Embed Size (px)
Citation preview
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 1 of 10
This document applies to the following Participating Organizations:
EHP Johns Hopkins Advantage MD Priority Partners US Family Health Plan
Keywords: Medical Food, Nutrition
Table of Contents Page Number
I. ACTION 1II. POLICY DISCLAIMER 1III. POLICY 1IV. POLICY CRITERIA 2V. DEFINITIONS 4VI. BACKGROUND 5VII. CODING DISCLAIMER 6VIII. CODING INFORMATION 6IX. REFERENCE STATEMENT 8X. REFERENCES 8XI. APPROVALS 10
I. ACTION New Policy
X Revising Policy Number CMS14.04
Superseding Policy Number
Archiving Policy Number
Retiring Policy Number
II. POLICY DISCLAIMERJohns Hopkins HealthCare LLC (JHHC) provides a full spectrum of health care products and services for Employer HealthPrograms, Priority Partners, Advantage MD and US Family Health Plan. Each line of business possesses its own uniquecontract and guidelines which, for benefit and payment purposes, should be consulted first to know what benefits are availablefor coverage.
Specific contract benefits, guidelines or policies supersede the information outlined in this policy.
III. POLICYCross Reference: CMS14.02 Nutritional Counseling
For Advantage MD, see:
• Medicare Coverage Database National Coverage Determination (NCD) for Medical Nutrition Therapy (180.1)• Medicare Coverage Database Local Coverage Determination (LCD): Enteral Nutrition (L33783)• Medicare Coverage Database Local Coverage Article: Enteral Nutrition - Policy Article (A52493)For Employer Health Programs (EHP), see: Plan specific Summary Plan Descriptions for available coverage
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 2 of 10
For Priority Partners see:
• Code of Maryland Regulations (COMAR) 10.09.67.04 Pharmacy Services• Code of Maryland Regulations (COMAR) 10.09.67.20 EPSDT Services• Medical Assistance Program Transmittal EPSDT No. 31, Pharmacy no. 189, February 3, 2009:
MMCP.Health.Maryland.gov/PT29-09.pdf • Maryland Department of Health, Women, Infants and Children Program (WIC): https://phpa.health.maryland.gov/• Maryland Department of Health, Division for Clinical Genetic Services, The Metabolic Nutrition Follow-up
Program: phpa.health.maryland.gov/genetics/
For US Family Health Plan see:
• TRICARE Policy Manual 6010.60-M April 1, 2015, Other Services: Chapter 8, Section 7.2. Medically Necessary Food -For Dates of Service On Or After December 23, 2017.
• Enteral and Oral Nutrition Products -Enteral Foods List https://www.health.mil
IV. POLICY CRITERIAA. General Considerations: When benefits are provided under the member’s contract, JHHC considers nutritional treatment
medically necessary when ALL of the following are met:1. The nutritional product must be prescribed, ordered, or recommended (as applicable) by a physician or other health
care professional qualified to provide medical treatment for the disease or condition for which the therapy is beingprescribed, ordered, or recommended.
2. The condition for which the nutritional product is being prescribed, ordered, or recommended is expected to persistfor a minimum of three months.
3. Adequate nutrition cannot be achieved by adjustment of regular diet.4. There is clear documentation of medical diagnosis and treatment plan indicating medical necessity of the nutritional
product.5. There is ongoing medical supervision by a physician or other qualified health care professional, who has determined
the need for the medical food. The supervision includes instruction on use of the medical food as part of the dietarymanagement of the given disease or condition.
