Embed Size (px)
Citation preview

It gives me immense pleasure to write a few words about Hayat Hospital. This
hospital was established in the year 2007 and the foundation stone was laid by
Hon'ble Health & F.W Minister of Assam Dr. Himanta Biswa Sarma. The main
person behind establishing the hospital was late Nezamot Ali, the father of Rajib
Saikia, the C.E.O of the hospital. Mr Rajib Saikia is a dynamic man having all the
qualities required to go ahead. Although he is non medical person, his
inquisitiveness to acquire knowledge of medical science stands in good stead. With
the expertise of imminent doctors he had planned to establish a multidimensional
hospital to give service to the people of this region in particular. The establishment
of this hospital which was along standing dream of Mr. Rajib Saikia was made into a
reality with the help of his close aides and friends Dr. Atanu Barthakur, Mr. Samsul
Alam Saikia,Mr. Mahibur Rahman and his wife Mrs Shareen Zia Rahman.
This hospital which has a capacity of 133 beds started functioning since 16th
February 2010. This hospital has 6 state of the art Operation Theatres with all the
modern instrumentations, beside 15 bedded ICU having all the facilities like
ventilators, bedside monitor and oxygen. This ICU is under the supervision and
guidance of experienced doctors and nurses.
This hospital at present is having all the speciality departments like Medicine,
Surgery, Obs & Gynae, Orthopedic, Eye, ENT, Radiology, Pathology, Clinical
Biochemistry, Microbiology and other superspeciality departments like
Cardiology, C.T.V.S, Neurosurgery, Neurology, Burn treatment unit, Urology,
Nephrology and Accident & Emergency Unit, IVF centre. As soon as these are made
fully functional the people of Assam and NE region can avoid going outside for
better treatment. With CTVS fully functioning, Angiography, Angioplasty and
Coronary Bypass will be easier. This vital unit will be made functional with the help
of renowned CTVS surgeons of Assam and outside the state. This will reduce the
expenditure drastically which will be the greatest relief to the patients and their
family. I hereby appeal to the people of Assam and NE regions to extend their
helping hand and blessings so that we can go forward and achieve the goal.
Dr Z RAHMAN
CMD
Newsletter
Issue:1, Vol:1, Febryary 2011
FROM CMD DESK
Hayat
Dr. Ziaur RahmanCMD, Hayat Hospital
Dr. Atanu BarthakurMedical Director, Hayat Hospital
CONTENTSKNOW YOUR RISK OF GETTING A HEARTATTACK AND MEASURES TO PREVENT IT- Prof Upendra Kaul
HAYAT HEART CENTREDr. Sasanka Baruah
BIOCHEMICAL CARDIAC MARKERSDr. Bikash Kumar Chaudhury
ACLS GUIDELINES -2010 KEY CHANGES IN THE MANAGEMENT OF ADULT CARDIAC ARREST Dr. Chandana Sarma
PROLENE HERNIA SYSTEM MESH – ITS EVOLUTIONA NEW TECHNIQUE TO REPAIR INGUINAL HERNIASDr. S. K. Nath
ANTIBIOTIC SUSCEPTIBILITY PATTERN OF INDOOR PATIENTS AT HAYAT HOSPITALDr. Paromita C. Barua
All editorial queries & feedback can be directed to:
The EditorHayat NewsletterHayat Hospital. Guwahati-34Ph:0361-2470088e-mail: [email protected], [email protected]
*For in-house distribution only

As I sit at my computer for a while now, trying to write the introduction to my editorial column of the first newsletter of the Hayat Hospital, a surge of thoughts ponder through my mind.
At the outset, our editorial team was often asked from different quarters the question of why do we need to generate such a newsletter?
Our motivation is certainly not based on any selfish means of launching a new instrument of promotion for our organization, but since the inception of Hayat Hospital exactly a year ago, this organization, especially in the last few months, has gained tremendous momentum and diversity as a result of different medical disciplines working together in a rich, synergistic and complementary fashion. The ethics and principles on which this hospital was founded is the nucleolus of networks that are creating synergies between different disciplines. Teamwork, I believe, is essentially a question of attitude and commitment. It is the insurance of keeping passion at the centre of learning activities and making our doctors more open minded to new methods and practices.
thOn the 16 of February 2011, the Hayat Hospital will complete its first year of inception. The hospital started off with highly dependable critical care services backed by a fully fledged trauma care centre and burns unit, a network of critical care vans and 24 critical care beds including dedicated Neuro/Stroke ICU, Medical & Surgical ICU, Neonatal and Paediatric ICU & High Dependency Units as per the international norms. The hospital, for the first time in the northeastern part of India, has commenced with “bloodless” urology surgeries with the advent of the LASER prostrate and renal stone surgery. Hayat or life in Arabic with its mission to help people achieve health for life has made tremendous strides in the last few months and will continue to put the time and effort that goes into ensuring that the high standard of quality patient care is maintained.
This newsletter aims to support this momentum and become a link between patients, doctors, and a broader audience of well wishers who may be interested in keeping informed of Hayat Hospital's recent advances, CMEs, trainings or event presentations.
At the advent of committing myself to the initiation of this newsletter I sought counsel with a number of my colleagues and I was surprised at the unanimous optimistic response I had received. Everyone was more than willing to contribute in whatever way they could and then I further realized that somewhere in the conundrum there was an enormous positive energy which was being translated into the day to day activities at the Hayat Hospital. We were not only tackling diseases but we are also endeavoring to touch the lives of patient visiting us to their better health in a healthy and sanguine way.
We at the Hayat Hospital aim to promote health awareness among the masses. We also intend take health care to new heights through the relentless endeavors of our doctors and our paramedical staff. I hope this newsletter will transmit this passion and in so doing, open up new initiatives and projects
As we trudge along into a new decade Hayat Hospital on its foundation day is yet again setting a benchmark in the northeastern region of India in Tertiary Heart Care. Valentine's Day precedes the foundation day of the hospital by two
days. Valentine's Day, February 14th, is a day that traditionally evokes feelings of the heart -- of flowers, romance and marriage proposals. But this year on the eve of the first Foundation Day, Hayat Hospital is thinking about hearts in a far more serious way.
Death from heart attack, stroke, and other cardiovascular diseases claims one American life every 34 seconds. In India too the largest ever study of deaths carried out in collaboration with the Registrar General of India (RGI) and the Indian Council of Medical Research (ICMR) shows hear t a i lments have replaced communicable diseases as the biggest killer in rural & urban India. Assam and the adjoining northeastern states too are not immune from the clutches of this dreadful disease.
In continuation of its commitment with its “Mission & Vision” of providing superior healthcare services of international standards in a comprehensive manner to every individual with an emphasis on quality, service excellence, empathy and respect; the Hayat Hospital on its first Foundation Day will formally commence with the functioning of the full fledged Hayat Heart Center with amenities which include a state of the art Cath Lab, modular CTVS OT, CTVS ICU, ICCU and High End MDCT Scan. This Hayat Heart Center will cease the need for people of this part of the country to venture out for want of excellence in heart care. Hayat Heart Center will endeavor to provide international standard quality heart care under one roof.
In conclusion The Hayat Newsletter will strive to grow and provide increased communication with our readers. With four issues planned for 2011, there is lots of great reading to come and we will always welcome your contributions. Please contact a member of the Hayat Newsletter Editorial Board or at
if you would like to submit an article or have any suggestions about the Newsletter.
On behalf of the editorial team of the Hayat Newsletter, I wish you all a happy, healthy, and successful 2011.
Editorial
HAYAT HOSPITAL for life
Dr. Bikash Kumar Chaudhury, M.D. Consultant Biochemist
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
From the Escritoire of the Medical Director
Welcome to the first edition of the Hayat Newsletter.As the Medical Director of this institution, it is my great pleasure to launch this newsletter as a part of the initiative to
provide all physicians and well wishers more information about Hayat Hospitals.At Hayat Hospital, we're more than just healthcare providers, we're your friends. We go the extra mile. We give you that
extra attention. And we provide you with high quality healthcare you know you can trust. That's our commitment to you and the feeling that radiates through our corridors day after day.
