Embed Size (px)
Citation preview

NÖRAL TÜP DEFEKTLERİ
DR. GÖKHAN YILDIRIM

En sık 2. konjenital anomali
İnsidansı 1/1000 doğum
Türkiye de insidansı ?
Folik asit kullanımı insidansı
azaltmıştır

Embriyoloji

Sınıflama
Kraniyal Defektler
Anensefali
Eksensefali
Ensefalosel
İniensefali
• Spinal defektler
Açık/kapalı
Meningosel/meningomiyelos
el
304 N. D. E. GREENE AND A. J. COPP
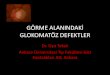
Figure 1—Schematic diagram of neural tube closure and the affected events leading to NTDs (indicated by red arrows). Neural tube closure isinitiated by closure 1 at the hindbrain/cervical boundary in mouse (a) and spreads caudally and rostrally from this site (black arrows). Closure 1in human (b) may occur in the rhombencephalon, more rostrally than in mouse. Failure of closure 1 results in craniorachischisis. A second site ofinitial closure (closure 2) occurs at the forebrain/midbrain boundary in most mouse strains (a), although the position of the site of closure 2 mayvary between strains. This site may be absent in humans (b). Closure also initiates at the rostral limit of the forebrain (closure 3) in mouse and anequivalent closure occurs in humans. Progress of neurulation from the initial sites of fusion results in shortening and closure of the anterior andhindbrain neuropores, indicated by arrows. Failure of initial closure sites or closure of neuropores results in anencephaly. Neurulation progressescaudally from the site of closure 1 until fusion is finally completed by closure of the posterior neuropore. Open spina bifida results from failureof posterior neuropore closure. Secondary neurulation proceeds from the level of the closed posterior neuropore. Modified from (Copp et al.,1994, 2003b)
In the human embryo, neural plate bending begins atabout 17–18 days after fertilization. Initiation of neuraltube closure occurs, as in mice, by a discontinuous pro-cess (Figure 1), and analogous events to closure 1 and 3have been described (O’Rahilly and Muller, 1994, 2002).The site of initial closure (equivalent to mouse closure1) may occur at a slightly more rostral level in humansthan in mouse, being located in the rhombencephalonas opposed to the rhombencephalon/cervical boundary(O’Rahilly and Muller, 2002). Closure at the extremerostral end of the neural plate (closure 3) appears tooccur in humans as in the mouse (O’Rahilly and Muller,2002). However, the existence of an event equivalent toclosure 2 is more controversial, having been proposedin some studies (Van Allen et al., 1993; Golden andChernoff, 1995; Seller, 1995b) but not others (O’Rahillyand Muller, 2002). The presence of closure 2 has beeninferred from observation of late stage anencephalicfetuses (Van Allen et al., 1993; Seller, 1995b), whereasdirect analysis of early human embryos has suggestedthat a closure 2 event either occurs at a more caudal posi-tion than in mice, in the hindbrain (Nakatsu et al., 2000),or not at all (O’Rahilly and Muller, 2002). Therefore,there may be variability in the position or occurrence ofclosure 2 in human neurulation. Closure in the cranialregion is completed on day 25 and closure of the poste-rior neuropore, which completes primary neurulation, at26–28 days postfertilization.
DIFFERING MECHANISMS OF CLOSURE IN THECRANIAL AND SPINAL REGIONS
Although the principles of neurulation are conservedthroughout primary neurulation, involving elevation andfusion of neural folds, the detailed mechanism appears
to differ markedly with axial level and developmentalstage. Thus, in the cranial region of the mouse embryobending of the neural folds during closure is quitedifferent from that in the spinal region. As they initiallyelevate, about a midline hinge point, the neural foldsassume a biconvex appearance in the midbrain with thetips of the folds facing away from the midline. The foldsthen switch orientation to assume a biconcave shapein which the tips approach each other in the midline,allowing fusion to occur (Morriss-Kay, 1981; Morriss-Kay et al., 1994).
Spinal neurulation contrasts with cranial closure inlacking a biconvex phase of neural fold elevation.Instead, the spinal neural folds exhibit a stereotypicalpattern of bending with hinge points at two locations:the median hinge point (MHP) overlying the notochord,which creates the midline ‘neural groove’ with itsV-shaped cross-section, and paired dorsolateral hingepoints (DLHPs), which create longitudinal furrows thatbring the neural fold tips toward each other in the dorsalmidline. Different combinations of bending points areutilized as closure progresses down the spinal neuraxis(Figure 2). In the early stages of spinal neurulation, atE8.5, the neural plate bends solely at the MHP, whereasby early E9.5, as closure progresses to the thoracic level,bending occurs at DLHPs in addition to the MHP. AtE10, when the low spinal neural tube is forming, MHPbending is lost and the neural plate bends solely atDLHPs (Shum and Copp, 1996).
FAILURE OF NEURULATION RESULTS INNEURAL TUBE DEFECTS
Open NTDs (including open spina bifida and anen-cephaly in mammals) result from failure of the neural
Copyright Ó 2009 John Wiley & Sons, Ltd. Prenat Diagn 2009; 29: 303–311.DOI: 10.1002/pd

