Embed Size (px)
DESCRIPTION
Rheumatism ppt
Citation preview
Kevin Latinis, M.D./Ph.D.Division of RheumatologyDept. of Internal [email protected]
Rheumatology Rheumatology 101:101:
What you need to know What you need to know for your ambulatory for your ambulatory
medicine experiencemedicine experience
Rheumatology 101Rheumatology 101
ArthritisArthritis-Inflammatory (RA, spondyloarthropathies)-Inflammatory (RA, spondyloarthropathies)-Mechanical (OA)-Mechanical (OA)LupusLupusFibromyalgiaFibromyalgiaLow back pain and other peri-articular Low back pain and other peri-articular complaintscomplaintsGeneral musculoskeletal exam (time General musculoskeletal exam (time permitting)permitting)
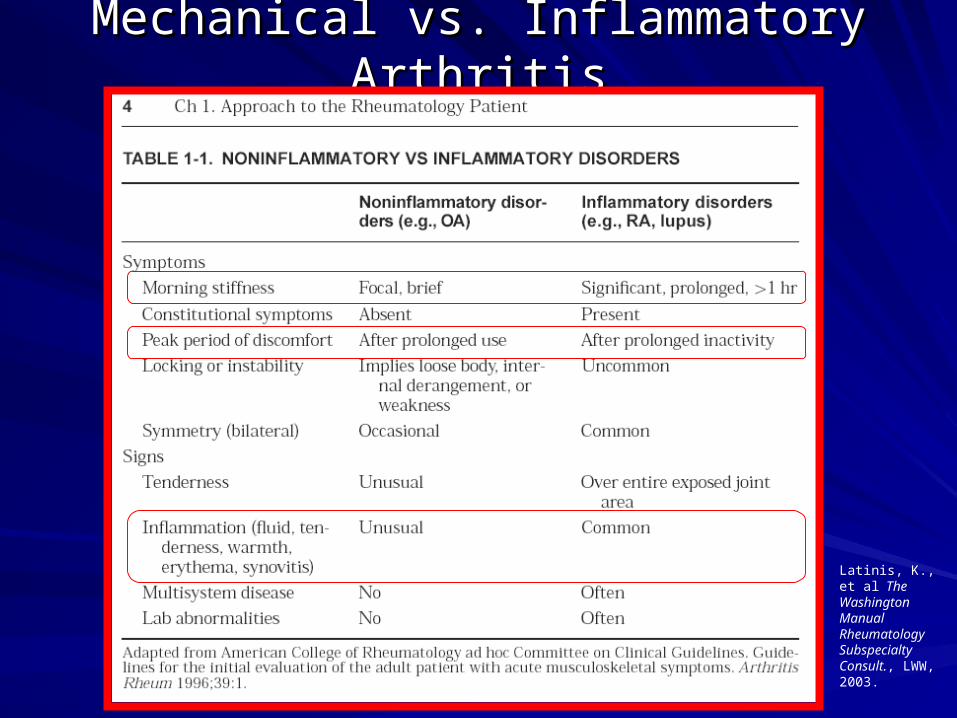
Mechanical vs. Inflammatory ArthritisMechanical vs. Inflammatory Arthritis
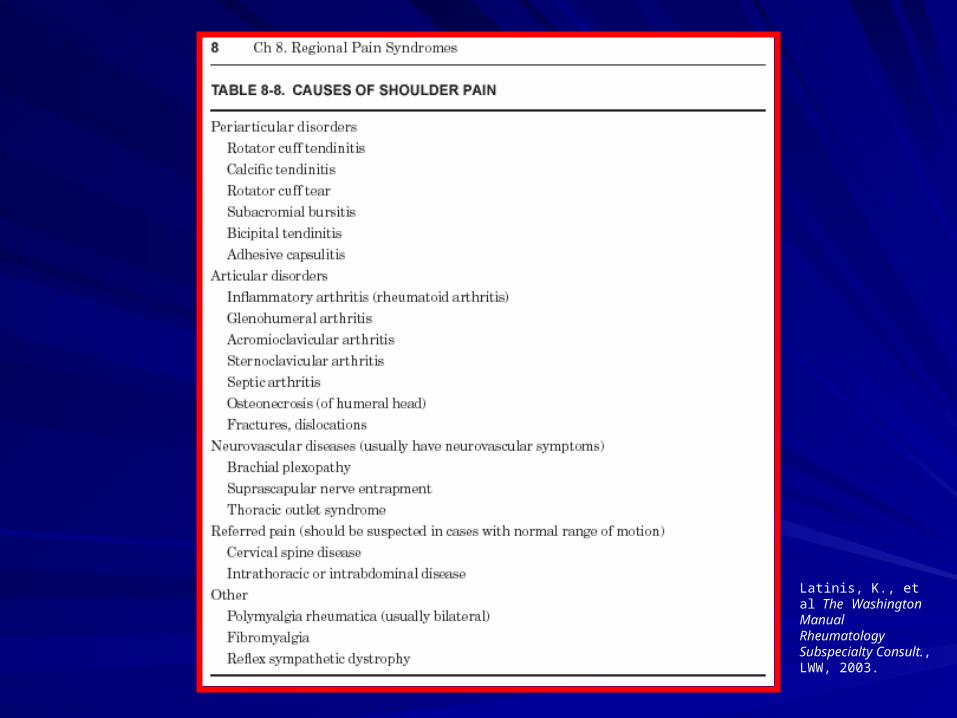
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
Osteoarthritis-BackgroundOsteoarthritis-Background
Very commonVery common-2-2ndnd leading cause for disability in USA leading cause for disability in USA-In patients 60 and older: affects 17% of -In patients 60 and older: affects 17% of men and 30% of womenmen and 30% of women-Estimated that 59.4 million patients will -Estimated that 59.4 million patients will have OA by the year 2020have OA by the year 2020EtiologyEtiology-primary idiopathic-primary idiopathic-secondary-secondary
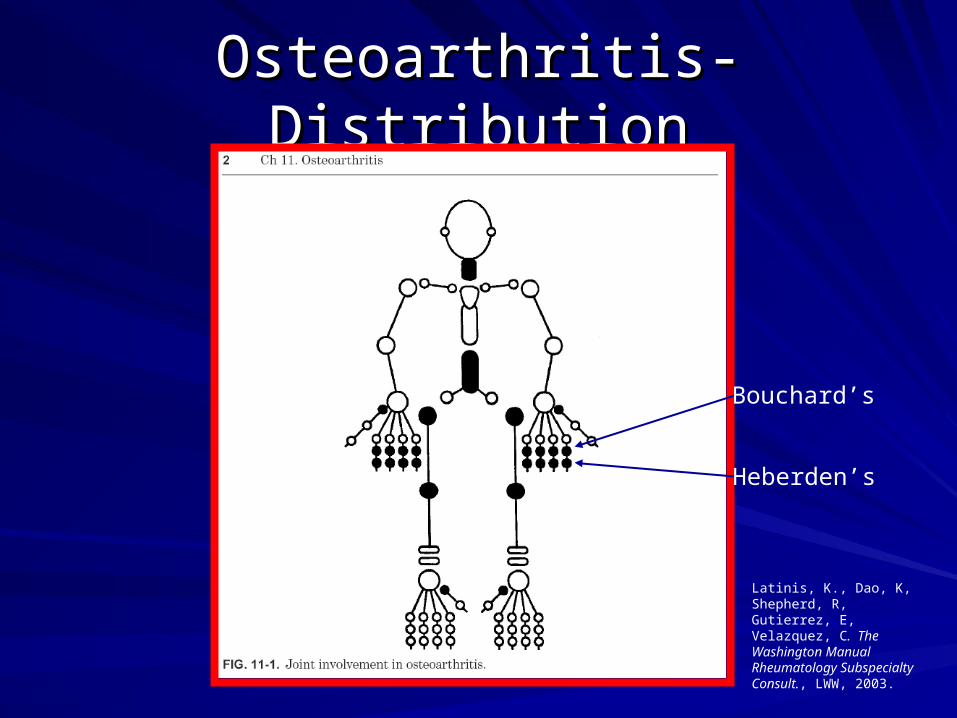
Osteoarthritis-DistributionOsteoarthritis-Distribution
Latinis, K., Dao, K, Shepherd, R, Gutierrez, E, Velazquez, C. The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
Bouchard’s
Heberden’s

Osteoarthritis-DiagnosisOsteoarthritis-Diagnosis
ClinicalClinical