Hayat Hospital is an independent, 133 bedded hospital. We offer health and wellness services to the regional population of Assam, as well as other Northeastern States. Since its functioning in 2010, Hayat Hospital has endeavored to provide high quality, safe, highly personal healthcare services for the patients and families we serve. Our total care team includes primary care physicians, specialists, surgeons, nurses and other healthcare professionals who are highly skilled and dedicated to providing the best possible care. Our goal is to be your trusted and lifelong partner for health and wellness services.
Beside the specialties of Medicine, Surgery, Orthopedics, Obstetrics & Gynecology, and a well equipped avant-garde Clinical Diagnostic Laboratory, Hayat Hospital have laid a special emphasis on Trauma and Critical care including burns. With Internationally trained and reputed team of physicians and staff, Hayat operates a fully functional Trauma and Critical Care
stDepartment which includes a dedicated 30 bedded ICU. Moreover on its 1 Anniversary Hayat Hospital is launching its Heart Centre with modern equipments like Cath Lab, modular CTVS OT, CTVS ICU & ICCU. The induction of this centre run by eminent physicians will cease the need of people of this region to venture out for the need of quality cardiac care. Minimal Invasive Urology surgeries have also been started with the introduction of the Holium Laser Surgery.
Hayat Hospital will soon begin the detailed planning and design of new state of the art centers which will include the departments of Neurosurgery including Head and Spine surgery, Joint Replacement Surgery, Neurology and IVF centre. We approach the planning and construction process with enthusiasm and excitement, knowing that a new facilities will enable us to serve our patients needs even better in the years to come.
In the end I want to take this opportunity to thank the staff, physicians, volunteers and especially Mr. Rajib Saikia and Dr. Ziaur Rahman at Hayat Hospital who have undertaken this mammoth task of of making the dream of a First-rate hospital in this region come true.
Best Wishes and Good Health!
Dr.Atanu Barthakur,MS(Specialist in Trauma & Critical Care
Trained in UK),Consultant Surgeon & Medical Director
HAYAT HOSPITAL
Prof. Umesh Ch. Sarma, M.B.B.S. (Gau) M.D. (B.H.U.)M. Sc. in Epidemiology (London Univ.), P.G. Trg. in Epidemiology (London Univ.)Vice Chancellor, Srimanta Sankerdev University of Health ScienceNarakasur Hilltop, Bhangagarh, Guwahati-32, Assam, India
MessageI am happy to learn that the Hayat Hospital is formally commencing the functioning of the full fleddged Advance Heart Centre with state of the art amenities for advanced cardic care. That the Inaugural Ceremony will be followed by CME on Advances in Coronary Heart Deases is indeed Ppraiseworthy
.
The last few decades have seen the field of Cardiology develop at an amazing pace, with numerous advance diagnostic facilities, procedures, techniques and modifications now being made available for improved patient care. This makes it necessary for members of this profession to keep themselves aware of new developments and skills. Such a mindset is the only way to maintain the standard of services being provided to the public at large.
I am sure the staff of the Advanced Heart Center will work with dedication and integrity, and provide help to the suffering people.
(Prof. U.C. Sarma)Vice Chancellor
Srimanta Sankardeva University of Health Sciences
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
Prof Upendra KaulExecutive Director and Dean Fortis Escorts Heart Institute and Research Centre, New DelhiVisiting Faculty, Hayat Heart Centre
Coronary Heart disease is one of the commonest causes of death, disability and hours at work lost in most communities. The incidence is increasing steadily and according to several prevalence studies carried out in our country around 10 per cent of population above the age of 35 years in our metros (Delhi, Jaipur, Mumbai, Chennai, Bangalore etc) have coronary heart disease. The figures from rural India, though lower, are also showing an increasing trend (around 4 per cent).
This is an alarming data, indicating that an estimated 60 million people in our country are suffering from problems related to blockages of coronary arteries. It is thus very important to understand the risk factors which are responsible for the problem.
The World Heart Day 2010 aptly is being used to propagate the message “
. INTERHEART, a very important international study, reported in 2000 that nine risk factors could explain the causation of heart attacks in 90 per cent instances. Thirty percent patients included in this study were from south Asian countries. The study is therefore very well applicable to our population.
The risk factors were divided in 2 categories:
Adverse Risk factors · levels of bad cholesterol (elevated ApoB/ApoA1 ratio)· Current Smoking· High blood pressure · Diabetes mellitus · Abdominal obesity · Psycho-social stress
Protective Risk factors · Daily consumption of 4 to 5 servings of fruits and
vegetables · Regular exercise at least 30 mins/day at least 5 times a
week.· Alcohol intake in moderation
Globally, all 9 risk factors were very significantly associated with heart attacks except alcohol, which had only a modest statistical significance. These risks were consistent in all regions, ethnic groups, and in men and women worldwide.
The strongest risk predictor globally was the apoB/apoA1 ratio (a more reliable marker of cholesterol risk), followed by current smoking (associated with a 4-fold and 3-fold increased risk of heart attack respectively). The risk associated with lipids and smoking was particularly marked in the young (Below 55 years in age in men and below 65 years in women) versus the old.
FACTS TO BE REMEMBERED TO REDUCE RISK OF HEART ATTACKS AND RELATED PROBLEMS
Current smoking
Smoking over 20 cigarettes or bidis per day increase the risk of heart attack by 5 times, 10 to 19 cigarettes or bidis increases the risk by 3 times and smoking less than 5 cigarettes or bidis per day increases
"Workplaces Wellness: Take responsibility for your own heart health"
the risk by 1.5 times.
Smoking one cigarette shortens life by 11 minutes and people exposed to second hand smoke have 90 per cent excessive rate of heat attacks.
Quitting smoking at any age nullifies this risk in 3 years. It is never too late to give up. Reducing smoking to minimum also helps.
What is normal Blood Pressure?
Optimal BP is a pressure less than 120/80 mms Hg. Any rise in BP above 110/75 mms is associated with a linear increase in stroke and heart attack rates. This has been proven by several epidemiologic studies and life insurance statistics. An increase of 10 mms in the systolic or diastolic pressure is associated with doubling of the risk of a vascular event. Unfortunately, high BP is invariably not accompanied by symptoms and therefore its detection and management is a challenge. It has been described by some as a “Silent Killer”.
Some myths about Blood Pressure
Blood pressure increases with age which levels of bad cholesterol (elevated ApoB/ApoA1 ratio) happens frequently. The normal BP of a 60 year old is 160 and at 80 years it is 180 (Age + 100). This is not true. Normal BP at all ages should be below 120/80 mms.
Low Blood Pressure is a disease: People with BP lower than 100 to 110 mms systolic in good health often seek medical attention.
Individuals with pressures on the lower side without any disease are blessed with the possibility of a long and healthy life. They should not waste their resources on taking tonics and BP increasing measures.
Indications for taking BP-Lowering Drugs
Ideal Blood pressure at all ages should be below 120/80. In general, medicines are recommended when BP is more than 140/85 mms Hg. In some situations, medicines are recommended even at levels of 130/80 mms Hg. These situations are: Patients with diabetes Patients with kidney disease and high blood urea and creatinine Patients with pre-existing heart disease or stroke.
Non Drug Methods reduce BP by 10 to 15 mms Hg: These measures are Regular exercise. Salt intake of not more than 4 to 5 grams per day. Fresh fruits and leafy vegetables (4 to 5 servings/day) Avoidance of alcohol or drinking in moderation.
Losing weight.
These measures should be adopted by everybody with high BP. The dosage of drugs and number of medicines can be brought down by these lifestyle methods. All healthy individuals should adopt these non drug measures, so their pressures remain below 120/80 mms Hg. Before starting drugs, make sure that you minimize consumption of following agents: Pain killers, Nasal drops, cough syrups, anti-depressant and mood elevating drugs.
Impact of Blood Cholesterol levels
High levels of bad cholesterol and low levels of good cholesterol promote heart disease. One per cent reduction in cholesterol leads to two per cent reduction in heart attacks. Low levels of good cholesterol (HDL cholesterol) are associated with a higher chance of getting a heart attack. Forty per cent of Indians have it. The levels of less than 40 mgs in men and 50 mgs in women are defined as low. Decreasing LDL cholesterol and increasing HDL cholesterol reduces this heightened risk. A one mg increase in HDL cholesterol is associated with 6 per cent reduction in dying from a heart attack.