6. Treatment is for ANY of the conditions listed in Section B or C.
B. When benefits are provided under the member’s contract, JHHC considers nutritional treatment with medical foods/medical formulas to be medically necessary when ALL the requirements in Section I are met and for ANY of thefollowing:1. Inborn errors of metabolism (IEM), including the following categories:
a. Disorders of amino acid metabolism, including but not limited to:i. maple syrup urine disease,ii. homocystinuria,iii. phenylketonuria,iv. citrullinemia,v. argininosuccinic aciduria,vi. tyrosinemia
b. Organic acidemias, including but not limited to:i. methylmalonic acidemia,ii. propionic acidemia,
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 3 of 10
iii. isovaleric acidemia, iv. multiple carboxylase deficiency,v. glutaric acidemia type 1vi. ß-Ketothiolase deficiency
c. Urea cycle defects, including but not limited to:i. argininosuccinate synthetase deficiency (also known as classic citrullinemia),ii. ornithine transcarbamylase deficiency,iii. carbamyl phosphate synthetase deficiency,iv. arginosuccinic lyase deficiency (also know as arginosuccinic aciduria)v. N-acetyl glutamate synthetase deficiencyvi. arginase deficiency (also know as argininemia)
d. Fatty acid oxidation disorders requiring dietary treatment, including:i. very long chain acyl-coA dehydrogenase deficiency (VLCADD),ii. long chain 3-hydroxyacyl-coA dehydrogenase deficiency (LCHADD),iii. trifunctional protein (TFP) deficiency,iv. HMG-coA lyase deficiencyv. medium-chain acyl-coA dehydrogenase deficiencyvi. carnitine uptake defect
e. Glycogen storage diseases
C. When benefits are provided under the member’s contract, JHHC considers nutritional treatment with amino acid-basedformulas to be medically necessary when ALL the requirements in Section A are met and for ANY of the following:1. Immunoglobulin E and non-immunoglobulin E mediated allergies to multiple food proteins2. Food protein induced enterocolitis syndrome (FPIES)3. Eosinophilic gastrointestinal disorders (EGID), as evidenced by the results of a biopsy4. Medical disorders resulting in malabsorption of nutrients caused by disorders affecting the absorptive surface,
functional length, and motility of the gastrointestinal tract which may include, but is not limited to cystic fibrosisand short gut syndrome.
5. Failure to initiate nutritional therapy will result in malnutrition, physical or mental disability, or death.
D. When benefits are provided under the member’s contract, nutrition products for oral or enteral tube feedingconsumption that may be approved under this policy when ALL the requirements in Section A are met and either therequirements of Section B or C are met (as applicable) include:1. For conditions listed in Section B above:
a. Formulas/products used as a main source of nutrition containing protein, without the offending amino acid, anda range of other nutrients - specially produced for the dietary treatment of the specific disease/condition (e.g.Propimex-1)
b. Low protein modified food products (excludes natural foods that are by nature low in protein) (e.g. Loprofinrice)
c. Modular food/Supplements:i. Amino acid mixtures (e.g. Nutricia Complete Amino Acid Mix)ii. Single amino acids to be added to the nutritional solutioniii. Medically necessary vitamins and minerals, or other compounds used to replace conditionally essential
nutrients or enhance enzyme activity2. For conditions listed in Section C above:
a. Amino acid-based elemental formulas (e.g. PurAmino, Elecare, Neocate)
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 4 of 10
E. Unless specific benefits are provided under the members contract, JHHC considers the following to be NOTMEDICALLY NECESSARY/NOT COVERED, (not an all-inclusive list):1. Food products consumed as part of a diet or treatment plan designed to reduce the risk of a disease or medical
condition or as weight-loss products, even if recommended by a physician or other health care professional2. Nutritional supplements administered for the sole purpose of boosting protein or caloric intake in the absence of a
medical condition for which the accepted treatment consists of or includes administration of nutritional supplements.3. Vitamin or mineral preparations, except as provided in section III.C (also refer to Pharmacy benefit).4. Nutritional products as follows:
a. Regular grocery itemsb. baby foodc. banked breast milk (unless specifically covered by benefit plan)d. food thickeners, fiber additivese. gluten-free food products for the management of celiac disease or non-celiac gluten sensitivityf. lactose-free productsg. food marketed for the management of diabetesh. products marketed to aid weight lossi. products used to replace fluids and electrolytes
5. Formulas, foods, or additives designed and marketed for the treatment of food intolerances (e.g. formulas forfussiness or gas)
6. In-line cartridge containing digestive enzyme(s) for enteral feeding (i.e. Relizorb), unless specifically covered bybenefit plan (Refer to Tricare Enteral Food List in Policy section above).
