Embed Size (px)
Citation preview

Nurses' and Physicians' Perceptions Nursing Authority
of
ELAINE M E N T E R K A T Z M A N , PHD, RN, C *
This study compared perceptions of 163 nurses and physicians of the current and ideal status of the de- cision-making authority of professional nurses. Each nurse and physician agreed or disagreed with 25 items, in two contexts, in the Authority in Nursing Roles Inventory (ANRI). Items in the ANRI describe a variety of nursing roles, functions, and behaviors in health and patient care. The results of the study were statistically significant overall both between and within professional groups. Disparities in several spe- cific areas were revealed. The findings support the premise that in spite of expanded nursing roles em- phasizing nursing authority, there are disagreements between nurses' and physicians' perceptions of the current and ideal authority of nurses as well as areas of dissatisfaction within each professional group, im- plications of continuing conflicts between nurses and physicians as barriers to professional nursing role enactment, as well as strategies to address the prob- lem, are discussed. (index words: Conflict; Percep- tions; Professional nursing; Authority; Power; Nurse- physician relations; Barriers; Decision making) J Prof Nuts 5:208-214, 1989. © 1989 by W.B. Saundets Com- pany.
O VER THE LAST several decades, changes have occurred in the work of professional nurses.
These changes have been discussed by several researchers. 14 Other scholars have examined the power, or lack of power, that nurses have to imple- ment changes in their roles and functions, particularly as such roles interface with those of their physician coworkers. 48
For some nurses the concept of power connotes neg- ative images9; however, the concept of authority has been found to be more acceptable. 10 Both concepts refer to the control nurses have over their own practice and over their independent decision making in health care and patient care. In a previous study conducted
in a Northeastern general hospital, lo the author found that, because of actual or perceived lack of decision- making authority, both staff nurses and nurse practi- tioners were frequently unable to carry out their legal and ethical roles in health and patient care. For ex- ample, the nurses' subordinate status often resulted in dilemmas over whether, or how, to clarify physician- ordered medications which in the nurses' professional judgment were inappropriate.
Furthermore, the study showed that nurses and physicians had disparate perceptions of what the nurs- es' decision-making authority was, as well as what it should be. Based on this qualitative data, the Author- ity in Nursing Roles Inventory (ANRI) was developed to specify quantitatively the amount and the areas of conflict between nurses and physicians, lo
Two primary goals of the ANRI are to identify and quantify the conflict areas between nurses and physi- cians and to evaluate programs and strategies to re- solve the conflicts. This article describes the results of a study using the ANRI to achieve the first goal and makes some suggestions for addressing the second.
Method
SUBJECTS
The sample for this study consisted of 110 nurses and 53 physicians from one southwestern general hos- pital. Their mean ages were 33.5 and 48.5 years, respectively (SD = 10). Most of the nurses were fe- male (98 per cent), and most of the physicians were male (79 per cent). In the nurse group, 19.8 per cent were diploma school graduates, 18.9 per cent had associate degrees, 48 per cent had bachelors' degrees, and 13.2 per cent had master's degrees.
*Assistant Professor, Arizona State University College of Nurs- ing, Tempe, Arizona.
Supported by grant no. 421394 from the Arizona State Uni- versity Faculty Grant-in-Aid Program.
Address reprint requests to Dr Katzman: Arizona State Uni- versity College of Nursing, Tempe, AZ 85287-2602.