Supported by X-raysSupported by X-rays
Non-inflammatory lab data, if anyNon-inflammatory lab data, if any
Osteoarthritis-TreatmentOsteoarthritis-Treatment
Pain reliefPain relief-Analgesics and NSAIDs/Cox-2 Inhibitors-Analgesics and NSAIDs/Cox-2 InhibitorsSMOADs (structure modifying osteoarthritis drugs)SMOADs (structure modifying osteoarthritis drugs)-Glucosamine Sulfate -Glucosamine Sulfate -see meta-analysis McAlindon et al. JAMA, 283: -see meta-analysis McAlindon et al. JAMA, 283: 3/2000, p. 14693/2000, p. 1469
-many under development-many under developmentNon-pharmacologic approachesNon-pharmacologic approaches-Reduce stress/load on joint-Reduce stress/load on joint-Strengthen surrounding muscles-PT/OT-Strengthen surrounding muscles-PT/OT-Weight reduction-Weight reduction-Patient education-Patient educationLimit disability and improve quality of lifeLimit disability and improve quality of life
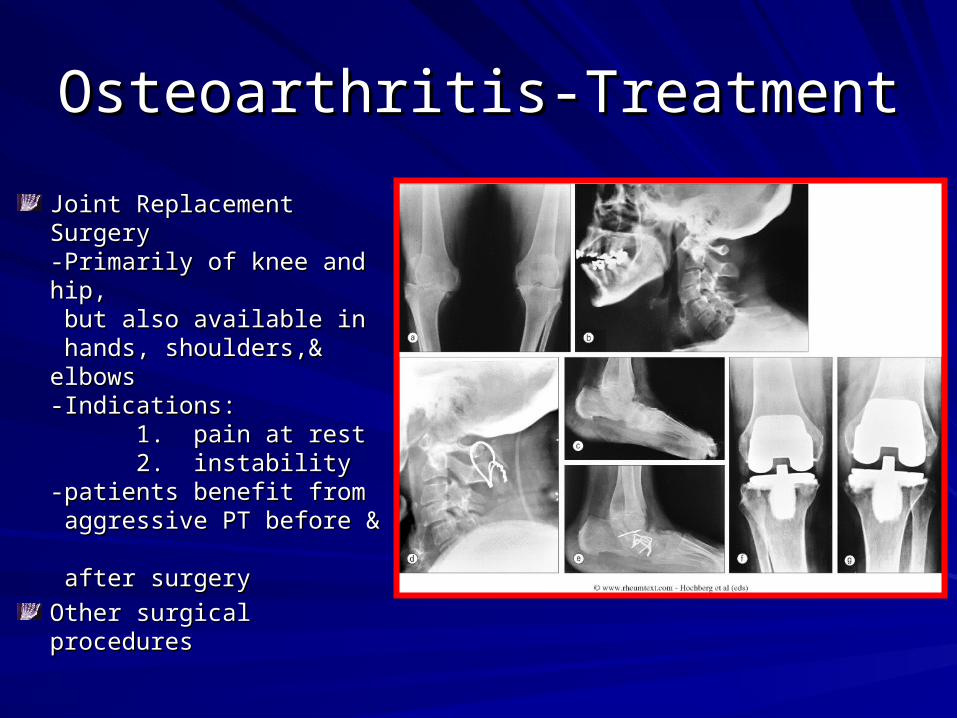
Osteoarthritis-TreatmentOsteoarthritis-Treatment
Joint Replacement SurgeryJoint Replacement Surgery-Primarily of knee and hip, -Primarily of knee and hip, but also available in but also available in hands, shoulders,& elbows hands, shoulders,& elbows-Indications:-Indications:
1. pain at rest1. pain at rest2. instability2. instability
-patients benefit from -patients benefit from aggressive PT before & aggressive PT before & after surgery after surgery
Other surgical proceduresOther surgical procedures
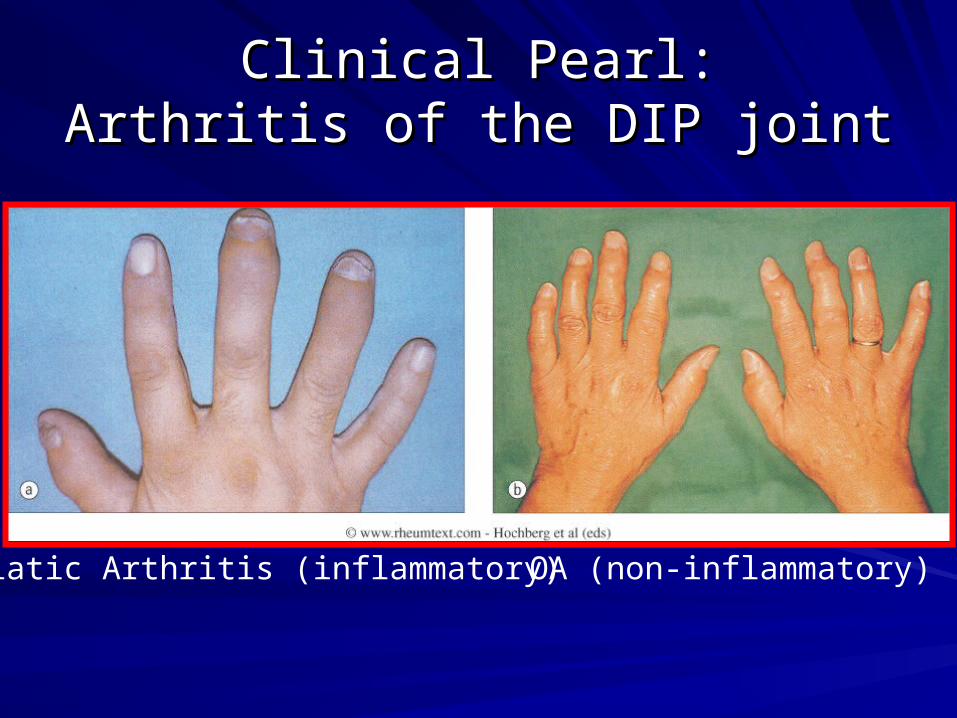
Clinical Pearl:Clinical Pearl:Arthritis of the DIP jointArthritis of the DIP joint
OA (non-inflammatory)Psoriatic Arthritis (inflammatory)
Inflammatory ArthritisInflammatory Arthritis
