Embed Size (px)
Citation preview

\NS Department ofVeterans Affairs
Journal of Rehabilitation Research andDevelopment Vol. 33 No . 2, April 1996Pages 123-132
Electrical stimulation to restore respiration
Graham Creasey, MD ; John Elefteriades, MD; Anthony DiMarco, MD ; Pasi Talonen, PhD;Manfred Bijak, MSc; Werner Girsch, MD ; Carole Kantor, MSMetroHealth Medical Center, Departments of Medicine and of Physical Medicine and Rehabilitation, Cleveland,OH 44109 ; Case Western Reserve University, Cleveland, OH 44106 Yale University School of Medicine,Department of Cardiothoracic Surgery, New Haven, CT 06520 ; Atrotech OY, Tampere, Finland SF33721;University of Vienna, Departments of Plastic Surgery and of Biomedical Engineering and Physics, Vienna, AustriaA-1090; Tantalus, Inc., Highland Park, NJ 08904
Abstract—Electrical stimulation has been used for over 25years to restore breathing to patients with high quadriplegiacausing respiratory paralysis and patients with central alveolarhypoventilation . Three groups have developed electricalpacing systems for long-term support of respiration inhumans . These systems consist of electrodes implanted on thephrenic nerves, connected by leads to a stimulator implantedunder the skin, and powered and controlled from a battery-powered transmitter outside the body . The systems differprincipally in the electrode design and stimulation waveform.Approximately 1,000 people worldwide have received one ofthe three phrenic pacing devices, most with strongly positiveresults: reduced risk of tracheal problems and chronicinfection, the ability to speak and smell more normally,reduced risk of accidental interruption of respiration, greaterindependence, and reduced costs and time for ventilatorycare . For patients with partial lesions of the phrenic nerves,intercostal muscle stimulation may supplement respiration.
This material is based upon work supported by the Cleveland FESCenter . Dr. DiMarco's work was supported in part by NIH and FDA.Drs . Creasey and DiMarco are affiliated with the Department of PhysicalMedicine and Rehabilitation and the Department of Medicine, respectively, atMetroHealth Medical Center, Cleveland, OH and with Case Western ReserveUniversity, Cleveland, OH.Dr. Elefteriades is with the Yale University School of Medicine, Departmentof Cardiothoracic Surgery, New Haven, CT . Dr . Talonen is with AtrotechOY, Tampere, Finland SF33721 . Mr. Bijak is with the University of Vienna,Department of Biomedical Engineering and Physics, Vienna. Austria, and Dr.Girsch is with the Department of Plastic Surgery of that University . Ms.Kantor is with Tantalus, Inc ., Highland Park, NJ.Address all correspondence and requests for reprints to: P . Hunter Peckham,PhD, Cleveland FES Center, 11000 Cedar Avenue, Suite 207, Case WesternReserve University, Cleveland, OH 44106-7211 .
Key words : central alveolar hypoventilation, diaphragmpacing, FES, phrenic nerve stimulation, respiratory paralysis.
INTRODUCTION
Electrical stimulation of the phrenic nerve torestore respiration was first suggested in 1783 byHufeland (1) and then demonstrated as a method ofcardiopulmonary resuscitation by Ure in 1819 (2),Duchenne de Boulogne in 1872 (3), and Beard andRockwell in 1878 (4) . In the early part of this century,
transcutaneous phrenic nerve stimulation was tested inthe acute treatment of apneic newborns by Israel and of
polio patients by Sarnoff (5) . Based on research startingin 1959, Glenn and colleagues developed chronic
phrenic nerve stimulation (6-10). In this life-sustainingapplication of electrical stimulation, patients can breatheentirely by diaphragm pacing . Several groups that useGlenn's method have demonstrated its effectiveness andclinical utility for long-term ventilation in patients with
high quadriplegia or central hypoventilation . Investiga-tors in Finland and Austria have developed variantelectrodes and stimulation techniques in an attempt toreduce muscle fatigue and produce smoother contrac-tion .
To expand the patient group who can be helped tobreathe with electrical stimulation, other workers arestudying intercostal muscle stimulation in patients withpartial lesions of motor neurons supplying the dia-phragm.
123

124
Journal of Rehabilitation Research and Development Vol . 33 No. 2 1996
This paper reviews the current status of chronicimplants for respiratory assist in humans by phrenicnerve stimulation to produce diaphragm contraction, andby extradural spinal cord stimulation to produce inter-costal muscle contraction. It represents what the authorshope is a dialogue between clinicians and engineers inthe service of improving electrical stimulation devicesthat will build on both commercial and researchadvances.
Phrenic Nerve StimulationRespiration is controlled principally by the medul-
lary respiratory control center with some voluntarycerebral influence. The upper motor neurons of thesystem originate in cell bodies in the medullaryrespiratory control center . The axons of these neuronshave synapses in the spinal cord in the neck at the levelsC3 to C5, where they communicate with the lowermotor neurons . The axons of the latter neurons form thephrenic nerves that innervate the diaphragm. Diaphragmpacing cannot treat primary neuromuscular disorder,primary phrenic nerve injury, or spinal cord injury (SCI)at levels C3 to C5 . It can only treat conditions thataffect the upper motor neurons or the medullaryrespiratory control center.
