Embed Size (px)
Citation preview

A Profile
Noncommunicable Diseasesin the Western Pacific Region
WHO Western Pacific RegionPUBLICATION
ISBN-13 978 92 9061 563 7


A Profile
Noncommunicable Diseasesin the Western Pacific Region

WHO Library Cataloguing in Publication Data
Noncommunicable diseases in the Western Pacific Region: a profile
1. Chronic diseases – prevention and control. 2. Data collection. 3. Registries.
I. World Health Organization Regional Office for the Western Pacific.
ISBN 978 92 9061 563 7 (NLM Classification: WT 500)
© World Health Organization 2012
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). For WHO Western Pacific Regional Publications, request for permission to reproduce should be addressed to the Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932, 1000, Manila, Philippines, (fax: +632 521 1036, e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile
Table of Contents
Preface 5
Summary 7
1. introduction 9
2. Burden of noncommunicable diseases 10
3. Risk factors for noncommunicable diseases 17
4. NCD country capacity 23
5. NCD country profiles 29
6. Key findings and recommendations 57
Annexes 59
Annex 1 - Regional Commitments on NCD 59
Annex 2 - Exploratory Notes on Country Estimates 63
Annex 3 - 2008 Comparable Estimates of NCD Mortality 68
Annex 4 - WHO STEPwise Surveillance for NCD Risk Factors 69

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile4
Acknowledgements
This profile was prepared with input from Dr Annette David, Dr Cherian Varghese, Dr Hai-Rim Shin, Ms Marie Clem Carlos, Dr Han Tieru, Ms Leanne Riley, Ms Regina Guthold, Ms Melanie Cowen, Dr Ashley Bloomfield, Ms Anjana Bhushan, Dr Manju Rani, and Professor Donald Matheson. It was reviewed by Professor Ruth Bonita and Dr Kyungwon Oh.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 5
Preface
Prevention and control of noncommunicable diseases (NCDs) are national, regional and global priorities. Despite progress, more needs to be done to address the burden and socioeconomic consequences of NCDs. Regional and global declarations in 2011 have reiterated the commitment of Member States to NCD prevention and control.
While efforts are ongoing to address the challenges of NCD prevention and control, a forceful response is required at the national and regional levels. Reliable and timely data are mandatory for the planning and evaluation of NCD programmes. However, setting up and maintaining surveillance systems can be difficult for low- and middle-income countries. Regardless, the NCD burden, in terms of mortality and risk factors, have to be kept under regular surveillance. Information on health system indicators and capacity are also critical for introducing and evaluating interventions. Policies in related domains such as trade, agriculture and marketing also need monitoring as they impact NCDs.
The political declaration of the United Nations High-level Meeting on Noncommunicable Diseases in September 2011 is a clear indication of the high level of commitment for NCD prevention and control worldwide. At the sixty-second session of the WHO Regional Committee for the Western Pacific, Member States discussed options for expanding and intensifying NCD prevention and control in the Region.
Given the huge burden and unacceptable rates of preventable premature morbidity and mortality from NCDs, we have to move towards time-bound targets with indicators and an accountability framework.
This regional profile, based on the WHO Global status report on noncommunicable diseases, will serve as a baseline for measuring the impact of our efforts in NCD prevention and control in the Western Pacific Region.
Let us continue to work together to prevent NCDs and promote health and development for all people of the Region.
Shin Young-soo, MD, Ph.D.Regional Director


NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 7
Summary
This profile of noncommunicable diseases (NCDs) in the Western Pacific Region is based largely on the WHo Global status report on noncommunicable diseases published in 2011. Country-specific data are classified by income category to reflect the variations among countries in the Region and to serve as a baseline for further monitoring.
Mortality from NCDs is higher in low- and middle-income countries (LMIC) than in high-income countries (HIC). The gap between the two income groups is even more pronounced for NCD deaths below the age of 70 years. Efforts are also needed to strengthen mortality registration and certification systems in LMIC.
Disease registries are not widely available in the Region, making it difficult to assess morbidity. National-level data on cancer burden are available from GLOBOCAN 2008, and are presented in terms of incidence and mortality. Variations in the rate of breast and uterine cervical cancer in women are also highlighted. Diabetes prevalence is more than 10% in almost all the Pacific island countries.
Prevalence of risk factors is a pointer to the burden of NCDs. The wide variation in tobacco prevalence in the Region indicates that there is potential to reduce tobacco use in many countries. Obesity and lack of physical activity are serious issues in most countries and indicate a need for the promotion of healthy diets and physical activity through multisectoral actions. Alcohol consumption also shows wide variation. Raised blood pressure and blood cholesterol levels are uniformly high in the region. Population trends help to estimate the future burden of NCDs.
National capacity for assessment of NCD prevention and control were undertaken by WHO in 2004 and 2010. NCD country profiles, which include mortality, risk factors, and capacity to prevent and control NCDs, are presented for all Member States in the Region. Periodic evaluation can help countries to scale up NCD prevention and control.
This regional profile presents a situational analysis and can serve as a baseline for Member States to move towards time-bound targets.


NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 9
1 Global status report on noncommunicable diseases. Geneva, WHO, 2011. Available online at http://www.who.int/chp/ncd_global_status_report/en/2 World Bank List of Economies. Washington, DC, The World Bank, 2011. Available online at http://siteresources.worldbank.org/DATASTATISTICS/Resources/CLASS.XLS
1. Introduction
Noncommunicable diseases (NCDs), principally cardiovascular diseases, cancer, diabetes and chronic respiratory diseases, impose a major and growing burden on health and development in the Western Pacific Region. NCDs are the leading causes of death and disability in the Region, responsible for 80% of all deaths in a region that is home to more than one quarter of the world’s population. Of particular concern is the high level of premature mortality from NCDs (deaths before 70 years of age) in several low- and middle-income countries (LMIC). There are indications that NCD-related morbidity and mortality will continue to rise if urgent measures are not taken.
The High-level Meeting of the General Assembly on the prevention and control of NCDs in September 2011 firmly placed NCD prevention and control as a global priority. Efforts are also ongoing at the regional and national levels to scale up NCD prevention and control. Regional commitments, particularly the Seoul Declaration and the Honiara Communiqué on the Pacific NCD Crisis (Annex 1), reflect the collective will to expand and intensify efforts for NCD prevention and control in the Region. One of the key ingredients for advancing the NCD agenda is to have an overview of the current NCD situation—mortality, morbidity, risk factors and country capacity.
The data and findings presented in the profile are mainly from the WHO Global status report on noncommunicable diseases released in 2011.1 The profile has four major sections: burden, risk factors, country capacity for NCD prevention and control, and NCD country profiles. All estimates were prepared by WHO, using multiple data sources and analytical methods (Annex 2).
The data are presented by country groupings—high-income countries (HIC) and low- and middle-income countries (LMIC)—as per the World Bank income categories as of July 2011.2 The NCD country profiles in Section 5, however, use the 2008 World Bank income categories.
There are many challenges in data collection and analysis in LMIC. Mortality registration is often weak, disease registries are suboptimal, and risk factor surveys are sporadic. National governments are responsible for leading and facilitating the collection of data and processing of information for action. Other groups such as academia and civil society are well positioned to support these efforts and use the data in innovative ways. The WHO STEPwise approach to surveillance of NCD risk factors (STEPS) has been adopted in some LMIC of the Region to measure trends, either as a stand alone format or incorporated into national health surveys.
WHO has been undertaking a major exercise in passive epidemiological surveillance, gathering published and unpublished data and information about key aspects of NCD globally. The findings in this profile are limited to the global comparisons. There is also a need to have better indicators to demonstrate the full information on the actual implementation of interventions.
This brief profile provides a baseline for measuring our efforts and encourages scaling up national surveillance frameworks for NCD prevention and control, especially in LMIC.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile10
High Income
Age
-sta
ndar
dize
d de
ath
rate
per
100
,000
Low- and middle-income
Japa
nAu
stra
liaSi
ngap
ore
New
Zeal
and
Brun
eiDa
russ
alam
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
aVi
et N
amSo
lom
on Is
land
s*Ph
ilippi
nes
Micr
ones
ia,
the
Fede
rate
d St
ates
of*
Vanu
atu*
Sam
oa*
Pala
u*
Niue
Kirib
ati
Papu
a Ne
w G
uine
a*La
o Pe
ople
’s
Dem
ocra
tic R
epub
lic, t
he*
Mon
golia
*
Fiji
Cam
bodi
a*
Tuva
luM
arsh
all I
sland
s, th
e*
Naur
u
Women
Men
1400
1200
1000
800
600
400
200
0
Repu
blic
ofKo
rea,
the
2. Burden of noncommunicable diseases
MORtALIty
In 2008, more than a quarter of the 36 million deaths from NCDs worldwide were from the Western Pacific Region. Globally, NCD deaths are projected to increase by 15% between 2010 and 2020 (to 44 million deaths), with the highest numbers predicted in the Western Pacific (12.3 million deaths) and South-East Asia (10.4 million deaths) Regions.
Comparable estimates of NCD mortality for 2008—total NCD deaths, percentage of NCD deaths occurring under the age of 70, and age-standardized death rates per 100 000—are presented for each Member State of the Region in Annex 3.
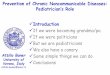
Overall mortality from noncommunicable diseases
Figure 1 presents the age-standardized death rate from NCDs in the Region. The data are presented in ascending order of mortality rates in HIC and LMIC. There is a two- to three-fold difference in male NCD mortality rates between HIC and LMIC.
*Countries have a high degree of uncertainty because they are not based on national NCD mortality data. The estimates for these countries are based on a combination of country life tables, cause of death models, regional cause of death patterns, and WHO and UNAIDS programme estimates for some major causes of death (not including NCDs).
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 1. Age-standardized death rate (per 100 000) from NCD, Western Pacific Region, 2008

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 11
High Income
% o
f all
NC
D d
eath
s
Low- and middle-income
Women
Men
100
75
50
25
0
Japa
n
Aust
ralia
Sing
apor
e
New
Zeal
and
Brun
eiDa
russ
alam
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds*
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of*
Vanu
atu*
Sam
oa*
Pala
u*
Niue
Kirib
ati
Papu
a Ne
w G
uine
a*
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he*
Mon
golia
*
Fiji
Cam
bodi
a*
Tuva
lu
Mar
shal
l Isla
nds,
the*
Naur
u
Repu
blic
ofKo
rea,
the
Premature mortality from noncommunicable diseases
Premature deaths from NCDs result in loss of productivity and have an impact on the economy. Figure 2 presents the proportion of all NCD deaths occurring under the age 70 in the Western Pacific Region, highlighting the greater burden borne by LMIC.
*Countries have a high degree of uncertainty because they are not based on national NCD mortality data. The estimates for these countries are based on a combination of country life tables, cause of death models, regional cause of death patterns, and WHO and UNAIDS programme estimates for some major causes of death (not including NCDs).
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 2. Percentage of all NCD deaths under age 70, Western Pacific Region, 2008

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile12
High Income
Age
-sta
ndar
dize
d de
ath
rate
per
100
,000
Low- and middle-income
Women
Men
1000
750
500
250
0
Japa
nAu
stra
lia
Sing
apor
e
New
Zeal
and
Brun
eiDa
russ
alam
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds*
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of*
Vanu
atu*
Sam
oa*
Pala
u*
Niue
Kirib
ati
Papu
a Ne
w G
uine
a*
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he*
Mon
golia
*
Cam
bodi
a*
Tuva
luM
arsh
all I
sland
s, th
e*
Naur
u
Repu
blic
ofKo
rea,
the Fiji
* Country data not available. Estimate based on a combination of country life tables, cause of death models, regional cause of death patterns, and WHO and UNAIDS programme estimates for some major causes (not including chronic diseases).
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 3. Age-standardized death rate (per 100 000) from cardiovascular disease and diabetes, Western Pacific Region, 2008
Cardiovascular disease and diabetes mellitus
Age-standardized death rates from cardiovascular disease and diabetes mellitus are provided in Figure 3. Substantial differences in mortality rates are seen between HIC and LMIC.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 13
High Income
Age
-sta
ndar
dize
d de
ath
rate
per
100
,000
Low- and middle-income
Women
Men
300
200
100
0
Japa
n
Aust
ralia
Sing
apor
eNe
w Ze
alan
d
Brun
eiDa
russ
alam
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds*
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of*
Vanu
atu*
Sam
oa*
Pala
u*
Niue
Kirib
ati
Papu
a Ne
w G
uine
a*
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he*
Mon
golia
*
Cam
bodi
a*
Tuva
lu
Mar
shal
l Isla
nds,
the*
Naur
u
Repu
blic
ofKo
rea,
the Fiji
Cancer
Within the Region, cancer deaths make up one quarter of all NCD deaths. Variation in death rates across countries is presented in Figure 4.
* Country data not available. Estimate based on a combination of country life tables, cause of death models, regional cause of death patterns, and WHO and UNAIDS programme estimates for some major causes (not including chronic diseases).
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 4. Age-standardized death rate (per 100 000) from cancer, Western Pacific Region, 2008

