-
7/29/2019 Normal _NEOPI
1/9
Psychological Assessment1992, Vol. 4, No . 1,5-13In the public
domain
Normal Personality Assessmentin Clinical Practice:The NEO
Personality InventoryPaul T. Costa, Jr.,and Robert R.
McCraeGerontology Research CenterNational Institute on Aging,
National Institutes of HealthBaltimore, Maryland
Personality psychologists from a variety of theoretical
perspectives have recently concluded thatpersonality traits can be
summarized in terms o f a 5-factor m odel. This article describes
the NEOPersonality Inventory (NEO-PI), a m easure of these 5
factors and some of the traits that definethem, and its use in
clinical practice. Recent studies suggest that NEO-PI scales are
reliable andvalid in clinical samples as in normal samples. The use
of self-report personality measures inclinical samples is
discussed, and data from 117 "normal" adult men and women are
presented toshow links between the NEO-PIscalesand psychopathology
as m easured by Jackson's (1989) BasicPersonality Inventory and
Morey's (1991) Personality Assessment Inventory. W e argue that
theNEO-PI m ay be useful to clinicians in understanding the
patient, formulating a diagnosis, estab-lishing rapport, developing
insight, anticipating the course of therapy, and selecting
theoptimalform o f treatment for the patient.
In the past two decades there has been remarkable progressin one
of the oldest branches of personality psychology: thestudy of
traits or individual differences. The conceptual statusof traits
has been clarified (Costa & McCrae, 1980; Funder,1991;
Tellegen, in press), and trait measures have shown evi-dence of
convergent and discriminant validity across instru-ments (McCrae,
1989) and observers (Kenrick & Funder, 1988).Longitudinal
studies of both self-reports and ratings haveshown impressive
stability of a wide range of traits across theadult lifespan
(Block, 1981; McCrae & Costa, 1990). Perhapsmost exciting is
the growing agreement among personality psy-chologists that most
individual differences in personality canbe understood in terms of
five basic dimensions: Neuroticism(N) vs. Emotional Stability;
Extraversion (E) or Surgency;Openness to Experience (O) or
Intellect; Agreeableness (A) vs.Antagonism; and Conscientiousness
(C) or Will to Achieve(Digman, 1990; John, 1990; Norman, 1963;
Wiggins & Trap-nell, in press). These factors have been
recovered in studies ofself-reports and ratings, lay adjectives and
standardized ques-tionnaires, adults and children, and several
different cultures.
This five-factor model is a theoretical advance that has
im-portant implications for many applied areas, including
clinicalpractice. By assessing traits f rom each of the five
factors, theclinician can obtain a comprehensive portrait of the
client'spersonality,and the clinical researcher can systematically
exam-ine relations between personality and treatment variables.
Re-cent articles and symposia have examined the utility of
thefive-factor model in counseling (McCrae & Costa, 1991),
ab-normal psychology (Widiger & Trull, in press), and
clinicalpsychology (Spielberger, 1989). This article is intended to
de-
Correspondence concerning this articleshould be addressed to
PaulT. Costa, Jr., Laboratory of Personality and Cognition,
GerontologyResearch Center, 4940 Eastern Avenue, Baltimore,
Maryland 21224.
scribe a measure of the five factors, the NEO Personality
Inven-tory (NEO-PI; Costa & McCrae, 1985, 1989), and its use
inclinical settings.
Of course, "normal" personality assessment, using such
in-struments as the Sixteen Personality Factor Questionnaire(16PF;
Cattell, Eber, &Tatsuoka, 1970) and the California
Psy-chological Inventory (CPI; Gough, 1957), has long been part
ofclinical practice. The NEO-PI is, however, the first
inventorybased on the five-factor model, and a discussion of its
use mayprovide some fresh perspectives on the relevance of
normalpersonality traits to clinical psychology.
Cliniciansoften think of psychological assessment as part ofthe
diagnostic process. Although not designed as a measure
ofpsychopathology, we believe the NEO-PI can contribute
infor-mation that is relevant to diagnosis. But perhaps more
impor-tant are the ways in which the instrument may help the
clini-cian understand the patient, select appropriate treatments,
andanticipate the course and outcome of therapy. For these
pur-poses, much more is needed than measures of psychopathol-ogy;
the full range of personality characteristics must be consid-ered,
and it is here that the five-factor model provides a guide.
The first factor, Neuroticism, ismost familiar to clinicians.
Itrepresents the individual's tendency to experience psychologi-cal
distress, and high standing on N is a feature of most psychi-atric
conditions. Indeed, differential diagnosis often amountsto a
determination of which aspect of N (e.g., anxiety or depres-sion)
is most prominent. Wewill discuss later the relations be-tween this
dimension of personality and psychopathology.
Extraversion is the dimension underlying a broad group oftraits,
including sociability,activity, and the tendency to experi-ence
positive emotions such as joy and pleasure. Patients withhistrionic
and schizoid personality disorders differ primarilyalong this
dimension (Wiggins & Pincus, 1989), and Miller(1991) has
pointed out that talkative extraverts respond very
-
7/29/2019 Normal _NEOPI
2/9
PAUL T. COSTA, JR., AND ROBERT R. McCRAEdifferently to
talk-oriented psychotherapies than do reservedand reticent
introverts.
Clinical psychologists may recognizeOpenness to Experienceasone
of the goalsofRogerian therapy. We use the term to referto abroader
constellation oftraits. High-Oindividuals areimag-inative and
sensitive to art and beauty and have a rich andcomplex emotional
life; they are intellectually curious, behav-iorally flexible, and
nondogmatic in their attitudes and values(McCrae & Costa, 1985,
in press). Although these traits areprobably considered desirable
by most clinicians, they are notnecessarily associated with good
mental health: Conventional-ity and conformity are also viable
paths to adjustment. Differ-ences in O are related, however, to the
manifestations of psycho-pathology (e.g., high-O individuals tend
to use intellectualiza-tion as a defense, whereaslow-O
individualsuse suppression ordenial, McCrae & Costa, in press)
and to the types of treatmentthat the patient is likely to find
acceptable.
