Embed Size (px)
Citation preview

MS # 200202503COLLINS 1
Nonsystemic Vasculitic Neuropathy: Insights from a Clinical Cohort
M.P. Collins, M.D.Neurosciences DepartmentMarshfield ClinicMarshfield, Wisconsin
M.I. Periquet, M.D.Department of NeurologyThe Ohio State University College of MedicineColumbus, Ohio
J.R. Mendell, M.D. Department of NeurologyThe Ohio State University College of MedicineColumbus, Ohio
Z. Sahenk, M.D., Ph.D. Department of NeurologyThe Ohio State University College of MedicineColumbus, Ohio
H.N. Nagaraja, Ph.D.Department of StatisticsThe Ohio State UniversityColumbus, Ohio
J.T. Kissel., M.D.Department of NeurologyThe Ohio State University College of MedicineColumbus, Ohio
Supplementary ContentDisclosures: NoneCharacter count (title): 66 Word count (abstract): 260 Word count (text): 4751
Corresponding Author: Michael P. Collins, M.D.Neurosciences DepartmentThe Marshfield Clinic1000 N. Oak AvenueMarshfield, WI 54449(715)-389-5357Fax: (715)-387-5727Email: [email protected]

COLLINS 2
Abstract
Background: Nonsystemic vasculitic neuropathy (NSVN) is an uncommon disorder. Few series with
small numbers of patients have been reported. The prognosis and treatment of patients presenting with
NSVN remain uninvestigated. We sought to address these issues by assembling a large retrospective
cohort with extended follow-up. Methods: All nerve biopsies performed over 20 years were reviewed;
cases with definite, probable, or possible vasculitis were segregated for clinical correlation. Patients
satisfying clinical criteria for NSVN at presentation were selected. Clinicopathologic, treatment, and
outcome measures were analyzed in patients followed for 6 months. Results: 48 patients (30 women,
18 men) with median 63 months follow-up were identified. Most patients (85%) had extensive,
overlapping involvement of multiple nerves. Only one had a symmetric polyneuropathy. Most
neuropathies (96%) were painful. In 96%, nerve damage was distally-accentuated, but most had
concurrent proximal weakness. Diagnostic sensitivity was 58% for superficial peroneal nerve/peroneus
brevis muscle biopsy and 47% for sural nerve biopsy. Combination corticosteroid/cytotoxic therapy was
more effective than corticosteroid monotherapy in inducing remission and improving disability, with
trends toward reduced relapses and chronic pain. Treatment with cyclophosphamide for > 6 months
decreased the relapse rate, which was 46% for all patients. Disease/treatment-related mortality was 10%.
Six percent developed cutaneous involvement. Although chronic pain persisted in 60% of survivors,
80% had good outcomes. Conclusions: NSVN nearly always presents as an asymmetric, distally-
accentuated, painful, sensorimotor polyneuropathy. Risks for systemic spread and death are small, and,
aside from pain, neurologic prognosis is unexpectedly good. Although not a randomized controlled
trial, combination therapy produced the best outcome in this cohort.

COLLINS 3
Introduction
In vasculitis, blood vessels become inflamed and partially destroyed, thereby damaging tissues
through ischemic, inflammatory, and immune mechanisms.1 Most classifications of vasculitis include
only systemic disorders that affect multiple organs.2,3 However, vasculitis can also present in a
“nonsystemic” fashion, confining itself to a single organ, such as skin,4 gastrointestinal5 or reproductive
tract,6 lungs,7 kidneys,8 or CNS.9 Vasculitis restricted to the peripheral nervous system (PNS) was first
recognized by Kernohan and Woltman in 1935.10 The concept then lay dormant until 1985 when seven
such patients were described.1 In 1987, Dyck and coworkers reported 20 patients and coined the term
“nonsystemic vasculitic neuropathy (NSVN).”11 Small numbers of patients have since appeared.12-17 The
largest cohort (25 patients) was reported in 1996.18 The two largest NSVN cohorts were assembled
retrospectively, with patients selected for absence of extra-neurologic involvement during follow-up.11,18
This selection criterion preordained a relatively benign prognosis and precluded an assessment of risk
for systemic spread in patients presenting with a nonsystemic-appearing vasculitic neuropathy.
An important but overlooked question concerns appropriate treatment of patients with vasculitic
neuropathy in general and NSVN in particular. There are no controlled data relevant to the treatment of
any type of vasculitic neuropathy, apart from one study of Churg Strauss syndrome (CSS)-associated
neuropathy.19 We have advocated combination therapy [corticosteroids (CS) and cyclophosphamide
(CYC)] in NSVN, except for mild cases. Others favor CS monotherapy.11,20 These recommendations
lack evidentiary support and are extrapolated from systemic vasculitis trials or anecdotal experience.
This paucity of evidence prompted us to gather data on all NSVN patients treated at our institution over
the past 20 years and analyze their long-term treatment outcomes. In contrast to other series, we
included all patients meeting a predetermined definition of NSVN at the time of diagnosis, consistent
with the manner in which clinicians actually function. Our goal was to systematically analyze treatment
responses, clinical presentation, relapse rate, neurologic outcome, and mortality in patients with NSVN.

COLLINS 4
Methods
Pathologic selection criteria
All nerve biopsies (sural nerve, SPN/PBM, or superficial radial nerve) performed in the
neuromuscular laboratory of The Ohio State University from 1981 to 2001 were reviewed. Biopsy
procedures and histological techniques have been previously described.16,21 Biopsies were classified as
showing (1) definite, (2) probable, or (3) possible vasculitis based on pre-established definitions.16
Definite vasculitis was diagnosed if at least one blood vessel was infiltrated by inflammatory cells
associated with signs of vascular injury, such as fibrinoid necrosis, endothelial cell disruption,
fragmentation of the internal elastic lamina, hemorrhage, or acute thrombus. Probable vasculitis
required transmural or perivascular inflammation unaccompanied by vascular destruction, but combined
with at least one other supportive finding, including vascular thickening, luminal obliteration,
recanalized thrombus, epineurial neovascularization, hemosiderin deposits, asymmetric nerve fiber loss,
ongoing Wallerian-like degeneration, focal perineurial inflammation/thickening, or muscle fiber
necrosis/regeneration. Possible vasculitis was diagnosed in non-inflammatory biopsies revealing
predominant axonal alterations and one or more of four pathologic changes previously shown by our
group to be predictive of PNS vasculitis: muscle fiber necrosis/regeneration, asymmetric nerve fiber
loss, ongoing Wallerian-like degeneration, and vascular immune deposits.16
Patient selection criteria
For all patients meeting pathologic criteria for definite, probable, or possible vasculitis, available
outpatient and inpatient records were reviewed. Each patient had been evaluated by at least one
neuromuscular clinician from Ohio State. In patients with pathologic diagnoses of probable or possible
vasculitis, a subset with “clinically probable” vasculitic neuropathy was determined by application of
published diagnostic criteria,16 consistent with precedent.11,18,22 All patients with definite or clinically
probable vasculitic neuropathy were then divided into systemic versus nonsystemic groups according to

