Embed Size (px)
Citation preview
New diagnostics and their potential role
in TB screening/diagnostic algorithms
31 May, 2011
Fuad Mirzayev MD, MPH
TB Diagnostics and Laboratory Strengthening unit, Stop TB Department
WHO, Geneva
2
New diagnostics and their potential role in TB
screening/diagnostic algorithms
New diagnostics and their role in TB diagnostic
algorithms
New diagnostics and their potential role in TB
screening algorithms
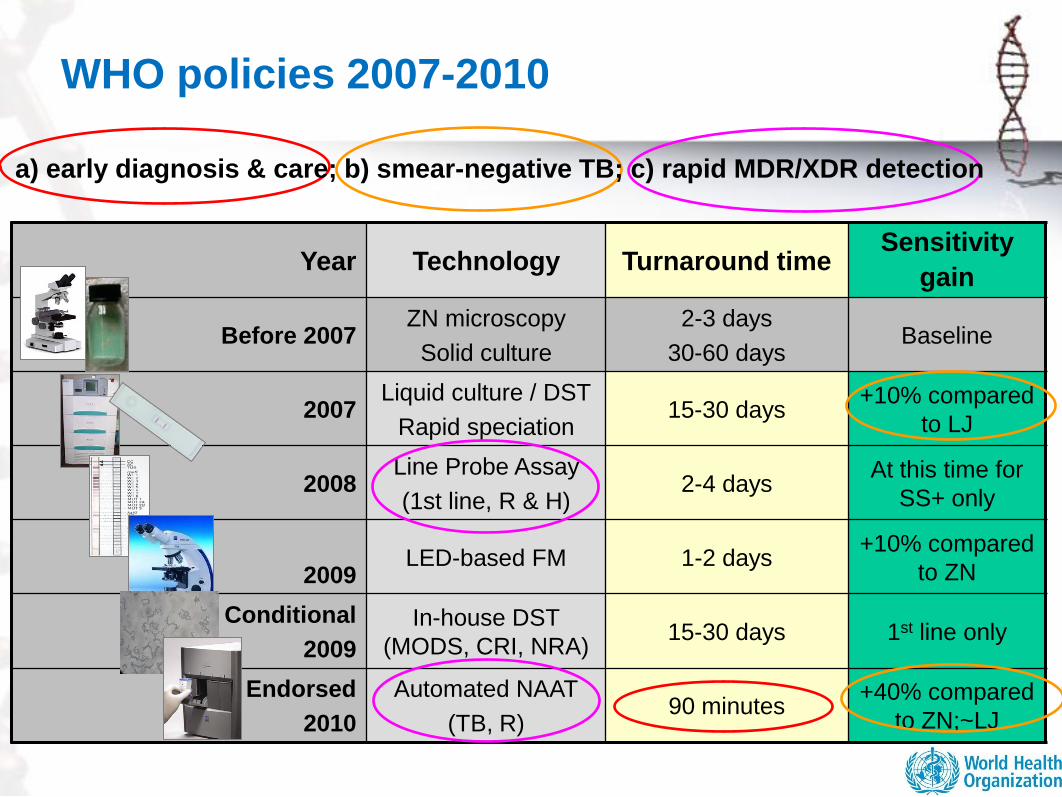
Year Technology Turnaround timeSensitivity
gain
Before 2007ZN microscopy
Solid culture
2-3 days
30-60 daysBaseline
2007Liquid culture / DST
Rapid speciation15-30 days
+10% compared
to LJ
2008Line Probe Assay
(1st line, R & H)2-4 days
At this time for
SS+ only
2009LED-based FM 1-2 days
+10% compared
to ZN
Conditional
2009
In-house DST
(MODS, CRI, NRA)15-30 days 1st line only
Endorsed
2010
Automated NAAT
(TB, R)90 minutes
+40% compared
to ZN;~LJ
a) early diagnosis & care; b) smear-negative TB; c) rapid MDR/XDR detection
WHO policies 2007-2010
4
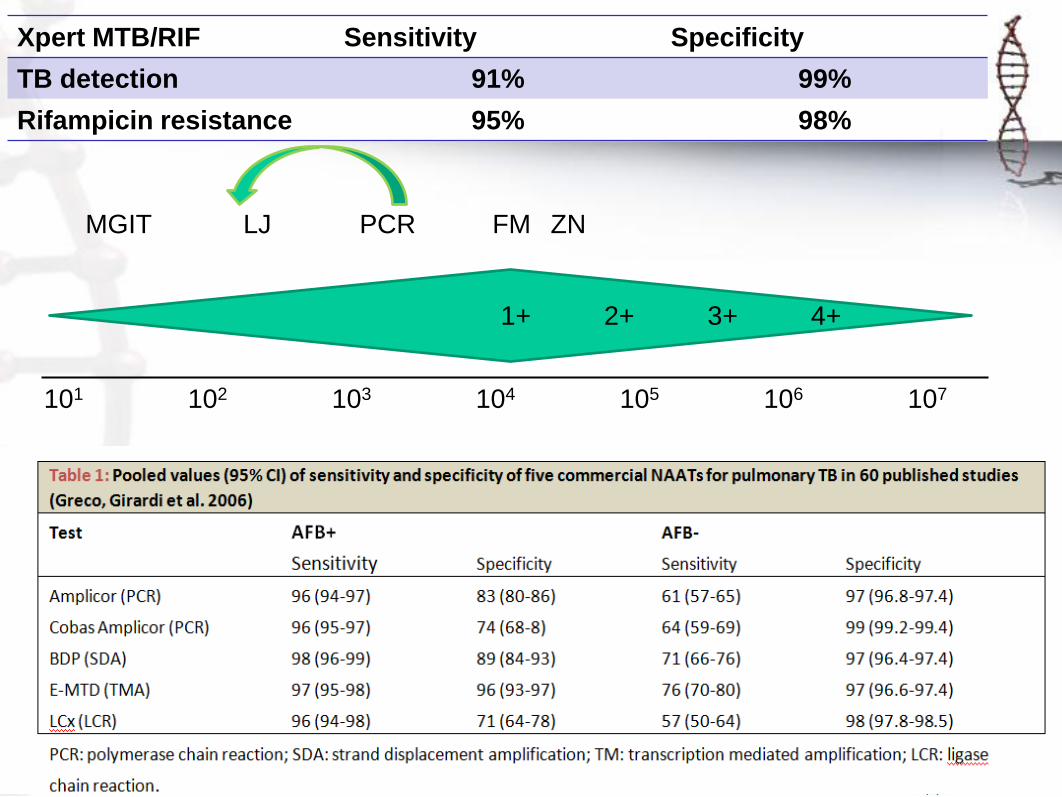
MGIT LJ PCR FM ZN
102 104 105 106 107103101
1+ 2+ 3+ 4+
Xpert MTB/RIF Sensitivity Specificity
TB detection 91% 99%
Rifampicin resistance 95% 98%
5
WHO policy recommendations