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile14
High Income
Age
-sta
ndar
dize
d ra
te p
er 1
00,0
00
Low- and middle-income
Women
Men
400
300
200
100
0
Japa
n
Aust
ralia
Sing
apor
e
New
Zeal
and
Brun
eiDa
russ
alam
Mal
aysia
Chin
a
Viet
Nam
Solo
mon
Isla
nds
Philip
pine
s
Vanu
atu
Sam
oa
Papu
a Ne
w G
uine
a
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he
Mon
golia
Cam
bodi
a
Repu
blic
ofKo
rea,
the Fiji
Micr
ones
ia,
the
Fede
rate
d St
ates
of
3 GLOBOCAN 2008. Lyons, International Agency for Research on Cancer, 2008 (http://globocan.iarc.fr/)
MORBIDIty
Morbidity data on the four principal NCDs are not uniformly available. Only cancer and diabetes mellitus are addressed in this profile. Population-based disease registries are essential to generate incidence data on NCDs.
Cancer Morbidity data on cancer come from GLOBOCAN 2008,3 which provides comparable estimates on incidence and mortality of cancers worldwide in 2008. Figure 5 presents age-standardized cancer incidence in men and women and demonstrates the wide variation across countries.
Source: IARC Globocan 2008
Figure 5. Age-standardized incidence rate of cancer (all sites except non-melanoma skin cancer), Western Pacific Region, 2008

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 15
High Income
Age
-sta
ndar
dize
d ra
te p
er 1
00,0
00
Low- and middle-income
Cervix
Breast
100
75
50
25
0
Japa
n
Aust
ralia
Sing
apor
e
New
Zeal
and
Brun
eiDa
russ
alam
Mal
aysia
Chin
a
Viet
Nam
Solo
mon
Isla
nds
Philip
pine
s
Vanu
atu
Sam
oa
Papu
a Ne
w G
uine
a
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he
Mon
golia
Cam
bodi
a
Repu
blic
ofKo
rea,
the Fiji
In women, breast and cervical cancer are among the leading causes of cancer deaths. The variation in incidence among countries is in large part a reflection of heterogeneous screening and early detection programmes throughout the Region in addition to the underlying differences in occurence (Figure 6).
Source: IARC Globocan 2008
Figure 6. Age-standardized incidence rate of breast and cervix uteri cancer, Western Pacific Region, 2008

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile16
High Income
Prev
alen
ce %
Low- and middle-income
Women
Men
40
30
20
10
0
Japa
n
Aust
ralia
Sing
apor
e
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of
Vanu
atu
Sam
oa
Kirib
ati
Papu
a Ne
w G
uine
a
Mon
golia
Cam
bodi
a
Mar
shal
l Isla
nds,
the
Naur
u
Repu
blic
ofKo
rea,
the Fiji
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 7. Age-standardized prevalence of diabetes mellitus in adults aged 25+ years, comparable estimates, Western Pacific Region, 2008
4 Diabetes is defined as having a fasting plasma glucose value ≥ 7.0 mmol/L (126 mg/dl) or being on medication for raised blood glucose.
Diabetes mellitus
Diabetes mellitus4 is an important marker of the burden of NCD in a population. It is the leading cause of renal failure in many populations. Figure 7 shows a marked variation in prevalence rates of diabetes in the Region, and very little difference in prevalence among men and women in most countries.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 17
High Income
Prev
alen
ce %
Low- and middle-income
Women
Men
75
50
25
0
Japa
n
Aust
ralia
Sing
apor
e
New
Zeal
and
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of
Vanu
atu
Sam
oa
Pala
u
Kirib
ati
Papu
a Ne
w G
uine
a
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he
Mon
golia
Cam
bodi
a
Tuva
lu
Mar
shal
l Isla
nds,
the
Naur
u
Repu
blic
ofKo
rea,
the Fiji
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 8. Age-standardized prevalence of daily tobacco smoking in adults aged 15+ years, comparable country estimates, Western Pacific Region, 2008
3. Risk factors for noncommunicable diseases
The levels of NCD risk factors in the population are important indicators of future disease burden. Four modifiable risk factors are responsible for two thirds of NCDs in the Region: tobacco use, unhealthy diets, physical inactivity and harmful use of alcohol. Significant gains can be made in the Region by addressing all of these risk factors as well as the metabolic and physiologic changes: obesity, raised blood pressure, raised blood glucose, and unhealthy lipid profiles.
BeHAvIOuRAL RIsk FACtORs
Tobacco use
Tobacco use is the leading cause of preventable deaths globally and within the Region. The percentage of men and women who smoke daily varies considerable by country, with rates ranging from less than 15% to 74% in men, and from under 2% to 62% in women (Figure 8). The variation in rates of tobacco use prevalence is a reflection of tobacco control efforts and indicates the huge potential for reducing rates further in countries.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile18
High Income
Prev
alen
ce %
Low- and middle-income
Women
Men
75
50
25
0
Japa
n
Aust
ralia
New
Zeal
and
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of
Sam
oa
Kirib
ati
Papu
a Ne
w G
uine
a
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he
Mon
golia
Cam
bodi
a
Mar
shal
l Isla
nds,
the
Naur
u
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 9. Age-standardized prevalence of insufficient physical activity in adults aged 15+ years, comparable country estimates, Western Pacific Region, 2008
5 Insufficient physical activity is defined as less than 30 minutes of moderate activity five times per week, or less than 20 minutes of vigorous activity three times per week, or equivalent.
unhealthy diet
Unhealthy diet is composed of multiple elements. Comparable data on the prevalence of this parameter across countries were not available. Metabolic and physiologic risk factors such as obesity, diabetes and high blood cholesterol are indirect indicators of the prevalence of unhealthy diets in the population.
Physical inactivity
Physical inactivity5 is variable across the Region, with prevalence rates ranging from 10% to 70% in men and women. Women tend to report more physical inactivity than men, especially in PIC (Figure 9).

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 19
High Income
Adu
lt ca
pita
con
sum
ptio
n of
pur
e al
coho
l (lit
res)
Low- and middle-income
20
15
10
5
0
Japa
n
Aust
ralia
Sing
apor
e
New
Zeal
and
Brun
eiDa
russ
alam
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of
Vanu
atu
Sam
oa
Pala
u
Niue
Kirib
ati
Papu
a Ne
w G
uine
a
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he
Mon
golia
Cam
bodi
a
Tuva
lu
Naur
u
Repu
blic
ofKo
rea,
the Fiji
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 10. total adult (15+ years of age) per capita consumption of pure alcohol (litres) for both sexes, Western Pacific Region, 2008
Harmful use of alcohol
There is a high level of variation in alcohol consumption. Total adult per capita consumption of pure alcohol (litres) for both sexes is presented in Figure 10.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile20
High Income
Prev
alen
ce %
Low- and middle-income
Women
Men
75
50
25
0
Japa
n
Aust
ralia
Sing
apor
e
New
Zeal
and
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of
Vanu
atu
Sam
oa
Kirib
ati
Papu
a Ne
w G
uine
a
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he
Mon
golia
Cam
bodi
a
Mar
shal
l Isla
nds,
the
Naur
u
Repu
blic
ofKo
rea,
the Fiji
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 11. Age-standardized prevalence of obesity in adults aged 20+ years, comparable country estimates, Western Pacific Region, 2008
6 Overweight is defined as body mass index (BMI) ≥25 kg/m2 , while obesity as BMI ≥30 kg/m2.7 The World health report 2002: Reducing risks, promoting healthy life. Geneva, World Health Organization, 2002.8 Policy and action for cancer prevention. Food, nutrition, and physical activity: a global perspective. Washington, DC, World Cancer Research Fund/American Institute for Cancer Research, 2009.
MetABOLIC/PHysIOLOgIC RIsk FACtORs
Behavioural risk factors lead to metabolic/physiologic risk factors such as overweight and obesity, raised blood pressure, raised blood glucose, and unhealthy lipid profiles. These risk factors operate on a risk continuum and population-based approaches are needed to reduce the mean levels in the population. Mean levels of systolic blood pressure, body mass index (BMI), blood glucose, and total cholesterol are incorporated in the NCD country profiles in Section 5. This section presents the prevalence of risk factors using the cut-off levels used in the WHO Global status report on noncommunicable diseases 2010.
Overweight and obesity
Overweight and obesity6 lead to adverse effects on blood pressure, cholesterol, triglycerides and insulin resistance. The risks of coronary heart disease, ischaemic stroke and type 2 diabetes mellitus increase steadily with increasing BMI. Raised BMI also increases the risk of cancer of the breast, colon/rectum, endometrium, kidney, oesophagus (adenocarcinoma) and pancreas.7,8
The prevalence of obesity among adults in the Region varies from under 5% to 75%. Women are more likely to be obese than men, especially in many PIC (Figure 11).

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 21
High Income
Prev
alen
ce %
Low- and middle-income
Women
Men
75
50
25
0
Japa
n
Aust
ralia
Sing
apor
e
New
Zeal
and
Cook
Isla
nds
Mal
aysia
Tong
a
Chin
a
Viet
Nam
Solo
mon
Isla
nds
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of
Vanu
atu
Sam
oa
Kirib
ati
Papu
a Ne
w G
uine
a
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
he
Mon
golia
Cam
bodi
a
Mar
shal
l Isla
nds,
the
Naur
u
Repu
blic
ofKo
rea,
the Fiji
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 12. Age-standardized prevalence of raised blood pressure in adults aged 25+ years, comparable country estimates, Western Pacific Region, 2008
9 Raised blood pressure is defined as systolic blood pressure of ≥140 mmHg and/or diastolic blood pressure of ≥90 mmHg, or using medication to lower blood pressure.
Raised blood pressure
Raised blood pressure9 has been shown to be positively linked to stroke and coronary heart disease and to multiple end-organ complications. All countries in the Region have prevalence rates of raised blood pressure over 20%, with country-specific rates ranging from 25% to 50%. Rates among women are almost as high as men in all the countries. Prevalence of raised blood pressure does not show a marked difference between HIC and LMIC (Figure 12).

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile22
High Income
Prev
alen
ce %
Low- and middle-income
Women
Men
75
50
25
0
Japa
n
Aust
ralia
Sing
apor
e
New
Zeal
and
Cook
Isla
nds
Tong
a
Chin
a
Solo
mon
Isla
nds
Philip
pine
s
Micr
ones
ia,
the
Fede
rate
d St
ates
of
Sam
oa
Kirib
ati
Papu
a Ne
w G
uine
a
Mon
golia
Cam
bodi
a
Mar
shal
l Isla
nds,
the
Naur
u
Repu
blic
ofKo
rea,
the Fiji
Source: Global status report on noncommunicable diseases. Geneva, WHO, 2011.
Figure 13. Age-standardized prevalence of raised total cholesterol11 in adults aged 25 years, comparable country estimates, Western Pacific Region, 2008
10 Ezzati M et al. Selected major risk factors and global and regional burden of disease. The Lancet, 2002, 360:1347–1360.11 Raised cholesterol was defined, in these estimates, as 5.0 mmol/L or 190 mg/dl or higher.
Raised cholesterol
raised cholesterol10 increases the risk of heart disease and stroke. The prevalence of raised cholesterol is higher in HIC than LMIC. Uniformly high rates are observed in both men and women (Figure 13).

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 23
NCD POLICy AND PROgRAMMe INFRAstRuCtuReIndicator
2004 (n=27)
2010 (n=35)
Number of countries with national NCD entity (focal point, unit or department) 14 32
Number of countries with an allocated budget for NCD prevention and control 24 30
Number of countries with an integrated NCD policy, strategy and/or action plan 15 28
Number of countries with legislation (acts, laws, regulations, ministerial decrees, policies,plans, procedures, etc.) on:
Tobacco Control 22 29
Nutrition 17 23
Physical Activity 9 21
Alcohol Consumption 12 19
Diabetes 15 25
Number of countries completing at least one round of WHO STEPS survey 10 22
Number of countries with surveillance system that covers the following risk factors:
Tobacco Control 17 31
Alcohol Consumption 13 29
Unhealthy Diet 12 30
Physical Inactivity 12 27
Diabetes/Raised Blood Glucose 18 28
Hypertension/Raised Blood Pressure 17 29
Overweight and Obesity 15 30
Dyslipidaemia 10 25
Number of countries with clinical protocols, guidelines, standards for the treatment/managementof the following:
Hypertension 16 32
Diabetes Mellitus 18 33
Source: NCD country capacity survey data, WHO Western Pacific Regional Office, 2004 and 2010.
table 1. Comparison of country capacity indicators, Western Pacific Region, 2004 and 2010
4. NCD country capacityNCD country capacity surveys (CCS) were undertaken by WHO in 2004 and 2010 to update information on individual country capacity to address NCD prevention and control. Collated information from countries is available in the Global Health Observatory Data Repository (http://apps.who.int/ghodata/).
COuNtRy CAPACIty suRveys: 2004 AND 2010
In the Region, twenty-seven countries and areas responded to the survey in 2004 and 35 responded in 2010. Table 1 shows the status of selected parameters in both years.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile24
table 2. Dedicated NCD unit, integrated NCD policy, and policies on risk factors, Western Pacific Region, 2010
Note: *Not a standalone policy but was reported as part of the integrated national policy
COuNtRy CAPACIty 2010
NCD unit and policies
Thirty-two of the 35 countries and areas that responded to the 2010 survey have a unit, branch or department in the Ministry of Health (or its equivalent) designated for NCD prevention and control. Twenty-eight have an integrated NCD policy, strategy and/or action plan and specific policies that address risk factors, most notably tobacco use.
Though structures and mechanisms vary, most countries and areas have a designated NCD unit and policies for NCD risk factor reduction (Table 2).
Country
Dedicated NCD office in Ministry of Health
IntegratedNCD Policy
Policy addressing specific risk factors
Alcohol unhealthy diet
Physical inactivity Tobacco
American Samoa Yes No No No No YesAustralia Yes Yes Yes Yes Yes YesBrunei Darussalam No No Yes Yes Yes YesCambodia Yes Yes Yes No* No* YesChina Yes No No Yes No NoCook islands Yes Yes No* No* No* YesFiji Yes Yes Yes Yes Yes YesFrench Polynesia Yes Yes Yes Yes Yes YesGuam Yes NoHong Kong (China) Yes Yes Yes Yes Yes YesJapan Yes Yes Yes Yes Yes YesKiribati Yes Yes Yes Yes Yes YesLao People’s Democratic Republic, the Yes Yes No* No* No* Yes
Macao (China) Yes No No Yes Yes YesMalaysia Yes Yes No Yes Yes YesMarshall Islands, the Yes Yes Yes No* No* YesMicronesia, the Federated States of Yes Yes Yes Yes Yes Yes
Mongolia Yes Yes Yes Yes Yes No*Nauru Yes Yes No* Yes Yes No*New Caledonia Yes Yes Yes Yes Yes YesNew Zealand No No Yes Yes Yes YesNiue Yes Yes Yes Yes Yes YesNorthern Mariana Islands, the Commonwealth of the Yes No Yes Yes Yes Yes
Palau Yes Yes No* Yes No* YesPapua New Guinea Yes Yes No* No* No*Philippines Yes Yes No* No* No* YesRepublic of Korea, the Yes Yes Yes Yes Yes YesSamoa Yes Yes No* Yes Yes YesSingapore Yes Yes Yes Yes Yes YesSolomon islands Yes Yes No* No* No* YesTokelau No Yes Yes Yes Yes YesTonga Yes Yes No* Yes No* No*Tuvalu Yes Yes No* No* No* YesVanuatu Yes Yes Yes Yes Yes YesViet Nam Yes Yes No No No Yes

