Embed Size (px)
Citation preview

Journal of the American College of Cardiology Vol. 62, No. 21, 2013� 2013 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2013.07.045
Cardiometabolic Risk
Non–High-Density Lipoprotein Cholesterol,Guideline Targets, and Population Percentilesfor Secondary Prevention in 1.3 Million Adults
The VLDL-2 Study (Very Large Database of Lipids)Mohamed B. Elshazly, MD,*y Seth S. Martin, MD,y Michael J. Blaha, MD, MPH,yParag H. Joshi, MD,y Peter P. Toth, MD, PHD,zx John W. McEvoy, MB BCH,yMohammed A. Al-Hijji, MD,y Krishnaji R. Kulkarni, PHD,k Peter O. Kwiterovich, MD,yRoger S. Blumenthal, MD,y Steven R. Jones, MDyCleveland, Ohio; Baltimore, Maryland; Sterling and Peoria, Illinois; and Birmingham, Alabama
From the *D
Ohio; yJohntimore, Mar
Sterling, Illi
kAtherotechinvestigators
did not pro
participate i
the investiga
Joshi are sup
supported b
a consultant
Ingelheim,
Objectives T
epartment of Cardiovas
s Hopkins Ciccarone Ce
yland; zDepartment of P
nois; xUniversity of IllinoDiagnostics Lab, Birm
with de-identified data
vide payments for the
n data analysis or influen
tors and did not receive a
ported by the Pollin Fello
y the Marie-Josée and He
for Atherotech Diagnost
Liposcience, and Merck;
his study sought to examine patient-level discordance between population percentiles of non–high-densitylipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C).
Background N
on–HDL-C is an alternative to LDL-C for risk stratification and lipid-lowering therapy. The justification for the presentguideline-based non–HDL-C cutpoints of 30 mg/dl higher than the LDL-C cutpoints remains largely untested.Methods W
e assigned population percentiles to non–HDL-C and Friedewald-estimated LDL-C values of 1,310,440 U.S. adultswith triglyceride levels <400 mg/dl who underwent lipid testing by vertical spin density gradient ultracentrifugation(Atherotech, Birmingham, Alabama) from 2009 to 2011.Results L
DL-C cutpoints of 70, 100, 130, 160, and 190 mg/dl were in the same population percentiles as non–HDL-C valuesof 93, 125, 157, 190, and 223 mg/dl, respectively. Non–HDL-C values reclassified a significant proportion ofpatients within or to a higher treatment category compared with Friedewald LDL-C values, especially at LDL-C levelsin the treatment range of high-risk patients and at triglyceride levels �150 mg/dl. Of patients with LDL-C levels <70mg/dl, 15% had a non–HDL-C level �100 mg/dl (guideline-based cutpoint) and 25% had a non–HDL-C level �93mg/dl (percentile-based cutpoint); if triglyceride levels were 150 to 199 mg/dl concurrently, these values were 22%and 50%, respectively.Conclusions T
here is significant patient-level discordance between non–HDL-C and LDL-C percentiles at lower LDL-C and highertriglyceride levels, which has implications for the treatment of high-risk patients. Current non–HDL-C cutpoints for high-risk patients may need to be lowered to match percentiles of LDL-C cutpoints. Relatively small absolute reductions innon–HDL-C cutpoints result in substantial reclassification of patients to higher treatment categories with potentialimplications for risk assessment and treatment. (The Very Large Database of Lipids [VLDL-2]; NCT01698489)(J Am Coll Cardiol 2013;62:1960–5) ª 2013 by the American College of Cardiology FoundationCardiovascular disease (CVD) is the leading cause of deathin the developed world, accounting for 33% of deaths in theUnited States and 47% of deaths in Europe (1,2). For the
cular Medicine, Cleveland Clinic, Cleveland,
nter for the Prevention of Heart Disease, Bal-
reventive Cardiology, CGH Medical Center,
is College of Medicine, Peoria, Illinois; and the
ingham, Alabama. Atherotech provided the
generated from commercial lipid analyses and
research or manuscript writing and did not
ce the conclusions. This study was initiated by
ny specific funding. Drs. Martin, McEvoy, and
wship in Preventive Cardiology. Dr. Martin is
nry R. Kravis endowed fellowship. Dr. Toth is
ics Lab, Amgen, Genzyme, Kowa, Boehringer
and is a member of the speaker’s bureau for
past 25 years, low-density lipoprotein cholesterol (LDL-C)has been the primary lipid parameter for risk stratificationand goal-directed therapy. However, an epidemic of obesity
AstraZeneca, Amarin, GlaxoSmithKline, Kowa, Merck & Co., and Genzyme. Dr.
