Embed Size (px)
Citation preview

Produced by the Science/AAAS Custom Publishing OfficeSponsored by
INNOVATION PARTNERSHIPS
FOR 21ST CENTURY HEALTH CARE:
THE AUSTRALIAN CHALLENGE
0703Abbot-Australian Commission_Cover.indd 10703Abbot-Australian Commission_Cover.indd 1 9/14/20 2:13 PM9/14/20 2:13 PM

www.ScienceTranslationalMedicine.org
GOLD OPEN ACCESS, DIGITAL , AND FREE TO ALL READERS
As AAAS’s first multidisciplinary, open access journal, Science Advances publishesresearch that reflects the selectivity of high impact, innovative research you expectfrom the Science family of journals, published in an open access format to servea vast and growing global audience. Check out the latest findings or learn how tosubmit your research: ScienceAdvances.org
Pushing the Boundaries of Knowledge

1
Introductions
2 What’s in a name? Sean Sanders Science/AAAS
3 A message from John CrothersJohn Crothers Abbott Diagnostics
Invited Articles
4 The Australian Cardiovascular Alliance: Implementing a new vision to tackle cardiovascular health challenges By Kerry Doyle, Meng-Ping Hsu, Gemma Figtree ACvA
6 Continued innovation in health is key to Australia’s recoveryBronwyn Le Grice ANDHealth
Reprinted Articles
8 Why University-Industry Partnerships Matter By Anthony M. Boccanfuso
11 Breaking Down Translation Barriers: Investigator’s Perspective By Nathan P. Staff, Bethany Kinseth Runge, Anthony J. Windebank
16 Changing the Mindset in Life Sciences Toward Translation: A Consensus By Georg N. Duda, David W. Grainger, Megan L. Frisk et. al.
22 Financing translation: Analysis of the NCATS rare-diseases portfolio By David E. Fagnan, N. Nora Yang, John C. McKew et. al.
29 Key elements for nourishing the translational research environment By Hans-Dieter Volk, Molly M. Stevens, David J. Mooney et. al.
Innovation partnerships for 21st century health care: The Australian challenge
Table of Contents
This booklet was produced by the Science/AAAS Custom Publishing Office and sponsored by Abbott.
Articles can be cited using the following format: [AUTHOR NAME(S)] [CHAPTER TITLE] Innovation partnerships for 21st century health care: The Australian challenge (Science/AAAS, Washington, DC, 2020), p. [xx-xx].
Editor: Sean Sanders, Ph.D. Proofreader/Copyeditor: Bob French Designer: JD Huntsinger
Tracy Holmes Director, Custom Publishing & Advertising Sales Science/AAAS [email protected] Tel: +44 (0) 7786 505557
© 2020 by The American Association for the Advancement of Science. All rights reserved. 16 October 2020
COVER IMAGE: © ARTEM FIRSOV/SHUTTERSTOCK.COM
SPECIAL CONFERENCE ISSUE

2
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
What’s in a name?
The phrase describing the goal of biomedical research as “bench to bedside” has been around for at least 40 years, possibly longer, but about 20 years ago its usage accelerated considerably, some might say to the point of overuse. Although it has now been replaced by the more medico-scientific
sounding “translational research,” I like the original coinage for its simplicity and clarity in describing how bioscience research matures from the laboratory bench, along a sometimes rocky path, to the patient in the clinic.
At its core, this moniker expresses the desire by researchers and patients alike—and the increasing demand of many funding entities—that the knowledge gained from basic bioscience research be used to its fullest to generate treatment, drugs, or devices that benefit the broadest possible population by alleviating suffering and reducing mortality. One could also look at it in more dispassionate, economic terms in which the return on investment for taxpayer-funded research must justify the financial stake.
Whichever way you view it, the notion that research funding should be used in the most efficient, productive, and beneficial way holds true around the world, including in Australia, the focus of this supplement. While infectious diseases such as the novel coronavirus, SARS-CoV-2, generate immediate and justifiable concern, noncommunicable diseases such as diabetes and cardiovascular disease (CVD) still kill many more people each year, numbering in the millions to tens of millions. Unlike COVID-19—the illness caused by SARS-CoV-2—for which we have few viable treatments, numerous effective diagnostics and therapies are available to address both diabetes and CVD, although the continued high death toll for these diseases indicates that we still have much work to do in generating more efficacious treatments and making them affordable and available to all. Australia is not immune to the impacts of noncommunicable disease; as is pointed out on page 4 of this publication, “CVD is also Australia’s most expensive disease in terms of health care, costing the nation $10.4 billion annually in direct health costs.”
In this supplement, we have compiled a range of articles, all published in Science Translational Medicine, which highlight some of the challenges inherent in bench-to-bedside research and provide helpful insights into possible paths to improve the chances for success. The voices in this co llection are international, because the obstacles to research are similar around the world, but the benefits can often be uniquely local. With its educated and innovative scientific workforce, Australia is well positioned to benefit from a continued and robust investment in translational research. Whatever you choose to call this type of scientific investigation, there seems to be little doubt that funding it will pay off in the future through a healthier, more productive, and happier population.
Sean Sanders, Ph.D. Director and Senior Editor for Custom Publishing Science/AAAS

3
INTRODUCTIONS
Dear Reader,
Abbott—one of the world’s leading health care companies, employing more than 1,700 scientists around the globe—is pleased to sponsor this special collection featuring contributions from Australian leaders in health care research and commercialization, alongside papers addressing the challenge of translating fundamental research into innovative health solutions. Abbott has been committed to providing innovative health solutions in Australia since 1938, and we have over 600 employees supporting Australian health care institutions around the country.
Although infectious diseases such as COVID-19 have shown they can stop us in our tracks, chronic conditions such as heart disease and diabetes are still the major causes of morbidity and mortality in advanced economies and increasingly in developing countries, threatening the health of millions and burdening health care systems worldwide. As we have learned from this pandemic, cooperation and partnerships between scientists, health care practitioners, universities, governments, and private companies are critical to create a healthy society and a safer world.
Looking beyond COVID-19, governments will be learning from the way their health care systems responded to the virus. With rapid mobilization, public–private partnerships, expert leadership, and public cooperation, Australia managed the pandemic as well as any country. Even so, better integration of public and private sector capabilities could speed public health responses and deliver results more efficiently. In the future, Australia’s solid base of well-resourced medical research institutions will benefit from stronger, institutional ties to global market leaders like Abbott.
Articles in this supplement examine the critical factors that enable translational medicine. Innovations in product development can be as impactful as the basic science discoveries that underpin new therapies. Bronwyn Le Grice, cofounder and CEO of ANDHealth, Australia’s national digital health initiative, describes areas of Australian competitiveness and the challenges of launching innovative health care firms in the country. Gemma Figtree, chair of the Australian Cardiovascular Alliance, points the way to a future where early-stage partnerships between Australian researchers and global developers can speed the path to translation.
Australia’s public and private investment in health research makes it well situated to continue to generate medical breakthroughs. The “tyranny of distance” is less of an impediment than in the past, and can even be considered an advantage—the country's location provides proximity to fast-growing health care markets in Asia, while also enabling the country to plug into “follow-the-sun” models for product development, bridging major markets in the United States and Europe. Building innovation partnerships that position Australia at the frontier of health delivery is an achievable goal, given the right mix of investment, policy, and partnership.
We ask you to learn more about these issues and partner with us in making strides against costly, chronic diseases. We look forward to being an active part of this complex solution. Together, we can make the world a healthier place, allowing all people to Live Life to the Fullest.
John Crothers Regional Director, Abbott Diagnostics, Australia and New Zealand Chair of Pathology Awareness Australia

4
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
Despite the common perception that cardiovascular disease (CVD), which includes heart, stroke, and blood vessel diseases, is well understood and largely conquered, it remains the biggest killer globally. In Australia, 1 in 5 deaths are from CVD, resulting in a death every 19 minutes. CVD is also Australia’s most expensive disease in terms of health care, costing the nation $10.4 billion annually in direct health costs (1).
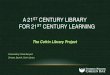
The Australian Cardiovascular Alliance (ACvA) is a not-for-profit, incorporated entity, representing the unified voice of cardiovascular researchers, industry, and care societies throughout the country. ACvA members believe the time is ripe for a new vision, new thinking, and new strategies to solve CVD and, with collaboration as a core value, ACvA is working to ensure a thriving, sustainable, world-class CVD ecosystem. In such a system, our very best research leaders and teams are strategically placed to work closely with the health system and industry toward solving prioritised health problems, providing greater value for money from government investments and greater impact for the Australian community. To this end, ACvA has established six strategic “flagships”: Implementation and Policy, Big Data, Clinical Trials, Drug Discovery, Bioengineering, and Precision Medicine. These flagships cut across the major clinical challenges where critical need is matched by scientific expertise, such as atherosclerosis, heart muscle disease, arrhythmia, and stroke.
The ACvA is a unique collaboration drawing in stakeholders from across the field of cardiac care. Adapted from G. A. Figtree et al., Heart Lung Circ. 28, 198–203 (2019).
The Australian Cardiovascular Alliance: Implementing a new vision to tackle cardiovascular health challengesKerry Doyle, Executive Director, ACvA Meng-Ping Hsu, Project Officer, ACvAGemma Figtree, President, ACvA and Professor, Sydney Medical School (Northern), Faculty of Medicine and Health, University of Sydney

5
INVITED ARTICLES
The flagship structure brings together the entire cardiovascular research community and our broad industry membership to promote a whole-of-nation approach along a bidirectional translational pipeline. This will ensure that Australian CVD research and development are aligned to the most urgent clinical challenges and that discoveries and innovative approaches to care are translated in an accelerated manner.
ACvA has a small but agile operations team whose work is enabled by a committed group of research and industry members, and a board comprising internationally renowned researchers (2).
ACvA’s members and team are:
• bringing our broadly based and highly committed industry members together with academia and government partners to participate in strategic roundtables to build productive partnerships and increase Australia’s attractiveness as a destination for global industry.
• supporting industry/academic and government working groups focused on:
{ strengthening industry and academic partnerships, with a significant emphasis on the clinical trials landscape.
{ accelerating the delivery of evidence- and value-based care to patients.
• celebrating the work of our researchers and their capabilities through social media and new awards for research excellence.
• delivering capacity building programs to support our emerging leaders, foster career development, build communications skills, and allow our research workforce to pursue diverse career pathways.
• facilitating the development of large, collaborative, impactful research proposals in line with knowledge gaps and the burden of disease, while also identifying potential funding sources.
• providing a unified advocacy voice to governments at all levels, including for innovative funding approaches and streamlined processes for translation and commercialisation.
• working with and aligning key stakeholders to raise the profile of CVD and the importance of research in fighting our nation’s biggest killer.
ACvA’s president, professor Gemma Figtree, states that “ACvA has achieved unprecedented collaboration across industry and academia, and the support for the one-stop shop provided by ACvA has received resounding support.” This sentiment is strongly endorsed by our industry colleague, John Crothers, Abbott’s regional director for Australia and New Zealand: “ACvA demonstrates the power of one—a critical asset in the Australian market.”
References1. Australian Institute of Health and Welfare. (2019). Disease expenditure in Australia 2015–
2016 (No. HWE 76). Retrieved from https://www.aihw.gov.au/getmedia/e966d2ce-c579-4f47-846d-47255f4aa7fc/aihw-hwe-76.pdf.aspx.
2. https://www.ozheart.org/directors-executive-australian-cardiovascular-alliance-acva.
ACvA is mobilizing partnerships along the continuum of cardiovascular health innovation. Adapted from G. A. Figtree et al., Heart Lung Circ. 28, 198–203 (2019).

6
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
Continued innovation in health is key to Australia’s recoveryBronwyn Le Grice Founder, CEO & Managing Director, ANDHealth
Australia has a lot to be proud of in health and medical innovation and commercialisation. It has a world-class research sector, an advanced health care system, and a successful, entrepreneurial technology sector. Over the past two decades, as innovations have matured through the commercialisation pathway, Australia’s biotechnology, pharmaceutical, and medical devices sectors have thrived, supported by proactive public policy and funding and by subsequent private investment.
However, our success in these areas should not be taken for granted. The delivery of health care products and services is changing, with the role of technology becoming increasingly important as governments and health care providers look for ways to deliver scalable, affordable, and clinically effective care.
In Australia, most of the focus on digital health has been and remains on creating digital infrastructure for health care: electronic health care records, collaborations around understanding health care data to improve cost efficiencies, electronic prescriptions, and—due to COVID-19—telehealth.
Looking internationally, other countries have taken a much broader approach to digital health. For example, the U.S. Food and Drug Administration provides a more holistic definition of the term, which includes mobile health, connected devices and wearables, telehealth and telemedicine, and personalised and precision medicine. This more encompassing global view opens the door to the emerging high-value, high-patient–impact areas of digital medicine and digital therapeutics.
As a result of Australia’s focus on digital health infrastructure, local companies that are innovating in evidence-based digital health—such as therapies, diagnostics, and integrated services—have found themselves largely without the usual pathways to obtain funding for research, development, and commercialisation that are more generally available in the broader health and medical research sector.
Most grants and funding schemes remain heavily weighted towards the sector’s more traditional criteria, such as patents, publications, and clinical milestones. In digital health, however, the most successful companies
We need to manifest a
post-pandemic future
in which care shifts
from the clinic to the
home, with digital health
solutions delivering
disease prevention,
diagnosis, management,
and treatment.
PHO
TO: ©
ALI
SON
MC
WH
IRTE
R

7
INVITED ARTICLES
may not have patents; their value and subsequent valuation may not be impacted by clinical evidence as much as they are by commercial validation and customer uptake. The result of these unique characteristics is that some of Australia’s most promising digital innovators are often unable to deliver against criteria that are simply not relevant to their long-term success, leaving them isolated from critical, early-stage funding.
Turning to private investment, if we look back to the policy settings that underpinned the significant growth in international competitiveness of our pharmaceutical and medical device industries, one common factor was the sustained investment in R&D in those sectors by governments at both the state and federal level. This early-stage investment created high-quality assets that led to the establishment of specialised venture fund and investment firms. These financial benefits have not materialized for the digital health sector—another example of how Australia’s funding and investment ecosystem is letting down our digital health innovators.
Looking to the future, COVID-19 has challenged us to reimagine our health care systems and to rapidly adopt best-in-class technologies that leverage digital connectivity and Australia’s significant historical investment in pre-existing digital health infrastructure.
After a years-long debate about whether or not to roll out and fund telehealth on a broad scale, policymakers and care providers around the world have now embraced virtual consultations as a way to protect both health care providers and citizens from infection during the coronavirus pandemic.
But when we consider our ideal post-COVID reality, telehealth is only the tip of the iceberg in a vibrant, world-class, technology-enabled health care system. We need to manifest a post-pandemic future in
which care shifts from the clinic to the home, with digital health solutions delivering disease prevention, diagnosis, management, and treatment, at the same time improving the efficiency of our health care system and the ability of all Australians to access it.
In Australia today, we have over 350 companies actively building digital health technologies that span a broad range of clinical indications. Over 45% of these technologies are focused on delivery of care in home, work, or community settings, and 33% address ways to drive patient behavioural changes, self-management, and adherence, demonstrating the potential inherent in engaging consumers in their health care journey, wherever they are.
In a global sense, Australia’s largely successful management of the COVID-19 pandemic has given us an unprecedented opportunity to position ourselves as a COVID-safe “cleanroom” destination for medical research and education, including in digital health. This leverages the significant need for industry players to continue to undertake clinical trials and gather real-world evidence in settings in which COVID is not an overwhelming factor.
Moving out of “pandemic mode,” digital health is an emerging sector that is well placed to achieve the triple aim of economic growth through high-value science, technology, engineering, and mathematics (STEM)-based job creation, increased advanced manufacturing and clinical trials activity, and sovereign health system capability and resilience. It is also essential to maintaining the competitiveness and attractiveness of our outstanding biotechnology, pharmaceutical, and medical device sectors. Australia has invested billions in becoming a powerhouse in health and medical innovation, and to stop investing in that now would be a tragedy.
PHO
TO: ©
LEA
H-A
NN
E TH
OM
PSO
N/S
HU
TTER
STO
CK.C
OM

8
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.orgOriginally published 29 September 2010www.ScienceTranslationalMedicine.org 29 September 2010 Vol 2 Issue 51 51cm25 1
C O M M E N TA R Y
“ ”
CR
ED
IT: C
. B
ICK
EL/S
CIE
NC
E T
RA
NS
LA
TIO
NA
L M
ED
ICIN
E
� e American higher education system has long been the envy of the world and has produced the discoveries that gave rise to innovations resulting in many of the prod-ucts that improve our lives (1). Although universities are outstanding at creating the base knowledge (discovery) used in the creation of new products (innovation), companies are relied on to take these in-ventions and develop them into usable products. � is process has worked well for an extended period, but there are oppor-tunities to expand the level, number, and depth of university-industry collaborations and bolster the creation of new products (Fig. 1). Some trends are also worthy of consideration. Large pharmaceutical com-panies are reassessing their investments in internal research and development (R&D) and looking to “purchase” promising in-ventions by partnering with universities (2) and small businesses [many of which rely on government funding, such as the small business innovation research (SBIR) and small business technology transfer programs] (3). Governments (federal and state) have increasingly recognized the value of university-industry partnerships and are starting to make investments that fund these e� orts; one can look at the Clin-ical Translation Scientist Award from the National Institutes of Health (NIH) as an example of the federal government’s invest-ment to spur and catalyze the discovery-to-innovation process.
A 2008 report prepared by the Presi-dent’s Council of Advisors on Science and Technology titled “University-Private Sec-tor Research Partnerships in the Innova-tion Ecosystem” (4) provides an overview of the U.S. R&D enterprise and focuses on
the critical role for university–private sec-tor research partnerships, their potential to improve research and innovation, and the obstacles standing in the way of further progress.
Small businesses play an increasingly important role in innovation and the health of the U.S. economy; the linkages of uni-versities with those businesses to support their R&D activities can be extremely valu-able. � at is why more than two-thirds of companies receiving SBIR support had at least one founder who previously served in the science/engineering academic sector. � ese companies o� en contracted and em-ployed universities (17%), faculty (27%), and graduate students (15%) to support their work (5).
GUIDING PRINCIPLES FOR UNIVERSITY-INDUSTRY ENDEAVORSIn April 2006, the National Council of Uni-versity Research Administrators and the Industrial Research Institute issued a joint
report on guiding principles for university-industry endeavors (6). � is project was dubbed the University-Industry Partner-ship and was the precursor to today’s Uni-versity-Industry Demonstration Partner-ship (UIDP). In the report, three guiding principles were identi� ed: (i) Successful university-industry collaboration should support the mission of each partner. Any e� ort in con� ict with the mission of either partner will ultimately fail. (ii) Institution-al practices and national resources should focus on fostering appropriate long-term partnerships between universities and industry. (iii) Universities and industry should focus on maximizing value result-ing from collaborations by streamlining negotiations and measuring results. � ese guiding principles provide an important foundation for university and industry representatives who seek to develop high-return relationships.
BENEFITS OF UNIVERSITY-INDUSTRY COLLABORATIONSIn an increasingly complex and multi-disciplinary research ecosystem, universi-ties and industries can bene� t from part-nering.
For universities, there are a number of � nancial and non� nancial motivations. For large research-intensive universities, in-dustry-sponsored research serves as an im-portant piece in the overall external fund-ing mosaic. According to the most recent data from the National Science Foundation (NSF) (7), universities in the United States expended $2.87 billion of industry research funding in � scal year 2008; this represent-
C O L L A B O R AT I O N S
Why University-Industry Partnerships Matter
Anthony M. Boccanfuso
E-mail: [email protected]
Published 29 September 2010; Volume 2 Issue 51 51cm25
National Academy of Sciences, University-Industry Demonstration Partnership, Washington, DC 20001, USA.
Basic research, much of which emanates from the outstanding academic laboratories located in the United States and abroad, is the foundation for the innovation that has created the new therapies, materials, and processes that bene� t humankind and generate wealth for companies that successfully translate discoveries to commercial success. This is not a linear, one-way process; optimizing the process of discovery to innovation demands dynamic and multifaceted approaches to teaming at the university-industry interface.
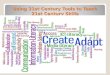
Fig. 1. Opportunity awaits. Although business funding of R&D has increased in the last 10 years
in the U.S. (16), the percentage of academic R&D fi nanced by business has decreased in the U.S. as
well as in a number of other countries (17). With industry’s increasing reliance on external alliances
to bolster its product pipeline, academic research is a likely place to seek partners.
0
5
10
15
20
25
30
35
40
19
81
19
83
19
85
19
87
19
89
19
91
19
93
19
95
19
97
19
99
20
01
20
03
20
05
20
07
Pe
rce
nt
Year
Percent of Academic R&D Financed by Business for Selected Countries
United States
Japan
China
Germany
France
South Korea
United Kingdom
Russia
Canada
Italy
www.ScienceTranslationalMedicine.org 29 September 2010 Vol 2 Issue 51 51cm25 1
C O M M E N TA R Y
“ ”
CR
ED
IT: C
. B
ICK
EL/S
CIE
NC
E T
RA
NS
LA
TIO
NA
L M
ED
ICIN
E
� e American higher education system has long been the envy of the world and has produced the discoveries that gave rise to innovations resulting in many of the prod-ucts that improve our lives (1). Although universities are outstanding at creating the base knowledge (discovery) used in the creation of new products (innovation), companies are relied on to take these in-ventions and develop them into usable products. � is process has worked well for an extended period, but there are oppor-tunities to expand the level, number, and depth of university-industry collaborations and bolster the creation of new products (Fig. 1). Some trends are also worthy of consideration. Large pharmaceutical com-panies are reassessing their investments in internal research and development (R&D) and looking to “purchase” promising in-ventions by partnering with universities (2) and small businesses [many of which rely on government funding, such as the small business innovation research (SBIR) and small business technology transfer programs] (3). Governments (federal and state) have increasingly recognized the value of university-industry partnerships and are starting to make investments that fund these e� orts; one can look at the Clin-ical Translation Scientist Award from the National Institutes of Health (NIH) as an example of the federal government’s invest-ment to spur and catalyze the discovery-to-innovation process.
A 2008 report prepared by the Presi-dent’s Council of Advisors on Science and Technology titled “University-Private Sec-tor Research Partnerships in the Innova-tion Ecosystem” (4) provides an overview of the U.S. R&D enterprise and focuses on
the critical role for university–private sec-tor research partnerships, their potential to improve research and innovation, and the obstacles standing in the way of further progress.
Small businesses play an increasingly important role in innovation and the health of the U.S. economy; the linkages of uni-versities with those businesses to support their R&D activities can be extremely valu-able. � at is why more than two-thirds of companies receiving SBIR support had at least one founder who previously served in the science/engineering academic sector. � ese companies o� en contracted and em-ployed universities (17%), faculty (27%), and graduate students (15%) to support their work (5).
GUIDING PRINCIPLES FOR UNIVERSITY-INDUSTRY ENDEAVORSIn April 2006, the National Council of Uni-versity Research Administrators and the Industrial Research Institute issued a joint
report on guiding principles for university-industry endeavors (6). � is project was dubbed the University-Industry Partner-ship and was the precursor to today’s Uni-versity-Industry Demonstration Partner-ship (UIDP). In the report, three guiding principles were identi� ed: (i) Successful university-industry collaboration should support the mission of each partner. Any e� ort in con� ict with the mission of either partner will ultimately fail. (ii) Institution-al practices and national resources should focus on fostering appropriate long-term partnerships between universities and industry. (iii) Universities and industry should focus on maximizing value result-ing from collaborations by streamlining negotiations and measuring results. � ese guiding principles provide an important foundation for university and industry representatives who seek to develop high-return relationships.
BENEFITS OF UNIVERSITY-INDUSTRY COLLABORATIONSIn an increasingly complex and multi-disciplinary research ecosystem, universi-ties and industries can bene� t from part-nering.
For universities, there are a number of � nancial and non� nancial motivations. For large research-intensive universities, in-dustry-sponsored research serves as an im-portant piece in the overall external fund-ing mosaic. According to the most recent data from the National Science Foundation (NSF) (7), universities in the United States expended $2.87 billion of industry research funding in � scal year 2008; this represent-
C O L L A B O R AT I O N S
Why University-Industry Partnerships Matter
Anthony M. Boccanfuso
E-mail: [email protected]
Published 29 September 2010; Volume 2 Issue 51 51cm25
National Academy of Sciences, University-Industry Demonstration Partnership, Washington, DC 20001, USA.
Basic research, much of which emanates from the outstanding academic laboratories located in the United States and abroad, is the foundation for the innovation that has created the new therapies, materials, and processes that bene� t humankind and generate wealth for companies that successfully translate discoveries to commercial success. This is not a linear, one-way process; optimizing the process of discovery to innovation demands dynamic and multifaceted approaches to teaming at the university-industry interface.
Fig. 1. Opportunity awaits. Although business funding of R&D has increased in the last 10 years
in the U.S. (16), the percentage of academic R&D fi nanced by business has decreased in the U.S. as
well as in a number of other countries (17). With industry’s increasing reliance on external alliances
to bolster its product pipeline, academic research is a likely place to seek partners.
0
5
10
15
20
25
30
35
40
19
81
19
83
19
85
19
87
19
89
19
91
19
93
19
95
19
97
19
99
20
01
20
03
20
05
20
07
Pe
rce
nt
Year
Percent of Academic R&D Financed by Business for Selected Countries
United States
Japan
China
Germany
France
South Korea
United Kingdom
Russia
Canada
Italy

