Embed Size (px)
Citation preview


New Frontiers New Frontiers and and Paradigm Changes Paradigm Changes inin
Optimizing Supportive Optimizing Supportive Care Care inin Cancer Cancer
Focus on Thrombosis Prevention, CINV, and Focus on Thrombosis Prevention, CINV, and Hematologic Complications of MalignancyHematologic Complications of Malignancy
Program ChairmanProgram ChairmanGary H. Lyman, MD, MPH, FRCP (Edin)Gary H. Lyman, MD, MPH, FRCP (Edin)
Editor-In-Chief, Editor-In-Chief, Cancer InvestigationCancer InvestigationProfessor of Medicine and DirectorProfessor of Medicine and Director
Health Services, Effectiveness and Outcomes ResearchHealth Services, Effectiveness and Outcomes ResearchDivision of Medical Oncology, Department of MedicineDivision of Medical Oncology, Department of Medicine
Duke University School of Medicine and the Duke Comprehensive Cancer CenterDuke University School of Medicine and the Duke Comprehensive Cancer CenterSenior Fellow, Duke Center for Clinical Health Policy ResearchSenior Fellow, Duke Center for Clinical Health Policy Research
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application

Program FacultyProgram Faculty
PROGRAM CHAIRMANPROGRAM CHAIRMAN GARY H. LYMAN, MD, MPH, FRCP GARY H. LYMAN, MD, MPH, FRCP (Edin)(Edin)Editor-In-Chief, Editor-In-Chief, Cancer InvestigationCancer InvestigationProfessor of Medicine and DirectorProfessor of Medicine and DirectorHealth Services, Effectiveness and Health Services, Effectiveness and Outcomes Outcomes ResearchResearchDivision of Medical Oncology, Department Division of Medical Oncology, Department of of MedicineMedicineDuke University School of Medicine and the Duke University School of Medicine and the Duke Duke Comprehensive Cancer CenterComprehensive Cancer CenterSenior Fellow, Duke Center for Clinical Senior Fellow, Duke Center for Clinical Health Health Policy ResearchPolicy Research Lee S. Schwartzberg, MD, FACP Lee S. Schwartzberg, MD, FACP Supportive Oncology Services, MemphisSupportive Oncology Services, MemphisAccelerated Community Oncology Research Accelerated Community Oncology Research NetworkNetworkClinical Professor of MedicineClinical Professor of MedicineUniversity of Tennessee Medical CenterUniversity of Tennessee Medical CenterMemphis, TennesseeMemphis, Tennessee
Jeffrey Crawford, MDJeffrey Crawford, MDGeorge Barth Geller Professor for George Barth Geller Professor for Research In CancerResearch In CancerChief of Division of Medical Chief of Division of Medical OncologyOncologyDepartment of MedicineDepartment of MedicineDuke University Medical CenterDuke University Medical CenterEditor-in-Chief, Supportive Care Editor-in-Chief, Supportive Care OncologyOncologyDurham, North CarolinaDurham, North Carolina Alok A. Khorana, MD, FACPAlok A. Khorana, MD, FACPVice-Chief, Division of Vice-Chief, Division of Hematology/OncologyHematology/OncologyAssociate Professor of Medicine and Associate Professor of Medicine and OncologyOncologyJames P. Wilmot Cancer CenterJames P. Wilmot Cancer CenterUniversity of RochesterUniversity of RochesterRochester, New YorkRochester, New York

An Evidence-Based Overview to An Evidence-Based Overview to Critical Issues in Supportive CareCritical Issues in Supportive Care
OverviewOverview
Program ChairmanProgram ChairmanGary H. Lyman, MD, MPH, FRCP (Edin)Gary H. Lyman, MD, MPH, FRCP (Edin)
Editor-In-Chief, Editor-In-Chief, Cancer InvestigationCancer InvestigationProfessor of Medicine and DirectorProfessor of Medicine and Director
Health Services, Effectiveness and Outcomes ResearchHealth Services, Effectiveness and Outcomes ResearchDivision of Medical Oncology, Department of MedicineDivision of Medical Oncology, Department of Medicine
Duke University School of Medicine and the Duke Comprehensive Cancer CenterDuke University School of Medicine and the Duke Comprehensive Cancer CenterSenior Fellow, Duke Center for Clinical Health Policy ResearchSenior Fellow, Duke Center for Clinical Health Policy Research
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application

Complications of Cancer ChemotherapyComplications of Cancer Chemotherapy
Kuderer NM et al. Cancer 2006;106:2258–2266 Chirivella I et al. J Clin Oncol 2006;24;abstract 668 Bosly A et al. Ann Hematol 2007, advance access published 20 October 2007; doi:10.1007/s00277-007-0399-y
Myelosuppressive chemotherapyMyelosuppressive chemotherapy
Febrile neutropenia (FN)Febrile neutropenia (FN) Chemotherapy dose delays Chemotherapy dose delays and dose reductionsand dose reductions
Decreased relative dose Decreased relative dose intensity (RDI)intensity (RDI)
Complicated life-Complicated life-threatening infection and threatening infection and prolonged hospitalizationprolonged hospitalization
NeutropeniaNeutropenia
Reduced survivalReduced survival

Meta-analysis of Randomized Controlled Trials Meta-analysis of Randomized Controlled Trials Relative risk of FNRelative risk of FN
0.1 0.2 0.5 1.0 2.0 5.0 10
Favours G-CSF
Favours no G-CSF
Combined filgrastim (n=9)Combined filgrastim (n=9)
Combined lenograstim (n=5)Combined lenograstim (n=5)
Combined pegfilgrastim (n=1)Combined pegfilgrastim (n=1)
All G-CSF (n=15)All G-CSF (n=15)
RRRR
0.61
0.62
0.08
0.54
95% CI95% CI
0.53–0.72
0.44–0.88
0.43–0.67
0.03–0.18
pp
<.001
0.007
<.001
<.001
Kuderer et al. J Clin Oncol 2007;25:3158–3167Kuderer et al. J Clin Oncol 2007;25:3158–3167
Febrile NeutropeoniaFebrile Neutropeonia(n = 3182)(n = 3182)

Primary Prophylactic CSF Primary Prophylactic CSF Administration Administration
► Required and recommended for “dose Required and recommended for “dose dense” regimens dense” regimens
► Recommended for the prevention of FN in Recommended for the prevention of FN in patients who have a high risk of FN based patients who have a high risk of FN based on:on:
• AgeAge• Medical historyMedical history• Disease characteristicsDisease characteristics• Myelotoxicity of the chemotherapy Myelotoxicity of the chemotherapy
regimenregimen
► Clinical trial data support the use of CSF Clinical trial data support the use of CSF when the risk of FN is in the range of when the risk of FN is in the range of 20% 20% or higheror higher

Primary Prophylactic CSF Administration: Primary Prophylactic CSF Administration: Special CircumstancesSpecial Circumstances
► When the following clinical factors are present, primary When the following clinical factors are present, primary prophylaxis with CSF is often appropriate prophylaxis with CSF is often appropriate even with even with regimens with FN rates of <20% :regimens with FN rates of <20% :
● Age >65 yearsAge >65 years● Poor performance statusPoor performance status● Previous FNPrevious FN● Poor nutritional statusPoor nutritional status● Open wounds or active infectionsOpen wounds or active infections● More advanced cancerMore advanced cancer● Extensive prior treatment, including large XRT portsExtensive prior treatment, including large XRT ports● Administration of combined chemoradiotherapyAdministration of combined chemoradiotherapy● Cytopenias due to bone marrow involvement by tumor Cytopenias due to bone marrow involvement by tumor ● Other serious comorbiditiesOther serious comorbidities

Evidence-based G-CSF Guidelines Evidence-based G-CSF Guidelines Key RecommendationsKey Recommendations
Summary of RecommendationsSummary of Recommendations EORTCEORTC11 ASCOASCO22 NCCNNCCN33
G-CSF primary prophylaxis with ≥20% overall FN risk
FN risk associated with chemotherapy
Consider patient risk factors for overall FN risk
G-CSF primary prophylaxis to maintain chemotherapy RDI
Dose-dense chemotherapy regimens
G-CSF for ongoing FN episode
G-CSF formulation and dosing
Secondary prophylaxis with G-CSF
1. Aapro et al. Eur J Cancer 2006;42:2433–2453; 2. Smith et al. J Clin Oncol 2006;24:3187–3205; 3. NCCN. Myeloid growth factors V.1.2009

Chemotherapy-Induced Acute Emesis Chemotherapy-Induced Acute Emesis Classes of AntiemeticClasses of Antiemetic
► Highest therapeutic index antiemetic agentsHighest therapeutic index antiemetic agents• 5-HT5-HT33 Serotonin Receptor Serotonin Receptor AntagonistsAntagonists• Corticosteroids (Dexamethasone)Corticosteroids (Dexamethasone)• NKNK11 Receptor Antagonists (Aprepitant) Receptor Antagonists (Aprepitant)
► These classes of antiemetic agentsThese classes of antiemetic agents• Highly effectiveHighly effective• Few significant side effects (whenFew significant side effects (when used appropriately)used appropriately)• Safe in combinationSafe in combination
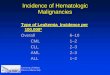
Emetic Risk of IV Administered Antineoplastic Agents
High (>90%) Moderate (30% to 90%) Low (10% to 30%) Minimal (<10%)
CarmustineCisplatin
Cyclophosphamide > 1500 mg/m2
DacarbazineDactinomycinMechlorethamineStreptozotocin
CarboplatinCyclophosphamide<1500 mg/m2
Cytarabine >1 gm/m2
DaunorubicinDoxorubicinEpirubicinIdarubicinIfosfamideIrinotecanOxaliplatin
5- FluorouracilBortezomibCetuximabCytarabine < 1000 mg/m2
DocetaxelEtoposideGemcitabineMethotrexateMitomycinMitoxantronePaclitaxelPemetrexedTopotecanTrastuzumab
2- ChlorodeoxyadenosineBevacizumabBleomycinBusulfanFludarabineRituximabVinblastineVincristineVinorelbine

Chemotherapy-Induced Acute Emesis Chemotherapy-Induced Acute Emesis Antiemetic Agents Antiemetic Agents
5-HT3 Serotonin
Receptor Antagonists
Dexamethasone
Aprepitant
Yields greatest antiemetic protection in randomized-multicenter studies
Chemotherapy of high emetic risk
Anthracycline + Cyclophosphamide
Indicated for patients receiving agents of moderate emetic risk other than anthracycline + cyclophosphamide
5-HT3 Serotonin
Receptor Antagonists
Dexamethasone
Kris M et al, JCO 2006:24: 2932-2947Kris M et al, JCO 2006:24: 2932-2947
Combinations of AntiemeticsCombinations of Antiemetics

Antiemetic Regimens Based on Emetic Risk Antiemetic Regimens Based on Emetic Risk ASCO GuidelinesASCO Guidelines
High (> 90%)High (> 90%)
Moderate (30-90%)Moderate (30-90%)
Low (10-30%)Low (10-30%)
► 5-HT5-HT33 SRA: day 1 SRA: day 1
► Dexamethasone: days 1-4Dexamethasone: days 1-4
► Aprepitant: days 1-3Aprepitant: days 1-3
► 5HT5HT33 SRA: day 1 SRA: day 1
► Dexamethasone: day 1 (2,3)* Dexamethasone: day 1 (2,3)* (may omit days 2,3 s/p aprepitant)(may omit days 2,3 s/p aprepitant)
► (Aprepitant: days 1-3 for AC) (Aprepitant: days 1-3 for AC) (AC- (AC- anthracycline + cyclophosphamide)anthracycline + cyclophosphamide)
► Dexamethasone: day 1Dexamethasone: day 1
Kris M et al, JCO 2006:24: 2932-2947Kris M et al, JCO 2006:24: 2932-2947


Program ChairmanProgram ChairmanGary H. Lyman, MD, MPH, FRCP (Edin)Gary H. Lyman, MD, MPH, FRCP (Edin)
Editor-In-Chief, Editor-In-Chief, Cancer InvestigationCancer InvestigationProfessor of Medicine and DirectorProfessor of Medicine and Director
Health Services, Effectiveness and Outcomes ResearchHealth Services, Effectiveness and Outcomes ResearchDivision of Medical Oncology, Department of MedicineDivision of Medical Oncology, Department of Medicine
Duke University School of Medicine and the Duke Comprehensive Cancer CenterDuke University School of Medicine and the Duke Comprehensive Cancer CenterSenior Fellow, Duke Center for Clinical Health Policy ResearchSenior Fellow, Duke Center for Clinical Health Policy Research
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application
Optimizing Management of Optimizing Management of Cancer Patients at Risk for Cancer Patients at Risk for Venous ThromboembolismVenous Thromboembolism

TumorTumorCellsCells
HemostaticHemostaticSystemSystem
Procoagulant ActivityProcoagulant Activity
CytokinesCytokinesGrowth FactorsGrowth Factors
Fibrinolytic ActivityFibrinolytic Activity
GrowthGrowthInvasionInvasion
MetastasesMetastasesAngiogenesisAngiogenesis
Kuderer NM et al J Clin Oncol 2009; 27: 4902-4911Kuderer NM et al J Clin Oncol 2009; 27: 4902-4911

VTE Inpatient Risk and MortalityVTE Inpatient Risk and MortalityHospitalized Cancer Patients* Hospitalized Cancer Patients*
0
2
4
6
8
10
12
14
1618
20
199519961997199819992000200120022003
Inp
ati
ent
Mort
alit
y (
%)
VTE
No VTE
P<0.0001P<0.0001
Khorana et al. Cancer 2007; 110: 2339-2346
VTE- patients on chemo
VTE-all patients
DVT-all patients
PE-all patients
0.00.51.01.52.02.53.03.54.04.55.05.56.06.57.0
199519961997199819992000200120022003
Rate
of
VTE (
%)
P<0.0001
133 U.S. academic medical centers, 133 U.S. academic medical centers, 1995 – 20031995 – 2003
* n = 1,015,598

8
7
6
5
4
3
2
1
0
ChemotherapyChemotherapy
Risk in cancer populationRisk in cancer population
RemissionRemission
Risk in general populationRisk in general population
TimeTime
DiagnosisDiagnosis
MetastasisMetastasis
End of lifeEnd of lifeHospitalizationHospitalization
Rela
tive R
isk
Rela
tive R
isk
Rao MV, et al. In: Khorana and Francis, eds. Cancer-Associated Thrombosis; 2007
Cancer and Venous ThromboembolismCancer and Venous ThromboembolismRisk of VTE Varies Over Natural History of CancerRisk of VTE Varies Over Natural History of Cancer

Risk Factors for VTE in Patients with Risk Factors for VTE in Patients with CancerCancer
Patient-related factorsPatient-related factors► Older age Older age ► Race Race
● Higher in AAHigher in AA● Lower in AsiansLower in Asians
► Major comorbiditiesMajor comorbidities► History of VTEHistory of VTE
Treatment-related factorsTreatment-related factors► Major surgery Major surgery ► Hospitalization Hospitalization ► ChemotherapyChemotherapy► Central venous catheters Central venous catheters ► Hormonal therapy Hormonal therapy ► Antiangiogenic agentsAntiangiogenic agents► ESAsESAs► ?Transfusions?Transfusions
Cancer-related factorsCancer-related factors• Site of cancer Site of cancer • Advanced stageAdvanced stage
Rao MV, et al. In: Khorana and Francis, eds. Cancer-Associated Thrombosis; 2007

► Increased morbidityIncreased morbidity● HospitalizationHospitalization● AnticoagulationAnticoagulation● Postphlebitic syndromePostphlebitic syndrome
► Increased mortalityIncreased mortality
► Increased risk of recurrent Increased risk of recurrent VTEVTE
► Bleeding complicationsBleeding complications
► Cancer treatment delaysCancer treatment delays
► Increased healthcare costsIncreased healthcare costs
Important Consequences of Important Consequences of VTE in Cancer PatientsVTE in Cancer Patients

Ambulatory Cancer Patients Ambulatory Cancer Patients Receiving ChemotherapyReceiving Chemotherapy
Cumulative Incidence of Cumulative Incidence of VTEVTE
Time (Days)
1501401301201101009080706050403020100
Cu
mla
tive
Su
rviv
al
1.00
.99
.98
.97
.96
.95
.94
.93
.92
.91
.90
Kuderer NM et al; J Clin Oncol 2008Kuderer NM et al; J Clin Oncol 2008
Time (Days)
1501401301201101009080706050403020100
Pro
po
rtio
n w
ith
VT
E
.04
.03
.02
.01
0.00
All Cause Early MortalityAll Cause Early Mortality
HR = 4.90 [2.27-10.60], P<.0001
Prospective Study at 115 Randomly Prospective Study at 115 Randomly Selected US Practice SitesSelected US Practice SitesMarch 2002 – February 2006 March 2002 – February 2006 [N = 4,458][N = 4,458]

Recommendations for Venous Thromboembolism Prophylaxis and Treatment in Patients with Cancer
ASCO Clinical Practice Guidelines
Lyman GH et al: J Clin Oncol 2007; 25:5490-5505Lyman GH et al: J Clin Oncol 2007; 25:5490-5505

Clinical QuestionsClinical Questions
1.1. Should patients with cancer receive Should patients with cancer receive anticoagulation for VTE prophylaxis while anticoagulation for VTE prophylaxis while hospitalized? hospitalized? √√
2.2. Should ambulatory patients with cancer receive Should ambulatory patients with cancer receive anticoagulation for VTE prophylaxis during anticoagulation for VTE prophylaxis during systemic chemotherapy? systemic chemotherapy? √√
3.3. Should patients with cancer undergoing surgery Should patients with cancer undergoing surgery receive perioperative VTE prophylaxis?receive perioperative VTE prophylaxis?
4.4. What is the best method for treatment of What is the best method for treatment of patients with cancer with established VTE to patients with cancer with established VTE to prevent recurrence? prevent recurrence? √√
5.5. Should patients with cancer receive Should patients with cancer receive anticoagulants in the absence of established VTE anticoagulants in the absence of established VTE to improve survival?to improve survival? √√
Lyman GH et al: J Clin Oncol 2007; 25:5490-5505Lyman GH et al: J Clin Oncol 2007; 25:5490-5505

► Hospitalized patients with cancer should be Hospitalized patients with cancer should be considered candidates for VTE prophylaxis considered candidates for VTE prophylaxis in the absence of bleeding or other in the absence of bleeding or other contraindications to anticoagulation. contraindications to anticoagulation.
ASCO Recommendations for VTE ASCO Recommendations for VTE Prophylaxis in Patients with CancerProphylaxis in Patients with Cancer
Lyman GH et al: J Clin Oncol 2007; 25:5490-5505Lyman GH et al: J Clin Oncol 2007; 25:5490-5505

Anticoagulant Prophylaxis to Prevent Anticoagulant Prophylaxis to Prevent Screen-Detected VTEScreen-Detected VTE
► 3 large, randomized, placebo-controlled, 3 large, randomized, placebo-controlled, double-blind trials in medical patients at high double-blind trials in medical patients at high risk including cancerrisk including cancer● MEDENOX (enoxaparin)MEDENOX (enoxaparin)11 ~ 15% ~ 15%● PREVENT (dalteparin)PREVENT (dalteparin)22 ~5% ~5%● ARTEMIS (fondaparinux)ARTEMIS (fondaparinux)33 ~15% ~15%
► Screening for asymptomatic DVT with Screening for asymptomatic DVT with venography venography or ultrasoundor ultrasound
11Samama MM, et al. Samama MM, et al. N Engl J Med.N Engl J Med. 1999;341:793-800 1999;341:793-8002 2 Leizorovicz A, et al. Leizorovicz A, et al. Circulation.Circulation. 2004;110:874-9 2004;110:874-933Cohen AT, et al. Cohen AT, et al. BMJ 2006; 332: 325-329BMJ 2006; 332: 325-329
High Risk Hospitalized Medical PatientsHigh Risk Hospitalized Medical Patients

