Embed Size (px)
Citation preview

OBESITY
Liz Brown
September 2005


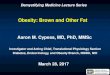
Examples of the prevalence of obesity in adults throughout the world

Defining Overweight & Obesity
• Body Mass Index (BMI)– (Weight (Kg)/(Height (m)2)
• Distribution of Body Fat– Measurement of waist circumference

WHO standard classification of obesity (WHO 1997)
BMI Risk of co-morbidities
Normal BMI18.5-24.9
average
Overweight:
Pre-obese25.0-29.9
increased
Obesity class I30.0-34.9
moderate
Obesity class II
35.0-39.9
severe
Obesity class III
40 very severe

Sex-specific waist circumferences for ‘increased risk’ and ‘substantially increased risk’ of metabolic complications associated with obesity in Caucasians
Risk of obesity-associated metabolic complications
Increased Substantially increased
Men 94 cm 102 cm
Women
80 cm 88 cm


Why is Obesity On the Increase
• Last 20 years calorie intake has not significantly changed– Decreased carbohydrate intake– Increased fat increase– Less home cooking more convenient food– More sedentary lifestyle


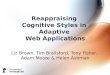
Relationship between BMI and cardiovascular risk factors


Cost
• 1998 NHS spent £50million/yr for treating obesity
• Indirect cost of treating co-morbidities £1.7 - £1.9 B
• 3.5-4% of all NHS expenditure

Weight Loss Treatments
Combination of:
controlled energy diet
increased physical activity
behaviour therapy
provide the most successful treatment for weight loss and maintenance of weight loss

Counselling & Support• Educate patients regarding hazards of
obesity and benefits of modest weight loss (5-10% of body weight)
• Help set realistic goals• Encourage to give up short term ‘diet’
mentality and stress need for long term lifestyle change
• Recommend increased physical activity and incorporating exercise into daily routine
• Acknowledge the difficulties of loosing weight

Drug Treatments• Adjuvant management of obesity • BMI>30 with no associated co-morbidity• BMI of 27 in presence of co-morbidity (e.g.
NIDDM)• NICE / SIGN & British Heart Foundation
provided guidance of use of drug treatments• All pt on drug treatment require regular review
and at 3/12 treatment stopped if 5% of wt loss not achieved
• RCT suggest that approx 60% of treated patients achieve & maintain a 5% wt loss after 12 months of treatment


ORLISTAT• Inhibits pancreatic & gastric lipase • Reduces approx. 30% of fat absorption• Very low quantities absorbed but SE on GI tract• Side effects
– Steatorrhoea
– Increased urgency & frequency of defecation
– Anal leakage
– Oily spotting
– Consider vitamin supplementation (esp. Vit D) if concerned about deficiency of fat sol vitamins

ORLISTAT
• Criteria– Age 18-75 yrs– Contra-indicated in pregnancy & breast feeding– Must have attempted long-term control of wt using
lifestyle measures without success– Need to loose 2.5Kg in 1 month prior to treatment– Review after 3/12- need to loose 5% of starting wt. to
continue treatment– Review after 6/12 need to loose 10% of starting wt.
continue treatment– Licensed for 2 years

ORLISTATCost– 49 pence/capsule– Dosing 3 capsules a day costs £537/yr– 2000 England & Wales spent £6 million on
prescriptions
Effectiveness– 14 trials have shown clinically effective in reducing wt
loss over 1 yr BUT only small reduction in wt decline compared to placebo.
– Significant but small reduction in total cholesterol and diastolic & systolic BP
– Wt loss on cessation of treatment regained over time, average 3 years
– Short term wt loss may not have as much effect on co-morbidities in longer term as been assumed


SIBUTRAMINE
• Re-uptake inhibitor or nor adrenaline and serotonin
• Promotes a sense of satiety
• Licensed for 1 year in 18-65 yr olds
• Costs between £456-£510/year
• Contra-indicated in breast feeding, pregnancy & BP>145/90

SIBUTRAMINE• Dosage
– Starting dose 10mg/day– Review at 4/52. If 2Kg wt loss can continue Rx and
increase dose to 15mg/day – Review at 3/12, require 5% wt loss from initial wt to
continue treatment
• Monitoring– Careful monitoring of BP– STOP if BP>145/90– STOP if BP rises more than 10mmHg (diastolic &
systolic)– STOP if resting HR increases by 10bpm

SIBUTRAMINE
• Effectiveness– 16 trials– RCT indicate dose related wt loss with an optimal dose
of 10-15mg/day.– Mean wt loss greater than placebo– More likely to maintain wt loss than pt randomised to
diet & exercise– No statistical difference between men & women or
ethnic groups– Risk factors, improvement seen but only some were
statistically significant


Future Research
• Need to assess if:– Pts who have had a successful treatment but regain
weight after cessation can have treatment recommenced– RCT to compare orlistat/sibutramine and behaviour
treatment alone– Effects and toxicity on longer treatments– Use in younger children now obesity in children is
increasing– Assess the benefits of short term wt loss by decreasing
co morbidities compared to permanent wt loss

FUTURE• Regard obesity as chronic disease requiring long
term support and follow up• GP magazine this week, article regarding obesity
as a disease requiring quality indicators• GMS contract offer 3 points directly to obesity-
measuring BMI in diabetics• Chronic condition affecting 25% of population but
only gets 0.3% of quality points• Management of independent markers of metabolic
syndrome comprises approx 30% of all available points

SURGICAL TREATMENTS• BMI > 40• BMI >35 with significant disease• 3 operations: gastric restriction: 40-60% XS wt loss gastric bypass: approx 50% wt loss 1% operative mortality biliopancreatic diversion:78% wt loss 1% operative mortality, nutritional deficiencies Most can be performed laparoscopically