© 1989 by W.B. Saunders Company. 8655 -7223/89/0504-0013 $ 3: 00/0
INSTRUMENT AND PROCEDURES
The ANRI is a questionnaire consisting of 25 items (Table 1). Originally, 50 items were generated from the qualitative study and from the literature. After examination by a panel of expert faculty members and nursing practitioners, consensus was achieved on the
2o8 Journal o? Professional Nursing, Vol 5, No 4 (July-August), 1989: pp 208-214
PERCEPTIONS OF NURSING AUTHORITY 209
TABLE 1. M e a n s a n d S t a n d a r d D e v i a t i o n s f o r E a c h I t e m S u b s c o r e
Nurses (n = 99")
Physicians (n = 44*)
Item Mean SD Mean SD Ft
Nurses 1. question unclear physician orders
Current 4.73 0.45 4.47 0.59 Ideal 4.92 0.44 4.71 [).46
2. change inappropriate diets Current 3.52 1.05 2.60 0.99 Ideal 4.04 1.03 2.84 1.14
3. have equal say with physicians re: health policy Current 2.68 1.23 2.18 0.91 Ideal 4.46 0.75 2.20 1.14
4. call physician to clarify medications Current 3.26 1.29 3.62 1.13 Ideal 4.29 1.01 4.22 0.87
5. question inappropriate physician orders Current 4.25 0.80 4.02 0.72 Ideal 4.75 0.44 3.73 1.06
6. decide standards of nursing care Current 4.28 0.77 3.62 1.01 Ideal 4.59 0.67 3.24 1.18
7. initiate physical assessments Current 4.53 0.65 3.87 0.79 Ideal 4.86 0.35 4.53 0.65
8. answer patients' questions re: medical treatment regimen Current 4.53 0.65 3.87 0.79 Ideal 4.38 0.91 3.85 0.98
9. decide what to teach patients Current 3.75 0.89 3.08 U.87 Ideal 4.63 0.61 3.88 0.95
10. modify medications Current 2,21 1.14 2.11 1.03 Ideal 2.98 1.33 1.92 0.95
11. teach health promotion Current 3.81 0,96 3.56 0.78 Ideal 4.69 0.51 4.14 0.61
12. decide care of chronically ill Current 3.67 1.08 3.51 0.81 Ideal 4.54 0.62 3.83 0.87
13. make decisions re: pain management Current 3.78 1.01 3.16 0.93 Ideal 3.65 1.26 2.04 0.96
14. teach self-care Current 4.12 0.74 3.89 0.65 Ideal 4.66 0.50 4.02 0.80
15. assess patients' responses to health problems Current 4.05 0.71 3.64 0.80 Ideal 3.94 1.07 2.96 1.20
16. do many things for patients not under physicians' directions Current 4.30 0.97 3.87 0.81 Ideal 4.62 0.58 3.86 0.91
17. make independent decisions re: changing dressings Current 3.30 1.06 2.84 1.11 Ideal 3.67 1.17 2.67 1.20
18. determine nursing care for patients Current 4.17 0.82 3.56 1.01 Ideal 4.64 0.52 3.31 1.21
19. decide frequency of taking vital signs Current 3.42 1.16 2.56 0.94 Ideal 4.23 0.89 2.63 1.03
20. are not primarily assistants to physicians Current 3.85 1.18 2.53 1.10 Ideal 4.07 1.20 2.63 1.17
8.78 7.21
25.28 41.82
6.03 210.50
NS NS
NS 69.04
18.86 79.6
28.75 16.85
28.7 10.45
17.83 35.2
NS 25.09
NS 33.13
NS 32
12.89 62.6
NS 35.7
9.79 25.4
9.70 38.5
5.62 23.9
~5.38 89.18
19.28 ~5.37
40.71 48.45
(Continued on following page)
210
TABLE 1. M e a n s and S t a n d a r d D e v i a t i o n s f o r Each I tem S u b s c o r e (Con t ' d )
ELAINE MENTER KATZMAN
Nurses Physicians (n = 99*) (n = 44")
Item Mean SD Mean SD F t
21. have as much say as physicians in patient care Current Ideal
22. question inaccurate physicians' medication orders Current Ideal
23. play dominant role in patients' transition to home Current Ideal
24. are accountable for evaluating nursing care Current Ideal
25, (community health nurses) plan programs to protect populations at risk
Current Ideal
2.72 1.13 1.98 0.62 17.47 4.46 0.62 2.98 1.13 107.85
4.25 0.76 3.98 0.75 4.09 4.82 0.57 4,61 0.53 4.74
4.17 0.81 3.58 0.99 12.11 4.61 0.58 3.94 0.90 30.19
4.31 0.83 3.96 0.88 5.55 4.76 0.45 4.16 0.90 30.2I
3.72 0.81 3.67 1.02 NS 4,53 0.60 3.96 0.95 19.72
Abbreviation: NS, not significant. *Numbers reduced because of missing data. 1-P < .0001, df = 1,141 between professional groups.