MEDENOX1
Study RRR Thromboprophylaxis Patients with VTE (%)
14.9
5.5
5.0
2.8
10.5
5.6
11Samama MM, et al. Samama MM, et al. N Engl J Med.N Engl J Med. 1999;341:793-800 1999;341:793-8002 2 Leizorovicz A, et al. Leizorovicz A, et al. Circulation.Circulation. 2004;110:874-9 2004;110:874-933Cohen AT, et al. Cohen AT, et al. BMJ 2006; 332: 325-329BMJ 2006; 332: 325-329
P < 0.001
P = 0.0015
RRR
63%
45%
47%
Placebo
Placebo
Placebo
Enoxaparin 40 mg
Dalteparin 5,000 units
Fondaparinux 2.5 mg
ARTEMIS3
PREVENT2
Anticoagulant Prophylaxis to Prevent Anticoagulant Prophylaxis to Prevent Screen-Detected VTEScreen-Detected VTE
High Risk Hospitalized Medical Patients: High Risk Hospitalized Medical Patients: VTEVTE

0.49%
0.16% 0.2%
1.7%
1.1%
Samama MM, et al. Samama MM, et al. N Engl J Med.N Engl J Med. 1999;341:793-800 1999;341:793-800Leizorovicz A, et al. Leizorovicz A, et al. Circulation.Circulation. 2004;110:874-9 2004;110:874-9Cohen AT, et al. Cohen AT, et al. BMJ 2006; 332: 325-329BMJ 2006; 332: 325-329
Inci
dence
of
Majo
r B
leedin
g (
%)
Study
Anticoagulant Prophylaxis to Prevent Anticoagulant Prophylaxis to Prevent Screen-Detected VTE Screen-Detected VTE
High Risk Hospitalized Medical Patients: High Risk Hospitalized Medical Patients: Major BleedingMajor Bleeding

ASCO Recommendations for VTE ASCO Recommendations for VTE Prophylaxis in Patients with CancerProphylaxis in Patients with Cancer
Lyman GH et al: J Clin Oncol 2007; 25:5490-5505Lyman GH et al: J Clin Oncol 2007; 25:5490-5505
Routine prophylaxis with an Routine prophylaxis with an antithrombotic agent in the ambulatory antithrombotic agent in the ambulatory setting is not recommended.setting is not recommended.
* This recommendation is based on extrapolation from studies of prophylaxis in other * This recommendation is based on extrapolation from studies of prophylaxis in other high risk cancer settings.high risk cancer settings.
NOTE: Patients receiving thalidomide or lenalidomide with chemotherapy NOTE: Patients receiving thalidomide or lenalidomide with chemotherapy or dexamethasone are at high risk for thrombosis and warrant prophylaxis. or dexamethasone are at high risk for thrombosis and warrant prophylaxis. LMWH or adjusted dose warfarin (INR~1.5) is recommended.*LMWH or adjusted dose warfarin (INR~1.5) is recommended.*
Ambulatory Cancer PatientsAmbulatory Cancer Patients

Characteristics of Prophylaxis StudiesCharacteristics of Prophylaxis StudiesVTE – Prophylaxis with LMWHVTE – Prophylaxis with LMWH
TrialTrial Year Year StageStage NNLMWH /LMWH /
DoseDoseControl Control
ArmArm DurationDuration Type of Type of PubPub
Specific Specific ChemoChemo
FAMOUS Solid Tumors
20042004 III/IVIII/IV 385385 DalteparinDalteparin PlaceboPlacebo 12 months12 months ManuscriptManuscript NoNo
TOPIC-I Breast Cancer
20052005 III/IVIII/IV 353353 CertoparinCertoparin PlaceboPlacebo 6 months6 months Abstract+Abstract+ NoNo
TOPIC-2 NSCLC
20052005 III/IVIII/IV 547547 CertoparinCertoparin PlaceboPlacebo 6 months6 months Abstract+Abstract+ NoNo
PRODIGE Glioma
20072007 AnyAny 186186 DalteparinDalteparin PlaceboPlacebo 6-12 6-12 monthsmonths AbstractAbstract NoNo
SIDERAS Solid Tumors
20062006 IVIV 141141 DalteparinDalteparin Non-Non-PlaceboPlacebo IndefinitelyIndefinitely ManuscriptManuscript NoNo
PROTECHT Solid Tumors
20082008 III/IVIII/IV 11661166 NadroparinNadroparin 2:1 2:1 PlaceboPlacebo
<< 4 months 4 monthswith chemowith chemo ManuscriptManuscript NoNo
CONKO-04 Pancreatic Cancer
20092009 AdvanceAdvancedd
312312 EnoxapariEnoxaparinn
Non-Non-PlaceboPlacebo
3 months3 months(to prog)(to prog)
AbstractAbstractYes*Yes*
FRAGEM Pancreatic Cancer
20092009 AdvanceAdvancedd
123123 DalteparinDalteparin## Non-Non-PlaceboPlacebo 3 months3 months AbstractAbstract Yes*Yes*
*Gemcitabine-based chemotherapy (1000 mg/m2) (1000 mg/m2) # Higher dose than standard # Higher dose than standard prophylactic doseprophylactic dose

Cancer TypeCancer Type Benefit Benefit HarmHarm
Venous ThromboembolismVenous Thromboembolism Major BleedingMajor Bleeding
Overall 3.1% 3.1% 0.9% 0.9%
Pancreatic 13.0% 13.0% 0.8% 0.8%
Non-Pancreatic 1.4% 1.4% 0.8% 0.8%
Systematic Review of LMWH Prophylaxis Systematic Review of LMWH Prophylaxis in Cancer Patientsin Cancer Patients
Kuderer NM et al. Kuderer NM et al. ASH Oral Presentation ASH Oral Presentation 20092009
VTE Versus Major Bleeding: Absolute RiskVTE Versus Major Bleeding: Absolute Risk

Clinical Risk Model for Chemotherapy-associated VTEClinical Risk Model for Chemotherapy-associated VTERisk Score Based on Pretreatment Risk FactorsRisk Score Based on Pretreatment Risk Factors
Risk FactorsRisk Factors Risk Risk scorescore
1. Site of cancer1. Site of cancer
a) Very high risk cancer (stomach, pancreas)a) Very high risk cancer (stomach, pancreas) 22
b) High risk (lung, lymphoma, gynecologic, bladder, b) High risk (lung, lymphoma, gynecologic, bladder, testicular)testicular)
11
2. Platelet count2. Platelet count >>350,000/mm350,000/mm33 11
3. Hemoglobin level3. Hemoglobin level < 10 g/dL or use of< 10 g/dL or use of Red cell growth factorsRed cell growth factors
11
4. Leukocyte count4. Leukocyte count >11,000 /mm>11,000 /mm33 11
5. BMI5. BMI >> 35 kg/m 35 kg/m22 11
Khorana AA et al. Blood. 2008; 111: 4902-4907

RISK SCORE:RISK SCORE: Low (0) Low (0) Intermediate (1-2) Intermediate (1-2) High ( High (>>3)3)
n=374 n=842 n=149
Rat
e o
f VT
E (
%)
Rat
e o
f VT
E (
%)
0%
1%
2%
3%
4%
5%
6%
7%
8%
n=734 n=1,627 n=340
0.3%
2.0%
6.7%
0%
1%
2%
3%
4%
5%
6%
7%
8%
n=734 n=1,627 n=340
0.8%
1.8%
7.1%
0.3%
2.0%
6.7%
n=374 n=842 n=149
VTE Prediction Risk ScoreVTE Prediction Risk ScoreChemotherapy – Associated ThrombosisChemotherapy – Associated Thrombosis
Khorana AA et al. Blood. 2008; 111:4902-4907
Development cohort
Validation cohort

Mortality and Progression-Free Survival Mortality and Progression-Free Survival By VTE Risk ScoreBy VTE Risk Score
OutcomesOutcomes
Low Low Risk Risk
N=1,206N=1,206
Intermediate Intermediate Risk Risk
N=2,709N=2,709
High High Risk Risk
N=543N=543
AllAll
N=4,458N=4,458
Mortality
Risk (%) 1.2%1.2% 5.9%5.9% 12.7%12.7% 5.6%5.6%
HR [+/- CI] 1.01.0 3.6 [1.9-6.7] 3.6 [1.9-6.7] 6.9 [3.5-13.6] 6.9 [3.5-13.6] --
Progression-free survival
Risk (%) 93%93% 82%82% 72%72% 84%84%
HR [+/- CI] 1.01.0 2.8 [2-3.9] 2.8 [2-3.9] 4.3 [2.9-6.3] 4.3 [2.9-6.3] --
Kuderer NM et al. ASH 2008

ASCO Recommendations for VTE ASCO Recommendations for VTE Prophylaxis in Patients with CancerProphylaxis in Patients with Cancer
Lyman GH et al: J Clin Oncol 2007; 25:5490-5505Lyman GH et al: J Clin Oncol 2007; 25:5490-5505
► LMWH is the preferred approach for the initial 5 to LMWH is the preferred approach for the initial 5 to 10 days of anticoagulant treatment of the patient 10 days of anticoagulant treatment of the patient with cancer with established VTE.with cancer with established VTE.
► LMWH for at least 6 months is also preferred for LMWH for at least 6 months is also preferred for long-term anticoagulant therapy. long-term anticoagulant therapy.
► After 6 months, indefinite anticoagulant therapy After 6 months, indefinite anticoagulant therapy should be considered for patients with active should be considered for patients with active cancer.cancer.
NOTE: Vena cava filters are only indicated for patients with contraindications to anticoagulant therapy and in those with recurrent VTE despite adequate long-term therapy with LMWH.
Preventing Recurrence in Cancer Patients Preventing Recurrence in Cancer Patients with Established VTEwith Established VTE

0 1 2 3 4 5 6 7 8 9101112
Time (months)Time (months)
0
10
20
30
Recu
rrent
VTE, %
Recu
rrent
VTE, %
Hazard ratio 3.2 [1.9-Hazard ratio 3.2 [1.9-5.4]5.4]Cancer 21%Cancer 21%
No Cancer 7%No Cancer 7%
Prandoni P et al. Blood 2002; 100: 3484-3488Prandoni P et al. Blood 2002; 100: 3484-3488
0 1 2 3 4 5 6 7 8 9 101112
Time (months)Time (months)
0
10
20
30
Majo
r B
leedin
g, %
Majo
r B
leedin
g, %
Cancer 12%Cancer 12%
No Cancer 5%No Cancer 5%
Hazard ratio 2.2 [1.2-4.1]Hazard ratio 2.2 [1.2-4.1]
Recurrent VTE and Bleeding During Recurrent VTE and Bleeding During Anticoagulant TreatmentAnticoagulant Treatment
Patients with cancer and venous thrombosisPatients with cancer and venous thrombosis

RCTs of Long-term Treatment in Cancer RCTs of Long-term Treatment in Cancer Patients with VTEPatients with VTE
1. Meyer G, et al. Arch Intern Med. 2002;162:1729-1735. 2. Lee AY, et al. N Engl J Med. 2003;349:146-153.3. Deitcher SR, et al. Clin Appl Thromb Hemost. 2006;12:389-396. 4. Hull RD, et al. Am J Med. 2006;119:1062-1072.
StudyStudy No.No. Long-Term Long-Term TreatmentTreatment
RecurreRecurrent VTE, nt VTE,
%%
Major Major Bleed, Bleed,
%%
DeathDeath, %, %
Meyer1
20027171 WarfarinWarfarin 21.1*21.1* 22.722.7
6767 Enoxaparin 1.5 mg/kgEnoxaparin 1.5 mg/kg 10.5*10.5* 11.311.3
Lee2
2003336336 WarfarinWarfarin 17*17* 44 4141
336336 Dalteparin 200/150 IU/kgDalteparin 200/150 IU/kg 9*9* 66 3939
Deitcher3
2006
3030 WarfarinWarfarin 1010 2.92.9 8.88.8
2929 Enoxaparin 1.0 mg/kgEnoxaparin 1.0 mg/kg 6.96.9 6.56.5 6.56.5
3232 Enoxaparin 1.5 mg/kgEnoxaparin 1.5 mg/kg 6.36.3 11.111.1 19.419.4
Hull4
2006100100 WarfarinWarfarin 10*10* 77 1919
100100 Tinzaparin 175 IU/kgTinzaparin 175 IU/kg 6*6* 77 2020
* P < .05
RCTs of LMWH vs. Vitamin K Antagonists in CancerRCTs of LMWH vs. Vitamin K Antagonists in Cancer

5 to 7 days5 to 7 days
Dalteparin 200 IU/kg OD
Vitamin K antagonist (INR 2.0 to 3.0) x 6 mo
Control GroupControl Group
Dalteparin 200 IU/kg OD x 1 mo then ~150 IU/kg OD x 5 mo
Experimental GroupExperimental Group
Ran
dom
izati
on
Ran
dom
izati
on
1 month1 month 6 months6 months
The CLOT TrialThe CLOT TrialStudy SchemaStudy Schema
Lee AY, et al. N Engl J Med. 2003;349:146-153.

0
5
10
15
20
25
Days Post RandomizationDays Post Randomization
0 30 60 90 120 150 180 210
Pro
babili
ty o
f R
ecu
rren
t V
TE,
%Pro
babili
ty o
f R
ecu
rren
t V
TE,
%
dalteparin, 9%dalteparin, 9%
VKA, 17%VKA, 17%
risk reduction = 52%risk reduction = 52%HR 0.48 (95% CI 0.30, 0.77)HR 0.48 (95% CI 0.30, 0.77)log-rank p = 0.002log-rank p = 0.002
The CLOT Trial:The CLOT Trial:Results: Symptomatic Recurrent VTEResults: Symptomatic Recurrent VTE
Lee AY, et al. N Engl J Med. 2003;349:146-153.

► Anticoagulants are not recommended at Anticoagulants are not recommended at this time as treatment to improve survival this time as treatment to improve survival in patients with cancer without VTE.in patients with cancer without VTE.
► Participation in clinical trials designed to Participation in clinical trials designed to evaluate anticoagulant therapy as an evaluate anticoagulant therapy as an adjunct to standard anticancer therapies is adjunct to standard anticancer therapies is encouraged.encouraged.
ASCO Recommendations for VTE ASCO Recommendations for VTE Prophylaxis in Patients with CancerProphylaxis in Patients with Cancer
Lyman GH et al: J Clin Oncol 2007; 25:5490-5505
Improving survival in absence of established VTEImproving survival in absence of established VTE

Systematic Review of Anticoagulants Systematic Review of Anticoagulants as Cancer Treatmentas Cancer Treatment
Kuderer, N. M. et al. J Clin Oncol; 27:4902-4911 2009Kuderer, N. M. et al. J Clin Oncol; 27:4902-4911 2009Kuderer NM, et al. Kuderer NM, et al. Cancer.Cancer. 2007;110:1149-1161 2007;110:1149-1161
Impact on All Cause MortalityImpact on All Cause Mortality

Kuderer, N. M. et al. J Clin Oncol; 27:4902-4911 2009Kuderer NM, et al. Cancer. 2007;110:1149-1161
Systematic Review of Anticoagulants Systematic Review of Anticoagulants as Cancer Treatmentas Cancer Treatment
Impact on Major BleedingImpact on Major Bleeding

Patient GroupPatient Group RecommendedRecommended Not RecommendedNot Recommended
Hospitalized patients with cancer VTE prophylaxis with anticoagulantsVTE prophylaxis with anticoagulants
If bleeding or If bleeding or contraindication to contraindication to anticoagulationanticoagulation
Ambulatory patients with cancer receiving chemotherapy
Myeloma patients receiving thalidomide or Myeloma patients receiving thalidomide or lenalidomide + chemotherapy/ dexamethasone. lenalidomide + chemotherapy/ dexamethasone. LMWH or adjusted dose warfarin. LMWH or adjusted dose warfarin.
Otherwise, no routine Otherwise, no routine prophylaxisprophylaxis
Patients with cancer undergoing surgery
Prophylaxis with low-dose UFH or LMWH Prophylaxis with low-dose UFH or LMWH
Prophylaxis with mechanical methods for Prophylaxis with mechanical methods for patients with contraindications to patients with contraindications to pharmacologic methodspharmacologic methods
Consider mechanical Consider mechanical methods when methods when contraindications to contraindications to anticoagulation.anticoagulation.
Patients with cancer with established VTE
Anticoagulation for at least 6 months. Consider Anticoagulation for at least 6 months. Consider continued anticoagulation beyond 6 months in continued anticoagulation beyond 6 months in those with active cancer. those with active cancer.
--
To improve survival -- Not recommendedNot recommended
ASCO Recommendations for VTE ASCO Recommendations for VTE Prophylaxis in Patients with CancerProphylaxis in Patients with Cancer
Lyman GH et al: J Clin Oncol 2007; 25:5490-5505Lyman GH et al: J Clin Oncol 2007; 25:5490-5505
SummarySummary

Recommendations for Primary Prevention Recommendations for Primary Prevention of VTE in Patients With Cancerof VTE in Patients With Cancer
Modified from Khorana AA et al J Clin Oncol 2009; 27: 4919-4926
Parameter ASCO NCCN AIOM/ESMO FNCLCC
Prevention of VTE in the hospitalized cancer patientRecommendation All hospitalized cancer
patients without contraindications
All hospitalized cancer patients in the absence of contraindications
Immobilized hospitalized cancer patients with acute medical illness
NA
Prevention of VTE in the surgical cancer patientRecommendation Initial: major cancer
surgeryProlonged : up to 4 weeks for major surgery with high-risk features
Initial: cancer surgeryProlonged : up to 4 weeks for high risk surgery
Initial: major cancer surgery;Prolonged; up to 35 days after surgery
NA
Prevention of VTE in the ambulatory cancer patientRecommendation Not recommended
Exception of thalid/ lenalid for MM
Not recommended Exception thalid/Lenalid for MM
Not recommended Exception of thalid/ lenalid for MM
NA
Prevention of VTE in cancer patients with central venous cathetersRecommendation NA Not recommended Not recommended Not
recommended
Comparisons of Guideline PanelsComparisons of Guideline Panels

Unanswered QuestionsUnanswered QuestionsA Call to Action for Future ResearchA Call to Action for Future Research
► Prevention of VTE in the ambulatory patient Prevention of VTE in the ambulatory patient with cancer: A role for targeted with cancer: A role for targeted prophylaxis?prophylaxis?
► Prevention of VTE in the hospitalized Prevention of VTE in the hospitalized patient with cancer: a need for cancer-patient with cancer: a need for cancer-specific studies?specific studies?
► Optimal treatment of recurrent VTEOptimal treatment of recurrent VTE
► Management of incidental or screen-Management of incidental or screen-detected VTEdetected VTE
► Impact of anticoagulation on survival of Impact of anticoagulation on survival of patients with cancerpatients with cancer
Khorana AA et al J Clin Oncol 2009; 27: 4919-4926

Cancer and Venous ThromboembolismCancer and Venous ThromboembolismConclusionsConclusions
► VTE is a common complication of cancer and VTE is a common complication of cancer and cancer treatment and is associated with cancer treatment and is associated with considerable morbidity, mortality and costs.considerable morbidity, mortality and costs.
► Hospitalized medical and surgical cancer Hospitalized medical and surgical cancer patients are at increased risk for VTE and should patients are at increased risk for VTE and should be considered for pharmacologic prophylaxis if be considered for pharmacologic prophylaxis if no contraindication to anticoagulation exists.no contraindication to anticoagulation exists.
► Cancer patients treated for documented VTE Cancer patients treated for documented VTE should be considered for continued should be considered for continued anticoagulation, preferably with LMWH, for up to anticoagulation, preferably with LMWH, for up to 6 months or longer in patients with active 6 months or longer in patients with active malignancy.malignancy.
► Routine thromboprophylaxis of ambulatory Routine thromboprophylaxis of ambulatory cancer patients is not currently recommended.cancer patients is not currently recommended.