Agreeableness, like E, is primarily a dimension of
interper-sonal behavior. High-A individuals are trusting,
sympathetic,and cooperative; low-A individuals are cynical,
callous, and an-tagonistic. As Homey (1945) pointed out in her
distinction be-tween moving toward and moving against others, both
ends ofthis factor may be associated with psychopathology. In
addi-tion, A is clinically important because it directly affects
therapport between patient and therapist (Muten, 1991).
Finally, Conscientiousness is a dimension that contrasts
scru-pulous, well-organized, and diligent people with lax,
disorgan-ized, and lackadaisical individuals. The former aremore
proneto compulsive personality disorder, the latter to antisocial
per-sonality disorder (Lyons, Merla, Ozer, & Hyler, 1990).
Con-scientiousness is associated with academic and vocational
suc-cess (Digman & Takemoto-Chock, 1981); to the extent
thatpsychotherapy can be considered work, C should also affect
theoutcome of therapy, and there is some evidence that it
does(Miller, 1991).
In a brief introduction such as this, it is natural to focus
onthefivebroad domains rather than on the individual traits
thatconstitute them, and those who are unfamiliar with the
five-factor model are well advised to attend first to the
distinctionsamong the domains. In the long run, however, the
detailedinformation that clinicians need can only be provided by
aninstrument that makes distinctions within the domains.
Forexample, anxiety and depression are both aspects of N, but
thedistinction between them is often critical in selecting
appro-priate treatment. The NEO-PI is intended to offer both
aglobal portrait of the individual's personality and more
detailedinformation on specific facets of the broad domains.
Assessing Personality: The NEO-PIThe NEO-PI wasdeveloped over
the past 15 years asa mea-
sure of the five-factor model. Our original interest was in
onlythreeof the factors that weconceptualized asbroad domainsN, E,
and Oeach containing many more specific traits orfacets (Costa
& McCrae, 1980, in press-c). The NEO Inventory(as it was then
called) included six8-item facet scales for each ofthe three
domains. Research on the five-factor model per-
suaded us to include two newer, 18-item scales to measure Aand C
when the NEO-PI was published in 1985. Facet scales forA and C are
being developed and should be available soon(Costa & McCrae, in
press-c; Costa, McCrae, & Dye, 1991) .
The current 181-item version of the inventory has two fo rms:S
for self-reports, and R for observer ratings, with parallel
itemsphrased in first- and third-person. Items are answered along
a5-point Likert scale from strongly disagree to strongly agree,and
scales are balanced to control for the effects of acquies-cence.
Table 1 lists the domain and facet scales of the NEO-PIand some of
their psychometric properties.
Despite the brevity of the facet scales, most have good
inter-nal consistency, and all show substantial stability (which is
alower-bound estimate of reliability) over a 6-year interval.
Per-haps the most important data in Table 1 are given in the
lastcolumn: These arevaliditycoefficients that demonstrate
signif-icant and substantial agreement across sources for all 18
facetsand five domain scales. Additional validity studies
haveexam-ined correlations with peer ratings, a wide variety of
other ques-tionnaires and adjective checklists, sentence
completions, andexpert ratings based on spontaneous self-concept
descriptions(Costa & McCrae, 1985, 1989). Recent reviews of the
instru-ment are providedby Hogan (1989) and Leong and
Dollinger(1990).
Although layobserver rating scales have been widely used
inpersonality research, they have rarely been published. Form Rof
the NEO-PI is available in two versions (one for rating menand the
other for rating women) and has profile sheets based onnormative
studies of adults. As Table 1 shows, the scales ofForm R show a
pattern of reliability and stability very similarto that seen for
Form S, and the self-spouse correlations in thefifth column are
also evidence of the validity of Form R scales.Similar results
(with rs ranging f rom .32 to .54, p < .001) arefound for
individual peer ratings, and larger correlations areseen when
ratings are aggregated across peers (McCrae &Costa, 1989).
Webelieve that ratings by knowledgeable otherscan and should be
more widely used as an adjunct to the self-re-ports usually found
in clinical assessment (cf. Muten, 1991).
Other features designed to make the NEO-PI more useful
toclinicians include computer administration, scoring, and
inter-pretation; a mail-in scoring system; separate norms for
collegestudents; a short, 60-item version (the NEO Five Factor
Inven-tory, or NEO-FFI) that gives scores for the five domains
onlyand may be useful when time for assessment is limited; and
atest feedback sheet (Your NEO Summary) that can be used toinvolve
the patient therapeuticalry in what McReynolds (1989)called
"client-centered assessment."Until recently, almost all research on
the NEO-PI was con-ducted on normal volunteer samples, and
clinicians may right-fully wonder how well its psychometric
properties hold up inclinical populations when used as part of
clinical assessment.The nature of the sample or the conditions of
administrationcould affect thevalidityof the instrument. Three
recent studieshave examined the instrument in three different
clinical set-tings: a behavioral medicine clinic (Muten, 1991), a
sexual be-haviorsconsultationunit (Pagan etal,1991), and aprivate
clini-cal practice (Miller, 1991). In all three samples, patients
scoredabout one standard deviation higher in N and about
one-half
-
7/29/2019 Normal _NEOPI
3/9
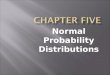
SPECIAL SECTION: NEO-PI IN CLINICAL PSYCHOLOGYTable1Some
Psychometric Properties of NEO-PI Scales fo r Self-Reports(Form S)
and Spouse Ratings (Form R )
Coefficient alpha
NEO-PI
scaleNeuroticismAnxietyHostilityDepressionSelf-consciousnessImpulsivenessVulnerabilityExtraversion
WarmthGregariousnessAssertivenessActivityExcitement
SeekingPositive
EmotionsOpennessFantasyAestheticsFeelingsActionsIdeasValuesAgreeablenessConscientiousness
FormS(n = 983)
.93.85.77.84.74.73.77.87.75.66.76.74.67.79.89.81.81.75.64.79.74.76.86
Form R(n = 167)
.94.89.87.87.74.79.82.88.84.79.72.82.66.81.91.84.86.79.73.84.76.88.91
6-year stabilityFormS
(n = 398).83.75.7 4.70.79.70.7
3.82.72.73.79.75.73.73.83.73.79.68.70.79.71
Form R(n = 167)
.83.75.78.7
2.76.75.68.77.75.73.72.68.69.77.80.73.79.70.75.75.76
Self-spouseagreement(=135)
.54.51.60.47.38.53.32.53.51.54.53.48.45.53.60.40.62.43.47.53.63.50.43Note.