1. Xpert MTB/RIF should be used as the initial diagnostic test in
individuals suspected of having MDR-TB or HIV-associated TB.
(Strong recommendation)
2. Xpert MTB/RIF may be considered as a follow-on test to microscopy in
settings where MDR-TB or HIV is of lesser concern, especially in
further testing of smear-negative specimens. (Conditional
recommendation acknowledging major resource implications)
Remarks:
• These recommendations apply to the use of Xpert MTB/RIF in sputum specimens (including pellets from
decontaminated specimens). Data on the utility of Xpert MTB/RIF in extra-pulmonary specimens are still
limited;
• These recommendations support the use of one sputum specimen for diagnostic testing, acknowledging
that multiple specimens increase the sensitivity of Xpert MTB/RIF but have major resource implications;
• These recommendations also apply to children, based on the generalisation of data from adults and
acknowledging the limitations of microbiological diagnosis of TB (including MDR-TB) in children;
• Access to conventional microscopy, culture and DST is still needed for monitoring of therapy, for
prevalence surveys and/or surveillance, and for recovering isolates for drug susceptibility testing other
than rifampicin (including second-line anti-TB drugs).
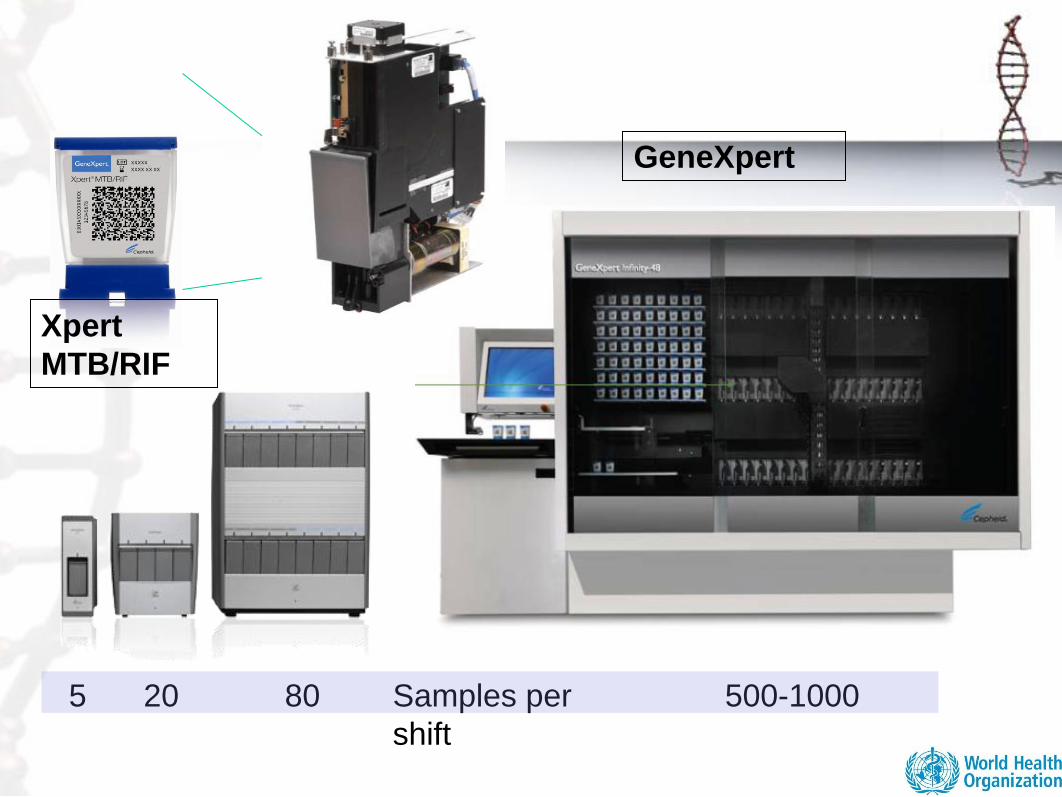
5 20 80 500-1000Samples per
shift
GeneXpert
Xpert
MTB/RIF
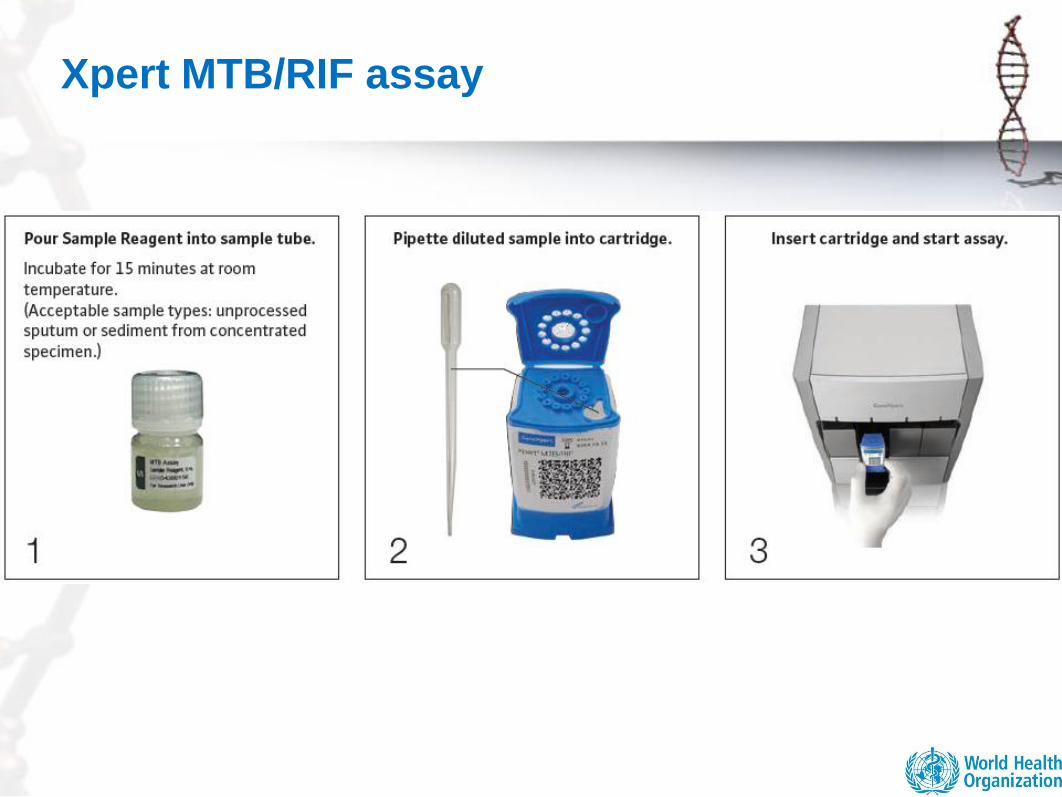
Xpert MTB/RIF assay

Positioning in tiered health system
SubDistrictLevel
MicroscopyLevel
CommunityLevel
ReferenceLabs
RegionalLabs
DistrictLevel
•Surveillance•Reference methods•Network supervision
Resolution testing (screening-test negativedrug resistance)
•Screening•Passive case finding•Detect and treat
•Clinical screening•Primary care
Integrated NAAT +40% /2h
LED FM +10%
LC / DST 15d/ 30d
LPA Rif / INH 2dSC / DST 30d / 60d
ZN 2-3d
LC / DST 15d / 30d
In house DST (MODS, NRA, CRI) Special settings and conditions
8
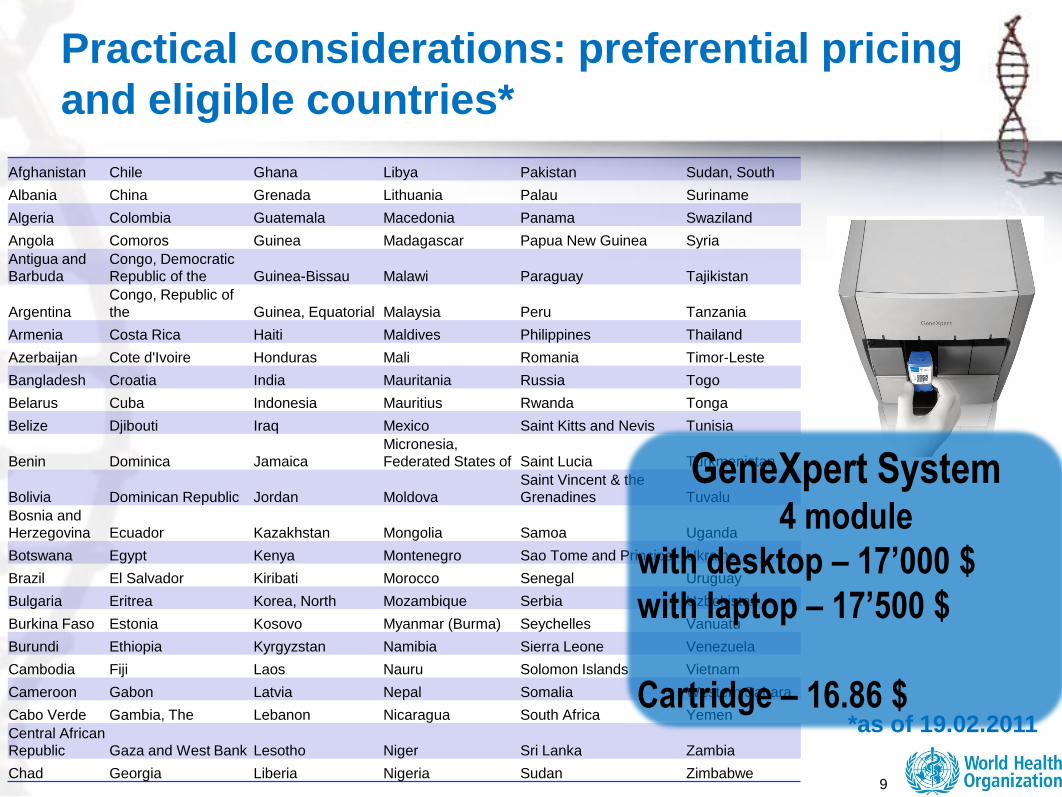
Practical considerations: preferential pricing
and eligible countries*
Afghanistan Chile Ghana Libya Pakistan Sudan, South
Albania China Grenada Lithuania Palau Suriname
Algeria Colombia Guatemala Macedonia Panama Swaziland
Angola Comoros Guinea Madagascar Papua New Guinea Syria
Antigua and
Barbuda
Congo, Democratic
Republic of the Guinea-Bissau Malawi Paraguay Tajikistan
Argentina
Congo, Republic of
the Guinea, Equatorial Malaysia Peru Tanzania
Armenia Costa Rica Haiti Maldives Philippines Thailand
Azerbaijan Cote d'Ivoire Honduras Mali Romania Timor-Leste