Kulkarni is a research director at Atherotech Diagnostics Lab; owns uncashable
stocks for Atherotech Diagnostics Labs; and receives royalties from the University of
Alabama at Birmingham. Dr. Kwiterovich is a consultant for Merck & Co.; and has
received research grants from Amarin, GlaxoSmithKline, and Pfizer. Dr. Jones is
a member of the scientific advisory board and has received research grant support
from Atherotech Diagnostics; and has unexercised stock options for and is on the
scientific advisory board of LabRoots/BioConference Live. All other authors have
reported that they have no relationships relevant to the contents of this paper to
disclose.
Manuscript received April 24, 2013; revised manuscript received July 10, 2013,
accepted July 30, 2013.

Abbreviationsand Acronyms
CVD = cardiovascular
disease
HDL-C = high-density
lipoprotein cholesterol
LDL-C = low-density
lipoprotein cholesterol
VAP = vertical auto profile
VLDL = very-low-density
lipoprotein cholesterol
JACC Vol. 62, No. 21, 2013 Elshazly et al.November 19/26, 2013:1960–5 Non–HDL-C and LDL-C Percentile Discordance
1961
and metabolic syndrome has evolved over the past fewdecades, mostly due to changes in diet and lifestyle.Approximately 1 of 3 U.S. adults currently has metabolicsyndrome (1). As a result, we have witnessed an increasingprevalence of elevated triglyceride-rich remnant lipoproteins,characteristic of insulin resistance. These lipoproteinsinclude very-low-density lipoproteins (VLDL) and theirremnants, intermediate-density lipoproteins, and chylomi-cron remnant particles, whose contribution to atherogenicrisk is accounted for by non–HDL-C not LDL-C.
Current guidelines recommend using non–HDL-C as asecondary treatment target in patients with triglyceridelevels�200 mg/dl (3–5), setting non–HDL-C goals 30 mg/dlhigher than respective LDL-C goals. However, some reportshave suggested using non–HDL-C goals at the same pop-ulation percentiles as the respective LDL-C goals (6,7).
In this report, we examine patient-level discordancebetween non–HDL-C and LDL-C percentiles at differentLDL-C and triglyceride strata and implications for riskassessment and treatment.
Table 1Equivalent Population Percentiles of LDL-C and Non–HDL-C From the Very Large Database of Lipids Study
Population Percentile LDL-C (mg/dl) Non–HDL-C (mg/dl)
1st 37 60
5th 54 76
10th 63 86
15th 70* 93*
20th 77 100
25th 82 106
44th 100* 125*
50th 106 132
72nd 130* 157*
75th 134 161
90th 160* 190*
95th 177 209
97th 190* 223*
99th 215 251
*LDL-C cutpoints in worldwide guidelines.HDL-C ¼ high-density lipoprotein cholesterol; LDL-C ¼ low-density lipoprotein cholesterol.