Adapted from Costa& McCrae, 1988. In the public domain.
Allcorrelationssignificantatp < 001.Agreeableness and
Conscientiousness were not measured at baseline.
standard deviation lower in A and C than did normal volun-teers;
they did not differ in E or O.Further, standard
deviationsthemselves were comparable to normative values,
suggestingthat the metric providedby the norms isappropriate fo r
clini-cal samples. Pagan et al. reported reliabilities for the
domainsof .94, .87, .90,'.76, and .85 fo r N, E, O, A, and C,
respectively(values that are virtually identical to those found in
the firstcolumn of Table 1) and replicated the factor structure of
thefacet scales. Muten showed that Form S NEO-PI scales
weremeaningfully related toother self-report scales in
hisbehavioralmedicine sample, and significantly correlated with
spouse rat-ings on FormR, withcross-observer correlations ranging
from.29 to .71. Piven et al. (1990) reported significant
correlationsbetween NEO-PI domain scales and expert ratings of four
ofthe factors based on psychiatric interviews. Suchfindings
sug-gest that clinician ratings of personality are likely to
concurwith patient self-reports.These studies are certainly
encouraging, but they representonly the first stages of research on
the use of the NEO-PI inclinical samples.Many questions
needtobeaddressed in futurestudies: For what other clinical
populations (inpatients, psy-chotics, adolescents) is the NEO-PI
appropriate? How doestreatment affect NEO-PI scores? Whatare the
personality pro-files of different diagnostic groups? How do
personality traitsof the clinician interact with thoseof the
patient? Howwell doself-reports or lay ratings agree with
clinician's views of thepatient's personality? Does the NEO-PI
offer incremental va-lidityover traditional measuresof
psychopathology in predict-
ing diagnosisor prognosis? Researchon all these topics
wouldbewelcome.
Special Concerns in Clinical AssessmentThe traditional
distinction between normal and abnormalpsychology has led some
clinicians to the belief that instru-
ments designed for the measurement of normal personality
di-mensions are irrelevant to or inappropriate for clinical
assess-ment. W e believe this conclusionis unjustified, for tw o
reasons.First, the populations overlap considerably: An
appreciablenumber of individuals in normal volunteer samples
wouldbefound to have diagnosable psychiatric disorders if they
weresystematically assessed, and many of the patients whom
clini-cal psychologists treat are relatively well-adjusted
individualsfacing situational stressors. Second, many aspects of
personal-ity are relatively unaffected by psychopathology. The
presenceof an anxiety disorder, fo r example, need no t affect
one's intel-lectual curiosity or need for achievement. Although
there arecertainly circumstances (such as advanced dementia or
cata-tonia) inwhich the assessment of normal personalityis
impossi-ble and perhaps meaningless,webelieve that most
patientscanbe profitably described in terms of the dimensionsof the
five-factor model, and that the NEO-PI will be a useful way
tomeasure standingonthese dimensions. However, thereare twoissues
that require special consideration here:(a)problems oftest
invaliditydue to defensiveness, socially desirable respond-
-
7/29/2019 Normal _NEOPI
4/9
8 PAUL T. COSTA, JR., AND ROBERT R. McCRAEing, or
malingering,and (b) effects ofpsychopathology itself onpersonality
scale scores.
Defensiveness, Social Desirability, an d MalingeringNEO-PI items
are obvious; that is, they ask directly about
the characteristics they are intended to measure. There arethree
major ways in which the resulting personality scale scorescan be
interpreted. The most straightforward is to view them
asmeasuresfallible measures, and thus actually estimatesofwhat the
individual is really like. A more subtle, second inter-pretation is
that they represent the individual's self-concept:how he or she
sees him- or herself. Third, questionnaire re-sponses, and thus
scale scores, can be seen as self-presentation.In this view, scores
represent the ways in which the individualwishes to be viewed by
others, either in general or on the spe-cific occasion when the
test is administered. It is probably thecase that allthree
interpretations arecorrect tosome extent; theinterpreter's task is
to determine howmuch weight to assign toeach.
It is in regard to this issue that the NEO-PI breaks mostclearly
with the traditions of testing in clinical psychology. Per-haps
because of the early influence of psychoanalysis (with itsemphasis
on unconscious processes and mechanisms of de-fense), concerns
about defensiveness, social desirability, faking,and malingering
have created in the minds ofmanyclinicians aprofound mistrust of
patient self-reports. In response, psycho-metricians have expended
prodigious efforts seeking ways toavoid, detect, or correct for
these sources of invalidity. TheMMPI used empirically keyed scales
with subtle items, andmost clinical instruments (suchasJackson's,
1989, Basic Person-ality Inventoryand Morey's, 1991, Personality
Assessment In-ventory) include validityscalesto measure lying,
defensiveness,or socially desirable responding. Although NEO-PI
inter-preters are of course advised to check protocols for missing
dataand evidence of gross acquiescence or random responding(Costa
& McCrae, 1989), special validity scales are not in-cluded. A
single item that baldly asks respondents whether theyhave answered
the questions honestly and accurately is the onlyvalidity
check.
The omission of validity scales was not an oversight, but
adecision based on several lines ofevidence and reasoning thatneed
to be understood by users of the NEO-PI. Wewould notdeny that
personality scores are sometimes distorted by re-sponse sets and
styles, and that individuals, particularly thosewith emotional and
interpersonal problems, frequently lack in-sight into their own
personalities. But we believe that theseproblems are not as
crippling as they are of ten portrayed, andthat there are better
ways to deal with them than through theuse of validity scales.
There is substantial evidence that self-reports from
patientsare, in general, trustworthy. For example, Jackson
(1989)showed convergent correlations between Basic Personality
In-ventory (BPI) scales and professional ratings of
hospitalizedpsychiatric patients, ranging from .31 to .51 (all p
< .05);corrected for unreliability of the ratings, these
correlations roseas high as .66. Muten's (1991) data show similar
levels of agree-ment between patients' self-reports and their
spouses' ratingson the NEO-PI.
