Embed Size (px)
DESCRIPTION
laporan kasus
Citation preview

CASE REPORT
DIFFUSE OTITIS EXTERNA
Presentator Koas THT periode 20 January-15 February 2014 :
Geetha Balasubramaniyam
Johannes Octan Daniel
Rizky Ajrina Meidiyana
Zahrifa Riandani Putri
Putri Riadhini
Resy
Moderator : dr Akmal
Otorinolaryngology and Head Neck Surgery Departments
Medical Faculty of Gadjah Mada University
DR Sardjito Hospital Yogyakarta
2014

CHAPTER II
INTRODUCTION
Otitis externa is an infection of the external auditory canal. Otitis externa
occurs in 4 of every 1000 people annually, and the chronic form affect 3-5% of
the population. Prompt diagnosis and treatment cures the majority of cases
without complication. Otitis externa is defined as chronic when the duration of the
infection exceeds more than 1 month or when more than 4 episode occur in 1
year.
If left untreated, the infection may invade the deeper adjacent structures
and progress into malignant otitis externa. This complication is almost exclusively
seen in immunocompromised patients such as those with diabetes, AIDS patients,
those undergoing chemotherapy, and patients taking immunosuppressant
medications (eg. Organ transplantation) such as glucocorticoids. Pseudomonas
Aueroginosa is the inciting organism in the vast majority of cases. When
untreated, malignant otitis externa has a mortality rate approaching 50%. This
complication should be suspected if tenderness, otalgia, rythema, or edema of the
external ear or adjacent tissues is present on physical examination.
People in some racial groups have small ear canals, which may predispose
them to obstruction and infection. Rates of occurrence of otitis externa are equal
in males and females. Although otitis externa is seen in all age groups, the peak
incidence is in children aged 7-12 years.
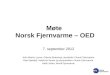
ANATOMY
The external ear is composed of the auricle and external auditory canal.
Both contain elastic cartilage derived from mesoderm and a small amount of
subcutaneous tisssue, covered by skin with its adnexal appendages. There is fat
but not cartilage in the lobule.

1. Auricle
The Auricula or Pinna is of an avoid form, with its langer end directed upward. Its
lateral surface is irregularly concave, directed slightly forward, and presents
numerous eminences and depressions to which names have been assigned.The
prominent rim of the auricula is called the helix; where the helix turns downward
behind, a small tubercle, the auricular tubercle of Darwin, is frequently seen; this
tubercle is very evident about sixth month of fetal life when the whole auricula
has a close resemblance to that of some of the adult monkeys. Another curved
prominence, parallel with and in front of the helix, is called the antihelix; this
divides above into two crura, between which is a triangular depression, fossa
triangularis. The narrow-curved depression between the helix and the antihelix is
called the scapha; the antihelix describes a curve around a deep,capacious cavity,
the concha, which is partially divided into two parts by the crus or commencement
of the helix; the upper part is termed the cymba concha, the lower part the cavum
concha. In front of the concha, and projecting backward over the meatus, is a
small pointed eminence, the tragus,so called from its being generally covered in
its under surface with a turf of hair, resembling a goat’s beard. Opposite the
tragus, and separated from it by intertragic notch, is small tubercle, the antitragus.
Below this is the lobule, composed of tough areolar and adipose tissues, and
wanting the firmness and elasticity of the rest of the auricula.
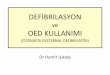
2. External Auditory Canal
The External Acoustic Meatus (muatus acusticus externus; external
auditory canal or meatus) exterds from the bottom of the concha to the tympanic
membrane. It is about 4 cm in length if measured from the tragus ; from the
bottom of the concha its length is about 2,5 cm. It forms an S-shaped curve, and is
directed at first inward and backward (pars media), and lastly is carried, inward,
forward and slightly downward (pars interna). It is oval cylindrical canal, the
greatest diameter being directed downward and backward at the external orifice,
but nearly horizontally at the inner end. It present two constrictions, one near

