Embed Size (px)
Citation preview
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1480
New Biomarkers forNeuromuscular Function andMyasthenia Gravis
CARL JOHAN MOLIN
ISSN 1651-6206ISBN 978-91-513-0390-1urn:nbn:se:uu:diva-356116

Dissertation presented at Uppsala University to be publicly examined in Auditorium Minus,Gustavianum, Akademigatan 3, Uppsala, Friday, 21 September 2018 at 13:00 for thedegree of Doctor of Philosophy (Faculty of Medicine). The examination will be conductedin English. Faculty examiner: Professor Jan Verschuuren (Department of Neurology, LeidenUniversity Medical Center).
AbstractMolin, C. J. 2018. New Biomarkers for Neuromuscular Function and Myasthenia Gravis.Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine1480. 84 pp. Uppsala: Acta Universitatis Upsaliensis. ISBN 978-91-513-0390-1.
Myasthenia gravis (MG) is an autoimmune disorder, which is caused by autoantibodies againstthe acetylcholine receptor (AChR). The cardinal symptom is muscle fatigue, which can rangefrom slight weakness of the extraocular muscles (causing droopy eyelids or double vision),to paralysis of the respiratory muscles. Antibodies towards other muscle proteins have beendiscovered, and MG is now considered a very heterogeneous disease with several subgroups.The severity of symptoms in MG patients is often fluctuating, and the antibody titers do notcorrelate with disease severity or treatment response. Therefore, there is a great need for reliablebiomarkers in MG, both for assessing neuromuscular function, but also for clinical aspects suchas disease progression and subgrouping.
In Study I, the use of compound motor action potential (CMAP) as a biomarker for musclestatus was examined in trained and untrained individuals. We found that trained individualshave a higher CMAP in proximal muscles, and the CMAP value in the biceps correlate withmuscle strength in these individuals, indicating that CMAP can be used as a biomarker formuscle function. In Study II, subjects from study I were examined with ultrasound to assess theeffect of high-resistance strength training (HRST) on peripheral nerves, and to compare musclethickness. We did not find a difference in nerve cross-sectional area between the two groups.Trained individuals had thicker biceps muscles. The results from study I and II has led to CMAPand ultrasound being used to evaluate the result of physical exercise as an intervention in MGpatients.
In Study III, the expression of inflammatory proteins in the sera of MG patients wascompared to healthy controls, in search for possible biomarkers. We found eleven proteins tobe elevated, which provide new insight to the inflammatory response in MG and have possiblefunctions as new biomarkers of inflammatory activity.
In Study IV, the effect of thymectomy on the potential microRNA MG biomarkersmiR-150-5p and miR-21-5p was examined. A decrease in miR-150-5p was seen 24 months afterthymectomy, which further validate the use of miR-150-5p as a disease-specific biomarker forclinical outcome in AChR positive MG patients.
Keywords: Biomarkers, myasthenia gravis, neuromuscular function, neurophysiology
Carl Johan Molin, Department of Neuroscience, Clinical Neurophysiology, Akademiskasjukhuset, Uppsala University, SE-75185 Uppsala, Sweden.
© Carl Johan Molin 2018
ISSN 1651-6206ISBN 978-91-513-0390-1urn:nbn:se:uu:diva-356116 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-356116)

To my family

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Molin, C.J. & Punga, A.R. (2016) Compound Motor Action Poten-tial: Electrophysiological Marker for Muscle Training. J Clin Neu-rophysiol, 33(4), 340-345.
II Molin, C.J., Widenfalk, J. & Punga, A.R. (2017) High-resistance strength training does not affect nerve cross sectional area - An ul-trasound study. Clinical Neurophysiology Practice 2, 163-169.
III Molin, C.J.*, Westerberg, E.* & Punga, A.R. (2017) Profile of up-regulated inflammatory proteins in sera of Myasthenia Gravis pa-tients. Sci Rep, 7, 39716.
IV Molin, C.J., Sabre, L., Weis, C.-A., Punga, T. & Punga, A. R. (2018) Thymectomy lowers the myasthenia gravis biomarker miR-150-5p. Neurology - Neuroimmunology Neuroinflammation 5.
* Equal first authors.
Reprints were made with permission from the respective publishers.

Related papers published during the PhD period
1. Westerberg, E., Molin C.J., Lindblad. I., Emtner, M. & Punga, A.R. (2017) Physical exercise in myasthenia gravis is safe and improves neuromuscular parameters and physical performance-based measures: A pilot study. Muscle Nerve 56, 207-214.
2. Westerberg, E., Molin, C.J., Spörndly Nees, S., Widenfalk, J. & Punga, A.R. (2018) The impact of physical exercise on functional muscle measures in myasthenia gravis patients - a single subject de-sign study. In press, Medicine.
Contents
Introduction ................................................................................................... 11Myasthenia gravis ..................................................................................... 11
Historical background .......................................................................... 11Pathophysiology ................................................................................... 12The thymus gland, autoimmunity, and inflammation .......................... 16Clinical signs and symptoms of MG .................................................... 18Diagnosis .............................................................................................. 19Treatment ............................................................................................. 21Epidemiology and genetics .................................................................. 23
Physical activity ........................................................................................ 24General recommendations and health benefits .................................... 24Muscle physiology of high-resistance strength training ...................... 25
Biomarkers ................................................................................................ 25Biomarkers for muscle training and neuromuscular function .............. 26Biomarkers for clinical use in MG ....................................................... 28
Aims .............................................................................................................. 31Specific aims ............................................................................................. 31
Methods ......................................................................................................... 32Patients and subjects ................................................................................. 32Ethics ........................................................................................................ 33Methods .................................................................................................... 34
Electrophysiological and muscle strength measurements .................... 34Ultrasound examinations ..................................................................... 35Inflammatory protein analysis ............................................................. 37miRNA analysis ................................................................................... 37Thymic lymphofollicular hyperplasia grading ..................................... 38
Statistics .................................................................................................... 38
Results ........................................................................................................... 41Study I – CMAP as an electrophysiological marker for muscle training . 41
Subjects and training habits ................................................................. 41CMAP and muscle strength recordings ............................................... 42
Study II – Nerve and muscle ultrasound in trained and untrained individuals ................................................................................................ 43
Subjects ................................................................................................ 43
Ultrasound of nerves and muscles ....................................................... 44Study III – Profile of upregulated inflammatory proteins in sera of MG patients ...................................................................................................... 46
Patients and subjects ............................................................................ 46Inflammatory protein expression ......................................................... 46
Study IV – miRNA in sera of MG patients in the MGTX study .............. 48Patients and clinical data ...................................................................... 48miRNA analysis ................................................................................... 49
Discussion ..................................................................................................... 53Neurophysiological biomarkers ................................................................ 53
CMAP as a biomarker for muscle training .......................................... 53Effect of HRST on peripheral nerves ................................................... 54Role of CMAP and ultrasound in exercise studies .............................. 55Drawbacks ............................................................................................ 57
Circulating biomarkers in MG .................................................................. 58Inflammatory proteins .......................................................................... 58miRNA ................................................................................................. 60Role of circulating biomarkers in MG ................................................. 62Drawbacks ............................................................................................ 63
Conclusions ................................................................................................... 65
Summary in Swedish – Sammanfattning på svenska .................................... 66
Acknowledgements ....................................................................................... 70
References ..................................................................................................... 72
Abbreviations
Ab ACh AChE AChEI AChR AChR+ AChR- ANCOVA APB β–NGF BDNF BMI CCL cDNA CMAP CNS CSA CT CXCL EAE EAMG EDB EMG EN-RAGE EOMG ETTX HC HHD HLA HRST IL IVIG LOMG LPF LRP4
Antibody Acetylcholine Acetylcholinesterase Acetylcholinesterase inhibitors Acetylcholine receptor Acetylcholine receptor antibody seropositive Acetylcholine receptor antibody seronegative Analysis of covariance Abductor pollicis brevis Nerve growth factor beta Brain-derived neurotrophic factor Body mass index C-C motif ligand Complementary DNA Compound motor action potential Central nervous system Cross sectional area Computed tomography C-X-C motif ligand Experimental autoimmune encephalomyelitis Experimental autoimmune myasthenia gravis Extensor digitorum brevis Electromyography Extracellular newly identified receptor for advanced end-products binding protein Early onset myasthenia gravis Extended transsternal thymectomy Healthy controls Hand-held dynamometer Human leukocyte antigen High-resistance strength training Interleukin Intravenous immunoglobulin Late onset myasthenia gravis Low-power field Lipoprotein receptor-related protein 4
LRP4+ MG MGC MGFA MGTX miRNA mRNA MMP MRI MuSK MuSK+ MuSK- NMJ OMG PNS QMG qPCR RNS RT SD SFEMG TFH TGF-α Tx
Lipoprotein receptor-related protein 4 seropositive Myasthenia gravis Myasthenia Gravis Composite Score Myasthenia Gravis Foundation of America Randomized Trial of Thymectomy in Myasthenia Gravis MicroRNA Messenger RNA Matrix metalloproteinase Magnetic resonance imaging Muscle-specific tyrosine kinase Muscle-specific tyrosine kinase antibody seropositive Muscle-specific tyrosine kinase antibody seronegative Neuromuscular junction Ocular myasthenia gravis Peripheral nervous system Quantitative Myasthenia Gravis test Quantitative real-time PCR Repetitive nerve stimulation Reverse transcriptase Standard deviation Single-fiber electromyography Thymic lymphofollicular hyperplasia Transforming growth factor alpha Thymectomy
11
Introduction
Myasthenia gravis Myasthenia gravis (MG) is a disorder where the cardinal symptom is fatiga-ble skeletal muscle weakness, which can range from slight weakness in the limb muscles or droopy eyelids, to a fulminant myasthenic crisis, which requires intensive care to support the paralyzed respiratory muscles. It is an autoimmune disorder, caused by autoantibodies against the neuromuscular junction (NMJ), i.e., the synapse between the peripheral motor nerve termi-nal and the muscle.
The word myasthenia comes from the Greek words µύς (mys), muscle, and ἀσθένεια (astheneia), where the prefix a- denotes lack of, and sthenia meaning strength. Gravis is the Latin word for grave, or severe. The name describes the nature of the disease quite well – severe muscle weakness.
Historical background The first description of MG, which dates back to the 17th century, was pre-sented by the English physician and anatomist Thomas Willis, sometimes called the father of neurology, whose name today perhaps is best known as the eponym for circulus Willisii1. During the next centuries, further case reports of MG were sparse, and more knowledge wasn’t available until the late 19th century. The term myasthenia gravis was suggested by the German physician Friedrich Jolly, who described two cases of MG in adolescent boys, suffering from what he called myasthenia gravis pseudo-paralytica. Jolly was also the first to describe the decreased muscle contraction as a result of repetitive nerve stimulation (RNS)2.
Another milestone in the history of MG was the first treatment of MG with acetylcholinesterase inhibitors (AChEI) by the physician Mary Walker in 19342,3, which led to improvement of clinical symptoms. The effect was temporary, but nonetheless was the first successful symptomatic treatment of MG.
The thought of MG as an autoimmune disorder was first suggested by Simpson in 19604, who wrote that “myasthenia is an ‘auto-immune’ re-sponse of muscle in which an antibody to end-plate protein may be formed”. In the early seventies, this hypothesis was proven to be true when Patrick and Lindstrom successfully immunized rabbits with acetylcholine receptors

12
(AChRs)5. The rabbits developed muscle fatigue, which was reversed with AChEI. The experimental model was named experimental autoimmune my-asthenia gravis (EAMG), and proved that MG was mediated by specific au-toantibodies rather than unspecific cellular immunity.
Pathophysiology Normal physiology of the neuromuscular junction and muscle contraction The area where the peripheral motor nerve terminal meets the muscle fiber is called the neuromuscular junction (NMJ). The main purpose of the NMJ is to propagate nerve impulses, action potentials, to skeletal muscle fibers. The nerve impulse is generated in the central nervous system, from the motor cortex in the brain to the spinal cord. Skeletal muscles are innervated by myelinated nerve fibers, which originate from α-motor neurons located in the anterior horn of the spinal cord. The motor nerve axon branches out on the muscle membrane, forming the structure called the NMJ, which is cov-ered by Schwann cells. The NMJ is located near the mid-point of the muscle fiber, where the nerve fiber synapses to the muscle. When an action potential reaches the NMJ, voltage-gated calcium channels open, causing release of vesicles packed with acetylcholine (ACh) into the synaptic cleft. ACh binds to postsynaptic nicotinic AChRs, located in the muscle fiber membrane. AChRs are ion channels that open when ACh attaches, which allows primar-ily Na+ to flow through to the inside of the fiber, causing an endplate poten-tial change which spreads along the muscle membrane, generating a muscle contraction6.
The motor neuron, its axon and the muscle fibers innervated by it together constitute a motor unit. Although each muscle fiber is only innervated by a single motor neuron, the number of muscle fibers innervated by a motor neuron can range from only a few in small muscles, to several hundred in larger muscles. All the muscle fibers in a motor unit are of the same fiber type, and when a motor unit is voluntarily activated, all the fibers in the mo-tor unit contract. The muscular contraction force can be enhanced in two ways. First, the impulse frequency of the nerve can be increased until every single muscle fiber in the motor unit is activated in a tetanic manner. The second way is by engaging more motor units, which increases the force of the entire muscle6,7.
As soon as ACh is released into the synaptic cleft, it activates AChRs. ACh is then rapidly destroyed by the enzyme acetylcholinesterase (AChE), which is ubiquitous in the synaptic cleft. ACh is actually only present in the synaptic cleft for a few milliseconds6.

13
Impaired neuromuscular signaling Abnormal functioning of the NMJ causes fatigable skeletal muscle weak-ness, regardless of how the NMJ is affected. The NMJ can be affected both pre- and postsynaptically. In MG, the postsynaptic part of the NMJ is affect-ed. Examples of disorders affecting the presynaptic part of the NMJ are Lambert-Eaton myasthenic syndrome, most often caused by antibodies against voltage-gated calcium channels (~90 %); congenital myasthenic syn-dromes, where the recycling of ACh vesicles or the function of AChE can be impaired; as well as tetanus and botulinum toxins, which impair the release of neurotransmittors7.
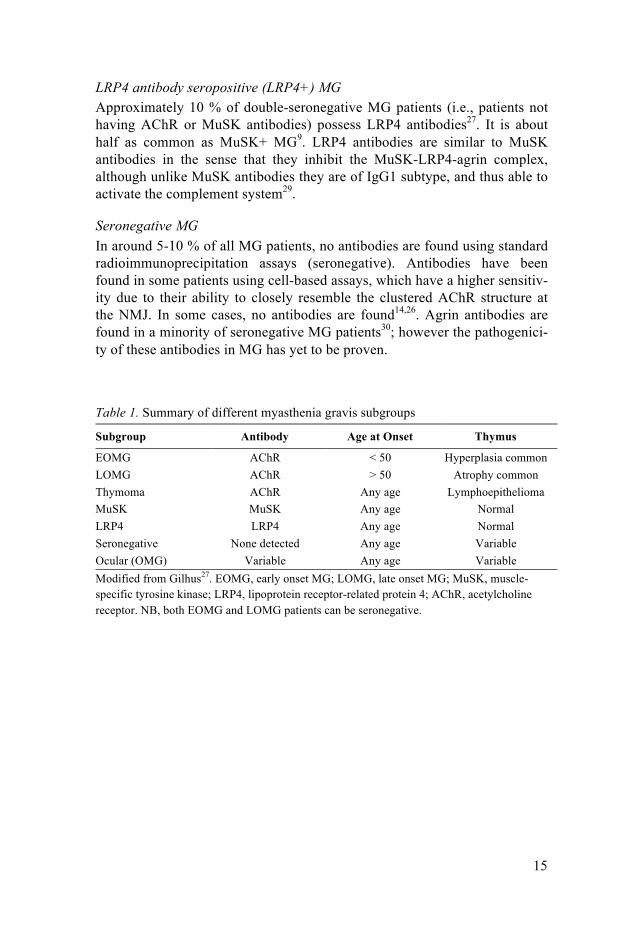
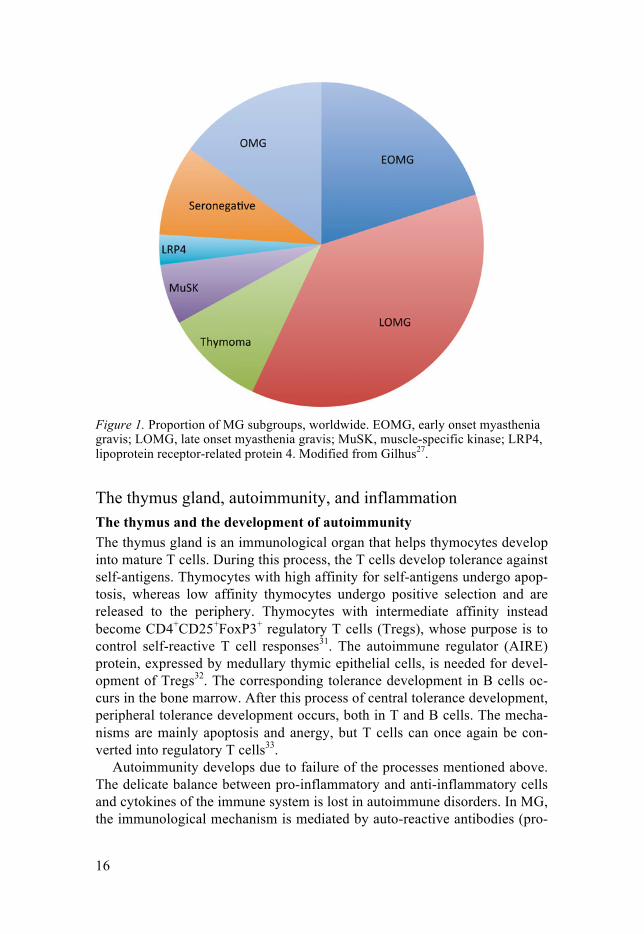
MG pathophysiology and subgroups MG can be classified into several different subgroups based on the different pathological mechanisms, age at onset and muscle groups affected. A sum-mary of the different subgroups and their approximate distribution is pre-sented in table 1 and figure 1.
Acetylcholine receptor antibody positive (AChR+) The most common antibody type in the sera of MG patients is directed against the AChR. About 80-85 % of patients possess AChR antibodies8,9, and are thus termed AChR antibody seropositive (AChR+). These antibodies impair the functions of the AChR in several ways: 1) blocking the ACh bind-ing site10 2) cross-linking the receptors to each other, which leads to internal-ization and destruction of the receptors11, and 3) activating the complement system, which causes destruction of AChRs and the postsynaptic folds11,12. The antibodies are mainly of IgG1 subtype, although IgG3 isotype is also present10,13, and these antibody subtypes are specifically able to activate the complement system. The destruction of the postsynaptic folds also reduces the number of sodium channels, and leads to an increased threshold for the endplate potential to reach in order to trigger the action potential. Both the motor nerve terminal and the postsynaptic muscle compensate for the im-paired transmission, by increasing the amount of ACh released from the nerve terminal during a nerve impulse, and by increasing the muscle AChR synthesis, respectively14.
Thymoma-associated MG Around 10-20 % of MG patients have a thymoma, and the percentage of thymoma patients with MG is approximately 30 %. Therefore, it is important to visualize the mediastinum in all MG patients, either with a computed to-mography scan (CT) or magnetic resonance imaging (MRI), in order to find possible thymomas. While not all thymoma patients present with clinical MG, almost all possess antibodies against the AChR15 and also against stri-ated muscle or the muscle protein titin16. Antibodies directed towards the

14
ryanodine receptor, and various cytokines (such as IL-17F) are also present, although to a lower extent15.
MuSK antibody seropositive (MuSK+) MG In 2001, a new type of MG antibody was discovered17,18. Until then, all pa-tients who did not possess AChR antibodies were classified as seronegative. These new antibodies were directed against muscle-specific tyrosine kinase (MuSK). MuSK is a co-receptor of lipoprotein receptor-related protein 4 (LRP4), and together they form a complex that is activated by neuronal agrin, secreted by the motor nerve ending. Agrin binds to LRP4, which in turn stimulates activation and phosphorylation of MuSK. MuSK then re-cruits Dok7, a docking protein, which further enhances MuSK activity and causes dimerization of MuSK. Dok7 recruitment also leads to anchoring of important proteins to the postsynaptic membrane and regulates specific gene expression through downstream signaling. Further phosphorylation, together with several other proteins, are important for the clustering and function of the AChR19. The activation of MuSK thus causes clustering of the AChRs, which is required for normal neuromuscular transmission20.
MuSK antibodies have proven to be disease specific, and both recombi-nant and patient MuSK antibodies induce myasthenic symptoms in mice. MuSK antibodies impair neuromuscular transmission by reducing the num-ber of AChRs, as well as inhibiting the MuSK-LRP4-agrin complex, disturb-ing the connection between the nerve terminal and the post-synaptic mem-brane21-23. However, MuSK antibodies also reduce the amount of released ACh, and thus affect neuromuscular transmission both pre- and postsynapti-cally24. The compensatory increase in ACh release in AChR+ MG is not seen in MuSK+ MG19. MuSK antibodies are found in as many as 40-50 % of AChR antibody seronegative (AChR-) MG patients in different regions of the world25,26. Compared with AChR+ MG, MuSK+ patients most often display normal thymus histology27. The MuSK antibodies are predominantly of IgG4 subtype, and thus cannot activate the complement system28. Further, since IgG4 antibodies are monovalent, they do not cause internalization of AChR.
15
LRP4 antibody seropositive (LRP4+) MG Approximately 10 % of double-seronegative MG patients (i.e., patients not having AChR or MuSK antibodies) possess LRP4 antibodies27. It is about half as common as MuSK+ MG9. LRP4 antibodies are similar to MuSK antibodies in the sense that they inhibit the MuSK-LRP4-agrin complex, although unlike MuSK antibodies they are of IgG1 subtype, and thus able to activate the complement system29.
Seronegative MG In around 5-10 % of all MG patients, no antibodies are found using standard radioimmunoprecipitation assays (seronegative). Antibodies have been found in some patients using cell-based assays, which have a higher sensitiv-ity due to their ability to closely resemble the clustered AChR structure at the NMJ. In some cases, no antibodies are found14,26. Agrin antibodies are found in a minority of seronegative MG patients30; however the pathogenici-ty of these antibodies in MG has yet to be proven.
Table 1. Summary of different myasthenia gravis subgroups
Subgroup Antibody Age at Onset Thymus
EOMG AChR < 50 Hyperplasia common LOMG AChR > 50 Atrophy common Thymoma AChR Any age Lymphoepithelioma MuSK MuSK Any age Normal LRP4 LRP4 Any age Normal Seronegative None detected Any age Variable Ocular (OMG) Variable Any age Variable Modified from Gilhus27. EOMG, early onset MG; LOMG, late onset MG; MuSK, muscle-specific tyrosine kinase; LRP4, lipoprotein receptor-related protein 4; AChR, acetylcholine receptor. NB, both EOMG and LOMG patients can be seronegative.
16
Figure 1. Proportion of MG subgroups, worldwide. EOMG, early onset myasthenia gravis; LOMG, late onset myasthenia gravis; MuSK, muscle-specific kinase; LRP4, lipoprotein receptor-related protein 4. Modified from Gilhus27.
The thymus gland, autoimmunity, and inflammation The thymus and the development of autoimmunity The thymus gland is an immunological organ that helps thymocytes develop into mature T cells. During this process, the T cells develop tolerance against self-antigens. Thymocytes with high affinity for self-antigens undergo apop-tosis, whereas low affinity thymocytes undergo positive selection and are released to the periphery. Thymocytes with intermediate affinity instead become CD4+CD25+FoxP3+ regulatory T cells (Tregs), whose purpose is to control self-reactive T cell responses31. The autoimmune regulator (AIRE) protein, expressed by medullary thymic epithelial cells, is needed for devel-opment of Tregs32. The corresponding tolerance development in B cells oc-curs in the bone marrow. After this process of central tolerance development, peripheral tolerance development occurs, both in T and B cells. The mecha-nisms are mainly apoptosis and anergy, but T cells can once again be con-verted into regulatory T cells33.
Autoimmunity develops due to failure of the processes mentioned above. The delicate balance between pro-inflammatory and anti-inflammatory cells and cytokines of the immune system is lost in autoimmune disorders. In MG, the immunological mechanism is mediated by auto-reactive antibodies (pro-

17
duced by B cells), and/or self-reactive T cells. Although the symptoms of MG are caused by antibodies against the NMJ, the thymus is the organ where the inflammatory process takes place. The role of the thymus in the development of MG is not yet fully understood. Pathogenic intrathymic germinal centers are believed to drive the hypermutation of B cell receptor genes and production of high affinity AChR antibodies in EOMG. AChRs are expressed by thymic myoid cells in the normal thymus, in order for T cells to develop immunological tolerance towards muscle tissue and related proteins. The number of B cells, plasma cells and germinal centers are in-creased in EOMG thymuses, and Tregs are defective15.
There is an imbalance between pro-inflammatory T helper 17 cells (Th17 cells), characterized by their ability to secrete the cytokine IL-17, and anti-inflammatory Tregs in MG patients. The Tregs display a defect in their regu-latory function, whereas effector T cells can be resistant to suppression34. The number of Tregs is not necessarily fewer, but their function seems to be impaired. Defective Th17 cells have not been found in thymuses of MG patients, but cytokines of the IL-17 family are overexpressed in hyperplastic AChR+ MG thymuses. In some studies, the expression of IL-17 in plasma and serum is increased also, although there are reports stating otherwise34.
Although autoantibodies are most common in MG, auto-reactive T cells have been found in MG patients, which may be important to consider, since many treatment options primarily target B cells35. In LOMG, it is believed that the autoimmunity is initiated by auto-reactive, non-tolerant T cells, which are exported from the atrophic thymus to the periphery, where they activate antibody production by B cells in lymph nodes15.
MG patients have an increased risk of concomitant autoimmune disor-ders, such as systemic lupus erythematosus, autoimmune thyroiditis and rheumatoid arthritis36, suggesting a common underlying pathophysiology. A similar relationship between different autoimmune disorders was confirmed in a Swedish cohort37, where MG patients had an increased risk of polymyo-sitis/dermatomyositis, systemic lupus erythematosus and Addison’s disease. It is well known that women are more susceptible to autoimmune disorders compared with men, and one possible explanation for this might be that es-trogen seems to have an effect on the expression of AIRE, which, as stated above, is important for the development of anti-inflammatory Tregs38.
Autoimmunity and inflammation The inflammatory cytokine IL-6 is upregulated in thymic epithelial cells in MG patients39 and it is believed to be involved in the inflammatory response in MG40, since its expression is impaired, together with other cytokines. IL-6 is also important for the autoimmune response in EAMG41, since it stimu-lates the development of Th17 cells. Th17 cells in turn secrete the cytokine IL-17A42, which is increased in sera of MG patients. Moreover, the levels of
18
IL-17A correlate with disease severity43 and with AChR antibody titer44 in MG patients.
IL-8 is another cytokine that is upregulated in MG patients45. It attracts neutrophils and T cells and it has also been linked to the occurrence of thy-moma in MG patients46.
Clinical signs and symptoms of MG Generalized MG The most common form of AChR+ MG is generalized MG, affecting skele-tal muscles outside of the extraocular area, i.e., limb, axial, oropharyngeal and/or respiratory muscles. The symptoms of MG fluctuate, and can vary a lot over longer time periods as well as during the course of one day. Typical-ly, the symptoms progress during the day, and are at their worst in the even-ing.
Generalized MG is further subcategorized into early onset MG (EOMG) and late onset MG (LOMG). The age cut-off between the two subgroups is not internationally defined and varies between different countries47. The most common cut-off is at 50 years of age48. The incidence peak for EOMG is around 30 years, and around 70 years for LOMG. Apart from the bimodal incidence pattern, EOMG is more associated with other autoimmune diseas-es and different human leukocyte antigens (HLA) compared with LOMG49. EOMG is three times more frequent in women, whereas men are more prevalent in the LOMG subgroup27. Further, thymic hyperplasia is more common in the EOMG group, whereas the LOMG often show no signs of thymic hyperplasia, but instead often present with thymic atrophy9,15.
Ocular MG When only the ocular muscles are affected, the disease is termed ocular MG (OMG). Symptoms include ptosis and/or diplopia. Approximately 15 % of MG patients have purely ocular symptoms, and half of them have no detect-able autoantibodies. Both AChR and LRP4 antibodies occur in the OMG subgroup, whereas MuSK antibodies are very rare. Progression of the dis-ease is not unusual, and often OMG patients develop generalized symptoms within a few years. The occurrence of antibodies, as well neurophysiological signs of disease activity in non-ocular muscles, are risk factors for develop-ing generalized disease, which is why glucocorticoid treatment is recom-mended to prevent generalization. However, if a patient only has ocular symptoms for more than more than two years, the risk of generalization is quite low9,27.