Rheumatoid arthritisRheumatoid arthritisSpondyloarthropathiesSpondyloarthropathies-Undifferentiated-Undifferentiated-Ankylosing spondylitis-Ankylosing spondylitis-Psoriatic arthritis-Psoriatic arthritis-Reactive arthritis (formerly Reiter’s syndrome)-Reactive arthritis (formerly Reiter’s syndrome)-Enteropathic arthritis-Enteropathic arthritisSLE, Sjogrens, Scleroderma, Polymyalgia SLE, Sjogrens, Scleroderma, Polymyalgia rheumatica, Vasculitis, Infectious (bacterial, viral, rheumatica, Vasculitis, Infectious (bacterial, viral, other), Undifferentiated connective tissue other), Undifferentiated connective tissue diseasedisease
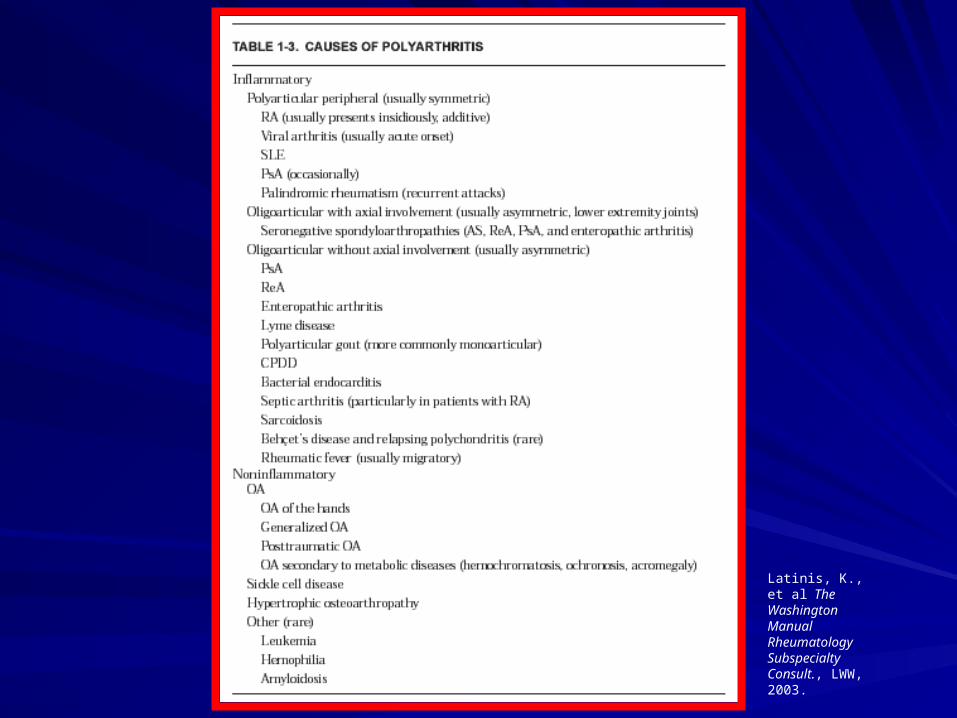
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
Rheumatoid Arthritis-BackgroundRheumatoid Arthritis-Background
Symmetric, inflammatory polyarthritisSymmetric, inflammatory polyarthritis
Affects ~1% of our populationAffects ~1% of our population
Occurs in women 3x more than menOccurs in women 3x more than men
EtiologyEtiology-Genetic, class II molecules (HLA-DRB1)-Genetic, class II molecules (HLA-DRB1)-Autoimmune-Autoimmune-?Environmental-?Environmental
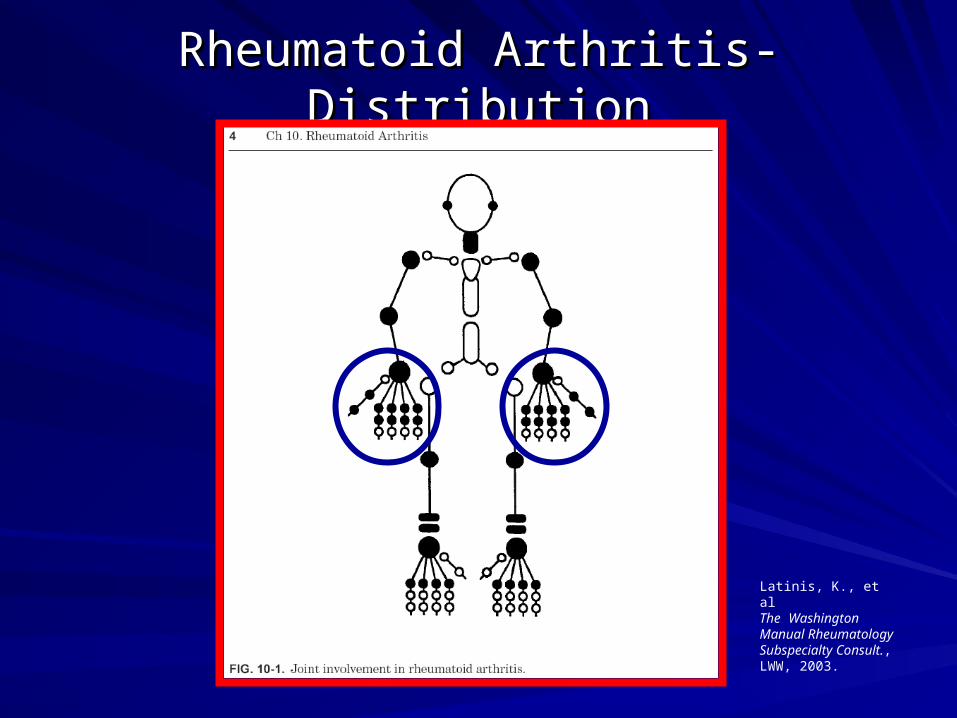
Rheumatoid Arthritis-DistributionRheumatoid Arthritis-Distribution
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
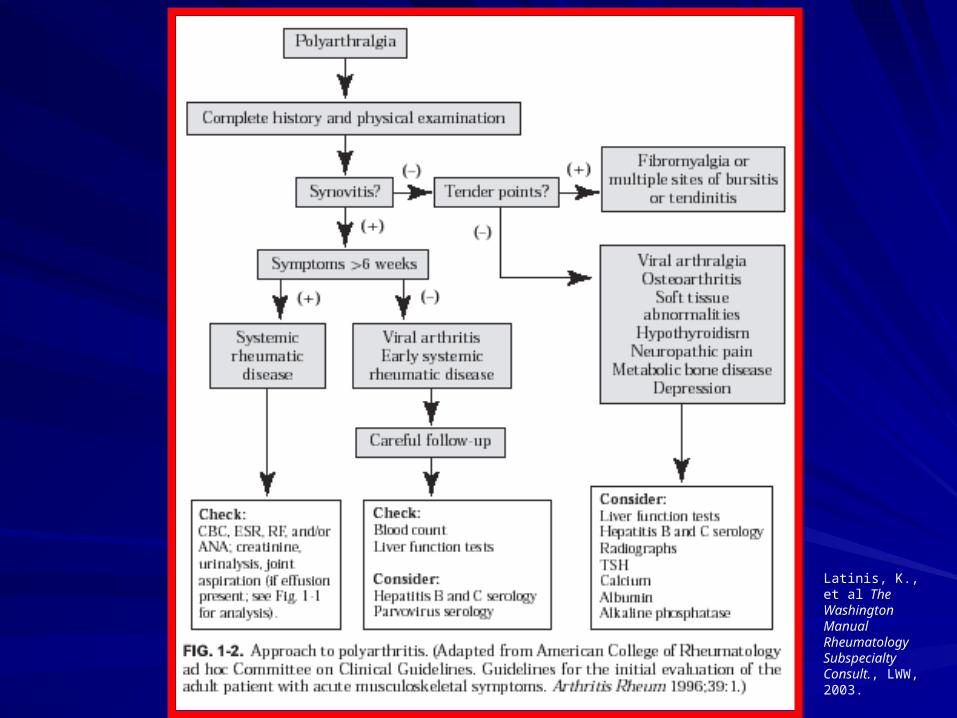
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
Definition-An inflammatory multisystem disease of unknown etiologywith protean clinical and laboratory manifestations and avariable course and prognosis.-Immunologic aberrations give rise to excessive autoantibodyproduction, some of which cause cytotoxic damage, whileothers participate in immune complex formation resulting inimmune inflammation.
