Embed Size (px)
Citation preview

Objec&ves
1. Review the importance of QI in thyroid & thyroidcancersurgery
2. Be aware of contemporary complica&on rates forthyroid/thyroidcanceropera<ons
3. AppreciatepostopRAIuptake,Tglevel,andLNyieldasthyroidcancersurgeryQIs
4. Understand the importance of surgeon volume inthyroidsurgery&thyroidcancersurgeryoutcomes

WhatIsHealthcareQuality?
The degree to which health services forindividuals and popula<ons increase thelikelihoodof desiredhealth outcomes and areconsistentwithcurrentprofessionalknowledge.
(Lohr et al N Eng J Med 1990;322;707-712)
Revolu&onaryThyroidSurgicalQualityImprovement:
Kocher’sThyroidectomyTechnique
CurrentthyroidsurgicaltechniquewaspioneeredbyEmilTheodorKocherthatledtoareduc&oninmortalityfrom
12.8%in1883tolessthan0.5%15yearslater
ThyroidectomySurgicalQIs:Complica&ons• Are important thyroid surgical quality
outcomes and thyroid surgeons should beaware of their own complica&on rates andhow they compare to current reportedoutcomes
• ThyroidectomySpecificComplica&ons– RecurrentLaryngealNerveInjury(Scope)– Hypoparathyroidism(Measurement)
• NonspecificSurgicalComplica&ons– Pneumonia– MyocardialInfarc<on– RenalFailure– WoundInfec<on– BloodLoss/TransfusionRequirement– UrinaryTractInfec<on– Postopera<veHemorrhage/ReturntoOR

• Objec<ve:Iden&fyopera&onsneedingmoreQI
• 10 procedures evaluated in ACS NSQIP databasebetween2008-20015(1.2millionopera<ons)
(Liu et al JACS 2018;226;1:30-36)
ThyroidectomyQIs:WhatAreContemporaryComplica&onRates?

ThyroidectomyCurrentComplica&onRates:BenchmarksForThyroidSurgeryQI
(Liu et al JACS 2018;226;1:30-36)

ThyroidectomyForCancerQIs:WhatAreContemporaryComplica&onRates?
• Objec<ve:– Todeterminethyroidcancersurgicalcomplica&onratesandiden&fyatriskpopula&ons
• SEERdatabase(1998-2011)– 22,867pa<ents30dayand1yearcomplica<onratesinDTC(97.2%)&MTC(2.8%)cases
• Complica<onsSeparatedinto:» General(Fever/Infec<on/Hematoma/Pneumonia/
Intuba<on/Trach/MI/PE/DVT)
» ThyroidectomySpecific(Hypoparathyroidism/VCparalysis)(Star<ngat31dayspostop)
(Papaleontiou et al JCEM; 2017;102:2543-2551)

– OverallComplica<onRates:• General(6.5%)• ThyroidectomySpecific(12.3%)
– 1152casesofvocalcordparalysis– 2553casesofhypoparathyroidism
(Papaleontiou et al JCEM; 2017;102:2543-2551)
ThyroidectomyForCancerQI:Complica&ons

• Retrospec<ve review of Na<onwide Inpa<entSample (2003-2009) to evaluate thyroidectomycomplica<ons and the effect of surgeonexperience/volume
• 62,722thyroidectomiesevaluated• 57.9%TotalThyroidectomy/42.1%Lobectomy• 3.3%Graves,60.8%BenignDisease,35.9%Cancer• 0.4%NeckDissec<on
• SurgeonVolumeClassifica&on• Low(<10)-50.2%• Intermediate(10-99)–44.8%• High(>99)–5.0%
(Hauch et al; Ann Surg Onc 2014;21:3844-3852)
ThyroidectomyQIs:WhatIsTheInfluenceofSurgeonVolumeOnComplica&ons?