► Prophylaxis may be considered in selective Prophylaxis may be considered in selective high risk settings such as multiple myeloma high risk settings such as multiple myeloma patients receiving thalidomide/lenalidomide .patients receiving thalidomide/lenalidomide .
► Consideration of prophylactic anticoagulation Consideration of prophylactic anticoagulation in cancer patients must always balance the in cancer patients must always balance the risk of VTE with the increased risk of bleeding risk of VTE with the increased risk of bleeding and other complications. and other complications.
► Improved methods for the identification of Improved methods for the identification of cancer patients at high risk for VTE and cancer patients at high risk for VTE and candidates for targeted thromboprophylaxis candidates for targeted thromboprophylaxis are needed and under active investigation.are needed and under active investigation.
Cancer and Venous ThromboembolismCancer and Venous ThromboembolismConclusionsConclusions

Chemotherapy-Induced Nausea Chemotherapy-Induced Nausea and Vomiting (CINV)and Vomiting (CINV)
Optimizing Clinical ManagementOptimizing Clinical Management
Lee S. Schwartzberg, MD, FACP Lee S. Schwartzberg, MD, FACP Supportive Oncology Services, MemphisSupportive Oncology Services, Memphis
Accelerated Community Oncology Research NetworkAccelerated Community Oncology Research NetworkClinical Professor of MedicineClinical Professor of Medicine
University of Tennessee Medical CenterUniversity of Tennessee Medical CenterMemphis, TennesseeMemphis, Tennessee
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application

Taste
Cha
nge
Taste
Cha
nge
Chemotherapy Experienced Patients Chemotherapy Experienced Patients Rank Severe CINV Near DeathRank Severe CINV Near Death
Sun C et al. Support Care Cancer. 2005Sun C et al. Support Care Cancer. 2005
Throm
bocy
tope
nia
Throm
bocy
tope
nia0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
Me
dia
n V
AS
Sco
res
Me
dia
n V
AS
Sco
res
Remiss
ion
Remiss
ion
CINV 1
CINV 1
Curre
nt H
ealth
Curre
nt H
ealth
Alopec
ia
Alopec
ia
Depre
ssion
Depre
ssion
Ototo
xicity
Ototo
xicity
Weig
ht G
ain
Weig
ht G
ain
Sexua
l Dys
func
tion
Sexua
l Dys
func
tion
Mem
ory l
oss
Mem
ory l
oss
Consti
patio
n
Consti
patio
n
Leg
pain
Leg
pain
Fatigu
e
Fatigu
eFluFlu
Periph
eral
Neuro
path
y
Periph
eral
Neuro
path
y
Diarrh
ea
Diarrh
ea
Dysur
ia
Dysur
ia
CINV 4
CINV 4
CINV 6
CINV 6
CINV 5
CINV 5
Death
Death
Perfe
ct Hea
lth
Perfe
ct Hea
lth
CINV 2
CINV 2
Muc
ositis
Muc
ositis
CINV 3
CINV 3
Febrile
Neu
trope
nia
Febrile
Neu
trope
nia
Complete Complete ControlControl
MucositisMucositis
DeathDeath
Moderate Delayed NauseaModerate Delayed Nausea
Poorly Controlled Poorly Controlled Acute & Delayed CINVAcute & Delayed CINV

Types of CINV: DefinitionsTypes of CINV: Definitions
► Acute (posttreatment)Acute (posttreatment)● Occurs within first 24 hours after administration of Occurs within first 24 hours after administration of
cancer chemotherapycancer chemotherapy
► DelayedDelayed● CINV that begins after first 24 hoursCINV that begins after first 24 hours● May last for 120 hoursMay last for 120 hours
► AnticipatoryAnticipatory● Learned or conditioned response from poorly Learned or conditioned response from poorly
controlled nausea and vomiting associated with controlled nausea and vomiting associated with previous chemotherapyprevious chemotherapy
► BreakthroughBreakthrough● CINV that occurs despite prophylaxis and requires CINV that occurs despite prophylaxis and requires
rescuerescue

Emetogenic Potential of Single Emetogenic Potential of Single Antineoplastic Agents Antineoplastic Agents
HIGH Risk in nearly all patients (> 90%)Risk in nearly all patients (> 90%)
MODERATE Risk in 30% to 90% of patientsRisk in 30% to 90% of patients
LOW Risk in 10% to 30% of patientsRisk in 10% to 30% of patients
MINIMAL Fewer than 10% at riskFewer than 10% at risk


Patient-Specific Risk Factors for CINVPatient-Specific Risk Factors for CINV
► Age <50 yearsAge <50 years► Women > menWomen > men► History of light alcohol use History of light alcohol use ► History of vomiting with prior exposure History of vomiting with prior exposure
to chemotherapeutic agents to chemotherapeutic agents ► Other risksOther risks
● History of motion sickness History of motion sickness ● History of nausea or vomiting during History of nausea or vomiting during
pregnancypregnancy● History of anxietyHistory of anxiety
ASHP. ASHP. Am J Health Syst Pharm.Am J Health Syst Pharm. 1999:56:729-764; Balfour and Goa. 1999:56:729-764; Balfour and Goa. DrugsDrugs. 1997:54:273-298. 1997:54:273-298

Other Causes of Nausea and Other Causes of Nausea and Vomiting in Cancer patientsVomiting in Cancer patients
► Brain metastasesBrain metastases► Electrolyte disturbancesElectrolyte disturbances► GastoparesisGastoparesis► Concurrent medicationsConcurrent medications► Bowel obstructionBowel obstruction► Vestibular dysfunctionVestibular dysfunction

Pathophysiology of Chemotherapy-Induced Emesis

Pharmacologic Agents for Pharmacologic Agents for Prevention of CINVPrevention of CINV
► CorticosteroidsCorticosteroids
► Dopamine antagonistsDopamine antagonists
► Serotonin (5-HT3) antagonistsSerotonin (5-HT3) antagonists
► NK-1 receptor antagonistsNK-1 receptor antagonists

Key Milestones in Antiemetic TreatmentKey Milestones in Antiemetic Treatment
1960 1970 1980 1990 2000 2002 2004
Phenothiazines: first agents to demonstrate antiemetic effect
High-dose metoclopramide shown to enhance antiemetic effect
Combination therapy: addition of
a corticosteroid shown to improve antiemetic response
First clinical studies of 5-HT3 antagonists
Introduction of 5-HT3 antagonists into clinical practice for CINV
New class of drug: NK-1 antagonists in clinical development for CINV
Aprepitant: March 2003
Palonosetron: July 2003
Viale PH. Clin J Onc Nurs. 2005;9(1):77-84Viale PH. Clin J Onc Nurs. 2005;9(1):77-84Hesketh PJ. Support Care Cancer. 2001;9:350-4Hesketh PJ. Support Care Cancer. 2001;9:350-4Grunberg SM, Hesketh PJ. New Engl J Med. 1993;329(24):1790-6Grunberg SM, Hesketh PJ. New Engl J Med. 1993;329(24):1790-6Hesketh PJ. Support Care Cancer. 2004;12:550-4Hesketh PJ. Support Care Cancer. 2004;12:550-4

Controlling Cisplatin-induced Emesis: Controlling Cisplatin-induced Emesis: Progress Over the Past 30 YearsProgress Over the Past 30 Years
19781978
100% -100% -
75% -75% -
50% -50% -
25% -25% -
Complete Response:Complete Response:
0%0%
50%50%
19881988
60%60%
19981998
70%70%
20082008
No Useful Rx HD-MCP/Dex 5-HT3/Dex No Useful Rx HD-MCP/Dex 5-HT3/Dex 5-HT3/Dex/5-HT3/Dex/NK1NK1
(24 hour control)(24 hour control) (120 hour control)(120 hour control)

Patterns of EmesisPatterns of EmesisCisplatin vs Cyclophosphamide and CarboplatinCisplatin vs Cyclophosphamide and Carboplatin
Martin M. Oncology. 1996;53(suppl 1): 26-31Martin M. Oncology. 1996;53(suppl 1): 26-31
CisplatinCisplatin
Cyclophosphamide/CarboplatinCyclophosphamide/Carboplatin
Inte
nsity
of E
mes
isIn
tens
ity o
f Em
esis
00 11 22 33 44 55
DaysDays

11stst Generation 5HT Generation 5HT3 3 RAs RAs are Therapeutically Equivalentare Therapeutically Equivalent
Pts receiving MEC* (N=1,085)Pts receiving MEC* (N=1,085)
80% of pts received prophylactic steroids80% of pts received prophylactic steroids*Cyclophosphamide 500 - 1200 mg/m*Cyclophosphamide 500 - 1200 mg/m22, carboplatin , carboplatin ≥300 mg/m≥300 mg/m22
59.0 60.0
71.0
58.0 58.0
72.0
Total Nausea Emesis
Oral granisetron 2 mgIV ondansetron 32 mg
Co
mp
lete
Con
trol
(%
)C
om
ple
te C
ontr
ol (
%)
►Highest Level Highest Level Evidence Evidence • MASCC 2009MASCC 2009
• NCCN 2010NCCN 2010
• ASCO 2006ASCO 2006
►11stst Generation Agents Generation Agents are therapeutically are therapeutically equivalentequivalent• DolasetronDolasetron
• OndansetronOndansetron
• GranisetronGranisetron
►11stst Generation oral, IV Generation oral, IV & patch forms & patch forms equally effectiveequally effectivePerez et al. J Clin Oncol 1998;16:754Perez et al. J Clin Oncol 1998;16:754

PalonosetronPalonosetron
► Second generation 5-HTSecond generation 5-HT33 antagonist antagonist
► Pharmacologic differences from older 5-HTPharmacologic differences from older 5-HT33 antagonists antagonists● Prolonged half-life (~40 hours)Prolonged half-life (~40 hours)● Enhanced receptor binding affinity (30-foldEnhanced receptor binding affinity (30-fold))
► FDA approved FDA approved ● IV formulation IV formulation July 25, 2003July 25, 2003● Oral formulation August 22, 2008Oral formulation August 22, 2008
► RegimensRegimens● IV 0.25 mg pre chemotherapyIV 0.25 mg pre chemotherapy
acute/delayed HEC/MECacute/delayed HEC/MEC● PO 0.50 mg pre chemotherapyPO 0.50 mg pre chemotherapy
acute MECacute MEC

Palonosetron vs. 1Palonosetron vs. 1stst gen HT-3RA: Complete gen HT-3RA: Complete Response on Day of Chemo & BeyondResponse on Day of Chemo & Beyond
Palonosetron 0.25 mg (n=378)Palonosetron 0.25 mg (n=378)Ondansetron/Dolasetron 32/100 mg (n=376)Ondansetron/Dolasetron 32/100 mg (n=376)
46.846.842.042.0
**57.757.7
**64.064.0
**72.072.0
60.660.6
00
2020
4040
6060
8080
100100
Time (hr)Time (hr)
Acute: 0-24Acute: 0-24(Day 1)(Day 1)
Delayed: 24-120Delayed: 24-120(Days 2-5)(Days 2-5)
Overall: 0-120Overall: 0-120(Days 1-5)(Days 1-5)
Com
plet
e R
espo
nse
(CR
)C
ompl
ete
Res
pons
e (C
R)
(% o
f Pat
ient
s)
(% o
f Pat
ient
s)
**pp<0.025 for pairwise difference (2-sided Fisher’s exact test) between palonosetron and ondansetron/dolasetron.<0.025 for pairwise difference (2-sided Fisher’s exact test) between palonosetron and ondansetron/dolasetron.
Gralla R et al. Gralla R et al. Ann OncolAnn Oncol. 2003; Eisenberg P et al. . 2003; Eisenberg P et al. CancerCancer. 2003. 2003Rubenstein EB et al. Rubenstein EB et al. Proc Am Soc Clin Oncol.Proc Am Soc Clin Oncol. 2003. Abstract 2932 2003. Abstract 2932
CR = no emetic episodes or use of rescue medicationsCR = no emetic episodes or use of rescue medications

Aapro M Support Care Cancer 2003:11:391 Aapro M Support Care Cancer 2003:11:391
Palonosetron vs Ondansetron Palonosetron vs Ondansetron
* *
N=447(67%)
High Emetic Risk Chemotherapy High Emetic Risk Chemotherapy Patients Also Receiving DexamethasonePatients Also Receiving Dexamethasone

Phase III Trial of IV Palonosetron vs. IV Phase III Trial of IV Palonosetron vs. IV Granisetron with Cisplatin or AC-Based Granisetron with Cisplatin or AC-Based
ChemotherapyChemotherapy► 1114 patients1114 patients
► Cisplatin (57%) or anthracycline/cyclophosphamide (43%) Cisplatin (57%) or anthracycline/cyclophosphamide (43%)
► Single 0.75 mg dose of palo vs. single 40 Single 0.75 mg dose of palo vs. single 40 μμg/kg dose of g/kg dose of granisetrongranisetron
► Dexamethasone 16 mg d1; 4mg/d d 2-3 (AC/EC); 8mg/d Dexamethasone 16 mg d1; 4mg/d d 2-3 (AC/EC); 8mg/d d 2-3 CDDPd 2-3 CDDP
► Objective: demonstrate non-inferiority d1 and superiority Objective: demonstrate non-inferiority d1 and superiority d 2-5 of palonosetrond 2-5 of palonosetron
► Primary endpoint complete response (no emesis/no Primary endpoint complete response (no emesis/no rescue)rescue)
Saito M et al. Lancet Oncol. 2009;10(2):115-24 Saito M et al. Lancet Oncol. 2009;10(2):115-24

Phase III Trial Palonosetron vs. Granisetron Phase III Trial Palonosetron vs. Granisetron both with Dexamethasone in HECboth with Dexamethasone in HEC
OutcomeOutcomePalo+ DexPalo+ Dex(n=555)(n=555)
%%
Grani+ DexGrani+ Dex(n=558)(n=558)
%%PP
Complete Response, Acute (0-24h) 73.773.7 72.172.1 NDND
CR, Delayed (24-120h) 53.053.0 42.442.4 0.0000.000
33
CR, Overall (0-120h) 47.947.9 38.138.1 0.0000.00077
No Nausea: 0-120 hours 3232 2525 0.010.01
No Emesis: 0-120 hours 5858 4949 0.0060.006
Saito M et al. Lancet Oncol. 2009;10(2):115-24 Saito M et al. Lancet Oncol. 2009;10(2):115-24

**
69.069.0
61.161.164.864.8
50.050.0
00
1010
2020
3030
4040
5050
6060
7070
8080
Acute (0-24 hrs)Acute (0-24 hrs) Delayed (24-120 hrs)Delayed (24-120 hrs) Overall (0-120 hrs)Overall (0-120 hrs)
9090
**52.752.7
42.842.8
* Fisher’s exact test indicates a difference between PALO and GRAN* Fisher’s exact test indicates a difference between PALO and GRAN† † Chi-square Chi-square test indicates a difference between PALO and GRANtest indicates a difference between PALO and GRAN
* p = 0.0165 * p = 0.0165 †† p = 0.030 p = 0.030
Palonosetron 0.75 mg IV (n=239)Palonosetron 0.75 mg IV (n=239)Granisetron Granisetron 40 mcg/kg IV (n=236)40 mcg/kg IV (n=236)
Com
plet
e R
espo
nse
Com
plet
e R
espo
nse
(% o
f pat
ient
s)(%
of p
atie
nts)
Saito M, et al. Lancet Oncol 2009;10:115-124Saito M, et al. Lancet Oncol 2009;10:115-124
Data on file, Taiho/Helsinn 2008Data on file, Taiho/Helsinn 2008
Please note that the EU approved dose is 0.25 mgPlease note that the EU approved dose is 0.25 mg
Palonosetron + Dexamethasone vs Granisetron + Palonosetron + Dexamethasone vs Granisetron + Dexamethasone in Japanese PatientsDexamethasone in Japanese Patients
Complete Response – AC/EC SubsetComplete Response – AC/EC Subset

5-HT35-HT3Treatment-Related Adverse Treatment-Related Adverse
ReactionsReactions
Adverse ReactionAdverse Reaction
PalonosetronPalonosetron0.25 mg IV0.25 mg IV
(n=187)(n=187)
PalonosetronPalonosetron0.75 mg IV0.75 mg IV
(n=188)(n=188)
OndansetronOndansetron32 mg IV32 mg IV(n=187)(n=187)
nn %% nn %% nn %%
Headache 9 4.8 10 5.3 10 5.3
Constipation 3 1.6 6 3.2 3 1.6
Dizziness 1 0.5 0 0.0 6 3.2
Adverse reaction = adverse event judged by the investigator to have a definite, probable, possible or unknown Adverse reaction = adverse event judged by the investigator to have a definite, probable, possible or unknown relationship to study medicationrelationship to study medication
n = number of patients with the adverse reactionn = number of patients with the adverse reaction
*Reported in *Reported in 2% of patients in any treatment group2% of patients in any treatment group
Gralla R, et al. Ann Oncol. 2003;14:1570-1577Gralla R, et al. Ann Oncol. 2003;14:1570-1577

Palonosetron: Palonosetron: 5-HT5-HT33 Antagonist of Choice? Antagonist of Choice?
► Palonosetron is a 5-HTPalonosetron is a 5-HT33 antagonist with strong receptor antagonist with strong receptor binding affinity and an extended half-life binding affinity and an extended half-life
► Comparable tolerability Comparable tolerability
► Ease of use and trends towards superiority in delayed Ease of use and trends towards superiority in delayed CINV favor palonosetron as the preferred 5-HTCINV favor palonosetron as the preferred 5-HT33 antagonist antagonist
► Definitive proof of superiority to first generation 5-HTDefinitive proof of superiority to first generation 5-HT33 antagonists would require trials with control arms utilizing antagonists would require trials with control arms utilizing corticosteroids, NKcorticosteroids, NK11 antagonists antagonists andand repetitive dosing of repetitive dosing of the first generation agentsthe first generation agents