theinner end of the cartilaginous portion, and another the isthmus, in the osseous
portion, about 2 cm from the botton of the concha. The tympanic membran, which
closes the inner end of the meatus, is obliquely directed; in consequence of this
the floor and anterior wall of the meatus are longer than the roof and posterior
wall.
The external acoustic meatus is formed partly by cartilage and membrane,
and partly by bone and lined by skin.
The Cartilaginous portion ( meatus acustiocus externus cartilageus)
The length is about 8mm in the length. It is continous with the cartilage of
the auricula, and firmly attached to the circuference of the auditory process of the
temporal bone. The cartilage is deficient at the upper and back part of the meatus,
its place being supplied by fibrous membran; two or three deep fissures are
present in the anterior part of the cartilage.
The skin of the cartilaginous canal contains many hair cells and sebaceous and
apocrine glands such as cerumen glands. Together, these three adnexal structures
provide a protective function and are termed the apopilosebaceous unit. Glandular
secretion combine with sloughed squamous epithelium to form an acidic coat of
cerumen, one of the primary barriers to infection of the canal.
The osseous portion (meatus acusticus externus osseus)
The length is about 16 mm and narrower than the cartilaginous portion. It
is directed in ward and a little forward, forming in its course a slight curve the
convexity of which is upward and backward. Its inner and smaller than the outer
and sloped the anterior wall projecting beyond the posterior for about 4 mm. It is
mark, except at its upper part, by a narrow groove, the tympanic sulcus in which
the circumference of the tympanic membrane is attached. Its outer end is dilated
and rough in the greater part of its circumference, for the attachment of the
cartilage of the auricula. The front and lower parts of the osseous portion are

formed by a curved plate of bone, the tympanic part of the temporal, which in the
fetus, exists as a separate ring (annulus tympanicus), incomplete at its upper part.
4. Vascularitation
The arteries of the auricula are the posterior auricular from the external
carotid, the anterior auricular from the superficial temporl, and a branch from the
occipital artery. The arteries supplying the meatus are branches from the posterior
auricular, internal maxillary, and temporal. The veins accompany the
corresponding arteries.
5. Innervation
The sensory nerve of the auricle are the great auricular, from the cervical
plexus the auricular branch of the vagus ; the auriculotemporal branch of the
mandibular nerve ; and the lesser occipital from the cervical plexus. The nerves of
meatus are chiefly derived from auriculotemporal branch of the mandibular nerve
and the auricular branch of the vagus.
6. Lympatic
Lympatic drainage of external ear consist of
Lnn Parotis superfisial
Receive drainage from tragus and anterior auricula
Lnn Retroauricular
Receive lymph drainage from posterior and cranial auricula
Lnn Cervical Superfisialis
Receive lymph drainge from lobulus

DIFFUSE OTITIS EXTERNA
1. Definition
Diffuse otitis externa is inflammation of the external ear canal, with or
without involment of the pinna or tympanic membrane. Diffuse otitis externa is
the most common form of otitis externa.
2. Etiology
The most common offending organisms that cause otitis externa are
Pseudomonas aeruginosa (50%), Stapylococcus aureus (23%), anaerobes and
gram-negative organisms (12,5%)
3. Risk Factor
The risk factor of diffuse otitis externa are swimming, swimming in water
where bacterial level are high, people with allergic condition, people who has
small ear canal because water can be trapped more easily, over cleaning the ear
canal, too much ear wax, making it more likely that water gets trapped.
Predisotition factors :
Moisture (swimming, perspiration, high warmth CAE
High ambient temperature
Contamination by water contaminated with bacteria
Habits take cerumen, cerumen impaction
The entry of foreign materials (cotton swab, fingernail, toys, insect, ear plugs)

