Diapositiva 1Alejandro1
1Sección de Inmunología, VIH y Alergias, Hospital Clínico
Universidad de Chile 2Laboratorio de Medicina Molecular, Hospital
Clinico Universidad de Chile
3Hospital Barros Luco Trudeau, Corporacion SIDA-Chile
NOTHING TO DISCLOSE
Background • 1993: resistance to Zidovudina "resistance transmitted
from person to person”
TDR occurs in patients with HIV infection who are not exposed to
antiretroviral drugs but who acquire a virus
has mutations associated with resistance
N Engl J Med 1993; 328:1163-1165.
Background
• Dynamic process that varies temporally and geographically
• The TDR impact is associated with greater virological failure in
first-line antiretroviral therapy (ART)
Background
• Genotypic studies are indicated: – At diagnosis and prior to
initiation of ART – Countries with TDR levels> 5 to 10%
• The genotypic studies, in Chile, are not recommended prior to the
start of TAR due to low rates of TDR: – 2005: 60 patients 0% –
2007: 70 patients2,5% – 2010: 75 patients 2,7%
Rios M, et al. Journal of medical virology. 2007;79(6):647-56 Afani
A et al, RevMed Chile 2010; 138: 669-676
Afani A, Ayala M, Meyer A, Cabrera R, Acevedo W. Rev Med Chile,
2005, 133:295–301.
Background
The aim of this study was to characterize patterns of reverse
transcriptase and HIV protease mutations associated to TDR in
HIV-infected naive patients in
Santiago of Chile between 2014 and 2017
Background
• Demographically and epidemiologically characterize the sample of
patients.
• Clinically characterize the sample of patients according to CD4
count and viral load.
• Characterize pattern of mutations and level of resistance of HIV
among ARV drugs: NTRI, NNTRI and PI.
• Subgroup analysis of patients reporting recent infection (history
of acute retroviral syndrome or prior negative serology within the
last 18 months).
Materials and methods • Transversal type • Collaborative project
between CHILE AIDS Corporation and
HIV Center of the Clinical Hospital of the University of
Chile
• Inclusion criteria: – > 18 years – HIV-1 infection confirmed
by the Institute of Public Health – Naive to TAR – Viral load>
1,000 copies / mL
• HIV Clinical Center of the University Hospital of Chile, Hospital
Barros Luco Trudeau and Fundación Arriarán between August 2014 and
January 2017
Materials and methods • A survey was applied in which data were
collected
concerning: – Age and gender – HIV diagnosis:
• recent infection defined as: acute retroviral syndrome or HIV
negative serology prior <18 months
• route of transmission
– HIV viral load, CD4 lymphocytes count and CDC classification at
the time of study entry
• Approval of the Ethics Committee of the Clinical Hospital
University of Chile
Materials and methods • Genotyping test: TRUGENE TM and
automatic
genotypic resistance test using ReCall TM
• Interpretation of the mutations associated with resistance: –
Stanford University Database (HIVdb Program) – Resistance defined
by Stanford Score (SS) in: 15-29 low
resistance, 30-59 intermediate resistance and> or equal to 60
high resistance
– List of TDR Surveillance Mutations (SDRMs) published by WHO
(2009)
Bennett DE, Camacho RJ, Otelea D, Kuritzkes DR, Fleury H, Kiuchi M,
et al. Drug resistance mutations for surveillance of transmitted
HIV-1 drug-resistance: 2009 update. PLoS One.
2009;4(3):e4724.
Results Table 1. Baseline Characteristics of Patients (n=77)
Age, years, median (range) 26 (19-65)
Gender 100% male
CD4 count, cels/mL, median (IQR) 408 (257-511)
Viral load, copies/mL, median (IQR) 58.000 (21.400-134.000)
CDC Classification, % (n) A 96,1% (74/77) B 1,3%(1/77) C
2,6%(2/77)
Recent infection,% (n) 49,3% (38/77)
Negative HIV serology 42,9% (33/77) Acute retroviral syndrome
6,4%(5/77)
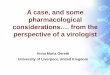
Results • TDR was detected in 7.79% (6/77 patients)
• No mutations associated with resistance to 2 or more ARV classes
were detected.