Methods
Study population. We examined consecutive lipid profilesfrom 1,310,440 U.S. adults �18 years of age with triglyc-eride levels <400 mg/dl who underwent direct ultracen-trifugation of cholesterol by the vertical auto profile (VAP;Atherotech Diagnostics Lab, Birmingham, Alabama) from2009 to 2011 (8,9). “Consecutive” indicates that we onlyincluded the first available lipid profile for each patient.Consistent with routine clinical practice, LDL-C levelswere estimated using the Friedewald formula, thusexcluding patients with triglyceride levels �400 mg/dl(9,10).VAP lipid measurement. The VAP is an inverted ratezonal, single vertical spin, density-gradient ultracentrifuga-tion technique that directly measures cholesterol concen-trations of the 5 lipoprotein classes (LDL-C, VLDLcholesterol, intermediate-density lipoprotein cholesterol,HDL-C, and lipoprotein[a]) and their subclasses. Triglyc-eride levels were directly measured using the AbbottArchitect C8000 system (Abbott Park, Illinois) (8,9). Theaccuracy of VAP lipid parameters was cross-validated withreference standards as previously described (9).Data management. Raw individual patient data wereextracted at Atherotech, cleaned of duplicate samples, andthen de-identified and transferred to the senior investigator.The master database, the Very Large Database of Lipids(VLDL), is maintained at The Johns Hopkins Hospital(Baltimore, Maryland) and registered at clinicaltrials.gov(NCT01698489). The Johns Hopkins Institutional ReviewBoard declared the study exempt.Statistical analysis. Friedewald-estimated LDL-C levelswere calculated as [total cholesterol –HDL-C – triglycerides/5].Non–HDL-C levels were calculated as [total cholesterol –
HDL-C]. We assigned population percentiles to LDL-C and
non–HDL-C levels and thendetermined the percentiles corre-sponding to LDL-C cutpoints incurrent guidelines (70, 100, 130,160, and 190 mg/dl) (3–5).
Reclassification was defined aspresent when the non–HDL-Clevel reclassified a patient withinor to a higher (upward) or lower(downward) treatment categorycompared with the FriedewaldLDL-C level. The analysis was
performed using guideline-based non–HDL-C cutpoints,defined as 30 mg/dl higher than LDL-C cutpoints, andpercentile-based cutpoints, defined as those at equivalentpercentiles to LDL-C cutpoints. We focused on upwardreclassification because current guidelines recommend usingnon–HDL-C level only as a secondary treatment target afterthe LDL-C target is reached; thus, downward reclassifica-tion becomes irrelevant.Statistical analyses and logarithmically scaled pseudocolordensity plots were generated in R Version 2.15.1 (Vienna,Austria) and Stata Version 11.0 (College Station, Texas).
Results
Population characteristics. Patients were 59 � 15 yearsof age (mean � SD), 52% were women, and lipid parameterdistributions were nearly superimposable with recent lipiddata from the 2007 to 2008 National Health and NutritionExamination Survey (11), as previously described by ourgroup (9) (Online Fig. 1).Population percentiles. LDL-C cutpoints of 70, 100, 130,160, and 190 mg/dl were at the same population percentilesas non–HDL-C values of 93, 125, 157, 190, and 223 mg/dl,respectively (Table 1).

Elshazly et al. JACC Vol. 62, No. 21, 2013Non–HDL-C and LDL-C Percentile Discordance November 19/26, 2013:1960–5
1962
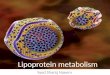
Non–HDL-C and LDL-C percentile discordance. Wevisually assesseddiscordance betweenLDL-Candnon–HDL-C percentiles and found greater discordance at lower LDL-Cand higher triglyceride levels (Fig. 1). Similarly, the absolutedifference between non–HDL-C and LDL-C percentiles wasmore pronounced with greater in-group variation at lowerLDL-C and higher triglyceride levels (Online Fig. 2).Reclassification of treatment category by non–HDL-Clevel. When using conventional non–HDL-C cutpoints,non–HDL-C levels reclassified 10.5% (n ¼ 137,744) of thestudygroupupward and22.3%(n¼ 291,499) downward.Usingpercentile-based cutpoints, 14.2% (n ¼ 186,106) were reclas-sified upward and 13.7% (n ¼ 178,860) downward (Fig. 2).