Methods to increase HDL cholesterol and reducing LDL cholesterol
heart Attack and Measures to Prevent It
Know Your Risk of Getting a
“Take responsibility for your own heart health"
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
are regular exercise, weight reduction, increase in consumption of Omega 3 fatty acids (olive oil, mustard oil, almonds, walnuts, cold water fish like salmon, trout etc).
High risk individuals with multiple risk factors and even modestly raised levels of LDL cholesterol need in addition the statin group of drugs (simvastatin, atorvastatin or rosuvastatin).
These tablets should be taken under medical supervision and once required, need to be continued for long term. If you are a diabetic your chance of having a heart attack in the next 7 years is 10 times more than a non diabetic everything remaining the same.
All diabetics over 60 years of age with one more risk factor must take 75 mgs of aspirin, atorvastatin or simvastatin in appropriate dose and measures to keep blood pressure less than 130/80 mms Hg besides a meticulous sugar control under medical supervision. This minimizes this heightened risk.
Consumption of vitamins and anti-oxidants in form of tablets and syrups has no role in preventing heart attacks. Vitamin supplements in the form of B6 , B12, Folic acid, Vitamin C, Vitamin E , beta carotene and anti-oxidant tablets all have been shown to have no cardiac protective effect in large trials with sufficient power to detect the difference between these compounds and placebo.
It is very important to understand the agents which are useful in preventing events in high-risk population: Aspirin, Statins
(simvastatin, atorvastatin etc), ACE inhibitors (ramipril, perindopril etc).
Stress and Heart attacks
Psycho-social stress is an important risk factor. It leads to increased secretion of adrenaline, chronic stress raises the blood pressure, invites diabetes and constricts the arteries of heart. Stress management programs comprising breathing exercises, stretching exercises, yoga, meditation and massage have been found to be useful in alleviating stress.
These are approaches that aim at blunting the adrenalin response to stress. These relaxing techniques have the added advantage of being very safe. The high-risk population will benefit the most.
Exercise is one of the most useful methods of reducing chronic stress and in addition, has the advantage of directly reducing the chance of a heart attack and controlling obesity.
This, coupled with eating a heart-healthy diet rich in fruits and vegetables, low in salt content is a very good adjunct.
Early recognition of risk factors and using preventive strategies to reduce their impact is one of the most cost effective ways to postpone heart attacks and strokes by more than one decade. This has been proven in large epidemiological studies.
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011

This is an appeal to all the
healthcare professionals in this region as
well as general masses to come forward
and join hands with us. Let us show the
path for others to follow. Our pledge is to
see a heart-healthy North-East in near
future.
To sum up as Robert Frost
would have said;
“The woods are lovely, dark and deep,
But I have promises to keep,
And miles to go before I sleep,
And miles to go before I sleep”...
HAYAT CENTREHEART Dr. Sasanka Baruah
Dr. Anupam Biswas
Dr. A. Zaman Ahmed
Dr. Arnab Paul
Coronary heart disease is the leading cause of mortality and morbidity worldwide.
The scenario in India is no better. In fact, mortality due to heart attacks in our country is on
an increasing trend such that the World Health Organization estimates it to be the biggest
healthcare problem in India by the year 2015.
Today medical science has come up to such a level that untimely death and
sufferings can be prevented and treated early; thus fulfilling the basic aim of all healthcare
professionals.
The western world has gone miles ahead in this process such that Mobile Cath
Labs and provision for Air Ambulance are available for treating acute coronary syndromes
(heart attacks). India, too is not lacking much behind with all latest facilities available for
treating cardiac ailments, but these facilities are limited only to the major metropolis. What
about the scenario in the North-East ? Are we really up-to-date ?
Do we still need to travel to a metropolitan city, when we can receive the same
treatment at our own place; hence saving a lot of vital time and money. All these questions
can be answered if we understand the basic mechanics of any Cardiac ailment. Any Cardiac
emergency needs immediate care, where “TIME IS MUSCLE”. Every second we save
increases the life expectancy of the patient. When facilities like Coronary Angiography,
Angioplasty & Stenting, emergency and routine coronary artery by-pass graft surgeries,
Intra Aortic Balloon Pump facilities for patients with Cardiogenic shock; besides all routine
procedures like Permanent Pacemaker Implantation, Cardiac Re-synchronization Therapy
for heart failure, AICD implantation etc. which are available at our disposal along with
skilled manpower, why do we need to run to far-off places searching for these facilities.
Apart from Coronary Heart Disease, Congenital & Valvular heart diseases
needing surgeries are abundant in the North-East. Now all these people can be treated at
their doorsteps, without the extra burden of travelling to another part of the country.
Hayat Heart Centre is an advanced tertiary care unit; which was what the people of
our region needed for many years now. We, at Hayat Heart Centre, have come up with an
updated Cardiac Centre with all state of the art facilities where we are ever prepared to
handle any kind of cardiac emergency. The North-Eastern region is still running far behind
the national norms as far as Cardiac care facilities are concerned. Hence let us all come
together and help build a centre which will henceforth cater to all kinds of Cardiac problems
in our region. Apart from our own doctors, we will also be guided by eminent Cardiologists
and Cardiac Surgeons, having international fame and repute.
But our work is only half done if means for prevention of heart diseases are not
looked after. We, at Hayat Heart Centre have started regular health education campaigns
for the general masses.
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
Biochemical Markers
Dr. Bikash Kumar Chaudhury MD
Consultant Biochemist
“It is the middle of the night or maybe the early hours of a busy
working day when you suddenly feel a pain in your chest. At first
you may try to ignore it, but the pain has you scared and worried.
Could you be having a heart attack? Should you call for help or
even go to the emergency room?”
Chest pain is one of the most common reasons people call
for emergency medical help. Fortunately, chest pain does not always
signal a heart attack. Often it is unrelated to any heart problem. But,
even if the chests pain you experience has nothing to do with your
cardiovascular system, the problem may still be important — and
worth the time spent in an emergency room to have it evaluated.
Statistics from around the world show that Heart Diseases
are the foremost cause of chest pains and also the primary cause of
illness and death in the world. “Cardiac Biomarkers”, as diagnostic
biochemistry blood tests, can detect substances that are present in
the blood that indicate either the disease or a future risk of the
development of the disease.
Definition: - Cardiac Biomarkers are enzymes,
proteins and hormones that are associated with heart function,
damage, injury or failure. Some of the markers are specific for the
heart while others are elevated with skeletal muscle damage.
Cardiac biomarkers play a vital role in the clinical
diagnosis, management and risk stratification of heart diseases.
Ideally a true biochemical marker should have the following
criteria:-
I. It should be myocardial tissue specific; with high
concentration in the myocardium and absent in non
myocardial tissue
II. It should be highly sensitive
III. Should be detected even after several days of injury
IV. Assay method should be simple and quick; i.e. low Turn-
Around-Time (TAT) in the first few hours is crucial for
medical intervention.
Factors Responsible for Release of Biomarkers:-
Myocardial ischemia/ reperfusion activates many protein
kinase pathways such as the MAP kinases (ERK 1/2, JNK 1/2, p38
a/ß) and the cell survival kinases (Akt, Sodium-Hydrogen
Exchanger (NHE) kinase, p90 RSK)
Oxygen deprivation due to prolonged ischemia leads to
altered metabolism in the myocardial tissues beginning from
anaerobic glycolysis, inhibition of ATP driven transport processes in
the cell membrane, electrolyte shift, cellular edema and finally to
loss of cell membrane integrity.
Due to increased concentrations of lactate (anaerobic
glycolysis), there is a decrease of the intracellular pH which in turn
activate the lysosomal proteolytic enzymes and thereby
Cardiacdisintegrating intracellular structures and bound proteins.
Appearances of biomarkers in the blood stream are due to these
metabolic changes and they depend on:-
Ÿ Their intracellular location - i.e. molecules in cytosol are
released first.
Ÿ Molecular weight – smaller molecules diffuse faster
Ÿ Rate of elimination – smaller molecules are eliminated
faster than larger molecules
Ÿ Blood flow in the necrotic region
Cardiac biomarkers can be categorized into Classical
Biomarkers, Cardiac Biochemical Markers of Choice and New
cardiac Markers.
(A) Classical Biomarkers
The following summarizes the classical biomarkers. Most
of them are being phased out but some of these tests still exist in
some institutions where newer tests are not available.
