Embed Size (px)
Citation preview
Rheum-inationsFor the physical therapist
All you wanted to know about rheumatology and more!
Susan Shenoi MD, MS, RhMsUSAssistant Professor
Clinical DirectorSeattle Children’s Hospital
10-2017
Disclosures
No financial disclosuresWill reference off label use of drugs
Disclaimer
I am not kind enough,not patient enough,not skilled enough…..to ever do what you do!
Thank you for all that you do to help our kids!
Objectives• Case based learning• Recognize patterns of joint pain• Recognize signs of arthritis• Recognize Juvenile Idiopathic Arthritis
– Categories– Medications used– Complications
• Impact exercise on child • Brief overview of Juvenile dermatomyositis (JDM)• Identify resources for further help
Pediatric Rheumatology “pearls”
Recognize Patterns of Joint Pain
ANA leg pain 3 months
• activity rest• Exam normal• Labs - not needed
If done normalOr + ANA (1:80)
Mechanical• Usually no/ minimal am stiffness
• Worsening pain with increased activity
• Lack systemic symptoms like fatigue
• Swelling/ Warmth/ Decreased ROM +/-
• Examples: hypermobility, tendonitis, osteoarthritis*
* Seen more commonly in adults
ANA leg pain 3 months
• activity rest such as after sitting for long time
• Exam shows swollen warm joint(s) that are not moving well
• Labs – ESR and CRP are highOr + ANA (1:640)
Inflammatory• AM stiffness/ Gelling
• Pain better with activity
• Fatigue +/-
• Swelling/ Warmth/ Decreased ROM present
• Examples: JIA, Inflammatory bowel disease related arthritis
ANA body pain 3 months
• activity rest• Pain all day long• Pain with light touch• Exam normal except
for allodynia• Labs - normal
Or + ANA (1:80)
Central Pain Sensitization• Prolonged AM stiffness
• Pain all over, several days (months/ years)
• Increasing pain with activity
• Systemic symptoms, fatigue +, non-restorative sleep
• Tender points/ Allodynia/ Hyperalgesia
• Joint exam usually normal – no swelling, warmth, normal
ROM
Rheumatology “Pearl” #1Pattern recognition
3 patterns to joint pain:
– Inflammatory
– Mechanical
– Central Pain Sensitization
Recognize signs of Arthritis
Arthritis = Juvenile Arthritis
A) True
B) False
False – arthritis can be secondary to many causes infection, cancers etc ……
ANA leg pain 3 months • Waking up at night
with pain• Fevers on and off • Exam arthritis of
knee• Labs –ESR 30 CRP 2.5
CBC platelet 90KWBC 3 K/mm3
Rheumatology “Pearl” #2
Arthritis ≠ Rheumatology
Juvenile arthritis is a diagnosis of exclusionMust rule out
– infection, malignancies,– metabolic, mechanical etc
Arthritis ≠ RheumatologyMalignancy–may mimic JIA– 21-33% of ALL present with bone pain– 62% have musculoskeletal symptoms
Examples leukemia, lymphoma, neuroblastoma, localizedbone tumors (Ewing's)
AVOID STEROIDS TILL DIAGNOSIS CLEARJones OY, Pediatrics, 2006
When do you suspect it!– pain at rest, at night, or out of proportion – back pain, bone pain, bone tenderness– atypical fevers– night sweats– weight loss
Useful studies– low counts (>2 cell lines down)– lactate dehydrogenase (LDH), uric acid– Imaging (CT chest, abdomen – mass/ lymph
nodes)– BM/ LN biopsy
Recognize Juvenile Arthritis
Vignette• DR 7 yr boy limp for12 months• Saw orthopedic 8/15
- X-ray foot and ankle normal- Told limp was behavioral
• Second opinion - orthopedic 11/15• Decreased range of motion (ROM) hip• Inflammatory markers –
– CRP normal (<0.8) ESR 28 (0-10)
• Blood counts - CBC normal• Bone scan normal• MRI ankle and pelvis ordered
Right hip arthritis/ synovitisRheumatology referral• ROM, pain right hip• warmth swelling both
ankles • Enthesitis (inflammation . tendons, muscle
insertion to bone)• Plantar fasciitis
DiagnosisJIA - Enthesitis related arthritis (ERA)
Arthritis = inflammation of joints
A) True
B) False
True – red, warm, swollen, decreased
range of motion
Shenoi S. JIA Pediatr Rev. 2017 May;38(5):221-232.
Arthritis is only for old people
A) True
B) False
False – kids get arthritis too,
CDC 1 in 250 kids have arthritis
Rheumatoid Arthritis Adult
Arthritis in Children
Juvenile Arthritis = JCA = JRA = JIA
A) True
B) False
True – one disease many names
Juvenile Idiopathic Arthritis
• < 16 years• > 6 weeks duration• No known cause
Petty R et al . ILAR Classification Edmonton J. Rheum. 2001
JIA is due to vitamin deficiency
A) True
B) False
False – we don’t know what causes it?