7. Nutrition product(s) covered for a member through a state agency (e.g. Women, Infants and Children (WIC)Nutrition Program)
8. Products determined to be investigational or experimental in the treatment of a specific disease or condition.
V. DEFINITIONSAmino Acid-Based Elemental Formula: A class of nutritional formulas designed for use in the treatment of patients withconditions of the bowel which cause maldigestion or malabsorption. These formulas contain 100% free amino acids as theonly protein source and are highly osmotic. They can be administered orally or enterally (through nasogastric, gastrostomy orjejunostomy tubes). The nutritional requirements for patients requiring these formulas are established by medical evaluationand medical supervision is required for their usage.
Eosinophilic Gastrointestinal Disorders (EGID): A group of immune-mediated chronic inflammatory disorders characterizedby pathologic eosinophilic (WBC) infiltration of the esophagus, stomach, small intestine, or colon leading to organ dysfunctionand clinical symptoms. Symptoms include abdominal pain, nausea, vomiting, early satiety, diarrhea, and weight loss(Gonsalves, 2019).
Food Protein–Induced Enterocolitis (FPIES): A non–IgE-mediated food allergy typically presenting in infancy, with repetitiveprotracted vomiting beginning approximately 1 to 4 hours after food ingestion with absence of classic IgE-mediated allergicskin or respiratory symptoms. Associated symptoms include: lethargy, pallor, diarrhea, hypotension, hypothermia, increasedneutrophil count (Nowak-Wegrzyn, 2017).
Inborn Errors of Metabolism (IEM): These include inherited biochemical disorders in which a specific enzyme defect interfereswith the normal metabolism of protein, fat, or carbohydrate. The diminished or absent enzyme activity in these disorders, causecertain compounds to accumulate in the body at toxic levels and the levels of others that the body normally makes may becomedeficient. Left untreated, these metabolic disturbances can result in intellectual disability, severe cognitive impairment or death(Camp, 2012).
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 5 of 10
Low Protein Modified Food: A food product that is specially formulated to have less than 1 gram of protein per serving andis intended to be used under the direction of a physician for the dietary treatment of an inherited metabolic disease, excludingnatural foods that are naturally low in protein (Maryland Code, Insurance § 15-807).
Medical Food: Food intended for the dietary treatment of a disease or condition for which nutritional requirements areestablished by medical evaluation and formulated to be consumed or administered enterally under the direction of a physician(Maryland Code, Insurance § 15-807). A medical food must be intended for a patient who has a limited or impaired capacityto ingest, digest, absorb, or metabolize ordinary foodstuffs or certain nutrients, or who has other special medically determinednutrient requirements, the dietary management of which cannot be achieved by the modification of the normal diet alone (21CFR 101.9(j)(8)(ii)).
Medical Nutrition Therapy: Nutritional diagnostic, therapy, and counseling services for the purpose of disease managementwhich are furnished by a registered dietitian or nutrition professional. MNT is a specific application of the Nutrition CareProcess in clinical settings that is focused on the management of diseases. MNT involves in-depth individualized nutritionassessment and a duration and frequency of care using the Nutrition Care Process to manage disease (Academy of Nutritionand Dietetics, 2019). It includes recommendations for foods or nutrients to treat conditions and may involve simple changes ina person’s diet, or intravenous or tube feeding. (Also called nutrition therapy) (NIH 2019).
VI. BACKGROUNDMedical Nutrition Therapy (MNT) is a practice which consists of administering personalized diet plans, nutritional therapyand counseling services to patients for the treatment and management of diseases and other medical conditions. MNT is atherapeutic approach often used for patients with diabetes, hypertension, and renal disease.
Dietary management of diseases or conditions also includes the treatment of severe allergies, disorders of the gastrointestinaltract and inborn errors of metabolism (IEM) for which the provision of medical foods may be required to allow for growthand development or to prevent death. Many inborn errors of metabolism for which nutritional treatments serve as the primarymedical treatment are identified through newborn screening programs (NSPs). Individual states determine what disorders areincluded in their NBS program however; most states include the disorders included on the Recommended Uniform ScreeningPanel supported by the Advisory Committee on Heritable Disorders in Newborns and Children (HRSA.gov, 2019).
