Embed Size (px)
Citation preview

tnstt(oaf
HBPBGarv
Pd
4
0d
Nomograms for Aortic Root Diameters in Children UsingTwo-Dimensional Echocardiography
Mathieu Gautier, MDa,b, Delphine Detaint, MDa,b, Christophe Fermanian, PhDc,Philippe Aegerter, MDc, Gabriel Delorme, MDa, Florence Arnoult, MDa,d, Olivier Milleron, MDa,
François Raoux, MDa, Chantal Stheneur, MDa, Catherine Boileau, PhDa,e, Alec Vahanian, MDb, andGuillaume Jondeau, MD, PhDa,b,f,*
The evaluation of aortic root dilation is of major importance for the diagnosis andfollow-up of patients with diverse diseases, including the Marfan syndrome. However, wenoted that the available nomograms suggested a lower aortic root dilation rate in adults(75%) than in children (90%), when the opposite would have been expected. To establishnew nomograms, we selected a population of 353 normal children. We took transthoracicechocardiographic measurements of the aortic root diameters at the level of the aorticannulus, sinuses of Valsalva, sinotubular junction, and ascending aorta according to theAmerican Society of Echocardiography recommendations. All diameters correlated wellwith the height, weight, body surface area, and age (r � 0.75 to 0.84, p <0.0001).Covariance analysis adjusting for body surface area showed slightly larger diameters at thelevel of the sinuses of Valsalva in male children than in female children (�1 mm, p �0.0002). Equations and derived nomograms were developed, giving the upper limit ofnormal (allowing simple recognition of aortic dilation) and the Z score (allowing finequantification of dilation and differentiation of normal growth from pathologic dilation) forall 4 aortic root diameters (ie, aortic annulus, sinuses of Valsalva, sinotubular junction, andproximal ascending aorta) according to body surface area and gender. We applied thenomograms to 282 children with confirmed Marfan syndrome, of whom 65.2% pre-sented with dilation of the sinuses of Valsalva. In conclusion, we propose equations tocalculate the upper limit of normal and Z-score for aortic root diameters measured by2-dimensional echocardiography, which should be useful tools for the diagnosis andfollow-up of aortic root aneurysms in children. © 2010 Elsevier Inc. All rights
reserved. (Am J Cardiol 2010;105:888 – 894)ppmescpppVn
M
owadt
TbMp
In our Marfan syndrome (MS) and related diseases mul-idisciplinary outpatient clinic, we have used recommendedomograms for aortic root diameters assessed by 2-dimen-ional echocardiography.1–3 We noted that aortic root dila-ion was overdiagnosed in children, because its incidence athe level of the sinuses of Valsalva was lower in adults75%) than in children �18 years old (90%), when thepposite would have been expected.4,5 This observation haslso been made by others.6 The recommended nomogramsor aortic root diameters in children were derived from a
aCentre de Référence pour le Syndrome de Marfan et Apparentés,ôpital Bichat, AP-HP, Paris, France; bService de Cardiologie, Hôpitalichat, AP-HP, Paris, France; cUnité de Biostatistiques, Hôpital Ambroisearé, Boulogne, France; dService d’Explorations Fonctionnelles, Hôpitalichat, AP-HP, Paris, France; eService de Biochimie, Hormonologie eténétique Moléculaire, Hôpital Ambroise Paré, AP-HP, Boulogne France;
nd fINSERM U698, Hôpital Bichat, AP-HP, Paris, France. Manuscripteceived August 14, 2009; revised manuscript received and accepted No-ember 6, 2009.
This study was supported by the French Ministry of Health (PHRC)aris, France, and Société Française de Cardiologie et Fédération Françaisee Cardiologie, Paris, France.
*Corresponding author: Tel: (�33) 0-1-4025-6811; fax: (�33) 0-1-025-6732.
aE-mail address: [email protected] (G. Jondeau).