9
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.orgwww.ScienceTranslationalMedicine.org 29 September 2010 Vol 2 Issue 51 51cm25 2
C O M M E N TA R Y
“ ”ed approximately 5.5% of all R&D expen-ditures but nearly 7% of external funding. Put in the context of a research university with $200 million of annual expenditures, industry support would represent $14 mil-lion, a tidy sum that can support a large number of talented researchers and the purchase of a substantial amount of sup-plies and relevant equipment. In order to e� ectively compete for federal grants (es-pecially large, multiyear awards) in today’s ultracompetitive environment, universities are asked to address speci� cally the rel-evance of the proposed research as well as how industry will be engaged with the pro-posed project. � is engagement can come in the form of direct cash investments or support via cross-fertilization of research teams who can work at the university-industry interface. In response to recom-mendations from the Committee of Visi-tors, the NSF’s Engineering Research Center (ERC) program clearly articulated the goals of the Generation � ree ERC program to place greater emphasis on innovation and speed the translation of knowledge to tech-nology through partnerships (8). A num-ber of state programs also directly support university-industry collaborations; some of these, such as the Maryland Industrial Partnerships (MIPS) program, have fund-ed more than 400 Maryland companies since 1987. Worth over $160 million, these MIPS projects have led to the creation of MIPS-supported products that have gener-ated more than $19.5 billion in sales and added jobs to the region. Some newer pro-grams, such as the South Carolina Centers for Economic Excellence program, simi-larly provide matching funding (as much as $5 million) and create centers to support the economic development interests of the states in targeted research areas of univer-sities and companies.
� ere are also important, non� nancial motivations. Universities want to ensure that they can recruit and retain the best tal-ent to their campuses. Contemporary fac-ulty and students seek greater relevance to their scholarly pursuits and want to work de� ly in both the academic and corporate environs. Some academic institutions have excelled at creating a supportive environ-ment, and many more institutions are em-bracing this approach. For example, Texas A&M University claims to be the � rst pub-lic university to o� cially consider tech-nology commercialization in tenure and promotion decisions; since implementing
the policy in 2007, the school has seen an increase in invention disclosures from ten-ure-track professors (9). Universities also seek to establish workforce pipelines from their institutions to companies. � e abil-ity to promote the successful placement of students in industry supports high-caliber undergraduate and graduate student re-cruitment.
� e bene� ts a� orded to industry paral-lel those to academia. Foremost, universi-ties are the greatest source of future work-ers who possess contemporary skills to help companies achieve their business ob-jectives. Additionally, as more companies have reduced their � nancial commitment for internally supported R&D, especially basic research, universities are one area in which companies can make an investment in early-stage technology development and potentially realize future bene� ts if com-mercial applications can be identi� ed. Ac-cess to facilities and specialized equipment also fosters collaboration. For startup � rms or � rms with fewer resources, the bene� ts can be much greater and can range from bolstering the company’s cash � ow and ac-cess to investment-grade funding to pro-viding substantial expertise to complement the employee pools found in these � rms.
CHALLENGES TO UNIVERSITY-INDUSTRY COLLABORATIONSUniversity-industry partnerships can pro-vide both parties substantial bene� ts, but there are challenges (some obvious and some more surprising) that can consider-ably a� ect the ability of these parties to partner.
Intellectual property. � e most com-mon issue has to do with intellectual prop-erty (IP) rights and who should “own” the results that emanate from an industry-sponsored research project. It is appealing to want to treat all projects (and the back-ground and foreground IP rights) the same for each negotiated agreement. However, agreements vary a great deal as a result of the di� erences in industry, the university lab’s overall � nancial support and the per-centage of the project being covered by an award, the origination of the project scope, and the likelihood for commercialization. � e UIDP has invested substantial resourc-es to help provide education on this topic; some of the fruits of this work are found in the Contract Accords booklet produced by a UIDP-supported working group (10).
Budget. Project cost and, speci� cally,
indirect cost rates can also lead to challeng-es—especially when universities work with companies that have limited experience engaging universities. Some universities have moved away from detailed budgets that separate indirect costs and instead are using budgets that show the overall costs of the project.
Regulatory. Because of the poor deci-sions made by some researchers to engage in criminal activities, violating laws as well as institutional con� ict of interest and dis-closure policies, the pendulum is moving toward greater regulation surrounding the topic of con� ict of interest. � e NIH has released dra� guidelines (11) for consid-eration that recognize the general public’s concern about these university-industry collaborations while also acknowledging that if these regulations go too far, they will substantially deter collaborations. In a recent Institute of Medicine report on the subject, the opening sentence asserts, “Patients and the public bene� t when phy-sicians and researchers collaborate with pharmaceutical, medical device, and bio-technology companies to develop products that bene� t individual and public health” (12). Regulations should not unduly limit collaboration.
� ere are also Internal Revenue Service (IRS) rules that reduce the options univer-sities possess when negotiating sponsored projects with industry. � ese rules severely restrict the ability of universities to value IP that may result from the work funded by companies, reducing the willingness of some � rms to fund university research (13). Recently, organizations such as the Association of University Research Parks have commented on the negative impact of these IRS regulations.
RECENT EFFORTS TO EXPAND PARTNERING OPPORTUNITIES� e rest of the world is making concerted e� orts to close the innovation gap and make their academic systems more at-tractive to industry collaboration. Fred Moavenzadeh, president of the Masdar In-stitute of Science and Technology in Abu Dhabi, United Arab Emirates, has stated that the institute (built with strategic input from the Massachusetts Institute of Tech-nology) will become the premier energy research university in the Middle East. � e Abu Dhabi government has clearly stated its commitment to building a top-tier school and an energy-e� cient emirate—

10
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.orgwww.ScienceTranslationalMedicine.org 29 September 2010 Vol 2 Issue 51 51cm25 3
C O M M E N TA R Y
“ ”and its belief that corporate partnerships will be vital for the school’s success.
� e state of Queensland in Australia has adopted a “Smart State” strategy with a goal of having knowledge-based industries ac-count for 50% of all business activity across Queensland by 2025. To accomplish this aim, the government is making substan-tial investments in world-class research infrastructure in collaboration with higher education and private organizations, facili-tating the exchange of ideas between mem-bers of the research community and sup-porting the development of the Queensland research base by targeting human capital. For the most recent stage (2008–2012), the state government is spending over $23 million to attract and retain some of the brightest minds in science and industry to solve Queensland’s challenges of the future, an additional $25 million for a Health and Medical Research Program (14) to attract world-class clinical researchers to trans-late research into better health services for Queenslanders, and $60 million to support collaborations between Queensland’s re-searchers and industry. � ese investments are part of a well-thought-out strategy for increasing the economic well-being of Queensland and address many of the most pressing R&D challenges.
One U.S. university employing a new approach to collaboration is the Rochester Institute of Technology (RIT), which has created an industry engagement program to complement its traditional approaches for working with industry. � e Corporate R&D program is designed to bring to-gether business and academia to enhance company development goals while giving business access to university expertise and student talent. � e terms of this program provide sponsoring companies ownership of any IP, providing that all parties agree up front. RIT will retain the right to publish and use research results for educational and internal research purposes. It is im-portant to note that this program comple-ments and retains traditional mechanisms and was implemented with the arrival of a new president, Bill Destler, who gave a clear vision for how the university should seek better strategies for partnering with industry.
Some companies have turned to gov-ernment-styled requests for proposals to seek proposals from nonpro� ts and small businesses. � is step is perceived by many companies as a cost-e� ective way to learn
about the assets at these organizations and bring new and innovative approaches for addressing their commercial interests. General Mills recently issued a request for information seeking new ways to develop food products and packaging that support the company’s sustainability goals.
� ese examples are illustrations that complement existing, more traditional ap-proaches and increase the options for part-nering.
A CALL TO ACTIONI o� er a few suggestions for bolstering in-creased university-industry linkages and catalyzing the discovery-to-innovation process.
Recognize that there is less “dating” occurring and a greater emphasis on longer-term relationships. Putting into place a university-industry transaction can be extremely di� cult and time consum-ing. More companies are seeking to work with fewer universities and develop deeper and more comprehensive relationships. � is change lowers the transaction costs and increases the return on investment. Research performers in the nonpro� t sec-tor must develop strategies for establish-ing these long-term, high-value partner-ships that transcend research, education, philanthropic, and service e� orts. In these instances, two parties can work across the entire “partnership continuum” to support each party’s mission (15).
Reduce the uncertainty and make longer-term commitments. Too o� en, companies and universities make public pronouncements that they want to have better relations and that they will make � -nancial and non� nancial investments in ex-panding these partnerships. Unfortunately, external pressures (from Wall Street, state legislatures, boards, or the public) or chang-es in in� uential personnel (provost, dean, or chief technology o� cer) can disrupt well-developed plans by shi� ing priorities or political pressures. Research is a long-term investment and must be supported over a reasonable period of time to yield results. � is anticipated return on investment can be the most di� cult aspect for industry to accept.
Get to know the people you work with. It is very di� cult to work with people you don’t know, like, or trust. � is doesn’t mean that faculty researchers or university administrators need to vacation with their industry collaborators, but having some
level of rapport is exceedingly important if you want to move beyond a single project.
Get buy-in at the right level. Facul-ty researchers run small businesses (their labs), and industry support can be a very important piece of a lab’s funding mosaic. In order to develop the long-term relation-ships that maximize yield, the institutional leadership must recognize this support as important to their organizations. Big phar-ma has made many announcements stat-ing that external alliances are important to its commercial success, and universities are logical partners for these e� orts. Clear statements and actions from the institu-tional leadership (presidents, chief execu-tive o� cers, provosts, and chief research and technology o� cers) regarding the im-portance and value of these linkages will enhance faculty enthusiasm and industry interest in partnerships.
Remove regulatory hurdles. IRS reg-ulations and other regulatory (for example, con� ict of interest) policies can put a large damper on university-industry relations. Reasonable regulations should be encour-aged, and many organizations have called for a review of some of the more trouble-some policies that negatively a� ect these partnerships.
When working collaboratively in thoughtful and meaningful ways, industry, academia, and other research organizations such as independent academic research centers and national labs can advance their goals by leveraging their collective intel-lectual and physical assets. � ese types of high-reward collaborations require work, but the payo� s for all participating parties can be substantial.
REFERENCES AND NOTES 1. “Sparking economic growth: How federally funded uni-
versity research creates innovation, new companies and
jobs.” The Science Coalition, April 2010. www.pagegang-
ster. com/p/VlM3O/ (accessed 6 September 2010).
2. H. Ledford, The future of pharma. Nature News 9 October
2008 (10.1038/news.2008.1161).
3. K. Wilgenbus, R. Hill, A. Warrander, S. Kakkar, E. Steiness,
R. Wessel, What pharma wants. Nat. Biotechnol. 25, 967–
969 (2007).
4. University-Private Sector Research Partnerships in the
Innovation Ecosystem (President’s Council of Advisors
on Science and Technology, 2008). www.nasa.gov/
pdf/404101main_past_research_partnership_report_
BOOK.pdf (accessed 6 September 2010).
5. C. W. Wessner, Ed., “An Assessment of the SBIR Program,
National Research Council” (2008). www.nap.edu/catalog.
php?record_id=11989 (accessed 6 September 2010).
6. “Guiding Principles for University-Industry Endeavors,” Na-
tional Council of University Research Administrators, 2006.
www.ncura.edu/content/regions_and_neighborhoods/

11
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
There are two broad pathways to improv-ing human health. The first is through public health initiatives designed on the basis of behavioral research and enacted through the application of current knowl-edge, public education, and policy change. The second pathway includes the discovery, development, and application of new med-ical products—diagnostic tools, biomarker predictors of disease, and therapeutic drugs, biologics, and devices (Fig. 1). In order for new medical products to enter widespread use, they must clear the hurdles of regula-tory institutions such as the U.S. Food and Drug Administration (FDA) and be ap-proved for insurance reimbursement by entities such as the U.S. Centers for Med-icaid and Medicare Services (CMS). Here, we discuss new approaches to streamlining and thus accelerating knowledge translation with the academic biomedical researcher in mind—many of whom are unfamiliar with
these new initiatives.Various estimates suggest that the aver-
age time for a basic scientific finding to be translated into a new therapy is 16 to 17 years in both the public health and medi-cal arenas (1–3). Mounting costs (clinical trials, drug manufacturing, and regulatory compliance) and declining return on invest-ment in research are also major concerns. The frequently quoted $1 billion to bring a new drug to market has risen to $4 to 5 billion by some estimates (www.forbes.com/sites/matthewherper/2012/02/10/the-truly- staggering-cost-of-inventing-new-drugs). To address this gap, the U.S. President’s Council of Advisors on Science and Tech-nology (PCAST) published a report in Sep-tember 2012 on propelling innovation in the pharmaceutical industry, which comment-ed that “the ecosystem for public health is under significant stress” and that research and development (R&D) productivity is declining (4). Using extensive national and global databases, PCAST demonstrated that investment in R&D by the pharmaceutical industry and the U.S. National Institutes of
Health (NIH) has risen significantly over the past 45 years with no increase in the in-troduction of new molecular entities (NME) or new biological entities (NBE) in the Unit-ed States.
SYSTEMIC BARRIERSOver the past 10 years, there have been de-tailed analyses of the translation process by funding agencies such as the U.S. Nation-al Cancer Institute (NCI) (5). NCI used case studies of 21 discoveries across the spectrum of drugs, biological agents, risk- assessment strategies, medical devices, and lifestyle alterations (5) to identify bottle-necks. Barriers included the hand-off of research from academia to industry, the transfer of manufacturing from research laboratory to good manufacturing practices (GMP), the development of robust disease biomarkers or drug screening assays, and difficulties in early-stage clinical trials be-cause of regulatory issues.
Another recent study conducted by An-gius and colleagues addressed translation barriers from the academic investigator’s perspective (6) by performing a systematic study of 416 publications to identify a cohort of academic investigators who published the results of largely positive, preclinical animal model studies in nerve regeneration; very few of these discoveries had been translat-ed into clinical practice. Similar to the NCI analysis, the study identified as barriers the hand-off of research between academia and industry, preclinical development using GMP, and lack of knowledge about the reg-
Originally published 3 September 2014www.ScienceTranslationalMedicine.org 29 September 2010 Vol 2 Issue 51 51cm25 4
C O M M E N TA R Y
“ ”resources/docs/guidance.pdf (accessed 6 September
2010).
7. Academic R&D Expenditures, FY 2008, NSF 10-311, April
2010. www.nsf.gov/statistics/nsf10311/pdf/nsf10311.pdf
(accessed 6 September 2010).
8. Engineering Research Center Fact Sheet, National Sci-
ence Foundation, 11 June 2009.
9. B. Butkus, Texas A&M’s use of tech commercialization
as basis for awarding tenure gains traction. Biotech
Transfer Week, 6 August 2007. http://2429-genomeweb.
voxcdn.com/biotechtransferweek/texas-am’s-use-tech-
commercialization-basis-awarding-tenure-gains-
traction (accessed 6 September 2010).
10. Contract Accords, Georgia Tech University, University-In-
dustry Demonstration Partnership, 2009. www.otl.gtrc.
gatech.edu/documents/UIDP_Contract_Accords_Book-
let.pdf (accessed 6 September 2010).
11. Responsibility of Applicants for Promoting Objectivity in
Research Which Public Health Service Funding Sought
and Responsible Prospective Contractors, Proposed
Rule, Federal Register 75, No. 98 /21 May, 2010. www.
thefederalregister.com/d.p/2010-05-21-2010-11885
(accessed 6 September 2010).
12. B. Lo, M. J. Field, Eds., Conflict of Interest in Medical
Research, Education, and Practice [Institute of Medi-
cine (US) Committee on Confl ict of Interest in Medical
Research, Education, and Practice, National Academies
Press (US), Washington, DC, 2009]. www.ncbi.nlm.nih.
gov/bookshelf/br.fcgi?book=nap12598 (accessed 5 Sep-
tember 2010).
13. Internal Revenue Bulletin, 2007-29, 16 July 2007. www.
irs.gov/pub/irs-irbs/irb07-29.pdf (accessed 6 September
2010).
14. www.health.qld.gov.au/ohmr/default.asp (accessed 13
September 2010).
15. See chart in (6).
16. National Science Foundation, Division of Science Re-
sources Statistics, National Patterns of R&D Resources.
Available at www.nsf.gov/statistics/seind10/fi gures.
htm#c4; see fi gure 4-3 (accessed 17 September 2010).
17. Organisation for Economic Co-operation and Develop-
ment, Main Science and Technology Indicators (2009/1).
Available at www.nsf.gov/statistics/seind10/fi gures.
htm#c4; see fi gure 4-19 (accessed 17 September 2010).
18. Disclaimer: The opinions expressed are those of the
author and not necessarily those of Government-Uni-
versity-Industry Research Roundtable or the National
Academies. Competing interests: The author declares
that he has no competing interests.
Citation: A. M. Boccanfuso, Why university-industry partner-
ships matter. Sci. Transl. Med. 2, 51cm25 (2010).
10.1126/scitranslmed.3001066
P O L I C Y
Breaking Down Translation Barriers: Investigator’s PerspectiveNathan P. Staff,* Bethany Kinseth Runge, Anthony J. Windebank
From our perspective as biomedical scientists, we analyze neww initiatives from U.S. federal regulatory and funding agencies aimed at accelerating the process of clinical translation.
Center for Regenerative Medicine and Department of Neurology, Mayo Clinic College of Medicine, Rochester, MN 55905, USA.*Corresponding author. E-mail: [email protected]