The two main indications are central alveolarhypoventilation (CAH, or Ondine's curse) and highquadriplegia . In CAH, the brain fails to tell the body tobreathe ; this can occur when there is dysfunction in thechemoreceptors in the medulla or in the corticalinfluence on the medulla. CAH may follow stroke orencephalitis, it may be congenital, and in many cases itis idiopathic . High quadriplegia can result from tumoror encephalitis affecting the brain stem, or from spinalcord trauma at the Cl–C2 level, which may be causedby motor vehicle accidents, gunshot wounds, falls, ordiving injuries . In addition, defects may result fromsurgical trauma.
Evaluation of Candidates for Phrenic PacingIn people with normal ventilatory control, an
increase in arterial CO2 (PaCO2) produces an increasein ventilation, which prevents a decrease of PaO2 .Although hypoxemia does not cause an increase ofventilation in normal people (11), Oz saturation is takenas the measure of ventilation because it is easier tomonitor than PaCO 2. In people with CAH, there isalmost no ventilatory response to hypercarbia.
When a person appears to have CAH, a 24-hourprofile of heart rate, CO2 level, 02 saturation, and
respiratory rate is performed in a sleep laboratory . Incases suspicious of acquired (adult) CAH, a full sleepstudy should be performed to exclude with certainty thepossibility of obstructive sleep apnea.
The following additional procedures should pre-cede any attempt to implant a stimulating device(10,12). The conduction of the phrenic nerve should beevaluated by transcutaneous stimulation with a thimbleor needle electrode in the neck, using an indifferentsurface electrode (anode) on the manubrium sterni . Thetrigger point lies against the scalene muscle lateral tothe clavicular head of the sternocleidomastoid muscle atthe level of the cricoid cartilage (13) . Surface electrodesare used to record responses from the diaphragm ; theactive one is placed in the eighth intercostal space onthe anterior axillary line, the reference electrode on thexiphoid, and the ground halfway between xiphoid andmanubrium.
In adults (age range 18–74 years), mean onsetlatency is 7 .5 ms (SD 0 .6 ms) with an upper limit of 9 .0ms (13). In children, latencies are different ; theydecrease from birth (mean 2 .6 ms, SD 0.3) to about 6months of age (2 .2 ms, SD 2.2) because of maturationof the nerve, and then increase (4 .2 ms between 5 and11 years) because of growing length (12,14).
The function of the diaphragm muscle should betested using standard conditions under fluoroscopy (15).At supramaximal tetanic stimulation of the nerve, thediaphragm should descend at least 4 cm in adults . Thedescent should be recorded independently for each sideto provide baseline values for possible future trouble-shooting . The test is most easily performed in connec-tion with measurement of phrenic nerve latency.
Additional requirements for receiving the phrenicpacing system are normal pulmonary function andnormal chest wall configuration. The diaphragm mustbe intrinsically intact except for disuse atrophy in thecase of quadriplegia . Good psychosocial conditions areimportant and a diaphragm pacer is not usually im-planted in persons with significant cognitive injury . Asupportive home situation is essential.
Implant ProcedureThree groups, located in the United States, Austria,
and Finland, have developed pacing systems for long-term support of respiration in humans . These systemsconsist of electrodes implanted on the phrenic nervesand connected by leads to a stimulator implantedsubcutaneously and powered and controlled by electro-magnetic coupling from a battery-powered transmitter

125
CREASEY et al . Electrical Stimulation to Restore Respiration
outside the body. The systems differ principally in theelectrode design and stimulation wavefoun . The implantprocedures also vary according to the devices and thesurgeons carrying out the implantations.
Yale GroupThe implantation procedure used by this group is a
relatively noninvasive thoracic operation . A minithor-acotomy, 3 to 4 in (7 .6 to 10 cm) long, is made in thesecond or third intercostal space on the anterior chestwall . The phrenic nerve is atraumatically mobilizedabove a flat spot of the mediastinum at the top of thecardiac structures . The half-cuff electrode is placedbehind the nerve, and the silastic portions of the elec-trode are secured to the pleura overlying the medias-tinum. The nerve must lie perfectly inside the half-cuffplatinum contact of the electrode with no distortion ortension. The full cuff used previously has potential forcircumferential scar which may impair the nerve . Withthe 180°, or half-cuff, electrode, if scar develops, it islimited to one side and cannot trap or pinch the nerve.
Through a smaller incision (2 inI5 cm) over a flatportion of the anterolateral lower rib cage, the implantedstimulator, the indifferent electrode, and the connectorto the phrenic nerve electrode are placed . The lead fromthe phrenic nerve electrode is tunneled subcutaneouslyand attached to this connector.
Avery Laboratories, Inc . (Commack, NY), whichdistributes the US-made device, favors implantation inthe neck in adults, with a subclavicular receiver pocketfashioned via the same incision.