There is also evidence that attempts to improve the validityof
self-reports through the use of special items or scales is
oftencounterproductive. Wrobel and Lachar (1982) showed thatscales
using subtle items were less valid than those composedofobvious
items. Aseries of studies using normal volunteer sam-ples hasshown
that correcting self-reports using lie, social desir-ability, and
defensiveness scales does not increase their validitywith respect
to external criteriaindeed, in many cases itsub-stantially reduces
their validity (McCrae, 1986; McCrae &Costa, 1983; McCrae et
al., 1989). These paradoxical findingsresult f rom the inability of
most social desirability scales todistinguish between individuals
who falsely present themselvesas having desirable characteristics
and those who accuratelyreport desirable traits. Certainly for
normal samples thedangers of mistakenly distrusting valid
self-reports outweighthe benefits of identifying invalid responses,
and we suspectthat the same will hold true in clinical samples.
Thesuccessof psychologicalassessment depends inconsider-able
measure on the clinician's ability to elicit the patient'strust,
interest, and cooperation. The use of instruments de-signed to
outwit or entrap the respondent hardly contributes tothe
development of rapport. We recommend that clinicianswho use the
NEO-PI explain to their patients that it measuressome of the
important ways in which people differ in theirthoughts, feelings,
and actions, and that honest responses wil lcontribute to the
success of clinical evaluation or therapy. Wethink these
instructions wil l lead to valid scores in most cases.
There are doubtless occasions when self-reports are not
trust-worthy. A patient may be uncooperative or cognitively
im-paired, or mayhavepowerful incentives to distort
self-presenta-tion. We think it is unlikely that useful information
wil l beobtained f rom self-reportsinsuch cases, withorwithoutthe
useof corrections, and this was one of the major reasons
wedevel-oped and validated the observer rating f o r m of the
NEO-PI.W e would encourage clinicians to use ratings f rom
knowledge-able informants such as spouses or parents as an adjunct
to orsubstitute for self-reports whenever there is reason to
suspectthat self-reports may be seriously distorted.
Effects of Psychopathology on Scale ScoresResponses to
personality questionnaire items are based on
the self-image, the view the individual has of him- or
herself.Studies comparing self-reports with observer ratings
supportthe conclusion that self-images are generally accurate
(McCrae&Costa, 1989), but clinical psychology provides many
counter-examples, f rom delusions of grandeur to distortions of
body-image among anorectics. In some cases, such irrational
beliefsabout the self may affect personality trait measures, and
theclinician must keep this possibility in mind when
interpretingscores.
One example is provided by narcissism. Narcissists have
aninflated self-image, and may portray themselves as
well-ad-justed, extraverted, and perhaps conscientious. But studies
us-ing both normal (Costa & McCrae, 1990) and psychiatric(Lyons
et al., 1990) samples have found negative correlationsbetween
narcissism and self-reported Agreeableness, so appar-ently
narcissists are not prone to describe themselves as hum-ble,
sympathetic, or self-effacing. Nevertheless, personality rat-
-
7/29/2019 Normal _NEOPI
5/9
SPECIAL SECTION: NEO-PI IN CLINICAL PSYCHOLOGYings might be
particularly useful in cases in whicha diagnosisof narcissism is
suspected.
A more pervasive problem, and one on which there isalreadysome
research, is the effect of mood disorders on self-presenta-tion.
There is considerable evidence that temporary moods donot influence
scores on personality inventories in normal sam-ples (Costa &
McCrae, in press-b; Underwood, Framing, &Moore, 1980). But
clinical depression does affect self-image:Depressed patientshave
loweredself-esteem that is manifestedin their responses. Itappears
that the primary effect ofthis biasis seen on measures related to
Neuroticism. Liebowitz, Stal-lone, Dunner,and Fieve (1979) have
reported that Neuroticismscores, but not Extraversion scores,
increased as patients en-tered a depressive phase. Hirschfeld et
al. (1983) administeredthe Maudsley Personality Inventory(MPI;
Eysenck, 1962) andthe Guilford Zimmerman Temperament Survey (GZTS;
Guil-ford, Zimmerman, & Guilford, 1976) twice to depressed
menand women and reported that measures of N (MPI Neurotic-ism and
GZTS Objectivity, reversed) decreased over a 1-yearperiod for
depressed patients who had recovered, but not forthose who had not.
Recovery from depression did not lead tochanges in GZTS General
Activity and Ascendance (measuresof E) or GZTS Thoughtfulness (a
measure of O).
Additional studies, especially including measures of A andC, are
needed here, but it appears that the major effect of de-pression is
to exaggerate scores on measures of N. Because indi-viduals who are
prone to depression are also likely to have ele-vated premorbid N
scores (Hirschfeld et al., 1989), this bias isunlikely to change
the overall shape of the personality profile.Most important,
depression isunlikely to affect scores on E andO,dimensions that
may be useful in selecting the optimal formof therapy
(Miller,1991).
Linking Clinical and Normal Personality InstrumentsW e have
argued that most clinical populations are not dra-
matically different f rom normal volunteer samples with regardto
the structure of personality. Similarly,wewould argue thatmost
dimensions of psychopathology have parallels in dimen-sions of
individual differences in the normal range. One of theintriguing
questions for future research concerns the nature ofthe relation
between traits and psychiatric disorders: Do traitspredispose
individuals to certain disorders or result f rom thedisorders, or
are mental disorders merely extremeforms ofoth-erwise normal
personality characteristics (cf. Widiger &Trull,in press)?
Whatever the form of the relationship, weknow frommany studies that
there is substantial overlap between mea-sures of personality and
psychopathology, and pointing outthese correspondences may be a
useful way to acquaint theclinician with the constructs measured by
the NEO-PI.
Previousstudies (Costa&McCrae, 1990; McCrae,1991)
haveexamined correlations between the NEO-PI factors and scalesfrom
two of the most widely used clinical instruments, theMinnesota
Multiphasic Personality Inventory (MMPI; Hatha-way & McKinley,
1983)and the Millon Clinical Multiaxial In-ventory (MCMI; Millon,
1983); most of the scales were relatedto N or E. Wehave recently
collected data on two newer mea-sures of psychopathology: Jackson's
BPI and Morey's Personal-ity Assessment Inventory (PAI).
