Embed Size (px)
Citation preview

CCR New Strategies
New Strategies in Endometrial Cancer: Targeting thePI3K/mTOR Pathway—The Devil Is in the Details
Andrea P. Myers1,2
AbstractEndometrial cancer is the most common gynecologic malignancy in the developed world and
affects approximately 40,000 women in the United States each year. The phosphoinositide 3-kinase
(PI3K) signaling pathway regulates key aspects of cancer biology including glucose uptake and
metabolism, cellular growth, and survival. Endometrial cancers harbor the highest rates of PI3K
pathway alterations reported to date. The PI3K pathway is highly druggable and several classes of
agents are in clinical development including rapalogs, pan-PI3K inhibitors, PI3K isoform-specific
inhibitors, dual PI3K/mTOR catalytic inhibitors, mTOR-specific catalytic inhibitors, and AKT
inhibitors. It has been 10 years since the initiation of the first studies of rapalogs as anticancer
agents. There are more than 20 registered clinical trials of PI3K/mTOR inhibitors as single agents or
in therapeutic combinations for the treatment of endometrial cancers. What have we learned from
the completed studies? What can we expect to learn from ongoing studies? What should we anticipate
moving forward? Clin Cancer Res; 19(19); 5264–74. �2013 AACR.
BackgroundEndometrial cancer
Endometrial cancer is the most common gynecolo-gic malignancy in the developed world and affectsapproximately 40,000 women in the United States eachyear (1, 2). Endometrial cancer is increasing in inci-dence, likely due to the growing epidemic of obesity,a strong risk factor for endometrial cancer (2–4).Although the majority of endometrial cancers are diag-nosed when localized to the uterus, up to 25% of casesrecur. Systemic therapies are limited in efficacy forrecurrent and metastatic disease and new therapies arein need (5).
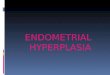
PI3K signalingThe phosphoinositide 3-kinase (PI3K) pathway (Fig. 1)
regulates key aspects of cancer biology including metab-olism, cellular growth, and survival (6). Upon stimula-
tion of receptor tyrosine kinases (RTK), PI3K phosphor-ylates the lipid phosphatidylinositol 4,5- biphosphate(PIP2), creating phosphatidylinositol 3,4,5- triphos-phate (PIP3) (7). PIP3 recruits pleckstrin homologydomain-containing proteins, including the proteinkinase AKT, to the membrane. AKT is phosphorylatedand activated by mTOR complex 2 (mTORC2) and 3-phosphoinositide-dependent protein kinase 1 (PDK1;ref. 8). Among its targets, AKT phosphorylates and inhi-bits tuberous sclerosis complex 2 (TSC2) within themultiprotein TSC complex, which indirectly inhibitsmTOR complex 1 (mTORC1). Hence, PI3K-AKT signal-ing activates mTORC1, a key regulator of metabolismand biosynthetic processes (9, 10). PTEN hydrolyzesPIP3 back to PIP2, deactivating the pathway (11, 12).The PI3K pathway contains numerous negative feedbackloops and is intricately networked with other signalingpathways including the RAS–ERK pathway. Signals fromboth AMP-activated protein kinase (AMPK), a sensor ofenergy stress, and estrogens are also integrated into PI3Ksignaling (13–16).
PI3K in endometrial cancerEndometrial cancers harbor the highest rates of
PI3K pathway alterations reported to date (17). Theimportance of the PI3K pathway in endometrial can-cers was underscored by the identification of germlinemutations in PTEN as the etiology of Cowden syn-drome, an inherited cancer syndrome for which endo-metrial cancer is a diagnostic criterion (18, 19). High
Author's Affiliations: 1Gynecology Oncology Program, Division ofWomen's Cancers, Department of Medical Oncology, Dana-FarberCancer Institute; and 2Division of Signal Transduction, Departmentof Medicine, Beth Israel Deaconess Cancer Center, Boston,Massachusetts
Corresponding Author: Andrea P. Myers, Novartis Institutes for BioMed-ical Research, Inc. Oncology Translational Medicine, 220 MassachusettsAvenue, Cambridge, MA 02139. Phone: 617-871-4991; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-13-0615
�2013 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 19(19) October 1, 20135264
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

rates of somatic PTEN mutations were reported insporadic cases of endometrial cancers shortly thereaf-ter and genetically engineered mouse models con-firmed the role of PTEN loss in endometrial cancerdevelopment (20–24). Candidate gene approachesidentified high rates of PIK3CA (25%–40%) andPIK3RI (15%–25%) mutations, which encode the cat-alytic and regulatory subunits of the PI3K holoenzyme(25–27). Recently completed high-throughput muta-
tion detection as well as whole exome sequencingstudies have confirmed these reports and haveidentified mutations in other key PI3K pathway mem-bers (Fig. 1; refs. 17, 28).
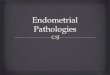
Targeting PI3KThe PI3K pathway is highly druggable and several
classes of agents are in clinical development (Fig. 2).The rapamycin analogs (rapalogs) directly bind and
ERBB2 amplification 15%FGFR2 mutation 13%
RTKInsulin andinsulin-like
growth factor
RAS p85
PIP2 PlP3p110
Pl3K
AKT
PPP2R1A
PDK
mTORC2
AKT1 mutation 2%AKT2 mutation 2.5%AKT3 mutation 5%PPP2R1A mutation 10%
???