Complex Genetic Trait
Gene-Environmental Factors
Pathogenesis
JIA
Environment
GenesOther
Prakken B et al . Lancet 2011
Chronic inflammation: imbalance between mediators
TNF� IL-1�IL-8
IL-12IFN�
IL-4/IL-13IL-1Ra
TGF� IL-10
Chronic inflammation: Imbalance between mediators
All juvenile arthritis is the same
A) True
B) False
False – 7 categories of JIA
different presentations
ILAR ClassificationInternational League of Associations for Rheumatology
7 mutually exclusive categories:Systemic arthritisOligoarthritis (persistent, extended)Polyarthritis (RF +)*Polyarthritis (RF -)Psoriatic arthritisEnthesitis-related arthritisUndifferentiated arthritis
Petty R et al . ILAR Classification Edmonton J. Rheum. 2001
Categories of JIA
JIAOligoarticular��4 joints
Polyarticular> 4 joints
Extended oligo> 4 joints
Enthesitis-related
Psoriatic arthritis
Systemic-onset Undifferentiated!
RF(-) RF(+)
Image courtesy: Kristin Hayward
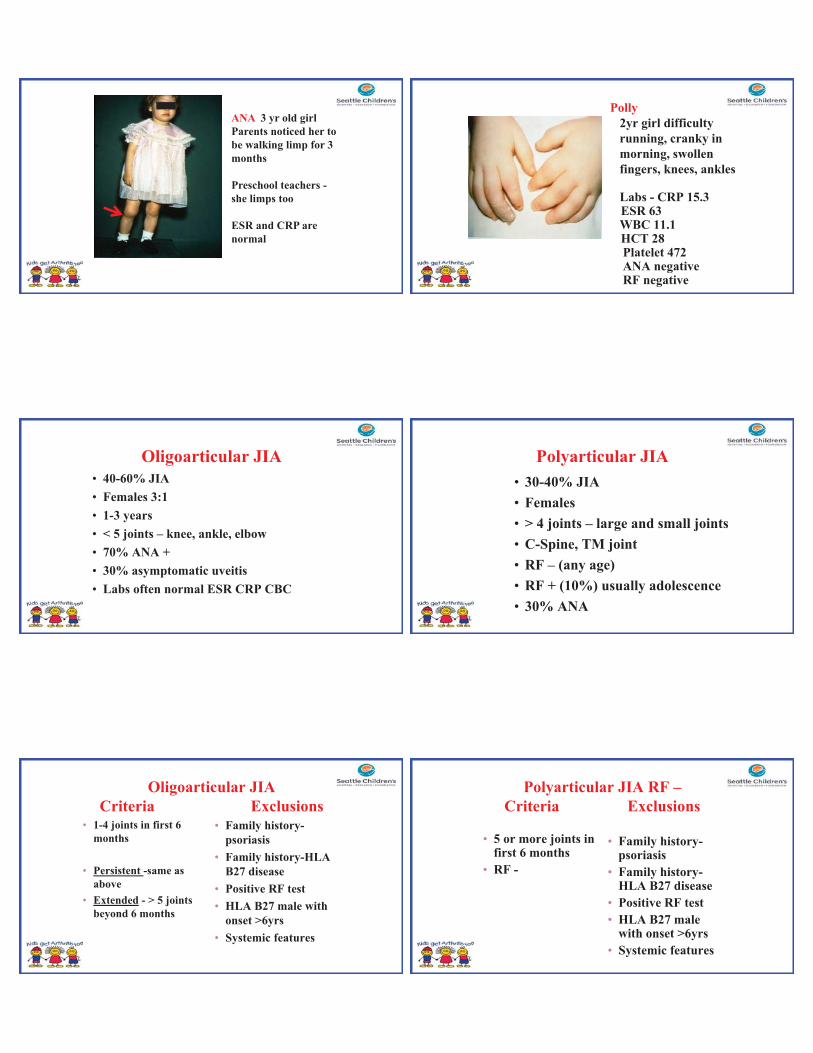
ANA 3 yr old girl Parents noticed her to be walking limp for 3 months
Preschool teachers -she limps too
ESR and CRP are normal
Oligoarticular JIA• 40-60% JIA• Females 3:1• 1-3 years• < 5 joints – knee, ankle, elbow• 70% ANA +• 30% asymptomatic uveitis• Labs often normal ESR CRP CBC
Oligoarticular JIA Criteria Exclusions
• 1-4 joints in first 6 months
• Persistent -same as above
• Extended - > 5 joints beyond 6 months
• Family history-psoriasis
• Family history-HLA B27 disease
• Positive RF test• HLA B27 male with
onset >6yrs• Systemic features
Polly2yr girl difficultyrunning, cranky inmorning, swollenfingers, knees, ankles
Labs - CRP 15.3 ESR 63 WBC 11.1 HCT 28 Platelet 472 ANA negativeRF negative
Polyarticular JIA• 30-40% JIA• Females • > 4 joints – large and small joints• C-Spine, TM joint• RF – (any age)• RF + (10%) usually adolescence• 30% ANA
Polyarticular JIA RF –Criteria Exclusions
• 5 or more joints in first 6 months
• RF -
• Family history-psoriasis
• Family history-HLA B27 disease
• Positive RF test• HLA B27 male
with onset >6yrs• Systemic features
Polyarticular JIA RF +Criteria Exclusions
• 5 or more joints in first 6 months
and• + RF test twice 3
months apart
• Family history-psoriasis
• Family history-HLA B27 disease
• HLA B27 male with onset >6yrs
• Systemic features
Rheumatoid Nodules
Micrognathia and Retrognathia
Spykar6 yr boy fevers high spiking103F X 2 wksRash on/ off,Recently shortnessof breathO/E big liver spleenarthritis
Systemic JIA
• Arthritis with or preceded by fever 2 weeks and
• any 1 of : -rash-adenopathy-serositis-liver-spleen
Systemic JIA– 10-20% JIA– fevers - daily spike (often pm) to >103F– 1/3 pericarditis, pleuritis– Adenopathy– Hepatosplenomegaly– Arthritis variable– Evanescent rash in about 80%– Anemia, Elevated WBC and platelets – Very high ESR, CRP, ferritin– ANA, RF negative
.Shenoi S, Wallace CA. Diagnosis & Rx of SJIA. J Pediatr. 2016 Oct;177:19-26.