AprepitantAprepitant
► Selective antagonist of the binding of Substance P to the Selective antagonist of the binding of Substance P to the neurokinin 1 (NK1) receptorneurokinin 1 (NK1) receptor
► FDA approved FDA approved ● Oral formulation: March 26, 2003Oral formulation: March 26, 2003● IV formulation (fosaprepitant): January 31, 2008IV formulation (fosaprepitant): January 31, 2008
► RegimenRegimen● 125 mg PO day 1, 80 mg PO days 2-3125 mg PO day 1, 80 mg PO days 2-3
acute/delayed HEC/MECacute/delayed HEC/MEC● 115 mg IV day 1, 80 mg PO days 2-3115 mg IV day 1, 80 mg PO days 2-3
acute/delayed HEC/MECacute/delayed HEC/MEC

Aprepitant in Anthracycline/ Aprepitant in Anthracycline/ Cyclophosphamide ChemotherapyCyclophosphamide Chemotherapy
**pp<0.05 <0.05 Complete response (CR): no emesis and no rescue medication.Complete response (CR): no emesis and no rescue medication.
Warr DG et al. Warr DG et al. J Clin Oncol J Clin Oncol 2005; 23:2822-2830 2005; 23:2822-2830
*
*
76
55 51
69
4942
0
20
40
60
80
100
Acute: 0-24Acute: 0-24(Day 1)(Day 1)
Delayed: 24-120Delayed: 24-120(Days 2-5)(Days 2-5)
Overall: 0-120Overall: 0-120(Days 1-5)(Days 1-5)
Com
plet
e R
espo
nse
(CR
)C
ompl
ete
Res
pons
e (C
R)
(% o
f P
atie
nts)
(% o
f P
atie
nts)
Aprepitant (n=433) Standard (n=424)
Time (hr)Time (hr)
Complete Response (N=857)Complete Response (N=857)

Aprepitant in Moderately Aprepitant in Moderately Emetogenic ChemotherapyEmetogenic Chemotherapy
Warr DG et al. Warr DG et al. J Clin OncolJ Clin Oncol 2005; 23:2822-2830 2005; 23:2822-2830
**pp<0.001<0.001
**
*88
817677
6959
0
20
40
60
80
100
Acute: 0-24Acute: 0-24(Day 1)(Day 1)
Delayed: 24-120Delayed: 24-120(Days 2-5)(Days 2-5)
Overall: 0-120Overall: 0-120(Days 1-5)(Days 1-5)
Em
esis
-Fre
eE
mes
is-F
ree
(% o
f Pa
tient
s)(%
of P
atie
nts)
Aprepitant (n=433) Standard (n=424)
Time (hr)Time (hr)
Percent of Patients with No Emesis

Aprepitant in Moderately Aprepitant in Moderately Emetogenic ChemotherapyEmetogenic Chemotherapy
No nausea: score <5 mm on 0-100 mm VAS.No nausea: score <5 mm on 0-100 mm VAS.
Warr DG et al. Warr DG et al. J Clin OncolJ Clin Oncol 2005; 23:2822-2830; Warr DG et al. 2005; 23:2822-2830; Warr DG et al. Support Care CancerSupport Care Cancer. 2004. Abstract A027. 2004. Abstract A027
61
3733
59
36 33
0
20
40
60
80
100
Acute: 0-24Acute: 0-24(Day 1)(Day 1)
Delayed: 24-120Delayed: 24-120(Days 2-5)(Days 2-5)
Overall: 0-120Overall: 0-120(Days 1-5)(Days 1-5)
Nau
sea-
Fre
eN
ause
a-F
ree
(% o
f Pa
tient
s)(%
of P
atie
nts)
Aprepitant (n=430) Standard (n=424)
Time (hr)Time (hr)
Percent of Patients with No NauseaPercent of Patients with No Nausea

Phase III Aprepitant Study (801):Phase III Aprepitant Study (801):Multiple-day OndansetronMultiple-day Ondansetron
Aprepitant Aprepitant
ControlControl
GroupGroup Day 4Day 4
16
8
Day 1Day 1
32 12 125
3232 20
Days 2-3Days 2-3
808
16
OO DD AA DDDD AA
O=ondansetron; D=dexamethasone; A=aprepitant; P=placeboO=ondansetron; D=dexamethasone; A=aprepitant; P=placebo
PPPP
P
16
P
16
OO OO
Schmoll et al: Ann Oncol 17:1000-6, 2006Schmoll et al: Ann Oncol 17:1000-6, 2006
•Initial cycle cisplatin Initial cycle cisplatin >> 70 mg/m2 70 mg/m2
•445 patients445 patients

Phase III Aprepitant Study (801):Phase III Aprepitant Study (801):Multiple-day OndansetronMultiple-day Ondansetron
► Identical design to Protocols 052 and 054 except Identical design to Protocols 052 and 054 except ondansetron dosed days 1-4 ondansetron dosed days 1-4
► Primary endpoint: complete response on days 1 - Primary endpoint: complete response on days 1 - 5 after cisplatin5 after cisplatin
► Aprepitant regimen superior to control regimen of Aprepitant regimen superior to control regimen of protracted ondansetron and dexamethasone protracted ondansetron and dexamethasone dosing, CR 72% vs. 61% respectively dosing, CR 72% vs. 61% respectively
Schmoll et al: Ann Oncol 17:1000-6, 2006Schmoll et al: Ann Oncol 17:1000-6, 2006

Perception vs Reality: Perception vs Reality: Emetogenic ChemotherapyEmetogenic Chemotherapy
Grunberg S. Grunberg S. CancerCancer. 2004;100:2261-2268. 2004;100:2261-2268
Highly Emetogenic ChemotherapyHighly Emetogenic ChemotherapyModerately Emetogenic ChemotherapyModerately Emetogenic Chemotherapy

Optimizing Supportive Optimizing Supportive Care Care inin Cancer Cancer
The best treatment of The best treatment of delayed CINV is to prevent delayed CINV is to prevent
it!it!

► 671 pts receiving doxorubicin-based 671 pts receiving doxorubicin-based chemotherapychemotherapy● All treated w/ All treated w/ 11stst generation generation 5HT5HT3 3 + Dex+ Dex on Day 1 of CT on Day 1 of CT
► Pts then randomized Pts then randomized for days 2 and 3for days 2 and 3::● Arm 1: Arm 1: Prochlorperazine 10 mg p.o. three times daily Prochlorperazine 10 mg p.o. three times daily
(q 8 h)(q 8 h)● Arm 2: Arm 2: Any oral 5-HTAny oral 5-HT3 3 antiemetic, using standard antiemetic, using standard
dosing dosing regimens regimens● Arm 3: Arm 3: Prochlorperazine 10 mg p.o. as needed for Prochlorperazine 10 mg p.o. as needed for
nauseanausea
► Rescue medications for control of symptoms Rescue medications for control of symptoms were allowedwere allowed
Are Oral Followup 5-HTAre Oral Followup 5-HT33 RAs Really RAs Really Effective for Delayed CINV? Effective for Delayed CINV?
Hickock et al ASCO 2005 Final Results URCC-CCOPHickock et al ASCO 2005 Final Results URCC-CCOP

Oral 5HTOral 5HT33 RAs: RAs:Majority of Patients Experience Majority of Patients Experience
NauseaNausea
• Patients randomized for days 2 and 3; rescue medications allowedPatients randomized for days 2 and 3; rescue medications allowedHickock et al ASCO 2005 Final Results URCC-CCOPHickock et al ASCO 2005 Final Results URCC-CCOP
* p = 0.002 (overall comparison); p = 0.06 (* p = 0.002 (overall comparison); p = 0.06 (Prochlorperazine q 8 h vs 5-HT q 8 h vs 5-HT3 3 ); );
p = NS (p = NS (Prochlorperazine prn vs 5-HT prn vs 5-HT3 3 ))
102030405060708090
100 Prochlorperazine q 8h*
5HT33**Prochlorperazine PRN*
% P
atie
nts
with
Del
ayed
Nau
sea
% P
atie
nts
with
Del
ayed
Nau
sea
7583 87

Oral 5HTOral 5HT33 RAs RAs Not Effective for Delayed CINV Not Effective for Delayed CINV
► Vomiting Vomiting ● Significantly Significantly more patients vomitedmore patients vomited at least once at least once
during the delayed period during the delayed period (34%)(34%) than on the day of than on the day of treatment treatment (19%) p <0.01(19%) p <0.01
► NauseaNausea● Nausea severity was significantly greater during the Nausea severity was significantly greater during the
delayed period than on the day of treatment delayed period than on the day of treatment p < 0.01p < 0.01
● More patients getting oral 5HTMore patients getting oral 5HT33 RAs required rescue RAs required rescue medications medications (45%)(45%) than patients getting Compazine than patients getting Compazine®® (27-30%)(27-30%) p=0.002p=0.002
Hickock et al ASCO 2005 Final Results URCC-CCOPHickock et al ASCO 2005 Final Results URCC-CCOP

Meta-Analysis of Efficacy of 5-HTMeta-Analysis of Efficacy of 5-HT33RA in Prevention RA in Prevention of Delayed Emesis from Chemotherapyof Delayed Emesis from Chemotherapy
► Reviewed 5 studies, 1,716 pts comparing 5-HTReviewed 5 studies, 1,716 pts comparing 5-HT3 3 RA to RA to placebo, placebo,
► 5 studies, 2,240 pts comparing 5-HT5 studies, 2,240 pts comparing 5-HT33 RA + RA + dexamethasone to dexamethasone alonedexamethasone to dexamethasone alone
5-HT5-HT33 RA as monotherapy RA as monotherapy
Absolute RR (95% CI) 8.2% (3.0-13.4)Absolute RR (95% CI) 8.2% (3.0-13.4)
NNT 12.2 Number of doses per protected pt: 74.4NNT 12.2 Number of doses per protected pt: 74.4
5-HT5-HT33 RA as adjunct to dexamethasone RA as adjunct to dexamethasone
Absolute RR (95% CI) Absolute RR (95% CI) 2.6% (-0.6-5.8)2.6% (-0.6-5.8)
NNT 38.8 NNT 38.8 Number of doses per protected pt: 423Number of doses per protected pt: 423Geling and Eichler, JCO 2005; 23:1289-1294Geling and Eichler, JCO 2005; 23:1289-1294

Breakthrough Medications for CINVBreakthrough Medications for CINV
► AntipsychoticsAntipsychotics
► CannabinoidsCannabinoids
► BenzodiazepinesBenzodiazepines
► PhenothiazinesPhenothiazines
► Dopamine Receptor AntagonistsDopamine Receptor Antagonists
Consider other classes, alone or in combinationConsider other classes, alone or in combination

Emetic Emetic
risk grouprisk group
Risk (% of Risk (% of
patients)patients)Acute preventionAcute prevention Delayed preventionDelayed prevention
High and AC combinations
>90% 5-HT3 RA
+ DEX + aprepitant
lorazepam H2 blocker
or proton pump inhibitor
DEX + aprepitant
lorazepam H2 blocker or
proton pump inhibitor
NCCN Antiemesis Guidelines NCCN Antiemesis Guidelines v.2.2010: HEC Recommendationsv.2.2010: HEC Recommendations
DEX, dexamethasone; AC, anthracycline-cyclophosphamideDEX, dexamethasone; AC, anthracycline-cyclophosphamide
For more information see: http://www.nccn.orgFor more information see: http://www.nccn.org

Emetic Emetic
risk grouprisk group
Risk (% of Risk (% of
patients)patients)Acute preventionAcute prevention Delayed preventionDelayed prevention
Moderate 30-90%
5-HT3 RA + DEX
lorazepam H2 blocker
or proton pump inhibitor
5-HT3 RA or DEX
lorazepam H2 blocker or
proton pump inhibitor
Low 10-30%
DEX, prochlorperazine, or metoclopramide
lorazepam H2 blocker
or proton pump inhibitor
No preventive measures
Minimal <10% No routine prophylaxis No preventive measures
NCCN Antiemesis Guidelines NCCN Antiemesis Guidelines v.2.2010:v.2.2010:
MEC RecommendationsMEC Recommendations
DEX, dexamethasoneDEX, dexamethasone
For more information see: http://www.nccn.orgFor more information see: http://www.nccn.org

MASCC / ESMO Committees II-VMASCC / ESMO Committees II-VCombined Statement #3 – Moderate*Combined Statement #3 – Moderate*
Prevention of nausea and vomiting following Prevention of nausea and vomiting following chemotherapy of moderate emetic risk:chemotherapy of moderate emetic risk:
To prevent acute and delayed vomiting and To prevent acute and delayed vomiting and nausea following chemotherapy of nausea following chemotherapy of moderate moderate emetic riskemetic risk, we recommend a regimen of , we recommend a regimen of palonosetron and multiday dexamethasone palonosetron and multiday dexamethasone beginning before chemotherapybeginning before chemotherapy
June 2009June 2009Multinational Association for Supportive Care in Cancer. Multinational Association for Supportive Care in Cancer. www.mascc.orgwww.mascc.org
* Does not include “AC” given its higher risk of nausea and * Does not include “AC” given its higher risk of nausea and vomiting, in which an NKvomiting, in which an NK11 RA is added to Dex + 5HT RA is added to Dex + 5HT33 RA RA

Summary Summary
► 11stst generation 5HT generation 5HT3 3 RA’s therapeutically equivalent & RA’s therapeutically equivalent & major advance in supportive care for control of major advance in supportive care for control of acute emesisacute emesis
► Newer agents include 2Newer agents include 2ndnd generation 5-HT3 RA generation 5-HT3 RA palonosetron and NK-1 antagonist aprepitantpalonosetron and NK-1 antagonist aprepitant
► Treatment guidelines have changed Treatment guidelines have changed ● Degree of nausea incurred has been refined for many Degree of nausea incurred has been refined for many
agentsagents● Delayed CINV recommendations are updatedDelayed CINV recommendations are updated
► Prevention of CINV has improved, but challenges Prevention of CINV has improved, but challenges remainremain● Improving detection of CINV, especially after 24 hoursImproving detection of CINV, especially after 24 hours● Educating patients and oncology healthcare giversEducating patients and oncology healthcare givers● The development and evaluation of clinically useful The development and evaluation of clinically useful
assessment tools assessment tools ● Further development of regimens to treat delayed Further development of regimens to treat delayed
CINVCINV

Risk Stratification Tools to Identify Risk Stratification Tools to Identify Patients for Primary and Secondary Patients for Primary and Secondary Prevention of VTE in the Setting of Prevention of VTE in the Setting of
MalignancyMalignancy
Screening and VTE Risk Assessment Across the Screening and VTE Risk Assessment Across the Complex Spectrum of Malignant Disorders—Complex Spectrum of Malignant Disorders—
What Works? What Doesn’t?What Works? What Doesn’t?
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application
Alok A. Khorana, MD, FACPAlok A. Khorana, MD, FACPVice-Chief, Division of Hematology/OncologyVice-Chief, Division of Hematology/Oncology
Associate Professor of Medicine and OncologyAssociate Professor of Medicine and OncologyJames P. Wilmot Cancer CenterJames P. Wilmot Cancer Center
University of RochesterUniversity of RochesterRochester, New YorkRochester, New York

Risk Assessment for VTE In Risk Assessment for VTE In Cancer PatientsCancer Patients Risk Factors for VTERisk Factors for VTE BiomarkersBiomarkers
Risk Assessment ModelsRisk Assessment Models
Implications for Study Design of Implications for Study Design of Prophylaxis TrialsProphylaxis Trials
Secondary ProphylaxisSecondary Prophylaxis
Optimizing Supportive Care in CancerOptimizing Supportive Care in Cancer

Risk Factors for VTERisk Factors for VTE
Patient-related factorsPatient-related factors Older age Older age Race, genderRace, gender ComorbiditiesComorbidities
Treatment-related Treatment-related factorsfactors
Hospitalization Hospitalization Chemotherapy Chemotherapy Anti-angiogenicsAnti-angiogenics Major surgeryMajor surgery Erythropoiesis-Erythropoiesis-
stimulating agents stimulating agents TransfusionsTransfusions
Cancer-related factorsCancer-related factors Site of cancer Site of cancer Advanced stageAdvanced stage Initial period after Initial period after
diagnosis diagnosis
Rao et al., in Rao et al., in Cancer-Associated Thrombosis. Cancer-Associated Thrombosis. (Khorana and Francis, Eds)(Khorana and Francis, Eds) 20072007

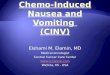
Type of Type of cancercancer
Adjusted OR Adjusted OR (95% CI)(95% CI)
Hematologic 28 (4-199.7)28 (4-199.7)
Lung 22.2 (3.6-136.1)22.2 (3.6-136.1)
GI 20.3 (4.9-83)20.3 (4.9-83)
Breast 4.9 (2.3-10.5)4.9 (2.3-10.5)
Prostate 2.2 (0.9-5.4)2.2 (0.9-5.4)
Blom JW et al. Blom JW et al. JAMA JAMA 20052005
VTE and Site of CancerVTE and Site of Cancer

VTE in the REAL-2 Study: VTE in the REAL-2 Study: Oxaliplatin vs CisplatinOxaliplatin vs Cisplatin
Starling et al JCO 2009
P=0.0003
HRHR for cisplatin for cisplatin 0.51; 95% CI, 0.34 to 0.76; P = .001 0.51; 95% CI, 0.34 to 0.76; P = .001

VTE With BevacizumabVTE With Bevacizumab
Bevacizumab(n=1,196)
Control (n=1,083)
Nalluri SR, et al. Nalluri SR, et al. JAMA.JAMA. 2008;300:2277-2285. 2008;300:2277-2285.
RR=1.29 (95% CI, 1.03-1.63)RR=1.29 (95% CI, 1.03-1.63)
Ra
te o
f V
TE
(%
)R
ate
of
VT
E (
%)
13%13%
9.9%
Bevacizumab (n=3,795)
Control (n=3,167)
6.2%6.2%
4.2%
RR=1.38 (95% CI, 1.12-RR=1.38 (95% CI, 1.12-1.70)1.70)
All-Grade VTEAll-Grade VTE((6 studies)6 studies)
High-Grade VTEHigh-Grade VTE((13 studies)13 studies)

VTE in MyelomaVTE in Myeloma
Palumbo et al. JTH 2006: 4 1842-45
MonthsMonths
Cum
ulat
ive
Per
cent
age
Cum
ulat
ive
Per
cent
age MPTMPT
MPT and EnoxaparinMPT and Enoxaparin
RMP and AspirinRMP and AspirinMPMP
00 5 5 10 10 15 20 25 15 20 25
0.20.2
0.10.1
00

Candidate BiomarkersCandidate Biomarkers
►Blood countsBlood counts Platelet countPlatelet count Leukocyte countLeukocyte count HemoglobinHemoglobin
►Tissue factorTissue factor
►Soluble P-selectinSoluble P-selectin
►D-dimerD-dimer
►C-reactive proteinC-reactive protein
►Factor VIIIFactor VIII

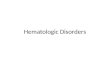
Incidence of VTE By Quartiles Of Incidence of VTE By Quartiles Of Pre-Chemotherapy Platelet CountPre-Chemotherapy Platelet Count
Khorana AA et al. Khorana AA et al. Cancer Cancer 20052005
0%
1%
2%
3%
4%
5%
6%
<250 250-300 300-350 >350
Pre-chemotherapy Platelet Counts (x1000)Pre-chemotherapy Platelet Counts (x1000)
Inci
dence
Of
VTE O
ver
2.5
Month
s(%
)
Inci
dence
Of
VTE O
ver
2.5
Month
s(%
)
•P =0.005

