Embed Size (px)
Citation preview

EVALUATION OF MEDIA CAMPAIGNS ON BREAST CANCER IN EDO STATE
OKEIBUNOR NGOZI BIBIAN
PG/MA/09/50934
A Research Project Submitted to the Department of Mass Communication, University of
Nigeria, Nsukka in Partial Fulfillment of the Requirement for the Award of Master of Arts
Degree in Mass Communication
DEPARTMENT OF MASS COMMUNICATION
UNIVERSITY OF NIGERIA, NSUKKA
FEBRUARY 2012.

TITLE PAGE
Evaluation of the Media Campaign on Breast Cancer in Edo State
By
Okeibunor Ngozi Bibian.
PG / MA /09/ 50934.
A Research Project Submitted to the Department of Mass Communication, University of
Nigeria, Nsukka in Partial Fulfillment of the Requirements for the Award of Master of Arts
Degree in Mass Communication.
February 2012.

CERTIFICATION
This research work is an original work of Okeibunor Ngozi Bibian with registration number
PG /MA / 09 / 50934. It satisfies the requirements for presentation of research report in the
Department of Mass Communication, University of Nigeria, Nsukka.
_________________ _______ ______________________ ________
Dr C.S. Akpan Date Prof Ike.S. Ndolo Date
Project Supervisor Head of Department
_______________________ ________
External Examiner Date

DEDICATION
This project is dedicated to all women who have in one time of their lives suffered and
survived breast cancer or have lost their loved ones because of the disease.
And finally to God Almighty, whose infinite strength and grace saw me through the thick
and thin clouds of this research work. To Him be all glory in Jesus name.

ACKNOWLEDGMENTS
This piece of work remains grossly incomplete without acknowledging the unflinching
moral, financial, and academic support of those who stood by me all through this work. I
hereby place on record my profound gratitude to the following deserving persons.
To my supervisor, Dr. C.S. Akpan, goes my sincere and heartfelt gratitude for his
scholarly advice, suggestions and constructive criticism that helped in no small measure in
refining, shaping and making this work a success.
I also remain eternally grateful to all the lecturers of the Department of Mass
Communication, University of Nigeria, Nsukka, for their love and care during my stay in
the University.
I specially bare my indebtedness to my darling husband, Rev. Blessing T. Okeibunor
and my children, Davidson, Alfred, Othniel and Adaobi Okeibunor for their immeasurable
love and prayers during the course of this study. I will not fail to appreciate my dear mother
Mrs. Rosecharity Eriobuna and my brothers, Chukwuma, Omata and Jideofor Eriobuna, for
their immense contribution of love and care and for being part of this vision.
My special thanks equally goes to Prof. J. C. Okeibunor and Dr. Nkechi Onyeho, for their
support and encouragements that gave me hope.
I cannot forget my classmates and roommates in room 325, Odili hall, whose concern
and understanding helped me through.
OKEIBUNOR NGOZI BIBIAN.
UNIVERSITY OF NIGERIA, NSUKKA.
FEBRUARY, 2012

TABLE OF CONTENTS
Page
Title page………………………………………………… ………………..i
Certification………………………………………… ……………………..ii
Dedication……………………………………………………………….…iii
Acknowledgements…………………………………………………….…..iv
Table of contents………………………………………………………..….v
List of tables/graphs and charts....…………………… …….…………....vii
Abstracts…………………………………………………………..……….viii
CHAPTER ONE: INTRODUCTION ……………………………………1
1.1 Background of Study………………………………………….… …...1
1.2 Statement of Problem……………………………………………………5
1.3 Objectives of Study………………………………………………………6
1.4 Research Questions……………………………………………………….6
1.5 Significance of Study……………………………………………………..6
1.6 Definition of Terms……………………………………………………....6
References……………………………………………………………..….9
CHAPTER TWO: LITERATURE REVIEW……………………………..11
2.1 Focus of Review…………………………………………………………..11
2.2 The Review itself………………………………………………………….11
2.3 Theoretical Framework…………………………………………………….37
References…………………………………………………………………40
CHAPTER THREE: METHODOLOGY …………………………………..43
3.1 Research Design…………………………………………………………….43
3.2 Population of Study………………………………………………………….43
3.3 Sample Size………………………………………………………………….43

3.4 Sampling Technique……………………………………………………..…….44
3.5 Measuring Instrument………………………………………………………….51
3.6 Validity/Reliability……………………………………………………………..51
3.7 Method of Data Analysis……………………………………………………….51
3.8 Limitations of Methodology…………………………………………………….52
References……………………………………………………………………….53
CHAPTER FOUR: DATA PRESENTATION AND ANALYSIS………………54
4.1 Description of the Sample………………………………………………………..54
4.2 Data Presentation and Analysis…………………………………………………..55
4.3 Discussion of Findings………………………………………………………...…90
CHAPTER FIVE: SUMMARY CONCLUSION AND
RECOMMENDATIONS ………………………………………………………..…94
5.1 Summary………………………………………………………………………....94
5.2 Conclussion………………………………………………………………………94
5.3 Recommendations………………………………………………………………..96
Bibliography……………………………………………………………………..98
Appendices.…………………………………………………………………..…102
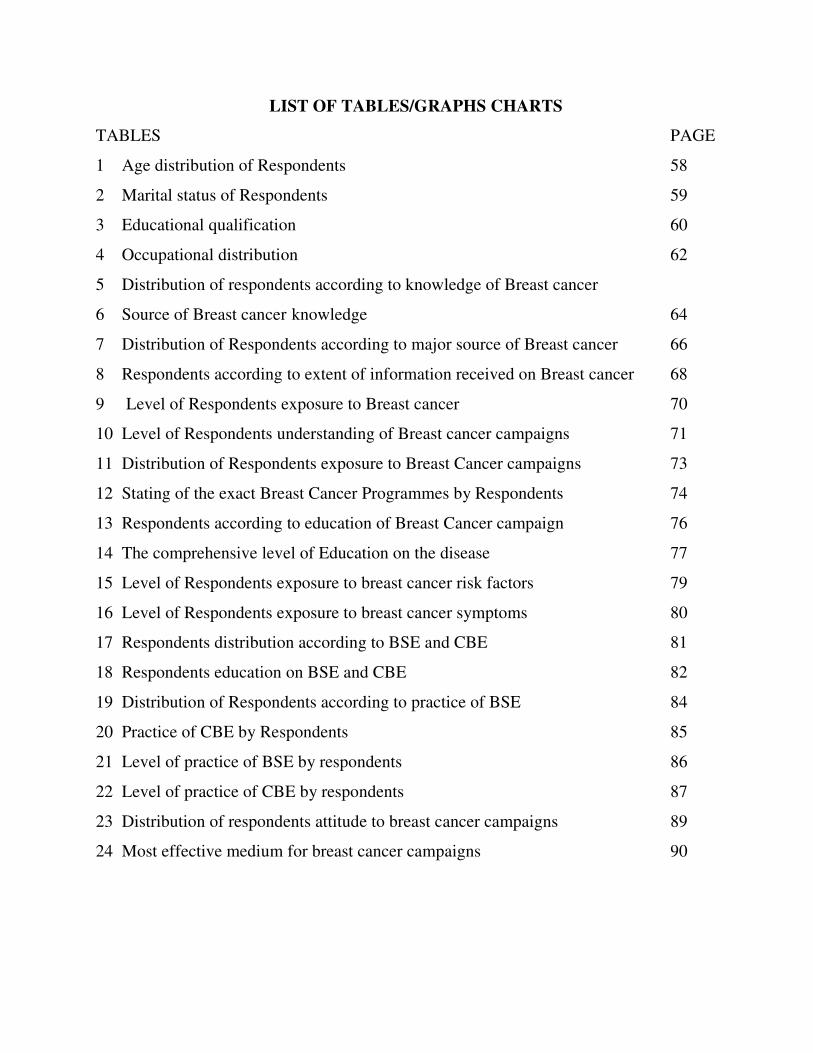
LIST OF TABLES/GRAPHS CHARTS
TABLES PAGE
1 Age distribution of Respondents 58
2 Marital status of Respondents 59
3 Educational qualification 60
4 Occupational distribution 62
5 Distribution of respondents according to knowledge of Breast cancer
6 Source of Breast cancer knowledge 64
7 Distribution of Respondents according to major source of Breast cancer 66
8 Respondents according to extent of information received on Breast cancer 68
9 Level of Respondents exposure to Breast cancer 70
10 Level of Respondents understanding of Breast cancer campaigns 71
11 Distribution of Respondents exposure to Breast Cancer campaigns 73
12 Stating of the exact Breast Cancer Programmes by Respondents 74
13 Respondents according to education of Breast Cancer campaign 76
14 The comprehensive level of Education on the disease 77
15 Level of Respondents exposure to breast cancer risk factors 79
16 Level of Respondents exposure to breast cancer symptoms 80
17 Respondents distribution according to BSE and CBE 81
18 Respondents education on BSE and CBE 82
19 Distribution of Respondents according to practice of BSE 84
20 Practice of CBE by Respondents 85
21 Level of practice of BSE by respondents 86
22 Level of practice of CBE by respondents 87
23 Distribution of respondents attitude to breast cancer campaigns 89
24 Most effective medium for breast cancer campaigns 90

ABSTRACT
The research focused on evaluating the media campaigns on breast cancer to which women in Edo
state are exposed. Five research questions guided the study. A survey method which employed a
structured questionnaire was employed for data collection from 400 Edo women. The findings
showed the inadequacies that characterized the media campaigns on breast cancer in the Edo
State. The result revealed that most women had knowledge of breast cancer but the knowledge was
not deep rooted. Consequently, most of the breast cancer programmes that were featured in these
media campaigns were found to be infrequent and incomprehensive to engender a positive
behaviour change in Edo women in observing their breast self examination(BSE) and clinical
breast examination (CBE) believed to save lives and reduce mortality rates, without the support of
face – to – face campaign. However, radio was found to be the major source of breast cancer
information to Edo women as well as the most effective medium for breast cancer campaign due to
its widest reach and the efficiency with which it transcends literacy level of the audience. It is
recommended that breast cancer programmes be featured frequently and programmes like drama,
radio jingles, television commercials and Internet be added to the available programmes while
employment of indigenous language be included in the packaging of the progammes. Finally, face –
to –face campaign should complement media campaign to reinforce credibility and clarity of media
campaign programmes on breast cancer.

CHAPTER ONE
INTRODUCTION
1.1 Background of Study
Breast cancer is the most common diagnosed cancer in women globally and the second
most common cancer in the world. (Azenha, Bass, Caleffi, Smith, Pretorius, Durstine and
Perez, 2011; Parkin, Bray, Ferlay and Pisani, 2005; Okobia, Bunker, Okonofua, and Osime,
2006) Its attacks on women is reported to be three times higher in developed parts of the
world than in less developed parts, but the death toll is greater in less developed regions
(Azenha et al, 2011),
It is however a cancer that originates from breast tissue; hence it is regarded as a
cancer of the glandular tissue of the breast. Though the disease is confirmed to be found
both in male and female patients, yet the incidence is hundred times more in women than in
men. (Russel 2007). Breast cancer is therefore a proliferation of breast cells that is
characterized by an abnormal growth and division of the cells to the destruction of the
surrounding tissues through the filtration of the cancerous cells into the blood stream
(Medical Women’s Association of Nigeria, 2011).
However, breast cancer is mostly detected by a painless lump or mass of tissues
called tumors, with genetic mutations and age, among the risk factor. (Blugs, Cummings,
Spencer, and Palladino, 2009). Historically, according to Russel (2007) breast cancer may
be one of the oldest known forms of cancerous tumors in women in Egypt and it dates back
to approximately 1600BC. It was first noted and recorded as tumors or ulcers of the breast.
During that time, Edwin, Papyrus described eight cases of tumors or ulcers of the breast that
were treated by cauterization as ‘there is no treatment’. This treatment by cauterization was
done with a tool called ‘Firedrill’. For centuries, physicians described similar cases in their
practices with the same conclusion. It was not until doctors achieved greater understanding
of the circulatory system in the 17th
century, that they could establish a link between breast
cancer and the lymph nodes in the armpit. However, the French surgeon, Jean Lewis Petit
(1674 – 1750) and Scottish Surgeon, Benjamin Bell (1749 – 1805) were the first to remove
the lymph nodes, breast tissue and chest muscle in an effort to save women from breast
cancer. Their successful works were carried on by William Stewart, who started performing
mastectomies in 1882. The Halsted radical mastectomy often involved removing both breast

associated with the lymph nodes and the underlying chest muscle. This often led to a long
term pain and disability, but was seen as necessary, in order to prevent the cancer from
reoccurring. Radical mastectomy therefore remained the standard until in the 1970s, when a
new understanding of metastasis led to perceiving cancer as the system illness as well as a
localized one. (Rusel, 2007).
Moreover, following the global trend, the incidence and mortality of breast cancer
constitute a major public health issue. In the view of the World Health Organization and
International Union against Cancer (2005), breast cancer comprises 10.45% of all cancer
incidence among women, making it the second most common type of non-skin cancer (after
lung cancer) and the fifth most common causes of cancer deaths.
For instance, it was observed in 2004, that the ailment claimed 579,000 lives world-
wide. This is evident in Pakistan, an Asian country, which has the highest rate of breast
cancer, for any Asian population accounting for 40,000 deaths per year. It is therefore
approximated that 35% of Pakistani women suffer from breast cancer at some points in their
lives. Every fifth woman, after the age of 40, develops the disease, 77%, after the age of 50,
develop invasive breast cancer. (Pielle, 2005). Similarly, it was also reported that it is the
most prevalent cancer in American women who have a one to eight lifetime chance of
developing the tumour/lump, coupled with 3% chance of the disease causing their death.
(Russel, 2007).
According to the American Cancer Society (2007) quoted in Udoudo (2008:365)
Female breast cancer incidence rates, for 2002, vary internationally by
more than 25 fold, ranging from 300 cases per 100,000 in Mozambique to
101.1 in the United States, North America, Australia and Northern and
Western Europe have the highest incidence of breast cancer. Large parts of
Africa and Asia have the lowest.
The alarming increase in the incidence and mortality of the disease not only has
posed a great threat to the world of women with slim survival rates, but also created a great
deal of concern to the entire world (WHO & UICC, 2005). It is in view of the above that
the United Nations, international organizations and national governments have initiated
combative strategies against the pandemic with the month of October declared as the
National Breast Cancer Awareness month and pink ribbon, symbolizing the awareness of
the disease. (King, 2006).