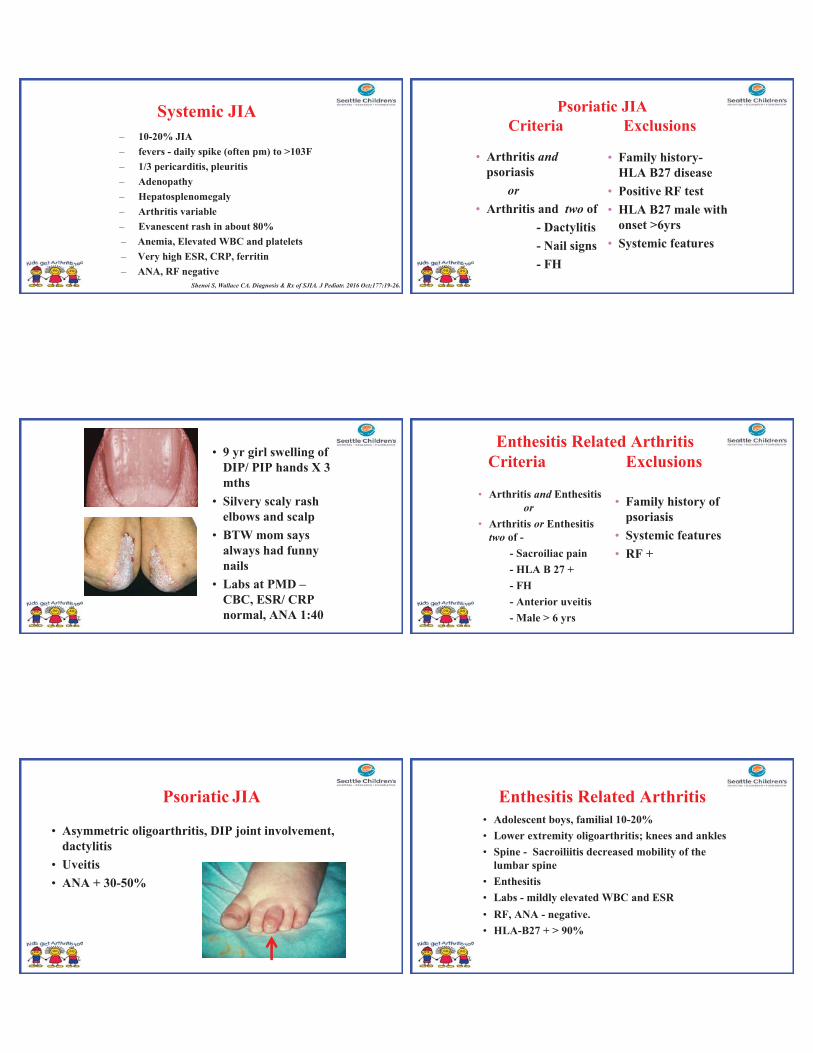
• 9 yr girl swelling of DIP/ PIP hands X 3 mths
• Silvery scaly rash elbows and scalp
• BTW mom says always had funny nails
• Labs at PMD –CBC, ESR/ CRP normal, ANA 1:40
Psoriatic JIA
• Asymmetric oligoarthritis, DIP joint involvement, dactylitis
• Uveitis• ANA + 30-50%
Psoriatic JIA Criteria Exclusions
• Arthritis and psoriasis
or• Arthritis and two of
- Dactylitis- Nail signs- FH
• Family history-HLA B27 disease
• Positive RF test• HLA B27 male with
onset >6yrs• Systemic features
• Arthritis and Enthesitis or
• Arthritis or Enthesitis two of -
- Sacroiliac pain- HLA B 27 +- FH- Anterior uveitis- Male > 6 yrs
• Family history of psoriasis
• Systemic features• RF +
Enthesitis Related ArthritisCriteria Exclusions
Enthesitis Related Arthritis• Adolescent boys, familial 10-20% • Lower extremity oligoarthritis; knees and ankles • Spine - Sacroiliitis decreased mobility of the