Incidence of VTE by Pre-Incidence of VTE by Pre-Chemotherapy Leukocyte CountChemotherapy Leukocyte Count
Khorana AA et al. Khorana AA et al. Blood Blood 20082008
0%0%
1%1%
2%2%
3%3%
4%4%
5%5%
6%6%
<4.5 (n=342)<4.5 (n=342) 4.5-11 (n=3202)4.5-11 (n=3202) >11 (n=513)>11 (n=513)
Pre-chemotherapy WBC Counts (x1000/mmPre-chemotherapy WBC Counts (x1000/mm33))
Inci
dence
Of
VTE O
ver
2.4
In
cidence
Of
VTE O
ver
2.4
Month
sM
onth
s (%
) (
%)
•P =0.0008

Incidence of VTE by Type of LeukocyteIncidence of VTE by Type of Leukocyte
Absolute Neutrophil Absolute Neutrophil Count Count
Absolute Monocyte Absolute Monocyte Count Count
P=0.0001
P<0.0001
Connolly et al ISTH 2009 Abs 1573Connolly et al ISTH 2009 Abs 1573
Pro
port
ion
with
VT
EP
ropo
rtio
n w
ith V
TE

Independent Effect of Platelet & Independent Effect of Platelet & Leukocyte Counts In A Multivariate Leukocyte Counts In A Multivariate
AnalysisAnalysis
VariableVariableOdds Ratio* Odds Ratio*
(95% CI)(95% CI)P valueP value
Platelet count >350,000/mm3 1.8 (1.1-3.2)1.8 (1.1-3.2) 0.030.03
Leukocyte count >11,000/mm3 2.2 (1.2-4.0)2.2 (1.2-4.0) 0.0080.008
*Adjusted for site of cancer, stage, hemoglobin < 10g/dl or use of ESAs and obesity
Khorana AA et al. Khorana AA et al. Blood Blood 20082008

Effect of Leukocyte and Platelet Effect of Leukocyte and Platelet Counts on VTE RiskCounts on VTE Risk
In the Vienna CATS registry, platelet count In the Vienna CATS registry, platelet count >>443,000 was associated with VTE (HR3.5)443,000 was associated with VTE (HR3.5)
Simanek et alSimanek et al, J Thromb Hemost , J Thromb Hemost 20092009
In the RIETE registry, patients with In the RIETE registry, patients with leukocytosis had increased risk of recurrent leukocytosis had increased risk of recurrent VTE and death (OR 2.7)VTE and death (OR 2.7)
Trujillo-Santos et al, Trujillo-Santos et al, Thromb Hemost Thromb Hemost 20082008
In the REAL-2 study of advanced GEJ/gastric In the REAL-2 study of advanced GEJ/gastric cancers, leukocytosis was associated with cancers, leukocytosis was associated with VTE during chemotherapy (HR 2.0)VTE during chemotherapy (HR 2.0)
Starling et al, Starling et al, J Clin Oncol J Clin Oncol 20092009

Mortality by Pre-chemotherapy Mortality by Pre-chemotherapy Leukocyte CountLeukocyte Count
14.0% (8.9%-21.6%) 14.0% (8.9%-21.6%)
4.4% (3.2%-6.1%) 4.4% (3.2%-6.1%)
P <0.0001P <0.0001
MVA for early mortality: HR 2.0, p = 0.001MVA for early mortality: HR 2.0, p = 0.001
Kuderer et al ASH 2008Kuderer et al ASH 2008Connolly et al ISTH 2009Connolly et al ISTH 2009
WBC>11x10WBC>11x1099/L/L
WBCWBC<<11x1011x1099/L/L
Time (Days)Time (Days)
Pro
port
ion
Die
dP
ropo
rtio
n D
ied
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 1500 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150
0.200.20
0.180.18
0.160.16
0.140.14
0.120.12
0.100.10
0.080.08
0.060.06
0.040.04
0.020.02
0.000.00

Tissue Factor in Cancer: Tissue Factor in Cancer: Lack of Standardized AssaysLack of Standardized Assays
► Immunohistochemistry of tumor Immunohistochemistry of tumor specimensspecimens
► TF ELISATF ELISA
► TF MP procoagulant activity TF MP procoagulant activity assayassay
► Impedance-based flow cytometryImpedance-based flow cytometry

Tissue Factor Expression and VTETissue Factor Expression and VTE
Khorana AA, et al. Clin Cancer Res. 2007;13:2870-2875.
Rat
e o
f V
TE
(%
)R
ate
of
VT
E (
%)
P = 0.04

Circulating Tissue Factor and VTECirculating Tissue Factor and VTE
Khorana AA, et al. Khorana AA, et al. J Thromb Haemost. J Thromb Haemost. 2008;6:1983-1985.2008;6:1983-1985.
Pla
sma
TF
(p
g/m
L)
Pla
sma
TF
(p
g/m
L)
P = .04
DVTDVT
DVTDVT Fatal PEFatal PE

Cumulative Incidence of VTE for Cancer Cumulative Incidence of VTE for Cancer Patients According to TF–bearing Patients According to TF–bearing
MicroparticlesMicroparticles
Zwicker J I et al. Clin Cancer Res 2009;15:6830-6840Zwicker J I et al. Clin Cancer Res 2009;15:6830-6840
Log Rank P=0.002Log Rank P=0.002
MonthsMonths
Cum
ulat
ive
Inci
denc
e of
VT
EC
umul
ativ
e In
cide
nce
of V
TE
0 5 10 15 20 250 5 10 15 20 25
0.60.6
0.50.5
0.40.4
0.30.3
0.20.2
0.10.1
0.00.0

FRAGEM and TF Biomarker DataFRAGEM and TF Biomarker Data
Maraveyas, et al. Blood Coagul Fibrinolysis 2010Maraveyas, et al. Blood Coagul Fibrinolysis 2010
250250
200200
150150
100100
5050
00
-50-50
ControlControl DalteparinDalteparin
Boxplot of the percentage change of tissue factor antigen in the Boxplot of the percentage change of tissue factor antigen in the sera of pancreatic cancer patients in both the control and dalteparin sera of pancreatic cancer patients in both the control and dalteparin
groupsgroups

TF and Survival In Pancreatic CancerTF and Survival In Pancreatic Cancer
Bharthuar et al Bharthuar et al ASCO GI ASCO GI 20102010
Median Survival in pts with TF MP-PCA >2.5 and </=2.5pg/ml. Median Survival in pts with TF MP-PCA >2.5 and </=2.5pg/ml.
Median survival was Median survival was 98.5 days 98.5 days for TF >2.5 for TF >2.5 pg/mL vs.pg/mL vs.231 days 231 days for TF </= for TF </= 2.5 pg/mL2.5 pg/mLp=< 0.0001p=< 0.0001
N=117 patients with N=117 patients with pancreaticobiliary pancreaticobiliary cancerscancers
Pro
por
tion
surv
ivin
gP
rop
ortio
n su
rviv
ing
Days on studyDays on study
TF (pg/mL) <2.5 >=2.5TF (pg/mL) <2.5 >=2.5
0 100 200 300 400 500 600 700 800 900 10000 100 200 300 400 500 600 700 800 900 1000
10100.90.90.80.80.70.70.60.60.50.50.40.40.30.30.20.20.10.1
00

Originally published in Ay C, et al. Originally published in Ay C, et al. Blood. Blood. 2008;112:2703-2708. Copyright © 2008 American Society 2008;112:2703-2708. Copyright © 2008 American Society of Hematology. of Hematology.
Soluble P-Selectin and VTE in CancerSoluble P-Selectin and VTE in Cancer
► 687 cancer patients 687 cancer patients followed for median of 415 followed for median of 415 daysdays
► sP-Selectin independent sP-Selectin independent predictor of VTEpredictor of VTE
► Cumulative 6-mo probability Cumulative 6-mo probability of VTE was 12% vs 4% for of VTE was 12% vs 4% for levels < 75levels < 75thth percentile percentile
Observation time (days)Observation time (days)
Cum
ula
tive
pro
babi
lity
of V
TE
(%
)C
umu
lativ
e p
roba
bilit
y of
VT
E (
%)
0 100 200 300 400 500 600 7000 100 200 300 400 500 600 700
0.250.25
0.200.20
0.150.15
0.100.10
0.050.05
0.000.00
>> 75 75thth percentile percentile
< 75< 75thth percentile percentile

Ay, C. et al. J Clin Oncol; 27:4124-4129 2009
D-dimer, F1/2 and VTE in CancerD-dimer, F1/2 and VTE in Cancer
Elevated D-dElevated D-d
Elevated D-d+F1/2Elevated D-d+F1/2
Elevated F1/2 aloneElevated F1/2 alone
NonelevaNonelevated D-d and F1/2
Observation Time (Days)Observation Time (Days)
Cum
ulat
ive
Ris
k (p
roba
bilit
y)C
umul
ativ
e R
isk
(pro
babi
lity)
0 100 200 300 400 500 600 7000 100 200 300 400 500 600 700
0.250.25
0.200.20
0.150.15
0.100.10
0.050.05

Risk Assessment for VTE In Risk Assessment for VTE In Cancer PatientsCancer Patients Risk FactorsRisk Factors BiomarkersBiomarkers
Risk Assessment ModelsRisk Assessment Models
Implications for Study Design of Implications for Study Design of Prophylaxis TrialsProphylaxis Trials
Optimizing Supportive Care in CancerOptimizing Supportive Care in Cancer

VTE in Cancer OutpatientsVTE in Cancer Outpatients
► The overwhelming majority of cancer The overwhelming majority of cancer patients are treated in the patients are treated in the outpatient/ambulatory settingoutpatient/ambulatory setting
► Which patients are most at risk?Which patients are most at risk?
► Which patients will benefit most from Which patients will benefit most from prophylaxis?prophylaxis?
How do you define “high” risk?► Level of risk for which prophylaxis is
considered acceptable by both patients and oncologists

Risk ModelRisk Model
Patient CharacteristicPatient Characteristic ScoreScore
Site of Cancer
Very high risk (stomach, pancreas)
High risk (lung, lymphoma, gynecologic, GU excluding prostate)
22
11
Platelet count > 350,000/mm3 11
Hb < 10g/dL or use of ESA 11
Leukocyte count > 11,000/mm3 11
BMI > 35 kg/m2 11
Khorana AA et al. Khorana AA et al. Blood Blood 20082008

Risk Model ValidationRisk Model Validation
Risk Low (0) Intermediate(1-2) High(Risk Low (0) Intermediate(1-2) High(>>3)3)
0%0%
1%1%
2%2%
3%3%
4%4%
5%5%
6%6%
7%7%
8%8%
Rate
of
VTE o
ver
2.5
mos
(%)
Rate
of
VTE o
ver
2.5
mos
(%)
n=734n=734 n=1627n=1627 n=340n=340
0.8%0.8%
1.8%1.8%
7.1%7.1%Development cohortDevelopment cohort
0.3%0.3%
2.0%2.0%
6.7%6.7%
Validation cohortValidation cohort
n=374n=374 n=842n=842 n=149n=149
Khorana AA et al. Khorana AA et al. Blood Blood 20082008

► Full data available in 839 patientsFull data available in 839 patients► Median observation time/follow-up: 643 days Median observation time/follow-up: 643 days
Score 0
Score 1
Score 2
Score ≥3
6 months
1.5%
3.8%
9.4%
17.7%
Number of
Patients Eventsn n (%)
Score ≥3 96 16 (17%)
Score 2 231 25 (11%)
Score 1 233 14 (6%)
Score 0 279 7 (3%)
Vienna CATS ValidationVienna CATS Validation
Ay et al ISTH 2009 Abs Ay et al ISTH 2009 Abs

Expanded Risk Score withExpanded Risk Score withD-Dimer and sP-selectinD-Dimer and sP-selectin
Score Score ≥≥55
Score 4Score 4
Score 3Score 3
Score 2Score 2Score 1Score 1Score 0Score 0
30.3%
1.0%
6 months
Number ofNumber ofPatients Patients EventsEvents
n n n (%)n (%)
Score Score ≥≥55 3131 9 (29%)9 (29%)
Score 4Score 4 5252 10 (19%)10 (19%)
Score 3Score 3 137137 15 (11%)15 (11%)
Score 2Score 2 226226 11 (5%) 11 (5%)
Score 1Score 1 192192 13 (7%)13 (7%)
Score 0Score 0 201201 4 (2%)4 (2%)
Ay et al ISTH 2009 Abs Ay et al ISTH 2009 Abs

Risk Model Is Highly Predictive of Short-Risk Model Is Highly Predictive of Short-Term Overall SurvivalTerm Overall Survival
Time (Days)
1201101009080706050403020100
Ove
rall
Su
rviv
al
1.00
.95
.90
.85
.80
.75
Low
Intermediate
High
P < 0.0001
Kuderer NM et al. Kuderer NM et al. ASH ASH 20082008
By VTE Risk Score CategoriesBy VTE Risk Score Categories

Progression-Free Survival and Overall Progression-Free Survival and Overall Survival by VTE Risk CategorySurvival by VTE Risk Category
Outcomes Outcomes
(at 4 months)(at 4 months)
Low Low Risk Risk
N=1,206N=1,206
IntermediatIntermediate Riske RiskN=2,709N=2,709
High High Risk Risk N=543N=543
All All Patients Patients
N=4,458N=4,458
MortalityRisk (%) 1.2%1.2% 5.9%5.9% 12.7%12.7% 5.6%5.6%
HR [+/- CI] 1.01.03.56 [1.91-3.56 [1.91-
6.66] 6.66] 6.89 [3.50-6.89 [3.50-
13.57] 13.57] --
PFSRisk (%) 93%93% 82%82% 72%72% 84%84%
HR [+/- CI] 1.01.02.77 [1.97-2.77 [1.97-
3.87] 3.87] 4.27 [2.90-6.27] 4.27 [2.90-6.27] --
Kuderer NM et al. Kuderer NM et al. ASH ASH 20082008

Risk Assessment for VTE In Risk Assessment for VTE In Cancer PatientsCancer Patients Risk FactorsRisk Factors BiomarkersBiomarkers
Risk Assessment ModelsRisk Assessment Models
Implications for Study Design of Implications for Study Design of Prophylaxis TrialsProphylaxis Trials
Optimizing Supportive Care in CancerOptimizing Supportive Care in Cancer

Rates of VTE in Recent Rates of VTE in Recent Prophylaxis StudiesProphylaxis Studies
N=930 N=312 N=123N=1165
Agnelli et al Agnelli et al Lancet Onc Lancet Onc 20092009Palumbo et al Palumbo et al ASH ASH 20092009Riess et al IRiess et al ISTHSTH 2009 2009Maraveyas et al Maraveyas et al ESMOESMO 2009 2009

VTE in Lung Cancer: VTE in Lung Cancer: PROTECHT and TOPIC studiesPROTECHT and TOPIC studies
sVTE LMWHsVTE
PlaceboAll VTE LMWH
All VTE Placebo
PROTECHT 3.5% 5% 4% 6.2%
TOPIC-2 3% 5.7% 4.5% 8.3%
All 3.2% 5.5% 4.3% 7.8%
Verso et al. JTH 2010 onlineVerso et al. JTH 2010 online
Major Major Bleeding Bleeding
LMWHLMWH
Major Major Bleeding Bleeding PlaceboPlacebo
PROTECHT 1%1% 0%0%
TOPIC-2 3.7%3.7% 2.2%2.2%
All 2.5%2.5% 1.7%1.7%
NNT=50 (sVTE)NNT=28 (allVTE)RRR=46%NNH=125

International Myeloma Working Group International Myeloma Working Group Thromboprophylaxis RecommendationsThromboprophylaxis Recommendations
Palumbo A, Rajkumar SV, Dimopoulos MA, et al. Prevention of thalidomide- and lenalidomide associated thrombosis in myeloma. Leukemia. 2008 Feb;22(2): 414-23.
Individual risk factors: Individual risk factors: obesity (BMI ≥ 30), prior VTE, central venous obesity (BMI ≥ 30), prior VTE, central venous cathetercatheter
Comorbid risk factors: Comorbid risk factors: cardiac disease, chronic renal disease, diabetes, cardiac disease, chronic renal disease, diabetes, acute infection, immobilizationacute infection, immobilization
Surgery risk factorsSurgery risk factors: trauma, general surgery or any anesthesia: trauma, general surgery or any anesthesia
Medications: Medications: erythropoietinerythropoietin
Myeloma-related risk factors: Myeloma-related risk factors: diagnosis, hyperviscositydiagnosis, hyperviscosity
Myeloma therapy risk factors: Myeloma therapy risk factors: multiagent chemotherapy, doxorubicin, high-multiagent chemotherapy, doxorubicin, high-dose steroidsdose steroidsPatients with ≤ 1 VTE risk factor: Aspirin (81-325 mg daily)Patients with ≤ 1 VTE risk factor: Aspirin (81-325 mg daily)Patients with ≥ 2 VTE risk factors: LMWH (enoxaparin 40 mg/d) or full-dose Patients with ≥ 2 VTE risk factors: LMWH (enoxaparin 40 mg/d) or full-dose warfarin, although less existing supporting data for the latterwarfarin, although less existing supporting data for the latterPatients receiving thalidomide/lenalidomide concurrently with high-dose Patients receiving thalidomide/lenalidomide concurrently with high-dose dexamethasone or doxorubicin should receive LMWH thromboprophylaxis dexamethasone or doxorubicin should receive LMWH thromboprophylaxis Anticoagulant treatment can continue for 4 to 6 months or longer if Anticoagulant treatment can continue for 4 to 6 months or longer if additional risk factors are presentadditional risk factors are present

PHACS : Prophylaxis in High-risk PHACS : Prophylaxis in High-risk Ambulatory Cancer Patients StudyAmbulatory Cancer Patients Study
R
Dalteparin prophylaxis x 12 weeks with 4-weekly screening US and start/end CT chest
Observe x 12 weekswith 4-weekly screening US and start/end CT chest
R01 HL095109-01, 9/2008R01 HL095109-01, 9/2008
Patients deemed high-risk for VTEstarting chemotherapy

Ongoing Clinical TrialsOngoing Clinical Trials
Study (Agent)Study (Agent) Criteria for Criteria for inclusion*inclusion* NN EndpointsEndpoints
PHACS (dalteparin x 12 wks) -Risk score >=3-Risk score >=3 404404
Asymptomatic Asymptomatic and symptomatic and symptomatic VTEVTE
SAVE-ONCO (semuloparin up to 4 mos)
-Lung, bladder, GI, ovary-Lung, bladder, GI, ovary-Metastatic or locally -Metastatic or locally advancedadvanced
32003200 DVT, PE, VTE-DVT, PE, VTE-related deathrelated death
MicroTEC (enoxaparin x 6 mos)
-Lung, colon, pancreas -Lung, colon, pancreas -Metastatic or -Metastatic or unresectableunresectable-Elevated TF MPs-Elevated TF MPs
227227 VTEVTE
* All studies enroll patients initiating a new chemotherapy regimen

Treatment of VTE in Cancer: Treatment of VTE in Cancer: The CLOT StudyThe CLOT Study
Lee, A. Y.Y. et al. N Engl J Med 2003;349:146-153Lee, A. Y.Y. et al. N Engl J Med 2003;349:146-153

CLOT Study:CLOT Study:Reduction in Recurrent VTEReduction in Recurrent VTE
00
55
1010
1515
2020
2525
Days Post RandomizationDays Post Randomization
00 3030 6060 9090 120120 150150 180180 210210
Pro
bab
ility
of R
ecu
rre
nt V
TE
, %P
roba
bili
ty o
f Re
curr
en
t VT
E, %
Risk reduction = Risk reduction = 52%52%
pp-value = 0.0017-value = 0.0017
DalteparinDalteparin
OACOAC
Recurrent VTERecurrent VTE
Lee et.al. Lee et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146

Summary of NCCN Guidelines Summary of NCCN Guidelines UpdatesUpdates
Summary of Major Changes in the Summary of Major Changes in the 1.2009 Version of the NCCN Venous 1.2009 Version of the NCCN Venous Thromboembolic Disease GuidelinesThromboembolic Disease Guidelines

Changes in 2009 NCCN GuidelinesChanges in 2009 NCCN Guidelines
Stage 1 Immediate:Stage 1 Immediate:► ““Stage 1 Immediate: Concomitant with diagnosis or while Stage 1 Immediate: Concomitant with diagnosis or while
diagnosis and risk assessment (heparin phase)” changed to diagnosis and risk assessment (heparin phase)” changed to “Stage 1 Immediate: At diagnosis or during diagnostic “Stage 1 Immediate: At diagnosis or during diagnostic evaluation”evaluation”
► Low –molecular-weight-heparin: New footnote “6” was added Low –molecular-weight-heparin: New footnote “6” was added that states, that states, “Although each of the low molecular weight “Although each of the low molecular weight heparins (LMWH), have been studies in randomized control heparins (LMWH), have been studies in randomized control trials in cancer patients, dalteparin’s efficacy in this trials in cancer patients, dalteparin’s efficacy in this population is supported by the highest quality evidence and it population is supported by the highest quality evidence and it is the only LMWH approved by the FDA for this indicationis the only LMWH approved by the FDA for this indication.”.”
► Unfractionated heparin (IV): target aPTT range changed from Unfractionated heparin (IV): target aPTT range changed from “2.0-2.9 x control) to “2.0-2.5 x control…” (Also for VTE-H) in “2.0-2.9 x control) to “2.0-2.5 x control…” (Also for VTE-H) in these patients.these patients.