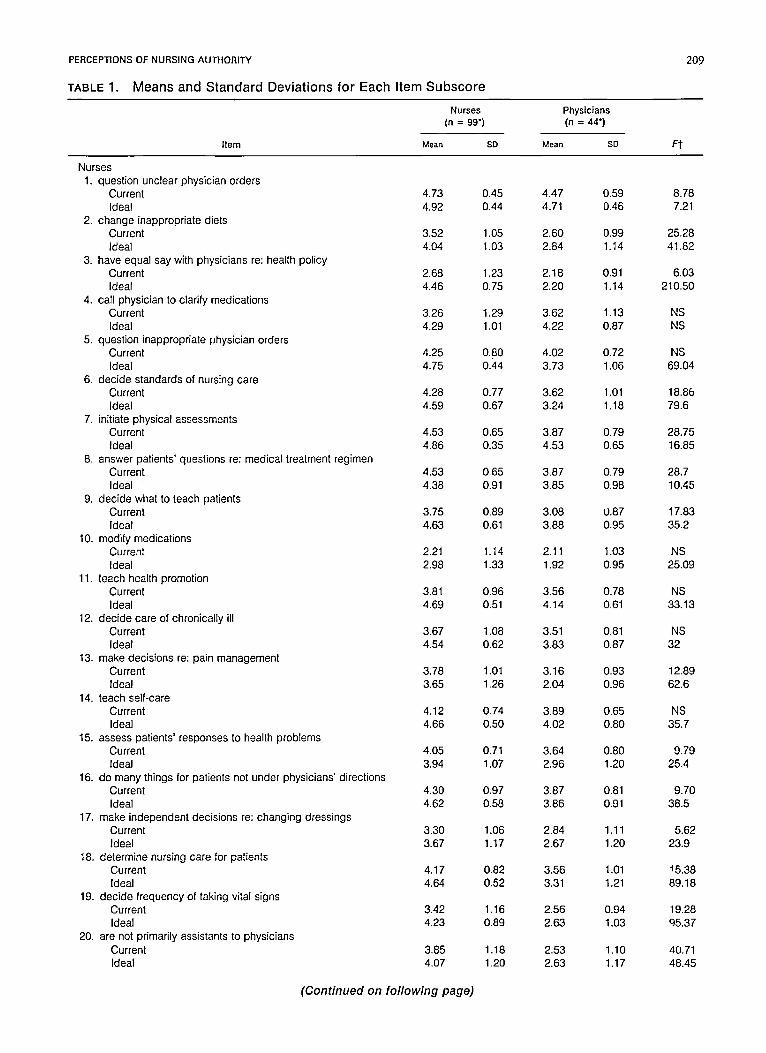
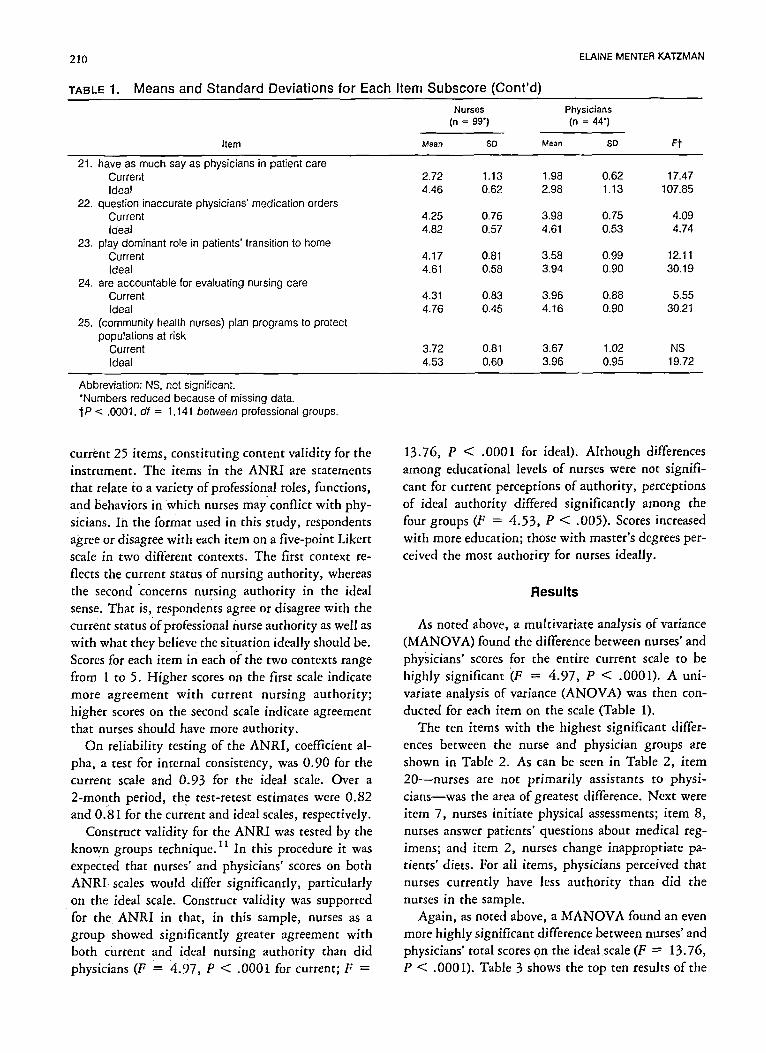
current 25 items, constituting content validity for the instrument. The items in the ANRI are statements that relate to a variety of professional roles, functions, and behaviors in which nurses may conflict with phy- sicians. In the format used in this stUdy, respondents agree or disagree with each item on a five-point Likert scale in two different contexts. The first context re- flects the current status of nursing authority, whereas the Second "concerns nursing authority in the ideal sense. That is, respondents agree or disagree with the current status of professional nurse authority as well as with what they believe the situation ideally should be. Scores for each item in each o[" the two contexts range from 1 to 5. Higher scores on the first scale indicate more agreement with current nursing authority; higher scores on the second scale indicate agreement that nurses should have more authority.