The Nigerian experience of the increase of breast cancer attacks and deaths is not
different. Organizations like. Lagos Chamber of Commerce and Industry (LCCI) and the
National Cancer Prevention Programme (NCPP) are joining forces to mount a fresh
onslaught on breast cancer. (Adebayo, 2010). Also in the fight, is the Breast without Spot
Initiative (BWSI), launched in April 2008 in Abuja, with the aim to sensitize and prevent
late presentation of women with breast cancer. (The international cancer week, 2010)
The above fight becomes necessary, considering the revealing news reports that 83%
of cases of cancer that arrive Nigerian hospitals, do so very late. According to the news
report, the late arrival of cancer patients to the hospitals only meet with palliative medical
assistance, which is not intended to cure the patients but to help manage them before the
inevitable happens. In regards to the state of the Nigerian government hospitals, the reports
disclosed that the Abuja National Hospital, for instance, does not have functional equipment
on ground, to offer proper diagnosis and treatment to cancer patients. The result, in the view
of this report is that most people suffer the disease and later die eventually because of poor
diagnosis and treatment. (NTA News, 2011).
In light of the above, experts and WHO warned that unless checked, the burden of
cancer in Nigeria and other developing countries will increase (Tell Magazine, 2011). It is
therefore pertinent at this juncture, to know as confirmed by the American Cancer Society
(2007) that early detection or diagnosis of breast cancer can save the life of the patient.
Implying that the disease is a preventable and a curable one as it is ascertained, that a
patient’s chances of surviving breast cancer is higher than 90%,only with early diagnosis,
and therefore need not be made fatal. (Kayode, Akande,& Osagbemi 2005).
The above therefore will depend on the positive response of women to media
awareness and campaigns on breast cancer, for the much emphasized ‘early detection’ of
the ailment and its preventable stage to become a reality. There is no doubt therefore that
the best way to create awareness is through the media, of which useful information can be
passed on from a reliable source to thousands of people around a target area. In other words,
mass media consisting of newspaper, radio, television, magazine, posters, pamphlet/leaflet,
billboards, internet, et cetera, in any society, are to inform, correlate and educate (among
others) in the process of being tools of change. It is on this note that the creation of
awareness on health issues, using the media of mass communication has served as vehicles
of fighting against onslaught of diseases in the past years.
(http://www.answers.com/topic/massmedia).
That is why the mass media are believed to be important tools in advancing public
health goals in societies. It follows that the employment of the mass media to disseminate
and deliver health news and medical therapies to their target audiences will certainly
achieve greater and positive results. (http://www.answers.com/topic/massmedia).
It then becomes evident that effective provisions of constant health information to
Nigerian women, to sensitize, educate and mobilize them on the causes of breast cancer, the
various common symptoms, the risk factors, preventive measures and possible treatments,
are in the domain of the media of mass communication since it is in the ability of the media
to inhibit or promote a change in a society.
It is in line with the view that Mboho (2003), observes that frequent and constant
projection of issues in cancer, as major health problems by the media has the ability of
inculcating in their audience, the knowledge of all that cancer entails. Therefore, constant
media campaign programmes against breast cancer are capable of evoking positive attitudes
in women by responding to do their Breast Self Examination (BSE) and Clinical Breast
Examiniation (CBE) and change wrong habits that can cause cancer and take the necessary
preventive measures.
It is against this backdrop, that the media campaigns have indeed been identified as
vital strategies to be employed in achieving a much needed quick and prompt compliance
from women in the struggle to combat the onslaught of breast cancer. In other words,
effective media campaigns for early presentation of breast cancer by women will make the
90 per cent chances of surviving breast cancer a reality.
Media campaigns can therefore be seen as a series of measures taken to influence
attitudes and opinions. It can be of short duration or over long periods. They are widely
employed to expose high proportion of large population to messages through existing media
such as billboards, radio, television, magazine, newspaper, internet, et cetera. (Wakefield,
Loken &Hornik, 2010).
It is believed therefore, that if media campaigns are properly designed and executed,
following `Coffman’s (2002) characteristics of effective campaign of delivering
understandable and credible messages, capturing the right audience attention and

dissemination of messages that are capable of influencing or causing a change in the
audience attitudes, will form a major link in the communication processes geared towards
achieving attitude or behavioural changes.
1.2 Statement of the Problem
Cancer is one of the deadly diseases that has threatened the world. According to
WHO (2005), about 12.5% of all deaths globally are caused by cancer, with the percentage
more than the percentage of deaths caused by HIV/AIDS, tuberculosis, and malaria put
together.
Therefore, the increase in the attacks and deaths of women with breast cancer in Edo
State poses a pertinent question on the effect of breast cancer campaigns on Edo women as
regards the their poor responses to early presentation of breast cancer. It is in view of the
above and given the confirmation of American Cancer Society (2007) that breast cancer
deaths remain preventable at the early stage, that the researcher critically evaluated the
effectiveness of the media campaign programmes on breast cancer, in causing a quick and
prompt positive changes of the women in performing their BSE and CBE for the reduction
in their mortality rate.
1.3 Objectives of Study
The objectives of the study are:
1. To ascertain the media campaign programmes on breast cancer and their frequency
2. To identify the medium women are most exposed to.
3. To find out the level of Edo women’s exposure to media campaign messages on
breast cancer.
4. To ascertain the medium that is most effective for media campaign on breast cancer.
5. To evaluate the effectiveness of the media campaigns on breast cancer awareness
1.4 Research Questions
The research questions are as follows:
1. How frequent are the media campaigns programmes on breast cancer in Edo State?
2. Which medium are women most exposed to?
3. Do Edo women have adequate exposure to media campaign on breast cancer?
4. Which medium is most effective for breast cancer campaigns?

5. How do Edo women perceive media campaign on breast cancer?
1.5 Significance of Study
1. This study has both theoretical and practical significance. Theoretically, it will
contribute to the articulation of the media campaign role in solving the problem of breast
cancer.
2. It will serve as a data base to mass communication researchers who may be interested
in learning the global fight on breast cancer and future researchers, who may embarking on
similar research in future.
3. It practical will serve as a document for government and non-governmental
organizations, policy makers and media campaigns planners in the field of breast cancer.
1.6 Definition of Terms
Media Campaigns
Media campaigns are intensive and organized form of persuasive communication sponsored
by an authority and packaged in the form of jingles, commercials, press release, articles,
news stories, and dramas and so on. These are published or disseminated through the
various mass media like newspaper, radio, television or internet, to the different targeted
audiences, with the mind to sensitize and mobilize the people into action or towards a
desired goal.
Women Responses/Compliance
Women’s responses are the way and manner the women who are exposed to the media
campaigns programmes or who are reached with the media campaigns messages react or
respond to the messages, to performing breast self examination (BSE) or clinical breast
examination (CBE) or acting otherwise.
Metastasis or Metastatic
This is the spread of cancerous cell from one organ to another organ or part.
Metastatic Breast Cancer

It is a stage of breast cancer where the cancerous cell has spread to distant sites or has
metastasized from one organ to another. For example breast cancer cell spreading to lungs,
bones, liver, lymph nodes and brain.
Invasive Breast Cancer
This is breast cancerous cell that invade normal healthy tissues.
Non Invasive breast cancer
This stays within the breast milk ducts or lobules in the breast, they do not invade the
normal tissue within or beyond/outside the breast. They are called carcinoma in situ
meaning in the same place
Ductal Carcinoma In Situ (DCIS)
It is a breast that has not spread beyond breast milk duct to any normal surrounding breast
tissue. It is the most common type of non-invasive breast cancer where Ductal refers to the
breast cancer that forms in the milk duct, Carcinoma refers to the breast cancer that forms in
the skin or tissue of the breast that covers the internal organs while ‘In situ’ means the
breast cancer that is in the same place where it started.
Mammogram
This is an x-ray picture of the breast which is used to check for breast cancer in women who
have no symptoms of the disease.
Mammography
Is a screening tool or low-energy x-ray used to examine or diagnose women breast for
detection of lumps or masses of tumors.

REFERENCES
Adebayo,F. (2010 April ). Cancer goes commercial. Tell magazine. Pp. 12.
American Cancer Society (2007) Global cancer facts and figures.
Atlanta: ACS
Azenha, G. Bass, L.P. Caleffi, M. Smith, R. Pretorius, L. Durstine A. and Perez CP. (2011).
The role of breast cancer civil society in different resources settings. Retrieved on 26
April , 2011.
Blug, W.S, Cummings, M.R, Spencer, C.A and Palladino, M.A (2009). Concepts of genetics. America: Pearson Prentice Hall.
Breast Without Spot (BWS). http://wwwinternationalcancerweekinitiativecan/index.php?.
Retrieved on 26 February , 2011.
Coffman, J. (2002). Public communication campaign evaluation: An environment scan of
challenges, criticism, practice, and opportunities. Cambridge, M.A. Hanard family
Research Project. Retrieved from www.thelancet.com
Kayode, F.O, Akande, T.M. and Osagbemi, G.K (2005). Knowledge, attitude and practice
of breast self examination among female secondary school teachers in Ilorin, Nigeria.
European journal of scientific research. Vol pp42.
King .S., (2006). Pink Ribbons Inc: Breast cancer and the politics of philanthropy.
Minneapolis: University of Minnesota press.
Medical Women’s Association of Nigeria, Edo State (2011). Breast self examination. Edo
State: Medical Women, Association of Nigeria.
Nigeria Television Authority (2011,February 4)7am Network News.
Okobia, M.N., Bunker, C.H., Okonofua, F.E and Osime, U. (2006). Knowledge, attitude
and practice of Nigeria women towards breast cancer, a cross-sectional study.
Retrieved from http://creativecommons.org/licenses/by/20.
Parkin, D.M., Bray, F., Ferlay, J. and Pisani, P. (2005). Global cancer statistics, 2005, CA:
A cancer journal for clinicians, 55(2), 74-108.
Pielle, (2005). Public service: breast cancer awareness campaign- Pakistan. Retrieved on 26
February, 2011.
The scourge of cancer (2011,Febuary 7). Tell magazine pp 5.
Udoudo, A.J, (2008) Rising cases of cancer and media social responsibility. International
journal of communication. Vol. 2 pp 364 – 373.

Wakefield, M.A. Loken, B. and Hornik R.C. (2010). Use of mass media campaigns
to changes health behaviour. Retrieved on 26 February, 2011.
WHO/UICC (2005) Global action against cancer, New Switzerland:
WHO|UICC
Russell, M. (2007) Understanding Diseases. http://EzineArticle.com/?expert=micheal
http://www.answers.com/topic/massmedia
CHAPTER TWO
LITERATURE REVIEW
2.1 Focus of Review
The focus of review of this study entails the different sub topics that are inter-related to the
main topic of the research work. The study will therefore review the different areas that
bordered on the research topic.
They are;
Overview of Breast cancer
Breast cancer stages
Breast cancer types
Breast cancer risk factors
Breast cancer symptoms
Breast cancer screening/Diagnosis
Breast cancer treatment
Overview of other media campaigns
Media campaign types
Empirical studies
Theoretical framework
2.2 Review Itself
Overview of Breast Cancer
Breast cancer is a malignant tumor which originates from breast tissue. It is a cancer of the
glandular breast tissue, where the tissues are destroyed due to excessive growth of the
cancer cells, leading to the destruction of the surrounding tissues and other organs through
the blood stream. (MWAN, 2011,Russel, 2007).
As earlier acknowledged, breast cancer is the most frequently diagnosed cancer in
women all over the world, accounting for almost 1 % of all deaths and ranking the fifth
most common form of cancer and a major cause of deaths among women of 30 years and
above (American Cancer Society, 2007, Parkin, Bray, Ferlay and Prsani, 2005, Azenha,
Bass, Caleffi, Smith, Pretorius, Durstine and Perez, 2011, Okobia, Bunker, Okonofua and
Osime, 2006, Dumittrescu ε Cataria, 2004, Russel,2007).