19
MuSK+ MG In MuSK+ MG patients, the symptoms are more often generalized compared with AChR+ MG, and also more localized to the bulbar and respiratory mus-cles. The symptoms include dysphagia, dysarthria and weakness of the facial and neck muscles, whereas ocular and limb weakness is relatively rare28. Compared with AChR+ MG, MuSK+ patients have a higher rate of myas-thenic crises. Further, they often have signs of muscle wasting, especially in the tongue and facial muscles25,50. MuSK is also expressed in the brain, pri-marily the hippocampus, and may be important for memory consolidation51. Cognitive impairments have been found in some MuSK+ MG patients52, and combined with the deviant clinical manifestation, there is a risk that MuSK+ MG patients initially are misdiagnosed50.
Assessing disease severity In order to evaluate the response to different treatments and provide prog-nostic information, there is a need to classify patients who share similar symptoms according to the severity of disease, mainly for research purposes. This is done using the MGFA Clinical Classification53,54, developed by the Myasthenia Gravis Foundation of America (MGFA). It should be noted that this classification should not be used to measure outcome; instead, the MGFA Post-intervention Status should be used to classify outcome status after therapy.
Diagnosis Diagnosis of MG can be confirmed by a combination of clinical, neurophys-iological and immunochemical methods.
Clinical tests Neurological examination The traditional medical diagnostic tools of patient history and clinical neuro-logical examination are important as first steps in the diagnostic process of MG. In order to validate the diagnosis, the other methods stated below should also be included as part of the investigation.
Besides a regular neurological examination, the clinical evaluation should include objective fatigability testing of different muscle groups, including neck, facial, bulbar and limb muscles, usually by repeated contractions or sustained isometric contraction. To facilitate the clinical evaluation, several scaling instruments have been developed. The most common internationally used instruments are the quantitative myasthenia gravis score (QMG)55 and the myasthenia gravis composite scale (MGC)56. These scaling instruments can be used to follow the progression of disease, both clinically and in clini-cal trials. It is recommended to use the MGC scale, since it does not only
20
evaluate the clinical picture, but also takes into account symptoms reported by the patient. This is especially important due to the fluctuating nature of MG.
Acetylcholinesterase inhibitor test Edrophonium is a short-acting AChEI, which is administered intravenously. As AChE is inhibited, more ACh is available at the NMJ, which temporarily improves neuromuscular transmission. This beneficial effect is visible within less than a minute, and slowly decreases over the course of a few minutes. Fatigability is tested in several muscles, and objective improvement is re-quired for the test to be positive. Several side effects can occur, mainly mus-carinergic in nature, such as hypersecretion, muscle fasciculations and gas-trointestinal discomfort. It should be noted that the edrophonium test is not specific to MG, and improvement after injection has been seen in several other disorders such as various myasthenic syndromes, as well as brain le-sions and aneurysms.
Neurophysiological examination Repetitive nerve stimulation Electroneurography can be used to study neuromuscular transmission, using recording surface electrodes over the muscle belly and repetitive nerve stim-ulation (RNS). With RNS, the nerve is repeatedly stimulated up to 10 times, typically using a low frequency of 3 Hz. The reduction of the amplitude, which is most prominent between the 1st and the 4th response, is called dec-rement, and should not exceed 5 % in healthy individuals. In MG patients, the decrement is usually higher, especially in muscles that are weak. The examination is performed at rest, after 20 seconds of maximal voluntary muscle activity, and then again after 1, 3 and 5 minutes post contraction. While decrement is seen at rest, after voluntary muscle contraction it should be close to normal (facilitation). After 1 minute of rest, the decrement is once again present, in some cases even greater than at the outset (exhaus-tion). The exhaustion might be even more pronounced after 3 minutes, but after 5 minutes the decrement level should return to the starting point. The test is not specific to MG, but it has good sensitivity for moderate or severe generalized MG, where up to 75 % of patients present with pathological decrement57.
Single-fiber Electromyography Single-fiber electromyography (SFEMG) is a more detailed variant of EMG, initially developed in the 1960’s58,59. The SFEMG electrode records activity from only a few muscle fibers (typically 2-3 fibers). SFEMG is used to study neuromuscular transmission and to diagnose NMJ transmission failure in-vivo. The method has a sensitivity of 95 % in MG patients57 and can detect
21
subclinical defects in neuromuscular transmission. SFEMG is therefore an important neurophysiological diagnostic examination method for MG60 in addition to RNS.
When examining neuromuscular transmission, the electrode records activ-ity from two muscle fibers from the same motor unit during voluntary mus-cle contraction. One action potential is used as a time reference, and the dif-ference in time between action potentials of the two muscle fibers is meas-ured. This difference changes slightly during repeated discharges, which is called neuromuscular jitter. The jitter is a result of the variation in time of transmission from the axon to the muscle fiber in the motor end plate during different nerve impulses. Usually, the jitter is less than 50 µs, but when neu-romuscular transmission is impaired, it is increased57. When jitter values exceed 100 µs, blocking of neuromuscular transmission usually arises.
Serum analysis of antibodies Analysis of serum antibodies has the highest specificity when it comes to diagnosing MG, and should always be a part of the diagnostic process. It is also equally important for classifying patients into immunological sub-groups, in order to individualize the treatment.
Anti-AChR antibodies AChR antibodies are disease specific and pathogenic for MG. As stated pre-viously, around 80 % of all MG patients8 are AChR antibody seropositive (AChR+). The antibodies are often detected with a radioimmunoassay (RIA), in which purified AChRs from human muscles serve as antigens, labeled with 125I-α-Bungarotoxin, which is a snake toxin that binds to the AChR8,61,62. As stated previously, antibodies can be detected in some sero-negative MG patients using cell-based assays, where the AChR are clustered on cell lines, representing a more physiological state, which increases the sensitivity63. About one third of seronegative patients with generalized MG are seropositive with cell-based assays27.
Anti-MuSK antibodies Because of the different clinical phenotypes and treatment responses, it is very important to test for anti-MuSK antibodies in AChR- MG patients. Detection of MuSK antibodies was originally done with the enzyme-linked immunosorbent assay technique17. Today, RIA of 125I-labeled-human MuSK extracellular domains64 or of recombinant human and rat MuSK extracellular domains65 are used, where the latter is commercially available66.
Treatment There is no curative treatment for MG. The treatment thus consists of symp-tomatic medication and disease modifying drugs. The goal of the treatment
22
is to reduce the symptoms, and to achieve minimal manifestation status54. In generalized AChR+ MG, AChEI, together with thymectomy in cases of EOMG or thymoma, is the first line of treatment. If no clinical remission occurs, prednisone and/or azathioprine are added. If this is still not efficient, other immunomodulatory drugs are added27.
Symptomatic treatment AChEIs are the most common treatment, and provides relief of symptoms, especially in AChR+ patients. AChEIs inhibits the degradation of ACh, which increases the concentration of ACh and thereby prolongs its effect at the NMJ. The most common drug is Pyridostigmine (Mestinon®), a reversi-ble, medium-lasting AChEI, administered at a dose of 60-120 mg, 3-6 times a day. AChEIs are also available for intravenous administration (Neostig-min®).
The dosage of AChEIs is highly individual. If the dose is too high, trou-blesome side effects, related to both nicotinergic and muscarinergic AChRs, appear. An overdose can be fatal, since it leads to a cholinergic crisis with severe muscle fatigue that mimics myasthenic weakness, and in the worst-case respiratory muscle paralysis.
Thymectomy and immunomodulatory treatment Immunosuppressive treatment is often necessary as a complement to AChE-Is, in order to achieve good physical function and quality of life, but also to prevent progression of the disease.
Thymectomy As stated previously, a CT-scan or an MRI of the chest should always be performed to exclude a thymoma. Thymectomy as a treatment for AChR+ MG has been used for many years due to the known presence of thymus hyperplasia in this type of MG67. The effect has been investigated in many retrospective studies, with varying results68,69. In 2016, a randomized, pro-spective study was published which confirmed lower dosage of prednisone and better clinical scores in patients who have undergone extended transster-nal thymectomy (ETTX)70. However, thymectomy is not recommended in patients with MuSK, LRP4, or agrin antibodies, since they most often dis-play normal thymus histology71.
Prednisone Prednisone is the most common immunosuppressive medication for MG. It can be administered on alternate days in order to minimize side effects. When prednisone treatment is started, the dose is gradually increased until sufficient disease control is achieved. When the disease is stable enough, the dose should slowly be reduced to the lowest effective level. Prednisone ther-apy is often used for OMG, in order to prevent generalization.

23
Immunosuppressive medication Unless clinical improvement is achieved with AChEIs and prednisone, ster-oid sparing immunosuppressive medication, such as azathioprine, cyclospor-ine, rituximab, tacrolimus and methotrexate, is added. Long-term steroid use is associated with several side effects, which is why the dose should be kept as low as possible. Azathioprine is often used as first-line therapy for long-term usage, with cyclosoprine as second-line therapy and tacrolimus or my-cophenolate mofetil as third-hand options, whereas the other mentioned drugs are used more sparsely. Azathioprine and mycophenolate mofetil in-hibit purine synthesis, thereby suppressing T and B cell proliferation, where-as other immunosuppressants, such as tacrolimus and cyclosporine, instead suppress T cells and natural killer cells. Methotrexate inhibits folate metabo-lism72. Rituximab is of particular interest in MG, since it’s a monoclonal antibody that specifically targets the CD20 surface antigen on B cells, lead-ing to reduced B cell count and function. In addition, rituximab also seems to have an effect on T cell function. It is used for several autoimmune disor-ders, and was recently approved as a treatment option for multiple sclerosis in Sweden. A newer immunosuppressant, Eculizumab, has recently been approved for treatment of refractory generalized MG in Europe, Japan and the United States. It is the only immunosuppressant targeting components the complement system73. Although the immunosuppressants mentioned above are included in most guidelines, the literature regarding their use in MG is sparse. Therefore, the use and choice of immunosuppressants varies between clinical centers.
Plasmapheresis and intravenous immunoglobulin (IVIG) In the most severe cases, with exacerbations or myasthenic crises, intrave-nous immunoglobulin (IVIG) or plasmapheresis are used. IVIG suppresses T cells and B cells and neutralizes autoantibodies, whereas plasmapheresis (most commonly plasma exchange) removes the autoantibodies. The results are similar between the two treatments74, and which treatment to use needs to be individually tailored for each patient.
Epidemiology and genetics The incidence and prevalence rates of MG vary between different reports, but the worldwide incidence is around 2-20 per million person-years, and the prevalence is around 15-180 per million9,27. The calculated pooled incidence and prevalence rates in studies ranging from 1950-2007 are 5.3 and 77.7, respectively75. However, a population-based study indicated that the preva-lence might actually be higher in Sweden, up to 25 per 100 00037. Both inci-dence and prevalence rates have been increasing with more recent stud-ies47,75. The increase in incidence rates is probably related to an increase in

24
LOMG and more widespread diagnostics, whereas the increase in prevalence rates might be due to improved disease knowledge and treatment, as well as different epidemiological methodology9,47,75.
The different MG subgroups display different HLA associations, which also differ between ethnicities. EOMG is associated with HLA-DR3 and HLA-B8, which also are risk genes for other autoimmune disorders, whereas LOMG is more associated with HLA-DR2, HLA-B7 and HLA-DRB1*15:01. MuSK+ MG is instead associated with HLA-DQ5, and is more common in females9,76. The prevalence of MuSK+ MG varies between geographical regions, and it is more common in Mediterranean countries compared with northern parts of Europe28,77.
The difference in HLA expression in MG subgroups, together with differ-ent clinical symptoms, antibody types and targets, response to treatment, pathophysiology and expression of miRNA and cytokines, indicate that the etiological mechanisms are substantially different, and that the subtypes of MG might be considered completely different disorders, with the common denominator of a malfunctioning NMJ.
Physical activity General recommendations and health benefits It is well known that physical exercise, and minimizing sedentary time78, benefits general health and reduces risk of coronary heart disease and stroke, diabetes, hypertension and depression. Physical inactivity is listed as the fourth leading risk factor for global mortality, and the recommendations for adults aged 18-64 years include 150 minutes of moderate-intensity aerobic physical activity per week, or at least 75 minutes of high-intensity aerobic physical activity combined with muscle strengthening activities on two or more days a week79. In addition, flexibility exercises are also recommended to maintain joint movement. Exercise should of course be adjusted to indi-vidual physical function and health status, and performing less exercise than recommended is still associated with health benefits80.
Considering this, it is surprising that these recommendations previously have not been considered valid for MG patients. In general, there is no con-sensus regarding recommendations for physical exercise in patients with neuromuscular diseases. More often than not, physical exercise has actually been discouraged, although based more on lack of knowledge rather than empirical evidence and scientific studies81. This is most unfortunate, since the state of the disease in combination with lack of exercise worsens overall health, which in turn worsens the physical function and cardiovascular ca-pacity of these patients, and leads to an increased risk of developing second-ary disease82.

25
Muscle physiology of high-resistance strength training It is well known that high-resistance strength training (HRST) causes both physiological as well as morphological muscular changes. These changes include growth of the muscle fibers, more powerful contraction83,84, better technique85 and improved central drive86-90. Strength training thus causes both increased muscle strength and muscle mass. The increase in muscle mass is mostly due to increased muscle fiber diameter, although an increase in the number of new muscle fibers also contributes to a small extent. The hypertrophy response to HRST is greater in arm muscles than in leg mus-cles91,92. The improved muscle strength is a result of an increased number of myofibrils, increased mitochondrial enzymes, improved metabolic systems, and increased storage of glycogen and fat6.
The hypertrophy response is greater in men than in women when training arm muscles, probably due to a higher concentration of androgen receptors93. Women possess approximately 60-80 % strength and muscle fiber area com-pared with men94, but the muscle force per square centimeter of the muscle cross-sectional area is almost exactly the same in men and women. Thus, the difference in muscle force between men and women is almost completely due to a higher proportion of muscle mass in men6. Apart from sex, age also has an effect on the muscle size and fiber diameter; elderly individuals have a lower response to HRST compared with young individuals, probably due to the fact that they have fewer muscle fibers95.
Biomarkers The term biomarker refers to any measure that can be used to indicate the state of a physiological condition or a specific disease. The most common use of biomarkers in medicine is as an indicator of disease severity or re-sponse to treatment. A biomarker can be a protein, hormone, gene or en-zyme, but also a measurement taken as part of the clinical examination, e.g., high blood pressure could be considered a biomarker for the risk of stroke and high cholesterol values as a biomarker for cardiovascular disease. Other examples, which perhaps are more linked to the word biomarker, are glucose consumption on PET-scan as a marker for cancer, troponin for heart muscle damage, or C-reactive protein as a marker for inflammation. Thus, a bi-omarker can be a substance that is added and measured, or the changed ex-pression or condition of a protein or substance.
The most important characteristic of a biomarker is that it actually func-tions as a marker for what it is intended to measure, regardless of whether that is clinical outcome, disease progression or treatment response. An ideal biomarker should also be easy to measure (the biological fluid or sample should be accessible), quick, economical, and have a stable expression re-
26
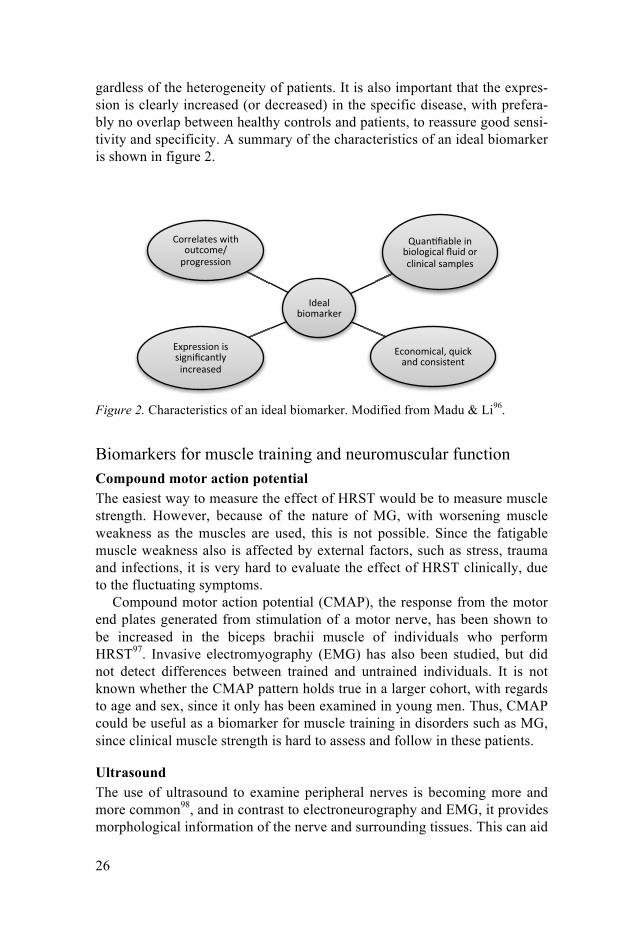
gardless of the heterogeneity of patients. It is also important that the expres-sion is clearly increased (or decreased) in the specific disease, with prefera-bly no overlap between healthy controls and patients, to reassure good sensi-tivity and specificity. A summary of the characteristics of an ideal biomarker is shown in figure 2.
Figure 2. Characteristics of an ideal biomarker. Modified from Madu & Li96.
Biomarkers for muscle training and neuromuscular function Compound motor action potential The easiest way to measure the effect of HRST would be to measure muscle strength. However, because of the nature of MG, with worsening muscle weakness as the muscles are used, this is not possible. Since the fatigable muscle weakness also is affected by external factors, such as stress, trauma and infections, it is very hard to evaluate the effect of HRST clinically, due to the fluctuating symptoms.
Compound motor action potential (CMAP), the response from the motor end plates generated from stimulation of a motor nerve, has been shown to be increased in the biceps brachii muscle of individuals who perform HRST97. Invasive electromyography (EMG) has also been studied, but did not detect differences between trained and untrained individuals. It is not known whether the CMAP pattern holds true in a larger cohort, with regards to age and sex, since it only has been examined in young men. Thus, CMAP could be useful as a biomarker for muscle training in disorders such as MG, since clinical muscle strength is hard to assess and follow in these patients.
Ultrasound The use of ultrasound to examine peripheral nerves is becoming more and more common98, and in contrast to electroneurography and EMG, it provides morphological information of the nerve and surrounding tissues. This can aid

27
in determining the etiology and localization of a lesion in a more precise way compared with electrodiagnostics. A nerve can be compressed either due to pressure from the outside, or entrapped by intrinsic structures, such as liga-ments. The cross-sectional area (CSA) of the nerve is often affected by vari-ous disorders, such as carpal tunnel syndrome and different neuropathies99. Moreover, the CSA is affected by factors such as BMI, height, weight, and age, in a somewhat contradicting manner100-103. Entrapment of a nerve causes nerve thickening (or constriction in severe entrapments) and reduced echo-genicity due to edema and inflammation, where the latter in turn causes in-creased vascularity. Fibrosis instead causes increased echogenicity. The mechanisms behind nerve swelling include endoneural edema and inflamma-tion, blocking of axonal transport, and development of perineural and epi-neural fibrosis104.
There is more knowledge regarding ultrasound of nerves compared with muscles. However, many neuromuscular disorders cause muscle atrophy and intramuscular architectural changes, which are detectable with ultrasound, often as increased echo intensity. Such diseases include Duchenne muscular dystrophy (increased echo intensity with normal muscle thickness), spinal muscular atrophy (increased echo intensity with severe atrophy), but also muscle dystrophies, inflammatory, congenital and metabolic myopathies amongst others. Moreover, muscle movement, such as contractions and fas-ciculations are also visible, which is an advantage compared with visualiza-tion with a CT-scan or MRI105,106. Ultrasound can therefore be used both as a screening and a diagnostic tool, but also as guidance when performing inva-sive procedures, such as biopsies and EMG. However, visual evaluation of muscle ultrasound is subjective, which can be limiting. Further, muscle ar-chitecture differs between muscles and changes with age, which can make visual evaluation difficult. Semi-quantitative and quantitative methods has been developed for more standardized evaluation, which can be helpful in difficult cases107.
As stated above, HRST causes greater hypertrophy in upper limbs than in lower limbs. This has been verified with ultrasound examination108. The knowledge about how HRST affects the morphology of peripheral nerves is, however, very limited. Only one previous case study has been published, where the subacute effects of strenuous exercise on peripheral nerves was examined with ultrasound109. Results from this study suggest that both the CSA and the conduction velocity of some nerves increase following a mara-thon run.
28
Biomarkers for clinical use in MG Antibody titers In AChR+ MG, the presence of AChR antibodies is crucial for correct grouping of patients. However, the antibody titer does not correlate with disease severity or predict response to therapy. In some studies, the antibody titer has been shown to correlate with the disease severity, but the relation-ship is still unclear, since several studies present numerous outliers and ex-ceptions26. In one study, levels of AChR antibodies correlated with MGFA score in patients with immunosuppression, but not in patients with only AChEI110. The antibody levels generally decrease with correct treatment, but this is not always the case111.
On the contrary, MuSK antibodies often correlate with poor treatment re-sponse to AChEI and other treatment options111, and also with disease se-verity26,28,112. Thymectomy typically has little or no effect in MuSK+ MG, consistent with the normal thymus histology and lack of reduction in anti-body titers after thymectomy.
Other possible clinical, genetic and immunological biomarkers There are several possible biomarkers in MG53. Clinical weakness could be used as a biomarker for disease state in clinical trials, but requires extended longitudinal assessment and a sufficient number of patients. SFEMG is a very good pharmacodynamic indicator, but unfortunately this technique is highly dependent on the skills of the examiner. Genomics could be used to predict metabolization of certain drugs, and regulatory T cells as a marker for disease severity and treatment response; however, more studies are need-ed before the clinical importance of these possible biomarkers can be deter-mined.
MicroRNA MicroRNA (miRNA) are small (≈ 22 nucleotides), non-coding RNA, which enable post-transcriptional regulation of gene expression by degrading or blocking their target messenger RNAs (mRNAs)113. Most of these miRNAs are found in the cytoplasm, but they can also be detected in the extracellular environment, as they are released from the cells in exosomes or microvesi-cles114-116. These extracellular miRNAs are termed circulating miRNA117, and can be detected and quantified with high sensitivity and specificity in several body fluids, making them accessible for clinical sampling. Another advantage is that they display a high stability in the extracellular space, en-capsulated in extracellular vesicles, but also in apoptotic bodies, or bound to protective proteins of the Argonaut family118. These miRNAs can thus func-tion as biomarkers, reflecting the course of a disease, or serving as diagnos-tic tools or markers of a therapeutic response.