lumbar spine • Enthesitis • Labs - mildly elevated WBC and ESR• RF, ANA - negative. • HLA-B27 + > 90%
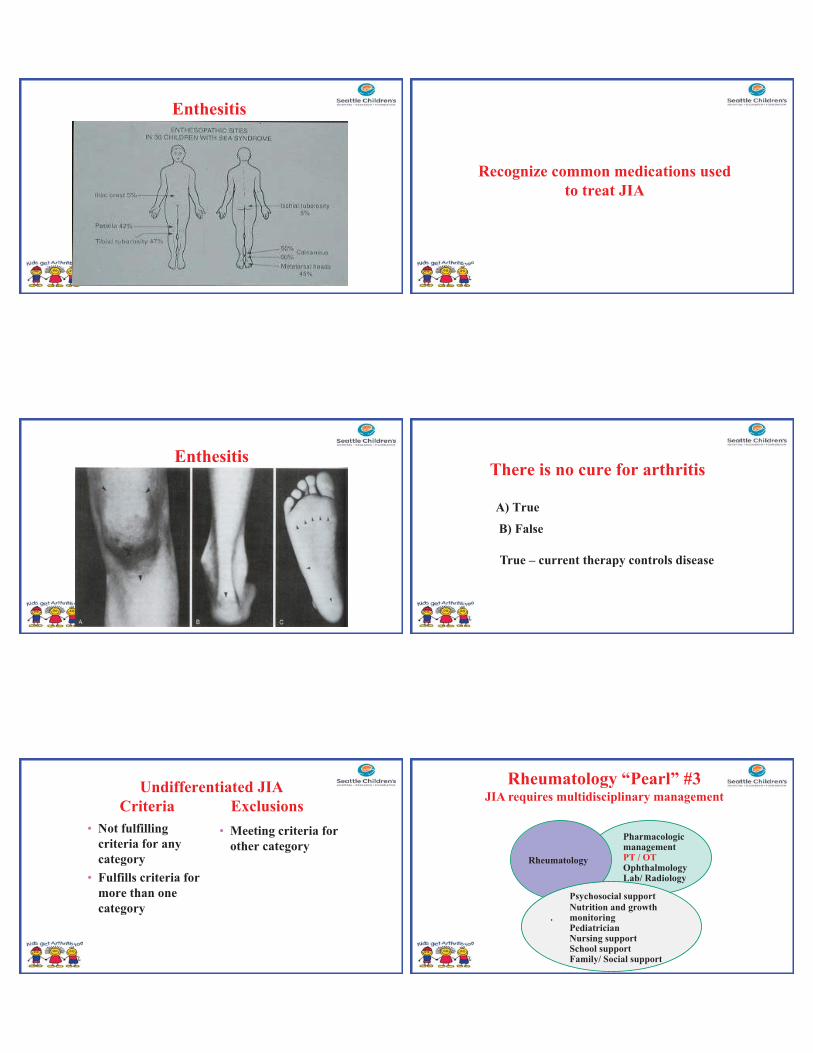
Enthesitis
Enthesitis
Undifferentiated JIACriteria Exclusions
• Not fulfilling criteria for any category
• Fulfills criteria for more than one category
• Meeting criteria for other category
Recognize common medications used to treat JIA
There is no cure for arthritis
A) True
B) False
True – current therapy controls disease
Pharmacologic managementPT / OT OphthalmologyLab/ Radiology
Rheumatology
Psychosocial supportNutrition and growth
. monitoringPediatrician Nursing supportSchool supportFamily/ Social support
Rheumatology “Pearl” #3JIA requires multidisciplinary management
Arthritis can lead to blindness
A) True
B) False
True – some children have uveitis
if untreated can cause blindness
ANA positive children more risk
regular ophthalmologic screening
Rheumatology “Pearl” #4Look into the Eyes
Besides the PT the ophthalmologist is the rheumatologists best friend!