PTEN
ERK
AMPK
Metformin
Estrogen
Nutrients
TSCcomplex
Cellsurvivalsignals
TSC1 mutation 4%TSC2 mutation 5%mTOR mutation 11%
NF2
NF2mutations 3%
Biomassgeneration
Proteintranslation
PTEN mutation 65%PIK3CA mutation 53%PIK3R1 mutation 34%PIK3CA amplification 15%
K-RAS mutation 20%
GF
mTORC1
© 2013 American Association for Cancer Research
Figure 1. Environmental signals and molecular alterations that may alter PI3K signals in endometrial cancer. Class Ia PI3Ks are holoenzymescomprised of a catalytic (p110) and regulatory subunit (p85) and can interact with RTKs upon their activation. PI3K phosphorylates PIP2 tocreate PIP3. PTEN hydrolyzes PIP3 to PIP2. With generation of PIP3, AKT is recruited to the membrane, phosphorylated and activated bymTORC2 and PDK. AKT phosphorylates and inactivates the TSC complex, which allows for downstream mTORC1 activation. RTK signaling alsoactivates the RAS pathway; ERK phosphorylates and suppresses TSC. AMPK senses cellular stress and nutrient availability and activatesTSC to suppress further growth signals. The role of PPP2R1A is less well defined but may have inhibitory effects on PI3K/mTOR signals. Rates ofsomatic mutation and amplification are shown in boxes. Reported rates were collected from The Cancer Genome Atlas data from cBIOPortal and may not represent functional mutations. Potential environmental signals common in endometrial cancer are shown in jaggedovals. Dashed lines represent indirect signals. PPP2R1A; Serine/threonine-protein phosphatase 2A 65 kDa regulatory subunit A a isoform;NF; neurofibromin; PIK3CA; the gene that encodes the p110 a catalytic subunit of PI3K; PIK3R1; the gene that encodes the p85 regulatorysubunit of PI3K.
Targeting the PI3K/mTOR Pathway in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 19(19) October 1, 2013 5265
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

allosterically inhibit mTORC1. Although they targetdownstream of PI3K they are often introduced as the firstclinical PI3K pathway inhibitors. Indeed, nearly 20 yearsof laboratory, translational, and clinical experience withthe rapalogs has offered great insight into basic PI3Ksignaling as well as potential pitfalls and challenges forclinical developing of these inhibitors as anticanceragents (29). Newer classes of PI3K pathway inhibitorsin clinical development include pan-PI3K inhibitors,
PI3K isoform-specific inhibitors, dual PI3K/mTOR cata-lytic inhibitors, mTOR-specific catalytic inhibitors, andAkt inhibitors (30, 31).
On the HorizonGiven the high rate of PI3K pathway alteration,
endometrial cancer seems to be an optimal diseasefor the development of PI3K pathway inhibitors.
© 2013 American Association for Cancer Research
PIP2
AKT
mTORC2
mTORC1
TSCcomplex
PIP3
αα
PI3KPI3Kβ
βδ
PI3Kβ
PI3K
Pan-PI3Kinhibitor
PI3K
PIP2
AKT
mTORC2
mTORC1
TSCcomplex
PIP3
AKTinhibitor
PI3K
PIP2
AKT
mTORC2
mTORC1
TSCcomplex
PIP3
PI3K
PIP2
AKT
mTORC2
mTORC1
TSCcomplex
PIP3 PI3K
PIP2
AKT
mTORC2
mTORC1
TSCcomplex
PIP3
PI3K/dualmTORC inhibitor
mTORCcatalytic inhibitor
PI3Kβinhibitor
α-PI3Kinhibitor
PI3K
PIP2
AKT
mTORC2
mTORC1
TSCcomplex
PIP3
Rapalog
α
Figure 2. Classes of PI3K/mTORpathway inhibitors. Themolecular targets of classes ofPI3K/mTOR pathway inhibitorsare shown in each panel.Rapalogs indirectly inhibitmTORC1. The Pan-PI3Kinhibitors target the three classIA PI3Ks (a, b, and d), which aredesignated by their p110catalytic subunits (a, b, and d).Dual PI3K/mTORC inhibitorstarget the Class Ia PI3Kisoforms, mTORC1, andmTORC2. mTORC catalyticinhibitors target mTORC1 andmTORC2. AKT inhibitors targetAKT. Isoform-specific inhibitorsinclude PI3Ka, PI3Kb, andPI3Kd and target theirrespective PI3K isoforms.
Myers
Clin Cancer Res; 19(19) October 1, 2013 Clinical Cancer Research5266
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

It has been 15 years since the initiation of thefirst studies of rapalogs as anticancer agents. Thereare numerous registered clinical trials of PI3K/mTOR inhibitors as single agents or in combina-tions for the treatment of endometrial cancers(Tables 1 and 2). What have we learned from thecompleted studies? What can we expect to learnfrom ongoing studies? What should we anticipatemoving forward?
The rapalogsRapalogs as single agents. Frommore than a half dozen
clinical trials of the rapalogs as single agents, it can beconcluded that rapalogs have a modest, but reproducibleantitumor activity in endometrial cancer (Table 1).Objective response rates range from 0%–30% dependingupon the clinical population; clinical response ratesare higher in populations that have not received priorchemotherapy and response occurs across histologicsubtypes including endometroid, high-grade papillaryserous, and clear cell cancers. Importantly, there is a sub-set, albeit small, of patients with complete and/or durableresponses (32–37).Predictive biomarkers for rapalogs. A molecular bio-
marker that predicts the clinical benefit of rapalogs hasyet to be identified for endometrial cancer. Several studieshave explored the association of molecular biomarkersand response (33, 38–40). The largest, most comprehen-sive study to date has been a combined analysis of threeNational Cancer Institute of Canada Clinical Trials Group(NCIC CTG) studies, each of which evaluated a rapalog assingle-agent therapy in advanced endometrial cancer(40). Seventy to eighty tumor samples were evaluatedfor common mutations in a set of 17 related cancer genesas well as for protein expression of PTEN and stathmin(STMN), a cytoskeletal protein with expression thatis associated with PI3K pathway activation (41). Thesestudies reported no association between clinical responserates and PTEN mutation, PIK3CA mutation, PTEN orSTMN protein expression.The strength of these studies is the large sample size.
Although the studies were exploratory in nature, giventhe rates of the PTEN mutations and protein loss,PIK3CA mutation and STMN expression in endometrialcancer, there was adequate power to detect clinicallymeaningful differences in outcomes of the definedmolecular subgroups. There were also weaknesses inthis study. First, the study population is clinically het-erogeneous and includes untreated and pretreatedpatients and patients who were treated with differentrapalogs. Second, although technologically advanced forthe time, the mutation analysis was limited to "hot-spots" and thus misclassification may have been intro-duced (26). Finally, associative analyses were limited toobjective response rates and did not include time toevent studies.Associative studies from the Group d’Investigateurs
Nationaux pour l’Etude des Cancers Ovariens (GINECO)
led study of everolimus were recently reported (38). Ina study of 34 patients, there was no identified asso-ciation of PTEN or PI3KCA mutation and clinical ben-efit. However, K-Ras mutation was associated with adecreased progression-free and overall survival in thispopulation.
