n i n gof the two nerve ends to debride the nerve and re-
move scar tissue is there f o re critical. Achieving ap-p ropriate nerve alignment can be aided by inspectingfor longitudinal blood vessels in the epineurium aswell as attending to fascicular alignment. The use oflateral stay sutures (Figure 2) also aids this pro c e s s .N e u ro r rhaphy is perf o rmed using 8-0 to 10-0 non-absorbable nylon sutures. A small bite of the inter-nal and external epineurium (being careful to avoidperineurium) is taken from both stumps and thes u t u re is tied using only mild to moderate tension( F i g u re 4). It is critical to avoid tying the knot undertoo great a tension, as this will cause overriding oran accordion effect on the fascicles or, in fact, pout-ing out of a fascicle from the epineurial repair site,thus defeating the purpose of suturing. The two ini-tial sutures are placed 180 degrees apart from eachother (Figure 4). This distance is then divided in halfand two further sutures are positioned. The numberof epineurial sutures re q u i red varies; in the majorityof cases, four to eight sutures suffice for appro x i m a t-ing the proximal and distal stumps in a tension-fre em a n n e r. Excess sutures may result in additionalscarring and are to be avoided.
F i g u re 4. Epineurial suture repair technique. Lateral stay sutures and vascular landmarks are usedto maintain topographic alignment. Sutures are placed with the needle passed through the intern a land external epineurium from both stumps to approximate the nerve ends, until the final repair isachieved (i n s e t).

MIDHA AND MACKAY : PERIPHERAL NERVE SUTURE TECHNIQUES 267
G rouped Fascicular Repair A grouped fascicular repair technique is a potentiallym o re accurate method than epineurial re p a i r. Theo-retically, a disadvantage of epineurial repair is theinability to precisely match the appropriate pro x i m a land distal fascicles. However, experimental and clini-cal studies have not shown a clear advantage of onetechnique over the other. For practical purposes, theg rouped fascicular technique is especially indicatedin situations where an easily identifiable part of thec ross section of the nerve supplies sensory function,while another portion of the nerve supplies motorfunction. More distal extremity nerves, such as theelbow-to-wrist segments of the ulnar and mediannerves, are examples of nerves that merit this type ofre p a i r. Another indication is the nerve injury re q u i r-ing a split re p a i r. In this situation, a portion of thenerve that is clearly regenerating (by clinical andelectrical criteria) is preserved in continuity usinge x t e rnal and internal neurolysis techniques, whilethe groups of fascicles that are clearly neuro t e m e t i c
u n d e rgo re p a i r. As in the epineurial repair method, the nerve ends
a re matched by resecting damaged tissue. Debride-ment is followed by careful analysis, under the oper-ating microscope, of the anatomical cross sectionalappearance of the nerve stump. Using the cross sec-tional appearance, the longitudinal blood supply,and other spatial landmarks (e.g., branching of nervejust proximal and distal to the injury site), the pro x i-mal and distal stumps can be matched. Interf a s c i c u-lar dissection is then perf o rmed within the intern a lepineurium to draw out groups of fascicles (Figure5). Groups of fascicles may vary from two to several,each surrounded by a variable amount of intern a lepineurium, with the external epineurium dissectedaway (Figure 5). Once groups of fascicles are ade-quately matched, 8-0 or 9-0 micro s u t u res are placedt h rough the interfascicular epineurial tissue, avoid-ing perineurium and allowing coaptation of fascicu-lar groups from the proximal to the distal stump( F i g u re 5).
F i g u re 5. G rouped fascicular repair technique. Micro s u t u res are placed through the interf a s c i c u l a repineurial tissue, avoiding perineurium and allowing coaptation of fascicular groups from the pro x i-mal to distal stumps. The sutures are tied using mild to moderate tension, preventing overriding offascicles.

NEUROSURGICAL OPERATIVE ATLAS. VOL. 8268
F i g u re 6. Fascicular re p a i r. A , an acutely lacerated nerve has its fascicular configuration dissected out,with topographical relationships used to align proximal and distal fascicles. B , fine 10-0 nylon micro s u-t u res, placed in the perineurium, are used to coapt individual or groups of two or three fascicles to eacho t h e r. Note that each fascicular repair re q u i res two or, at most, three sutures. (Figure 6B re p ro d u c e dcourtesy of Dr. Jack Tu p p e r )
F i g u re 7. Graft repair of the peripheral nerve. Thei n t e rfascicular technique is used to repair individ-ual graft segments to groups of fascicles from thehost proximal and distal stumps. A , s c h e m a t i cdrawing of interpositional grafts being sutured tothe host nerve. Note that in the graft underg o i n gsuturing, the needle bites of the graft and hoststumps allow widening (or “fishmouthing”) of thec ross sectional area of the graft to allow completecoverage of the host stump. B, operative photo-graph showing the completed repair of posteriortibial nerve injury with four interposed sural nervegrafts. (Figure 7B re p roduced courtesy of Dr. DavidKline and from Dubuisson A, Kline D: N e u rol ClinNorth Am 10:935-951, 1992 with perm i s s i o n )
A B
A
B