002-9149/10/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2009.11.040
ediatric population of 52 children referred for innocentrecordial murmur.1–3 We sought (1) to establish new no-ograms using a large population of healthy children, for
ach of the 4 diameters of the aortic root (eg, aortic annulus,inuses of Valsalva, sinotubular junction, and proximal as-ending aorta) measured by 2-dimensional echocardiogra-hy according to the American Society of Echocardiogra-hy (ASE) recommendations;3 and (2) to determine therevalence of aortic dilation at the level of the sinuses ofalsalva in children with MS, as assessed using these newomograms.
ethods
All children included in the present study had come tour outpatient clinic devoted to MS from 1995 to 2009 andere �18 years old at their first examination. All patients
nd/or their guardians provided informed consent. Two in-ependent groups of children were retrospectively consti-uted for the purposes of the present study.
The first group was used to determine the normative data.he main reason for consultation was familial screeningecause one first-degree relative had been diagnosed withS. Our rule was to ask all first-degree relatives of affected
robands to come for MS screening with a complete clinical
nd paraclinical evaluation (including genetic, ophthalmo-www.AJConline.org

loowraos
A1wicsgd
tqEqwpwacqvdlusVwt(rmw(Tl
D
Fd(v
Fod
889Miscellaneous/Normal Aortic Diameters in Children
ogic, cutaneous, orthopedic, and cardiologic examinations)n the same day. Only children in whom no anomaly wasbserved were included in the present study. All children forhom MS was either confirmed or could not be completely
uled out were excluded, as were patients with a bicuspidortic valve, a history of familial thoracic aortic aneurysm,r significant aortic regurgitation (defined as moderate orevere).
The second group was a population of children with MS.ll patients who came to our clinic for consultation from995 and 2009 and were �18 years old at the examinationith a MS diagnosis fulfilling the international criteria were
ncluded in the second group.2 Only data from the firstonsultation was kept for each patient when they cameeveral times. This population was used to test our nomo-rams and to determine the proportion of dilated aortic root
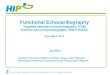
igure 1. Four aortic root diameters measured in 2-dimensional echocar-iography: aortic annulus (1), sinuses of Valsalva (2), sinotubular junction3), and ascending aorta (4). Ao � aorta; LA � left atrium; LV � leftentricle.
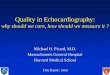
igure 2. Off-line 2-dimensional echocardiographic measurement at levelf sinuses of Valsalva, sinotubular junction, and ascending aorta in lateiastole (magnified view of aortic root, parasternal long axis).
iameters in children with MS. D
Transthoracic echocardiography was performed by 1 of 5rained echocardiographists (all cardiologists) using a Se-uoia (Siemens Saint-Denis, France) or a Vivid 7 (Generallectric, France) ultrasound system. Adequate multifre-uency transducers, ranging from 2 to 5 and 3 to 8 MHz,ere used. Patients were placed in the left lateral decubitusosition, in at rest conditions. The aortic root diametersere measured in 2-dimensional mode at 4 levels (ie, aortic
nnulus, sinuses of Valsalva, sinotubular junction, and as-ending aorta), according to the latest 2005 ASE chamberuantification guidelines.3 The best parasternal long-axisiew was used. Great care was taken to align the echocar-iographic plane with the aortic root and to obtain theargest aortic diameters. Appropriately magnified views weresed for greater precision. The aortic annulus was measured inystole at the hinge point of the aortic leaflets. The sinuses ofalsalva, sinotubular junction, and proximal ascending aortaere all measured in diastole, perpendicular to the long axis of
he aorta, using the leading edge to leading edge techniqueFigures 1 and 2). Thus, our measurements included the ante-ior wall of the aorta and not the posterior wall. The measure-ents were done the day of the consultation by the cardiologistho did the ultrasound examination, both on-line and off-line
digitized images). The diameters were given in millimeters.he largest of several measurements at each of the 4 predefined
evels was kept in the database.The quantitative data are reported as the mean � SD.
ifferences in proportions were tested using the chi-square test.The body surface area (BSA) was computed using the
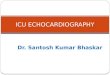
Figure 3. Number of cases per age interval (years of age).