Changes in 2009 NCCN GuidelinesChanges in 2009 NCCN Guidelines
Stage 3 Chronic:Stage 3 Chronic:
► ““Third bullet: “Consider indefinite Third bullet: “Consider indefinite anticoagulation….” changed to “anticoagulation….” changed to “Recommend Recommend indefinite anticoagulation….”indefinite anticoagulation….”
► Fourth bullet: “For catheter associated Fourth bullet: “For catheter associated thrombosis, anticoagulate as long as catheter is in thrombosis, anticoagulate as long as catheter is in place and for at least 3 months after catheter place and for at least 3 months after catheter removal”.removal”.

Changes in 2009 NCCN GuidelinesChanges in 2009 NCCN Guidelines
► 66Although each of the low molecular weight Although each of the low molecular weight heparins (LMWH) have been studied in heparins (LMWH) have been studied in randomized controlled trials in cancer patients, randomized controlled trials in cancer patients, dalteparin’s efficacy in this population is dalteparin’s efficacy in this population is supported by the highest quality evidence and is supported by the highest quality evidence and is the only LMWH approved by the FDA for this the only LMWH approved by the FDA for this indication.indication.
Lee AYY, Levine MN, Baker RI, Bowden C, et al. Low-molecular-Lee AYY, Levine MN, Baker RI, Bowden C, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism on patients with cancer. New Eng J Med venous thromboembolism on patients with cancer. New Eng J Med 2003;349(2): 146-153.2003;349(2): 146-153.

(VTE-D): Therapeutic Anticoagulation (VTE-D): Therapeutic Anticoagulation Treatment for VTETreatment for VTE
► The NCCN panel recommends VTE thromboprophylaxis The NCCN panel recommends VTE thromboprophylaxis for all hospitalized patients with cancer who do not for all hospitalized patients with cancer who do not have contraindications to such therapy, and the panel have contraindications to such therapy, and the panel also emphasized that an increased level of clinical also emphasized that an increased level of clinical suspicion of VTE should be maintained for cancer suspicion of VTE should be maintained for cancer patients. patients. Following hospital discharge, it is Following hospital discharge, it is recommended that patients at high-risk of VTE (e.g. recommended that patients at high-risk of VTE (e.g. cancer surgery patients) continue to receive VTE cancer surgery patients) continue to receive VTE prophylaxis for up to 4 weeks post-operation.prophylaxis for up to 4 weeks post-operation. Careful Careful evaluation and follow-up of cancer patients in whom evaluation and follow-up of cancer patients in whom VTE is suspected and prompt treatment and follow-up VTE is suspected and prompt treatment and follow-up for patients diagnosed with VTE is recommended after for patients diagnosed with VTE is recommended after the cancer status of the patient is assessed and the the cancer status of the patient is assessed and the risks and benefits of treatment are considered. risks and benefits of treatment are considered.

Therapeutic Anticoagulation FailureTherapeutic Anticoagulation Failure
Therapeutic INR
Switch to heparin (LMWH preferred)
or fondaparinux
Increase warfarin dose and treat with
parenteral agent until INR target achieved or consider switching
to heparin (LMWH preferred) or fondaparinux
Patient on
warfarin
Check INR
Sub-therapeutic
INR

Therapeutic Anticoagulation FailureTherapeutic Anticoagulation Failure
Therapeutic aPTT
Increase dose of heparin or Switch to LMWH or Switch to fondaparinux and Consider placement of IVC filter and Consider HIT
Increase dose of heparin to reach therapeutic level
Patient on
heparin
Check aPTT levels
Sub-therapeutic
aPTT

ConclusionsConclusions
Cancer patients are clearly at increased Cancer patients are clearly at increased risk for VTE but risk is highly variablerisk for VTE but risk is highly variable
TF is an emerging candidate TF is an emerging candidate biomarker predictive of VTE and biomarker predictive of VTE and survivalsurvival
?generalizability to all cancers?generalizability to all cancers Lack of standardized assayLack of standardized assay
A recently validated risk model can A recently validated risk model can predict risk of VTE (and mortality) using predict risk of VTE (and mortality) using 5 simple clinical and laboratory 5 simple clinical and laboratory variablesvariables

ConclusionsConclusions
►Thromboprophylaxis is safe and effective in Thromboprophylaxis is safe and effective in certain high-risk settingscertain high-risk settings
►LMWH-base prophylaxis is guideline-based LMWH-base prophylaxis is guideline-based standard of carestandard of care● Hospitalized and surgical patientsHospitalized and surgical patients● Highly selected cancer outpatients (myeloma, ?Highly selected cancer outpatients (myeloma, ?
pancreas, ?? lung)pancreas, ?? lung)
►Ongoing studies are adopting novel Ongoing studies are adopting novel approaches to selecting patients for approaches to selecting patients for prophylaxisprophylaxis

Hematologic Complications of Hematologic Complications of ChemotherapyChemotherapy
Balancing Benefits and Risks of InterventionBalancing Benefits and Risks of Intervention
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application
Jeffrey Crawford, MDJeffrey Crawford, MDGeorge Barth Geller Professor for Research In CancerGeorge Barth Geller Professor for Research In Cancer
Chief of Division of Medical OncologyChief of Division of Medical OncologyDepartment of MedicineDepartment of Medicine
Duke University Medical CenterDuke University Medical CenterEditor-in-Chief, Supportive Care OncologyEditor-in-Chief, Supportive Care Oncology
Durham, North CarolinaDurham, North Carolina


APPRISE – APPRISE – AAssisting ssisting PProviders and Cancer roviders and Cancer PPatients atients with with RRisk isk IInformation for the nformation for the SSafe Use of afe Use of EESAsSAs
► Doctors will be required to register and Doctors will be required to register and undergo training on risks and benefits of undergo training on risks and benefits of ESAs in order to continue prescribing.ESAs in order to continue prescribing.
► As part of the program, patients will be As part of the program, patients will be given a medication guide that outlines given a medication guide that outlines the risks and benefits of ESAs.the risks and benefits of ESAs.
► Enrollment of providers begins March 24, Enrollment of providers begins March 24, 2010.2010.

Biological Characteristics of Biological Characteristics of Erythroid Stimulating Agents (ESAs)Erythroid Stimulating Agents (ESAs)
► Epoetin alfa Epoetin alfa – FDA approval for chemotherapy induced anemia – FDA approval for chemotherapy induced anemia (CIA) - 1993(CIA) - 1993
● In vivo half-life 8.5 h (IV) and 16-19 h (SC) in healthy In vivo half-life 8.5 h (IV) and 16-19 h (SC) in healthy subjectssubjects11
► Darbepoetin alfa Darbepoetin alfa – FDA approval for CIA -2002 – FDA approval for CIA -2002 ● Higher proportion of sialic acid-containing carbohydrate, Higher proportion of sialic acid-containing carbohydrate,
resulting inresulting in a 3-fold longer half-life and a 4-fold weaker a 3-fold longer half-life and a 4-fold weaker binding affinity for the EPO receptorbinding affinity for the EPO receptor22
► Epoetin beta Epoetin beta – Approved for CIA in Europe – Approved for CIA in Europe ● Less sialated than epoetin alfa and a slightly longer half-Less sialated than epoetin alfa and a slightly longer half-
life when given SC (~24 h in healthy subjects)life when given SC (~24 h in healthy subjects)33 ► Despite pharmacodynamic differences, efficacy/safety of ESAs in Despite pharmacodynamic differences, efficacy/safety of ESAs in
CIA patients appear similarCIA patients appear similar
11Procrit prescribing information 2002; Procrit prescribing information 2002; 22Egrie JC et al. Egrie JC et al. Oncology (Huntingt)Oncology (Huntingt) 2002; 2002; 33Halstenson CE Halstenson CE et al. et al. Clin Pharmacol TherClin Pharmacol Ther 1991 1991

Rescue by Transfusion vs an Improvement/ Rescue by Transfusion vs an Improvement/ Maintenance Strategy with ESAs: a Conceptual Maintenance Strategy with ESAs: a Conceptual
ModelModel
ODAC Meeting, 5/20/07ODAC Meeting, 5/20/07
Weeks of Chemotherapy
Hb
Lev
el
Transfusion Rescue Strategy
Individualized patient trigger
ESA improvement/ maintenance strategy
Asymptomatic Zone

Modeled Probability of Receiving a Blood Modeled Probability of Receiving a Blood Transfusion as a Function of Baseline HbTransfusion as a Function of Baseline Hb
4 Phase 3, placebo-controlled CIA Studies, n=1641 (980297, 20000161, 20010145, 20030232)4 Phase 3, placebo-controlled CIA Studies, n=1641 (980297, 20000161, 20010145, 20030232)
5566778899101011111212131314141515
Baseline Hb (g/dL)Baseline Hb (g/dL)
00
0.10.1
0.20.2
0.30.3
0.40.4
0.50.5
0.60.6
0.70.7
0.80.8
0.90.9
11
Pre
dict
ed P
roba
bilit
y T
FN
Pre
dict
ed P
roba
bilit
y T
FN
PlaceboPlaceboDADA
OR=0.41, 95%CI (0.33, 0.51)OR=0.41, 95%CI (0.33, 0.51)
ODAC Meeting, 5/20/07ODAC Meeting, 5/20/07

Summary of HRQoL Data from Systematic Summary of HRQoL Data from Systematic Review of Randomized Placebo-controlled TrialsReview of Randomized Placebo-controlled Trials
QOL ScaleQOL Scale(ESA vs control)(ESA vs control)
MeanMeanChangeChange P-valueP-value
FACT-F (5 studies, 1418 max pts) 3.6 vs -0.83.6 vs -0.8 <0.001<0.001
LASA (4 studies, 1076 max pts) 4.8 vs -3.64.8 vs -3.6 <0.001<0.001
Favors ControlFavors Control Favors EPO/DARBFavors EPO/DARB
SourceSourceDifference in Standardized Difference in Standardized
Mean FACT-F Values Mean FACT-F Values (95% CI)(95% CI)
PPDifference in Standardized MeansDifference in Standardized Means
(95% CI)(95% CI)
0.000.00 0.500.50-0.50-0.50-1.00-1.00 1.001.00
LittlewoodLittlewood 0.23 (-0.02 to 0.48)0.23 (-0.02 to 0.48) 0.0760.076
BoogaertsBoogaerts 0.11 (-0.16 to 0.38)0.11 (-0.16 to 0.38) 0.4280.428
IconomouIconomou 0.44 (0.07 to 0.82)0.44 (0.07 to 0.82) 0.0210.021
WitzigWitzig 0.11 (-0.12 to 0.33)0.11 (-0.12 to 0.33) 0.3600.360
Random-effects modelRandom-effects model 0.22 (0.10 to 0.36)0.22 (0.10 to 0.36) 0.0010.001Fixed-effects modelFixed-effects model 0.22 (0.10 to 0.34)0.22 (0.10 to 0.34) 0.0000.000
SavonijeSavonije 0.42 (0.12 to 0.71)0.42 (0.12 to 0.71) 0.0050.005
11Cella D et al, J Pain Symptom Manage. 2002;24(6):547-561Cella D et al, J Pain Symptom Manage. 2002;24(6):547-561Ross, S et al. Clin Ther. 2006; 28(6): 1-31Ross, S et al. Clin Ther. 2006; 28(6): 1-31
3-point difference in FACT-F 3-point difference in FACT-F defined as clinically importantdefined as clinically important11

Higher Hb is Associated Higher Hb is Associated with Higher HRQoLwith Higher HRQoL
Crawford J, et al. Crawford J, et al. CancerCancer. 2002;95(4):888-895. . 2002;95(4):888-895.
4545
5050
5555
6060
6565
77 88 99 1010 1111 1212 1313 1414
Hb level (g/dL)Hb level (g/dL)
LAS
A O
vera
ll Q
OL
Sco
reLA
SA
Ove
rall
QO
L S
core
00
1 study (n=1580)1 study (n=1580)

Across all studies, recommendation for transfusion was Hb <8 g/dL Across all studies, recommendation for transfusion was Hb <8 g/dL (or signs & symptoms of anemia)(or signs & symptoms of anemia)
9.2%
When and Why do Physicians Transfuse? When and Why do Physicians Transfuse? Data from 5 Phase 3 CIA Darbepoetin alfa StudiesData from 5 Phase 3 CIA Darbepoetin alfa Studies
Prophylactic (1.2%)Prophylactic (1.2%)Medically Indicated (4.4%)Medically Indicated (4.4%)
8 – 10 g/dL8 – 10 g/dL54.3% 54.3%
<8 g/dL 35.9%
Reasons Given for Transfusion Reasons Given for Transfusion (n=2227 CRF responses ) (n=2227 CRF responses )
10-12 g/dL10-12 g/dL ≥≥12 g/dL (0.7%)12 g/dL (0.7%)
Hb at Time of TransfusionHb at Time of Transfusion(n=2185 transfusion episodes)(n=2185 transfusion episodes)
Hb Trigger34.7%Therapeutic
46.0%
Other13.7%
(n=2286)(n=2286)

Common Risks of Blood Product InfusionsCommon Risks of Blood Product Infusions
Upile, T, et al. Clinical Advances in Hematology & Oncology Volume 7, Issue 10 October 2009Upile, T, et al. Clinical Advances in Hematology & Oncology Volume 7, Issue 10 October 2009
Some of the Risks of TransfusionSome of the Risks of Transfusion
► Febrile nonhemolyticFebrile nonhemolytic► Acute transfusion reaction from Acute transfusion reaction from
mismatchmismatch► Acute hemolyticAcute hemolytic► Delayed hemolyticDelayed hemolytic► AllergicAllergic AnaphylacticAnaphylactic Human leukocyte antigen Human leukocyte antigen
sensitizationsensitization Red blood cell allosensitizationRed blood cell allosensitization Graft-versus-host diseaseGraft-versus-host disease
► Clotting disturbancesClotting disturbances► Electrolyte disturbancesElectrolyte disturbances► Volume overload in the young Volume overload in the young
and elderlyand elderly► Transfusion-related acute lung Transfusion-related acute lung
injuryinjury► Peri-operative infection Peri-operative infection
susceptibilitysusceptibility► Blood borne infectoons – viral Blood borne infectoons – viral
(HIV, hepatitis), bacterial, prions, (HIV, hepatitis), bacterial, prions, parasites (malaria)parasites (malaria)
► Increased tumor recurrence from Increased tumor recurrence from peri-operative transfusionperi-operative transfusion
► Worsensed cancer prognosis from Worsensed cancer prognosis from peri-operative transfusionperi-operative transfusion

Background: Background: Erythropoiesis-stimulating agents Erythropoiesis-stimulating agents (erythropoietin and darbepoietin) have been approved to (erythropoietin and darbepoietin) have been approved to reduce the number of blood transfusions required during reduce the number of blood transfusions required during chemotherapy; however, concerns about the risks of venous chemotherapy; however, concerns about the risks of venous thromboembolism and mortality exist.thromboembolism and mortality exist.
Methods: Methods: Study of patients aged 65 years or older in the Study of patients aged 65 years or older in the Surveillance, Epidemiology and End Results-Medicare Surveillance, Epidemiology and End Results-Medicare database; with colon, non-small cell lung or breast cancer or database; with colon, non-small cell lung or breast cancer or with diffuse large B-cell lymphoma from 1991 through 2001; with diffuse large B-cell lymphoma from 1991 through 2001; and who received chemotherapy. The main outcome and who received chemotherapy. The main outcome measures were claims for use of an erythropoiesis-measures were claims for use of an erythropoiesis-stimulating agent, blood transfusion, venous stimulating agent, blood transfusion, venous thromboembolism (i.e., deep vein thrombosis or pulmonary thromboembolism (i.e., deep vein thrombosis or pulmonary embolism), and overall survival.embolism), and overall survival.
Patterns of Use and Risks Associated with Patterns of Use and Risks Associated with Erythropoiesis-Stimulating Agents Among Medicare Erythropoiesis-Stimulating Agents Among Medicare
Patients with CancerPatients with Cancer
Hershman, D. JNCI 101 (23):1-9, 2009Hershman, D. JNCI 101 (23):1-9, 2009

Hershman, D. JNCI 101 (23):1-9, 2009Hershman, D. JNCI 101 (23):1-9, 2009
ResultsResults
►56,210 patients received chemotherapy56,210 patients received chemotherapy
►15,346 (27%) received an ESA15,346 (27%) received an ESA
►22% received transfusions22% received transfusions
►14.3% of ESA patients had VTE14.3% of ESA patients had VTE
►9.8% of nonESA patients had VTE9.8% of nonESA patients had VTE
ESA – erythroid stimulating agentESA – erythroid stimulating agent
VTE – venous thromboembolismVTE – venous thromboembolism
Patterns of Use and Risks of ESAsPatterns of Use and Risks of ESAs

Hershman, D. JNCI 101 (23):1-9, 2009Hershman, D. JNCI 101 (23):1-9, 2009
Trends in ESA and Transfusion Trends in ESA and Transfusion Use in All PatientsUse in All Patients
% of Patients Receiving ESA% of Patients Receiving ESA% of Patients Receiving Blood Transfusion% of Patients Receiving Blood Transfusion
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 20021991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002
7070
6060
5050
4040
3030
2020
1010
00
% o
f Pati
ents
% o
f Pati
ents

Overall SurvivalOverall Survival
Hershman, D. JNCI 101 (23):1-9, 2009Hershman, D. JNCI 101 (23):1-9, 2009
Pro
port
ion a
live
Pro
port
ion a
live
Time to death (years)Time to death (years)
EAS useEAS use
ESA non-useESA non-use
0 2 0 2 4 4 6 6 8 8 10 10
1.001.00
0.750.75
0.500.50
0.250.25

Khorana, Francis, Blumberg, Culakova, Refaai, Lyman.Khorana, Francis, Blumberg, Culakova, Refaai, Lyman.Arch Intern Med 2008;168:2377-2381.Arch Intern Med 2008;168:2377-2381.
Blood Transfusions, Thrombosis and Mortality Blood Transfusions, Thrombosis and Mortality in Hospitalized Patients with Cancerin Hospitalized Patients with Cancer
Population Population 504,208 pts 504,208 pts with cancer with cancer admitted admitted between between 1995-2003 at 1995-2003 at 60 medical 60 medical centerscenters

Blood Transfusions, Thrombosis and Mortality in Hospitalized Patients with CancerBlood Transfusions, Thrombosis and Mortality in Hospitalized Patients with Cancer
Khorana, Francis, Blumberg, Culakova, Refaai, Lyman.Khorana, Francis, Blumberg, Culakova, Refaai, Lyman.Arch Intern Med 2008;168:2377-2381.Arch Intern Med 2008;168:2377-2381.