Bangladesh Croatia India Mauritania Russia Togo
Belarus Cuba Indonesia Mauritius Rwanda Tonga
Belize Djibouti Iraq Mexico Saint Kitts and Nevis Tunisia
Benin Dominica Jamaica
Micronesia,
Federated States of Saint Lucia Turkmenistan
Bolivia Dominican Republic Jordan Moldova
Saint Vincent & the
Grenadines Tuvalu
Bosnia and
Herzegovina Ecuador Kazakhstan Mongolia Samoa Uganda
Botswana Egypt Kenya Montenegro Sao Tome and Principe Ukraine
Brazil El Salvador Kiribati Morocco Senegal Uruguay
Bulgaria Eritrea Korea, North Mozambique Serbia Uzbekistan
Burkina Faso Estonia Kosovo Myanmar (Burma) Seychelles Vanuatu
Burundi Ethiopia Kyrgyzstan Namibia Sierra Leone Venezuela
Cambodia Fiji Laos Nauru Solomon Islands Vietnam
Cameroon Gabon Latvia Nepal Somalia Western Sahara
Cabo Verde Gambia, The Lebanon Nicaragua South Africa Yemen
Central African
Republic Gaza and West Bank Lesotho Niger Sri Lanka Zambia
Chad Georgia Liberia Nigeria Sudan Zimbabwe
GeneXpert System4 module
with desktop – 17’000 $
with laptop – 17’500 $
Cartridge – 16.86 $
9
*as of 19.02.2011
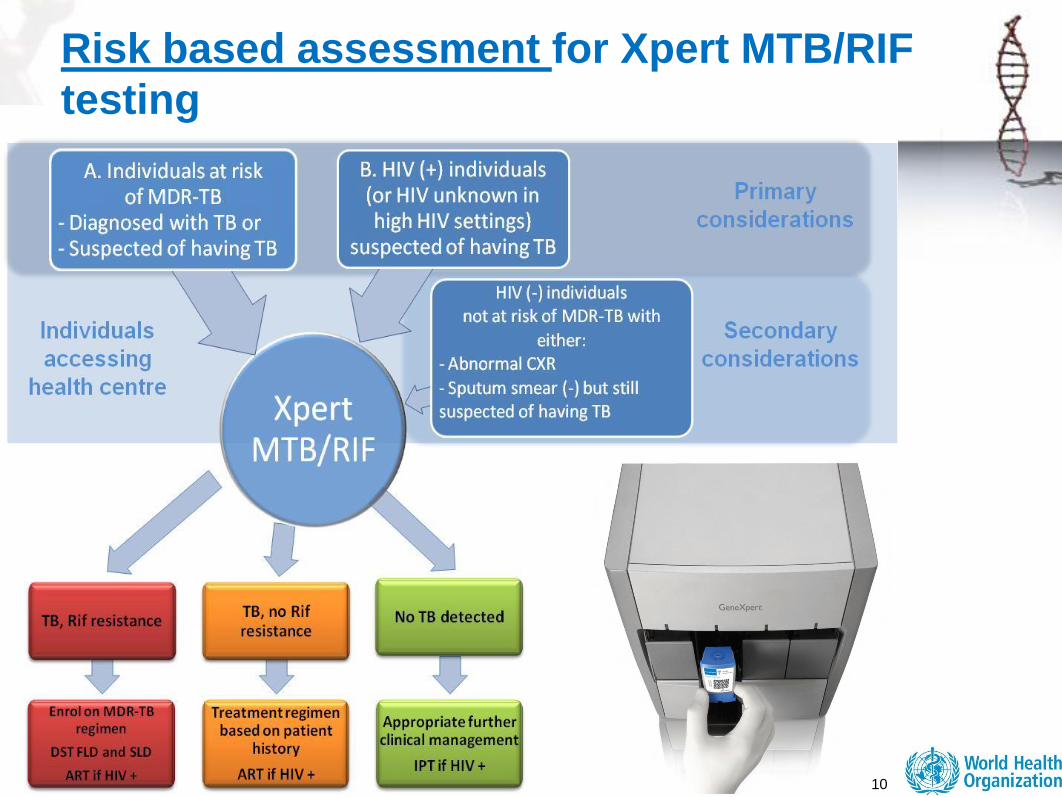
Risk based assessment for Xpert MTB/RIF
testing
10

Where MDR-TB or HIV associated TB is of
lesser concern
Sputum smear microscopy remains the recommended first test for TB
diagnosis.