On reliability testing of the ANRI, coefficient al- pha, a test for internal consistency, was 0.90 for the current scale and 0.93 for the ideal scale. Over a 2-month period, the test-retest estimates were 0.82 and 0.81 for the current and ideal scales, respectively.
Construct validity for the ANRI was tested by the known groups technique.ll In this procedure it was expected that nurses' and physicians' scores on both A N R I scales would differ significantly, particularly on the ideal scale. Construct validity was supported for the ANRI in that, in this sample, nurses as a group showed significantly greater agreement with both current and ideal nursing authority than did physicians (F = 4.97, P < .0001 for current; F =
13.76, P < .0001 for ideal). Although differences among educational levels of nurses were not signifi- cant for current perceptions of authority, perceptions of ideal authority differed significantly among the four groups (F = 4.53, P < .005). Scores increased with more education; those with master's degrees per- ceived the most authority for nurses ideally.
Results
As noted above, a multivariate analysis of variance (MANOVA) found the difference between nurses' and physicians' scores for the entire current scale to be highly significant "(F = 4.97, P < .0001). A uni- variate analysis of variance (ANOVA) was then con- ducted for each item on the scale (Table 1).
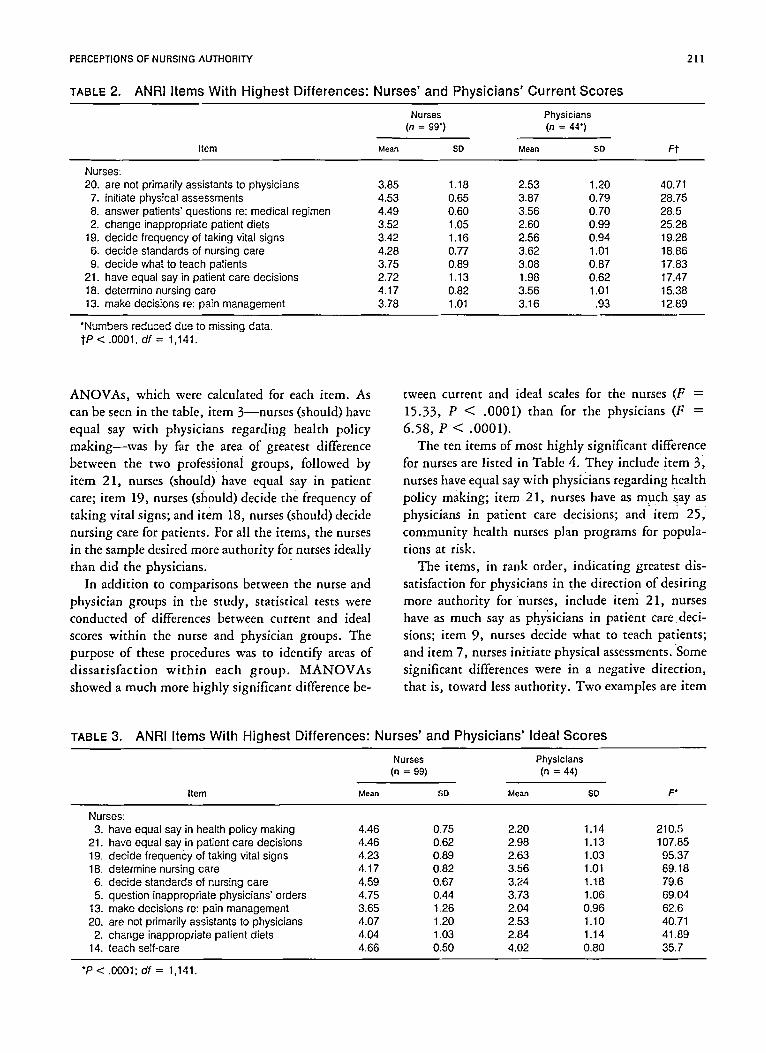
The ten items with the highest significant differ- ences between the nurse and physician groups are shown in Table 2. As can be seen in Table 2, item 20---nurses are not primarily assistants to physi- c ians-was the area of greatest difference. Next were item 7, nurses initiate physical assessments; item 8, nurses answer patients' questions about medical reg- imens; and item 2, nurses change inappropriate pa- tients' diets. For all items, physicians perceived that nurses currently have less authority than did the nurses in the sample.