The Yale group, which has done much of the USclinical work, believes that tracheostomy in all patientsis very important, even though the tracheostomy may becapped for much of the time. Those who have usedpositive pressure ventilation will already have thetracheostomy . It provides a reserve access to the airwayin case of a problem with the pacing system. Inaddition, diaphragm pacing produces such a vigorouscontraction of the diaphragm that it tends to close theglottis, and there is no coordinated opening of the glottisduring stimulated inspiration . While this may be accept-able when the patient is awake, upper airway obstruc-tion can result during sleep . Pacing patients with atracheostomy are advised to remove the inner cannulaof their (uncuffed) tracheal tubes during sleep.
Finnish GroupAs with the Avery system, surgical implantation
may be accomplished either in the neck or the thorax .
However, placement in the thorax is preferred, as itoffers more space and is sure to stimulate any accessoryphrenic nerves, originating normally at C5 and C6 lev-els, which join the phrenic nerve below the level of theclavicle (16) . The only additional step is to place and fixthe anterior strip of the electrode over the nerve . Place-ment of the receiver-stimulators and the cables from theelectrode array are similar to the Avery system . Incarefully selected cases with normal function of nervesand muscles and the ability to increase the sigh volumeby using the accessory ventilatory muscles in the neck,the tracheostomy may be closed, because suctioning isno longer needed . However, this group advises that thetracheostomy should not be closed if a pulse oximeter isnot used during sleep (17) . The frequency and severityof complications with a pulse oximeter or with apersisting tracheostomy are comparable.
Austrian GroupThe Austrian group usually uses median ster-
notomy for implantation . The receiver is implanted in asubcutaneous pocket in the abdominal wall . The elec-trode leads are pulled through to the mediastinum, andfour electrodes are applied to each phrenic nerve in theupper part of the mediastinum. Occasionally, electrodeimplantation has been performed on the phrenic nervein the neck.
All quadriplegic patients treated with the Austrianphrenic pacemaker underwent a program to achieveauxiliary breathing via neck muscle contraction. As aresult of such training, patients suffering from SCIbelow level C2 were able to breathe for at least 20minutes spontaneously. These patients had theirtracheostomies closed (18) . No disadvantages haveresulted from this maneuver ; none of the tracheostomieshave had to be reopened . Production of mucus dimin-ished greatly . External compression of the thorax wassufficient for expectoration.
Commercial DevicesThree systems are commercially available for
phrenic pacing: from Avery Laboratories in the UnitedStates, from Atrotech OY in Finland, and fromMedlmplant of Austria . Table 1 summarizes the charac-teristics of the systems.
AveryThe Avery I-107A device (Figure 1), used
unipolar stimulation to each phrenic nerve with aremote indifferent electrode .

126
Journal of Rehabilitation Research and Development Vol . 33 No . 2 1996
Table 1.Technical features of phrenic nerve stimulators.
DeviceAVERY I-107A(superceded) AVERY I-110A ATROTECH MEDIMPLANT
Receiver size (mm) 46 (diam) x 16 30 (diam) x 8 49 (diam) x 8 .5 56 x 53 x 14
Battery life (hr) 160 100 160-320 (12V) 248 (9V)
Controller + battery weight (kg) 3 .6 0 .54 0 .45+0.6(12V) 0 .8 + 0 .620 .45 + 0 .045 (9V)
Controller size (mm) 179x 114x97 146 x 140 x 25 185x88x28 170x130x51
Breaths/min 10-50 6-24 8-35 5-60
Pulse interval (ms) 35-170 40-130 10-100 25-170
Pulse width (microsec) 150 150 200 100-1000
Sigh possible yes yes yes yes
Electrodes Monopolar ; bipolar Monopolar ; bipolar Quadripolar Quadripolar
No. of receivers to stimulate both 2 2 2 1hemidiaphragms
This device used trains of pulses, typically at afrequency of 7—10 Hz, lasting 1 .3 sec and delivered 6 to10 times per minute to produce contraction of thediaphragm and inspiration. The pulsewidth was 150microseconds and currents were 1—3 mA . A higherinspiratory rate and shorter duration of inspiration isused for children, consistent with their physiology.
It has been found in recent years that body fluidscan enter the Avery I-107A device, leading to stimulatorfailure between 1 .5 and 3 .0 years after surgical place-ment . In 1990, Avery Laboratories introduced a newmodel (I-110A) to overcome hermetic sealing problemswith the original, which has not been available since theend of 1994. The new system is adapted from a paincontrol stimulator approved by the Food and DrugAdministration (FDA) for diaphragm pacing . Uncou-pling between receiver and antenna of the new systemcan occur with movements of only 1 cm, which couldpose a potential clinical problem.