Pre-test screening strategies for Xpert MTB/RIF testing of all persons
suspected of having TB should be considered to optimise assay
performance, efficiency and cost and will be strongly dependent on
available resources and the TB screening and diagnostic algorithms at
country level. Chest X-ray example
TB suspects who test negative with sputum smear microscopy should
be referred (or their sputum sent) for further testing, preferably in a
facility with Xpert MTB/RIF, if there is clinical suspicion of TB and
sufficient resources are available.
Individuals with sputum smear-positive microscopy results do not need
to be tested with Xpert MTB/RIF unless they belong to the risk groups
described above.
11
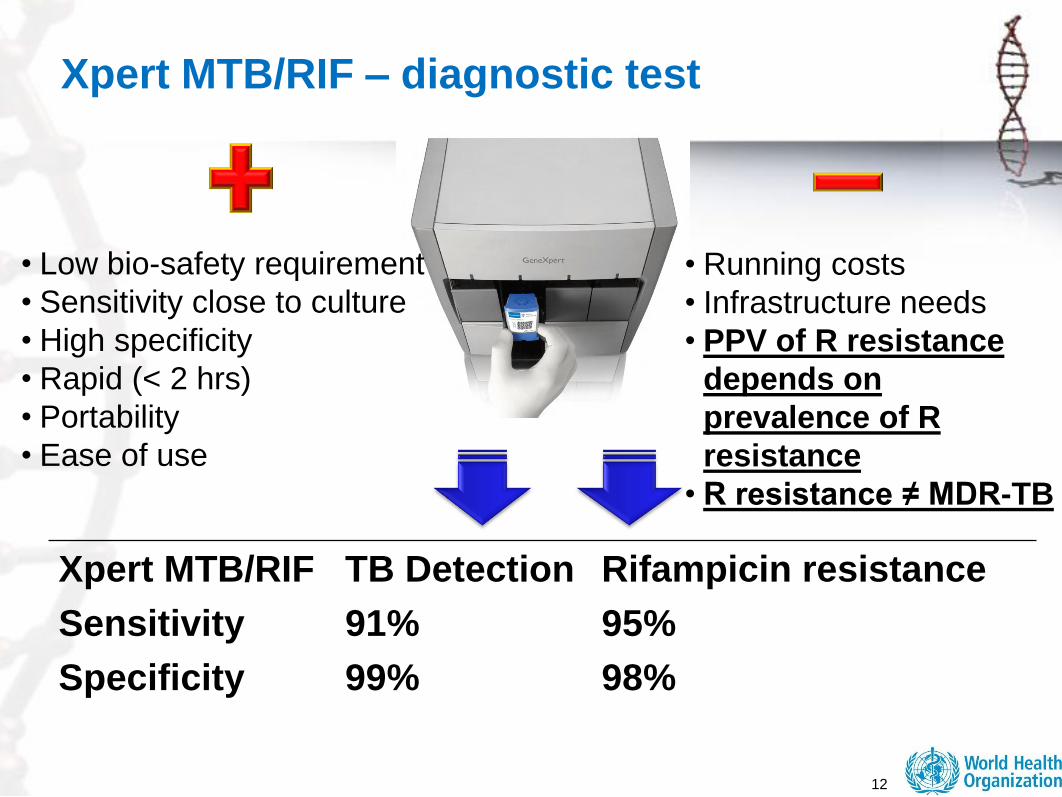
Xpert MTB/RIF – diagnostic test
12
Xpert MTB/RIF TB Detection Rifampicin resistance
Sensitivity 91% 95%
Specificity 99% 98%
• Low bio-safety requirement
• Sensitivity close to culture
• High specificity
• Rapid (< 2 hrs)
• Portability
• Ease of use
• Running costs
• Infrastructure needs
• PPV of R resistance
depends on
prevalence of R
resistance
• R resistance ≠ MDR-TB
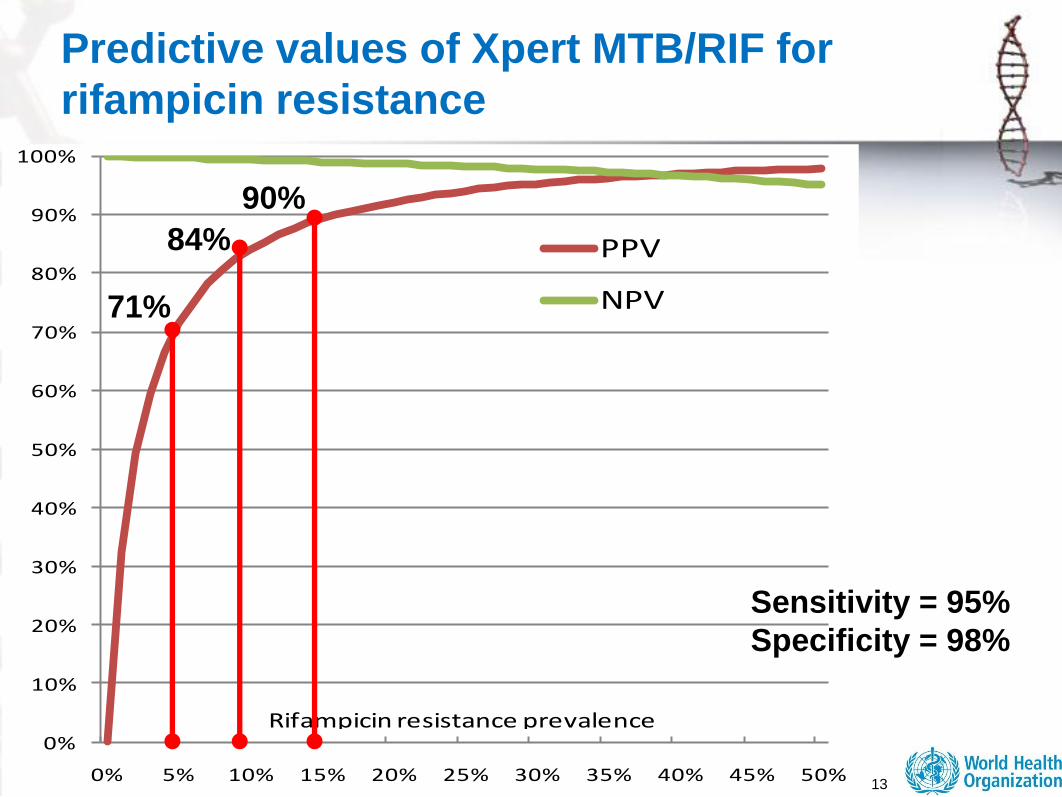
13
Predictive values of Xpert MTB/RIF for
rifampicin resistance
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
PPV
NPV
Rifampicin resistance prevalence
71%
84%
90%
Sensitivity = 95%
Specificity = 98%

Management of patients with MDR-TB
Rifampicin resistance is a reliable proxy for MDR-TB in high burden
settings. Patients with confirmed resistance to rifampicin by Xpert
MTB/RIF should therefore be started on appropriate MDR-TB
treatment immediately and treatment adjusted based on the results of
further DST.
Testing cases not at risk for MDR-TB in low MDR-TB prevalence
settings will result in low PPV for rifampicin resistance, and require that
rifampicin resistance detected by Xpert MTB/RIF be confirmed by
conventional DST or LPA.
TB patients identified by Xpert MTB/RIF without rifampicin
resistance should be referred for appropriate first-line anti-TB
treatment.
If TB is not detected, the individual should be referred for further
investigations and clinical management according to national
guidelines.
14
15
New diagnostics and their potential role in
TB screening/diagnostic algorithms
New diagnostics and their role in TB diagnostic algorithms
New diagnostics and their potential role in TB screening
algorithms
• Medical diagnosis refers to the process of attempting to determine
and/or identify a possible disease or disorder and the opinion reached
by this process that allow medical decisions about treatment and
prognosis to be made.
• Screening - the examination of a group of usually asymptomatic
individuals to detect those with a high probability of having or
developing a given disease.
The American Heritage® Medical Dictionary Copyright © 2007

16
Asymptomatic
?
?

17
Screening for TB and/or MDR-TB?