12
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 3 September 2014 Vol 6 Issue 252 252cm7 2
C O M M E N TA R Y
“ ”FDA staf and guest lecturers to augment the training of current and future clinical in-vestigators. T e goals of the training course include but are not limited to “foster[ing] a cadre of clinical investigators with knowl-edge, experience, and commitment to in-vestigational medicine”; “promot[ing] com-munication between clinical investigators and FDA”; and “[enhancing] investigators’understanding of FDA’s role in experimen-tal medicine” (8). T e goal of strengthening communication between investigators and regulatory agencies has been stressed by others (9). T e third goal, directed toward improving product manufacturing, is be-ing addressed by FDA’s recent introduction of a new Investigational Device Exemption (IDE) process for early clinical studies of feasibility for medical devices, including certain f rst-in-human studies (10). T is new process allows for small clinical trials to start before product design is f nalized. T e way this process works is to permit just-in-time (JIT) testing wherein certain nonclinical testing is evaluated in collabora-tion with FDA and completed during or af-ter the initiation of a study. In addition, this new process allows for f exible device and clinical protocol modif cations during the study. T ese increased risks are balanced by requiring investigators to outline enhanced risk-mitigation strategies and patient-protection measures (10). T e IDE process is intended to be a more iterative and inter-active approach toward f nal approval.
Funding. Agencies that provide funding can drive the process of translation with two tools: funding to support acceleration and peer review of applications for funding. A major shif in this direction began in Sep-tember 2004 when the then–NIH director published the NIH Roadmap for Medical Re-search. T e Roadmap put forward a series of themes, implementation groups, and initia-tives aimed at redef ning the ways in which medical research is conducted and, ulti-mately, how scientif c research leads to im-provements in human health (11). A major pathway for implementation of the Roadmapwas through the Clinical and Translational Science Awards (CTSAs) (www.ctsacentral.org). A prime example of a CTSA initia-tive was the inauguration of a national pre-doctoral clinical and translational science meeting that brings together research train-ees at the professional (M.D., D.D.S., D.P.T., Pharm.D.) and graduate school (Ph.D.) levels to present and discuss their research. T e emphasis of these annual meetings has
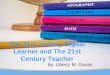
Fig. 1. More talk, more action. (A) Shown is a simplifi ed scheme of U.S. biomedical discovery re-search and regulatory science processes. Funding comes from three sources—government agen-cies (federal and state), nonprofi t institutions (private philanthropies and disease-focused founda-tions), and the private sector (investment from venture capital and industry). R&D is carried out in both industry (pharmaceutical and medical technology companies) and academic centers, which also conduct increasing amounts of public health and new-product implementation research that require policy changes rather than FDA approval. Over the past 50 years, the relative return on biomedical research investment has declined (as measured by FDA submissions and product ap-provals) and the rate of knowledge transfer (translation) from discovery to improvements in clinical medicine has not improved. Bottlenecks include lack of knowledge in academia about the regu-latory process; the essential requirement for acceptance and coverage of a new product by the CMS in order for it to be widely implemented; and the miniscule amount of prospective planning among academia, industry, FDA, and CMS. (B) Strengthening of communication pathways—most of which converge on individual institutions and investigators—can accelerate the pace of transla-tion. Federal funding agencies and FDA also should exchange information about strategic priori-ties and required regulatory expertise in the funding review and regulatory approval processes.
Funding sources
Federal and state
sources
(NIH, DOD, NSF)
Nonprofit
foundations and
personal
philanthropy
Private capital
investment
(pharma, biotech,
startups, etc.)
Process of research
and discoveryRegulatory policy
Policy change
Improved health
of the
community
Approval to
conduct
human trials
(IND, IDE)
Approval to
market
Approval
FDA
CMS
Public health
Public health and
implementation
research
Academia
(universities,
medical centers,
institutes)
Pharma
(pharmaceutical
and device
companies)
Funding sources
Federal and state
sources
(NIH, DOD, NSF)
Nonprofit
foundations and
personal
philanthropy
Private capital
investment
(pharma, biotech,
startups, etc.)
Process of research
and discoveryRegulatory policy
Policy change
Improved health
of the
communityFDA
CMS
Public health
Public health and
implementation
research
Academia
(universities,
medical centers,
institutes)
Pharma
(pharmaceutical
and device
companies)
A
B
CR
ED
IT: H
. M
CD
ON
ALD
/SC
IEN
CE
TR
AN
SLA
TIO
NA
L M
ED
ICIN
E
www.ScienceTranslationalMedicine.org 3 September 2014 Vol 6 Issue 252 252cm7 2
C O M M E N TA R Y
“ ”FDA staf and guest lecturers to augment the training of current and future clinical in-vestigators. T e goals of the training course include but are not limited to “foster[ing] a cadre of clinical investigators with knowl-edge, experience, and commitment to in-vestigational medicine”; “promot[ing] com-munication between clinical investigators and FDA”; and “[enhancing] investigators’understanding of FDA’s role in experimen-tal medicine” (8). T e goal of strengthening communication between investigators and regulatory agencies has been stressed by others (9). T e third goal, directed toward improving product manufacturing, is be-ing addressed by FDA’s recent introduction of a new Investigational Device Exemption (IDE) process for early clinical studies of feasibility for medical devices, including certain f rst-in-human studies (10). T is new process allows for small clinical trials to start before product design is f nalized. T e way this process works is to permit just-in-time (JIT) testing wherein certain nonclinical testing is evaluated in collabora-tion with FDA and completed during or af-ter the initiation of a study. In addition, this new process allows for f exible device and clinical protocol modif cations during the study. T ese increased risks are balanced by requiring investigators to outline enhanced risk-mitigation strategies and patient-protection measures (10). T e IDE process is intended to be a more iterative and inter-active approach toward f nal approval.
Funding. Agencies that provide funding can drive the process of translation with two tools: funding to support acceleration and peer review of applications for funding. A major shif in this direction began in Sep-tember 2004 when the then–NIH director published the NIH Roadmap for Medical Re-search. T e Roadmap put forward a series of themes, implementation groups, and initia-tives aimed at redef ning the ways in which medical research is conducted and, ulti-mately, how scientif c research leads to im-provements in human health (11). A major pathway for implementation of the Roadmapwas through the Clinical and Translational Science Awards (CTSAs) (www.ctsacentral.org). A prime example of a CTSA initia-tive was the inauguration of a national pre-doctoral clinical and translational science meeting that brings together research train-ees at the professional (M.D., D.D.S., D.P.T., Pharm.D.) and graduate school (Ph.D.) levels to present and discuss their research. T e emphasis of these annual meetings has
Fig. 1. More talk, more action. (A) Shown is a simplifi ed scheme of U.S. biomedical discovery re-search and regulatory science processes. Funding comes from three sources—government agen-cies (federal and state), nonprofi t institutions (private philanthropies and disease-focused founda-tions), and the private sector (investment from venture capital and industry). R&D is carried out in both industry (pharmaceutical and medical technology companies) and academic centers, which also conduct increasing amounts of public health and new-product implementation research that require policy changes rather than FDA approval. Over the past 50 years, the relative return on biomedical research investment has declined (as measured by FDA submissions and product ap-provals) and the rate of knowledge transfer (translation) from discovery to improvements in clinical medicine has not improved. Bottlenecks include lack of knowledge in academia about the regu-latory process; the essential requirement for acceptance and coverage of a new product by the CMS in order for it to be widely implemented; and the miniscule amount of prospective planning among academia, industry, FDA, and CMS. (B) Strengthening of communication pathways—most of which converge on individual institutions and investigators—can accelerate the pace of transla-tion. Federal funding agencies and FDA also should exchange information about strategic priori-ties and required regulatory expertise in the funding review and regulatory approval processes.
Funding sources
Federal and state
sources
(NIH, DOD, NSF)
Nonprofit
foundations and
personal
philanthropy
Private capital
investment
(pharma, biotech,
startups, etc.)
Process of research
and discoveryRegulatory policy
Policy change
Improved health
of the
community
Approval to
conduct
human trials
(IND, IDE)
Approval to
market
Approval
FDA
CMS
Public health
Public health and
implementation
research
Academia
(universities,
medical centers,
institutes)
Pharma
(pharmaceutical
and device
companies)
Funding sources
Federal and state
sources
(NIH, DOD, NSF)
Nonprofit
foundations and
personal
philanthropy
Private capital
investment
(pharma, biotech,
startups, etc.)
Process of research
and discoveryRegulatory policy
Policy change
Improved health
of the
communityFDA
CMS
Public health
Public health and
implementation
research
Academia
(universities,
medical centers,
institutes)
Pharma
(pharmaceutical
and device
companies)
A
B
CR
ED
IT: H
. M
CD
ON
ALD
/SC
IEN
CE
TR
AN
SLA
TIO
NA
L M
ED
ICIN
E
ulatory approval process among academic scientists. In addition, a significant number of investigators expressed the opinion that the end product of their research was pub-lication and that they expected a company to take the knowledge and translate it into a product.
STRATEGIES TO DRIVE TRANSLATIONFDA. The FDA collected input from all seg-ments of the biomedical research enterprise that resulted in the publication of a strate-gic plan for advancing translation (August 2011) that introduced the concept of regula-tory science and set out eight priority areas designed to “allow the agency both to meet today’s public health needs and to be fully prepared for the challenges and opportu-nities of tomorrow” (7). The plan also rec-ognizes that FDA has a pivotal role in the translation process and that the regulatory segment needs improvement. The plan em-phasizes the primary role of the agency in maintaining safety and expressly states that its goal is not to fundamentally change the regulatory process.
The eight goals are to (i) modernize toxi-cology to enhance product safety; (ii) stim-ulate innovation in clinical evaluations and personalized medicine to improve product development and patient outcomes; (iii) support new approaches to improve prod-uct manufacturing and quality; (iv) en-sure FDA readiness to evaluate innovative emerging technologies; (v) harness diverse data through information sciences to im-prove health outcomes; (vi) implement a new prevention-focused food safety system to protect public health; (vii) facilitate devel-opment of medical countermeasures to pro-tect against threats to U.S. and global health and security; and (viii) strengthen social and behavioral sciences to help consumers and professionals make informed decisions about regulated products.
Although the plan describes detailed ap-proaches for achieving these goals, the im-plementation processes, milestones, time-lines, and resources are not clearly defined. In addition—and probably more important-ly—although biomedical thought leaders outside of FDA provided major input, the outcome of this planning process is gener-ally unknown to the majority of academic scientists. In a small survey of leaders in the biomedical translation field, only 2 of 11 were aware of the plan or any of the pro-posed outputs. One investigator who knew about the plan commented that “it was very helpful in formulating our regulatory strat-

13
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
egy for the specific technology being devel-oped.” This comment suggests a need for increased marketing and dissemination of the plan.
The second goal centers on clinical tri-als—their designs, end points, use of bio-markers, and the use of “virtual physio-logical patients”—that is, device testing that uses robust computer models of hu-man anatomy. Clinical trial innovation is a ripe area for strong collaboration between FDA and academic investigators. To this end, FDA now offers a three-day training course led by FDA staff and guest lecturers to augment the training of current and fu-ture clinical investigators. The goals of the training course include but are not limited to “foster[ing] a cadre of clinical investiga-tors with knowledge, experience, and com-mitment to investigational medicine”; “pro-mot[ing] communication between clinical investigators and FDA”; and “[enhancing] investigators’ understanding of FDA’s role in experimental medicine” (8). The goal of strengthening communication between in-vestigators and regulatory agencies has been stressed by others (9). The third goal, direct-ed toward improving product manufactur-ing, is being addressed by FDA’s recent in-troduction of a new Investigational Device Exemption (IDE) process for early clinical studies of feasibility for medical devices, in-cluding certain first-in-human studies (10). This new process allows for small clinical trials to start before product design is final-ized. The way this process works is to permit just-in-time (JIT) testing wherein certain nonclinical testing is evaluated in collabora-tion with FDA and completed during or af-ter the initiation of a study. In addition, this new process allows for flexible device and clinical protocol modifications during the study. These increased risks are balanced by requiring investigators to outline enhanced risk-mitigation strategies and patient- protection measures (10). The IDE process is intended to be a more iterative and inter-active approach toward final approval.Funding. Agencies that provide funding
can drive the process of translation with two tools: funding to support acceleration and peer review of applications for funding. A major shift in this direction began in Sep-tember 2004 when the then–NIH director published the NIH Roadmap for Medical Research. The Roadmap put forward a se-ries of themes, implementation groups, and initiatives aimed at redefining the ways in which medical research is conducted and, ultimately, how scientific research leads
to improvements in human health (11). A major pathway for implementation of the Roadmap was through the Clinical and Translational Science Awards (CTSAs) (www.ctsacentral.org). A prime example of a CTSA initiative was the inauguration of a national predoctoral clinical and transla-tional science meeting that brings together research trainees at the professional (M.D., D.D.S., D.P.T., Pharm.D.) and graduate school (Ph.D.) levels to present and discuss their research. The emphasis of these annual meetings has been on “articulating the path to translation.” From the beginning of their research training careers, these future inves-tigators should be able to describe how their research will be taken through the next steps in the translational pathway. The ability to articulate future steps will inform the design of their current experiments. The Institute of Medicine (IOM) recently endorsed the CTSA program in a report (12) that reviews the program’s mission and strategic goals. The IOM committee concluded that “the CTSA program is contributing significantly to advancing clinical and translational re-search” and emphasized that “[t]he program must continue to emphasize innovative training, mentoring, and education to better prepare the next generation of researchers.”
The shift toward translation in the context of limited resources has evoked concern in the academic biomedical research commu-nity centered on fundamental discovery re-search. Although basic science discoveries through implementation of new therapies are essential for improving clinical medi-cine, the value of increasing investments at various points in the translational pathway has not been rigorously evaluated. The 17- year life cycle from bench to bedside exceeds the 5- to 10-year terms of NIH directors and many other national scientific leaders. Thus the process of change tends to be influenced by preconception rather than data. Reliable markers of productive change in the transla-tion process are needed that resemble qual-ified biomarkers for disease progression, a concept familiar to physician-scientists. Thus investigators must collaborate with program evaluators to develop robust mark-ers of success for educational, funding, and R&D programs.
Funding is probably the most powerful tool for influencing the course of biomedical research. Virtually all academic investigators and programs require extramural funding, and strong arguments have been made for supporting fundamental discovery research to illuminate disease mechanisms that will
pinpoint new therapeutic targets. Clinician- scientists and translational scientists pro-pose research projects directed toward dis-covering and developing disease-specific therapies; however, these research projects rarely are judged on the basis of their like-lihood of success in developing a new ther-apy. In the United States, most biomedical research funding to the academic commu-nity is awarded through a rigorous peer- review process to ensure that strong science and new ideas are supported. However, this selection process also guarantees that major changes in the biomedical research process will not occur, as the grant reviewers are all rooted in the status quo. Study section and scientific review board members often have little personal experience with the process of translation and may be poorly equipped to judge the likelihood that a project will pro-duce translatable knowledge. The responsi-bility for raising this discussion is often in the hands of the administrative Scientific Review Officer, whose opinion may not car-ry weight in the discussion of the merits of the “hard science.” Credible scientists with personal experience in translation of knowl-edge to product should be incorporated into review bodies.
An example in which NIH has provided direct funding to aid translation is the Net-work for Excellence in Neuroscience Clini-cal Trials (NeuroNEXT) program (13, 14). This is a National Institute of Neurological Disorders and Strokes (NINDS) initiative with the goal of accelerating phase 2 clini-cal trials and biomarker validation studies for the treatment of neurological diseases by providing funding and a consortium that supports clinical investigators in academia, private foundations, and industry. The con-sortium includes multiple clinical sites, a clinical coordinating center, and a data co-ordinating center, made available to assist investigators with accepted proposals to conduct their clinical studies. NeuroNEXT is involved in all stages of the clinical trial process, starting with the conceptual stage. To date, it has funded phase 2 projects on spinal muscular atrophy, multiple sclerosis, myasthenia gravis, and stroke.
Another funding strategy to improve translation began in 2010 with a joint initia-tive between FDA and NIH (15) that focuses on combining translational science and reg-ulatory science principles to speed clinical translation. Although this is not the first time the two agencies have collaborated, the fact that this effort was designed to improve the regulatory review process made this par-

14
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
ticular joint effort unique. The initiative has since provided significant grant support for cooperative grants (U01) throughout the country and established Centers of Excel-lence in Regulatory Science and Innovation at the University of Maryland and George-town University (in 2011).
U.S. federal Small Business Innovation Research (SBIR) and Small Business Tech-nology Transfer (STTR) grants focus on commercialization of translated medical technology and fund small U.S. business-es that might otherwise not attract private investors. Many of the companies that use the SBIR funding mechanism are start-up companies associated with academic cen-ters, and the STTR program requires an ac-ademic center partner. Congress has man-dated that 11 federal agencies that support research (including NIH) allocate 2.5% of their budget for SBIR and 0.3% for STTR (totaling $2.35 billion in 2010). In 2012, these percentages were targeted to rise to 3.2% and 0.45% for SBIR and STTR in 2017. An average of 1163 new awards were made yearly over the last 10 years. The funding rate for these programs has averaged 21.2% of applications, which is a little higher than the overall average at NIH (http://report.nih.gov/catalog.aspx).Reimbursement. A federal agency within
the U.S. Department of Health and Human Services, CMS is responsible for administer-ing Medicare and Medicaid and determines whether drugs, devices, or biologics will be paid for by these federal health insurance programs. Most private health insurance companies follow payment coverage recom-mendations set forth by CMS. The process to determine whether CMS will provide coverage for a medical procedure can take years and, therefore, has a great impact on biomedical research. Increased collabora-tion between funding (NIH) and regulatory agencies (FDA and CMS) could focus fund-ing review processes so that new preclinical projects with an unclear pathway to imple-mentation could be discouraged and those with a clearly articulated pathway through regulatory approval could be encouraged. Currently, there is virtually no commu-nication between academic clinician- investigators and CMS. Many laboratory- based investigators are not even aware of CMS’s role despite its importance in the trans-lation process.
CMS has aided clinical translation by en-acting changes designed to increase enroll-ment of Medicare and Medicaid patients in clinical trials. Coverage by the CMS for pa-
tient care costs associated with clinical trials is critical for patient enrollment in clinical trials and for new discoveries to be widely implemented. An executive order (referred to as the 2000 Clinical Trial Policy) signed by President Bill Clinton on 7 June 2000 authorized Medicare payments to cover routine costs and costs related to medical complications that occur during clinical tri-al participation (16). More senior patients may be able to enroll in clinical trials when the financial burden associated with partici-pation is reduced by CMS coverage. An NCI study was able to make this conclusion after assessing the percentage of seniors with can-cer who enrolled in a cancer therapy–related clinical trial before and after the 2000 execu-tive memorandum (17).Clinician-investigators. The clinician-
investigator needs to adopt a translation-centered research perspective in order to successfully accelerate translation. Research destined for translation must be designed from the outset in a way that ensures that ex-perimental data are gathered such that they will be suitable for use in future submissions to the FDA. This approach requires a sub-stantially expanded two-way knowledge- transfer highway between the community of academic investigators and FDA, who share the responsibility for expanding this knowl-edge exchange path. Two examples in which this strong two-way communication has yielded advances in the regulatory approval process are in the areas of stem-cell/regen-erative medicine and tissue engineering.
Amyotrophic lateral sclerosis (ALS, Lou Gehrig’s disease) is a uniformly fatal neu-rodegenerative condition that leads to pro-gressive loss of muscle function and death within 2 to 3 years after symptom onset. De-spite 50 years of intensive, mechanism-based research, no effective treatments exist. There was great excitement in 1994 when Gurney and colleagues discovered that a mouse ex-pressing a mutation associated with human familial ALS developed a motor neuron disease (18). The hope was that this genet-ic model would yield a mechanistic under-standing of the disease and provide a system for assessing the efficacy of potential ther-apies. Unfortunately, many treatments that were successful in treating the mouse did not translate to humans (18–20).
With the advent of putative stem cell– based therapies for neurodegenerative dis-eases, investigators began to ask whether autologous adipose-derived mesenchymal stem cells (MSCs) that were genetically modified to secrete biologics might be effec-
tive vehicles for the delivery of neuroprotec-tive molecules across the blood-brain bar-rier. But this approach would involve first developing a treatment platform (unmodi-fied MSCs) in patients to deliver a therapy that had not yet been tested in a preclinical model.
Investigators entered advisory discus-sions with staff at the FDA Center for Bi-ologics Evaluation and Research (CBER). Great attention was paid to preclinical stud-ies of safety, with less emphasis on efficacy for a disease in which any step forward is important progress. The ethical justification accepted by FDA and institutional review boards for testing the treatment platform in patients was that the unmodified MSCs de-liver a wide range of neuroprotective mole-cules that may have efficacy on their own. In addition, if this delivery route were demon-strated to be safe in patients, the treatment platform might be useful for delivering neu-roprotective molecules not just for treatment of ALS but also for other brain disorders such as Parkinson’s or Alzheimer’s disease. FDA approved the strategy in a single- patient study in 2009 [investigational new drug application (IND) 13851, national clin-ical trial number (NCT) 01142856)] and an ongoing dose-escalation safety trial in 2011 (IND 14788, NCT01609283). This example illustrates how communication between ac-ademic investigators and regulatory scien-tists can reduce barriers to translation.
An example of a U.S. federal funding mechanism that drives clinical research to-ward product development is the Armed Forces Institute of Regenerative Medicine. In 2008, the U.S. Department of Defense provided funding for this initiative in re-sponse to the large numbers of life-altering injuries such as limb destruction and ex-tensive burns suffered by young military survivors returning from recent theaters of war. The goal of the funding initiative was to bring together teams of investigators from a broad range of civilian institutions to focus on injuries that might benefit from tissue-engineering solutions, such as critical defects in nerve, bone, muscle, tendon, skin, and other organs, with a focus on limb in-jury.
One of the features of the funding was that it came with a contract that specified timelines and deliverables monitored on an annual basis, with funding expanding or contracting depending on the investiga-tors’ success in meeting milestones. This is a foreign concept and mode of operation for academic investigators; but in the first 4