1. CK or CPK (Creatine Phosphokinase):- It exists in
three isoforms as CKMM, CKMB and CKBB in the
skeletal muscles, heart and brain. Its appearance indicates
injury to muscle cells and appears 4 - 6 hrs after injury with
a peak in 18 - 24 hrs.
2. CPK – MB:- This isoform of CK has been considered
as the “ Gold Standard” for confirmation of Myocardial
Injury. This heart related portion of Ck enzyme indicates
heart cell injury appearing as early as 4 - 6 hrs after injury. It
is not very specific as in addition it appears in skeletal
muscle injury too. Nowadays it is used where new
diagnostic tests are not available.
3. LDH (Lactate Dehydrogenase):- This enzyme is found
in almost all body tissues and is a general marker of injury
to cells. It exists as five isoenzymes of which LDH-1 is
more heart specific but it may also rise in hepatitis. It is
being phased out as a cardiac marker as it is not specific.
4. SGOT or AST (Aspartate Tranaminase):- T h i s
enzyme found in the heart, liver and muscles indicate
cellular damage. It has been phased out as it is not specific.
(B) Biochemical Cardiac Markers of Choice
1. Cardiac Troponins:- Troponin is a protein complex
on the thin filament of striated muscles consisting of 3
(three) subunits i.e. Tn-T, Tn-I and Tn-C. Out of these Tn-C
is not specific for the heart where as Tn-T and Tn-I are now
regarded as most specific markers of myocardial injury.
The presence of Tn-T and Tn-I I the blood even in the
absence of CPK-MB indicates low levels of myocardial
injury. Cardiac Troponins appear within 3 - 4 hrs of heart
damage or injury and remains elevated for 7 - 14 days.
Cardiac Troponins are now being considered the “New
Gold Standard” for the diagnosis of Myocardial Injury
because:-
I. High Cardio-specificity especially Tn-I (100%)
II. Prolonged elevation i.e. diagnosis possible after
several days
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
III. High sensitivity even for minor degrees of
Myocardial Infraction
IV. Excellent prognostic indicator
V. Useful parameter for risk stratification
VI. Convenient and cost effective
Although Tn-T and Tn-I are good markers, Tn-I is more
specific for the heart because of its 31 amino acid sequence
on the N-terminus. Tn-I is 100% cardio-specific and not
elevated in chronic renal disease, skeletal muscle disease rdand trauma as opposed to Tn-T. However 3 generation Tn-
T assays do not allow skeletal Tn-T interference and
moreover life span of Tn-T in blood is greater than Tn-I.
2. Myoglobin:- This is a small (18 kd) oxygen storing
cytosolic protein that appears within 2 - 3 hrs of
myocardial injury with a peak in about 8 - 12 hrs and falls
back to normal by 24hrs. It is not cardio-specific as it may
be elevated in kidney diseases but it is often ordered with
CPK-MB and Troponin to help diagnose cardiac injuries.
3. HS-CRP (High Sensitivity C - reactive protein):-
Heart attacks and failures are usually the end result of
blockages in the arteries of the heart caused by
atherosclerosis. CRP is now used as marker of
inflammation and atherosclerosis. Elevated levels of CRP
correlate with an increased risk of heart attack, stroke,
sudden death and vascular disease.
4. BNP (B-Type Natriuretic Peptide):- BNP is a 32
amino acid polypeptide neurohormone secreted from
membrane granules of the cardiac ventricles (especially
the left) in response to stress including volume expansion
and pressure overload. Recently NT-proBNP (precursor of
BNP) has also been used as a cardiac biomarker.
Elevated levels of BNP and NT-proBNP correlate with the
severity of symptoms and prognosis. Their amount in
circulation is proportional to the degree of Left Ventricular
Dysfunction. They help to detect the presence of heart
failure, determine its severity and estimate prognosis.
5. MPO (Myeloperoxidase):- Myeloperoxidase is a
leukocytic enzyme that is produced by inflamed arteries
that have rupture prone fatty deposits. Inflamed arteries
can lead to blood clot and eventually to a heart attack or
stroke. MPO activity is significantly associated with CAD
but as neutrophil activation is not induced by ischemia,
MPO is a marker of plaque instability and not myocyte
damage.
Most cardiac biomarkers become present in the blood
stream only after myocardial injury has been done. By
measuring MPO levels in blood, it is possible to predict
whether a person is in the risk of heart attack or death in the
subsequent six months.
6. Homocysteine:- Homocysteine is a sulfur containing
amino acid derived from dietary Methionine and it has
been associated with cardiovascular events. The adverse
effect of Homocysteine involve oxidative damage to
vascular endothelial cells, increased proliferation of
smooth muscle cells and oxidative modification of Low
Density Lipoprotein (LDL) all leading to atherosclerosis.
Homocysteine due to its high sensitivity and accuracy is
considered an independent risk factor for Coronary Artery
Diseases (CAD). It is used to screen people at high risk
including patients who have a family history of CAD but
no other risk factors. Nevertheless routine screening is not
yet recommended as its role has not yet been established.
(C) New Cardiac Biomarkers
1. Matrix Metalloproteins (MMPs):- MMPs are
normally protective in nature and they limit and stabilize
plaque growth. MMP-9 is of particular interest as its value
relates to future cardiovascular death. MMP levels are
lowered by Renin-angiotensin system, aspirin, atorvastatin
and doxycycline. An ongoing study for this marker is still
going on.
2. Pregnancy Associated Plasma Protein A (PAPP-A):-
PA P P - A i s a Z i n c b i n d i n g m a t r i x
metalloproteinase which is abundantly expressed in
eroded and ruptured plaques whereas its levels are lower in
stable plaques. Although the release time of PAPP-A is yet
to be defined, increased circulating levels have been found
in hypercholesterolemia and coronary atherosclerosis and
even in some asymptomatic patients. Therefore PAPP-A
may serve as marker for total lipid burden.
3. Soluble CD40 Ligand:- Soluble CD40 ligand , a
marker of platlet activation and inflammation has been
shown to be associated with increased risk of
cardiovascular events in apparently healthy women.
Chronic elevations are of CD40 ligand is possible due to
shedding into the plasma from unstable atherosclerotic
plaque where as reduced levels maybe due to statins,
glitazones, glycoprotein IIb/IIIa inhibitors and
clopidogrel.
4. Placental Growth Factor (PlGF):- Placental Growth
factor stimulates angiogenesis by activating Vascular
Endothelial Growth Factor (VEGF) which in turn
improves circulation. VGEF plays an essential role in both
physiological and pathological angiogenesis where as
PlGF is restricted to only pathological conditions. PlGF is
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011

up-regulated in ischemic myocardium and plays a key role
in atheroma expansion. PlGF is a powerful independent
predictor of adverse cardiac events in Acute Coronary
Syndrome. PlGF does not correlate with Troponin levels
and therefore can be possibly used as a complementary
prognostic information marker.
5. Unbound Free Fatty Acids (FFAu):- Most of the
FFAs are bound to albumin. Free Fatty Acids (FFAu) that
are present are in the soluble form. Studies have shown that
there is a positive correlation between FFAu and Tn-I at
presentation of Acute Myocardial infarction.
6. Heart Type – Fatty Acid Binding Protein (H-FABP):-
It is a low molecular weight (15 kd) cytoplasmic
protein present in the myocardium and is released into
circulation following myocardial injury. It is more specific
and sensitive as compared to CPK-MB or myoglobin. It
has potential to be a useful prognostic indicator of
myocardial damage as well as clinical outcome of cardiac
surgeries.
7. Whole Blood Choline (WBCHO) & Plasma Choline
(PLCHO):- Both WBCHO & PLCHO rise rapidly
after stimulation of phospholipase D during tissue
ischemia and plaque destabilization. Phospholipase D
plays a key role in destabilizing plaques. Cholines released
into plasma are taken up by red blood cells. Cholines are
less specific for myocardial infarction than Unstable
Angina.
a. For Acute Myocardial Infarction:-
i. Sensitivity :- 40.5%
ii.Specificity:- 78.7%
b. Unstable Angina:-
i. Sensitivity :- 86.4%
ii.Specificity:- 86.2%
8. Ischemia Modified Albumin (IMA):- IMA is a
highly sensitive marker which is produced when
circulating albumin comes in contact with heart tissue.