COLLINS 5
standard classification schemes.2,3 Diagnosis of NSVN required (1) clinicopathologic evidence of
vasculitic neuropathy; (2) no clinicopathologic signs of CNS or extra-neurologic involvement; and (3)
no demonstrable etiology or predisposing condition (see Appendix). Patients were not excluded a priori
for constitutional symptoms (weight loss, fever, arthralgias, anorexia, malaise, night sweats) or
monoclonal gammopathy of undetermined significance (MGUS).
All patients satisfying criteria for NSVN were next assessed for adequacy of follow-up. For
patients lacking at least two years follow-up at our institution, attempts were made to acquire additional
information by (1) telephone interviews with patients and relatives, (2) retrieval of medical records from
physician offices and hospitals, and (3) re-examination of selected patients. Patients who had less than
six months follow-up after these efforts were excluded.
Data collection
In this manner, a cohort of 48 NSVN patients with 6 months follow-up was assembled. For
each patient, historical, demographic, laboratory, and pathologic information was tabulated.
Electrodiagnostic data was not tracked due to multiple examiners employing heterogeneous protocols.
Charted treatment variables included agents, dosages, durations of therapy, adverse effects, and
infectious complications (excluding upper respiratory syndromes, gastroenteritis, and oral/vaginal
thrush). Treatment protocols were not standardized and at the discretion of the treating neurologist.
Outcome variables included: (1) pain (better, unchanged, worse); (2) sensory loss (better,
unchanged, worse); (3) objective weakness (better, unchanged, worse); (4) composite Medical Research
Council (MRC) strength score ( 4+ or 5- = 4.5, 4- or 3+ = 3.5, 3- = 2.5, and 2- = 1.5), obtained by
summing the most-affected-side scores for shoulder abductors, elbow flexors, elbow extensors, wrist
flexors, wrist extensors, hip flexors, knee flexors, knee extensors, ankle invertors, and ankle
dorsiflexors; and (5) disability score using the Prineas scale.18,23,24 The primary outcome measure was
“long-term response,” defined as positive if at least one of the preceding five outcome variables

COLLINS 6
improved and none worsened, with improvement sustained for 6 months; and negative if any of the
variables worsened or all were unchanged at 6 months. Patients who improved initially but worsened
prior to 6 months were treated as non-responders (negative long-term response). In patients with a
positive long-term response followed for 12 months, relapses were tracked. Relapse was defined as a
new sign or symptom of weakness, sensory loss, or neuropathic pain after a sustained response to
therapy. Secondary outcome measures for assessment of treatment responses were: (1) change in
composite MRC score, (2) change in disability score, (3) relapse rate, (4) disease or initial treatment-
related mortality rate, and (5) chronic pain in patients followed for at least 24 months. Final MRC and
disability scores were determined at the most recent follow-up encounter, just prior to relapse, or just
prior to death. All thromboembolic events occurring within six months of follow-up were categorized as
disease/treatment-related, in view of the recognized potential of CS and pro-inflammatory cytokines
(e.g., interleukin-1, tumor necrosis factor-) to promote thrombosis.25,26
Statistical Analyses
Statistical analyses were performed using SAS JMP, Version 4 (NC). For assessment of
treatment responses, patients were divided into CS monotherapy and CS plus adjunct (combination
therapy) groups according to their initial treatment. The two groups were compared for potentially
confounding variables such as age, neuropathic symptom duration, initial composite MRC score, initial
disability score, erythrocyte sedimentation rate (ESR), and pathologic muscle involvement, using one-
way analysis of variance or ANOVA (Student’s t test with equal variances and Welch ANOVA with
unequal variances) for parametric analysis of continuous variables, Wilcoxan rank-sum test for
nonparametric analyses, and Fisher’s exact test for comparison of qualitative variables. Differences
between the two groups in long-term response rate were analyzed with Fisher’s exact test. Differences in
relapse rate and chronic pain were assessed with the Pearson chi-square test. Comparisons between the
groups for changes in composite MRC and disability scores were conducted with Wilcoxan rank-sum

COLLINS 7
and t tests. The relationship between duration of CYC exposure and relapse rate was addressed with a 2
x 2 contingency table and Fisher’s exact test. Kaplan-Meier survival analysis was performed for the
entire NSVN cohort, initial CS monotherapy subgroup, and initial CS plus adjunct subgroup. Survival
data for the two subgroups was compared using the Mantel-Cox log-rank and Wilcoxan rank-sum tests.
The influence of weight loss on long-term response rate and change in disability score for the entire
NSVN cohort was evaluated with Fisher’s exact, Wilcoxan rank-sum, and t tests.
The initial CS group was next subdivided based on the presence or absence of an inaugural IV
pulse of methylprednisolone. The effects of the IV pulse on long-term response rate, relapse rate, change
in composite MRC score, and change in disability score were analyzed using similar techniques to the
CS monotherapy versus combination therapy comparisons, with the addition of an analysis of
covariance (ANCOVA) adjusting for the initial MRC and disability scores. To determine potential
predictors of a long-term response to initial CS monotherapy, five clinical variables (age of onset,
gender, symptom duration, initial composite MRC score, and initial disability scores) and four
laboratory variables (ESR, antinuclear antibodies (ANA), rheumatoid factor (RF), and leukocytosis)
were subjected to separate logistic regressions.
For assessment of complications, the incidence of CS-related side effects in patients exposed to
prednisone was compared to the incidence of CYC-related side effects in patients exposed to CYC using
Fisher’s exact test. Infection rates for patients treated with CS alone versus CS plus immunosuppressive
agents were analyzed in a similar fashion. The yield of definite pathologic evidence of vasculitis in
patients undergoing sural nerve compared to SPN/PBM biopsies was analyzed with Fisher’s exact test.
Results
Clinical characteristics
Clinical characteristics of the cohort are summarized in Table E-1 on the Neurology Web site. Of
the 48 NSVN patients, 14 were previously reported,1,16 albeit without the follow-up and treatment data

COLLINS 8
obtained in this study. Thirty patients were women and 18 men (ratio 1.7:1). Age at onset of neuropathy
ranged from 21 to 88 years (mean ± SD = 61.8 ± 14.5 years). Symptom duration prior to diagnosis
varied from 2 weeks to 8 years (mean 8.9 ± 14.9 months; median 5 months). Weight loss (mean 21 ±
10.2 pounds) occurred in 35% and unexplained fevers in 15%.
Ninety-six percent of the neuropathies were painful, and most were sensorimotor in character.
Only 13% of patients had predominantly or, less commonly, purely sensory findings. No patient
presented with pure motor deficits. One patient had small fiber-restricted sensory loss; all others
exhibited mixed sensory findings, involving both small and large fiber modalities. Most patients had
extensive, overlapping involvement of multiple individual nerves, with legs more commonly affected
than arms and distal nerves more commonly affected than proximal nerves (Table 1). The common
peroneal was the most frequently involved nerve overall, and the ulnar nerve was most commonly
affected in the arm. Despite the propensity for distally-accentuated damage (seen in all but two patients),
proximal nerves were not routinely spared: 60% of patients had hip flexor weakness, 40% shoulder
abductor and elbow flexor weakness, and 13% sensory loss in thoracic dermatomes. Only 8% of patients
had cranial neuropathies, typically involving cranial nerve seven. All but one patient had asymmetric
findings at presentation. Patterns of involvement were 77% asymmetric polyneuropathy (overlapping
multifocal neuropathy), 13% true multiple mononeuropathy, 8% asymmetric lumbosacral plexopathy,
and 2% distal symmetric polyneuropathy. Neurologic disability at presentation ranged from mild
multifocal numbness and pain to severe quadriparesis and complete dependence. Median disability was
4 on the Prineas scale, consistent with partial dependence, a need for assistance with some bodily
functions, and a preference for some type of walking aide. There was no significant difference in median
disability or mean composite MRC score between the groups of patients with or without weight loss.
Laboratory findings