Although imperfect and validation from other largerstudies is needed, these data suggest that PTEN andPIK3CA alterations are not reliable biomarkers for pre-dicting clinical benefit to the rapalogs and that K-Rasmutation may predict a group unlikely to benefit fromrapalogs. Indeed, these results are consistent with pre-clinical and translational data which highlight potentialclinical pitfalls of the rapalogs as single agents. Rapalogexposure relieves mTORC1-dependent negative feed-back loops affecting RTK signaling resulting in upregula-tion of both RAS-ERK and PI3K pathways (13). Tumorscan thus circumvent rapalog inhibition by relying onRAS-ERK signaling or PI3K signals that are independentof mTORC1.
Other candidate biomarkers. Although not yet molecu-larly defined, there remains a subset of patients who greatlybenefit from rapalog monotherapy. The clinical use ofprospectively classifying these patients mandates that wecontinue the search for a predictive biomarker. Recentclinical data on rapalogs in other cancers as well as labo-ratory studies of mTOR signaling suggest additional ave-nues to explore.
In bladder cancer, TSC1 mutation is associated withclinical response to a rapalog (42). Iyer and colleaguesconducted whole genome sequencing on archivedtumor from a patient who had a complete and durableresponse to everolimus. Analysis revealed mutations inTSC1 and neurofibromin 2 (NF2), genes whose proteinproducts regulate mTORC1 signaling. Targeted sequenc-ing of the tumors from the other trial participants iden-tified an association with TSC1 mutation and best tumorresponse. These data suggest that TSC1 and NF2 beevaluated as biomarkers for rapalogs in endometrialcancer and also highlight the benefit of deep sequencingexploration of tumors from patients with an unexpectedlevel and duration of benefit to molecularly targeteddrugs.
The perspective that mTORC1 functions only torelay proliferative signals from PI3K is a limited view ofmTORC1 regulation and function. Recent laboratory-based studies highlight that our understanding ofmTORC1 is incomplete. In addition to signals from theTSC complex, mTORC1 is directly regulated by othernutrient-sensing proteins including the recently de-scribed ragulator complex (43). In addition, two researchgroups have identified the importance of mTORC1 inregulating de novo pyrimidine synthesis by its phosphory-lation and activation of the enzyme CAD (carbamoyl-phosphate synthetase 2, aspartate transcarbamylase, anddihydroorotase; refs. 44, 45). Tumors with microsatelliteinstability have been reported to have CAD amplifica-tion, perhaps suggesting a heavy reliance on de novo
Targeting the PI3K/mTOR Pathway in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 19(19) October 1, 2013 5267
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

Tab
le1.
Com
pletedan
don
goingpha
seIIclinical
trials
ofsing
leag
entPI3K/m
TORpathw
ayinhibito
rsin
endom
etria
lcan
cera
Inve
stigationa
lag
ent
Target
Treatmen
tpopulation
NCT#
(dateregistered)
Clin
ical
resu
lts
(n)
Toxicities
Referen
ce
Temsirolim
usmTO
RC1
Che
mo-na
ïve
NCT0
0072
176
(11/20
03)
CR(0/33)
bMos
tco
mmon
�grad
e3
AEs:
fatig
ue,d
iarrhe
a,pne
umon
itis
33PR(4/33)
b
SD�
8wee
ksc(20/33
)
Temsirolim
usmTO
RC1
1prio
rline
NCT0
0072
176
(11/20
03)
CR(0/27)
Mos
tco
mmon
�grad
e3
AEs:
fatig
ue,d
iarrhe
a,pne
umon
itis,
dys
pne
a,hy
pok
alem
ia
33PR(1/27)
SD�
8wee
ksc(12/27
)
Eve
rolim
usmTO
RC1
1-2prio
rlines
dNCT0
0087
685
(7/200
4)CR(0/35)
PR(0/35)
SD�
8wee
ks(12/35
)
Mos
tco
mmon
�grad
e3
AEs:
fatig
ue,n
ause
alympho
pen
ia,a
nemia,
hyperglyc
emia
32
Ridaforolim
use
mTO
RC1
1-2prio
rlines
NCT0
0122
343
(7/200
5)CR(0/45)
Mos
tco
mmon
�grad
e3
AEs:
anem
ia,
hyperglyc
emia,m
outh
sores
35PR(5/45)
SD�
16wee
ks(8/45)
Ridaforolim
usmTO
RC1
Adjuva
nton
lyNCT0
0770
185
(10/20
08)
CR(0/35)
Mos
tco
mmon
�grad
e3
AEs:
lympho
pen
ia,a
nemia
36PR(2/35)
SD�
8wee
ksc(15/35
)
Ridaforolim
us(vs.proge
stins)
mTO
RC1
1-2lines
NCT0
0739
830
(8/201
0)CR(0/64)
bMos
tco
mmon
�grad
e3
AEs:
anem
ia,
hyperglyc
emia,b
ackpain,
asthen
ia
37PR(0/64)
b
SD�
8wee
ksc(22/64
)med
ianPFS
3.6vs
.1.9mon
ths(ridaforolim
usvs
.proge
stins)
Eve
rolim
usmTO
RC1
1-2prio
rlines
NCT0
0870
337
(3/200
9)CR(0/44)
Mos
tCom
mon
�grad
e3
AEs:
fatig
ue,a
norexia,
infection,
diarrhea
,lympho
pen
ia,a
nemia,
thromboe
mbolic
even
t,hy
perglyc
emia
34PR(4/44)
SD�
12wee
ks(14/44
)
SAR24
5408
Pan
-PI3K
1-2prio
rlines
NCT0
1013
324
(11/20
09)
Not
yetreported
Not
yetreported
Com
pleted,
notreported
(Con
tinue
don
thefollo
wingpag
e)
Myers
Clin Cancer Res; 19(19) October 1, 2013 Clinical Cancer Research5268
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

Tab
le1.