29
Studies have shown that miRNAs regulate over 60 % of human protein-coding genes119, although a more recent study claims that the number of mRNAs actually targeted by miRNAs might be substantially lower120. The function of a specific miRNA is of course dependent on what type of gene it regulates, but the exact role of circulating miRNAs is not yet known. There are two contradicting theories. One of them is that circulating miRNAs func-tion as communication molecules, mediating cell-to-cell communication through paracrine or endocrine signaling. Selected miRNAs are proposedly released in extracellular vesicles from a special cell type, and taken up by a recipient cell, where they alter gene expression and functionality. The other theory suggests that miRNA are merely by-products of cell death and normal cellular activity, passively released from different cells, with no specific function117. The strongest argument against a specific cell-to-cell communi-cation is perhaps the very low concentration of miRNA in relation to cell volume and concentrations of active hormones in plasma.
Regardless of their function, a specific pattern of miRNA expression has been found in several diverse disorders, such as cardiovascular disorders, cancer and diabetes111, and altered miRNA expression has also been found in several autoimmune disorders121, such as rheumatoid arthritis122, systemic lupus erythematosus123 and multiple sclerosis124 amongst others. Thus, it is not surprising that miRNAs are becoming more and more common as bi-omarkers, due to their disease specific profiles and stable expression in plasma and serum125,126.
The expression of circulating miRNA in MG has been examined in a few previous studies. In AChR+ MG, the miRNAs miR-150-5p and miR-21-5p display an increased serum expression compared with healthy controls, where miR-150-5p had the strongest association with MG. It and also corre-lated with disease state in nine patients who underwent thymectomy127. An-other study validated the increased expression of miR-150-5p in MG, but did not find a correlation with and clinical score (MGC). However, these pa-tients were not analyzed pre- and post thymectomy128. Intriguingly, miR-150-5p is involved in the maturation process of T cells, controlling prolifera-tion and survival. It is upregulated during the maturation of both T and B cells, but downregulated during further differentiation of T cells129. Both miR-150-5p and miR-21-5p are increased in extracellular vesicles from regulatory T cells, compared with Th1 and Th17 cells130. The increased ex-pression of miR-150-5p and miR-21-5p in sera of MG patients was once again confirmed in a recently published study of LOMG patients131, together with miR-30e-5p. Furthermore, they all correlated with clinical status, since a positive correlation between MGC score and miRNA levels was found.
A similar profile of altered miRNA expression has been found in MuSK+ patients, where let-7a-5p, let-7f-5p, miR-151a-3p and miR-423-5p are ex-pressed at higher levels in the serum compared with healthy controls132.

30
Other, non-circulating miRNAs have also been discovered in the context of MG, and a recent miRnome study analyzed the expression of intracellular miRNA in thymuses of EOMG patients. In these patients, miR-7-5p was downregulated and miR-125a-5p was upregulated. Intriguingly, miR-7-5p was associated with thymic epithelial cells, and controlled release of CCL21, a chemokine that is important for formation of germinal centers. miR-125-5p, on the other hand, is known to regulate expression of FoxP3, a transcrip-tion factor that is crucial for the development of Tregs133.
31
Aims
The general aim of this thesis consists of two parts, which is reflected in the title: 1) to investigate new ways to assess neuromuscular function and mus-cle status with neurophysiological examination methods, in order to evaluate muscle response in future studies of physical exercise in MG patients, and 2) to identify new biomarkers for clinical symptoms, treatment response and disease activity in MG.
Specific aims I To study whether the compound motor action potential
(CMAP) differs between men and women who perform and do not perform high-resistance strength training, and whether it is possible to use the CMAP as an electrophysiological biomarker for muscle training.
II To study if the cross-sectional area of peripheral nerves, and muscle thickness of distal and proximal muscles, differ between men and women who perform and do not perform high re-sistance strength training.
III To characterize the profile of inflammatory proteins in the sera of MG patients and different subgroups in order to gain knowledge of possible biomarkers.
IV To study the hypothesis that mean values of proposed MG bi-omarkers miR-150-5p and miR-21-5p would be reduced over time after thymectomy, in parallel with clinical improvement. Further, to investigate the relation between prednisone dose and miRNA levels.
32
Methods
Patients and subjects
Study I and II Subjects were recruited through advertisements posted at local gyms, librar-ies, student organizations and the internal web page of Uppsala University Hospital. Those who wanted to participate were asked to fill in a form con-cerning their health and training habits. 83 subjects were recruited for study I, divided into two groups: one group that performed HRST, and one who did not. In order to qualify for the trained group, subjects needed to have performed HRST ≥ two times per week during the last year. The untrained group consisted of subjects who reported no training at all, or cardiovascular training but no HRST. Subjects were excluded if they had a family history of neurological illness affecting the muscles, took medication that affected the muscles (primarily muscle relaxants) or if they reported suffering from mus-cle weakness or muscle fatigue. The subjects were asked not to exercise on the day of study participation. Examinations were performed from Novem-ber 2014 to March 2015.
For study II, subjects who had participated in study I were asked to partic-ipate in a follow-up study. The criterion for remaining in the trained group was that the training intensity was not less than when they participated in study I. To remain in the untrained group, subjects had to confirm that they had not started performing HRST. Examinations were performed from March 2016 to June 2016.
Study III In study III, sera from 45 MG patients were collected at the Neurology Clin-ics at Uppsala University Hospital and Jönköping County Hospital, Sweden. Sera from 43 healthy controls (HC), matched for age and sex, were collected at the transfusion unit of Uppsala University Hospital. Diagnostic criteria, according to the Myasthenia Gravis Foundation of America (MGFA)54, in-cluded clinically objective muscle fatigue and neurophysiological evidence of disturbed neuromuscular transmission (decrement of repetitive nerve stimulation and/or increased jitter on single-fiber electromyography), further supported by the presence of serum antibodies against AChR134. Classifica-tion of MG status was performed according to MGFA, assessing symptoms

33
according to only ocular weakness (MGFA class I) and generalized weak-ness of mild (MGFA class II), moderate (MGFA class III) or severe (MGFA class IV) degree, predominantly affecting limb or axial muscles (subtype A) or bulbar muscles (subtype B). The degree of clinical MG fatigue was as-sessed at the time of serum sampling with the MGC56. The MG patients were divided into four subgroups, depending on (1) EOMG (defined as < 50 years) vs. LOMG (≥ 50 years); (2) patients who had undergone thymectomy vs. those who had not; (3) thymus hyperplasia vs. thymoma; and (4) current treatment with immunosuppressant medication vs. no immunosuppressive therapy.
Study IV The patients in Study IV consisted of patients included in the Randomized Trial of Thymectomy in Myasthenia Gravis (MGTX trial)70. The inclusion criteria for participating in the MGTX trial were: age ranging from 18 to 65 years; generalized myasthenia gravis (MGFA class II-IV), a disease duration of less than 5 years and AChR antibody seropositivity. Patients were ran-domized to thymectomy plus prednisone, or prednisone treatment only. Full details on trial design and study protocol are available in the original arti-cle70.
126 patients were accepted into the MGTX trial, and we obtained serum samples from 80 patients, drawn at baseline and at 12, 24, and 36 months post randomization. Clinical and demographic data (obtained from the MGTX study group) included age at enrollment, disease duration, predni-sone naïveté at enrollment, actual and time-weighted QMG score and pred-nisone dose, as well as data on other treatments (plasmapheresis, intravenous immunoglobulin and immunosuppressant medication) at each time point.
Ethics The studies were approved by Uppsala Ethical Review Board (study I and II, Dnr 2014/430; study III, Dnr 2010/446; study IV, Dnr 2010/446/2) and Lin-köping Ethical Review Board (study III, Dnr 2014/459-31). All experiments were performed in accordance with relevant guidelines and regulations. Par-ticipants gave voluntary written informed consent to participate in the stud-ies.
34
Methods Electrophysiological and muscle strength measurements CMAP recordings The CMAP recordings were performed at the Department of Clinical Neuro-physiology at Uppsala University Hospital. Key Point Classic (Alpine Bio-med; Skovlunde, Denmark) was used, with standard surface electrodes, 10 mm in diameter. The stimulating surface electrode had a fixed distance (23 mm) between anode and cathode. Skin temperature of the hand and foot was measured with a digital thermometer before the recordings, and was not al-lowed to be lower than 28 °C, since lower temperature affects the nerve con-duction velocity135. Stimulus duration of 0.1 milliseconds was used, except for stimulation of the femoral nerve where the stimulus duration was set to 0.2 milliseconds. The current was increased until a supramaximal CMAP was obtained, and the amplitude was measured from baseline to negative peak. Apart from CMAP amplitude, the distal motor latency, and area of the CMAP were noted. RNS with a frequency of 3 Hz was performed after the single supramaximal stimulation of each nerve, with the recording and stim-ulating electrode in the same positions, in order to rule out any neuromuscu-lar transmission deficiencies.
Subjects lay supine on a bed, and recordings were obtained with the re-cording electrode placed over the middle of the muscle belly from the fol-lowing muscles:
1. Abductor pollicis brevis muscle (APB), with stimulation of the median
nerve 8 cm proximal to the recording electrode, and the reference elec-trode placed over the medial part of the interphalangeal joint of the thumb.
2. Biceps brachii muscle, with stimulation of the musculocutaneous nerve in the axilla, and the reference electrode placed over the lateral epicon-dyle of the humerus.
3. Rectus femoris muscle, with the recording electrode in the middle be-tween the anterior superior iliac spine and the proximal edge of the pa-tella, with stimulation of the femoral nerve below the inguinal ligament, and the reference electrode placed over the medial femur epicondyle.
4. Extensor digitorum brevis muscle (EDB), with stimulation of the pero-neal nerve 8 cm proximal to the recording electrode, and reference elec-trode placed over the lateral part of the 5th metatarsophalangeal joint.
Muscle strength measurements with a HHD A HHD (model 01165; Lafayette Instrument Company, Lafayette, Ind., USA) was used to measure muscle strength. The test started when the force applied by the muscle exceeded 2 kg. The peak force (in kg) was measured
35
during a 5-second period, which was indicated with audible beeps from the dynamometer. A “make test” was used, where the subjects were asked to push maximally against the dynamometer, while the observer held the dy-namometer as static as possible, as opposed to a “brake test” were the exam-iner pushes the dynamometer against the subject’s limb until the joint gives way136. Muscles were examined in the following order: ABP muscle, biceps brachii muscle, EDB muscle and rectus femoris. After one test-measurement, three repeated measurements were performed, with 30 se-conds between each, and the mean value was calculated. Standardized test-ing positions and dynamometer placement were used according to previous studies137. The right arm and leg were examined, except if subjects reported any sensory or motor symptoms in the right-sided extremities, in which case the left side was examined instead.
All neurophysiological and muscle strength measurements were performed by C.J.M., to rule out possible inter-observer variability, such as electrode placement138.
Ultrasound examinations Nerve and muscle examinations were performed with a stationary ultrasound device (LOGIQ S8; GE Healthcare, Milwaukee, USA). C.J.M., J.W. or bio-medical technicians at the Department of Clinical Neurophysiology at Upp-sala University Hospital performed the measurements. C.J.M. participated in all evaluations in order to gain uniform judgments. Unless subjects reported sensory or motor symptoms in the right-side extremities, the right arm and leg were examined.
Nerve measurements The probe was adjusted so that it was perpendicular to the nerve. The tracer tool of the ultrasound device was used to measure the CSA, measuring just inside the epineurium. The largest CSA at each predetermined level was measured, since it is the parameter most commonly used in clinical practice when diagnosing neuropathies. As with the HHD measurements, three con-secutive images and measurements were recorded, and the mean value was calculated. There were only minimal differences between the three meas-urements. Three nerve sites were chosen for examination: 1. Median nerve at the wrist, just proximal to the carpal ligament. 2. Median nerve in the forearm, 12 cm proximal to the carpal ligament. 3. Musculocutaneous nerve at the axillary fossa, in the crest between the
biceps and deltoid muscle.
36
Patients were sitting up during examination of the median nerve, and lay supine when measuring the musculocutaneous nerve, with their right hand placed behind their head, in order to expose the crest between the biceps and the deltoid muscle. For the median nerve, an L8-18i MHz linear-array trans-ducer was used. For the musculocutaneous nerve, a ML6-15 MHz linear-array transducer was used. Subjects who reported symptoms of carpal tunnel syndrome, such as numbness, paresthesia and tingling, were excluded from the examination of the median nerve at the wrist.
Muscle measurements The thickness of the four muscles examined in study I was also measured. Measurements were taken at the muscle belly center. In order to obtain a correct muscle thickness, the transducer was held against the skin with min-imal pressure, with a visible layer of ultrasound gel between the transducer and the skin on the ultrasound image, i.e. the transducer had no direct con-tact with the skin. The largest measured diameter was recorded. Once again, three consecutive images and measurements were performed, and the mean value was calculated. The following muscles were examined:
1. Abductor pollicis brevis muscle (APB), with the probe perpendicular to
the first metacarpal bone, measured from the superficial fascia down to the princeps pollicis artery.
2. Biceps brachii muscle, measured approximately two thirds of the dis-tance from the acromion to the elbow crease.
3. Quadriceps muscle, measured approximately in the middle between the anterior superior iliac spine and the proximal edge of the patella. The vastus intermedius muscle belly and the rectus femoris muscle belly were measured individually, with the values then added together in order to obtain a total value of the quadriceps muscle thickness.
4. Extensor digitorum brevis muscle (EDB), measured at the largest part of the muscle as visualized when extending the toes.
Subjects were sitting up during examination of the APB muscle, and lay supine with extended legs and muscles relaxed during the other muscle ex-aminations. An L8-18i MHz linear-array transducer was used for the APB and EDB muscles, and an ML6-15 MHz linear-array transducer for the bi-ceps and quadriceps muscles. The measurements of the biceps brachii mus-cle included the brachialis muscle, since the muscle belly was measured from the superficial part of the fascia, down to the part of the fascia adjacent to the humerus. When measuring the APB and the biceps muscle, the fore-arm was held supine.
37
Inflammatory protein analysis The collected serum samples from MG patients and HC were analyzed with the Olink Proseek Multiplex Inflammation I 96x96 kit (Olink Biosciences, Uppsala, Sweden). This includes 92 human proteins related to inflammation and different inflammatory conditions, analyzed in up to 96 samples simul-taneously (http://www.olink.com/products/inflammation/). The analysis was performed at the Clinical Biomarkers Facility (Science for Life Laboratory, Uppsala, Sweden).
The Olink Proseek Multiplex uses the Proximity Extension Assay tech-nology139,140. Antibody-labeled oligonucleotides bind in pairs to their specific biomarker or target protein. If two correct antibody pairs bind to the same protein, they will hybridize and be extended by DNA polymerase. These sequences are then amplified by quantitative real-time PCR (qPCR). Details on data validation, limit of detection, specificity and reproducibility can be obtained at Olink’s website (http://www.olink.com/data-you-can-trust/validation/). The results are expressed as normalized protein expression units (NPX), which are arbitrary units, unique for each of the 92 proteins. A fold change of 0.5 NPX is considered a biological difference, and not due to technical variation. Curves for correlating the NPX values to actual protein concentrations are available at Olink’s website http://www.olink.com/products/inflammation/biomarkers/).
miRNA analysis The received serum samples were stored at -80°C until further processing. RNA was isolated from 200 µL serum samples by using miRCURY RNA Isolation Kit (#300112; Exiqon, Denmark), according to the manufacturer's instructions. 2 µL of isolated RNA were used for cDNA synthesis in a 10 µL reaction mix, using the Universal cDNA Synthesis Kit II (Exiqon, #203301).
The qPCR reactions were prepared with ExiLENT SYBR Green master mix (Exiqon, #203421), supplied with ROX Reference Dye (#12223-012; Life Technologies, Carlsbad, CA). The cDNA templates were diluted x50 in nuclease-free water. The qPCR reactions were applied to 384-well Pick-&-Mix plates (Exiqon, #203819), pre-coated with validated primers to amplify target miRNAs, which were miR-150-5p, miR-21-5p, miR-103a-3p, miR-191-5p, miR-93-5p, and miR-423- 5p. Inter-plate calibration (UniSp3), RNA extraction control (UniSp2 and UniSp4), cDNA synthesis control (UniSp6) and hemolysis markers (miR-23a-3p and miR-451a) were also included in the Pick-&-Mix PCR panel plates. All plates included rows with no reverse transcriptase enzyme added or pure H2O added as contamination controls. Amplifications were performed with the Applied Biosystems 7900 HT Fast Real-Time PCR System (Life Technologies). In order to rule out contamina-tion of cellular miRNA due to hemolysis, a ΔCT(hemolysis) value was calculated

38
(ΔCT(hemolysis) = CT(miR-23a-3p) - CT(miR-451a)). ΔCT value > 7 indicate a high risk of hemolysis, and samples with a value higher than 7 were excluded from further analysis. Reference genes included in the panel were miR-93-5p, miR-191-5p, miR-423-5p and miR-103a, since they all have a stable expres-sion in MG patients127. Reference gene miR-191-5p was chosen as the nor-malizing gene, as suggested by the “NormFinder” function in the GenEx software. The qPCR raw data were analyzed with the GenEx software, sup-plied by Exiqon. Quantification of relative miRNA expression was per-formed with the comparative CT method using the formula 2-ΔΔC
T, where ΔΔCT = (CT(miRNA of interest) - CT(reference miRNA)) sample A - (CT(miRNA of interest) - CT(reference miRNA)) sample B141.
Thymic lymphofollicular hyperplasia grading Data on thymus histology from patients who had undergone thymectomy were received from the Department of Pathology, Medical Faculty Mann-heim, and University of Heidelberg, Mannheim, Germany. Immunohisto-chemistry for CD23 was used for grading of thymic lymphofollicular hyper-plasia (TFH). If CD23 grading was missing, hematoxylin and eosin staining was used instead. Follicle content was assessed as the percentage of follicle-positive area per 20 low-power fields (LPFs, x50 magnification). In grade I, follicles are present in 1-33 % of all analyzed LPFs, and in grade II and III, follicles are present in 34-66 % and 67-100 % of all analyzed LPFs, respec-tively. In grade IV, more than 3 follicles per any LPF are observed. Normal thymic tissue can display TFH grade I, whereas grade II and III are associat-ed with EOMG (but also rarely occur in other autoimmune diseases), and TFH grade IV is considered a definite sign of EOMG. Full details on the thymus pathology in the MGTX trial has been published previously142.
Statistics
Study I and II In study I and II, an unpaired two-tailed t-test was used to compare paramet-ric data between the trained and untrained group, with a null hypothesis of equal means. CMAP amplitude and muscle strength were assumed to have a normal distribution. In study I, correlation analyses between CMAP and age, isometric muscle strength and BMI were performed with Spearman’s rank correlation coefficient.
In study II, correlation analysis between CSA and age, height and weight was performed with Pearson’s product-moment correlation coefficient. Mul-tivariate linear regression was performed to assess the effect of age, height and weight, with CSA as the dependent variable. BMI was neither included

39
in the correlation analysis nor the multivariate linear regression, since BMI does not take into account an individual’s ratio between muscle tissue and body fat, which can be especially misleading in trained individuals. Correla-tion analysis with Pearson’s correlation coefficient was also performed to assess the relationship between CSA and CMAP amplitude, CMAP area, and isometric muscle strength (measured in study I).
Data are presented as mean ± SD unless otherwise stated. A p-value < 0.05 was considered significant. In study I, analyses were performed with GraphPad Prism 6, whereas R version 3.2.4143 was used in study II.
Study III In order to obtain data more similar to normal distribution, a log2 base trans-formation was performed. 73 out of the 92 proteins followed a normal distri-bution. For these proteins, an unpaired two-tailed Welch t-test was per-formed for comparison between the MG group versus HC. For the non-normally distributed proteins, a Mann-Whitney U test was performed. The False discovery rate method was used to account for multiple testing errors. A two-way ANOVA was performed to test if gender had any effect on the protein expression of the three most significant proteins. Welch t-test was performed to test different subgroup analysis of protein expression. To iden-tify possible clusters of the three proteins that differed the most between MG and HC, a non-parametric dynamic principal component analysis (PCA) was performed. Spearman’s rank correlation coefficient was used to analyze the relation between protein levels and MGC score or disease duration.
Data are presented as mean ± SD unless otherwise stated. A p-value < 0.05 was considered significant. Subgroup analyses were performed with R version 3.2.4143.
Study IV The miRNA raw data were multiplied by 100, and then log2-converted in order to obtain more normally distributed data. QMG score and prednisone data were considered non-parametric. An unpaired two-tailed t-test was per-formed to examine between-group differences in miR-150-5p and miR-21-5p at baseline, and 12, 24 and 36 months post baseline, with a null hypothe-sis of equal means. A paired, two-tailed t-test was performed to examine if there was a difference in miR-150-5p and miR-21-5p levels between base-line and 12, 24 and 36 months post baseline within the same group, with a null hypothesis of no difference in means. Only if significant, a Wilcoxon’s signed rank test would also be performed to see if the decrease in miRNA level was accompanied by a reduction in QMG score or prednisone dose, to reduce the risk of error inflation. A post hoc analysis of covariance (AN-COVA) was performed to test group differences in miRNA levels adjusted for miRNA baseline values, sex, and age. Spearman’s rank correlation coef-ficient was used to determine the correlation between the miRNA levels,