However, Breast cancer is mostly detected by a painless lump or mass of tissues
called tumors (Blugs, Cummings, Spencer and Palladino, 2009 and Okobia, Bunker,
Okonofua and Osime, 2006). The cancer cells usually start either in the cells of the lobules
or the ducts. The lobules are the milk-producing glands while the ducts are the passages
where the produced milk is collected from, to the nipples. The cancerous cells can also
develop into the stomal tissues such as the fatty and fibrous connective tissues of the breast,
though this occurrence is not common.
(http://wwwbreastcancer.org/illustration/10013.html) and Blugs, Cummings, spencer ε
Palladino, 2009)
However according to Breast Cancer.Org, (2009) there are different stages of breast
cancer that explicitly show how far the cancer cells have metastasized or spread beyond the
original tumor.

Stages of Breast Cancer
Breast cancer stages are characterized by the cancer size, the invasiveness or non
invasiveness of the cancer, the lymph nodes and the metastasis of the cancer.
Breast cancer stages can also be described as local, regional and distant. Breast
cancer stage can be local when the cancer is confined within the breast. It is regional when
the cancer is in the lymph nodes, primarily in the armpit. While distant breast cancer stage
is where the cancer has metastasized to other parts of the body.
Moreover, TNM is another staging system used to describe cancer. This comprises
the size of the tumor (T), the lymph node (N), and the spread, or metastasis of the cancer to
other parts of the body (M).
Stage 0
This stage explains non-invasive breast cancers as in DCIS (ductal carcinoma in
situ). It is a stage where no evidence of cancer cells forming on any part of the breast
invading neighboring normal tissue exists.
Stage I
Stage I portrays invasive breast cancer invading normal surrounding breast tissue. In
this stage, the tumor measures up to 2 cm and no lymph nodes are involved.
There can also be a microscopic invasion in stage I breast cancer. In microscopic
invasion, the cancer cells just began o invade the tissue outside the lining of the duct or
lobule, but the invading cancer cells do not measure more than 1 mm.
Stage II
Stage II consists of subcategories known as IIA and IIB. Stage IIA is a stage of invasive
breast cancer where cancer cells are found in the lymph nodes under the arm but not in the
breast. Then in this stage the tumor which has spread to the axillary lymph nodes measures
2cm or smaller but the tumor can be larger than 2 cm but not larger than 5 cm and has not
spread to the axillary lymph nodes

Stage IIB – Here the invasive breast cancer either shows where the tumor is larger than 2
cm but no larger than 5 cm and has also metastasized to the axillary lymph nodes or it
shows where the tumor is larger than 5 cm but has not spread to the axillary lymph nodes
Stage III
Stage III is divided into there categories known as IIIA, IIIB, and IIIC.
Stage IIIA portrays the invasive breast cancer with either no tumor but cancer found
in axillary lymph nodes, clumped together to other structures, or may have spread to lymph
nodes near the breastbone
Stage IIIB explains invasive breast cancer where the cancer involved is of any size
and has spread to the chest wall and/or skin of the breast and have also spread to axillary
lymph nodes, and sticking to other structures, near the breastbone. For instance,
inflammatory breast cancer is considered a stage IIIB example with the typical features as:
reddening of a large part of the breast skin, swollen or warmth feeling of the breast and
spreading of the cancer cells to the lymph nodes.
Stage IIIC explains invasive breast cancer where no symptom of breast cancer exists or
where a lump of any size has spread to the chest wall and/or the skin of the breast.
Additionally it involves the spreading of the cancer to lymph nodes above or below the
collarbone as well as the cancer spread to the axillary lymph nodes near the breastbone
Stage IV
In this stage iv invasive breast cancer has spread beyond the breast and nearby lymph nodes
to other organs of the body, such as the lungs, distant lymph nodes, skin, bones, liver, or
brain.
Advanced and “metastatic” are words used to describe stage IV breast cancer. Cancer
may be stage IV at first diagnosis or it can be a recurrence of a previous breast cancer that
has metastasized to other parts of the body.
Breast cancer type with pictures are
1. HER2-Positive Breast Cancer

In about 20% of patients, breast cancer cells have too many receptors for a protein called
HER2. This type of cancer is known as HER2-positive, and it tends to spread faster than other
forms of breast cancer. It's important to determine whether a tumor is HER2-positive, because there
are special treatments for this form of cancer.
2. Hormone-Sensitive Breast Cancer
Some types of breast cancer are fueled by the hormones estrogen or progesterone. A biopsy can
reveal whether a tumor has receptors for estrogen (ER-positive) and/or progesterone (PR-positive).
About two out of three breast cancers are hormone sensitive. There are several medications that
keep the hormones from promoting further cancer growth.
3. Signs of Inflammatory Breast Cancer
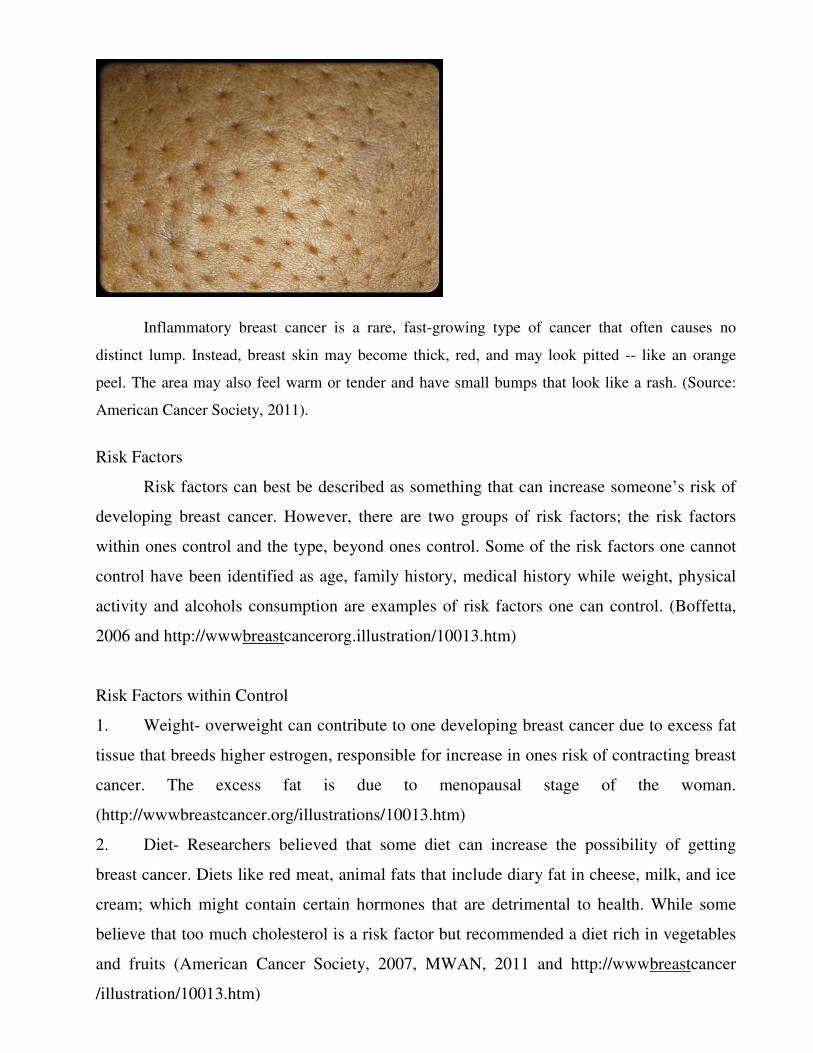
Inflammatory breast cancer is a rare, fast-growing type of cancer that often causes no
distinct lump. Instead, breast skin may become thick, red, and may look pitted -- like an orange
peel. The area may also feel warm or tender and have small bumps that look like a rash. (Source:
American Cancer Society, 2011).
Risk Factors
Risk factors can best be described as something that can increase someone’s risk of
developing breast cancer. However, there are two groups of risk factors; the risk factors
within ones control and the type, beyond ones control. Some of the risk factors one cannot
control have been identified as age, family history, medical history while weight, physical
activity and alcohols consumption are examples of risk factors one can control. (Boffetta,
2006 and http://wwwbreastcancerorg.illustration/10013.htm)
Risk Factors within Control
1. Weight- overweight can contribute to one developing breast cancer due to excess fat
tissue that breeds higher estrogen, responsible for increase in ones risk of contracting breast
cancer. The excess fat is due to menopausal stage of the woman.
(http://wwwbreastcancer.org/illustrations/10013.htm)
2. Diet- Researchers believed that some diet can increase the possibility of getting
breast cancer. Diets like red meat, animal fats that include diary fat in cheese, milk, and ice
cream; which might contain certain hormones that are detrimental to health. While some
believe that too much cholesterol is a risk factor but recommended a diet rich in vegetables
and fruits (American Cancer Society, 2007, MWAN, 2011 and http://wwwbreastcancer
/illustration/10013.htm)

3. Exercise- Lack of exercise can increase the risk of breast cancer while engaging in
45-60 minutes exercise for about 5 or more days a week according to American Cancer
Society, (2007) can reduce the risk of breast cancer, (MWAN, 2011 and
http://wwwbreastcancerorg.illustration/10013.htm)
4. Alcohol and smoking – It has been found out that partakers of alcohol and smoking
are liable to contract breast cancer more than non-partakers. The detrimental effect of
alcohol can limit ones liver’s ability to control blood levels of the estrogen hormone
(American Cancer Society, 2007 and http://wwwbreastcancer.org/illustrations/100013.html)
Risk Factors beyond Control
1. Age – Age has been attributed the second biggest risk factors of breast cancer.
Studies have shown that women from age 30-39 have 1 in 233 or 43% chances of
developing breast cancer while at 60 years of age, risk increases to 1 in 27 or 4% chances of
contracting the disease. In other words about 95% of the diseases are predicted on the
genetic abnormalities that take place as an aftermath of aging process as well as “wear and
tear of life. (Medical Women Association of Nigeria, 2011, American Cancer Society, 2007
& http://wwwbreastcancer.org/illustrations/10013.html)
2. Gender/Sex – This is about being a woman. Researchers have confirmed gender as
the primary risk factor of breast cancer. Though it has been found in men, but is
100% more in women than in men, mainly due to the activities of estrogen and
progesterone, (female hormones) that make the female breast experience continuous
changes and growths.
(http://wwwbreastcancer.org/illustrations/10013.html)
3. Race – It has also been discover that white women are quite prone to getting the
disease than Asian, Hispanic, Native American, African American women
(http://wwwbreastcancer.org/illustrations/10013.html)
4. Family history of breast cancer – This moreover has been attributed to causing
women with family history of mothers, daughters and sisters with breast cancer to
stand a higher risk of getting the disease (MWAN 2011and
(http://wwwbreastcancer.org/illustrations/10013.html)
5. Pregnancy and Breast Feeding. However, Pregnancy and breast feeding are widely
believed to reduce future attacks of breast cancer due to engaging in a larger period
of breast feeding, such as from 1 to 2 years. While women who got their first

pregnancy at the age of 30, are at a higher risk of breast cancer. (MWAN, 2001,
Ogbodo, 2010)
http://wwwbreastcancer.org/illustrations/10013.html
Symptoms
Symptoms of breast cancer in the view of American, Cancer Society, (2007) and Medical
Women’s Association of Nigeria, (2011), only show physical signs of a painless lump or
tumor at the early treatable stage when the cancerous cells in question exhibit no symptoms
due to the smallness of the lump.
It then implies that the symptoms of the disease at the later stage of the cancerous
cells include:
1. Lump or thickening within the breast, whether tender or not.
2. Changes in size and shapes of the breasts.
3. Depressions on the surface of the breasts
4. Rashes or scaling of the skin
5. Drawing in of the nipples
6. Newly visible veins
7. Nipple Discharge or bleeding from the nipple
Screening/Diagnosis
Screening and diagnosis are very vital in the early detection and treatment of breast cancer
(Gallagher, Updegraff, Rothman & Sims, 2011, Blugs, Cummings Spencer ε Palladino,
2009, Okoboa, Bunker, Okonofua & Osime, 2006).
Breast cancer screening therefore refers to testing an otherwise healthy woman for
breast cancer in an attempt to achieve an early diagnosis, which has been established to
greatly improve outcomes or the odds of successful treatment and survival (Blugs,
Cummings, Spencer and Palladino, 2009, Gallagher Updegraff, Rothuman and Sims, 2011).
It is a process whereby women examine their breast by themselves in order to detect
any abnormal lump or swelling for prompt medical assistance. This is called breast
examination. (Kayode, Akande, and Osagbemi, 2005). While CBE is the clinically
examination of breast for the diagnosis of cancer cells. In the same vein, mammography

screening is the use of X-rays to examine the breast for any uncharacteristic masses or
lumps (http://www.breastcancer.org/illustrations/fooiz.html). Moreover; couple with the
aforementioned screening tools, Giordano (2003) affirms the use and inclusion of Fine
Needle Aspiration and Cytology (FNAC), for breast cancer diagnosis.
Nevertheless, mammography has been recommended for women adherence as the
most effective method of early detection and reduction in breast cancer mortality
(Gallagher, Rothman, and Sims, 2011, Humphrey, Helfanel, Chan and Woolf, 2002)
Treatment
Breast cancer treatment depends on the type of cancer, the stage of cancer, age, health status
and additional personal characteristics (Blugs, Cummings, Spencer and Palladino, 2009).
The treatment can be done by surgery, radiotherapy (radiation), chemotherapy and drugs.
There is no single treatment of breast cancer but a combination of the aforementioned
therapies. Often, surgery is employed at the early stage of the cancer while chemotherapy is
applied at the advanced stage of the cancer
Overview of Media Campaigns
In the opinion of the following organizations, Joanneum, Nielsen, University of Sheffield
onto text, Hs – Art, University of Twente, Softcopies Mat and TNO, (2006), a media
campaign can be defined as a series of measures taken to affect attitudes and opinions.
According to them, the scope of a media campaign should comprise discovering,
interrelating and navigating different media campaign knowledge, widely automating the
detection and tracking of various media campaigns in the press, television and internet.
Media campaigns are widely used to expose high proportions of large population to
messages through routine use of existing media such as television, radio and newspapers.
(Wakefield, Loken and Hornik, 2010). According to them, campaigns have been employed,
over past decades, to affect different health behaviours in large populations. However, the
great promise of these media campaigns anchors on their competence to carry well defined
behaviorally focused messages to target audience repeatedly over time. (Wakefield, Loken
and Hornik, 2010).