Com
pletedan
don
goingpha
seIIclinical
trials
ofsing
leag
entPI3K/m
TORpathw
ayinhibito
rsin
endom
etria
lcan
cera
(Con
t'd)
Inve
stigationa
lag
ent
Target
Treatmen
tpopulation
NCT#
(dateregistered)
Clin
ical
resu
lts
(n)
Toxicities
Referen
ce
MK-220
6AKT
1-2prio
rlines
NCT0
1312
753
(12/20
10)
CR(0/36)
Mos
tco
mmon
�grad
e3
AEs:
rash
,hyp
erglyc
emia,
52PR(2/36)
SD�
8wee
ksd(12/36
)PFS
�6mon
ths(4/36)
NVP-B
KM12
0Pan
-PI3K
1prio
rlines
NCT01
2890
41(1/201
1)Not
yetrepo
rted
Not
yetreported
Not
recruitin
g,no
treported
GDC-098
0Dua
lmTO
RC/PI3K
1–2prio
rlines
NCT0
1455
493
(10/20
11)
Not
yetrepo
rted
Not
yetreported
Not
recruitin
g,no
treported
PF-05
2123
84Dua
lmTO
RC/PI3K
1–2prio
rlines
NCT0
1420
081
(8/201
1)Not
yetrepo
rted
Not
yetreported
Rec
ruiting
PF-04
6915
02
NVP-B
KM12
0Pan
-PI3K
Adjuva
nton
lyNCT0
1397
877
(7/201
1)Not
yetrepo
rted
Not
yetreported
Rec
ruiting
NVP-B
KM12
0Pan
-PI3K
Adjuva
nton
lyNCT0
1550
380
(8/201
1)Not
yetrepo
rted
Not
yetreported
Not
yet
recruitin
g
NOTE
:NCT#,
Nationa
lClinical
Trialiden
tifier;tem
sirolim
uswas
previou
slykn
ownas
CCI-77
9;ev
erolim
uswas
prev
ious
lykn
ownas
RAD00
1;rid
aforolim
usha
sbe
enpreviou
sly
know
nas
deforolim
us,A
P23
573,
andMK-866
9;SAR24
5408
was
previou
slykn
ownas
XL1
47;PF-05
2123
84was
previou
slykn
ownas
PKI-58
7;CR,c
omplete
resp
onse
;PR,p
artia
lresp
onse
;SD,s
table
disea
se;P
FS,p
rogres
sion
-freesu
rvival;G
rade
3AE,a
dve
rseev
ents
asper
Com
mon
Term
inolog
yCriteria
forAdve
rseEve
nts.
aStudies
wereiden
tified
throug
hwww.clinicaltrials.gov
anddataco
llected
throug
hwww.clinicaltrials.gov
andTrialTrove
(www.cite
line.co
m/produc
ts/tria
ltrov
e).P
hase
IIstud
ieswith
aprim
aryfocu
sof
endo
metria
lcan
cerareinclud
ed.P
hase
IBex
pan
sion
andph
aseIIstud
ieswith
multip
leca
ncersof
origin
areno
tinc
luded
.Allnu
mbersin
theden
ominator
are
enrolledpatientson
thestud
y.Mos
tco
mmon
toxicitie
sreflec
ttoxicitie
sreportedat
approximately10
%or
more.
bObjectiveresp
onse
byindep
enden
treview
.cDurationof
SDwas
presu
med
tobefirstplann
edradiograp
hicev
alua
tionof
dise
aseifno
tsp
ecifica
llyreported
dElig
ibility
was
restric
tedto
endom
etroid
histolog
y.eTh
iswas
astud
yof
AP23
573,
anIV
form
ulationof
ridaforolim
us.
Targeting the PI3K/mTOR Pathway in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 19(19) October 1, 2013 5269
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

Tab
le2.
Com
pletedan
don
goingpha
seIIclinical
trials
ofPI3K/m
TORpathw
ayinhibito
rsin
combinationwith
othe
rtherap
iesin
endom
etria
lca
ncer
a
Inve
stigationa
l/therap
euticag
ents
Targets
Treatmen
tpopulation
NCT#
(dateregistered)
Clin
ical
resu
lts
Toxicities
Referen
ce
Temsirolim
usan
dca
rbop
latin
/pac
litax
elmTO
RC
and
cytotoxic
Che
mo-na
ïve
NCT0
0977
574
(9/200
9)Not
yetreported
Not
yetreported
Not
yetrep
orted
Temsirolim
usan
dbev
acizum
abmTO
Ran
dVEGFA
1–2prio
rlines
NCT0
0723
255
(7/200
8)CR(1/53)
PR(11/53
)SD�
8wee
ksb(27/53
)PFS
�6mon
ths(23/53
)
Mos
tco
mmon
�grad
e3
AEs:
Neu
trop
enia,c
ardiac,
cons
titutiona
l,ga
strointestinal,infec
tion,
metab
olic,p
ain.
49
(3dea
thspo
ssibly
attributed
todrug)
Temsirolim
usvs.
temsirolim
us/m
egac
e/tamox
ifen
mTO
Ran
dho
rmon
altherap
y
Adjuva
nton
lyNCT0
0729
586
(8/200
8)Com
boarm:
CR(0/22)
PR(3/22)
SD�
8wee
ksb(11/22
)
Com
boarm:m
ost
common
�grad
e3AE:
Vas
cular,ed
ema,
fatig
ue.