Atrotech
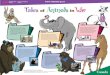
The nerve electrode of the Atrotech system con-sists of two connected strips of Teflon matrix, each stripcontaining two electrode contacts (Figure 2) . One stripis placed in front of the nerve and the second behind thenerve, about 5 mm away longitudinally . Each of thefour electrode contacts in turn serves as a cathode, and a
contact on the opposite side of the nerve as an anode.Because of the separation of about 5 mm between anodeand cathode, the stimulation is due to longitudinal ratherthan transverse current flow, reducing the chargerequirements for nerve activation (19) . When properlyadjusted, sequential stimulation is intended to imitatenatural activation of the nerve and reduce fatigue byrecruiting groups of motor units asynchronously andallowing smooth contraction of the muscle at lowerfrequencies for each group of motor units.
At regular intervals the stimulation level is in-creased beyond that required for an adequate tidalvolume . This causes a larger than normal tidal volume,known as a sigh. Thus, a larger muscle mass than thatneeded for normal tidal volume is conditioned andavailable if needed for increased metabolic demands(19) .
The Atrotech control unit (Figure 2) provides forboth everyday adjustments and special programming . Itallows modification of the stimulated side of thediaphragm, alternating or bilateral stimulation, respira-tory rate, and the sigh function.
During the conditioning phase, the clinician orengineer sets and modifies the stimulus parameters foreach patient with a special programming unit. Later, thisunit is rarely used (19) . For each electrode combination,a threshold current and a current adequate to achieve a

127
CREASEY et al . Electrical Stimulation to Restore Respiration
Figure 2.Respiratory pacing system of Atrotech, Tampere, Finland . (Top)Placement of front and back strips of four-electrode array on phrenicnerve . (Lower left) Two electrode arrays and one implantablestimulator. (Lower right) External controller with two antenna coils.
x
Figure 1.A. Diaphragm pacing apparatus includes transmitter, externalantenna, implantable receiver, and the phrenic nerve electrode . Thetransmitter and the antenna coil, which is taped to the skin over theimplanted receiver, remain outside the body.B. The phrenic nerve electrode is placed at the level of the upperthorax and the implanted receiver is placed over a flat portion of thelower chest wall . Avery I-107A system, Avery Laboratories, Inc .,Commack NY. (Reprinted with permission from TW Shields, ed .,General Thoracic Surgery, Vol . 1, Fourth Edition, Williams &Wilkins, 1993 .)
normal tidal volume are set . The maximum current ofeach combination is then reduced to avoid overlapof excitation areas but still to produce an adequatetidal volume. The pulse interval is set between 40and 60 ms, giving an overall stimulus frequency of25–16 Hz. Smooth, graded diaphragm contraction isachieved by adjusting recruitment and frequency . Respi-ratory rate and inspiration duration are then adjustedover the conditioning period for individual patients.Stimulation is maintained during axial displacement ofthe transmitting coil by 4 .5 cm and radial displacementby 2 .5 cm .
Medlmplant
In 1973, the Austrian group started clinical stimu-lation of the phrenic nerve with single channel,nonimplantable devices . A technique called "carouselstimulation" for stimulation at different sites around thecircumference of the nerve was patented by Thoma in1976 (20) and was used for the first time in a humansubject in 1979 . Technical improvement led to the firstimplantable nerve stimulator for carousel stimulation in1981, now provided by Medlmplant (Figure 3).
This system uses sequential stimulation of fourelectrodes placed around each phrenic nerve; theelectrode combination is changed with each inspiration,with the intention of reducing fatigue . The 0.2 mmepineural electrodes are stranded stainless steel wire (12strands, 0 .05 mm diameter), formed into 0 .8 mm innerdiameter loops and sutured to the epineurium with 8-0prolene sutures using microsurgical techniques . Theelectrodes are applied as close to the nerve as possiblewithout damaging neural structures (21-23).
Carousel stimulation allows stimulation at nearphysiologic respiratory rates : 11–17/min in adults and15–25/min in children and infants . Duration of inspira-tion is set between 0.6 and 1 .3 s to achieve aphysiologic inspiration/expiration ratio . Mean minute

128
Journal of Rehabilitation Research and Development Vol . 33 No . 2 1996
{11111111111~1l1 ' ~ ;
111111111
111111111
111111111
12
14
15
16
17
Cm
Figure 3.(Top) The respiratory pacemaker package of Medlmplant, Vienna,Austria: 1) battery-powered control for eight stimulation channels, 2)external RF transmission coil, 3) 8-channel implantable nervestimulator, 4) electrode leads, 5) annular electrode tips, 6) householdcurrent power transformer, 7) car battery power transformer, and 8)trigger unit for respirator for use during training . (Middle) Epineuralelectrode tip alongside a common match head . (Bottom) Four-in-oneelectrode lead with epineural electrode tips.
volume is 150±24 ml/kg body weight which corre-sponds to mild hyperventilation with a PaCO2 ofapproximately 30 mmHg (18) . A stimulation frequencyof 26 Hz is used to provide tetanic diaphragmcontraction. Pulse trains are delivered with increasingcurrent amplitude (threshold to maximum) to generate asmooth contraction.
