Embed Size (px)
Citation preview
Nursing and MidwiferyWorkload and Workforce
Planning Project:A Good Practice Guide in the
Use of Supplementary Staffing
Nursing and MidwiferyWorkload and Workforce
Planning Project:A Good Practice Guide in theUse of Supplementary Staffing
The Scottish Government, November 2007
© Crown copyright 2007
ISBN: 978-0-7559-5442-1
The Scottish GovernmentSt Andrew’s HouseEdinburghEH1 3DG
Produced for the Scottish Government by RR Donnelley B51843 12/07
Published by the Scottish Government, December, 2007
Further copies are available fromBlackwell’s Bookshop53 South BridgeEdinburghEH1 1YS
The text pages of this document are printed on recycled paper and are 100% recyclable

Contents
Foreword by the Chief Nursing Officer iv
Introduction 2
1. The Bigger Picture 3
2. Getting the best from the Nurse Bank 7
3. Getting the best from the Bank Nurse 11
iii
iv
Foreword by the Chief Nursing Officer
Ensuring that there are sufficient numbers of nursing staff with the rightskills and competencies to deliver the high quality of care people inScotland demand of their NHS is part and parcel of the day-to-day lifeof operational managers and nurse leaders throughout the country.
Their primary resource in meeting this demand is the nurses employedwithin the substantive workforce of NHS boards. When short- or longer-term deficiencies in supply of nurses from the substantive workforceoccur, they turn to what is termed “supplementary staffing” resources –nurses employed through the nurse bank.
Nurse banks consist of groups of nurses employed to work on aflexible as-and-when-required basis to cover for planned andunplanned shortfalls in the nurse staffing establishment. Bank nursescan work across all the clinical services provided by NHS boards inhospital and community settings, depending on their skills,competencies and experience.
The Nationally Co-ordinated Nurse Bank Arrangements report,published in 2005, analysed the pattern of usage of bank nurses inNHSScotland at that time. While the report found much to be admiredin the way supplementary staffing was being handled within the NHS, italso highlighted areas in which a different approach would providebetter standards of care for service users and better value for moneyfor the service.
It is fair to say that the management and deployment of supplementarystaff in NHS boards in Scotland has come a long way since that time,with significant improvements in appropriate use of bank nurses ratherthan more expensive options. But nurse bank managers across Scotlandfeel there is still more that can be done to improve the situation.
Nurse bank managers have been putting forward a clear message thatthey can help their local NHS boards to manage the supply ofsupplementary staffing, but that their sphere of influence does notextend to managing the demand for supplementary staff – aresponsibility that lies with managers in direct care settings. As a result,nurse bank managers across Scotland have developed this GoodPractice Guide for frontline staff and managers.
It is a practical guide that will help them review and improve their roleand responsibilities in the management of nurse staffing and whichsets out the qualities substantive staff can expect to see in banknurses. It also provides helpful support to nurse bank managers in therunning of nurse banks by setting out what works well (and why itworks well) from the perspectives of people who have significantexperience in managing a supplementary staffing service.
The Guide also helps to promote the importance of nurse banks tonurses’ professional development. Providing services via a nurse bankis becoming increasingly recognised as an important point in a nurse’scareer. It is not the end-point of that career – a “winding down” towardsretirement – but is a stage in a career development profile that fits withindividuals’ lifestyles and in which nurses can gain excellent experiencethat will position them well to attain substantive posts in the NHS whenthe time is right for them.
But the most important thing is to emphasise the ultimate end-point ofa nurse bank service - the delivery of a high quality service for patientsand clients. Bank nurses make a significant contribution to frontlineservices in the NHS, and the better trained, developed and supportedthey are, the higher the quality of care they will deliver to patients andclients.
This Good Practice Guide will, I believe, help managers and frontlinestaff in NHSScotland put together the diverse elements that make upan excellent nurse bank service, resulting in significant clinical benefitsfor patients and clients, significant professional benefits for banknurses, and significant cost savings for the NHS.
Paul MartinChief Nursing Officer
1
2
Introduction
In 2005, the Scottish Executive charged NHS boards in Scotland withaddressing the recommendations of the report Nationally Co-ordinatedNurse Bank Arrangements.1 This was followed by a second report in20062 with further detail on methodology and fuller results of theoriginal project.
The reports were produced to support NHS employers to maximise thecontribution of nursing staff employed in nurse banks, consequentlyreducing reliance on agency nursing staff. National spend on nurseagency at the time was unacceptably high.
The main ways of implementing the recommendations of the reportswere through:
• improving the management of nurse banks;• consolidating the management of nurse banks to NHS board level;• ensuring effective information technology was in place to supportnurse bank management; and
• introducing a national contract for nurse agency use in NHSScotland.
Nurse bank managers across Scotland have been networking anddeveloping best practice as part of the process of implementation.Their aim is to ensure that nurse banks are run as effectively andefficiently as possible, and that nurse banks are promoted as an optionto help substantive staff manage their demand for bank or agencystaff.