Although screening programs may vary, major categories tested include fatty acid oxidation disorders, amino acids disordersand organic acidurias (Camp, 2012). Fatty acid oxidation disorders (FAODs) are inborn errors of metabolism that resultin failure of mitochondrial beta-oxidation or the carnitine-based transport of fatty acids into mitochondria (Merritt, 2017).The recommended diet for FAODs is fat restricted with carbohydrate supplementation. Treatment of long-chain FAODs aresupplemented with medium-chain triglyceride (MCT) oil to provide a substrate for beta-oxidation. Carnitine supplementationis given when secondary carnitine deficiency is identified. Essential to treatment of FAODs is avoidance of prolonged fastingand maintenance of a constant energy supply during times of catabolism (Merritt). Inborn errors of metabolism involvingamino acid metabolism include phenylketonuria (PKU), the first newborn screening disorder. It is the most common IEMrequiring nutritional treatment and is caused by insufficient or absent phenylalanine hydroxylase, the enzyme that convertsthe amino acid phenylalanine to tyrosine (Camp). Medical nutrition therapy for inborn errors of metabolism involving aminoacid disorders include two different forms of medical foods - one containing protein without the amino acid(s) specific to theIEM and the other consisting of foods that have been modified to be low in protein (Camp). Organic acidurias, also referredto as organic acidemias, are a class of inborn errors of metabolism characterized by accumulation of abnormal and often toxicorganic acid metabolites with increased excretion of organic acids in urine. They result primarily from deficiencies of specificenzymes in the breakdown pathways of amino acids (Bodamer, 2019). Successful treatment of organic acidurias involvessynthetic amino acid-based formulas which should provide about 50% of daily protein needs. Simultaneously, the dietaryprecursor amino acid has to be restricted and fasting must be avoided (Vaidyanathan, 2011).
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 6 of 10
Nutritional products classified as medical foods used to treat inborn errors of metabolism include three main categories.Products with a full complement of nutrients excluding the offending nutrient which come in powders to be reconstituted,ready to drink products, and bars. This category includes specialty infant formulas. Secondly, are modular products whichinclude amino acid mixtures, ready to drink products, low volume, low calorie foods, and tablets. Lastly, foods modified to below in protein include specialty baked goods, pasta, rice, meat and cheese substitutes, and snack foods (Camp, 2016). Medicalfoods are distinct from the broader category of foods for special dietary use, as medical foods must be intended to meetdistinctive nutritional requirements of a disease or condition, be intended for the specific dietary management of a diseaseor condition, and require medical supervision. Medical foods do not include all foods recommended by a physician as partof an overall diet to manage the symptoms or reduce disease risk, and not all foods administered to patients with a disease,including diseases that require dietary management, like diabetes, are medical foods. Instead, medical foods are foods thatare specially formulated and processed for a patient who requires use of the product as a major component of a disease orcondition’s specific dietary management (HHS, 2016).
VII. CODING DISCLAIMERCPT Copyright 2018 American Medical Association. All rights reserved. CPT is a registered trademark of the AmericanMedical Association.
Note: The following CPT/HCPCS codes are included below for informational purposes and may not be all inclusive. Inclusionor exclusion of a CPT/HCPCS code(s) below does not signify or imply that the service described by the code is a covered ornon-covered health service. Benefit coverage for health services is determined by the member’s specific benefit plan documentand applicable laws that may require coverage for a specific service. The inclusion of a code does not imply any right toreimbursement or guarantee of payment. Other policies and coverage determination guidelines may apply.
Note: All inpatient admissions require preauthorization.