Again, as noted above, a MANOVA found an even more highly significant difference between nurses' and physicians' total scores on the idealscale (F --- 13.76, P < .0001). Table 3 shows the top ten results of the
PERCEPTIONS OF NURSING AUTHORITY
TABLE 2. ANRI I tems Wi th H i g h e s t D i f f e r e n c e s : Nu rses ' and P h y s i c i a n s ' C u r r e n t S c o r e s
211
Nurses Physicians (n = 99") (n = 44")
Item Mean SD Mean SD F t
Nurses: 20. are not primarily assistants to physicians 3.85 1.18 2.53 1.20 40.71
7. initiate physical assessments 4.53 0.65 3.87 0.79 28.75 8. answer patients' questions re: medical regimen 4.49 0.60 3.56 0.70 28.5 2. change inappropriate patient diets 3.52 1.05 2.60 0.99 25.28
19. decide frequency of taking vital signs 3.42 1.16 2.56 0.94 19.28 6. decide standards of nursing care 4.28 0.77 3.62 1.01 18.86 9. decide what to teach patients 3.75 0.89 3.08 0.87 17.83
21. have equal say in patient care decisions 2.72 1.13 1.98 0.62 17.47 18. determine nursing care 4.17 0.82 3.56 1.01 15.38 13. make decisions re: pain management 3.78 1.01 3.16 .93 12.89
*Numbers reduced due to missing data. I"P < .0001, df = 1,141.
ANOVAs, which were calculated for each item. As can be seen in the table, item 3--nurses (should) have equal say with physicians regarding health policy making--was by far the area of greatest difference between the two professionai groups, followe d by item 21, nurses (should) have equal say in patient care; item 19, nurses (should) decide the frequency of taking vital signs; and item 18, nurses (should) decide nursing care for patients. For all the items, the nurses in the sample desired more authority for nurses ideally than did the physicians.
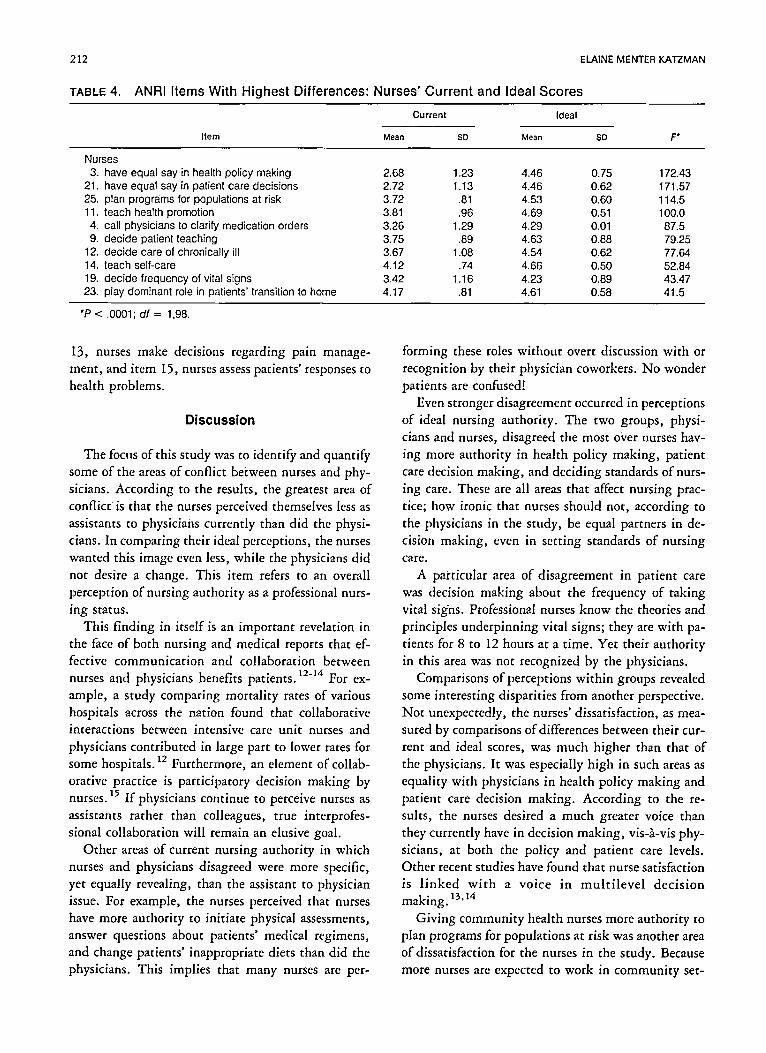
In addition to comparisons between the nurse and physician groups in the study, statistical tests were conducted of differences between current and ideal scores within the nurse and physician groups. The purpose of these procedures was to identify areas of dissatisfaction wi th in each group. MANOVAs showed a much more highly significant difference be-
tween current and ideal scales for the nurses (F = 15.33, P < .0001) than for the physicians (F = 6.58, P < .0001).