15
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
years, 12 clinical trials, 4 INDs, and 3 IDEs were generated by investigators within the consortium. This project demonstrates that with some sacrifice of academic flexibility, it is possible for a federal funding agency to speed biomedical research translation, at least in the short term.
Academic investigators who choose to pursue commercialization of a product face many singular challenges. Consider-ing intellectual property (IP) early in the translational process is crucial to future commercialization success. This process can be facilitated by technology offices within academic centers. Once IP is established, an investigator can pursue commercialization either independently by establishing a start-up company or via a licensing agreement with an established or privately held compa-ny. However, challenges arise when assem-bling a team to build and run a new compa-ny and when attempting to procure funding. Also, agreements on the legal relationships among an investigator, the academic insti-tution, and an established company can be a long-drawn-out process.
A successful strategy that we have used at the Mayo Clinic is to create a new position called “translational integrator.” This pro-fessional serves as a project manager whose responsibility is to facilitate negotiations between clinician-investigators, regulato-ry agencies, funding agencies, commercial sponsors, and contracting suppliers. Mak-ing this the “day job” for an appropriately trained person has transformed processes that used to take months or years into ones that can be accomplished in weeks.
UNMET MEDICAL NEEDThere is an urgent need for evaluation and change in the process of therapy approval and translation at the very highest levels. Strategic plans forged at agencies includ-ing FDA, CMS, DOD, and NIH will have difficulty inffluencing change across ad-ministrative barriers. At the highest level, the PCAST report (4) identified two of the opportunities that directly address issues discussed here: Innovators require greater clarity about regulatory pathways for inno-vative products and approaches, and inno-vators require greater consistency, efficien-cy, and communication with respect to their individual drug applications. However, the report may not engender political action at a time when other health care delivery poli-cies are the subject of intense debate.
However, members of the biomedical re-search community, individual institutions,
and funding agencies can still take actions that responsibly speed the translation of biomedical discoveries to improvements in patient care. The ALS and AFIRM examples demonstrate that change is possible.
Two avenues to consider: (i) Individual institutions and investigators should take responsibility for learning about and under-standing the process of translation from dis-covery to application. They should use this knowledge to inform, from the beginning, the design of experiments, studies, and clin-ical trials. The vehicle for disseminating this knowledge to students, trainees, and inves-tigators is in place at 60 major institutions that received CTSAs from NIH. Evaluation of the success of awardees should hinge on productivity related to the discovery of new diagnostics or therapies or on other mark-ers that indicate improvements in human health and not only on the traditional mark-ers of grants and publications. (ii) Agencies that fund research that has expressed trans-lational or preclinical goals should adjudi-cate whether proposals clearly articulate a path to translation. This requires the incor-poration in study sections of reviewers, such as regulatory scientists, who can critically evaluate the impact of a proposal using this criterion.
Science moves forward because of the work of individual scientists. In the process of bringing new therapies to communities, the biomedical investigator can play a crit-ical role in accelerating translation within the existing framework. Institutions and funding agencies can facilitate this process by providing knowledge and incentivized direction to the individual research team.
REFERENCES AND NOTES1. R. C. Brownson, M. W. Kreuter, B. A. Arrington, W. R. True,
Translating scientific discoveries into public health ac-tion: How can schools of public health move us forward? Public Health Rep. 121, 97–103 (2006).
2. J. M. Westfall, J. Mold, L. Fagnan, Practice-based re-search—“Blue Highways” on the NIH roadmap. JAMA 297, 403–406 (2007).
3. E. A. Balas, S. A. Boren, Managing clinical knowledge for healthcare improvement. Yearbook of Medical Informat-ics 2000. 2000, 65–70 (2000); www.ihi.org/resources/ Pages/Publications/Managingclinicalknowledgefor-healthcareimprovement. aspx.
4. PCAST, “Report to the President on Propelling Innovation in Drug Discovery, Development, and Evaluation” (Execu-tive Office of the President, Washington, DC, 2012); www.whitehouse.gov/sites/default/files/microsites/ostp/pcast-fda-final.pdf.
5. Report of the Translational Research Working Group of the National Cancer Advisory Board, “Transforming Translation—Harnessing Discovery for Patient and Public Benefit” (National Cancer Institute, Bethesda, MD, 2007); www.ida.org/~/media/Corporate/Files/ Publications/STPIPubs/transformingtranslationfinalre-port. ashx.
6. D. Angius, H. Wang, R. J. Spinner, Y. Gutierrez-Cotto, M. J. Yaszemski, A. J. Windebank, A systematic review of
animal models used to study nerve regeneration in tissue-engineered scaffolds. Biomaterials 33, 8034–8039 (2012).
7. U.S. Food and Drug Administration, “Advancing Reg-ulatory Science at FDA” (2011); www.fda.gov/down-loads/scienceresearch/specialtopics/regulatoryscience/ ucm268225.pdf.
8. U.S. Food and Drug Administration, Clinical investigator training course. Fed. Regist. 76, 45577–45578; www.gpo.gov/fdsys/pkg/FR-2011-07-29/html/2011-19149.htm.
9. S. Olson, A. B. Claiborne, Accelerating the development of new drugs and diagnostics: Maximizing the impact of the cures acceleration network: Workshop summary (National Academies Press, Washington, DC, 2012), p. 115.
10. U.S. Department of Health and Human Services and FDA, IDEs for early feasibility medical device clinical studies, including certain first-in-human studies (2013); www.fda.gov/downloads/medicaldevices/deviceregulation-andguidance/guidancedocuments/ucm279103.pdf.
11. E. Zerhouni, Medicine. The NIH Roadmap. Science 302, 63–72 (2003).
12. Committee to Review the Clinical and Translational Sci-ence Awards Program at the National Center for Advanc-ing Translational Sciences, “The CTSA Program at NIH. Opportunities for Advancing Clinical and Translational Research” (Institute of Medicine, Washington DC, 2013); www.iom.edu/~/media/Files/Report%20 Files/2013/ CTSA-Review/CTSA-Review-RB.pdf.
13. National Institutes of Health, Neuro NEXT. The NEXT generation of neurologic treatments. NIH-Network for Excellence in Neuroscience Clinical Trials (2013); www.ninds.nih.gov/news_and_events/proceed-ings/20101217-NEXT.htm.
14. The Lancet Neurology, NeuroNEXT: Accelerating drug development in neurology. Lancet Neurol. 11, 119 (2012).
15. U.S. Food and Drug Administration, NIH and FDA an-nounce collaborative initiative to fast-track innova-tions to the public (2010); www.nih.gov/news/health/feb2010/od-24.htm.
16. Center for Medicare and Medicaid Services, Medicare Clinical Trial Policies (2013); www.cms.gov/Medicare/Coverage/ClinicalTrialPolicies.
17. Medicare Advantage: Reforms needed to ensure access to clinical trials. J. Oncol. Pract. 5, 144–145 (2009).
18. M. E. Gurney, H. Pu, A. Y. Chiu, M. C. Dal Canto, C. Y. Pol-chow, D. D. Alexander, J. Caliendo, A. Hentati, Y. W. Kwon, H.-X. Deng, W. Chen, P. Zhai, R. L. Sufit, T. Siddique, Mo-tor neuron degeneration in mice that express a human Cu,Zn superoxide dismutase mutation. Science 264, 1772–1775 (1994).
19. H. B. van der Worp, D. W. Howells, E. S. Sena, M. J. Porritt, S. Rewell, V. O’Collins, M. R. Macleod, Can animal models of disease reliably inform human studies? PLOS Med. 7, e1000245 (2010).
20. E. J. Sorenson, A. J. Windbank, J. N. Mandrekar, W. R. Bamlet, S. H. Appel, C. Armon, P. E. Barkhaus, P. Bosch, K. Boylan, W. S. David, E. Feldman, J. Glass, L. Gutmann, J. Katz, W. King, C. A. Luciano, L. F. McCluskey, S. Nash, D. S. Newman, R. M. Pascuzzi, E. Pioro, L. J. Sams, S. Scelsa, E. P. Simpson, S. H. Subramony, E. Tiryaki, C. A. Thornton, Subcutaneous IGF-1 is not beneficial in 2-year ALS trial. Neurology 71, 1770–1775 (2008).
10.1126/scitranslmed.3008252
Citation: N. P. Staff , B. K. Runge, A. J. Windebank, Breaking down translation barriers: Investigator’s perspective. Sci. Transl. Med. 6, 252cm7 (2014).

16
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.orgOriginally published 26 November 2014
www.ScienceTranslationalMedicine.org 26 November 2014 Vol 6 Issue 264 264cm12 1
C O M M E N TA R Y
“ ”
T e pace of basic discoveries in all areas of biomedicine is accelerating. Yet, translation of this knowledge into concrete improve-ments in clinical medicine continues to lag behind the pace of discovery. Stakeholders from around the world who seek successful biomedical translation met in May 2014 in Berlin, Germany, to identify barriers and redef ne translation by critically analyz-ing characteristics of successful endeavors. T e charge of this meeting was unique: to focus not on research data but instead on factors that have contributed to or hindered the successful translation of a variety of methods, technologies, drugs, or devices toward patient benef t. Together, the speak-ers presented dif erent stories that, while varied, were consistent in emphasizing that improved translation of basic research to clinical benef t can happen only with wide-spread changes in mindset.
Here, we share key factors that could alter scientif c, political, and industry per-spectives on translation. Only through new ways of thinking and a new set of attitudes will the biomedical community more ef-fectively initiate—and sustain—technology translation. T is Commentary is the f rst
in a collection of articles in Science Trans-lational Medicine that emphasize the most important themes from Translate! and rep-resents the participant consensus statement on challenges of changing the stakeholder mindset. T ree articles in future issues will elaborate on major factors raised herein: specif cally, infrastructure, funding, and derisking issues in biomedical technology translation to clinical use.
WHAT IS “TRANSLATION”? (AND WHO
DOES IT?)
Translation is not the rebranding of old-style approaches that tentatively link basic biomedical research results to possible or potential clinical utility. It is also not simply the pairing of a clinical investigator with a basic researcher. Translation is innovation with a def ned, specif c clinical practicality and active engagement toward achieving that critical end goal of reduction to practice—a def nition that highlights a mindset in which clinical utility, beyond scientif c or medical concepts, is key to the process. T e business sector of en def nes innovation as “value-cre-ating novelty.” For industry, new biomedical concepts and early-stage products are con-
sidered “innovative applications” when they create new health care value and impact. T is is of en def ned by the clinical market, not in research publications. Academic circles de-f ne innovation as creative novelty—science or technology that has not yet been reported regardless of its application or commercial impact. T ese disparate views are of en not reconciled in current discussions of biomedi-cal translation.
Ef ective translational biomedical re-search addresses a clear clinical need and is typically based on a strong understanding of underlying biological mechanisms. To reach such quality in translation, an itera-tive approach [either bench to bed to bench or bed (clinical need) to bench to bed and back] is of en necessary. Such a strategy goes beyond “reverse translation” and in-cludes f rst-in-human study experiences, followed by more basic research to decipher the actual mechanisms behind the clinical need and the therapeutic results in humans. Such reciprocal translation allows substan-tial derisking for new therapies. Merely pointing to a distant goal of translation is not the same as actively building a concep-tual, scientif c, and then practical bridge to reach that goal. By insisting on improved translational ef ciency, technical expert communities must take great care not to subvert or confuse basic and translational principles among experts or society at large.
Don’t abandon the basics. Basic bio-medical research drives the discovery en-gine of developed world economies and is essential to gain new knowledge about hu-man biology for next steps in research and technology development. Although basic research may lead to innovative products, it is in itself insuf cient for direct transla-tion. Only select basic science discoveries are appropriate for translational consid-eration. An imaginative, large net must be cast within the research community to best
W H I T E P A P E R
Changing the Mindset in Life Sciences Toward Translation: A Consensus
Georg N. Duda,1,2* David W. Grainger,3 Megan L. Frisk,4
Leena Bruckner-Tuderman,5,6 Andrew Carr,7 Ulrich Dirnagl,8,9
Karl Max Einhäupl,10 Stephen Gottschalk,11 Elliott Gruskin,12
Christoph Huber,13 Carl H. June,14 David J. Mooney,15,16 Ernst Th. Rietschel,17
Georg Schütte,18 Werner Seeger,19,20 Molly M. Stevens,21,22 Robert Urban,23
Alex Veldman,24,25,26 Günther Wess,27 Hans-Dieter Volk1,28
Participants at the recent Translate! 2014 meeting in Berlin, Germany, reached a consensus on the rate-limiting factor for advancing translational medicine.
*Corresponding author. E-mail: [email protected]
1Berlin-Brandenburg Center for Regenerative Therapies, Charité–Universitätsmedizin Berlin, Germany. 2Julius Wolf Institut, Charité–Universitätsmedizin Berlin, Germany. 3Depart-ment of Pharmaceutics and Pharmaceutical Chemistry, Health Sciences, University of Utah, Salt Lake City, UT 84112, USA. 4Science Translational Medicine, American Association for the Advancement of Science (AAAS), Washington, DC 20005, USA. 5Department of Dermatology, Medical Center–University of Freiburg, 79104 Freiburg, Germany. 6German Research Foundation (DFG), Bonn, Germany. 7NIHR Biomedical Research Unit, Botnar Research Centre, Nuf eld Department of Orthopaedics Rheumatology and Musculoskeletal Sciences, University of Oxford, UK. 8Center for Stroke Research, Charité–Universitätsmedizin Berlin, Germany. 9Department of Experimental Neurology, Charite–Universitätsmedizin Berlin, Germany. 10Chairman of the Executive Board, Charité–Universitätsmedizin Berlin, Charitéplatz 1, 10117 Berlin, Germany. 11Center for Cell and Gene Therapy, Texas Children’s Hospital, Houston Methodist Hospital, Baylor College of Medicine, Houston, TX 77030, USA. 12DePuy Synthes Biomaterials, 1302 Wrights Lane East, West Chester, PA 19380, USA. 13Translational Oncology (TRON), Mainz University Medical Center, Germany. 14Department of Pathology and Laboratory Medicine, Perelman School of Medicine, Philadelphia, PA 19104, USA. 15School of Engineering & Applied Sciences, Harvard University, Cambridge, MA, USA. 16Wyss Institute, Center for Life Science Boston Bldg., Boston, MA 02115, USA. 17Berlin Institute of Health, Luisenstr. 56, 10117 Berlin, Germany. 18Federal Ministry of Education and Research, D-53175 Bonn, Germany. 19Department of Pneumologie, Universities of Giessen & Marburg Lung Center (UGMLC), 35392 Giessen, Germany. 20German Center for Lung Research (DZL), 35392 Giessen, Germany. 21Department of Materials, Impe-rial College London, London, SW7 2AZ, UK. 22Department of Bioengineering, Institute for Biomedical Engineering, Imperial College London, London, SW7 2AZ, UK. 23J&J Boston Innovation Center, One Cambridge Center, 7th Floor, Cambridge, MA 02142, USA. 24Monash Newborn, Monash Medical Centre, Clayton, Melbourne, Victoria 3168, Australia. 25The Ritchie Centre, Monash Institute of Medical Research Prince Henry’s Institute (MIMR-PHI), Institute of Medical Research, Clayton, Melbourne, Victoria 3168, Australia. 26Department of Paediatrics, Monash University, Melbourne, Australia. 27Helmholtz Zentrum München–German Research Center for Environmental Health, Germany. 28Institute for Medical Im-munology, Charité–Universitätsmedizin Berlin, Germany.

17
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 26 November 2014 Vol 6 Issue 264 264cm12 2
C O M M E N TA R Y
“ ”capture those few discoveries that might deliver products to the clinical marketplace. T us, it is critical for researchers, funders, and the general public to understand that fundamental and of en purely exploratory basic research is the platform from which major technical advances are launched. T e history of technical innovation is replete with examples wherein hypothesis-driven research led to unanticipated, serendipitous observations that then served to open up entirely new f elds. Attempts to divert or constrain the basic biomedical research’s scope, diversity, or magnitude compromise innovation and possible health care ad-vances.
For better or worse, an “invent and dis-cover” approach is widely used in the life sciences, especially with technology-driven research. T is eponymous approach centers on inventing new technologies and discov-ering new pathways, yet typically avoids the challenge of validating basic discoveries in a clinical scenario and further ref ning technologies to be reliable, robust, scalable, and capable of passing through regula-tory hoops. When inventing and discover-ing, many researchers believe that they are also translating, when in fact they rely on the passing of of their research f ndings to someone else for possible future transla-tion. In many of these cases, the most dif-f cult decisions and work remain to be done af er discovery: T e hand-of requires that careful due diligence be done on the discov-ery to discern what is valued in translation. Movement of discoveries out of the basic science arena is rare, leaving the specula-tive promise of impact unfulf lled. Accord-ing to the U.S. National Institutes of Health (NIH), 80 to 90% of research projects fail before they are tested in humans; and those precious few that do proceed to human studies require up to 15 years to see clini-cal use (1). Nonetheless, few basic research projects likely warrant translation beyond discovery. If the work is truly new, it of en begets further discovery research instead, with its own intrinsic merits, before ratio-nal translational decisions can be made.
T is focus on a basic research–oriented mindset leaves many potent basic research results in a technological no man’s land, with translational feasibility and value fre-quently untested and unvalidated, without addressing the possible extension of further technological capabilities, product vision, and market- or investor-related aspects. Recognizing and addressing these chal-
lenges in moving select, promising ideas beyond basic research, while formidable, are precisely what counts in getting discov-eries and inventions translated into both products and patients. Passive “hand-of ” of early scientif c discoveries (for example, by publishing details, hoping that someone else moves it forward) is ine% cient and in-ef ective in vetting new biomedical technol-ogies for translation. And although a delib-erate systematic process might yield better results, it is di% cult and tedious to identify only those few ideas uniquely qualif ed for translation.
Whose job is it, then, to bridge this di% -cult “in-between” step in order to shepherd early discoveries to the next level of transla-tional impact? It is the responsibility of life scientists aimed at making a dif erence to patients and those who identify themselves as translational scientists. It is imperative that the global research and development community changes its attitudes to assume more active responsibility for ensuring best practices in translation, together with the appropriate structures, resources, and deci-sion trees to make it happen.
A statement in this regard was published a decade ago: “Without mechanisms and infrastructure to accomplish this transla-tion in a systematic and coherent way, the sum of the data and information produced by the basic science enterprise will not re-sult in tangible public benef t” (2). T is ini-tiated a “call to action” that, in the United States, resulted in NIH’s launching of the Clinical and Translational Science Awards (CTSA) program in 2006 and the more recent creation of the NIH National Cen-ter for Advancing Translational Sciences (NCATS), which focuses on improving the national translational medicine mission. NCATS currently funds a U.S. consortium of 61 medical research institutions.
In Germany six Centers for Health Re-search, launched by the German federal government, are addressing the challenge of translational research. As interinstitu-tional centers with a decentralized struc-ture, knowledge and expertise from the best universities and their teaching hospi-tals and extra-university institutions are pooled in these Centers. T e Berlin Insti-tute of Health (BIH) is another example of the German commitment. T e BIH is set up to provide a common research area de-signed to harness basic and clinical research within a joint approach and with a focus on systems medicine.
We now need an international discus-sion about who plays what role in produc-ing translation: Who is actually responsible for catalyzing the transformation of useful ideas into products? Who matches clinical unmet needs with the risk of new technol-ogy developments? Who moves these prod-ucts into clinical use or a competitive mar-ketplace? How are these goals best molded into a concrete coordinated and e% cient process (3, 4)? T e cost of translating every biomedical discovery is absolutely prohibi-tive and misses the mark, as most ideas are not worth translating. However, missing those few clinically impactful innovation opportunities because of poor selection processes is equally costly. Commercial vetting of academic basic discoveries is central to current translational strategies, a testament to the value and impact of prof t-motivated product development. Yet, this process is not foolproof, and the industrial bottom line must balance; for a stable busi-ness, the costs of commercial translational failures are borne by the pricing of com-mercial product successes. While a prof t motive is critical to the commercial process, the ultimate metric for translational success is an improved standard of health care and patient quality of life globally. To this end, all participants at Translate! agreed that the following considerations are needed up-front to improve translational success.
COME TOGETHER, RIGHT NOW
Because translation involves coordinated hand-of s and transitions between teams with dif erent expertise sets and compe-tencies, a multidisciplinary approach is re-quired throughout in which players meet, transfer knowledge and know-how, and form teams for follow-through (5). In this scenario, clinical scientists and researchers in the biological and biomedical sciences and engineering would partner with health care providers, patent agents, industrial partners, and regulatory authorities, aim-ing for ef ective transfer of basic f ndings to preclinical models and then to early clini-cal validation. Cross-fertilization of ideas, capabilities, perspectives, and seamless in-teractions across both discipline- and fund-ing-related siloes are essential to assemble the resources, inform of risks and benef ts, and streamline the selection process. But all of this is much easier said than actually done: evaluations of translational processes and results have identif ed a complex ma-trix of issues that inform future action and

18
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 26 November 2014 Vol 6 Issue 264 264cm12 3
C O M M E N TA R Y
“ ”
decisions (3, 4). T e decision to translate or not to translate hinges on expertise, evi-dence, resources, and engaged dialogue at each step in the process.
Most basic and applied research is pur-sued in academic settings, whereas most product development and late-stage clini-cal trials, regulatory approval, manufactur-ing, and distribution are accomplished by industry and requisite commercial ef orts. Logically, the two ef orts should be linked to share expertise and facilitate transfer of ideas. Nonetheless, barriers persist in pri-orities, culture, philosophy, and process. Current academic structures and career pathways reward individual scientif c mer-it, chief y based on novelty and innovation regardless of practicality. In most academic institutions, translation-oriented ef orts are rewarded less well than the “classical” mea-sures, such as publication output or award-ed grants.
Academic reward systems should focus on not only publication quality, number, or journal impact factor, but also tangible impacts of research on medical treatments and patient benef ts. Naturally, ef ective translation requires team-based expertise and coordination throughout the bench-to-bedside-and-back, ideally as a develop-mental continuum; however, a team-based approach may not lead to clear individual credit and visibility as other, more classi-cal academic pursuits. Junior academics have only a few years to demonstrate their
intellectual creativity and scientif c im-pact to obtain tenure and career stability. T is timeline is of en not commensurate with one that recognizes the benef ts from clinical translation, which requires longer development timelines. New academic in-centives should be tailored to allow demon-stration of longer-term benef ts from team-based approaches and provide metrics for promoting and def ning career stability. T is would encourage the best and bright-est minds to engage in translation-oriented basic research and the risks of participating in clinical proof-of-concept trials.
Although a creative, productive scien-tif c career is essential for a junior academic to thrive, an open ear and eye toward other complementary disciplines are frequently necessary for shaping long-term career suc-cess (5). Current funding mechanisms and graduate-student training and mentoring too of en focus on narrow science or technol-ogy topics, lacking a big-picture perspective important for understanding the context of moving early-stage ideas toward medical ap-plications and the pitfalls of uninformed or hasty vetting methods. Graduate students and young investigators should be educated in the challenges, rewards, and multidisci-plinary nature of translating basic research into medical applications (6, 7). Multidisci-plinary approaches in teaching can unexpect-edly produce benef ts by marrying seemingly unrelated biomedical disciplines in graduate and medical professional training.
Translation also benef ts from carefully considering the mindset of stakeholders not directly involved in the research. Clini-cal and patient representatives and prod-uct end-users are essential resources and partners (3). Patient advocates can help to generate support for research and f rst-in-human trials, which best inform the path to translation. Most clinical indications re-quire costly multicenter approaches for re-liable and reproducible clinical assessment. Such a goal may be best accomplished with international interactions among scientists, industrialists, commercial authorities, pa-tient advocacy organizations, and clinical investigators.
PROFESSIONALIZING TRANSLATION
Investigators who consistently aim to change standards of patient care should seek train-ing and experience as “professional transla-tors.” A key to professionalization is early, dedicated training on the diverse spectrum of translational components. Such a mind-set requires (i) strong roots in basic science to realize the importance of mechanism; (ii) an understanding of funding and related barriers across basic, applied, and clinical research and development; (iii) dedicated knowledge about clinical trial requirements and how these follow from preclinical stud-ies and regulatory mandates; and (iv) prod-uct development awareness surrounding simplicity, good manufacturing practice (GMP), and end-user requirements. Un-derstanding the risks and adverse, wasteful impacts of improper translational selection is a powerful negative reinforcement to the process. If proper design requirements for clinical trials are included early in preclini-cal research, guided by informed product design and quality system expertise, unnec-essary and of en costly product redesigns and trial repetitions can be avoided. Young scientists are then essentially trained on the job to fulf ll critical translational require-ments.
Professional translators recognize that many preclinical disease models and labo-ratory scenarios lack the expected predic-tive reliability to ensure transfer of the con-cept to a treatment in people within real-life settings (8, 9). T is gap results from inher-ent limitations in common disease models (physiological, pathological, anatomical, metabolic); a lack of understanding of the medical indication or human pathologies being modeled; or poor study design. Sys-tematic reviews of preclinical research have
Join forces. Advancing clinical medicine to improve health care value and outcomes requires professional translators—competently trained translational scientists who are educated across the diverse spectrum of translational components and capable of effi cient communication with diverse stakeholders across multiple disciplines and areas of expertise required to vet early-stage ideas into products.
CR
ED
IT: D
. SC
HT
UT
MA
N/S
HU
TT
ER
ST
OC
K
www.ScienceTranslationalMedicine.org 26 November 2014 Vol 6 Issue 264 264cm12 3
C O M M E N TA R Y
“ ”
decisions (3, 4). T e decision to translate or not to translate hinges on expertise, evi-dence, resources, and engaged dialogue at each step in the process.
Most basic and applied research is pur-sued in academic settings, whereas most product development and late-stage clini-cal trials, regulatory approval, manufactur-ing, and distribution are accomplished by industry and requisite commercial ef orts. Logically, the two ef orts should be linked to share expertise and facilitate transfer of ideas. Nonetheless, barriers persist in pri-orities, culture, philosophy, and process. Current academic structures and career pathways reward individual scientif c mer-it, chief y based on novelty and innovation regardless of practicality. In most academic institutions, translation-oriented ef orts are rewarded less well than the “classical” mea-sures, such as publication output or award-ed grants.
Academic reward systems should focus on not only publication quality, number, or journal impact factor, but also tangible impacts of research on medical treatments and patient benef ts. Naturally, ef ective translation requires team-based expertise and coordination throughout the bench-to-bedside-and-back, ideally as a develop-mental continuum; however, a team-based approach may not lead to clear individual credit and visibility as other, more classi-cal academic pursuits. Junior academics have only a few years to demonstrate their
intellectual creativity and scientif c im-pact to obtain tenure and career stability. T is timeline is of en not commensurate with one that recognizes the benef ts from clinical translation, which requires longer development timelines. New academic in-centives should be tailored to allow demon-stration of longer-term benef ts from team-based approaches and provide metrics for promoting and def ning career stability. T is would encourage the best and bright-est minds to engage in translation-oriented basic research and the risks of participating in clinical proof-of-concept trials.
Although a creative, productive scien-tif c career is essential for a junior academic to thrive, an open ear and eye toward other complementary disciplines are frequently necessary for shaping long-term career suc-cess (5). Current funding mechanisms and graduate-student training and mentoring too of en focus on narrow science or technol-ogy topics, lacking a big-picture perspective important for understanding the context of moving early-stage ideas toward medical ap-plications and the pitfalls of uninformed or hasty vetting methods. Graduate students and young investigators should be educated in the challenges, rewards, and multidisci-plinary nature of translating basic research into medical applications (6, 7). Multidisci-plinary approaches in teaching can unexpect-edly produce benef ts by marrying seemingly unrelated biomedical disciplines in graduate and medical professional training.
Translation also benef ts from carefully considering the mindset of stakeholders not directly involved in the research. Clini-cal and patient representatives and prod-uct end-users are essential resources and partners (3). Patient advocates can help to generate support for research and f rst-in-human trials, which best inform the path to translation. Most clinical indications re-quire costly multicenter approaches for re-liable and reproducible clinical assessment. Such a goal may be best accomplished with international interactions among scientists, industrialists, commercial authorities, pa-tient advocacy organizations, and clinical investigators.
PROFESSIONALIZING TRANSLATION
Investigators who consistently aim to change standards of patient care should seek train-ing and experience as “professional transla-tors.” A key to professionalization is early, dedicated training on the diverse spectrum of translational components. Such a mind-set requires (i) strong roots in basic science to realize the importance of mechanism; (ii) an understanding of funding and related barriers across basic, applied, and clinical research and development; (iii) dedicated knowledge about clinical trial requirements and how these follow from preclinical stud-ies and regulatory mandates; and (iv) prod-uct development awareness surrounding simplicity, good manufacturing practice (GMP), and end-user requirements. Un-derstanding the risks and adverse, wasteful impacts of improper translational selection is a powerful negative reinforcement to the process. If proper design requirements for clinical trials are included early in preclini-cal research, guided by informed product design and quality system expertise, unnec-essary and of en costly product redesigns and trial repetitions can be avoided. Young scientists are then essentially trained on the job to fulf ll critical translational require-ments.
Professional translators recognize that many preclinical disease models and labo-ratory scenarios lack the expected predic-tive reliability to ensure transfer of the con-cept to a treatment in people within real-life settings (8, 9). T is gap results from inher-ent limitations in common disease models (physiological, pathological, anatomical, metabolic); a lack of understanding of the medical indication or human pathologies being modeled; or poor study design. Sys-tematic reviews of preclinical research have
Join forces. Advancing clinical medicine to improve health care value and outcomes requires professional translators—competently trained translational scientists who are educated across the diverse spectrum of translational components and capable of effi cient communication with diverse stakeholders across multiple disciplines and areas of expertise required to vet early-stage ideas into products.
CR
ED
IT: D
. SC
HT
UT
MA
N/S
HU
TT
ER
ST
OC
K