JIA Anterior Uveitis - Asymptomatic
Increasedrisk if
ANA+
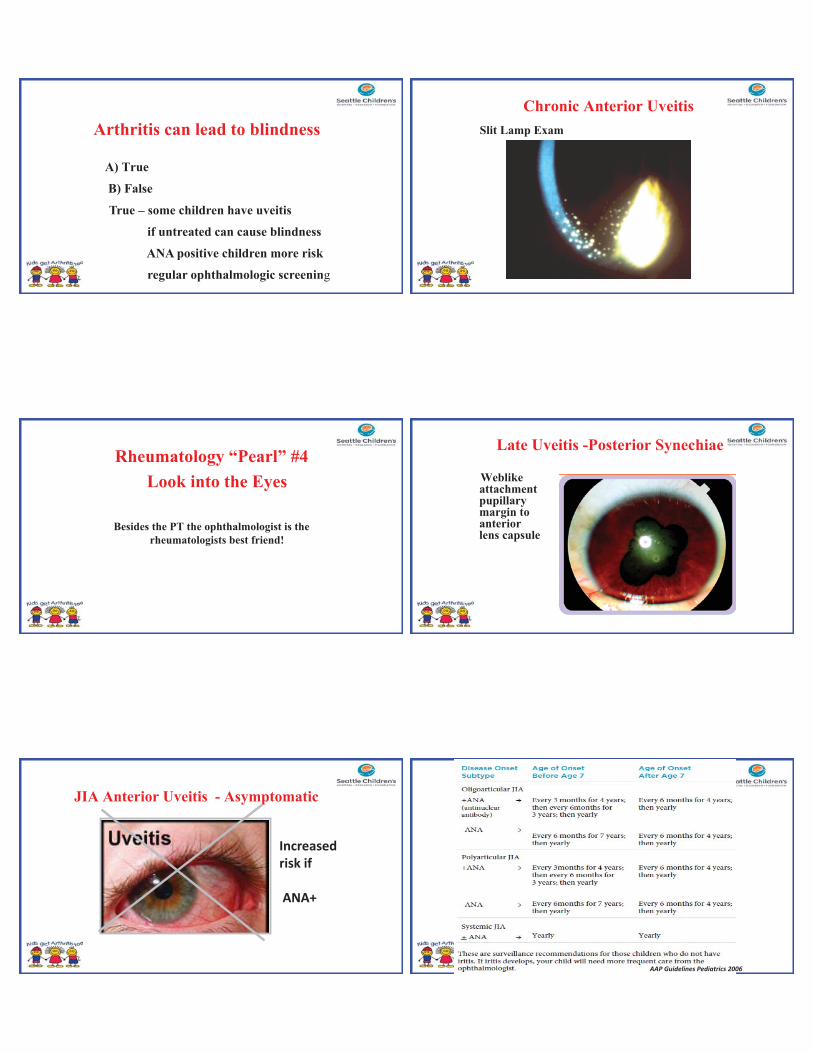
Chronic Anterior UveitisSlit Lamp Exam
Late Uveitis -Posterior Synechiae
Weblike attachment pupillary margin to anterior lens capsule
AAP Guidelines Pediatrics 2006
We use chemotherapy to Rx JIAA) True
B) False
True – many medications are known
chemotherapeutic meds (methotrexate,
cyclosporine, cyclophosphamide)
Powerful medicines
Knowing how and when to use them
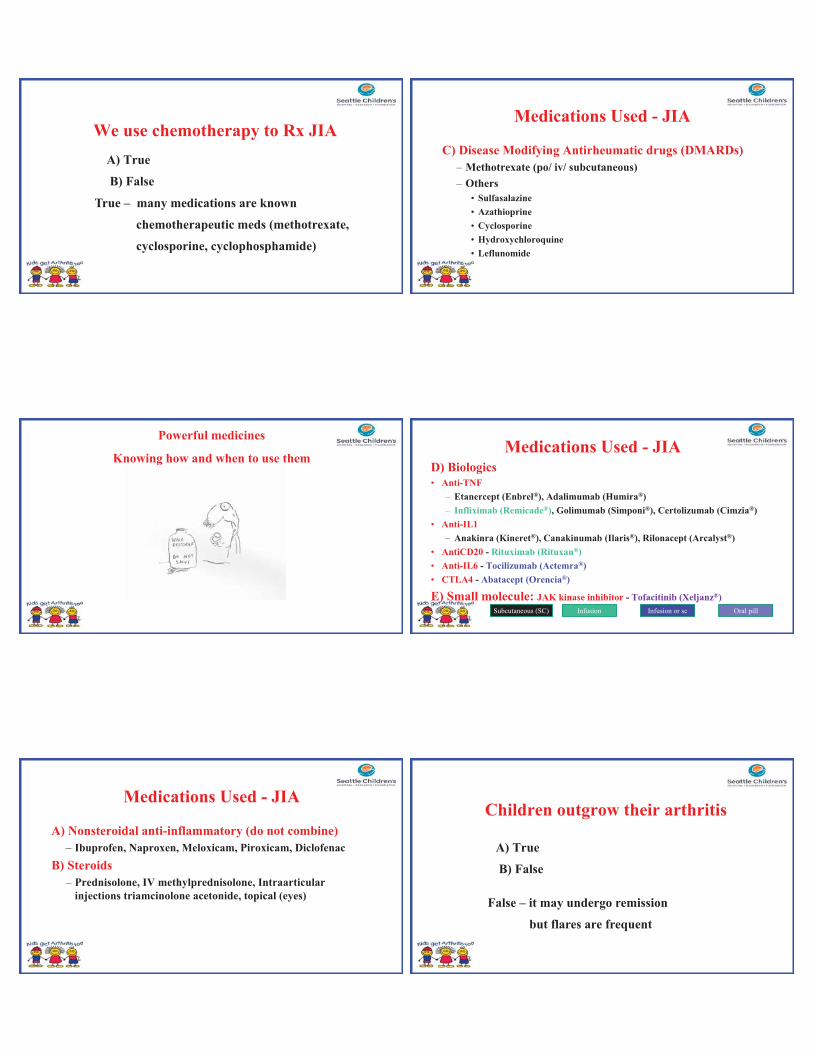
Medications Used - JIA
A) Nonsteroidal anti-inflammatory (do not combine)– Ibuprofen, Naproxen, Meloxicam, Piroxicam, Diclofenac
B) Steroids– Prednisolone, IV methylprednisolone, Intraarticular
injections triamcinolone acetonide, topical (eyes)
Medications Used - JIA
C) Disease Modifying Antirheumatic drugs (DMARDs)– Methotrexate (po/ iv/ subcutaneous)– Others
• Sulfasalazine• Azathioprine• Cyclosporine• Hydroxychloroquine• Leflunomide
Medications Used - JIAD) Biologics • Anti-TNF
– Etanercept (Enbrel®), Adalimumab (Humira®)– Infliximab (Remicade®), Golimumab (Simponi®), Certolizumab (Cimzia®)
• Anti-IL1– Anakinra (Kineret®), Canakinumab (Ilaris®), Rilonacept (Arcalyst®)
• AntiCD20 - Rituximab (Rituxan®)• Anti-IL6 - Tocilizumab (Actemra®)• CTLA4 - Abatacept (Orencia®)
E) Small molecule: JAK kinase inhibitor - Tofacitinib (Xeljanz®)Infusion Infusion or sc Oral pillSubcutaneous (SC)
Children outgrow their arthritis
A) True
B) False
False – it may undergo remission
but flares are frequent
• 80% of children continue to have active disease
• Joint damage frequently occurs, and is greatest in the first 2 years of disease