The Good Practice Guide highlights the organisational policies andresponsibilities of those who manage the nurse staffing resourcethrough, for example, staff rostering, use of workload tools, managingsickness and absence and annual leave, providing both the rationaleand a means of assessing the ward, care setting or organisationalposition. It has three main sections:
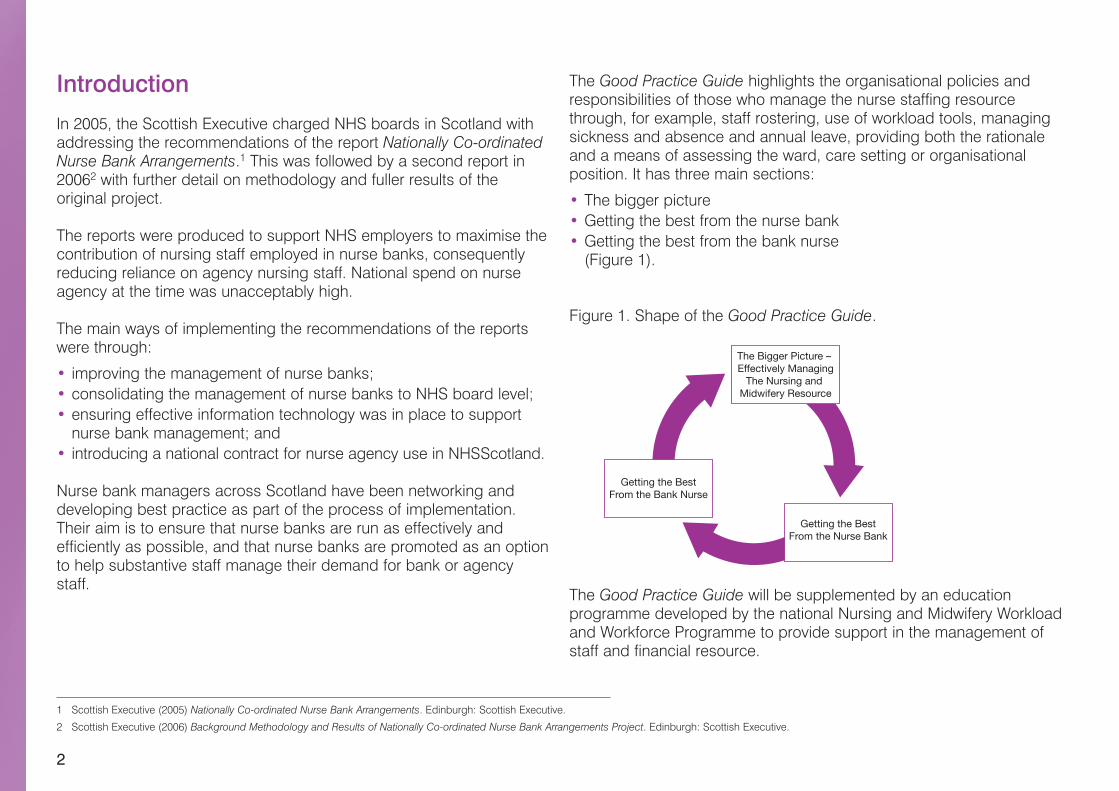
• The bigger picture• Getting the best from the nurse bank• Getting the best from the bank nurse(Figure 1).
Figure 1. Shape of the Good Practice Guide.
The Good Practice Guide will be supplemented by an educationprogramme developed by the national Nursing and Midwifery Workloadand Workforce Programme to provide support in the management ofstaff and financial resource.
1 Scottish Executive (2005) Nationally Co-ordinated Nurse Bank Arrangements. Edinburgh: Scottish Executive.
2 Scottish Executive (2006) Background Methodology and Results of Nationally Co-ordinated Nurse Bank Arrangements Project. Edinburgh: Scottish Executive.
The Bigger Picture – Effectively Managing
The Nursing and Midwifery Resource
Getting the BestFrom the Nurse Bank
Getting the BestFrom the Bank Nurse

1. The Bigger Picture
4
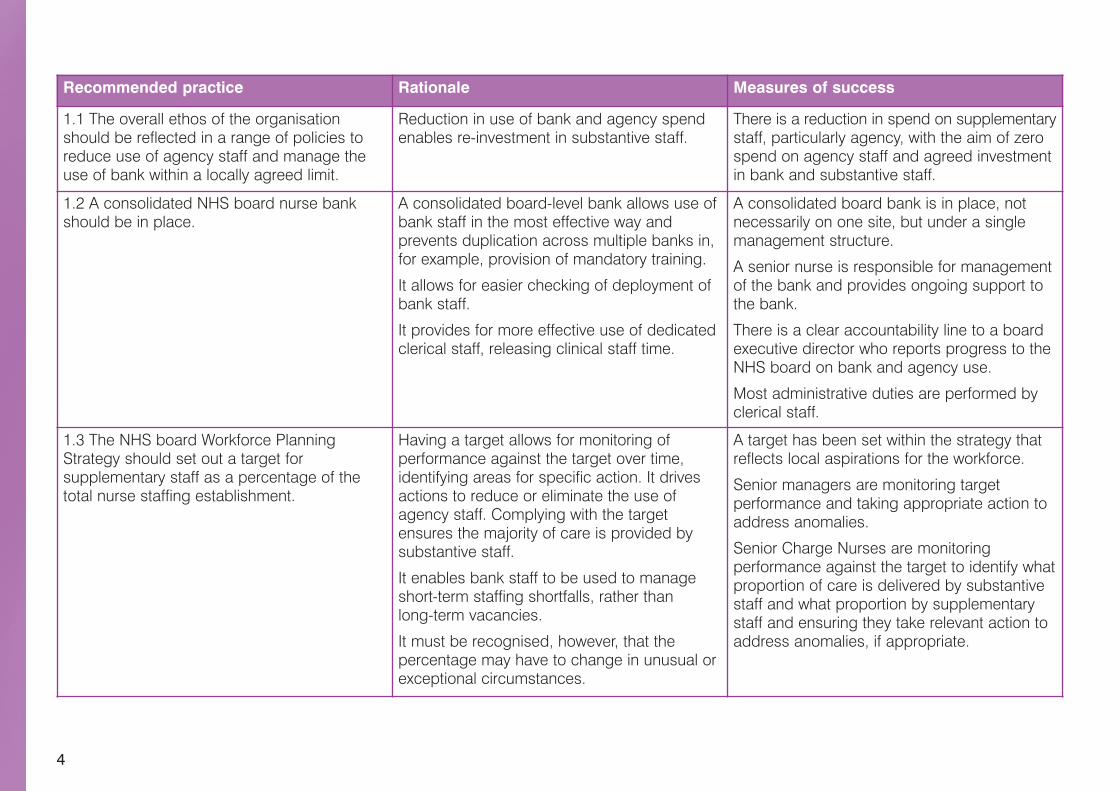
Recommended practice Rationale Measures of success
1.1 The overall ethos of the organisationshould be reflected in a range of policies toreduce use of agency staff and manage theuse of bank within a locally agreed limit.