(Hauch et al; Ann Surg Onc 2014;21:3844-3852)
• Higher complica&on riskacerTotal Thyroidectomy (20.8%) compared toLobectomy(10.8%)(p<0.0001):
• Hypocalcemia(7.1%vs16.1%,p<0.0001)• RespiratoryComplica<ons(0.84%vs1.34%,p<0.0001)• Bleeding(0.15%vs0.23%,p=0.0403)• Hematoma(1.24vs1.54%,p=0.0027)• Tracheostomy(0.004%vs0.024%,p=0.0493)• VocalCordParalysis(0.59vs1.33%,p<0.001)
• Evenhighvolumesurgeonshaveahighercomplica&onriskforTotalThyroidectomycomparedtoLobectomy
• Lowvolume surgeonsweremore likely tohave complica&ons thenhighvolumesurgeons(OR1.53,95%CI1.12,2.11,p=0.0083)– TrueforbothLobectomyandTotalThyroidectomy
EvenHighVolumeSurgeonsHaveComplica&ons
ThyroidectomyQIs:InfluenceofSurgeonVolumeOnComplica&ons

TotalThyroidectomySurgicalQIs:Complica&ons&InfluenceofSurgeonVolume
• Retrospec<ve reviewofNa<onwide Inpa<entSample (1998-2009) to evaluate totalthyroidectomycomplica<onsandtheeffectofsurgeonexperience/volume
• 16,954TotalThyroidectomiesevaluated• 47%ThyroidCancer,53%BenignDisease• Medianannualsurgeonvolumewas7cases• 51%ofsurgeonsperformed1case/year
(Abdelgadir et al; Ann Surg 2017;265:402-407)

TotalThyroidectomySurgicalQIs:InfluenceofSurgeonVolumeOnComplica&ons
• Likelihood of experiencing a complica<ondecreased with increasing surgeon volume up to26cases/year(p<0.01)
• Pa<ents undergoing thyroidectomy by lowcomparedtohighvolumesurgeonswere:
• Morelikelytoexperiencecomplica&ons(OR1.51,p=0.002)• Havelongerhospitaladmissions(+12%,P=0.006)
(Abdelgadir et al; Ann Surg 2017;265:402-407)

WhatisQualityCancerCare?
“Theprovisionofevidence-based,pa<ent-centeredservices throughout the con<nuum of care in a&mely and technically competent manner, withgood communica<on, shared decisionmaking, andcultural sensi<vity, with the aim of improvingclinical outcomes, including pa&ent survival andhealth-relatedqualityoflife”
(NIHPublica<onNo.03e4373.Bethesda:U.S.DepartmentofHealthandHumanServices,Na<onalIns<tutesofHealth;2002)

QualityImprovementForCancerPa&entsIsChallenging
• Ongoingandcon<nuousmodifica&onofcancertreatmentplan
• Mul&disciplinarytreatmentparadigm
• Lengthy&meintervalsforoutcomes
(Albert et et al; I J Rad Onc 2012;83:773-780)

WhatAreCancerCareQualityIndicators?
• Diseasespecific,reliable,scien<ficallyvalidated/evidence or consensus based measures thatreflect quality of care and can be u&lized toguidecancerpa&ent&caregiver:
Ø AssessmentØ BenchmarkingØ Accredita&onØ Creden&alingØ ReimbursementØ QualityImprovement
(Albert et et al; I J Rad Onc 2012;83:773-780)

• Diversityinpathophysiology/prognos<cators/treatmentsfordifferentcancertypesandsoQIsmustbetailoredtothecancertype
• QIdevelopmenthasfocusedoncancertypes:» HighMortality/RecurrenceRisk» HighRiskOpera&ons» MostCommonOpera&ons
SurgicalQualityIndicatorsInCancerPa&ents

ThyroidCancerSurgicalQI:Challenges• ThyroidCancertendsto:
– Haveanexcellentprognosis• Mortalityisuncommon
» PoorQIOutcomeMeasure
– Mayrecuroverdecades• Recurrencemaybehardtotrack
» QIOutcomeMeasureofinterest
– Mostconsidered‘lowrisk’• MayNOTrequire:
» TotalThyroidectomy» CentralNeckNeckDissec<on» RAItreatment
(Mazzaferri at al. Journal Clin Endocin and Metab 2001)
• Goal of the surgeon when performing athyroidectomyforcancer is tosafely removeallthyroid cancer/&ssue (including primary tumorand nodal disease) on the side that is beingoperatedupon
• Thyroid cancer surgical QIs are based oncompleteness of thyroid/thyroid cancerresec&on
• None of these oncological QIs are consideredstandardofcarecurrently
ThyroidCancerSurgicalQIs

NotAllThyroidectomiesAreTotal• Theremnantofthyroid<ssuethatisinten&onally lec by the surgeon inthe thyroid bed in order to reducethe risk of RLN and Parathyroidinjury is influenced by mul<plefactors:
Ø SurgicalIndica&onØ ClinicalSelngØ SurgicalAnatomyØ Surgeon
– Training– Comfort– Experience– Judgment
• Near-totalthyroidectomy(<1g)