During myocardial ischemia, albumin's capacity to bind to
cobalt is reduced. IMA typically rises within minutes if
ischemia stays up for 6-12 hours and returns back to
normal within 24 hours. IMA is detected even in reversible
myocardial ischemia where even troponins are difficult to
detect. Although it can be used as an early marker for
ischemia its usefulness is limited as it is also found in
patients with some cancers, infections, liver diseases, end
stage renal disease and brain ischemia. Another drawback
for IMA is that its levels are inhibited by endogenous
lactate production. Therefore its utility as a marker is
limited in diabetic ketoacidosis (DKA), sepsis, renal
failure and other causes of increased lactic acid.
9. PLAQ Test:- This new test measures the levels of
Lipoprotein Phospholipase A (Lp-PA ) which generates 2 2
oxidized molecules within blood vessel wall that leads to
both atherosclerosis and irritability of the atherosclerotic
plaque. An elevated level of Lp-PA2 indicates greater risk
of plaque formation and rupture and therefore greater risk
of cardiac events.
10. Glycogen Phosphorylase BB (GP-BB):- This is an
isoform of the key enzyme of glycogenolysis. With onset
of tissue hypoxia (e.g. myocardial infarction) when
glycogen is broken down, GP-BB is converted from a
structurally bound to a cytoplasmic form. This cytoplasmic
form is released into circulation in cell injury and hence it
is a sensitive marker for early diagnosis of Acute
Myocardial Infarction (AMI) or perioperative myocardial
injury. However it is cleared from circulation within 72
hours and therefore cannot be used as a late marker.
Conclusion
“Emergency Department Physicians are……………
……………..94.7% sensitive
……………..74% specific
…………………. In identifying patients who were subsequently
diagnose with Acute Coronary Syndrome (ACS) within 30 days of
Emergency Department visit. ”
Christenson et al. CMAJ 2004; 170: 1803
The goal of biochemical cardiac markers is to be able to
detect the presence and severity of an acute heart condition as soon
as possible so that appropriate treatment can be initiated. None of the
markers available so far meet all the criteria of an ideal marker.
Other cardiac biomarkers such as CNP, IGF-1, Endothelin-1,
Myotrophin, Cardiotrophin-1, etc have appeared in literature their
role yet remains to be ascertained. Moreover different biomarkers
have different time of their level of rise, peak and fall within the
body.
Therefore nowadays a multi-marker approach combining
each of these markers is used for cardiac assessment. Proteomic and
Genomic strategies (i.e. protein mapping and gene expression
studies) will further extend the approach and probably drive the
sensitivity above 99%. Currently most physicians order a “panel” of
markers containing:-
Ÿ inflammatory marker
Ÿ platelet aggregation marker
Ÿ ischemia marker
Ÿ necrosis marker
Ÿ hemodynamic marker
One of the most popular panels, the “TRIAGE CARDIO
PROFILER” includes Tn-I, CK-MB, Hs-CRP, BNP, Myoglobin and
Myeloperoxidase.
Most markers are promising but the search for the ideal
marker is still on and till such a marker is found we will be stuck with
a huge number of false positive cases which we will be required to
justify in some manner.
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
ACLS GUIDELINES -2010 KEY CHANGES IN THE MANAGEMENT OF ADULT CARDIAC ARREST Dr. Chandana Sarma M.D(Trained in Emergency Medicine and Critical Care , U.K) Chief Consultant Internal Medicine & Critical Care Hayat Hospital .
stIn1966, AHA developed the 1 CPR guidelines. Over the past 50
years these modern-era basic life support fundamentals of early recognition and activation , early CPR and early defibrillation have saved hundreds of thousands of lives around the world. These lives stand as a testament to the importance of resuscitation research and clinical translation.
In October 2010 the American Heart Association released their new guidelines for BLS and ACLS.
There were some major changes to BLS Guidelines and minor changes to ACLS Guidelines. Although the optimal approach to CPR may vary , depending on the rescuer , the victim and the available resources , the fundamental challenge remains : how to achieve early and effective CPR. Given this challenge , recognition of arrest and prompt action by the rescuer continue to be priorities for the 2010 AHA guidelines for CPR and Emergency Cardiovascular Care .
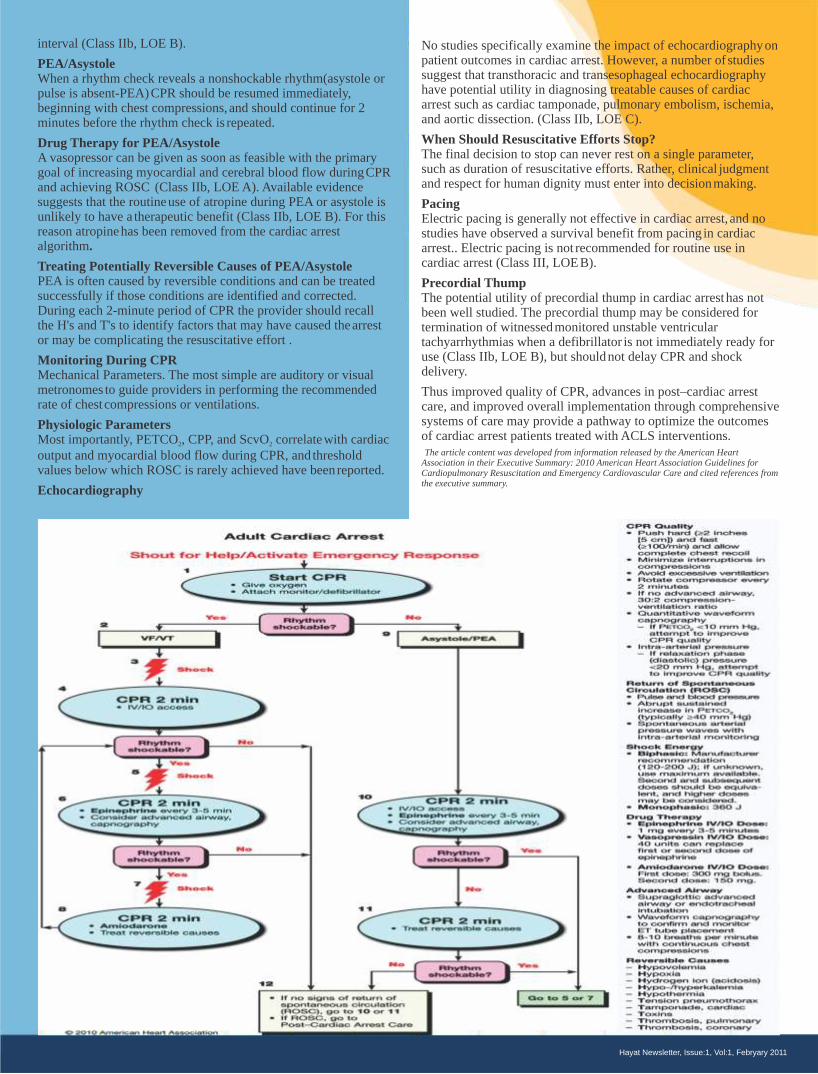
Key changes from the 2005 ACLS Guidelines include · Continuousquantitative waveform capnography is
recommended for confirmationand monitoring of endotracheal tube placement.
· Cardiac arrest algorithms are simplified and redesigned to emphasize the importanceof high-quality CPR
(including chest compressionsof adequate rate and depth, allowing complete chest recoil after each compression,
minimizing interruptions in chest compressionsand avoidingexcessive ventilation).
· Atropine is no longer recommendedfor routine use in the managementof pulseless electrical activity
(PEA)/asystole. · There is an increased emphasis on physiologic
monitoring tooptimize CPR quality and detect ROSC. · Chronotropicdrug infusions are recommended as an
alternative to pacing in symptomatic and unstable bradycardia.
· Adenosine is recommendedas a safe and potentially effective therapy in the initial managementof stable
undifferentiated regular monomorphic wide-complex tachycardia.
Overview of Airway Management. The purposeof ventilation during CPR is to maintain adequate oxygenationand sufficient elimination of carbon dioxide.