Etiyoloji ve Risk Faktörleri

Tekrarlama Riski


Biyokimyasal Tarama

Ultrasonografi

Transver/aksiyel kesit
Sagittal kesit Koronal kesit


İkinci trimester USG bulguları:
Kranyumun üst kısmı izlenmez
Heterojen kitle görünümü
Polihidroamnios
SONOEMBRYOLOGY OF CNS AND EARLY PRENATAL DIAGNOSIS 319
Figure 8—Section through heads of embryos with acrania/exencephaly; the contours of the brain are irregular (arrows), the braincavities are ‘empty’ (a) CRL 22 mm (b) CRL 28 mm
brain tissue can be seen, as we have reported in a caseof craniorachischisis (Figure 9a) at 13 weeks of gesta-tion (Blaas and Eik-Nes, 1999b). As in acrania, cran-iorachischisis may also have ‘empty’ brain cavities. Inaddition, one will often find anomalous shape of thespine (Figure 9b).
Spina bifida
According to the embryological process of neurulation,neural tube defects have different modes of origin, sug-gesting different pathomechanisms (Copp et al., 1990).Myelomeningocele (commonly called spina bifida)results from the failure of fusion in the spinal regionof the neural tube. The defective development of themidbrain and hindbrain with elongation of the midbrainand a herniation of the cerebellum and medulla towardsthe foramen magnum is called Arnold–Chiari malfor-mation. The time of its origin is almost certainly inthe embryonic period at the time of neural tube closure,especially the closure of the caudal neuropore (Gardneret al., 1975).
The typical features of spina bifida at midgestationare: the ‘lemon’ shape of the head, BPD somewhat
Figure 9—(a) Post abortem photography and ultrasound image ofcoronal section through the head of a 13-week-old foetus with cran-iorachischisis; the head was fluid-filled and covered by a membrane(arrows) that ruptured during the delivery (b) Craniorachischisis in a22-mm CRL embryo; the brain cavities are ‘empty’, there is a sharpbend of the dysraphic spine (arrow) Y, yolk sac
smaller than expected, ‘hanging’ choroid plexuses in thedilated lateral ventricles, curved shape of the cerebellum(banana sign) and dysraphic defect of the spine.
The diagnosis of neural tube defect (NTD) has beenmade at early post-embryonic stages, in other wordsafter 10 weeks: Blumenfeld and coworkers presented10 cases with first-trimester and early second-trimesterNTD detected by ultrasound (Blumenfeld et al., 1993).In their earliest case, a sacral irregularity was suspectedin a 10-week-old pregnancy (no biometric data pre-sented). Bernard and coworkers described a 10-week-5-day-old foetus (CRL 31 mm) with a lumbo-sacralmyelomeningocele (Bernard et al., 1997). In this foetus,the lemon shape and cerebellar signs of Arnold–Chiarimalformation could not be detected at 12 weeks, priorto termination of the pregnancy.
Hernadi and Torocsik reported three cases of spinabifida at 12 to 14 weeks detected in a screening programin a population consisting of 3758 pregnancies at lowrisk for congenital anomalies, and 233 pregnanciesat high risk (Hernadi and Torocsik, 1997). They didnot report the diagnostic key for their diagnosis. The‘lemon’ sign was found in three first-trimester cases ofspina bifida at 12, 13 and 14 weeks (CRL 56, 62 and