Bothofthese instruments were
intended to provide psychometrically sophisticated measuresof
major dimensions of psychopathology in both normal andclinical
populations. Both instruments were administered to asubsample of
men and women in the Baltimore LongitudinalStudy of Aging (BLSA;
Shock et al., 1984) who had completedthe NEO-PI 2 years earlier.
The 60 men and 57 women whoprovided data on one or both instruments
ranged in age from21 to 94, with mean agesof 67.5 and 64.5,
respectively.
Because both these instruments are relatively new, it is
ofinterest to consider first their convergent and discriminant
va-lidity as alternative measures of psychopathology. In
general,good agreement was found. For example, PAI Somatic
Com-plaint had its highest correlation (r = .72) with BPI
Hypochon-driasis; PAI Anxiety and Anxiety-Related Disorder scales
hadtheir highest correlations with BPI Anxiety (rs= .66, .48,
respec-tively). Intercorrelations among all the scales in Tables 2
and 3are available from us.
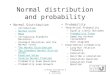
Table 2 gives correlations between the NEO-PI domainscales and
BPI scales. The correlations of Anxiety with N, So-cial
Introversionwith E,Denial with O,Interpersonal Problemswith A, and
Impulse Expression withC require little comment;they show the
parallelism between psychopathological andnormal personality
dimensions that we hypothesized. The neg-ativecorrelation between
BPI Denial and N illustrates the prob-lematic nature of validity
scales. Should we conclude that someindividuals score low on N
because they deny undesirable traitsthey possess,
orshouldweconclude that people lowon Nreallyhave fewer undesirable
traits? Both are logically possible, andwe suspect the latter is
more plausible. Data f rom observerratings would be needed to
resolve this issue.
It is notable that only one of the BPI scales, Thinking
Dis-order, is unrelated to any of the five factors. This finding
isconsistent with earlier speculations that "a sixth dimension
ofaberrant cognitions might be needed to fully describe
personal-ity disorders"(Costa &McCrae, 1990, p. 370)and
illustrates thecomplementary nature of measures of personality and
psycho-pathology.
The PAI is a new instrument designed "to provide informa-tion on
critical clinical variables" (Morey, 1991, p. 1). In addi-tion to
11 clinical scales (most with subscales), it also containsfour
validity scales, two interpersonal scales, and five scalesrelated
to treatment and case management. Table 3 providesmeans, standard
deviations, and coefficients alpha for the PAIclinical and
treatment scales, aswellascorrelations with NEO-PI domain scales.
Comparison of means shows that the presentsample is similar to the
normative group of normals in mostrespects. Internal consistencies
are high except for the DrugProblems and Stress scales, which show
relativelylittle variancein this predominantly older sample.
Correlations of the clinical scales with the NEO-PI domainsshow
a pattern previously seen in analyses of the MMPI andMCMI.
Borderline Features, Anxiety, and Schizophrenia arestrongly related
to N; Mania is related to E; Paranoia and Anti-social Features are
negatively related to A, and none of thescales is strongly related
to O or C.
The inclusion of treatment scales is an interesting feature
ofthe PAI. Aggression and Suicidal Ideation refer to
characteris-tics of the individual that clinicians should attend
to, although
-
7/29/2019 Normal _NEOPI
6/9
10 PAUL T. COSTA, JR., AN D ROBERT R. McCRAETable 2Correlations
ofNEO Personality Inventory Domain Scales With Jackson'sBasic
Personality Inventory (BPI) Scales (N = 109)
NE O Personality Inventory domainBPI scale Neuroticism
Extroversion Openness Agreeableness Conscientiousness
HypochondriasisDepressionDenialInterpersonal
ProblemsAlienationPersecutory IdeasAnxietyThinking DisorderImpulse
ExpressionSocial IntroversionSelf DepreciationDeviation
.29**.32***-.48***.33***.1 2.29**.60***.07.33***.1
6.38***.26**
-.19*-.27**-.19*.05.1 2.00-.08.01.29***-.44***-.43***.02
-.02-.05-.45***.1 4.1 5-.03.06-.13.30***-.15-.35***.01
-.08-.18.1 8-.56***-.40***-.21*-.01.00-.16-.28**-.17-.17
-.17-.21*.21*-.07-.09-.07-.28**-.11-.36***-.04-.35***-.02* /
> < . 0 5 . **p
-
7/29/2019 Normal _NEOPI
7/9
SPECIAL SECTION: NEO-PI IN CLINICAL PSYCHOLOGY 11not a world
apart from dimensions o f personality; both arespanned by the same
five dimensions.
Clinical Uses of Personality DataIn 1986 we argued that
clinicians could benefit from routineassessment of the five basic
factors of personality (McCrae &Costa, 1986). It seemed obvious
to us that they would want tounderstand the enduring emotional,
interpersonal, experien-tial, attitudinal, and motivational styles
of their patients, justasthey need to consider age, sex, education,
and cultural back-ground. It soon became clear to us, however, that
more isneeded than a guide to the elements o f personality:
Cliniciansalso need to learn how to use this information.No t
surprisingly,many of the most important insights in this regard
have comefrom practicing psychotherapists w ho have used the
NEO-PIthemselves (Pagan et al, 1991; Miller, 1991; Muten, 1991). W
esummarize some o f their experience here.
UnderstandingThe most basic function of psychological assessment
is togive the clinician a sense of what the patient is like.
Althoughself-reports are not infallible, there is considerable
evidencethat the NEO-PI provides relatively accurate information o
npatients from a varietyof clinical populations. Because the
five-factor model is comprehensive, the profile the NEO-PI
pro-vides coversthe full rangeof personality traits and can give
theclinician a senseof both the patient's strengths and
weaknesses.Knowledge o f personality traits can also set in context
the spe-cific problems that led the patient to therapy: Are they
reac-tions to recent events or difficult situations, or are they
symp-toms of enduring and pervasive maladjustments?