40
QMG score and prednisone dose as a post hoc analysis of the subgroup of non-prednisone naïve in the prednisone group. Pearson’s χ2 test was used to compare clinical characteristics between the groups. Post hoc subgroup analyses with t-tests of miRNA levels were performed as follows: (1) male vs. female and (2) age (<50 and ≥50 years) at enrollment. No imputation methods were used for missing data. Crossover patients (patients random-ized to only prednisone who underwent thymectomy and vice versa) were analyzed according to the treatment they received.
Data are presented as mean ± SD unless otherwise stated. A p-value < 0.05 was considered statistically significant. Analyses were performed with R version 3.2.4143.
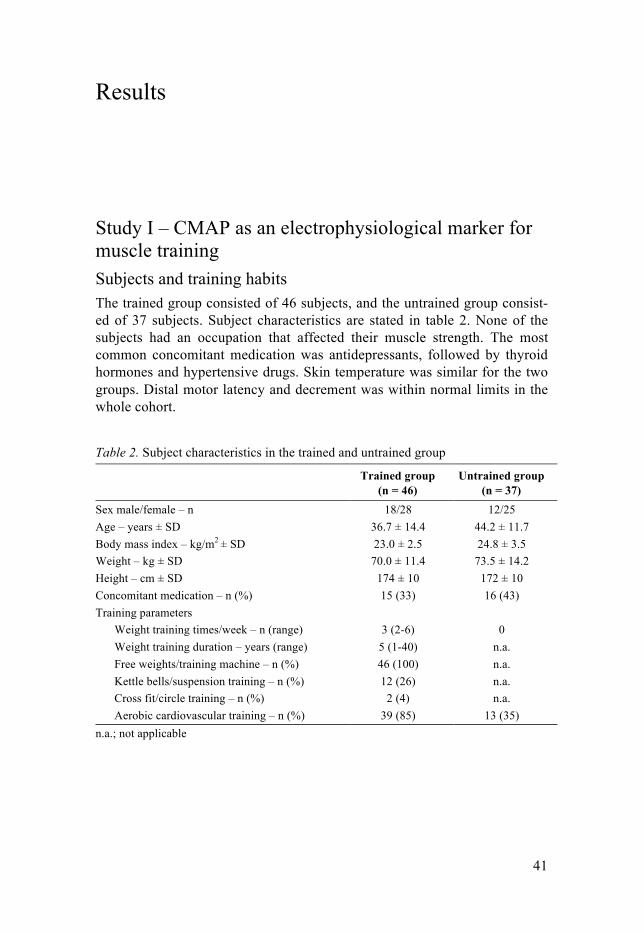
41
Results
Study I – CMAP as an electrophysiological marker for muscle training Subjects and training habits The trained group consisted of 46 subjects, and the untrained group consist-ed of 37 subjects. Subject characteristics are stated in table 2. None of the subjects had an occupation that affected their muscle strength. The most common concomitant medication was antidepressants, followed by thyroid hormones and hypertensive drugs. Skin temperature was similar for the two groups. Distal motor latency and decrement was within normal limits in the whole cohort.
Table 2. Subject characteristics in the trained and untrained group
Trained group (n = 46)
Untrained group (n = 37)
Sex male/female – n 18/28 12/25 Age – years ± SD 36.7 ± 14.4 44.2 ± 11.7 Body mass index – kg/m2 ± SD 23.0 ± 2.5 24.8 ± 3.5 Weight – kg ± SD 70.0 ± 11.4 73.5 ± 14.2 Height – cm ± SD 174 ± 10 172 ± 10 Concomitant medication – n (%) 15 (33) 16 (43) Training parameters
Weight training times/week – n (range) 3 (2-6) 0 Weight training duration – years (range) 5 (1-40) n.a. Free weights/training machine – n (%) 46 (100) n.a. Kettle bells/suspension training – n (%) 12 (26) n.a. Cross fit/circle training – n (%) 2 (4) n.a. Aerobic cardiovascular training – n (%) 39 (85) 13 (35)
n.a.; not applicable
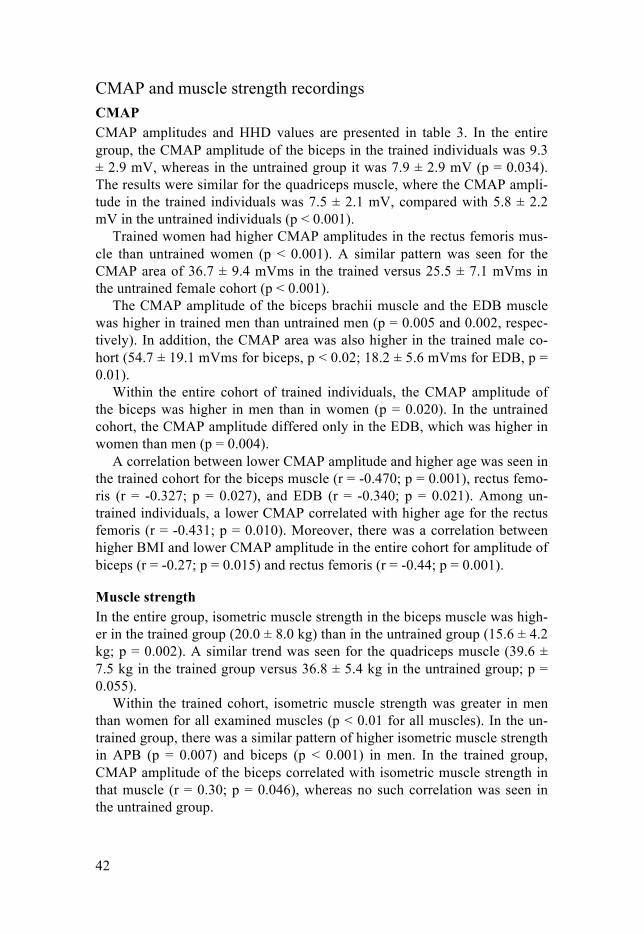
42
CMAP and muscle strength recordings CMAP CMAP amplitudes and HHD values are presented in table 3. In the entire group, the CMAP amplitude of the biceps in the trained individuals was 9.3 ± 2.9 mV, whereas in the untrained group it was 7.9 ± 2.9 mV (p = 0.034). The results were similar for the quadriceps muscle, where the CMAP ampli-tude in the trained individuals was 7.5 ± 2.1 mV, compared with 5.8 ± 2.2 mV in the untrained individuals (p < 0.001).
Trained women had higher CMAP amplitudes in the rectus femoris mus-cle than untrained women (p < 0.001). A similar pattern was seen for the CMAP area of 36.7 ± 9.4 mVms in the trained versus 25.5 ± 7.1 mVms in the untrained female cohort (p < 0.001).
The CMAP amplitude of the biceps brachii muscle and the EDB muscle was higher in trained men than untrained men (p = 0.005 and 0.002, respec-tively). In addition, the CMAP area was also higher in the trained male co-hort (54.7 ± 19.1 mVms for biceps, p < 0.02; 18.2 ± 5.6 mVms for EDB, p = 0.01).
Within the entire cohort of trained individuals, the CMAP amplitude of the biceps was higher in men than in women (p = 0.020). In the untrained cohort, the CMAP amplitude differed only in the EDB, which was higher in women than men (p = 0.004).
A correlation between lower CMAP amplitude and higher age was seen in the trained cohort for the biceps muscle (r = -0.470; p = 0.001), rectus femo-ris (r = -0.327; p = 0.027), and EDB (r = -0.340; p = 0.021). Among un-trained individuals, a lower CMAP correlated with higher age for the rectus femoris (r = -0.431; p = 0.010). Moreover, there was a correlation between higher BMI and lower CMAP amplitude in the entire cohort for amplitude of biceps (r = -0.27; p = 0.015) and rectus femoris (r = -0.44; p = 0.001).
Muscle strength In the entire group, isometric muscle strength in the biceps muscle was high-er in the trained group (20.0 ± 8.0 kg) than in the untrained group (15.6 ± 4.2 kg; p = 0.002). A similar trend was seen for the quadriceps muscle (39.6 ± 7.5 kg in the trained group versus 36.8 ± 5.4 kg in the untrained group; p = 0.055).
Within the trained cohort, isometric muscle strength was greater in men than women for all examined muscles (p < 0.01 for all muscles). In the un-trained group, there was a similar pattern of higher isometric muscle strength in APB (p = 0.007) and biceps (p < 0.001) in men. In the trained group, CMAP amplitude of the biceps correlated with isometric muscle strength in that muscle (r = 0.30; p = 0.046), whereas no such correlation was seen in the untrained group.
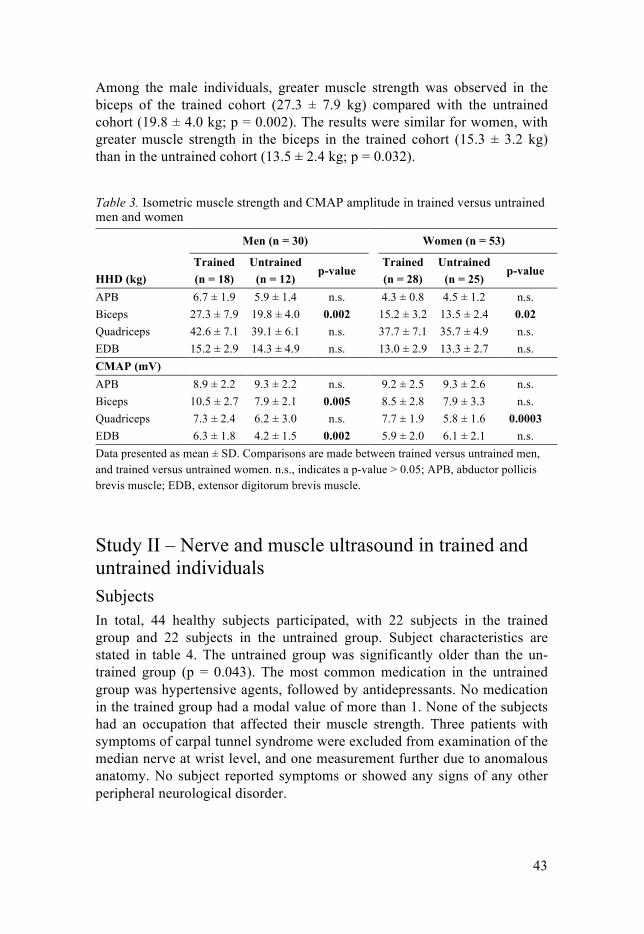
43
Among the male individuals, greater muscle strength was observed in the biceps of the trained cohort (27.3 ± 7.9 kg) compared with the untrained cohort (19.8 ± 4.0 kg; p = 0.002). The results were similar for women, with greater muscle strength in the biceps in the trained cohort (15.3 ± 3.2 kg) than in the untrained cohort (13.5 ± 2.4 kg; p = 0.032).
Table 3. Isometric muscle strength and CMAP amplitude in trained versus untrained men and women
HHD (kg)
Men (n = 30) Women (n = 53)
Trained (n = 18)
Untrained (n = 12)
p-value Trained (n = 28)
Untrained (n = 25)
p-value
APB 6.7 ± 1.9 5.9 ± 1.4 n.s. 4.3 ± 0.8 4.5 ± 1.2 n.s. Biceps 27.3 ± 7.9 19.8 ± 4.0 0.002 15.2 ± 3.2 13.5 ± 2.4 0.02 Quadriceps 42.6 ± 7.1 39.1 ± 6.1 n.s. 37.7 ± 7.1 35.7 ± 4.9 n.s. EDB 15.2 ± 2.9 14.3 ± 4.9 n.s. 13.0 ± 2.9 13.3 ± 2.7 n.s. CMAP (mV) APB 8.9 ± 2.2 9.3 ± 2.2 n.s. 9.2 ± 2.5 9.3 ± 2.6 n.s. Biceps 10.5 ± 2.7 7.9 ± 2.1 0.005 8.5 ± 2.8 7.9 ± 3.3 n.s. Quadriceps 7.3 ± 2.4 6.2 ± 3.0 n.s. 7.7 ± 1.9 5.8 ± 1.6 0.0003 EDB 6.3 ± 1.8 4.2 ± 1.5 0.002 5.9 ± 2.0 6.1 ± 2.1 n.s. Data presented as mean ± SD. Comparisons are made between trained versus untrained men, and trained versus untrained women. n.s., indicates a p-value > 0.05; APB, abductor pollicis brevis muscle; EDB, extensor digitorum brevis muscle.
Study II – Nerve and muscle ultrasound in trained and untrained individuals Subjects In total, 44 healthy subjects participated, with 22 subjects in the trained group and 22 subjects in the untrained group. Subject characteristics are stated in table 4. The untrained group was significantly older than the un-trained group (p = 0.043). The most common medication in the untrained group was hypertensive agents, followed by antidepressants. No medication in the trained group had a modal value of more than 1. None of the subjects had an occupation that affected their muscle strength. Three patients with symptoms of carpal tunnel syndrome were excluded from examination of the median nerve at wrist level, and one measurement further due to anomalous anatomy. No subject reported symptoms or showed any signs of any other peripheral neurological disorder.
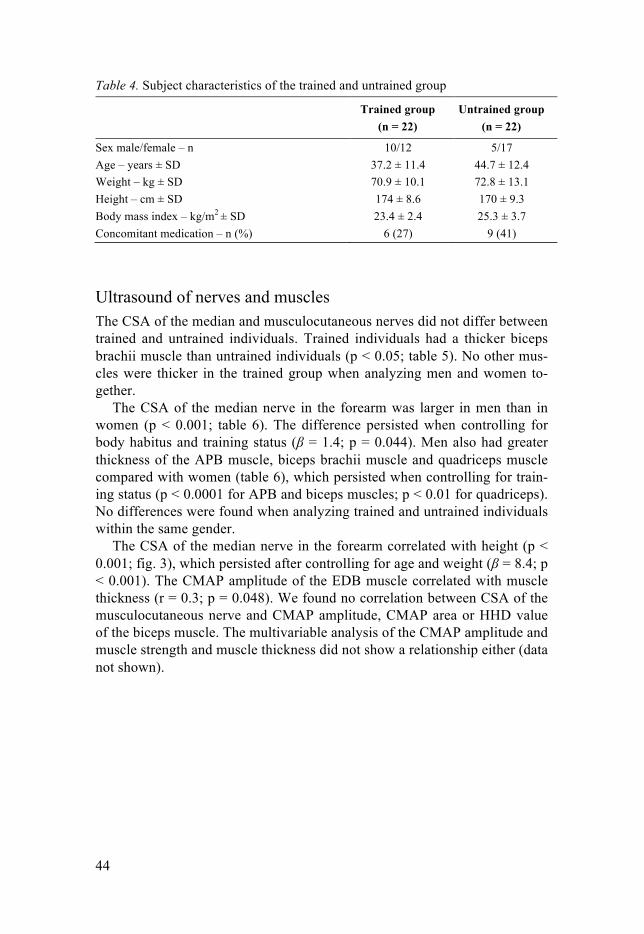
44
Table 4. Subject characteristics of the trained and untrained group
Trained group (n = 22)
Untrained group (n = 22)
Sex male/female – n 10/12 5/17 Age – years ± SD 37.2 ± 11.4 44.7 ± 12.4 Weight – kg ± SD 70.9 ± 10.1 72.8 ± 13.1 Height – cm ± SD 174 ± 8.6 170 ± 9.3 Body mass index – kg/m2 ± SD 23.4 ± 2.4 25.3 ± 3.7 Concomitant medication – n (%) 6 (27) 9 (41)
Ultrasound of nerves and muscles The CSA of the median and musculocutaneous nerves did not differ between trained and untrained individuals. Trained individuals had a thicker biceps brachii muscle than untrained individuals (p < 0.05; table 5). No other mus-cles were thicker in the trained group when analyzing men and women to-gether.
The CSA of the median nerve in the forearm was larger in men than in women (p < 0.001; table 6). The difference persisted when controlling for body habitus and training status (β = 1.4; p = 0.044). Men also had greater thickness of the APB muscle, biceps brachii muscle and quadriceps muscle compared with women (table 6), which persisted when controlling for train-ing status (p < 0.0001 for APB and biceps muscles; p < 0.01 for quadriceps). No differences were found when analyzing trained and untrained individuals within the same gender.
The CSA of the median nerve in the forearm correlated with height (p < 0.001; fig. 3), which persisted after controlling for age and weight (β = 8.4; p < 0.001). The CMAP amplitude of the EDB muscle correlated with muscle thickness (r = 0.3; p = 0.048). We found no correlation between CSA of the musculocutaneous nerve and CMAP amplitude, CMAP area or HHD value of the biceps muscle. The multivariable analysis of the CMAP amplitude and muscle strength and muscle thickness did not show a relationship either (data not shown).
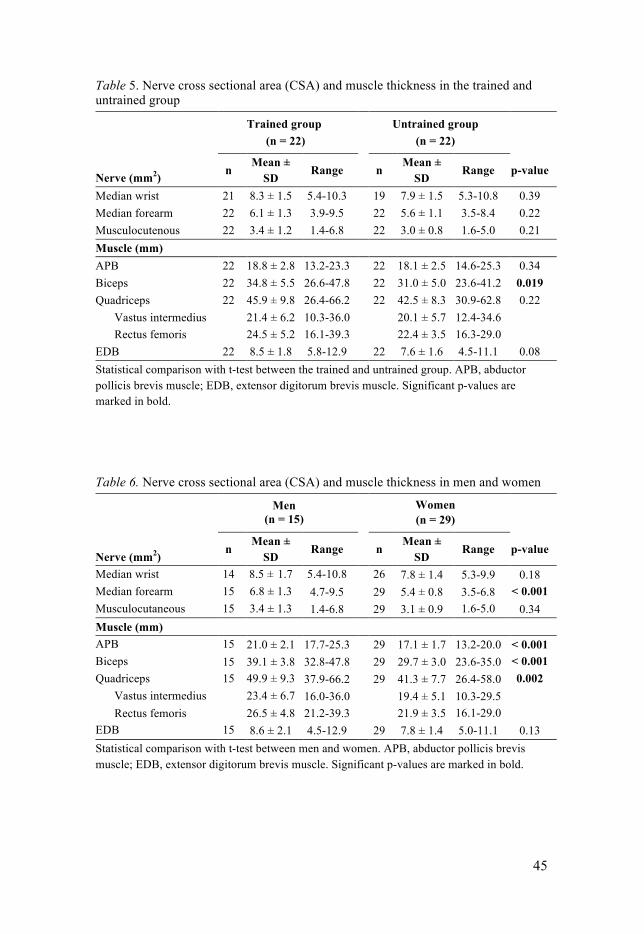
45
Table 5. Nerve cross sectional area (CSA) and muscle thickness in the trained and untrained group
Nerve (mm2)
Trained group (n = 22)
Untrained group
(n = 22)
n Mean ±
SD Range n
Mean ± SD
Range p-value
Median wrist 21 8.3 ± 1.5 5.4-10.3 19 7.9 ± 1.5 5.3-10.8 0.39 Median forearm 22 6.1 ± 1.3 3.9-9.5 22 5.6 ± 1.1 3.5-8.4 0.22 Musculocutenous 22 3.4 ± 1.2 1.4-6.8 22 3.0 ± 0.8 1.6-5.0 0.21 Muscle (mm) APB 22 18.8 ± 2.8 13.2-23.3 22 18.1 ± 2.5 14.6-25.3 0.34 Biceps 22 34.8 ± 5.5 26.6-47.8 22 31.0 ± 5.0 23.6-41.2 0.019 Quadriceps 22 45.9 ± 9.8 26.4-66.2 22 42.5 ± 8.3 30.9-62.8 0.22
Vastus intermedius 21.4 ± 6.2 10.3-36.0 20.1 ± 5.7 12.4-34.6 Rectus femoris 24.5 ± 5.2 16.1-39.3 22.4 ± 3.5 16.3-29.0
EDB 22 8.5 ± 1.8 5.8-12.9 22 7.6 ± 1.6 4.5-11.1 0.08 Statistical comparison with t-test between the trained and untrained group. APB, abductor pollicis brevis muscle; EDB, extensor digitorum brevis muscle. Significant p-values are marked in bold.
Table 6. Nerve cross sectional area (CSA) and muscle thickness in men and women
Nerve (mm2)
Men (n = 15)
Women (n = 29)
n Mean ±
SD Range
n
Mean ± SD
Range p-value
Median wrist 14 8.5 ± 1.7 5.4-10.8 26 7.8 ± 1.4 5.3-9.9 0.18 Median forearm 15 6.8 ± 1.3 4.7-9.5 29 5.4 ± 0.8 3.5-6.8 < 0.001 Musculocutaneous 15 3.4 ± 1.3 1.4-6.8 29 3.1 ± 0.9 1.6-5.0 0.34 Muscle (mm) APB 15 21.0 ± 2.1 17.7-25.3 29 17.1 ± 1.7 13.2-20.0 < 0.001 Biceps 15 39.1 ± 3.8 32.8-47.8 29 29.7 ± 3.0 23.6-35.0 < 0.001 Quadriceps 15 49.9 ± 9.3 37.9-66.2 29 41.3 ± 7.7 26.4-58.0 0.002
Vastus intermedius 23.4 ± 6.7 16.0-36.0 19.4 ± 5.1 10.3-29.5 Rectus femoris 26.5 ± 4.8 21.2-39.3 21.9 ± 3.5 16.1-29.0
EDB 15 8.6 ± 2.1 4.5-12.9 29 7.8 ± 1.4 5.0-11.1 0.13 Statistical comparison with t-test between men and women. APB, abductor pollicis brevis muscle; EDB, extensor digitorum brevis muscle. Significant p-values are marked in bold.
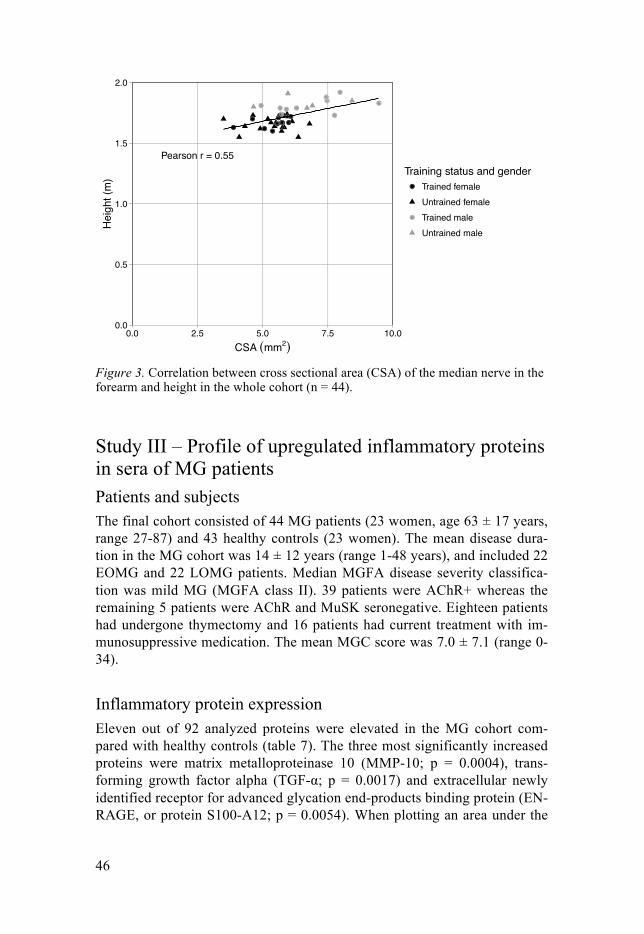
46
Figure 3. Correlation between cross sectional area (CSA) of the median nerve in the forearm and height in the whole cohort (n = 44).
Study III – Profile of upregulated inflammatory proteins in sera of MG patients Patients and subjects The final cohort consisted of 44 MG patients (23 women, age 63 ± 17 years, range 27-87) and 43 healthy controls (23 women). The mean disease dura-tion in the MG cohort was 14 ± 12 years (range 1-48 years), and included 22 EOMG and 22 LOMG patients. Median MGFA disease severity classifica-tion was mild MG (MGFA class II). 39 patients were AChR+ whereas the remaining 5 patients were AChR and MuSK seronegative. Eighteen patients had undergone thymectomy and 16 patients had current treatment with im-munosuppressive medication. The mean MGC score was 7.0 ± 7.1 (range 0-34).
Inflammatory protein expression Eleven out of 92 analyzed proteins were elevated in the MG cohort com-pared with healthy controls (table 7). The three most significantly increased proteins were matrix metalloproteinase 10 (MMP-10; p = 0.0004), trans-forming growth factor alpha (TGF-"; p = 0.0017) and extracellular newly identified receptor for advanced glycation end-products binding protein (EN-RAGE, or protein S100-A12; p = 0.0054). When plotting an area under the
Pearson r = 0.55
0.0
0.5
1.0
1.5
2.0
0.0 2.5 5.0 7.5 10.0CSA (mm2)
Hei
ght (
m) Training status and gender
Trained femaleUntrained femaleTrained maleUntrained male
47
curve figure for these three proteins, MMP-10 had the strongest association with MG, with an area of 0.76. The PCA indicated a tendency to clustering in healthy controls, but no clear separation between the groups was seen due to greater dispersion in the MG cohort (data not shown).
Other significantly increased levels of inflammatory proteins included nerve growth factor beta (β–NGF), cytokines IL-6, IL-8, IL-10 and IL-17A and C as well as chemokines C-C motif ligand 19 (CCL19) and C-X-C motif ligand 1 (CXCL1).
There was a positive correlation between disease duration and MMP-10 (r = 0.416; p = 0.0050) as well as CXCL-1 (r = 0.310; p = 0.040).
None of the proteins had a lower expression in the MG group compared with HC. No correlation was seen between protein expression and clinical MGC score, and no difference was found between men and women.
Table 7. Significantly elevated proteins in MG patients
Protein p-value
MMP-10 0.0004 TGF-α 0.0017 EN-RAGE (Protein S100-A12) 0.0054 β -NGF 0.0133 IL-6 0.0220 IL-8 0.0220 CCL19 0.0220 IL-17C 0.0256 CXCL1 0.0256 IL-10 0.0256 IL-17A 0.0348 MMP-10, metalloproteinase 10; TGF-α, transforming growth factor alpha; EN-RAGE, extracellular newly identified receptor for ad-vanced glycation end-products binding protein; β-NGF, nerve growth factor beta; IL, interleukin; CCL19, C-C motif ligand 19; CXCL1, C-X-C motif ligand 1.
In the subgroup analysis, MMP-10 and CXCL1 had a higher expression in EOMG patients (p = 0.0092 and 0.033, respectively), whereas brain-derived neurotrophic factor (BDNF) had a higher expression in the LOMG group (p = 0.0318). Significantly higher levels of three proteins were found in the patients with thymoma compared with patients with thymic hyperplasia: IL-8 (p = 0.011), IL-6 (p = 0.0123) and EN-RAGE (p = 0.0174). No difference in protein expression was found in the subgroup analyses of immunosup-pressive medication or previous thymectomy (data not shown).
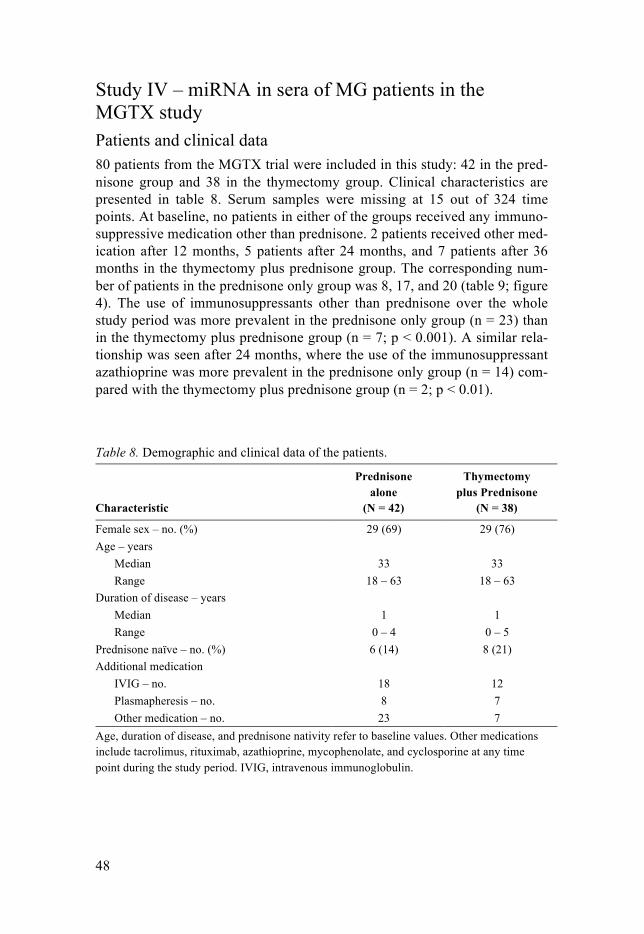
48
Study IV – miRNA in sera of MG patients in the MGTX study Patients and clinical data 80 patients from the MGTX trial were included in this study: 42 in the pred-nisone group and 38 in the thymectomy group. Clinical characteristics are presented in table 8. Serum samples were missing at 15 out of 324 time points. At baseline, no patients in either of the groups received any immuno-suppressive medication other than prednisone. 2 patients received other med-ication after 12 months, 5 patients after 24 months, and 7 patients after 36 months in the thymectomy plus prednisone group. The corresponding num-ber of patients in the prednisone only group was 8, 17, and 20 (table 9; figure 4). The use of immunosuppressants other than prednisone over the whole study period was more prevalent in the prednisone only group (n = 23) than in the thymectomy plus prednisone group (n = 7; p < 0.001). A similar rela-tionship was seen after 24 months, where the use of the immunosuppressant azathioprine was more prevalent in the prednisone only group (n = 14) com-pared with the thymectomy plus prednisone group (n = 2; p < 0.01).
Table 8. Demographic and clinical data of the patients.
Characteristic
Prednisone alone
(N = 42)
Thymectomy plus Prednisone
(N = 38)
Female sex – no. (%) 29 (69) 29 (76) Age – years
Median 33 33 Range 18 – 63 18 – 63
Duration of disease – years Median 1 1 Range 0 – 4 0 – 5
Prednisone naïve – no. (%) 6 (14) 8 (21) Additional medication
IVIG – no. 18 12 Plasmapheresis – no. 8 7 Other medication – no. 23 7
Age, duration of disease, and prednisone nativity refer to baseline values. Other medications include tacrolimus, rituximab, azathioprine, mycophenolate, and cyclosporine at any time point during the study period. IVIG, intravenous immunoglobulin.