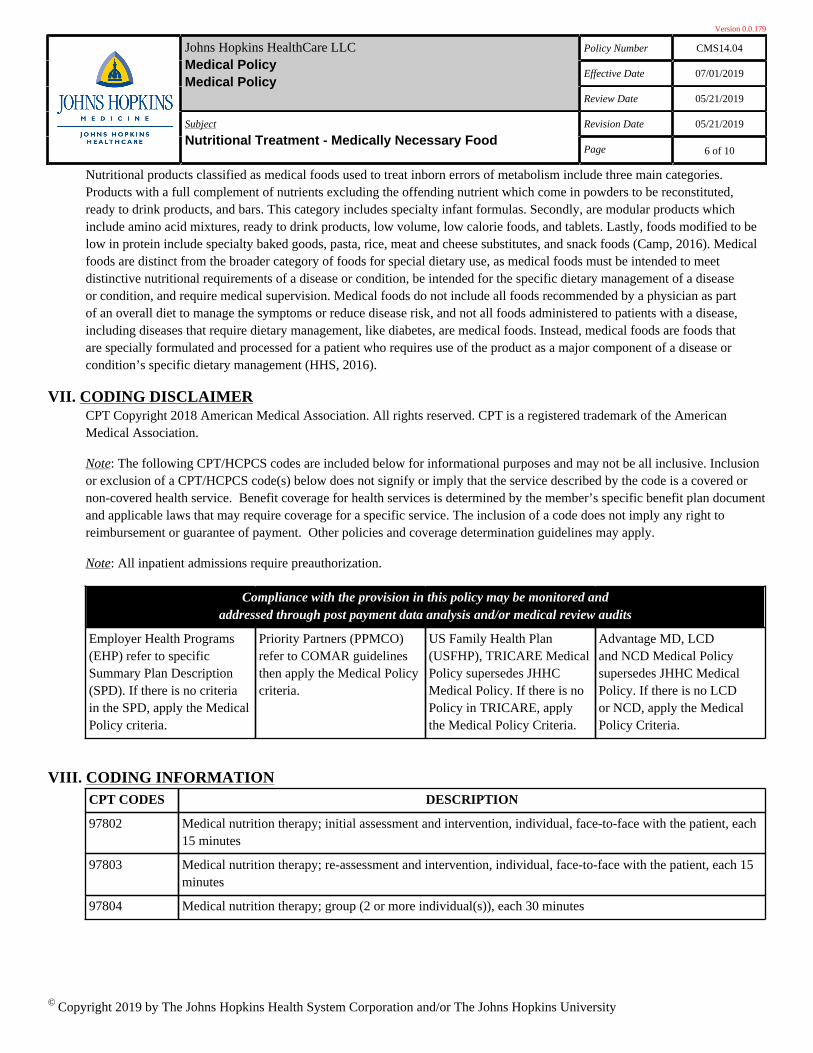
Compliance with the provision in this policy may be monitored andaddressed through post payment data analysis and/or medical review audits
Employer Health Programs(EHP) refer to specificSummary Plan Description(SPD). If there is no criteriain the SPD, apply the MedicalPolicy criteria.
Priority Partners (PPMCO)refer to COMAR guidelinesthen apply the Medical Policycriteria.
US Family Health Plan(USFHP), TRICARE MedicalPolicy supersedes JHHCMedical Policy. If there is noPolicy in TRICARE, applythe Medical Policy Criteria.
Advantage MD, LCDand NCD Medical Policysupersedes JHHC MedicalPolicy. If there is no LCDor NCD, apply the MedicalPolicy Criteria.
VIII. CODING INFORMATIONCPT CODES DESCRIPTION
97802 Medical nutrition therapy; initial assessment and intervention, individual, face-to-face with the patient, each15 minutes
97803 Medical nutrition therapy; re-assessment and intervention, individual, face-to-face with the patient, each 15minutes
97804 Medical nutrition therapy; group (2 or more individual(s)), each 30 minutes
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 7 of 10
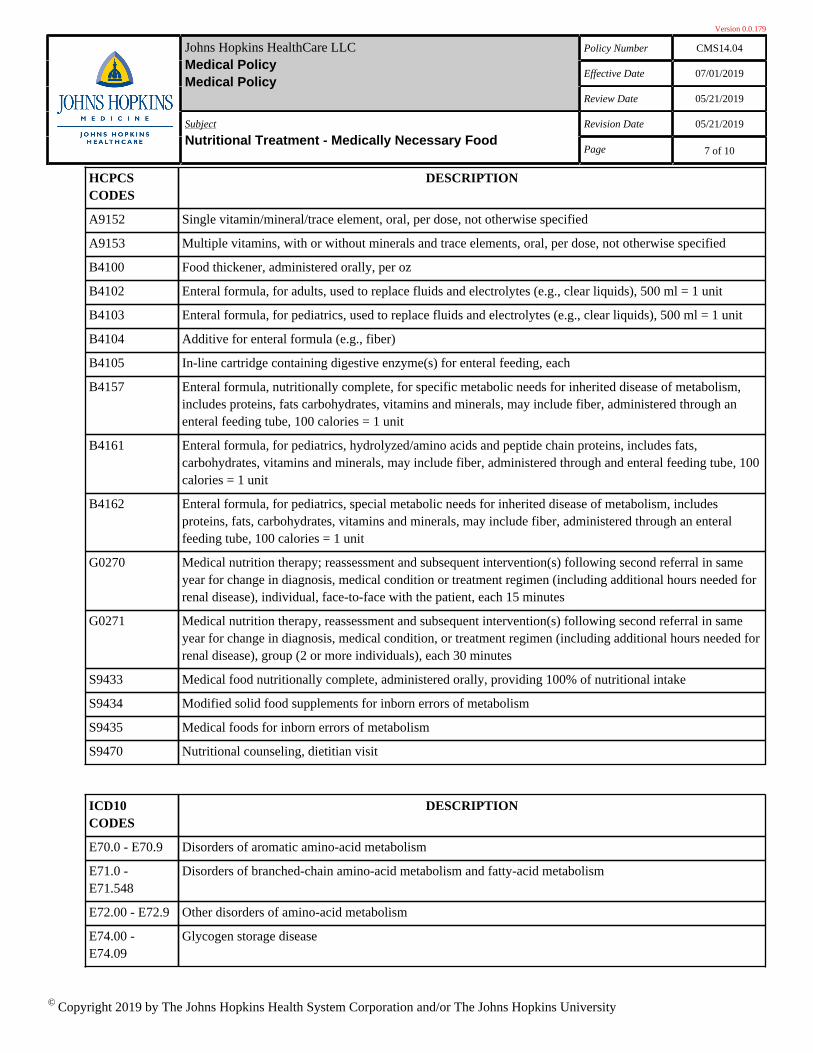
HCPCSCODES
DESCRIPTION
A9152 Single vitamin/mineral/trace element, oral, per dose, not otherwise specified
A9153 Multiple vitamins, with or without minerals and trace elements, oral, per dose, not otherwise specified
B4100 Food thickener, administered orally, per oz
B4102 Enteral formula, for adults, used to replace fluids and electrolytes (e.g., clear liquids), 500 ml = 1 unit
B4103 Enteral formula, for pediatrics, used to replace fluids and electrolytes (e.g., clear liquids), 500 ml = 1 unit
B4104 Additive for enteral formula (e.g., fiber)
B4105 In-line cartridge containing digestive enzyme(s) for enteral feeding, each
B4157 Enteral formula, nutritionally complete, for specific metabolic needs for inherited disease of metabolism,includes proteins, fats carbohydrates, vitamins and minerals, may include fiber, administered through anenteral feeding tube, 100 calories = 1 unit