19
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 26 November 2014 Vol 6 Issue 264 264cm12 4
C O M M E N TA R Y
“ ”revealed low internal validity, such as a lack of randomization and blinding or insu% -cient statistical power, as well as low exter-nal validity (for example, modeling diseases of elderly humans in young, healthy mice). T ese limitations of en preclude translation of basic f ndings to any kind of relevant clinical application. Post-hoc “prediction” of clinical trial failures might help to im-prove or innovate preclinical models to be more reliable, reproducible, and predictive.
To enhance reproducibility, some journals, including Science Translational Medicine, Science, and Nature (10–12), and funding bodies, such as the U.S. National In-stitute of Neurological Disorders and Stroke (NINDS) (13), have devised technical study reporting checklists (f g. S1) and publication requirements. Although these requirements are more of en imposed at the manuscript revision stage, their implementation even sooner in the process—for example, at study conception (hypothesis generation and study design)— would better transform the mindset of translational scientists to ensure that preclinical studies are designed to yield higher clinical success rates.
Appreciating and discerning that failure is an e% cient mode of drug and target se-lection is also requisite to improving trans-lation and to providing teaching examples for young researchers. Too frequently, basic academic research lacks the inherent ability to fail early and quickly, as is now the com-mon mindset for product-pipeline develop-ment in the pharmaceutical industry. Nega-tive results have few publication venues. On this issue, journals are also working to f ght this publication bias, with certain journals introducing a “negative results section” and other new journals starting only to report signif cant negative results (14). It is not clear yet if these are equalizing solutions or are just another way to segregate nega-tive results. One mechanism for highlight-ing the importance of negative results may be to publish them alongside positive ones when the negative results illustrate some-thing fundamental and distinct about ther-apeutics discovery or human pathophysiol-ogy (versus simply descriptive results of a failed investigation).
Unfortunately, failed studies and nega-tive results of en have no respected place in an academic portfolio. T e tenure and promotion systems do not rate such studies highly, however important they are for ac-curate reporting and translation. Many in-depth mechanistic analyses lack relevance
to human biology, but instead ref ect only the experimental context in which they were generated (that is, the lab bench); yet, these studies are viewed more positively than those that report a failed clinical trial in which direct knowledge and insight are learned about human disease, about a new drug’s mechanism of action, or about hu-man toxicity. Learning how to fail quickly in a clinically relevant setting, to gain and exploit the knowledge from these failures, and to better educate the community to value failures are essential for professional-izing translation and should be actively em-braced, discussed, and rewarded.
INFRASTRUCTURE
Education alone—including professionaliza-tion—cannot single-handedly improve translational success. A well-oiled research infrastructure represents a central back-bone in a system designed to vet and sort innovations, identify potential solutions that address medical needs and therapeutic concepts, and move even the simplest but most reliable technologies forward, cull-ing from the system those that fail. In some
cases, academia provides consultancy hubs, linking industry and academia as a one-stop service with integrated access to clinical needs, cutting-edge technologies, intellec-tual property management, knowledgeable business development capacity, and even bridge f nancing. Other solutions hand ba-sic research to an internal business develop-
ment team that carries an idea through de-velopment to product concept, production, and marketing. Industry has also set up its own technology scouting teams to broadly survey emerging, early-stage ideas and steward only select innovations forward through translation. Something can be learned from each of these infrastructures about changing the mindset of stakehold-ers and promoting a culture of translational medicine in academia; this topic is tackled in-depth in a forthcoming partner article in Science Translational Medicine.
ELEPHANT IN THE ROOM
Ask investigators what the elephant in the translational research room is, and most will say “funding.” Adequate bridge fund-ing, economic incentives, and market forces are essential to driving and directing suc-cessful translation. Current basic research funding [NIH in the United States, the Ger-man Research Foundation (DFG), and the Federal Ministry of Education and Research (BMBF) and European Commission across Europe] cannot cover all clinical trial costs (although some new government programs
now seek to ease this problem). Industry is eager to take over projects af er success in phase 2 and beyond, af er substantial derisking has occurred. Despite major ef-forts by the above-mentioned authorities, funding for early-phase (that is, 1 and 2) development in this riskier gap remains a fundamental challenge. Few resources exist
Never forget the elephant in the room. It’s about the money. Lack of funding mechanisms and selection processes for riskier, early-phase development blocks translation.
CR
ED
IT: M
. L. F
RIS
K A
ND
N. K
. N
GU
YỄ
N/S
CIE
NC
E T
RA
NSLA
TIO
NA
L M
ED
ICIN
E

20
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 26 November 2014 Vol 6 Issue 264 264cm12 5
C O M M E N TA R Y
“ ”for bridging early-stage, unvetted research to more mature, validated technologies. In addition, precious resources should be ex-pended on identifying only the most meri-torious concepts to move forward while avoiding the majority of less promising or more costly, riskier ideas.
Once the mindset of translational in-vestigators changes—in other words, once participants have been educated in the vari-ous dimensions of translational medicine, are supported by their institutions, and recognize how to develop and vet prod-ucts for translation—the next challenge is to interest investors and industry in setting up partnerships. Pharma has pulled out of several f elds, citing costly struggles with a lack of predictive models and low success rates for drugs in clinical trials (15). Derisk-ing and adding value are major challenges. T e mindset of a translational researcher should, at the outset, recognize these chal-lenges in engaging industry and be dili-gent in seeking partnerships and collecting market data. Two future articles in Science Translational Medicine will take on funding barriers and derisking.
THE RUBBER MEETS THE ROAD
Translate! 2014 brought together voices on the translational process, the keys to success, the regulatory requirements, the clinical needs, the partnering essentials, the value of proper resource use, and the pos-sible (and very real) pitfalls. Every transla-tional researcher is a stakeholder as well as an important cog in the translational medi-cine machine. With an improved def nition of “translation” in place, the interest groups identif ed, and the tools chosen, the pro-cess of changing the attitudes that histori-cally have limited this process can begin. T is transformation at academic levels will be accomplished by revamping traditional funding schemes, better partnering with experts in commercial-product translation, adding to academic promotional and per-formance incentives, altering publishing priorities and reliability, and updating grad-uate and postdoctoral education priorities.
Another component is establishing stronger partnerships between academia and commerce that better informs the pro-cess with industrial development strategy, market opportunities, and critical interac-tions with both patenting and regulatory bodies. Ideally, this business relationship also provides a direct path to economic forecasts and intelligent f nancing decisions
for product investments. Focus on respon-sible product investment timelines helps to establish parameters for determine product development “go–no go” points, provid-ing some early derisking guidelines. T is essentially mirrors aspects of industrial product selection processes for new tech-nology adoption and makes translation an economically driven process. Discoveries at the bench cannot reach the bedside without the third “B”: business. Translation neces-sitates consistent, intelligent, and prudent f nancial guidance—knowing when to “pull the plug” on a project (that is, to fail con-f dently and e% ciently)—and the essential manufacturing and marketing resources from business. Partnering early and then continuously with industrial technology transfer experts appears critical to the end-game of improving success in providing in-novative products for patient care.
Overall, ef ective translation will require a change in the scientif c mindset to value much more interactive and collaborative relationships. T is starts with young in-vestigators who learn to maintain a trained open eye and ear to other disciplines be-yond their individual educational experi-ence. Translational investigators should be skilled at properly identifying unmet clini-cal needs, matching appropriate strategies and partners, and including nonscientif c parameters in their evaluation. T is ap-proach requires interactions across f elds
within medicine and scientif c disciplines and across the various stakeholder, patient, and interest groups. Success also requires involvement of funding agencies, intel-lectual property experts, and regulatory authorities as accessible consultants early in the process of innovative thinking and translation-oriented basic research. As the conference title Translate! implies, transla-tion is not a passive process, it is an impera-tive to improve health care value, health outcomes, and patient quality of life.
SUPPLEMENTARY MATERIALSwww.sciencetranslationalmedicine.org/cgi/content/full/6/264/264cm12/DC1
Manuscript checklist
REFERENCES AND NOTES 1. “Crossing over the Valley of Death: Translational
research.” www.fastercures.org/assets/Uploads/VOD-
TranslationalResearch.pdf.
2. N. S. Sung, W. F. Crowley Jr., M. Genel, P. Salber, L. Sandy,
L. M. Sherwood, S. B. Johnson, V. Catanese, H. Tilson, K.
Getz, E. L. Larson, D. Scheinberg, E. A. Reece, H. Slavkin, A.
Dobs, J. Grebb, R. A. Martinez, A. Korn, D. Rimoin, Central
challenges facing the national clinical research enter-
prise. J. Am. Med. Assoc. 289, 1278–1287 (2003).
3. W. M. Trochim, D. M. Rubio, V. G. Thomas, Evaluation Key
Function Committee of the CTSA Consortium, Evalua-
tion guidelines for the Clinical and Translational Science
Awards (CTSAs). Clin. Transl. Sci. 6, 303–309 (2013).
4. W. Trochim, C. Kane, M. J. Graham, H. A. Pincus, Evaluat-
ing translational research: A process marker model. Clin.
Transl. Sci. 4, 153–162 (2011).
5. P. von Roth, B. J. Canny, H.-D. Volk, J. A. Noble, C. G.
Prober, C. Perka, G. N. Duda, The challenges of modern
interdisciplinary medical research. Nat. Biotechnol. 29,
1145–1148 (2011).
Go–no go. Responsible product-development parameters modeled from commercial decision-making algorithms help turn red lights green on the road to clinical translation.
CR
ED
IT: R
. SA
XO
N/A
SSO
CIA
TE
D P
RE
SS
www.ScienceTranslationalMedicine.org 26 November 2014 Vol 6 Issue 264 264cm12 5
C O M M E N TA R Y
“ ”for bridging early-stage, unvetted research to more mature, validated technologies. In addition, precious resources should be ex-pended on identifying only the most meri-torious concepts to move forward while avoiding the majority of less promising or more costly, riskier ideas.
Once the mindset of translational in-vestigators changes—in other words, once participants have been educated in the vari-ous dimensions of translational medicine, are supported by their institutions, and recognize how to develop and vet prod-ucts for translation—the next challenge is to interest investors and industry in setting up partnerships. Pharma has pulled out of several f elds, citing costly struggles with a lack of predictive models and low success rates for drugs in clinical trials (15). Derisk-ing and adding value are major challenges. T e mindset of a translational researcher should, at the outset, recognize these chal-lenges in engaging industry and be dili-gent in seeking partnerships and collecting market data. Two future articles in Science Translational Medicine will take on funding barriers and derisking.
THE RUBBER MEETS THE ROAD
Translate! 2014 brought together voices on the translational process, the keys to success, the regulatory requirements, the clinical needs, the partnering essentials, the value of proper resource use, and the pos-sible (and very real) pitfalls. Every transla-tional researcher is a stakeholder as well as an important cog in the translational medi-cine machine. With an improved def nition of “translation” in place, the interest groups identif ed, and the tools chosen, the pro-cess of changing the attitudes that histori-cally have limited this process can begin. T is transformation at academic levels will be accomplished by revamping traditional funding schemes, better partnering with experts in commercial-product translation, adding to academic promotional and per-formance incentives, altering publishing priorities and reliability, and updating grad-uate and postdoctoral education priorities.
Another component is establishing stronger partnerships between academia and commerce that better informs the pro-cess with industrial development strategy, market opportunities, and critical interac-tions with both patenting and regulatory bodies. Ideally, this business relationship also provides a direct path to economic forecasts and intelligent f nancing decisions
for product investments. Focus on respon-sible product investment timelines helps to establish parameters for determine product development “go–no go” points, provid-ing some early derisking guidelines. T is essentially mirrors aspects of industrial product selection processes for new tech-nology adoption and makes translation an economically driven process. Discoveries at the bench cannot reach the bedside without the third “B”: business. Translation neces-sitates consistent, intelligent, and prudent f nancial guidance—knowing when to “pull the plug” on a project (that is, to fail con-f dently and e% ciently)—and the essential manufacturing and marketing resources from business. Partnering early and then continuously with industrial technology transfer experts appears critical to the end-game of improving success in providing in-novative products for patient care.
Overall, ef ective translation will require a change in the scientif c mindset to value much more interactive and collaborative relationships. T is starts with young in-vestigators who learn to maintain a trained open eye and ear to other disciplines be-yond their individual educational experi-ence. Translational investigators should be skilled at properly identifying unmet clini-cal needs, matching appropriate strategies and partners, and including nonscientif c parameters in their evaluation. T is ap-proach requires interactions across f elds
within medicine and scientif c disciplines and across the various stakeholder, patient, and interest groups. Success also requires involvement of funding agencies, intel-lectual property experts, and regulatory authorities as accessible consultants early in the process of innovative thinking and translation-oriented basic research. As the conference title Translate! implies, transla-tion is not a passive process, it is an impera-tive to improve health care value, health outcomes, and patient quality of life.
SUPPLEMENTARY MATERIALSwww.sciencetranslationalmedicine.org/cgi/content/full/6/264/264cm12/DC1
Manuscript checklist
REFERENCES AND NOTES 1. “Crossing over the Valley of Death: Translational
research.” www.fastercures.org/assets/Uploads/VOD-
TranslationalResearch.pdf.
2. N. S. Sung, W. F. Crowley Jr., M. Genel, P. Salber, L. Sandy,
L. M. Sherwood, S. B. Johnson, V. Catanese, H. Tilson, K.
Getz, E. L. Larson, D. Scheinberg, E. A. Reece, H. Slavkin, A.
Dobs, J. Grebb, R. A. Martinez, A. Korn, D. Rimoin, Central
challenges facing the national clinical research enter-
prise. J. Am. Med. Assoc. 289, 1278–1287 (2003).
3. W. M. Trochim, D. M. Rubio, V. G. Thomas, Evaluation Key
Function Committee of the CTSA Consortium, Evalua-
tion guidelines for the Clinical and Translational Science
Awards (CTSAs). Clin. Transl. Sci. 6, 303–309 (2013).
4. W. Trochim, C. Kane, M. J. Graham, H. A. Pincus, Evaluat-
ing translational research: A process marker model. Clin.
Transl. Sci. 4, 153–162 (2011).
5. P. von Roth, B. J. Canny, H.-D. Volk, J. A. Noble, C. G.
Prober, C. Perka, G. N. Duda, The challenges of modern
interdisciplinary medical research. Nat. Biotechnol. 29,
1145–1148 (2011).
Go–no go. Responsible product-development parameters modeled from commercial decision-making algorithms help turn red lights green on the road to clinical translation.
CR
ED
IT: R
. SA
XO
N/A
SSO
CIA
TE
D P
RE
SS

21
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 26 November 2014 Vol 6 Issue 264 264cm12 6
C O M M E N TA R Y
“ ” 6. K. Kurpinski, T. Johnson, S. Kumar, T. Desai, S. Li, Master-
ing translational medicine: Interdisciplinary education
for a new generation. Sci. Transl. Med. 6, 218fs2 (2014).
7. G. D. Prestwich, Culture of impact: Faculty as mentors for
student entrepreneurs. Sci. Transl. Med. 5, 169ed2 (2013).
8. H. B. van der Worp et al., Can animal models of disease
reliably inform human studies? PLOS Med. 7, e1000245
(2010).
9. I. W. Y. Mak, N. Evaniew, M. Ghert, Lost in translation: Ani-
mal models and clinical trials in cancer treatment. Am. J.
Transl. Res. 6, 114–118 (2014).
10. K. L. Kelner, Playing our part. Sci. Transl. Med. 5, 190ed7
(2013).
11. M. McNutt, Reproducibility. Science 343, 229 (2014).
12. Reducing our irreproducibility. Nature 496, 398 (2013).
13. S. C. Landis et al., A call for transparent reporting to opti-
mize the predictive value of preclinical research. Nature
490, 187–191 (2012).
14. U. Dirnagl, M. Lauritzen, Fighting publication bias: Intro-
ducing the Negative Results section. J. Cereb. Blood Flow
Metab. 30, 1263–1264 (2010).
15. S. E. Hyman, Revolution stalled. Sci. Transl. Med. 4,
155cm11 (2012).
Acknowledgments: The authors acknowledge the contribu-
tion of M. Goldman to the discussions at the Translate! 2014
meeting. Competing interests: The Center for Cell and Gene
Therapy (S.G.) has research collaborations with Celgene and
Bluebird Bio. C.H. is board member of the cutting edge tech-
nology cluster CI3 of the German federal government and
cofounder and deputy chairman of the supervisory boards of
Ganymed Pharmaceuticals and BioNTech AG. D.W.G. is scien-
tifi c co-founder and equity holder of medical device start-up
Elute, Inc. (USA), and scientifi c advisory board member and
equity holder for Jade Therapeutics (USA) and CellSeed, Ltd.
(Tokyo, Japan). R.U. is an employee of Johnson & Johnson (J&J)
Innovation LLC, a member of the J&J family of companies. E.
Gruskin is an employee of DePuy Synthes Biomaterials, a divi-
sion of DePuy Orthopedics, Inc., a member of the J&J family
of companies. The opinions expressed herein are those of the
authors and are not attributable to their respective employers
or companies. Funding: M.M.S. is supported by the UK Re-
generative Medicine Platform Hub “Acellular Approaches for
Therapeutic Delivery” (MR/K026682/1), which is funded by the
Medical Research Council, the Engineering and Physical Sci-
ences Research Council, and the Biotechnology and Biological
Sciences Research Council. G.N.D. and H.-D.V. are supported
by the DFG and BMBF.
Citation: G. N. Duda, D. W. Grainger, M. L. Frisk, L. Bruckner-
Tuderman, A. Carr, U. Dirnagl, K. M. Einhäupl, S. Gottschalk,
E. Gruskin, C. Huber, C. H. June, D. J. Mooney, E. T. Rietschel,
G. Schütte, W. Seeger, M. M. Stevens, R. Urban, A. Veldman, G.
Wess, H.-D. Volk, Changing the mindset in life sciences toward
translation: A consensus. Sci. Transl. Med. 6, 264cm12 (2014).
10.1126/scitranslmed.aaa0599

