Embed Size (px)
Citation preview
ECMO: Choice/Technique
Joseph B. Zwischenberger MD Johnston-Wright Professor
Chairman: Department of SurgerySurgeon-in-Chief UK Healthcare
859-229-6635 (mobile)[email protected]
The University of KentuckyLexington, Kentucky
Presenter Disclosure Information
Research supported in part through • Competitive funding: National Institutes of Health (SBIR,STTR,T-32)• Contracts:MC3, Ann Arbor MiExotherm, Lexington Ky W-Z Biotek, Lexington KyMaquet
Patent: Avalon Elite™ (4 more, 3 pending)NovalungFree App: “Zwisch Me”
Joseph B. Zwischenberger, M.D.
Bartlett/Zwischenberger 1984
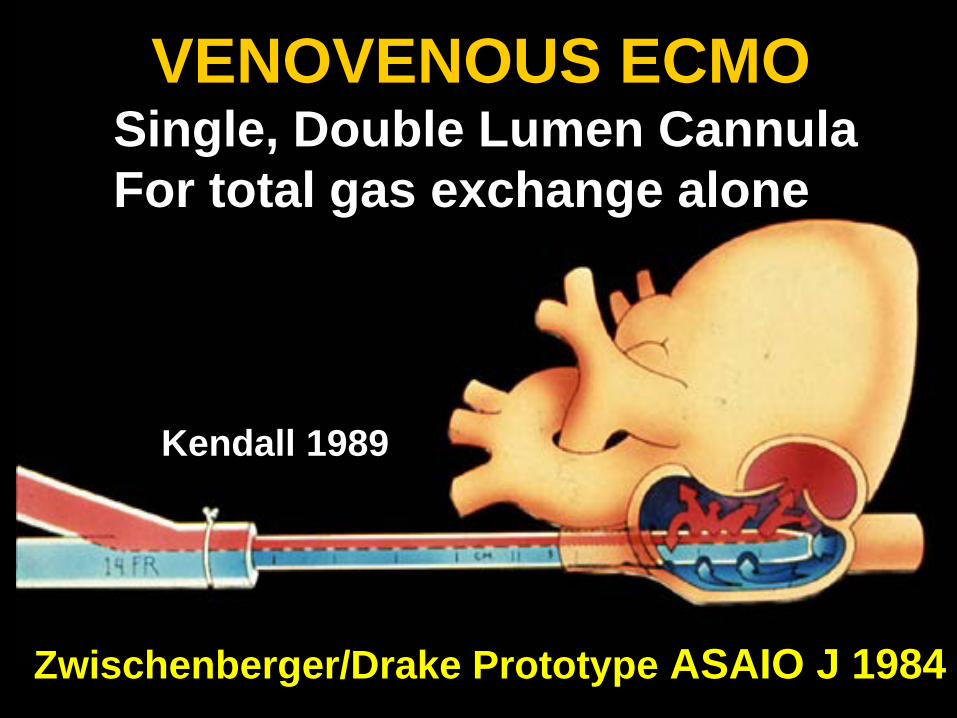
VENOVENOUS ECMOSingle, Double Lumen CannulaFor total gas exchange alone
Zwischenberger/Drake Prototype ASAIO J 1984
Kendall 1989
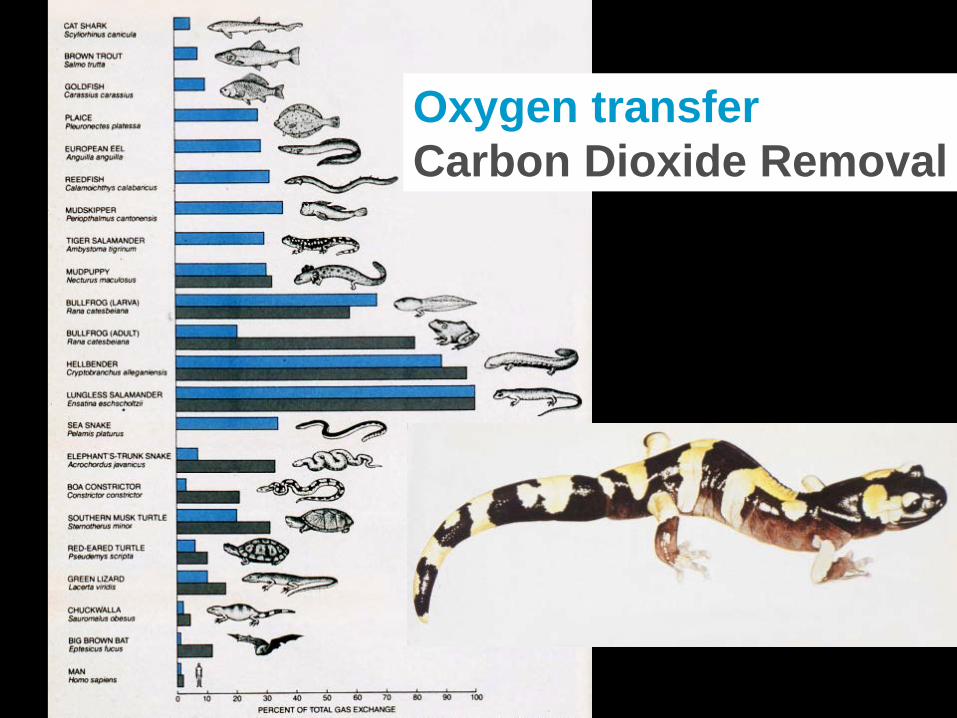
Oxygen transferCarbon Dioxide Removal

CO2 RemovalCO2 removal and O2 transfer are
uncoupled: – CO2 is transferred across the
membrane gas exchanger– Low Frequency Ventilation:
O2 diffuses across the native lungs
Ted Kolobow 1977

AVCO2R: Carbon Dioxide Removal (get the bad air out) with a low-resistance gas exchanger in a simple arterio-venous shunt
Zwischenberger 1996
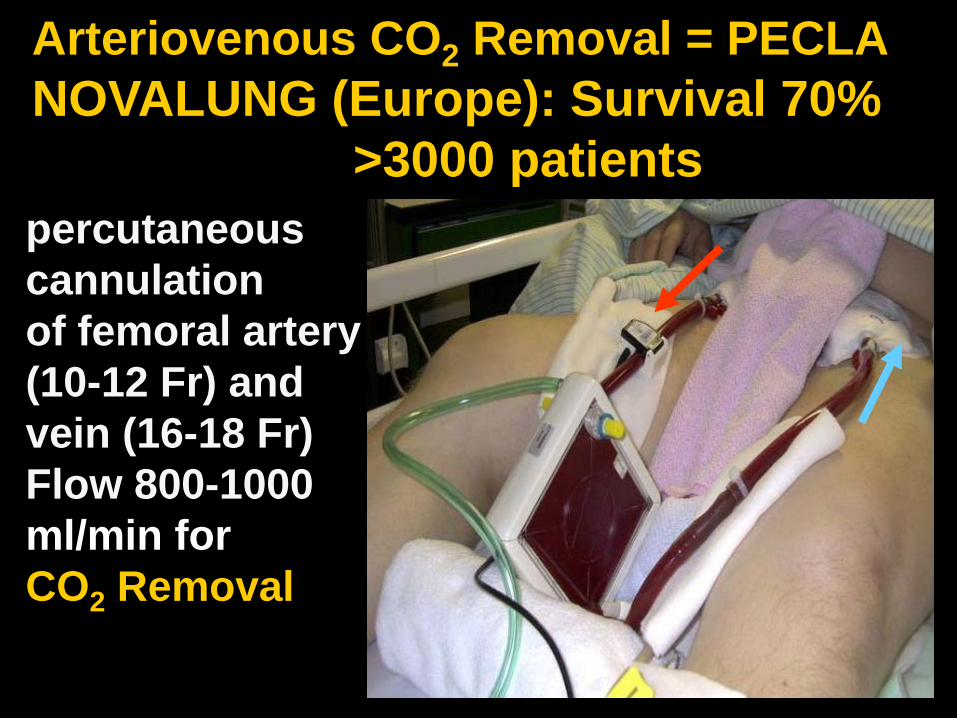
percutaneouscannulationof femoral artery(10-12 Fr) andvein (16-18 Fr)Flow 800-1000 ml/min forCO2 Removal
Arteriovenous CO2 Removal = PECLANOVALUNG (Europe): Survival 70%
>3000 patients