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 25
Health reporting, information systems, monitoring and surveillance
Twelve of the 35 countries and areas have incorporated population-based, cause-specific mortality data into their national health reporting systems. While many countries and areas in the Region have a cancer registry, only 10 countries maintain a population-based cancer registry. Twenty-six countries and areas reported having risk factor surveys, and of which, 23 are based on populations (Table 3). The WHO STEPwise approach to surveillance of NCD risk factors (STEPS) has been used in 22 countries and areas of the Region either in a “stand alone” format or incorporated into national health surveys (Annex 4). Repeated surveys at regular intervals are essential to measure trends.
table 3. surveillance data in national health reporting systems, Western Pacific Region, 2010
*Population-based data
Country Mortality Cancer Registry Risk Factors
American Samoa No Yes Yes*Australia Yes* Yes* Yes*Brunei Darussalam Yes* Yes Yes*Cambodia Yes Yes NoChina Yes* Yes* YesCook islands Yes Yes* YesFiji Yes Yes* YesFrench Polynesia Yes Yes NoGuam Yes Yes* YesHong Kong (China) Yes* Yes* Yes*Japan Yes* Yes* YesKiribati Yes Yes* YesLao People’s Democratic Republic, the No Yes* YesMacao (China) Yes Yes YesMalaysia Yes Yes* Yes*Marshall Islands, the Yes Yes YesMicronesia, the Federated States of Yes Yes* YesMongolia Yes Yes* YesNauru Yes Yes* YesNew Caledonia Yes* Yes* YesNew Zealand Yes* Yes* Yes*Niue Yes Yes* YesNorthern Mariana Islands, the Commonwealth of the Yes Yes Yes
Palau Yes* Yes NoPapua New Guinea Yes* Yes* YesPhilippines Yes Yes* Yes*Republic of Korea, the Yes* Yes* Yes*Samoa Yes No NoSingapore Yes* Yes* Yes*Solomon islands No Yes NoTokelau Yes* Yes* YesTonga Yes Yes* YesTuvalu Yes No NoVanuatu Yes Yes* Yes*Viet Nam Yes Yes No

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile26
Health system capacity for NCD prevention, early detection, treatment and care within the primary health care system
A majority of the respondent countries and areas have evidence-based national guidelines, protocols and/or standards for diabetes (94%) and hypertension (91%) (Table 4). Nearly half of the 35 countries and areas have insurance coverage for NCDs (46%), while 29 countries and areas have a list of essential NCD-related medicines. Accessibility to community or home care for people with advanced or end-stage NCDs was reported by 14 countries and areas.
Health promotion, partnerships and collaboration
Thirty-two of the 35 countries and areas reported engaging in partnerships to implement NCD activities (Table 5). Key stakeholders are nongovernmental organizations, the private sector, and non-health government ministries or departments.
A majority of countries and areas reported implementing fiscal interventions for NCD prevention and control (86%). About one third reported having established earmarking of taxes on substances such as tobacco and alcohol. Fifteen have regulations on the marketing of food to children, while nine have enforcement mechanisms.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 27
Coun
try
/ A
rea
gui
delin
es/p
roto
cols
/sta
ndar
ds fo
r th
e m
gmt
of c
ondi
tion
s fo
r N
CDs
Hea
lth
care
sys
tem
fact
ors
affe
ctin
g N
CD m
anag
emen
t
Dia
bete
sH
yper
tens
ion
Ove
rwei
ght
and
obes
ity
Bloo
d lip
ids
Alc
ohol
de
pend
ence
Toba
cco
depe
nden
ceD
ieta
ry
coun
selin
g
Phys
ical
ac
tivi
ty
coun
selin
g
esse
ntia
l lis
t of
m
edic
ine
Hea
lth
insu
ranc
e co
vera
ge
Amer
ican
Sam
oaYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sAu
stra
liaYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
oYe
sBr
unei
Dar
ussa
lam
Yes
Yes
No
Yes
No
Yes
Yes
No
Yes
No
Cam
bodi
aYe
sYe
sN
oN
oN
oN
oYe
sYe
sYe
sN
oCh
ina
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
Cook
isla
nds
Yes
Yes
Yes
No
No
No
Yes
Yes
Yes
No
Fiji
Yes
Yes
Yes
Yes
No
No
Yes
Yes
Yes
No
Fren
ch P
olyn
esia
Yes
Yes
Yes
Yes
No
No
No
Yes
Gua
m
Hon
g Ko
ng (C
hina
)Ye
sYe
sN
oYe
sYe
sYe
sYe
sYe
sYe
sYe
sJa
pan
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Kirib
ati
Yes
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
No
Lao
Peop
le’s
Dem
ocra
tic R
epub
lic, t
heYe
sYe
sN
oN
oN
oN
oYe
sYe
sM
acao
(Chi
na)
Yes
Yes
Yes
Yes
No
Yes
No
No
Yes
No
Mal
aysi
aYe
sYe
sYe
sYe
sN
oYe
sYe
sYe
sYe
sYe
sM
arsh
all I
slan
ds, t
heYe
sYe
sYe
sYe
sN
oN
oYe
sYe
sYe
sN
oM
icro
nesi
a, th
e Fe
dera
ted
Stat
es o
fYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sM
ongo
liaYe
sYe
sN
oN
oYe
sYe
sYe
sYe
sYe
sYe
sN
auru
Yes
Yes
No
Yes
No
No
No
No
Yes
No
New
Cal
edon
iaYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
oYe
sN
ew Z
eala
ndYe
sYe
sYe
sYe
sN
oYe
sYe
sYe
sYe
sYe
sN
iue
Yes
Yes
Yes
Yes
No
Yes
Yes
No
Yes
No
Nor
ther
n M
aria
na Is
land
s, th
e Co
mm
onw
ealth
of t
heYe
sYe
sN
oYe
sYe
sYe
sN
oYe
sYe
sPa
lau
Yes
Yes
Yes
Yes
Yes
Yes
No
No
Yes
No
Papu
a N
ew G
uine
aYe
sYe
sYe
sYe
sYe
sYe
sYe
sPh
ilipp
ines
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
Yes
Yes
Repu
blic
of K
orea
, the
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Sam
oaYe
sYe
sYe
sN
oN
oN
oN
oYe
sN
oSi
ngap
ore
Yes
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
Yes
Solo
mon
isla
nds
Yes
No
No
No
No
Yes
Yes
Yes
Yes
No
Toke
lau
Yes
Yes
No
No
No
No
No
No
Yes
No
Tong
aYe
sYe
sN
oYe
sN
oN
oYe
sYe
sYe
sYe
sTu
valu
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
Yes
No
Vanu
atu
Yes
Yes
Yes
No
No
Yes
Yes
Yes
Yes
No
Viet
Nam
No
No
No
No
No
No
No
No
Yes
Yes
tabl
e 4.
H
ealt
h sy
stem
cap
acit
y fo
r N
CD p
reve
ntio
n, e
arly
det
ecti
on, t
reat
men
t an
d ca
re w
ithi
n th
e pr
imar
y he
alth
car
e sy
stem
,
Wes
tern
Pac
ific
Regi
on, 2
010

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile28
Coun
try
/ A
rea
Wit
h pa
rtne
rshi
ps /
co
llabo
rati
ons
key
stak
ehol
ders
Hea
lth
prom
otio
n in
itia
tive
sO
ther
g
over
nmen
t M
inis
trie
s (N
on-h
ealt
h)
Oth
er
inte
rnat
iona
l in
stit
utio
ns
Aca
dem
ia
and
rese
arch
ce
ntre
s
Ng
Os
/ co
mm
unit
y-ba
sed
orga
niza
tion
s /
civi
l soc
iety
Priv
ate
Sect
orFi
scal
in
terv
enti
ons
earm
arki
ng o
f ta
xes
Init
iati
ves
to
regu
late
food
m
arke
ting
to
child
ren
enfo
rcem
ent
of fo
od
mar
keti
ng
regu
lati
ons
Amer
ican
Sam
oaYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
oN
o Au
stra
liaYe
sYe
sN
oN
oYe
sYe
sYe
sYe
sYe
sYe
sYe
sBr
unei
Dar
ussa
lam
Yes
Yes
Yes
Yes
Yes
Yes
No
No
No
Cam
bodi
aYe
sN
oYe
sYe
sYe
sYe
sYe
sYe
sN
oN
o N
o Ch
ina
No
Yes
No
No
No
Cook
isla
nds
Yes
Yes
Yes
No
No
Yes
Yes
Yes
No
No
No
Fiji
Yes
Yes
No
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Fren
ch P
olyn
esia
Yes
Yes
No
Yes
No
Yes
No
Yes
Yes
No
No
Gua
mYe
sYe
sN
oN
oYe
sYe
sYe
sYe
sYe
sYe
s N
o H
ong
Kong
(Chi
na)
Yes
Yes
No
No
Yes
Yes
Yes
Yes
No
No
No
Japa
nYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
o
Yes
Yes
Kirib
ati
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
Yes
Yes
Yes
Lao
Peop
le’s
Dem
ocra
tic
Repu
blic
, the
No
Ye
sYe
s*M
acao
(Chi
na)
Yes
Yes
No
No
Yes
Yes
Yes
Yes
No
No
No
Mal
aysi
aYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
oYe
sYe
s*M
arsh
all I
slan
ds, t
heYe
sYe
sN
oN
oN
oYe
sYe
sYe
sN
oN
o N
o M
icro
nesi
a, th
e Fe
dera
ted
Stat
es o
fYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
oYe
sYe
sM
ongo
liaYe
sYe
sYe
sYe
sYe
sYe
sN
oYe
sYe
sN
o N
o N
auru
Yes
Yes
No
Yes
No
Yes
Yes
Yes
No
No
No
New
Cal
edon
iaYe
sYe
sN
oYe
sN
oYe
sYe
sYe
sYe
sYe
sYe
s*N
ew Z
eala
ndYe
sN
oN
oN
oYe
sYe
sYe
sYe
sN
oN
o N
o N
iue
Yes
Yes
No
No
No
Yes
Yes
Yes
No
No
No
Nor
ther
n M
aria
na Is
land
s, th
e Co
mm
onw
ealth
of t
heYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
o N
o Pa
lau
Yes
Yes
No
Yes
Yes
Yes
Yes
Yes
No
No
No
Papu
a N
ew G
uine
aYe
sYe
sN
oYe
sN
oYe
sYe
sYe
s
Yes
Yes
Phili
ppin
esYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
o N
o Re
publ
ic o
f Kor
ea, t
heN
o
Ye
sYe
sYe
sYe
sSa
moa
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
Ye
sYe
sSi
ngap
ore
Yes
Yes
Yes
Yes
Yes
No
No
Yes
No
Yes
Yes*
Solo
mon
isla
nds
Yes
Yes
Yes
Yes
No
Yes
No
No
N
o N
o To
kela
uYe
sN
oYe
sYe
sN
oN
oN
oN
o
No
No
Tong
aYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sN
oN
o N
o Tu
valu
Yes
Yes
Yes
Yes
No
Yes
No
Yes
No
Yes
Yes
Vanu
atu
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes*
Viet
Nam
Yes
Yes
Yes
Yes
Yes
Yes
No
Yes
No
No
No
tabl
e 5.
H
ealt
h pr
omot
ion,
par
tner
ship
s, a
nd c
olla
bora
tion
, Wes
tern
Pac
ific
Regi
on, 2
010
Not
es: *
Yes=
Food
mar
ketin
g re
gula
tion
to c
hild
ren
is s
elf-r
egul
ated

