Embed Size (px)
Citation preview
Supplement February 2017
New Advances In Nutrition And Eye Health
Laboratoires Théa Satellite Symposium16th EURETINA Congress
10 September 2016Copenhagen, Denmark
Interest of Early Screening for AMD PreventionGerhard Garhöfer MD, Department of Clinical Pharmacology, Medical University of Vienna, Austria
Early screening makes sense in the context of AMD. AMD is a major global health problem: 1.2 million people in the USA alone suffer from neovascular AMD and
970,000 more have geographic atrophy. More than 8 million people have at least one large drusen – often considered a precursor to full-blown AMD – in one eye, and an estimated 3.6 million people have bilateral large drusen.1
The disease is not just restricted to Europe or the USA. A recent study by Wong et al looking at the prevalence of AMD by geographical region pinpointed Asia as the region that will see the largest projected number of cases of AMD in the future, despite having the lowest estimated prevalence currently.1 With life expectancy increasing in all parts of the world, the projected number of people with AMD is around 196 million in 2020, increasing to 288 million in 2040.
This looming epidemic poses an enormous challenge for global healthcare systems. One particular strategy that may help to reduce the burden of AMD therapy in the future is to use screening in order to identify high-risk patients much earlier in the disease process.
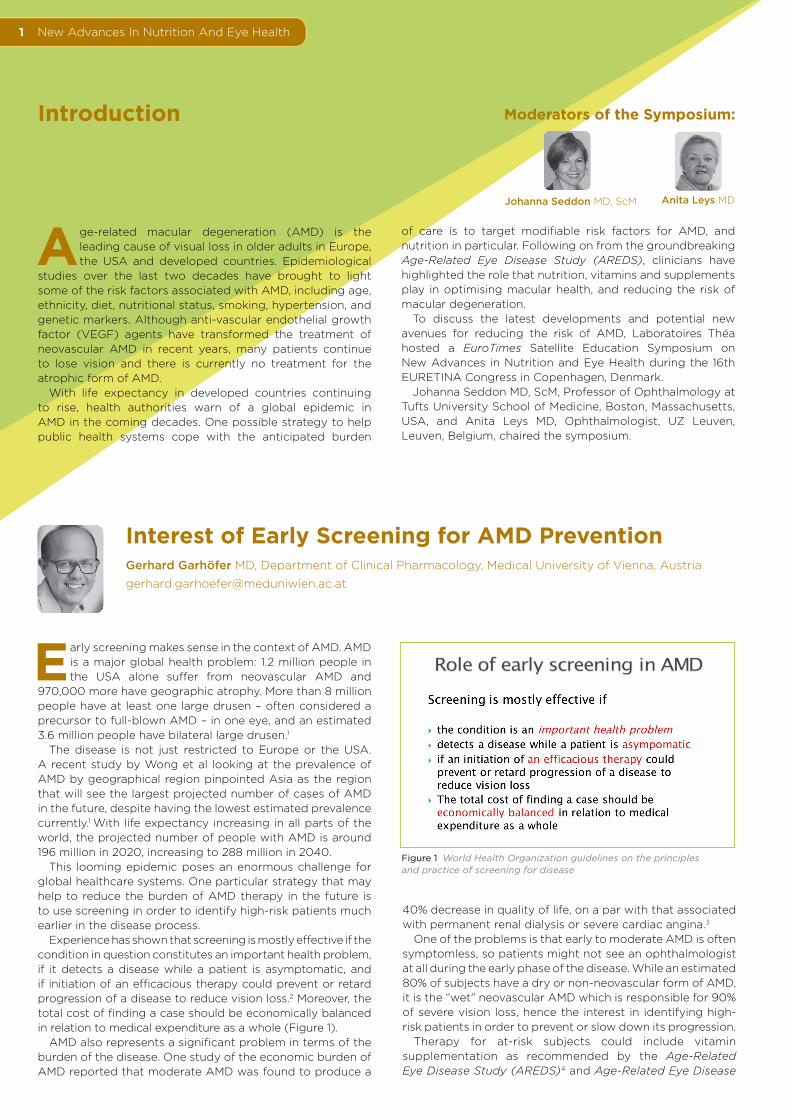
Experience has shown that screening is mostly effective if the condition in question constitutes an important health problem, if it detects a disease while a patient is asymptomatic, and if initiation of an efficacious therapy could prevent or retard progression of a disease to reduce vision loss.2 Moreover, the total cost of finding a case should be economically balanced in relation to medical expenditure as a whole (Figure 1).
AMD also represents a significant problem in terms of the burden of the disease. One study of the economic burden of AMD reported that moderate AMD was found to produce a
New Advances In Nutrition And Eye Health1
Age-related macular degeneration (AMD) is the leading cause of visual loss in older adults in Europe, the USA and developed countries. Epidemiological
studies over the last two decades have brought to light some of the risk factors associated with AMD, including age, ethnicity, diet, nutritional status, smoking, hypertension, and genetic markers. Although anti-vascular endothelial growth factor (VEGF) agents have transformed the treatment of neovascular AMD in recent years, many patients continue to lose vision and there is currently no treatment for the atrophic form of AMD.