(7thromboe
mbolicev
ents,
1su
dden
dea
th,1
myo
cardialinfarction)
48
Singlearm:C
R(2/20)
PR(4/20)
SD�
8wee
ksb(11/20
)Singlearm:m
ostco
mmon
�grad
e3AE:a
nemia,
naus
ea,h
yperglyc
emia
Eve
rolim
usan
dletroz
ole
mTO
Ran
dho
rmon
altherap
y
1–2lines
NCT0
1068
249
(2/201
0)CR(5/42)
PR(2/42)
SD�8
wee
ksb(10/42
)
Themos
tco
mmon
drug
relatedtoxicitie
swere
fatig
ue,d
iarrhe
a,thromboc
ytop
enia
47
Eve
rolim
usan
dletroz
olean
dmetform
in
mTO
Ran
dho
rmon
altherap
yan
dce
llularnu
trient
with
drawalc
1–2lines
NCT0
1797
523
(2/201
3)Not
yetreported
NCT#,
Nationa
lClinicalTrialIden
tifier;tem
sirolim
uswas
previou
slykn
ownas
CCI-77
9;ev
erolim
uswas
previou
slykn
ownas
RAD00
1;CR,com
plete
resp
onse
;PR,p
artia
lres
pon
se;
SD,s
table
dise
ase;
PFS
,progres
sion
-freesu
rvival;A
E,a
dve
rseev
ents;G
rade3,
aspe
rCom
mon
Term
inolog
yCriteria
forAdve
rseEve
nts.
aStudieswereiden
tified
throug
hwww.clinicaltrials.gov
anddataco
llected
throug
hwww.clinicaltrials.gov
andTrialtrov
e(www.cite
line.co
m/produc
ts/tria
ltrov
e).P
hase
IIstud
ieswith
aprim
aryfocu
sof
endom
etria
lcan
cerareinclud
ed.P
hase
IBex
pans
ionan
dpha
seIIstud
ieswith
multip
leca
ncersof
origin
areno
tinc
lude
d.A
llnu
mbersin
thede
nominator
are
enrolledpatientson
thestud
y.bDurationof
SDwas
presu
med
tobefirstplan
nedradiograp
hicev
alua
tionof
disea
seifno
tsp
ecifica
llyreported.
cTh
isdes
cribed
target
reco
gnizes
theinco
mplete
understan
dingof
metform
inas
apoten
tiala
ntican
certherap
y.
Myers
Clin Cancer Res; 19(19) October 1, 2013 Clinical Cancer Research5270
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

pyrimidine synthesis and potential sensitivity to rapalogtreatment (46).Rapalogs in combination. The rapalogs continue to
be studied in combination with other cytotoxic andbiologic agents. Phase II studies of rapalogs with hor-monal agents as well as antiangiogenic agents have beencompleted (refs. 47–49; Table 2). Toxicity of these classcombinations may be limiting. The combination armof GOG 248, a randomized study of temsirolimuswith or without hormonal therapy was terminatedbecause of thromboembolic events (48). Combinationsof rapalogs and antiangiogenic agents also report highrates of vascular events (49; Susan Campos; personalcommunication).GOG 86P is a "pick-the-winner" randomized phase II
study evaluating 3 different agents, including temsirolimus,in combination with carboplatin and paclitaxel. Thisstudy has embedded translational studies that could beinformative. Should a predictive biomarker for single-agentrapalog response be identified, it will be important toknow whether it can be generalized to rapalogs in thera-peutic combinations.
PI3K pathway inhibitorsRapalogs are incomplete inhibitors of mTORC1 tar-
gets and, due to feedback loops, can result in activationof upstream PI3K signals (50, 51). It has been hypoth-esized that newer PI3K pathway agents, which targetfurther upstream in the pathway, will be more clinicallyeffective. Numerous phase Ib/II clinical trials areunderway including pan-PI3K, dual PI3K/mTOR, AKT,and catalytic mTOR inhibitors (www.clinicaltrials.gov; Table 1). Although clinical reports are expectedsoon, the results for the majority of these studies haveyet to be reported.Results from a phase II study of MK-2206, an allosteric
AKT inhibitor were recently reported (52). This study wasprospectively stratified for PIK3CA mutations and wasdesigned to explore the hypothesis that patients withtumors that harbor PIK3CA mutation would be morelikely to derive benefit from MK-2206. Of the 36 patientsenrolled, 9 were classified as PIK3CA mutant and 27 werePIK3CA wild-type. There was 1 event of clinical benefit inthe PIK3CA-mutant group and 4 events of clinical benefitin the PIK3CA wild-type group suggesting that there islimited clinical use for prospective PIK3CA mutationtesting predict response to AKT inhibitors. All 4 partici-pants who were on treatment for more than 6months hadtumors of serous histology, a histology that represents adisproportionate number of deaths from endometrialcancer.PI3K pathway inhibitors are also being evaluated
in combination studies. On the basis of the tight net-working with the RAS-ERK pathway combination ofMEK and other RTK inhibitors are of great interest. PhaseI studies of combination have identified notable re-sponses in endometrial cancer though exploration ofdosing to minimizing toxicity continues (53). PI3K
pathway inhibitors are also being studied in combina-tion with cytotoxics (Table 2 and www.clinicaltrials.gov)though efficacy results in endometrial cancer have yetto be reported.
The future: contextualizing PI3K signalingResults from many PI3K pathway inhibitors trials
are anticipated. (Tables 1 and 2). However, these firstreports suggest that PI3K/mTOR pathway inhibitors assingle agents are not as efficacious as hoped. In recog-nition that clinical trials should generate as well as testhypotheses, there are some avenues that warrant furtherexploration.
Of drugs and targets. Preclinical and translationaldata strongly support that PI3K signaling underpinsendometrial cancer biology and this prior knowledgeneeds to be accounted for in the interpretation ofPI3K/mTOR pathway inhibitor trial results. At this earlyjuncture, negative studies in this disease should steerfocus to the investigational agents as much as challengethe validity of PI3K as a target. Pharmacodynamic stud-ies to verify pathway inhibition at achievable exposuresshould remain an integral part of these early-phasestudies as the maximal tolerated may not equate tothe biologically optimal dose. The enhanced specificityand potency of newer classes of agents such as themTORC1/2 catalytic and PI3K isoform-specific inhibi-tors hold promise and should also be evaluated inendometrial cancer.