TheRealityRegardingThyroidRemnants
• Incomplete thyroid/cancer resec&on predicts aworse outcome (reduced survival and increasedrecurrencerisk)
• LargerthyroidremnantsmaynotadequatelybeablatedbypostopRAI– S<mulated WBS (5 mCi iodine-131) 6-12 monthspostoppredictedsuccessofremnantabla<onby100mCiiodine-131
(Hayetal.Surgery1998)(Rosario et al Clin Nuc Med;2004;6;358-361)
MACISSCORE

ProposedThyroidCancerSurgicalQIs
1. RemnantThyroidUptakeofRAI
2. Postopera&veThyroglobulinLevel
3. Metasta&cLymphNodeRa&o
RemnantThyroidRAIUptake• Post-radioac<veiodineabla<ontreatmentawholebodyscan iscarriedout3-7dayslater to evaluate for remnant thyroid&ssue&thepresenceofregional/distantmetastases
• Remnant thyroid radioiodine uptake(RTRU) is calculated as a % of the totalradioisotopegiventhatisdetectedinthethyroidbedaceradjus&ngfordecay

RemnantThyroidRAIUptake• RTRU correlateswith volume of residual thyroid&ssuepresentwhenevaluatedbyneckUS
– 66 thyroidectomy pa<ents (benign) had remnantvolumeanduptakeevaluatedbyUS,TSH,andRAIscan1monthpostop
(Erbil et al JLO;2008;122;615-622)

• Retrospec<vereviewofcasesundergoingTTandpostopRAIforthyroidcancertreatment
• Remnant uptake analyzed as ra<o of the % uptake ofdose received (UDR) andevaluated for associa<onwithrecurrence
• 21/223pa<entsrecurred(FU25mo)
• Pa&entswithrecurrencehada10xhigherUDRthenthosethatdidn’trecur• ThehigherUDR,thehighertherecurrencerisk
RemnantThyroidTissueRAIUptake
(Schneider et al Thyroid;2013;23;1269-76)

IsThereAnInfluenceOfSurgeonVolumeOnRTRU?• Surgeonsclassifiedashigh(3)orlow(5)volume(definedby20thyroidopera<ons/year)
• UDRs of high volume surgeonswere significantly lower thenlowvolumesurgeons
• Overall33complica&ons(24temporary/9permanent)
• High volume surgeons had significantly lower permanentcomplica&ons,evenathighUDR
• Lowvolumesurgeons,hadastepwiseincreaseincomplica<onsasUDRrises
UDR
COMPLICAT
IONS
(Schneider et al Thyroid;2013;23;1269-76)
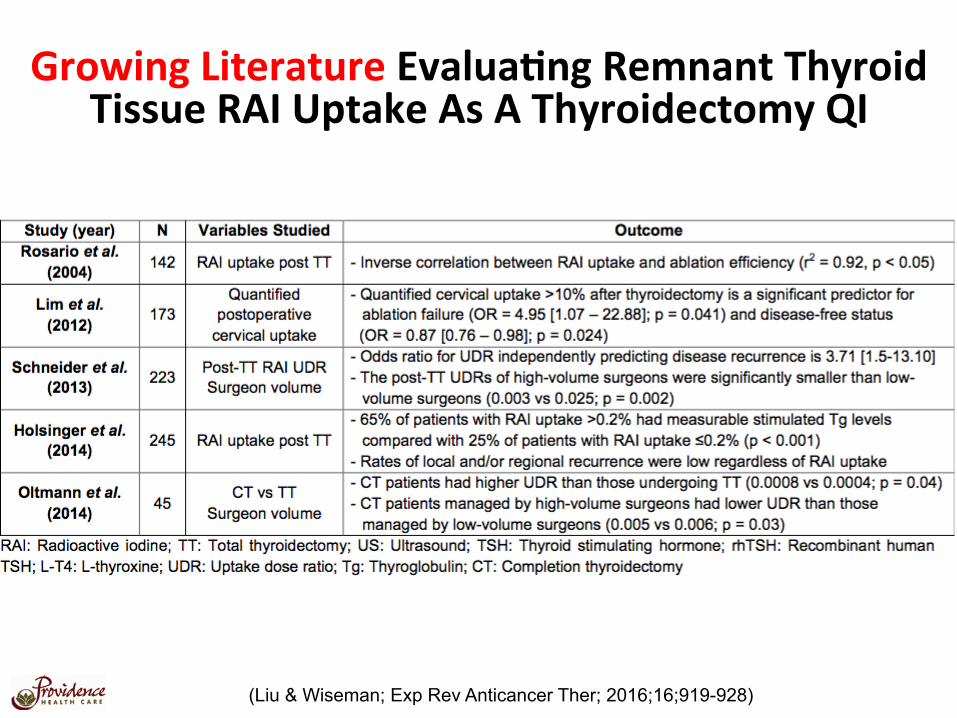
GrowingLiteratureEvalua&ngRemnantThyroidTissueRAIUptakeAsAThyroidectomyQI
(Liu & Wiseman; Exp Rev Anticancer Ther; 2016;16;919-928)
RemnantThyroidRAIUptakeAsAQI• RTRUmayserveasaQIforthyroidcancersurgerybecauseitcorrelateswith
‘completenessofthyroidectomy’andrecurrencerisk
• Thoughts&Limita<ons– Cannotbeu&lizedinlobectomy(LowRisk)pa&ents– U&litylimitedinRAInon-avidrecurrence– Notappropriateforlocallyadvanced/completelyresectablecases– Notaccurateinthepresenceofsignificantmetasta&cdisease– Influenceofotherconcurrentthyroiddisease(ie.Graves)– Whatisan“acceptable”RTRU?– ShouldRTRUinfluencepostopera<vesurveillanceandfollowup?– IsthereaRTRUthatmandatesreopera<onorrepeatRAItreatment?
Doyouknowyourpa&ent’sRTRU?
Postopera&veThyroglobulinLevel• Tg isaglycoprotein,aprohormone,onlysynthesizedby thyrocytes stored in colloid, that’s produc<on iss<mulatedbyTSH
• S<mulatedanduns<mulatedTgmeasurementisusedforpostopsurveillanceofallthyroidcancerpa<ents
• Tg measu rement ace r To ta lThyroidectomy correlates withvolumeof remnant thyroid&ssue&/or cancerandmay serve as a thyroidcancersurgicalQI