COLLINS 9
Laboratory results are detailed in Table E-1. Seventy-one percent of patients had an elevated
ESR ( 20 mm/hour); in 25%, ESR was 50 mm/hour. Other laboratory markers of inflammation or
autoantibody production were abnormal in a minority of patients, including positive ANA in 39%,
anemia in 31%, leukocytosis in 23%, thrombocytosis in 21%, positive RF in 20%, and decreased
complement (C3 or C4) in 11%. Nineteen patients underwent cerebrospinal fluid (CSF) examination;
mild pleocytosis was noted in only one patient (5%). CSF protein was elevated (> 50 mg/dl) in 5/19
(26%), with a mean of 47.2 + 21.9 mg/dl and maximum of 106 mg/dl. Immunofixation electrophoresis
revealed a MGUS in three patients (IgG, IgG, IgM), representing 8% (3/37) of patients older than
50 years.
Nerve biopsy was performed in all patients: sural nerve in 28, SPN/PBM in 18, and superficial
radial nerve in two. Two patients with non-diagnostic SPN/PBM biopsies later had sural biopsies;
conversely, one patient with a non-diagnostic sural biopsy subsequently underwent SPN/PBM biopsy.
Thus, a total of 30 sural nerve, 19 SPN/PBM, and two superficial radial nerve biopsies were performed.
Pathologic diagnoses and diagnostic sensitivities for these procedures are summarized in Table 2.
SPN/PBM biopsy had a higher sensitivity for definite vasculitis than sural nerve biopsy, but the
difference was not significant. In the 19 patients undergoing SPN/PBM biopsies, muscle revealed
definite vasculitis in three patients (16%), inflammatory infiltrates in eight (42%), and muscle necrosis
or regeneration in 13 (68%).
Treatment
Treatment regimens and follow-up. Treatment and outcome measures are abstracted in Table E-2 on
the Neurology Web site. In survivors of the initial 6 months of therapy, follow-up ranged from 6-260
months (median 63 months; mean 75 ± 54 months). Twenty-eight patients were initially treated with CS
alone (prednisone, IV pulse methylprednisolone, or both) and 20 with combination therapy [CS plus an
adjunctive agent – oral CYC in 18, azathioprine (AZA) in one, and intravenous immunoglobulin (IVIg)

COLLINS 10
in one]. Starting prednisone doses ranged from 40-100 mg/day. The most common protocol consisted of
prednisone 100 mg/day for 1-2 weeks, followed by 100 mg q.o.d. A starting dose of 100 mg q.o.d. was
employed next most frequently. Starting CYC doses were 100 or 150 mg/day. In patients successfully
tapered off prednisone (no progression or relapse), duration of therapy ranged from 2-45 months
(median 12.5, mean 14.0 ± 8.8). In the 25 patients treated with CYC as a primary or rescue agent,
duration of therapy ranged from 1-30 months (median 5 months). CYC had to be discontinued in 40% of
patients because of adverse effects (pneumonia, cellulitis, sepsis, leukopenia, anemia, thrombocytopenia,
rash, or diarrhea).
Comparison between initial CS monotherapy and combination therapy groups. For these two
groups, baseline clinical and laboratory characteristics of potential relevance to therapeutic responses are
charted in Table 3. There were no differences between the groups in any of these attributes. For
survivors of the initial 6 months of therapy, median follow-up was 54.5 months (range 12-172, mean 61
± 36 months) in the CS monotherapy group and 77 months (range 6-260, mean 94 ± 68 months) in the
combination group. Methylprednisolone (1 gm/day IV for 3-6 days) preceded oral therapy in 57% of
patients treated with CS alone and 65% of patients initially receiving combination therapy.
Outcome analyses are summarized in Table 4. For the primary outcome measure – long-term
response rate – there was a significant difference favoring the initial combination therapy group. Of the
secondary response variables, the combination therapy group also exhibited a significantly greater
improvement in disability and a trend toward reduced incidence of chronic pain. Eighty-five percent
(17/20) of patients initially treated with CS plus a second agent had improved disability at end of follow-
up compared to 57% (16/28) of those receiving CS monotherapy. Long-term responders to CS
monotherapy were twice as likely to relapse as responders to combination therapy, but this difference
was not quite significant. The two groups had similar disease or initial treatment-related mortality rates
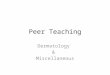
and changes in composite MRC score. Kaplan-Meier survival plots for the CS monotherapy and

COLLINS 11
combination therapy groups are depicted in the Figure. There was no significant difference between the
groups. Estimated 5-year survival for the entire cohort was 87% (SE 13%).
Management of non-responding and relapsing patients. Of the 28 patients initially treated with CS
alone, 11 were non-responders (failed to achieve a long-term response). Of these eleven, two died, three
survived but received no further treatment, and six were managed by the addition of CYC (n = 4) or
IVIg (n = 2) to CS. Five of these six (83%) exhibited a long-term response to the retreatment. The only
non-responder to initial combination therapy died without retreatment. Ten of the 17 long-term
responders to initial CS monotherapy later relapsed; of these, four were retreated with CS alone, three
received CS and CYC, one CS and IVIg, and two were not retreated. Seven of eight retreated patients
responded. Of the 25 patients initially or secondarily treated with combined CS/CYC, 23 responded and
seven later relapsed. For the seven relapsers, 4/5 responded to retreatment with CS, 1/1 responded to
CS/CYC, and 0/1 responded to CS/AZA. Retreated patients who progressed on CS and CS/AZA
subsequently responded to CS/CYC.
Weight loss. There was no significant difference in long-term response rate and change in disability
score for patients with and without weight loss. Seventy-six percent (13/17) of patients with weight loss
exhibited a long-term treatment response versus 74% (23/31) of patients without weight loss. Likewise,
71% (12/17) of patients with weight loss had improved disability at end of follow-up compared to 68%
(21/31) of patients without weight loss.
Efficacy of IV methylprednisolone pulse in initial CS monotherapy group. Of the 28 patients
initially treated with CS monotherapy, 16 received IV pulse methylprednisolone. This subgroup was
significantly more affected than the non-pulsed group by composite MRC score (mean 37.8 ± 7.0 for
pulsed versus 46.7 ± 5.0 for non-pulsed groups) and median disability (4 for pulsed versus 3 for non-
pulsed groups). The two groups had similar long-term response rates (63% pulsed; 58% non-pulsed) and
relapse rates (63% pulsed; 57% non-pulsed). Likewise, there were no differences between the groups for