DiagnosisNEO-PI scores maysuggest possible diagnoses or be used
torule o ut various disorders. Elevated N scores are commonam ong
patients in psychotherapy, but the particular facetso f Nthat are
most elevated m ay focus attention on specific diag-noses. Very
high Self-Consciousness scores, fo r example, shouldlead the
clinician to consider the diagnosis ofSocial Phobia,which is
distinguished by a persistent fear o f acting in a waythat will be
humiliating o r embarrassing. Extreme scores onnormal personality
traits are not necessarily an indication o fpsychopathology (e.g.,
a patient m ay be very extraverted with-o ut being histrionic), but
extreme scores are often contraindica-tive of certain diagnoses
(e.g., very high E scores are inconsis-
tent with the diagnosis of schizoid personality
disorder).Empathy and Rapport
Patients wantto be understood, and they expect therapists tobe
experts at understanding human nature. When therapistsare informed
by NEO-PI results early in the therapeutic pro-cess, they appear
more knowledgeableand empathic to the pa-tient, allowing a more
rapid development of rapport. This isparticularly important in
short-term therapy, in which sessionsspent learning about the
patient m ay be time lost from treat-ment. Clinicians themselves m
ay also find it easier to empa-
thize with patients when they consider nonpathological aspectsof
personality, such as the individual's intellectual interests o
rcapacity fo r joy.Feedback and Insight
Traditionally, the results of clinical assessments have been fo
rtheeyesof the therapist only; it wasassumed that they
wouldbeconfusing and upsetting to patients. Certainly, this is true
fo rsome instruments and some patients. Bu t more recently,
thevalue ofsharing test results has been emphasized;
McReynolds(1989) has called this approach client-centered
assessment.Clearly, it is easier to discuss with patients the
results from ameasure of normal personality than from measures o f
psycho-pathology, and a brief, nontechnical sheet, Your NE O
Summary,has been developed to provide feedback to individuals
whotake the NEO-PI or NEO-FFI. At least one clinician (Muten,1991)
routinelyreviews the full profile sheet with patients, tak-ing the
time toexplain the labels fo r the scalesand the interpre-tation o
f normedscores; further, he refers back to this profile asrelevant
issues arise in therapy. In this way, the scale scores aretied to
concrete examples ofproblematic behavior to help thepatient achieve
insight into his or her behavior. Research isneeded to establish
the utility of this process and the patientpopulations fo r which
it is appropriate, but clinical experiencetodate is
encouraging.Anticipating th e Course of Therapy
The success ofpsychotherapy depends notonlyon the thera-pist's
skill, but also on the patient's cooperation, motivation towork,
and capacity fo r therapeutic benefit. Patients with defi-ciencies
in these areas need special attention from the thera-pist, and the
NEO-PI can signal potential problems in theseareas. Scores on A are
particularly relevant to issues of trust andcooperation. The
patient with very low A scores m ay be skepti-cal about the entire
therapeutic enterprise and expect the clini-cian to prove him- or
herself. Conversely, excessively high Ascores can point to an
overly compliant patient who easily be-comes dependent on the
therapist.Many kinds of therapy require that the patient dosome
formof homework between sessions (e.g., record dreams, chart
eatingbehaviors, keep a diary of emotional reactions). As in
academicsettings, some people are more prone to take such
assignmentsseriously than others are, and this is gauged chiefly by
C. Pa-tients who are very low in C m ay not even remember to
keeptherapy appointments. Law C scores can alert the clinician
tothe need to provide structure and motivation for the
patient.Finally, scores on N are prognostic of ultimate outcome.
Pa-tients who are relatively well-adjusted to begin with are
thosewho benefit most from therapy. In the case of extremely high
Nscores, the clinician needs to foster realistic expectations
aboutthe benefits of therapy. No form of therapy is likely to
affect acomplete cure o f lifelong dysthymia o r a borderline
personalitydisorder; instead, thegoal oftherapy may be to limit
distressorteach the patient how to manage it. Personality
dispositionsand the disorders to which they predispose individuals
tend tobe very stable in adulthood; clinicians should measure
progress
-
7/29/2019 Normal _NEOPI
8/9
12 PAUL T. COSTA, JR., AND ROBERT R. McCRAEagainst this
standard, rather than against the often unrealisticstandard of
perfect mental health (Costa & McCrae, 1986).Matching
Treatments to Patients
Therapists have known fo r decades that some treatmentswork
better with some patients than with others. The medicalmodel
suggests that the diagnosis should dictate the treatment,but this
model isoften inapplicable topsychotherapy. Researchon the
differential effectiveness of different kinds o f therapyhas
emphasized patient characteristics such as gender and so-cial class
(Garfield, 1978) and has offered only limited insights.We believe
that a consideration of personality traits may bemore fruitful.The
two dimensions of clearest relevance to the choice oftherapies are
E and Q Extraverts are sociable, talkative, anddemonstrative, and
will find therapies that require interper-sonal interaction
congenial. Miller (1991) has noted that bothclient-centered therapy
and psychoanalysis require consider-able spontaneous speech from
the patient and are difficult fo rintroverts. By contrast, low-E
patients m ay prefer and benefitmo re from behavior therapy
orGestalt, inwhich the therapisthas a more active role. Shea (1988)
has shown that interperson-ally involved depressed patients benefit
more from interper-sonal therapy; detached patients benefit more
fromantidepres-sant medications.It isalso reasonable tohypothesize
that differences in O willaffect the patient's response to therapy.
Individuals who areclosed toexperience areconventional intheir
tastesand beliefs,and they will probably prefer directive
psychotherapies thatoffer sensible advice, behavioral techniques
that teach concreteskills, or client-centered therapies that
provide emotional sup-port. Patients who are high in O are much
more willing toconsider novel ideas and to try out unusual
approaches to prob-lem solving. Gestalt, psychoanalysis, or Jungian
analysis m ayappeal to them.It is certainly true that whatthe
patient prefers is no t necessar-ily what the patient needs: Group
therapy m ay be exactly whatan avoidant introvert requires. But the
clinician w ho under-stands the enduring dispositions of the
patient will be in amuch better position toselect a treatment and
toexplain to thepatient why it is needed and how it should work.
This is an areain which much more research is needed, and the
five-factormodel provides a comprehensive framework within which
toconduct research on the relation o f individual differences
totreatment outcomes.