With life expectancy in developed countries continuing to rise, health authorities warn of a global epidemic in AMD in the coming decades. One possible strategy to help public health systems cope with the anticipated burden
Introduction
40% decrease in quality of life, on a par with that associated with permanent renal dialysis or severe cardiac angina.3
One of the problems is that early to moderate AMD is often symptomless, so patients might not see an ophthalmologist at all during the early phase of the disease. While an estimated 80% of subjects have a dry or non-neovascular form of AMD, it is the “wet” neovascular AMD which is responsible for 90% of severe vision loss, hence the interest in identifying high-risk patients in order to prevent or slow down its progression.
Therapy for at-risk subjects could include vitamin supplementation as recommended by the Age-Related Eye Disease Study (AREDS)4 and Age-Related Eye Disease
of care is to target modifiable risk factors for AMD, and nutrition in particular. Following on from the groundbreaking Age-Related Eye Disease Study (AREDS), clinicians have highlighted the role that nutrition, vitamins and supplements play in optimising macular health, and reducing the risk of macular degeneration.
To discuss the latest developments and potential new avenues for reducing the risk of AMD, Laboratoires Théa hosted a EuroTimes Satellite Education Symposium on New Advances in Nutrition and Eye Health during the 16th EURETINA Congress in Copenhagen, Denmark.
Johanna Seddon MD, ScM, Professor of Ophthalmology at Tufts University School of Medicine, Boston, Massachusetts, USA, and Anita Leys MD, Ophthalmologist, UZ Leuven, Leuven, Belgium, chaired the symposium.
Moderators of the Symposium:
Johanna Seddon MD, ScM Anita Leys MD
Figure 1 World Health Organization guidelines on the principles and practice of screening for disease

New Advances In Nutrition And Eye Health 2
Study 2 (AREDS2).5 Data from the first AREDS study showed a clear benefit in administering a mixture of antioxidant vitamins and mineral supplements in terms of progression of AMD. The formulation given in AREDS to patients included vitamin C, vitamin E, beta-carotene, zinc and copper, which reduced the risk of progression to late AMD in high-risk patients by up to 25%.
The public health impact of this 25% reduction is significant. Several studies have looked at this issue and concluded that it is very cost effective, with potential savings in the billions
of dollars if the 25% reduction in the AREDS study is attained (Figure 2).6,7 The notable success of the AREDS studies opened the path for investigation into the potential of other minerals and supplements such as lutein and zeaxanthin, docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA), resveratrol and vitamin D in the prevention of AMD.
REFERENCES1 Wong, Wan Ling et al, Global prevalence of age-related macular
degeneration and disease burden projection for 2020 and 2040L a systematic review and meta-analysis. The Lancet Global Health, Vol. 2, Issue 2, e106-e116.
2 Chew, EY, Schachat AP, Should we add screening of age-related macular degeneration to current screening programs for diabetic retinopathy? Ophthalmology. 2015 Dec; 122 (12): 2490-6.
3 Brown, MM et al. Age-related macular degeneration: economic burden and value-based medicine analysis. Can J Ophthalmol. 2005 Jun; 40(3): 277-87.
4 The Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of highdose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss. AREDS report no. 8. Arch Ophthalmol 2001;119:1417–36.
5 Age-Related Eye Disease Study 2 Research Group. Lutein þ zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013;309: 2005–15.
6 Age-Related Eye Disease Study Research Group. Potential public health impact of age-related eye disease results. AREDS report no. 11. Arch Ophthalmol 2003;121:1621–4.
7 Gupta OP, Brown GC, Brown MM. Age-related macular degeneration: the costs to society and the patient. Curr Opin Ophthalmol 2007;18:201–5.
STARS: A Validated Score to Screen Patients at Risk of AMDCécile Delcourt MD, University Hospital Bordeaux, France
The past 20 years have seen many risk factors identified for AMD. Strong and consistent associations include age and ethnicity, with a higher incidence in people
of European and Asian origin compared to those of African descent. Smoking and genetic factors are also important, with more than 50 identified polymorphisms now linked to the risk for AMD. Finally, low dietary intakes in key nutrients such as antioxidants, lutein and zeaxanthin, and omega 3 fatty acids have been associated with an increased risk of AMD in many observational studies.1, 2
Other risk factors for AMD with moderate and consistent associations include higher body mass index (BMI), history of cardiovascular disease, hypertension, and also some ocular factors such as hyperopia and cataract surgery. Risk factors with weaker associations and inconsistent associations include gender, diabetes, iris colour, history of stroke, and plasma lipid levels.3
There is a need for better prediction models for AMD. Some current models are based on available risk scores that include genetic single-nucleotide polymorphisms (SNPs), which are not yet readily available to ophthalmologists and patients. On the contrary, available risk scores include only limited information on environmental factors, usually age, smoking and BMI. Furthermore, the risk scores have been developed on the basis of limited datasets (AREDS, three population-based studies and two clinical studies),4, 5, 6 so there is still
some room for alternative, and hopefully more accurate, prediction models.
With this in mind, the STARS (Simplified Théa AMD Risk-Assessment Scale) questionnaire was elaborated in order to develop a simple risk score based on a self-completed 13-item questionnaire for large-scale detection of patients at risk of AMD (Figure 1).