The Medlmplant device consists of one receiver (8channels) and two multiple leads connecting to four
electrodes on each phrenic nerve to activate bothhemidiaphragms simultaneously (23) . The externalequipment consists of the control unit, the transmissioncoil, and various devices for power supply and batterycharging . The control unit generates the stimulationinformation for both phrenic nerves . Up to 16 electrodecombinations can be individually adjusted and activatedfor each nerve. The stimulation is maintained duringtransmission coil displacement of up to 6 cm in theaxial direction and 3 cm in the radial direction.
The first version of the stimulation program is setup in the clinic . After training, the patient or an assistantcan change the stimulation parameters of thresholdcurrent, maximum current, inspiration duration, andrespiratory rate. Changes to pulse width and stimulationfrequency must be made in the clinic.
Outcomes of Diaphragm PacingAvery Device
The I-107A stimulator has been in use for 25 yearsand has been implanted for respiratory pacing in almost1,000 patients worldwide . At least five patients havebeen paced for more than 20 years (24).
At Yale, long-term follow-up of 14 quadriplegicpatients who use bilateral low frequency stimulationrecorded the longest use of the device as 15 years with amean of 7 .6 years (25) . Tidal volume was maintainedlong-term without decrement, and the threshold andamplitude of stimulation required for maximum excur-sion of the diaphragm were unchanged over thelong-term follow-up . Transition to full-time pacingrequired 3 to 9 months (25) . Limited pathologic materialhas shown no evidence of significant damage to nerve,diaphragm, or lungs (26).
While the possibility exists that phrenic pacingimproves life expectancy for people with high quad-riplegia, there are no controlled studies . Carter reported63 percent survival at 9 years with positive pressureventilation (27,28) . In the Yale experience, 100 percentof quadriplegic patients who completed the protocol(n=12) were alive at 9 years . Survival was probably dueto avoidance of mechanical failure of ventilators,tracheal problems, and pulmonary infection—all ben-efits afforded by diaphragm pacing.
Persons with central hypoventilation, whose condi-tion is not severe enough to require positive pressureventilation, may develop chronic hypoxia with braindysfunction and subsequent pulmonary hypertension.Comparative clinical trials are needed to determine the

129
CREASEY et al . Electrical Stimulation to Restore Respiration
influence of diaphragm pacing on this natural history,but they would have to be multicenter trials because ofthe small numbers of patients involved.
Atrotech Device
The Atrotech device had been used in 79 patientsin 16 countries by the end of 1994 and is beingimplanted under Investigational Device Exemption fromthe FDA in the USA. This device has reduced theconditioning phase of the atrophied diaphragm from 6to 2 months (29) . Preliminary results also suggest thatthe sequential stimulation protocol of the Atrotechdevice allows longer fatigue resistant electrical ventila-tion. Clinical trials currently underway are expected toprovide definitive data about fatigue resistance . Earlycommencement of full-time electrical ventilation for thepatient with high quadriplegia means that he or she canbe treated as a patient with low quadriplegia and thusreceive the benefits of early rehabilitation (29).
Medlmplant Device
Twenty-four patients have been treated with theMedlmplant phrenic pacemaker between 1983 and1994, mainly in Austria and Germany . Twenty-twosuffered from total ventilatory insufficiency, and twowere dependent on mechanical ventilation during sleep.Fifteen use electrophrenic respiration chronically duringday and night; two, suffering from CAH, use electro-phrenic respiration at night only ; four patients could notbe totally weaned off mechanical ventilation.
Closure of the tracheostomy reduces the danger ofpulmonary infection and allows the patient to speak andsmell normally . Some patients regard this as the mostremarkable improvement in their quality of life.
Intercostal Muscle StimulationMethods to activate the intercostal muscles of the
rib cage have also been investigated, since thosemuscles contribute up to 40 percent of the vital capacity(30) . The intercostal muscles contain both inspiratoryand expiratory components : external intercostal musclesare inspiratory in function, while the internal intercostalare expiratory . However, in the upper rib interspaces,the external intercostal muscles are five to six times asthick as the internal intercostal muscles, and thus theupper rib cage musculature is predominantly inspiratoryin function.
It is possible to activate the upper thoracic ventralroots supplying the intercostal muscles with a single
electrode positioned on the epidural surface of thespinal cord (31) . In animal studies, such an electrode atthe T2 level achieved inspired volumes of 35–40percent of vital capacity, comparable to volumesachieved by stimulation of the four upper thoracicspinal roots (32).
The technique of epidural spinal cord stimulationhas been applied to ventilator-dependent quadriplegicpatients with phrenic nerve injury (33) . A quadripolarspinal cord electrode (8 mm x 45 mm: Medtronic,Minneapolis, MN) was placed on the ventral surface ofthe upper thoracic spinal cord following a laminectomyat T4-T5 . In the month following electrode implanta-tion, the four electrode terminals were tested todetermine which two produced the greatest inspiredvolumes . In a second surgical procedure, the selectedelectrodes were connected to the cathodic leads of aradio frequency receiver implanted subcutaneously overthe anterior rib cage . Anodic leads from the receiverwere connected to indifferent electrodes, implantedsubcutaneously over the back musculature.