Postopera&veThyroglobulinLevel
(ATA Guidelines 2015)
Nomen&onofearlypostopera&veserumTgmeasurement

• Retrospec<ve review of all thyroid opera<ons(DTC≥1cm) during 2011 in a regional healthsystem(UPit)
• 42surgeons/volumeevaluatedfor:– Extentofini&alopera&on– %uptakeonI123pre-RAITSHs&mulateduptakescan– Pre-abla&onTSH-s&mulatedTglevel– DoseofI131administered
(Adkisson et al; Surgery; 2014;156;1453-60)
IsThereAnInfluenceOfSurgeonVolumeOnPostopera&veThyroglobulinLevel?

HigherSurgeonVolume>30ThyroidORs/Year
– TotalThyroidectomy– More‘complete’
%uptakeonI123S&mulatedTgAdministeredI131dose
– Fewercomplica&ons>50ThyroidORs/YearForStage3&4Disease
– More‘complete’%uptakeonI123
SurgeonVolume&ThyroidCancerSurgicalQIs
(Adkisson et al; Surgery; 2014;156;1453-60)

GrowingLiteratureEvalua&ngPostopera&veThyroglobulinLevelAsAQI
(Liu & Wiseman; Exp Rev Anticancer Ther; 2016;16;919-928)
• PostopTgmayserveasaQIforthyroidcancersurgerybecauseitcorrelateswith‘completenessofthyroidectomy’andrecurrencerisk
• Thoughts&Limita<ons– U&lityinlobectomy(LowRisk)pa&entsunknown– Notusefulfortumorsthatdon’tsynthesizeTg– Notappropriateinlocallyadvanced/notcompletelyresectablecancers– Notaccurateinthepresenceofbulkymetasta&cdisease– Influenceofotherconcurrentthyroiddisease(ie.Hashimoto’s)?– Whatistheop<mal<mingofTgmeasurementrela<vetosurgeryandRAI?– Whatisanacceptablepostopera<veTglevel?– ShouldTginfluencepostopera<vesurveillanceandfollowup?– IsthereaTglevelthatmandatesreopera<onorrepeatRAItreatment?
Doyouknowyourpa&ent’spostopera&veTglevel?
Postopera&veThyroglobulinLevelAsAQI