• 44% achieve remission
• But by 2 yrs off of meds, most have flared
• <10% are successfully off meds >5 years
Ringold & Wallace. Rheumatology 2009.
Children DO NOT outgrow their arthritis
Early treatment
TREAT – Inactive disease (ID) and clinical remission on medications are
achievable – Best chance of achieving
• Rapid and early initiation of therapy • For each month earlier a subject was treated
odds ID increased by 1.32; p = 0.011
Wallace CA et al. TREAT trial A & R 2012
Early treatmentACUTE - JIA
– Compelling evidence for early aggressive therapy – 3 groups: open label study
• Infliximab and methotrexate• Combination DMARD therapy (methotrexate, hydroxychloroquine,
sulfasalazine)• Methotrexate
– Response seen in • 100% infliximab and methotrexate• 65% combination DMARD• 50% methotrexate (p<0.0001) Tynjälä P et al. Ann. Rheum. Dis. 2011
Rheumatology “Pearl” #5
EARLY RECOGNITION IS KEY (you can help!)
Once diagnosed early and aggressive therapy improves outcomes!
Treatment JIA - CARRA • Consensus Treatment Plans• Childhood Arthritis and Rheumatology Research Alliance • North American organization • > 400 pediatric rheumatologists, researchers and research
coordinators
www.carragroup.org
CARRA - CTP
Consensus treatment plans (CTP) – SJIA– Polyarticular JIA
Dewitt E et all. AC & R 2012Ringold S, Shenoi S et al . AC & R 2014
Kimura Y et al . AC & R 2014
Ringold S, Shenoi S et al. AC & R 2014
Polyarticular JIA CTP
Recognize common complications JIA
Complications Ana who had OligoJIA is doing well and in remission without active arthritis – she still has a gait that is limping and off – why?