Impact of CO2 Homeostasis
CO2 flux is greatly reduced by AVCO2R, and may be important in:
• organ tissue neutrophil apoptosis • resolution of inflammation• maintaining a normal alveolar milieu
Zwischenberger et. al. Ann Surg 2007;246:512-521
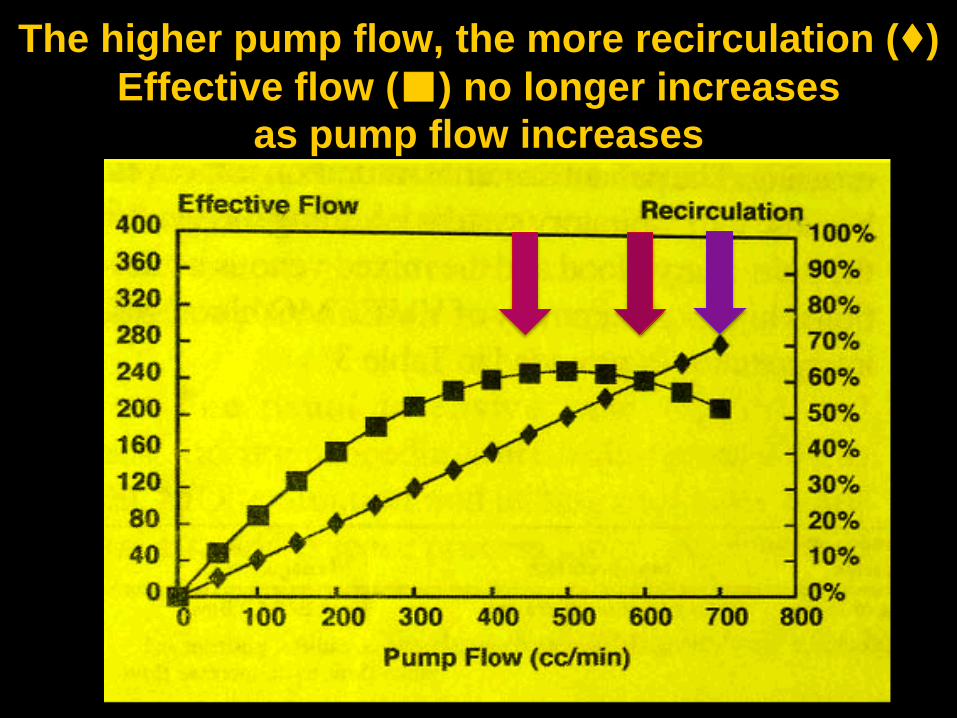
The higher pump flow, the more recirculation (♦)Effective flow (■) no longer increases
as pump flow increases
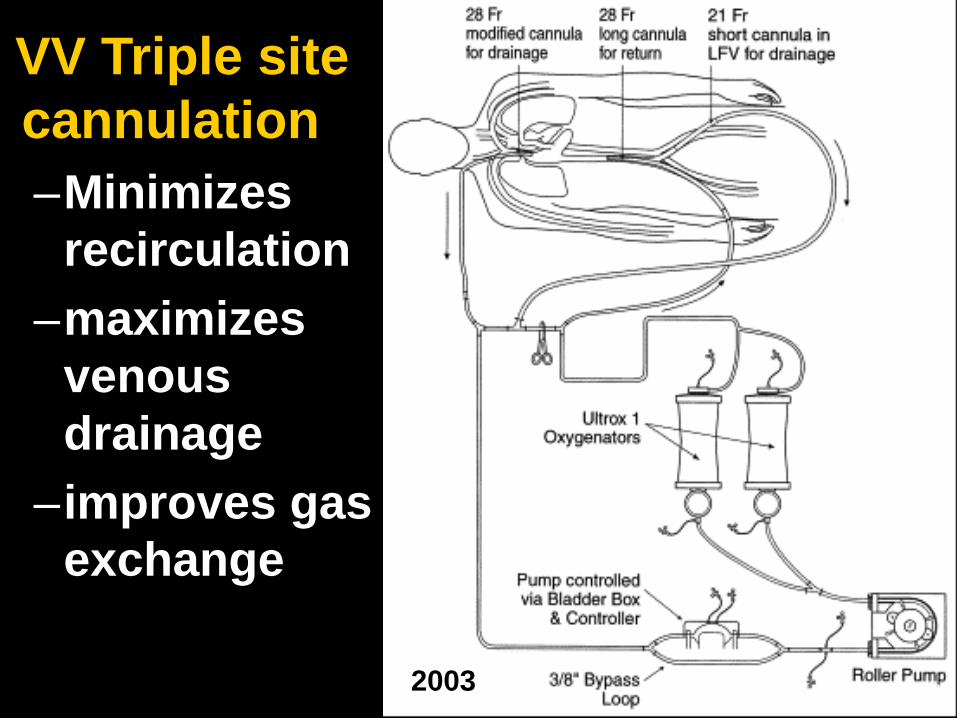
VV Triple site cannulation–Minimizes
recirculation –maximizes
venous drainage
–improves gas exchange
2003
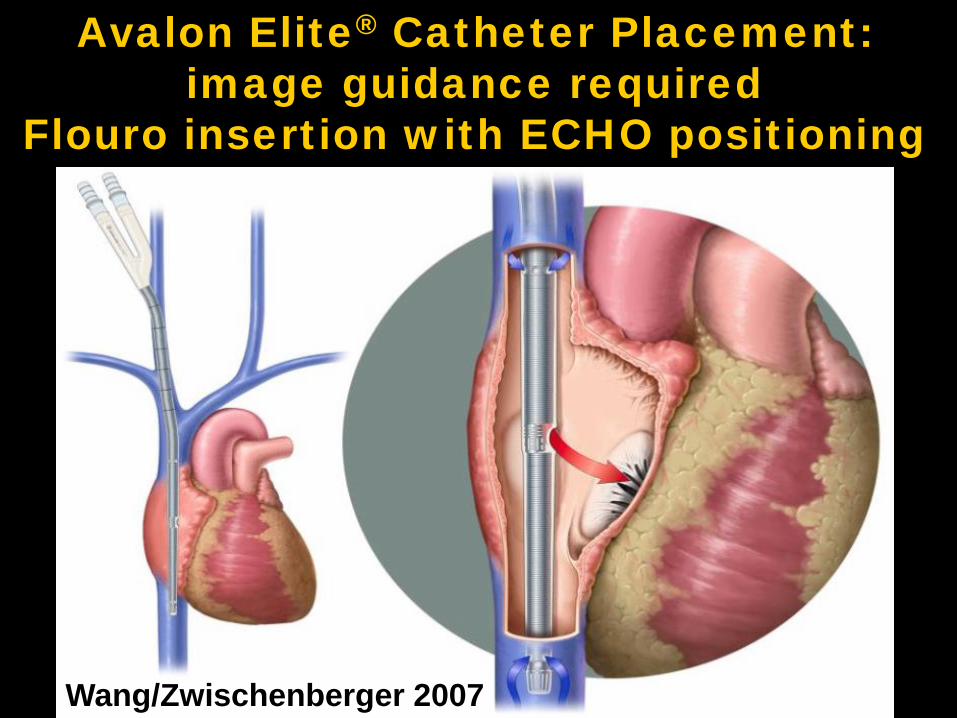
Avalon Elite® Catheter Placement: image guidance required
Flouro insertion with ECHO positioning
Wang/Zwischenberger 2007
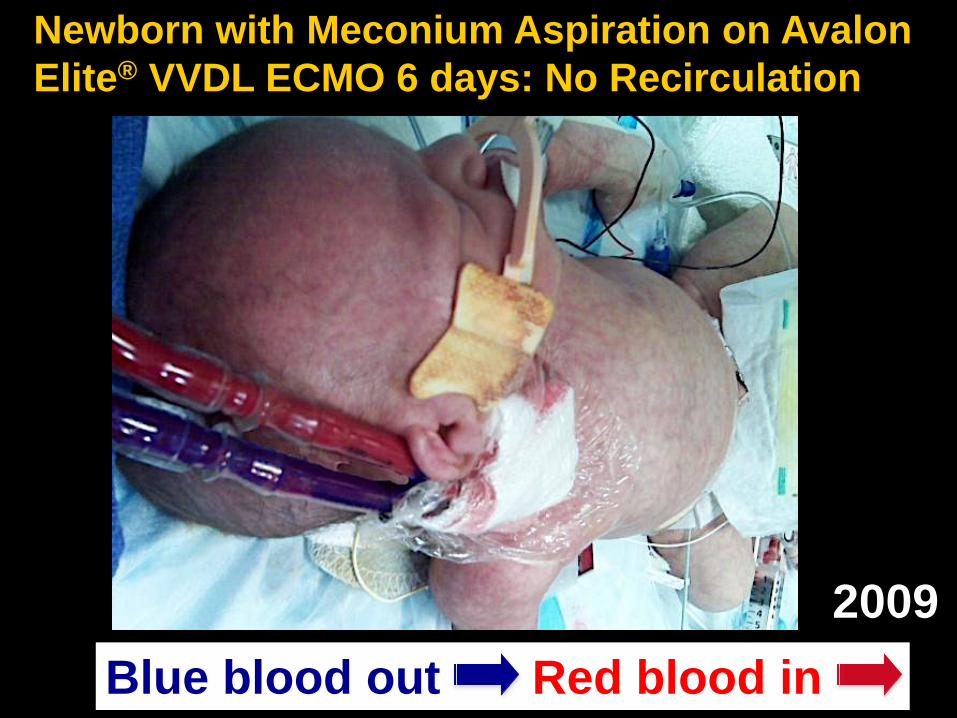
Newborn with Meconium Aspiration on Avalon Elite® VVDL ECMO 6 days: No Recirculation
Blue blood out Red blood in2009
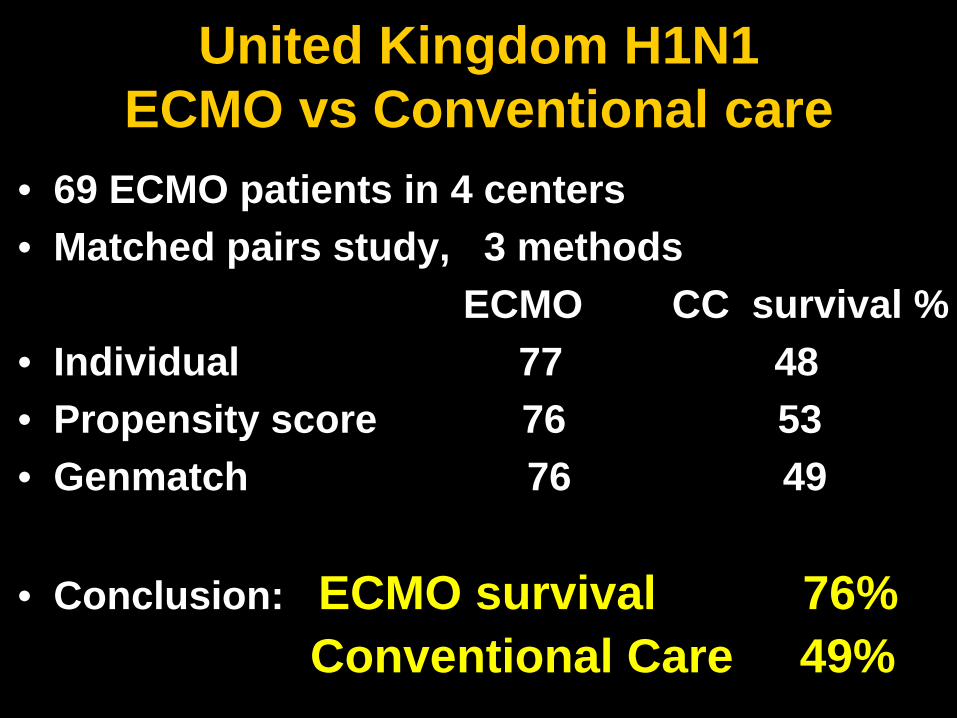
United Kingdom H1N1ECMO vs Conventional care
• 69 ECMO patients in 4 centers• Matched pairs study, 3 methods
ECMO CC survival %• Individual 77 48• Propensity score 76 53• Genmatch 76 49
• Conclusion: ECMO survival 76%Conventional Care 49%
IVC
SVC
RV
TV
IVC
SVC
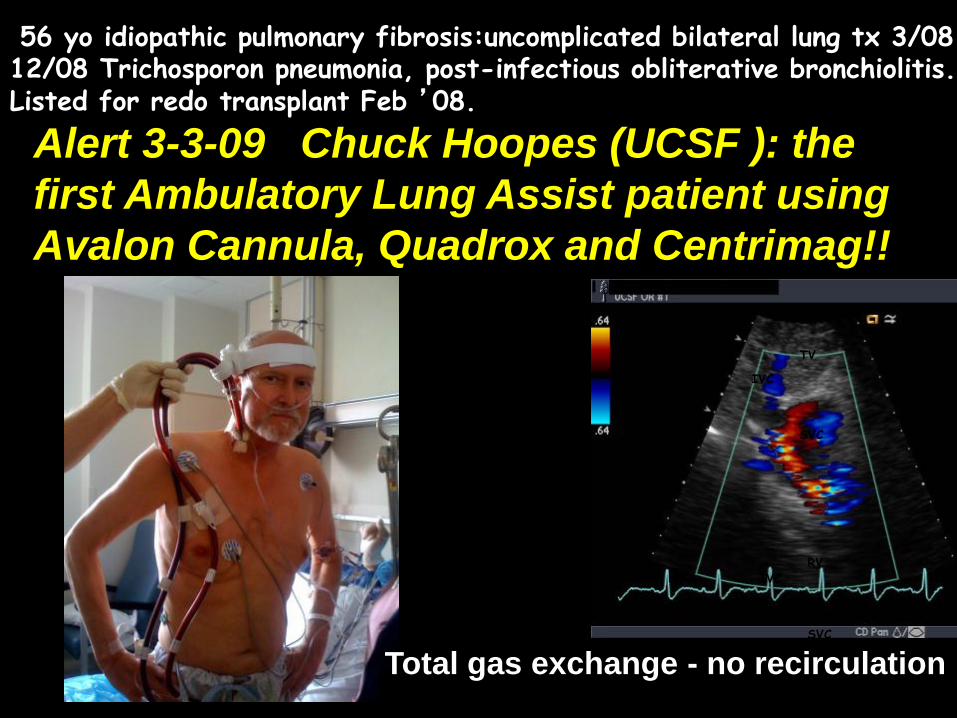
56 yo idiopathic pulmonary fibrosis:uncomplicated bilateral lung tx 3/08 12/08 Trichosporon pneumonia, post-infectious obliterative bronchiolitis. Listed for redo transplant Feb ’08.
Alert 3-3-09 Chuck Hoopes (UCSF ): the first Ambulatory Lung Assist patient using Avalon Cannula, Quadrox and Centrimag!!
Total gas exchange - no recirculation



Exercise at the bedside
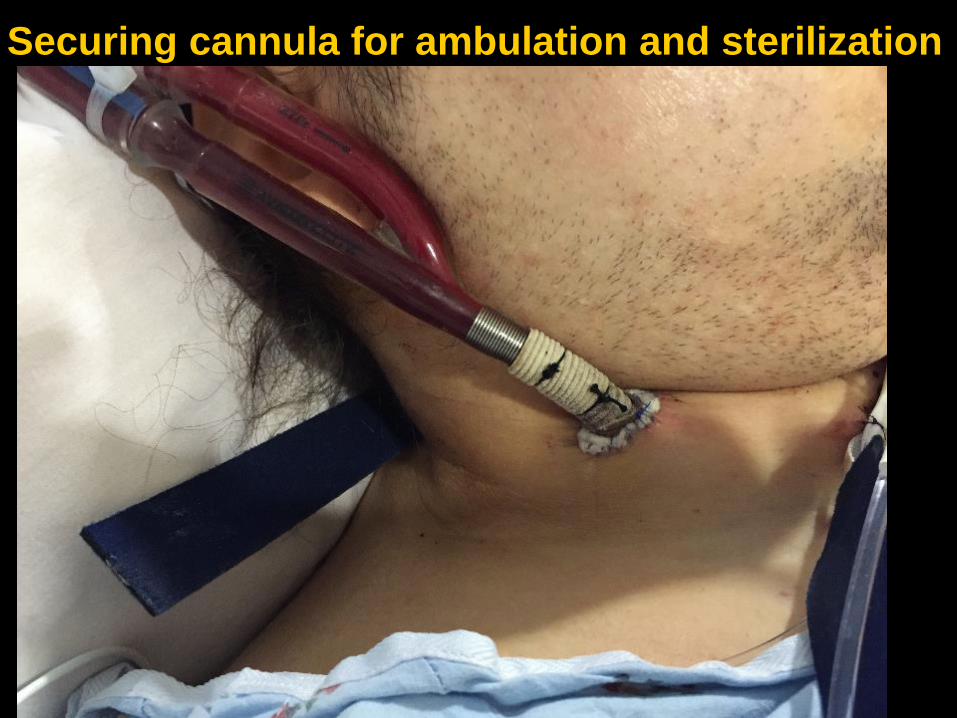
Securing cannula for ambulation and sterilization
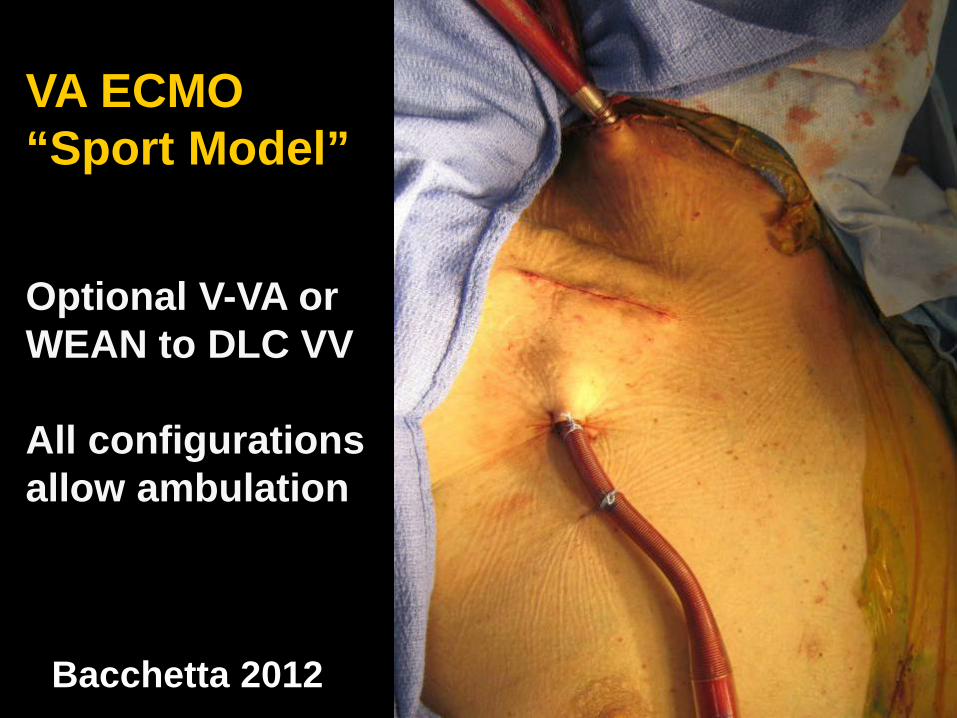
VA ECMO “Sport Model”
Optional V-VA or WEAN to DLC VV
All configurations allow ambulation
Bacchetta 2012