B4161 Enteral formula, for pediatrics, hydrolyzed/amino acids and peptide chain proteins, includes fats,carbohydrates, vitamins and minerals, may include fiber, administered through and enteral feeding tube, 100calories = 1 unit
B4162 Enteral formula, for pediatrics, special metabolic needs for inherited disease of metabolism, includesproteins, fats, carbohydrates, vitamins and minerals, may include fiber, administered through an enteralfeeding tube, 100 calories = 1 unit
G0270 Medical nutrition therapy; reassessment and subsequent intervention(s) following second referral in sameyear for change in diagnosis, medical condition or treatment regimen (including additional hours needed forrenal disease), individual, face-to-face with the patient, each 15 minutes
G0271 Medical nutrition therapy, reassessment and subsequent intervention(s) following second referral in sameyear for change in diagnosis, medical condition, or treatment regimen (including additional hours needed forrenal disease), group (2 or more individuals), each 30 minutes
S9433 Medical food nutritionally complete, administered orally, providing 100% of nutritional intake
S9434 Modified solid food supplements for inborn errors of metabolism
S9435 Medical foods for inborn errors of metabolism
S9470 Nutritional counseling, dietitian visit
ICD10CODES
DESCRIPTION
E70.0 - E70.9 Disorders of aromatic amino-acid metabolism
E71.0 -E71.548
Disorders of branched-chain amino-acid metabolism and fatty-acid metabolism
E72.00 - E72.9 Other disorders of amino-acid metabolism
E74.00 -E74.09
Glycogen storage disease
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 8 of 10
IX. REFERENCE STATEMENTAnalyses of the scientific and clinical references cited below were conducted and utilized by the Johns Hopkins HealthCareLLC (JHHC) Medical Policy Team during the development and implementation of this medical policy. The Medical PolicyTeam will continue to monitor and review any newly published clinical evidence and revise the policy and adjust the referencesbelow accordingly if deemed necessary.