The ten items of most highly significant difference for nurses are listed in Table 4. They include item 3' nurses have equal say with physicians regarding health policy making; item 21, nurses have as much say as physicians in patient care decisions; and item 25, community health nurses plan programs for popula- tions at risk.
The items, in rank order, indicating greatest dis- satisfaction for physicians in the direction of desiring more authority for nurses, include item 21, nurses have as much say as ph.ysicians in patient care deci- sions; item 9, nurses decide what to teach patients; and item 7, nurses initiate physical assessments. "Some significant differences were in a negative direction, that is, toward less authority. Two examples are item
TABLE 3. ANRI I tems Wi th H i g h e s t D i f f e rences : Nu rses ' and P h y s i c i a n s ' Idea l S c o r e s
Nurses Physicians (n = 99) (n = 44)
Item Mean SD Mean SD F °
Nurses; 3. have equal say in health policy making 4.46 0.75 2.20 1.14 210.5
21. have equal say in patient care decisions 4.46 0.62 2.98 1.13 107.85 19. decide frequency of taking vital signs 4.23 0.89 2.63 1.03 95.37 18, determine nursing care 4.17 0.82 3.56 1.01 89.18 6. decide standards of nursing care 4.59 0.67 3.24 1.18 79.6 5. question inappropriate physicians' orders 4.75 0.44 3.73 1.06 69.04
13. make decisions re: pain management 3.65 1.26 2.04 0.96 62.6 20. are not primarily assistants to physicians 4.07 1.20 2.53 1.10 40.71 2. change inappropriate patient diets 4.04 1.03 2.84 1.14 41.89
14. teach self-care 4.66 0.50 4.02 0.80 35.7
*P < .0001;d f = 1,141.
212 ELAINE MENTER KATZMAN
TABLE 4. ANRI Items With Highest Differences: Nurses' Current and Ideal Scores
Current Ideal
Item Mean SD Mean SD F*
Nurses 3. have equal say in health policy making 2.68 1.23 4.46 0.75 172.43
21. have equal say [n patient care decisions 2.72 1.13 4.46 0.62 171.57 25. plan programs for populations at risk 3.72 .81 4.53 0.60 114.5 11. teach health promotion 3.81 .96 4.69 0.51 100.0 4. call physicians to clarify medication orders 3.26 1.29 4.29 0,01 87.5 9. decide patient teaching 3.75 .89 4.63 0,88 79.25
12. decide care of chronically ill 3.67 1.08 4.54 0.62 77.64 14. teach self-care 4.12 .74 4.66 0.50 52.84 19. decide frequency of vital signs 3.42 1.16 4.23 0.89 43.47 23. play dominant role in patients" transition to home 4.17 .81 4.61 0.58 41.5
"P < .0001; df = 1,98.
13, nurses make decisions regarding pain manage- ment, and item 15, nurses assess patients' responses to health problems.