Upward reclassification occurred more frequently at lowerLDL-C and higher triglyceride levels (for additionaldiscussion, see Reclassification Analysis in the OnlineAppendix). Of patients with an LDL-C level <70 mg/dl,15% had a non–HDL-C level �100 mg/dl (the guideline-based cutpoint) and 25% had a non–HDL-C level�93 mg/dl (the percentile-based cutpoint); these values
Figure 1 Patient-Level Discordance Between Population Percentiles
(A) The total population and (B) 4 different triglyceride categories. The density of data is
patients per pixel, from light blue to purple.
were 22% and 50%, respectively, if triglyceride levels wereconcurrently 150 to 199 mg/dl (Fig. 3A). Similarly, ofpatients with LDL-C levels between 70 and 99 mg/dl,12% had a non–HDL-C level �130 mg/dl and 17% had anon–HDL-C level �125 mg/dl; these values were17% and 35%, respectively, if triglyceride levels wereconcurrently 150 to 199 mg/dl (Fig. 3B).
Discussion
Our study highlights the magnitude of patient-leveldiscordance between LDL-C and non–HDL-C percen-tiles. They are most discordant when accuracy is mostcrucial, at low LDL-C and high triglyceride levels. There-fore, conventional non–HDL-C cutpoints for high-riskpatients may need to be lowered to match percentiles ofLDL-C cutpoints.Non–HDL-C: a better marker for CVD risk assessment andtreatment. The National Cholesterol Education ProgramAdult Treatment Panel III guidelines state that “In most
of LDL-C and non–HDL-C
expressed by different shades of color, which represent increasing densities of

Figure 2Treatment Category Reclassification Using Guideline-Based Non–HDL-C Cutpoints Versus Percentile-Based Cutpointsfor the Total Population
Four triglyceride categories were analyzed and each assigned a color as depicted. N ¼ 1,310,440.
JACC Vol. 62, No. 21, 2013 Elshazly et al.November 19/26, 2013:1960–5 Non–HDL-C and LDL-C Percentile Discordance
1963
persons with triglycerides <200 mg/dl, adding VLDL-C toLDL-C would be expected to provide little additional powerto predict CVD” (3); this is a disputable statement given theincreasing prevalence of obesity, diabetes mellitus, andmetabolic syndrome. Non–HDL-C represents the aggre-gate cholesterol content of apolipoprotein B–containingatherogenic lipoproteins, including LDL, VLDL,intermediate-density lipoprotein, remnants, and lip-oprotein(a); in principle, this is a broader, more inclusivemeasure of atherogenic risk. Recent evidence suggests thatnon–HDL-C is superior for risk prediction and might bea more effective target for lipid-lowering therapy, particu-larly in high-risk patients (12–15). A meta-analysis of233,455 patients showed that non–HDL-C is a more potentmarker of CVD risk than LDL-C (16). Calculating thenumber of clinical events prevented by a high-risk treatmentregimen in those in the >70th percentile of the U.S. adultpopulation, Sniderman et al. (16) suggested that a non–HDL-C based strategy may prevent 300,000 more eventsthan an LDL-C strategy over a 10-year period.
In addition, measurement of the non–HDL-C level hasno additional cost or inconvenience because it is easilycalculated from the standard lipid profile without the need
for prior fasting. Moreover, the adoption of non–HDL-Cacross all levels of triglycerides would substantially simplifyimplementation of clinical guidelines.Potential implications for guideline development.Guideline-based non–HDL-C cutpoints are based on theassumption that a normal VLDL cholesterol level existswhen triglyceride levels are <150 mg/dl, which is <30 mg/dlas estimated by the Friedewald formula (3). More recentevidence suggests that a biologically optimal fasting triglyc-eride level is <100 mg/dl (17); thus, a normal VLDLcholesterol level is likely closer to 20 mg/dl, also suggestingthat non–HDL-C cutpoints should be 20 mg/dl higher thanLDL-C cutpoints.