The questionnaire focused on a more comprehensive inclusion of environmental risk factors taking account of cardiovascular disease, s o c i o - d e m o g r a p h i c characteristics, family history of AMD, and systemic and ocular risk factors.
The questionnaire is very simple and takes only a few minutes to complete, a self-completed questionnaire
Figure 2 Frost & Sullivan’s Report: Smart Prevention— Health Care Cost Savings Resulting from the Targeted Use of Dietary Supplements 2013
Figure 1
New Advances In Nutrition And Eye Health
Resveratrol and Regulation of AutophagyKai Kaarniranta MD, PhD, University of Eastern Finland, Kuopio University Hospital, Finland
AMD is a multifactorial disease with many environmental, lifestyle and genetic factors. It is also a very complex disease in terms of understanding the key role
that inflammation plays in the pathogenesis of AMD. In the human body, the inflammatory process induces oxidative stress and reduces cellular antioxidant capacity, contributing to the development of age-related diseases such as AMD. Furthermore, the deposition of abnormal aggregated proteins is highly associated with oxidative stress and directly implicated in the senescence of retinal pigment epithelial (RPE) cells, believed to play a central role in the aetiology of AMD.
Chronic oxidative stress and the presence of chronic inflammation has been shown to decrease the ability of RPE cells to remove damaged or non-functional proteins via the lysosomal clearance system, including autophagy. There is growing evidence that autophagy, a key process in the maintenance of cellular homeostasis that serves to remove dysfunctional organelles and proteins, makes a significant contribution to lipofuscin accumulation in the RPE cells and thus the pathogenesis of AMD.
As our understanding of the role of autophagy in age-related diseases has increased in recent years, so interest has grown in the potential of using naturally-derived compounds to counteract oxidative stress and halt the development
3
filled out by the patient. The second part comprising a fundus examination is filled out by the ophthalmologist.
The questionnaire’s feasibility and relevance were first assessed in an Italian nationwide study, in which 127 ophthalmologists invited all their patients over 55 years of age to complete the questionnaire during a one-week period. A total of 12,639 subjects were included in the Italian study. This was followed by a validation study in France, which included 6,837 patients at 80 different ophthalmic centres between March 2013 and March 2014.
Using the questionnaire enables ophthalmologists to allocate a final risk score which is very easy to calculate. All of the risk factors, with the exception of iris colour, were found to be statistically significant and contribute to the final score.
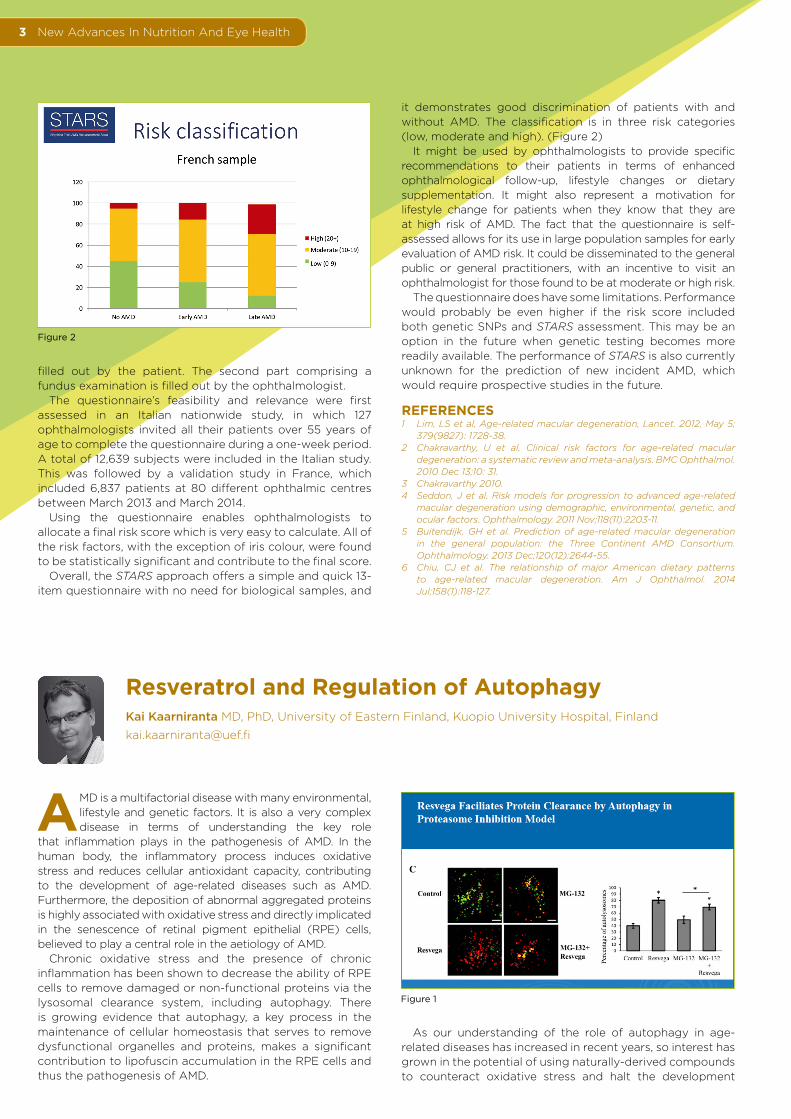
Overall, the STARS approach offers a simple and quick 13-item questionnaire with no need for biological samples, and
it demonstrates good discrimination of patients with and without AMD. The classification is in three risk categories (low, moderate and high). (Figure 2)
It might be used by ophthalmologists to provide specific recommendations to their patients in terms of enhanced ophthalmological follow-up, lifestyle changes or dietary supplementation. It might also represent a motivation for lifestyle change for patients when they know that they are at high risk of AMD. The fact that the questionnaire is self-assessed allows for its use in large population samples for early evaluation of AMD risk. It could be disseminated to the general public or general practitioners, with an incentive to visit an ophthalmologist for those found to be at moderate or high risk.