X. REFERENCESAcademy of Nutrition and Dietetics. (2019). RDNs and Medical Nutrition Therapy Services. Retrieved: http://www.eatright.org/
Academy of Nutrition and Dietetics. (2012). Statement to members in regards to Aetna’s denials. Retrieved: http://www.eatrightwashington.org/
Academy of Nutrition and Dietetics. (2019). MNT vs. Nutrition Education. Retrieved: https://www.eatrightpro.org/
Aills, L., Blankenship, J., Buffington, C., et al. (2008). ASMBS Guidelines: Allied Health Nutritional Guidelines for theSurgical Weight Loss Patient. Allied Health Services Sciences Section Ad Hoc Nutrition Committee. Surgery for Obesity andRelated Diseases, Vol. 4, p. 73-108.
Bodamer, O. (2018). Overview of phenylketonuria. UpToDate. Retrieved: https://www.uptodate.com/
Bodamer, O. (2018). Overview of maple syrup urine disease. UpToDate. Retrieved: https://www.uptodate.com/
Bodamer, O. (2019). Organic acidemias: An overview and specific defects UpToDate. Retrieved: www.uptodate.com/
Camp, K. (2016). Medical Foods for Inborn Errors of Metabolism: Issues in Patient Access. National Institutes of Health(NIH), Advisory Committee on Heritable Disorders in Newborns and Children. Retrieved: https://www.hrsa.gov/
Camp, K., Lloyd-Puryear, M., Huntington, K. (2012). Nutritional treatment for inborn errors of metabolism: Indications,regulations, and availability of medical foods and dietary supplements using phenylketonuria as an example. MolecularGenetics and Metabolism, Vol. 107, p. 3-9. Retrieved: https://www.ncbi.nlm.nih.gov/pubmed/
Centers for Medicare & Medicaid Services. (2017). Medicare Coverage: Nutrition Therapy Services (Medical). Retrieved: https://www.medicare.gov
Cigna. (2019). Medical Coverage Policy: Nutritional Support. Medical Coverage Policy Number: 0136. Retrieved: https://cignaforhcp.cigna.com/
Christensen, N.K., Steiner, J., Whalen, J., et al. (2000). Contribution of medical nutrition therapy and diabetes self-managementeducation to diabetes control as assessed by hemogloblin A1c, Diabetes Spectrum, Vol. 13, p.72-75.
Craigen, W., Darras, B. (2017). Overview of inherited disorders of glucose and glycogen metabolism. UpToDate. Retrieved: https://www.uptodate.com
Daly, A., Michael, P., Johnson, E., et al. (2009). Diabetes White Paper: Defining the Delivery of Nutrition Services inMedicare Medical Nutrition Therapy vs Medicare Diabetes Self-Management Training Programs. Journal of the Academy ofNutrition and Dietetics, Vol. 109 (3), p.528-539.
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 9 of 10
Gonsalves, N. (2019). Eosinophilic Gastrointestinal Disorders. Clinical Reviews in Allergy & Immunology, p.1-14.Retrieved: https://doi.org/
Grompe, M. (2018). Disorders of tyrosine metabolism. UpToDate. Retrieved: https://www.uptodate.com
Health Resources & Services Administration. (2019). Advisory Committee on Heritable Disorders in Newborns and Children.Newborn Screening: Toward a Uniform Screening Panel and System. Retrieved: https://www.hrsa.gov/
Kumar, T., Suraj Sharma, G., Rajendrakumar Singh, L. (2016). Homocystinuria: Therapeutic Approach. Clinica Chimica Acta,Vol. 458, p.55-62.