0,00% 1,00% 2,00% 3,00% 4,00%
NTRI
NNTRI
PI
2,60%
3,90%
1,30%
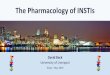
Results Table 2: ARV-associated mutations and resistance
level
PATIENT TDR MUTATION NTRI NNTRI PI
L210W AZT1, D4T1
-K M41L AZT1, D4T1
K103N NVP1, EFV1
K103N NVP1, EFV1
G190A NVP1, EFV2, RPV3
I84V ATV1, FPV1, RIT1, IDV1, NFV1, SQN1, LPV2, TPV2, DVR3
Recent infection patients: TDR 3/387,9% Chronically infected
patients: TDR 3/397,7%
1 High Resistance 2 Intermediate Resistance 3 Low Resistance
Discussion
• TDR is a consequence of the emergence of resistant virus in
patients under ART principal reservoir
• TDR is higher in those regions of the world where ARVs have been
available with universal access for over 20 years
• Early reservoirs were initially established in developed
countries, such as the US and Europe, due to: – Use of
mono-bitherapy prior to HAART – Use of suboptimal ART regimens –
Difficulties in tolerance and adherence – Difficulties in universal
access
Rhee SY, Taylor J, Fessel WJ, et al. . Anti- microb Agents
Chemother 2010; 54 (10): 4253- 61
Discussion • High prevalence in the USA:
– New York City, 2012, 600 patients with recent infection (<6
months) since 1995-2010
– 10 North American states, 11 surveillance areas, 2,030 patients,
reciently diagnosed:
• Overall prevalence TDR: 14.6% (292/2030). • TDR among ARV group:
5.6% NRTI, 7.8% NNRTI, and 4.5% PI
Castor D, Low A, et al. J Acquir Immune Defic Syndr 2012; 61: 1-8
Wheeler WH, Ziebell RA, Zabina H, et al. AIDS. 2010; 24:
1203–1212.
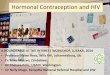
SPREAD: program systematically collects data to gain insight into
TDR occurring in Europe since 2001
TDR Prevalence, 2002-2013
Hofstra LM, et al. Clin Infect Dis2016;62:655-663.
Discussion
• Latin America/Caribbean (LAC): – Overall prevalence of TDR is
7.7% (1996-2009)
• Argentina TDR 13% (31/239)
– RTD among ARV group: • NRTI is 4.4% • NNTRI of 2.3% • PI
2.08%
– Mutations • K103N most common: 29/148 studies (19.6%) • Followed
by 215Y / F / rev (27/148, 18.2%) and 41L
(26/148, 17.6%) Rhee S-Y, et al. PLoS Med 2015 12(4): e1001810.
Bissio E, et al.J Antimicrob Chemother 2017; 72: 504–510
Frentz D, et al. AIDS Rev 2012; 14: 17–27 Pineda-Pena AC, et al.
AIDS Rev 2012; 14:256–267.
Discussion
to 2.8%, p <0.001) – Increase in NNRTIs (0.6% to
2.7% p <0.001) – IP a slight increase (1.6% to
2.4% p = 0.05)
Rhee S-Y, et al. PLoS Med 2015 12(4): e1001810. Bissio E, et al.J
Antimicrob Chemother 2017; 72: 504–510
Frentz D, et al. AIDS Rev 2012; 14: 17–27 Pineda-Pena AC, et al.
AIDS Rev 2012; 14:256–267.
Discussion
Conclusions
• Our results TDR : 7.8% according to WHO SDMRs
• When comparing last published in Chile in 2010, 74 patients,
recent infection: – Analysis by drug group
• NTRI: 2.7% v / s 2.59% • NNTRI: 1.3% v / s 3.9% • PI: 0% v / s
1.3%
• Mutations: – K103N: 2.6%: concordant with international
literature
Afani A et al, Rev Med Chile 2010; 138: 669-676
Conclusions
• Conclusions – Increase in RTD – Genotype resistance test prior to
initiation of ART – Change in behavior in the initial management of
patients
prior to initiation of ART – Which drugs will be the most
appropriate for starting ART
• Surveillance over time
Dianummer 2