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 29
12 Noncommunicable diseases country profiles. Geneva , WHO, 2011. Available online at http://www.who.int/nmh/countries/en/index.html.
5. NCD country profilesThe NCD country profiles in this section present data of each country related to their NCD mortality, risk factors and capacity to prevent and control NCDs.12 The data presented in each of the country profiles were derived from several sources, as detailed in Annex 2.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile30
Australia
Income group: High
2008 estimates males females
Total NCD deaths (000s) 63.4 63.2
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 364.8 246.3
Cancers 140.8 92.9
Chronic respiratory diseases 25.6 15.5
Cardiovascular diseases and diabetes 136.3 88.6
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 18.3 15.4 16.8
Physical inactivity 38.0 42.5 40.3
2008 estimated prevalence (%) males females total
Raised blood pressure 41.1 32.0 36.4
Raised blood glucose 10.8 8.0 9.4
Overweight 68.2 59.3 63.7
Obesity 26.4 27.1 26.8
Raised cholesterol 55.9 58.9 57.4 NCDs are estimated to account for 90% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control Yes Cancer Yes
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes No
Alcohol Yes
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes
NCD cause-specific mortality Yes Physical inactivity Yes
NCD morbidity Yes Tobacco Yes
NCD risk factors Yes
Has a national, population-based cancer registry Yes
World Health Organization - NCD Country Profiles , 2011.
13.4
NCD mortality
9.2
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
2010 total population: 22 268 384
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement3/5
118
121
124
127
130
133
136
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.8
5.0
5.2
5.4
5.6
5.8
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
20
22
24
26
28
30
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
5.0
5.2
5.4
5.6
5.8
6.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
35%
Cancers
29%
Respiratory
diseases
6%
Other NCDs
17%
Injuries
6%
Diabetes
3%
Communicable,
maternal,
perinatal and
nutritional
conditions
4%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 31
Brunei Darussalam
Income group: High
2008 estimates males females
Total NCD deaths (000s) 0.5 0.5
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 534.3 488.7
Cancers 97.0 98.1
Chronic respiratory diseases 69.0 44.0
Cardiovascular diseases and diabetes 292.7 275.4
2008 estimated prevalence (%) males females total
Current daily tobacco smoking … … …
Physical inactivity ... ... ...
2008 estimated prevalence (%) males females total
Raised blood pressure ... ... ...
Raised blood glucose ... ... ...
Overweight ... ... ...
Obesity ... ... ...
Raised cholesterol … … … NCDs are estimated to account for 82% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs No
There is funding available for: Cardiovascular diseases No
NCD treatment and control Yes Cancer No
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes
Alcohol Yes
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes
NCD cause-specific mortality Yes Physical inactivity No
NCD morbidity Yes Tobacco Yes
NCD risk factors No
Has a national, population-based cancer registry Yes
… = no data available
World Health Organization - NCD Country Profiles , 2011.
41.4
NCD mortality
30.0
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
2010 total population: 398 920
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement1/5
116
120
124
128
132
136
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.6
4.8
5.0
5.2
5.4
5.6
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
18
20
22
24
26
28
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.6
4.8
5.0
5.2
5.4
5.6
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
33%
Cancers
16%
Diabetes
11%
Other NCDs
14%
Communicable,
maternal,
perinatal and
nutritional
conditions
10%
Injuries
8%
Respiratory
diseases
8%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile32
Cambodia
Income group: Low
2008 estimates males females
Total NCD deaths (000s) 31.1 25.5
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 957.9 592.2
Cancers 144.9 90.0
Chronic respiratory diseases 129.0 60.4
Cardiovascular diseases and diabetes 480.4 338.7
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 45.6 3.7 23.7
Physical inactivity 10.8 10.9 10.9
2008 estimated prevalence (%) males females total
Raised blood pressure 30.5 25.1 27.6
Raised blood glucose 3.9 4.5 4.2
Overweight 10.8 13.2 12.1
Obesity 1.5 2.7 2.1
Raised cholesterol 26.4 31.1 29.0 NCDs are estimated to account for 46% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors No
Has a national, population-based cancer registry No
* The mortality estimates for this country have a high degree of uncertainty because they are not based ** = covered by integrated policy/programme/action plan
on any national NCD mortality data. The estimates are based on a combination of country life tables,
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
56.2
NCD mortality*
34.8
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
2010 total population: 14 138 255
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
110
112
114
116
118
120
122
124
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.4
4.6
4.8
5.0
5.2
5.4
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
16
18
20
22
24
26
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
3.8
4.0
4.2
4.4
4.6
4.8
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
21%
Cancers
7%
Other NCDs
11%
Communicable,
maternal,
perinatal and
nutritional
conditions
46%
Injuries
7%
Respiratory
diseases
5%
Diabetes
3%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 33
China
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 4323.3 3675.5
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 665.2 495.2
Cancers 182.3 105.0
Chronic respiratory diseases 118.4 88.7
Cardiovascular diseases and diabetes 311.5 259.6
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 49.3 2.1 26.3
Physical inactivity 29.3 32.0 30.6
2008 estimated prevalence (%) males females total
Raised blood pressure 40.1 36.2 38.2
Raised blood glucose 9.5 9.3 9.4
Overweight 25.5 25.4 25.4
Obesity 4.7 6.7 5.7
Raised cholesterol 31.8 35.3 33.5 NCDs are estimated to account for 83% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control Yes Cancer Yes
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes No
Alcohol No
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes
NCD cause-specific mortality Yes Physical inactivity No
NCD morbidity Yes Tobacco No
NCD risk factors Yes
Has a national, population-based cancer registry Yes
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 1 341 335 152
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
22.8
NCD mortality
17.4
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
119
121
123
125
127
129
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.8
5.0
5.2
5.4
5.6
5.8
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
18
20
22
24
26
28
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.0
4.2
4.4
4.6
4.8
5.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
38%
Cancers
21%
Respiratory
diseases
15%
Other NCDs
7%
Diabetes
2%
Communicable,
maternal,
perinatal and
nutritional
conditions
7%
Injuries
10%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile34
Cook Islands
Income group: Upper middle
2008 estimates males females
Total NCD deaths (000s) 0.0 0.0
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 592.0 326.3
Cancers 58.6 57.4
Chronic respiratory diseases 61.3 26.3
Cardiovascular diseases and diabetes 350.7 180.0
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 38.9 29.7 34.4
Physical inactivity 71.6 73.0 72.3
2008 estimated prevalence (%) males females total
Raised blood pressure 46.0 36.8 41.5
Raised blood glucose 19.5 20.5 20.0
Overweight 91.0 89.9 90.5
Obesity 59.7 67.9 63.7
Raised cholesterol 58.8 57.3 58.1 NCDs are estimated to account for 74% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 20 288
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement1/5
39.4
NCD mortality
30.6
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
Mean fasting blood glucose
Mean body mass index
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
37%
Cancers
10%Respiratory
diseases
7%
Other NCDs
15%
Injuries
7%Communicable,
maternal,
perinatal and
nutritional
conditions
19%
Diabetes
5%
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 35
Fiji
Income group: Upper middle
2008 estimates males females
Total NCD deaths (000s) 2.4 1.8
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 928.4 590.9
Cancers 106.2 121.6
Chronic respiratory diseases 91.1 44.2
Cardiovascular diseases and diabetes 579.9 328.2
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 15.0 1.7 8.4
Physical inactivity ... ... ...
2008 estimated prevalence (%) males females total
Raised blood pressure 40.1 37.5 38.8
Raised blood glucose 12.0 15.6 13.8
Overweight 58.3 71.7 65.0
Obesity 20.3 41.1 30.6
Raised cholesterol 56.1 48.9 52.5 NCDs are estimated to account for 77% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
… = no data available
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 860 623
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
45.6
NCD mortality
38.0
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
120
122
124
126
128
130
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
5.1
5.3
5.5
5.7
5.9
6.1
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
21
23
25
27
29
31
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.4
4.6
4.8
5.0
5.2
5.4
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
42%
Cancers
12%
Other NCDs
13%
Injuries
5%Communicable,
maternal,
perinatal and
nutritional
conditions
18%
Respiratory
diseases
6%
Diabetes
4%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile36
Japan
Income group: High
2008 estimates males females
Total NCD deaths (000s) 473.2 435.5
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 336.7 178.1
Cancers 150.5 76.6
Chronic respiratory diseases 22.5 8.0
Cardiovascular diseases and diabetes 118.1 65.0
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 36.6 8.7 22.2
Physical inactivity 64.4 66.1 65.3
2008 estimated prevalence (%) males females total
Raised blood pressure 47.1 41.0 43.9
Raised blood glucose 8.9 6.7 7.7
Overweight 30.1 19.2 24.4
Obesity 5.8 4.4 5.0
Raised cholesterol 57.0 58.5 57.8 NCDs are estimated to account for 80% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry Yes
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 126 535 920
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
11.6
NCD mortality
7.0
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
124
126
128
130
132
134
136
138
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.7
4.9
5.1
5.3
5.5
5.7
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
18
20
22
24
26
28
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.4
4.6
4.8
5.0
5.2
5.4
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
32%
Cancers
31%
Respiratory
diseases
5%
Other NCDs
11%
Communicable,
maternal,
perinatal and
nutritional
conditions
14%
Diabetes
1%
Injuries
6%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 37
Kiribati
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 0.3 0.2
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 832.4 548.3
Cancers 39.0 64.2
Chronic respiratory diseases 61.8 19.1
Cardiovascular diseases and diabetes 425.9 223.8
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 73.3 61.7 67.4
Physical inactivity 42.4 57.1 49.8
2008 estimated prevalence (%) males females total
Raised blood pressure 39.1 28.7 33.7
Raised blood glucose 22.0 22.8 22.4
Overweight 78.4 82.8 80.7
Obesity 37.7 53.8 46.0
Raised cholesterol 32.8 36.6 34.8 NCDs are estimated to account for 69% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control No Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases Yes**
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 99 546
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
66.5
NCD mortality
47.6
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
Mean fasting blood glucose
Mean body mass index
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
23%
Cancers
5%
Other NCDs
28%
Communicable,
maternal,
perinatal and
nutritional
conditions
29%
Diabetes
8%
Respiratory
diseases
4%
Injuries
3%
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile38
Lao People's Democratic Republic
Income group: Low
2008 estimates males females
Total NCD deaths (000s) 12.1 11.7
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 849.4 689.0
Cancers 145.4 111.1
Chronic respiratory diseases 122.8 103.4
Cardiovascular diseases and diabetes 467.9 392.8
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 41.4 2.5 21.6
Physical inactivity 15.6 19.5 17.6
2008 estimated prevalence (%) males females total
Raised blood pressure 34.4 30.0 32.1
Raised blood glucose ... ... ...
Overweight 10.0 16.4 13.3
Obesity 1.4 3.7 2.6
Raised cholesterol … … … NCDs are estimated to account for 48% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases DK
NCD treatment and control Yes Cancer DK
NCD prevention and health promotion Yes Chronic respiratory diseases DK
NCD surveillance, monitoring and evaluation Yes Diabetes DK
Alcohol DK
National health reporting system includes: Unhealthy diet / Overweight / Obesity DK
NCD cause-specific mortality No Physical inactivity DK
NCD morbidity No Tobacco No
NCD risk factors Yes
Has a national, population-based cancer registry No
* The mortality estimates for this country have a high degree of uncertainty because they are not based … = no data available
on any national NCD mortality data. The estimates are based on a combination of country life tables, DK = Country responded "don't know"
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 6 200 894
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
38.6
NCD mortality*
32.6
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
116
118
120
122
124
126
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.6
4.8
5.0
5.2
5.4
5.6
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
16
18
20
22
24
26
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.0
4.2
4.4
4.6
4.8
5.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
24%
Cancers
9%
Injuries
10%
Respiratory
diseases
7%
Diabetes
1%Other NCDs
8%
Communicable,
maternal,
perinatal and
nutritional
conditions
41%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 39
Malaysia
Income group: Upper middle
2008 estimates males females
Total NCD deaths (000s) 50.4 39.1
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 605.7 436.5
Cancers 118.8 89.9
Chronic respiratory diseases 74.7 42.1
Cardiovascular diseases and diabetes 318.7 236.5
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 40.9 1.6 21.5
Physical inactivity 56.0 65.0 60.5
2008 estimated prevalence (%) males females total
Raised blood pressure 36.9 32.4 34.7
Raised blood glucose 10.6 10.3 10.5
Overweight 42.1 46.3 44.2
Obesity 10.4 17.6 14.0
Raised cholesterol … … … NCDs are estimated to account for 67% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol No
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes
NCD risk factors Yes
Has a national, population-based cancer registry Yes
… = no data available
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 28 401 017
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement1/5
33.7
NCD mortality
26.3
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
120
122
124
126
128
130
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
5.0
5.2
5.4
5.6
5.8
6.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
18
20
22
24
26
28
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.4
4.6
4.8
5.0
5.2
5.4
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
32%
Cancers
15%
Respiratory
diseases
7%
Other NCDs
11%
Communicable,
maternal,
perinatal and
nutritional
conditions
24%
Injuries
9%
Diabetes
2%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile40
Marshall Islands
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 0.3 0.3
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 1280.1 1316.0
Cancers 100.7 129.0
Chronic respiratory diseases 135.1 107.1
Cardiovascular diseases and diabetes 818.5 831.4
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 31.6 3.8 17.3
Physical inactivity 46.3 57.1 51.7
2008 estimated prevalence (%) males females total
Raised blood pressure 37.4 28.4 32.7
Raised blood glucose 23.8 29.0 26.5
Overweight 77.4 81.0 79.2
Obesity 37.9 52.4 45.4
Raised cholesterol 42.8 45.9 44.4 NCDs are estimated to account for 73% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control No Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation No Diabetes Yes
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
* The mortality estimates for this country have a high degree of uncertainty because they are not based ** = covered by integrated policy/programme/action plan
on any national NCD mortality data. The estimates are based on a combination of country life tables,
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 54 038
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement1/5
52.2
NCD mortality*
42.8
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
Mean fasting blood glucose
Mean body mass index
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
40%
Respiratory
diseases
7%
Other NCDs
14%
Communicable,
maternal,
perinatal and
nutritional
conditions
22%
Cancers
7%Diabetes
5%
Injuries
5%
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 41
Micronesia (Federated States of)
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 0.2 0.2
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 753.7 622.8
Cancers 79.3 90.1
Chronic respiratory diseases 80.2 50.8
Cardiovascular diseases and diabetes 459.4 363.1
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 22.4 12.4 17.5
Physical inactivity 56.4 74.3 65.2
2008 estimated prevalence (%) males females total
Raised blood pressure 42.7 34.1 38.3
Raised blood glucose 12.8 18.3 15.6
Overweight 67.9 82.5 75.2
Obesity 28.1 53.2 40.6
Raised cholesterol 47.1 45.4 46.2 NCDs are estimated to account for 67% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control No Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
* The mortality estimates for this country have a high degree of uncertainty because they are not based ** = covered by integrated policy/programme/action plan
on any national NCD mortality data. The estimates are based on a combination of country life tables,
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 111 064
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
38.8
NCD mortality*
37.0
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
118
120
122
124
126
128
130
132
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
5.2
5.4
5.6
5.8
6.0
6.2
6.4
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
22
24
26
28
30
32
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.2
4.4
4.6
4.8
5.0
5.2
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
35%
Cancers
8%Other NCDs
14%
Communicable,
maternal,
perinatal and
nutritional
conditions
28%
Injuries
5%
Diabetes
4%
Respiratory
diseases
6%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile42
Mongolia
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 6.1 4.8
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 867.7 569.0
Cancers 259.5 166.4
Chronic respiratory diseases 33.6 22.7
Cardiovascular diseases and diabetes 456.4 303.6
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 43.0 5.2 23.7
Physical inactivity 7.9 8.4 8.2
2008 estimated prevalence (%) males females total
Raised blood pressure 44.6 36.4 40.4
Raised blood glucose 9.7 7.8 8.7
Overweight 40.7 45.7 43.2
Obesity 10.4 18.3 14.4
Raised cholesterol 36.4 36.2 36.3 NCDs are estimated to account for 72% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
* The mortality estimates for this country have a high degree of uncertainty because they are not based ** = covered by integrated policy/programme/action plan
on any national NCD mortality data. The estimates are based on a combination of country life tables,
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 2 756 001
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
48.0
NCD mortality*
35.4
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
124
126
128
130
132
134
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.8
5.0
5.2
5.4
5.6
5.8
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
20
22
24
26
28
30
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.4
4.6
4.8
5.0
5.2
5.4
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
37%
Cancers
21%
Communicable,
maternal,
perinatal and
nutritional
conditions
14%
Injuries
13%
Other NCDs
12%
Diabetes
0%
Respiratory
diseases
3%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 43
Nauru
Income group: Upper middle
2008 estimates males females
Total NCD deaths (000s) 0.0 0.0
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 1367.4 845.5
Cancers 114.7 190.6
Chronic respiratory diseases 86.3 72.3
Cardiovascular diseases and diabetes 922.3 473.0
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 44.3 50.5 47.5
Physical inactivity 47.7 51.2 49.4
2008 estimated prevalence (%) males females total
Raised blood pressure 45.0 34.6 39.6
Raised blood glucose 11.6 13.3 12.5
Overweight 93.5 92.3 92.9
Obesity 67.7 74.4 71.1
Raised cholesterol 41.2 48.1 44.7 NCDs are estimated to account for 70% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control Yes Cancer No
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 10 255
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement1/5
54.0
NCD mortality
48.5
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
Mean fasting blood glucose
Mean body mass index
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
40%
Cancers
9%
Injuries
11%
Communicable,
maternal,
perinatal and
nutritional
conditions
19%
Other NCDs
12%
Respiratory
diseases
5%
Diabetes
4%
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile44
New Zealand
Income group: High
2008 estimates males females
Total NCD deaths (000s) 13.1 12.8
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 410.7 285.1
Cancers 149.1 110.8
Chronic respiratory diseases 30.1 20.5
Cardiovascular diseases and diabetes 171.2 106.1
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 21.4 20.1 20.7
Physical inactivity 45.9 50.2 48.1
2008 estimated prevalence (%) males females total
Raised blood pressure 40.8 33.0 36.8
Raised blood glucose ... ... ...
Overweight 69.2 62.6 65.8
Obesity 27.3 29.3 28.3
Raised cholesterol 57.5 57.9 57.7 NCDs are estimated to account for 91% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs No
There is funding available for: Cardiovascular diseases Yes
NCD treatment and control Yes Cancer Yes
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes
Alcohol Yes
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes
NCD cause-specific mortality Yes Physical inactivity Yes
NCD morbidity Yes Tobacco Yes
NCD risk factors Yes
Has a national, population-based cancer registry Yes
… = no data available
World Health Organization - NCD Country Profiles , 2011.
14.1
NCD mortality
11.1
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
2010 total population: 4 368 136
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement3/5
120
124
128
132
136
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.9
5.1
5.3
5.5
5.7
5.9
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
22
24
26
28
30
32
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
5.0
5.2
5.4
5.6
5.8
6.0
6.2
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
37%
Cancers
29%
Other NCDs
15%
Respiratory
diseases
7%
Diabetes
3%
Injuries
6%
Communicable,
maternal,
perinatal and
nutritional
conditions
3%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 45
Niue
Income group: Upper middle
2008 estimates males females
Total NCD deaths (000s) 0.0 0.0
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 790.3 314.6
Cancers 79.7 80.5
Chronic respiratory diseases 81.1 24.2
Cardiovascular diseases and diabetes 486.3 160.4
2008 estimated prevalence (%) males females total
Current daily tobacco smoking … … …
Physical inactivity ... ... ...
2008 estimated prevalence (%) males females total
Raised blood pressure ... ... ...
Raised blood glucose ... ... ...
Overweight … … …
Obesity … … …
Raised cholesterol … … … NCDs are estimated to account for 72% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control No Cancer DK
NCD prevention and health promotion Yes Chronic respiratory diseases DK
NCD surveillance, monitoring and evaluation No Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
… = no data available
** = covered by integrated policy/programme/action plan
DK = Country responded "don't know"
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 1 468
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
45.6
NCD mortality
21.3
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
Mean fasting blood glucose
Mean body mass index
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
36%
Cancers
11%Respiratory
diseases
7%
Other NCDs
13%
Injuries
8%
Communicable,
maternal,
perinatal and
nutritional
conditions
21%
Diabetes
4%
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile46
Palau
Income group: Upper middle
2008 estimates males females
Total NCD deaths (000s) 0.0 0.0
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 777.3 413.7
Cancers 91.4 105.3
Chronic respiratory diseases 78.7 27.9
Cardiovascular diseases and diabetes 469.6 214.8
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 33.0 7.1 19.7
Physical inactivity … … …
2008 estimated prevalence (%) males females total
Raised blood pressure ... ... ...
Raised blood glucose ... ... ...
Overweight ... ... ...
Obesity ... ... ...
Raised cholesterol … … … NCDs are estimated to account for 74% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control No Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation No Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity No Tobacco Yes**
NCD risk factors No
Has a national, population-based cancer registry No
* The mortality estimates for this country have a high degree of uncertainty because they are not based … = no data available
on any national NCD mortality data. The estimates are based on a combination of country life tables, ** = covered by integrated policy/programme/action plan
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 20 472
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
43.6
NCD mortality*
38.1
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
Mean fasting blood glucose
Mean body mass index
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
38%
Cancers
13%
Other NCDs
13%
Communicable,
maternal,
perinatal and
nutritional
conditions
20%
Respiratory
diseases
6%
Diabetes
4%
Injuries
6%
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 47
Papua New Guinea
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 11.1 9.1
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 836.9 664.7
Cancers 151.8 106.9
Chronic respiratory diseases 99.9 74.1
Cardiovascular diseases and diabetes 459.8 395.4
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 56.9 24.8 40.9
Physical inactivity 14.1 18.1 16.1
2008 estimated prevalence (%) males females total
Raised blood pressure 29.4 24.6 27.0
Raised blood glucose 13.4 13.2 13.3
Overweight 45.3 51.2 48.3
Obesity 11.7 20.6 16.2
Raised cholesterol 36.1 37.5 36.8 NCDs are estimated to account for 44% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry DK
* The mortality estimates for this country have a high degree of uncertainty because they are not based ** = covered by integrated policy/programme/action plan
on any national NCD mortality data. The estimates are based on a combination of country life tables, DK = Country responded "don't know"
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 6 858 266
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
49.1
NCD mortality*
48.4
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
108
110
112
114
116
118
120
122
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
5.1
5.3
5.5
5.7
5.9
6.1
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
18
20
22
24
26
28
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.0
4.2
4.4
4.6
4.8
5.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
21%
Cancers
8%
Communicable,
maternal,
perinatal and
nutritional
conditions
47%
Injuries
9%
Other NCDs
8%
Respiratory
diseases
5%
Diabetes
2%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile48
Philippines
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 175.7 133.9
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 711.6 482.8
Cancers 98.6 74.6
Chronic respiratory diseases 80.7 32.5
Cardiovascular diseases and diabetes 394.8 295.3
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 34.7 7.7 21.2
Physical inactivity 20.0 25.7 22.9
2008 estimated prevalence (%) males females total
Raised blood pressure 35.4 30.0 32.7
Raised blood glucose 5.7 5.9 5.8
Overweight 24.6 28.4 26.5
Obesity 4.6 8.0 6.3
Raised cholesterol 39.0 44.5 41.8 NCDs are estimated to account for 61% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases Yes**
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry Yes
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 93 260 798
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
44.4
NCD mortality
35.6
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
118
120
122
124
126
128
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.6
4.8
5.0
5.2
5.4
5.6
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
18
20
22
24
26
28
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.2
4.4
4.6
4.8
5.0
5.2
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
30%
Cancers
10%
Communicable,
maternal,
perinatal and
nutritional
conditions
30%
Other NCDs
13%
Respiratory
diseases
5%
Diabetes
4%
Injuries
8%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 49
Republic of Korea
Income group: High
2008 estimates males females
Total NCD deaths (000s) 112.3 96.7
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 465.0 246.8
Cancers 190.5 77.1
Chronic respiratory diseases 36.1 12.1
Cardiovascular diseases and diabetes 167.9 115.2
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 50.4 4.9 27.2
Physical inactivity … … …
2008 estimated prevalence (%) males females total
Raised blood pressure 33.3 28.0 30.6
Raised blood glucose 6.8 5.7 6.3
Overweight 34.3 29.2 31.8
Obesity 7.2 8.3 7.7
Raised cholesterol 42.2 44.1 43.2 NCDs are estimated to account for 82% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases Yes**
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry Yes
… = no data available
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 48 183 584
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement1/5
24.2
NCD mortality
12.5
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
117
119
121
123
125
127
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.9
5.1
5.3
5.5
5.7
5.9
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
18
20
22
24
26
28
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.2
4.4
4.6
4.8
5.0
5.2
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
29%
Cancers
30%
Diabetes
5%
Other NCDs
13%
Injuries
12%
Respiratory
diseases
5%
Communicable,
maternal,
perinatal and
nutritional
conditions
6%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile50
Samoa
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 0.4 0.4
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 772.1 583.2
Cancers 68.5 40.2
Chronic respiratory diseases 83.3 50.2
Cardiovascular diseases and diabetes 477.4 373.6
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 53.6 17.1 36.2
Physical inactivity 35.1 65.6 49.7
2008 estimated prevalence (%) males females total
Raised blood pressure 43.5 36.2 40.0
Raised blood glucose 19.7 22.5 21.1
Overweight 81.2 88.2 84.6
Obesity 43.6 65.5 54.1
Raised cholesterol 31.0 36.6 33.7 NCDs are estimated to account for 70% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control Yes Cancer No
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation Yes Diabetes No
Alcohol No
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes
NCD cause-specific mortality Yes Physical inactivity Yes
NCD morbidity Yes Tobacco No
NCD risk factors No
Has a national, population-based cancer registry No
* The mortality estimates for this country have a high degree of uncertainty because they are not based
on any national NCD mortality data. The estimates are based on a combination of country life tables,
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 183 081
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
36.1
NCD mortality*
27.7
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
118
120
122
124
126
128
130
132
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
5.0
5.3
5.6
5.9
6.2
6.5
6.8
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
24
26
28
30
32
34
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.0
4.2
4.4
4.6
4.8
5.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
37%
Cancers
6%Respiratory
diseases
7%
Diabetes
5%
Other NCDs
15%
Communicable,
maternal,
perinatal and
nutritional
conditions
25%
Injuries
5%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 51
Singapore
Income group: High
2008 estimates males females
Total NCD deaths (000s) 10.1 7.8
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 372.1 238.8
Cancers 141.6 90.9
Chronic respiratory diseases 22.6 7.2
Cardiovascular diseases and diabetes 171.2 108.9
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 25.1 4.0 14.5
Physical inactivity … … …
2008 estimated prevalence (%) males females total
Raised blood pressure 39.7 33.9 36.8
Raised blood glucose 8.0 5.9 6.9
Overweight 33.9 26.4 30.2
Obesity 7.0 7.1 7.1
Raised cholesterol 57.9 62.1 60.0 NCDs are estimated to account for 79% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases Yes**
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry Yes
… = no data available
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 5 086 418
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement2/5
24.4
NCD mortality
18.9
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
120
122
124
126
128
130
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
5.0
5.2
5.4
5.6
5.8
6.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
18
20
22
24
26
28
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.6
4.8
5.0
5.2
5.4
5.6
5.8
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
33%
Cancers
30%
Other NCDs
9%
Respiratory
diseases
4%
Diabetes
3%
Injuries
5%
Communicable,
maternal,
perinatal and
nutritional
conditions
16%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile52
Solomon Islands
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 0.8 0.6
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 709.7 524.3
Cancers 85.9 85.9
Chronic respiratory diseases 74.5 41.4
Cardiovascular diseases and diabetes 425.0 303.7
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 42.4 14.4 28.8
Physical inactivity 36.8 48.6 42.6
2008 estimated prevalence (%) males females total
Raised blood pressure 32.7 28.9 30.8
Raised blood glucose 14.3 15.4 14.9
Overweight 61.0 69.6 65.2
Obesity 22.6 37.7 30.0
Raised cholesterol 29.5 35.4 32.4 NCDs are estimated to account for 60% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control Yes Cancer No
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation No Diabetes Yes
Alcohol No
National health reporting system includes: Unhealthy diet / Overweight / Obesity No
NCD cause-specific mortality No Physical inactivity No
NCD morbidity No Tobacco No
NCD risk factors No
Has a national, population-based cancer registry No
* The mortality estimates for this country have a high degree of uncertainty because they are not based
on any national NCD mortality data. The estimates are based on a combination of country life tables,
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 538 148
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
38.8
NCD mortality*
38.7
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
115
117
119
121
123
125
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
5.1
5.3
5.5
5.7
5.9
6.1
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
22
24
26
28
30
32
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.0
4.2
4.4
4.6
4.8
5.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
29%
Cancers
10%
Respiratory
diseases
5%Other NCDs
12%
Communicable,
maternal,
perinatal and
nutritional
conditions
35%
Injuries
5%
Diabetes
4%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 53
Tonga
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 0.2 0.3
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 649.3 672.6
Cancers 67.4 93.9
Chronic respiratory diseases 68.8 53.2
Cardiovascular diseases and diabetes 395.9 395.0
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 36.6 7.5 22.0
Physical inactivity 30.6 52.1 41.4
2008 estimated prevalence (%) males females total
Raised blood pressure 42.1 38.0 40.1
Raised blood glucose 15.8 19.1 17.5
Overweight 84.2 89.9 87.0
Obesity 46.6 68.5 57.6
Raised cholesterol 52.5 44.9 48.7 NCDs are estimated to account for 74% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer No
NCD prevention and health promotion Yes Chronic respiratory diseases Yes**
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry No
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 104 058
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
25.6
NCD mortality
35.1
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
117
119
121
123
125
127
129
131
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
5.3
5.5
5.7
5.9
6.1
6.3
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
25
27
29
31
33
35
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.4
4.6
4.8
5.0
5.2
5.4
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
38%
Respiratory
diseases
7%
Other NCDs
15%
Cancers
9%Diabetes
5%
Communicable,
maternal,
perinatal and
nutritional
conditions
22%
Injuries
4%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile54
Tuvalu
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 0.0 0.0
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 992.3 991.9
Cancers 106.9 153.8
Chronic respiratory diseases 98.4 77.3
Cardiovascular diseases and diabetes 605.8 568.0
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 47.8 15.5 32.0
Physical inactivity … … …
2008 estimated prevalence (%) males females total
Raised blood pressure ... ... ...
Raised blood glucose ... ... ...
Overweight … … …
Obesity … … …
Raised cholesterol … … … NCDs are estimated to account for 73% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases No
NCD treatment and control Yes Cancer Yes
NCD prevention and health promotion Yes Chronic respiratory diseases No
NCD surveillance, monitoring and evaluation No Diabetes Yes
Alcohol No
National health reporting system includes: Unhealthy diet / Overweight / Obesity No
NCD cause-specific mortality Yes Physical inactivity No
NCD morbidity Yes Tobacco Yes
NCD risk factors No
Has a national, population-based cancer registry No
… = no data available
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 9 827
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
36.6
NCD mortality
37.0
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
Mean fasting blood glucose
Mean body mass index
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
38%
Cancers
10%Respiratory
diseases
6%
Other NCDs
15%
Diabetes
5%
Communicable,
maternal,
perinatal and
nutritional
conditions
21%
Injuries
5%
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available
1980 1984 1988 1992 1996 2000 2004 2008
No Data Available