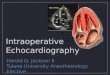
Figure 4. Number of cases per BSA interval (m2).
ubois and Dubois formula7: BSA (m2) � 0.007184 �

h(m
ad4o
rBnatlar(oaarv
nbfmwndl2nlS
atbddbmi�
aise
R
ofBg0pTittt3TeBsmo
Foc
TM
V
SAHWBBASSA 22.4
890 The American Journal of Cardiology (www.AJConline.org)
eight (cm)0.725 � weight (kg).0.425 The body mass indexBMI) was determined using the Quetelet index: BMI (kg/
2) � weight (kg)/height (m2).The gender differences for morphologic parameters, age,
nd aortic root diameters were evaluated using the indepen-ent samples t test. The influence of gender on each of theaortic root diameters was further assessed using analysis
f covariance to adjust for BSA.For homogeneity of variance, the values of all 4 aortic
oot diameters, morphologic parameters (height, weight,SA, body mass index), and age were transformed to theiratural logarithm. Linear regression statistics were thenpplied to determine the correlations among the logarithmicransformed values of the 4 aortic root diameters, morpho-ogic parameters (height, weight, BSA and its square root,nd body mass index), and age. The strength of each cor-elation was evaluated by Pearson’s correlation coefficientr). The relation among the logarithmic transformed valuesf the 4 aortic root diameters, morphologic parameters, andge was described using equations of the form: ln(y) �.ln(x) � b, with “y” the mean predicted diameter, “a” theegression line multiplier, “x” the morphologic parameteralue, and “b” the regression line intercept.
A first set of nomograms displaying the upper limit oformal for the aortic annulus, sinuses of Valsalva, sinotu-ular junction, and proximal ascending aorta was derivedrom linear regression analysis of the transformed logarith-ic values. The morphologic parameter that correlated bestith the aortic diameters was chosen. The upper limit oformal was defined as 2 SDs greater than the mean pre-icted diameter. The form of the equation giving the upperimit of normal was therefore: ln(ULN) � a.ln(x) � b �SD, ULN � e(b � 2SD).(x)a, with ULN, the upper limit oformal, “a” the regression line multiplier, “x” the morpho-ogic parameter value, “b” the regression line intercept, andD, the standard deviation.
Second, the Z-score equations were established for all 4ortic root diameters using linear regression analysis of theransformed logarithmic values, with Z defined as the num-er of SDs greater than or less than the predicted meaniameter: Z � [ln(measured diameter) �ln(predicted meaniameter)]/(SD), Z � [ln(measured diameter) � (a.ln(x) �)]/(SD), with “a” the regression line multiplier, “x” theorphologic parameter value, and “b” the regression line
ntercept. Of the normal subjects, 95.4% had a Z score of
able 1ean values � SD of morphologic parameters, age, and 4 aortic root dia
ariable Total Population
ubjects (n) 353ge (years) 12.7 � 4.5eight (cm) 156.7 (�25.4)eight (kg) 45.5 (�18.4)
ody mass index (kg/m2) 17.6 (�3.2)ody surface area (m2) 1.41 (�0.4)ortic annulus (mm) 18.5 (�3.2)inuses of Valsalva (mm) 25.9 (�4.6)inotubular junction (mm) 21.5 (�3.7)scending aorta (mm) 21.6 (�3.8)
2% to �2% and 2.3% a Z score of �2. Therefore, an o
ortic diameter can be considered dilated when the Z scores �2, with a specificity of 97.7%. Nomograms giving the Zcore for the 4 aortic root diameters were derived from thesequations.