The questionnaire does have some limitations. Performance would probably be even higher if the risk score included both genetic SNPs and STARS assessment. This may be an option in the future when genetic testing becomes more readily available. The performance of STARS is also currently unknown for the prediction of new incident AMD, which would require prospective studies in the future.
REFERENCES1 Lim, LS et al, Age-related macular degeneration, Lancet. 2012, May 5;
379(9827): 1728-38.2 Chakravarthy, U et al, Clinical risk factors for age-related macular
degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010 Dec 13;10: 31.
3 Chakravarthy 2010.4 Seddon, J et al. Risk models for progression to advanced age-related
macular degeneration using demographic, environmental, genetic, and ocular factors. Ophthalmology. 2011 Nov;118(11):2203-11.
5 Buitendijk, GH et al. Prediction of age-related macular degeneration in the general population: the Three Continent AMD Consortium. Ophthalmology. 2013 Dec;120(12):2644-55.
6 Chiu, CJ et al. The relationship of major American dietary patterns to age-related macular degeneration. Am J Ophthalmol. 2014 Jul;158(1):118-127.
Figure 2
Figure 1

New Advances In Nutrition And Eye Health 4
Going forward, it is clear that nutrient supplementation will remain part of the therapeutic spectrum against AMD
of disease.1,2 A lot of research has focused on stilbene compounds, natural compounds found in a number of plant families, known for their ability to decrease oxidative stress and ameliorate oxidative stress-related diseases.3,4,5
One such compound, resveratrol, a natural polyphenolic compound found mainly in grapes, peanuts, and berries, has received particular scientific attention due its potential health benefits. In the context of AMD, resveratrol was shown in one recent study to have produced long-term beneficial effects on retinal structure and visual function in human patients.6 Resveratrol also protected RPE cell lines from UV-induced oxidative stress, suppressed VEGF expression in human RPE cells and, together with omega-3 fatty acids, prevented the development of AMD in a mouse model.7,8,9
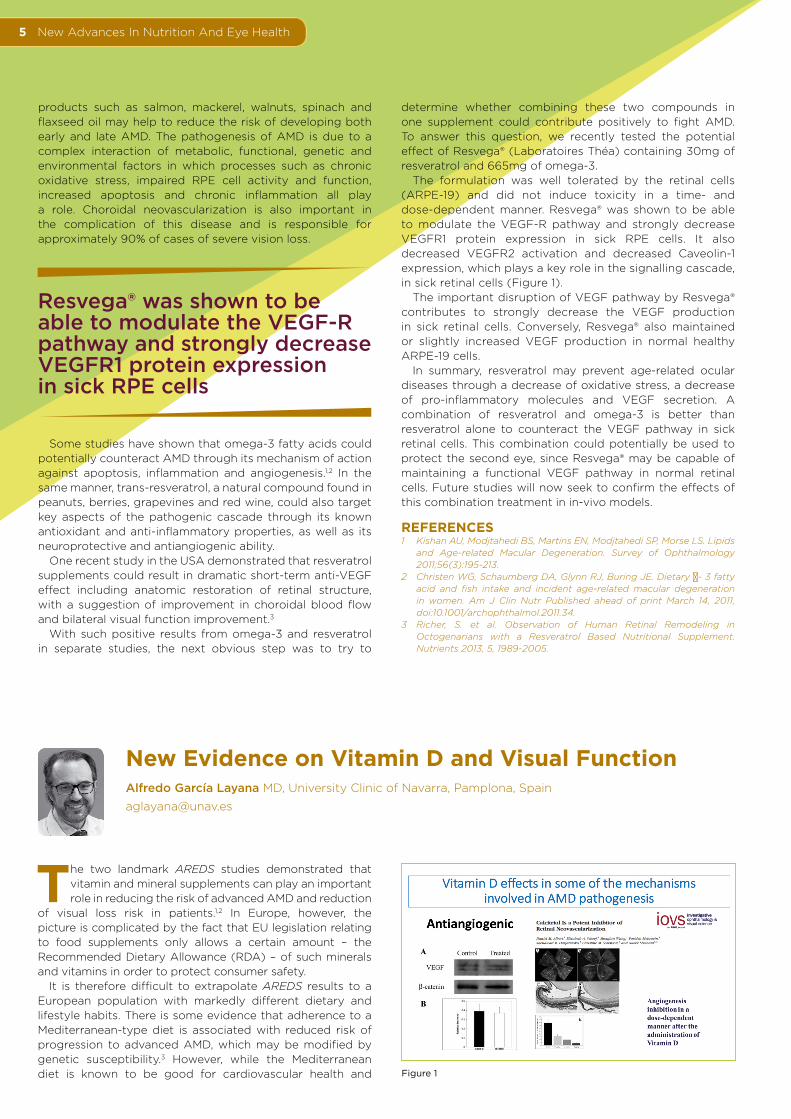
To investigate the potential of resveratrol to potentially combat AMD, our laboratory recently carried out a study using Resvega®, a commercial product formulated by Laboratoires Théa. In this work, ARPE-19 cells were treated with 288ng of Resvega®, containing 30mg of trans-resveratrol and 665mg of omega-3 fatty acids, among other nutrients, with proteasome inhibitor MG-132 or autophagy inhibitor bafilomycin A1 for up to 48 hours.