Lee, Brendan. (2018). Urea Cycle Disorders: Management. UpToDate. Retrieved: https://www.uptodate.com
Maryland Department of Health. (2019). Division of Newborn & Childhood Screening. Retrieved: https://health.maryland.gov/
Maryland General Assembly. (2009). Department of Legislative Services. House Bill 578. Health Insurance- Coverage forAmino Acid-Based Elemental Formula. Retrieved: http://mlis.state.md.us
Mason, J., & Milovic, V. (2018). Overview of the treatment of malabsorption. UpToDate. Retrieved: https://www.uptodate.com
Mechanick, J., Kushner, R., Sugerman, H., et al. (2008). American Association of Clinical Endocrinologists, The ObesitySociety, and American Society for Metabolic & Bariatric Surgery Medical Guidelines for Clinical Practice for thePerioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient. Surgery for Obesity andRelated Diseases, Vol. 4, p.109-184.
Mechanick, J., Youdim, A., Jones, D., et al. (2013). Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic,and Nonsurgical Support of the Bariatric Surgery Patient-2013 Update: Co-sponsored by American Association of ClinicalEndocrinologists, The Obesity Society, and the American Society for Metabolic & Bariatric Surgery. Surgery for Obesity andRelated Diseases, Vol. 9, p.159-191
Merritt, J. L., Vockley, J. (2019). Overview of fatty acid oxidation disorders. UpToDate. Retrieved: https://www.uptodate.com/
Morris, S., Wylie-Rosett, J. (2010). Medical Nutrition Therapy: A Key to Diabetes Management and Prevention. ClinicalDiabetes, Vol. 28(1), p.12-18.
National Institutes of Health (NIH). (2019). National Cancer Institute Dictionary of Terms. Definition of Medical NutritionTherapy. Retrieved: https://www.cancer.gov
Nowak-Wegrzyn, A. (2019). Food protein-induced enterocolitis syndrome (FPIES). UpToDate. Retrieved: https://www.uptodate.com
Nowak-Wegrzyn, A, Chehade, M., Groetch, M. E. et al. (2017). International consensus guidelines for the diagnosis andmanagement of food protein–induced enterocolitis syndrome: Executive summary—Workgroup Report of the AdverseReactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. Journal of Allergy and ClinicalImmunology. Vol. 139 (4), p. 1111-1126.
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University
Version 0.0.179
Policy Number CMS14.04
Effective Date 07/01/2019
Johns Hopkins HealthCare LLCMedical PolicyMedical Policy
Review Date 05/21/2019
Revision Date 05/21/2019Subject
Nutritional Treatment - Medically Necessary FoodPage 10 of 10
Pastors, J.G., Warshaw, H., Daly, A., et al. (2002). The evidence of medical nutrition therapy in diabetes management.Diabetes Care, Vol. 25, p.608-613.
Sun, A. (2018). Glucose-6-phosphatase deficiency (glycogen storage disease I, von Gierke disease). UpToDate. Retrieved:https://www.uptodate.com
TRICARE. Policy Manual 6010.60-M, April1, 2015. Chapter 8, Section 7.2. Medically Necessary Food - For Dates of ServiceOn or After December 23, 2017. Retrieved: https://manuals.health.mil
United Healthcare. (2018). Oral and Enteral Nutrition. Medical Policy Guideline Number: CS136.G. Retrieved: https://www.unitedhealthcareonline.com
US Department of Health and Human Services (HHS). (2016). Food and Drug Administration, Center for Food Safety andApplied Nutrition. Frequently Asked Questions About Medical Foods; Second Edition - Guidance for Industry. Retrieved:https://www.fda.gov
Vaidyanathan, K., Narayanan, M.P., Vasudevan, D. M. (2011). Organic Acidurias: An Updated Review. Indian Journal ofClinical Biochemistry. Vol 26 (4), p. 319-325. Retrieved: https://www.ncbi.nlm.nih.gov
XI. APPROVALSHistorical Approval Dates: 03/03/2017, 07/01/2019
© Copyright 2019 by The Johns Hopkins Health System Corporation and/or The Johns Hopkins University





