ReferencesBlock, J. (1981). Some enduring and consequential
structures of per-sonality. In A. I. Rabin, J. Aronoff, A. M.
Barclay, & R. A. Tucker
(Eds.), Further explorations in personality (pp. 27-43). New
York:Wiley-Interscience.
Cattell, R. B., Eber, H. W, & Tatsuoka, M. M. (1970). The
handbook forthe Sixteen Personality Factor Questionnaire.Champaign,
IL: Insti-tute for Personality and Ability Testing.Costa, P. T,
Jr., & McCrae, R. R. (1980). Still stableafter all
theseyears:Personality as a key to some issues inadulthoodand old
age. In P. B.Baltes & O. G. Brim, Jr. (Eds), Life span
development and behavior(Vol. 3, pp. 65-102). New York: Academic
Press.
Costa, P. X, Jr., &McCrae, R. R. (1985). The NEO Personality
Inventorymanual. Odessa, FL: Psychological Assessment
Resources.Costa, P.T., Jr., & McCrae, R. R. (1986). Personality
stability and its
implications fo r clinical psychology. Clinical Psychology
Review, 6,407-423.Costa, P.T., Jr., & McCrae, R. R. (1988).
Personality in adulthood:Asix-year longitudinal study
ofself-reports and spouse ratingson the
NE O Personality Inventory. Journal of Personality and Social
Psy-chology, 54, 853-863.Costa, P. X, Jr., &McCrae, R. R.
(1989). The NEO-Pl /NEO-FFI man-ual supplement. Odessa, FL:
Psychological Assessment Resources.Costa, P. X, Jr., &McCrae,
R. R. (1990).Personalitydisorders and thefive-factor model of
personality. Journal of Personality Disorders, 4,362-371.Costa, P.
X, Jr., & McCrae, R. R. (in press-a). Manual for the RevisedNE
O Personality Inventory (NEO-PIR) and NEO Five-Factor Inven-
tory (NEO-FFI). Odessa, FL: Psychological Assessment
Resources.Costa, R X, Jr., &McCrae, R. R. (in press-b).
Multiple uses for longitu-
dinal personality data. European Journal of Personality.Costa,
P. X, Jr., & McCrae, R. R. (in press-c). The NEO
PersonalityInventory. In S. R. Briggs & J. Cheek (Eds.),
Personality measures(Vol. 1). Greenwich, CT: JA I Press.Costa, P.
X, Jr., McCrae, R. R., & Dye, D. A. (1991). Facet scales
for
Agreeableness and Conscientiousness: A revision of the NEO
Per-sonality Inventory. Personality and Individual Differences, 12
, 887-898.Digman, J. M. (1990). Personality structure: Emergence of
the five-fac-
tor model. Annual Review of Psychology, 41, 417-440.Digman,
J.M., &Xakemoto-Chock, N. K. (1981). Factors in the natu-
ral language of personality: Re-analysis, comparison, and
interpre-tation of six major studies. Multivariate Behavioral
Research, 16,149-170.
Eysenck, H. J. (1962). The Maudsley Personality Inventory. San
Diego,CA: EdITS.
Pagan, P. J., Wise, T. N, Schmidt, C. W, Ponticas, Y, Marshall,
R. D.,&Costa, P X, Jr. (1991). A comparison of five-factor
personality di-mensions in males with sexual dysfunction and males
with para-philia. Journal of Personality Assessment, 57 ,
434-448.Funder, D. C. (1991).Global traits: ANeo-Allportian
approach to per-sonality. Psychological Science, 2, 31-39.Garfield,
S. L. (1978). Researchonclient variables in psychotherapy. InS. L.
Garfield & A. E. Bergin (Eds.), Handbook of psychotherapy
andbehavior change:An empirical analysis (2nd ed.; pp. 19 1 -232).
NewYork: Wiley.Gough, H. G. (1957). California Psychological
Inventory manual. PaloAlto, CA: Consulting Psychologists
Press.Guilford, J. S., Zimmerman, W S., & Guilford, J. P.
(1976). The Guil-ford-Zimmerman Temperament Survey Handbook:
Twenty-five yearsof research and application. San Diego, CA:
EdITS.Hathaway, S. R., & McKinley, J. C. (1983). The Minnesota
MultiphasicPersonality Inventory manual. New \brk: Psychological
Corpora-tion.Hirschfeld, R. M. A., Klerman, G. L., Clayton, P.,
Keller, M. B.,McDonald-Scott, P., & Larkin, B.(1983). Assessing
personality: Ef-fects of depressive state of trait measurement.
American Journal ofPsychiatry, 140, 695-699.
Hirschfeld, R. M. A., Klerman, G. L., Lavori, P, Keller, M. B.,
Grif-fith, P., &Coryell, W (1989). Premorbid personality
assessments offirst onset of major depression. Archives of General
Psychiatry, 46,345-350.
Hogan, R. (1989). [Review of The NEO Personality tinattory]. In
J. C.Conoley & J. J. Kramer (Eds), The tenth mental
measurements year-book. Lincoln, NE: Buros InstituteofMental
Measurements.Horney, K.. (1945). Ou r innerconflict's. Ne w York:
Norton.
-
7/29/2019 Normal _NEOPI
9/9
SPECIAL SECTION: NEO-PI IN CLINICAL PSYCHOLOGY 13Jackson, D. N.
(1989). BasicPersonality Inventory manual.Port Huron,
MI: Sigma Assessment Systems.John, O. P. (1990). The "big five"
factor taxonomy: Dimensions of
personality in the natural language and in questionnaires. In L.
Per-vin (Ed.), Handbook of personality theory and research. New
York:Guilford.
Kenrick, D. X, & Funder, D. C. (1988). Profiting from
controversy:Lessons from the person-situation debate. American
Psychologist,43, 23-34.
Leong,F. T.L,&Dollinger, S. J. (1990). NEO Personality
Inventory. InD. J.Keyser &R. C. Sweetland (Eds.), Test
critiques (Vol. 8; pp. 527-539). Austin,TX: PRO-ED
Liebowitz, M. R., Stallone, F., Dunner, D. L,& Fieve, R. F.