Ventilation and Oxygen Administration During CPR During low blood flow states such as CPR, oxygen delivery to the
heart and brain is limited by blood flow rather than byarterial , oxygen content.12 Therefore, rescue breaths are less important
than chest compressions during the first few minutesof resuscitation from witnessed VF cardiac arrest .
Passive Oxygen Delivery During CPR Chest compressions cause
air to be expelled from the chest and oxygen to be drawn into the chest passively due to the elastic recoil of the chest. In theory,
because ventilation requirements are lower than normalduring cardiac arrest, oxygen supplied by passive delivery is likely to be
sufficient for several minutes after onset of cardiacarrest . However at this time there is insufficient evidence to support the
removal of ventilations from CPR performedby ACLS providers.
Bag-MaskVentilation Bag-mask ventilation is an acceptable method of providing
ventilationand oxygenation during CPR..
AirwayAdjuncts Oropharyngeal Airways.To facilitatedelivery of ventilations with
a bag-mask device, oropharyngeal airways can be used in unconscious (unresponsive) patients withno cough or gag reflex
.(Class IIa, LOE C).
Nasopharyngeal AirwaysNasopharyngeal airways are useful in patients with airway
obstructionor those at risk for developing airway obstruction, particularlywhen conditions such as a clenched jaw prevent
placement of an oral airway. (Class IIa, LOE C).
Advanced Airways. Although insertion of an endotracheal tubecan be accomplished
during ongoing chest compressions, intubation frequently is associated with interruption of compressions formany seconds.
Placement of a supraglottic airway is a reasonablealternative .
Management of Cardiac Arrest Overview
Cardiac arrest can be causedby 4 rhythms: ventricular fibrillation (VF), pulseless ventricular tachycardia (VT), pulseless electric
activity (PEA), and asystole. The foundation of successful ACLS is high-quality CPR, and, for
VF/pulseless VT, attempted defibrillation within minutesof collapse
Rhythm-Based Management of Cardiac Arrest In most cases of witnessed and unwitnessed cardiac arrest the first
provider should start CPR with chest compressions and the second provider should get or turn on the defibrillator, place the adhesive
pads or paddles, and check the rhythm.
VF/Pulseless VT When a rhythm check reveals VF/VT, the first provider should
resume CPR while the second providercharges the defibrillator,CPR is paused to "clear" the patient and a single
shock is givenas quickly as possible to minimize the interruption in chest compressions ("hands-off interval"). The first provider resumesCPR immediately after shock delivery (without a rhythm or pulsecheck and beginning with chest compressions) and
continues for2 minutes.
Defibrillation Strategies If a biphasic defibrillator is available, providers should use the
manufacturer's recommended energy dose (eg, initial doseof 120 to 200 J) for terminating VF (Class I, LOE B). If a monophasic
defibrillator is used, providers should deliveran initial shock of 360 J and use that dose for all subsequent shocks.
Drug Therapy in VF/Pulseless VTWhen VF/pulseless VT persists after at least 1 shock and a 2-
minuteCPR period, a vasopressor can be given with the primary goalof increasing myocardial blood flow during CPR and
achievingROSC Amiodarone is the first-line antiarrhythmic agent given duringcardiac arrest because it has been clinically
demonstrated to improve the rate of ROSC and hospital admission in adults with refractory VF. Magnesium sulfate should be
considered only for torsades de pointes associatedwith a long QT
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
interval (Class IIb, LOE B).
PEA/AsystoleWhen a rhythm check reveals a nonshockable rhythm(asystole or
pulse is absent-PEA)CPR should be resumed immediately, beginning with chest compressions, and should continue for 2
minutes before the rhythm check is repeated.
Drug Therapy for PEA/Asystole A vasopressor can be given as soon as feasible with the primary
goal of increasing myocardial and cerebral blood flow duringCPR and achieving ROSC (Class IIb, LOE A). Available evidence
suggests that the routineuse of atropine during PEA or asystole is unlikely to have a therapeutic benefit (Class IIb, LOE B). For this
reason atropinehas been removed from the cardiac arrest algorithm.
Treating Potentially Reversible Causes of PEA/Asystole PEA is often caused by reversible conditions and can be treated
successfully if those conditions are identified and corrected. During each 2-minute period of CPR the provider should recall
the H's and T's to identify factors that may have caused thearrest or may be complicating the resuscitative effort .
Monitoring During CPRMechanical Parameters. The most simple are auditory or visual
metronomes to guide providers in performing the recommended rate of chest compressions or ventilations.
Physiologic Parameters Most importantly, PETCO , CPP, and ScvO correlatewith cardiac 2 2
output and myocardial blood flow during CPR, and threshold values below which ROSC is rarely achieved have been reported.
Echocardiography
No studies specifically examine the impact of echocardiographyon patient outcomes in cardiac arrest. However, a number of studies
suggest that transthoracic and transesophageal echocardiography have potential utility in diagnosing treatable causes of cardiac
arrest such as cardiac tamponade, pulmonary embolism, ischemia, and aortic dissection. (Class IIb, LOE C).
When Should Resuscitative Efforts Stop? The final decision to stop can never rest on a single parameter,
such as duration of resuscitative efforts. Rather, clinical judgment and respect for human dignity must enter into decisionmaking.
Pacing Electric pacing is generally not effective in cardiac arrest, and no
studies have observed a survival benefit from pacing in cardiac arrest.. Electric pacing is not recommended for routine use in
cardiac arrest (Class III, LOEB).
Precordial Thump The potential utility of precordial thump in cardiac arresthas not
been well studied. The precordial thump may be considered for termination of witnessedmonitored unstable ventricular
tachyarrhythmias when a defibrillator is not immediately ready for use (Class IIb, LOE B), but shouldnot delay CPR and shock
delivery. Thus improved quality of CPR, advances in post–cardiac arrest
care, and improved overall implementation through comprehensive systems of care may provide a pathway to optimize the outcomes
of cardiac arrest patients treated with ACLS interventions. The article content was developed from information released by the American Heart Association in their Executive Summary: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care and cited references from the executive summary.
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011

mass and the defect in the abdominal wall. So, the preperitoneal
space is the logical site to implant a prosthesis. The prosthesis is held
in place by intra-abdominal pressure. Care of the Myopectineal
orifice is paramount to the successful repair and prevention of hernia
recurrence. Out of all the repairs only the laparoscopic repair and the
PHS mesh provide complete coverage of the myopectineal orifice.
In laparoscopic inguinal hernia repair: the mesh is placed in
preperitoneal space. Laparoscopic repair is definitely, inherently
riskier than open hernioplasty. Unlike open hernioplasty it requires a
surgeon who is very experienced and highly skilled with the
technique otherwise morbidity, mortality and recurrence rates are
significantly higher. Moreover laparoscopic inguinal hernia repair
has a steep learning curve and also a high cost and always needs
general anesthesia.
In 1998 Prolene hernia system (PHS) mesh consisting of an onlay
and an underlay patch attached with a connector, was introduced by
Gilbert as an option
For tension free open repair of inguinal hernias combining benefits
of posterior and anterior repair from an anterior approach the overall
concept of its design was to include the best features of all currently
available techniques while eleminating their undesirable features.
Different studies have shown improved outcomes extremely low
recurrence rates, ease of placement, less post-op pain, rapid return to
work by using PHS mesh compared with the time honoured
Lichtenstein repair. PHS mesh has been designed for the repair of
direct, indirect and femoral hernias with extremely low recurrence
rates secondary to complete coverage of the myopectineal orifice.
Unlike laparoscopic inguinal hernia, PHS mesh repair can be
performed under local or regional anaesthesia and it needs less
operative time.
We have performed 18 cases (paraumbilical, epigastric hernias 6
cases, inguinal hernias 12 cases) of PHS mesh repair in last 2 years.
There is no incidence of infection, seroma or hematoma.
Postoperative pain is significantly less and so the recovery is
excellent and return to work is early. Only one female patient in
inguinal hernia series complained of mild groin pain on flexion of
the lower limb. There is no recurrence till now. We have also
experienced low learning curve of this procedure.