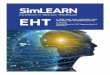
A two-channel radio frequency transmitter (Med-tronic Model #7520) delivered control signals throughthe skin. The transmitter allowed settings of cycleon-time, cycle off-time, pulse amplitude (0–10V), andstimulus frequency (8 .6–32 Hz) . Pulse duration was0.15 msec. Pulse train rate (breaths/minute) could bevaried between 6 and 23 . At stimulation frequencies of20–30 Hz, evidence of system fatigue was initiallyobserved after 15–20 min . Over the course of a 20-weekreconditioning program using gradually increasing peri-ods of stimulation (Figure 4), it was possible to reducestimulation frequencies gradually to 12–14 Hz, and tidalvolume increased from about 200 ml to between 670and 850 ml in three of four subjects (33) . The results foreach patient in terms of the maximum tidal volume,vital capacity, negative inspiratory pressure, and timetolerated off mechanical ventilation are shown in Table2.
While it was possible to generate large inspiredvolumes with intercostal pacing, the maximum durationoff mechanical ventilation was relatively brief, rangingfrom 20 to 165 minutes, when using intercostal pacingalone (33) . It is hypothesized that patients with partialdiaphragm function, insufficient for phrenic nervepacing alone, may benefit from combined intercostaland unilateral diaphragm pacing . In support of thishypothesis, previous work in animals suggests thatcombined intercostal muscle and diaphragm activationresults in airway pressures (34) and inspired volumes

130
Journal of Rehabilitation Research and Development Vol . 33 No . 2 1996
v0c0
1000
CM
PT:w W
Figure 4.Changes in maximum inspired volume during the reconditioningperiod for each patient. These changes generally were progressiveincrements in inspired volume production . The arrows in the figureof patient KM indicate when the dose of antispasmodic agents wasreduced and then increased again.
Table 2.Effects of intercostal pacing alone on maximum time offventilatory support, inspired volume and negative inspiratorypressure.
Patient
Max.Pacing
DurationAchieved
(min)
InspiredVolume at
InspiredVolume at
NegativeInspiratorypressure at32 Hz (cm
water)13 Hz (ml.) 32 Hz (ml .)
CMWWGLKM
2060
16515
500450550300
850710670470
-16 .5-19.0-14.0— 8 .5
(35) equal to or greater than the arithmetic sum of thoseproduced by either muscle group alone.
Combined intercostal and diaphragm pacing hasbeen evaluated in two patients . A single-channel stimu-lator was used to activate the intercostal muscles and acommercially available phrenic pacer to activate onehemidiaphragm . A linking circuit was used to providesynchronous stimulation of both muscle groups . In thefirst patient in whom combined pacing was used,
unilateral diaphragm stimulation resulted in a maximuminspired volume of 600 ml, while combined diaphragmand intercostal stimulation resulted in an inspiredvolume of 1,200 ml . This subject is now comfortablysupported with combined pacing 24 h/day and ismaintaining a PaCO 2 of -33 mmHg. The secondpatient is comfortably maintained off mechanical venti-lation for about 12 h/day; she has chosen to remain onmechanical ventilation at night . Work is in progress todevelop a single system to provide combined intercostaland diaphragm stimulation.
CONCLUSIONS
Ventilation by diaphragm pacing appears to pro-vide both health and lifestyle advantages to the user(36,37). Freedom from the positive pressure ventilatorreduces the risk of tracheal problems : tracheo-malacia,chronic infection, bleeding, and tracheo-esophagealfistula. These are caused by the cuffed tracheostomytube and are often insurmountable . Mechanically venti-lated patients can die suddenly if they become discon-nected from the ventilator or if there is electrical ormechanical device failure . Such risks may be reducedfor the person who uses electrophrenic stimulation.Added benefits of phrenic nerve pacing are the ability tospeak more normally (provided the tracheostomy isclosed, either surgically or with a stopper) and apreserved sense of smell. The phrenic pacer user canexpect increased independence over the mechanicalventilator user ; teenage patients have attended college,others have been gainfully employed, and many havetraveled (27,38,39) . Annual costs of supplies, total timein ventilatory care, and number of assistant hours are allless for phrenic pacing than for mechanical ventilation(40) .
When Glenn reviewed the history of phrenic nervestimulation for respiratory assist in 1988, 488 patientsworldwide were known to have been treated withimplantable devices (10) . The current number is over1,000 . Phrenic pacing is a successful, life-sustainingtechnique proven over 25 years, but the electronictechnology has lagged behind developments in otherapplications, such as heart pacing . It may be that thedevice manufacturers perceive the potential profit fromphrenic pacing to be too limited to expend the effort todevelop better systems.