Discussion
The focus of this study was to identify and quantify some of the areas of conflict between nurses and phy- sicians. According to the results, the greatest area of conflict is that the nurses perceived themselves less as assistants t o physicians currently than did the physi- cians. In comparing their ideal perceptions, the nurses wanted this image even less, while the physicians did not desire a change. This item refers to an overall perception of nursing authority as a professional nurs- ing status.
This finding in itself is an important revelation in the face of both nursing and medical reports that ef- fective communication and collaboration between nurses and physicians benefits patients. 12-1~i For ex- ample, a study comparing mortality rates of various hospitals across the nation found that collaborative interactions between intensive care unit nurses and physicians contributed in large part to lower rates for some hospitals. 12 Furthermore, an element of collab- orative practice is participatory decision making by nurses. 15 If physicians continue to perceive nurses as assistants rather than colleagues, true interprofes- sionaI collaboration will remain an elusive goal.
Other areas of current nursing authority in which nurses and physicians disagreed were more specific, yet equally revealing, than the assistant to physician issue. For example, the nurses perceived that nurses have more authority to initiate physical assessments, answer questions about patients' medical regimens, and change patients' inappropriate diets than did the physicians. This implies that many nurses are per-
forming these roles without overt discussion with or recognition by their physician coworkers. No wonder patients are confused!
Even stronger disagreement occurred in perceptions of ideal nursing authority. The two groups, physi- cians and nurses, disagreed the most over nurses hav- ing more authority in health policy making, patient care decision making, and deciding standards of nurs- ing care. These are all areas that affect nursing prac- tice; how ironic that nurses should not, according to the physicians in the study, be equal partners in de- cision making, even in setting standards of nursing care.
A particular area of disagreement in patient care was decision making about the frequency of taking vital signs. Professional nurses know the theories and principles underpinning vital signs; they are with pa- tients for 8 to 12 hours at a time. Yet their authority in this area was not recognized by the physicians.
Comparisons of perceptions within groups revealed some interesting disparities from another perspective. Not unexpectedly, the nurses' dissatisfaction, as mea- sured by comparisons of differences between their cur- rent and ideal scores, was much higher than that of the physicians. It was especially high in such areas as equality with physicians in health policy making and patient care decision making. According to the re- sults, the nurses desired a much greater voice than they currently have in decision making, vis-a-vis phy- sicians, at both the policy and patient care levels. Other recent studies have found that nurse satisfaction is l inked wi th a voice in mul t i l eve l decision making. 13,14
Giving community health nurses more authority to plan programs for populations at risk was another area of dissatisfaction for the nurses in the study. Because more nurses are expected to work in community set-

PERCEPTIONS OF NURSING AUTHORITY 213
tings than in hospitals by the new century, this find- ing has particular futuristic implications for nursing. An essential aspect of nursing in communities is the programmatic approach to reaching large numbers of people for health promotion and health teaching.
The physicians' dissatisfaction with the status quo was much less than the nurses' and was limited to more authority for nurses in patient care decisions, patient teaching, and physical assessments. While the nurses were also dissatisfied with their status in each of these areas, the physicians were much less so, in- dicating further discrepancies between levels of nurs- ing authority desired by each group.
Summary and Conclusions
The results of this study showed that a sample of nurses and physicians had conflicting perceptions of the status of nursing authority, currently and ideally, in health and patient care. The tests of differences were statistically significant overall for the ANRI, both between and within groups. The analyses re- vealed a number of areas of disagreement and dissat- isfaction in nursing roles and functions.
These findings support the thesis that, in spite of expanded nursing roles with an emphasis on nursing authority (power), not all health professionals are sup- portive of true professional status for nurses. In fact, the conflicts between nurses and physicians have be- come barriers to professional nursing role enactment which in turn place patients and the health care sys- tem at risk.
The findings indicate a need for closer communi- cation and consensus regarding nursing's scope of practice. This effort is critical considering the amount of time nurses spend with patients compared with physicians, 1° the difficulty of and amount of time nurses spend contacting physicians, 1o and the content of educational programs for preparing professional
16,17 nurses. Once recognized and acknowledged by both
groups, the disparities between nurses and physicians can begin to be addressed. Programs and strategies can be designed to promote understanding of the link
between quality, cost-effective health and patient care and the authority of nurses to function fully within their legal and ethical scope of practice. In one pro- gram, a focus might be on role modeling and men- toring by experienced nurses to show novice nurses that knowledge and expertise can be powerful medi- ators of seemingly unequal relationships among pro- fessionals. Another program might emphasize net- working among nurses to provide support for all nurs- ing peers w i t h i n and b e t w e e n s e t t i n g s . Interprofessional dialogues sponsored by health, med- ical, and nursing administrators can focus on improv- ing nurse-physician relations at the patient's bedside so that patients can observe them firsthand. Such di- alogues can also help set the stage for acceptance of new entreprenurial nursing roles. 18 In these ways, as well as others already in place, health professionals can work toward promoting collegial, collaborative inter- professional relationships and toward excellence in health and patient care.