Evidently, they can be of short period of time or of long duration. In the same vein,
they might stand alone or be combined with other organized programmes like clinical/health
or institutional outreach or may complement policy change. Therefore, multi ways of
disseminating campaign messages are employed, if health campaigns are part of broader
social marketing programmes (Wakefield, Loken and Hornik, 2010).
Types of Media Campaign
There are two types of media campaign: social marketing and media advocacy. (Joanneum
et al, 2006). According to Andreasen in ORCMACRO and APCO (2004), social marketing
as a conceptual approach to media campaigns is defined as “the application of commercial
marketing technology to the analysis, planning, execution and evaluation of programmes
designed to influence the voluntary behaviour of target audiences in order to improve their
personal welfare and that of their society”.
It employs traditional advertising techniques to affect individual behaviour by buying
of the television, radio or printed space. While in contrast to public health communication,
social marketing uses persuasive messages, audience research and participation to target a
particular segment of a population (ORC Macro and APCO, 2004 and Joanneum et al
2006). Social marketing key principles comprise the following:
1. Targeting behaviour change
2. Leveraging resources
3. Creating audience centered strategies and tactics
4. Using the four P’s of marketing product, price, place and promotion.
5. Understanding the target audience through research.
6. Grouping audiences into segments that have similar characteristics and
7. Recognizing competition. (Andreasen in ORC macro and Apco, 2006:2)
Media advocacy on the other hand, entails garnering of attention of the media on
issues through development of relationship with radio, television, print reporters etcetera. It
is mostly employed to influence public policy such as disseminating information to law
makers through the media.
Similar to the above perspective is public communication campaigns, where media,
messaging and organized communication activities are used to produce particular results in
a large number of individuals and in a particular period of time. Multi-communication

channels are employed in this aspect of campaign to often coordinate mass media effort
with the aim to sharpen behavioural patterns to achieving desired social results, such other
channels are interpersonal and community based communication channels. (Coffman, 2002)
Public communication campaigns, according to Coffman (2002) are categorized into
two, namely: individual behaviour change campaign and public will campaign. Individual
behaviour change campaign are packaged to change individual behaviours capable of
endangering their wellness or to promote behaviours that can engender their social well
being. Campaigns under this type, target behaviours such as drug use, smoking, recycling,
and seatbelt usage, fire and crime prevention, and designated driving. Moreover, some of
these campaigns border on criminal justice, education and early childhood and adults and
children together against violence campaign, national youth anti-drug media campaign, and
voluntary ozone action program campaign.
As opined by Coffman (2002), this campaign type, employing social marketing
strategies uses public services affairs programming, radio, print, television, electronic
advertising as media vehicles to reach out to the segment of the population whose behaviour
need to change with the following campaign objectives:
1. To influence beliefs and knowledge about a behaviour and its consequences
2. Affect attitudes in support of behaviour and persuade
3. Affect perceived social norms about the acceptability of a behaviour among one’s
peers
4. Affect intensions to perform the behaviour
5. Produce behaviour change (if accompanied by supportive programme components)
Public - will campaigns are geared towards the mobilization of public action for
public change to take place. Examples of these types of campaign include: the truth
campaign/violence prevention initiative and there’s no excuse for domestic violence
campaign. This campaign type employing media advocacy, community organizing and
mobilization strategies, uses news media, print, television, radio, electronic advertising as
media vehicles to reach out to the segments of the general public that needed mobilization
with the following objectives:
1. Increase visibility of an issue and its importance.
2. Affect perceptions of social issues and who is seen as responsible
3. Increase knowledge about solutions based on who is seen as responsible

4. Affect criteria used to judge policies and policy-makers.
5. Help determine what is possible for service introduction.
6. Engage and mobilize constituencies to action (Coffman, 2002:6)
For instance, some of the studies carried out on alcohol and illicit drugs, heart disease
risk factors and cancer screening campaigns ,geared towards changes in health related
behaviours have been discovered to have produced positive results while some have not
produced outright evidence to indicate that exposure to media campaigns can produce
positive changes or prevent negative ones. (Wakefield, Loken Hornik, 2010 and Hororik
and Yanavitzky, 2003).
The aforementioned campaigns have placed messages in the media with far reaching
large audience through the aid of television, radio, billboards, posters and print media such
as newspaper and magazines. (Wakefield, Loken and Hornik, 2010),
However, such campaigns constantly compete with various hindering factors as
powerful social norms, pervasive products marketing and addictive or habitual behaviours
(Wakefield, Loken and Hornik, 2010). In other words, a positive outcome of campaigns will
only be sustained with a greater and a lasting investment to extend the effects of campaigns.
(Wakefield, Loken and Hornik, 2010).
But in the view of Hornik and Yanavitzky (2003), an effective campaign must
answer the following questions (1) what are its route of effects individual, social or
institutional? (2) What is the expected lag between initiation of campaign exposure and
effects? (3) What is the nature of expected outcomes? (4) The effects expected to vary
across sub-populations? (5) How much exposure is needed before effects can be expected?
(6) Are effects dependent on exposure across channels over time?
Explaining the above question, Hornik and Yanavitzky (2003), note that the three
ways media campaigns may influence behaviours are through audience direct exposure to
the persuasive campaign messages, behavioural change through influence from social
institution (the justice, The executive, legislative arm of government, religious organizations
and law enforcement system) whose attention have been attracted to the campaign messages
and behaviour change through social interaction with peers, family members and other
people in the community.
They however, stressed that failure to find no campaign effects can depict a true
failure of the campaign due to employment of poor behavioural objectives, poor design

messages or usually due to inadequate exposure to campaign messages. While a particular
campaign effects on behaviour can take place after some delay.
Generally, therefore, an effective campaign will anchor on the following
characteristics:
1. Capturing the attention of the right audience
2. Delivering an understandable and credible message
3. Delivering a message that influence the beliefs or understanding of the audience and
4. Creating social norms that lead toward desired outcomes (Coffman, 2002:20)
Explicitly therefore, number one characteristic entail defining the target audience,
choosing channels to get the audiences, and attracting their sufficient attention. In same
vein, number two ensures the credibility of the source, clarity of the message that is fit with
prior knowledge and the duration of exposure. Moreover, executing number three implies
providing information, directing attention of the audience engendering changes in norms
that underlie values and preferences. Finally, number four means having an understanding
of the various pressures that govern the behaviour of interest.
Magazine Campaign
Tell magazine, from available data, features breast cancer messages to aid increase
awareness and education of the disease (Shaibu, 2008, Adebayo 2010, Oyetayo 2010 and
Adebayo 2010). Numerous publications in form of articles have been featured under its
‘Health Xtra’ column. Shaibu, (2008) in her article, on ‘Tiny RNA Molecules Control
Breast Cancer’s spread’’ showed how researchers have discovered ribonucleic acid (RNA)
molecules that serve as brakes on the rapid spread of cancer to controlling cancerous cells
from traveling to the lungs and skeletal system. Another report from Adebayo (2010) on
‘Cancer Goes Commercial’ reveals the number of deaths that has been caused by both
cervical and breast cancer, and the different treatment available, but in all, recommend
prevention to be better than any cure of the disease, which according to the article, is the
most common cancer in women, with breast self examination (BSE) and mammography,
the screening tools for the disease.
Similarly, in an article titled ‘Between Early Menstruation and cancer by Adebayo
(2010), from research findings, it was discovered in 1998 and 2007 by researchers from

Clinical Endocrinology and Metabolism in the United Kingdom, that women who had their
menstruation before the age of 12 years are the ones likely to die of cancer, high blood
pressure and heart diseases before those who started later.
Newspaper Campaign
Several campaigns have been launched and started in Nigeria to expose women to all that
the killer disease entails. According to Ogbodo (2010) in her newspaper write up ‘Nigeria:
Bauchi NAWOJ begins Breast Cancer Awareness Campaign’ reports a one day cancer
programme organized by Nigeria Association of Women Journalist (NAWOJ), Bauchi State
chapter, tagged “ Breast Cancer Too Can Be Prevented” to sensitize and educate women on
the risk factors and breast Self Examination (BSE) of the disease. According to the report,
Dr John Omaga of Abubakar Tafawa Balewa Hospital Bauchi, who delivered a lecture that
day, made it known that lack of breast feeding which is one of the risk factors of breast
cancer should be discouraged, for it will go a long way to reducing cancer diseases.
Leaflet/Billboard Campaigns
In the words of the cyber source (2010:5) “Pamphlets, brochure, and posters constitute other
print media used to disseminate health messages.” These print media, according to this
source, are commonly preferred by the America Cancer Society, the American Heart
Association and the American Lung Association as educational tools to reach out to their
target audiences with maximum results.
However, the Medical Women’s Association of Nigeria (2011), Edo chapter, in their
self-sponsored effort to sensitize and educate women on breast cancer produced leaflets
titled ‘Breast Self Examination’, The leaflets which state: What breast self examination is
all about why Breast Self Examination is necessary, what breast cancer is, how breast self
examination can be done, how often breast self examination should be done, the
abnormalities one can find during self examination, the age Breast Self Examination starts,
those prone to developing breast cancer, different tests to detect the disease, and the chances
of a cure of the disease are quite limited in numbers and in far reaching of the Edo Women.
Elaborating more on the above, Dr Edith Kayode Iyasere, the President of the Medical
Women’s Association of Nigeria, Edo Chapter in a personal interview, disclosed the various

self sponsored efforts made by MWAN in creating and sustaining the knowledge of breast
cancer awareness among women in Edo State. According to her, the production of the
leaflets titled ‘Breast Self-Examination and three standard billboards displayed at king
square (Oredo Local Government), Uselu Market (Egor Local Government) and Oregbeni
Park (Ikpoba Okha Local Government) by them were expedient to educate women on how
to screen their breast by themselves because of the fundamental importance of early
detection of lump that prevents untimely deaths. [Iyesere, K.E 2011, June 18, personal
interview].
Radio, Television and Internet Campaigns
Couple with the above is the Bournvita intensive media campaign running a radio
campaign, a press campaign and national television commercials on Nigeria Television
Authority (NTA) and Channels, and advocating extensive breast screening for Nigeria
women as a way of preventing deaths related to breast cancer in the Country.
(http://businessworldng.com/web/artide&238/1/CRS).
While Kingston, (2010) acknowledges how advertising campaign on facebook has
inspired the internet users to remind them about breast cancer.

Empirical Studies
There have been numerous quantitative and qualitative studies on breast cancer awareness
campaigns in developed and less developed countries. (Sulik, 2010, King 2006, Kingston
2010, Pielle 2006, and Nazrul 2010). In Nigeria, majority of such studies have examined
women’s knowledge, attitude and practice of breast cancer (Kayode, Akande and Osagbemi
2005 and Okobia, Bunker, Okonofua and Osime 2006).
Few studies investigated strategies of media in creating awareness of breast cancer
and also on media campaign use to change health behaviours but none has measured strictly
on evaluating media campaigns on breast cancer. This study is therefore set to evaluate on a
strict basis the media campaigns on breast cancer with data from Edo women.
This research therefore reviewed foreign and local literatures related and anchoring
on the topic. Crucially, the review covered various scholarly writings and studies addressing
the research questions stated in this study. They comprise studies on women exposure to
breast cancer campaigns, the media preference, and the effectiveness of the breast cancer
campaigns messages on Edo women.
Looking at the level of exposure of women to breast cancer awareness campaigns,
Sulik (2010) in her work ‘Pink Ribbon Blues How Breast Cancer Culture Undermines
Women’s Health’ indicates high women exposure to campaigns messages. She found that
breast cancer receives much more attention than any other cancer in women’s magazines.
The increased awareness has therefore multiplied the number of the disease detected
and the number of women receiving mammogram and biopsies. This is ascertained by
Okobia, Bunker, Okonofua and Osime (2006), as they observe from available data; that
most women in the developed countries within the screening age bracket undergo routine
screening using three screening tools which are BSE, CBE and mammography. Besides,
studies have shown that the three screening methods are fundamental to facilitating early
diagnosis and treatment of breast cancer, which also engender reduced mortality ratio, are
mainly carried in numerous media campaigns in these regions (Sinhpush and Signh, 2002).
Buttressing further, Azenha, Bass, Caleffi, Smith, Pretorius, Durstine & Perez 2011,
Kamanger, Dores & Anderson, 2006 affirm that incidence of breast cancer is higher in
developed countries than less developed regions, whereas, the mortality ratio is higher in
these less developed countries. There are evident disparities in access to and quality of
information being received with screening, treatment and services being given to women of