Metabolic context. Obesity is an established risk fac-tor for developing endometrial cancer with a nearly 3-fold increase in risk (4). The biology underlying theassociations between obesity, endometrial cancer risk,and outcomes remains incompletely understood. How-ever, chronic overexposure to hormones elevated in theobese state such as insulin, insulin-like growth factors,and estrogens, likely contribute (54). The PI3K pathwayis the key-regulating pathway of glucose uptake andmetabolism (6) perhaps suggesting that PI3K pathwayalteration may need to be explored in the context of apatient’s metabolic state. Recent studies evaluating theassociation of PI3K pathway alterations show an inter-action between PTEN protein loss, obesity, and prog-nosis. Patients with obesity with PTEN loss haveimproved outcomes as compared with those with PTENretained. In contrast, in the nonobese population,patients with PTEN loss have worse outcomes (55). Inaddition, retrospective analysis of the combinationstudy of everolimus and letrozole show a clinical ben-efit rate that is twice as high in patients taking theantidiabetic agent metformin as compared with thosewho are not (56). Whether metformin is merely asso-ciated with a subpopulation of patients whose endo-metrial cancer is more like to response to rapalogs orwhether there is a causal effect (direct or indirect)remains unclear.
Histologic context. Unlike breast cancers, treatmentrecommendations for endometrial cancers are not based
Targeting the PI3K/mTOR Pathway in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 19(19) October 1, 2013 5271
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

on upfront molecular classifications. The most commonendometrial cancer histologies (endometroid, papillaryserous, clear cell, mixed) are treated with the same che-motherapeutic regimens. Results from the MK-2206 trial,in which all patients with 6 months of progression-freesurvival had tumors of serous histology suggest that amore nuanced approach may be warranted. Isolatedmolecular differences between these histologies havebeen described (27). Recent studies of whole-exomesequencing of uterine papillary serous cancers furtherdetail the differences and have identified candidate mole-cular changes to explore as potential molecular biomar-kers for AKT inhibitor response (57–59). In addition,these studies may be useful for the classification of endo-metrial cancers that are challenging to classify by histo-logy alone (60).
Mutational context. Comprehensive genome studiesincluding the The Cancer Genome Atlas highlightssome interesting features of the PI3K pathway that seemto be particular to endometrial cancer (17, 28). Unlikeother cancers, comutations within the PI3K pathwayare common. There is a strong association of PIK3CAand PTEN as well as PIK3R1 and PTEN mutations.PIK3R1 and PIK3CA comutation are uncommon(17, 28). PIK3CA mutations are distributed differentlyin endometrial cancers than other cancers in whichPIK3CA mutations are common such as breast cancer(26). Functional studies suggest that not all mutations inPIK3CA and PIK3RI have the same cellular impact (28).How these very specific mutational features impactendometrial cancer biology and clinical outcomes areunder investigation.
In conclusion, the PI3K pathway underlies endo-metrial cancer development and remains a key targetfor new therapeutics. Ongoing and future clinical inves-tigation should recognize the intricacies of this path-way as highlighted above. Translational studies shouldbe comprehensive including complete sequencingand copy number analysis and pharmacodynamic stud-ies; tumors from patients with robust responsesshould be studied in detail metabolic data such as bodymass index, presence of diabetes, and use of antidia-betic agents should be collected. Together with emerg-ing clinical reports these data can help guide the opti-mal development of PI3K pathway inhibitors in endo-metrial cancer.
Disclosure of Potential Conflicts of InterestA.P. Myers is employed as a clinical program leader for
Novartis and is a consultant/advisory board member of EISAI andSanofi.
AcknowledgmentsThe authors thank C. Dibble and B. Emerling for thought-
ful input and L. Cantley, G. Mills, and U. Matulonis for mentor-ship. The author would like to apologize in advance to investi-gators whose work could not be primarily cited due to spacelimitation.
Grant SupportThis work was supported by a Stand Up To Cancer Dream Team Trans-
lational Cancer Research Grant, a Program of the Entertainment IndustryFoundation (SU2C-AACR-DT 0209).
Received April 29, 2013; revised July 17, 2013; accepted July 28, 2013;published online October 2, 2013.
References1. JemalA,BrayF,CenterMM, Ferlay J,WardE, FormanD.Global cancer
statistics. CA Cancer J Clin 2011;61:69–90.2. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer
J Clin 2013;63:11–30.3. Calle E, Rodriguez C, Walker-Thurmond K, Thun M. Overweight,
obesity, and mortality from cancer in a prospectively studied cohortof U.S. adults. NEJM 2003;348:1625–38.
4. Reeves GK, Pirie K, Beral V, Green J, Spencer E, Bull D. Cancerincidence and mortality in relation to body mass index in the MillionWomen Study: cohort study. BMJ 2007;335:1134.
5. Fleming GF. Systemic chemotherapy for uterine carcinoma: metastat-ic and adjuvant. J Clin Oncol 2007;25:2983–90.
6. Engelman JA, Luo J, Cantley LC. The evolution of phosphatidylinositol3-kinases as regulators of growth and metabolism. Nat Rev Genet2006;7:606–19.
7. Whitman M, Downes CP, Keeler M, Keller T, Cantley L. Type Iphosphatidylinositol kinase makes a novel inositol phos-pholipid, phosphatidylinositol-3-phosphate. Nature 1988;332:644–6.
8. Stephens L, Anderson K, Stokoe D, Erdjument-Bromage H, PainterGF, Holmes AB, et al. Protein kinase B kinases that mediate phos-phatidylinositol 3,4,5-trisphosphate-dependent activation of proteinkinase B. Science 1998;279:710–4.
9. Pearce LR, Komander D, Alessi DR. The nuts and bolts of AGC proteinkinases. Nat Rev Mol Cell Biol 2010;11:9–22.
10. Ma XM, Blenis J. Molecular mechanisms of mTOR-medi-ated translational control. Nat Rev Mol Cell Biol 2009;10:307–18.
11. Maehama T, Dixon JE. The tumor suppressor, PTEN/MMAC1,dephosphorylates the lipid second messenger, phosphati-dylinositol 3,4,5-trisphosphate. J Biol Chem 1998;273:13375–8.
12. Stambolic V, Suzuki A, de la Pompa JL, Brothers GM, MirtsosC, Sasaki T, et al. Negative regulation of PKB/Akt-depend-ent cell survival by the tumor suppressor PTEN. Cell 1998;95:29–39.
13. Carracedo A, PandolfiPP. The PTEN-PI3K pathway: of feedbacks andcross-talks. Oncogene 2008;27:5527–41.
14. Ramjaun AR, Downward J. Ras and phosphoinositide 3-kinase:partners in development and tumorigenesis. Cell Cycle 2007;6:2902–5.