Copyright Ó 2009 John Wiley & Sons, Ltd. Prenat Diagn 2009; 29: 312–325.DOI: 10.1002/pd
SONOEMBRYOLOGY OF CNS AND EARLY PRENATAL DIAGNOSIS 319
Figure 8—Section through heads of embryos with acrania/exencephaly; the contours of the brain are irregular (arrows), the braincavities are ‘empty’ (a) CRL 22 mm (b) CRL 28 mm
brain tissue can be seen, as we have reported in a caseof craniorachischisis (Figure 9a) at 13 weeks of gesta-tion (Blaas and Eik-Nes, 1999b). As in acrania, cran-iorachischisis may also have ‘empty’ brain cavities. Inaddition, one will often find anomalous shape of thespine (Figure 9b).
Spina bifida
According to the embryological process of neurulation,neural tube defects have different modes of origin, sug-gesting different pathomechanisms (Copp et al., 1990).Myelomeningocele (commonly called spina bifida)results from the failure of fusion in the spinal regionof the neural tube. The defective development of themidbrain and hindbrain with elongation of the midbrainand a herniation of the cerebellum and medulla towardsthe foramen magnum is called Arnold–Chiari malfor-mation. The time of its origin is almost certainly inthe embryonic period at the time of neural tube closure,especially the closure of the caudal neuropore (Gardneret al., 1975).
The typical features of spina bifida at midgestationare: the ‘lemon’ shape of the head, BPD somewhat
Figure 9—(a) Post abortem photography and ultrasound image ofcoronal section through the head of a 13-week-old foetus with cran-iorachischisis; the head was fluid-filled and covered by a membrane(arrows) that ruptured during the delivery (b) Craniorachischisis in a22-mm CRL embryo; the brain cavities are ‘empty’, there is a sharpbend of the dysraphic spine (arrow) Y, yolk sac
smaller than expected, ‘hanging’ choroid plexuses in thedilated lateral ventricles, curved shape of the cerebellum(banana sign) and dysraphic defect of the spine.
The diagnosis of neural tube defect (NTD) has beenmade at early post-embryonic stages, in other wordsafter 10 weeks: Blumenfeld and coworkers presented10 cases with first-trimester and early second-trimesterNTD detected by ultrasound (Blumenfeld et al., 1993).In their earliest case, a sacral irregularity was suspectedin a 10-week-old pregnancy (no biometric data pre-sented). Bernard and coworkers described a 10-week-5-day-old foetus (CRL 31 mm) with a lumbo-sacralmyelomeningocele (Bernard et al., 1997). In this foetus,the lemon shape and cerebellar signs of Arnold–Chiarimalformation could not be detected at 12 weeks, priorto termination of the pregnancy.
Hernadi and Torocsik reported three cases of spinabifida at 12 to 14 weeks detected in a screening programin a population consisting of 3758 pregnancies at lowrisk for congenital anomalies, and 233 pregnanciesat high risk (Hernadi and Torocsik, 1997). They didnot report the diagnostic key for their diagnosis. The‘lemon’ sign was found in three first-trimester cases ofspina bifida at 12, 13 and 14 weeks (CRL 56, 62 and
Copyright Ó 2009 John Wiley & Sons, Ltd. Prenat Diagn 2009; 29: 312–325.DOI: 10.1002/pd