Analysis of the autophagy markers p62/SQSTM1 (p62) and LC3 showed that Resvega® induced autophagy by showing increased autolysosome formation and autophagy flux, and the change in the p62 and LC3 protein levels
further confirmed the fluorescent microscopy results. Moreover, Resvega® provided a clear cytoprotection under proteasome inhibition. These findings highlight the potential of nutraceuticals containing resveratrol, omega-3 fatty acids and other nutrients in the prevention of ARPE-19 cell damage (Figure 1).
Going forward, it is clear that nutrient supplementation will remain part of the therapeutic spectrum against AMD. Resvega® has the potential to protect RPE cells from oxidative stress and reduce neovascularization in the eye, and it merits further study in the prevention and treatment of AMD.
REFERENCES1 Rhone M., Basu A. Phytochemicals and age-related eye diseases. Nutr.
Rev. 2008;66:465–472.2 Chuang S.Y., Lin C.H., Fang J.Y. Natural compounds and aging: Between
autophagy and inflammasome. Biomed. Res. Int. 2014;2014.3 Petrovski G., Gurusamy N., Das D.K. Resveratrol in cardiovascular
health and disease. Ann. N. Y. Acad. Sci. 2011;1215:22–33.4 Koskela A., Reinisalo M., Hyttinen J.M., Kaarniranta K., Karjalainen R.O.
Pinosylvin-mediated protection against oxidative stress in human retinal pigment epithelial cells. Mol. Vis. 2014;20:760–769.
5 Reinisalo M., Kårlund A., Koskela A., Kaarniranta K., Karjalainen R.O. Polyphenol stilbenes: Molecular mechanisms of defence against oxidative stress and aging-related diseases. Oxid. Med. Cell. Longev. 2015.
6 Richer S., Patel S., Sockanathan S., Ulanski L.J., 2nd, Miller L., Pdella C. Resveratrol based oral nutritional supplement produces long-term beneficial effects on structure and visual function in human patients. Nutrients. 2014;6:4404–4420.
7 Chan C.M., Huang C.H., Li H.J., Hsiao C.Y., Su C.C., Lee P.L., Hung C.F. Protective effects of resveratrol against UVA damage in ARPE-19 cells. Int. J. Mol. Sci. 2015;16:5789–5802.
8 Nagineni C.N., Raju R., Nagineni K.K., Kommineni V.K., Cherukuri A., Kutty R.K., Hooks J.J., Detrick B. Resveratrol suppresses expression of VEGF by human retinal retinal pigment epithelial cells: Potential nutraceutical for age-related macular degeneration. Aging Dis. 2014;5:88–100.
9 Ivanescu A.A., Fernández-Robredo P., Heras-Mulero H., Sádaba-Echarri L.M., García-García L., Fernández-García V., Moreno-Orduna M., Redondo-Exposito A., Recalde S., García-Layana A. Modifying choroidal neovascularization development with a nutritional supplement in mice. Nutrients. 2015;7:5423–5442.
Resveratrol and Omega-3: A Synergetic Action in AMDDominique Delmas PhD, University of Burgundy, INSERM Research Center U866, Dijon, France
Numerous immunological studies have suggested that various environmental factors such as metabolic disease or air pollution contribute to increased risk of
cardiovascular diseases, diabetes, cancer and AMD. On the contrary, eating a well-balanced diet of green vegetables, fibre, fruit, fatty acids and food micro-components rich in antioxidants and omega-3 fatty acids could help to reduce the risk of these pathologies and extend lifespan.
Since many of these environmental factors also increase the risk of ocular diseases such as diabetic retinopathy, glaucoma and AMD, it stands to reason that vitamins, polyunsaturated fatty acids or food micro-components could be used as a supplement to counteract these ocular diseases through their antioxidant properties.
In the case of AMD in particular, studies have shown that polyunsaturated fatty acids found in various natural Figure 1
New Advances In Nutrition And Eye Health
New Evidence on Vitamin D and Visual FunctionAlfredo García Layana MD, University Clinic of Navarra, Pamplona, Spain
The two landmark AREDS studies demonstrated that vitamin and mineral supplements can play an important role in reducing the risk of advanced AMD and reduction
of visual loss risk in patients.1,2 In Europe, however, the picture is complicated by the fact that EU legislation relating to food supplements only allows a certain amount – the Recommended Dietary Allowance (RDA) – of such minerals and vitamins in order to protect consumer safety.