Reduction in use of bank and agency spendenables re-investment in substantive staff.
There is a reduction in spend on supplementarystaff, particularly agency, with the aim of zerospend on agency staff and agreed investmentin bank and substantive staff.
1.2 A consolidated NHS board nurse bankshould be in place.
A consolidated board-level bank allows use ofbank staff in the most effective way andprevents duplication across multiple banks in,for example, provision of mandatory training.
It allows for easier checking of deployment ofbank staff.
It provides for more effective use of dedicatedclerical staff, releasing clinical staff time.
A consolidated board bank is in place, notnecessarily on one site, but under a singlemanagement structure.
A senior nurse is responsible for managementof the bank and provides ongoing support tothe bank.
There is a clear accountability line to a boardexecutive director who reports progress to theNHS board on bank and agency use.
Most administrative duties are performed byclerical staff.
1.3 The NHS board Workforce PlanningStrategy should set out a target forsupplementary staff as a percentage of thetotal nurse staffing establishment.
Having a target allows for monitoring ofperformance against the target over time,identifying areas for specific action. It drivesactions to reduce or eliminate the use ofagency staff. Complying with the targetensures the majority of care is provided bysubstantive staff.
It enables bank staff to be used to manageshort-term staffing shortfalls, rather thanlong-term vacancies.
It must be recognised, however, that thepercentage may have to change in unusual orexceptional circumstances.
A target has been set within the strategy thatreflects local aspirations for the workforce.
Senior managers are monitoring targetperformance and taking appropriate action toaddress anomalies.
Senior Charge Nurses are monitoringperformance against the target to identify whatproportion of care is delivered by substantivestaff and what proportion by supplementarystaff and ensuring they take relevant action toaddress anomalies, if appropriate.
5
Recommended practice Rationale Measures of success
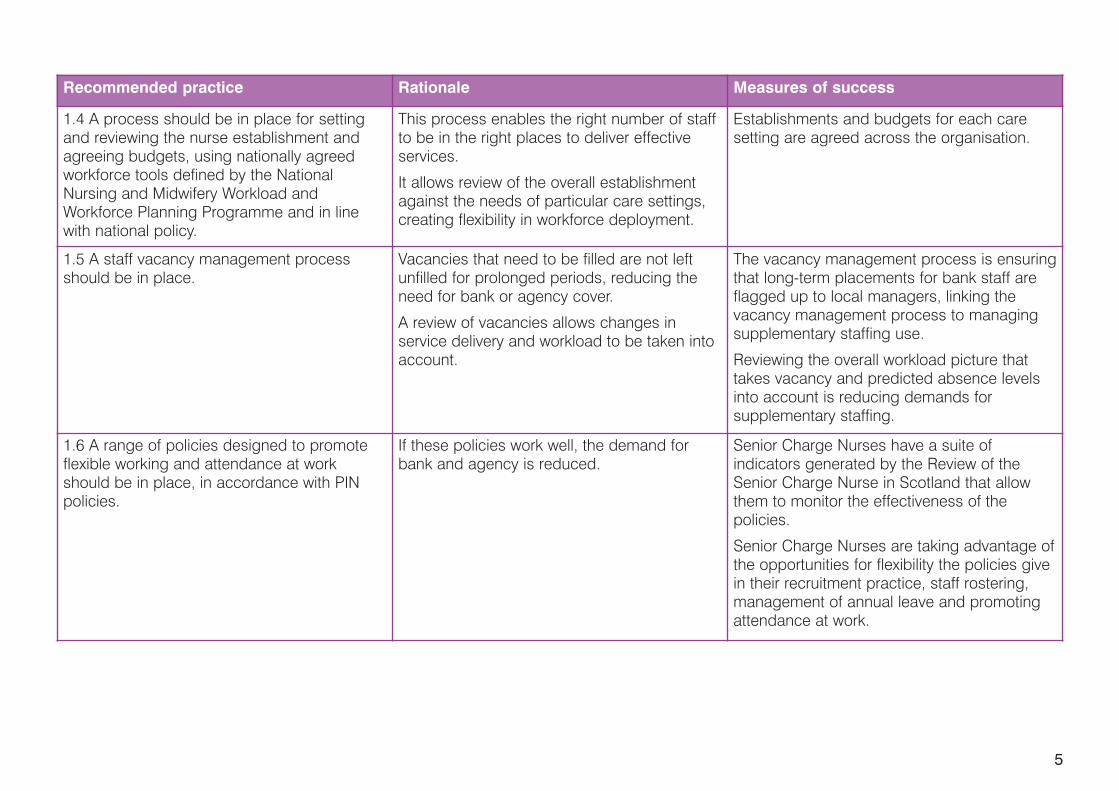
1.4 A process should be in place for settingand reviewing the nurse establishment andagreeing budgets, using nationally agreedworkforce tools defined by the NationalNursing and Midwifery Workload andWorkforce Planning Programme and in linewith national policy.