These goals have been recognized by the American Nurses' Association (ANA) which, in responding to the nursing shortage and the American Medical As- sociation's (AMA) proposed new health care worker (the registered care technologist or RCT), has sug- gested that a voice in decisions that affect patients will help retain nurses and also attract new nurses into the profession. Furthermore, the ANA believes that the AMA should support nurses in these endeavors. 19
In the current climate in health care delivery and nurse-physician relations, the ANRI can play an im- portant role in identifying nurse-physician conflicts in various settings. 2° In turn, the ANRI can measure changes brought about by conflict resolution and other programmatic strategies. Such efforts can go a long way toward achieving excellence in health and patient care which is, of course, what both nursing and medicine profess to be about.
Acknowledgment
The author gratefully acknowledges the assistance of Kathryn Coe, MA, writer/editor, and Joseph 1". Hepworth, PhD, statistician, grant no. 5, D10 NU29151, Division of Nurs- ing, USDHHS, in reviewing this article for publication.
References
1. Belez E: Is nursing's public image up to date? Nuts Outlook 22:432-435, 1974
2. Hughes L: The public image of the nurse. Adv Nurs Sci 2:55-72, 1980
3. Kalisch P, Kalisch B: The Changing Image of the Nurse. Menlo Park, CA, Addison-Wesley, 1987
4. Damrosch S, Sullivan P, Haldeman L: How nurses get their way: Power strategies in nursing. J Prof Nurs 3:284-289, 1987
5. Katzman E: Nurse-physician conflicts as barriers to the enactment of nursing roles. West J Nurs Res 10:576- 599, 1988
214 ELAINE MENTER KATZMAN
6. Weiss S, Remen N: Self-limiting patterns of nursing behavior within a tripartite context involving consumers and physicians. West J Nurs Res 5:77-79, 1983
7. Weiss S: The influence of discourse on collaboration among nurses, physicians, and consumers. Res Nurs Health 8:49-59, 1985
8. Kalisch B, Kalisch P: An analysis of the sources of physicians' and nurses' conflict, in MuffJ (ed) Socialization, Sexism, and Stereotyping. St Louis, Mosby, 1982
9. Heineken J: Power: Conflicting views. J Nurs Adm 15:36, 1985
10. Katzman E: The influence of stereotypical male- female attitudes and behaviors on role transitions in nurs- ing and on nurse-physician interprofessional relations. Doc- toral dissertation, Syracuse University, Syracuse, NY, 1985
11. Polk D, Hungler B: Nursing Research: Principles and Methods. Philadelphia, Lippincott, 1983
12. Knaus WA, Draper EA, Wagner DP, et al: An evaluation of outcome from intensive care in major medical centers. Ann Intern Med 104:410-418, 1986
13. Michelson EL: Collaborative practice. Heart Lung 17:390-391, 1988
14. Cannon P: The professional ethics and practice com- mittee: A step toward the achievement of excellence. Nuts Adm Q 12:53-56, 1988
15. Cape LS: Collaborative practice models and struc- tures, In England DA (ed) Collaboration in Nursing. Rock- ville, MD, Aspen, 1986
16. Keenan R, Aiken L, Cluff L: Nurses and Doctors: Their Education and Practice. Cambridge, MA, Oelgescha- lager, 198i
17. Mechanic D, Aiken L: A cooperative agenda for medicine and nursing. N Engl J Med 307:747-750, 1982
18. Clark L, Quinn J: The new entrepreneurs. Nurs Health Care 9:6-15, 1988
19. American Nurses' Association Position Paper. Lou- isville, KY, American Nurses' Association, June 1988
20. Melosh B: The Physician's Hand: Work Culture and ConflictAn American Nursing. Philadelphia, Temple University, 1982





