Feinberg, B. Community Oncology, June 2009, 257-261Feinberg, B. Community Oncology, June 2009, 257-261
Community Oncology ESA Community Oncology ESA ExperienceExperience
TimepointTimepoint
Pre-NCD cohortPre-NCD cohort Post NCD cohortPost NCD cohort
P ValueP ValueNumberNumber Hb level Hb level
(SD)(SD) NumberNumber Hb level Hb level (SD)(SD)
Baseline 225225 10.7 (0.9)10.7 (0.9) 144144 9.7 (0.8)9.7 (0.8) <0.0001<0.0001
Week 4 206206 11.0 (1.2)11.0 (1.2) 138138 10.2 (1.2)10.2 (1.2) <0.0001<0.0001
Week 8 138138 11.2 (1.3)11.2 (1.3) 102102 10.3 (1.1)10.3 (1.1) <0.0001<0.0001
Mean hemoglobin levels at different time pointsMean hemoglobin levels at different time points

Feinberg, B. Community Oncology, June 2009, 257-261Feinberg, B. Community Oncology, June 2009, 257-261
Community Oncology ESA Community Oncology ESA ExperienceExperience

Focused ESA Safety DataFocused ESA Safety Data
ENHANCE ENHANCE 20032003‡‡
DAHANCA DAHANCA 12/0612/06††
EPO-CAN-20 EPO-CAN-20 20072007‡‡
BEST BEST 20052005‡‡
20000161 20000161 4/05, 4/074/05, 4/07††
20010103 20010103 1/071/07††
GOG-191 GOG-191 20072007† †
PREPARE PREPARE 11/0711/07† †
Survival, Tumor Progression, TVESurvival, Tumor Progression, TVE**
*8 trials selected by FDA for label inclusion out of 57 total, ‡ publication date, † = date data reported to FDA
Lancet 2003;632:1255-60. J Natl Cancer Inst 2006:98:708-14. Lancet 2003;632:1255-60. J Natl Cancer Inst 2006:98:708-14. J Clin Oncol J Clin Oncol 2005;23:5960-72. J2005;23:5960-72. J Natl Cancer Inst 2005;97:489-98. Natl Cancer Inst 2005;97:489-98. J Clin Oncol 2007;25:1027-J Clin Oncol 2007;25:1027-32. http://www.fda.gov (accessed 3/20/08). JAMA 2008;299:914-2432. http://www.fda.gov (accessed 3/20/08). JAMA 2008;299:914-24

EPO CAN-20 EPO CAN-20
► 300 patients 300 patients not on active treatmentnot on active treatment► Primary endpoint: QOL at 12 weeksPrimary endpoint: QOL at 12 weeks► Target hemoglobin Target hemoglobin 12-14 g/dL12-14 g/dL► Unplanned safety analysis Unplanned safety analysis 70 patients70 patients► Result : Survival decrement Result : Survival decrement HR 1.84 HR 1.84

Wright et alOverall Survival
Wright JR., et al. J Clin Onc. 2007:25;1027-1032
Post-random Assignment (weeks)
0 12 16 20 24 28 32 36 40 44 48 52 56 604 8
0.10.2
0.30.4
0.50.60.70.80.91.0
Log-rank P = 0.04
Placebo
Epoetin alfa
Su
rviv
al P
rob
abil
ity
No. at risk:Epoetin alfa 33 28 20 15 13 12 12 9 5 3 1 1 1 1 1 1Placebo 37 34 30 26 22 17 15 15 12 11 9 7 6 5 5 3
Results of unplanned interim analysis (n = 70)
0.041.84Overall Survival
p valueHR
Eprex® is a registered trademark of Ortho Biotech

Wright J et al. JCO 2007 Mar 20;25(9):1027-32. Epub 2007 Feb 20Wright J et al. JCO 2007 Mar 20;25(9):1027-32. Epub 2007 Feb 20
EPO-CAN-20 (Advanced NSCLC)EPO-CAN-20 (Advanced NSCLC)
Cause of DeathCause of Death
PlaceboPlacebo(34 deaths)(34 deaths)
Epoetin Alfa Epoetin Alfa (32 deaths)(32 deaths)
No. of No. of PatientsPatients %%
No. of No. of PatientsPatients %%
Progressive lung cancer 3131 91.291.2 2828 87.587.5
Pneumonia 11 2.92.9 11 3.13.1
Myocardial infarction 11 2.92.9 11
Renal failure 11 2.92.9 --
Hyponatremia -- 11 3.13.1
Bowel perforation -- 11 3.13.1
Unknown cause -- 11 3.13.1
Reported Causes of DeathReported Causes of Death

Meta-analysis: Lung Cancer TrialsMeta-analysis: Lung Cancer Trials
Study NameStudy Name
No. of No. of Deaths/TotalDeaths/Total Odds Odds
RatioRatio
95% CI95% CI
ESAESA ControlControl Lower Lower LimitLimit
Upper Upper LimitLimit
AoC NSCLC
Wright 2007 (EPO-CAN-20) 32/3332/33 34/3734/37 2.822.82 0.280.28 28.5628.56
CIA NSCLC
EPO-GER-22 146/195146/195 159/190159/190 0.580.58 0.350.35 0.960.96
Vansteenkiste 2002 NSCLC 72/10872/108 82/11482/114 0.780.78 0.440.44 1.381.38
Milroy 2003 (INT-49) 136/214136/214 126/210126/210 1.161.16 0.790.79 1.721.72
Random Effects Model: NSCLCRandom Effects Model: NSCLC 0.830.83 0.540.54 1.271.27 CIA SCLC
Vansteenkiste 2002 SCLC 28/4728/47 37/4537/45 0.320.32 0.120.12 0.830.83
Pirker 2007 (AMG 20010145) 241/298241/298 251/298251/298 0.790.79 0.520.52 1.211.21
EPO-CAN-15 28/5228/52 29/5229/52 0.930.93 0.430.43 2.002.00
Thatcher 1999 7/867/86 3/443/44 1.211.21 0.300.30 4.934.93
Grote 2005 (N93-004) 100/109100/109 101/115101/115 1.541.54 0.640.64 3.723.72
Random Effects Model: SCLCRandom Effects Model: SCLC 0.830.83 0.530.53 1.281.28
0.1 0.2 0.5 1 2 5 10Favors ESA Favors Control
ODAC 2008 SupplementODAC 2008 Supplement

Cochrane Meta Analysis – Cochrane Meta Analysis – Summary of ResultsSummary of Results
Study Study populationpopulation NN
Hazard Ratio Hazard Ratio (95% CI)(95% CI) P-valueP-value
On-study mortality1
All cancer pts 13, 93313, 933 1.17 (1.06, 1.17 (1.06, 1.30)1.30) 0.0020.002
Chemotherapy trials 10, 44110, 441 1.10 (0.98, 1.10 (0.98,
1.24)1.24) 0.120.12
Overall survival2
All cancer pts 13, 93313, 933 1.06 (1.00, 1.06 (1.00, 1.12)1.12) 0.050.05
Chemotherapy trials 10, 44110, 441 1.04 (0.97, 1.04 (0.97,
1.11)1.11) 0.260.26
1deaths during active study phase; 2 deaths during longest follow-up availableBohlius et al, (Lancet 2009)Bohlius et al, (Lancet 2009)

Meta Analysis of Disease ProgressionMeta Analysis of Disease Progression
Glaspy, Crawford, Vansteenkiste, Henry, Rao, Bowers, Berlin, Tomita, Bridges, Ludwig British Journal of Cancer
102, 301-315 (5 January 2010)



A Randomized, Double-Blind, Placebo-A Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Long-Controlled Study to Evaluate the Long-
Term Safety and Efficacy of Darbepoetin Term Safety and Efficacy of Darbepoetin Alfa Administered at 500 µg Once-Every-Alfa Administered at 500 µg Once-Every-
3-Weeks in Anemic Subjects With 3-Weeks in Anemic Subjects With Advanced Stage Non-Small Cell Lung Advanced Stage Non-Small Cell Lung
Cancer Receiving Multi-Cycle Cancer Receiving Multi-Cycle Chemotherapy Chemotherapy
Clinical Trials Identifier Clinical Trials Identifier NCT00858364NCT00858364

Clinical Trials Identifier Clinical Trials Identifier NCT00858364NCT00858364
► SponsorSponsorAmgen Inc.Amgen Inc.
► General DesignGeneral DesignRandomized, double-blind, placebo-controlled Phase 3, non-Randomized, double-blind, placebo-controlled Phase 3, non-inferiority study intended to evaluate the long term safety inferiority study intended to evaluate the long term safety and efficacy of darbepoetin alfaand efficacy of darbepoetin alfa
► InterventionInterventionAranesp or placebo administered Q3W (2:1 randomization)Aranesp or placebo administered Q3W (2:1 randomization)
► Study populationStudy populationSubjects with advanced stage non-small cell lung cancer and Subjects with advanced stage non-small cell lung cancer and anemia (Hb <=11 g/dL) receiving or about to receive first-line anemia (Hb <=11 g/dL) receiving or about to receive first-line chemotherapychemotherapy
► Sample sizeSample size3000 subjects3000 subjects

Clinical Trials Identifier Clinical Trials Identifier NCT00858364NCT00858364
► Primary outcome measurePrimary outcome measure● Overall Survival (OS)Overall Survival (OS)
► Secondary outcome measuresSecondary outcome measures● Progression-free survival (PFS)Progression-free survival (PFS)● Objective tumor response Objective tumor response ● Incidence of at least 1 RBC transfusion or hemoglobin less Incidence of at least 1 RBC transfusion or hemoglobin less
than or equal to 8.0 g/dL from week 5 (day 29) to end of than or equal to 8.0 g/dL from week 5 (day 29) to end of efficacy treatment period efficacy treatment period
● Incidence of at least 1 RBC transfusion or hemoglobin less Incidence of at least 1 RBC transfusion or hemoglobin less than or equal to 8.0 g/dL from study day 1 to end of treatment than or equal to 8.0 g/dL from study day 1 to end of treatment periodperiod
● Incidence of neutralizing antibody formation to darbepoetin Incidence of neutralizing antibody formation to darbepoetin alfaalfa
● Change in hemoglobin from baseline to end of efficacy Change in hemoglobin from baseline to end of efficacy treatment periodtreatment period
● Incidence of adverse events (AEs) such as thrombovascular Incidence of adverse events (AEs) such as thrombovascular events (TVE), venous thromboembolic events (VTE), and AEs events (TVE), venous thromboembolic events (VTE), and AEs associated with RBC transfusionsassociated with RBC transfusions

Study Status as of June 2010Study Status as of June 2010
► Study start date: June 2009Study start date: June 2009
► Currently recruiting subjects in Currently recruiting subjects in North America, Europe, Asia and North America, Europe, Asia and Latin AmericaLatin America● Study sites planned for a total of Study sites planned for a total of
approximately 400 sites in over approximately 400 sites in over 30 countries30 countries

Chemotherapy-induced Neutropenia Chemotherapy-induced Neutropenia and Its Complicationsand Its Complications
Kuderer NM et al. Kuderer NM et al. CancerCancer 2006;106:2258–2266 2006;106:2258–2266 Chirivella I et al. Chirivella I et al. J Clin OncolJ Clin Oncol 2006;24;abstract 668 2006;24;abstract 668 Bosly A et al. Bosly A et al. Ann HematolAnn Hematol 2008;87:277-283 2008;87:277-283
Myelosuppressive chemotherapy
Febrile neutropenia (FN) Chemotherapy dose delays and dose reductions
Decreased relative dose intensity (RDI)
Complicated life-threatening infection and prolonged hospitalization
Neutropenia
Reduced survival

Risk of FN Increases with Duration of Risk of FN Increases with Duration of
Severe Neutropenia*Severe Neutropenia*
Adapted from Blackwell S, Crawford J. In: Morstyn G, Dexter TM. Filgrastim; (r-metHuG-CSF) in Clinical Practice. New York: Marcel Dekker; 1994 p 103–116Crawford J et al. N Engl J Med 1991;325:164–170
Days of severe neutropeniaDays of severe neutropenia
Pre
dict
ed p
roba
bilit
y of
FN
(%
)P
redi
cted
pro
babi
lity
of F
N (
%)
(tem
pera
ture
>38
.2(t
empe
ratu
re >
38.2
◦◦ C a
nd
C a
nd
AN
C <
0.5
x 10
AN
C <
0.5
x 10
99 /L)
/L)
100
80
60
40
20
00 1 2 3 4 5 6 7 8 9
*ANC <0.5 x 109/L

Most Initial FN Events Occur During Most Initial FN Events Occur During the First Cycle of Chemotherapythe First Cycle of Chemotherapy
Adapted from Crawford J et al. Adapted from Crawford J et al. JNCCN JNCCN 2008;6:109–1182008;6:109–118
Proportion of first FN events in cycle 1 by cancer type
Eve
nts
in c
ycle
1 (
%)
Eve
nts
in c
ycle
1 (
%)
• FN events documented in 287/2692 (10.7%) of adult cancer patients during the 1st three cycles of chemotherapy NSCLC – non-small cell lung cancer;
SCLC – small cell lung cancer; NHL - non-Hodgkin’s lymphoma; HD – Hodgkin’s disease

Death as a Result of FN HospitalizationDeath as a Result of FN Hospitalization
Kuderer NM et al. Kuderer NM et al. Cancer Cancer 2006;106:2258–22662006;106:2258–2266
Overall No major One major >one major (n=41,779) comorbidity comorbidity comorbidity
(n=21,386) (n=12,398) (n=7,995)
25
20
15
10
5
0
9.5
2.6
10.3
21.4Mortality following hospital admission of adult cancer patients with FN*
Inpa
tient
mor
talit
y (p
erce
nt p
atie
nts
adm
itted
for
FN
)
*Data based on a single admission per patient

Clinical Consequences of Clinical Consequences of Neutropenia and Febrile NeutropeniaNeutropenia and Febrile Neutropenia
• Reduced RDI resulted in lower Reduced RDI resulted in lower OS in patients with DLBCL receiving OS in patients with DLBCL receiving CHOP-21 chemotherapyCHOP-21 chemotherapy22
• Reduced RDI resulted in lower OS in Reduced RDI resulted in lower OS in ESBC receiving anthracycline-ESBC receiving anthracycline-containing chemotherapycontaining chemotherapy11
Est
ima
ted
Su
rviv
al
Est
ima
ted
Su
rviv
al
0 1 2 3 4 5 6 7 8
Years Post ChemotherapyYears Post Chemotherapy
0.0
0.2
0.4
0.6
0.8
1.0
≤85%
86–≤90%
>90%
ARDI
OS, overall survival; ARDI, average relative dose intensity
Suboptimal chemotherapy reduces survivalSuboptimal chemotherapy reduces survival
1 Chirivella I, et al. Breast Cancer Res Treat 2009;114(3):479-4842 Bosly A, et al. Ann Hematol 2008; 87:277–283
Disease-Free Survival (years)Disease-Free Survival (years)
Cum
Pro
port
ion
Sur
viva
lC
um P
ropo
rtio
n S
urvi
val
RDI
< 85%
85%
< 85%, censored
85%, censored
1.0
0.8
0.6
0.4
0.2
0.00 2 4 6 8 10
+ +++
+
+
+ +
+
+

Myelosuppression Predicts for Survival Benefit of Myelosuppression Predicts for Survival Benefit of Adjuvant Chemotherapy in Breast Cancer PatientsAdjuvant Chemotherapy in Breast Cancer Patients
Mayers C, Tannock IF. Cancer 2001;91:2253Mayers C, Tannock IF. Cancer 2001;91:2253Lyman G. JNCCN 2009;7:99-108Lyman G. JNCCN 2009;7:99-108

Analysis of 4626 Hodgkin’s Lymphoma patients on Analysis of 4626 Hodgkin’s Lymphoma patients on German HDSG Trials 1988-1998German HDSG Trials 1988-1998
Klimm B. J Clin Oncol 2005;23:8003-8011
Hypothesis: Hypothesis: The better outcome of female HL patients is The better outcome of female HL patients is due to greater systemic chemotherapy exposure.due to greater systemic chemotherapy exposure.
ResultsResults FemaleFemale MaleMale P valueP value
G3/4 leukopenia 69.9069.90 52.2052.20 p<0.0001p<0.0001
FFTF at 66 months 81%81% 74%74%
Neutropenia as a Pharmacodynamic Neutropenia as a Pharmacodynamic Endpoint of Clinical BenefitEndpoint of Clinical Benefit

No neutropeniaMild neutropeniaSevere neutropenia
No neutropenia 208 150 102 68 43 29 20 13 10Mild neutropenia
138 98 74 54 38 33 21 13 11
Severe neutropenia
90 69 50 28 21 14 14 8 4
104
0.8
0.6
0.4
0.2
0917865523926130
1.0
Time From Landmark Day (Weeks)
Pro
babili
ty o
f Surv
ival
Patients at Risk
Log-rank P=0.0118(stratified by treatment)
Overall Survival by Grade of Chemotherapy-Overall Survival by Grade of Chemotherapy-Induced Neutropenia for Advanced NSCLC Induced Neutropenia for Advanced NSCLC
PatientsPatients
Di Maio M et al. Lancet Oncol 2005;6:669

Strategies For Management of Strategies For Management of Chemotherapy-Induced NeutropeniaChemotherapy-Induced Neutropenia
► PreventionPrevention● Chemotherapy Dose reduction/delayChemotherapy Dose reduction/delay● Myeloid growth factorsMyeloid growth factors
• G-CSF (filgrastim, lenograstim)G-CSF (filgrastim, lenograstim)• GM-CSF (sargramostim, molgramostim)GM-CSF (sargramostim, molgramostim)• PegfilgrastimPegfilgrastim
- Antibiotics- Antibiotics
► TreatmentTreatment● Observation if afebrileObservation if afebrile● AntibioticsAntibiotics● Myeloid growth factors (limited benefit)Myeloid growth factors (limited benefit)