22
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.orgOriginally published 25 February 2015
P E R S P E C T I V E
www.ScienceTranslationalMedicine.org 25 February 2015 Vol 7 Issue 276 276ps3 1
T e U.S. Food and Drug Administration’s (FDA’s) Of ce of Orphan Product Develop-ment (OOPD) def nes an “orphan” rare dis-ease as one that af ects fewer than 200,000 U.S. patients. Although each rare disease has a low prevalence, an estimated 25 million to 30 million Americans are af ected by the collection of more than 6800 rare diseases recognized by the U.S. National Institutes of Health (NIH). Globally, rare diseases af ect ~350 million people and are responsible for 35% of deaths within the f rst year of life (1). Drug development for rare diseases poses a particular set of challenges, including small patient populations and diagnostic delays re-sulting from a lack of medical expertise and public awareness. Moreover, the small market size of individual orphan diseases and per-ceived lack of prof tability have been barriers to private-sector investment in orphan drugs. To address these challenges, the U.S. Con-gress enacted the Orphan Drug Act of 1983, which provides incentives to sponsors of or-phan drugs—including 7-year market exclu-sivity, tax credits equal to half of the devel-
opment costs, grants for drug development, and fast-track approvals of drugs indicated for rare diseases—and was later amended to include waiver of user fees charged under the Prescription Drug User Fee Act (PDUFA). Before 1983, only 10 new drugs for rare dis-eases were developed by the pharmaceutical industry (2), whereas according to the FDA database, 221 orphan-designated products received FDA approval over the decade end-ing 3 November 2014 (3).
Recent work by Fagnan et al. (4) shows that orphan drug development is particu-larly well suited to be f nanced through a megafund—a f nancial investment fund in which investors commit capital to be used for developing a portfolio of orphan drugs and receive the proceeds of these investigational drugs or intellectual property (IP) rights as they are sold to venture capitalists (VCs) or licensed by pharmaceutical companies. By diversifying the risk of drug development across many “shots on goal,” the likelihood of success increases, and the f nancial risk-reward prof le of an investment in the mega-fund becomes more attractive than that of any single project. T e more attractive the megafund’s returns are, the more likely it is that large amounts of capital can be raised to support such diversif cation. Using standard industry parameters for development costs, revenue projections, and historical success rates for orphan drug development, Fagnan et al. show that a portfolio of 10 to 20 projects can yield double-digit annualized returns with a $575 million megafund (4). However, their simulated results are based on industry
averages and anecdotal data and therefore may not be achievable in practice. In fact, one of the main challenges to adopting the mega-fund structure is the lack of a business model to manage such a fund; portfolio selection and project management require deep do-main knowledge of both drug development and f nancial engineering.
In this article, we apply the megafund concept to analyze a real-life rare-disease portfolio from NIH’s National Center for Advancing Translational Sciences (NCATS) (5). Two late-stage preclinical drug-devel-opment programs operated at NCATS’s Di-vision of Preclinical Innovations (DPI)—the T erapeutics for Rare and Neglected Dis-eases (TRND) and Bridging Interventional Development Gaps (BrIDGs) programs—are particularly relevant for providing a concrete example of a potential business model for an orphan drug megafund. Using pooled data from TRND and BrIDGs com-bined with industry averages from Fagnan et al. (4) for typical orphan diseases, we have constructed a more ref ned and realistic simulation of the performance of a hypo-thetical orphan drug megafund. Realized costs, timelines, and success rates are used to compute performance, and valuations for each project in the NCATS portfolio are obtained by averaging the assessments of a panel of independent industry experts.
Using the total horizon time of 11 years, we estimated that the average annualized returns of this hypothetical megafund range from 12 to 15%. Moreover, average inter-nal rates of return measured on net cash f ows—a metric typically used by venture capitalists—can be more than twice these raw annualized returns. NCATS data suggest substantially lower costs and higher success rates but longer preclinical timelines than the industry averages used by Fagnan et al. (4). In particular, the simulated performance of an NCATS rare-disease portfolio is comparable with that of a VC fund with an internal rate of return of more than 25%. T e addition of debt tranches and a third-party guarantee of principal can increase the average raw return by 200 percentage points. Last, although the hypothetical megafund calibrated to NCATS data is simulated as a private enterprise, ad-ditional benef ts could be obtained from a public-private partnership model.
SELECTING PROJECTS
T e TRND program within the NCATS DPI considers applications for projects in the translational medicine space in which
F U N D I N G
Financing translation: Analysis of the NCATS rare-diseases portfolio
David E. Fagnan,1,2* N. Nora Yang,3* John C. McKew,3† Andrew W. Lo1,2,4,5‡
*These authors contributed equally to this work. †Pres-ent address: aTyr Pharma, 3545 John Hopkins Court, Suite 250, San Diego, CA 92121, USA. ‡Corresponding author. E-mail: [email protected]
1Operations Research Center, Massachusetts Institute of Technology (MIT), Cambridge, MA 02142, USA. 2Sloan School of Management and Laboratory for Financial Engineering, MIT, Cambridge, MA 02142, USA. 3Na-tional Center for Advancing Translational Sciences, U.S. National Institutes of Health, Rockville, MD 20850, USA. 4Computer Science and Artif cial Intelligence Labora-tory and Department of Electrical Engineering and Computer Science, MIT, Cambridge, MA 02139, USA. 5AlphaSimplex Group, LLC, Cambridge, MA 02142, USA.
P E R S P E C T I V E
The portfolio of the National Center for Advancing Translational Sciences (NCATS) rare-diseases therapeutic development program comprises 28 research projects initiated at the preclinical stage. Historical data reveal substantially lower costs and higher success rates but longer preclinical timelines for the NCATS projects relative to the industry averages for early-stage translational medical research and development (R&D) typi-cally cited in literature. Here, we evaluate the potential risks and rewards of investing in a portfolio of rare-disease therapeutics. Using a “megafund” f nancing structure, NCATS data, and valuation estimates from a panel of industry experts, we simulate a hypo-thetical megafund in which senior and junior debt yielded 5 and 8%, respectively. The simulated expected return to equity was 14.7%, corresponding to a modif ed internal rate of return of 21.6%. These returns and the likelihood of private-sector funding can be enhanced through third-party funding guarantees from philanthropies, patient advo-cacy groups, and government agencies.

23
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
P E R S P E C T I V E
www.ScienceTranslationalMedicine.org 25 February 2015 Vol 7 Issue 276 276ps3 2
the target disease qualif es for FDA’s orphan product designation or is on the World Health Organization (WHO) neglected tropical disease list. TRND accepts projects with investigational drug candidates be-tween the lead-optimization and investiga-tional new drug (IND)–f ling stages. In four years, TRND has taken four new molecular entities (NMEs) or repurposed drugs into the clinic for both phase 1 and phase 2 stud-ies. T e goal of TRND is to take projects to the earliest stage at which they are commer-cially attractive to private investors such as industry or VCs, who are able to take the commercialization process to completion. T e TRND program also explores innova-tions aimed at improving preclinical success rates, managing risk, and reducing costs of advancing research breakthroughs into treatments, such as the development of plat-form technologies and new business mod-els. T e BrIDGs program focuses primarily on generating data for IND applications but is not limited to rare or neglected diseases projects. As with TRND, BrIDGs is not a grant-based program; successful applicants are provided with access to government contract resources to complete the IND-enabling studies required by FDA. For both the TRND and BrIDGs programs, the cur-rent NCATS operation model is to perform milestone activities sequentially; this means that subsequent milestone studies are initi-ated only af er the preceding ones have been completed successfully. T is sequential ap-proach has been adopted largely because of a limited budget; with larger budgets, launch-ing carefully selected key-project studies in parallel likely can shorten project timelines and enhance overall portfolio return.
NCATS hosts public solicitations to invite abbreviated applications to both programs, and selected applications are reviewed by a committee of external drug-development experts for scientif c merit and technical feasibility. NIH discipline and disease experts then review top-tier applica-tions for disease-specif c merits. If selected, applicants are then requested to submit a complete data package and all relevant supplementary materials so that the TRND and BrIDGs sta$ s can conduct a detailed re-view under a standard conf dentiality agree-ment. T e f nal portfolio-selection decision balances several considerations, including disease area, currently available therapies, treatment modalities, stage of development, platform technologies, NCATS technical expertise and overall mission, and f nancial
factors such as portfolio impact and budget.Once a project is selected for the portfo-
lio, a team consisting of both NCATS sta$ and applicant investigators is formed, and a detailed project plan is developed, in-cluding timelines, milestones, deliverables, and clearly def ned quantitative go/no-go decision criteria. Milestones include lead optimization, completion of IND-enabling studies, IND f ling, and phase 1 and phase 2 clinical trials. Project execution is guided under a three-tiered governance structure and managed by a project-team leader who has extensive industry drug-development experience. T e project team has full au-tonomy to execute against the project plan without having to go through layers of approval for decisions. A joint research committee is formed to play a key role in providing technical feedback and sugges-tions to help the team during project ex-ecution. NCATS leadership is informed of program progress on a regular basis, and only changes to the plan’s scope require ad-ditional NCATS approvals. When projects fail to meet a predetermined milestone, the TRND or BrIDGs project team will propose and conduct a closeout of the project and o$ er consultation and assistance to the ap-plicants with respect to moving forward.
If a project meets all milestones, NCATS completes its investments and assists its partners in securing private investments from either pharmaceutical and biotech-nology companies or VCs through various business-development activities. Among the 28 rare-disease projects at NCATS ana-lyzed in this study, more than a third of the projects have obtained funding from other sources, including VCs, venture philan-thropy, the NIH Clinical Center, and phar-maceutical companies.
ANALYZING THE NCATS PORTFOLIO
Data were collected for 28 rare-disease proj-ects—15 from TRND and 13 from BrIDGs, all selected before September 2013—that spanned a diverse range of therapeutic ar-eas, including oncology (3), hematology (5), musculoskeletal diseases (5), cardiovas-cular diseases (2), central nervous system diseases (6), endocrine disorders (4), oph-thalmology (2), and respiratory disorders (1). A complete list of the 28 projects is pro-vided in table S4. Projects within BrIDGs that are not rare disease–focused were not included in our data set or analysis. For treatment modalities, there were 5 projects involving existing drugs repurposed for
orphan indications, 13 NMEs, 8 large mol-ecules (including antisense oligos, peptides, and biologics), 1 stem cell therapy, and 1 gene vector therapy. Collaborating organi-zations included 15 academic institutions, 9 small biotech companies, 3 NIH intramural laboratories or clinical groups, and 2 large pharmaceutical companies. T e diversity of the portfolio in terms of therapeutic area, modality, and collaborating organization was designed to achieve maximum im-pact of limited program funding through “multiple shots on goal” as well as to help NCATS sta$ identify systemwide bottle-necks and develop models and tools to help improve the ef ciency of the translational medicine pipeline.
T e data cuto$ date for our analysis was 31 December 2013, and included in the analysis were items such as the clinical and regulatory success or failure of observed transitions between established milestones, the durations of such transitions (including time spent active and on hold), and expens-es incurred by NCATS and other project collaborators during each transition period. Within the 28 rare-disease projects, 20 were ongoing at this time, requiring measure-ment at intermediate milestones to capture the depth of the data. Twenty-four and four projects entered the NCATS pipeline at the IND-enabling phase and lead-optimization phase, respectively. Ten projects achieved at least one or more of the following mile-stone transitions: lead optimization (n = 1), IND-enabling (n = 9), IND f ling (n = 9), initiation of phase 1 clinical trials (n = 8), and initiation of phase 2 clinical trials (n = 5). One project failed to reach any transi-tion milestone. Additional success-rate data were obtained by including projects that were continued by collaborators af er com-pletion of the BrIDGs program, resulting in an additional f ve measured transitions from phase 1 clinical trials and three from phase 2. As a result of the small number of transition observations (1 to 10 depending on the parameter), we applied a weighted average using estimates drawn from the orphan drug literature (4) and prior belief weights. For example, we considered it un-likely that phase 2 projects would typically take 6 months, so for this parameter, we used a prior with increased weight (95%) on literature estimates. To provide a fair com-parison, we combined the two IND phases that we associated with the preclinical phase in (4). Details of the other prior weights can be found in supplementary materials.

24
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
P E R S P E C T I V E
www.ScienceTranslationalMedicine.org 25 February 2015 Vol 7 Issue 276 276ps3 3
VALUATION PANEL
In addition to data on the transition prob-abilities from one phase to the next, mar-ket valuations of the projects are needed to simulate investment returns. Previous stud-ies have used industry averages to calibrate such simulations (4), but these averages are unlikely to ref ect the singular aspects of the NCATS portfolio. T erefore, to provide val-uation estimates for our 28 sample projects, we convened a panel of f ve industry ex-perts, all of whom were active in the biotech industry and had a relevant mixture of past experience (in biotech, drug development, VC, and biotech investment banking) and job titles (including chief executive of cer, company founders, managing partners, and vice president). We asked these profession-als to provide valuation estimates for our 28 sample projects (Fig. 1). Our motivation for engaging these individuals was not only because of their deep expertise in biotech investing but also because they represented the most natural acquirers of NCATS port-folio projects; hence, even though their es-timates may not be any more precise than those of other experts, their valuations are more practically relevant than are generic industry averages.
T e data provided to the panel on the portfolio of projects included the collabora-tor organizations and disease-specif c infor-mation (such as prevalence, incidence, and standard of care) but not information on re-alized costs and project stage durations. T e panelists were asked to estimate the fair mar-ket value for each project in its current state and were given the option of providing up to three estimates: a low valuation, a best-guess valuation, and a high valuation. Results were sorted by project stage (using a log scale) (Fig. 1) [in contrast to the industry-average estimates in (4), which apply to the current phase only and are not based on any proj-ect-specif c information]. Vertical bars rep-resent the range of the low and high values provided by the respondents (6, 7), whereas the points represent their best guesses, which were taken to be the average of the high and low valuations if not explicitly specif ed. T e range of estimates underscores the challenge of valuing early-stage translational medicine projects; any valuation of these projects is likely to yield highly speculative estimates of true economic value. In fact, one panelist prefaced his valuations with the caveat that his estimates should be treated as coarse ap-proximations because normally, he would spend substantial resources and weeks of
time to determine the value of a single proj-ect (the full set of comments provided by the panel members is included in supplementary materials).
For the majority of projects, the best guesses of at least two panelists were higher than the corresponding estimates from the literature. T e values of one panelist for some projects were orders of magnitude higher than those of the other respondents. To reduce the impact of these outliers and improve the accuracy of our estimates of market value, we used the median estimates among the f ve panelists rather than the maximum (which is what a typical bidding process would do). Last, in our simulation we captured the imprecision of valuing early-stage biotech projects by specifying a large standard deviation (more than 80% of the value of the mean) for the distribution from which we simulated our valuations.
SIMULATION CALIBRATION
T e megafund simulation model of Fagnan et al. (4) relies on several key model parameters (Fig. 2), including clinical trial costs, clinical
trial durations, market valuations, and prob-ability of technical and regulatory success. To calibrate these parameters for a simulation of a hypothetical megafund of rare diseases based on the NCATS data, we took a weight-ed average of the parameters used in (4) and the parameters obtained from the NCATS data using weights based on prior beliefs and knowledge about the NCATS process. We then used the medians of the valuation pan-el’s estimates to compute the f nancial rate of return of NCATS projects by stage.
T e impact of these calibrations results in lower costs and higher success rates for all phases, longer preclinical development times, shorter clinical development times, and lower economic valuations relative to literature averages from (4). T e impact was greatest at the preclinical stage, for which we had the greatest number of ob-servations, and was smallest at the phase 2 stage, for which fewer transitions were ob-served. Other simulation parameters were used as well, including pairwise correla-tions among asset valuations; probability distributions of costs, valuations, and stage
Fig. 1. Value proposition. Summarized are the valuation estimates (log scale), from panel members (selected by A.W.L.) for the NCATS rare-disease portfolio compared with literature estimates (4) based on project phase alone. Vertical bars represent the range of the panelists’ lower and higher values. Projects are sorted by the stage at which they were valued, from lead optimization to phase 3 clinical trials. The responses of the panel members were formulated independently. The identities of panel-ists (who received no compensation or recognition for their participation) were not disclosed to each other or to NCATS personnel (including this article’s NCATS coauthors), and minimal direction was provided on how they should complete their task (supplementary materials).
Va
lua
tio
n e
stim
ate
($
mill
ion
s)
104
102
100
5 10 15 20 25
101
10-1
10-2
10-3
103
Project #
Res.1
Ref. (4)
Res. 2
Res. 3
Res. 4
Res. 5
Source
CR
ED
IT: H
. M
CD
ON
ALD
/SC
IEN
CE
TR
AN
SLA
TIO
NA
L M
ED
ICIN
E
P E R S P E C T I V E
www.ScienceTranslationalMedicine.org 25 February 2015 Vol 7 Issue 276 276ps3 3
VALUATION PANEL
In addition to data on the transition prob-abilities from one phase to the next, mar-ket valuations of the projects are needed to simulate investment returns. Previous stud-ies have used industry averages to calibrate such simulations (4), but these averages are unlikely to ref ect the singular aspects of the NCATS portfolio. T erefore, to provide val-uation estimates for our 28 sample projects, we convened a panel of f ve industry ex-perts, all of whom were active in the biotech industry and had a relevant mixture of past experience (in biotech, drug development, VC, and biotech investment banking) and job titles (including chief executive of cer, company founders, managing partners, and vice president). We asked these profession-als to provide valuation estimates for our 28 sample projects (Fig. 1). Our motivation for engaging these individuals was not only because of their deep expertise in biotech investing but also because they represented the most natural acquirers of NCATS port-folio projects; hence, even though their es-timates may not be any more precise than those of other experts, their valuations are more practically relevant than are generic industry averages.
T e data provided to the panel on the portfolio of projects included the collabora-tor organizations and disease-specif c infor-mation (such as prevalence, incidence, and standard of care) but not information on re-alized costs and project stage durations. T e panelists were asked to estimate the fair mar-ket value for each project in its current state and were given the option of providing up to three estimates: a low valuation, a best-guess valuation, and a high valuation. Results were sorted by project stage (using a log scale) (Fig. 1) [in contrast to the industry-average estimates in (4), which apply to the current phase only and are not based on any proj-ect-specif c information]. Vertical bars rep-resent the range of the low and high values provided by the respondents (6, 7), whereas the points represent their best guesses, which were taken to be the average of the high and low valuations if not explicitly specif ed. T e range of estimates underscores the challenge of valuing early-stage translational medicine projects; any valuation of these projects is likely to yield highly speculative estimates of true economic value. In fact, one panelist prefaced his valuations with the caveat that his estimates should be treated as coarse ap-proximations because normally, he would spend substantial resources and weeks of
time to determine the value of a single proj-ect (the full set of comments provided by the panel members is included in supplementary materials).
For the majority of projects, the best guesses of at least two panelists were higher than the corresponding estimates from the literature. T e values of one panelist for some projects were orders of magnitude higher than those of the other respondents. To reduce the impact of these outliers and improve the accuracy of our estimates of market value, we used the median estimates among the f ve panelists rather than the maximum (which is what a typical bidding process would do). Last, in our simulation we captured the imprecision of valuing early-stage biotech projects by specifying a large standard deviation (more than 80% of the value of the mean) for the distribution from which we simulated our valuations.
SIMULATION CALIBRATION
T e megafund simulation model of Fagnan et al. (4) relies on several key model parameters (Fig. 2), including clinical trial costs, clinical
trial durations, market valuations, and prob-ability of technical and regulatory success. To calibrate these parameters for a simulation of a hypothetical megafund of rare diseases based on the NCATS data, we took a weight-ed average of the parameters used in (4) and the parameters obtained from the NCATS data using weights based on prior beliefs and knowledge about the NCATS process. We then used the medians of the valuation pan-el’s estimates to compute the f nancial rate of return of NCATS projects by stage.
T e impact of these calibrations results in lower costs and higher success rates for all phases, longer preclinical development times, shorter clinical development times, and lower economic valuations relative to literature averages from (4). T e impact was greatest at the preclinical stage, for which we had the greatest number of ob-servations, and was smallest at the phase 2 stage, for which fewer transitions were ob-served. Other simulation parameters were used as well, including pairwise correla-tions among asset valuations; probability distributions of costs, valuations, and stage
Fig. 1. Value proposition. Summarized are the valuation estimates (log scale), from panel members (selected by A.W.L.) for the NCATS rare-disease portfolio compared with literature estimates (4) based on project phase alone. Vertical bars represent the range of the panelists’ lower and higher values. Projects are sorted by the stage at which they were valued, from lead optimization to phase 3 clinical trials. The responses of the panel members were formulated independently. The identities of panel-ists (who received no compensation or recognition for their participation) were not disclosed to each other or to NCATS personnel (including this article’s NCATS coauthors), and minimal direction was provided on how they should complete their task (supplementary materials).
Va
lua
tio
n e
stim
ate
($
mill
ion
s)
104
102
100
5 10 15 20 25
101
10-1
10-2
10-3
103
Project #
Res.1
Ref. (4)
Res. 2
Res. 3
Res. 4
Res. 5
Source
CR
ED
IT: H
. M
CD
ON
ALD
/SC
IEN
CE
TR
AN
SLA
TIO
NA
L M
ED
ICIN
E