İntrakranyal içeriğin karanyal defektten protrüzyonu
Sonografik bulgular;
Kistik ve/veya solid kitle
Kalvaryumda defekt
Kist içinde kist
Ventrikülomegali
• Karyotip
404 M. CAMERON AND P. MORAN
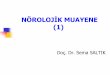
Figure 2—Occipital encephalocele
Figure 3—Classical lemon shaped head with ventriculomegaly seenin a fetus with spinabifida
the frontal bones (Campbell et al. 1987; Nyberg et al.,1988).
Figure 4—Banana cerebellum associated with spina bifida
The banana sign refers to the shape of the cerebellum,which is distorted as part of the Chiari type II malfor-mation. The cerebellum may also be absent as part ofthe Chiari type II malformation which is seen in 95%of open NTD and does not resolve as the pregnancyadvances.
Pooled data from 234 fetuses with spina bifida showedthat 99% had at least one cranial finding at less than24 weeks (Watson et al., 1991). Lemon and banana (orabsent cerebellum) signs were both seen in 97% offetuses, with ventriculomegaly seen in 75%, cisternamagna obliteration in 68% and small biparietal diameterin 61%. An Italian study recently reported on 49 fetuseswith spina bifida and assessed six sonographic signs inprenatal diagnosis (D’Addario et al. 2008). They founda small cerebellum in 96% of cases, an effaced cisternamagna in 93% and a small posterior fossa in 96%. Lessconsistent cranial signs were ventriculomegaly (81%)and “lemon” sign (53%).
Subtle supratentorial signs are seen with the Chiaritype II malformation. Fujisawa et al. (2006) describedlate pregnancy changes in the shape of the enlargedposterior horn of the lateral ventricle in the coronal view,and Callen and Filly described a lateral ventricle witha pointed shape in axial view although this was morecommon prior to 24 weeks and in ventricles of normalsize (Callen and Filly 2008).
Ghi et al. (2006) reported that while all 53 casesof open spina bifida had alterations in cranial anatomy(including the “banana” and “lemon” signs), with closedspina bifida (7% of their population) cranial signs donot develop. They conclude that the “the differentiationbetween open and closed spina bifida is best shown bythe sonographic demonstration of abnormal or normalcranial anatomy.”
To accurately identify the type and extent of the lesionsagittal, coronal and axial spinal views are all required(Figure 5). The bony defect is identified by splaying ofthe posterior lamina ossification centers in the coronaland axial plane (Figure 6). The bony defect may lie ator cranial to, the level at which there is protrusion of themeninges (meningocele) or meninges plus neural tissue(myelomeningocele).
All lesions arise from a dysraphism (defect of closure)and are classified as open or closed depending on
Copyright Ó 2009 John Wiley & Sons, Ltd. Prenat Diagn 2009; 29: 402–411.DOI: 10.1002/pd
404 M. CAMERON AND P. MORAN
Figure 2—Occipital encephalocele
Figure 3—Classical lemon shaped head with ventriculomegaly seenin a fetus with spinabifida
the frontal bones (Campbell et al. 1987; Nyberg et al.,1988).
Figure 4—Banana cerebellum associated with spina bifida
The banana sign refers to the shape of the cerebellum,which is distorted as part of the Chiari type II malfor-mation. The cerebellum may also be absent as part ofthe Chiari type II malformation which is seen in 95%of open NTD and does not resolve as the pregnancyadvances.
Pooled data from 234 fetuses with spina bifida showedthat 99% had at least one cranial finding at less than24 weeks (Watson et al., 1991). Lemon and banana (orabsent cerebellum) signs were both seen in 97% offetuses, with ventriculomegaly seen in 75%, cisternamagna obliteration in 68% and small biparietal diameterin 61%. An Italian study recently reported on 49 fetuseswith spina bifida and assessed six sonographic signs inprenatal diagnosis (D’Addario et al. 2008). They founda small cerebellum in 96% of cases, an effaced cisternamagna in 93% and a small posterior fossa in 96%. Lessconsistent cranial signs were ventriculomegaly (81%)and “lemon” sign (53%).
Subtle supratentorial signs are seen with the Chiaritype II malformation. Fujisawa et al. (2006) describedlate pregnancy changes in the shape of the enlargedposterior horn of the lateral ventricle in the coronal view,and Callen and Filly described a lateral ventricle witha pointed shape in axial view although this was morecommon prior to 24 weeks and in ventricles of normalsize (Callen and Filly 2008).
Ghi et al. (2006) reported that while all 53 casesof open spina bifida had alterations in cranial anatomy(including the “banana” and “lemon” signs), with closedspina bifida (7% of their population) cranial signs donot develop. They conclude that the “the differentiationbetween open and closed spina bifida is best shown bythe sonographic demonstration of abnormal or normalcranial anatomy.”
To accurately identify the type and extent of the lesionsagittal, coronal and axial spinal views are all required(Figure 5). The bony defect is identified by splaying ofthe posterior lamina ossification centers in the coronaland axial plane (Figure 6). The bony defect may lie ator cranial to, the level at which there is protrusion of themeninges (meningocele) or meninges plus neural tissue(myelomeningocele).
All lesions arise from a dysraphism (defect of closure)and are classified as open or closed depending on
Copyright Ó 2009 John Wiley & Sons, Ltd. Prenat Diagn 2009; 29: 402–411.DOI: 10.1002/pd

İniensefali Kompleks ve lethal bir malformasyon
3 temel özelliği var;
Foramen magnumu tutan oksiput defekt
Spinada retroflaksiyon
Açık spina bifida

Spinadaki kemik defekti
Primer nörolasyon kusurlu
İnsidansı 0.5-1/1000 gebelik
Tipleri
Açık %85 – 90 (miyelosel/miyelomeningosel)
Kapalı %10 – 15
%80’ni lumbar, torakolumbar veya lumbosakral
Prenatal sonografinin sensitivitesi %97-98; spesifitesi %100
Spina Bifida

İntrakranyal bulgular;
Mikrosefali
Limon belirtisi
Muz belirtisi
Ventrikülomegali
Chiari II malformasyonu

Spinal bulgular;
Dorsal vertebral yapılarda
genişleme
Meningosel kesesi
Miyelomeningosel kesesi
Kifoskolyoz

İlk Trimesterde Tanı İntracranial Translucency

BS/BSOB Oranı <1 BS/BSOB Oranı >1