0 000
e
s
WeeksWeeksn Ckw~~
S
c.,
1
a
.411CIK.Lvi e,
sr
Weeks
PT :KM
'000
000
0
,000
PT:CT

131
CREASEY et al . Electrical Stimulation to Restore Respiration
Recommendations for Further ResearchFurther development of respiratory neuroprosthetic
devices should address the need for:
• A fully implanted battery system of the type thatexists for cardiac pacemakers . This would eliminateexternal antennas and the dangerous possibility ofdecoupling between transmitter and receiver.• A system whose rate is responsive to metabolicneeds. Current systems can be adjusted manually toalter the depth and rate of respiration ; permanentmonitoring of blood gas values would allow moresophisticated closed-loop control.• A system that would coordinate stimulated breathswith the patient's respiratory efforts, if any . Currentlypatients can be taught to synchronize opening of theglottis with stimulation of the diaphragm ; it has beensuggested that opening of the glottis might be sensedand used to trigger the phrenic stimulator.
Some of these principles have been implemented incardiac pacemakers . Even though the population thatcan benefit from phrenic pacemakers is much smaller,there are opportunities for innovative engineers in boththe commercial and academic arenas to work withphysicians to develop totally implanted systems thatwould respond to metabolism and activity.
ACKNOWLEDGMENTS
This paper arose from presentations at the Engi-neering Foundation Conference, "Neural Prostheses:Motor Systems IV," July 23-28, 1994 in Mt. Sterling,OH. The conference was supported by grants from theWhitaker Foundation, the Paralyzed Veterans ofAmerica Spinal Cord Research Foundation, the NationalScience Foundation Grant No . BES-9319988, the Uni-versity of Miami, and the Bakken Research Centre . ThePublic Health Service participated in the support of thismeeting under grant #1R13 HDIN631603-01 from theNational Institute of Child Health and Human Develop-ment of the National Center for Medical Rehabilitationand Research, and the National Institute of NeurologicalDisorders and Stroke.
Instrumentarium Scientific Foundation, Helsinki,generously supported the development of the Finnishphrenic nerve stimulator.
The Austrian group acknowledges the financialsupport of the Austrian Research Foundations FWF and
FFF, the Ministry of Research and Science, and theAustrian National Bank.
REFERENCES
1. Hufeland CW. Usum uis electriciae in asphyxia experimentisillustratum . In: Dissertatio Inauguralis Medica . Germany:Gottingen, 1783.
2. Ure A . An account of some experiments made on the body ofa criminal immediately after execution, with physiological andpractical observations . J Sci Arts (Lond) 1819 :6 :283.
3. Duchenne GBA. De l'Electrisation Localisee et de sonApplication a la Pathologie et a le Therapeutique par CourantInduits et par Courants Galvaniques Interrompus et Continuspar le Dr. Duchenne . Paris: Bailliere, 1872.
4. Beard GM, Rockwell AD . A practical treatise on the medicaland surgical uses of electricity . New York : William Wood,1878 :664.
5. Elefteriades JA. Pacing of the diaphragm. In : Shields TW, ed.General thoracic surgery . Baltimore: Williams & Wilkins,1993 :613-27.
6. Glenn WWL, et al . Total ventilatory support in a quadriplegicpatient with radio frequency electrophrenic respiration . NewEngl J Med 1972 :286 :513-6.
7. Glenn WWL, Gee BL, Schachter EN . Diaphragm pacing:Application to a patient with chronic obstructive pulmonarydisease . J Thorac Cardiovasc Surg 1978 :75 :273-81.
8. Glenn WWL, et al . Ventilatory support for pacing of theconditioned diaphragm in quadriplegia . New Engl J Med1984 :310 :1150-5.
9. Glenn WWL, et al . Twenty years of experience in phrenicnerve stimulation to pace the diaphragm . PACE Pacing ClinElectrophysiol 1986 :9 :780-4.
10. Glenn WWL, Brouillette RT, Dentz B, et al . Fundamentalconsiderations in pacing of the diaphragm for chronicventilatory insufficiency : A multi-center study . PACE PacingClin Electrophysiol 1988:11 :2121-7.
11. Strauss RH, ed . Diving medicine. London : Grune & Stratton,1976.
12. Brouillette RT, Ilbawi MN, Hunt CE . Phrenic nerve pacing ininfants and children : A review of experience and report on theusefulness of phrenic nerve stimulation studies . J Pediatr1983 :102(1) :32-9.
13. MacLean IC, Mattioni TA . Phrenic nerve conduction studies:A new technique and its application in tetraplegic patients.Arch Phys Rehabil 1981 :62:70-3.
14. Moosa A . Phrenic nerve conduction in children . Develop MedChild Neurol 1981 :23 :434-8.
15. Glenn WWL, Sairenji H. Diaphragm pacing in the treatmentof chronic ventilatory insufficiency . In : Roussos C, MacklemPT, eds . The thorax, Part B . New York/Basel : Marcel Dekker,Inc ., 1985 :1407-40.
16.
Kelley WF. Phrenic nerve paralysis . Special consideration ofthe accessory phrenic nerve . J Thoracic Surg 1950 :19 :923-8.