Studying patients with acute coronary syndromes,Ballantyne et al. suggested that the current non–HDL-Cgoal should be lowered by 8 to 10 mg/dl to match LDL-C and apolipoprotein B treatment goals in the very-high-risk category (18). Other reports have recommendedlowering non–HDL-C cutpoints to match percentiles ofLDL-C cutpoints (6,7). In our study, the non–HDL-Cvalues with percentile equivalence to LDL-C cutpointsof 100 and 70 mg/dl were 125 and 93 mg/dl, respec-tively. Therefore, non–HDL-C cutpoints may need to

Figure 3Treatment Category Reclassification Using Guideline-Based Non–HDL-C Cutpoints Versus Percentile-Based Cutpoints atSecondary Prevention LDL-C Range
LDL-C levels: (A) <70 mg/dl and (B) 70 to 99 mg/dl.
Elshazly et al. JACC Vol. 62, No. 21, 2013Non–HDL-C and LDL-C Percentile Discordance November 19/26, 2013:1960–5
1964
be lowered by 5 mg/dl and 7 mg/dl for the high-risk andvery-high-risk categories, respectively. This leads tosubstantial upward reclassification of patients, particularlyat concurrent high triglyceride levels. For example, ofpatients with LDL-C levels <70 mg/dl and concurrenttriglyceride levels of 150 to 199 mg/dl, more than twiceas many patients were reclassified upward when the non–HDL-C cutpoint was lowered from 100 to 93 mg/dl(Fig. 3A).
Our study also showed that the triglyceride thres-hold in the current guidelines of �200 mg/dl for usingnon–HDL-C as a secondary treatment target may need to
be lowered given that considerable upward reclassificationoccurs also at triglyceride levels of 150 to 199 mg/dl (Fig. 2).Study limitations. We have limited clinical and demo-graphic data regarding the full risk factor profile of ourpopulation. Therefore, reclassification analyses are inferredon the basis of the lipid profile only and we cannot deter-mine its impact on clinical outcomes.
The nearly superimposable age, sex, and lipid distribu-tions between the samples from the VLDL study and theNational Health and Nutrition Examination Survey suggestthat our study comprises a reasonable population of patientsengaged in prevention and treatment of atherosclerosis, not

JACC Vol. 62, No. 21, 2013 Elshazly et al.November 19/26, 2013:1960–5 Non–HDL-C and LDL-C Percentile Discordance
1965
a special population that underwent VAP testing. We do notknow the percentage of patients who were taking a statin.Some samples in our study may have been acquired ina nonfasting state, but this is not uncommon in routinepractice.
Despite focusing on upward reclassification in accor-dance with current guidelines, there was considerabledownward reclassification in patients with triglyceridelevels <150 mg/dl (Fig. 2). The significance of downwardreclassification remains unclear in the literature andcurrent guidelines, and whether these patients should betreated to LDL-C versus non–HDL-C goal needs furtherscrutiny.
Conclusions
Our study of 1.3 million patients builds on prior evidencethat there is significant patient-level discordance betweenpercentiles of LDL-C and non–HDL-C, particularlywhen accuracy is most crucial, at lower LDL-C andhigher triglyceride levels. Therefore, lowering conventionalnon–HDL-C cutpoints for high-risk patients to matchpercentiles of LDL-C cutpoints as well as wider adoption ofnon–HDL-C in clinical practice may potentially improvesecondary prevention outcomes and residual risk assessmentand treatment.
Reprint requests and correspondence: Dr. Mohamed B. Elsha-zly, Department of Cardiovascular Medicine, Cleveland Clinic,9500 Euclid Avenue, J3-4, Cleveland, Ohio 44195. E-mail:[email protected].
REFERENCES
1. Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and strokestatisticsd2012 update: a report from the American Heart Association.Circulation 2012;125:e2–220.
2. Nichols M, Townsend N, Luengo-Fernandez R, et al. 2012 EuropeanCardiovascular Disease Statistics. European Heart Network, Brussels,European Society of Cardiology, Sophia Antipolis.
3. National Cholesterol Education Program (NCEP) Expert Panel onDetection, Evaluation, and Treatment of High Blood Cholesterol inAdults (Adult Treatment Panel III). Third Report of the NationalCholesterol Education Program (NCEP) Expert Panel on Detection,Evaluation, and Treatment of High Blood Cholesterol in Adults (AdultTreatment Panel III) final report. Circulation 2002;106:3143–421.