CONCLUSION: More than thirty techniques of repair are
performed for inguinal hernias in last hundred years. Attempts are
still carried on to achieve the best repair. Lichtenstein anterior mesh
PROLENE HERNIA SYSTEM MESH –
ITS EVOLUTIONA NEW TECHNIQUE TO REPAIR INGUINAL HERNIASDr. S. K. Nath, Senior Surgeon
Inguinal Hernia is a very common surgical condition. Since more
than a century surgical repairs are attempted to correct this
condition. More than thirty techniques of operation have been tried
till now. Every time a new technique has evolved it is thought if we
have achieved the best ultimately. But it seems that the best is yet to
come.
The anterior approach is used for repair for more than a
century. Tension is the principal cause of failure of all the
hernioplasties that close the myopectineal orifice by apponeurotic
approximation. Bassini wrote 6 papers about his surgical technique
of inguinal tissue repair and experiences between 1887 to 1894. This
procedure was justifiably criticized because it did not repair the
femoral canal and might actually cause some femoral hernias by
straining the femoral sheath. Anterior preperitoneal approach of
inguinal hernia repair was first described by Annandale in 1876.
Ruggi (1892) and Lotheissen (1898) later furthered its popularity.
Posterior preperitoneal approach for femoral and inguinal
hernia repair was used sporadically in the nineteenth century. But
credit is given to Cheatle (1920) and Henry (1936) who popularized
the virtues of this approach. They used a midline incision. Nyhus
(1959) and later Read were enthusiastic to use the preperitioneal
approach through a lower transverse incision. The repair closes the
direct space by suturing the iliopubic tract to the transverse
aponeurotic arch and narrows the deep ring.
Tension free Hernioplasties : Credit for originating the first
tension free and sutureless hernioplasty goes to Stoppa who in 1969
introduced a preperitoneal hernioplasty in which parietal defects
were not closed and peritoneal herniation were prevented by a large
piece of unsutured polyster mesh. He used Pfannestiel incision.
Recurrence and post-operative pain decreased. Lichtenstein
popularized the anterior tension free hernioplasty in 1986 by using 8
x 16 cm synthetic mesh. Lichtenstein tension free mesh repair has
been the most widely performed groin hernia repair and is used as
the standard to which newer techniques are compared.
Plug Hernioplasty: Gilbert discovered that a cone shaped plug
made from polypropylene mesh when passed through the deep ring
to preperitoneal space would retain inverted indirect inguinal
hernial sac. He surmised, the plug unfolded like an umbrella to
occlude the deep ring. The unfixed plug was reinforced with a patch
similar in size and shape to that of the Lichtenstein repair but
without fixation. Lichtenstein also tried plug repair which was
sutured flush in place with 4 or more permanent synthetic sutures.
Ratkow and Robbins also used plugs for repairing inguinal hernias.
But it was ineffective because the plugs were expellable without a
covering barrier of mesh.
All hernial surgeons have recognized the irrefutable fact that ideal
location for a prosthetic mesh barrier is between forceful hernia
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
repair is the most popular and well accepted technique since 1986
and it is still the mostly performed inguinal hernia repair today. But
in recent time all hernia surgeons have agreed that preperitoneal
space is the logical site to implant a mesh so that whole of
myopectineal orifice can be taken care of to achieve zero recurrence.
Out of all recent hernia repair techniques only the laparoscopic
repair and PHS mesh repair fulfill this requirement. Somehow
laparoscopic technique, has not gained popularity due to its steep
learning curve, higher cost involvement, higher and disasterous
morbidity and mortality if this is not performed by properly trained,
highly skilled lap surgeon. In that comparison, PHS mesh repair can
be performed under LA or SA and has a low learning curve, low
morbidity, low recurrence rates and early recovery and results are
reproducible by all general surgeons even in remote peripheral
hospitals.
Our experience with PHS mesh repair of inguinal hernias and small
ventral and paraumbilical hernias is excellent. As Mr. Gilbert, the
inventor of PHS mesh repair has felt, we also have started thinking
“Have we achieved the best in inguinal Hernia Surgery?”
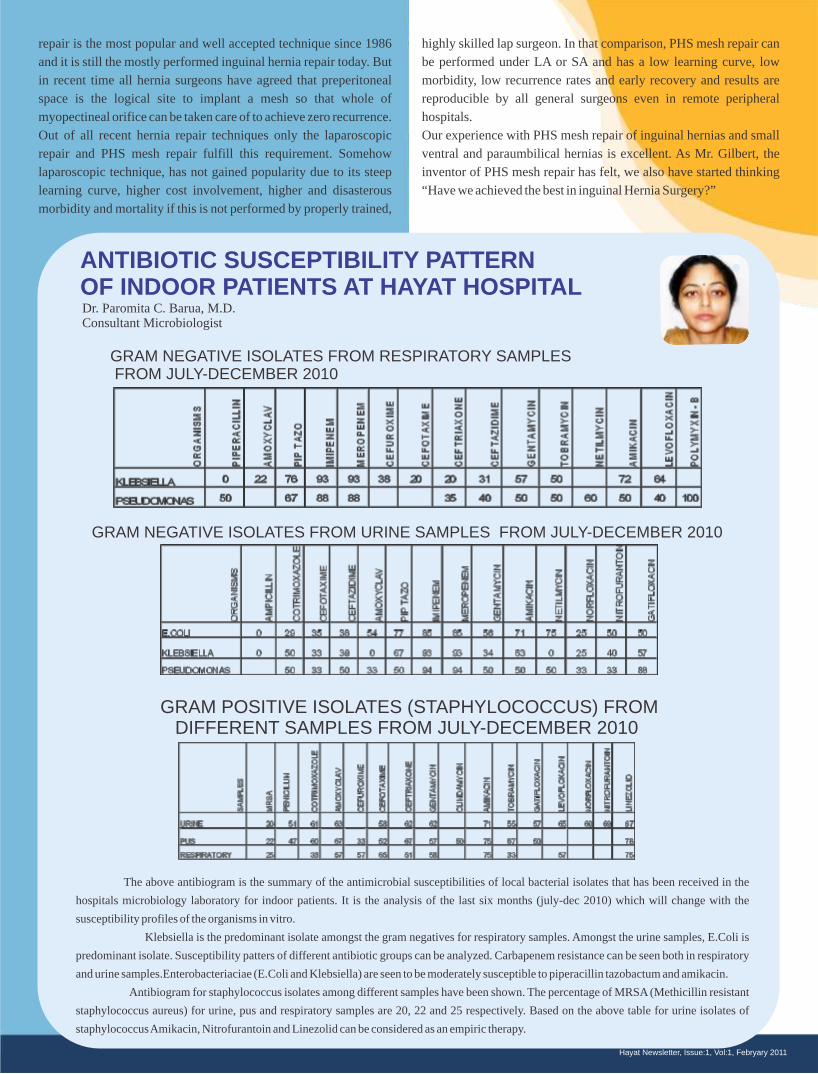
GRAM NEGATIVE ISOLATES FROM RESPIRATORY SAMPLES FROM JULY-DECEMBER 2010
ANTIBIOTIC SUSCEPTIBILITY PATTERN OF INDOOR PATIENTS AT HAYAT HOSPITAL
GRAM NEGATIVE ISOLATES FROM URINE SAMPLES FROM JULY-DECEMBER 2010
GRAM POSITIVE ISOLATES (STAPHYLOCOCCUS) FROM DIFFERENT SAMPLES FROM JULY-DECEMBER 2010
The above antibiogram is the summary of the antimicrobial susceptibilities of local bacterial isolates that has been received in the
hospitals microbiology laboratory for indoor patients. It is the analysis of the last six months (july-dec 2010) which will change with the
susceptibility profiles of the organisms in vitro.
Klebsiella is the predominant isolate amongst the gram negatives for respiratory samples. Amongst the urine samples, E.Coli is
predominant isolate. Susceptibility patters of different antibiotic groups can be analyzed. Carbapenem resistance can be seen both in respiratory
and urine samples.Enterobacteriaciae (E.Coli and Klebsiella) are seen to be moderately susceptible to piperacillin tazobactum and amikacin.
Antibiogram for staphylococcus isolates among different samples have been shown. The percentage of MRSA (Methicillin resistant
staphylococcus aureus) for urine, pus and respiratory samples are 20, 22 and 25 respectively. Based on the above table for urine isolates of
staphylococcus Amikacin, Nitrofurantoin and Linezolid can be considered as an empiric therapy.