Affected leg grows longer Leg length discrepancy Shoe lift
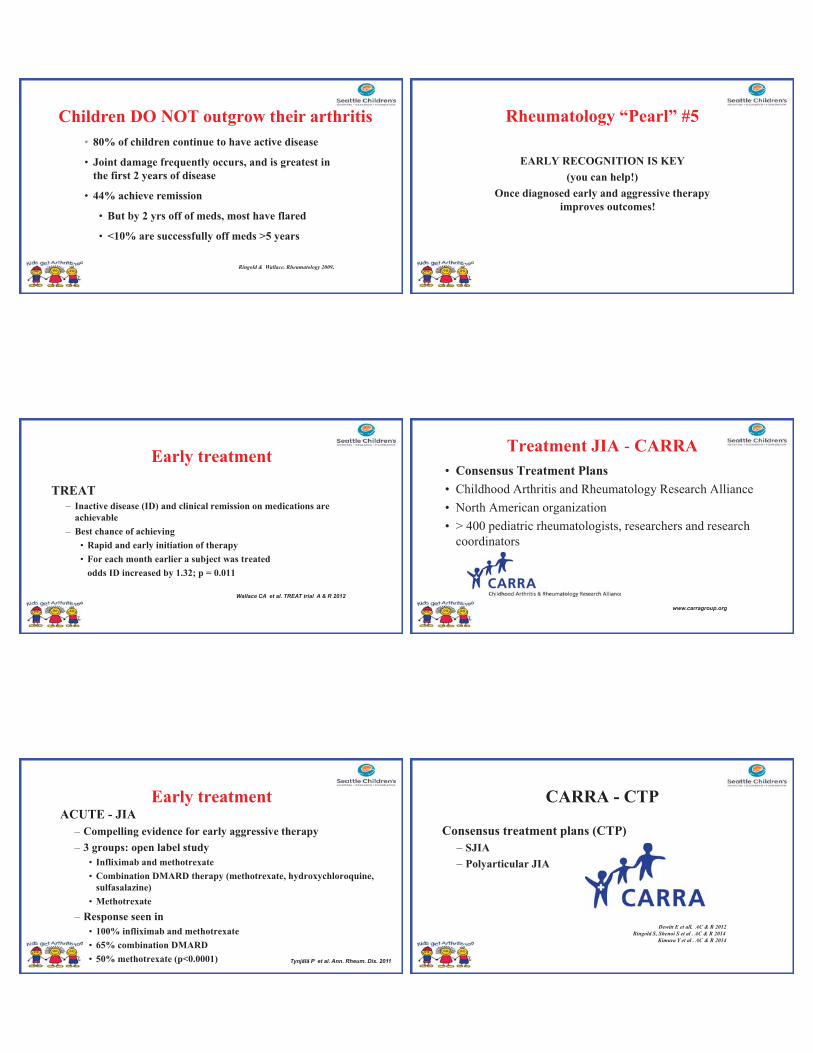
Other complications of JIA
• Joint space narrowing• Destruction of cartilage• Erosions• Chronic pain • Joint damage
Impact Exercise in rheumatic diseases
PT = great resource for children with joint pain
A) True
B) False
100% TRUE
How can JIA impact ChildPhysicalpain, weakness, stiffness after sitting, swelling joints, difficulty writing, unable to participate PE, medication side effects (steroids – chubby, methotrexate - nausea)
Emotionalneed for chronic medications, long term injections/ infusions, sense of being different from peers, drain on family resources (doctors appts, bills, copay, hospital stays)
Educationmissing school (doctor visits, OT/PT, infusions, flares), difficulty with vision (rarely), completing assignments/ exams (stiff hands)
Exercise can damage the joints A) True
B) False
False - exercise helps maintain
good range of motion
- modifications in case of flares
Rheumatology “Pearl” #6Exercise is the ideal drug
• Safe • Inexpensive• Widely available• Dose it (pace, self-limit, modify)
Houghton K. The Physician and Sports medicine. 2012 Sep 1;40(3):77 82.Hebestreit, H et al. Journal of Rheumatology, 1998. 25(8): p. 1626 33.Lelieveld, O.T. et al. Arthritis & Rheumatism, 2008. 59(10): p. 1379Henderson, C.J. et al. Arthritis Care & Research, 1995. 8(2): p. 11Houghton K et al. Journal of Rheumatology, 2013:40(6):979.
Exercise in JIA
• Exercise may improve ROM, active joint count, function, QOL & fitness
• Exercise DOES NOT worsen disease activity or cause flares• Intervention trials small to no effect