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 55
Vanuatu
Income group: Lower middle
2008 estimates males females
Total NCD deaths (000s) 0.5 0.3
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 767.8 576.8
Cancers 94.7 94.3
Chronic respiratory diseases 79.5 44.8
Cardiovascular diseases and diabetes 462.4 333.4
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 21.3 3.1 12.3
Physical inactivity … … …
2008 estimated prevalence (%) males females total
Raised blood pressure 44.5 39.1 41.8
Raised blood glucose 8.1 8.0 8.0
Overweight 59.2 65.7 62.4
Obesity 21.0 34.2 27.5
Raised cholesterol … … … NCDs are estimated to account for 70% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases Yes**
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol Yes**
National health reporting system includes: Unhealthy diet / Overweight / Obesity Yes**
NCD cause-specific mortality Yes Physical inactivity Yes**
NCD morbidity Yes Tobacco Yes**
NCD risk factors Yes
Has a national, population-based cancer registry Yes
* The mortality estimates for this country have a high degree of uncertainty because they are not based … = no data available
on any national NCD mortality data. The estimates are based on a combination of country life tables, ** = covered by integrated policy/programme/action plan
cause of death models, regional cause of death patterns, and WHO and UNAIDS program estimates
for some major causes of death (not including NCDs).
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 239 651
Proportional mortality (% of total deaths, all ages)*
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
37.9
NCD mortality*
42.0
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
122
124
126
128
130
132
134
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.4
4.6
4.8
5.0
5.2
5.4
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
20
22
24
26
28
30
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.2
4.4
4.6
4.8
5.0
5.2
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
36%
Cancers
12%Respiratory
diseases
6%
Other NCDs
13%
Diabetes
4%
Communicable,
maternal,
perinatal and
nutritional
conditions
24%
Injuries
5%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile56
Viet Nam
Income group: Low
2008 estimates males females
Total NCD deaths (000s) 208.0 222.0
NCD deaths under age 60
(percent of all NCD deaths)
All NCDs 687.2 508.2
Cancers 137.3 94.3
Chronic respiratory diseases 76.6 45.5
Cardiovascular diseases and diabetes 381.5 298.2
2008 estimated prevalence (%) males females total
Current daily tobacco smoking 40.4 1.0 20.1
Physical inactivity 14.2 15.6 14.9
2008 estimated prevalence (%) males females total
Raised blood pressure 36.0 30.0 33.0
Raised blood glucose 6.6 7.2 6.9
Overweight 9.5 10.9 10.2
Obesity 1.2 2.1 1.7
Raised cholesterol … … … NCDs are estimated to account for 75% of all deaths.
Country capacity to address and respond to NCDs
Has a Unit / Branch / Dept in MOH with responsibility for NCDs Yes
There is funding available for: Cardiovascular diseases Yes**
NCD treatment and control Yes Cancer Yes**
NCD prevention and health promotion Yes Chronic respiratory diseases Yes
NCD surveillance, monitoring and evaluation Yes Diabetes Yes**
Alcohol No
National health reporting system includes: Unhealthy diet / Overweight / Obesity No
NCD cause-specific mortality Yes Physical inactivity No
NCD morbidity Yes Tobacco Yes
NCD risk factors No
Has a national, population-based cancer registry No
… = no data available
** = covered by integrated policy/programme/action plan
World Health Organization - NCD Country Profiles , 2011.
2010 total population: 87 848 445
Proportional mortality (% of total deaths, all ages)
Has an integrated or topic-specific policy / programme / action
plan which is currently operational for:
Number of tobacco (m)POWER measures
implemented at the highest level of achievement0/5
26.4
NCD mortality
19.4
Metabolic risk factor trends
Age-standardized death rate per 100 000
Behavioural risk factors
Metabolic risk factors
116
118
120
122
124
126
1980 1984 1988 1992 1996 2000 2004 2008
mm
Hg
4.6
4.8
5.0
5.2
5.4
5.6
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean fasting blood glucose
16
18
20
22
24
26
1980 1984 1988 1992 1996 2000 2004 2008
kg
/m2
Mean body mass index
4.0
4.2
4.4
4.6
4.8
5.0
1980 1984 1988 1992 1996 2000 2004 2008
mm
ol/l
Mean total cholesterol
Males
Mean systolic blood pressure
Females
CVD
40%
Cancers
14%
Respiratory
diseases
8%
Other NCDs
10%
Diabetes
3%
Communicable,
maternal,
perinatal and
nutritional
conditions
16%
Injuries
9%