49
Table 9. Patients receiving immunosuppressive medication
Drug
Prednisone alone
(n = 42)
Thymectomy plus Prednisone
(n = 38)
0 12 24 36 0 12 24 36
Azathioprine 0 6 14 17 0 1 2 3 Azathioprine + Cyclosporine 0 0 1 0 0 0 0 0 Azathioprine + Tacrolimus 0 1 0 0 0 0 1 1 Cyclosporine 0 1 1 1 0 0 0 0 Mycophenolate 0 0 0 1 0 0 0 1 Rituximab 0 0 0 1 0 0 0 0 Rituximab + Tacrolimus 0 0 0 0 0 0 1 1 Tacrolimus 0 0 1 0 0 1 1 1 Number of patients receiving immunosuppressive medication at baseline, 12 months, 24 months and 36 months after baseline in the two treatment groups.
miRNA analysis One sample had a hemolysis ΔCT(hemolysis) > 7, and was excluded from further analysis. 34 serum samples were excluded due to miRNA levels below the detection limit (CT > 38) according to the guidelines on miRNA data analy-sis provided in GenEx software.
Longitudinal analysis of circulating miR-150-5p and miR-21-5p expression in the thymectomy group Levels of miR-150-5p were reduced 24 months after thymectomy (5.2 ± 1.2), compared with baseline (6.2 ± 1.3; figure 4; p = 0.0011). This reduction was accompanied by an improved QMG score (p < 0.001) and a reduced prednisone dosage (p < 0.001). Levels were reduced in 21 patients after 24 months, whereas 5 patients did not have reduced levels, 10 patients had un-detectable levels due to bad serum samples, and 4 samples were missing. Levels of miR-150-5p were reduced in 11 patients after 36 months compared with baseline, 14 patients did not have reduced levels, 5 patients had unde-tectable levels, and 1 sample was missing. The pattern of reduced levels of miR-150-5p 24 months post baseline was also seen in patients aged < 50 years (p = 0.0058) as well as in female patients (p = 0.01). Levels of miR-21-5p were not lower at 24 months post baseline, but were instead higher at 36 months post baseline (p = 0.005), with the same pattern seen in patients aged < 50 years (p = 0.0082) as well as in female patients (p = 0.02).
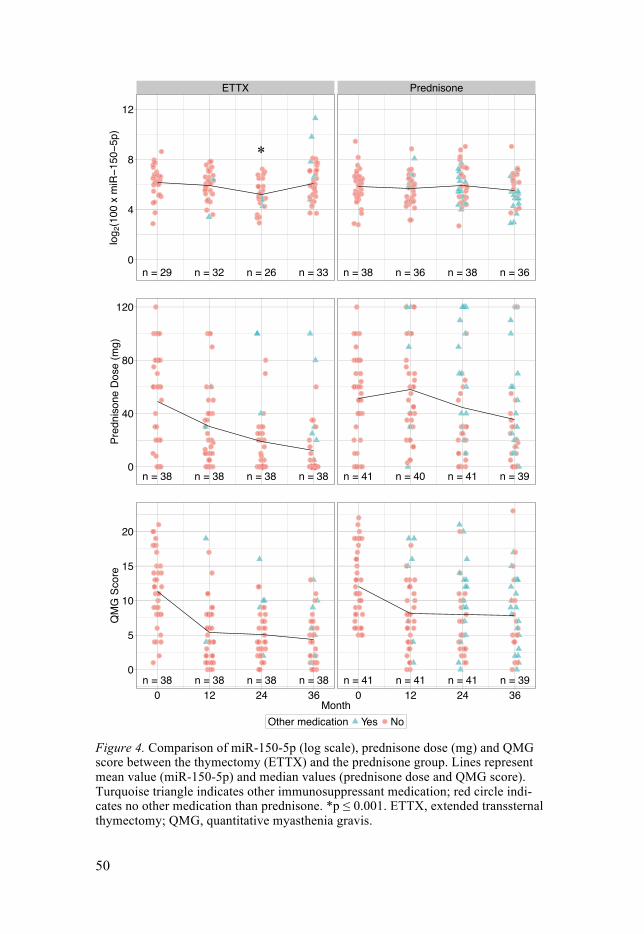
50
Figure 4. Comparison of miR-150-5p (log scale), prednisone dose (mg) and QMG score between the thymectomy (ETTX) and the prednisone group. Lines represent mean value (miR-150-5p) and median values (prednisone dose and QMG score). Turquoise triangle indicates other immunosuppressant medication; red circle indi-cates no other medication than prednisone. *p 0 0.001. ETTX, extended transsternal thymectomy; QMG, quantitative myasthenia gravis.
ETTX
ETTX
ETTX
Prednisone
Prednisone
Prednisone
n = 29 n = 32 n = 26 n = 33
n = 38 n = 38 n = 38 n = 38
n = 38 n = 38 n = 38 n = 38
n = 38 n = 36 n = 38 n = 36
n = 41 n = 40 n = 41 n = 39
n = 41 n = 41 n = 41 n = 39
0
4
8
12
0
40
80
120
0
5
10
15
20
0 12 24 36 0 12 24 36Month
log 2
(100
x m
iR!1
50!5
p)Pr
edni
sone
Dos
e (m
g)Q
MG
Sco
re
Other medication Yes No
*
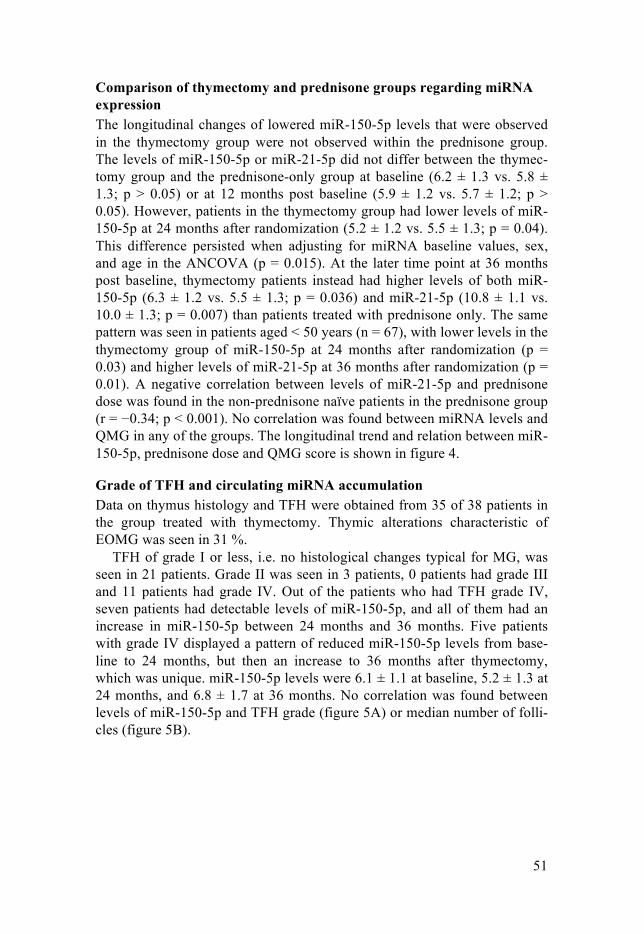
51
Comparison of thymectomy and prednisone groups regarding miRNA expression The longitudinal changes of lowered miR-150-5p levels that were observed in the thymectomy group were not observed within the prednisone group. The levels of miR-150-5p or miR-21-5p did not differ between the thymec-tomy group and the prednisone-only group at baseline (6.2 ± 1.3 vs. 5.8 ± 1.3; p > 0.05) or at 12 months post baseline (5.9 ± 1.2 vs. 5.7 ± 1.2; p > 0.05). However, patients in the thymectomy group had lower levels of miR-150-5p at 24 months after randomization (5.2 ± 1.2 vs. 5.5 ± 1.3; p = 0.04). This difference persisted when adjusting for miRNA baseline values, sex, and age in the ANCOVA (p = 0.015). At the later time point at 36 months post baseline, thymectomy patients instead had higher levels of both miR-150-5p (6.3 ± 1.2 vs. 5.5 ± 1.3; p = 0.036) and miR-21-5p (10.8 ± 1.1 vs. 10.0 ± 1.3; p = 0.007) than patients treated with prednisone only. The same pattern was seen in patients aged < 50 years (n = 67), with lower levels in the thymectomy group of miR-150-5p at 24 months after randomization (p = 0.03) and higher levels of miR-21-5p at 36 months after randomization (p = 0.01). A negative correlation between levels of miR-21-5p and prednisone dose was found in the non-prednisone naïve patients in the prednisone group (r = −0.34; p < 0.001). No correlation was found between miRNA levels and QMG in any of the groups. The longitudinal trend and relation between miR-150-5p, prednisone dose and QMG score is shown in figure 4.
Grade of TFH and circulating miRNA accumulation Data on thymus histology and TFH were obtained from 35 of 38 patients in the group treated with thymectomy. Thymic alterations characteristic of EOMG was seen in 31 %.
TFH of grade I or less, i.e. no histological changes typical for MG, was seen in 21 patients. Grade II was seen in 3 patients, 0 patients had grade III and 11 patients had grade IV. Out of the patients who had TFH grade IV, seven patients had detectable levels of miR-150-5p, and all of them had an increase in miR-150-5p between 24 months and 36 months. Five patients with grade IV displayed a pattern of reduced miR-150-5p levels from base-line to 24 months, but then an increase to 36 months after thymectomy, which was unique. miR-150-5p levels were 6.1 ± 1.1 at baseline, 5.2 ± 1.3 at 24 months, and 6.8 ± 1.7 at 36 months. No correlation was found between levels of miR-150-5p and TFH grade (figure 5A) or median number of folli-cles (figure 5B).
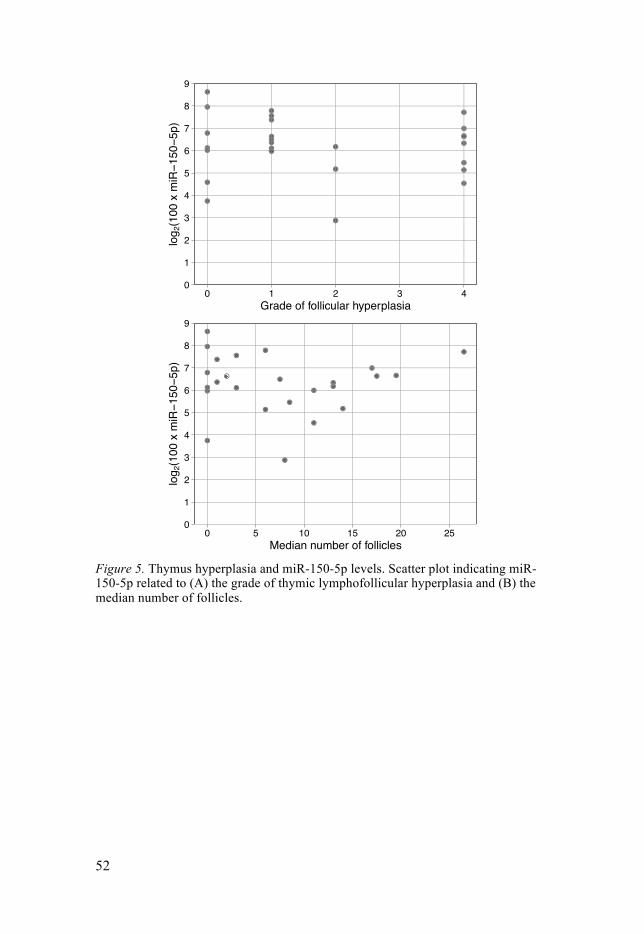
52
Figure 5. Thymus hyperplasia and miR-150-5p levels. Scatter plot indicating miR-150-5p related to (A) the grade of thymic lymphofollicular hyperplasia and (B) the median number of follicles.
0
1
2
3
4
5
6
7
8
9
0
1
2
3
4
5
6
7
8
9
0 1 2 3 4
0 5 10 15 20 25
Grade of follicular hyperplasia
Median number of follicles
log 2
(100
x m
iR!1
50!5
p)lo
g 2(1
00 x
miR!1
50!5
p)
53
Discussion
Neurophysiological biomarkers CMAP as a biomarker for muscle training The main aim of this thesis was to investigate possible biomarkers for neu-romuscular function and MG, both for muscle training and for treatment response and disease state.
Our finding that trained individuals have higher CMAP amplitudes in biceps brachii (in men) and rectus muscles femoris (in women) are in line with pre-vious studies97. The higher CMAP indicates that hypertrophy most likely is the prominent response to HRST, rather than improved motor control or contraction apparatus. This is further strengthened by the correlation be-tween muscle strength and CMAP amplitude of the biceps muscle in the trained group.
The isometric muscle strength in the biceps muscle was greater in both trained men and women compared with untrained individuals of the same sex, which is in line with the higher CMAP amplitudes (although only in men) and greater muscle thickness as assessed with ultrasound. The fact that isometric muscle strength, CMAP amplitude and muscle thickness of the biceps muscle tend to be greater in trained individuals indicates that these parameters all represent muscle status, and that CMAP amplitude can be used as a biomarker for muscle strength. The fact that this relationship was only seen for the biceps muscle could be because proximal muscles often are the focus of HRST. Nonetheless, these data are in line with previous studies stating that leg muscles do not respond as well as arm muscles to HRST95,108. A reason that the same relationship between CMAP amplitude and isometric muscle strength was not found in the quadriceps muscle could be that these proximal leg muscles are passively trained to a much higher extent in every-day life than the biceps muscle, since they are used for walking, running and cycling, resulting in a smaller difference when comparing with individuals who perform HRST.
The differences regarding isometric muscle strength between men and women were largely expected. The muscle force in all examined muscles was greater in men than in women within the trained cohort in study I, and all muscles except EDB were thicker in men than women in the whole co-

54
hort in study II. These differences are possibly due to larger type I muscle fibers in men. Also, women have approximately 45 % smaller muscle fiber CSA and posses around 50 % of the strength of men in the biceps muscle144. This, together with the fact that men and women probably focus on different muscle groups when performing HRST, serves as an explanation as to why the findings were most prominent for the biceps muscle.
When men and women in study I were analyzed together, trained individ-uals had higher CMAP amplitudes of both the biceps brachii and the quadri-ceps muscles, and greater muscle strength of the biceps muscle. A similar result was found for the strength of the quadriceps muscle, although non-significant (p = 0.55). As discussed above, the reason for this might be due to the fact that men and women differ in CMAP response due to different training regimens, but it could also be due to loss of statistical power when dividing the cohort according to sex. However, the finding that the biceps muscle was thicker in trained individuals when men and women in study II were analyzed together proves that HRST has a considerable effect on mus-cle hypertrophy.
Effect of HRST on peripheral nerves Study II is the first study to examine the potential effects of HRST on the CSA of peripheral nerves. We found no difference in nerve CSA between trained and untrained individuals for any of the examined nerve sites. As stated, one previous case study found nerve remodeling after strenuous exer-cise109. The CSA values of the median nerve were enlarged 24 hours after a marathon race, and were indicative of median nerve neuropathy. Altered nerve CSAs were found in the ulnar nerve, as well as the tibial and sural nerves of the lower extremities. The reason that we did not find enlarged CSA of nerves in study II might of course be due to the fact that endurance running is a completely different training form than HRST. Furthermore, the CSA in the study by Kerasnoudis was only increased at wrist level, and was unchanged (and even decreased) at other levels and nerve sites, which makes the results somewhat contradictory. Also, the results are presented in cm2 with only 2 decimals, as opposed to mm2, which makes the results hard to compare, as the CSA is relatively small.
Although HRST did not have an effect on nerve CSA, men had larger CSA of the median nerve in the forearm compared with women, which is in line with previous studies103,145. Nevertheless, results indicating no difference between men and women have also been published102. That we did not see the same difference between trained and untrained when analyzing men and women separately is probably due to loss of statistical power when sub-grouping, resulting in fewer subjects in each group.
The finding of a correlation between the CSA of the median nerve in the forearm and height is in line with previous studies, but the scientific litera-

55
ture is somewhat ambiguous when assessing the relationship between nerve CSA and other factors. Correlations between median nerve CSA at the wrist and BMI, weight, and age (although not height) have been reported, as well as between nerve CSA and BMI for several other nerves103. Correlation be-tween height and weight with nerve CSA of the median nerve has also been reported146, but without any apparent effect of age or BMI. On the contrary, another study found correlations between nerve CSA and age for several nerves, both in upper and lower extremities147, which is actually the opposite of a study reporting decreasing CSA of the median nerve in the axilla with decreasing age102. Yet another study found a stronger correlation between nerve CSA and BMI and weight, with no relationship to age and height100. The lack of uniform results implicates that this research area is not yet fully understood, and it is not unlikely that a lot of results actually are false posi-tives.
The musculocutaneous nerve is not as thoroughly studied as the median nerve. However, the results from study II are in line with a previous study, where no correlation was found between nerve CSA and height, weight, BMI or age100. A somewhat surprising finding was that the mean CSA values of the musculocutaneous from study II are notably smaller compared with two previous studies100,148. Different ultrasound devices, measurement sites and use of zoom functions are all possible explanations for these differences in CSA. Values are known to differ between labs, which is why it is im-portant for each ultrasound laboratory to have its’ own reference values102.
The differences in muscle thickness between men and women were most-ly expected. As stated previously91,92, proximal arm muscles have a greater response to HRST, and the finding that the biceps brachii muscle was thicker in trained individuals, even though men and women were analyzed together, supports this. Once again, we did not find any differences when analyzing men and women separately, probably again due to loss of statistical power.
Enlargement of peripheral nerves as an acute or subacute result of exer-cise, could result in misdiagnosis of neuropathies. The results from study II provide valuable data that long term effects of regular HRST does not affect ultrasound diagnostics of neuropathies.
Role of CMAP and ultrasound in exercise studies Physical exercise in MG has been subject to a lot of debate, and the general traditional recommendation has been that MG patients should not perform physical exercise. A few case studies have been published, with varying results (although all patients managed to perform physical exercise on a reg-ular basis, and also experienced wellness, except for one patient, who partic-ipated in an endurance marathon)149-151. Other studies mainly focused on respiratory training152-154, but one study examined the effect of HRST155, and concluded that HRST is safe and improves muscle strength in mild MG.

56
However, more research is needed as scientific consensus in the area is lack-ing.
As stated previously, because of the fluctuations in fatigability in MG pa-tients, muscle status cannot be assessed by just measuring muscle strength. For this reason, CMAP amplitude might prove to be valuable in future exer-cise studies in patients with neuromuscular disorders. A prospective inter-ventional study on physical exercise in MG patients has recently been pub-lished, which provides evidence that physical exercise according to general recommendations for healthy adults is safe for MG patients, and contributes to well-being, with no sign of disease deterioration156. This is somewhat of a paradigm shift, since MG patients traditionally have been advised not to perform physical exercise, due to the subsequent worsening of muscle fa-tigue. CMAP amplitudes and muscle strength were measured before and after a 12-week training period, and the CMAP amplitude increased in the biceps and quadriceps muscles after the training period, whereas no change in muscle strength was seen (measured by HHD). However, resistance weights increased for the biceps curls and leg extension exercises. This indi-cates that a physiological adaption occurred in the muscles, but perhaps not detectable with HHD. Still, if the increase in resistance weights were only due to improved technique, and not due to improved muscle force, an in-crease in CMAP amplitudes of the same muscles probably wouldn’t be seen.
In another similar, prospective, interventional study157, the muscle func-tion of eleven MG patients improved after performing HRST for 12 weeks. Once again, CMAP and HHD measurements were performed, although this time ultrasound was also used to evaluate the muscle response. The reason for this was that muscle thickness108,158 and CSA86 of muscles increases in response to HRST, although somewhat dependent on the type of training159. In this interventional study of MG patients, an increase of CMAP amplitude, isometric muscle force (assessed with HHD) and muscle thickness (meas-ured with ultrasound) was seen in the quadriceps muscle. However, contrary to previous results, no change was seen in the biceps muscle. This might be due to the fact that there was a slight female predominance in the cohort, and as seen in study I, trained men have higher CMAP amplitudes of biceps, whereas trained women have larger CMAP amplitudes in quadriceps. None-theless, the cohort was quite small and definite conclusions cannot be drawn from such a small sample.
It is however important to remember that the initial morphological changes in muscles seen early on might be signs of edema or muscle dam-age, rather than hypertrophy160. Magnetic resonance imaging is considered the gold standard when assessing muscle mass161, and muscle thickness as measured with ultrasound correlates with muscle CSA assessed with MRI162. Further, muscle CSA do not differ when measured with ultrasound compared with MRI163. Therefore, ultrasound can be considered a satisfactory option
57
when assessing muscle mass, also being more accessible, easier to use and less expensive.
Drawbacks The CMAP recording technique can be subject to inter-rater variability due to different placements of the active and stimulating electrode. However, we applied a standardized placement of the electrodes, and all examinations were performed by one examiner, which minimized variability between measurements. The biceps muscle is also considered suitable for measuring CMAP, since its motor points are uniform due to the muscle architecture164. Another possible drawback is that the untrained group had a slightly higher BMI, which could have had an effect on the lower CMAP in the untrained group, since we found a negative correlation between higher BMI and lower CMAP. Nevertheless, if this was true, the same relationship should have been observed in the other muscles, and not only the biceps. Furthermore, the differences in BMI were not significant.
Another possible drawback when assessing muscle force is the use of isometric muscle force as an outcome measurement – isometric muscle con-traction is not a common use of muscle force during everyday life, and most often it is not involved in HRST either, which might explain why there were no differences in muscle strength in the interventional studies of MG pa-tients. Other outcomes, such as one-repetition maximum, might be a more physiological measurement of muscle force, but are probably ill suited for MG patients.
A drawback in study II was that the untrained group was older than the trained group. Since several studies have found a positive correlation be-tween age and nerve CSA, this could mask a true difference in nerve CSA between the two groups. The trained group was younger, and if HRST caus-es an enlargement of nerve CSA, the nerve CSA in the untrained group could match it due to higher age. The lack of a correlation between nerve CSA and the previously measured parameters CMAP amplitude, area, or muscle strength may be due to the fact that the ultrasound values were ob-tained at a different occasion than the neurophysiological and muscle meas-urements, or because the study group was too small. Ideally, all measure-ments should be obtained on the same occasion. Such a correlation, between the thickness of the EDB muscle and CMAP amplitude of the fibular nerve, has previously been reported165. Still, the CMAP is a measurement of the muscle response to nerve stimuli, and the nerve CSA is affected by many physiological parameters, and does not necessarily correlate with nerve func-tion or muscle thickness. Another drawback is the predominance of females in the untrained group, which makes the groups somewhat unequal and more difficult to compare.
58
When examining both CMAP and HHD measurements as biomarkers, the ideal study design would have been a prospective, randomized, single-blinded interventional study, where two groups were examined: one group which performed HRST, and one group not performing any physical exer-cise (or ideally, performing “placebo training”, which is hard to design). Subjects would be randomized to one of the groups, and a blinded rater would examine the subjects before and after the training period, not knowing which group the subject belonged to. In study I and II, the use of a blinded examiner could have made the results more reliable. A French multi-center study is ongoing at the moment, where MG patients will be randomized to either performing rowing exercise for 3 months, or receiving usual care with no additional treatment166. The outcome of the study will primarily be quali-ty of life, but also cardiovascular and physical measurements, as well as muscle force assessed with an isokinetic dynamometer, and inflammatory cytokines.
Circulating biomarkers in MG Inflammatory proteins The aim of study III was to explore the profile of inflammatory proteins in MG patients, and eleven proteins were found to be elevated, where MMP-10, TGF-α and EN-RAGE were the most significant. MMP-10 had the strongest association with MG. Matrix metalloproteinases essentially break down the extracellular matrix enzymatically, degrading collagens, fibron-ectin and gelatins in processes related to normal physiological function as well as disease. MMP-10 has been found to be elevated and related to prog-nosis in sepsis, a severe condition with systemic inflammation167. One study found that the level of MMP-10 secreted by microglia and macrophages was increased in experimental autoimmune encephalomyelitis (EAE)168, which is an animal model for multiple sclerosis. This model has many similarities to EAMG, in the sense that they respond in the same way to immunomodula-tors169.
TGF-α is a growth factor that is part of the epidermal growth factor fami-ly. It is important for epithelial proliferation and differentiation, and is pro-duced by macrophages, neurons, astrocytes and keratinocytes. It has im-portant neurotrophic characteristics in both the developing brain and mature central nervous system (CNS), and has also been shown to stimulate prolif-eration, migration and differentiation in a rat model of Parkinson’s dis-ease170. It has also been suggested that TGF-α reduces the size of an infarct following stroke in mice171. It appears to have no effect on peripheral nerve regeneration after injury172. Further effects of the neurotrophic properties of TGF-α in the peripheral nervous system (PNS) are not known.