It is therefore difficult to extrapolate AREDS results to a European population with markedly different dietary and lifestyle habits. There is some evidence that adherence to a Mediterranean-type diet is associated with reduced risk of progression to advanced AMD, which may be modified by genetic susceptibility.3 However, while the Mediterranean diet is known to be good for cardiovascular health and
5
determine whether combining these two compounds in one supplement could contribute positively to fight AMD. To answer this question, we recently tested the potential effect of Resvega® (Laboratoires Théa) containing 30mg of resveratrol and 665mg of omega-3.
The formulation was well tolerated by the retinal cells (ARPE-19) and did not induce toxicity in a time- and dose-dependent manner. Resvega® was shown to be able to modulate the VEGF-R pathway and strongly decrease VEGFR1 protein expression in sick RPE cells. It also decreased VEGFR2 activation and decreased Caveolin-1 expression, which plays a key role in the signalling cascade, in sick retinal cells (Figure 1).
The important disruption of VEGF pathway by Resvega® contributes to strongly decrease the VEGF production in sick retinal cells. Conversely, Resvega® also maintained or slightly increased VEGF production in normal healthy ARPE-19 cells.
In summary, resveratrol may prevent age-related ocular diseases through a decrease of oxidative stress, a decrease of pro-inflammatory molecules and VEGF secretion. A combination of resveratrol and omega-3 is better than resveratrol alone to counteract the VEGF pathway in sick retinal cells. This combination could potentially be used to protect the second eye, since Resvega® may be capable of maintaining a functional VEGF pathway in normal retinal cells. Future studies will now seek to confirm the effects of this combination treatment in in-vivo models.
REFERENCES1 Kishan AU, Modjtahedi BS, Martins EN, Modjtahedi SP, Morse LS. Lipids
and Age-related Macular Degeneration. Survey of Ophthalmology 2011;56(3):195-213.
2 Christen WG, Schaumberg DA, Glynn RJ, Buring JE. Dietary ω- 3 fatty acid and fish intake and incident age-related macular degeneration in women. Am J Clin Nutr Published ahead of print March 14, 2011, doi:10.1001/archophthalmol.2011.34.
3 Richer, S. et al. Observation of Human Retinal Remodeling in Octogenarians with a Resveratrol Based Nutritional Supplement. Nutrients 2013, 5, 1989-2005.
products such as salmon, mackerel, walnuts, spinach and flaxseed oil may help to reduce the risk of developing both early and late AMD. The pathogenesis of AMD is due to a complex interaction of metabolic, functional, genetic and environmental factors in which processes such as chronic oxidative stress, impaired RPE cell activity and function, increased apoptosis and chronic inflammation all play a role. Choroidal neovascularization is also important in the complication of this disease and is responsible for approximately 90% of cases of severe vision loss.
Some studies have shown that omega-3 fatty acids could potentially counteract AMD through its mechanism of action against apoptosis, inflammation and angiogenesis.1,2 In the same manner, trans-resveratrol, a natural compound found in peanuts, berries, grapevines and red wine, could also target key aspects of the pathogenic cascade through its known antioxidant and anti-inflammatory properties, as well as its neuroprotective and antiangiogenic ability.
One recent study in the USA demonstrated that resveratrol supplements could result in dramatic short-term anti-VEGF effect including anatomic restoration of retinal structure, with a suggestion of improvement in choroidal blood flow and bilateral visual function improvement.3
With such positive results from omega-3 and resveratrol in separate studies, the next obvious step was to try to
Resvega® was shown to be able to modulate the VEGF-R pathway and strongly decrease VEGFR1 protein expression in sick RPE cells
Figure 1

New Advances In Nutrition And Eye Health
protective against diabetes, is it sufficient to protect against AMD (which is not a deficiency disease)?
This is where vitamin D supplementation may play a potentially important role. While reported estimates of vitamin D status within different European countries show large variation, it is apparent that levels are frequently below recommended ranges, particularly among older populations.
Several studies in recent years have explored the association between vitamin D and visual function. There is, for instance, emerging evidence of a link between vitamin D and myopia.4,5,6 Vitamin D may also have a role to play in immune regulation and barrier function in ocular barrier epithelial cells, with recent research by Alsalem et al demonstrating that ocular cells can convert inactive vitamin D to the active form.7
Macular thickness may also change according to serum vitamin D concentration in older patients.8 Vitamin D may also suppress the cascade of inflammation that occurs at RPE-choroid, with significant reductions in the number of markers of inflammation in the subretinal space following vitamin D administration in aged mice.9 In another recent study, Pahl et al postulated that a sufficient vitamin D supply – especially for elderly people – could be an efficient way to prevent AMD development and progression.10
Vitamin D also affects some of the key mechanisms involved in AMD pathogenesis, including angiogenesis, fibrosis and inflammation (Figure 1). A study by Albert et al found that vitamin D is a potent inhibitor of retinal neovascularization and may be of benefit in the treatment of a variety of eye diseases with a neovascular component.11 It has also been shown to have potent anti-inflammatory and anti-fibrotic properties as well.12,13
It is evident that vitamin D has a more relevant role in the retina than previously thought, and has several protective effects in some of the mechanisms involved in AMD pathogenesis. On this basis, additional studies concerning the role of new relevant micronutrients such as vitamin D in addition to other RDA vitamin and mineral doses are recommended.