Central Neck Dissection For Thyroid Cancer • Varia&on in surgical prac&ce regarding
CNDforthyroidcancertreatment
• Centralnecklymphnodemetastasescanbedetectedin20-50%ofcases
• Lymph node metastases increase risk ofcancerrecurrence
• TheAHNSdefinesacentralneckdissec<onacomprehensiveremovalof:
NECKNODELEVELVI• Prelaryngeal(Delphian)LymphNodes• PretrachealLymphNodeand• Lev +/or Right Paratracheal Lymph
Nodes+/-
NECKNODELEVELVII(Agrawal et al; Head Neck;2017;39;1269-1279)

CentralNeckDissec&on:ATAGuidelines
Therapeu&cCNDProphylac&cCNDNoCND
(ATA Guidelines 2015)

What Is Metastatic Lymph Node Ratio? • ProposedasaQIforthyroidcancersurgery
• Reflectsthesuccessofthesurgeonincentralneckcompartmentlymphadenectomy
#Metasta&cLymphNodesTotal#ofLymphNodes(LymphNodeYield)

• Evalua<onofMLNRin10,955DTCpa<entswith>3LNremovedintheSEERdatabase(1988-2007)(medianfollowup25months)
• MLNRwasstronglyassociatedwithDSM(HR4.33,95%CI1.68-11.18,p<0.01)
• MLNR≥0.42separatedcasesbasedondiseasespecificmortality
Metastatic Lymph Node Ratio
1.72%
0.65%
(Schneider et al; Ann Sug Onc;2013;20;1906-1911)

GrowingLiteratureEvalua&ngMetasta&cLymphNodeRa&oAsAQI
(Liu & Wiseman; Exp Rev Anticancer Ther; 2016;16;919-928)

• MLNRmay serve as a QI for thyroid cancer surgery because it correlateswith‘completenessoflymphadenectomy’andrecurrencerisk
• Thoughts&Limita<ons– U<lityinthesexngofbulkydiseaseispoor(cannotachievealowra<o)– Surgicalinten<on:Therapeu<cvsProphylac<cmustbeconsidered– Impactofnodalmetastasessize/extranodalextensionunknown– Influenceofotherconcurrentthyroiddisease(ie.Hashimoto’s)– Whatisan“acceptable”MLNR?– ShouldMLNRinfluencepostopera<vesurveillanceandfollowup?
Doyouknowyourpa&ent’sMLNR?
Metasta&cLymphNodeRa&oAsAQI

• Could address difficulty withfindingthyroidcancersurgeryQIsforLowRiskpa<ents
• Guidelines are Guidelines andconstantly changing based uponnewevidence
• Should not following guidelinesbe an i nd i ca to r o f pooroncologicalsurgicalquality?
FinalThoughts:ShouldGuidelineAdherenceBeConsidered
AThyroidSurgicalQI?
FinalThoughts:HowManyHighVolumeSurgeonsWouldItTakeToPerformAllThe
ThyroidectomiesInTheUSAAnnually?Realis&c?
Es<mate:Total#ThyroidectomiesInUS/Year=150,000
HighVolumeSurgeon>99Thyroidectomies/YearTotal#HighVolumeThyroidSurgeonsNeeded=1,500
HighVolumeSurgeon>24Thyroidectomies/Year
Total#HighVolumeThyroidSurgeonsNeeded=6,000
(Hauch et al; Ann Surg Onc 2014;21:3844-3852) (Al-Qurayashi et al; JAMA Oto HNS 2016;142:32-39)

Conclusions• ThyroidsurgicalQIsarefocusedonsurgicalcomplica&ons
• Thyroid cancer surgical QIs allow for evalua<on of thecompletenessof:
• Thyroidectomy– RemnantThyroidUptakeofRAI– Postopera&veThyroglobulinLevel
• CentralNeckLymphadenectomy– Metasta&cLymphNodeRa&o
• Applica<on of these QIs is largely limited to pa<ents whohaveundergoneatotalthyroidectomy+/-RAI
(primarilyHighRisk)

Conclusions
• Despite no specific QI currently considered standard, and furtherstudy being needed, surgeons who perform thyroid opera<onsshouldbeawareoftheir:
Ø Pa<ent’sthyroidsurgicalQIsØ Morbidity&MortalityØ RecurrenceRisk
Ø Pa<ent’sthyroidcancersurgicalQIsØ PostopRAIuptakeØ PostopTGØ MLNRØ Other?
Ø Ownthyroidectomysurgicalvolumes
• This informa<on is readily available, quan&fiable, is associatedwith surgicalandoncological outcomes, andallows forquality improvement (NOWHOWDOWEAPPLYTHESEQIsINTHEREALWORLD???)





