these different regions. These advertently bring about marked differences in survival rates
between the developed and less developed worlds.
Research and report have shown that the outcome of the media campaign on breast
cancer demonstrated extremely high level of exposure among women in Western World
(Grunfeld, Ramirez, Hunter and Richards 2002 and Sinhpush & Singh 2002), However
regarding the exposure of women in less developed regions to breast cancer awareness,
Nazrul, (2010) in his work in assessing the level of ‘Awareness on breast cancer among the
women of reproductive age in Bangladesh’ found low women exposure to breast cancer
awareness campaigns. He discovered that out of 175 women in out – patient department of
Dhaka Medical College Hospital (DMCH), used for the cross sectional descriptive study,
majority did not know any information relevant to breast cancer, so they are unaware of the
risk factors, preventive measures and so on. While only 22.86% had knowledge about
screening methods, 34% of the women do not known the disease to be common among
women, and more than a three-quarter of them do not know any of the screening procedures
of breast cancer. Therefore a continuous health education programme with emphasis on
high profile media campaign nationwide need to be in place. According to him, the above
recommendation will help the women to know better about breast cancer so as to reduce the
disease burden.
Pielle (2005) in his work titled: ‘2005 Public Service Breast Cancer Awareness
Campaign Pakistan’ found low women exposure to breast cancer awareness where only
very little information on breast cancer were made available with its late presentation,
before the launching and establishment of nationwide Breast Cancer Awareness Campaign.
But with the launching of media campaigns on breast cancer in the form of press
releases, interviews, investigative news stories , through the print and electronic media,
including internet, has succeeded in causing general acceptance of the disease by the public
as part of a national agenda for women (no longer as a taboo subject).
Whereas in Nigeria, the breast cancer campaigns and the awareness level of women,
vary from community to community and from State to State. In a survey of knowledge,
attitude, and practice of BSE among female secondary school teachers in Ilorin, Nigeria,
Kayode, Akande and Osagbemi, (2005) found that, out of the 406 female teachers in Ilorin
West L.G.A. of Kwara State, 95.6% of the women were aware of BSE, having majority of
them being informed about the disease through television. However least source of

information were the health workers, while others heard from friends and from multiple
sources. It was also discovered that the attitude of the teachers to health information on BSE
was positive but it was accompanied by a low practice by 4.8% of them.
In regards to the exposure of Edo women to the breast cancer campaigns, Okobia,
Bunker okonofua and Osime, (2006), on the area of ‘Knowledge Attitude and Practice of
Nigeria Women Towards Breast Cancer: A cross sectional studies’ found low women
knowledge of breast cancer and low practice of BSE and CBE. The study indicated that
1000 community dwelling women recruited from Egor Local Government Area of Edo
State, a semi-urban community had inadequate exposure to breast cancer campings.
Osemeke, in her work on ‘Role of Radio in the creation of awareness on breast cancer:
a study of rhythm 93.7 FM Benin City, found that the breast cancer messages that are said
in the Silverbird radio and television after newscasting: ‘Remember every woman is at risk
of breast cancer, examine yourself today’, or early detection is the key to surviving breast
cancer, examine yourself today” just began in 2010. a period, considered too short to have
sensitized Edo women enough.
Moreover, the question of the media, the women are most exposed to is closely
linked with media preference. However, in addressing it as it pertains to breast cancer
campaign messages, Okobia, Bunker, Okonofua and Osime (2006) observe that women are
more exposed to television and radio as breast cancer information source. Regarding the
media preference as it is highly called; scholars and researchers believe an audience can
prefer one medium to the others due to the following contributory factors: the characteristics
of the various mass media, the socio-psychological dispositions of the audience, the
audience literacy level and the level of socio-economic status of the audience.
Looking at the characteristics of television as it pertains to media preference’
Ibagere, (2009) in his book on Social Development, Television and Politics in Nigeria’,
acknowledges the allure inherent in the blend of pictures and colours in television, coupled
with the power to attract, capture, retain and direct audience attention to issues considered
more important by the way these issues are prominently featured on the television. These
features invariably promote the level of confidence and trust the audience place on it while
these give credence to the medium of being capable of delivering health education
messages.

In reaction to the above view, a cyber source (2010) condemns the influence of
television in promoting false norms of violence, drinking, smoking and sexual behaviour,
While its coverage of health issues reveals the weakness, as a health educator, where health
segments incorporated into news broadcasts, last only one to three minutes, leaving the
audience with only a brief report or sound bite. Stressing further the source highlights
involvement in the televised health messages.
The cyber source (2011) however, acknowledges television as a powerful appealing
medium, that reaches the audience irrespective of age, sex, income or educational level,
with the blend of sight and sound features that produce dramatic and life-like
representations of people and products (Russell, 2007).
Media preference as it regards audience literacy level indicates that the literate
audience extensively engages their time and interest in television than in other media.
Available data have shown that newspaper gives detailed information on issues unlike the
broadcast media. A study on the use of mass media to deliver health information by a cyber
source (2010) captioned ‘Encyclopedia of public health: mass media’ affirms that
newspaper permit a level of detail in health reporting that is not feasible with broadcast
media. According to this source, a miss of a television broadcast about breast cancer means
a lost to its entire messages, but a newspaper consumer can avail himself of the same
information in a newspaper, but in a detailed form. In addition to the above potential
strengths of newspaper, are the possession of consumers’ flexibility, in terms of what the
audience read and when, as well as its brief shelf life, and the media reach of health issues
to and diverse people (Russell, 2007).
Considering the above attributes, researchers affirm that newspaper has the potential
to deliver health messages. But in the other hand, Soola, (2009) in his work
‘Communication and educational approaches and strategies for effective environmental
awareness’, states the limited rural media reach peculiar with newspaper consumption in
developing country as Nigeria, where most of the population are rural dwellers, (mostly
illiterate) and therefore not among the elite groups. He however notes the literate upgrading
of the consumers, in their local language, (not English language) that carries more than 70%
of information published.
Highlighting the several attributes of a magazine and why health messages like breast
cancer can receive repeated exposure, a cyber source, (2010), notes the strengths of a

magazine to include: reproduction quality, audience selectivity, prestige, reader loyalty and
a relatively long shelf life.
Furthermore, the preference of outdoor media in dissemination of health messages is
consequent on the several potential strengths. For instance, researchers believe that these
media provide repeated exposure to messages for passersby and public transport users.
Available data have shown that tobacco and alcohol producers have made extensive use of
these media. Examples are billboards, signs, placards, flying billboards, blimps and
skywriting. (Russell, 2007).
Similarly radio preference in the broadcasting of health message campaigns has been
affirmed by researchers to have been effective in developing countries especially when
combined with other mass media. Some research findings on media preference or
acceptability posit that radio is considered more efficient than TV, considering the
cheapness of the placement and production cost, the requirement of greater audience
involvement and the power of mental image creation capable of reinforcing complementary
messages portrayed on TV. (Russell, 2007).
Supporting the above view, Nigerian media scholars, described radio as the cheapest,
most portable and simplest medium of mass communication and the most effective, and
pervasive medium reaching the country remotest heterogeneous audiences. In furtherance of
the above, Soola (2009) buttresses the unlimited nature of radio in a country where
electricity supply is quite epileptic and rare to come by, and its mobility potentials in being
used in offices, homes and vehicles.
Reports from available research studies, according to Anyaegbudike (2005) in his
work titled “The impact of HIV/AIDS campaigns on audience behavioural changes”
conducted by the 2003 national HIV/AIDS and reproductive health survey, indicated high
radio preference for communicating HIV/AIDS messages to the audience than for television
and print media. Moreover, the survey also found that rural dwellers less accepted television
and print media while print media are considered by the less educated ones as the least
preferred media of communicating HIV/AIDS messages.
The available data also disclosed high radio ownership and consumption (50 percent)
than television ownership and consumption (28 percent). The researchers therefore tended
to agree that radio is preferred because it transcends boundaries, illiteracy, economy

downturn, and the likes of them in Nigeria (Anyaegbudike, 2005). Radio is therefore a
veritable tool for campaigning in a developing country such as Nigeria.
On the effectiveness of the breast cancer campaign messages in achieving a quick
and prompt compliance from women, several studies measuring on the effectiveness of
different conducted media campaigns have been reviewed to indicate varied findings.
The review of various media campaigns on health related behaviours have shown
that tobacco, alcohol and illicit drugs studies indicated reductions in adult smoking and
decline in young people smoking though with a support of taxation and smoke free policies
(Wakefield, Loken and Hornick, 2010). Moreover, findings from cancer screening and
prevention studies revealed increased access to screening services, but with a media support
of reminder letters. (Wakefield, Loken and Hornick 2010).
Wakefield, Loken and Hornik, (2010) in their work on the ‘Use’ of Mass Media
Campaigns to change Health ‘Behaviour, found that mass media campaigns can directly and
indirectly engender positive changes or prevent negative ones in health related behaviours
across extensive populations.
However, their analytical review on the outcomes of media campaigns in regards to
various health risk behaviours such as heart disease risk factors, tobacco, alcohol and illicit
drugs, sex-related behaviours, road safety, cancer screening and prevention, child survival
and so on, revealed various conditions for an effective media campaigns and various factors
to the failure of media campaigns.
These conditions according to Keller and Armstrong (2009) substantially entail the
application of several interventions on the episodic behaviour (e.g screening, vaccination,
children’s asprin use) and not on habitual or ongoing behaviour (e.g food, choices, sun
exposure, physical activate).
Finally, findings from Bottoff, Mckeown, Carey, Haines, Okoli, Johnson, Easley,
Ferrence, Baillie and Ptolemy’s (2010) research study on young women’s responses to
smoking and breast cancer risk information; revealed women high exposure to breast cancer
risk factors found to include their personal susceptibility and tobacco smoking. This
therefore has established their personal connection to the breast cancer risk factors and
overcome tobacco desensitization related messages.

2.3 Theoretical Framework
Evaluation of media campaigns on breast cancer based on theories and models
They are: Transthearetical model of Behaviour change (stages of change model),
Health Belief model Agenda Setting Theory, Framing theory, Priming theory.
Health Belief Model
This model by Becker and Maiman, 1975, Rosenstock, 1974 in ORCMacro/ APCO, (2004),
has been adopted by a number of public health campaigns and is therefore pertinent to this
research work.
It states that individuals have the likelihood to adopt preventive behaviours when
they believe that:
1. They are susceptible to the potential problem.
2. The problem has serious consequences.
3. There are few barriers to taking the preventive action.
4. The preventive action will be effective in minimizing the risk and
5. They are capable of performing and maintaining the behaviour as is needed to obtain
the desired effect.
Certainly, with above points, the people will have more tendencies to adopt the
preventive behaviour. (Coffman, 2002 and ORC Macro.APCO, 2006). It then follows that
Edo women have the likelihood to adhere to early presentation of breast cancer to avert
deaths, if they believe that:
1. They are individually threatened to contract breast cancer.
2. That late presentation of breast cancer amounts to untimely death of the patient.
3. That practicing the entire screening test would not be difficult or problematic.
4. That adhering to the screening exercise would be helpful in detecting early breast
cancer.
5. That they are capable of carrying out all the examinations required to survive the
disease.
Agenda Setting Theory
Agenda setting theory as propounded by Mc- combs and Shaw 1973 posits that the mass
media do not instruct what people think but what they should think about.

Due to their gate keeping function, they determine and direct public attention to
issues considered more important, by the emphasis and prominence given to the issues in
the media. It is to this end that the theory maintains that the issue or message that constantly
features in the media becomes the public agenda of the people. (Coffman, 2002). The theory
becomes apt to this study due to the critical nature of breast cancer that needs a quick and
prompt adherence and action from the women to always examine themselves for early
detectation that aids prevention and reduction of untimely deaths.
Therefore, the mass media should through breast cancer campaigns frequently and
unyieldingly give prominence to breast cancer issues and programmes so that the reality of
the risk associated with the disease will be drummed into the ears and consciousness of
woman to complying totally.
Transtheoretical Model of Behaviour Change - (Stages of change model)
(Prochaska, Diclemente, and Norcross, 1992). This model identifies five stages, individuals
go through on the way to attempt, make or sustain behaviour change. Behaviour change is
therefore regarded as a sequence of events and actions, where varying degrees of motivation
and participation of target audience through the five stages need different messages and
interventions to get them to change their behaviours. The five stages are: precontemplation,
contemplation, preparation, action and maintainance, (ORCMacro/ APCO, 2006 and
Coffman, 2002).
Therefore different persuasive media programmes on breast cancer should be
packaged and featured constantly at different quarters of the campaign period to involve and
motivate the women from the first stage down to the last stage of behaviour change.
Framing (Tversky and Kahneman, 1981)
Framing theory focuses on how media organization design and package information or
messages about issues to influence or change the perception of the receivers concerning the
particular message. (Coffman, 2002 and Ibagere, 2009). Media campaign organization
should therefore use framing theory to design and package the breast cancer programmes
disseminated to the Edo women. In other words, the construct of the languages and visuals

used should be designed to be properly interpreted and understood by the woman to
avoiding late presentation of the disease. Priming (Iyengar and Kinder, 1987)
This theory is based on the assumption that individuals do not have enough knowledge
about many things, while the ones known are not employed in decision making process.
Priming theory is therefore putting a deliberately focus on particular issues and neglects of
others so as to alter individuals’ standard of evaluating people, issues or other things.
(Coffman, 2006 and Ibagere, 2009). This theory becomes apt to this study considering the
increase in the mortality rate of Edo women with low awareness level of breast cancer
campaigns presently going on in Edo State. The mass media should therefore deliberately
play up varieties of breast cancer messages, to down play campaigns on other diseases to
elicit compliance to early presentation of breast cancer to the reduction its mortality rates.