21
Tips for percutaneous technique 1• Guidewire placement
– Ultrasound – vessel identification• Vascular transducer to guide needle
– Fluoroscopy – ensures guidewire location• Encouraged for single-lumen cannula placement• Recommended for dual-lumen cannula
placement– Echocardiography
• Precise placement for flow: dual-lumen cannula• Guidewire should have no resistance
22
Complications - prevention Vessel perforation Ultrasound for intraluminal placement Fluoroscopy to identify guidewire Atrial perforation Fluoroscopy for guidewire placement Wrong vessel cannulation Ultrasound for vessel identification Inadequate drainage Malpositioning Inadequate cannula size
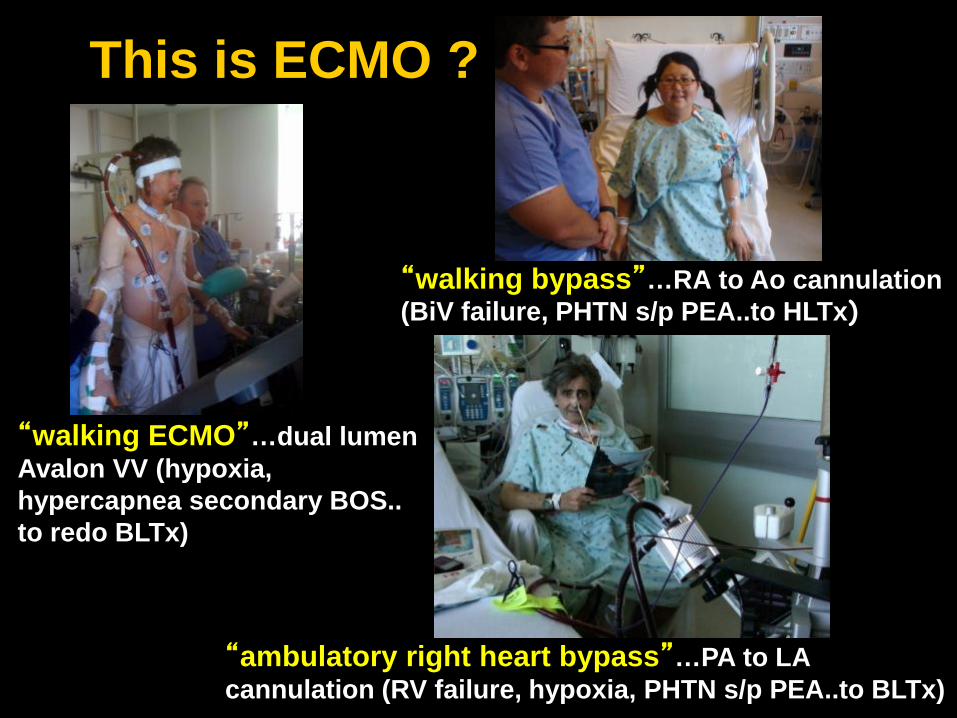
This is ECMO ?
“walking ECMO”…dual lumen Avalon VV (hypoxia, hypercapnea secondary BOS.. to redo BLTx)
“ambulatory right heart bypass”…PA to LA cannulation (RV failure, hypoxia, PHTN s/p PEA..to BLTx)
“walking bypass”…RA to Ao cannulation(BiV failure, PHTN s/p PEA..to HLTx)
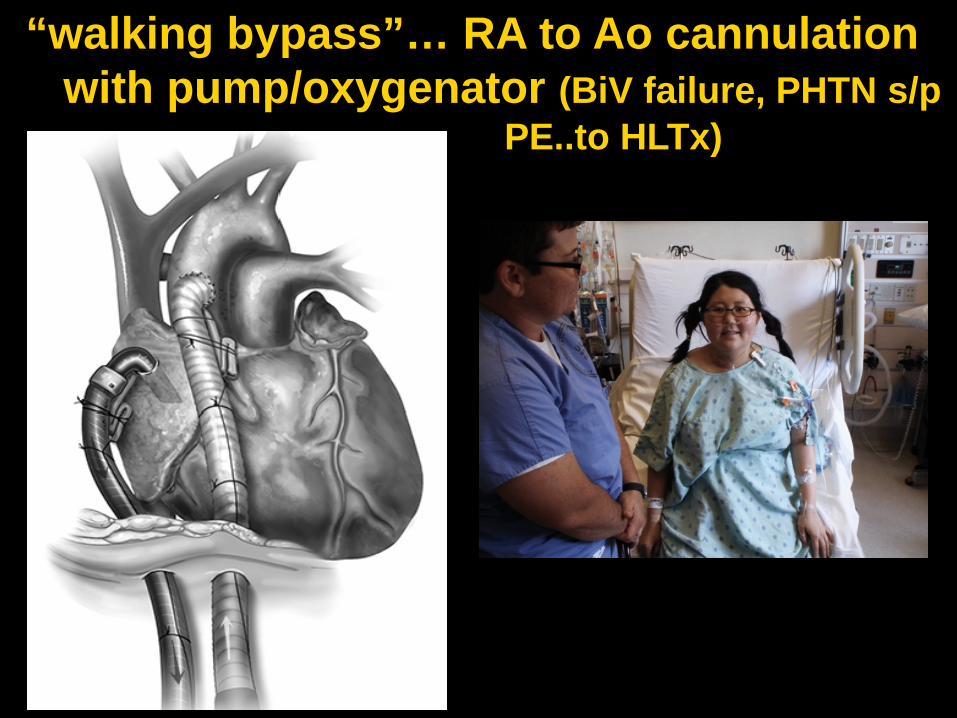
“walking bypass”… RA to Ao cannulationwith pump/oxygenator (BiV failure, PHTN s/p
PE..to HLTx)
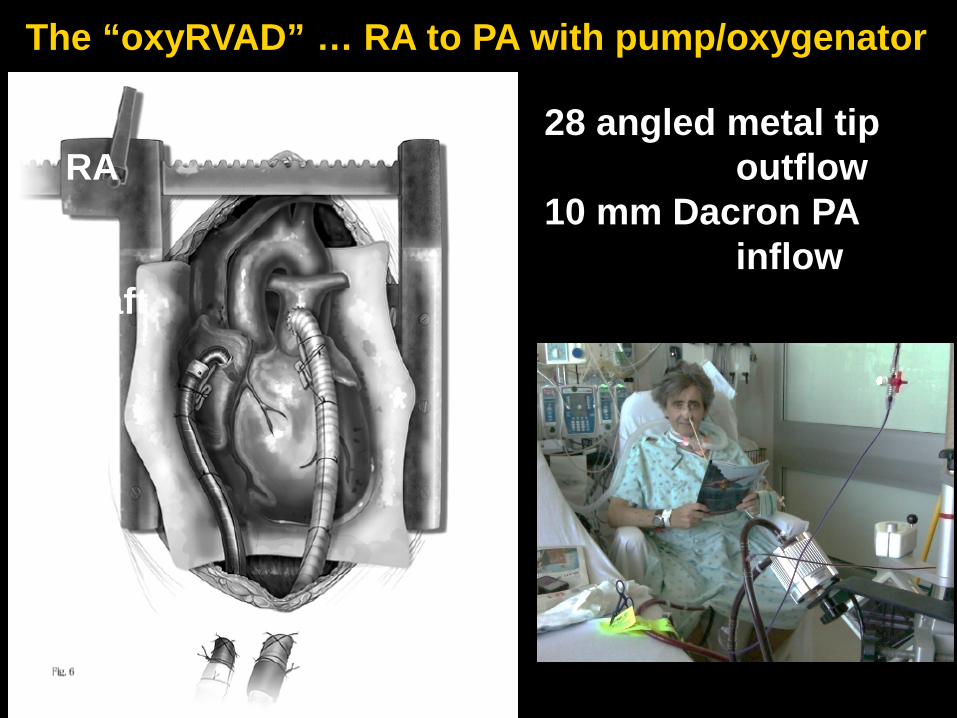
28 angled metal tip RA outflow
10 mm Dacron PA inflow
graft
The “oxyRVAD” … RA to PA with pump/oxygenator
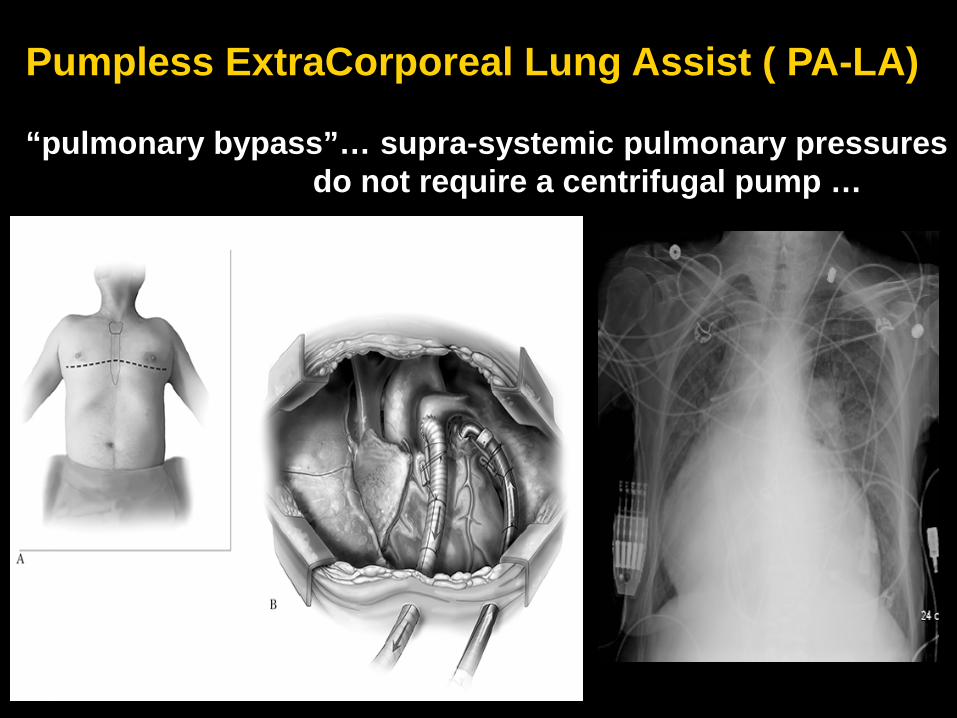
Pumpless ExtraCorporeal Lung Assist ( PA-LA)
“pulmonary bypass”… supra-systemic pulmonary pressures do not require a centrifugal pump …
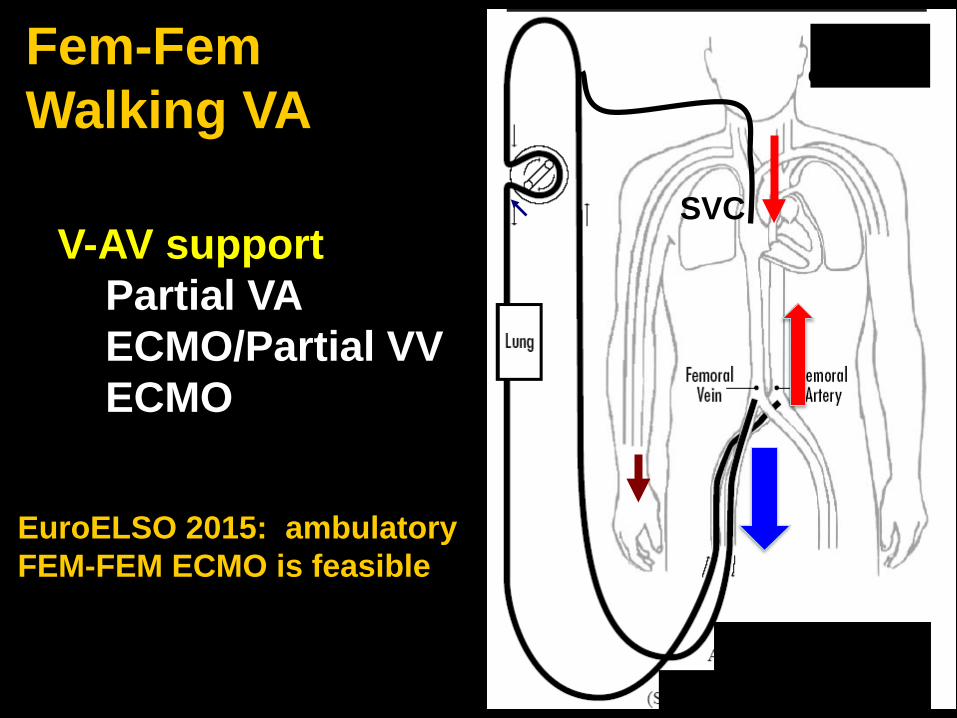
Fem-Fem Walking VA
V-AV supportPartial VA ECMO/Partial VV ECMO
SVC
EuroELSO 2015: ambulatory FEM-FEM ECMO is feasible
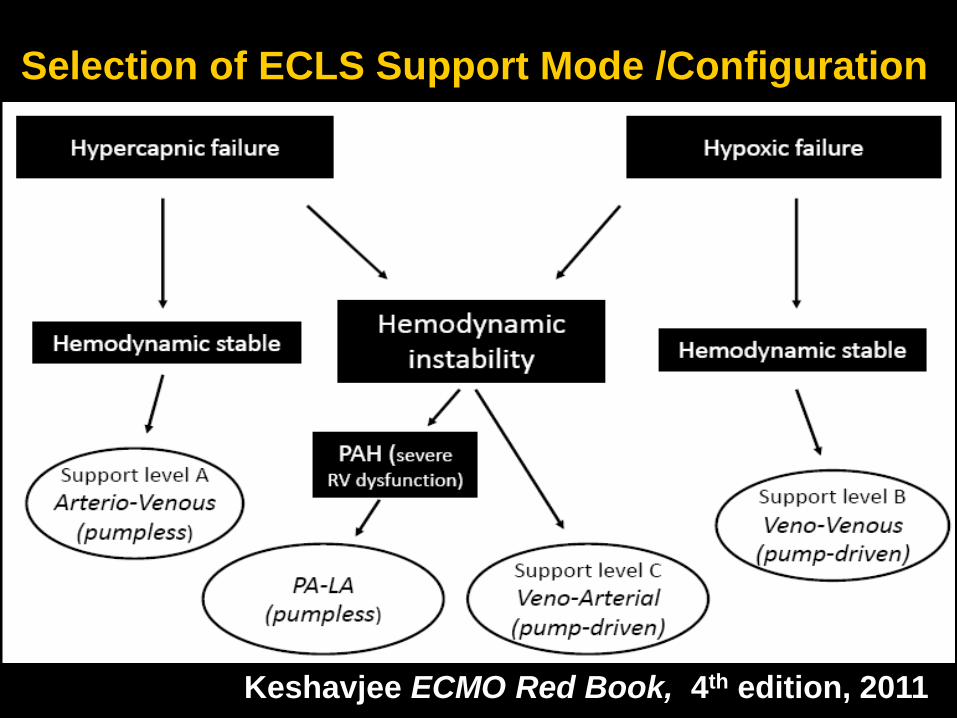
Keshavjee ECMO Red Book, 4th edition, 2011
Selection of ECLS Support Mode /Configuration