This process enables the right number of staffto be in the right places to deliver effectiveservices.
It allows review of the overall establishmentagainst the needs of particular care settings,creating flexibility in workforce deployment.
Establishments and budgets for each caresetting are agreed across the organisation.
1.5 A staff vacancy management processshould be in place.
Vacancies that need to be filled are not leftunfilled for prolonged periods, reducing theneed for bank or agency cover.
A review of vacancies allows changes inservice delivery and workload to be taken intoaccount.
The vacancy management process is ensuringthat long-term placements for bank staff areflagged up to local managers, linking thevacancy management process to managingsupplementary staffing use.
Reviewing the overall workload picture thattakes vacancy and predicted absence levelsinto account is reducing demands forsupplementary staffing.
1.6 A range of policies designed to promoteflexible working and attendance at workshould be in place, in accordance with PINpolicies.
If these policies work well, the demand forbank and agency is reduced.
Senior Charge Nurses have a suite ofindicators generated by the Review of theSenior Charge Nurse in Scotland that allowthem to monitor the effectiveness of thepolicies.
Senior Charge Nurses are taking advantage ofthe opportunities for flexibility the policies givein their recruitment practice, staff rostering,management of annual leave and promotingattendance at work.

6
Recommended practice Rationale Measures of success
1.7 There must be complete compliance withHDL (2006) 39,3 which mandates the use ofnationally contracted agency suppliers.
Compliance with this HDL is mandatory inNHSScotland; failure to do so breachesEuropean procurement law.
Contract compliance is monitored on aquarterly basis at a national level. IndividualNHS boards are measuring and reacting totheir own data on contract compliance.
1.8 Strategies that prevent manipulation of thenurse staffing market should be in place.
Appropriate strategies will protect NHS fundsand ensure the service gets best value formoney from spend on supplementary staffing.
No current member of staff is engaged towork in the service on a regional basis throughan agency.
1.9 The organisation should agree the mostappropriate forum to performance manage allof the above, with appropriate representationacross partnership organisations, humanresources, finance, nursing and the bank.
This will put in place the mechanisms toensure organisational accountability for goodfinancial management, staff, corporate andclinical governance and good patient care. Itwill also identify areas for specific action.
An identified forum within the organisation isundertaking ongoing review of performanceagainst board policy and putting mechanismsin place to deal with problems.
Reports on performance are prepared andpresented to the board for scrutiny.
3 For more on HDL (2006) 39, see: http://www.sehd.scot.nhs.uk/mels/HDL2006_39.pdf.

2. Getting the best from the Nurse Bank

8
Recommended practice Rationale Measures of success
2.1 There should be adequate office spaceand resource and facilities to enable effectivefunctioning of the bank.
The bank requires accommodation andresource commensurate with its importance tothe organisation.
There are recognisable nurse bank premiseswith good facilities within the organisation, onsingle or multiple sites.
2.2 The bank should use one of the twoaccredited software systems for managingnurse banks in Scotland.
Complex information systems in nurse banksrequire adequate IT provision. Using anaccredited system ensures the software meetsthe Scottish Government’s prescribedspecification for nurse bank IT systems.
There is consistency in capability of accreditedsoftware systems.
An accredited software system withappropriate staff training programmes tooptimise use is in place.
The bank is supported by a nationallyaccredited IT system.
2.3 The same pre-employment checks used inthe recruitment of nurses to the substantiveworkforce should be used for recruiting banknurses.
This helps to ensure consistency inrecruitment practice across the nursingworkforce.
The message that bank nurses are consideredequal employees is promoted.
There is equality in the recruitment processesused for recruiting nurses to the substantiveand bank workforce.
2.4 There should be adequate capacity withinNHS boards to ensure that bank nurses haveaccess to mandatory training opportunities asappropriate.
Supplying appropriate mandatory trainingopportunities for staff is a requirement of allNHS boards and is an essential element inensuring patient, public and staff safety.
Capacity and systems are in place within NHSboards to ensure that mandatory trainingrequirements of bank nurses are recognised,supplied, recorded and regularly monitored.Findings are managed through a plannedprogramme of development.