REFERENCES
Adebayo, F. (2010 April). Cancer goes commercial. Tell magazine, pp 12.
Adebayo, F. (2010 February). Between early menstruation and cancer. Tell magazine,pp
13.
America Cancer Society (2007) Breast cancer facts and figures. Atlanta: ACS, Inc.
Anyaegbudike, V. (2005) The impact of HIV/AIDS campaigns on audience behavioural
changes. An unpublished project work of the department of mass communication.
University of Nigeria Nsukka.
Azenha, G., Bass, L.p., Caleffi, M., Smith, R., Pretorius, L., Durstine, A. and C.P.
(2011) The role of breast cancer civil society in different resources settings.
www.elsevier.com/brst.
Becker, M.H. (ed) (1974) The health belief model and personal health behaviour.
Thorofare, NJ: Charles B. Slack.
Blugs, W.S., Cummungs, M.r., Spencer, C.A. and Palladino, M.A. (2009)
concepts of genetics. America: Pearson Prentice Hall.
Bottoff, J., Mckcown, S.B., Grey, J., Haines, R., Okoli, C., Johnson, K.C., Easley, J.,
Ferrence., B., Baillie, L., and Ptolemy E. (2010) Young women’s response to smoking
and breast cancer risk information. Oxford Journal Medicine, 25, 668 677.
Breast Without Spot Initiative (BWS)
http://www.internationalcancerweekinitiative.com/index.php?
Buffetla, P. Hashibe, M., La Vecchia C., Zatonski, W. and Rehm, J. (2006) The burden of
cancer attributes to alcohol drinking. International Journal of cancer, 119(4) 884-7.
Cadbury Bournvita pushes the envelop against breast cancer
http://businessworldng.com/web/articles/238/1/CRS
Coffman, J. (2002) public communications campaign evaluation: An environment scan
challenges, criticism, practice and opportunities. Cambridge, M.A family Research
project. Retrieved from www.thelancet.com.
Dumitrescu, G. and Cotaria, I (2004) Understanding breast cancer risk: Where do we stand?
Journal of cell molecular medicine, 9(11), 208-11.
Gallagher, K.M., Updegraff, J.A., Rothman, A.J, and Sims L. (2011) perceived
susceptibility moderates framed messages. Retrieved 26 Feb. 2011.
Grunfeld, E.A., Ramirez, A.J., Hunter M.S. and Richards, M.A. (2002). Women’s
knowledge and beliefs regarding breast cancer. Breast Cancer Journal 86: 1373-1378.

Hormik, R.C., and Yanovitzky, I. (2003) Using theory to design evaluations of
communication campaigns: the case of the national youth anti-drug media campaign.
From http://repository.upenn.edu/asc.papers/a8.
http://EzinneArticle.com/?export=Micheal
Humphrey, L.L., Helfand, M., Chan, B.K.S and Woolf S.H. (2002) breast cancer Igbare, E.
(2009) social Development, Television and politics in Nigeria. Ibadan: Kraft Books
limited.
Joanneum Research, Nielsen media Research, University of Shelfield, Ontotext lab.
University of Twente, HS-ART Softeco Sismat and TNO Netherlands (2009) Media
Campaign.http://blog.thoughpick.com/2009/06/10-social-campaigns-that-rock-learn-
how-to-do-the-game.html//more877.
Kahneman, D and Tversky, A. (1979)prospect theory: an analysis of decision under risk.
Econometrica, 47,263-291.
Kamangar, F. Dores, G.M. and Anderson, W.F. 92006 patterns of cancer incidence,
mortality and prevalence across five continents: defining priorities to reduce cancer
disparities in different geographic regions of the world. Journal of clinical Oncology.
24:2137-50
Kayoed, F.O., Akande, T.M. and Osagbemi, G.k. (2005). Knowledge, attitude and practice
of breast self examination among female secondary school teachers in Ilorin, Nigeria.
European Journal of Scientific Research, PP 42.
King, S., (2006). Pink Ribbons Inc: breast cancer and the politics of philanthropy.
Minneapolis?: University of Minnesota Press.
Kingston, A. (2010) A nice rack of slogan. Maclean’s 123(41) 73
http://www.worldcat.org/issn/0024-9262.
Kotter, P. and Armstrong, G., (2009) principles of marketing, (13th
ed) Upper Saddle, River,
NJ: Prentice Hall.
Iyasere, K.E., (2011,june 18) {personal interview}.
McCombs and Shaw, D.L (1973) The agenda-setting function of the mass media. Public
opinion Quarterly, 37,63-75.
Medical Women Association of Nigeria, Edo State. (2011) Breast self examination. Edo
state: medical women association of Nigeria.
Nazrul, M.O. (2010). Awareness on breast cancer among the women of reproductive age in
Bangladesh. Retrieved on 26 Feb., 2011.
Ogbodo, P. (2010, November 11). Nigeria: Bauchi Awol begins breast cancer awareness
campaign. Daily Independent, P.
Okobia, M.N., Bunker C.H., and Osime, U. (2006) Knowledge, attitude and practice of
Nigeria women towards breast cancer, a cross sectional study. Retrieved from
http://creativecommons.org/licenses/by/120
Olson, J.S. (2002). Bathsheba’s breast: Women, Cancer and History. Baltimore: The John
Hopkins University Press.
ORCMacro and APCO (2004). Theoretical framework multi-year mass media campaign
plan. Retrieved on 26 Feb., 2011.
Osemeke, I.T., (2011) Role of radio in the creation of awareness on breast cancer: A study
of Rhythm 93.7 fm. Benin-City. An unpublished project work of the department of mass
communication. Benson Idahosa University, Benin-City Ed. State.
Oyetayo, A. (2010 April). Prevention is better than cancer. Tell magazine, pp 12.
Parkin, D.M., Bray, F., Ferlay, J. and Pisani, P. (2005) Global Cancer Statistics. 2005. CA:
A Cancer Journal for Clinicians, 55(2), 74-108.
Pielle, (2005). Public Service: breast cancer awareness campaigns – Pakistan. Retrieved 26
Feb., 2011.
Prochaska, J.O., Diclemente, C.C., and Norcross, J.C. (1992) In search of how people
change: Applications to addictive behaviour. American psychologist, 47, 1102-1114.
Rimal, R.N. (2000). Closing the knowledge-behaviour gap in health promotion: The
mediating roles of self-efficacy. Health Communication, 12(3), 219-237.
Shaibu, R. (2008 February). Tiny RNA molecules control breast cancer’s spread. Tell
magazine, p 13.
Siahpush, M. and Singhm, G.K. (2002). Sociodemagraphic predictors of pap test receipt,
currency and knowledge among Australian women. 35:362-368.
Soola, E.O. (2009). Communication and educational approaches and strategies for effective
environmental awareness. European Journal of Social Sciences, 9(1), 15-28.
Stober, C., (Newscaster). (2011 Feb., 4). 9pm Network news. Abuja: Nigeria.
Sulik, G. (2010). Pink Ribbon Blues: How breast cancer culture undermine women’s
health. New York Oxford University press.
Wakefield, M.A., Loken, B. and Hornik, R.C. (2010). Use of mass media campaigns to
change health behavior. Retrieved on 26 Feb., 2011.
WHO/UICC (2005) Global action against cancer. New Switzerland: WHO/UICC.
Wikipedia (2011) Breast cancer awareness www.wikipedia.com.
CHAPTER THREE:
METHODOLOGY

3.1 Research Design
The study utilized the survey method. Survey research design, scientifically samples
and interviews people to analyze and report what they said. Ohaja (2003) avers that survey
is usually employed in studies of attitudinal and behavioral trends with the researcher
seeking to uncover their demographic psychological underpinnings.
3.2 Population of Study
For the purpose of this study, the target population was the adult females in Edo
State. Edo state consist of three senatorial districts namely: Edo-South, Edo-Central and
Edo- North Senatorial districts. But, because of the large size of Edo State population, the
researcher covered only the Benin metropolis (which is among the Edo–South senatorial
district) because of the impossibility to cover the whole state.
Due to the large size Benin metropolis, consisting of three local governments areas
namely Oredo, Egor and Ikpoba-Okha, the researcher narrowed it down to Oredo
municipality that comprised of 185, 620 females and 12 wards (source National Population
Commission, 2006). The population of the study was therefore 185, 620 females in Oredo
municipality.
The above choice of population sufficed for the purpose of this study because the 12
wards in the Oredo local government area are the interplay of the very urban, the semi-
urban and the rural dwellers. These mixtures therefore engendered and ensured a
comprehensive and balance data from women, with a true picture and state of media
campaigns on breast cancer in the state, portrayed.
3.3 Sample Size
The sample size of this study was 400 women from Oredo local government area. The
sample size was determined by Taro Yamane formula as stated in Ogbuoshi (2006:85) as

n = __N_____
1 + N (e) 2
.
Where ‘n’ stands for the desired sample size, ‘N’ stands for the population under
study, ‘e’ stands for the limit of tolerable error assumed to be 5% or 0.05, and ‘1’ for the
unity in value which is always constant. (Ogbuoshi, 2006). With stated formula, the above
sample size is thus derived as follows:
n = ____N______
1 +N (e) 2
n = 185, 620______
1+185, 620 X 0.052
BODMAS
= 185, 621X0.052
= 185, 621X0.0025
= 185, 620
464.0525
= 399.99
= 400 (approximately)
:. n = 400 (desired sample size)
3.4 Sampling Technique
The study employed systematic sampling of non-probability sampling method. The
sampling technique was chosen by the researcher because of its aptness in the division of
the Oredo municipality into 12 wards. That is, with the distribution pattern of the 12 wards
into streets / villages, the researcher observered every 1st and 10
th street that make up each
ward. In other words, the technique was to ensure that every 1st and 10
th street were
administered with questionnaire. The wards with their grouped streets/villages are shown
below:
Ward 1
A) Adesogbe road
B) Ekenwan road
C) Goodwill street
D) Obakhavbaye street
E) Asemota street
F) Oba market / urhokpota / oredo secretariat premisises
G) Adesogbe / plymouth road
H) Ring road axis
I) Airport road
J) Akenzua road
K) Stadium road
L) Asabo / osagiede uzzi street
Ward 2: Basically Rural Settlements
A) Amagba village
B) Evbhorhunmwon village
C) Ugbor village
D) Egbire village
E) Obazagbon village
F) Okhoromi village
G) Urogbeni village
H) Emwiniyomwanru village
I) Umegbe village
J) Iguekpe village
K) Ikpebo village
L) Aibangee village
M) Irhirhi village
N) Irhue village
O) Okhue village

P) Irhue n’owina village
Q) Igogogin village
R) Akwakwari village
S) Uregbin village
T) Ogiza village
U) Evhuokhae village
V) Evbirodia village
W) Ugiokhuen community
X) Enamuma village
Y) Utagban village
Z) Evbuowe village
A) Ekae village
B) Boundary road
C) Red cross / afe close g.r.a
D) Ikpokpan road / delta crescent
E) Ihama road
F) Eghosa crescent g.r.a
G) Biu / ugiokhan road
H) Ogbetuo avenue g.r.a
I) Sapele road
J) Odba road
K) Jemide avenue g.r.a
L) Evbuomwan avenue
M) Emakpae / ogunbor street
N) Akhionbare street g.r.a
O) ugbor / benson idahosa boulevard, g.r.a
P) Guobadia street
Ward 3
A) Eghosa street, uzebu quarters
B) Oliha market axis
C) Owegie primary school
D) Owina street

E) Osa street
F) Ekenwan road ( between eharkpen / agbonma junction )
G) Agho street
H) Iyeye street
I) Osama lane
J) Utomwen street
Ward 4
A) Evbiemwen lane
B) Emokpae primary school &mission road environs
C) Iguisi street
D) Lagos street
Ward 5
A) Ihogbe / ire junction
B) Usama ground
C) Uwa market
D) Nosayaba street
E) Agadagudu street
F) Iyase street
G) Osuma lane
H) 2nd west circular road
I) Oghenosa street
J) Akugbe street, off west circular
Ward 6
A) Emwanta street
B) Lovely street
C) Iheya street
D) Utomwen street
E) Lawani street
F) Owoseni street
Ward 7
A) Umagbe street, off upper mission
B) New benin axis and environs (akugbe street)

C) Edokpolor grammar school
D) Upper lawani street
E) Guobadia street
F) Emokpae street
G) Ogunbor street
H) Edokpolor street
I) Okaeben street
J) Chief alonge avenue
K) Aluyi street
L) Ewah road
Ward 8
A) Ofumwengbe street, igun junction by 2nd
east circular road
B) Ogiso market and environs
C) 1st cementary axis & 2
nd east circular road environ
D) Upper nohuwa street
E) Esigie street
F) Agbonmoba street
Ward 9
A) Ewasede Street / Apostolic Street
B) Agbado market axis
C) Igun street (agbado axis)
D) Eki street
E) Agbado street
F) Ikpema street
G) Arousa street
Ward 10
A) Sakponba road (ohuoba street axis)
B) Owina street (sakponba road axis)
C) 1nd
east circular road (sakponba road axis)
D) Umuaru quarters
E) Awo street
F) Emele street