esults
Our first group included 353 children, aged 2 to 18 yearsld. The male/female ratio was 1.2 (194 male and 159emale children). As shown in Figures 3 and 4, all age andSA intervals were well represented, except for the ageroup of 2 to 3 years old (n � 10) and BSA group of 0.5 to.69 m2 (n � 3). The mean value � SD of the morphologicarameters, age, and the 4 aortic root diameters are listed inable 1. The mean values of age, height, weight, body mass
ndex, and BSA were significantly lower in female childrenhan in the male children (p �0.0001). The mean values ofhe 4 aortic root diameters were greater in the male childrenhan in the female children (p �0.0001). The difference was.1 mm (p �0.0001) at the level of the sinuses of Valsalva.he analysis of covariance indicated that the gender differ-nce remained statistically significant after adjusting for theSA at the level of aortic annulus and the level of the
inuses of Valsalva. The male children had larger adjustedean values than the female children: 0.6 mm at the level
f the aortic annulus (p � 0.004) and 1 mm at the level
igure 5. Upper limit of normal for aortic root diameter at level of sinusesf Valsalva according to BSA. Dotted line indicates limit for femalehildren; solid line, limit for male children. ULN � upper limit of normal.
in normative population
Children Female Children p Value (t Test)
(54.9%) 159 (45.1%)� 4.3 11.7 � 4.4 �0.0001(�25.7) 148.9 (�22.9) �0.0001(�18.7) 40.2 (�16.6) �0.0001(�3) 17.2 (�3.3) 0.016(�0.4) 1.29 (�0.36) �0.0001(�3.2) 17.4 (�2.9) �0.0001(�4.7) 24.2 (�3.8) �0.0001(�3.8) 20.4 (�3.2) �0.0001(�3.8) 20.6 (�3.5) �0.0001
meters
Male
19413.5
163.149.917.91.5119.427.322.4
f the sinuses of Valsalva (p � 0.0002). In contrast, the

asi
asidwobf
tv
aVauwBai
F2 sinotu
TEc
A
A
S
S
P
f norma
891Miscellaneous/Normal Aortic Diameters in Children
djusted mean of the aortic diameter at the level of theinotubular junction and ascending aorta was not signif-cantly different.
Strong correlations were observed between each of the 4ortic root diameters and age, height, weight, BSA, BSAquare root (r � 0.76 to r � 0.85). All were highly signif-cant (p �0.0001). The BMI correlated poorly with alliameters (r � 0.49 to r � 0.54). When all the variablesere log transformed, slightly stronger correlations werebtained. The greatest correlation coefficients were foundetween the log-transformed aortic diameters and log-trans-
igure 6. Nomograms giving Z score (y axis) as function of aortic diametto 18 years. Ao an � aortic annulus; Asc ao � ascending aorta; STJ �
able 2quations for upper limit of normal and Z score for 4 aortic root diametehildren as function of body surface area (BSA)
ortic Root Level Gender
ortic annulus Male yFemale y
inuses of Valsalva Male yFemale y
inotubular junction Male yFemale y
roximal ascending aorta Male yFemale y
d � measured diameter; ln � natural logarithm; ULN � upper limit o
ormed values of BSA (r � 0.81 to r � 0.85). After dividing e
he population between the male and female children, the ralues were not significantly modified.
Nomograms displaying the upper limit of normal for theortic diameter (in millimeters) at the level of the sinuses ofalsalva as a function of BSA (square meters) in the male
nd female children are presented in Figure 5. The equationssed to build these nomograms are listed in Table 2, alongith those giving the upper limit of normal as a function ofSA and gender for the aortic diameters at the level of theortic annulus, sinotubular junction, and proximal ascend-ng aorta. These nomograms have been designed to allow
ved lines, with diameter printed) and BSA (x axis) in male children agedbular junction; SV � sinuses of Valsalva.
ured using 2-dimensional echocardiography for male and female
Equation Z Score Equations
x (BSA)0.47 Z � [ln(d) � 2.78–0.47 � ln(BSA)]/0.1x (BSA)0.44 Z � [ln(d) � 2.75–0.44 � ln(BSA)]/0.1x (BSA)0.49 Z � [ln(d) � 3.1–0.49 � ln(BSA)]/0.1x (BSA)0.44 Z � [ln(d) � 3.1–0.44 � ln(BSA)]/0.09x (BSA)0.47 Z � [ln(d) � 2.9–0.47 � ln(BSA)]/0.1x (BSA)0.42 Z � [ln(d) � 2.9–0.42 � ln(BSA)]/0.09x (BSA)0.46 Z � [ln(d) � 2.9–0.46 � ln(BSA)]/0.11x (BSA)0.46 Z � [ln(d) � 2.9–0.46 � ln(BSA)]/0.1
l.