17. Baer GA, Watt J, Partanen-Talsta AA, Talonen PP, KrishnanKR, Hakkinen V . Mechanism of sudden death in patients with

132
Journal of Rehabilitation Research and Development Vol . 33 No . 2 1996
C2 quadriplegia ventilated by aid of a phrenic nerve
stimulator. Amer J Phys Med Rehabil 1992:71(1) :39—40
18. Mayr W, Bijak M, Girsch W, et al . Multichannel stimulation
30.of phrenic nerves by epineural electrodes : Clinical experience
and future developments . ASAIO J 1993 :39(3) :M729—35.
19. Talonen PP, Baer GA, Hakkinen V, Ojala JK . Neurophysi- 31.ological and technical considerations for the design of animplantable phrenic nerve stimulator . Med Biol Eng Comput1990 :28 :31—7.
20. Thoma H. Vorrichtung zur oertlichen and zeitlich variablenelektrischen Reizstrom-Langzeitstimulation eines Reizobjekts,wie Nerven and Muskeln Patent: OS-PS330342, September1976.
21. Girsch W, Koller R, Gruber H, et al . Histological assessmentof nerve lesions caused by epineural electrode application inrat sciatic nerve . J Neurosurg 1991 :74:636—42.
22. Koller R, Girsch W, Liegl CH, et al . Long-term results of 34.nervous tissue alterations caused by epineural electrodeapplication : An experimental study in rat sciatic nerve . PACEPacing Clin Electrophysiol 1992:15(1):108—15.
23. Thoma H, Girsch W, Holle J, Mayr W . Technology andlong-term application of an epineural electrode . ASAIO Trans
1989 :35(3) :490-4.24. Dobelle WH, D'Angelo MS, Goetz BF, et al . 200 cases with a
new breathing pacemaker dispel myths about diaphragmpacing . ASAIO J 1994 :40(3) :M21'1 252.
25. Elefteriades JA, Hogan IF, Handler A, Loke JS . Long-termfollow-up of bilateral pacing of the diaphragm in quadriplegia.New Engi J Med 1992 :326(21) :1433—4.
26. Kim JH, Manuelidis HE, Glenn WWL, Kaneyuki T. Dia-phragm pacing . Histopathological changes in the phrenicnerve following long-term electrical stimulation. J ThoracCardiovasc Surg 1976 :72(4) :602—8.
27. Carter RE. Comparative study of electrophrenic nerve stimu-lation and mechanical ventilation in traumatic spinal cordinjury . Paraplegia 1987 :25 :86—91.
28. Carter RE. Respiratory aspects of spinal cord injury manage-
40.ment . Paraplegia 1987 :25 :262—6.
29. Baer GA, Talonen PP, Shneerson JM, Markkula H, Exner G,Wells FC . Phrenic nerve stimulation for central ventilatory
failure with bipolar and four-pole electrode systems . PACEPacing Clin Electrophysiol 1990:13(8) :1061—72.Agostoni E, Magnoni F, Toni G, Agostoni AF. Static featuresof the passive rib cage and abdomen-diaphragm . J ApplPhysiol 1965 :20:1187—93.DiMarco AF, Altose MD, Cropp A, Durand D . Activation ofthe inspiratory intercostal muscles by electrical stimulation ofthe spinal cord . Am Rev Respir Dis 1987 :136 :1385—90.DiMarco AF, Budzinska K, Supinski GS . Artificial ventilationby means of electrical activation of the intercostal/accessorymuscles alone in anesthetized dogs . Am Rev Respir Dis1989 :139 :961—7.DiMarco AF, Supinski GS, Petro JA, Takaoka Y . Evaluationof intercostal pacing to provide artificial ventilation inquadriplegics. Amer J Respir Crit Care Med 1994:150 :934-40.DiMarco AF, Supinski GS, Budzinska K. Inspiratory muscleactivation in the generation of changes in airway pressure . JAppl Physiol 1989 :66 :2573—8.Supinski GS . Effect of synchronizing intercostal muscle anddiaphragm contraction on inspired volume production (Ab-stract) . Am Rev Respir Dis 1991 :143 :A566.Marcus CL, Jansen MT, Poulsen MK, et al . Medical andpsychosocial outcome of children with congenital centralhypoventilation syndrome . J Pediatr 1991 :119(6) :888—95Ilbawi MN, Idriss FS, Hunt CE, Brouillette RT, DeLeon SY.Diaphragmatic pacing in infants : Techniques and results . AnnThoracic Surg 1985 :40 :323—9Meisner H, Schober JG, Struck E, Lipowsky B, Mayser P,Sebening F. Phrenic nerve pacing for the treatment of centralhypoventilation syndrome: state of the art and case report.Thorac Cardiovasc Surg 1983 :31 :21—5Garrido H, Mazaira J, Gutierrez P, Gonzalez E, Rivas J,Madrazo J . Continuous respiratory support in quadriplegicchildren by bilateral phrenic nerve stimulation . Thorax1987 :42 :573—7Esclarin A, Bravo P, Arroyo 0, Mazaira J, Garrido H, AlcarazMA. Tracheostomy ventilation versus diaphragmatic pace-maker ventilation in high spinal cord injury. Paraplegia1994 :32 :687—93
32.
33.
35.
36.
37.
38.
39 .