*prevent barotrauma and activation of inflammatory mediators
*Limit end organ injury
*avoid sedation and muscle atrophy (frailty)
VV DLC ECMO pre BLTx (cystic fibrosis)
Does anyone with severe respiratory failure really benefit from mechanical intubation and positive pressure ventilation? …..With ECMO…..
20/22 consecutive ambulatory ECMO adult patients are alive to 6 months
AATS 5/2015: 12 ECMO talks
AATS Guidelines: Bridge to transplant and Extracorporeal lung support: Ambulatory ECMO recommended
(Bacchetta and Cypel 2015)
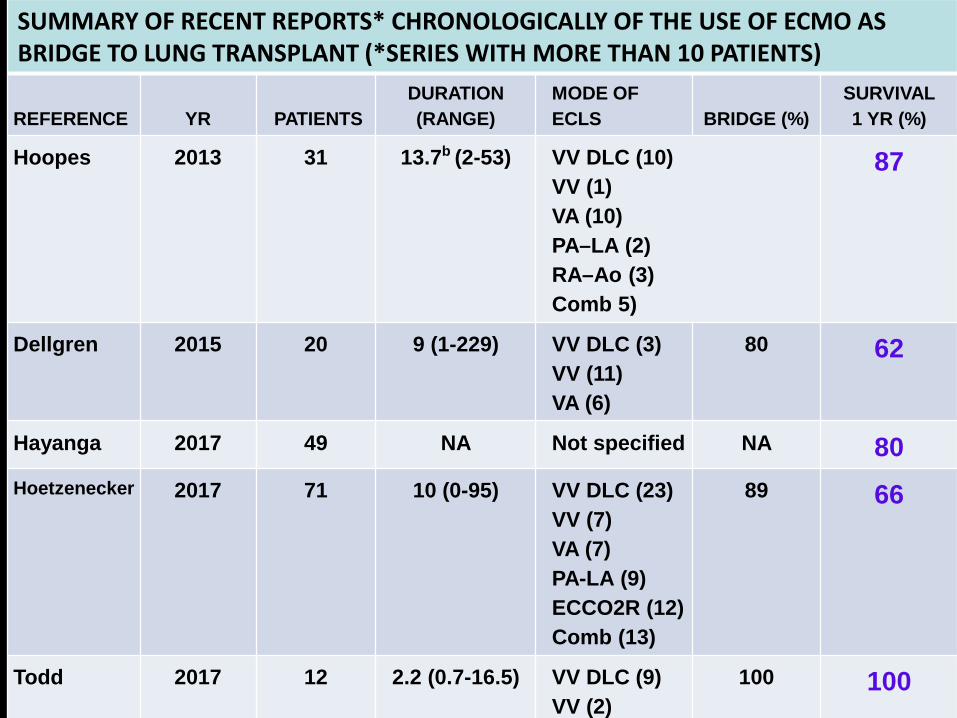
SUMMARY OF RECENT REPORTS* CHRONOLOGICALLY OF THE USE OF ECMO AS BRIDGE TO LUNG TRANSPLANT (*SERIES WITH MORE THAN 10 PATIENTS)
REFERENCE YR PATIENTSDURATION (RANGE)
MODE OF ECLS BRIDGE (%)
SURVIVAL 1 YR (%)
Hoopes 2013 31 13.7b (2-53) VV DLC (10)VV (1)VA (10)PA–LA (2)RA–Ao (3)Comb 5)
87
Dellgren 2015 20 9 (1-229) VV DLC (3)VV (11)VA (6)
80 62
Hayanga 2017 49 NA Not specified NA 80Hoetzenecker 2017 71 10 (0-95) VV DLC (23)
VV (7)VA (7)PA-LA (9)ECCO2R (12)Comb (13)
89 66
Todd 2017 12 2.2 (0.7-16.5) VV DLC (9)VV (2)
100 100
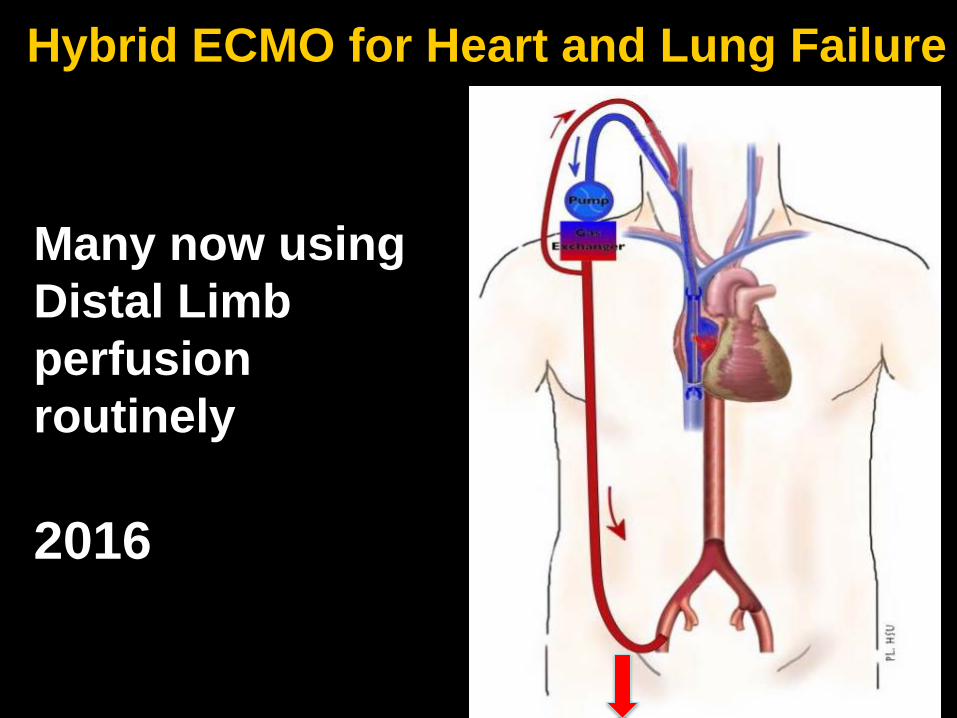
Hybrid ECMO for Heart and Lung Failure
Many now using Distal Limb perfusion routinely
2016
eCPR: ER ECMOSurvey of Centers participating in
Extracorporeal Life Support Organization (ELSO)
• VA ECMO with groin cannulation• Cardiology, CT, Emerg Med, Vascular• Over 33% of centers that submit adult
ECMO perform ED ECMO
Resuscitation 107 (2016) 38-46

Thiagarajan RR, et al. ASAIO 2017, 63(1):60-67
40% Peds
30% Adult
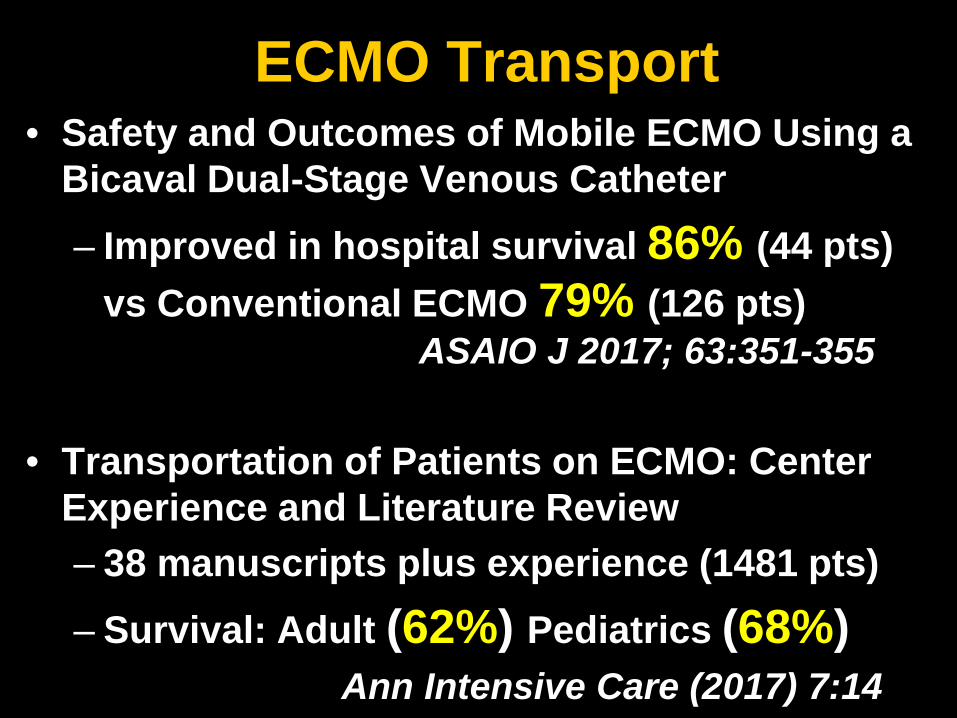
ECMO Transport• Safety and Outcomes of Mobile ECMO Using a
Bicaval Dual-Stage Venous Catheter – Improved in hospital survival 86% (44 pts)
vs Conventional ECMO 79% (126 pts)ASAIO J 2017; 63:351-355
• Transportation of Patients on ECMO: Center Experience and Literature Review– 38 manuscripts plus experience (1481 pts)– Survival: Adult (62%) Pediatrics (68%)
Ann Intensive Care (2017) 7:14
ECMO FUTURECatheter based Technology (Ambulatory)
– Recipient Support– Donor Support: DCD– Organ Block Support : Lung in a Box
Transplantation
Neonates, Children, Adults Acute Severe Respiratory failure Acute Cardiac support
ER Transport Resuscitation/Shock
Will play for drinks and tips
You should ALWAYS listen to a harmonica player
ECMO: Choice/Technique
Joseph B. Zwischenberger MD Johnston-Wright Professor
Chairman: Department of SurgerySurgeon-in-Chief UK Healthcare
859-229-6635 (mobile)[email protected]
The University of KentuckyLexington, Kentucky
ECMO: Cannulation Techniques
Joseph B. Zwischenberger MD Johnston-Wright Professor
Chairman: Department of SurgerySurgeon-in-Chief UK Healthcare
859-229-6635 (mobile)[email protected]
The University of KentuckyLexington, Kentucky
42
Cannulae choiceOxygen Consumption determines
DeliveryNewborn: 5-8 cc O2/kg/minChild: 4-6 cc O2/kg/minAdult: 3-5 cc O2/kg/min
Translated into flow (for normal Hgb)Neonate 100 to 150 mL/min/kgPediatric 75 to 100 mL/min/kgAdult 50 to 75 mL/min/kg
43
Cannulae choiceVenous drainageDetermines the flowDrains bloodPassivelyActively
Venous Drainage will be the most important factor in determining the maximum flowBiggest and Shortest cannula practical
44
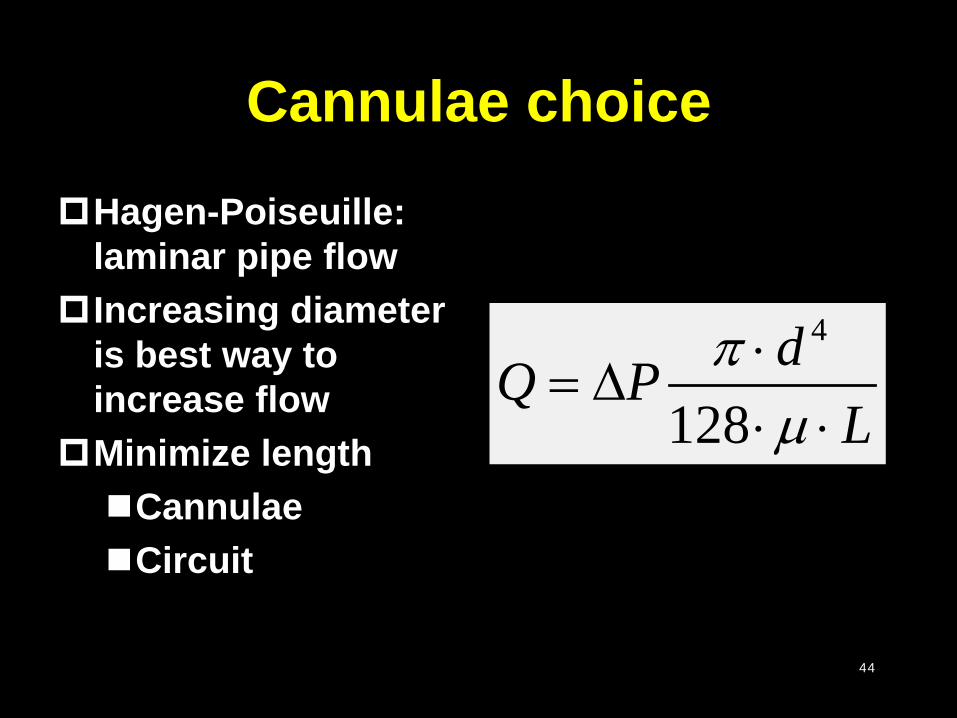
Cannulae choiceHagen-Poiseuille:
laminar pipe flowIncreasing diameter
is best way to increase flow
Minimize lengthCannulaeCircuit
4
128dPQ
Lπ
µ⋅
=⋅ ⋅
∆
45
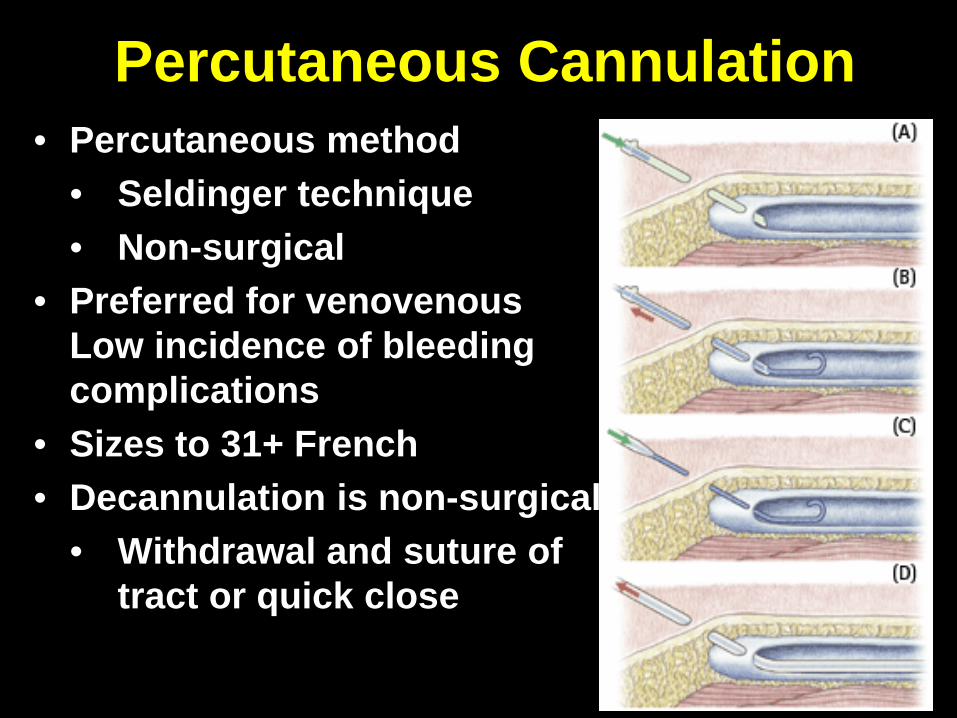
Percutaneous Cannulation• Percutaneous method
• Seldinger technique• Non-surgical
• Preferred for venovenousLow incidence of bleeding complications
• Sizes to 31+ French• Decannulation is non-surgical
• Withdrawal and suture of tract or quick close
46
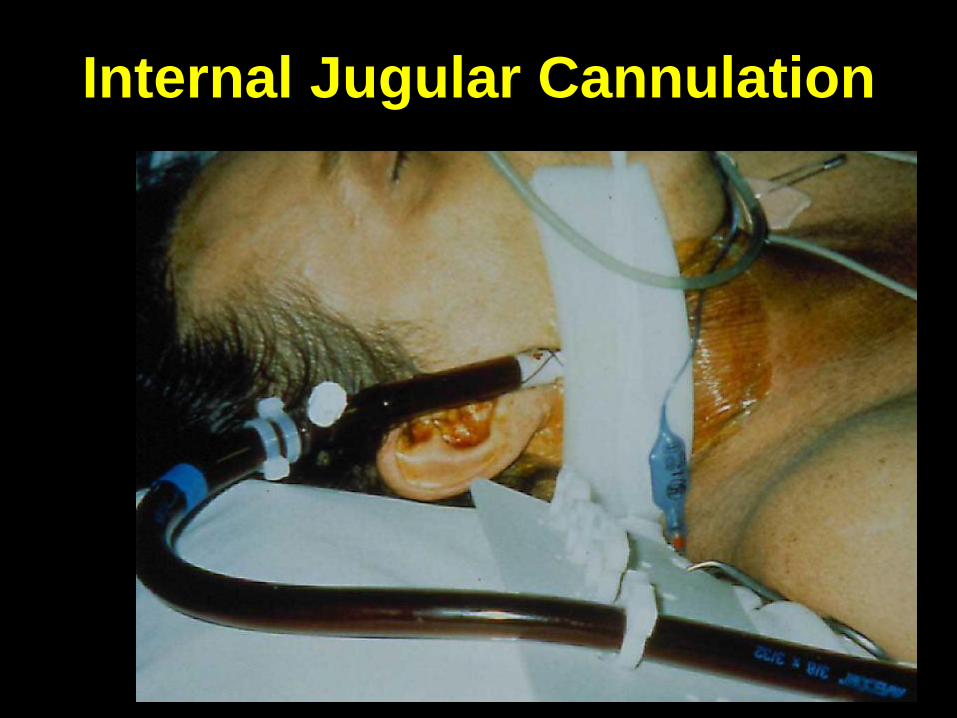
Internal Jugular Cannulation