er (cur
rs meas
ULN
� 19.57� 19.11� 26.95� 26.36� 22.29� 21.76� 22.74� 22.20
asy recognition of aortic dilation in children.

ftbie
aFa2tmf
prTadwV
F2
Fcls
TMa
A
ASSA
892 The American Journal of Cardiology (www.AJConline.org)
The nomograms allowing determination of the Z scoreor the aortic diameters as a function of gender and BSA athe level of the aortic annulus, sinuses of Valsalva, sinotu-ular junction, and proximal ascending aorta are displayedn Figures 6 (male children) and 7 (female children). An
igure 7. Nomograms giving Z score (y axis) as function of aortic diameteto 18 years. Abbreviations as in Figure 6.
igure 8. Example showing how to use Z score nomograms. For a malehild with a BSA of 1.45 m2 (A), a measured diameter of 30 mm (B) atevel of sinuses of Valsalva gives a Z score of 1.3 (C). In this case, theinuses of Valsalva were not dilated (Z score �2).
xample illustrating how the Z score of a given measure for t
given BSA can be read from these nomograms is shown inigure 8. The Z score at all 4 levels can also be more easilynd accurately calculated using the equations listed in Table. As an example, if the measured diameter at the level ofhe sinuses of Valsalva in a male child with a BSA of 1.45
2 is 30 mm, the corresponding Z score can be computed asollows: Z � [ln(30) � 3.1 – 0.49 � ln(1.45)]/0.1 � 1.2.
The second population (children with MS) included 282atients (155 male and 127 female children; male/femaleatio 1.2). The mean age was 9.7 � 4.7 years (range 0 to 18).he mean BSA was 1.24 � 0.45 m2. The mean Z-score � SDt the 4 predefined levels and the percentage of patients withilated aortic segments are listed in Table 3. The aortic rootas most frequently dilated at the level of the sinuses ofalsalva, with 65.2% of patients having a Z score of �2. Of
ed lines, with diameter printed) and BSA (x axis) in female children aged
able 3ean � SD Z score and proportion of dilated cases (Z score �2) at 4
ortic root levels in children with Marfan syndrome (MS)
ortic Root Level Mean Z Score Patients With Z Score �2 (n)
ortic annulus 1.3 � 1.3 80 (28.4%)inuses of Valsalva 2.6 � 1.5 184 (65.2%)inotubular junction 1.8 � 1.4 113 (40.1%)scending aorta 1.1 � 1.2 55 (19.5%)
r (curv
he children with MS and nondilated sinuses of Valsalva (Z

ssdascs
D
awlavaacndf
clthcallpt
mAaptwdfsaoaidmstttmdtidsdo
adct
unnpan
gaaFwpslmcp
mssfiaFcagTsarteo
Mdtlt
acfMdsiaZ
893Miscellaneous/Normal Aortic Diameters in Children
core �2), 20.2% had at least one other diameter with a Zcore of �2 (5% had a dilated aortic annulus, 15.1% had ailated sinotubular junction, and 5% had a dilated proximalscending aorta). Among those with dilated sinuses of Val-alva, the Z score for the ascending aorta was �2 in 26% ofases. This proportion increased �77.1% for those with a Zcore of �3 at the level of the sinuses of Valsalva.