Systemic Lupus Erythematosus Systemic Lupus Erythematosus (Lupus)-Background(Lupus)-Background
Clinical features-Clinical manifestations may be constitutional or result frominflammation in various organ systems including skin andmucous membranes, joints, kidney, brain, serous membranes,lung, heart and occasionally gastrointestinal tract.-Organ systems may be involved singly or in any combination.-Involvement of vital organs, particularly the kidneys andcentral nervous system, accounts for significant morbidityand mortality.-Morbidity and mortality result from tissue damage due tothe disease process or its therapy.
Systemic Lupus Erythematosus Systemic Lupus Erythematosus (Lupus)-Background(Lupus)-Background
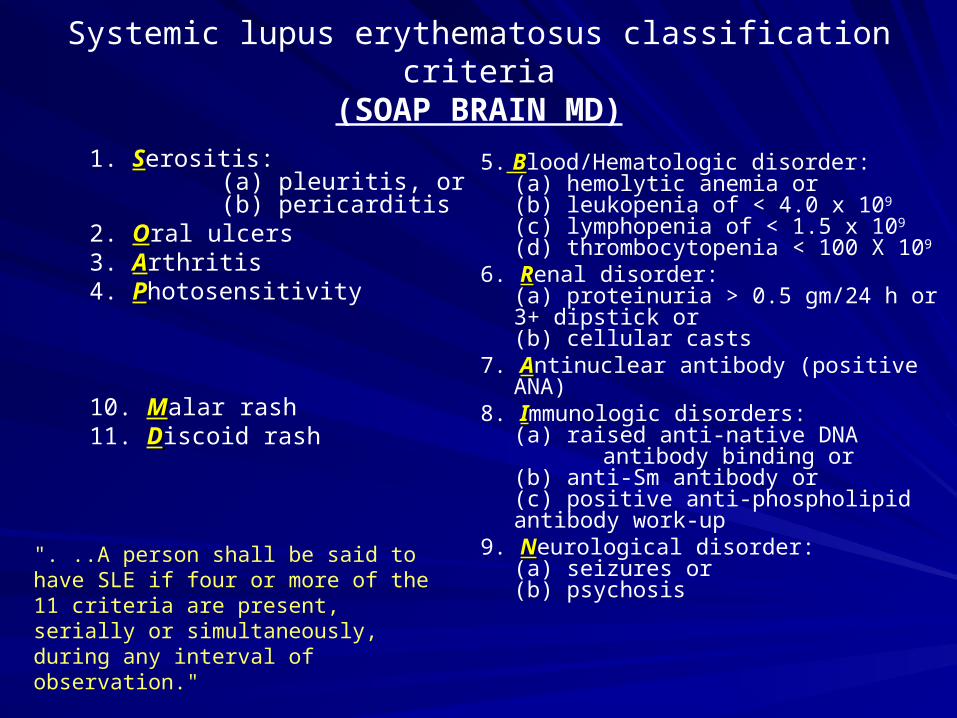
Systemic lupus erythematosus classification criteria(SOAP BRAIN MD)
1. SSerositis: (a) pleuritis, or (b) pericarditis
2. OOral ulcers3. AArthritis4. PPhotosensitivity
10. MMalar rash11. DDiscoid rash
5. B Blood/Hematologic disorder: (a) hemolytic anemia or(b) leukopenia of < 4.0 x 109 (c) lymphopenia of < 1.5 x 109 (d) thrombocytopenia < 100 X
109
6. RRenal disorder: (a) proteinuria > 0.5 gm/24 h
or 3+ dipstick or(b) cellular casts
7. AAntinuclear antibody (positive ANA) 8. IImmunologic disorders:
(a) raised anti-native DNA antibody binding or(b) anti-Sm antibody or (c) positive anti-phospholipid antibody work-up
9. NNeurological disorder: (a) seizures or (b) psychosis