COLLINS 12
change in composite MRC score and change in disability score, adjusting for the baseline differences in
these scores.
Predictors of long-term response to initial CS monotherapy. None of the clinical (age of onset,
gender, symptom duration, composite MRC score, disability score) or laboratory (ESR, leukocytosis,
ANA, RF) variables predicted a long-term response to initial treatment with CS alone.
Duration of CYC and relapse rate. Eighteen patients were initially treated with CS and CYC; 17
exhibited a long-term response and one died at two months. Seven more patients were treated with
CS/CYC after an initial failure or relapse on CS monotherapy; six responded and one died. Of the 23
long-term responders to CS/CYC, 22 were followed for 12 months, permitting an assessment of
relapse risk. Relapses occurred in seven (32%) of these 22 patients. In patients treated with CYC for ≤ 6
months, the relapse rate was 7/13 (54%). In patients treated with CYC for > 6 months, no relapses
occurred (0/9), a significant reduction (p = 0.017).
Adverse effects. Complications of treatment are summarized in Tables 5 and 6.
Prognosis and outcome
Table 7 itemizes outcome measures for the entire NSVN cohort. Of the five patients whose
deaths were felt related to the disease or its treatment, three died within two to four months of diagnosis,
two from pulmonary emboli and one from myocardial infarction. The two patients with pulmonary
emboli had limited mobility secondary to vasculitic involvement of the lower limbs. The fourth patient
expired from Pseudomonas sepsis at 12 months and the fifth from metastatic bladder cancer 5 years after
her last exposure to CYC. In three patients, vasculitis spread to the skin (livedoid rashes in two cases
and ulcers in the third) 2, 12, and 60 months after initiation of therapy (two patients on prednisone; one
untreated). The 18 patients (46%) who relapsed did so from 6-47 months after onset of treatment
(median 15, mean 19 ± 12 months). The number of relapses per patient ranged from one to four (median

COLLINS 13
1.5). At the time of first relapse, 10 patients had been tapered off treatment altogether and eight were on
prednisone doses ranging from 10-70 mg q.o.d. (mean 40 mg q.o.d.). No patient relapsed on CYC.
Discussion
The NSVN cohort assembled for this study was larger than previous cohorts and had more
extensive follow-up, permitting more representative characterization of the clinical features and
evolution of NSVN. The most important aspect of the study was its attention to therapeutic outcomes, as
no controlled treatment data on NSVN has been reported. The key finding was that combination therapy
(generally CS and CYC) was more effective than CS monotherapy in inducing remission (long-term
response) and improving disability in NSVN, with trends toward reduced relapse rate and chronic pain.
The increased efficacy of combination therapy in NSVN parallels observational studies in systemic
vasculitides27-29 and corroborates the only other NSVN study permitting comparative assessment of
treatments.18 In that report, disability scores improved in 91% (10/11) administered combination therapy
and only 55% (6/11) of those receiving CS alone, figures similar to ours.
The evidence favoring combination therapy in NSVN runs contrary to expert advice and, to
some extent, our own practice over the past 20 years. There appears to be a hesitancy to use CYC in this
ostensibly non-life-threatening disease because of side effects. In this study, patients treated with both
CS and CYC had more adverse effects than patients exposed to CS alone, but this difference was not
significant. Pneumonia and sepsis, in particular, occurred primarily in patients treated with standard
therapy, and there were two combination therapy-related deaths (one sepsis and one bladder cancer).
Nevertheless, (1) CYC did not increase overall disease or treatment-related mortality; (2) combination
therapy produced greater improvement in disability than CS monotherapy; and (3) prednisone-related
side effects were more common than those associated with CYC. From a side effect standpoint, it may,
thus, be more important to accelerate prednisone tapering than to reduce or eliminate CYC.

COLLINS 14
Our study also showed that longer (> 6 month) courses of CYC were more effective in
preventing relapses than shorter courses. This finding is concordant with standard therapy for Wegener’s
granulomatosis, where oral CYC is continued for 12 months after remission is achieved.27 However,
there has been a push in recent years to reduce patient exposure to CYC in systemic vasculitides and,
thereby, minimize CYC-related toxicity.30-34 One approach is to replace continuous oral CYC with
periodic IV pulses. Many controlled trials in patients with systemic vasculitis have shown that pulse
CYC is as effective as oral CYC in inducing remission, with decreased infections and CYC-specific side
effects, but at the expense of a higher relapse rate.34 A second approach involves replacing oral CYC
with an alternate agent once remission is induced, typically in 3-6 months.30-33 The most commonly
employed maintenance drug is AZA (1-2 mg/kg/day) for 12-24 months.30,32, An 18-month, randomized,
controlled trial in anti-neutrophil cytoplasmic autoantibody-associated vasculitis showed AZA to be as
effective as continued oral CYC in maintaining remission.32 There is also uncontrolled data supporting
the use of methotrexate,31,35 cyclosporine,36 and mycophenolate mofetil37 for maintenance of remission.
Sixty percent of our NSVN patients treated with CS alone achieved remission. No clinical or
laboratory variable predicted CS-responsiveness. In particular, mild neuropathies were no more likely to
respond than severe ones, and the use of IV methylprednisolone did not influence outcome. Thus, if
NSVN is treated with CS alone, close follow-up is mandatory, with CYC added for any signs of
neuropathy progression.
Important conclusions on the clinical presentation of NSVN can also be drawn from this study.
First, 96% of neuropathies in this series were painful. Second, 98% of our patients had asymmetric
findings, consistent with other recent reports,22,38 but contrasting with a 25% prevalence of distal
symmetric distributions in the overall vasculitic neuropathy literature and in series dedicated to NSVN
alone.11-13,15,18 The basis for this discrepancy is unclear, but may relate to the fact that even minor
asymmetries in sensory, motor, or reflex function were recorded for this study’s data set. Third, only

COLLINS 15
13% of our NSVN patients exhibited a discrete multifocal pattern; in the rest, individual
mononeuropathies “overlapped.” This contrasts with an ~50% prevalence of multiple mononeuropathies
in the general vasculitic neuropathy literature and in NSVN-restricted series.11,15,18 We suspect this
inconsistency is due to differing definitions of discrete versus overlapping multifocal neuropathy.
Fourth, although findings were distally-accentuated in all but two of our patients, proximal weakness
was common. Fifth, our data showed a much higher prevalence of individual motor nerve involvement
than that described in the literature, especially for tibial and proximal leg nerves (Table 1). Sixth,
although sensorimotor presentations were the norm, 13% of patients had pure or primarily sensory
findings, a proportion compatible with other series.11,16,19,22,24,39,40 Pure motor presentations are almost
unheard of. Translating these conclusions into practice, vasculitic neuropathy is unlikely in patients with
1) no asymmetries, 2) pure motor involvement, 3) no pain, or 4) entirely proximal findings.
Weight loss occurred in 35% of our patients and fever in 15%. Although potentially indicative of
a systemic process, weight loss might also result from the pain and anorexia associated with vasculitic
neuropathy. We opted not to exclude patients with such constitutional symptoms based on precedent in
other localized vasculitides4,7-9 and one previous NSVN series.11 Analysis of weight loss as a predictor of
initial disease severity and treatment responsiveness revealed no differences between patients with and
without weight loss in initial composite MRC and disability scores, long-term response rate, and post-
treatment change in disability. Thus, our decision to include such patients appears reasonable. The
number of patients with fever was too small (n=7) to permit similar analyses. However, review of these
patients suggested that fever was not a predictor of disease severity or treatment response.
The estimated 5-year survival of 87% for our cohort was less than that for another large cohort,
in which only one of 25 patients died over a median 2.8 years follow-up.18 In the Mayo Clinic series,
three of 20 patients died, but survival analysis was not reported.11 Both of these cohorts probably
included a greater proportion of benign cases than ours, as absence of systemic involvement over long-