iscussion
We have proposed a new tool for both the recognition ofortic root dilation and the quantification of its evolutionith time in children aged �18 years. It can be used at the
evel of the aortic annulus, the sinuses of Valsalva (usuallyffected in MS),2 the sinotubular junction (critical for aorticalve continence),8 and 1 cm above at the level of thescending aorta (often dilated in association with bicuspidortic valves).9,10 Nomograms for these diameters areritical for diagnostic purposes, for the differentiation oformal growth from pathologic aortic dilation, and forecision making, including determining the optimal timeor surgery.11
The population we selected for our normative data in-luded the unaffected relatives of patients with MS or re-ated disorders, who were not complaining of any symp-oms, and were consulting because of familial screening. Allad undergone a complete multidisciplinary evaluation, in-luding genetic, ophthalmologic, cutaneous, orthopedic,nd cardiologic examinations. All pathologic findingseading to aortic root dilation (ie, MS and related patho-ogic disorders, familial thoracic aortic aneurysms, bicus-id aortic valve, significant aortic regurgitation) had beenhoroughly excluded.
The echocardiographic measurements were taken usingodern technology and the latest chamber quantificationSE recommendations.3 Apart from the study by Roman et
l,1 other nomograms published to date have either pro-osed normal values of 2-dimensional measurements ob-ained in systole12–15 or used the M-mode measurement,hich has greater variability and might miss the largeriameter.6,16–19 As have several investigators, we haveound it crucial that the echocardiographic measurements betandardized.20 This was one of the main reason we chose topply the ASE recommendations,3 which were not thor-ughly followed in previous studies.6,12–19 The theoreticaldvantage of measuring the aortic diameters during diastoles that, because the aortic pressure is more stable duringiastole than during systole, the aortic diameters should beore stable, thereby improving the reproducibility. During
ystole, the acute increase in aortic pressure leads to aransient increase of the aortic diameter of �10%; thus, theiming of the measurement is critical. In addition, the foot ofhe QRS allows a simple and precise timing for measure-ents made during diastole. In patients with MS, aortic
istensibility is decreased, indicating that the aortic diame-er is closer to the systolic diameter in those with MS thann healthy subjects.21,22 This could artificially decrease theifference between normal subjects and those with MS inystole and therefore decrease the ability to differentiate theilated aorta of a patient with MS from the nondilated aorta
f a normal subject, although this phenomenon is of limitedmplitude. The choice between using the inner to inneriameter or the leading edge to leading edge diameter is lessritical.3 We decided to follow what has been chosen his-orically.1
Our nomograms were determined in a large normal pop-lation. We used the data from 353 children to calculate theormative data and determine the nomograms. The onlyormative data from a larger population than ours wasublished by Pettersen et al.15 In their study, however, theortic root diameters were measured in systole, and they didot give the normal values for the proximal ascending aorta.
We were able to demonstrate a small, but significant,ender difference in the normal aortic root diameters (aorticnnulus and sinuses of Valsalva), adjusted to the BSA. Suchgender difference has been suggested in adults by the
ramingham Heart Study, which included 3,249 adults,23 asell as in MS patients24 and healthy adults.25,26 Only oneublication has reported gender differences in the 2-dimen-ional echocardiographic measurements of the aortic annu-us, in a population of 748 healthy children.27 Other studiesight have failed to show gender-related differences be-
ause of lack of power owing to the small size of theopulation1,13,14 or failed to investigate such a difference.15
We have proposed 2 different presentations of our nor-ative data for the aortic annulus, sinuses of Valsalva,
inotubular junction, and proximal ascending aorta. A firstet of equations provided the upper limit of normal (ninety-fth percentile) according to the BSA and gender (Figure 5nd Table 2). They allow easy recognition of aortic dilation.or more advanced use, we have provided equations andorresponding nomograms that give the Z score of a givenortic root diameter measurement according to the patient’sender and BSA at the examination (Figures 6 and 7 andable 2). The Z score allows for the comparison of mea-urements for a given patient at different periods, making itperfect tool for follow-up of normal aortic growth (Z score
emains constant) versus dilation (Z score increases). It is,herefore, particularly useful in children. Now that comput-rs can include sophisticated calculations easily, this modef presentation should become the standard.14,15,20,27
Using our nomogram, 65.2% of the children with provenS according to international criteria presented with aortic
ilation at the level of the sinuses of Valsalva, confirminghe greater sensibility of aortic measurements made at theevel of the sinuses of Valsalva for diagnostic purposes inhis population.