9
Recommended practice Rationale Measures of success
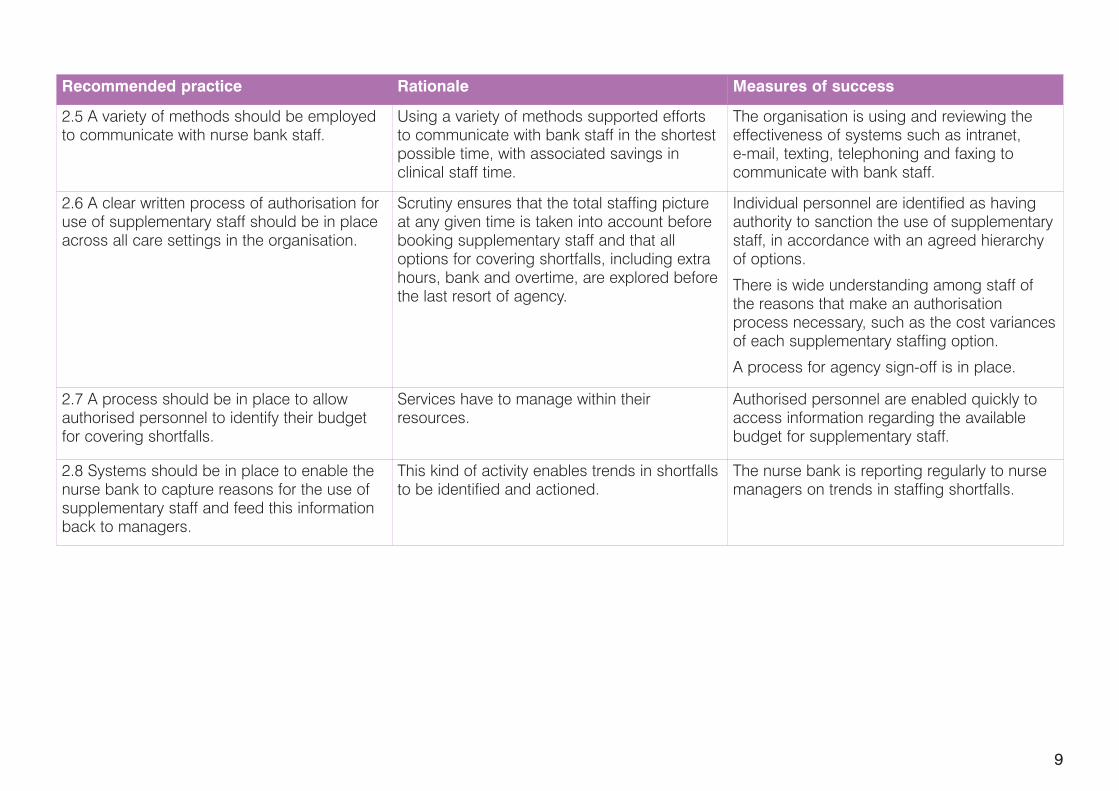
2.5 A variety of methods should be employedto communicate with nurse bank staff.
Using a variety of methods supported effortsto communicate with bank staff in the shortestpossible time, with associated savings inclinical staff time.
The organisation is using and reviewing theeffectiveness of systems such as intranet,e-mail, texting, telephoning and faxing tocommunicate with bank staff.
2.6 A clear written process of authorisation foruse of supplementary staff should be in placeacross all care settings in the organisation.
Scrutiny ensures that the total staffing pictureat any given time is taken into account beforebooking supplementary staff and that alloptions for covering shortfalls, including extrahours, bank and overtime, are explored beforethe last resort of agency.
Individual personnel are identified as havingauthority to sanction the use of supplementarystaff, in accordance with an agreed hierarchyof options.
There is wide understanding among staff ofthe reasons that make an authorisationprocess necessary, such as the cost variancesof each supplementary staffing option.
A process for agency sign-off is in place.
2.7 A process should be in place to allowauthorised personnel to identify their budgetfor covering shortfalls.
Services have to manage within theirresources.
Authorised personnel are enabled quickly toaccess information regarding the availablebudget for supplementary staff.
2.8 Systems should be in place to enable thenurse bank to capture reasons for the use ofsupplementary staff and feed this informationback to managers.
This kind of activity enables trends in shortfallsto be identified and actioned.
The nurse bank is reporting regularly to nursemanagers on trends in staffing shortfalls.