COLLINS 16
term follow-up was a selection criterion. Ten percent of our patients died from the vasculitis or its
treatment, contrasting with 12-17% of patients in modern systemic vasculitis series.27,29,33,41 Thus, NSVN
is less likely to be lethal than the systemic vasculitides.
In our cohort, only three patients (6%) developed vasculitis in non-neural, non-muscular tissues
over long-term follow-up, and in these three, the only organ affected was the skin. In the only other
study to address this issue, 37% of 29 patients with isolated vasculitic neuropathy followed for a mean
of 6 years developed systemic manifestations.20 However, this cohort was incompletely described and
included patients with systemic disease at outset, as 22% had chronic hepatitis B.12 Our observation of
several patients with restricted nerve and skin vasculitis complements similar reports in the dermatologic
literature, suggesting a relationship between some NSVN and cutaneous periarteritis nodosa.4,42-44
More common than systemic spread in our patients was emergence of new neuropathy symptoms
following a sustained treatment response. Relapses of this nature occurred in 46% of responders,
typically 1-2 years after initiation of treatment. All relapsers were off therapy or receiving low doses of
CS, an argument for longer courses of CYC or an alternate agent. In two other NSVN studies with fewer
patients and shorter follow-up, relapses occurred in 24% and 32%.18,20 The relapse rate for NSVN
overlaps with those for most systemic vasculitides (20-60%).27-30,32,33,41
Final neurologic disability in our long-term survivors (Table 7) was similar to that in another
NVSV cohort – 17% no signs or symptoms, 65% mild to moderate disability, 13% moderately severe
disability (assisted ambulation), and 4% severe disability (non-ambulatory).18 These outcomes are
surprisingly good and suggest that NSVN-related deficits are not exclusively the result of ischemia-
induced axonal degeneration.18 Structural or functional conduction blocks likely also contribute,
supported by our observation that many patients show improved motor function (especially in proximal
muscle groups) during the first 1-2 months of follow-up, prior to expected effects from axonal
regeneration. Possible mechanisms for conduction block in this disease include acute ischemia-induced

COLLINS 17
axonal swelling and attenuation with secondary segmental demyelination,45 chronic ischemia-induced
structural alterations at nodes of Ranvier,46 reperfusion-precipitated and macrophage-mediated
segmental demyelination,47 and inactivation of nodal voltage-gated sodium channels by regional
anoxia.48 Most clinical recovery in vasculitic neuropathy, however, evolves after months have passed
and continues for 1-2 years, consistent with axonal regeneration. Although most of our patients had
relatively mild neurologic deficits at last follow-up, chronic pain was a persistent concern in 60%.
Many features of NSVN overlap with the systemic vasculitides. For example, a substantial
minority of patients develop constitutional symptoms. Most patients have elevated ESRs, and 20-40%
have anemia, leukocytosis, thrombocytosis, and autoantibodies. Muscle biopsies often reveal co-existing
muscle involvement. Vasculitis extends to the skin in some patients. Nerve pathology is similar to that
observed in systemic vasculitic neuropathy.16,49 The disease is better controlled with combination
therapy than CS alone, analogous to most systemic vasculitides. Relapse rates are similar. Taken
together, these observations support the premise that “nonsystemic” vasculitic neuropathy is actually a
systemic process, but unique in its predilection for peripheral nerve involvement, perhaps predicated on
a PNS-enriched antigen or inflammatory nidus.
Acknowledgement
The authors thank Lucia F. Dunn, PhD and Stephen Cosslett, PhD for their assistance with several of the
statistical analyses.
References
1. Kissel JT, Slivka AP, Warmolts JR, Mendell JR. The clinical spectrum of necrotizing angiopathy of
the peripheral nervous system. Ann Neurol 1985;18:251-257.
2. Hunder GG, Arend WP, Bloch DA, et al. The American College of Rheumatology 1990 criteria for
the classification of vasculitis: introduction. Arthritis Rheum 1990;33:1101-1107.

COLLINS 18
3. Jennette JC, Falk AJ, Andrassy K, et al. Nomenclature of systemic vasculitides: proposal of an
international consensus conference. Arthritis Rheum 1994;37:187-192.
4. Daoud MS, Hutton KP, Gibson LE. Cutaneous periarteritis nodosa: a clinicopathological study of 79
cases. Br J Dermatol 1997;136:706-713.
5. Burke AP, Sobin LH, Virmani R. Localized vasculitis of the gastrointestinal tract. Am J Surg Pathol
1995;19:338-349.
6. Francke ML, Mihaescu A, Chaubert P. Isolated necrotizing arteritis of the female reproductive tract:
a clinicopathologic and immunohistochemical study of 11 cases. Int J Gynecol Pathol 1998;17:193-
200.
7. Jennings CA, King TE, Tuder R, Cherniack RM, Schwarz MI. Diffuse alveolar hemorrhage with
underlying isolated, pauciimmune pulmonary capillaritis. Am J Respir Crit Care Med
1997;155:1101-1109.
8. Medvedev G, Al-Shamari AE, Copland MA, Magil AB. Isolated renal giant cell arteritis. Am J
Kidney Dis 2002;40:658-661.
9. Calabrese LH, Furlan AJ, Gragg LA, Ropos TJ. Primary angiitis of the central nervous system:
diagnostic criteria and clinical approach. Cleve Clin J Med 1992;59;293-306.
10. Kernohan JW, Woltman HW. Periarteritis nodosa: a clinicopathological study with special reference
to the nervous system. Arch Neurol Psychiatry 1938;39:655-686.
11. Dyck PJ, Benstead TJ, Conn DL, Stevens JC, Windebank AJ, Low PA. Nonsystemic vasculitic
neuropathy. Brain 1987;110:843-854.
12. Said G, LaCroix-Ciaudo C, Fujimura H, Blas C, Faux N. The peripheral neuropathy of necrotizing
arteritis: a clinicopathological study. Ann Neurol 1988;23:461-465.