Dr. Paromita C. Barua, M.D. Consultant Microbiologist
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
THE HAYAT TEAM
HAYAT HEART CENTRE
Dr Bhabananda Das,MS ,M.Ch.Chairman cum CTVS SurgeonDr Sasanka Baruah,MD,DNBDirector cum Chief CardiologistDr Bishnu Deka,MS,MChDirector cum Chief CTVS SurgeonDr Hemjit Talukdar,MBBS,DADirector cum Chief Cardiac IntensivistProf. Upendra Kaul,MD,DM,FACCVisiting CardiologistDr Balbir Singh, MD,DM,FACCVisiting CardiologistDr Robin Chakraborty,MD,DNB,DMVisiting CardiologistDr Dibya J.Baruah,MD,DMVisiting CardiologistDr Neil Bordoloi,MD,DMVisiting CardiologistDr Jayanta Kr. Das, MS,M.ChVisiting CTVS SurgeonDr S,Gupta,MS,MchVisiting Cardiac SurgeonDr Arnab Paul,MBBS,PGDCCJunior CardiologistDr A. Zaman Ahamed, MBBS, PGDCCJunior CardiologistDr. Anupam Biswas, MBBS, PGDCCJunior CardiologistMr. Chitranjan Das Bsc, Dip. in Perfusion TechnologyChief Perfusionist
HAYAT KIDNEY AND UROLOGY CENTRE
Dr Joy Chakraborty,MS,FRCS(UK),DNB(Surgery),DNB(Uro)Director UrologyDr Anjan Borkotaky,MD,DMChief Consultant NephrologyDr U.Choudhury,MSDeputy Consultant
DEPARTMENT OF NEPHROLOGY & DIALYSIS
Dr Anjan Borkotaky,MD,DMConsultant NephrologyDr A.Kr.Barman,MD,DMVisiting Consultant
DEPARTMENT OFNEUROSURGERY
Dr Shameem Ahmed,MS,MChChief Neuro SurgeonDr M.L.A.Rahman,MChVisiting Neuro SurgeonDr R.J.Hazarika,MS,MChVisiting Neuro Surgeon
Dr. Zakir Hussain,MS,MChVisiting Neuro Surgeon
DEPARTMENT OFNEUROLOGY & NEUROSCIENCE
Dr Monalisha S.Goswami.MD,DNBConsultant NeurologistDr Mridula Shyam,MDConsultant Neurophychiatry
HAYAT EMERGENCY& TRAUMA CENTRE
Dr. Atanu Borthakur ,MSDirector cum Consultant Surgeon, Trauma,Burn & Critical Care SpecialistTrained in Uk & SingaporeDr Shameem Ahmed,MS,MchChief Neuro Trauma SurgeonSpecialist in Head injury & Gunshot injuryTrained in AIIMSDr.Parag Neog, MS, Consultant Surgeon,Trained in burns, plastic & maxillofacial surgeryMicro-vascular surgery (AIMS, Kochi) Dr. S.K. Nath, MS(Del), FAIS, FICS, MAMS (VIENNA)Consultant Sr. SurgeonDr. Iran Bharali, MS Orthopaedic & Reconstructive SurgeonDr. C.Nag.Choudhury, MSConsultant ,Hand,Foot,and Orthopaedic Reconstructive SurgeonDr. Uttam Choudhury,MSConsultant SurgeonDr. Karabi Borgohain, MSConsultant Surgeon (ENT)Dr.Tulika Baruah Deka,MSConsultant OpthalmologyDr.Pompy Choudhury,MDConsultant RadiologistDr. Sajida Sultana, RMODr. Pranamee Das Bora, RMODr. Pragyan Kalita,RMODr. Kishor Kumar,RMODr. Vineeta Sharma,RMO
HAYAT EMERGENCY AND CRITICAL CARE
Dr. Chandana Sharma, MDChief ConsultantEmergency & Critical Care Specialist, trained in UKDr. D. Patowari, MDSenior ConsultantDr. Debajit Das, MDSenior Consultant Internal MedicineDr. Bivas Bhagabati,MBBS, DASenior IntensivistDr. Babu Pathak, MBBS, DASenior IntensivistDr. Homen Deka, MBBS, DA
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011
Dr Z.Rahman,CMD
Mr. Rajib SaikiaCEO
Dr Atanu Barthakur,Medical Director
Mr. Manoj Kr. DekaGM
Consultant IntensivistDr. Pranjal Deka MBBS DAConsultant IntensivistDr. Diganta Brahma,MBBSJounior Consultant Dr. Manoj Kr. Saikia,MDSenior Visiting Intensivist
HAYAT BURN CENTRE
Dr. Atanu Borthakur, MSConsultant SurgeonTrauma,Burn & Critical Care SpecialistTrained in Uk & SingaporeDr. Parag Neog, MSConsultant Cosmetic & Plastic SurgeonTrained in burns, plastic & maxillofacial surgeryMicro-vascular surgeryDr. C. Sarma,MDConsultant Internal Medicine & Critical CareDr. Uttam Choudhury,MSDeputy Consultant Surgeon
HAYAT GI SURGERY& ENDO-LAPROSCOPY CENTRE
Dr. S.K.Nath,MS(Del), FAIS, FICS, MAMS (VIENNA)Dr. N.N.Das,MS,FAIS,FICS,FIAGESG I Surgery(AIIMS)Dr A.Borthakur,MSDr. Pankaj Bhagawati,MSDr A.K.Deb,MSTrained in Advance Laproscopy surgery UKDr Arnab Baruah,MS,FIAGESDr Abhijit Baruah,MSDr.Uttam Choudhury,MS
DEPARTMENT OFORTHOPAEDICS
Dr. C.Nag.Choudhury, MSConsultant ,Hand,Foot,andOrthopaedic Reconstructive SurgeonDr. Iran Bharali, MSOrthopaedic & Reconstructive SurgeonDr. Rakesh Das,MSVisiting Consultant Orthopaedic SurgeonDr. Bikas Bordoloi,MSVisiting Consultant Orthopaedic Surgeon
DEPARTMENT OFINTERNAL MEDICINE
Dr. Chandana Sharma, MD, Chief ConsultantDr. D. Patowari, MD, Senior ConsultantDr. D. Das, MD, Senior ConsultantDr. Surajit Baruah, MDSenior Visiting Consultant
DEPARTMENT OFOBSTETRICS & GYNAECOLOGY
Dr. Minakshi Sarma,MDConsultant O&GDr. Arpita Sarma, MDConsultant O&GDr. Dippy Aggarwal, MDConsultant O&GDr. J.P.More,MDConsultant O&G
DEPARTMENT OFPADETRICS
Dr. Geetima Deka Dey ,MBBS,DCHDr. Surajit Mazumdar,MBBS,DCH
DEPARTMENT OF OPHTHALMOLOGY
Dr Santanu Barthakur, MSVisiting Consultant OpthalmologistDr.Tulika Baruah Deka,MSConsultant OpthalmologistDr. A.Latif,MSVisiting Consultant Opthalmologist
DEPARTMENT OF ENT
Dr. Karabi Borgohain,MSConsultant ENT surgeonDr. R.B.Goswami,MSConsultant ENT surgeon
DEPARTMENT OFPSYCHIATRY
Dr. Mridula Shyam,MDConsultant PhychiatristDr. Madhukar J. Choudhury,MDConsultant Phychiatrist
DEPARTMENT OFRADIOLOGY & IMAGING
Dr.Pompy Choudhury,MDConsultant RadiologistDr.Gazi S. Ahamed,MDVisiting Consultant RadiologistDr. Satradhar ChoudhuryVisiting Consultant Radiologist
DEPARTMENT OF CLINICAL LABORATORY
Dr.Paromita Baruah,MD Consultant MicrobiologistDr.Bikash Kr Chaudhury,MD Consultant BiochemistDr.Kasturi Kalita, MBBS, DCP Consultant Pathologist
DEPARTMENT OF PMRD
Dr. Sambit Kesori, PhysiothearapistDr. Duyu Nipa, Physiothearapist
Hayat Newsletter, Issue:1, Vol:1, Febryary 2011

KAHILIPARA ROAD, ODALBAKRA, LALGANESH, GUWAHATI-781 034, ASSAM,, Ph: 0361-2470088, 80110-03110 (M), email: [email protected]





