6
...more than 50% of the world’s population is at risk for vitamin D deficiency...
REFERENCES1 The Age-Related Eye Disease Study Research Group. A randomized,
placebo-controlled, clinical trial of highdose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss. AREDS report no. 8. Arch Ophthalmol 2001;119:1417–36.
2 Age-Related Eye Disease Study 2 Research Group. Lutein þ zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013;309: 2005–15.
3 Merle, BM et al. Adherence to a Mediterranean diet, genetic susceptibility, and progression to advanced macular degeneration: a prospective cohort study. Am J Clin Nutr. 2015 Nov; 102(5):1196-206.
4 Tideman JW, Polling JR, Voortman T, Jaddoe VW, Uitterlinden AG, Hofman A, Vingerling JR, Franco OH, Klaver CC. Low serum vitamin D is associated with axial length and risk of myopia in young children. Eur J Epidemiol. 2016 May;31(5):491-9.
5 Mutti, DO. Vitamin D may reduce the prevalence of myopia in Korean adolescents. Invest Ophthalmol Vis Sci. 2014 Apr 3;55(4):2048.
6 Guggenheim JA, Williams C, Northstone K, Howe LD, Tilling K, St Pourcain B, McMahon G, Lawlor DA. Does vitamin D mediate the protective effects of time outdoors on myopia? Findings from a prospective birth cohort. Invest Ophthalmol Vis Sci. 2014 Nov 18;55(12):8550-8.
7 Alsalem, JA. Characterization of vitamin D production by human ocular barrier cells. Invest Ophthalmol Vis Sci. 2014 Apr 7;55(4):2140-7.
8 Graffe, A. et al. Vitamin D and macular thickness in the elderly: an optical coherence tomography study. Invest Ophthalmol Vis Sci. 2014 Jul 15;55(8):5298-303.
9 Lee, V. et al. Vitamin D rejuvenates aging eyes by reducing inflammation, clearing amyloid beta and improving visual function. Neurobiol Aging. 2012 Oct;33(10):2382-9.
10 Pahl, L. et al. 1,25-Dihydroxyvitamin D decreases HTRA1 promoter activity in the rhesus monkey--a plausible explanation for the influence of vitamin D on age-related macular degeneration? Exp Eye Res. 2013 Nov;116:234-9.
11 Albert, D. et al. Calcitriol is a potent inhibitor of retinal neovascularization. Invest Ophthalmol Vis Sci. 2007 May;48(5):2327-34.
12 Calton, E. et al. The Impact of Vitamin D Levels on Inflammatory Status: A Systematic Review of Immune Cell Studies. PLoS One. 2015 Nov 3;10(11:e0141770.
13 Ramirez, AM. et al. Vitamin D inhibition of pro-fibrotic effects of transforming growth factor beta1 in lung fibroblasts and epithelial cells. J Steroid Biochem Mol Biol. 2010 Feb 15;118(3):142-50.
Is There Vitamin D Deficiency in AMD Patients?Isabelle Aknin MD, Golfe-Juan and Cannes, France
The pathogenesis of AMD involves a complex interaction of genetic predisposition, oxidative stress, light damage and inflammation, among other factors.
The landmark AREDS studies1,2 demonstrated that nutritional antioxidants and minerals such as carotenoid, zinc, copper, vitamin E and vitamin C can all play a protective role against the development of AMD.
Given that nutrition is now an accepted part of the therapeutic arsenal against AMD, it makes sense that vitamin D, because of its role in combating inflammation, neovascularization and fibrosis, might be the next candidate to add to our list of supplements.
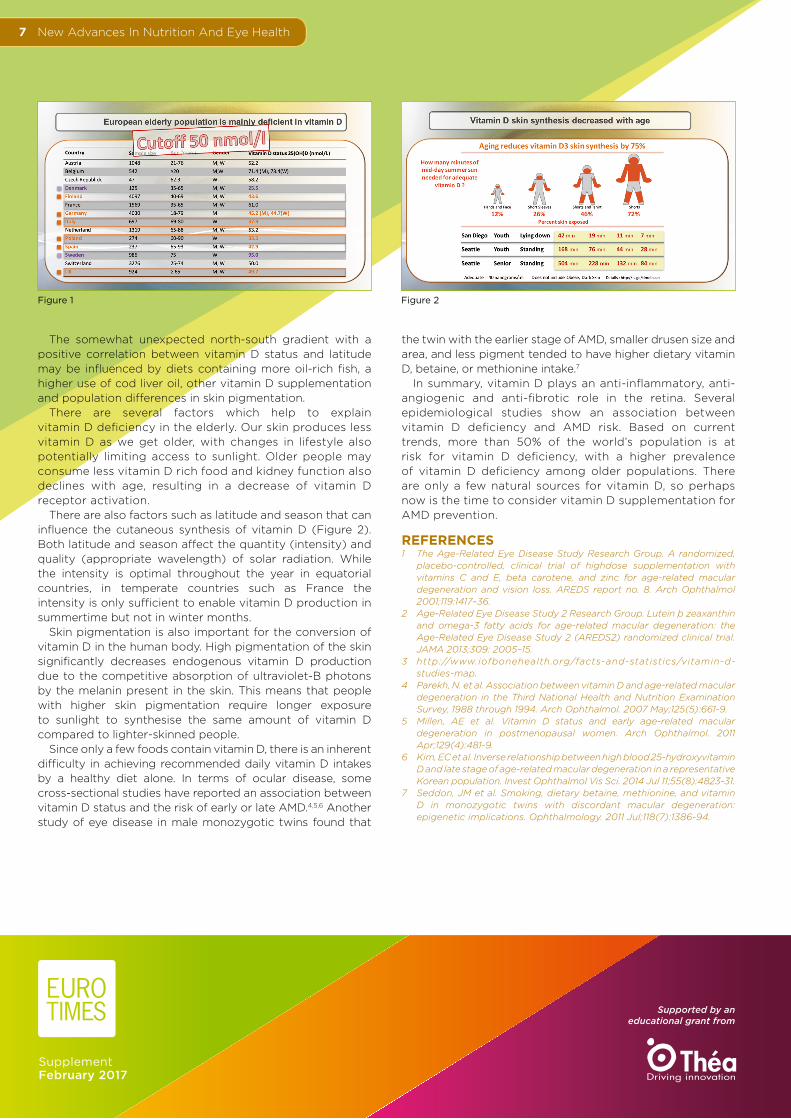
The European elderly population is primarily deficient in vitamin D, as shown in a map of worldwide representation of vitamin D serum concentration status drawn up by the International
Osteoporosis Foundation and DSM Nutritional Products (DSM).3 The map, based on a systemic review of worldwide literature published between 1990 and 2011, confirmed a north-south gradient in Europe with some Scandinavian countries surprisingly showing higher values for vitamin D than southern European countries such as Spain and Italy (Figure 1).
New Advances In Nutrition And Eye Health7