Traumatic ear canal
Chronic skin diseases (eczema, psoriasis, seborrheic dermatitis, acne)
Diabetes mellitus
Immunocompromised state
Exostosis at CAE
4. Pathogenesis
Excessive cleansing and water exposure will remove the protective layer
and acid mantle from the canal, so the stratum corneum become edematous
resulting in plugging of the apopilosebaceous unit. As obstruction continues, a
sense of fullness and itching begins. The disruption of the epithelial layer due to
scratching allows invasion of bacteria that either reside in the canal or are
introduced on foreign objects inserted into the canal, such as a cotton swab or a
dirty fingernails
5. Sign and symptoms
Pain, fullness, itching, and hearing loss are the four major symptoms of
external otitis, although not every patient has each symptom. Throughout the
examination, the examiner should remember the innervation of auditory external
canal and recall that pain from other areas of the upper aerodigestive tract may be
referred to the ear.
Typically, the preinflammatoory stage begins when the stratum corneum
becomes edematous because of removal of the protective lipid layer and acid
mantle from the canal, resulting in lugging of the apopilosebaceous unit. As
obstruction continues, a sense of fullness and itching begins.

The disruption of the epithelial layer allows invasion of bacteria that either
reside introduced on foreign objects inserted into the canal, such as a cotton swab
or a dirty fingernails,. This produces the acute inflammatory stage, which is
accompanied by pain and tenderness of the auricle. In the earliest stage, the skin
of the external auditory canal shows mild erythema and minimal edema. A small
amount of clear or slightly cloudy secretion may be seen in the canal.
As pain and itching increase, the patient progresses to the moderate stage
in which the canal shows more edema and a thicker more profuse exudates.
Further progression of the inflammation in the absence of treatment the severe
inflammatory stage characterized by increased pain and obliteration of the lumen
of the canal. A profuse, purulent exudate and edema of the canal skin may obscure
the tympanic membrane. In addition, small white papules are often visible on the
surface of the canal skin. P. aeruginosa or another gram-negative bacillus can
almost always be cultured at this stage.
In the severe stage, the physician often sees evidence of extension of
infection beyond the canal to involve the adjacent soft tissue and cervical lymph
nodes. In the chronic inflammatory stage, patient experience less pain but more
profound itching. The skin of the external canal is thickened, and superficial
ulceration. This condition is likened to eczema and may range from mild drying
and thickening of the canal to complete obliteration of the external canal by
chronically infected hypertropic skin.
6. Diagnosis
Diagnosis of diffuse otitis externa is made based on the history and
physical examination. History of pain. Fullness, itching, and discharge is the
common symptom of diffuse otitis externa. From physical examination, we may
find various condition depends on its stage. In preinflammatory stage we will find
mild erythema and tenderness. In acute inflammatory, there are auricular
tenderness, erythema, edema, and discharge. And in chronic inflammatory stage,
we will find thickening or flaking of canal skin, eczematization, ulceration.

7. Management
The four fundamental principles in the treatment of external otitis in all
stages are frequent and thorough cleaning, judicious use of appropriate antibiotics,
treatment of associated inflammation and pain, and recommendation regarding the
prevention of future infection. In any stage of infection, thorough cleaning is a
priority. Meticulous debridement of exfoliated debris, purulence, and cerumen
will do as much if not more than simply placing the patient on ear drops. In the
preinflammatory stage, a complete cleaning may be all that is required. In the
absence of purulence, a brief course of an acidifying drop such as aluminum
sulfate or calcium sulfate (Domeboro) is efficacious in discouraging bacterial or
fungal growth.
Treatment of the acute inflammatory stage varies with the extent of
disease. In mildest form, cleaning as described previously is indicated. An
antibiotic drop is recommended to cover what is probably a Pseudomonas
infection. There is an emerging body of evidence that the fluoroquinolone
preparations with or without steroids (ciprofloxacin, ofloxacin, dexamethasone,
hydrocortisone (Cipro HC, Ciprodex, Floxin)) may have advantages over the
neomycin/polymyxin.hydrocortisone preparation (Cortisporin or Coly-Mycin S
Otic). At this time, no significant antibiotic resistance has been shown to emerge
due to the use of the fluoroquinolone ototopic medications. At this stage, edema
of the external auditory canal should not be severe, and the patient should be able
to instill drops into the ear by tilting the head to the side or by lying down with he
involved ear upright.
In the moderate stage of inflammation, edema of the canal may interfere
with the instillation of drops. The physician should then insert a wick into the
canal and instill drops on it. Often the canal may accommodate two or even three
wicks. As the wicks expands, it presses the soft tissues and periosteum toward the
nondistended position; this alone may relieve pain. All instrumentation of the ear
is best done under the microscope. The wick is removed by the physician at the