G) Oza street
H) 2nd east circular road between sakponba / akpakpava road
I) 1st east circular road between sakponba / akpakpava road
J) Asoro street
K) Africa church road
Ward 11
A) Ikpokpan street between sapele road and 2nd
east circular
B) Ekhiosa axis
C) Oguola market and environs (upper uwa street)
D) Evbarunegbeifo street by 2nd
east circular road
E) 2nd
east circular road (sakponba road axis)
F) Awo street
G) Sakponba road (between 1st and 3
rd junction)
H) Sapele road (between 3rd
and ogbalaka)
I) Ofunmwegbe street
Ward 12
A) Lagos street
B) Iwegie street axis
C) Forestry road
D) Akpakpava road
E) Mission road
F) Iriemila street
G) Cooke road
H) Ring road(mission road axis)
Therefore based on the number of the sample size (400) 14 questionnaire each, were
randomly administered to the women in all the 1st and 10
th street of these wards. The simple
random sampling technique employed here, was to ensure that every woman stands an equal
chance of being represented.
However the systematic observation of the 1st and 10
th street of the entire 12 wards
with 14 questionnaire each, gave ward 1(which comprise 12 streets) 3 streets with a total

number of 42 questionnaire administered to the women in the 3 streets. It gave ward 2
(which comprise 42 streets) 9 streets, with a total of 126 questionnaire administered in the 9
streets. It gave ward 3 (which comprise 10 streets) 2 streets, with a total of 28 questionnaire
distributed. Ward 4 (with 4 streets) got 1 street that was administered with14 questionnaire.
Ward 5 (10 streets) got 2 streets that were administered with 28 questionnaire. Ward 6 (6
streets) got 1 street that were administered with 14 questionnaire. Ward 7 (12 streets) got 3
streets that were administered with 42 questionnaire. Ward 8 (6 streets) got 1 street that was
distributed with 14 questionnaire. Ward 9 (7 streets) got 1 street that was distributed with 14
questionnaire. Ward 10 (11 streets) got 3 streets that were administered with 42
questionnaire. Ward 11 (9 streets) got 1 street that were administered with 14 questionnaire.
Finally ward 12 (8 streets) which got 1 street as well, was administered with 14
questionnaire but with an addition of 8 remaining questionnaire which made it a total of 22
questionnaire.
Summary of the above on table
Wards
No.of Str according to systematic
Observation of the 1st and 10
th
street of each ward
Total No. of questionnaire
administered according to the
systematic No. of street
1:12 streets 3 42
2:42 streets 9 126
3:10 streets 2 28
4:4 streets 1 14
5:10 streets 2 28
6:6 streets 1 14
7:12 streets 3 42
8:6 streets 1 14
9:7 streets 1 14
10:11 streets 3 42
11:9 streets 1 14

12:8 streets 1 14 + 8 = 22
Total-137 street 400
3.5 Measuring Instrument
The researcher employed the primary source of data collection, which were the use of a
questionnaire, personal /group interviews, discussions etc
3.6 Validity and Reliability of the research Instrument
Reliability and validity are similar and very relevant in carrying out research works.
Reliability is the need to ensure that the measuring instruments for data collection are
reliable and data obtained are able to bring about objective interpretation of results.
Therefore to ensure the validity and reliability of this study, the researcher first
embarked on a pilot test with administration of 30 copies of the questionnaire to women in
Irhirhi village and women lecturer in Benson Idahosa University (BIU) in ward 2. The
project supervisor also made corrections on the instrument before the researcher embarked
on the final distributed of the questionnaire to the actual sample respondents
3.7 Method of Data Analysis
Tables and simple percentages were used by the researcher in analyzing the data collated
from the questionnaire copies that were administered to the women in Oredo Local
Government Area in Benin metropolis of Edo State. The researcher also presented her
findings using statistical means of presentations which included Pie Charts and Bar Charts.
3.8 Limitations of Methodology
The researcher was not able to cover beyond the research topic. Due to the large size of the
population of the women in Edo State, covering the whole women in the State was not
possible; therefore, the researcher limited herself to the women in Oredo local Government
area of the state.

REFERENCES
Ogbuoshi, L.I (2006). Understanding research methods and thesis
writing. Enugu: Linco Publishers.
Ohaja, E.U (2003). Mass communication research project report writing.
Lagos: John Letterman Ltd.
Commonwealth Africa communication (2006).Landmark achievements of Oredo local
government council under the leadership of Victor Edos Ebomoyi(May 2004-December
2006)Benin-city: Commonwealth Africa Communication
CHAPTER FOUR

DATA ANALYSIS AND PRESENTATION
4.1 Description of the Sample
The sample was drawn to consist of all adult females in Edo state. The 400 sample was
drawn from urban, semi-urban and rural dwelling women of oredo local government area of
Edo state which is made up of 185, 620 females with 12 wards. (national population
commission). From the 12 wards, responses were systematically and randomly gathered
from Adesogbe road, Akenzua road, Stadium road, Amagba village, Iguekpe village, Ikpebo
village, Ogiza village, Evhuokhae village Ikpokpan/delta crescent, Ihama road Akhionbare
street G.R.A, Ugbor, Benson Idahosa boulevard, G.R.A., Eghosa street, Uzebu quarters,
Utomwen street, Evbiemwen lane, hogbe/ire junction, Akugbe street off west circular,
Emwanta street, Umagbe street off upper mission, Chief Alonge avenue, Aluyi street,
Ofumwengbe street, Igun junction by 2nd
east circular road, Ewasede street/Apostolic street,
Sakponba road (Ohuoba street axis), Asoro street, Africa church road, Ikpokpan street
between Sapele road and 2nd
East circular and Lagos street with observations of the 1st and
10th
street of the 12 wards.
The sample provided information on demographic data on variables like age, marital
status, educational status and occupational status which proved significant relationship to
the level of the women’s exposure to media campaigns on breast cancer and the level of
their compliance to early presentation of breast cancer through the practice of Breast Self
Examination (BSE) and Clinical Breast Examination (CBE) to the reduction of breast
cancer mortality.
A majority of the sample were found to be in their susceptible age range of
contracting the disease as 110 (28%) and 162 (42%) fell within the age bracket of 26-35 and
36-45 respectively. The above groups of women served for the target group for the
evaluation of media campaigns on breast cancer.
More than half of the women (296 or 76%) in table 2 were found to be married while
majority of the sample were educationally backward as shown in table 3. However,
fundamental relationship has been discovered in this study to exist between level of the
women’s education and that of their media preference or exposure to breast cancer
campaigns and their adherence to practicing of BSE and CBE. Therefore, table 3 revealed
the low educational status of the sample as 104 out of 388 women had primary six

education, 108 women had secondary school education and 24 women had no education.
Therefore low breast cancer exposure and compliance were found to be linked to low
educational attainment among the women.
Largest proportion of the sample, as shown in table 4, was found to be engaged in
low occupational status. These were seen in the number of women engaged in petty trading
(168 or 43%) and the number that were in business class (82 or 21%) while 35 of them were
engaged in small scale farming. Irrespective of the civil/public servants (91 or 24%) and
professionals (12 or 3%) among the 388 women, the findings buttressed the fact that the
sample’s low occupational status was consequent on their level of education. This
notwithstanding, result obtained proved that the women’s occupation was related to the
level of their compliance as majority of the women who engaged in the lower occupational
cadre were among the respondents found with low and inadequate exposure to breast cancer
campaigns. This was evident from some of the reasons advanced by the women for not
participating in the practice of BSE and CBE which discourages early presentation of breast
cancer and prevention of its mortality rates. According to the women, the busy nature of
their businesses, that is lack of ample time and lack of adequate knowledge and information
on breast cancer, contributed to their poor performance of BSE and CBE.
4.2 Data Presentation and Analysis
The presentation began with the demographic and psychographic characteristics of the
respondents. The study presented four demographic data comprising age range, marital
status, educational qualifications and occupation and twenty four psychographic questions
in the questionnaire. The exercise is however presented below with appropriate tables and
percentages, pie charts and bar charts.

Table 1: Age Distribution of the Respondents
RANGE IN YEARS FREQUENCY PERCENTAGE
18 – 25
26 – 35
36 – 45
46 and above
22
110
162
94
6
28
42
24
TOTAL 388 100
Bar Graph and Pie Chart Showing Age Range of Respondents
Table 1 shows the age distribution of respondents according to their age brackets.
The result indicates that 22 out of 388 respondents fell within the age bracket of 18 – 25
years, 110 respondents representing 28% of the study population were in the age bracket of

26 – 35, while 162 or 42% respondents were in the range of 36 – 45, with the 94 or 24 % of
the respondents within the bracket of 46 years and above. The above distribution
significantly portrayed that the target audience of breast cancer campaign fell within the
susceptible age of breast cancer.
Table 2: Marital Status of Respondents
Marital Status Frequency Percentage
Single
Married
Divorced
Widowed
72
296
0
20
19
76
0
5
Total 388 100

Bar Graph and Pie Chart Showing Marital Status of Respondents
Table 2 shows the marital status of the women. It indicates that most of the women,
constituting 296 in number or 76% of the sample size were married, while 72 or 19% of
women were single. No respondent was divorced but 20 or 5% of them were widowed. The
above table also showed that the married women who constituted the largest number formed
a major target audience of breast cancer campaign.
TABLE 3: Educational Qualification of Respondents
Education qualification Frequency Percentage
No Education
Primary Six
WAEC/GCE
OND/NCE
HND/BSC/BA
MSC/MA
PHD and above
24
104
108
66
62
18
6
6
27
28
17
16
5
1
TOTAL 388 100

Bar Graph and Pie Chart Showing Educational Status of Respondents
The above table shows the educational distribution of respondents. The result
indicates that only 6 respondents had PHD and above while 24 had no education. A great
number of respondents totaling 104 and 108 respectively had primary six and WAEC/GCE
while 66 respondents had OND/NCE. The remaining 62 had HND/BSC/BA with 18
respondents obtaining MSC/MA qualifications.

TABLE 4: Occupational Distribution of Respondents
Occupation Frequency Percentage
Farmers
Traders
Business women
Civil/public servants
Professionals
35
168
82
91
12
9
43
21
24
3
Total 388 100
Bar Graph and Pie Chart showing Occupational Status of Respondents
As shown in Table 4, 9% of the respondents were farmers, about 43% or 168 out of
388 respondents belonged to the group of petty traders and 82 or 21% of respondents
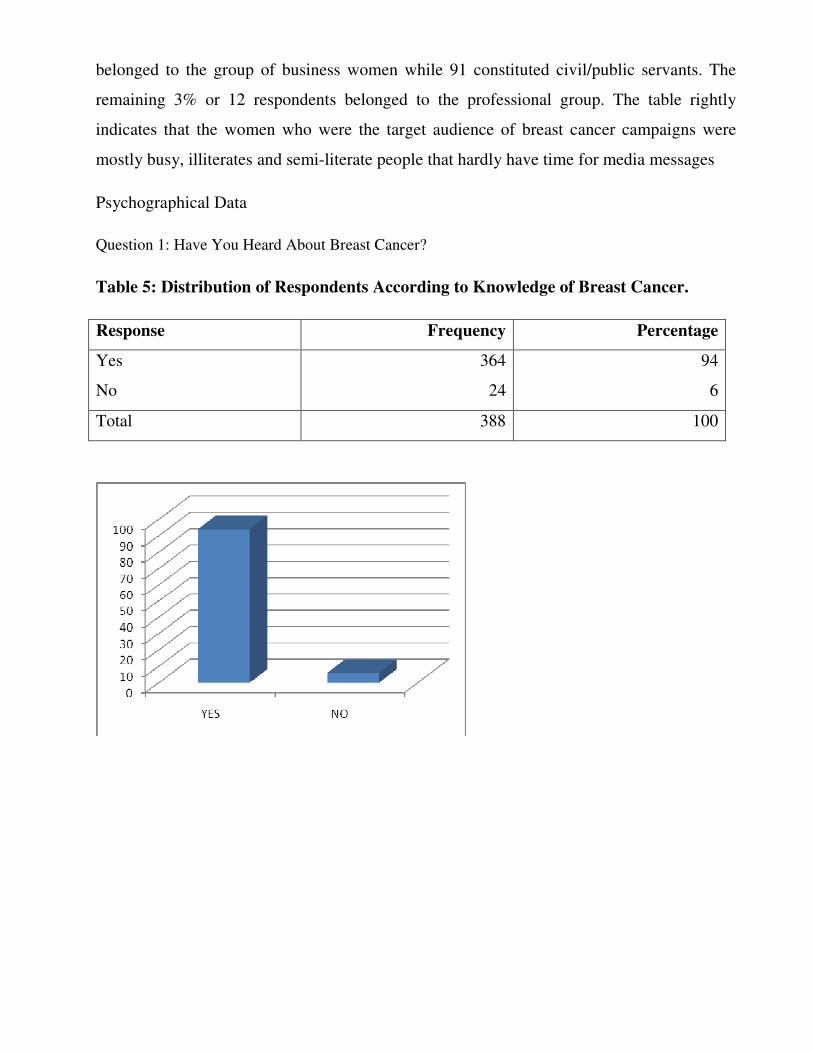
belonged to the group of business women while 91 constituted civil/public servants. The
remaining 3% or 12 respondents belonged to the professional group. The table rightly
indicates that the women who were the target audience of breast cancer campaigns were
mostly busy, illiterates and semi-literate people that hardly have time for media messages
Psychographical Data
Question 1: Have You Heard About Breast Cancer?
Table 5: Distribution of Respondents According to Knowledge of Breast Cancer.
Response Frequency Percentage
Yes
No
364
24
94
6
Total 388 100

Bar Graph and Pie Chart Showing Knowledge of Breast Cancer by Respondents
The table above shows the distribution of respondents on their knowledge of breast
cancer. The figures indicate that majority of the women had knowledge of breast cancer as
364 out of 388 women agreed they have heard about breast cancer while only 6% or 24
respondents had no knowledge of the disease.
Question 2: From Where Did You Hear About Breast Cancer?
TABLE 6: Source of Breast Cancer Knowledge
Response Frequency Percentage
Mass media
People
All of the above
None of the above
34
40
290
24
9
10
75
6
Total 388 100

Bar Graph and Pie Chart Showing Source of Knowledge by Respondents
The table shows the responses of the respondents on the source of breast cancer
knowledge. The result indicates that majority of the respondents source of information on
breast cancer were both from mass media and people as 75% or 290 respondents responded
to “all of the above” while 9% or 34 respondent acknowledged only mass media as their
source of information on breast cancer. The remaining 40 out of 388 respondent or 10% of
the study population acknowledged “people” as their source of information on breast
cancer. But 24 respondents, who did not respond, belonged to the group of people who have
no knowledge of the disease.
Question 3: If the answer to number 2 is mass media, then which of the media is your major
source of breast cancer knowledge?