25
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
P E R S P E C T I V E
www.ScienceTranslationalMedicine.org 25 February 2015 Vol 7 Issue 276 276ps3 4
durations; upfront and milestone payments; and equity-sharing percentages (parameters and methodological details are provided in the supplementary materials). Using these additional assumptions and procedures, log-normal distributions were calibrated for project costs, valuations, and durations, and random draws from these distributions were simulated to generate the statistical behavior of megafund returns. Results for distributions other than log-normal are pro-vided in the supplementary materials.
Although the NCATS data and valuation panel estimates provided more realistic val-ues with which to calibrate the simulation parameters, obtaining accurate parameter values was challenging and required sus-tained collaboration between biomedical and f nancial experts. For example, a key set of inputs into these simulations was the pairwise correlation of market valuations among projects in the portfolio; although we specif ed a f xed value of 20%, in prac-tice these correlations are likely to depend on the similarity of the underlying scien-tif c pathways, mechanisms, and targets on which the projects are based. As more em-pirical research is published on the histori-cal performance of individual biopharma investments, the estimation errors will be reduced. To facilitate this process, our simu-lation sof ware is available online with an open-source license that allows others to use, modify, and redistribute it.
MEGAFUND SIMULATIONS
Fernandez et al. (8) presented results of a detailed set of simulation experiments in-cluding stochastic phase transitions, corre-lations, and management of cash f ows for future clinical trials. T eir framework uses a multistate, multiperiod approach in which transitions occur according to a Markov-chain transition matrix and all costs and valuations are drawn from (capped) log-normal distributions. Investigational drugs are only given further investment for later-stage trials if there is suf cient capital for short-term debt-coupon and principal pay-ments. If suf cient capital is not available, the compounds either are sold to cover debt payments or held until additional capital be-comes available.
Fagnan et al. (9) extend this framework by analyzing the impact of third-party de-fault guarantees for the debt tranches. Such guarantees can increase the attractiveness of research-backed obligations (RBOs) to both equity and bond holders with relatively low expected cost. More recently, Fagnan et al. (4) explore simulations focused on rare diseases, highlighting their suitability for inclusion in a megafund as a result of several factors, in-cluding higher chance of success, lower clini-cal costs, and faster average approval times.
We modeled the NCATS portfolio as a hypothetical private-sector megafund, ig-noring any potential public-private partner-ship benef ts and the value of new IP, such as
general translational medical expertise and patents generated by NCATS sta$ indepen-dently or jointly with collaborators. Follow-ing the approaches in (8) and (4), we consid-ered an RBO structure consisting of a senior tranche, a mezzanine tranche, and an equity tranche. Because of the complexities of the debt-coupon and principal payments and the drug-approval process, numerical simula-tions were used to evaluate the f nancial per-formance of the RBO securities. We focused on early-stage investments, simulating the sale of preclinical projects upon completion of phase 2 clinical trials, if successful. T is early stage represents a particularly challeng-ing part of the drug-development process for which funding is scarcest and traditional f -nancing models have struggled. In addition to the calibration of inputs discussed in the previous section, we made a key change from (4) by using a more realistic model for sto-chastic clinical times by use of a log-normal distribution, abandoning the Markov-chain approach used in many previous studies, which implicitly imposes a geometric distri-bution of stage duration (results for alterna-tive distributions are provided in the supple-mentary materials).
T e results of three sets of simulations using the NCATS rare-disease portfolio–calibrated parameters are shown in Table 1, with each set based on 2 million simulated paths. Each set of simulations acquires sole-ly preclinical compounds, with the intent to carry the compounds through completion of a phase 2 trial. T e f rst set of simulations consisted of an RBO structure in which the senior and junior debt tranches were as-sumed to pay 5 and 8% semiannual coupon rates, respectively. Using capital of $420 million ($189 million in debt, $231 million in equity), 16 preclinical compounds were acquired and funded. T e second set of simulations consisted of an all-equity struc-ture in which nine preclinical compounds were acquired by using a similar amount of equity capital ($230 million) as in the f rst simulation. T e third set of simulations was similar to the RBO structure but contained the added feature of a third-party default guarantee for the junior debt tranche, pro-tecting the principal of these bond holders in case of default. T is guarantee has the ef-fect of shif ing the junior debt tranche into the senior tranche, yielding a single (senior) debt issue for the RBO structure. All three simulations used a maximum 11-year hori-zon, including a 6-month set-up time and 1 year for terminal liquidation of projects.
Fig. 2. Simulation calibration. Shown are weighted averaging of parameter estimates based on NCATS rare-disease portfolio, valuation panel, and literature estimates (4), using prior belief weights (methodological details are provided in the supplementary materials).
SourceDDT 2014NCATS Obs.Combined
Phase II
Probability of success
0.00 0.25 0.50 0.75 1.00 0 10 20 30
0 20 40 60 80 0 2 4 6 8
Duration (months)
Value ($ millions) Cost ($ millions)
Phase I
Preclinical
Phase II
Phase I
Preclinical
CR
ED
IT: H
. M
CD
ON
ALD
/SC
IEN
CE
TR
AN
SLA
TIO
NA
L M
ED
ICIN
E

26
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
P E R S P E C T I V E
www.ScienceTranslationalMedicine.org 25 February 2015 Vol 7 Issue 276 276ps3 5
In addition to the performance metrics used in (4), we included two other metrics in order to provide a more detailed comparison. Motivated by industry practice, we included the mean raw return, with no discounting performed (for example, a mean raw return of 2.0 would mean that for every $1 of equity capital committed, an average of $3 was re-turned at the end of the simulation). In ad-dition to the internal rates of return for the all-equity simulation, we included the modi-f ed internal rates of return (MIRR) on net cash f ows, for which the f nancing rate for negative cash f ows was set to zero. T e MIRR
was computed by f xing the f nancing rate at zero and solving iteratively until the average MIRR equaled the (forward) reinvestment rate (supplementary materials).
As shown in Table 1, the average annual-ized return on equity for the all-equity model is 11.6%; this corresponds to a substantially higher internal rate of return of 26.7%, re-sulting from the possibility of equity holders receiving cash payments sooner than at the end of the 11-year horizon. By adding se-nior and junior debt of $105 million and $84 million, respectively, the average annualized equity return was increased to 14.7%, with
a corresponding MIRR of 21.6%, which is higher than the 18.3% MIRR simulated for the all-equity model. Although it is useful for comparison, the MIRR might not be a realis-tic performance measure for a structure with debt because the full amount of capital might need to be held as collateral.
Also shown in Table 1, the default risk to the bonds is quite low, with a <1 basis point default rate on the senior tranche, which is comparable with the historical performance of bonds with the highest credit ratings. Ig-noring discounting, the average benef t to equity holders when bonds are also used to
Table 1. Structure and function. Simulated performance comparing an all-equity structure (using no debt fi nancing); an RBO structure using a senior and junior debt tranche paying 5 and 8% annual coupon rates, respectively; and a second RBO structure with a single guaranteed senior tranche. The senior tranche is paid before the junior (mezzanine) tranche, which is paid before the equity holder. In the event that the fund defaults or fails to meet its debt obligations, the guarantor will pay the diff erence. Each structure acquires only preclinical compounds, with a target goal of reaching phase 3 within a maximum horizon of 11 years. Dashes indicate cases in which the corresponding type of fi nancing and/or guarantee is not used. IRR, internal rate of return; ROE, return on equity.
Simulation results All equity
(similar equity)
Research-backed
obligation (RBO)
RBO with guarantee
(no mezzanine)
Number of compounds
Preclinical or IND-enabling 9 16 16
Research impact
Number sold in phase 2 0.4 1.9 1.6
Number sold in phase 3 3.4 5.3 5.6
Liabilities
Capital ($ millions) 230 420 420
Senior tranche ($ millions) — 105 189
Junior tranche ($ millions) — 84 —
Equity tranche ($ millions) 230 231 231
Guarantee ($ millions) — — 100
Equity tranche performance
Equity tranche performance 3.25 5.14 5.32
Average IRR 26.7% N/A N/A
Average MIRR (0% fi nancing) 18.3% 21.6% 22.7%
Average annualized ROE 11.6% 14.7% 15.4%
Probability (equity wiped out) 1.3 bp 0.52% 0.34%
Probability (return on equity <0) 8.0% 6.2% 5.1%
Probability (return on equity >10%) 61.9% 76.8% 78.6%
Probability (return on equity >25%) 2.2% 10.4% 11.0%
Debt tranches performance
Senior tranche: default probability, expected loss (bp) — 0.1, <0.1 <0.1, <0.1
Junior tranche: default probability, expected loss (bp) — 50, 15 —
Guarantee performance
Probability (cost of guarantee >0) — — 0.3%
Expected cost, 2% discount ($) — — 65,000
No-arbitrage cost of guarantee ($) — — 110,000

27
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
P E R S P E C T I V E
www.ScienceTranslationalMedicine.org 25 February 2015 Vol 7 Issue 276 276ps3 6
f nance the megafund was an almost twofold increase over the initial equity investment.
As a result of the increased amount of capital and larger number of projects, the probability of loss to the equity tranche for the RBO structure was only 6.2%, compared with 8.0% for the all-equity model. T e use of debt also increased by a factor of nearly 5, and the probability of annualized returns was in excess of 25%. Moreover, this f nanc-ing structure yielded an additional 1.9 proj-ects completing phase 2 trials as compared with an all-equity model that used a com-parable amount of equity capital.
A further increase in returns can be obtained by the addition of a third-party guarantee of $100 million, presumably pro-vided by either a government agency or a philanthropic organization. Specif cally, we considered a guarantee that had the e$ ect of combining the two debt tranches into one single senior tranche paying a 5% coupon rate. In addition to potential fundraising benef ts and higher bond ratings, the im-pact of this guarantee on equity returns was substantial, increasing the average annual-ized return on equity from 14.7 to 15.4%. Despite the high face value, the expected discounted cost to the guarantor was quite small, at $65,000, with an estimated Black-Scholes price of $110,000 (details are pro-vided in the supplementary materials).
A sensitivity analysis of these results is provided in the supplementary materials, in which we describe the same simulation experiments conducted under a variety of di$ erent parameter values. One illustra-tive example used a 15% relative decrease in success probabilities at each project stage, which caused the simulated return on equity for the RBO to drop from 14.7 to 10.6%—still an attractive investment in the current economic climate. Moreover, under this alternate specif cation the default risk to the senior bond did not increase, where-as the junior bond default rate increased by only 18 basis points.
BREAKING WITH TRADITION
In response to the growing consensus that traditional models for f nancing drug dis-covery are inadequate, a number of alter-nate business models and funding struc-tures have emerged. Although drug royalty companies such as Royalty Pharma (10) have achieved f nancial success in funding later-stage drug development, they have not yet played a large role in the earlier stages. And despite promising simulation results,
the megafund structure has yet to be imple-mented in practice. T e NCATS portfolio of rare-disease therapeutics provides a live example with which to calibrate megafund simulations for orphan drug portfolios.
At the time of this analysis, the NCATS rare-disease portfolio has been in operation for only 4 years; hence, none of the port-folio projects has reached FDA approval. Nevertheless, the combination of NCATS data and industry averages allows us to provide an interim f nancial analysis of the viability of the megafund structure for f -nancing early-stage translational medicine research involving rare diseases. Our simu-lations show that a rare-disease megafund based on the NCATS business and opera-tion model could achieve average annual-ized returns from 12 to 15% depending on the debt structure and with substantially higher internal rates of returns, a metric of en used by the VC industry. T e issu-ance of a guarantee on the debt can increase clinical impact per dollar of equity, return on equity, and fundraising potential for the debt. In particular, the average impact of adding guaranteed debt to the traditional all-equity model is an increase in the total cash payout to equity holders of twice their initial equity investment.
T ese simulation results must be quali-f ed by the caveat that they are only simula-tions—not actual investment returns—and are based on a large set of assumed param-eter values, some of which can be specif ed only imprecisely. For example, a key driver of the market value of candidate drugs is the cumulative sum of their future potential sales, and it is well known that drug sales are notoriously dif cult to forecast (6). Sci-entists are of en dismayed by the inaccuracy of f nancial forecasts, which are sometimes orders of magnitude more uncertain than the outcomes of laboratory experiments. T is imprecision is an unavoidable feature of f nancial investments of all types, includ-ing biotech; nevertheless, investors con-tinue to invest in the stock market despite comparably inaccurate forecasts of corpo-rate earnings (11). Recent examples of other uncertain investments for which the meth-ods described in this paper have been suc-cessfully applied include music royalties, Hollywood f lms, and the future earnings of professional athletes. In each of these cases, investors understand the limitations of his-torical and simulated performance metrics and are, nevertheless, willing to invest as long as they have some sense of what that
uncertainty entails [for example, the credit analysis underlying the securitization of f lm rights (7)]. T e analysis presented in this article and our open-source sof ware are intended to address this need for the biopharma industry.
T e use of NCATS data to calibrate our simulations and as a template for an orphan-disease megafund might also seem optimistic at best, given the dearth of evi-dence regarding the economic impact of this f edgling organization. However, on 9 July 2014 the NCATS rare-disease portfo-lio collected a pair of data points: Two of its portfolio partner-companies were inde-pendently acquired by large pharmaceuti-cal companies. AesRx, LLC, was acquired by Baxter International, Inc. ($15 million upfront, up to $278 million and $550 mil-lion in future development/regulatory and sales milestone payments, respectively), and BIKAM Pharmaceuticals was acquired by Shire ($2.5 million upfront, up to $92 million in future development/regulatory/sales milestone payments). As with most biopharma acquisitions, even these ob-servable market transactions are not trivial to value because of the many contingent payments that are triggered by conf den-tially specif ed events. However, a crude but commonly used (12) approximation of the economic value of these transactions can be computed by measuring the 1-day impact on the stock prices of the acquirers when these deals were announced on 9 July 2014: $238.3 million for Baxter and $423.1 mil-lion for Shire (supplementary materials), for a total of $661.4 million. As noisy as these estimates are, they provide the most current commercial assessment of the po-tential economic value generated by the NCATS rare-disease portfolio.
T e fact that NCATS does not use f -nancial return as a metric of its success suggests that our simulated megafund re-turns are conservative estimates of what can be achieved by a purely prof t-driven private-sector institution. T is nonf nan-cial motivation is embedded in both project selection and the operation of the TRND and BrIDGs programs. For example, some TRND applications were selected solely on the basis of the severity of unmet medical needs, even though the applicant did not have IP ownership of the proposed investi-gational drugs. T is selection bias increases the risk that certain NCATS projects may never attract commercial interest from the private sector, which could substantially re-

28
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
P E R S P E C T I V E
www.ScienceTranslationalMedicine.org 25 February 2015 Vol 7 Issue 276 276ps3 7
duce the economic valuation of the NCATS rare-disease portfolio. Operationally, ap-proaches are taken by NCATS to ensure the maximum success rate at the lowest cost to taxpayers by launching key project studies sequentially at the preclinical stage, which increases the average time to IND relative to running key project studies in parallel to accelerate the speed to proof of concept, a common industry practice. In practice, a megafund would apply more sophisticated f nancial analytics to balance the cost of multiple projects and project-related stud-ies against the benef ts of higher success probability so as to achieve the best risk-adjusted return for investors. Because of the complex and dynamic nature of drug development—which requires deep do-main expertise at every step of the portfolio management process—we postulate that building shared drug-development infra-structure within a megafund can maximize operational ef ciency and enhance the fund’s risk-adjusted return.
T e NCATS TRND and BrIDGs pro-grams underscore the fact that translational science is a team endeavor, and rare-disease research, in particular, relies heavily on aca-demia, the biotech and pharma industries, patient communities, advocacy groups, reg-ulators, and government support (through both NIH and legislation). T e ability to tap into resources from these various stake-holders can save tremendous amounts of time and money by ensuring that the right studies are designed and conducted, the right patient populations are recruited, and the proper regulatory guidance is obtained at the earliest relevant time. Such a busi-ness model, supported by the appropriate private-sector f nancing structures, can
help the translational medicine community traverse the translational Valley of Death.
SUPPLEMENTARY MATERIALSwww.sciencetranslationalmedicine.org/cgi/content/full/7/276/276ps3/DC1
Table S1. Observations of NCATS rare-disease projects including success, duration, and cost of trials.
Table S2. Prior weight given to literature data for orphan dis-eases (4), with lower values relying more on the NCATS obser-vations.
Table S3. Posterior estimates of parameters for simulating an NCATS rare-disease megafund, combining literature estimates for orphan diseases (4).
Table S4. NCATS portfolio of rare-disease projects in TRND and BrIDGs.
Table S5. Summary of key comments from valuation panel re-spondents when asked to value a portfolio of rare-disease proj-ects within NCATS.
Table S6. Panel median valuations compared with literature es-timates for orphan diseases (4).
Table S7. Parameters and distributions used in simulation framework for an NCATS rare-disease megafund.
Fig. S1. Plot of density functions for various Phase 2 clinical trial time distributions calibrated by matching fi rst and second mo-ments.
Table S8. Performance metrics for RBO structure (without guar-antee) from Table S2 for alternative clinical trial time distribu-tions.
Table S9. Calibrated parameters for valuation distributions at phase 3.
Fig. S2. Plot of density functions for various Phase 3 valuation distributions calibrated using fi rst and second moment match-ing.
Table S10. Performance metrics for RBO structure (without guarantee) from Table S2 for alternative valuation distributions.
Table S11. Performance metrics for RBO structure (without guarantee) from Table S2 for adjusted probability of success ap-plied to all stages.
Fig. S3. Performance metrics for RBO structure (without guar-antee) from Table S2 for adjusted probability of success applied to all stages.
Fig. S4. Performance metrics for RBO structure (without guaran-tee) from Table S2 for adjusted mean and standard deviation of Phase 3 valuation.
Table S12. Performance metrics for RBO structure (without guarantee) from Table S2 for adjusted mean and standard de-viation of Phase 3 valuation.
Fig. S5. NCATS rare disease portfolio diversity by disease and drug modality.
REFERENCES AND NOTES 1. The Global Genes Project, “The Global Genes Project”
(2014); https://globalgenes.org/rare-diseases-facts-
statistics.
2. National Organization of Rare Diseases, 4 January 2013;
www.rarediseases.org/news-events/news/30-years-oda.
3. FDA, Search orphan drug designations and approvals;
www.accessdata.fda.gov/scripts/opdlisting/oopd.
4. D. E. Fagnan, A. A. Gromatzky, R. M. Stein, J. M. Fernan-
dez, A. W. Lo, Financing drug discovery for orphan dis-
eases. Drug Discov. Today 19, 533–538 (2014).
5. Scientifi c Management Review Board, Report on Transla-
tional Medicine and Therapeutics (NIH, Bethesda, 2010).
6. M. Cha, B. Rifai, P. Sarraf, Pharmaceutical forecasting:
Throwing darts? Nat. Rev. Drug Discov. 12, 737–738
(2013).
7. DBRS, Inc., Rating Global Film Rights Securitizations
(DBRS, New York, 2010).
8. J.-M. Fernandez, R. M. Stein, A. W. Lo, Commercializing
biomedical research through securitization techniques.
Nat. Biotechnol. 30, 964–975 (2012).
9. D. E. Fagnan, J. M. Fernandez, A. W. Lo, R. M. Stein, Can
fi nancial engineering cure cancer? Am. Econ. Rev. 103,
406–411 (2013).
10. A. W. Lo, S. V. Naraharisetti, New fi nancing methods in
the biopharma industry: A case study of Royalty Pharma,
Inc. J. Invest. Manag. 12, 3–19 (2014).
11. S. Ro, CHART: 27 years of failed Wall Street earnings fore-
casts, 18 December 2012; www.businessinsider.com/
gerard-minack-forecasting-earnings-2012-12.
12. J. Y. Campbell, A. W. Lo, A. C. MacKinlay, The Econometrics
of Financial Markets (Princeton Univ. Press, Princeton, NJ,
1996).
Acknowledgments: We thank C. P. Austin and NCATS—es-
pecially the TRND and BrIDGs staff s—for their support and
cooperation throughout this study. We also thank J. Broderick,
J. Cummings, A. Gadicke, I. Ganot, T. McGuire, B. Stephenson,
participants in the NCATS-MIT meeting on 28 January 2014,
and three anonymous reviewers for helpful comments and
discussion. Funding: We gratefully acknowledge research
support from the MIT Laboratory for Financial Engineering.
This research was supported in part by the Intramural Re-
search Program of the NIH, NCATS. Competing interests: The
authors declare that they have no competing interests.
Citation: D. E. Fagnan, N. N. Yang, J. C. McKew, A. W. Lo, Financ-
ing translation: Analysis of the NCATS rare-diseases portfolio.
Sci. Transl. Med. 7, 276ps3 (2015).
10.1126/scitranslmed.aaa2360

29
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org Originally published 8 April 2015
www.ScienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282cm2 1
C O M M E N TA R Y
“ ”
SEEKING NOURISHMENT
Biomedical innovations arising from aca-demic settings of en f nd their way to trans-lation by chance: scouting by industry, personal relationships with academic and industrial key opinion leaders, or individu-al entrepreneurial ef orts (forming spin-of companies), for example. Some say that this is to be expected because most academic biomedical research falls into the category of “discovery,” which includes extend-ing general understandings of operational principles and biological mechanisms; in other words, basic research. Many investi-gators do apply this knowledge to address-ing disease pathogenesis and developing therapeutics and medical devices (applied research). However, very few academic dis-coveries are appropriate to seriously con-sider translating.
Clinical development of new therapeutic strategies—from identifying lead candidates to their animal model and human safety and ef cacy testing to their approval and f nal product release—is driven primarily by the biotech and pharmaceutical industries. In-dustry funds more life science research and development than all academic enterprises; worldwide, about US $200 billion—about US $90 billion alone in the United States—went to R&D in life science last year. About
70% of this R&D budget was invested by in-dustry, 13% by academia (1, 2).
Academic partners generally play a rather passive role during this translational process for drug and medical device devel-opment, restricted of en to preclinical test-ing of device prototypes and drug lead can-didates and limited clinical testing of new drug candidates in phase II/III trials. Fur-thermore, industry-driven developments frequently fail at late stages, owing partly to inadequate relationships with clinical scientists that result in critical def ciencies (inappropriate animal models, poor human adaptations of preclinical device designs, or inaccurate dosage scaling from preclinical to clinical studies).
Currently elevated socioeconomic pres-sures and trends toward more individual-ized therapies amplify the technical chal-lenges for developing new therapies. In parallel, regulatory hurdles have increased in recent years; in addition to conventional therapeutic principles, such as small mol-ecules, devices, and biologics, a new thera-py class—the advanced therapy medicinal products (ATMPs), covering cell therapy, gene therapy, and tissue engineering—has been def ned by the United States Food and Drug Administration (FDA) and the Eu-ropean Medicines Agency (EMA). Similar discussions are ongoing for conventional medical devices as well as combination devices. Requirements for asserting safety to proceed into human trials have become more rigorous and complex, meaning more time and money are required to fulf ll regu-latory expectations. But money is drying up, too; industry and venture capital are pulling away from the high-risk, early-stage collab-orations and partnerships with academia, reducing opportunities for successfully tra-versing the translational path.
As a result of the confusing translational agenda and accompanying mix of require-
ments and priorities, we in academia now experience an increasing discrepancy be-tween general academic goals to discover and a more mature development of innova-tive therapeutic concepts from such knowl-edge toward application. Academicians are at the ill-def ned crossroads of risk-taking, funding, translation, discovery, and profes-sional advancement. As a result, ef orts and resources are of en wasted on misguided intentions and misunderstandings of what constitutes translation; what few, but se-lect, qualif ed ideas are best translated; and who is qualif ed to do this important task. Infrastructure, expertise, and resources nec-essary to enable this process are of en not present or poorly used.
In a consensus statement issued from the results of discussions at the recent Translate 2014! event in Berlin, Germany, a mindset that supports valid, ef cient biomedical translation was forwarded (3). In that con-sensus, the authors asserted the need for a proper “well-oiled research infrastructure” that would vet and sort innovations, iden-tify solutions to unmet clinical needs, and move the most promising technologies for-ward. T us, a supply of essential infrastruc-ture, expertise, and resources is requisite to “nourish” translational academic research through to clinical proof of mechanism (PoM) or proof of concept (PoC) (Fig. 1). Here, we attempt to identify important translational nourishment “checkpoints” associated with challenges in resources and structures needed to facilitate ef cient and correct transitions from basic research to specif c targeted applications through to their clinical validation.
STEP 1: SELECTING TRANSLATIONAL
PROJECTS
Because very few discoveries are appropri-ate for translation, a critical translational process is the f rst step of early-stage idea selection. If selection strategy is poor, this step can be exceedingly costly and waste-ful. Proper selection of candidate projects among the plethora of projects claiming translational value is challenging. Techno-logical feasibility, probability of success, intellectual property value, reasonable de-velopment costs and timelines to PoM and PoC, importance of the unmet medical need, requests from the end users (physi-cians), and clear regulatory requirements must all be considered carefully in this se-lection process.
Assessing the unmet medical need. Be-
I N N O V AT I O N
Key elements for nourishing the translational research environment
Hans-Dieter Volk,1,2* Molly M. Stevens,3,4,5 David J. Mooney,6
David W. Grainger,7 Georg N. Duda1,8
*Corresponding author. E-mail: [email protected]
1Berlin-Brandenburg Center for Regenerative Therapies (BCRT), Charité–Universitätsmedizin Berlin, Germany. 2Institute for Medical Immunology, Charité–Uni-versitätsmedizin Berlin, Germany. 3Department of Materials, Imperial College London, London SW7 2AZ, UK. 4Department of Bioengineering, Imperial College London, London SW7 2AZ, UK. 5Institute for Biomedical Engineering, Imperial College London, London SW7 2AZ, UK. 6Wyss Institute and Harvard School of Engi-neering and Applied Sciences, Cambridge, MA 02138, USA. 7Department of Pharmaceutics and Pharmaceuti-cal Chemistry, and Department of Bioengineering, University of Utah, Salt Lake City, UT 84112, USA. 8Julius Wolf Institute, Charité–Universitätsmedizin Berlin, Germany.
Translation in an academic environment requires a support system—people, goals, models, partnerships, and infrastructures—that will push promising basic science and technology projects forward into the clinic.