COLLINS 19
13. Panegyres PK, Blumbergs PC, Leong AS-Y, Bourne AJ. Vasculitis of peripheral nerve and skeletal
muscle: clinicopathological correlation and immunopathogenic mechanisms. J Neurol Sci
1990;100:193-202.
14. Singhal BS, Khadilkar SV, Gursahani RD, Surya N. Vasculitic neuropathy: profile of twenty
patients. J Assoc Physicians India 1995;43:459-461.
15. Murthy JM, Sundaram C, Meena AK. Nonsystemic vasculitic neuropathy. J Assoc Physicians India
1998;46:204-206.
16. Collins MP, Mendell JR, Periquet MI, et al. Superficial peroneal nerve/peroneus brevis muscle
biopsy in vasculitic neuropathy. Neurology 2000;55:636-643.
17. Abgrall S, Mouthon L, Cohen P, et al. Localized neurological necrotizing vasculitides. Three cases
with isolated mononeuritis multiplex. J Rheumatol 2001;28:631-633.
18. Davies L, Spies JM, Pollard JD, McLeod JG. Vasculitis confined to peripheral nerves. Brain
1996;119:1441-1448.
19. Hattori N, Ichimura M, Nagamatsu M, et al. Clinicopathological features of Churg-Strauss
syndrome-associated neuropathy. Brain 1999;122:427-439.
20. Said G. Vasculitic neuropathy. Ballieres Clin Neurol 1995;4:489-503.
21. Barohn RJ, Sahenk Z, Warmolts JR, Mendell JR. The Bruns-Garland syndrome (diabetic
amyotrophy) revisited 100 years later. Arch Neurol 1991;48:1130-1135.
22. Chia L, Fernandez A, LaCroix C, Adams D, Plante V, Said G. Contribution of nerve biopsy findings
to the diagnosis of disabling neuropathy in the elderly: a retrospective review of 100 consecutive
patients. Brain 1996;119:1091-1098.
23. Prineas J. Polyneuropathies of undetermined cause. Acta Neurol Scand Suppl 1970;44:1-72.
24. Hawke SH, Davies L, Pamphlett R, Guo Y-P, Pollard JD, McLeod JG. Vasculitic neuropathy: a
clinical and pathological study. Brain 1991;114:2175-2190.

COLLINS 20
25. Fatti LM, Bottasso B, Invitti C, Coppola R, Cavignini F, Mannucci PM. Markers of coagulation and
fibrinolysis in patients with Cushing’s syndrome. J Endocrinol Invest 2000;23:145-150.
26. Grignani G, Maiolo A. Cytokines and hemostasis. Haematologica 2000;85:967-972.
27. Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann
Intern Med 1992;116:488-498.
28. Nachman PH, Hogan SL, Jennette JC, Falf RJ. Treatment response and relapse in antineutrophil
cytoplasmic autoantibody-associated microscopic polyangiitis and glomerulonephritis. J Am Soc
Nephrol 1996;7:33-39.
29. Gayraud M, Guillevin L, le Toumelin P, et al. Long-term followup of polyarteritis nodosa,
microscopic polyangiitis, and Churg-Strauss syndrome: analysis of four prospective trials including
278 patients. Arthritis Rheum 2001;44:666-675.
30. Westman KW, Bygren PG, Olsson H, Ranstam J, Wieslander J. Relapse rate, renal survival, and
cancer morbidity in patients with Wegener’s granulomatosis or microscopic polyangiitis with renal
involvement. J Am Soc Nephrol 1998;9:842-852.
31. Langford CA, Talar-Williams C, Barron KS, Sneller MC. A staged approach to the treatment of
Wegener’s granulomatosis. Induction of remission with glucocorticoids and daily cyclophosphamide
switching to methotrexate for remission maintenance. Arthritis Rheum 1999;42:2666-2673.
32. Jayne D. Evidence-based treatment of systemic vasculitis. Rheumatology 2000;39:585-595.
33. Reinhold-Keller E, Beuge N, Latza U, et al. An interdisciplinary approach to the care of patients
with Wegener’s granulomatosis. Long-term outcome in 155 patients. Arthritis Rheum 2000;43:1021-
1032.
34. De Groot K, Adu D, Savage CO. The value of pulse cyclophosphamide in
ANCA-associated vasculitis: meta-analysis and critical review. Nephrol Dial
Transplant 2001;16:2018-2027.

COLLINS 21
35. De Groot K, Reinhold-Keller E, Tatsis E, et al. Therapy for the maintenance of remission in
sixty-five patients with generalized Wegener’s granulomatosis. Methotrexate versus
trimethoprim/sulfamethoxazole. Arthritis Rheum 1996;39:2052-2061.
36. Haubitz M, Koch KM, Brunkhorst R. Cyclosporin for the prevention of disease reactivation in
relapsing ANCA-associated vasculitis. Nephrol Dial Transplant 1998;13:2074-2076.
37. Nowack R, Gobel U, Klooker P, Hergesell O, Andrassy K, van der Woude FJ.
Mycophenolate mofetil for maintenance therapy of Wegener’s granulomatosis
and microscopic polyangiitis: a pilot study in 11 patients with renal involvement.
J Am Soc Nephrol 1999;10:1965-1971.
38. Hattori N, Mori K, Misu K, Koike H, Ichimura M, Sobue G. Mortality and morbidity in peripheral
neuropathy associated Churg-Strauss syndrome and microscopic polyangiitis. J Rheumatol
2002;29:1408-1414.
39. Moore PN, Fauci AS. Neurologic manifestations of systemic vasculitis: a retrospective study of the
clinicopathologic features and responses to therapy in 25 patients. Am J Med 1981;71: 517-524.
40. Castaigne P, Brunet P, Hauw JJ, Leger JM, Gherardi R, Guillevin L. Systeme nerveux peripherique
et panarterite noueuse: revue de 27 cas. Rev Neurol (Paris) 1984;140:343-352.
41. Aasarod K, Iversen BM, Hammerstrom J, Bostad L, Vatten L, Jorstad S.
Wegener’s granulomatosis: clinical course in 108 patients with renal
involvement. Nephrol Dial Transplant 2000;15:611-618.
42. Diaz-Perez JL, Winkelmann RK. Cutaneous periarteritis nodosa. Arch Dermatol 1974;110:407-414.
43. Moreland LW, Ball GV. Cutaneous polyarteritis nodosa. Am J Med 1990;88:426-430.
44. Satoh J, Yamamoto T, Kuroda Y. Vasculitis confined to the peripheral nerve and skin: a variant of
non-systemic vasculitic neuropathy. Eur J Neurol 1999;6:241-244.

COLLINS 22
45. Nukada H, Dyck PJ. Acute ischemia causes axonal stasis, swelling, attenuation, and secondary
demyelination. Ann Neurol 1987;22:311-318.
46. Sladky JT, Tschoepe RL, Greenberg JH, Brown MJ. Peripheral neuropathy after chronic endoneurial
ischemia. Ann Neurol 1991;29:272-278.
47. Nukada H, McMorran PD, Shimizu J. Acute inflammatory demyelination in reperfusion nerve
injury. Ann Neurol 2000;47:71-79.
48. Lindstrom P, Brismar T. Mechanism of anoxic conduction block in mammalian nerve. Acta Physiol
Scand 1991;141:429-433.
49. Kissel JT, Riethman JL, Omerza J, Rammohan KW, Mendell JR. Peripheral nerve vasculitis:
immune characterization of the vascular lesions. Ann Neurol 1989;25:291-297.