". ..A person shall be said to have SLE if four or more of the 11 criteria are present, serially or simultaneously, during any interval of observation."
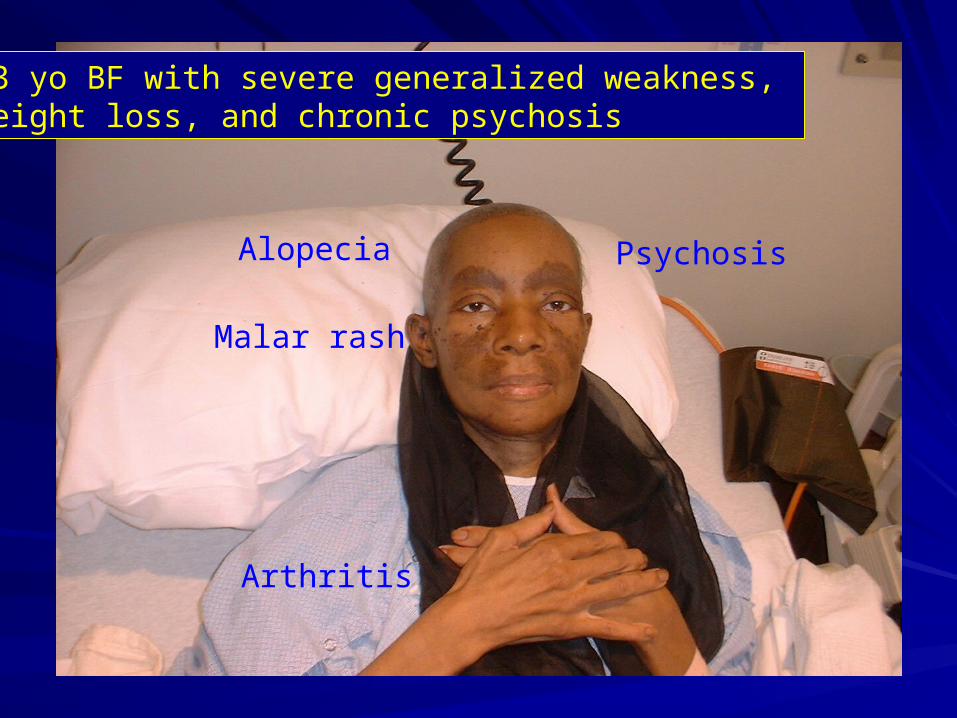
53 yo BF with severe generalized weakness, weight loss, and chronic psychosis
Alopecia
Malar rash
Arthritis
Psychosis
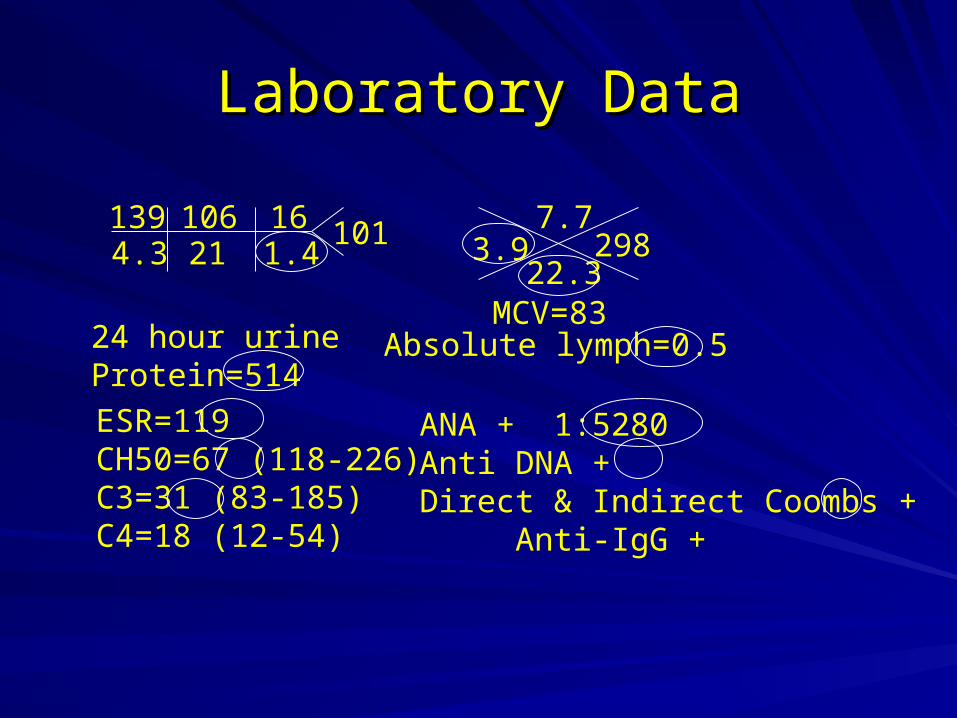
Laboratory DataLaboratory Data
1394.3
10621
161.4
101 7.7
22.33.9
Absolute lymph=0.5
298
MCV=83
ESR=119CH50=67 (118-226)C3=31 (83-185)C4=18 (12-54)
ANA + 1:5280Anti DNA +Direct & Indirect Coombs +
Anti-IgG +
24 hour urineProtein=514
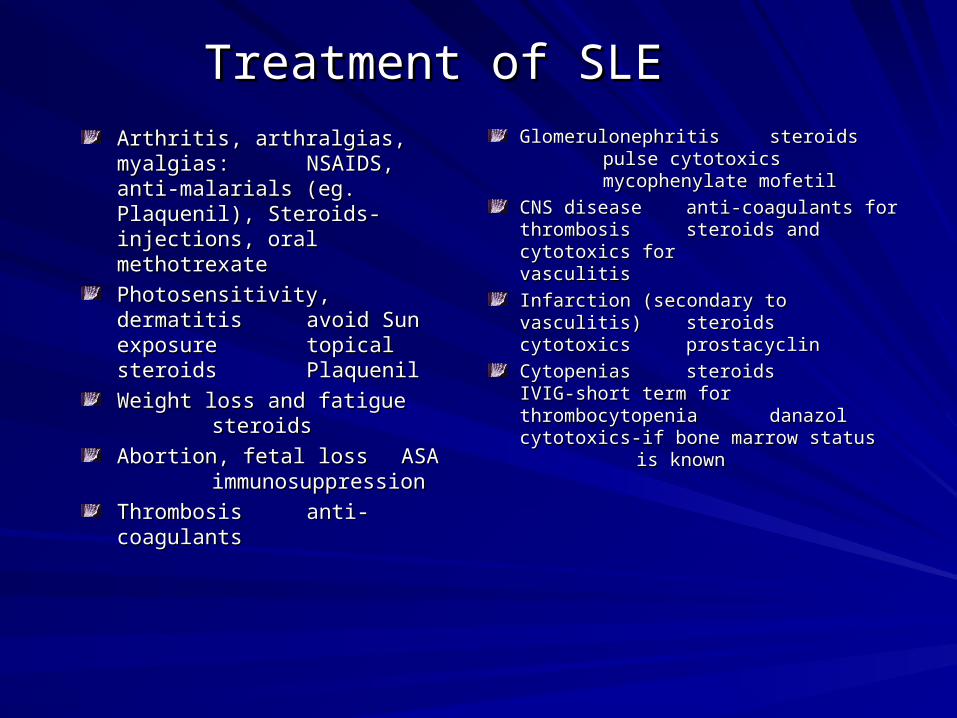
Treatment of SLETreatment of SLE
Arthritis, arthralgias, myalgias:Arthritis, arthralgias, myalgias:NSAIDS, anti-malarials (eg. NSAIDS, anti-malarials (eg. Plaquenil), Steroids-Plaquenil), Steroids-injections, oral methotrexateinjections, oral methotrexate
Photosensitivity, dermatitisPhotosensitivity, dermatitis avoid avoid Sun exposureSun exposuretopical steroidstopical steroidsPlaquenilPlaquenil
Weight loss and fatigueWeight loss and fatiguesteroidssteroids
Abortion, fetal lossAbortion, fetal loss ASAASA
immunosuppressionimmunosuppression
ThrombosisThrombosisanti-coagulantsanti-coagulants
GlomerulonephritisGlomerulonephritis steroidssteroidspulse cytotoxicspulse cytotoxics
mycophenylate mofetilmycophenylate mofetil