The somewhat unexpected north-south gradient with a positive correlation between vitamin D status and latitude may be influenced by diets containing more oil-rich fish, a higher use of cod liver oil, other vitamin D supplementation and population differences in skin pigmentation.
There are several factors which help to explain vitamin D deficiency in the elderly. Our skin produces less vitamin D as we get older, with changes in lifestyle also potentially limiting access to sunlight. Older people may consume less vitamin D rich food and kidney function also declines with age, resulting in a decrease of vitamin D receptor activation.
There are also factors such as latitude and season that can influence the cutaneous synthesis of vitamin D (Figure 2). Both latitude and season affect the quantity (intensity) and quality (appropriate wavelength) of solar radiation. While the intensity is optimal throughout the year in equatorial countries, in temperate countries such as France the intensity is only sufficient to enable vitamin D production in summertime but not in winter months.
Skin pigmentation is also important for the conversion of vitamin D in the human body. High pigmentation of the skin significantly decreases endogenous vitamin D production due to the competitive absorption of ultraviolet-B photons by the melanin present in the skin. This means that people with higher skin pigmentation require longer exposure to sunlight to synthesise the same amount of vitamin D compared to lighter-skinned people.
Since only a few foods contain vitamin D, there is an inherent difficulty in achieving recommended daily vitamin D intakes by a healthy diet alone. In terms of ocular disease, some cross-sectional studies have reported an association between vitamin D status and the risk of early or late AMD.4,5,6 Another study of eye disease in male monozygotic twins found that
the twin with the earlier stage of AMD, smaller drusen size and area, and less pigment tended to have higher dietary vitamin D, betaine, or methionine intake.7
In summary, vitamin D plays an anti-inflammatory, anti-angiogenic and anti-fibrotic role in the retina. Several epidemiological studies show an association between vitamin D deficiency and AMD risk. Based on current trends, more than 50% of the world’s population is at risk for vitamin D deficiency, with a higher prevalence of vitamin D deficiency among older populations. There are only a few natural sources for vitamin D, so perhaps now is the time to consider vitamin D supplementation for AMD prevention.
REFERENCES1 The Age-Related Eye Disease Study Research Group. A randomized,
placebo-controlled, clinical trial of highdose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss. AREDS report no. 8. Arch Ophthalmol 2001;119:1417–36.
2 Age-Related Eye Disease Study 2 Research Group. Lutein þ zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013;309: 2005–15.
3 http://www.iofbonehealth.org/facts-and-statistics/vitamin-d-studies-map.
4 Parekh, N. et al. Association between vitamin D and age-related macular degeneration in the Third National Health and Nutrition Examination Survey, 1988 through 1994. Arch Ophthalmol. 2007 May;125(5):661-9.
5 Millen, AE et al. Vitamin D status and early age-related macular degeneration in postmenopausal women. Arch Ophthalmol. 2011 Apr;129(4):481-9.
6 Kim, EC et al. Inverse relationship between high blood 25-hydroxyvitamin D and late stage of age-related macular degeneration in a representative Korean population. Invest Ophthalmol Vis Sci. 2014 Jul 11;55(8):4823-31.
7 Seddon, JM et al. Smoking, dietary betaine, methionine, and vitamin D in monozygotic twins with discordant macular degeneration: epigenetic implications. Ophthalmology. 2011 Jul;118(7):1386-94.
Supplement February 2017
Supported by an educational grant from
Figure 1 Figure 2