15. Schultze SM, Hemmings BA, Niessen M, Tschopp O. PI3K/AKT,MAPK and AMPK signalling: protein kinases in glucose homeostasis.Expert Rev Mol Med 2012;14:e1.
16. Miller TW, Balko JM, Arteaga CL. Phosphatidylinositol 3-kinase andantiestrogen resistance in breast cancer. J Clin Oncol 2011;29:4452–61.
17. The Cancer Genome Atlas Research Network Integrated geno-mic characterization of endometrial carcinoma. Nature 2013;497:67–73.
Myers
Clin Cancer Res; 19(19) October 1, 2013 Clinical Cancer Research5272
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

18. NelenMR, vanStaverenWC,Peeters EA,HasselMB,Gorlin RJ, HammH, et al. Germlinemutations in the PTEN/MMAC1 gene in patients withCowden disease. Hum Mol Genet 1997;6:1383–7.
19. Liaw D, Marsh DJ, Li J, Dahia PL, Wang SI, Zheng Z, et al.Germline mutations of the PTEN gene in Cowden disease, aninherited breast and thyroid cancer syndrome. Nature Genet1997;16:64–7.
20. Stambolic V, Tsao MS, Macpherson D, Suzuki A, Chapman WB, MakTW. High incidence of breast and endometrial neoplasia resemblinghuman Cowden syndrome in ptenþ/- mice. Cancer Res 2000;60:3605–11.
21. Podsypanina K. Mutation of PTEN/Mmaci in mice causes neoplasiain multiple organ systems. Proc Natl Acad Sci U S A 1999;96:1563–8.
22. Daikoku T, Hirota Y, Tranguch S, Joshi AR, DeMayo FJ, Lydon JP,et al. Conditional loss of uterine Pten unfailingly and rapidlyinduces endometrial cancer in mice. Cancer Res 2008;68:5619–27.
23. Risinger JI, Hayes AK, Berchuck A, Barrett JC. PTEN/MMAC1mutations in endometrial cancers. Cancer Res 1997;57:4736–8.
24. Tashiro H, Blazes MS, Wu R, Cho KR, Bose S, Wang SI, et al.Mutations in PTEN are frequent in endometrial carcinoma but rarein other common gynecological malignancies. Cancer Res1997;57:3935–40.
25. Urick ME, Rudd ML, Godwin AK, Sgroi D, Merino M, Bell DW. PIK3R1(p85alpha) is somatically mutated at high frequency in primary endo-metrial cancer. Cancer Res 2011;71:4061–7.
26. Rudd ML, Price JC, Fogoros S, Godwin AK, Sgroi DC, Merino MJ,et al. A unique spectrum of somatic PIK3CA (p110alpha) mutationswithin primary endometrial carcinomas. Clin Cancer Res 2011;17:1331–40.
27. Weigelt B, Banerjee S. Molecular targets and targeted thera-peutics in endometrial cancer. Curr Opin Oncol 2012;24:554–63.
28. Cheung LW, Hennessy BT, Li J, Yu S, Myers AP, Djordjevic B, et al.High frequency of PIK3R1 and PIK3R2 mutations in endometrialcancer elucidates a novel mechanism for regulation of PTEN proteinstability. Cancer Discov 2011;1:170–85.
29. Laplante M, Sabatini DM. mTOR signaling in growth control anddisease. Cell 2012;149:274–93.
30. Courtney KD, Corcoran RB, Engelman JA. The PI3K pathway as drugtarget in human cancer. J Clin Oncol 2010;28:1075–83.
31. Slomovitz BM, Coleman RL. The PI3K/AKT/mTOR pathway as atherapeutic target in endometrial cancer. Clin Cancer Res 2012;18:5856–64.
32. Slomovitz BM, Lu KH, Johnston T, Coleman RL, Munsell M, BroaddusRR, et al. A phase 2 study of the oral mammalian target of rapamycininhibitor, everolimus, in patientswith recurrent endometrial carcinoma.Cancer 2010;116:5415–9.
33. Oza AM, Elit L, Tsao MS, Kamel-Reid S, Biagi J, Provencher DM, et al.Phase II study of temsirolimus in women with recurrent or metastaticendometrial cancer: a trial of the NCIC Clinical Trials Group. J ClinOncol 2011;29:3278–85.
34. Ray-Coquard I, Favier L, Weber B, Roemer-Becuwe C, Bougnoux P,Fabbro M, et al. Everolimus as second- or third-line treatment ofadvanced endometrial cancer: ENDORAD, a phase II trial of GINECO.Br J Cancer 2013;108:1771–7.
35. Colombo N, McMeekin DS, Schwartz PE, Sessa C, Gehrig PA, Hollo-way R, et al. Ridaforolimus as a single agent in advanced endometrialcancer: results of a single-arm, phase 2 trial. Br J Cancer 2013;108:1021–6.
36. Mackay H,Welch S, TsaoMS, Biagi JJ, Elit L, Ghatage P, et al. Phase IIstudy of oral ridaforolimus in pateints with metastatic and/or locallyadvanced recurrent endometrial cancer. J Clin Oncol 29, 2011 (suppl;abstr 5013).
37. Oza A, Poveda A, Clamp A, Pignata S, Scambia G, Del Campo J, et al.A randomized phase II trial of ridaforolimus compared with progestinor chemotherapy in female adult patients with advanced endometrialcarcinoma. J Clin Oncol 29, 2011 (suppl; abstr 5009).
38. Tredan O, Treilleux I, Wang Q, Gane N, Pissaloux D, Bonnin N, et al.Predicting everolimus treatment efficacy in patients with advancedendometrial carcinoma: a GINECO group study. Target Oncol. 2012Dec 13. [Epub ahead of print].
39. Meyer LA, Slomovitz BM, Djordjevic B, Galbincea JM, Johnston TA,Munsell M, et al. The search continues: looking for predictive biomar-kers for response mTOR inhibition in endometrial cancer. J Clin Oncol29, 2011 (suppl; abstr 5016).