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 57
6. key findings and recommendations
NCDs are a major public health problem in all countries of the Region. Age-standardized death rates show a wide variation among countries, indicating a large potential for reducing NCD mortality. The high proportion of NCD deaths among people under 70 years in LMIC is of concern. Cause-specific mortality data, with International Classification of Diseases (ICD) coding, are required for monitoring NCD mortality and serve as unbiased indicators of the effectiveness of the overall NCD prevention and control programme. Mortality registration and certification should be strengthened, especially in LMIC, as it is an important basis for implementing and monitoring NCD programmes, as well as for assessing other health programmes.
There is a two- to three-fold variation in cancer incidence in the Region. HIC have managed to reduce the incidence of cervical cancer through screening, early detection and prompt management. Population-based disease registries are available for cancer in many HIC. However, there are many challenges in establishing population-based disease registries in LMIC; hospital-based registries offer an entry point prior to coverage of a defined catchment population.
Trends in NCD risk factors serve as indicators of the effectiveness of risk reduction programmes. Collection of comparable data in a periodic manner is essential for measuring trends between and within countries. WHO STEPS offers a standardized approach that can be adopted by countries.
WHO has proposed a framework for a national NCD surveillance scheme with three major components as given in Box 1.
Box 1. Framework for national NCD surveillance
exposures Behavioural risk factors: tobacco use, physical inactivity, the harmful use of alcohol and unhealthy diet.Physiological and metabolic risk factors: raised blood pressure, overweight/obesity, raised blood glucose, and raised cholesterol.Social determinants: educational level, household income, and access to health care.
Outcomes Mortality: NCD-specific mortality.Morbidity: Cancer incidence and type (as core).
Health system capacity and response Interventions and health system capacity: infrastructure, policies and plans, access to key health-care interventions and treatments, and partnerships.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile58
There has been substantial progress in the overall country capacity for NCD prevention and management in the Region. The profile has not gone into an analytical approach as the data on country capacity were limited to availability of policies and programmes and did not include detailed information on implementation.
Interventions to prevent NCDs on a population-wide basis are not only feasible but also cost-effective. Low-cost solutions can work anywhere to reduce the major risk factors for NCDs. While many interventions may be cost-effective, some are considered “best buys”—actions that should be undertaken immediately to produce accelerated results in terms of lives saved, diseases prevented and heavy costs avoided. A set of best buys and cost-effective interventions from the Global status report on noncommunicable diseases 2010, as listed below, can be considered as priority interventions.
Best buys include:
• protecting people from tobacco smoke and banning smoking in public places;• warning about the dangers of tobacco use;• enforcing bans on tobacco advertising, promotion and sponsorship;• raising taxes on tobacco;• restricting access to retailed alcohol;• enforcing bans on alcohol advertising;• raising taxes on alcohol;• reducing salt intake and salt content of food;• replacing trans-fat in food with polyunsaturated fat; and• promoting public awareness about diet and physical activity, including through mass media.
Cost-effective approaches in individual health care interventions include:
• counselling and multidrug therapy, including glycaemic control for diabetes for people older than 30 years with a 10-year risk of fatal or nonfatal cardiovascular events;
• aspirin therapy for acute myocardial infarction;• screening for cervical cancer, once at age 40, followed by removal of any discovered cancerous
lesion;• early case finding for breast cancer through biennial screening with mammography (for
women aged 50–70 years) and treatment of all stages;• early detection of colorectal and oral cancer; and• treatment of persistent asthma with inhaled corticosteroids and beta-2 agonists.
Given the health and economic burden caused by NCDs and the urgent need to scale up action and monitor progress, countries should move towards time-bound targets and improved monitoring frameworks for NCD prevention and control.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 59
Annexes
ANNex 1 - RegIONAL COMMItMeNts ON NCD
seOuL DeCLARAtION ON NONCOMMuNICABLe DIseAse PReveNtION AND CONtROL IN tHe WesteRN PACIFIC RegION
18 March 2011
Recognizing the serious and rapidly increasing adverse impact of noncommunicable diseases (NCD), including cardiovascular diseases, cancers, diabetes and chronic respiratory diseases, on individuals, families, communities, health systems and national economies, and the high prevalence of the major risk factors, the countries and areas of the WHO Western Pacific Region participating at the Regional High-level Meeting on Scaling Up Multisectoral Action for Noncommunicable Disease Prevention and Control, declare their commitment to:
(1) provide strong and sustained high-level political support for NCD prevention and control to reduce premature NCD death and disability and health inequalities;
(2) ensure a supportive multisectoral whole-of-government policy environment across all levels of government and a coordinating mechanism to mainstream the response to NCD involving all stakeholders, including civil society and, where appropriate, the private sector to protect health over commercial and other vested interests and to ensure that healthy choices are the easiest choices;
(3) reduce the common modifiable NCD risk factors (tobacco use; diets high in saturated fats and trans-fats, salt and sugar; the harmful use of alcohol; and physical inactivity); and• in line with the WHO global and regional action plans and using the full range of
mechanisms including legislation, regulation, fiscal measures and healthy public policies and, in particular, accelerate the full implementation of the WHO Framework Convention on Tobacco Control; and
• by addressing the social determinants of health and by leveraging the power of local governments and civil society actions;
(4) strengthen and integrate health systems, based on primary health care to ensure that NCD prevention and control is part of a funded coherent, balanced, realistic and comprehensive health planning process that is financially feasible and to:• deliver services for NCD and their risk factors utilizing team-based care and the most
appropriate professional health care for the patient’s needs, including affordable and cost-effective drugs and technologies to support evidence-based priority interventions; and
• work towards continuity of quality care from prevention to palliation across all components of health systems and promote a people-centred approach;
(5) prioritize human and financial resources and infrastructure to ensure equitable coverage of complementary priority evidence-based NCD prevention and control interventions, including resource mobilization through innovative financing mechanisms; and
(6) provide integrated but practical monitoring and accountability systems based on strengthened health information systems and a small number of quantified and timed targets and indicators to assess progress nationally to be reported publicly and to the United Nations General Assembly and other appropriate forums.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile60
In support of these commitments, participating countries and areas request the global community, through the UN High-level Meeting on the Prevention and Control of Noncommunicable Diseases, to act in a coordinated way to facilitate global and national multisectoral actions by:
(1) raising the priority of NCD on their agendas;(2) strengthening synergies between NCD programmes and other development priorities,
including the Millennium Development Goals and the future global development agenda; and
(3) mobilizing additional resources and supporting innovative approaches to financing NCD prevention and control.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 61
HONIARA COMMuNIQuÉ ON tHe PACIFIC NONCOMMuNICABLe DIseAse CRIsIs9th Meeting of Ministers of Health for the Pacific Island Countries
30 June 2011
Ministers of Health for the Pacific island countries are gravely concerned that the rapid increase in the incidence and prevalence of noncommunicable disease (NCD) in the Pacific island countries and areas over the past decade is responsible for up to 75% of all deaths and a similar percentage of long-term illness and disability, and declared at their 9th Meeting in Honiara, Solomon Islands, on 28–30 June 2011 that the Pacific island countries and areas are in an NCD crisis requiring urgent attention.
Pacific island countries and areas are in crisis due to an epidemic of noncommunicable disease (NCD) such as heart disease, cancer and diabetes. The burden of NCD in the region is already extremely high, causing up to 75% of deaths and much long-term illness and disability. Our prevalence of NCD risk factors are among the highest in the world—up to three of every four adults are obese and up to four of every five adults smoke—meaning that without real action things will only get worse.
The Pacific NCD crisis is not just a concern for the health of our people. It drains limited national budgets, reduces worker productivity, separates families, and robs communities of leadership and wisdom, as adults suffer long-term illness and die early. While adult NCD rates continue to rise, the next generation—more overweight and less active than any other Pacific generation in history—is the tsunami of the future. High childhood obesity rates in the Pacific, if left unchecked, suggest that a true health catastrophe is just a generation away.
There is hope, however. There has been some early progress in the fight against NCD, and effective actions are available across a spectrum ranging from prevention to early detection and treatment. But what is missing is a sense of urgency in the region, and the recognition among Pacific island countries and areas that a whole-of-government and whole-of-society approach is needed to tackle this health and development crisis.
There is a great opportunity this year with the United Nations General Assembly holding a High-level Meeting on the Prevention and Control of Noncommunicable Diseases from 19–20 September 2011 in New York. In the lead-up to this meeting, there have already been a number of key regional and global meetings that have considered the NCD crisis. The resulting Nadi Statement and Moscow Declaration made important recommendations on ways forward and this communiqué builds on those important initiatives. We have an opportunity to address this crisis if we act now.
Recognizing the fundamental importance of the upcoming United Nations High-level Meeting in tackling this crisis at the global level, and the need for the outcomes of this meeting to reflect Pacific realities, we call on the outcome document of the High-level Meeting to include the following:
• recognize NCD as a crisis in the Pacific to be addressed with the utmost urgency; • address the need for better information and guidance on cost-effective interventions in
resource-limited settings;• initiate and sustain effective action across the life-course; • ensure sustainable resourcing for NCD prevention, treatment and control;