Takken T et al. Eur J Phys Rehab Med 2008;44(3):287 97.Cavallo S et al. 2016. Arch Phys Med Rehabil. 2016 Dec 6.
Switching gears!
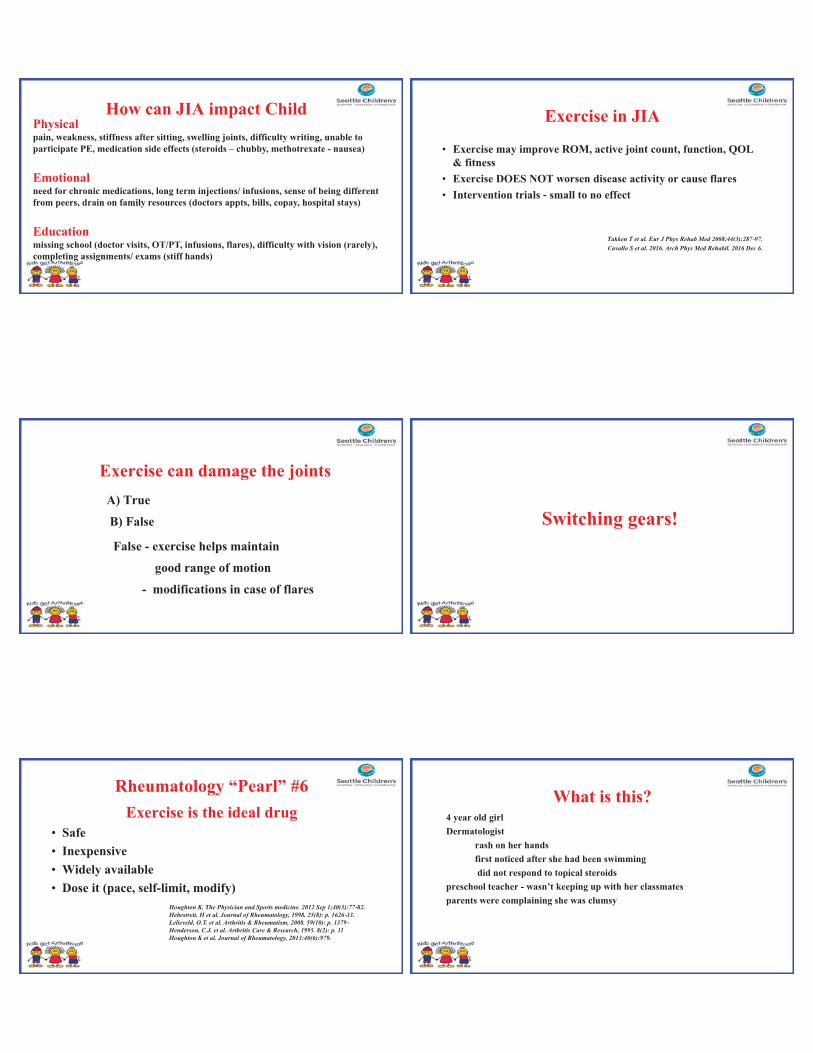
What is this?4 year old girl Dermatologist
rash on her handsfirst noticed after she had been swimmingdid not respond to topical steroids
preschool teacher - wasn’t keeping up with her classmatesparents were complaining she was clumsy
Visual diagnosis
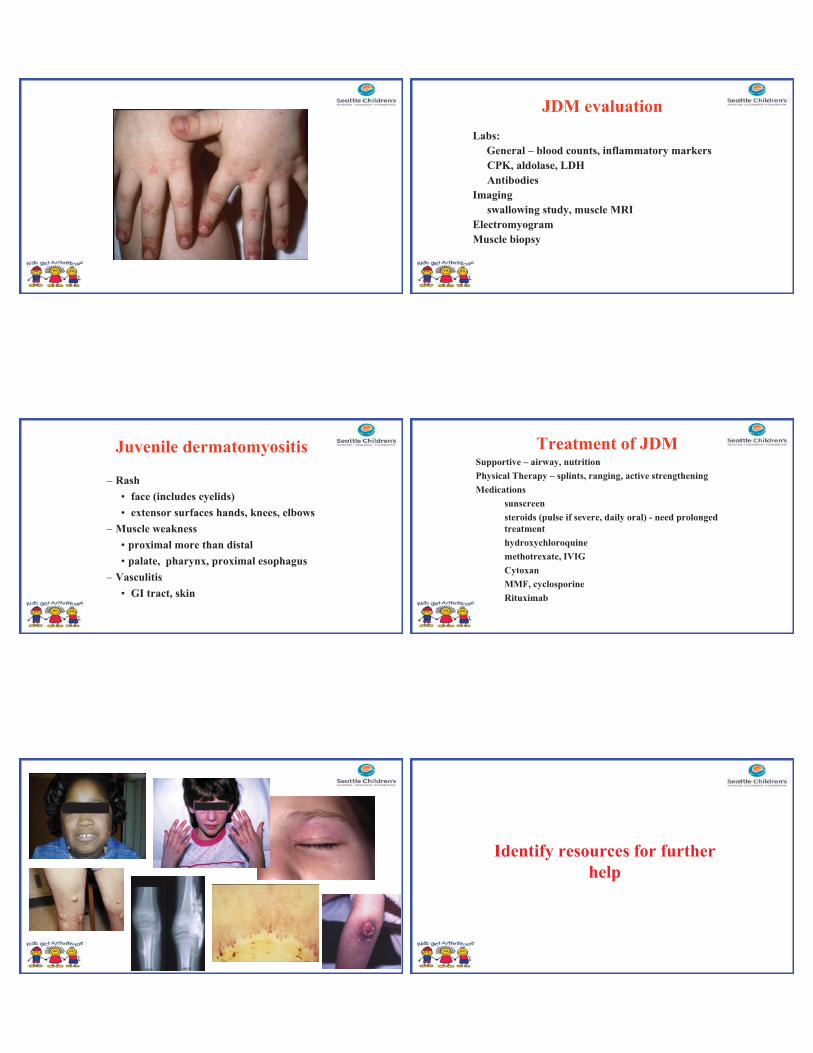
Juvenile dermatomyositis
– Rash • face (includes eyelids)• extensor surfaces hands, knees, elbows
– Muscle weakness • proximal more than distal• palate, pharynx, proximal esophagus
– Vasculitis • GI tract, skin
JDM evaluationLabs:
General – blood counts, inflammatory markersCPK, aldolase, LDHAntibodies
Imagingswallowing study, muscle MRI
ElectromyogramMuscle biopsy
Treatment of JDMSupportive – airway, nutritionPhysical Therapy – splints, ranging, active strengtheningMedications
sunscreensteroids (pulse if severe, daily oral) - need prolonged treatmenthydroxychloroquinemethotrexate, IVIGCytoxanMMF, cyclosporineRituximab
Identify resources for further help
Resources
• Pediatric Rheumatology Staff – Seattle Children’s– 206-987-2193 (parents permission)– Doctor on call 206-987-7777– [email protected]
• Other resourceswww.arthritis.orgwww.rheumatology.org
Arthritis Foundation
This is a picture of Arthritis Camp – 1970’s
A) True
B) False
True
This is a picture ofArthritis Camp in 2010
A) True
B) False
True
THANK YOU
For the invitation
And your attention
AND MY HOPE…...
“Too late is the medicine prepared, when the diseasehas gained strength by long delay”
Questions





