47
Femoral Vein Cannulation
48
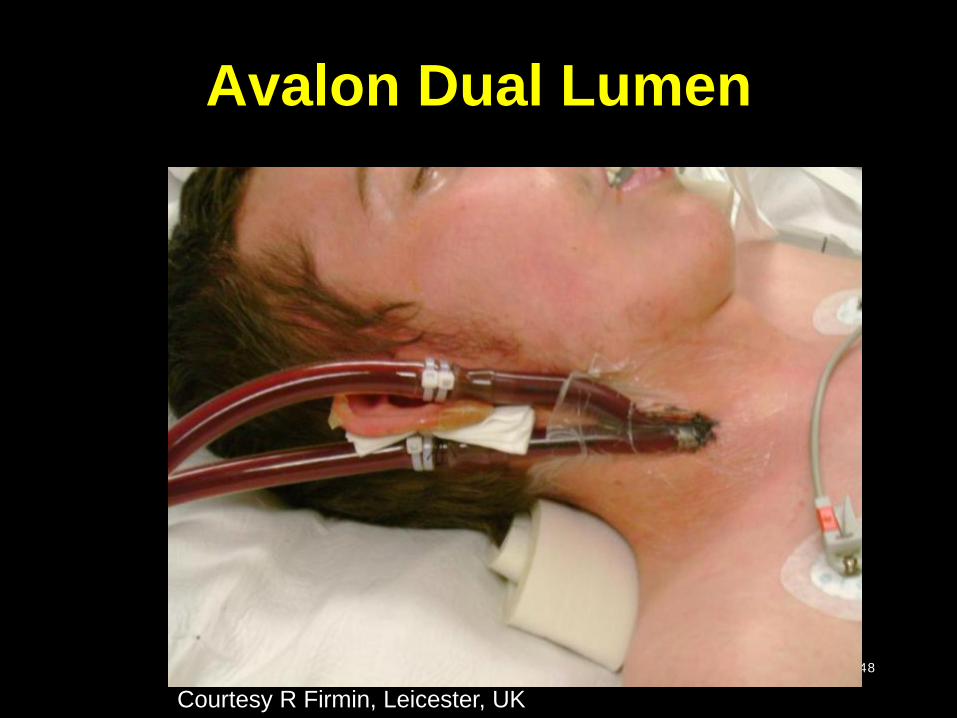
Avalon Dual Lumen
Courtesy R Firmin, Leicester, UK
49
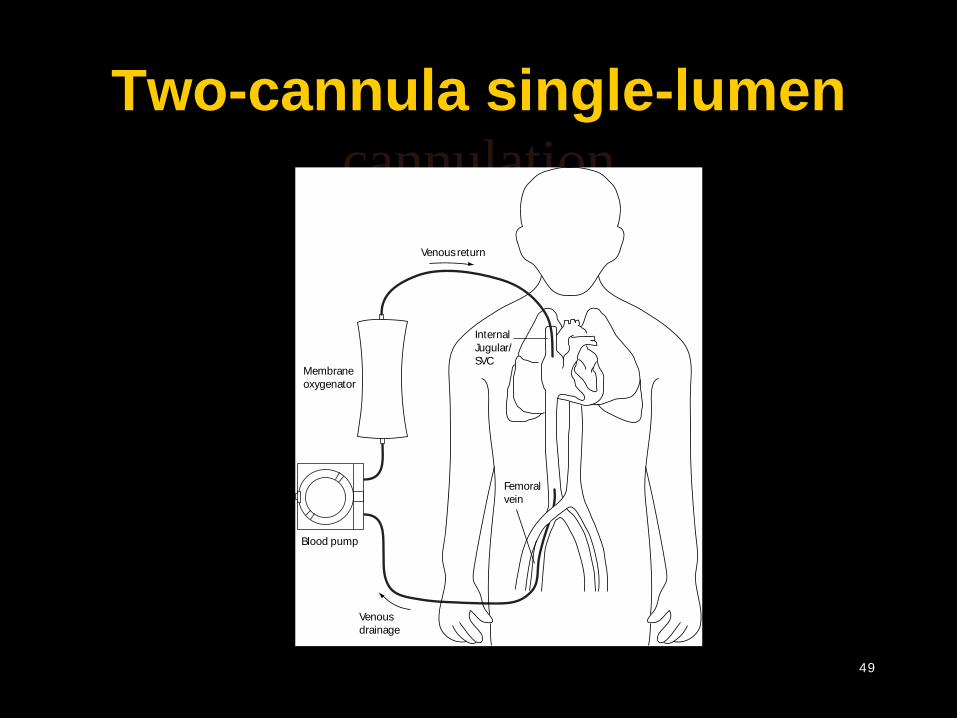
Two-cannula single-lumen cannulation
Venousreturn
Venousdrainage
InternalJugular/SVC
Blood pump
Membraneoxygenator
Femoralvein
50
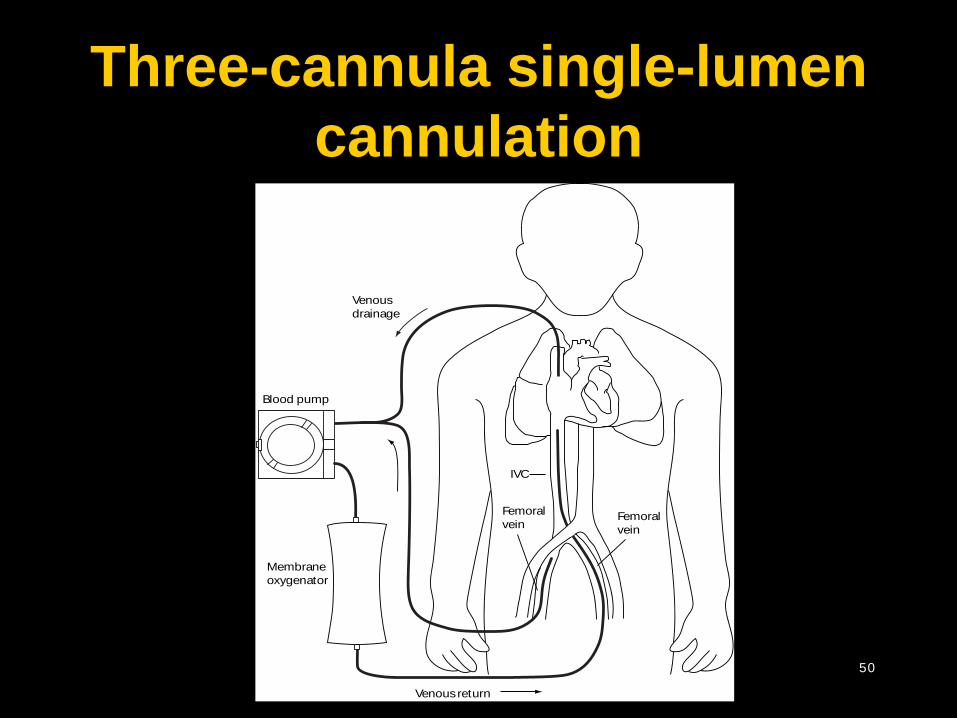
Three-cannula single-lumen cannulation
Venousdrainage
Venousreturn
Femoralvein
IVC
Blood pump
Membraneoxygenator
Femoralvein
51
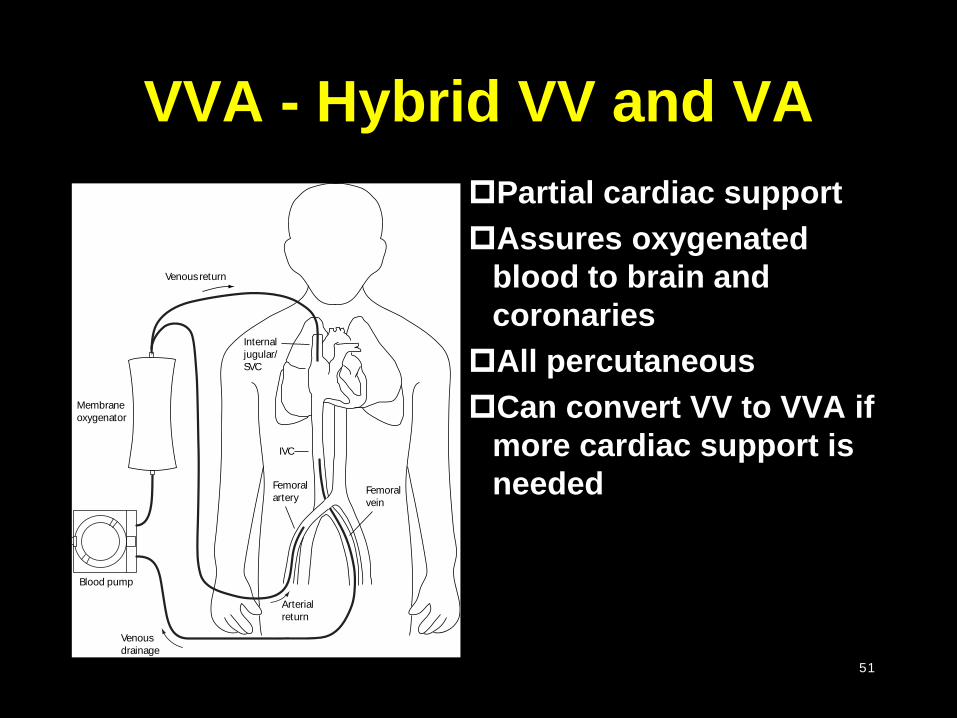
VVA - Hybrid VV and VAPartial cardiac supportAssures oxygenated
blood to brain and coronariesAll percutaneousCan convert VV to VVA if
more cardiac support is needed
Venousdrainage
Venousreturn
Femoralvein
IVC
Blood pump
Membraneoxygenator
Femoralartery
Arterialreturn
Internaljugular/SVC
52
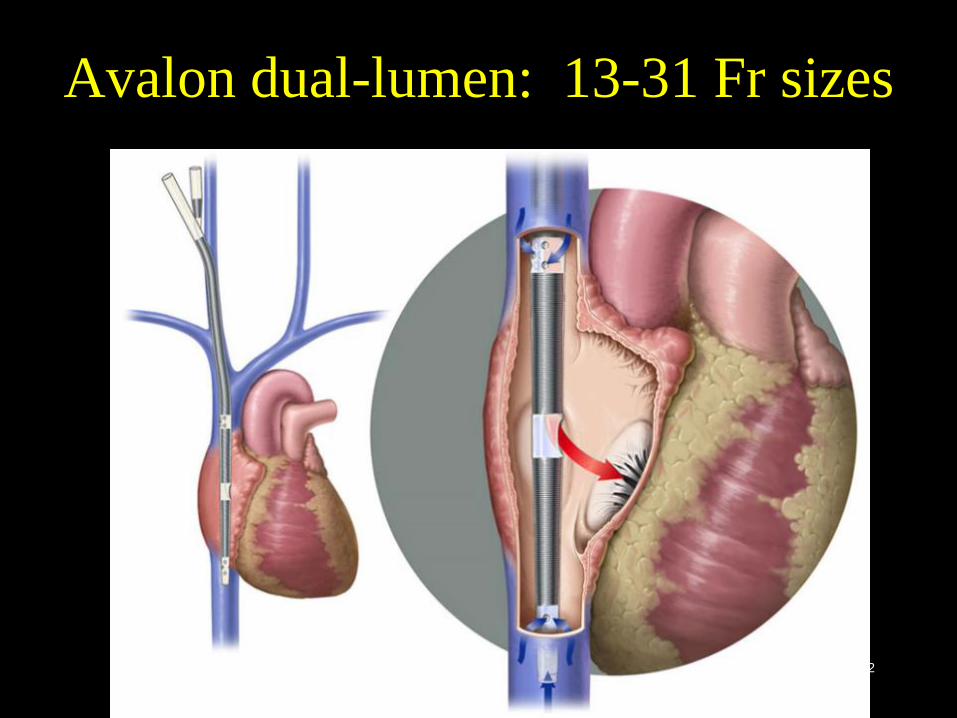
Avalon dual-lumen: 13-31 Fr sizes
Unconventional Institutional Volume Outcome Associations in
Adult ECMO in the US
No significant survival difference between Low, Medium and High volume ECMO programs in bridge to Heart or Lung transplant patients
McCarthy et.al. Presented at STSA 11/15
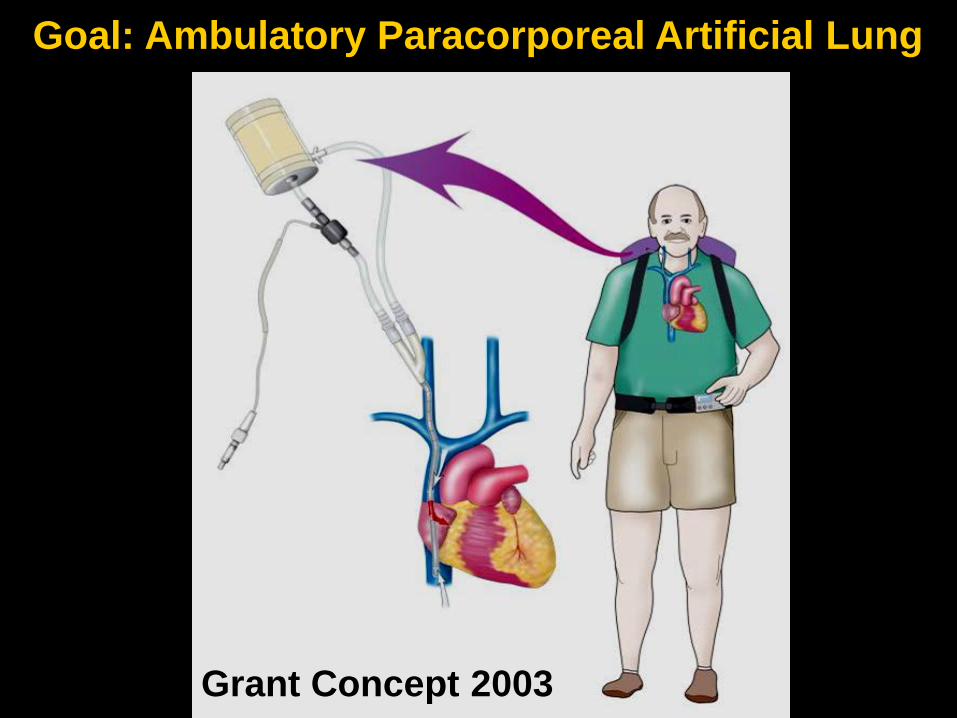
Goal: Ambulatory Paracorporeal Artificial Lung
Grant Concept 2003
56
Disclosures
Check
xCheck
x
• No Relevant Financial Interests to Report
• Products discussed for patient use are FDA approved
• Many products discussed are used “extended label”