Our normative data for the 4 aortic root levels (ie, aorticnnulus, sinuses of Valsalva, sinotubular junction, and as-ending aorta) in children should be useful for diagnosis andollow-up of various aneurismal pathologic disorders (eg,
arfan syndrome, bicuspid aortic valve, connective tissueisorders). Our nomograms meet all the criteria required fortandardization of echocardiographic aortic measurementsn children, including correlation to BSA, measurementsccording to the ASE recommendations, and the use of thescore.3,20
1. Roman MJ, Devereux RB, Kramer-Fox R, O’Loughlin J. Two-dimen-sional echocardiographic aortic root dimensions in normal children
and adults. Am J Cardiol 1989;64:507–512.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
894 The American Journal of Cardiology (www.AJConline.org)
2. De Paepe A, Devereux RB, Dietz HC, Hennekam RC, Pyeritz RE.Revised diagnostic criteria for the Marfan syndrome. Am J Med Genet1996;62:417–426.
3. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pel-likka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, SolomonSD, Spencer KT, Sutton MS, Stewart WJ; Chamber QuantificationWriting Group; American Society of Echocardiography’s Guidelinesand Standards Committee; European Association of Echocardiogra-phy. Recommendations for chamber quantification: a report from theAmerican Society of Echocardiography’s Guidelines and StandardsCommittee and the Chamber Quantification Writing Group, developedin conjunction with the European Association of Echocardiography, abranch of the European Society of Cardiology. J Am Soc Echocardiogr2005;18:1440–1463.
4. Aburawi EH, O’Sullivan J. Relation of aortic root dilatation and age inMarfan’s syndrome. Eur Heart J 2007;28:376–379.
5. Faivre L, Masurel-Paulet A, Collod-Béroud G, Callewaert BL, ChildAH, Stheneur C, Binquet C, Gautier E, Chevallier B, Huet F, LoeysBL, Arbustini E, Mayer K, Arslan-Kirchner M, Kiotsekoglou A,Comeglio P, Grasso M, Halliday DJ, Béroud C, Bonithon-Kopp C,Claustres M, Robinson PN, Adès L, De Backer J, Coucke P, FranckeU, De Paepe A, Boileau C, Jondeau G. Clinical and molecular study of320 children with Marfan syndrome and related type I fibrillinopathiesin a series of 1009 probands with pathogenic FBN1 mutations. Pedi-atrics 2009;123:391–398.
6. Rozendaal L, Groenink M, Naeff MS, Hennekam RC, Hart AA, vander Wall EE, Mulder BJ. Marfan syndrome in children and adoles-cents: an adjusted nomogram for screening aortic root dilatation. Heart1998;79:69–72.
7. Dubois D, Dubois EF. A formula to estimate the approximate surfacearea if height and weight be known. Arch Intern Med 1916;17:863–871.
8. Maselli D, De Paulis R, Scaffa R, Weltert L, Bellisario A, Salica A,Ricci A. Sinotubular junction size affects aortic root geometry andaortic valve function in the aortic valve reimplantation procedure: anin vitro study using the Valsalva graft. Ann Thorac Surg 2007;84:1214–1218.
9. Hahn RT, Roman MJ, Mogtader AH, Devereux RB. Association ofaortic dilation with regurgitant, stenotic and functionally normal bi-cuspid aortic valves. J Am Coll Cardiol 1992;19:283–288.
0. Gurvitz M, Chang RK, Drant S, Allada V. Frequency of aortic rootdilation in children with a bicuspid aortic valve. Am J Cardiol 2004;94:1337–1340.
1. Roman MJ, Rosen SE, Kramer-Fox R, Devereux RB. Prognosticsignificance of the pattern of aortic root dilation in the Marfan syn-drome. J Am Coll Cardiol 1993;22:1470–1476.