CNS diseaseCNS diseaseanti-coagulants for thrombosisanti-coagulants for thrombosis steroids and steroids and cytotoxics for cytotoxics for vasculitis vasculitis
Infarction (secondary to vasculitis)Infarction (secondary to vasculitis)steroidssteroids cytotoxicscytotoxics
prostacyclinprostacyclin
CytopeniasCytopeniassteroidssteroids IVIG-short IVIG-short term for term for thrombocytopeniathrombocytopenia danazoldanazol
cytotoxics-if bone cytotoxics-if bone marrow status marrow status is known is known
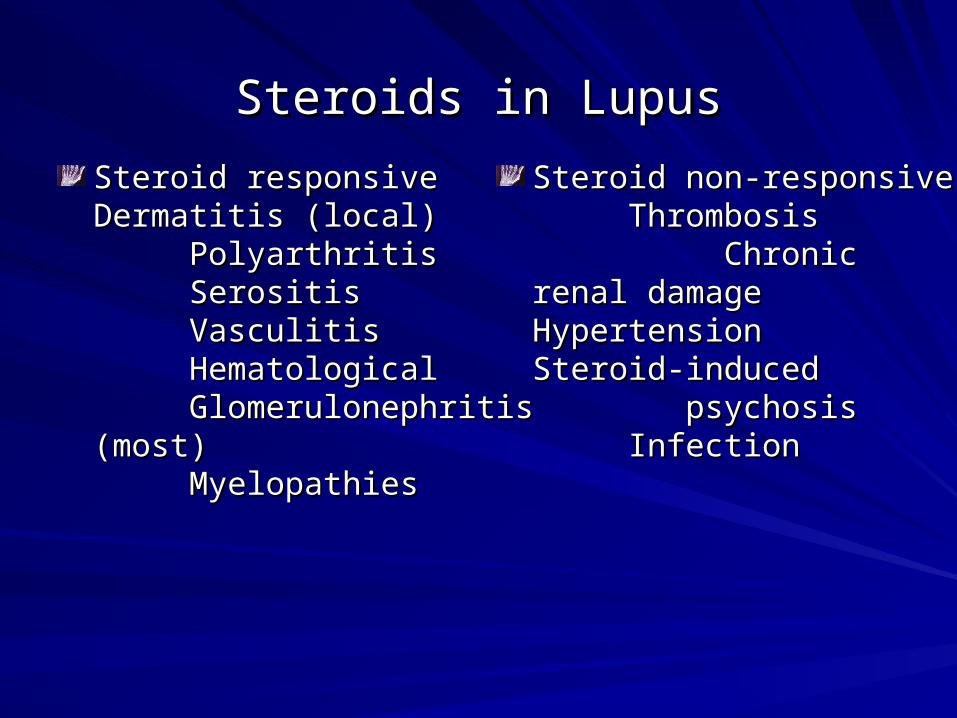
Steroids in LupusSteroids in Lupus
Steroid responsiveSteroid responsive Dermatitis Dermatitis (local)(local)
PolyarthritisPolyarthritisSerositisSerositisVasculitisVasculitisHematological Hematological Glomerulonephritis Glomerulonephritis
(most)(most)MyelopathiesMyelopathies
Steroid non-responsiveSteroid non-responsiveThrombosisThrombosisChronic renal damageChronic renal damageHypertensionHypertension Steroid-Steroid-inducedinduced psychosispsychosis InfectionInfection
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
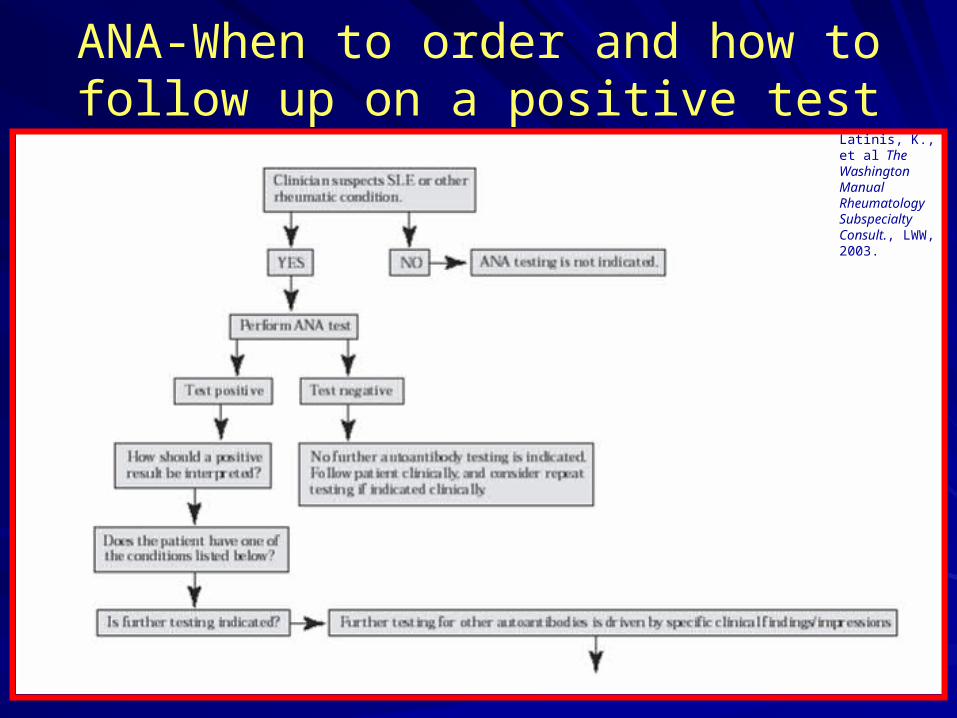
ANA-When to order and how to follow up on a positive test
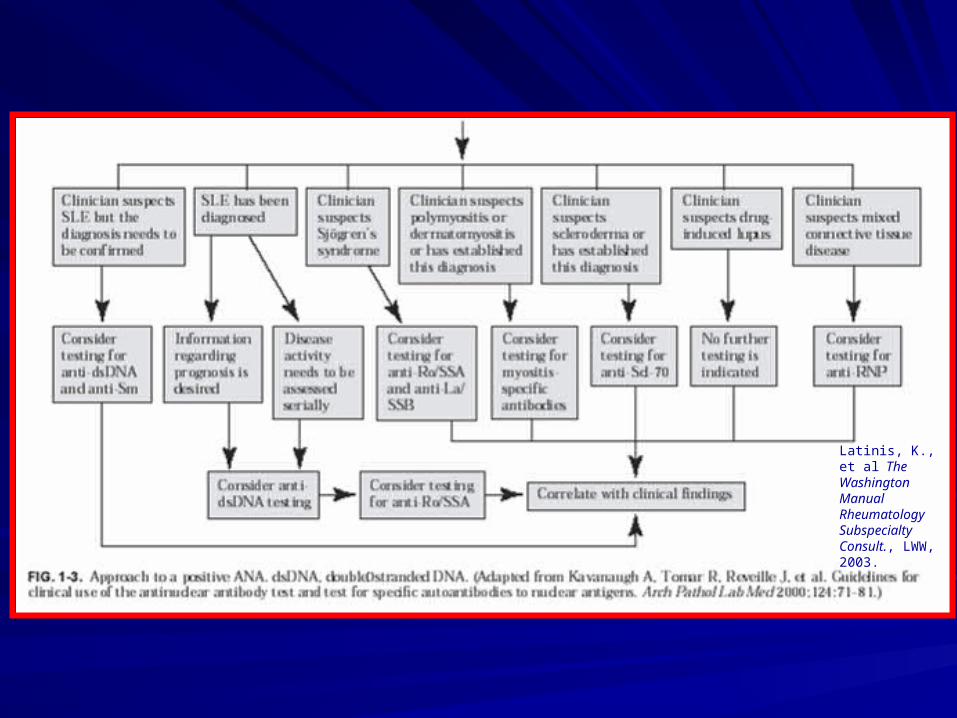
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
Fibromyalgia-BackgroundFibromyalgia-Background
Chronic musculoskeletal pain syndrome of Chronic musculoskeletal pain syndrome of unknown etiologyunknown etiology