57
Learning Objectives
CannulationHow to choose a cannulaeHow to put it in
Initiation Process
58
Cannulation: Achilles' heel of ECMO
Venousreturn
Venousdrainage
InternalJugular/SVC
Blood pump
Membraneoxygenator
Femoralvein
59
Cannulation
The first of many opportunities to kill your patient Choices
Venous cannulaeDiameterLengthWhich veinHow many
ArterialDiameterLengthWhich arteryProtect the limb
60
Cannulae choice
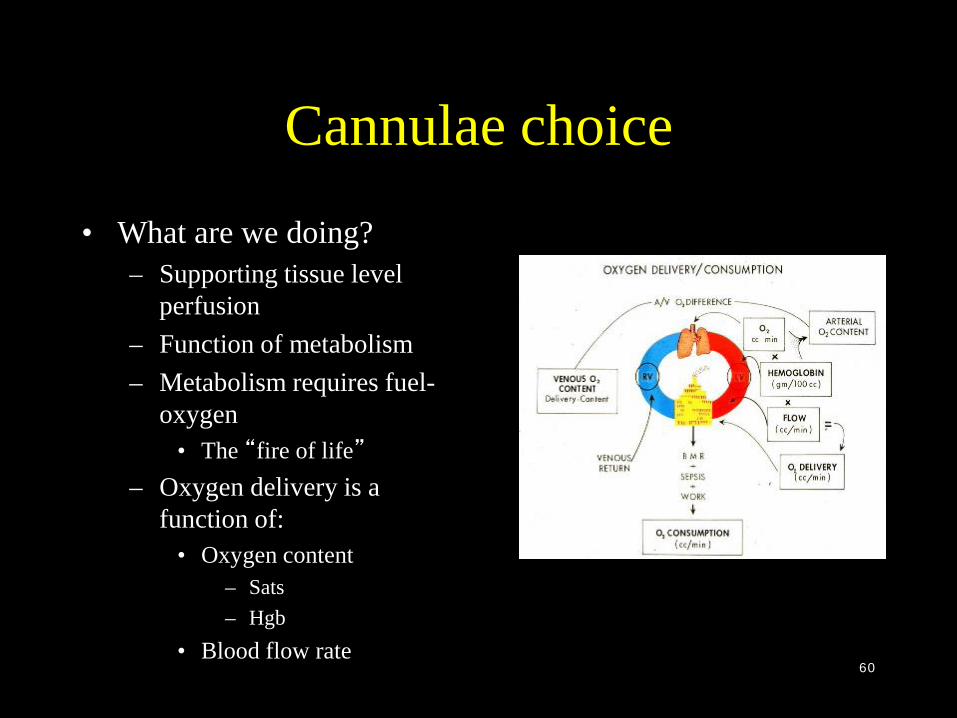
• What are we doing?– Supporting tissue level
perfusion– Function of metabolism– Metabolism requires fuel-
oxygen• The “fire of life”
– Oxygen delivery is a function of:
• Oxygen content– Sats– Hgb
• Blood flow rate
61
Cannulae choice
OK, I can determine flow.Which cannulae do I use?
62
Cannulae choice
Mode of cannulationWhy are we doing this again?Tissue level perfusionGas exchange failure?
Venovenous Venoarterial
Perfusion failure? Venoarterial
63
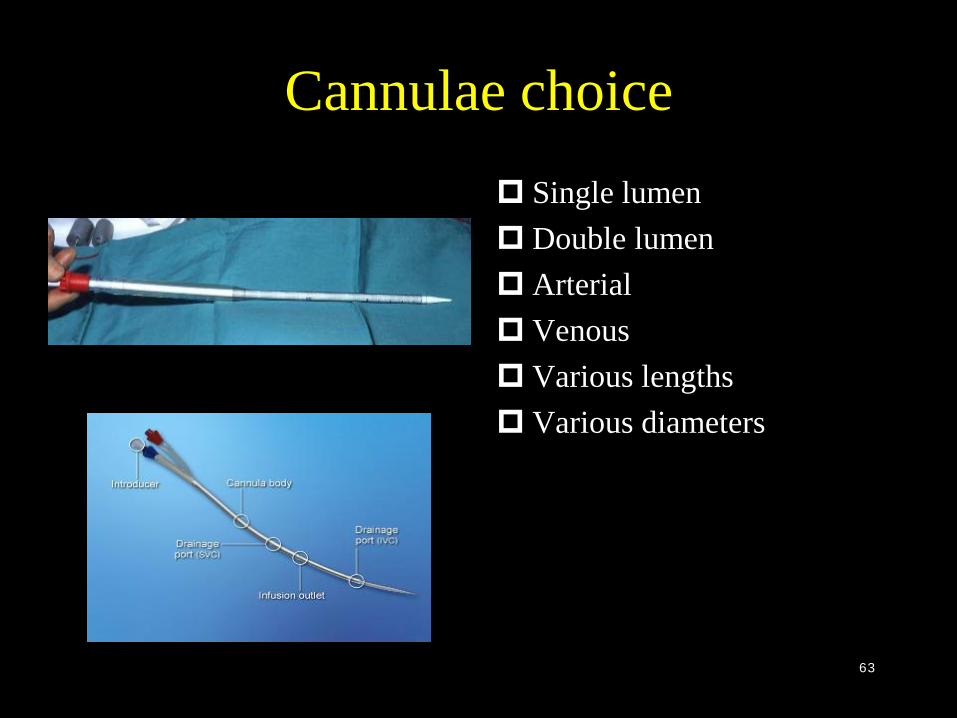
Cannulae choice Single lumen Double lumen Arterial Venous Various lengths Various diameters
64
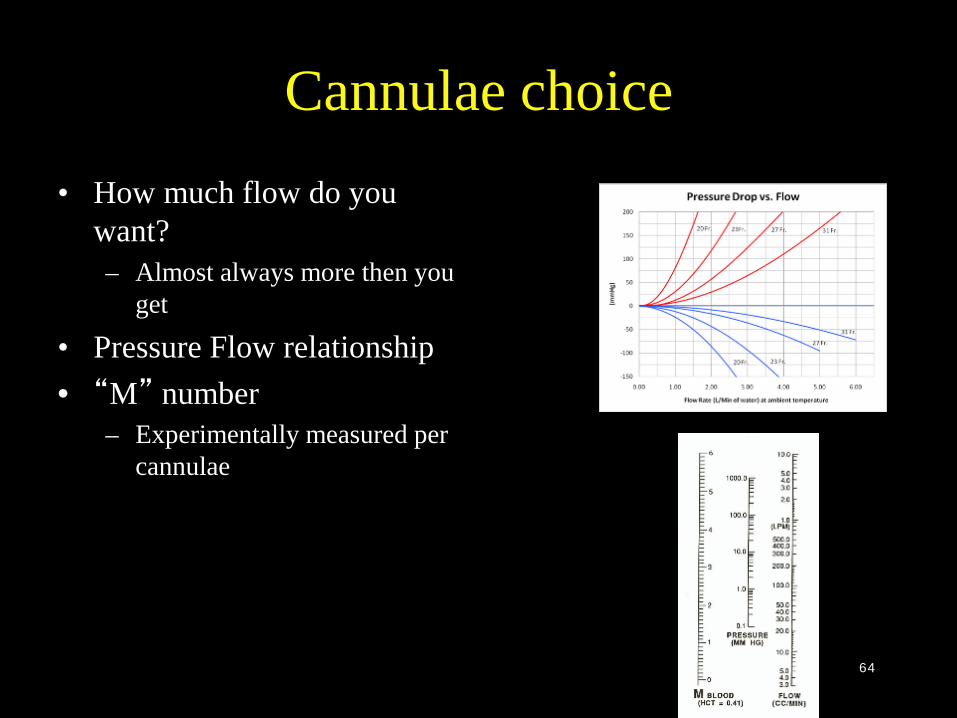
Cannulae choice• How much flow do you
want?– Almost always more then you
get
• Pressure Flow relationship• “M” number
– Experimentally measured per cannulae
65
Cannulae choice
Finally, you can choose your cannulae.About time!
66
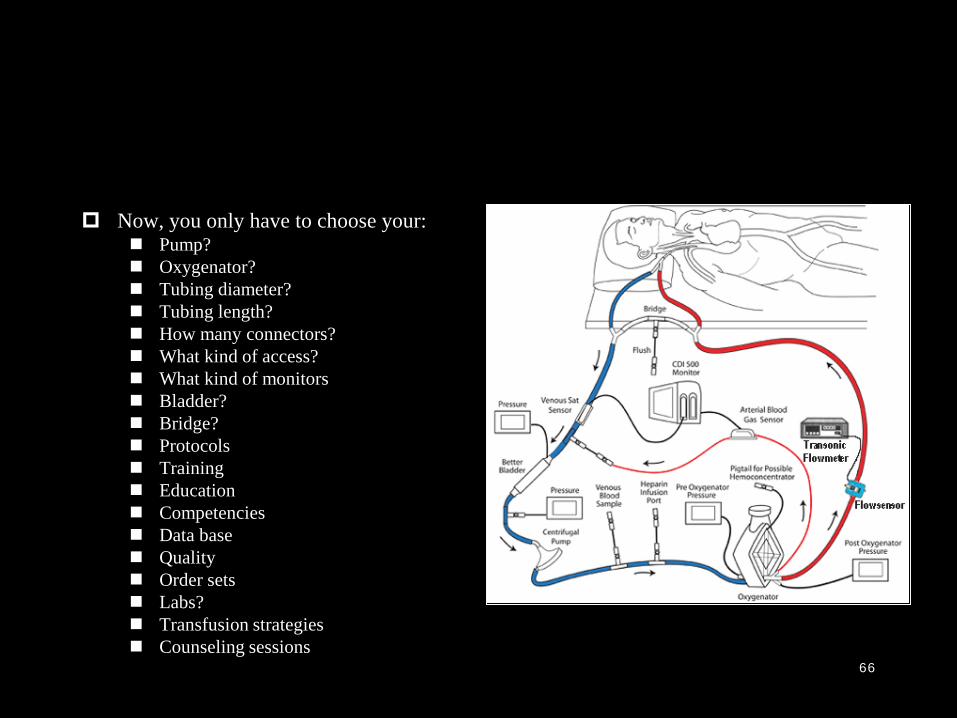
Now, you only have to choose your: Pump? Oxygenator? Tubing diameter? Tubing length? How many connectors? What kind of access? What kind of monitors Bladder? Bridge? Protocols Training Education Competencies Data base Quality Order sets Labs? Transfusion strategies Counseling sessions
67
Cannulation techniques“how to put it in”
PercutaneousPrimary technique for adult venovenous support
Semi-open (surgically-guided percutaneous)Visual guidance of percutaneous insertionDeveloped for neonatal VV cannulationAn option for adult cannulation
Open (surgical venotomy)Traditional approach to cannulationRequires vessel ligationBackup option for failed percutaneous technique