times of reexamination. If the edema has not significantly reduced, repacking is
indicated. Antibiotic drops should be continued for at least 2 to 3 days after the
cesation of pain, itching, and drainage, so that complete eradication of infection
may be ensured.
In the moderate stage, an oral analgesic is often prescribed because pain
can be pronounced. Caution the patient to avoid manipulation of the canal. Teach
swimmers to towel dry the concha and lateral canal, to shake water out of the
canal, or to instill an acidifying drop after swimming. If the infection has not
spread beyond the boundaries of the external canal, the use of oral antibiotics will
be of little if any value. A final office visit is important to ensure that the infection
has completely resolved and the canal is back to its normal state.
In the severe stage, infection usually extends beyond the limit of the canal.
In addition to the cleaning, packing, and use of antibiotic drops as discussed
previously, attend to any soft tissue involvement by using an oral antibiotic with
broad spectrum coverage. Successive generations of the cephalosporins widen
gram negative coverage at the expense of gram positive coverage. In addition to
anti Pseudomonas eardrops, common choices of oral antibiotics are
antistaphylococcal penicillins, first-generation cephalosporins, or one of the
antipseudomonal fluoroquinolones such as ciprofloxacin or levofloxacin. The
fluoroquinolone antibiotics are effective against Pseudomonas species but at
present are not approved for use in patients under age 18 because of the risk of
arthropathy formation. Multiple reports over the last 10 years have indicated the
safe use of ciprofloxacin in the pediatric patient with little if any increased
development of arthropathy over adults. The fluoroquinolones remain contra-
indicate, however, except in extraordinary circumstances, such as in the treatment
of respiratory disease in children with cystic fibrosis. Warm soaks (normal saline
or diluted aluminum sulfate calcium sulfate solution) are also useful in the
treatment of the crusting and edema involving the auricle and surrounding skin.
Culture of the canal is indicated only for severe stage or for patients who have
previously been treated without resolution. Treatment is generally continued for

10 to 14 days if there is a good response. In rare patients who do not respond to
this regime, hospitalization, vigorous daily local care, repeat culturing, and
intravenous antibiotics are indicated.
In chronic phase, treatment aims at reduction of meatal swelling so that ear
toilet can be effectively done, and alleviation of itching so that scratching is
stopped and further recurrences controlled . A gauze wick soaked in 10%
ichthammol glycerine and inserted into the canal helps to reduce .swelling. This is
followed by ear toilet with particular attention to anteroinferior meatal recess.
Itching can be controlled by topical application of antibiotic steroid cream. When
the meatal skin is thickened to the point of obstruction and resists all forms of
medical treatment, i.e. chronic stenotic otitis externa, it is surgically excised, bony
meatus is widened with a drill and lined by split-skin graft.
In all cases of acute or chronic external otitis, instruct the patient to avoid
future infections by not placing any objects or instrument into the canal. These
often excoriate the canal skin and push debris further into the canal rather than
remove it. Patients who have repeated infections despite adhering to these
measures are best advised to use an acidifying drop composed of equal measures
of vinegar and water, or ethyl alcohol and water, when exposed to high humidity.
Alternatively, an acidifying power such as boric acid may be used. Custom-made
ear molds are useful for these patients.