(1979).Personality features ofpatients with primary affective
disorder. AdaPsychiatrica Scandinavica, 60, 214-224.
Lyons, M. I, Merla, M. E, Ozer, D.J,& Hyler, S. E. (1990,
August).Relationship of the "big-five" factors to DSM-IH
personality dis-orders. Paper presented at the98th Annual
Conventionof theAmeri-can Psychological Association, Boston.
McCrae, R. R. (1986). Well-being scales do not measure social
desir-ability. Journal of Gerontology, 41, 390-392.
McCrae, R. R. (1989). Why I advocate the five-factor model:
Jointanalyses of the NEO-PI and other instruments. In D. M. Buss
& N.Cantor (Eds.), Personality psychology: Recent trends and
emergingdirections (pp. 237-245). New York: Springer-Verlag.
McCrae, R. R. (1990). Controlling neuroticism in the measurement
ofstress. Stress Medicine, 6, 237-241.
McCrae, R. R. (1991). The five-factor model and its assessment
inclinical settings. Journal of Personality Assessment, 57,
399-414.
McCrae, R. R.,& Costa, P. X, Jr. (1983). Social desirability
scales:Moresubstance than style. Journal of Consulting and Clinical
Psychology,51, 882-888.
McCrae, R.R,&Costa, P. T, Jr. (1985). Openness to
experience. In R.Hogan & W H. Jones (Eds.), Perspectives in
personality (Vol . 1; pp.145-172). Greenwich, CT: JA I Press.
McCrae, R. R., &Costa, P. X, Jr. (1986). Clinical assessment
can bene-fit from recent advances in personality psychology.
American Psy-chologist, 41,1001-1003.
McCrae, R. R., & Costa, P. X, Jr. (1989). Different points
of view:Self-reports and ratings in the assessment of personality.
In J. P.Forgas& J. M. Innes (Eds.), Recent advances in social
psychology: Aninternational perspective (pp. 429-439). Amsterdam:
Elsevier.
McCrae, R. R., &Costa, P. X, Jr. (1990). Personality
inadulthood. NewYork: Guilford.McCrae, R. R., &Costa, P. X, Jr.
(1991). The NEO Personality Inven-
tory: Using the five-factor model in counseling. Journal of
Counsel-ing and Development, 69, 367-372,375-376.McCrae, R. R,
&Costa, P. X, Jr. (in press). Conceptions and correlates
ofOpenness toExperience. In S. R. Briggs, R. Hogan, & W H.
Jones(Eds.), Handbook of personality psychology. New \brk:
AcademicPress.
McCrae, R. R., Costa, P. X, Jr., Dahlstrom, WG, Barefoot, J.
C,Siegler, I.C,&Williams, R. B, Jr. (1989). Acautionon the use
of the
MMPI / -correction in research onpsychosomatic medicine.
Psycho-somatic Medicine, 51, 58-65.McReynolds, P. (1989). Diagnosis
and clinical assessment: Current sta-
tus and major issues. AnnualReview of Psychology, 40,
83-108.Miller, X (1991). The psychotherapeutic utility of the
five-factor
model ofpersonality: Aclinician's experience. Journal of
PersonalityAssessment, 57, 415-433.
Millon, T. (1983). Millon Clinical Multiaxial Inventory
manual(3rd.ed.). Minneapolis, MN: Interpretive Scoring
Systems.Morey, L. (1991). Personality Assessment Inventory:
Professional man-
ual. Odessa, FL: Psychological Assessment Resources.Muten,
E.(1991).Self-reports, spouse ratings,and psychophysiological
assessment ina behavioral medicine program: An application of
thefive-factor model. Journal of Personality Assessment, 57,
449-464.
Norman, W X (1963). Toward an adequate taxonomy of
personalityattributes: Replicated factor structure in peer
nomination personal-ityratings. Journal of Abnormaland Social
Psychology, 66,574-583.
Piven, J,Landa, R., Wzorek, M., Gayle, J,Costa, P. X, Jr.,
Boulton, P.,Cloud, D.,Chase, G, &Folstein,S. (1990).
Personality characteristicsof the first degree relatives of
autistic individuals. Manuscript submit-ted for publication.
Shea, M. X (1988, August). Interpersonal styles and short-term
psycho-therapy for depression. Paper presented at the 96th Annual
Conven-tion of the American Psychological Association, Atlanta,
GA.
Shock, N. W, Greulich, R.C,Andres,R,Arenberg, D,Costa, P. X,
Jr.,Lakatta, E. G, & Xobin, J. D. (1984). Normal human aging:
TheBaltimore Longitudinal Study of Aging (NIH Publication No.
84-2450). Bethesda, MD: National Institutes of Health.
Spielberger, C. D. (Chair). (1989, April). Use of the
five-factor model inclinical assessment. Symposium presented at the
1989 MidwinterMeeting of the Society for Personality Assessment,
NewYork.
Xellegen, A. (in press). Personality traits: Issues of
definition, evidenceand assessment. In D. Cicchetti & W Grove
(Eds.), Thinking clearlyabout psychology: Essays in honor of Paul
Everett Meehl. Minneapo-lis: University of Minnesota Press.
Underwood, B., Froming, W J., &Moore, B. S.(1980). Mood and
per-sonality: Asearch for the causal relationship. Journal of
Personality,48,15-23.
Widiger, X A., &Trull, T. J. (in press). Personality and
psychopathol-ogy: An application of the five-factor model. Journal
of Personality.
Wiggins, J. S, & Pincus, A. L. (1989). Conceptions of
personality dis-orders and dimensions of personality. Psychological
Assessment: AJournal of Consulting and Clinical Psychology, 1,
305-316.
Wiggins, J. S., & Xrapnell, P. D. (in press). Personality
structure: Thereturn of the big five. In S. R. Briggs,R. Hogan,
& W H. Jones(Eds.),Handbook of personality psychology. New
\brk: Academic Press.
Wrobel, X A., & Lachar, D. (1982). Validity of the Wiener
subtle andobviousscales fo r theMMPI: Another exampleof the
importanceofinventory-item content. Journal of Consulting and
Clinical Psychol-ogy, 50, 469-470.
Received March 4,1991Revision received March 20,1991Accepted
March 20,1991