COLLINS 23
Appendix Diagnostic Criteria for Nonsystemic Vasculitic Neuropathy (NSVN)
I. Inclusions
Clinical evidence of neuropathy by history and examination
Electrodiagnostic findings consistent with neuropathy
Nerve or nerve/muscle biopsy diagnostic of or suspicious for necrotizing vasculitis
II. Exclusions
Clinical, laboratory, radiologic, or pathologic evidence of organ involvement outside
peripheral nervous system (except muscle).
Identified etiologic agent (drug exposure or infection, especially hepatitis B, hepatitis C,
human immunodeficiency virus, cytomegalovirus, or varicella-zoster virus).
Underlying systemic condition predisposing to vasculitis (connective tissue diseases,
malignancies, diabetes mellitus, mixed cryoglobulinemia).

COLLINS 24
Table E-1 Clinical and Laboratory Features
Pt#
Age(yrs) Sex Dur
(mos) S/SM Pattern CN WBC Hgb Plts ESR ANA RF CompBxsite
Bxdx
1 71 F 5 SM ASP no no no no 25 + SPN poss
2 88 F 13 SM ASP no no yes no 100 - - sural def
3 75 M 9 SM ASP yes no yes no 7 - - SPN poss
4 73 F 12 SM ASP no no no no 30 + - N sural def
5 69 M 8 SM LSP no no no no 30 - - SPN prob
6 65 M 36 SM ASP no no no no 27 - - N sural prob
7 61 F 2 SM ASP no no yes no 94 - + sural def
8 66 M 6 SM MFN no no no no 13 - - N radial def
9 69 M 3 SM ASP no no yes yes 28 - - N sural def
10 40 F 5 SM MFN no no no no 9 - + sural poss
11 28 F 2.5 S MFN no no no yes 38 + - N radial poss
12 57 M 7 SM ASP no no no no 3 SPN poss
13 21 F 3 S MFN no no no no 38 + - N sural def
14 74 F 6 SM ASP no no yes yes 70 - - N sural prob
15 59 F 15 SM LSP no no no no 38 - - sural prob
16 68 F 3 SM ASP no no no no 22 + - N SPN def
17 59 M 13 SM ASP no no no no 24 - - SPN def
18 68 F 4 SM ASP no yes yes no 54 + + N sural def
19 70 F 3 SM ASP no yes yes yes 140 + + sural def
20 67 F 4 SM LSP no no no no 37 + - SPN def
21 73 F 1 SM ASP yes no no no 66 + - sural poss
22 68 F 36 SM ASP no no no no 57 + - SPN def

COLLINS 25
23 47 F 4 S ASP no no no no 9 - sural prob
24 69 M 96 S ASP no no no no 5 + sural def
25 64 F 7 SM ASP no no no no 72 - - N sural prob
26 58 F 2 SM ASP no yes yes yes 53 - + N SPN def
27 63 M 5 SM ASP no no no no 7 - - SPN def
28 69 F 2 SM ASP no yes yes yes 36 + + N sural def
29 74 F 5 SM ASP no no no no 41 + - N sural prob
30 73 M 2 SM ASP no yes yes yes 30 - - N SPN def
31 50 M 4 SM ASP no no yes no 48 - N SPN def
32 65 M 12 SM MFN yes no no no 8 - N SPN poss
33 60 M 2 SM ASP no yes yes no 35 - - sural prob
34 35 F 2 SM MFN no no no no 5 - N sural prob
35 51 F 6 SM ASP no no no no 33 - - sural prob
36 69 M 6 SM ASP no no no no 14 - SPN def
37 75 F 1 SM ASP no yes yes yes 74 - - sural def
38 31 M 4 S ASP no no no no 2 + - sural poss
39 39 F 2 SM ASP no no no no 16 - - N SPN prob
40 82 F 3 SM DSP no no no no 16 + + sural def
41 59 F 8 SM ASP no yes no no 35 + - N sural def
42 46 M 6 SM ASP yes yes yes no 19 + - sural def
43 78 F 4 SM ASP no no no no 46 - - N SPN def
44 50 M 12 SM ASP no no no no 46 - - N SPN poss
45 78 F 1 SM ASP no yes yes yes 51 - N SPN def
46 50 F 24 S ASP no no no no 150 + - N sural poss
47 73 F 0.5 SM ASP no yes no yes 35 - + N sural def
48 67 M 9 SM LSP no no no no 26 - - sural prob

COLLINS 26
Age=age of onset; ANA=antinuclear antibodies; ASP=asymmetric polyneuropathy; Bx=biopsy; CN=cranial
nerve involvement; Comp=circulating C3 or C4; def=definite; DSP=distal symmetric polyneuropathy;
Dx=diagnosis; ESR=erythrocyte sedimentation rate; F=female; Hgb=anemia; LSP=lumbosacral plexopathy;
M=male; MFN=multifocal neuropathy; N=normal; plts=thrombocytosis; poss=possible; prob=probable;
RF=elevated rheumatoid factor; S/SM=affected modality (S=sensory, SM=sensorimotor, M=motor), Sx
dur=duration of neuropathy symptoms; SPN=superficial peroneal nerve;WBC=leukocytosis.

COLLINS 27
Table 1 Motor Nerve Involvement
Nerve Frequency of Involvement (%)
Current Series Literature Review *
Per Patient Per Nerve Per Patient
Peroneal 90 82 91
Tibial 81 73 42
Ulnar 65 58 41
Femoral 63 59 7
Superior Gluteal 52 49 -
Median 48 45 29
Radial 44 42 18
Musculocutaneous 40 39 -
Axillary 40 38 -
*Based on review of up to 485 cases in nine vasculitic neuropathy series.

COLLINS 28
Table 2 Diagnostic Sensitivity of Nerve Biopsies
Biopsy Site
Sural Nerve Superficial Peroneal Nerve/Peroneus Brevis Muscle
SuperficialRadial Nerve
Biopsies performed 30 19 2
# with definite vasculitis 14 11 1
# with probable vasculitis 10 3 0
# with possible vasculitis 6 5 1
Sensitivity for definite
vasculitis47% (14/30)* 58% (11/19)* 50% (1/2)
* No significant difference (p=0.56)

COLLINS 29
Table E-2 Disability, Therapy and Outcome
Pt
#
F/U
(mos)
Initial
MRC
Initial
disabilit
y
IV
MP
Initial
adjunct
LT
responseRelapse
Death
(mos)Cause
Final
MRC
Final
disabilit
y
Final
pain
1 31 49 3 no none yes no 50 2 no
2 4 35 5 yes CYC no no 4 MI 37.5 5 yes
3 12 50 2 no none no no 12 sepsis 26 5 ?
4 20 30.5 5 yes none yes no 40 4 yes
5 27 42 4 yes none yes no 47 3 yes
6 75 40 4 no CYC yes yes 75 panCA 48 3 yes
7 15 37 5 yes CYC yes no 15 CHF 47 4 yes
8 72 49 2 yes CYC yes yes 49 4 yes
9 6 38.5 4 yes CYC yes no 44.5 3 no
10 133 49.5 2 no none yes yes 50 2 no
11 41 50 2 no CYC yes yes 50 2 yes
12 138 46.5 4 no CYC yes no 50 2 no
13 260 50 2 no AZA yes no 50 1 no
14 51 34 4 yes none yes yes 45.5 4 yes
15 48 37 4 yes none yes yes 50 2 yes
16 152 43 3 yes CYC yes no 50 1 no
17 63 45 3 yes none yes yes 50 2 no
18 65 45.5 3 yes CYC yes yes 50 2 yes
19 24 21 5 yes none yes yes 37 4 yes
20 58 39 4 yes none yes no 50 2 no
21 31 46.5 4 yes none yes no 50 2 yes