10
Recommended practice Rationale Measures of success
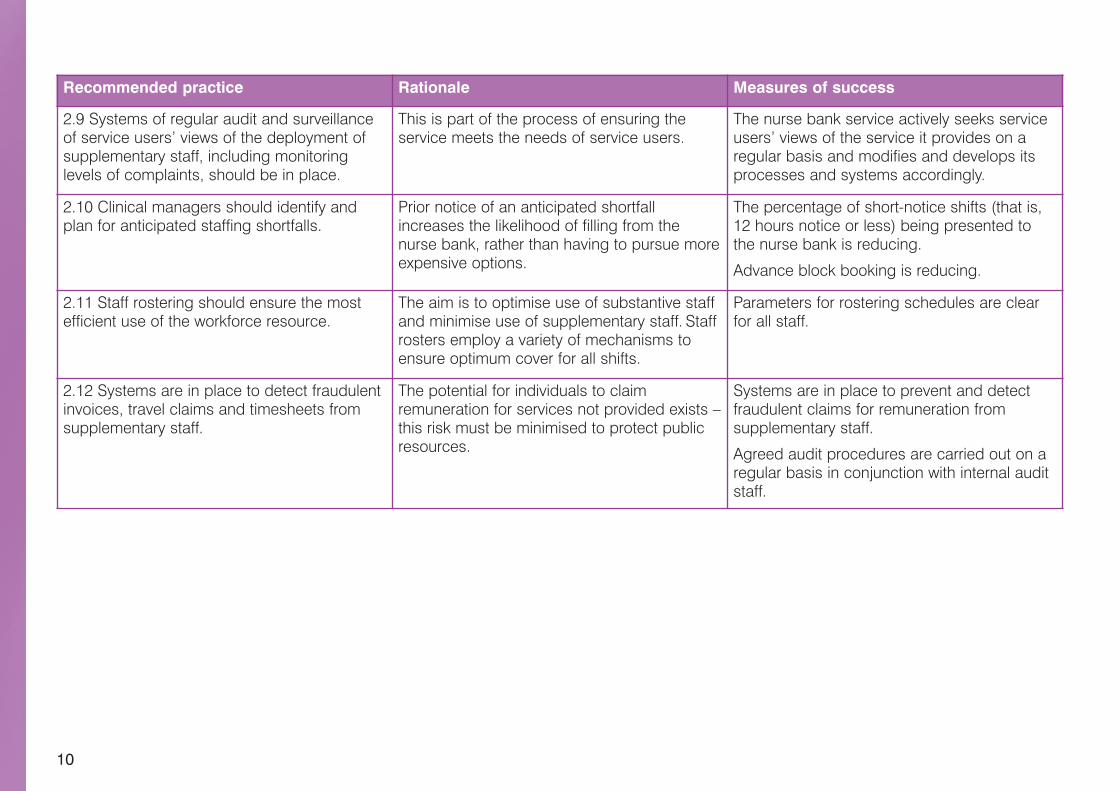
2.9 Systems of regular audit and surveillanceof service users’ views of the deployment ofsupplementary staff, including monitoringlevels of complaints, should be in place.
This is part of the process of ensuring theservice meets the needs of service users.
The nurse bank service actively seeks serviceusers’ views of the service it provides on aregular basis and modifies and develops itsprocesses and systems accordingly.
2.10 Clinical managers should identify andplan for anticipated staffing shortfalls.
Prior notice of an anticipated shortfallincreases the likelihood of filling from thenurse bank, rather than having to pursue moreexpensive options.
The percentage of short-notice shifts (that is,12 hours notice or less) being presented tothe nurse bank is reducing.
Advance block booking is reducing.
2.11 Staff rostering should ensure the mostefficient use of the workforce resource.
The aim is to optimise use of substantive staffand minimise use of supplementary staff. Staffrosters employ a variety of mechanisms toensure optimum cover for all shifts.
Parameters for rostering schedules are clearfor all staff.
2.12 Systems are in place to detect fraudulentinvoices, travel claims and timesheets fromsupplementary staff.
The potential for individuals to claimremuneration for services not provided exists –this risk must be minimised to protect publicresources.
Systems are in place to prevent and detectfraudulent claims for remuneration fromsupplementary staff.
Agreed audit procedures are carried out on aregular basis in conjunction with internal auditstaff.