59
EN-RAGE (or S100-A12, as it’s also called) is a protein that is involved in cell cycle progression and differentiation, just like MMP-10 and TGF-α. It has pro-inflammatory properties, and is an activator for mast cells and mon-ocytes, and additionally inhibits MMPs. It is expressed by monocytes and macrophages in several inflammatory disorders, and is upregulated by IL-6 in macrophages173. IL-6, as stated previously, is an inflammatory cytokine which is upregulated in thymic epithelial cells in MG patients It is a ligand for the receptor for advanced end products (RAGE), which is a pro-inflammatory receptor involved in diabetic neuropathy, cardiovascular dis-orders and neuroinflammatory and neurodegenerative disorders174,175. Acti-vation of the receptor causes secretion of cytokines and has pro-inflammatory effects on lymphocytes, neutrophils and endothelial cells176. β-NGF, a protein belonging to the neurotrophin family, is released by T
cells, B cells, mast cells, eosinophils and macrophages, and is part of a com-plex network of inflammation. It is upregulated by inflammatory cytokines, activates inflammatory cells and stimulates chemotaxis and further release of cytokines. Further, it is important for the survival and development of neu-rons in both the PNS and the CNS177.
Interleukins are signaling molecules of the immune system, and several interleukins are linked to autoimmune diseases including MG. IL-6 and IL-10 are produced by activated B and T cells178. IL-6 promotes antibody pro-duction, and affects the induction of regulatory T cells to pathogenic Th1 cells42. Furthermore, blocking of IL-6 can actually suppress the development of EAMG41. IL-6 stimulates development of Th17 cells, which in turn re-lease IL-17A42. IL-17A is increased in plasma of MG patients, and levels seem to correlate with disease severity43 and to the AChR antibody titer44. However, IL-17C has not previously been linked to MG. It is important for the development of EAE, and regulates the autoimmune response through its receptor, IL-17E, which is expressed in Th17 cells179. IL-8, another pro-inflammatory cytokine, is also increased in MG patients45. It attracts neutro-phils and T cells, and has been linked to the occurrence of thymoma in MG patients46. That IL-6, IL-8 and IL-17A were upregulated was mostly ex-pected, since all of these proteins have strong connections with MG. Thus, our findings further validate the importance of these inflammatory cytokines in MG and emphasize the possibility that they could serve as targets for more specific novel treatments in subgroups of MG.
CCL19 is secreted by medullary thymic epithelial cells, and seems to promote migration of CD4+ or CD8+ thymocytes toward the medullary zone180, but it is also involved in exporting mature thymocytes towards the periphery181. Further, it is upregulated in the thymus of MG patients with thymic hyperplasia. The chemokine CXCL1 has not been linked to MG pre-viously, but shares its receptor (CXCR2) with IL-8, which is present on mast cells, neutrophils, basophils and T cells182. CXCL1 stimulates chemotaxis of neutrophils and is produced by macrophages and neutrophils183,184. CXCR2
60
seems to play an important part in inflammation, since CXCR2 knock-out mice display defect neutrophil recruitment in wounds and delayed wound healing185. Other proteins of the CCL and CXCL families have previously been linked to MG, such as CXCL13 and CCL2134. CCL21 is believed to drive the sensitization of naïve B cells towards the AChR. CCL19, together with CCL21, most certainly are important for the inflammatory response in MG, and their expression is decreased in patients treated with glucocorti-coids180.
EOMG patients had significantly higher levels of MMP-10 and CXCL1 compared with LOMG patients. On the contrary, BDNF, a neurotrophic protein secreted from neurons, was almost four times as high in LOMG pa-tients. A similar relationship regarding BDNF was seen when comparing patients who had undergone thymectomy with those who had not, which is expected as patients with LOMG rarely are treated with thymectomy. BDNF is essential for differentiation and neuron growth in the CNS and PNS. Pro-inflammatory cytokines reduce the expression of BDNF genes186, but in-flammatory cells can also produce BDNF, which may have a neuroprotective role during inflammation187. The difference in BDNF levels between EOMG and LOMG patients might be due to the fact that the pathophysiology in EOMG is more driven by inflammation (which is supported by concomitant autoimmune disorders, thymic hyperplasia etc.), thereby causing a reduction of BDNF. Further, BDNF is important in late-phase long-term potentiation and long-term memory storage188,189. A small number of MG patients actual-ly suffer spatial, logical and visual memory deficits190. The reason for this is not known, but impaired cholinergic signaling in the CNS is possible, since AChR antibodies also are found in the cerebrospinal fluid191. However, the central nicotinic AChR have a different structure than the ones found on skeletal muscle, and they do not bind α-bungarotoxin, which is why it not very likely that the AChR antibodies affect AChRs in the brain192. However, cognitive symptoms seems to improve following plasmapheresis190, indicat-ing that there is some circulating entity affecting the brain. Impaired expres-sion of BDNF may play a role in this.
miRNA Study IV is the first ever randomized, prospective, single-blinded study to examine the longitudinal effect of thymectomy on miRNAs miR-150-5p and miR-21-5p. Since these two miRNAs have previously been shown to be elevated in AChR+ MG patients, we focused on these when performing study IV. The main finding that the reduction of miR-150-5p 24 months after thymectomy was accompanied by an improved QMG score, implies that a longitudinal reduction in miR-150-5p accompanies clinical improvement after thymectomy, especially in female patients aged < 50 years. This is in line with a previous study, where levels of miR-150-5p were reduced in a

61
cohort of 9 female AChR+ MG patients who had undergone thymectomy127. However, as stated previously, a follow-up study did not find a correlation between miR-150-5p levels and MGC score, but on the other hand, these patients were only analyzed at one time point128. Our findings in study IV strengthen the hypothesis that miR-150-5p can be used as a disease specific biomarker in AChR+ MG. The temporal difference between reductions in miRNA levels and QMG score indicates that the immunological changes from the thymectomy occur over a longer time period, compared with clini-cal improvement. That the reduction of miR-150-5p was only seen in the thymectomy group emphasize the effect thymectomy has on the immune response, compared with only prednisone treatment.
The finding that the levels of miR-150-5p were not decreased 36 months post baseline in the thymectomy group is somewhat puzzling. Ideally, the levels should be continually declining and preferably staying low, in con-cordance with clinical QMG score. All the patients with TFH grade IV had an increase in miR-150-5p between 24 and 36 months, but other than that we found no other common denominator for these patients. As seen in figure 4, the two patients who had the highest levels of miR-150-5p also had ongoing treatment with immunosuppressants other than prednisone. The effect of physical exercise on both miR-150-5p and miR-21-5p in MG patients has been examined in a study156, and interestingly, these miRNA seem to in-crease following a single training session, indicating an inflammatory re-sponse to exercise. However, miR-150-5p and miR-21-5p both decreased after the whole training period of 12 weeks, indicating a more long-term, anti-inflammatory effect193, also seen in chronic obstructive pulmonary dis-ease194 or autoimmune disorders such as rheumatoid arthritis195 and multiple sclerosis196. In one patient, the level of miR-150-5p was instead increased after the training period, and similarly to the two outliers in the thymectomy group in study IV, this patient was treated with the immunomodulatory drug rituximab.
The finding that thymectomy did not have a profound effect on miR-21-5p is in line with previous studies, where miR-21-5p had a weaker associa-tion with MG compared with miR-150-5p. The use of immunomodulatory drugs other than prednisone was much more prevalent in the prednisone-only group, which of course could influence the results. Additionally, many patients initiated treatment with these drugs at the visit after 24 months, which might explain why levels of miR-150-5p and miR-21-5p were lower in the prednisone-only group after 36 months. On the other hand, the use of immunosuppressants was more prevalent in the prednisone-only group al-ready after 24 moths. That the levels of miR-150-5p were still lower in the thymectomy group strengthens the effect of thymectomy.
The negative correlation between miR-21-5p and prednisone dose in non-prednisone naïve patients in the prednisone-only group indicates that differ-ent miRNAs respond differently to various immunosuppressive treatments.

62
When taking into account the large effect of thymectomy on the inflammato-ry response, it’s not surprising that this relationship was not found in the whole cohort.
miR-150-5p is an immuno-miRNA that is important for the development, maturation, proliferation and survival of T cells197. During the maturing of T cells, a process where the thymus gland is very important, miR-150-5p is upregulated198, but as further differentiation of naïve T cells occurs, it is on the contrary downregulated129. As stated previously, regulatory T cells are important for development of immunological self-tolerance199. However, in MG, the function of Tregs is impaired200. It has been suggested that Tregs use extracellular vesicle-associated miRNAs to suppress T cell-mediated diseases, by inhibiting proliferation and cytokine secretion from Th1 cells201. The exact role of Tregs in the pathogenesis of MG is not yet known, but the number of impaired Tregs in EOMG seems to be increased15, and, even more interesting, both miR-150-5p and miR-21-5p are enriched in extracellular vesicles released by Tregs, compared with those released by Th1 and Th17 cells130. miR-150-5p has also been suggested as a candidate biomarker for patients with multiple sclerosis, an autoimmune disease of the central nerv-ous system, which has many similarities to MG202. In multiple sclerosis pa-tients, miR-150-5p in the CSF was increased compared with healthy con-trols, and decreased following treatment with immunosuppressants, which correlated with increased levels of miR-150-5p in plasma together with a corresponding change in immune cell number in CSF and plasma. This sug-gests that immune cells are the source of miR-150-5p.
miR-21-5p is also associated with other autoimmune disorders. Similar to miR-150-5p, miR-21-5p also is involved in T cell function203,204. Previous studies have found an increased expression in multiple sclerosis patients205, and it also seems to play an important part in the autoimmune response in type 1 diabetes206 and lupus erythematosus207.
Role of circulating biomarkers in MG The Olink Inflammation panel is commercially available, and one study has been published where MMP-10 was elevated in sera from inflammatory bowel disease patients compared with healthy controls208. No other study that focuses on autoimmune disorders has been published, but several of the proteins have been linked to other inflammatory diseases, and most likely they are markers of inflammation in general, and thus not disease specific for MG. This makes their potential role as biomarkers for MG somewhat limited – ideally a biomarker should be disease specific. Even though this is not the case, some of the elevated proteins might still be useful as biomarkers, or in understanding the pathogenesis of MG. The fact that we did not see a corre-lation between MGC score and elevated proteins could also limit the possi-bility to use these proteins as biomarkers. Nevertheless, this would have to

63
be examined in a longitudinal fashion, taking into account the clinical changes over time in relation to protein levels.
The issue of MG specificity of course is applicable to miR-150-5p and miR-21-5p as well. These are not necessarily disease specific for MG. When comparing MG patients with other autoimmune disease controls, such as Psoriasis, Addison’s and Crohn’s disease, levels of miR-150-5p were in-creased in MG patiens127, but as stated above, increased levels of miR-150-5p have been found in MS patients. Intriguingly, candidate protein bi-omarkers of the CXCL and MMP families have been found for MS as well209. In the case of miR-150-5p, there seems to be at least some specificity to inflammation or autoimmunity in both the central and peripheral nervous system. An advantage of miRNA compared with inflammatory cytokines and chemokines is their stability – protein-based biomarkers are more sensi-tive to degradation, and have less exact measurement protocols. This limits widespread use of protein-based biomarkers in everyday clinical practice and different laboratories. miRNA instead display very little biological variance in healthy subjects210. They appear to tolerate high RNAse concentration, boiling, freeze-thaw cycles, extended storage and pH variations, as well as extended storage211,212.
Due to the complexity of MG, with fluctuating symptoms and disease ac-tivity, as well as different subgroups with different pathophysiological mechanisms, it is not likely that one single biomarker will fulfill all needs for disease monitoring and therapeutic response. In line with this, MuSK+ MG patients display a completely different pattern of miRNA expression. The subgrouping of AChR+ MG patients in terms of EOMG and LOMG is not altogether clear, with the age cut off somewhat arbitrarily set at 40 or 50 years, despite (probably) different disease mechanisms and treatment. A suitable miRNA for defining which subgroup patients belong to would be of great use in clinical settings.
Another area in which miRNA might prove to be useful is therapeutics. Since miRNA possibly regulate many cellular processes, and many diseases display specific accumulation patterns, both mimicking and inhibiting the function of an endogenous miRNA are possible strategies for miRNA thera-peutics (by miRNA mimics and antagomirs, respectively)213. At the moment, there are ongoing clinical trials involving miRNA therapeutics for hepatitis C, several cancer forms, and diabetes type 2214.
Drawbacks In study III, the levels of the examined proteins are presented as normalized protein expression units (NPX), which is an arbitrary unit. This means that the protein levels cannot be compared with each other, or to the same protein in another assay. This is because different batches of antibodies are used, which is a drawback from a biomarker perspective, where a stable and easily

64
quantifiable expression is desired. Another drawback of study III is that many patients were treated with immunosuppressants, which most certainly affects the protein levels. The reason why we did not see significant differ-ences in protein levels between patients with and without immunosuppres-sion could be due to an insufficient number of patients in each subgroup, taking into account that different immunosuppressive agents were used at various doses during the disease course.
In study IV, the low number of prednisone-naïve patients at randomiza-tion is a drawback. It could however not be avoided due to the study design. Ideally, all patients should have been prednisone-naïve at baseline. That way, the effect of both thymectomy and prednisone treatment on disease progression and miRNA levels would be investigated in a better way. Since both prednisone treatment and thymectomy have an effect on the immune response, the results were most certainly affected by the fact that many pa-tients were treated with prednisone pre randomization. That the patients re-cruited to the MGTX study had to reach minimal manifestation status, de-fined as “no symptoms or functional limitations from myasthenia gravis, but there may be some weakness on examination of some muscles”, in fact makes the possibility for detecting clinical improvement much smaller than if patients would have been recruited and randomized at disease onset, with more severe symptoms and higher antibody titers. This was the design in the study published by Sabre et al.131, and as stated previously, a correlation between miRNA levels and clinical status was found, especially significant in the early stages of the disease.
The lack of prednisone naïveté probably also affected the lack of results regarding thymus histology and miRNA levels. In concordance with this, a recently published study found no relationship between clinical parameters and thymus histology in the MGTX trial215. A relationship between intra-thymic fat content and prednisone dose was seen, but with low predictive power. Once again, the lack of prednisone naïveté probably influenced the results, as extensive treatment with prednisone causes atrophy of the thymus, which was seen in many of these cases.
A drawback regarding miRNA as biomarkers is that non-overlapping sets of miRNAs have been reported for the same disease216, but this is probably a result of different methodological approaches by different research groups, highlighting the need for a standardized analytical method. Limited overlap of miRNA might also prove to be the case for MG, due to small cohorts because of the limited number of patients, but also because of the complexity of the disease.
Due to the nature of the study, another thing that would benefit study IV would be the use of a standardized testing and blood-sampling protocol. Because of the fluctuating nature of the disorder, both clinical testing and the drawing of blood samples should be done on the same time of day, to mini-mize the impact of fluctuations on results.
65
Conclusions
In conclusion, our main findings were the following:
• CMAP amplitudes are higher in the biceps brachii muscle for men and rectus femoris muscle in women who perform HRST, compared with untrained individuals of the same sex.
• CMAP amplitude correlates with isometric muscle strength, and can be used as a neurophysiological biomarker for muscle status and training effects in interventional studies of patients with neuromus-cular disorders.
• HRST does not affect the nerve CSA of peripheral nerves. • Sex has a prominent effect on both nerve CSA and muscle thickness. • The CSA of the median nerve correlated with height, and was larger
in men compared with women. • The inflammatory proteins MMP-10, TGF-α and EN-RAGE are all
elevated in sera of MG patients. MMP-10 and CXCL1 have a higher expression in EOMG patients compared with LOMG, whereas BDNF has a higher expression in LOMG patients.
• Thymectomy lowers the levels of the proposed biomarker miR-150-5p.
66
Summary in Swedish – Sammanfattning på svenska
Denna avhandling har två huvudspår, det ena är att undersöka nya biomarkö-rer för att utvärdera neuromuskulär funktion, och det andra är att undersöka nya biomarkörer för sjukdomen myasthenia gravis (MG). En biomarkör kan vara vad som helst som används för att mäta ett biologiskt tillstånd eller en sjukdom, såsom proteiner, enzymer, gener eller en specifik klinisk under-sökning. Såväl kolesterol som blodtryck skulle kunna betraktas som biomar-körer, men det som oftast åsyftas inom medicinen är någon form av mätbar indikator för ett sjukdomstillstånd.
MG är en autoimmun sjukdom, vilket innebär att kroppens immunförsvar angriper sina egna vävnader. Symptomen hos en autoimmun sjukdom beror på vilket sätt kroppen angriper sig själv, samt vilken typ av vävnad eller organ som drabbas. Varför vissa personer får autoimmuna sjukdomar är inte helt klarlagt. Som vid många olika sjukdomar kan uppkomsten av autoim-muna sjukdomar förklaras med hjälp av stress-sårbarhetsmodellen. Olika individer har olika benägenhet (sårbarhet) att utveckla en sjukdom, som be-ror på både arv- och miljöfaktorer. För att faktiskt utveckla sjukdomen krävs det i tillägg till denna sårbarhet oftast någon form av yttre stressor, som utlö-ser sjukdomen.
Vid MG bildar kroppen antikroppar mot receptorer som sitter på muskel-cellerna. Dessa receptorers funktion är att ta emot signaler som skickas från centrala delar av nervsystemet, och föra över dessa nervimpulser till musk-lerna. När en nervimpuls når änden på nerven frisätts acetylkolin i synaps-klyftan mellan nerven och muskeln. Acetylkolinet binder sedan till recepto-rer på muskelfibern, vilket leder till att muskeln kontraherar. När antikrop-parna vid MG angriper receptorerna på musklerna fungerar impulsöverfö-ringen mellan nerv och muskel sämre än vanligt, och musklerna blir onormalt uttröttade. Namnet ”myasthenia gravis” består av både grekiska och latin, och betyder ordagrant ”svår muskelsvaghet”. Vilka muskler som drabbas och hur allvarliga symptomen är varierar mycket. En del patienter får enbart besvär med muskler som styr ögonen, vilket kan resultera i dub-belseende eller hängande ögonlock. Andra får påverkan på muskulatur som styr tal, tuggrörelser och sväljning, medan vissa får påverkan på armar och ben och därför har svårt för fysisk ansträngning. Symptomen kan dessutom variera kraftigt, både från dag till dag, men även under loppet av några tim-

67
mar, och muskeltröttheten blir oftast mer uttalad efter ansträngning. I allra värsta fall kan andningsmuskulaturen påverkas, och man kan då behöva assi-sterad andning med hjälp av respirator. Beroende på vid vilken ålder man får sjukdomen, vilken typ av antikroppar man har, och vilka muskler som på-verkas, delas MG upp i flera subgrupper. Dessa skiljer sig åt vad gäller symptom och framför allt behandling. Uppdelningen mellan dessa subgrup-per är till stor del klinisk, vilket innebär att det i en del fall inte finns något objektivt sätt att avgöra vilken subgrupp patienten tillhör, utan det baseras på läkarens bedömning.
Biomarkörer för neuromuskulär funktion Eftersom symptomen oftast blir värre efter ansträngning har man traditionellt sett avrått patienter med MG från att utöva fysisk aktivitet och träning. Detta har dock i större utsträckning baserats på avsaknad av kunskap, snarare än bevis på att träning skulle vara skadligt. Eftersom muskelsvagheten fluktue-rar så uttalat är det svårt att utvärdera effekten av styrketräning hos MG-patienter enbart genom att mäta muskelstyrkan. Det behövs därför andra metoder för att objektivt kunna uppskatta muskelfunktionen hos dessa pati-enter. Ett sätt att undersöka muskeln, och nerven som innerverar den, är med neurografi, en neurofysiologisk undersökningsmetod som mäter nervled-ningsförmågan. Neurografi mäter också hur en muskel svarar på elektrisk stimulering av nerven som innerverar den, vilket kallas för compound motor action potential (CMAP), som är det samlade muskelsvaret på motorisk nervstimulering.
Studie I I den första studien undersöktes 83 friska personer med neurografi, för att ta reda på om CMAP skilde sig mellan personer som tränade styrketräning minst 2 gånger i veckan och personer som inte tränade styrketräning. 4 olika muskler undersöktes (2 armmuskler och 2 benmuskler), och vi mätte även muskelstyrkan hos dessa muskler med en dynamometer. Vi fann att den trä-nade gruppen hade större CMAP-värde i överarms- och lårmuskler (biceps och quadriceps) jämfört med otränade individer, samt att CMAP-värdet i bicepsmuskeln korrelerade med den uppmätta muskelstyrkan. Detta innebär att CMAP skulle kunna användas som ett sätt att utvärdera muskelfunktion-en i träningsstudier med MG-patienter.
Studie II I denna studie undersöktes deltagare från studie I på nytt, men denna gång med ultraljud, för att utvärdera om styrketräning har någon effekt på nerv-storleken och om den skilde sig åt mellan grupperna. Samma muskler som i studie I undersöktes, samt därutöver två stycken nerver i överarmen. Totalt undersöktes 44 friska personer, varav hälften styrketränade. Vi fann inte någon skillnad i nervstorlek mellan grupperna, men som väntat hade de del-

68
tagare som styrketränade större muskeltjocklek i överarmsmusklerna. Vi fann även att män hade större nervtjocklek än kvinnor (oavsett om de styrke-tränade eller inte), samt att nervtjockleken ökar ju längre man är.
Biomarkörer för MG Den andra delen av avhandlingen fokuserar på biomarkörer vid MG. Som tidigare nämnts orsakas MG av antikroppar mot acetylkolinreceptorerna. Dessa antikroppar går att mäta i blodet, vilket är ett av sätten att diagnosti-sera MG. Tyvärr finns det inget tydligt samband mellan nivåerna av dessa antikroppar och sjukdomens allvarlighetsgrad. Antikroppsnivåerna skiljer sig ganska mycket mellan patienter, men även vid upprepade mätningar hos en och samma patient. Det går således inte att använda antikroppsnivåerna för att se hur sjukdomen utvecklas över tid, eller hur patienterna svarar på be-handling. Detta skulle ha varit mycket användbart eftersom det kan vara svårt att bedöma detta kliniskt på grund av den kraftiga fluktuationen av symptom.
För MG finns det i nuläget inga pålitliga biomarkörer för att objektivt kunna uppskatta sjukdomstillståndet. Biomarkörer vid MG skulle även kunna användas för att bättre kunna förutsäga prognosen för sjukdomsför-loppet, samt för att avgöra vilken subgrupp en patient tillhör, för att på så sätt kunna erbjuda bästa möjliga behandling. Även i forskningssammanhang skulle en pålitlig biomarkör för MG vara mycket användbar, för att på ett objektivt och tillförlitligt sätt kunna utvärdera olika interventioner och be-handlingar. En grupp proteiner som på senare tid fått allt större roll som möj-liga biomarkörer vid olika sjukdomar är microRNA (miRNA). Det är små molekyler som reglerar uttrycket av proteiner inne i cellerna, men de finns även i blodbanan och kan eventuellt fungera som signalmolekyler. Vid olika sjukdomar verkar uttrycket av specifika miRNA vara ändrat, vilket gör att de går att använda som biomarkörer. Specifika uttrycksprofiler har hittats vid olika cancerformer, diabetes och hjärt-kärlsjukdom. Tidigare studier av miRNA vid MG har påvisat förhöjda nivåer av ett miRNA som heter miR-150-5p, som skulle kunna vara aktuell som potentiell biomarkör vid MG.
Studie III I studie III undersöktes uttrycket av 92 inflammatoriska proteiner i blodet, och hur dessa skilde sig åt mellan 44 stycken MG-patienter och 43 friska personer. Samtliga proteiner som undersöktes är inblandade i kroppens svar på inflammation, och har flera biologiska funktioner. Elva proteiner var för-höjda hos MG-patienter jämfört med friska, varav tre proteiner (MMP-10, TGF-α och EN-RAGE) var särskilt förhöjda. Vi fann dock inget samband mellan dessa proteiners uttryck och hur sjuka patienterna var, eller hur länge de varit sjuka, vilket begränsar deras roll som möjliga biomarkörer.