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile62
• adopt a small number of global and publicly reported targets for NCD that can be adapted to national context; and
• initiate multisectoral action at the international level to complement national level action, and make an explicit expectation that international organizations will work together in a coordinated way to tackle NCD.
And in support of these recommendations, consistent with the Pacific Plan endorsed by the leaders of the Pacific Islands Forum at their October 2005 meeting and in support of our goal of Healthy Islands, we, the Ministers of Health for the Pacific island countries and areas, declare our commitment to the following critical actions:
(1) provide strong and sustained leadership and support for NCD prevention and control; (2) lead the advocacy for a whole-of-government and whole-of-society response and a coordinating
mechanism to mainstream the response to NCD; (3) ensure implementation of evidence-based initiatives to reduce the common modifiable NCD risk
factors across the life-course, and address the social determinants of health, including leveraging the power of local government and civil society, with a focus on interventions across the life-course;
(4) strengthen health systems, based on primary health care, to ensure that effective NCD prevention and control is funded and part of a coherent, balanced, realistic and comprehensive programme of health services as reflected in a costed national health plan;
(5) ensure monitoring and accountability systems are in place, along with a small number of quantified and timed national targets, with progress to be reported publicly; and
(6) fully implement the WHO Framework Convention on Tobacco Control as a critical step in reducing the impact of tobacco use on the prevalence of NCD.
Recognizing that many of the factors underlying this pandemic are outside the control of the health sector, and that as a result a whole-of-government, whole-of-society and whole-of- region response is needed, we also call on the Pacific Forum Leaders to give the highest priority to NCD, and to lead and champion tackling the crisis in the Pacific by:
(1) declaring NCD as a health and development crisis;(2) driving a whole-of-government and whole-of-society response involving all sectors;(3) integrating NCD prevention and control into national development agendas; (4) mobilizing additional resources locally and internationally to support the fight against NCD;(5) setting national targets for NCD and regularly and publicly reporting results;(6) calling on all Council of Regional Organizations in the Pacific (CROP) agencies and regional
health agencies to play an active part in a coordinated regional response to the crisis, and to report back every two years to Pacific Islands Forum Leaders on actions and progress;
(7) considering setting an ambitious regional tobacco elimination target, inspired by (8) New Zealand’s smoke-free by 2025 goal; and (9) championing the cause of prevention and control of this NCD epidemic.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 63
ANNex 2 - exPLORAtORy NOtes ON COuNtRy estIMAtes
Mortality
Age- and sex-specific all-cause mortality rates were estimated for the year 2008 for the 193 WHO Member States from revised life tables, published in World Health Statistics 2011. Total deaths by age and sex were estimated for each country by applying these death rates to the estimated resident populations prepared by the United Nations Population Division in its 2008 revision. To calculate causes of death for countries with complete or incomplete death registration data, vital registration data were used to estimate deaths by cause. Death registration data from 1980 up to 2008 (if available) were used to project recent trends for specific causes, and these trend estimates were used to estimate the cause distribution for 2008. Adjustments for deaths due to HIV, drug use disorders, war and natural disasters were based on other sources of information using similar data sources and methods as previous estimates.
For countries without any nationally representative data, cause-specific estimates of deaths for children under age 5 were estimated as described by Black et al. For ages five years and over, previous estimated distributions of deaths by cause were projected forward from 2004 to 2008, excluding human immunodeficiency virus (HIV), war and natural disasters. Detailed proportional cause distributions within the three broad groups were based on death registration data from within each region. Further information on these methods is available from WHO. Specific causes were further adjusted on the basis of epidemiological evidence from registries, verbal autopsy studies, disease surveillance systems and analyses from WHO technical programmes. Cause-specific estimates for HIV, tuberculosis and malaria deaths for 2008 were derived from previously published WHO estimates. Country-specific estimates of maternal mortality and cause-specific maternal mortality were based on the recent estimates for 2008 together with an analysis of regional cause patterns.
Risk factors
The crude adjusted estimates presented are based on aggregated data provided by countries to WHO or obtained through a review of published and unpublished literature. The inclusion criteria for estimation analysis stipulated that data had to come from a random sample of the general population, with clearly indicated survey methods (including sample sizes) and risk factor definition.
Adjustments were made for the following factors so that the same indicator could be reported for a standard year (in this case 2008) in all countries: standard risk factor definition; standard set of age groups for reporting; standard reporting year, and representativeness of population. Using regression modelling techniques, crude adjusted rates were produced for each indicator. Additionally, means for each of the four metabolic indicators were also estimated for the years 1980-2009. These means are presented in the risk factor trend graphs. Uncertainty in the estimates was analysed by taking into account sampling error and uncertainty due to statistical modelling. Further detailed information on the methods and data sources used to produce these estimates is available from WHO.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile64
Prevalence estimates for the year 2008 are given for the following behavioural and metabolic risk factors:
• Current daily tobacco smoking: the percentage of the population aged 15+ years who currently smoke tobacco on a daily basis.
• Physical inactivity: the percentage of the population aged 15+ years engaging in less than 30 minutes of moderate activity per week or less than 3 times 20 minutes of vigorous activity per week, or the equivalent.
• Raised blood pressure: the percentage of the population aged 25+ years having systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥90 mmHg or on medication to lower blood pressure.
• Raised blood glucose: the percentage of the population aged 25+ years having a fasting plasma glucose value ≥ 7.0 mmol/L (126 mg/dl) or on medication for raised blood glucose.
• Overweight: the percentage of the population aged 20+ years having a body mass index (BMI) ≥ 25 kg/m2.
• Obesity: the percentage of the population aged 20+ years having a body mass index (BMI) ≥ 30 kg/m2.
• Raised cholesterol: the percentage of the population aged 25+ years having a total cholesterol value ≥ 5.0 mmol/L (190 mg/dl).
Country Capacity survey
All information provided in this section of the profile, with the exception of the indicator on the highest level of implementation of the tobacco (m)POWER measures, were taken from country responses to the recent WHO NCD country capacity survey (CCS). Conducted in 2009-2010, the NCD CCS was undertaken by WHO to update the information about individual country capacity to respond to NCD prevention and control. An excel-based questionnaire was sent to the NCD focal points (i.e. the person responsible for the prevention and control of NCDs) or designated colleagues within the Ministry of Health or a national institute/agency in all 37 countries and areas in the Region. The questionnaire was sent in 2009 and the focal points were requested to respond by end of March 2010, but responses were accepted until June 2010. Thirty-five countries and areas responded to the survey, compared to 29 in 2004. The questionnaires used were not completely identical, but some questions on key indicators were unchanged. Just prior to this publication, countries were given the opportunity to update their profiles, with a closing date of July 2011. All countries and areas, except Pitcairn Islands and Wallis and Futuna, completed the questionnaire.
the questionnaire is composed of 5 domains and is discussed briefly below.
Public Health InfrastructureThis domain queried countries about having a designated NCD unit/branch/department within the Ministry of Health (or its equivalent), the designated unit’s responsibilities, and the existence of an established budget allocation to sustain this unit’s operations.
Status of NCD Policies, Strategies and Action PlansThis section queried countries about the existence of integrated NCD policies/strategies and action plans and the inclusion of key components in the policies/strategies/action plans as well as separate policies for individual risk factors. The questionnaire also asked about the availability of budgetary resources to implement the policies/strategies/action plans.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 65
Health Reporting/Information Systems, Monitoring and SurveillanceThis section of the assessment questionnaire queried countries about the inclusion of NCD-related data into national health reporting mechanisms, the existence of NCD registries, and the conduct of risk factor surveys.Health System Capacity for NCD Prevention, Early Detection, Treatment and Care within the Primary Health Care SystemThis section queried countries on the integration of the various components of the spectrum of NCD-related health interventions into the primary health care system and factors within the health care system affecting the management of NCDs.
Health Promotion, Partnerships, and CollaborationThis section covers the health promotion initiatives, partnerships and collaboration related to NCDs. These include the mechanisms for partnership, the stakeholders, and the content areas of these collaborations.
Country Profiles
The 2010 population estimates from the most recent United Nations Population Division World Population Prospects are reported in each profile. For income category, the 2008 World Bank income categories are reported.
In addition to the methods as stated under Country Capacity Survey above, information about the MPOWER package of six evidence-based tobacco control measures was included in the country profiles. To help countries fulfil their WHO FCTC obligations, WHO, in 2008, introduced the MPOWER that are proven to reduce tobacco use. MPOWER refers to M: Monitoring tobacco use and prevention policies; P: Protecting people from tobacco smoke; O: Offering help to quit tobacco use; W: Warning about the dangers of tobacco; E: Enforcing bans on tobacco advertising, promotion and sponsorship; and R: Raising taxes on tobacco. Each measure reflects one or more provisions of the WHO FCTC, and the package of six measures is an important entry point for scaling up efforts to reduce the demand for tobacco.
The NCD profile includes an assessment of progress in countries to implement only the POWER measures. (W focussed on Health Warnings only). Data for assessing the progress of Member States against the POWER measures were gathered by WHO from various country-level sources. These included original tobacco control legislation documents, detailed information on cessation services, mass media campaigns, cigarette prices and tobacco-related tax and revenues.
The final data for each country were sent to the respective government for review and signoff. In cases where national authorities explicitly did not approve the data, this is noted in the WHO Report on the Global Tobacco Epidemic, 2011.
Using these data, countries were then assessed at the highest level of achievement if they met the best-practice criteria for each POWER measure. A full description of these criteria can be found in the WHO Report on the Global Tobacco Epidemic, 2011 (13). For each of the POWER measures, countries were allocated a score of 1 if they were assessed by WHO as having attained the highest level of achievement, else a score of 0. This means that each individual country score is out of a total of 5 with a minimum of 0/5 to a maximum of 5/5.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile66
Cancer
Method used to estimate incidence cases and deaths by country in GLOBOCAN
Member States Incidence Mortality
Australia National incidence rates (1986-2005) projected to 2008 and applied to 2008 population. The numbers were scaled to the estimated total number of new cancer cases by sex provided by the Australian Institute of Health and Welfare for 2008.
National mortality rates (1985-2004, source WHO) projected to 2008 and applied to 2008 population.
Brunei Darussalam Local incidence data and national mortality data: incidence was estimated from national mortality by modelling, using incidence mortality ratios derived from recorded data in local cancer registries in neighbouring countries
Local incidence data and national mortality data: incidence was estimated from national mortality by modelling, using incidence mortality ratios derived from recorded data in local cancer registries in neighbouring countries
Cambodia Frequency data: age/sex specific incidence rates for all cancers were partitioned using data on relative frequency of different cancers (by age and sex) obtained from local source.
No data: the number of cancer deaths was estimated from incidence estimates and site specific survival, provided by neighbouring countries.
China Local incidence data and national mortality data: incidence was estimated from national mortality by modelling, using incidence mortality ratios derived from recorded data in country-specific cancer registries.
Sample mortality data: estimated national mortality for 2008 for “all cancers” (WHO) was partitioned by site and age using the sample mortality data.
Fiji National incidence rates observed in the Fiji Cancer Registry (1991-1999) were applied to the 2008 population
The number of cancer deaths in 2008 was estimated from incidence estimates and site specific survival, estimated by the GDP method.
Japan Sample mortality data: estimated national mortality for 2008 for “all cancers” (WHO) was partitioned by site and age using the sample mortality data.
National mortality data: recorded mortality in 2008.
Korea, Republic of National incidence rates (2000-2007) projected to 2008 (except for thyroid cancer for which incidence rates for 2007 were applied to 2008 population).
National mortality rates (2000-2007, source WHO) projected to 2008
Lao People’s Democratic Republic
Simple mean of rates observed in the cancer registries of Khon Kaen and Chiang Mai (Thailand).
Mortality was estimated from the 2008 national incidence estimate, using site specific relative survival from Thai and Chinese cancer registries. The number of cancer deaths (all ages) was partitioned by sex and age using proportions from Chinese cancer registries mortality files.
Malaysia Simple mean of incidence rates recorded in peninsular Malaysia (2003), Penang (1998-2002) and Sarawak (1998-2002).
The number of cancer deaths in 2008 was estimated from incidence estimates and site specific survival, estimated by the GDP method.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 67
Mongolia National incidence data: reliable estimates of the national incidence in 2008.
National mortality data: recorded mortality in 2008.
New Zealand National incidence rates (1986-2005) projected to 2008 and applied to the 2008 population
National mortality rates (1986-2005, source WHO) projected to 2008 and applied to the 2008 population.
Papua New Guinea Frequency data: age/sex specific incidence rates for all cancers were partitioned using data on relative frequency of different cancers (by age and sex).
No data: the number of cancer deaths was estimated from incidence estimates and site specific survival, estimated by the GDP method.
Philippines Local incidence data and national mortality data: incidence was estimated from national mortality by modelling, using incidence mortality ratios derived from recorded data in local cancer registries in neighbouring countries.
Sample mortality data: estimated national mortality for 2008 for “all cancers” (WHO) was partitioned by site and age using the sample mortality data.
Samoa National incidence rates (1981-1987) applied to the population (2008).
Estimated incidence for 2008 was converted to mortality using mortality incidence ratios obtained by the aggregation of data from French Polynesia and Guam.
Singapore National incidence data: incidence rates projected to 2008
National mortality data: mortality rates projected to 2008
Solomon islands No data: Incidence was estimated as the simple mean of the country-specific estimates for Fiji and Vanuatu.
No data: the number of cancer deaths was estimated from incidence estimates and site specific survival, estimated by the GDP method.
Vanuatu Mortality rates (1998-2002, provided by cancer registry) applied to the population (2008)
The number of cancer deaths in 2008 was estimated from incidence estimates and site specific survival, estimated by the GDP method.
Viet Nam Local incidence data and national mortality data: incidence was estimated from national mortality by modelling, using incidence mortality ratios derived from recorded data in local cancer registries in neighbouring countries
Sample mortality data: estimated national mortality for 2008 for “all cancers” (WHO) was partitioned by site and age using the sample mortality data.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile68
Coun
try
Tota
l NCD
de
aths
(‘00
0s)
NCD
dea
ths
unde
r ag
e 70
(p
erce
nt o
f all
NCD
dea
ths)
Age
-sta
ndar
dize
d de
ath
rate
per
100,
000
(Mal
es)
Age
-sta
ndar
dize
d de
ath
rate
per
100,
000
(Fem
ales
)La
test
ye
ar o
f D
ata
Mal
esfe
mal
esM
ales
fem
ales
All
NCD
sCa
ncer
sCR
DCV
D a
nd
diab
etes
All
NCD
sCa
ncer
sCR
DCV
D a
nd
diab
etes
Aust
ralia
63.4
63.2
28.8
18.6
364.
814
0.8
25.6
136.
324
6.3
92.9
15.5
88.6
2006
Brun
ei D
arus
sala
m0.
50.
559
.146
.453
4.3
97.0
69.0
292.
748
8.7
98.1
44.0
275.
420
08Ca
mbo
dia*
31.1
25.5
77.1
56.6
957.
914
4.9
129.
048
0.4
592.
290
.060
.433
8.7
no d
ata
Chin
a43
23.3
3675
.543
.932
.066
5.2
182.
311
8.4
311.
549
5.2
105.
088
.725
9.6
2007
Cook
isla
nds
0.0
0.0
61.0
52.5
592.
058
.661
.335
0.7
326.
357
.426
.318
0.0
2001
Fiji
2.4
1.8
71.5
61.1
928.
410
6.2
91.1
579.
959
0.9
121.
644
.232
8.2
2000
Japa
n47
3.2
435.
529
.315
.733
6.7
150.
522
.511
8.1
178.
176
.68.
065
.020
08Ki
ribat
i0.
30.
277
.766
.583
2.4
39.0
61.8
425.
954
8.3
64.2
19.1
223.
820
02La
o Pe
ople
’s D
emoc
ratic
Re
publ
ic, t
he*
12.1
11.7
60.3
53.0
849.
414
5.4
122.
846
7.9
689.
011
1.1
103.
439
2.8
no d
ata
Mal
aysi
a50
.439
.158
.446
.060
5.7
118.
874
.731
8.7
436.
589
.942
.123
6.5
2006
Mar
shal
l Isl
ands
, the
*0.
30.
380
.370
.612
80.1
100.
713
5.1
818.
513
16.0
129.
010
7.1
831.
4no
dat
aM
icro
nesi
a, th
e Fe
dera
ted
Stat
es o
f*0.
20.
255
.851
.275
3.7
79.3
80.2
459.
462
2.8
90.1
50.8
363.
1no
dat
a
Mon
golia
*6.
14.
869
.254
.786
7.7
259.
533
.645
6.4
569.
016
6.4
22.7
303.
6no
dat
aN
auru
0.0
0.0
72.5
69.9
1367
.411
4.7
86.3
922.
384
5.5
190.
672
.347
3.0
1996
New
Zea
land
13.1
12.8
29.9
22.1
410.
714
9.1
30.1
171.
228
5.1
110.
820
.510
6.1
2007
Niu
e0.
00.
064
.036
.679
0.3
79.7
81.1
486.
331
4.6
80.5
24.2
160.
420
00Pa
lau*
0.0
0.0
64.2
66.8
777.
391
.478
.746
9.6
413.
710
5.3
27.9
214.
8no
dat
aPa
pua
New
Gui
nea*
11.1
9.1
72.2
69.0
836.
915
1.8
99.9
459.
866
4.7
106.
974
.139
5.4
no d
ata
Phili
ppin
es17
5.7
133.
967
.655
.071
1.6
98.6
80.7
394.
848
2.8
74.6
32.5
295.
320
03Re
publ
ic o
f Kor
ea, t
he11
2.3
96.7
45.1
23.5
465.
019
0.5
36.1
167.
924
6.8
77.1
12.1
115.
220
06Sa
moa
*0.
40.
455
.643
.777
2.1
68.5
83.3
477.
458
3.2
40.2
50.2
373.
6no
dat
aSi
ngap
ore
10.1
7.8
46.0
34.9
372.
114
1.6
22.6
171.
223
8.8
90.9
7.2
108.
920
08So
lom
on is
land
s*0.
80.
661
.158
.170
9.7
85.9
74.5
425.
052
4.3
85.9
41.4
303.
7no
dat
aTo
nga
0.2
0.3
45.9
53.0
649.
367
.468
.839
5.9
672.
693
.953
.239
5.0
1998
Tuva
lu0.
00.
063
.156
.399
2.3
106.
998
.460
5.8
991.
915
3.8
77.3
568.
020
00Va
nuat
u*0.
50.
360
.362
.276
7.8
94.7
79.5
462.
457
6.8
94.3
44.8
333.
4no
dat
aVi
et N
am20
8.0
222.
042
.732
.468
7.2
137.
376
.638
1.5
508.
294
.345
.529
8.2
2008
AN
Nex
3 -
200
8 CO
MPA
RABL
e es
tIM
Ates
OF
NCD
MO
RtA
LIty
Not
e: C
ount
ries
with
ast
eris
k ha
ve fi
gure
s w
ith a
hig
h de
gree
of u
ncer
tain
ty b
ecau
se th
ey a
re n
ot b
ased
on
any
natio
nal N
CD
mor
talit
y da
ta. T
he e
stim
ates
for t
hese
cou
ntrie
s ar
e ba
sed
on a
com
bina
tion
of c
ount
ry li
fe ta
bles
, ca
use
of d
eath
mod
els,
regi
onal
cau
se o
f dea
th p
atte
rns,
and
WH
O a
nd U
NA
IDS
pro
gram
me
estim
ates
for s
ome
maj
or c
ause
s of
dea
th (n
ot in
clud
ing
NC
Ds)
.