MIDHA AND MACKAY : PERIPHERAL NERVE SUTURE TECHNIQUES 269
Fascicular RepairIn rare situations, a specific fascicular repair may beindicated. An example of where this repair would bea p p ropriate is a clean lacerating injury of the medianor ulnar nerve at the wrist, re p a i red primarily whereindividual motor and sensory fascicles can be de-fined. Another example is a partial injury across aportion of the cross section of the nerve. Here, indi-vidual injured fascicles from the proximal and distalstumps may be specifically re p a i red to each other.This repair re q u i res the use of high magnificationand fine 10-0 nylon micro s u t u res swaged on a 75-µmneedle. The suture is placed through the perineuriumof the proximal and distal stumps with careful avoid-ance of the internal endoneural contents (Figure 6).Again, the purpose is to attain tension-free coapta-tion of the proximal and the distal stumps. Tight su-t u re ties should be avoided, as they will result in lat-eral bulging and herniation of endoneural contents.Also, only two or three sutures should be used in thissituation, placed circ u m f e rentially around the nerveat approximately equal distances. The fascicular re-pair can then be strengthened by repairing looseepineurial sutures of the surrounding nerve andg rouped fascicle repairs of the remaining nerve ele-ments. In this sense, many direct nerve repair tech-niques are a combination of epineurial and gro u pfascicular repairs. In the minority of situations, thefascicular repair of a specific nerve component maybe re q u i red. Thus, the surgeon should be adept in allof the techniques described here. The use of a giventechnique or combinations will depend on the specificnerve injury encountered and the underlying specificfascicular pattern.
GRAFT REPAIR The surgical technique of nerve grafting is similar inmany ways to that of direct nerve re p a i r. From a sim-plistic viewpoint, when direct repair cannot be per-f o rmed without undue tension, nerve grafting mustbe undertaken. A corollary to this is that when nervegrafting is perf o rmed, there must be no tension atthe proximal and distal repair sites to prevent post-operative distraction. There f o re, nerve grafting isgenerally perf o rmed with the extremity in full exten-sion. In general, a nerve graft should be about 10%longer than the existing nerve gap. The majority ofautologous nerve grafts are cutaneous nerves of the lower (e.g., sural) and upper extremities. (Donornerves that are available for nerve grafting and meth-ods for procuring these are discussed in the next vol-ume of the atlas.) It is imperative to harvest the max-imum amount of nerve graft material available.When the caliber of the host nerve stump underg o i n g
grafting is the same dimension as the nerve graft, aslightly larger segment than the gap is needed. Fre-quently, the cross sectional area of the host nervestump will be several folds larger than the diameterof the nerve graft. Several segments of nerve graftwill there f o re be needed to allow coverage of thee n t i re cross sectional surface of the host nervestumps. This must be taken into consideration whenharvesting the donor nerve.
The graft repair technique is similar to the variousrepair methods already outlined, with the exceptionthat there are two suture lines. When preparing thep roximal and distal stumps, the interfascicular ande x t e rnal epineurial tissue must be dissected away toallow groups of fascicles (or fingers) to be created ateach stump (Figure 7). The diameter of the group offascicles should approximate that of the cutaneousnerve graft obtained. The nerve graft is then sewn inplace to the proximal group of fascicles, using epineu-rial and interfascicular epineurial techniques (Figure s5 and 7). Sutures, approximately 180 degrees apart,a re positioned and passed through the epineurium ofthe nerve graft and then through the interf a s c i c u l a repineurium of the host stump, spreading the cro s ssection of the graft in a fish-mouth configuration (Fig-u re 7). The end of the graft segment then covers asmuch of the fascicular area of the host nerve stumpas possible, allowing capture of the maximum num-ber of regenerating axons. Typically, two sutures, andoccasionally three or four sutures, are re q u i red foreach nerve graft at each coaptation site. The nervegraft segments are sutured to the distal group of fas-cicles in a similar manner. It is important to re - i n-spect all proximal and distal coaptation sites at thecompletion of the repair to ensure that no graft endsbecame disconnected while others were being su-t u red in place.
As much as possible, the grafts are aligned in ori-entation so that groups of proximal fascicles will bed i rected to appropriate groups of distal fascicles.This allows for the most precise repair possible. Foreach nerve treated, an understanding of the gro s sanatomy and the branching pattern of the nerve, aswell as knowledge of interfascicular anatomy, ishelpful. As Sunderland has shown, the plexiform na-t u re of the more proximal nerve elements, whereg roups of fibers are exchanged among fascicles in alongitudinal manner, defeats exact matching. In gen-eral, when dealing with proximal nerves and nerveelements such as the brachial plexus, spatial align-ment of fascicles allows the best possible matching.In the most distal nerves (e.g., the median and theulnar nerve at the wrist), more precise anatomicalmatching with re g a rd to group fascicular and, occa-sionally, specific fascicular anatomy is possible.