69
Studie IV I den fjärde studien ingick 80 patienter från en stor, internationell studie, som undersökte huruvida tymektomi (kirurgiskt avlägsnande av brässen, en körtel som är viktig för immunförsvarets utveckling) förbättrar symptomen vid MG, och om det minskar behovet av symptomlindrande mediciner. Blodprov, klinisk bedömning och läkemedelsdos registrerades från dessa patienter innan operationen, samt 12, 24 och 36 månader efteråt. Vi analyse-rade dessa blodprov för att undersöka om tymektomi även hade en påverkan på nivåerna av miR-150-5p. Patienter som genomgått tymektomi hade lägre nivåer av miR-150-5p 24 månader efter operationen, jämfört med dem som enbart fått läkemedelsbehandling.
Slutsats Resultaten från studie I och II har lett till att både CMAP och ultraljud har använts i träningsstudier, för att tillsammans med klinisk testning och styrkemätning utvärdera effekten av styrketräning hos MG-patienter. Resul-taten, som nyligen publicerats i en avhandling, visar att patienter med MG tolererar styrketräning väl och upplever ökat välbefinnande, utan någon på-visbar försämring av symptom, såväl subjektivt som kliniskt. I en av studier-na syntes en ökning av CMAP-nivåer i såväl armar som ben, och i en annan studie ökade såväl CMAP-värdet som muskeltjockleken (mätt med ultraljud) i benmuskler.
Biomarkörstudierna har bidragit med ny information vad gäller den in-flammatoriska komponenten vid MG, samt ytterligare förstärkt miR-150-5p som biomarkör. Den biologiska funktionen för såväl de inflammatoriska proteinerna som för miR-150-5p vid uppkomsten av MG och dess sjuk-domsmekanismer är dock fortsatt okänd och bör undersökas närmare i fram-tida studier.
70
Acknowledgements
This work was carried out at the Department of Neuroscience, Uppsala Uni-versity, and the Department of Clinical Neurophysiology, Uppsala Universi-ty Hospital.
This thesis would not have been finished without support from several peo-ple, and I would like to express my sincere gratitude to you:
First of all, I would like to thank my supervisor, Anna Rostedt Punga. Thank you for taking me on as a PhD student (and initially as a master’s student during medical school), introducing me to research and believing in me. Your dedication, problem solving, wide range of knowledge and hard work is truly inspirational! You have an incredible ability to see the best in people. With you as a supervisor, being a PhD student is an enjoyable chal-lenge.
My co-supervisor Johan Widenfalk – for teaching me ultrasound, for al-ways offering a helping hand, for your attention to detail, and for your friendly and positive attitude. Having an experienced clinician and research-er as a mentor outside the research group has meant a lot to me.
Nils Hailer, my other co-supervisor – although in the end we did not do much research together, thank you for being a mentor during my time as a newly graduated physician at the Department of Orthopaedics.
My colleagues and co-researchers in the Clinical Neurophysiology group: Liis Sabre – for your invaluable (and endless!) work with all the blood sam-ples in the MGTX study, and for lab company. Without you, this thesis would not even be close to finished. Ida Lindblad – for introducing me to lab work, for great taste in music, for conquering the PCR robot and for be-ing equally as confused as me. Elisabet Westerberg – for collaboration on several studies and for leading the way as a PhD student. Evgenii Bogatikov – for support in the lab. Marta Lewandowska – for all the help with proof-reading manuscripts and scientific papers. Milos Radivojevic – for bringing new energy to the research group.
71
To all biomedical technicians, physicians and other staff at the Department of Clinical Neurophysiology, especially Margareta Grindlund, Lena Eriksson, Susanne Östgren, and Carolina Brink – thank you for being so nice and friendly, for teaching me to perform neurographies and for all the help when examining research participants. Your helpful attitude made eve-rything go smooth! A special thank you to Erik Stålberg, who was the one who suggested Anna as a supervisor for my master’s thesis, which eventual-ly led to me becoming a PhD student.
Christina Asplund and Erik Salaneck – for giving me the opportunity to combine research with a medical internship at Uppsala University Hospital.
Friends from medical school: especially Thomas, Joel and Emil – for all the fun and hard times going through medical school, and fellow medical interns at Akademiska – you know who you are. Thank you for making life at the hospital more bearable. Friends that I’ve made during my time as a student in Uppsala – you are far too many to mention, so I won’t even try. I never could have imagined that these past years would be so much fun, and they have taught me infinitely more than just a university degree can.
Allmänna Sången, Västgöta Nations Manskör Korgossarna and Orphei Drängar – for giving me the chance to practice music, for being a source of energy (most of the time…) and for all the friends and unforgettable con-certs, performances and tours. Also, thank you to all the people I’ve played with during the past couple of years, and the people involved in creating the show at Uppsala stadsteater (where a large part of the draft for this thesis was written…).
My soon to be parents-in-law Anna and Krister – for being so nice and welcoming, for your generosity and for the summers in Båstad.
Mom, for always listening, for pep-talk, for being an inspiration and for never giving up, and Dad, for your extensive knowledge, always answering questions and your will do to right. Thank you for all the support! My sisters Louise and Cecilia, with your great families - for supporting me and being such great role models. All of our family’s dogs throughout the years – for being an endless source of joy.
My fiancée Ida – thank you for putting up with me. Thank you for your unconditional love, for always listening, and for always supporting me, no matter what. I look forward to soon being able to call you my wife!
72
References
1 Hughes, T. The early history of myasthenia gravis. Neuromuscul Disord 15, 878-886, doi:10.1016/j.nmd.2005.08.007 (2005).
2 Vincent, A. Unravelling the pathogenesis of myasthenia gravis. Nature reviews. Immunology 2, 797-804, doi:10.1038/nri916 (2002).
3 Walker, M. B. Treatment of Myasthenia Gravis with Physostigmine. The Lancet 223, 1200-1201, doi:http://dx.doi.org/10.1016/S0140-6736(00)94294-6 (1934).
4 Simpson, J. A. Myasthenia Gravis: A New Hypothesis. Scottish Medical Journal 5, 419-436, doi:10.1177/003693306000501001 (1960).
5 Patrick, J. & Lindstrom, J. Autoimmune response to acetylcholine receptor. Science 180, 871-872 (1973).
6 Hall, J. E. Guyton and Hall textbook of medical physiology. (Elsevier, 2015). 7 Purves, D. Neuroscience. (Sinauer Associates ;, 2012). 8 Vincent, A. & Newsom-Davis, J. Acetylcholine receptor antibody as a
diagnostic test for myasthenia gravis: results in 153 validated cases and 2967 diagnostic assays. Journal of neurology, neurosurgery, and psychiatry 48, 1246-1252 (1985).
9 Gilhus, N. E. & Verschuuren, J. J. Myasthenia gravis: subgroup classification and therapeutic strategies. Lancet Neurol 14, 1023-1036, doi:10.1016/S1474-4422(15)00145-3 (2015).
10 Lefvert, A. K., Cuenoud, S. & Fulpius, B. W. Binding properties and subclass distribution of anti-acetylcholine receptor antibodies in myasthenia gravis. J Neuroimmunol 1, 125-135 (1981).
11 Drachman, D. B., Adams, R. N., Stanley, E. F. & Pestronk, A. Mechanisms of acetylcholine receptor loss in myasthenia gravis. Journal of neurology, neurosurgery, and psychiatry 43, 601-610 (1980).
12 Sahashi, K., Engel, A. G., Linstrom, J. M., Lambert, E. H. & Lennon, V. A. Ultrastructural localization of immune complexes (IgG and C3) at the end-plate in experimental autoimmune myasthenia gravis. J Neuropathol Exp Neurol 37, 212-223 (1978).
13 Rodgaard, A., Nielsen, F. C., Djurup, R., Somnier, F. & Gammeltoft, S. Acetylcholine receptor antibody in myasthenia gravis: predominance of IgG subclasses 1 and 3. Clin Exp Immunol 67, 82-88 (1987).
14 Phillips, W. D. & Vincent, A. Pathogenesis of myasthenia gravis: update on disease types, models, and mechanisms. F1000Res 5, doi:10.12688/f1000research.8206.1 (2016).
15 Marx, A. et al. The different roles of the thymus in the pathogenesis of the various myasthenia gravis subtypes. Autoimmun Rev 12, 875-884, doi:10.1016/j.autrev.2013.03.007 (2013).
16 Marx, A. et al. Thymoma and paraneoplastic myasthenia gravis. Autoimmunity 43, 413-427, doi:10.3109/08916930903555935 (2010).
73
17 Hoch, W. et al. Auto-antibodies to the receptor tyrosine kinase MuSK in patients with myasthenia gravis without acetylcholine receptor antibodies. Nature medicine 7, 365-368, doi:10.1038/85520 (2001).
18 Bartoccioni, E. et al. Identification of disease-specific autoantibodies in seronegative myasthenia gravis. Ann N Y Acad Sci 998, 356-358 (2003).
19 Burden, S. J., Yumoto, N. & Zhang, W. The role of MuSK in synapse formation and neuromuscular disease. Cold Spring Harb Perspect Biol 5, a009167, doi:10.1101/cshperspect.a009167 (2013).
20 Zong, Y. et al. Structural basis of agrin-LRP4-MuSK signaling. Genes Dev 26, 247-258, doi:10.1101/gad.180885.111 (2012).
21 Cole, R. N., Reddel, S. W., Gervasio, O. L. & Phillips, W. D. Anti-MuSK patient antibodies disrupt the mouse neuromuscular junction. Ann Neurol 63, 782-789, doi:10.1002/ana.21371 (2008).
22 Shigemoto, K. et al. Induction of myasthenia by immunization against muscle-specific kinase. J Clin Invest 116, 1016-1024, doi:10.1172/JCI21545 (2006).
23 Jha, S. et al. Myasthenia gravis induced in mice by immunization with the recombinant extracellular domain of rat muscle-specific kinase (MuSK). J Neuroimmunol 175, 107-117, doi:10.1016/j.jneuroim.2006.03.016 (2006).
24 Mori, S. et al. Antibodies against muscle-specific kinase impair both presynaptic and postsynaptic functions in a murine model of myasthenia gravis. Am J Pathol 180, 798-810, doi:10.1016/j.ajpath.2011.10.031 (2012).
25 Hurst, R. L. & Gooch, C. L. Muscle-Specific Receptor Tyrosine Kinase (MuSK) Myasthenia Gravis. Curr Neurol Neurosci Rep 16, 61, doi:10.1007/s11910-016-0668-z (2016).
26 Meriggioli, M. N. & Sanders, D. B. Muscle autoantibodies in myasthenia gravis: beyond diagnosis? Expert Rev Clin Immunol 8, 427-438, doi:10.1586/eci.12.34 (2012).
27 Gilhus, N. E. Myasthenia Gravis. N Engl J Med 375, 2570-2581, doi:10.1056/NEJMra1602678 (2016).
28 Evoli, A. & Padua, L. Diagnosis and therapy of myasthenia gravis with antibodies to muscle-specific kinase. Autoimmun Rev 12, 931-935, doi:10.1016/j.autrev.2013.03.004 (2013).
29 Higuchi, O., Hamuro, J., Motomura, M. & Yamanashi, Y. Autoantibodies to low-density lipoprotein receptor-related protein 4 in myasthenia gravis. Ann Neurol 69, 418-422, doi:10.1002/ana.22312 (2011).
30 Gasperi, C. et al. Anti-agrin autoantibodies in myasthenia gravis. Neurology 82, 1976-1983, doi:10.1212/WNL.0000000000000478 (2014).
31 Kronenberg, M. & Rudensky, A. Regulation of immunity by self-reactive T cells. Nature 435, 598-604, doi:10.1038/nature03725 (2005).
32 Aschenbrenner, K. et al. Selection of Foxp3+ regulatory T cells specific for self antigen expressed and presented by Aire+ medullary thymic epithelial cells. Nat Immunol 8, 351-358, doi:10.1038/ni1444 (2007).
33 Owen, J. A., Punt, J., Stranford, S. A. & Jones, P. P. Kuby immunology. (W.H. Freeman, 2013).
34 Villegas, J. A., Van Wassenhove, J., Le Panse, R., Berrih-Aknin, S. & Dragin, N. An imbalance between regulatory T cells and T helper 17 cells in acetylcholine receptor-positive myasthenia gravis patients. Ann N Y Acad Sci 1413, 154-162, doi:10.1111/nyas.13591 (2018).
35 Cao, Y. et al. Autoreactive T Cells from Patients with Myasthenia Gravis Are Characterized by Elevated IL-17, IFN-gamma, and GM-CSF and Diminished IL-10 Production. J Immunol 196, 2075-2084, doi:10.4049/jimmunol.1501339 (2016).
74
36 Nacu, A., Andersen, J. B., Lisnic, V., Owe, J. F. & Gilhus, N. E. Complicating autoimmune diseases in myasthenia gravis: a review. Autoimmunity 48, 362-368, doi:10.3109/08916934.2015.1030614 (2015).
37 Fang, F. et al. The autoimmune spectrum of myasthenia gravis: a Swedish population-based study. J Intern Med 277, 594-604, doi:10.1111/joim.12310 (2015).
38 Dragin, N. et al. Estrogen-mediated downregulation of AIRE influences sexual dimorphism in autoimmune diseases. J Clin Invest 126, 1525-1537, doi:10.1172/JCI81894 (2016).
39 Cohen-Kaminsky, S. et al. High IL-6 gene expression and production by cultured human thymic epithelial cells from patients with myasthenia gravis. Ann N Y Acad Sci 681, 97-99 (1993).
40 Yilmaz, V. et al. Differential Cytokine Changes in Patients with Myasthenia Gravis with Antibodies against AChR and MuSK. PLoS One 10, e0123546, doi:10.1371/journal.pone.0123546 (2015).
41 Aricha, R., Mizrachi, K., Fuchs, S. & Souroujon, M. C. Blocking of IL-6 suppresses experimental autoimmune myasthenia gravis. J Autoimmun 36, 135-141, doi:10.1016/j.jaut.2010.12.001 (2011).
42 Dalakas, M. C. Future perspectives in target-specific immunotherapies of myasthenia gravis. Ther Adv Neurol Disord 8, 316-327, doi:10.1177/1756285615605700 (2015).
43 Xie, Y. et al. Elevated plasma interleukin-17A in a subgroup of Myasthenia Gravis patients. Cytokine 78, 44-46, doi:10.1016/j.cyto.2015.06.011 (2016).
44 Roche, J. C. et al. Increased serum interleukin-17 levels in patients with myasthenia gravis. Muscle Nerve 44, 278-280, doi:10.1002/mus.22070 (2011).
45 Chunjie, N., Huijuan, N., Zhao, Y., Jianzhao, W. & Xiaojian, Z. Disease-specific signature of serum miR-20b and its targets IL-8 and IL-25, in myasthenia gravis patients. Eur Cytokine Netw 26, 61-66, doi:10.1684/ecn.2015.0367 (2015).
46 Uzawa, A., Kawaguchi, N., Himuro, K., Kanai, T. & Kuwabara, S. Serum cytokine and chemokine profiles in patients with myasthenia gravis. Clin Exp Immunol 176, 232-237, doi:10.1111/cei.12272 (2014).
47 Binks, S., Vincent, A. & Palace, J. Myasthenia gravis: a clinical-immunological update. J Neurol 263, 826-834, doi:10.1007/s00415-015-7963-5 (2016).
48 Berrih-Aknin, S., Frenkian-Cuvelier, M. & Eymard, B. Diagnostic and clinical classification of autoimmune myasthenia gravis. J Autoimmun 48-49, 143-148, doi:10.1016/j.jaut.2014.01.003 (2014).
49 Vincent, A., Palace, J. & Hilton-Jones, D. Myasthenia gravis. Lancet 357, 2122-2128, doi:10.1016/S0140-6736(00)05186-2 (2001).
50 Reddel, S. W., Morsch, M. & Phillips, W. D. Clinical and scientific aspects of muscle-specific tyrosine kinase-related myasthenia gravis. Curr Opin Neurol 27, 558-565, doi:10.1097/WCO.0000000000000136 (2014).
51 Garcia-Osta, A. et al. MuSK expressed in the brain mediates cholinergic responses, synaptic plasticity, and memory formation. J Neurosci 26, 7919-7932, doi:10.1523/JNEUROSCI.1674-06.2006 (2006).
52 Lanfranconi, S. et al. Anti-MuSK-Positive Myasthenia Gravis in a Patient with Parkinsonism and Cognitive Impairment. Neurol Res Int 2011, 859802, doi:10.1155/2011/859802 (2011).
53 Benatar, M. et al. Recommendations for myasthenia gravis clinical trials. Muscle Nerve 45, 909-917, doi:10.1002/mus.23330 (2012).
75
54 Jaretzki, A., 3rd et al. Myasthenia gravis: recommendations for clinical research standards. Task Force of the Medical Scientific Advisory Board of the Myasthenia Gravis Foundation of America. Neurology 55, 16-23 (2000).
55 Bedlack, R. S. et al. Quantitative myasthenia gravis score: assessment of responsiveness and longitudinal validity. Neurology 64, 1968-1970, doi:10.1212/01.WNL.0000163988.28892.79 (2005).
56 Burns, T. M., Conaway, M., Sanders, D. B., Composite, M. G. & Group, M.-Q. S. The MG Composite: A valid and reliable outcome measure for myasthenia gravis. Neurology 74, 1434-1440, doi:10.1212/WNL.0b013e3181dc1b1e (2010).
57 Fagius, J. & Nyholm, D. Neurologi. Vol. 5 (Liber, 2013). 58 Ekstedt, J. & Stålberg, E. A method of recording extra cellular action potentials
of single muscle fibres and measuring their propagation velocity in voluntary activated human muscles. Bulletin of the American Association of EMG and Electrodiagnostics 10, 16 (1963).
59 Ekstedt, J. & Stålberg, E. Myasthenia gravis. Diagnostic aspects by a new electrophysiological method. Oposcula medica 12, 73-76 (1967).
60 Stalberg, E. Clinical electrophysiology in myasthenia gravis. Journal of neurology, neurosurgery, and psychiatry 43, 622-633 (1980).
61 Lefvert, A. K., Bergstrom, K., Matell, G., Osterman, P. O. & Pirskanen, R. Determination of acetylcholine receptor antibody in myasthenia gravis: clinical usefulness and pathogenetic implications. Journal of neurology, neurosurgery, and psychiatry 41, 394-403 (1978).
62 Lindstrom, J. An assay for antibodies to human acetylcholine receptor in serum from patients with myasthenia gravis. Clin Immunol Immunopathol 7, 36-43 (1977).
63 Leite, M. I. et al. IgG1 antibodies to acetylcholine receptors in 'seronegative' myasthenia gravis. Brain 131, 1940-1952, doi:10.1093/brain/awn092 (2008).
64 McConville, J. et al. Detection and characterization of MuSK antibodies in seronegative myasthenia gravis. Ann Neurol 55, 580-584, doi:10.1002/ana.20061 (2004).
65 Matthews, I. et al. Muscle-specific receptor tyrosine kinase autoantibodies--a new immunoprecipitation assay. Clin Chim Acta 348, 95-99, doi:10.1016/j.cccn.2004.05.008 (2004).
66 Leite, M. I., Waters, P. & Vincent, A. Diagnostic use of autoantibodies in myasthenia gravis. Autoimmunity 43, 371-379, doi:10.3109/08916930903541208 (2010).
67 Blalock, A., Harvey, A., Ford, F. R., Lilienthal, J. L. & Jr. The treatment of myasthenia gravis by removal of the thymus gland: Preliminary report. Journal of the American Medical Association 117, 1529-1533, doi:10.1001/jama.1941.02820440037009 (1941).
68 Grob, D., Brunner, N., Namba, T. & Pagala, M. Lifetime course of myasthenia gravis. Muscle Nerve 37, 141-149, doi:10.1002/mus.20950 (2008).
69 Cea, G., Benatar, M., Verdugo, R. J. & Salinas, R. A. Thymectomy for non-thymomatous myasthenia gravis. Cochrane Database Syst Rev, CD008111, doi:10.1002/14651858.CD008111.pub2 (2013).
70 Wolfe, G. I. et al. Randomized Trial of Thymectomy in Myasthenia Gravis. N Engl J Med 375, 511-522, doi:10.1056/NEJMoa1602489 (2016).
71 Sanders, D. B. et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology 87, 419-425, doi:10.1212/WNL.0000000000002790 (2016).
76
72 Wang, S. et al. Advances in autoimmune myasthenia gravis management. Expert Rev Neurother 18, 573-588, doi:10.1080/14737175.2018.1491310 (2018).
73 Howard, J. F., Jr. et al. Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3, randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol 16, 976-986, doi:10.1016/S1474-4422(17)30369-1 (2017).
74 Barth, D., Nabavi Nouri, M., Ng, E., Nwe, P. & Bril, V. Comparison of IVIg and PLEX in patients with myasthenia gravis. Neurology 76, 2017-2023, doi:10.1212/WNL.0b013e31821e5505 (2011).
75 Carr, A. S., Cardwell, C. R., McCarron, P. O. & McConville, J. A systematic review of population based epidemiological studies in Myasthenia Gravis. BMC Neurol 10, 46, doi:10.1186/1471-2377-10-46 (2010).
76 Meriggioli, M. N. & Sanders, D. B. Autoimmune myasthenia gravis: emerging clinical and biological heterogeneity. Lancet Neurol 8, 475-490, doi:10.1016/S1474-4422(09)70063-8 (2009).
77 Evoli, A. et al. Myasthenia gravis with antibodies to MuSK: an update. Ann N Y Acad Sci 1412, 82-89, doi:10.1111/nyas.13518 (2018).
78 Biswas, A. et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med 162, 123-132, doi:10.7326/M14-1651 (2015).
79 WHO. Global Recommendations on Physical Activity for Health. Pages (World Health Organization, Geneva, 2010).
80 Garber, C. E. et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 43, 1334-1359, doi:10.1249/MSS.0b013e318213fefb (2011).
81 Anziska, Y. & Sternberg, A. Exercise in neuromuscular disease. Muscle Nerve 48, 3-20, doi:10.1002/mus.23771 (2013).
82 Abresch, R. T., Han, J. J. & Carter, G. T. Rehabilitation management of neuromuscular disease: the role of exercise training. J Clin Neuromuscul Dis 11, 7-21, doi:10.1097/CND.0b013e3181a8d36b (2009).
83 D'Antona, G. et al. Skeletal muscle hypertrophy and structure and function of skeletal muscle fibres in male body builders. J Physiol 570, 611-627, doi:10.1113/jphysiol.2005.101642 (2006).
84 Seynnes, O. R., de Boer, M. & Narici, M. V. Early skeletal muscle hypertrophy and architectural changes in response to high-intensity resistance training. J Appl Physiol (1985) 102, 368-373, doi:10.1152/japplphysiol.00789.2006 (2007).
85 Moritani, T. & deVries, H. A. Neural factors versus hypertrophy in the time course of muscle strength gain. Am J Phys Med 58, 115-130 (1979).
86 Folland, J. P. & Williams, A. G. The adaptations to strength training : morphological and neurological contributions to increased strength. Sports Med 37, 145-168 (2007).
87 Jones, D. A. & Rutherford, O. M. Human muscle strength training: the effects of three different regimens and the nature of the resultant changes. J Physiol 391, 1-11 (1987).
88 Narici, M. V., Roi, G. S., Landoni, L., Minetti, A. E. & Cerretelli, P. Changes in force, cross-sectional area and neural activation during strength training and
77
detraining of the human quadriceps. Eur J Appl Physiol Occup Physiol 59, 310-319 (1989).
89 Yue, G. & Cole, K. J. Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractions. J Neurophysiol 67, 1114-1123 (1992).
90 Zijdewind, I., Toering, S. T., Bessem, B., Van Der Laan, O. & Diercks, R. L. Effects of imagery motor training on torque production of ankle plantar flexor muscles. Muscle Nerve 28, 168-173, doi:10.1002/mus.10406 (2003).
91 Cureton, K. J., Collins, M. A., Hill, D. W. & McElhannon, F. M., Jr. Muscle hypertrophy in men and women. Med Sci Sports Exerc 20, 338-344 (1988).
92 Wilmore, J. H. Alterations in strength, body composition and anthropometric measurements consequent to a 10-week weight training program. Med Sci Sports 6, 133-138 (1974).
93 Kadi, F., Bonnerud, P., Eriksson, A. & Thornell, L. E. The expression of androgen receptors in human neck and limb muscles: effects of training and self-administration of androgenic-anabolic steroids. Histochem Cell Biol 113, 25-29 (2000).
94 Edwards, R. H., Young, A., Hosking, G. P. & Jones, D. A. Human skeletal muscle function: description of tests and normal values. Clin Sci Mol Med 52, 283-290 (1977).
95 Welle, S., Totterman, S. & Thornton, C. Effect of age on muscle hypertrophy induced by resistance training. J Gerontol A Biol Sci Med Sci 51, M270-275 (1996).
96 Madu, C. O. & Lu, Y. Novel diagnostic biomarkers for prostate cancer. J Cancer 1, 150-177 (2010).