NoNcommuNicable Diseases iN the WesterN Pacific regioN: a Profile 69
ANNex 4 - WHO stePwise suRveILLANCe FOR NCD RIsk FACtORs
No. Country Coverage survey period
1 American Samoa National 2004
2 Cambodia National 2010
3 China National 2004, 2007, 2010
4 Cook islands National 2004
5 Fiji National 2002
6 Kiribati National 2004-06
7 Lao People’s Democratic Republic, the Subnational (Vientiane) 2008
8 Malaysia National 2005-06
9 Marshall Islands, the National 2002
10 Micronesia, the Federated States of Subnational (Pohnpei) 2002, 2006, 2008
11 Mongolia National 2005 & 2009
12 Nauru National 2004
13 Palau National 2011-12 (ongoing)
14 Papua New Guinea Subnational (Capital, Manus, Gulf, Madang, Simbu)
2007-08
15 Philippines National 2003-04, 2008
16 Samoa National 2002
17 Solomon islands Subnational 2005-06
18 Tokelau National 2005
19 Tonga National 2004
20 Tuvalu National 2006-07
21 Vanuatu National 2011
22 Viet Nam Subnational(3 surveys) 2005


A Profile
Noncommunicable Diseasesin the Western Pacific Region
WHO Western Pacific RegionPUBLICATION
ISBN-13 978 92 9061 563 7