Wilson and Jungner criteria for screening
1. Condition is an important health problem for individual and community.
2. There is accepted treatment for patients with the disease.
3. The natural history of the disease should be adequately understood.
4. There should be a latent or early symptomatic stage.
5. There should be a suitable and acceptable screening test.
6. Facilities for diagnosis and treatment should be available.
7. There should be an agreed policy on whom to treat as patients.
8. Early treatments has more benefit than treatment started later.
9. The cost should be economically balanced.

2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Dis
tan
ce
fro
m P
ati
en
ts
Peripheral Lab
First Referral Level
Community Health Care
Abbreviations
DST: Drug Susceptibility Test
NAAT: Nucleic Acid Amplification Test
LTBI: Latent TB Infection
POC: Point of Care
MODS: Microscopic observation drug-
susceptibility
NRA: Nitrate reductase assay
CRI: Colorimetric redox indicator assay
LED: Light-emitting diode
LPA: Line probe assay
Technologies or processes endorsed by WHO
Technologies for which WHO review is in process
10-40%
70%
95%
% A
ccess a
fter 5
years
TB Diagnostics pipeline
19
The TB test we need*
• Detection of active TB in adults regardless of HIV
status
• Improved diagnostic in children
• Result that allow decision on treatment initiation
• Patient can receive result on the same day
• Point-of-care: easy to perform in peripheral health
centres
• DST (preferable but not minimum requirement)
• Need to aim to a NON-sputum sample base test
*MSF led POC TB test consultation, 2009
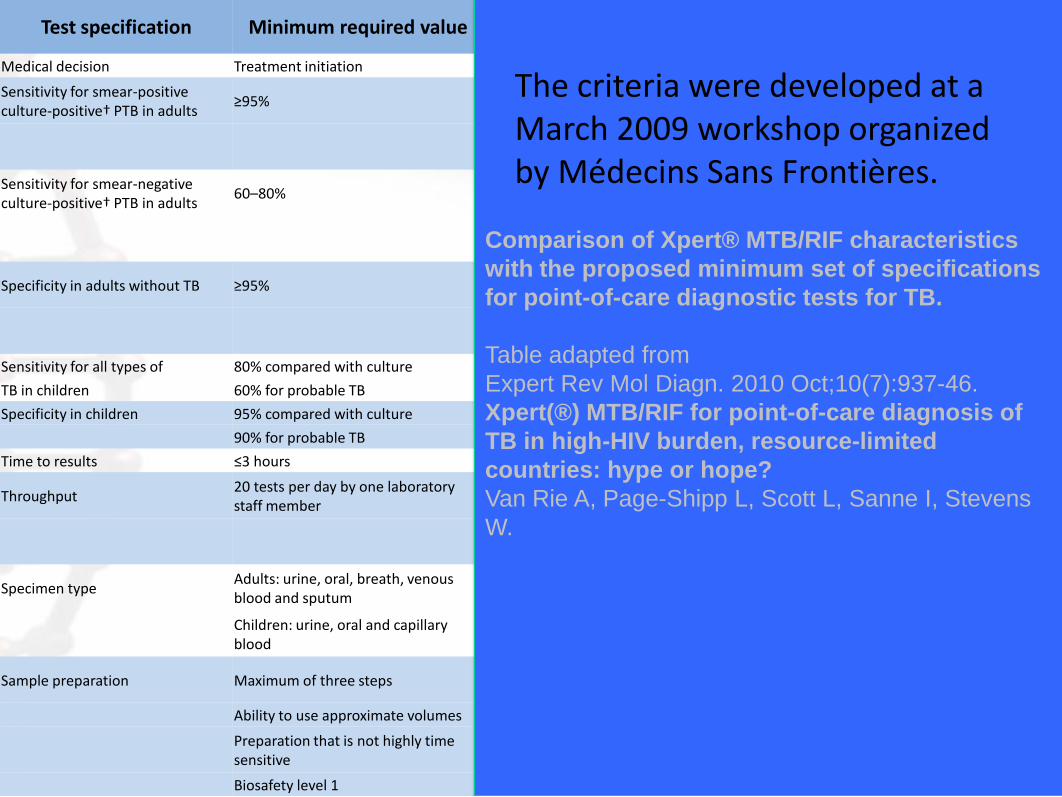
Test specification Minimum required value Xpert MTB/RIF specificationsComparison with
minimum requirementMedical decision Treatment initiation Treatment initiation. Selection of regimen Exceeded
Sensitivity for smear-positive culture-positive† PTB in adults
≥95% 99.8% (95% CI: 99.0–100; three Xpert MTB/RIF assays compared with culture†)
Satisfied
98.2% (95% CI: 96.8–99.0; one Xpert MTB/RIF assay compared with culture†)
Sensitivity for smear-negative culture-positive† PTB in adults
60–80% 90.2% (95% CI: 84.9–93.8; three Xpert MTB/RIF assays compared with culture†)
Satisfied
72.5% (95% CI: 42.4–79.9; one Xpert MTB/RIF assay compared with culture†)
Specificity in adults without TB ≥95% 98.1% (95% CI: 96.6–98.9; three Xpert MTB/RIF assays compared with culture)
Satisfied
99.2% (95% CI: 98.1 –99.6; one Xpert MTB/RIF assay compared with culture)
Sensitivity for all types of 80% compared with culture No data available No data
TB in children 60% for probable TB
Specificity in children 95% compared with culture No data available No data
90% for probable TB
Time to results ≤3 hours 2 h Exceeded
Throughput 20 tests per day by one laboratory staff member
Total hands-on time of 2 min Satisfied
Total daily throughput depends on the size of the instrument
Specimen type Adults: urine, oral, breath, venous blood and sputum
Sputum Satisfied
Children: urine, oral and capillary blood
May work with other samples except for venous blood
Sample preparation Maximum of three steps Two steps: sputum liquefaction followed by loading of sample into cartridge
Exceeded
Ability to use approximate volumes Cartridges can handle a variety of starting volumes Satisfied
Preparation that is not highly time sensitive
Preparation not highly time sensitive Satisfied
Biosafety level 1 Biosafety level 1 Satisfied
Comparison of Xpert® MTB/RIF characteristics
with the proposed minimum set of specifications
for point-of-care diagnostic tests for TB.