68
Percutaneous Cannulation
Courtesy of Jonathan Haft
69
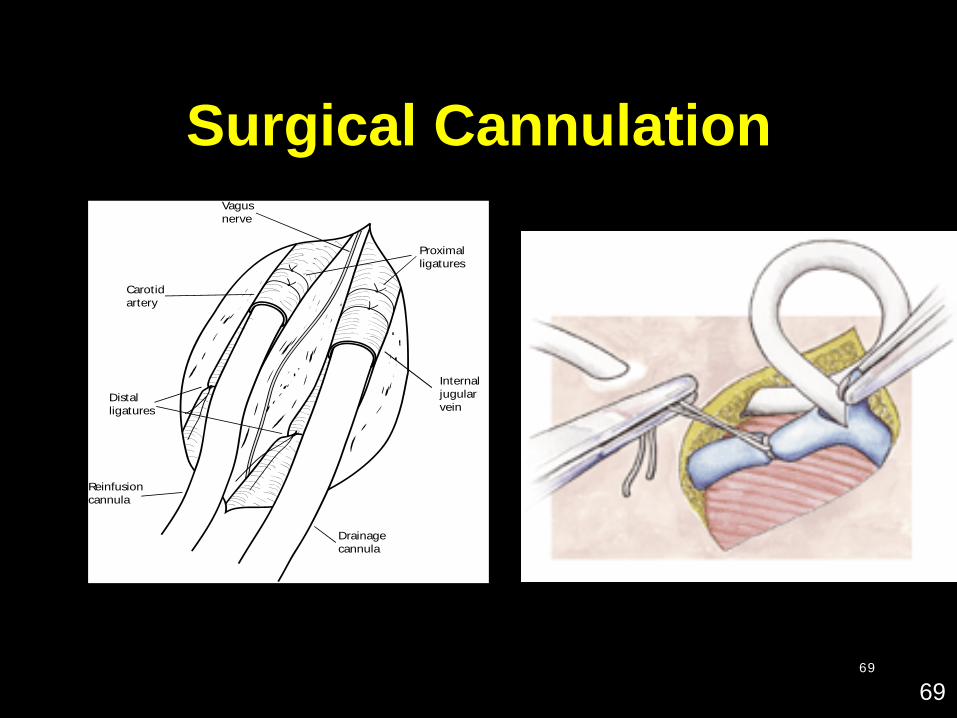
Surgical Cannulation
Distalligatures
Carotidartery
Internaljugularvein
Drainagecannula
Reinfusioncannula
Vagusnerve
Proximalligatures
69
70
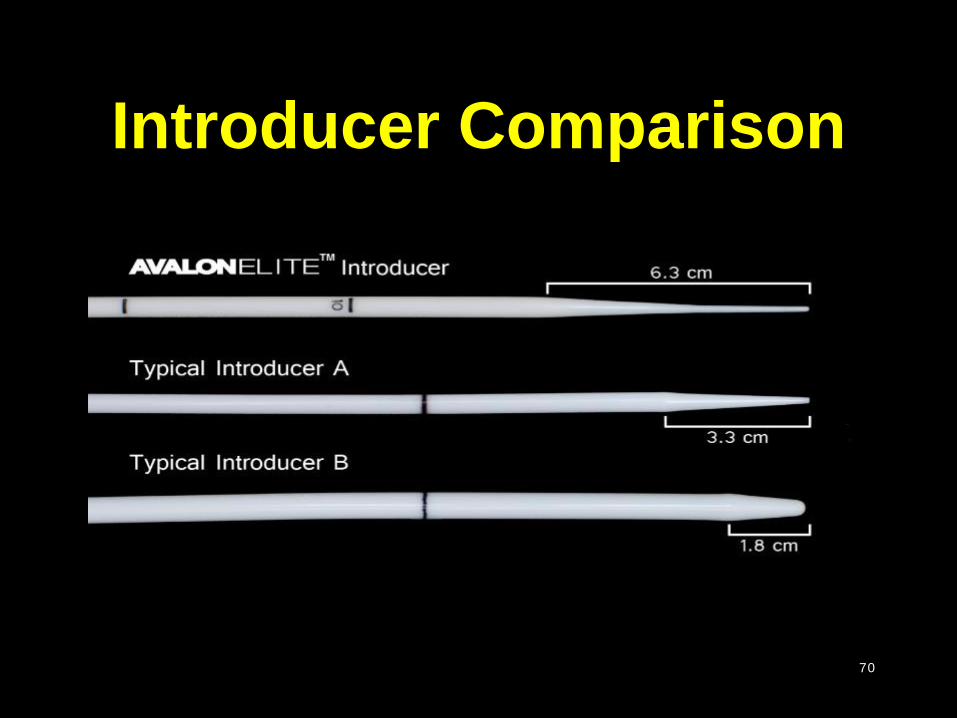
Introducer Comparison

71
Vessel Dilatation
72
Pharmacologic management during cannulation
Deep sedation with intravenous analgesiaLocal infiltration anesthesia at cannulation
siteElevated airway pressuresUsually not a problemShort-acting neuromuscular blockade
during cannula insertionPrevention of air embolism

73
Tips for percutaneous technique 2
• Guidewire kinking– Occurs when advancing dilator– Usually in the tissue outside of the vessel
• Prevention– Patient positioning – ‘straight shot’– Long tapered dilators (Coon’s dilators)– Rotational motion >> forward motion– No more than 4 Fr increments – retreat if needed– Ensure adequate dilatation at each step– Adequate tension on guidewire
• Minimize skin incision – snug fit = less bleeding
74
Typical cannula sizes for percutaneous use
• Internal Jugular– Vein size usually about 40 to 50 Fr (I’ve seen 75 Fr!)– 23 to 24 Fr short– 27 to 31 Fr dual lumen
• Femoral vein– Vein size usually 35 to 45 Fr– 23 to 24 Fr short– 24 to 28 Fr long
• Femoral artery– 16 to 17 Fr
75
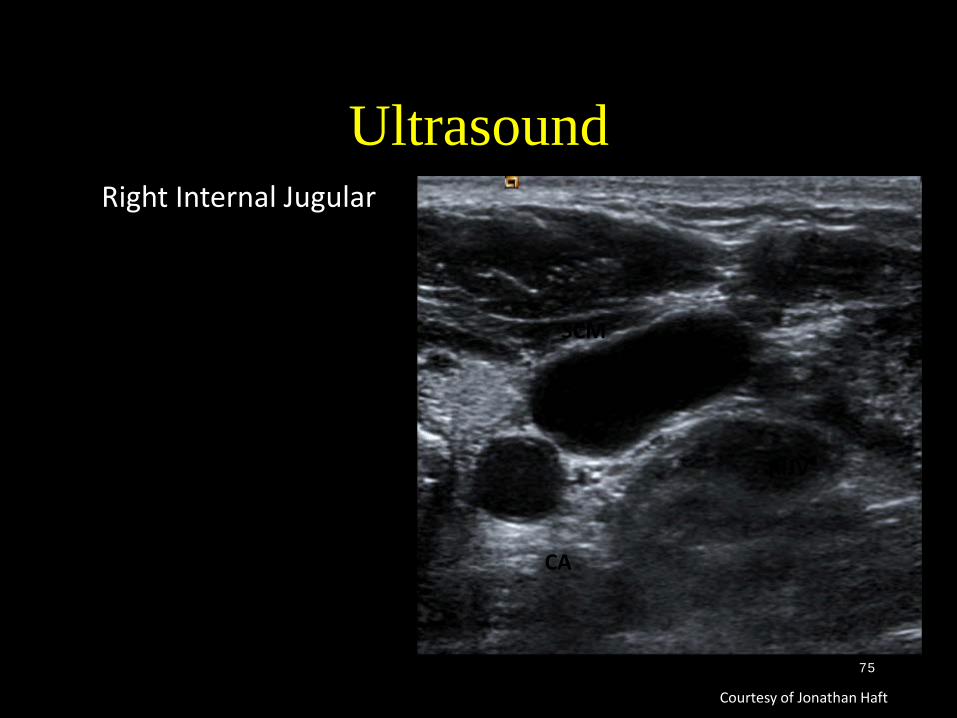
UltrasoundRight Internal Jugular
Courtesy of Jonathan Haft
RIJV
SCM
RIJV
CA
CA
SCM
76
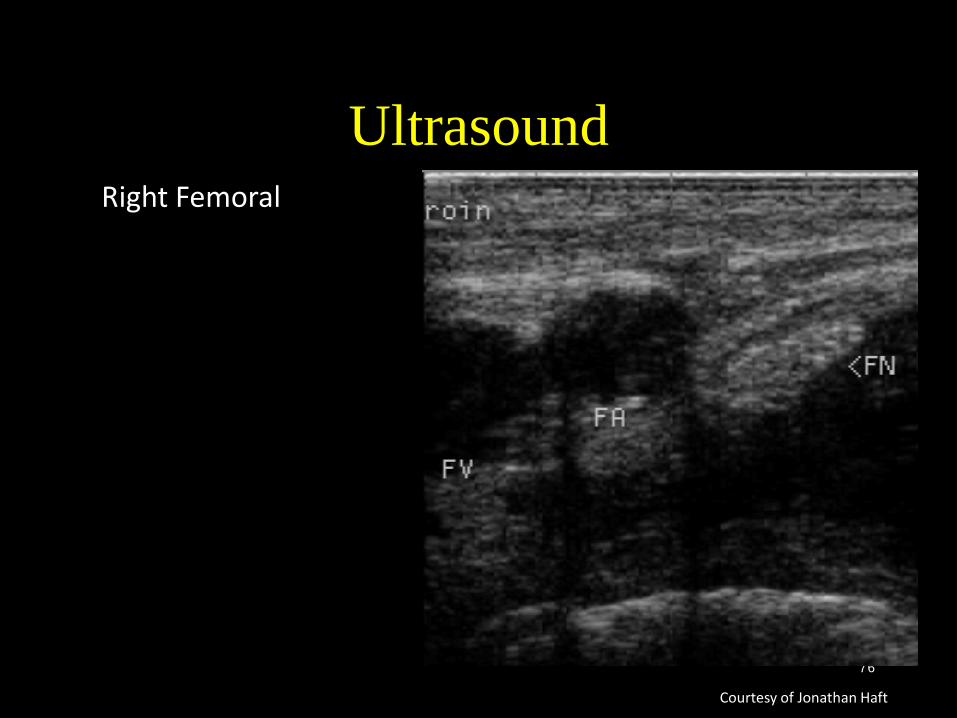
UltrasoundRight Femoral
Courtesy of Jonathan Haft