30
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282cm2 2
C O M M E N TA R Y
“ ”cause they serve at the pa-tient interface and of en identify unmet needs, ju-nior clinicians should be engaged early in transla-tional development, includ-ing in the formal educa-tion and student training processes. Early exposure could involve research/clinical rotations and inter-disciplinary training expe-riences that cross dif erent medical and research f elds. Such an introduction pro-vides initial understanding to identify the underlying clinical needs and to assess them in the context of clini-cal practices, priorities, and preferences. Careful screen-ing and scouting of the state-of-the-art approaches are important to recognize benchmarks for success in any given f eld. Early health technology assessments will help to identify cur-rent product and practical def ciencies and def ne the putative cost/value ratio re-lated to addressing the un-met medical need.
Transforming basic knowledge into ideas and candidates for translation. As a primary source of discovery, basic scientists may be unaware of translational opportunities and their intrinsic challenges; thus, within an institution it is important to associate them with academic translational centers. T is will also help to engage them in translation-al projects that require basic science—for example, clinical trials integrating mecha-nism-based research. An internal scouting system at academic centers can also help to identify promising basic research proj-ects. Basic scientists should be involved in decision-making boards within academic translation centers (steering committees, technology assessment, and outcomes pan-els) and be extended professional and aca-demic incentives to experience and engage in translational research.
Cutting-edge technologies from innova-tive fundamental ideas. Key issues in assess-ment of early-stage concepts for translation include technical feasibility, reasonable development costs, appropriate regulatory requirements and pathways, intellectual
property scenarios, and freedom to operate. Early feasibility studies assessing these fac-tors with each new technology are essential, as will be full analysis of manufacturing and regulatory hurdles to be faced later in the translational process.
Needs. A translational support structure at academic centers that critically evaluates the requirements for translating each con-cept is essential to better facilitate, stream-line, and improve the selection processes. Such a support group should supply the fol-lowing:
• An opportunity check (before start of translation): technological and f nancial fea-sibility assessments, analysis of targeted un-met medical needs, cost/value ratio of end product, advice on the therapy category for regulatory guidance, and putative industrial partners.
• Risk assessment procedures: routine checks on project progress, new opportuni-ties, and challenges arising over time that require a willingness to fail/explore multiple ideas in parallel.
• Preregulatory support: identif cation of
appropriate disease mod-els and end points, study design and validation, and adequate documentation of preclinical work.
• Core facilities: bio-marker laboratories, good laboratory practice (GLP) animal research facilities, and good manufacturing practice (GMP) production.
• Intellectual property support: prior art searches (including patent and prod-uct searches in databases), patenting strategies, free-dom to operate analysis, and strategic patent advice/support.
• Early health technol-ogy assessment (HTA): potential for payer reim-bursement and cost-benef t analysis.
• Partnering opportuni-ties: academic and indus-try partners, including li-censing models, return on investment (ROI) assess-ments, and reward based on assumption of risk.
• Funding support for bridging basic to transla-
tional R&D mechanisms. • Acknowledgment of the value of trans-
lational research that does not result in technical publications, and ability to reward individuals who play substantial roles in translational teams and products.
Building these infrastructures requires long-term funding to hire capable, com-mitted people experienced in technical in-novation and to make the entire endeavor a “living concept” that all interested scientists at an academic center can be trained to ap-preciate and become involved with when appropriate and required.
STEP 2: CLINICALLY RELEVANT IN
VITRO AND IN VIVO STUDIES
(PRECLINICAL POC)
Approval for testing novel therapies in pa-tients requires quality preclinical PoC stud-ies as a key element. Most conventional in vitro and in vivo biomedical research ex-periments and study designs do not attain su$ cient quality, precision, reproducibility, documentation, and clinical relevance or prediction to qualify as reliable preclinical
Fig. 1. The nature of nurture. Following the mandates identifi ed by accurately assessing unmet clinical needs, the most appropriate translational approaches to address these needs are advanced to candidacy. Validation of the strategy with judicious, proven preclinical models, validation criteria, and markers is critical to achieve confi dent proof of concept before clinical testing. Clinical performance might be further optimized by iterative returns to modifi ed bench prototypes, new preclinical testing, and improvements to aid other important commercial fac-tors, including manufacturing, packaging, and sterilization.
Translational
ideas/candidates
Step 1: Selecting translational projects
Step 2: Clinically relevant in vitro and in vivo
models (preclinical PoC)
Step 4: “Back to bench
and forth to bed”
iterative improvements
Step 3: Proof-of-mechanism/proof-of-concept (PoM/PoC)
clinical studies
(including accompanying research/biomarker studies)
Cutting edge
technologies
Unmet
medical need
CR
ED
IT: C
. B
ICK
EL/S
CIE
NC
E T
RA
NSLA
TIO
NA
L M
ED
ICIN
E
www.ScienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282cm2 2
C O M M E N TA R Y
“ ”cause they serve at the pa-tient interface and of en identify unmet needs, ju-nior clinicians should be engaged early in transla-tional development, includ-ing in the formal educa-tion and student training processes. Early exposure could involve research/clinical rotations and inter-disciplinary training expe-riences that cross dif erent medical and research f elds. Such an introduction pro-vides initial understanding to identify the underlying clinical needs and to assess them in the context of clini-cal practices, priorities, and preferences. Careful screen-ing and scouting of the state-of-the-art approaches are important to recognize benchmarks for success in any given f eld. Early health technology assessments will help to identify cur-rent product and practical def ciencies and def ne the putative cost/value ratio re-lated to addressing the un-met medical need.
Transforming basic knowledge into ideas and candidates for translation. As a primary source of discovery, basic scientists may be unaware of translational opportunities and their intrinsic challenges; thus, within an institution it is important to associate them with academic translational centers. T is will also help to engage them in translation-al projects that require basic science—for example, clinical trials integrating mecha-nism-based research. An internal scouting system at academic centers can also help to identify promising basic research proj-ects. Basic scientists should be involved in decision-making boards within academic translation centers (steering committees, technology assessment, and outcomes pan-els) and be extended professional and aca-demic incentives to experience and engage in translational research.
Cutting-edge technologies from innova-tive fundamental ideas. Key issues in assess-ment of early-stage concepts for translation include technical feasibility, reasonable development costs, appropriate regulatory requirements and pathways, intellectual
property scenarios, and freedom to operate. Early feasibility studies assessing these fac-tors with each new technology are essential, as will be full analysis of manufacturing and regulatory hurdles to be faced later in the translational process.
Needs. A translational support structure at academic centers that critically evaluates the requirements for translating each con-cept is essential to better facilitate, stream-line, and improve the selection processes. Such a support group should supply the fol-lowing:
• An opportunity check (before start of translation): technological and f nancial fea-sibility assessments, analysis of targeted un-met medical needs, cost/value ratio of end product, advice on the therapy category for regulatory guidance, and putative industrial partners.
• Risk assessment procedures: routine checks on project progress, new opportuni-ties, and challenges arising over time that require a willingness to fail/explore multiple ideas in parallel.
• Preregulatory support: identif cation of
appropriate disease mod-els and end points, study design and validation, and adequate documentation of preclinical work.
• Core facilities: bio-marker laboratories, good laboratory practice (GLP) animal research facilities, and good manufacturing practice (GMP) production.
• Intellectual property support: prior art searches (including patent and prod-uct searches in databases), patenting strategies, free-dom to operate analysis, and strategic patent advice/support.
• Early health technol-ogy assessment (HTA): potential for payer reim-bursement and cost-benef t analysis.
• Partnering opportuni-ties: academic and indus-try partners, including li-censing models, return on investment (ROI) assess-ments, and reward based on assumption of risk.
• Funding support for bridging basic to transla-
tional R&D mechanisms. • Acknowledgment of the value of trans-
lational research that does not result in technical publications, and ability to reward individuals who play substantial roles in translational teams and products.
Building these infrastructures requires long-term funding to hire capable, com-mitted people experienced in technical in-novation and to make the entire endeavor a “living concept” that all interested scientists at an academic center can be trained to ap-preciate and become involved with when appropriate and required.
STEP 2: CLINICALLY RELEVANT IN
VITRO AND IN VIVO STUDIES
(PRECLINICAL POC)
Approval for testing novel therapies in pa-tients requires quality preclinical PoC stud-ies as a key element. Most conventional in vitro and in vivo biomedical research ex-periments and study designs do not attain su$ cient quality, precision, reproducibility, documentation, and clinical relevance or prediction to qualify as reliable preclinical
Fig. 1. The nature of nurture. Following the mandates identifi ed by accurately assessing unmet clinical needs, the most appropriate translational approaches to address these needs are advanced to candidacy. Validation of the strategy with judicious, proven preclinical models, validation criteria, and markers is critical to achieve confi dent proof of concept before clinical testing. Clinical performance might be further optimized by iterative returns to modifi ed bench prototypes, new preclinical testing, and improvements to aid other important commercial fac-tors, including manufacturing, packaging, and sterilization.
Translational
ideas/candidates
Step 1: Selecting translational projects
Step 2: Clinically relevant in vitro and in vivo
models (preclinical PoC)
Step 4: “Back to bench
and forth to bed”
iterative improvements
Step 3: Proof-of-mechanism/proof-of-concept (PoM/PoC)
clinical studies
(including accompanying research/biomarker studies)
Cutting edge
technologies
Unmet
medical need
CR
ED
IT: C
. B
ICK
EL/S
CIE
NC
E T
RA
NSLA
TIO
NA
L M
ED
ICIN
E

31
REPRINTED ARTICLES
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282cm2 3
C O M M E N TA R Y
“ ”support for human safety assessments. Pre-clinical studies are divided into two catego-ries. T e f rst is adequate preclinical disease models with high clinical relevance (vali-dated, predictive models) that can be used for PoC comparable with planned clinical protocols and for biomarker validation. T e second type of preclinical study involves in vitro and ex vivo testing on patient-derived material (tissues, biopsies, or blood) to validate targets and ef ects and to discover clinical parameters and biomarkers for risk or outcome stratif cation of patients. All preclinical studies require adequate stan-dardization, bioinformatics analyses, qual-ity management, and documentation ac-cording to the Investigational New Drug/Investigational Medicinal Product Dossier guidelines for later submission to regulatory agencies such as FDA and EMA.
Needs. Preclinical studies are an impor-tant step for reducing risk from new devel-opments moving from basic science toward clinical application. Academia can learn from the high levels of both standardiza-tion and documentation in industry-driven preclinical studies. T ere is a substantial need for public and private grant organiza-tions to support this type of preclinical work because it is of en less enticing than testing new ideas or entering early clinical trials. In this vein, young scientists should be incen-tivized to fully evaluate the translational po-tential of their ideas by advocating the value of making science tangibly useful.
On the other side, academic translational centers should exploit their relatively easy access to clinical data and patient samples. T is requires the formation of (of en proj-ect-related) multidisciplinary teams com-prising physicians, engineers, and experts from translational support structures, as mentioned. It also requires high-level qual-ity management systems for preclinical data surveys. An expert board of clinicians and basic scientists is highly useful for discuss-ing the quality and relevance of preclinical in vitro and in vivo data before entering the next step of applying these data to initiate clinical trials.
Although key to translational ef orts, such preclinical model development and pa-tient sample analysis are more involved (re-garding cost, ef ort, and time) than are the preliminary “novel” studies of en reported by academicians in peer-reviewed literature. Moving too quickly past early model valida-tion and patient relevance studies to the pre-clinical “e$ cacy” studies can produce false
impressions of success for an early approach that is actually wasting valuable resources. It is better that ideas fail quickly and cheaply. T erefore, moving forward to mature phas-es of preclinical testing as suggested above requires careful selection of the project ma-turity and the type of potential product en-visioned (from low to high risk): predicate versus new mode-of-action products. Each project will have dif erent testing require-ments and levels of evidence.
STEP 3: CLINICAL POM/POC TRIALS
Although fundamental progress that takes basic science f ndings forward toward ap-plication is frequently an important goal of the academic research mission, a complete and mature biomedical translational pro-cess must reach a clinical PoM or PoC at a clinical trials level to produce any benef t in human patients. To make this substan-tial commitment and investment requires a discerning vetting process that does not fall within the typical core expertise of bio-medical academics. Clinical PoM/PoC is a key translational hurdle—and one most of en lef unattempted by basic researchers developing innovative new ideas. Vetting processes in translational pathways should both push the most promising ideas forward from discovery toward PoM/PoC while al-lowing distinct exits as early as possible in this process for those ideas that fail to ap-proach or surmount this clinical hurdle.
Because of f nancial and regulatory hur-dles, the “f rst in human trial” is the most challenging translational step in an aca-demic environment. However, investigator-driven studies can have more versatility as compared with classical industry-driven phase I/II study protocols. Key features that increase the value of investigator-driven trials include (i) highly selective and more f exible inclusion of “most appropriate” pa-tients (patient subgroups) by specialized academic centers, (ii) observation of treated patients by experienced clinical experts, (iii) accompanying (biomarker) research and functional assessment, and (iv) greater freedom to explore combination therapies. Because safety is the key issue of early-stage clinical trials, adequate regulatory and clini-cal trial management is a precondition.
Determining the therapy category for reg-ulatory processing. A therapy category rec-ognized by prevailing regulatory authorities should be def ned as early as possible (best case, at the preclinical project start) because this designation has a major impact on the
feasibility and ultimate success of the trans-lational project. Both regulatory and feasi-bility hurdles increase with the following sequence of therapy categories:
• Optimization of an approved therapy in the given indication.
• Of -label use of approved therapies in new indications (which requires new risk assessments and careful dosing).
• Biomarker-driven therapy by using ap-proved drugs (secondary companion diag-nostics for stratif ed therapy).
• Completely new therapies (need for complete preclinical studies, toxicology, phase I/IIa, for example).
• New therapies in patient subgroups based on biomarker prof les (companion diagnostics).
Regulatory hurdles. To jump the hurdles for obtaining all approvals needed for an investigator-initiated clinical trial, an ad-equate clinical development infrastructure is required. Dif erent levels of approvals are needed for new trials: (i) study protocol approval by regulatory authorities (such as EMA or FDA)—recent changes in Europe now allow one multinational application by using the Voluntary Harmonisation Proce-dure; (ii) obtain manufacturing authoriza-tion (if the therapeutic product is produced by the academic centers themselves); (iii) obtain institutional review board (IRB) ap-proval, ensure written informed consent from patients, and provide adequate insur-ance for the trial.
Accompanying biomarker studies. Aims of biomarker studies include identifying in vivo markers for safety, pharmacokinet-ics/pharmacodynamics, early therapeutic responsiveness, patient stratif cation, and nonresponder prof les to identify new tar-gets. Such biomarker research is the basis for improved understanding of the thera-peutic mode of action, reasons for non- or low response, and criteria for producing success or failure benchmarks or clinical trial end points, allowing more rational, it-erative improvements for new or next-step approaches.
Whereas the f rst three points listed above (in “therapy category”) are reasonable for experienced academic medical research centers, introduction of completely new therapies with or without companion diag-nostics is currently very challenging. How-ever, the increasing availability of academic and contract research organization (CRO)–based GMP-certif ed laboratories for manu-facturing biologics and ATMPs (e.g., gene

32
INNOVATION PARTNERSHIPS FOR 21ST CENTURY HEALTH CARE: THE AUSTRALIAN CHALLENGE
www.ScienceTranslationalMedicine.org
www.ScienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282cm2 4
C O M M E N TA R Y
“ ”therapy, cell therapy, tissue engineering) for clinical studies as required by regulatory au-thorities opens new opportunities for these academic translational centers to enable and direct even more complex, innovative trans-lational research goals, including completely new therapeutic approaches.
STEP 4: REFINED TRANSLATION—
ITERATIVE IMPROVEMENTS
T e commonly used one-way path from phase I to eventual approval and commer-cialization has several limitations because af er conf rming safety, it focuses on as-serting the statistical power of e$ cacy only. Hence, therapies can be approved even if many patients are nonresponders. Addi-tionally, a statistical failure frequently kills the project—a costly end point occurring far too of en at late stage. Insight into clini-cal trial designs that allow candidate ap-proaches to fail earlier at reduced expense or to modify trial designs to obtain less risky end points would improve e$ ciency in translation. Opportunities for moving back and forth during less costly, early phases of clinical development along the translational path in an iterative, f exible way are very useful before moving forward into the late-stage development. T e capacity to do such early, iterative risk reduction is an essential advantage of academic-based translational research approaches. T is f exibility also helps to direct more basic academic research toward mechanisms-oriented studies.
A “ref ned translation” process can be a facile iterative strategy going from “bed” back to “bench” and forth again to bed. T is process can dynamically respond to improve the original concept af er a deep analysis of initial PoM/PoC trials informed by early pa-tient data and allow performance of the next steps in clinical development with improved approaches, focus, trial designs, and ref ned clinical end points.
Analyzing data from early PoM/PoC clinical trials in detail, in particular from accompanying biomarker and clinical phe-notyping studies, provides valuable oppor-tunities to obtain important insights about trial failure in general or in individual pa-
tients (nonresponders). Basic science and technological investigations test the hypoth-esis, inform therapeutic metrics, improve the candidate pipeline, and bolster revised preclinical PoC studies. Although perhaps considered “iterative improvement,” inclu-sion of basic science in ref ned translation can better inform the second generation of PoM/PoC clinical trials. T is next genera-tion could feature a new design to verify the improvements, uncover new therapeutic approaches, and help to decide whether the approach or technology is ready to move forward to late clinical development (or go back for another iterative translational cycle).
Need. Reliable performance of investi-gator-driven early clinical PoM/PoC trials requires mature translational infrastructure and resources dedicated to covering regu-latory aspects; patient monitoring; safety management; GMP manufacturing; bio-informatics; biomarker development, vali-dation, and studies; and multidisciplinary groups of basic and clinical scientists. Be-cause independent structures within single clinics or institutes are not typically very cost-ef ective and professionally oriented toward translation, academic institutions of ering infrastructure with modern inter-disciplinary clinical research units have a great advantage.
CONCLUSIONS
T e model proposed here for a complete, comprehensive formalized translational re-search process that runs through all clini-cal phases, including the promising option of a ref ned internal translational process, requires long-term vision, expertise, and investment. T ese are required to recognize, acquire, and build key processes and capa-bilities, infrastructure, and resources that together nourish the translational research process while emphasizing strategy, e$ cien-cy, and careful decision-making. Academic translational centers that support multidis-ciplinary research, translational activities, and dovetailed educational programs may be able to optimize structures along our guidelines to improve translational research.
However, development of this capability also needs leadership and committed atti-tudes that overcome the many diverse chal-lenges in funding long-lasting structures and providing incentives for translational research (1). T e academic performance metrics require adjustments to reward those who pursue less elegant but more impact-ful research routes that lead—at substantial risk of failure—to patient quality-of-life improvements. In addition, collaborations between academia, biotech, and pharma industrial partners (4) must be facilitated at early development stages to produce new levels of interactions and access to mutual, shared expertise.
REFERENCES AND NOTES 1. E. R. Dorsey, J. de Roulet, J. P. Thompson, J. I. Reminick,
A. Thai, Z. White-Stellato, C. A. Beck, B. P. George, H. Mo-
ses 3rd, Funding of US biomedical research, 2003–2008.
JAMA 303, 137–143 (2010).
2. 2014 Global R&D Funding Forecast (2014); www.battelle.
org/docs/tpp/2014_global_rd_funding_forecast.pdf;
accessed March 2015.
3. G. N. Duda, D. W. Grainger, M. L. Frisk, L. Bruckner-Tuder-
man, A. Carr, U. Dirnagl, K. M. Einhäupl, S. Gottschalk, E.
Gruskin, C. Huber, C. H. June, D. J. Mooney, E. T. Rietschel,
G. Schütte, W. Seeger, M. M. Stevens, R. Urban, A. Veld-
man, G. Wess, H. D. Volk, Changing the mindset in life sci-
ences toward translation: A consensus. Sci. Transl. Med. 6,
264cm12 (2014).
4. A. M. Boccanfuso, Why university-industry partnerships
matter. Sci. Transl. Med. 2, 51cm25 (2010).
Funding: D.W.G. is grateful for support from the George S. and
Dolores Doré Eccles Foundation (USA) and the U.S. National
Institutes of Health (NIH). M.M.S. is supported by the UK Re-
generative Medicine Platform Hub “Acellular Approaches for
Therapeutic Delivery” (MR/K026682/1), which is funded by the
Medical Research Council, the Engineering and Physical Sci-
ences Research Council, and the Biotechnology and Biological
Sciences Research Council. D.J.M. is supported by the NIH. H.-
D.V. and G.N.D. are supported by the Berlin-Brandenburg Cen-
ter for Regenerative Therapies (BCRT) and Berlin-Brandenburg
School for Regenerative Therapies (BSRT), which are funded
by the German Federal Ministry of Education and Research,
the German Research Organization (DFGH), States of Berlin
and Brandenburg, Charité. Competing interests: The authors
declare no competing interests.
Citation: H.-D. Volk, M. M. Stevens, D. J. Mooney, D. W. Grainger,
G. N. Duda, Key elements for nourishing the translational re-
search environment. Sci. Transl. Med. 7, 282cm2 (2015).
10.1126/scitranslmed.aaa2049

20-397250_LakeCounty Ad.indd 120-397250_LakeCounty Ad.indd 1 9/21/20 10:30 AM9/21/20 10:30 AM

www.ScienceTranslationalMedicine.org