Characterized by diffuse pain, tender Characterized by diffuse pain, tender points, fatigue, and sleep disturbancespoints, fatigue, and sleep disturbances
Prevalence is 2-5% with a female to male Prevalence is 2-5% with a female to male predominance of 8:1predominance of 8:1
Mean age is 30-60Mean age is 30-60
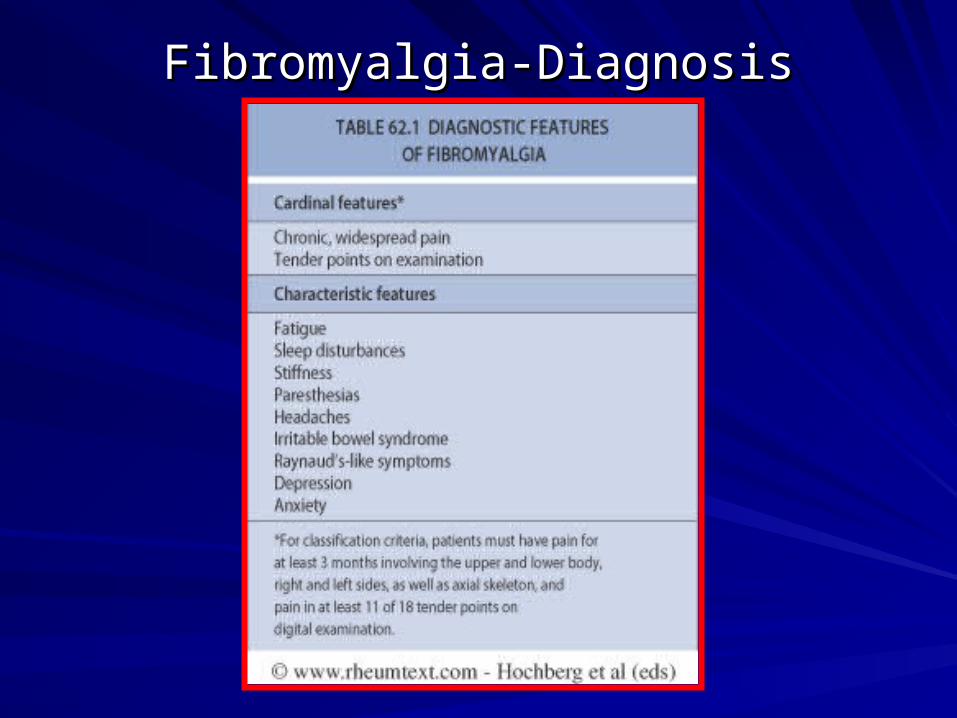
Fibromyalgia-DiagnosisFibromyalgia-Diagnosis
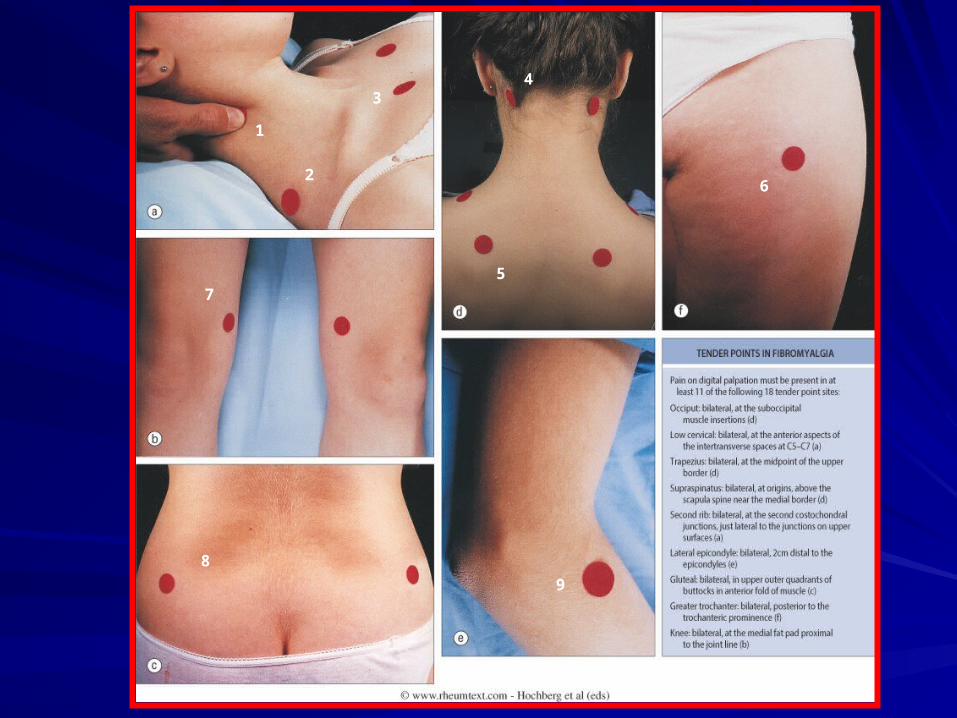
1
2
34
5
6
7
8
9
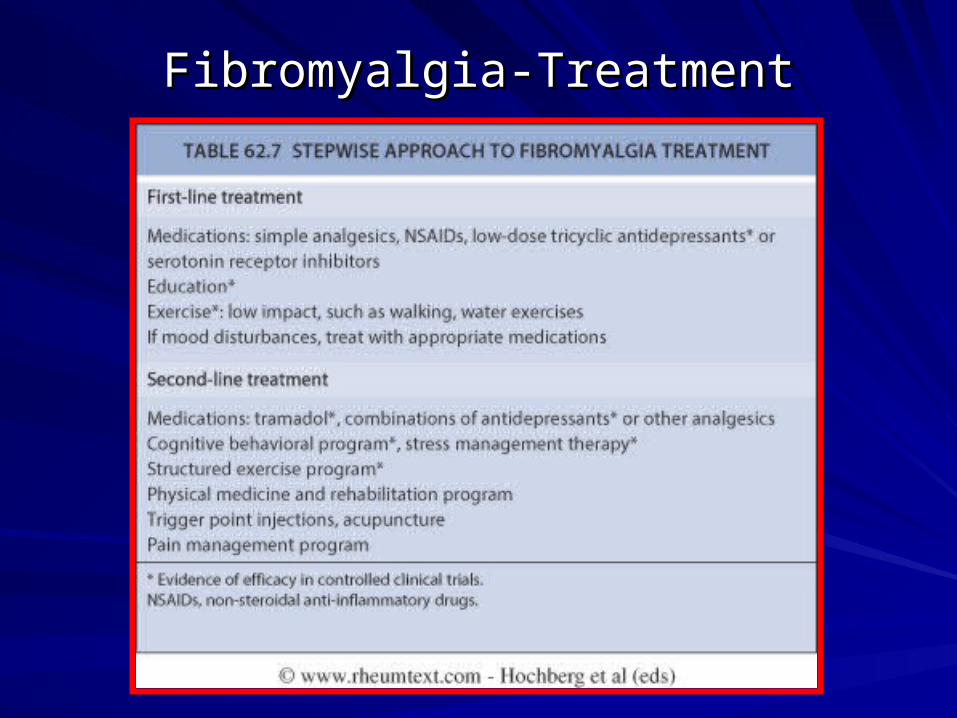
Fibromyalgia-TreatmentFibromyalgia-Treatment
Low back pain and Low back pain and other peri-articular complaints-other peri-articular complaints-
backgroundbackground
Very common, one of the most frequent reasons to visit Very common, one of the most frequent reasons to visit primary care physiciansprimary care physiciansArticular vs peri-articular problemsArticular vs peri-articular problems-Articular pain is generally deep or diffuse and worsens -Articular pain is generally deep or diffuse and worsens with active and passive motion with active and passive motion-Periarticular pain usually exibits point tenderness and -Periarticular pain usually exibits point tenderness and increased tenderness with active, but NOT passive increased tenderness with active, but NOT passive motion motion
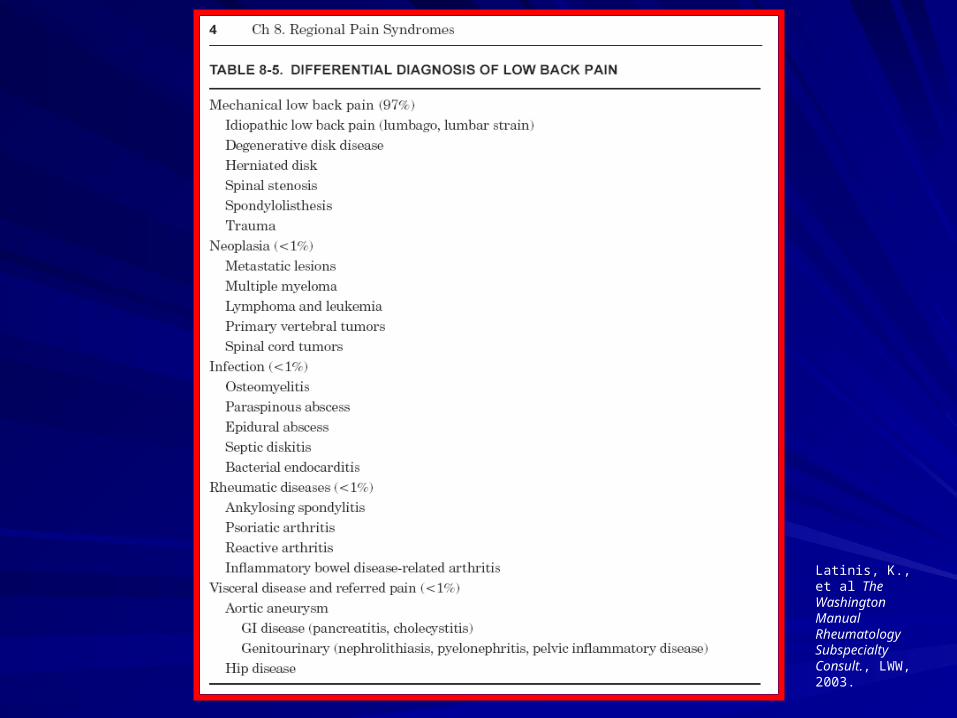
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
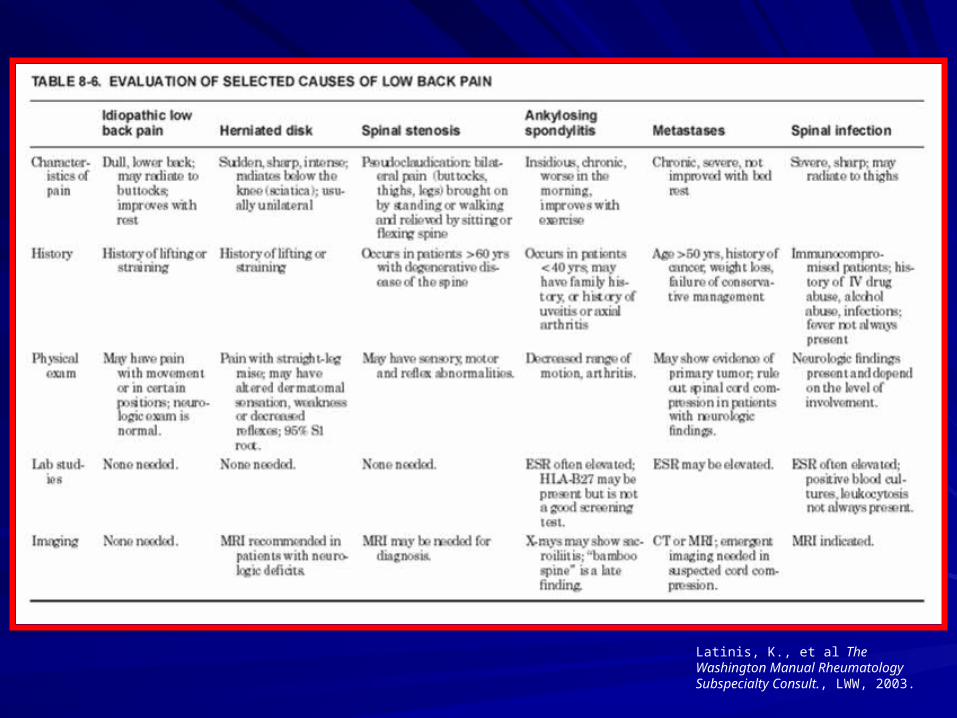