77
Measuring vessel size
Fr size = diameter * 3
Fr size ≅ circumference in mm
78
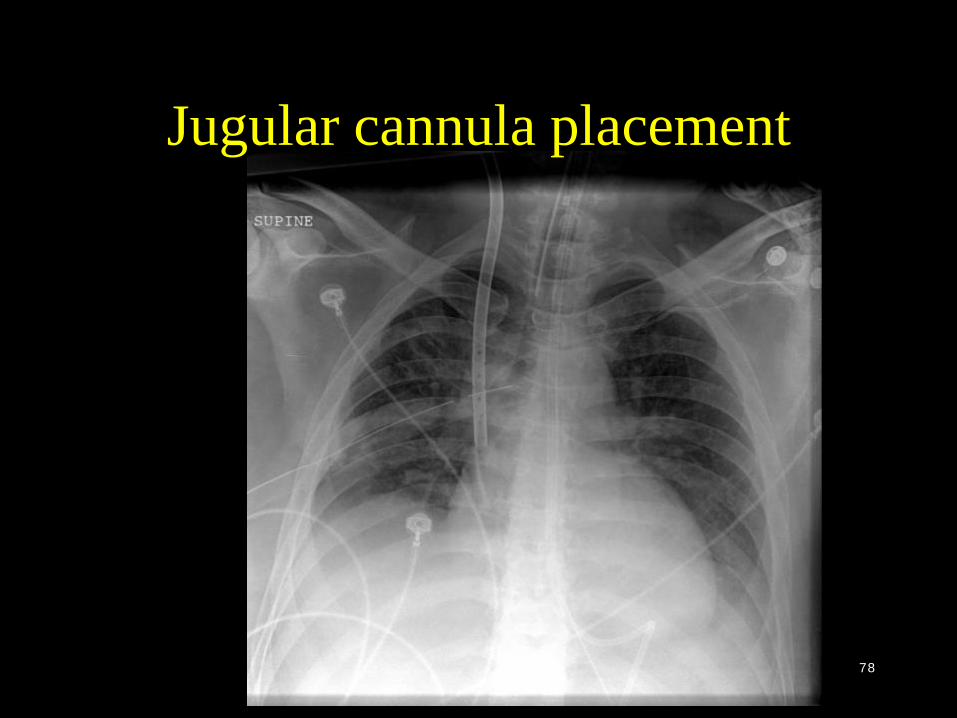
Jugular cannula placement
79
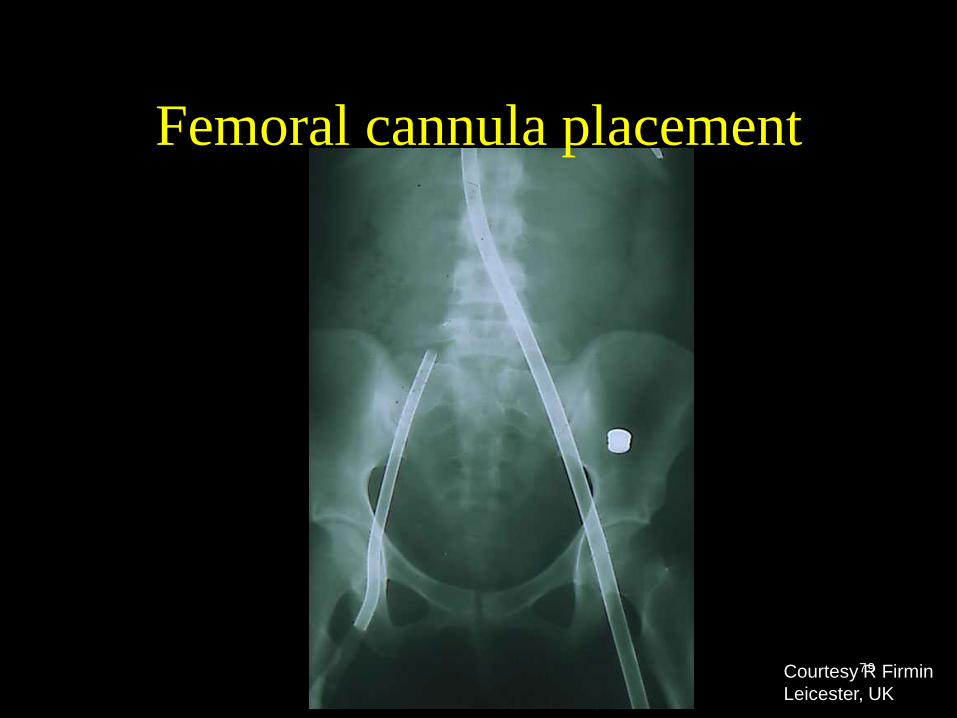
Femoral cannula placement
Courtesy R FirminLeicester, UK

80
Avalon Placement

81
Positioning of the dual lumen cannula
82
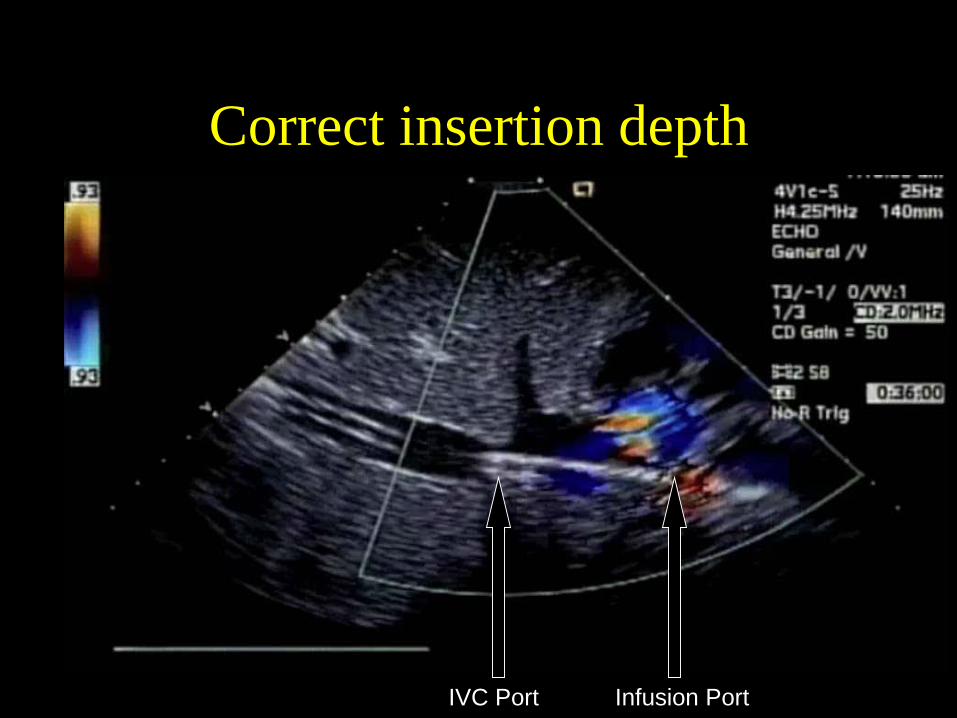
Correct insertion depth
IVC Port Infusion PortCourtesy of Mark Ogino, MD
83
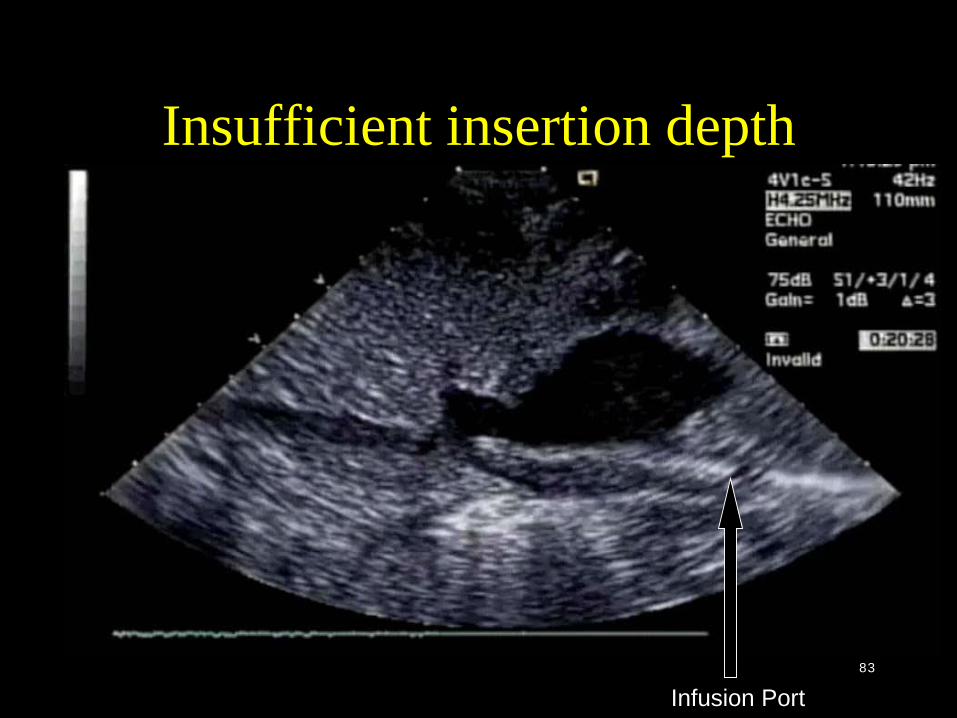
Insufficient insertion depth
Infusion PortCourtesy of Mark Ogino, MD

84
Deep insertion depth
Liver DiaphragmCatheter Tip Liver DiaphragmCatheter Tip
Courtesy of Mark Ogino, MD
85
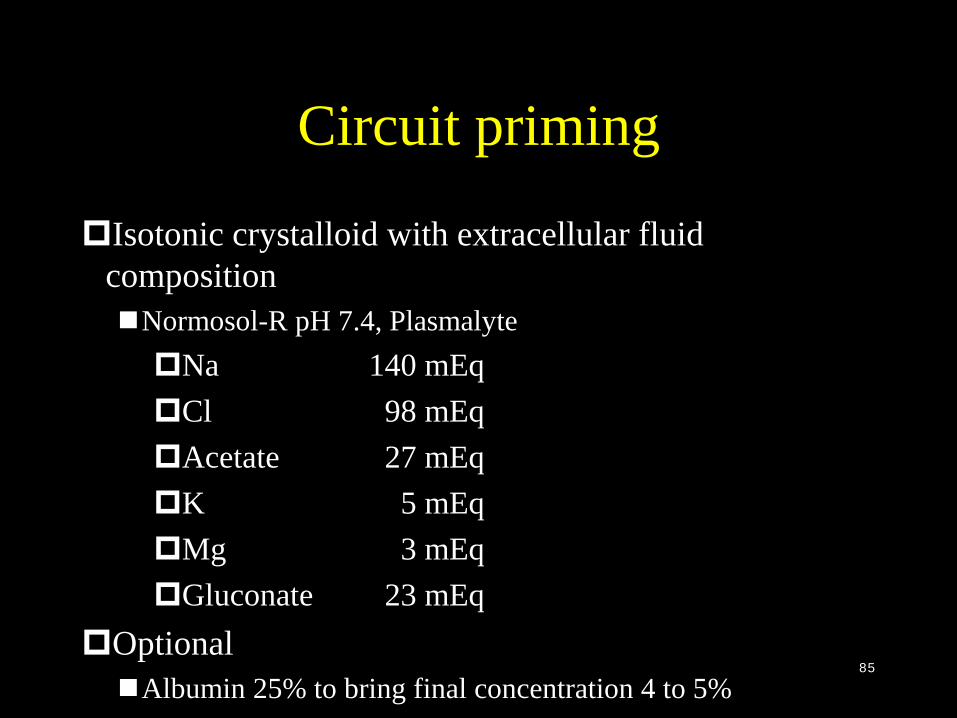
Circuit priming
Isotonic crystalloid with extracellular fluid compositionNormosol-R pH 7.4, PlasmalyteNa 140 mEqCl 98 mEqAcetate 27 mEqK 5 mEqMg 3 mEqGluconate 23 mEq
OptionalAlbumin 25% to bring final concentration 4 to 5%
86
Initiation
• Your second opportunity to kill your patient– “Crashing on”
• VA• You can only look good
– Elective• VV• VA• You can only look bad
– Be prepared– Have a plan in your head– Have a plan outside of your head
» Say it “out loud” to each other» “closed loop communication”

87
Initiation• “Crashing on”
– Chaotic– CPR– Cannulator cannulates
• VA• Cut down• Percutanous
– Team manages the patient– Team readies the circuit– Focus on your job– Go on fast– Air– Connecting “backwards”
88
Initiation
ElectiveWhenAlways after midnightAlways for about 6 hours
WhereFluroCath labORICU
Should simulate the processElevator big enough?E h t bi l th t t i t ?

89
Initiation• How
– Commence support slowly• Hypotension with VV• Prepare with pressors
– Make sure blood is going the right direction– Watch for air– Double check each other
• Trust no one• Giving heparin is everyone’s job
– Change nothing until supports established– Stabilize– Evaluate circuit
• Maximum flow?• Evaluate support
– Minimize the unnecessary– Define support goals
• Tissue level perfusion

90
InitiationCommencing support Mix prime in slowlyIncrease pump speed slowly to achieve max flowDecrease flow to lowest level to provide adequate supportArterial saturation > 85% (lower if necessary)Physiologic goalsHemodynamicsTissue perfusionOrgan function
Blood flow regulated over time to meet goals

91
Thank youQuestions?
“To clinicians who have witnessed first-hand ECMO’s ability to salvage anunstable life that would presumably belost without it, today’s study will representthe sentinel paper on adult ECMO foryears to come. After all, 63% of patients who were dying survived to 6 months withECMO referral…”
Zwischenberger JB, Lynch JE; Will CESARanswer the adult ECMO debate? The Lancet 2009; 374
CESAR Trial
ECMO: When, Where, and by Whom?
Joseph B. Zwischenberger MD Johnston-Wright Professor
Chairman: Department of SurgerySurgeon-in-Chief UK Healthcare
859-229-6635 (mobile)[email protected]
The University of KentuckyLexington, Kentucky