Table adapted from
Expert Rev Mol Diagn. 2010 Oct;10(7):937-46.
Xpert(®) MTB/RIF for point-of-care diagnosis of
TB in high-HIV burden, resource-limited
countries: hype or hope?
Van Rie A, Page-Shipp L, Scott L, Sanne I, Stevens
W.
The criteria were developed at a March 2009 workshop organized by Médecins Sans Frontières.
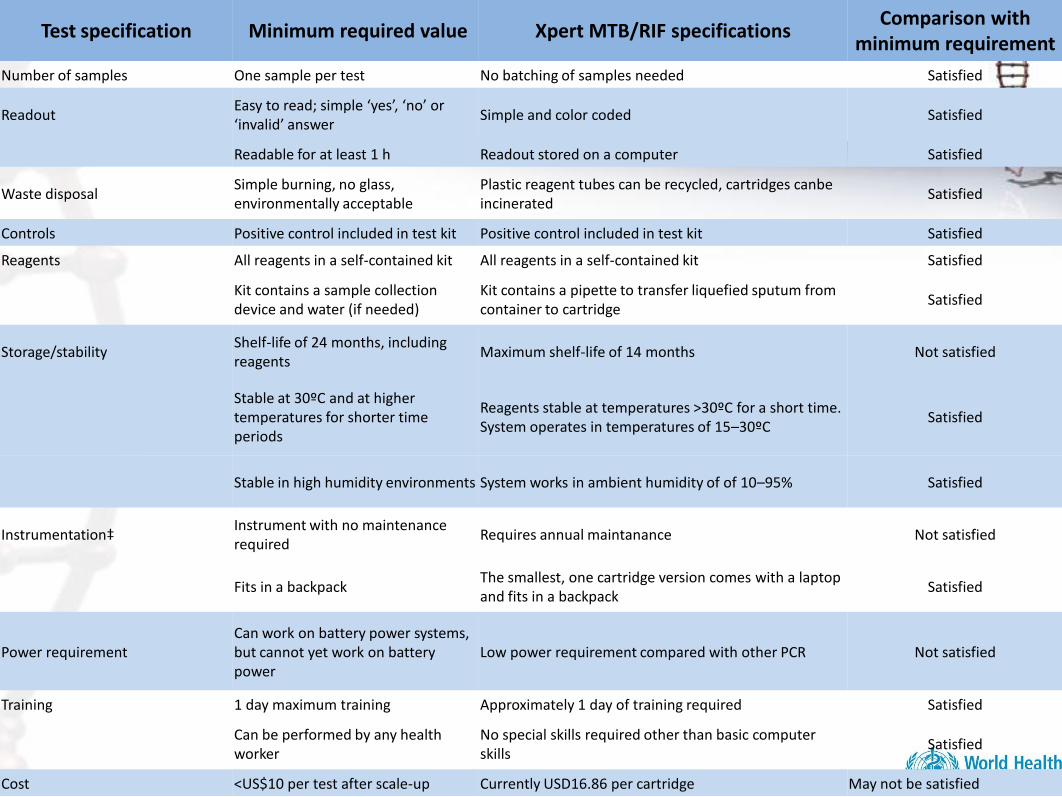
Test specification Minimum required value Xpert MTB/RIF specificationsComparison with
minimum requirement
Number of samples One sample per test No batching of samples needed Satisfied
Readout Easy to read; simple ‘yes’, ‘no’ or ‘invalid’ answer
Simple and color coded Satisfied
Readable for at least 1 h Readout stored on a computer Satisfied
Waste disposal Simple burning, no glass, environmentally acceptable
Plastic reagent tubes can be recycled, cartridges canbe incinerated
Satisfied
Controls Positive control included in test kit Positive control included in test kit Satisfied
Reagents All reagents in a self-contained kit All reagents in a self-contained kit Satisfied
Kit contains a sample collection device and water (if needed)
Kit contains a pipette to transfer liquefied sputum from container to cartridge
Satisfied
Storage/stability Shelf-life of 24 months, including reagents
Maximum shelf-life of 14 months Not satisfied
Stable at 30ºC and at higher temperatures for shorter time periods
Reagents stable at temperatures >30ºC for a short time. System operates in temperatures of 15–30ºC
Satisfied
Stable in high humidity environments System works in ambient humidity of of 10–95% Satisfied
Instrumentation‡ Instrument with no maintenance required
Requires annual maintanance Not satisfied
Fits in a backpack The smallest, one cartridge version comes with a laptop and fits in a backpack
Satisfied
Power requirement Can work on battery power systems, but cannot yet work on battery power
Low power requirement compared with other PCR Not satisfied
Training 1 day maximum training Approximately 1 day of training required Satisfied
Can be performed by any health worker
No special skills required other than basic computer skills
Satisfied
Cost <US$10 per test after scale-up Currently USD16.86 per cartridge May not be satisfied

22
THANK YOU





