CHAPTER III
CASE REPORT
A. Identity
• Name : Mrs. J
• Age : 30 years old
• Gender : Female
• Religion : Moslem
• Adress : Mandungan RT 2/RW 5, Manis Renggo
• Date of visit : Januari 28th 2014
• Med.Record : 664555
B. Anamnesis
Chief complaint : Continous pain in the right ear
History of Present Illness:
• 3 days before patient came to the polyclinic, patient complaint about
continuous pain in the right ear although there was no contact to the ear. The pain
felt was accompanied with a heat sensation that affected the patient’s daily
activities. The patient felt that the complaint worsen day by day.The patient also
felt a sensation of aural fullness in the right ear which decrease her hearing ability.
No blood was present but the patient did admit that there was a little bit of serous

discharge seen on the cotton bud that she used to clean her ear. The patient had no
complaint regarding her left ear. The patient has a history of routinely using
cotton bud ( every 3 days once). Patient denied the entrance of water or any other
foreign objects into the ear. There was no tinnitus, dizziness and fever present.
The patient had no complaints regarding nose, mouth and throat.
History of Past Illness
• Previous history regarding her right ear in which she went to the ENT
polyclinic on the 13th February 2013 with complaint of yellow discharge present
in the right ear and was diagnosed as Chronic Suppurative Otitis Media.
Medication given was Tarivid ear drops 2x4, Aldesa 2x1 and Ambroxol 3x1. The
patient failed to show up for her follow up session.
• History of allergy denied
• History of flu (-)
• History of hypertension (-)
• History of DM (-)
• History of admitted to the hospital (-)
• History of smoking (-)
History of Illness in Family Members
• History of the same complaints (-)
History of medication : Patient has never bought any ear drop medication
unprescribed
Nutritional status : Good, eats 3x a day, home cooked meals
Psychological status : Good

Socioeconomic status : Well off
Anamnesis Summary
• Pain in the right ear
• Heat sensation in the right ear
• Sensation of aural fullness in the right ear
• Serous discharge from the right ear
• History of right ear infection
C. Physical Examination
• General status: well conscious, adequatly nourished
• Vital sign:
Blood Pressure : 120/80 mmHg
Respiratory Rate : 88 x/minute
Heart rate : 20x/minute
Temperature : 37 0C
• Head and neck : Normal
• Conjungtiva anemia (-), enlargement of lymph node (-)

D. ENT Examination
Ear
Dextra Sinistra
Outer Inspection Auricular deformity
(-), Hyperemis (-),
swelling (-)
Auricular deformity
(-), Hyperemis (-),
swelling (-)
Palpation Tenderness (+) Tenderness (-)
Otoscopy EAC hyperemis (+),
swelling (+),minimal
discharge (+)
Tympanic membrane
can’t be asseseed
Normal EAC,
hyperemis (-),
swelling (-), normal
cerumen.
Intact tympanic
membrane, pearl-
white coloured,
perforation (-), cone
of light (+)
Nose
Dextra Sinistra
Inspection Deformity (-),
hyperemis (-),
swelling (-) discharge
Deformity (-),
hyperemis (-),
swelling (-) discharge

(-) (-)
Palpation Tenderness (-)
Anterior
Rhinoscopy
Septum deviation(-),
hyperemis (-),
swelling (-), massa(-),
discharge (-)
Septum deviation(-),
hyperemis (-),
swelling (-), massa(-),
discharge (-)
Posterior
rhinoscopy
(Not performed)
Paranasal sinus
examination
Maxilla and frontal tenderness (-)
Throat
Structure Finding
Lip Normal color
Buccal mucose Hiperemic (-)
Tongue and palate Hiperemic (-) stomatitis (-)
Dental and gingiva oedema (-), hiperemis (-), caries
(-)
Uvula Deviation (-)
Tonsil and pharyng T1-T1, hyperemic (-)
Indirect Laryngoscopy Not perfomed