4. Genest J, McPherson R, Frohlich J, et al. 2009 Canadian Cardiovas-cular Society/Canadian guidelines for the diagnosis and treatment ofdyslipidemia and prevention of cardiovascular disease in theadultd2009 recommendations. Can J Cardiol 2009;25:567–79.
5. Developed with the special contribution of: European Association forCardiovascular Prevention & Rehabilitation, Authors/Task ForceMembers, Reiner Z, et al. ESC/EAS Guidelines for the managementof dyslipidaemias: the Task Force for the management of dyslipidae-mias of the European Society of Cardiology (ESC) and the EuropeanAtherosclerosis Society (EAS). Eur Heart J 2011;32:1769–818.
6. Contois JH, McConnell JP, Sethi AA, et al. Apolipoprotein B andcardiovascular disease risk: position statement from the AACC Lipo-proteins and Vascular Diseases Division Working Group on BestPractices. Clin Chem 2009;55:407–19.
7. Sniderman AD, De Graaf J, Couture P. Low-density lipoprotein-lowering strategies. Curr Opin Cardiol 2012;27:405–11.
8. Kulkarni KR. Cholesterol profile measurement by vertical auto profilemethod. Clin Lab Med 2006;26:787–802.
9. Martin SS, Blaha MJ, Elshazly MB, et al. Friedewald estimated versusdirectly measured low-density lipoprotein cholesterol and treatmentimplications. J Am Coll Cardiol 2013;62:732–9.
10. Friedewald WT, Levy RI, Fredrickson DS. Estimation of theconcentration of low-density lipoprotein cholesterol in plasma, withoutuse of the preparative ultracentrifuge. Clin Chem 1972;18:499–502.
11. Kuklina EV, Yoon PW, Keenan NL. Trends in high levels of low-density lipoprotein cholesterol in the United States, 1999-2006.JAMA 2009;302:2104–10.
12. Bittner V, Hardison R, Kelsey SF, et al. Non-high-density lipoproteincholesterol levels predict five-year outcome in the Bypass AngioplastyRevascularization Investigation (BARI). Circulation 2002;106:2537–42.
13. Cui Y, Blumenthal RS, Flaws JA, et al. Non-high-density lipoproteincholesterol level as a predictor of cardiovascular disease mortality. ArchIntern Med 2001;161:1413–9.
14. Varbo A, Benn M, Tybjærg-Hansen A, Jørgensen AB, Frikke-Schmidt R, Nordestgaard BG. Remnant cholesterol as a causal riskfactor for ischemic heart disease. J Am Coll Cardiol 2013;61:427–36.
15. Boekholdt SM, Arsenault BJ, Mora S, et al. Association of LDLcholesterol, non-HDL cholesterol, and apolipoprotein B levels withrisk of cardiovascular events among patients treated with statins:a meta-analysis. JAMA 2012;307:1302–9.
16. Sniderman AD,Williams K, Contois JH, et al. A meta-analysis of low-density lipoprotein cholesterol, non-high-density lipoprotein choles-terol, and apolipoprotein b as markers of cardiovascular risk. CircCardiovasc Qual Outcomes 2011;4:337–45.
17. Miller M, Stone NJ, Ballantyne C, et al. Triglycerides and cardiovas-cular disease: a scientific statement from the American Heart Associ-ation. Circulation 2011;123:2292–333.
18. Ballantyne CM, Pitt B, Loscalzo J, Cain VA, Raichlen JS. Alteration ofrelation of atherogenic lipoprotein cholesterol to apolipoprotein B byintensive statin therapy in patients with acute coronary syndrome (fromthe Limiting UNdertreatment of lipids in ACS With Rosuvastatin[LUNAR] Trial). Am J Cardiol 2013;111:506–9.
Key Words: discordance - LDL cholesterol - lipids - non–HDLcholesterol - percentiles - secondary prevention.
APPENDIX
For reclassification analysis information and supplemental figures, pleasesee the online version of this article.