3. Getting the best from the Bank Nurse
12
Recommended practice Rationale Measures of success
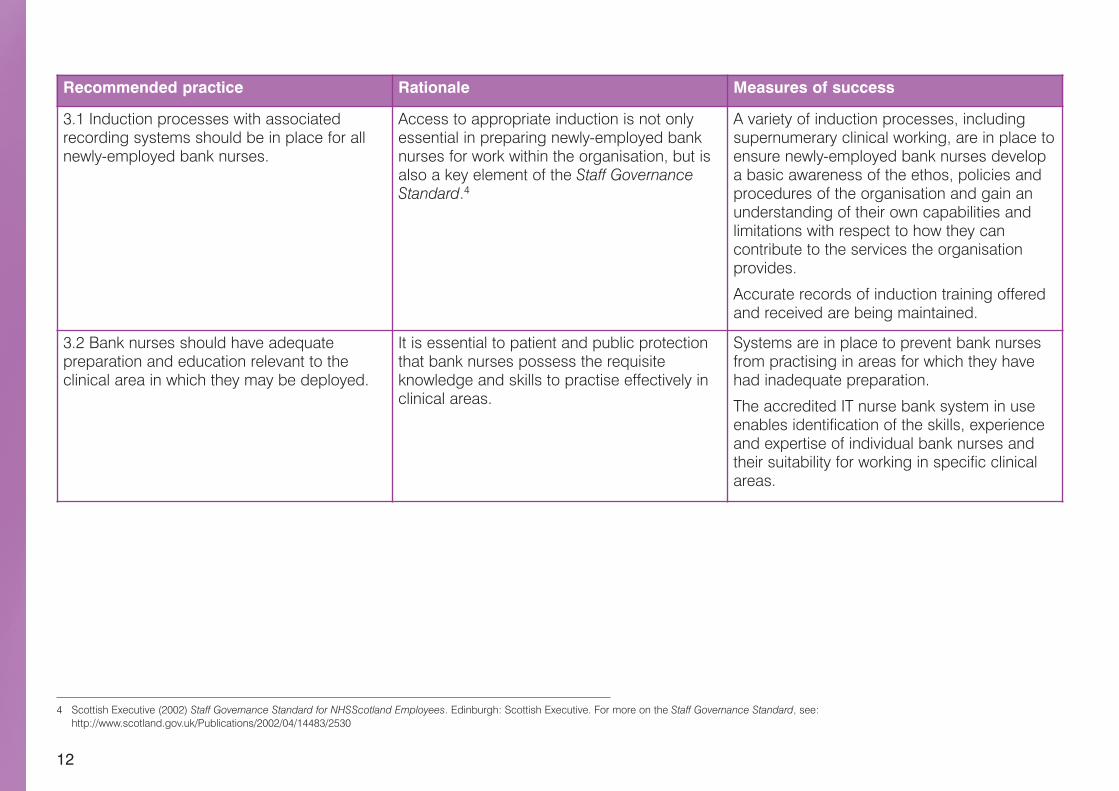
3.1 Induction processes with associatedrecording systems should be in place for allnewly-employed bank nurses.
Access to appropriate induction is not onlyessential in preparing newly-employed banknurses for work within the organisation, but isalso a key element of the Staff GovernanceStandard.4
A variety of induction processes, includingsupernumerary clinical working, are in place toensure newly-employed bank nurses developa basic awareness of the ethos, policies andprocedures of the organisation and gain anunderstanding of their own capabilities andlimitations with respect to how they cancontribute to the services the organisationprovides.
Accurate records of induction training offeredand received are being maintained.
3.2 Bank nurses should have adequatepreparation and education relevant to theclinical area in which they may be deployed.
It is essential to patient and public protectionthat bank nurses possess the requisiteknowledge and skills to practise effectively inclinical areas.
Systems are in place to prevent bank nursesfrom practising in areas for which they havehad inadequate preparation.
The accredited IT nurse bank system in useenables identification of the skills, experienceand expertise of individual bank nurses andtheir suitability for working in specific clinicalareas.
4 Scottish Executive (2002) Staff Governance Standard for NHSScotland Employees. Edinburgh: Scottish Executive. For more on the Staff Governance Standard, see:http://www.scotland.gov.uk/Publications/2002/04/14483/2530
13
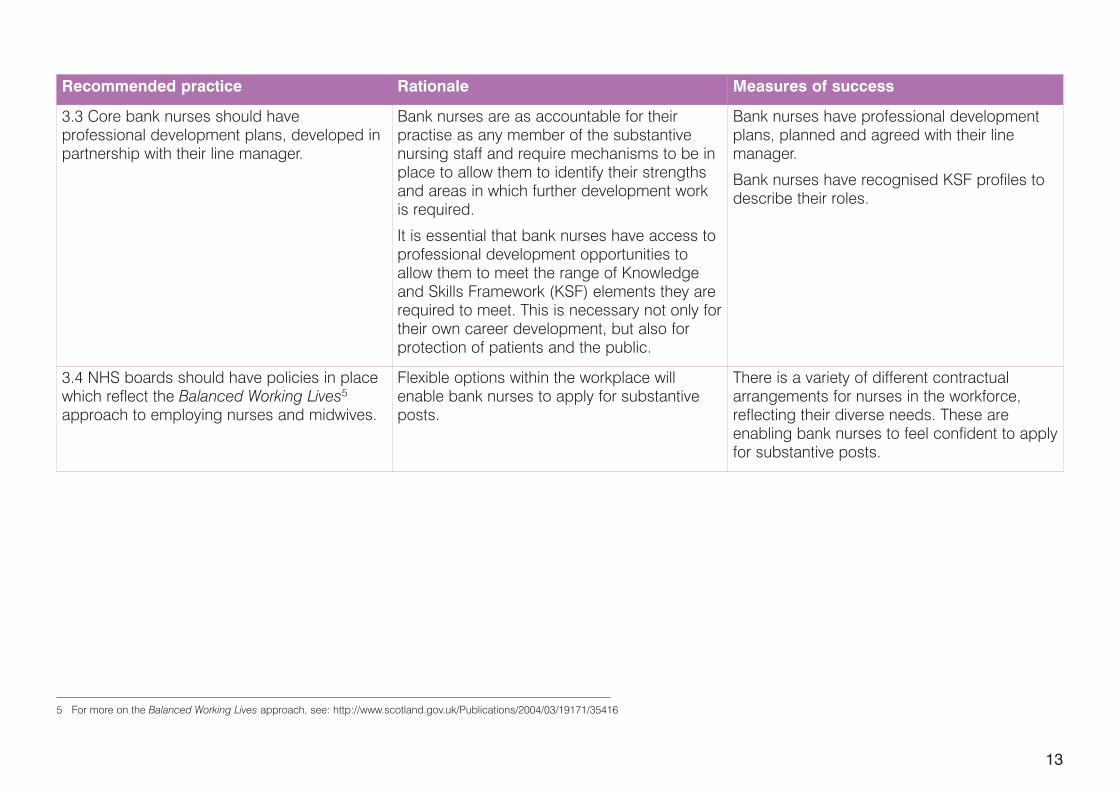
Recommended practice Rationale Measures of success
3.3 Core bank nurses should haveprofessional development plans, developed inpartnership with their line manager.
Bank nurses are as accountable for theirpractise as any member of the substantivenursing staff and require mechanisms to be inplace to allow them to identify their strengthsand areas in which further development workis required.
It is essential that bank nurses have access toprofessional development opportunities toallow them to meet the range of Knowledgeand Skills Framework (KSF) elements they arerequired to meet. This is necessary not only fortheir own career development, but also forprotection of patients and the public.
Bank nurses have professional developmentplans, planned and agreed with their linemanager.
Bank nurses have recognised KSF profiles todescribe their roles.
3.4 NHS boards should have policies in placewhich reflect the Balanced Working Lives5approach to employing nurses and midwives.