E. Supporting examination : Not performed
F. Diagnosis
Otitis externa diffusa auris dextra
G. Therapy
Tampon sofratule
Natrium Diklofenak 2x 50 mg
H. Education
•The patient should meet the doctor for follow-up to know the progress of the
disease.
•Take care of the ear cleanliness and hygiene, prevent the entrance of water or any
foreign objects into the ear.
I. Problem
Management of Otitis Externa Diffusa (preferences between Ear wick or
Antibiotic Otic Drop)
J. Plan
Control every two until three days to reapply tampon (2 weeks)
K. Prognosis
Dubia ad bonam

CHAPTER IV
DISCUSSION
Diffuse otitis externa is an inflammation that affect whole externa ear
canal, with or without involvement of the pinna or tympanic membrane. The main
clinical features of diffuse otitis externa are pain, fullness, itching, hearing loss.
The severity of each symptoms depend on the severity of infection (mild,
moderate, severe). In this case, we conclude that patient suffers from acute
inflammatory stage (moderate severity) because the main complaint of this patient
was continuous pain in her right ear. The canal shows edema so that we could not
see the tympanic membrane. But the inflammation is not spreading to adjacent
soft tissue as in the severe stage.
In this case, patient complains about feeling continuous pain in the right
ear although there was no contact to the ear. The pain felt was accompanied with a
heat sensation that affected the patient’s routine activities. The patient felt that the
complaint worsen day by day.The patient also felt a sensation of aural fullness in
the right ear which affected her hearing in which she presumed that the sound
heard was from a distant source but in reality it is from a near source. The patient
has a history of routinely using cotton bud ( every 3 days once). From the
anamnesis and physical examination, the patient was diagnosed with diffuse otitis
externa auris dextra
Whether patient needs wick or otic drop depends on the severity of oedema.
In mild inflammatory stage, edema of the external auditory canal should not be
severe, and the patient should be able to instill drops into the ear by tilting the

head to the side or by lying down with the involved ear upright. Starting from
moderate stage, edema of the canal may interfere with the instillation of drops.
Hence the physician should then insert a wick into the canal. We chose sofratule
because of its functions as wick and antibiotic (framycetin). Antibiotic drops are
still be used for at least 2 to 3 days after the cesation of pain, itching, and
drainage, so that complete eradication of infection may be ensured. In severe
stage, the oral antibiotic is needed in addition of ear wicks and antibiotic otic
drops because the inflammation has spread to the surrounding tissue.

CHAPTER V
CONCLUSION
A female patient of age 30 years old being diagnosed with Otitis externa
diffusa auris dextra has been reported. This patient was tamponed with sofratule
wick and given natrium diclofenac 2x50mg as well as education. The patient is
adviced to control every two until three days to reapply tampon (2 weeks)

REFERENCE
1. Carr, MM. 2000. Otitis Eksterna. Available from : http://www.
icarus.med.utoronto.ea/carr/manual/otitisexterna. htm. Accessed : 2013,
February 3
2. Fatih, M. 2007. Otitis Eksterna. Available from :
http://hennykartika.wordpress.com/2007/12/29/otitis-eksterna/. Accessed :
2013, February 3worth Heinea ltd. Oxford 1992: 81-97
3. Gary RF. Anatomy of the ear. In: Synopsis of Otolaryngology 5th ed.
Butter
4. Oghalai, J.S. 2003. Otitis Eksterna. Available from : http://www.
bcm.tme.edu/oto/grand/101295.htm. Accessed : 2013, February 3
5. Soepardi E., Iskandar N, 2007. Telinga Hidung Tenggorok Kepala Leher.
Edisi keenam. Fakultas Kedokteran Universitas Indonesia. Jakarta: UI