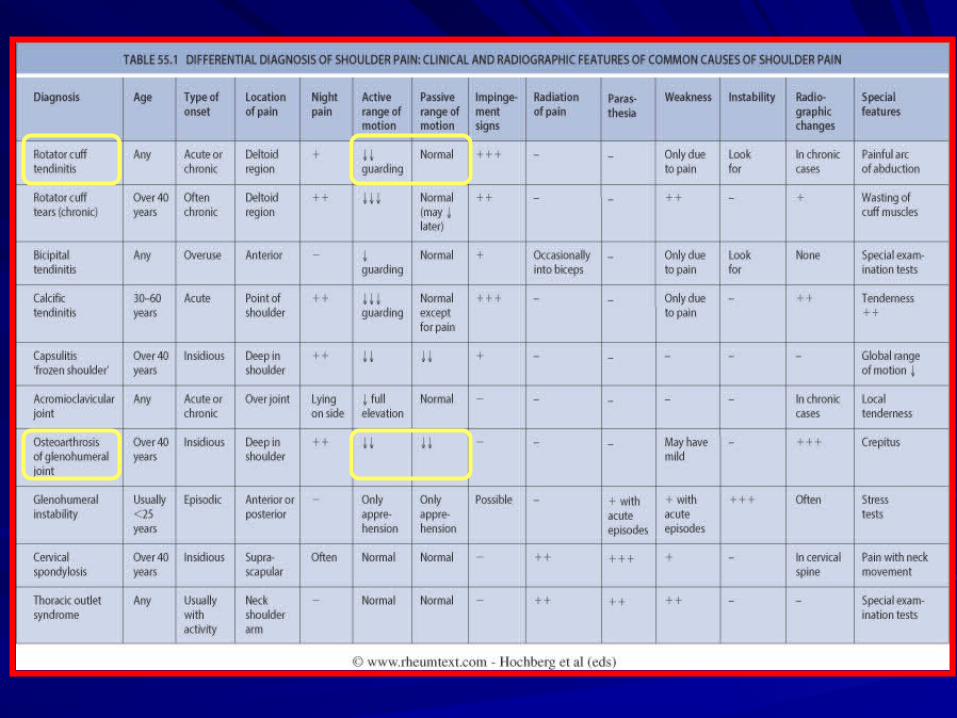
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
Latinis, K., et al The Washington Manual Rheumatology Subspecialty Consult., LWW, 2003.
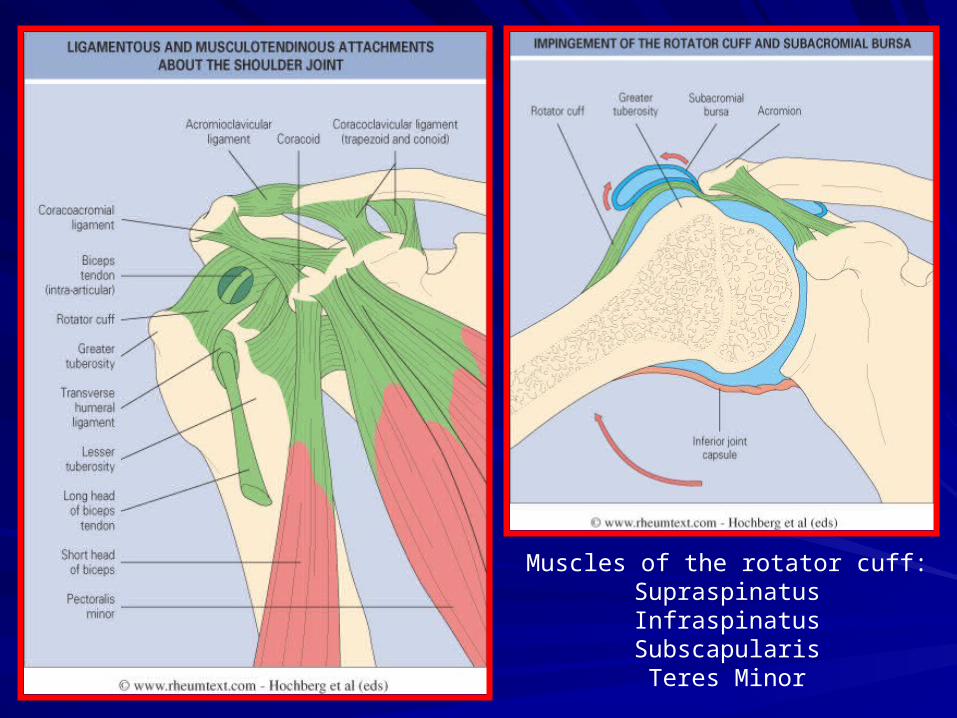
Muscles of the rotator cuff:SupraspinatusInfraspinatusSubscapularisTeres Minor
Low back pain and Low back pain and other peri-articular complaints-other peri-articular complaints-
TreatmentTreatment
RICERICE-Rest-Rest-Ice-Ice-Compression-Compression-Elevation-Elevation
NSAIDs and NSAIDs and analgesics analgesics
TimeTime
OtherOther
General Musculoskeletal ExamGeneral Musculoskeletal Exam
Underutilized by primary care providersUnderutilized by primary care providers
Should be simple and quickShould be simple and quick
Goal is to recognize signs of Goal is to recognize signs of rheumatological diseases and determine if rheumatological diseases and determine if it is appropriate to refer to a it is appropriate to refer to a rheumatologist or manage independentlyrheumatologist or manage independently

SummarySummary
ArthritisArthritis-Inflammatory (RA, spondyloarthropathies)-Inflammatory (RA, spondyloarthropathies)-Mechanical (OA)-Mechanical (OA)LupusLupusFibromyalgiaFibromyalgiaLow back pain and other peri-articular Low back pain and other peri-articular complaintscomplaintsGeneral musculoskeletal exam (time General musculoskeletal exam (time permitting)permitting)





