Flexible options within the workplace willenable bank nurses to apply for substantiveposts.
There is a variety of different contractualarrangements for nurses in the workforce,reflecting their diverse needs. These areenabling bank nurses to feel confident to applyfor substantive posts.
5 For more on the Balanced Working Lives approach, see: http://www.scotland.gov.uk/Publications/2004/03/19171/35416
14
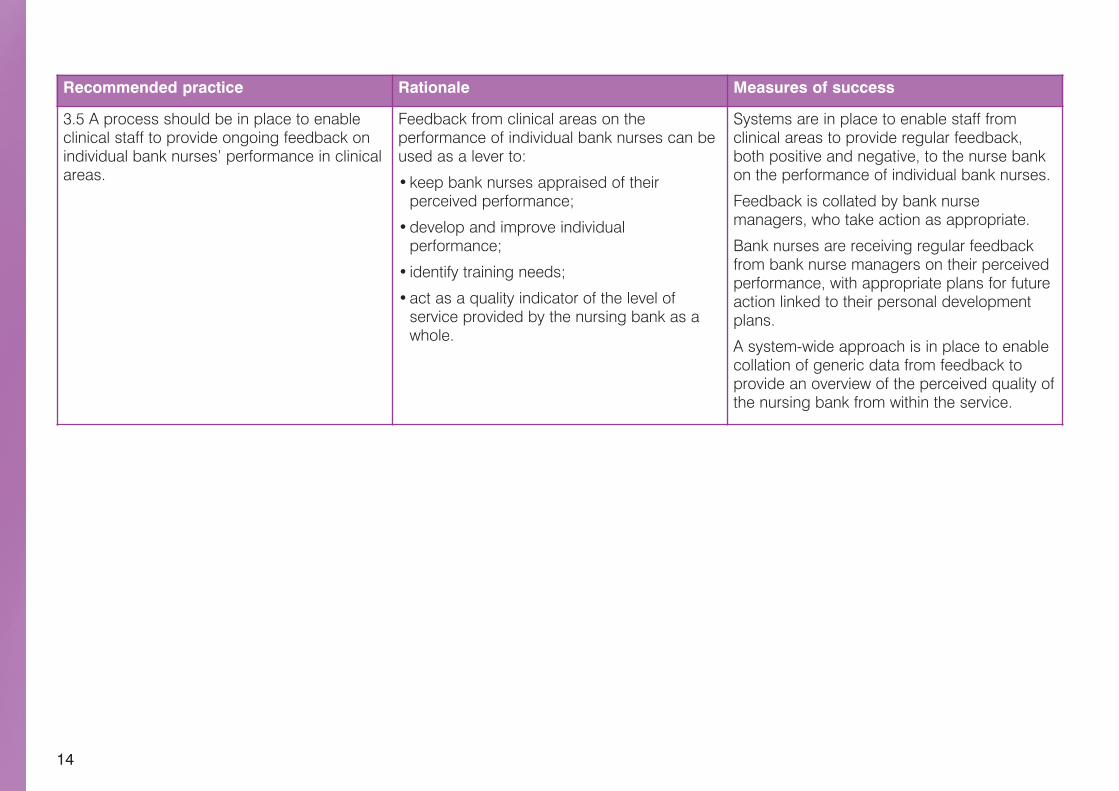
Recommended practice Rationale Measures of success
3.5 A process should be in place to enableclinical staff to provide ongoing feedback onindividual bank nurses’ performance in clinicalareas.
Feedback from clinical areas on theperformance of individual bank nurses can beused as a lever to:
•keep bank nurses appraised of theirperceived performance;
•develop and improve individualperformance;
• identify training needs;
•act as a quality indicator of the level ofservice provided by the nursing bank as awhole.
Systems are in place to enable staff fromclinical areas to provide regular feedback,both positive and negative, to the nurse bankon the performance of individual bank nurses.
Feedback is collated by bank nursemanagers, who take action as appropriate.
Bank nurses are receiving regular feedbackfrom bank nurse managers on their perceivedperformance, with appropriate plans for futureaction linked to their personal developmentplans.
A system-wide approach is in place to enablecollation of generic data from feedback toprovide an overview of the perceived quality ofthe nursing bank from within the service.

Further reading
16
Scottish Executive (2003) Good Practice Guidelines for EstablishingContact Centres. Edinburgh: Scottish Executive.
Scottish Executive (2005) Nationally Co-ordinated Nurse BankArrangements: Report and Action Plan. Edinburgh: Scottish Executive.
Scottish Executive (2006) Background Methodology and Results ofNationally Co-ordinated Nurse Bank Arrangements Project,NHSScotland. Edinburgh: Scottish Executive.
National Procurement: Use of National Contracts For Agency LabourPurchase and Review of Procurement in Scotland. HDL (2006) 39, July2006.
Implementation of Nursing and Midwifery Workload and WorkforcePlanning Tools and Methodologies. CEL (6) 2007, August 2007.
Audit Scotland (2007) Planning Ward Nursing – Legacy or Design?A follow-up report. Edinburgh: Audit Scotland.
w w w . s c o t l a n d . g o v . u k
© Crown copyright 2007
RR Donnelley B51843 12/07
Further copies are available fromBlackwell's Bookshop53 South BridgeEdinburghEH1 1YS
Telephone orders and enquiries0131 622 8283 or 0131 622 8258
Fax orders0131 557 8149
Email [email protected]