40. Mackay H, Eisenhauer EA, Kamel-Reid S, Clarke B, Walsh W,Karakasis K, et al. Molecular determinants of outcome with mTORinhibition in endometrial cancer. J Clin Oncol 30, 2012 (suppl; abstr5010).
41. Salvesen HB, Carter SL, Mannelqvist M, Dutt A, Getz G,Stefansson IM, et al. Integrated genomic profiling of endo-metrial carcinoma associates aggressive tumors with indi-cators of PI3 kinase activation. Proc Natl Acad Sci U S A 2009;106:4834–9.
42. Iyer G, Hanrahan AJ, Milowsky MI, Al-Ahmadie H, Scott SN, Janakira-man M, et al.Genome sequencing identifies a basis for everolimussensitivity. Science 2012 338:221.
43. Bar-Peled L, Schweitzer LD, Zoncu R, Sabatini DM. Ragulator is a GEFfor the rag GTPases that signal amino acid levels to mTORC1. Cell2012;150:1196–208.
44. Robitaille AM, Christen S, Shimobayashi M, Cornu M, Fava LL,Moes S, et al. Quantitative phosphoproteomics reveal mTORC1activates de novo pyrimidine synthesis. Science 2013;339:1320–3.
45. Ben-Sahra I, Howell JJ, Asara JM,Manning BD. Stimulation of de novopyrimidine synthesis by growth signaling through mTOR and S6K1.Science 2013;339:1323–8.
46. Chen S, Bigner SH, Modrich P. High rate of CAD gene amplification inhuman cells deficient in MLH1 or MSH6. Proc Natl Acad Sci U S A2001;98:13802–7.
47. Slomovitz BM, Brown J, Johnston A, Mura D, Levenback C, Wolf J,et al. A phase II study of everolimus and letrozole in patients withrecurrent endometrial carcinoma. J Clin Oncol 29, 2011 (suppl; abstr2012).
48. Fleming G, Filiaci V, Hanjani P, Burke JJ, Davidson SA, Leslie KK, et al.Hormone therapy plus temsirolimus for endometrial carcinoma (EC):Gynecologic Oncology Group trial #248.J Clin Oncol 20, 2011 (suppl;abstr 5014).
49. Alvarez EA, Brady WE, Walker JL. Phase II trial of combination bev-acizumab and temsirolimus in the treatment of recurrent or persistentendometrial carcinoma: a Gynecologic Oncology Group study. Gyne-col Oncol 2013;129:22–7.
50. Thoreen CC, Kang SA, Chang JW, Liu Q, Zhang J, Gao Y, et al. AnATP-competitive mammalian target of rapamycin inhibitor revealsrapamycin-resistant functions of mTORC1. J Biol Chem 2009;284:8023–32.
51. Choo AY, Yoon SO, Kim SG, Roux PP, Blenis J. Rapamycindifferentially inhibits S6Ks and 4E-BP1 to mediate cell-type-specificrepression of mRNA translation. Proc Natl Acad Sci U S A 2008;105:17414–9.
52. Myers AP, Broaddus RR, Makker V, Konstantinopoulos P, Drapkin R,Liu JF, et al. Phase II, 2-stage, 2-arm, PIK3CAmutation stratified trial ofMK-2206 in recurrent endometrial cancer (EC). J Clin Oncol 31, 2013(suppl;abstr 5524).
53. Shapiro G, LoRusso P, Kwak EJ, Cleary J, Musib L, Jones C,et al. Clinical combination of the MEK inhibitor GDC-0973 andthe PI3K inhibitor GDC-0941: a first-in-human phase Ib studytesting daily and intermittent dosing schedules in patientswith advanced solid tumors. J Clin Oncol 29, 2011 (suppl;abstr 3005).
54. Schmandt RE, Iglesias DA, Co NN, Lu KH. Understanding obesity andendometrial cancer risk: opportunities for prevention. Am J ObstetGynecol 2011;205:518–25.
55. Ju Z, Westin SN, Broaddus RR. PTEN loss is a context dependentdeterminant of patient outcomes in obese and non-obese endome-trioid endometrial cancer patients. J Clin Oncol 31, 2013 (suppl; abstr5521).
Targeting the PI3K/mTOR Pathway in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 19(19) October 1, 2013 5273
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

56. Slomovitz BM, Soliman PT, Levenback C, Brown J, Wolf J,Schmeler K, et al. Everolimus (E) and letrozole (L) in womenwith previously treated recurrent endometrial cancer (EC): amultiinstitutional phase II clinical trial. 14th Biennial Meetingof the International Gynecologic Cancer Society. Vancouver,Canada; 2012.
57. Le Gallo M, O'Hara AJ, Rudd ML, Urick ME, Hansen NF, O'NeilNJ, et al. Exome sequencing of serous endometrial tumorsidentifies recurrent somatic mutations in chromatin-remodel-ing and ubiquitin ligase complex genes. Nat Genet 2012;44:1310–5.
58. Zhao S, Choia M, Overtona J. Landscape of somaticsingle-nucleotide and copy-number mutations in uterineserous carcinoma. Proc Natl Acad Sci U S A 2012;110:2916–21.
59. Kuhn E, Wu RC, Guan B, Wu G, Zhang J, Wang Y, et al. Iden-tification of molecular pathway aberrations in uterine serouscarcinoma by genome-wide analyses. J Natl Cancer Inst 2012;104:1503–13.
60. McConechy MK, Ding J, Cheang MC, Wiegand KC, Senz J, Tone AA,et al. Use of mutation profiles to refine the classification of endometrialcarcinomas. J Pathol 2012;228:20–30.
Myers
Clin Cancer Res; 19(19) October 1, 2013 Clinical Cancer Research5274
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from

2013;19:5264-5274. Clin Cancer Res Andrea P. Myers
The Devil Is in the Details−−Pathway New Strategies in Endometrial Cancer: Targeting the PI3K/mTOR
Updated version
http://clincancerres.aacrjournals.org/content/19/19/5264
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/19/19/5264.full#ref-list-1
This article cites 49 articles, 23 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/19/19/5264.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/19/19/5264To request permission to re-use all or part of this article, use this link
on June 26, 2018. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from