97 Duez, L., Qerama, E., Fuglsang-Frederiksen, A., Bangsbo, J. & Jensen, T. S. Electrophysiological characteristics of motor units and muscle fibers in trained and untrained young male subjects. Muscle Nerve 42, 177-183, doi:10.1002/mus.21641 (2010).
98 Suk, J. I., Walker, F. O. & Cartwright, M. S. Ultrasonography of peripheral nerves. Curr Neurol Neurosci Rep 13, 328, doi:10.1007/s11910-012-0328-x (2013).
99 Hobson-Webb, L. D. & Padua, L. Ultrasound of Focal Neuropathies. J Clin Neurophysiol 33, 94-102, doi:10.1097/WNP.0000000000000233 (2016).
100 Cartwright, M. S. et al. Cross-sectional area reference values for nerve ultrasonography. Muscle Nerve 37, 566-571, doi:10.1002/mus.21009 (2008).
101 Cartwright, M. S., Mayans, D. R., Gillson, N. A., Griffin, L. P. & Walker, F. O. Nerve cross-sectional area in extremes of age. Muscle Nerve 47, 890-893, doi:10.1002/mus.23718 (2013).
102 Kerasnoudis, A., Pitarokoili, K., Behrendt, V., Gold, R. & Yoon, M. S. Cross sectional area reference values for sonography of peripheral nerves and brachial plexus. Clin Neurophysiol 124, 1881-1888, doi:10.1016/j.clinph.2013.03.007 (2013).
103 Qrimli, M. et al. Reference values for ultrasonograpy of peripheral nerves. Muscle Nerve 53, 538-544, doi:10.1002/mus.24888 (2016).
104 Rempel, D., Dahlin, L. & Lundborg, G. Pathophysiology of nerve compression syndromes: response of peripheral nerves to loading. J Bone Joint Surg Am 81, 1600-1610 (1999).
105 Pillen, S., Arts, I. M. & Zwarts, M. J. Muscle ultrasound in neuromuscular disorders. Muscle Nerve 37, 679-693, doi:10.1002/mus.21015 (2008).
78
106 Zaidman, C. M. & van Alfen, N. Ultrasound in the Assessment of Myopathic Disorders. J Clin Neurophysiol 33, 103-111, doi:10.1097/WNP.0000000000000245 (2016).
107 Pillen, S. & Van Alfen, N. Muscle ultrasound from diagnostic tool to outcome measure--Quantification is the challenge. Muscle Nerve 52, 319-320, doi:10.1002/mus.24613 (2015).
108 Abe, T., DeHoyos, D. V., Pollock, M. L. & Garzarella, L. Time course for strength and muscle thickness changes following upper and lower body resistance training in men and women. Eur J Appl Physiol 81, 174-180, doi:10.1007/s004210050027 (2000).
109 Kerasnoudis, A. Ultrasound visualization of nerve remodeling after strenuous exercise. Muscle Nerve 53, 320-324, doi:10.1002/mus.24948 (2016).
110 Heldal, A. T., Eide, G. E., Romi, F., Owe, J. F. & Gilhus, N. E. Repeated acetylcholine receptor antibody-concentrations and association to clinical myasthenia gravis development. PLoS One 9, e114060, doi:10.1371/journal.pone.0114060 (2014).
111 Kaminski, H. J. et al. Biomarker development for myasthenia gravis. Ann N Y Acad Sci 1275, 101-106, doi:10.1111/j.1749-6632.2012.06787.x (2012).
112 Bartoccioni, E. et al. Anti-MuSK antibodies: correlation with myasthenia gravis severity. Neurology 67, 505-507, doi:10.1212/01.wnl.0000228225.23349.5d (2006).
113 Krol, J., Loedige, I. & Filipowicz, W. The widespread regulation of microRNA biogenesis, function and decay. Nat Rev Genet 11, 597-610, doi:10.1038/nrg2843 (2010).
114 Valadi, H. et al. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat Cell Biol 9, 654-659, doi:10.1038/ncb1596 (2007).
115 Ha, M. & Kim, V. N. Regulation of microRNA biogenesis. Nat Rev Mol Cell Biol 15, 509-524, doi:10.1038/nrm3838 (2014).
116 Keller, A. & Meese, E. Can circulating miRNAs live up to the promise of being minimal invasive biomarkers in clinical settings? Wiley Interdiscip Rev RNA 7, 148-156, doi:10.1002/wrna.1320 (2016).
117 Turchinovich, A., Tonevitsky, A. G. & Burwinkel, B. Extracellular miRNA: A Collision of Two Paradigms. Trends Biochem Sci 41, 883-892, doi:10.1016/j.tibs.2016.08.004 (2016).
118 Punga, A. R. & Punga, T. Circulating microRNAs as potential biomarkers in myasthenia gravis patients. Ann N Y Acad Sci 1412, 33-40, doi:10.1111/nyas.13510 (2018).
119 Friedman, R. C., Farh, K. K., Burge, C. B. & Bartel, D. P. Most mammalian mRNAs are conserved targets of microRNAs. Genome research 19, 92-105, doi:10.1101/gr.082701.108 (2009).
120 Pinzon, N. et al. microRNA target prediction programs predict many false positives. Genome research 27, 234-245, doi:10.1101/gr.205146.116 (2017).
121 Chen, J. Q., Papp, G., Szodoray, P. & Zeher, M. The role of microRNAs in the pathogenesis of autoimmune diseases. Autoimmun Rev 15, 1171-1180, doi:10.1016/j.autrev.2016.09.003 (2016).
122 Filkova, M., Jungel, A., Gay, R. E. & Gay, S. MicroRNAs in rheumatoid arthritis: potential role in diagnosis and therapy. BioDrugs 26, 131-141, doi:10.2165/11631480-000000000-00000 (2012).
123 Amarilyo, G. & La Cava, A. miRNA in systemic lupus erythematosus. Clin Immunol 144, 26-31, doi:10.1016/j.clim.2012.04.005 (2012).
79
124 Gandhi, R. et al. Circulating microRNAs as biomarkers for disease staging in multiple sclerosis. Ann Neurol 73, 729-740, doi:10.1002/ana.23880 (2013).
125 Weiland, M., Gao, X. H., Zhou, L. & Mi, Q. S. Small RNAs have a large impact: circulating microRNAs as biomarkers for human diseases. RNA biology 9, 850-859, doi:10.4161/rna.20378 (2012).
126 Wang, J., Chen, J. & Sen, S. MicroRNA as Biomarkers and Diagnostics. J Cell Physiol 231, 25-30, doi:10.1002/jcp.25056 (2016).
127 Punga, T. et al. Circulating miRNAs in myasthenia gravis: miR-150-5p as a new potential biomarker. Ann Clin Transl Neurol 1, 49-58, doi:10.1002/acn3.24 (2014).
128 Punga, A. R., Andersson, M., Alimohammadi, M. & Punga, T. Disease specific signature of circulating miR-150-5p and miR-21-5p in myasthenia gravis patients. J Neurol Sci 356, 90-96, doi:10.1016/j.jns.2015.06.019 (2015).
129 Monticelli, S. et al. MicroRNA profiling of the murine hematopoietic system. Genome Biol 6, R71, doi:10.1186/gb-2005-6-8-r71 (2005).
130 Torri, A. et al. Extracellular MicroRNA Signature of Human Helper T Cell Subsets in Health and Autoimmunity. J Biol Chem 292, 2903-2915, doi:10.1074/jbc.M116.769893 (2017).
131 Sabre, L., Maddison, P., Sadalage, G., Ambrose, P. A. & Punga, A. R. Circulating microRNA miR-21-5p, miR-150-5p and miR-30e-5p correlate with clinical status in late onset myasthenia gravis. J Neuroimmunol, doi:10.1016/j.jneuroim.2018.05.003 (2018).
132 Punga, T. et al. Disease specific enrichment of circulating let-7 family microRNA in MuSK+ myasthenia gravis. J Neuroimmunol 292, 21-26, doi:10.1016/j.jneuroim.2016.01.003 (2016).
133 Cron, M. A. et al. Analysis of microRNA expression in the thymus of Myasthenia Gravis patients opens new research avenues. Autoimmun Rev 17, 588-600, doi:10.1016/j.autrev.2018.01.008 (2018).
134 Spillane, J., Beeson, D. J. & Kullmann, D. M. Myasthenia and related disorders of the neuromuscular junction. Journal of neurology, neurosurgery, and psychiatry 81, 850-857, doi:10.1136/jnnp.2008.169367 (2010).
135 Todnem, K., Knudsen, G., Riise, T., Nyland, H. & Aarli, J. A. The non-linear relationship between nerve conduction velocity and skin temperature. Journal of neurology, neurosurgery, and psychiatry 52, 497-501 (1989).
136 Stratford, P. W. & Balsor, B. E. A comparison of make and break tests using a hand-held dynamometer and the Kin-Com. J Orthop Sports Phys Ther 19, 28-32, doi:10.2519/jospt.1994.19.1.28 (1994).
137 Bohannon, R. W. Test-retest reliability of hand-held dynamometry during a single session of strength assessment. Phys Ther 66, 206-209 (1986).
138 Bromberg, M. B. & Spiegelberg, T. The influence of active electrode placement on CMAP amplitude. Electroencephalogr Clin Neurophysiol 105, 385-389 (1997).
139 Assarsson, E. et al. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS One 9, e95192, doi:10.1371/journal.pone.0095192 (2014).
140 Lundberg, M., Eriksson, A., Tran, B., Assarsson, E. & Fredriksson, S. Homogeneous antibody-based proximity extension assays provide sensitive and specific detection of low-abundant proteins in human blood. Nucleic Acids Res 39, e102, doi:10.1093/nar/gkr424 (2011).
141 Schmittgen, T. D. & Livak, K. J. Analyzing real-time PCR data by the comparative C(T) method. Nat Protoc 3, 1101-1108 (2008).
80
142 Marx, A., Pfister, F., Schalke, B., Nix, W. & Strobel, P. Thymus pathology observed in the MGTX trial. Ann N Y Acad Sci 1275, 92-100, doi:10.1111/j.1749-6632.2012.06799.x (2012).
143 R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/. (2016).
144 Miller, A. E., MacDougall, J. D., Tarnopolsky, M. A. & Sale, D. G. Gender differences in strength and muscle fiber characteristics. Eur J Appl Physiol Occup Physiol 66, 254-262 (1993).
145 Bathala, L., Kumar, P., Kumar, K., Shaik, A. & Visser, L. H. Normal values of median nerve cross-sectional area obtained by ultrasound along its course in the arm with electrophysiological correlations, in 100 Asian subjects. Muscle Nerve 49, 284-286, doi:10.1002/mus.23912 (2014).
146 Zaidman, C. M., Al-Lozi, M. & Pestronk, A. Peripheral nerve size in normals and patients with polyneuropathy: an ultrasound study. Muscle Nerve 40, 960-966, doi:10.1002/mus.21431 (2009).
147 Cartwright, M. S. et al. Validity and reliability of nerve and muscle ultrasound. Muscle Nerve 47, 515-521, doi:10.1002/mus.23621 (2013).
148 Schafhalter-Zoppoth, I. & Gray, A. T. The musculocutaneous nerve: ultrasound appearance for peripheral nerve block. Reg Anesth Pain Med 30, 385-390 (2005).
149 Stout, J. R., Eckerson, J. M., May, E., Coulter, C. & Bradley-Popovich, G. E. Effects of resistance exercise and creatine supplementation on myasthenia gravis: a case study. Med Sci Sports Exerc 33, 869-872 (2001).
150 Lucia, A. et al. Double trouble (McArdle's disease and myasthenia gravis): how can exercise help? Muscle Nerve 35, 125-128, doi:10.1002/mus.20645 (2007).
151 Scheer, B. V., Valero-Burgos, E. & Costa, R. Myasthenia gravis and endurance exercise. Am J Phys Med Rehabil 91, 725-727, doi:10.1097/PHM.0b013e31824663c6 (2012).
152 Elsais, A., Johansen, B. & Kerty, E. Airway limitation and exercise intolerance in well-regulated myasthenia gravis patients. Acta Neurol Scand Suppl, 12-17, doi:10.1111/j.1600-0404.2010.01369.x (2010).
153 Rassler, B. et al. The effect of respiratory muscle endurance training in patients with myasthenia gravis. Neuromuscul Disord 17, 385-391, doi:10.1016/j.nmd.2007.01.001 (2007).
154 Fregonezi, G. A., Resqueti, V. R., Guell, R., Pradas, J. & Casan, P. Effects of 8-week, interval-based inspiratory muscle training and breathing retraining in patients with generalized myasthenia gravis. Chest 128, 1524-1530, doi:10.1378/chest.128.3.1524 (2005).
155 Lohi, E. L., Lindberg, C. & Andersen, O. Physical training effects in myasthenia gravis. Archives of physical medicine and rehabilitation 74, 1178-1180 (1993).
156 Westerberg, E., Molin, C. J., Lindblad, I., Emtner, M. & Punga, A. R. Physical exercise in myasthenia gravis is safe and improves neuromuscular parameters and physical performance-based measures: A pilot study. Muscle Nerve 56, 207-214, doi:10.1002/mus.25493 (2017).
157 Westerberg, E., Molin, C. J., Spörndly Nees, S., Widenfalk, J. & Punga, A. R. The impact of physical exercise on functional muscle measures in myasthenia gravis patients - a single subject design study. In press, Medicine (2018).
81
158 Schoenfeld, B. J., Contreras, B., Vigotsky, A. D. & Peterson, M. Differential Effects of Heavy Versus Moderate Loads on Measures of Strength and Hypertrophy in Resistance-Trained Men. J Sports Sci Med 15, 715-722 (2016).
159 Schoenfeld, B. J. et al. Effects of different volume-equated resistance training loading strategies on muscular adaptations in well-trained men. Journal of strength and conditioning research / National Strength & Conditioning Association 28, 2909-2918, doi:10.1519/jsc.0000000000000480 (2014).
160 Damas, F. et al. Early resistance training-induced increases in muscle cross-sectional area are concomitant with edema-induced muscle swelling. Eur J Appl Physiol 116, 49-56, doi:10.1007/s00421-015-3243-4 (2016).
161 Heymsfield, S. B., Adamek, M., Gonzalez, M. C., Jia, G. & Thomas, D. M. Assessing skeletal muscle mass: historical overview and state of the art. J Cachexia Sarcopenia Muscle 5, 9-18, doi:10.1007/s13539-014-0130-5 (2014).
162 Franchi, M. V. et al. Muscle thickness correlates to muscle cross-sectional area in the assessment of strength training-induced hypertrophy. Scand J Med Sci Sports 28, 846-853, doi:10.1111/sms.12961 (2018).
163 Walton, J. M., Roberts, N. & Whitehouse, G. H. Measurement of the quadriceps femoris muscle using magnetic resonance and ultrasound imaging. Br J Sports Med 31, 59-64 (1997).
164 Behringer, M., Franz, A., McCourt, M. & Mester, J. Motor point map of upper body muscles. Eur J Appl Physiol 114, 1605-1617, doi:10.1007/s00421-014-2892-z (2014).
165 Seok, J. I., Walker, F. O. & Kwak, S. G. Evaluation of extensor digitorum brevis thickness in healthy subjects: A comparative analysis of nerve conduction studies and ultrasound scans. Clin Neurophysiol 127, 1664-1668, doi:10.1016/j.clinph.2015.07.025 (2016).
166 Birnbaum, S. et al. The benefits and tolerance of exercise in myasthenia gravis (MGEX): study protocol for a randomised controlled trial. Trials 19, 49, doi:10.1186/s13063-017-2433-2 (2018).
167 Lorente, L. et al. Matrix metalloproteinase-9, -10, and tissue inhibitor of matrix metalloproteinases-1 blood levels as biomarkers of severity and mortality in sepsis. Crit Care 13, R158, doi:10.1186/cc8115 (2009).
168 Toft-Hansen, H., Nuttall, R. K., Edwards, D. R. & Owens, T. Key metalloproteinases are expressed by specific cell types in experimental autoimmune encephalomyelitis. J Immunol 173, 5209-5218 (2004).
169 Karussis, D. M. et al. Immunomodulation of experimental autoimmune myasthenia gravis with linomide. J Neuroimmunol 55, 187-193 (1994).
170 Guerra-Crespo, M. et al. Transforming growth factor-alpha induces neurogenesis and behavioral improvement in a chronic stroke model. Neuroscience 160, 470-483, doi:10.1016/j.neuroscience.2009.02.029 (2009).
171 Leker, R. R. et al. Transforming growth factor alpha induces angiogenesis and neurogenesis following stroke. Neuroscience 163, 233-243, doi:10.1016/j.neuroscience.2009.05.050 (2009).
172 Xian, C. J., Li, L., Deng, Y. S., Zhao, S. P. & Zhou, X. F. Lack of effects of transforming growth factor-alpha gene knockout on peripheral nerve regeneration may result from compensatory mechanisms. Exp Neurol 172, 182-188, doi:10.1006/exnr.2001.7771 (2001).
173 Goyette, J. & Geczy, C. L. Inflammation-associated S100 proteins: new mechanisms that regulate function. Amino Acids 41, 821-842, doi:10.1007/s00726-010-0528-0 (2011).
82
174 Chuah, Y. K., Basir, R., Talib, H., Tie, T. H. & Nordin, N. Receptor for advanced glycation end products and its involvement in inflammatory diseases. Int J Inflam 2013, 403460, doi:10.1155/2013/403460 (2013).
175 Ray, R., Juranek, J. K. & Rai, V. RAGE axis in neuroinflammation, neurodegeneration and its emerging role in the pathogenesis of amyotrophic lateral sclerosis. Neurosci Biobehav Rev 62, 48-55, doi:10.1016/j.neubiorev.2015.12.006 (2016).
176 Pietzsch, J. & Hoppmann, S. Human S100A12: a novel key player in inflammation? Amino Acids 36, 381-389, doi:10.1007/s00726-008-0097-7 (2009).
177 Freund, V. & Frossard, N. Expression of nerve growth factor in the airways and its possible role in asthma. Prog Brain Res 146, 335-346, doi:10.1016/S0079-6123(03)46021-4 (2004).
178 Dalakas, M. C. Invited article: inhibition of B cell functions: implications for neurology. Neurology 70, 2252-2260, doi:10.1212/01.wnl.0000313840.27060.bf (2008).
179 Chang, S. H. et al. Interleukin-17C promotes Th17 cell responses and autoimmune disease via interleukin-17 receptor E. Immunity 35, 611-621, doi:10.1016/j.immuni.2011.09.010 (2011).
180 Berrih-Aknin, S. et al. CCL21 overexpressed on lymphatic vessels drives thymic hyperplasia in myasthenia. Ann Neurol 66, 521-531, doi:10.1002/ana.21628 (2009).
181 Ueno, T. et al. Role for CCR7 ligands in the emigration of newly generated T lymphocytes from the neonatal thymus. Immunity 16, 205-218 (2002).
182 Lippert, U. et al. Expression and functional activity of the IL-8 receptor type CXCR1 and CXCR2 on human mast cells. J Immunol 161, 2600-2608 (1998).
183 Moser, B., Clark-Lewis, I., Zwahlen, R. & Baggiolini, M. Neutrophil-activating properties of the melanoma growth-stimulatory activity. J Exp Med 171, 1797-1802 (1990).
184 Iida, N. & Grotendorst, G. R. Cloning and sequencing of a new gro transcript from activated human monocytes: expression in leukocytes and wound tissue. Mol Cell Biol 10, 5596-5599 (1990).
185 Devalaraja, R. M. et al. Delayed wound healing in CXCR2 knockout mice. J Invest Dermatol 115, 234-244, doi:10.1046/j.1523-1747.2000.00034.x (2000).
186 Calabrese, F. et al. Brain-derived neurotrophic factor: a bridge between inflammation and neuroplasticity. Front Cell Neurosci 8, 430, doi:10.3389/fncel.2014.00430 (2014).
187 Kerschensteiner, M. et al. Activated human T cells, B cells, and monocytes produce brain-derived neurotrophic factor in vitro and in inflammatory brain lesions: a neuroprotective role of inflammation? J Exp Med 189, 865-870 (1999).
188 Bekinschtein, P. et al. BDNF is essential to promote persistence of long-term memory storage. Proc Natl Acad Sci U S A 105, 2711-2716, doi:10.1073/pnas.0711863105 (2008).
189 Lu, Y., Christian, K. & Lu, B. BDNF: a key regulator for protein synthesis-dependent LTP and long-term memory? Neurobiol Learn Mem 89, 312-323, doi:10.1016/j.nlm.2007.08.018 (2008).
190 Paul, R. H., Cohen, R. A., Gilchrist, J. M., Aloia, M. S. & Goldstein, J. M. Cognitive dysfunction in individuals with myasthenia gravis. J Neurol Sci 179, 59-64 (2000).
83
191 Bohbot, V. D., Jech, R., Bures, J., Nadel, L. & Ruzicka, E. Spatial and nonspatial memory involvement in myasthenia gravis. J Neurol 244, 529-532 (1997).
192 Keesey, J. C. Does myasthenia gravis affect the brain? J Neurol Sci 170, 77-89 (1999).
193 Forti, L. N. et al. Effects of resistance training at different loads on inflammatory markers in young adults. Eur J Appl Physiol 117, 511-519, doi:10.1007/s00421-017-3548-6 (2017).
194 van der Vlist, J. & Janssen, T. W. The potential anti-inflammatory effect of exercise in chronic obstructive pulmonary disease. Respiration 79, 160-174, doi:10.1159/000233264 (2010).
195 Perandini, L. A. et al. Exercise as a therapeutic tool to counteract inflammation and clinical symptoms in autoimmune rheumatic diseases. Autoimmun Rev 12, 218-224, doi:10.1016/j.autrev.2012.06.007 (2012).
196 Kierkegaard, M. et al. High-intensity resistance training in multiple sclerosis - An exploratory study of effects on immune markers in blood and cerebrospinal fluid, and on mood, fatigue, health-related quality of life, muscle strength, walking and cognition. J Neurol Sci 362, 251-257, doi:10.1016/j.jns.2016.01.063 (2016).
197 Kroesen, B. J. et al. Immuno-miRs: critical regulators of T-cell development, function and ageing. Immunology 144, 1-10, doi:10.1111/imm.12367 (2015).
198 Ghisi, M. et al. Modulation of microRNA expression in human T-cell development: targeting of NOTCH3 by miR-150. Blood 117, 7053-7062, doi:10.1182/blood-2010-12-326629 (2011).
199 Ohkura, N., Kitagawa, Y. & Sakaguchi, S. Development and maintenance of regulatory T cells. Immunity 38, 414-423, doi:10.1016/j.immuni.2013.03.002 (2013).
200 Balandina, A., Lecart, S., Dartevelle, P., Saoudi, A. & Berrih-Aknin, S. Functional defect of regulatory CD4(+)CD25+ T cells in the thymus of patients with autoimmune myasthenia gravis. Blood 105, 735-741, doi:10.1182/blood-2003-11-3900 (2005).
201 Okoye, I. S. et al. MicroRNA-containing T-regulatory-cell-derived exosomes suppress pathogenic T helper 1 cells. Immunity 41, 89-103, doi:10.1016/j.immuni.2014.05.019 (2014).
202 Bergman, P. et al. Circulating miR-150 in CSF is a novel candidate biomarker for multiple sclerosis. Neurol Neuroimmunol Neuroinflamm 3, e219, doi:10.1212/NXI.0000000000000219 (2016).
203 Stagakis, E. et al. Identification of novel microRNA signatures linked to human lupus disease activity and pathogenesis: miR-21 regulates aberrant T cell responses through regulation of PDCD4 expression. Ann Rheum Dis 70, 1496-1506, doi:10.1136/ard.2010.139857 (2011).
204 Smigielska-Czepiel, K. et al. Dual role of miR-21 in CD4+ T-cells: activation-induced miR-21 supports survival of memory T-cells and regulates CCR7 expression in naive T-cells. PLoS One 8, e76217, doi:10.1371/journal.pone.0076217 (2013).
205 Fenoglio, C. et al. Expression and genetic analysis of miRNAs involved in CD4+ cell activation in patients with multiple sclerosis. Neurosci Lett 504, 9-12, doi:10.1016/j.neulet.2011.08.021 (2011).
206 Ruan, Q. et al. The microRNA-21-PDCD4 axis prevents type 1 diabetes by blocking pancreatic beta cell death. Proc Natl Acad Sci U S A 108, 12030-12035, doi:10.1073/pnas.1101450108 (2011).
84
207 Garchow, B. G. et al. Silencing of microRNA-21 in vivo ameliorates autoimmune splenomegaly in lupus mice. EMBO Mol Med 3, 605-615, doi:10.1002/emmm.201100171 (2011).
208 Kalla, R. et al. OC-015 Proximity extension assay technology identifies novel serum biomarkers for predicting inflammatory bowel disease: IBD character consortium. Gut 64, A8-A8, doi:10.1136/gutjnl-2015-309861.15 (2015).
209 Khademi, M. et al. Intense inflammation and nerve damage in early multiple sclerosis subsides at older age: a reflection by cerebrospinal fluid biomarkers. PLoS One 8, e63172, doi:10.1371/journal.pone.0063172 (2013).
210 Keller, A. et al. Toward the blood-borne miRNome of human diseases. Nat Methods 8, 841-843, doi:10.1038/nmeth.1682 (2011).
211 Chen, X. et al. Characterization of microRNAs in serum: a novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res 18, 997-1006, doi:10.1038/cr.2008.282 (2008).
212 Turchinovich, A., Weiz, L., Langheinz, A. & Burwinkel, B. Characterization of extracellular circulating microRNA. Nucleic Acids Res 39, 7223-7233, doi:10.1093/nar/gkr254 (2011).
213 van Rooij, E. & Kauppinen, S. Development of microRNA therapeutics is coming of age. EMBO Mol Med 6, 851-864, doi:10.15252/emmm.201100899 (2014).
214 Rupaimoole, R. & Slack, F. J. MicroRNA therapeutics: towards a new era for the management of cancer and other diseases. Nat Rev Drug Discov 16, 203-222, doi:10.1038/nrd.2016.246 (2017).
215 Weis, C. A. et al. Histopathology of thymectomy specimens from the MGTX-trial: Entropy analysis as strategy to quantify spatial heterogeneity of lymphoid follicle and fat distribution. PLoS One 13, e0197435, doi:10.1371/journal.pone.0197435 (2018).
216 Witwer, K. W. Circulating microRNA biomarker studies: pitfalls and potential solutions. Clin Chem 61, 56-63, doi:10.1373/clinchem.2014.221341 (2015).


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1480
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-356116
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018