Meta-Analysis: Antibiotic Prophylaxis Meta-Analysis: Antibiotic Prophylaxis Reduces Mortality in Neutropenic PatientsReduces Mortality in Neutropenic Patients
► 95 randomized controlled trials, 1973-2004 95 randomized controlled trials, 1973-2004 (n=9283)(n=9283)
► 79 studies were on inpatients with 79 studies were on inpatients with hematologic malignancies and/or PSCThematologic malignancies and/or PSCT
► 52 trials involved quinolone prophylaxis52 trials involved quinolone prophylaxis► 7 trials included CSFs7 trials included CSFs
Gafter-Gvili, A. Ann Intern Med. 2005:142(12):979-995Gafter-Gvili, A. Ann Intern Med. 2005:142(12):979-995

Meta-Analysis: Antibiotic Prophylaxis Meta-Analysis: Antibiotic Prophylaxis Reduces Mortality in Neutropenic PatientsReduces Mortality in Neutropenic Patients
Results of Prophylaxis with FluoroquinolonesResults of Prophylaxis with Fluoroquinolones
OutcomeOutcome Relative Risk (CI)Relative Risk (CI)
FeverFever .67 (.56-.81).67 (.56-.81)
Documented InfectionDocumented Infection .50 (.35-.70).50 (.35-.70)
Infection Related DeathInfection Related Death .38 (.21-.69).38 (.21-.69)
All cause mortalityAll cause mortality .52 (.35-.77).52 (.35-.77)
Adverse EventsAdverse Events 1.30 (.61-2.76)1.30 (.61-2.76)
Development of resistant bacteriaDevelopment of resistant bacteria 1.69 (.73-3.92)1.69 (.73-3.92)
Gafter-Gvili, A. Ann Intern Med. 2005:142(12):979-995Gafter-Gvili, A. Ann Intern Med. 2005:142(12):979-995

Meta-Analysis: Antibiotic Prophylaxis Meta-Analysis: Antibiotic Prophylaxis Reduces Mortality in Neutropenic PatientsReduces Mortality in Neutropenic Patients
► Insufficient number of outpatient solid Insufficient number of outpatient solid tumor/chemotherapy patients to be applicabletumor/chemotherapy patients to be applicable
► Not recommended by IDSA guidelines Not recommended by IDSA guidelines because of concerns regarding antibiotic because of concerns regarding antibiotic resistanceresistance
► Routine application limited to high risk Routine application limited to high risk inpatients with hematologic inpatients with hematologic malignancies/stem cell transplantsmalignancies/stem cell transplants
Limitations of Prophylactic AntibioticsLimitations of Prophylactic Antibiotics
Gafter-Gvili, A. Ann Intern Med. 2005:142(12):979-995Gafter-Gvili, A. Ann Intern Med. 2005:142(12):979-995

Role of Prophylactic Antibiotics in the Role of Prophylactic Antibiotics in the Prevention of Infection after ChemotherapyPrevention of Infection after Chemotherapy
SIGNIFICANT TrialSIGNIFICANT Trial
►Solid tumor/lymphoma patients (n-1565) Solid tumor/lymphoma patients (n-1565) receiving standard dose multicycle receiving standard dose multicycle chemotherapychemotherapy
►Randomized to levofloxacin 500 mg qd x 7 day Randomized to levofloxacin 500 mg qd x 7 day vs placebovs placebo
►Primary endpoint – reduction in febrile episodes Primary endpoint – reduction in febrile episodes attributed to infectionattributed to infection
SIGNIFICANT Trial. Cullen, et al. NEJM 2005; 353:988-998SIGNIFICANT Trial. Cullen, et al. NEJM 2005; 353:988-998

Role of Prophylactic Antibiotics in the Role of Prophylactic Antibiotics in the Prevention of Infection after Prevention of Infection after
ChemotherapyChemotherapy
OutcomeOutcome LevofloxaciLevofloxacinn
PlaceboPlaceboRR ReductionRR Reduction(95% CI)(95% CI)
Number Number Needed to Needed to Treat (CI)Treat (CI)
In first cycle Febrile episode 3.53.5 7.97.9 56 (32-72)56 (32-72) 23 (15-46)23 (15-46) Probable infection 1414 1919 28 (10-43)28 (10-43) 19 (11-58)19 (11-58) Hospitalization 6.76.7 1010 36 (10-54)36 (10-54) 28 (16-109)28 (16-109) In any Cycle Febrile episode 1111 1515 29 (8.1-45)29 (8.1-45) 23 (13-91)23 (13-91) Probable infection 3434 4141 18 (6.3-27)18 (6.3-27) 14 (9-41014 (9-410 Hospitalization 1616 2222 27 (9.9-410)27 (9.9-410) 18 (11-52)18 (11-52) Severe Infection or Death
11 22 50 (-14 to 78)50 (-14 to 78) Not significantNot significant
SIGNIFICANT Trial
Values are percentages unless otherwise specified.
Moon, S. et al. Supportive Cancer Therapy, 2006 3(4):207-13Moon, S. et al. Supportive Cancer Therapy, 2006 3(4):207-13

Primary Prophylaxis with MGFs Primary Prophylaxis with MGFs Reduces Febrile NeutropeniaReduces Febrile Neutropenia
RR = 0.538RR = 0.53895% CI (0.430-0.673)95% CI (0.430-0.673)
46% reduction 46% reduction in in riskrisk of febrile of febrile neutropenia with neutropenia with primary prophylaxisprimary prophylaxis
Kuderer NM et al. Kuderer NM et al. J Clin Oncol. J Clin Oncol. 2007;25:3158-31672007;25:3158-3167

Primary Prophylaxis with MGFs Primary Prophylaxis with MGFs Reduces Infection-related MortalityReduces Infection-related Mortality
RR = 0.552RR = 0.55295% CI (0.338-0.902)95% CI (0.338-0.902)
45% reduction 45% reduction in in risk of risk of infection-infection-related mortality related mortality with primary with primary prophylaxisprophylaxis
Kuderer NM et al. Kuderer NM et al. J Clin Oncol. J Clin Oncol. 2007;25:3158-31672007;25:3158-3167

Primary Prophylaxis with MGFs Primary Prophylaxis with MGFs Reduces Early MortalityReduces Early Mortality
RR = 0.599RR = 0.59995% CI (0.4330.830)95% CI (0.4330.830)
40% reduction 40% reduction in in risk of early risk of early mortality with mortality with primary prophylaxisprimary prophylaxis
Kuderer NM et al. Kuderer NM et al. J Clin Oncol. J Clin Oncol. 2007;25:3158-31672007;25:3158-3167

What impact does pegfilgrastim have on early, all-What impact does pegfilgrastim have on early, all-cause mortality in patients receiving cause mortality in patients receiving
chemotherapy?chemotherapy?
DesignDesign
Inclusion Inclusion criteriacriteria
Patient Patient populationpopulation
EndpointsEndpoints Time to febrile neutropenia, progression-free and Time to febrile neutropenia, progression-free and overall survivaloverall survival
Lyman GH, Lyman GH, et alet al. J Clin Oncol 2008; May 20 suppl:6552 . J Clin Oncol 2008; May 20 suppl:6552
Community-based, prospective observational studyCommunity-based, prospective observational study
Eligibility was not restricted on the basis of older age Eligibility was not restricted on the basis of older age or major co-morbidities; 3 month life expectancy and 4 or major co-morbidities; 3 month life expectancy and 4 cycles chemotherapy planned cycles chemotherapy planned
4,458 consecutive adult patients initiating 4,458 consecutive adult patients initiating chemotherapy at 115 U.S. practice sites chemotherapy at 115 U.S. practice sites

Pegfilgrastim Primary Prophylaxis Demonstrates Significant Pegfilgrastim Primary Prophylaxis Demonstrates Significant Impact on Early Overall and Progression-free SurvivalImpact on Early Overall and Progression-free Survival
Lyman GH, Lyman GH, et alet al. J Clin Oncol 2008; May 20 suppl:6552 . J Clin Oncol 2008; May 20 suppl:6552
0 10 20 30 40 50 60 70 80 900.75
0.80
0.85
0.90
0.95
1.00
Sur
viva
lS
urvi
val
Time (Days)Time (Days)
Hazard Ratio = 0.412 Hazard Ratio = 0.412 [[0.210,0.2110.210,0.211]] P P = 0.010= 0.010
PegfilgrastimPegfilgrastimPrimary ProphylaxisPrimary Prophylaxis
No PegfilgrastimNo PegfilgrastimProphylaxisProphylaxis
900 10 20 30 40 50 60 70 800.75
0.80
0.85
0.90
0.95
1.00
Pro
gre
ssio
n F
ree
Su
rviv
alP
rog
ress
ion
Fre
e S
urv
ival
Time (Days)Time (Days)
Hazard Ratio = 0.554 Hazard Ratio = 0.554 [[0.453,0.9230.453,0.923]] PP = 0.015 = 0.015
PegfilgrastimPegfilgrastimPrimary ProphylaxisPrimary Prophylaxis
No PegfilgrastimNo PegfilgrastimProphylaxisProphylaxis

Impact of Pegfilgrastim on Overall and Disease Free Impact of Pegfilgrastim on Overall and Disease Free Survival was Apparent in Major Prognostic SubgroupsSurvival was Apparent in Major Prognostic Subgroups
Lyman GH, Lyman GH, et alet al. J Clin Oncol 2008; May 20 suppl:6552 . J Clin Oncol 2008; May 20 suppl:6552
CPegfilgrastim
No Pegfilgrastim
Hazard Ratio = 0.383 [0.192,0.761] P = 0.006
ECOG ≥ 1 N = 2,024
0 10 20 30 40 50 60 70 80 900.75
0.80
0.85
0.90
0.95
1.00
Su
rviv
al
Time (Days)
D
Hazard Ratio = 0.274 [0.110,0.684] P = 0.006
Liver DysfunctionN = 1,045
Pegfilgrastim
No Pegfilgrastim
0 10 20 30 40 50 60 70 80 900.75
0.80
0.85
0.90
0.95
1.00
Su
rviv
al
Time (Days)
Hazard Ratio = 0.310 [0.133,0.723] P = 0.007
Planned RDI ≥ 85%N = 2,623
Pegfilgrastim
No Pegfilgrastim
A
0 10 20 30 40 50 60 70 80 900.75
0.80
0.85
0.90
0.95
1.00
Su
rviv
al
Time (Days)
B
Hazard Ratio = 0.346 [0.125,0.954] P = 0.040
Pegfilgrastim
No Pegfilgrastim
Lung CancerN = 907
0 10 20 30 40 50 60 70 80 900.75
0.80
0.85
0.90
0.95
1.00
Su
rviv
al
Time (Days)

Risk of Mortality in Patients with Cancer Risk of Mortality in Patients with Cancer Experiencing Febrile NeutropeniaExperiencing Febrile Neutropenia
Barron, R. Abstract 9561, ASCO 2009Barron, R. Abstract 9561, ASCO 2009
Kaplan-Meier Survival Curve for Early MortalityKaplan-Meier Survival Curve for Early Mortality
Length of Follow-up in MonthsLength of Follow-up in Months
Non febrile neutropenia patientsNon febrile neutropenia patientsFebrile neutropenia patientsFebrile neutropenia patients
00 2 2 4 4 6 8 10 12 6 8 10 12
Sur
viva
lS
urvi
val
1.001.00
0.990.99
0.980.98
0.970.97
0.960.96
0.950.95
Log rank test: Chi2(1)=4.79, p=0.0287Log rank test: Chi2(1)=4.79, p=0.0287

Risk of Mortality in Patients with Cancer Risk of Mortality in Patients with Cancer Experiencing Febrile NeutropeniaExperiencing Febrile Neutropenia
Barron, R. Abstract 9561, ASCO 2009Barron, R. Abstract 9561, ASCO 2009
Kaplan-Meier Survival Curve for Overall MortalityKaplan-Meier Survival Curve for Overall Mortality
Log rank test: Chi2(1)=23.15, p<0.0001Log rank test: Chi2(1)=23.15, p<0.0001
Length of Follow-up in MonthsLength of Follow-up in Months
Non febrile neutropenia patientsNon febrile neutropenia patientsFebrile neutropenia patientsFebrile neutropenia patients
Sur
viva
lS
urvi
val
1.001.00
0.950.95
0.900.90
0.850.85
0.800.80
0.750.7500 1010 2020 3030 4040 5050 6060 7070

Guidelines at a Glance: Guidelines at a Glance: Primary Prophylactic CSF Primary Prophylactic CSF
AdministrationAdministration
Neutropenic Neutropenic Event RiskEvent Risk
EORTCEORTC20062006
ASCOASCO 20062006
NCCNNCCN20072007
Moderate to High
Use CSF Use CSF ≥ 20% ≥ 20% Use CSF Use CSF ~~ 20% 20% Use CSF > 20%Use CSF > 20%
IntermediateConsider CSFConsider CSF
10 - 20%10 - 20%with risk factorswith risk factors
Recommend Recommend < 20% < 20%
(with risk factors)(with risk factors)
Consider CSFConsider CSF10 - 20%10 - 20%
with risk factorswith risk factors
LowCSF is not CSF is not
recommended recommended < 10%< 10%
Not specified Not specified CSF is not CSF is not
recommended for recommended for most patientsmost patients
< 10%< 10%
Risk Factor Assessment ++++++ ++++++ ++++
NCCN Clinical Practice Guidelines in Oncology: Myeloid Growth Factors. v.1.2007. Available at: NCCN Clinical Practice Guidelines in Oncology: Myeloid Growth Factors. v.1.2007. Available at: http://www.nccn.org, accessed May 23, 2007http://www.nccn.org, accessed May 23, 2007
Smith TJ, et al. J Clin Oncol. 2006;24(19):3187-3205Smith TJ, et al. J Clin Oncol. 2006;24(19):3187-3205Aapro MS, et al. European J Cancer. 2006;42:2433-2453 Aapro MS, et al. European J Cancer. 2006;42:2433-2453

NCCN Practice Guidelines in Oncology NCCN Practice Guidelines in Oncology v.1.2010v.1.2010
Myeloid Growth FactorsMyeloid Growth FactorsPatient Risk Factors for Developing Febrile NeutropeniaPatient Risk Factors for Developing Febrile Neutropenia
In addition to the risk of the chemotherapy regimen and the In addition to the risk of the chemotherapy regimen and the specific malignancy being treated, these factors need to be specific malignancy being treated, these factors need to be considered when evaluating a patient’s overall risk for febrile considered when evaluating a patient’s overall risk for febrile neutropenia.neutropenia.
►Older patient, notably patients age 65 and older (see NCCN Older patient, notably patients age 65 and older (see NCCN Senior Adult Oncology Guidelines)Senior Adult Oncology Guidelines)►Previous chemotherapy or radiation therapyPrevious chemotherapy or radiation therapy►Pre-existing neutropenia or bone marrow involvment with tumorPre-existing neutropenia or bone marrow involvment with tumor►Pre-existing conditionsPre-existing conditionsNeutropeniaNeutropeniaInfection/open woundsInfection/open woundsRecent surgeryRecent surgery►Poor performance statusPoor performance status►Poor renal functionPoor renal function►Liver dysfunction, most notably elevated bilirubinLiver dysfunction, most notably elevated bilirubin



AdverseAdverse Events Associated with Events Associated with Myeloid Growth FactorsMyeloid Growth Factors
CommonCommonBone/musculoskeletal pain (25-50%)Bone/musculoskeletal pain (25-50%)
Less CommonLess CommonSplenomegaly (3%)Splenomegaly (3%)Headache, nauseaHeadache, nauseaFever (1%)Fever (1%)
RareRareAllergic reactionAllergic reactionSweet’s syndromeSweet’s syndrome
ControversialControversialAcute myeloid leukemia – epidemiologic association, Acute myeloid leukemia – epidemiologic association, but not confirmed in randomized prospective trialsbut not confirmed in randomized prospective trials
Myeloid Growth Factor Guidelines v.1.2008, www.NCCN.orgMyeloid Growth Factor Guidelines v.1.2008, www.NCCN.org
Filgrastim/PegfilgrastimFilgrastim/Pegfilgrastim

Relative Risk for AML/MDS by Cancer TypeRelative Risk for AML/MDS by Cancer Type
Acute Myeloid Leukemia or Myelodysplastic Syndrome Acute Myeloid Leukemia or Myelodysplastic Syndrome and Overall Mortality with Chemotherapy and and Overall Mortality with Chemotherapy and
Granulocyte Colony-Stimulating FactorGranulocyte Colony-Stimulating Factor
Meta-Analysis of Randomized Controlled TrialsMeta-Analysis of Randomized Controlled Trials
Lyman, G. ASCO Abstract 9524, 2009

AML/MDS by Planned CT Regimen CategoryAML/MDS by Planned CT Regimen Category
Lyman, G. ASCO Abstract 9524, 2009
Acute Myeloid Leukemia or Myelodysplastic Syndrome Acute Myeloid Leukemia or Myelodysplastic Syndrome and Overall Mortality with Chemotherapy and and Overall Mortality with Chemotherapy and
Granulocyte Colony-Stimulating FactorGranulocyte Colony-Stimulating Factor
Meta-Analysis of Randomized Controlled TrialsMeta-Analysis of Randomized Controlled Trials

All-Cause Mortality by Tumor TypeAll-Cause Mortality by Tumor Type
Lyman, G. ASCO Abstract 9524, 2009
Acute Myeloid Leukemia or Myelodysplastic Syndrome Acute Myeloid Leukemia or Myelodysplastic Syndrome and Overall Mortality with Chemotherapy and and Overall Mortality with Chemotherapy and
Granulocyte Colony-Stimulating FactorGranulocyte Colony-Stimulating Factor
Meta-Analysis of Randomized Controlled TrialsMeta-Analysis of Randomized Controlled Trials

All-Cause Mortality by Regimen CategoryAll-Cause Mortality by Regimen Category
Lyman, G. ASCO Abstract 9524, 2009Lyman, G. ASCO Abstract 9524, 2009
Acute Myeloid Leukemia or Myelodysplastic Syndrome Acute Myeloid Leukemia or Myelodysplastic Syndrome and Overall Mortality with Chemotherapy and and Overall Mortality with Chemotherapy and
Granulocyte Colony-Stimulating FactorGranulocyte Colony-Stimulating Factor
Meta-Analysis of Randomized Controlled TrialsMeta-Analysis of Randomized Controlled Trials

Neutropenia / Management Neutropenia / Management SummarySummary
► Neutropenia is the major risk factor for fever and Neutropenia is the major risk factor for fever and infection, as well as reduced chemotherapy dose infection, as well as reduced chemotherapy dose delivery; both of which can be associated with delivery; both of which can be associated with reduced survival of the cancer patient.reduced survival of the cancer patient.
► In patients at significant risk of febrile neutropenia In patients at significant risk of febrile neutropenia (>20%) prophylactic CSFs are warranted in the first (>20%) prophylactic CSFs are warranted in the first and all subsequent cycles of chemotherapy.and all subsequent cycles of chemotherapy.
► Prophylactic antibiotics may add to the benefit of Prophylactic antibiotics may add to the benefit of CSFs in selected settings, but cannot replace them.CSFs in selected settings, but cannot replace them.
► Further prospective studies evaluating Further prospective studies evaluating chemotherapy RDI and outcomes in cancer patients chemotherapy RDI and outcomes in cancer patients are needed.are needed.