COLLINS 30
22 73 37 4 yes none no no 39 4 yes
23 62 50 3 no none no no 62 COPD 50 3 yes
24 78 50 2 no none yes yes 78 CHF 50 2 yes
25 74 30 5 yes none no no 74 bladCA 41 4 yes
26 106 42 4 yes CYC yes no 50 2 no
27 31 47 2 yes none yes yes 50 2 yes
28 60 47.5 3 yes CYC yes no 50 1 no
29 77 40 4 no CYC yes no 50 1 no
30 159 39 4 yes CYC yes yes 49 3 yes
31 85 40 4 yes CYC yes no 50 2 yes
32 39 42 4 yes none no yes 46 3 yes
33 52 40 5 yes CYC yes no 49 3 no
34 91 50 3 no none yes no 50 0 no
35 76 37.5 4 no none yes yes 49 4 no
36 61 36 4 no none yes yes 48 3 yes
37 2 41.5 4 no none no no 2 PE 25 5 yes
38 40 50 3 no none no yes 50 2 yes
39 172 47 3 no none yes no 50 2 yes
40 51 46 3 yes none yes yes 50 2 no
41 221 40.5 4 yes CYC yes no 50 3 yes
42 115 39 4 no CYC yes no 49 3 no
43 36 33.5 5 yes none no no 36 CHF 34 5 yes
44 3 41.5 4 yes none no no 3 PE 43.5 5 no
45 81 43.5 4 no CYC yes no 50 2 no
46 85 50 2 no none no no 50 3 yes
47 108 33 5 yes none no yes 43 4 yes

COLLINS 31
48 8 48 3 yes IVIg yes no 50 2 yes
AZA=azathioprine; bladCA=bladder cancer; CHF=congestive heart failure; COPD=chronic obstructive
pulmonary disease; CYC=cylophosphamide; F/U=follow-up; IVIg=intravenous immunoglobulin; IVMP=
intravenous methylprednisolone; LT=long term; MI=myocardial infarction; MRC=composite Medical Research
Council score; panCA=pancreatic cancer; PE=pulmonary embolus.

COLLINS 32
Table 3 Baseline Characteristics of Treatment Cohorts
Clinical Features Initial Therapy
Corticosteroids alone Corticosteroids & Adjunct
Number of Patients 28 20
Age of Onset (mean ± SD, years) 62 ± 14 61 ± 16
Median duration of symptoms (months) 5.5 3.5
Composite MRC score (mean ± SD) 41.6 ± 7.8 42.7 ± 4.5
Disability score (median/mean ± SD) 4/3.6 ± 1.0 4/3.7 ± 0.9
Erythrocyte Sedimentation Rate
(mean ± SD)38.3 ± 37.4 39.6 ± 23.6
Incidence of muscle (PBM) vasculitis 2/12 (17%) 1/7 (14%)
Incidence of muscle (PBM) inflammation 5/12 (42%) 3/7 (43%)
Incidence of muscle (PBM)
necrosis/regeneration9/12 (75%) 4/7 (57%)
MRC=Medical Research Council; PBM=peroneus brevis muscle.

COLLINS 33
Table 4 Outcome Measures for Treatment Cohorts
Variable Initial Therapy p-Value
Corticosteroids alone Corticosteroids & Adjunct
Disease or initial treatment-
related mortality2/28 (7%) 1/20 (5%) NS
Long-term response rate 17/28 (61%) 19/20 (95%) .0077
Relapse rate in responders 10/17 (59%) 5/17 (29%) .084
Change in disability score
(mean ± SD)0.54 ± 1.17 1.20 ± 1.05 .021
Change in composite MRC score
(mean ± SD)3.54 ± 8.36 5.95 ± 3.75 NS
Chronic pain in 24 month
survivors17/24 (71%) 7/16 (44%) .087
NS=not significant; MRC=Medical Research Council.

COLLINS 34
Table 5 Infectious Complications of Treatment
Infection Entire Cohort Pts exposed to CS or CS/IVIg
Pts exposed to CS & IS agent
Any 18/48 (38%) 6/22 (27%)* 12/26 (46%)*
Pneumonia† 7/48 (15%) 1/22 (5%) 6/26 (23%)
Varicella-Zoster 5/48 (10%) 2/22 (9%) 3/26% (12%)
Sepsis 3/48 (6%) 0/22 (0%) 3/26 (12%)
Wound 3/48 (6%) 2/22 (9%) 1/26 (4%)
* No significant difference
†No Pneumocystis carinii pneumonia
CS=corticosteroids; IS=immunosuppressive; IVIg=intravenous immunoglobulin.

COLLINS 35
Table 6 Non-infectious Complications of Treatment
Adverse Effect Incidence (# of affected/# of exposed)
Prednisone
Any related side effect 30/48 (63%)*
Treated hyperglycemia 12/48 (25%)
Treated osteoporosis 11/48 (23%)
Treated mood disorder 9/48 (19%)
Impaired wound healing 8/48 (17%)
Compression fracture 7/48 (15%)
Significant cataracts 3/48 (6.3%)
Treated hypertension 3/48 (6.3%)
Significant myopathy 2/48 (4.2%)
Peptic ulcer disease/Gastrointestinal bleed 1/48 (2.1%)
Avascular hip necrosis 1/48 (2.1%)
Congestive heart failure decompensation 1/48 (2.1%)
Diverticular rupture 1/48 (2.1%)
Cyclophosphamide
Any related side effect 11/25 (44%)*
Leukopenia 8/25 (32%)
Nausea, vomiting, diarrhea 2/25 (8%)
Anemia 1/25 (4%)
Alopecia 1/25 (4%)
Rash 1/25 (4%)
Bladder cancer 1/25 (4%)
Myelodysplastic syndrome 1/25 (4%)
Gross hematuria 0/25 (0%)
*No significant difference

COLLINS 36
Table 7 Final Outcome in NSVN Cohort
Outcome Measure Result
A. Mortality Rate
Total
Disease/Treatment-Related
Kaplan-Meier
21% (10/48)
10% (5/48)
13% at 5 years
B. Relapse Rate in long-term responders 46% (18/39)
C. Spread to extra-neurologic tissues 6% (3/48) – all skin
D. Chronic pain in ≥24 month survivors 60% (24/40)
E. Final disability in ≥24 month survivors
Asymptomatic (DS 0-1)
Mild/Moderate (DS 1-3)
Moderately severe (DS 4; assistance with walking)
Severe (DS 5; non-ambulatory)
12.5% (5/40)
67.5% (27/40)
17.5% (7/40)
2.5% (1/40)
DS = disability score.

COLLINS 37
Figure Legend
Figure. Kaplan-Meier survival analysis for nonsystemic vasculitic neuropathy cohort, according to
initial treatment (log-rank p = 0.2314). Solid line = total cohort; dotted line = group initially treated with
corticosteroid monotherapy; dashed line = group initially treated with combination therapy.