2. Nidorf SM, Picard MH, Triulzi MO, Thomas JD, Newell J, King ME,Weyman AE. New perspectives in the assessment of cardiac chamberdimensions during development and adulthood. J Am Coll Cardiol1992;19:983–988.
3. Sheil ML, Jenkins O, Sholler GF. Echocardiographic assessment of
aortic root dimensions in normal children based on measurement of anew ratio of aortic size independent of growth. Am J Cardiol1995;75:711–715.
4. Daubeney PE, Blackstone EH, Weintraub RG, Slavik Z, Scanlon J,Webber SA. Relationship of the dimension of cardiac structures tobody size: an echocardiographic study in normal infants and children.Cardiol Young 1999;9:402–410.
5. Pettersen MD, Du W, Skeens ME, Humes RA. Regression equationsfor calculation of Z-scores of cardiac structures in a large cohort ofinfants, children and adolescents: an echocardiographic study. J AmSoc Echocardiogr 2008;21:922–934.
6. Gutgesell HP, Rembold CM. Growth of the human heart relative tobody surface area. Am J Cardiol 1990;65:662–668.
7. Kampmann C, Wiethoff CM, Wenzel A, Stolz G, Betancor M, Wip-permann CF, Huth RG, Habermehl P, Knuf M, Emschermann T,Stopfkuchen H. Normal values of M mode echocardiographic mea-surements of more than 2000 healthy infants and children in centralEurope. Heart 2000;83:667–672.
8. Poutanen T, Tikanoja T, Sairanen H, Jokinen E. Normal aortic dimen-sions and flow in 168 children and young adults. Clin Physiol FunctImaging 2003;23:224–229.
9. Kervancioglu P, Kervancioglu M, Tuncer CM. Echocardiographicstudy of aortic root diameter in healthy children. Saudi Med J 2006;27:27–30.
0. Kaski JP, Daubeney PE. Normalization of echocardiographically de-rived paediatric cardiac dimensions to body surface area: time for astandardized approach. Eur J Echocardiogr 2009;10:44–45.
1. Adams JN, Brooks M, Redpath TW, Smith FW, Dean J, Gray J,Walton S, Trent RJ. Aortic distensibility and stiffness index measuredby magnetic resonance imaging in patients with Marfan’s syndrome.Br Heart J 1995;73:265–269.
2. Nollen GJ, Groenink M, Tijssen JG, van der Wall EE, Mulder BJ.Aortic stiffness and diameter predict progressive aortic dilatation inpatients with Marfan syndrome. Eur Heart J 2004;25:1146–1152.
3. Vasan RS, Larson MG, Levy D. Determinants of echocardiographicaortic root size. The Framingham heart study. Circulation 1995;91:734–740.
4. Meijboom LJ, Timmermans J, Zwinderman AH, Engelfriet PM, Mul-der BJ. Aortic root growth in men and women with the Marfan’ssyndrome. Am J Cardiol 2005;96:1441–1444.
5. Lin FY, Devereux RB, Roman MJ, Meng J, Jow VM, Jacobs A,Weinsaft JW, Shaw LJ, Berman DS, Callister TQ, Min JK. Assess-ment of the thoracic aorta by multidetector computed tomography:age- and sex-specific reference values in adults without evident car-diovascular disease. J Cardiovasc Comput Tomogr 2008;2:298–308.
6. Wolak A, Gransar H, Thomson LE, Friedman JD, Hachamovitch R,Gutstein A, Shaw LJ, Polk D, Wong ND, Saouaf R, Hayes SW,Rozanski A, Slomka PJ, Germano G, Berman DS. Aortic size assess-ment by noncontrast cardiac computed tomography: normal limits byage, gender, and body surface area. JACC Cardiovasc Imaging 2008;1:200–209.
7. Zilberman MV, Khoury PR, Kimball RT. Two-dimensional echocar-diographic valve measurements in healthy children: gender specific
differences. Pediatr Cardiol 2005;26:356–360.