Table 7: Distribution of Respondents According to Major Source of Breast Cancer
Knowledge
Response Frequency Percentage
Radio Nig. Benin, ITV,
EBS, Raypower, Silverbird
Radio
180
46
NTA Benin, ITV, EBS,
STV, AIT Television.
120
33
Observer, Vanguard, Punch,
Guardian, Tribune, The
Nation.
16
4
Tell, Newswatch, This
week, Source, Insider,
South South, The News
0
0
Breast cancer leaflets 0 0
Breast cancer
Billboards/posters
0 0
Internet 0 0 Total 388 100

Bar Graph and Pie Chart Showing Respondents Major Source of Breast Cancer
Knowledge
The table above displays the responses of the respondents according to the mass
medium that serve as their major source of information on breast cancer. The result
indicates that a greater number of respondents 180 or 46% indicated mainly Silverbird, ITV
and EBS radio as their major source of breast cancer messages, while 128 or 33% indicated
STV, ITV, and EBS television, The Nation and Guardian newspapers had 16 or 4% of the
responses and 64 respondents did not respond. However, none responded to Tell,
Newswatch, South South, Thisweek, etc magazine, breast cancer billboards/posters, breast
cancer leaflets and Internet.
Question 4: For How Long Have You Received Information About Breast Cancer From the
Mass Media ?
Table 8: Distribution of Respondents According To Extent of Information Received on
Breast Cancer.
Response Frequency Percentage
6 months
One year
Two years
Three years
Above three years
22
50
22
16
214
6
13
6
4
55
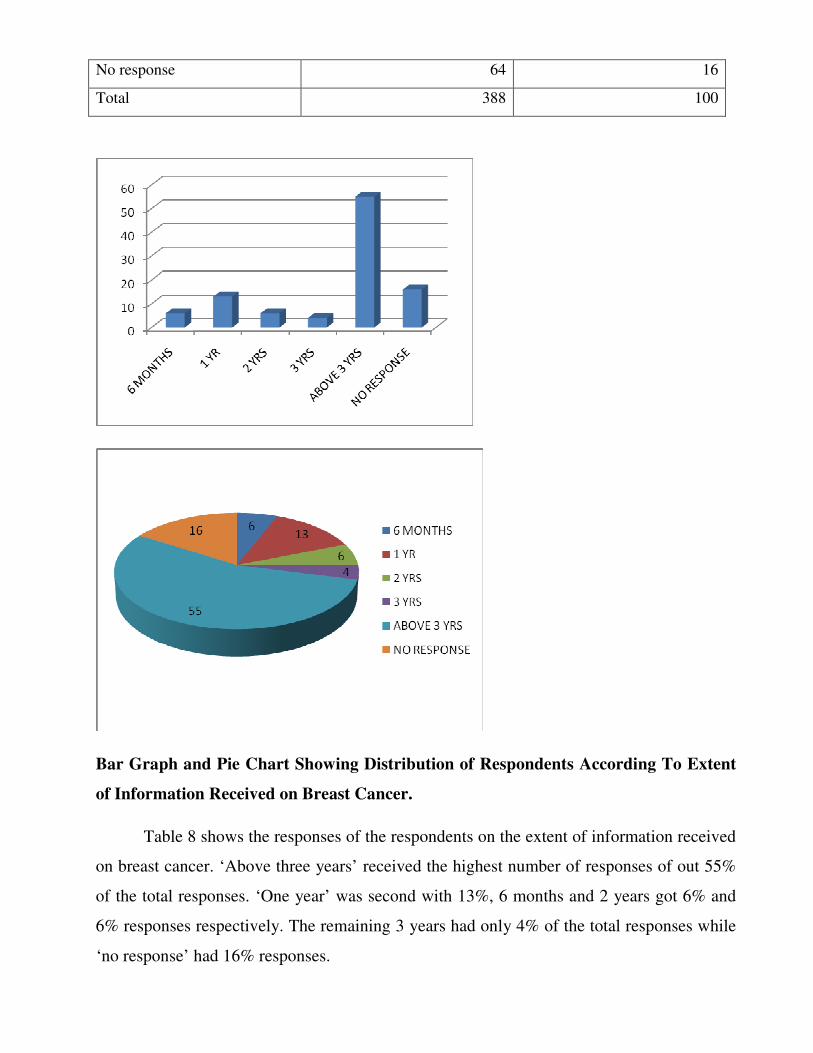
No response 64 16
Total 388 100
Bar Graph and Pie Chart Showing Distribution of Respondents According To Extent
of Information Received on Breast Cancer.
Table 8 shows the responses of the respondents on the extent of information received
on breast cancer. ‘Above three years’ received the highest number of responses of out 55%
of the total responses. ‘One year’ was second with 13%, 6 months and 2 years got 6% and
6% responses respectively. The remaining 3 years had only 4% of the total responses while
‘no response’ had 16% responses.

Question 5: How often does the medium of your major source features breast cancer
programmes (Indicate the medium please)
The result from question 5 indicates that greater number of the surveyed women
(210) severally indicated monthly for television channels like EBS, ITV and Silverbird, The
Nation and Guardian Newspapers, and EBS and ITV radio. While 24 respondents indicated
daily for only Silverbird radio and television. The remaining 90 respondents indicated bi-
weekly for ITV, Silverdird and EBS radio. 64 respondents did not respond.
Question 6: How often do you listen/read or watch breast cancer programmes from the
medium/media?
Table 9: Level of respondents’ exposure to breast cancer campaign programmes
Response Frequency Percentage
Daily
Weekly
Every two weeks
Monthly
No response
24
0
62
12
90
6
0
16
55
23
Total 388 100

Bar Graph and Pie Chart Showing Level of Respondent’s Exposure to Breast Cancer
Campaign Programmes
The above table shows the distribution of respondents according to their different
media exposure to breast cancer campaigns. The result indicates that majority of the
respondents had no adequate exposure to breast cancer campaigns, as the largest number of
them totaling 212 out of 388 or 55% of the respondents fell within the group of audience
that listen, read or watch about breast cancer campaign programmes monthly, while the
lowest number; 24 out of 388 or 6% of the respondents had adequate exposure to breast
cancer messages daily. The remaining 62 respondents were exposed to programmes every
two weeks while another 23% gave no response.
Question 7: What is the level of your understanding of breast cancer campaign
programmes?
Table 10: Level of respondents understanding of breast cancer campaign programmes
Responses Frequency Percentage
Very well 36 9

Well
Very little
Little
No response
56
80
144
72
14
21
37
19
Total 388 100
Bar graph and Pie chart showing Level of respondents’ understanding of breast
cancer campaign programmes.
Table 10 shows the distribution of respondents according to the level of their
understanding of breast cancer campaign programmes. From all indications, small number
of respondents representing 9% or 36 out of 388 respondents understood breast cancer
campaign programmes very well while 21% or 80 out of the 388 respondents did not
understand the programmes very well while 37% or 144 respondents understood just little
of the programmes. The remaining 19% or 72 respondents did not respond.

Question 8: The various campaign programmes on breast cancer that are exposed to
you fall within the following; Drama, Newspaper news stories/interviews, Magazine news
stories/interviews, Radio newsbits, Radio interview/health talks, Radio jingles, Television
newsbits, Television interviews/health talks, Television commercial, Billboard breast
cancer messages, Leaflet breast cancer messages and Internet
Table 11: Distribution of respondents’ exposure to various breast cancer campaign
programmes.
Response Frequency Percentage
Yes
No
324
64
84
16
Total 388 100
Bar graph and Pie chart showing distribution of respondents’ exposure to various
breast cancer campaign programmes.

The above table shows the distribution of the respondents according to their
acknowledgement of the various breast cancer campaign programmes they are exposed to.
The result indicates that 324 out of 388 or 84% of the respondents agreed to their being
exposed to different breast cancer campaign programmes while 16% or 64 respondents gave
a negative answer.
Question 9: If your answer to question 8 is yes indicate the one(s)
Table 12: Stating of the exact breast cancer programme by respondents
Response Frequency Percentage
Drama
Newspaper, health stories/interviews
Magazine, health stories/interviews
Radio news bits
Radio interview/health talks
Television News bits
TV interviews/health talks
Billboard breast cancer messages
Leaflet breast cancer messages
Jingles (Radio adverts)
Commercials (TV Adverts)
Internet breast cancer messages
None of the above
No response
0
16
8
131
14
61
36
32
26
0
0
0
0
64
0
4
2
34
4
16
9
8
7
0
0
0
0
16
Total 388 100

Bar graph and Pie chart stating of the exact breast cancer programme by respondents
Table 12 shows the responses of the respondents according to the exact breast cancer
campaign programmes they are exposed to. From all indications, a greater number of
respondents totaling 131 out of 388 or 34% were exposed to radio news bits while 61 or
16% of respondents were exposed to TV news bits, 36 respondents indicated TV interviews
/health talks as breast cancer campaign programmes they are exposed to, 14 respondents
identified radio interviews/health talks programmes while 4% stated newspaper
healthstories / interviews. Moreover, 32 respondents identified billboard breast cancer
messages, 26 or 7 % identified leaflets breast cancer messages, while 8 or 2 % of the
respondents identified magazine health stories / interviews. The remaining 16% or 64 out of

388 respondents gave no answer. Meanwhile, no respondent indicated, drama, jingles (radio
adverts), commercials (TV adverts), Internet and none of the above.
Question 10: If no, specify the exact breast cancer campaign programme, you are exposed
to.?
In question 10, no one out of the 388 respondents specified any other breast cancer
campaign programmes because none have any outside the above listed ones.
Question 11: The media campaign programmes on breast cancer are educative.
Table 13: Responses of respondents according to education of breast cancer campaign
programmes
Response Frequency Percentage
Strongly agree
Agree
Strongly disagree
Disagree
No response
15
29
106
160
78
4
8
27
41
20
Total 388 100

Bar graph and Pie chart showing respondents’ of responses according to education of
breast cancer campaign programmes.
The above table shows the responses of respondents according to the education of
media campaign programmes on breast cancer. The result indicates that 106 or 27% of the
respondents strongly disagreed that breast cancer campaign programmes carried in the
media were educative while 160 or 41% disagreed also to the education of the programmes.
About 29 out of 388 respondents agreed to the education of the programmes, with 4% of the
respondents that strongly agreed that breast cancer campaign programmes were educative.
About 20% or 78 respondents did not respond.
Question 12: Education on the disease is a comprehensive one
Table 14: The comprehensive level of education on the disease
Response Frequency Percentage
Strongly agree
Agree
Strongly disagree
Disagree
No response
11
66
79
84
148
3
17
20
22
38
Total 388 100

Bar graph and Pie chart showing comprehensive level of education on the disease by
respondents
Table 14 shows the distribution of the respondents on the comprehensive level of the
education on the disease. From all indications, the largest number of the respondents, 148
out of 388 did not respond on how comprehensive the education on breast cancer campaigns
was 3% of the respondents strongly agreed that education on the disease was a
comprehensive one while 66 respondents only agreed. But 84 out of 388 respondents
disagreed while 20% respondents strongly disagreed that education on the breast cancer
were are not comprehensive.
Question 13: The breast cancer campaign is on the risk factors (factors likely to contribute
to the formation of breast lump)
Table 15: Level of respondents’ exposure to breast cancer risk factors
Response Frequency Percentage

Strongly agree
Agree
Strongly disagree
Disagree
No response
40
69
49
106
124
10
18
13
27
32
Total 388 100
Bar graph and Pie chart showing Level of respondents’ exposure to breast cancer risk
factors
The above table shows the level of respondents’ exposure to breast cancer risk
factors. The result indicates that majority of the respondents had no media knowledge on the
risk factors of breast cancer as 124 out of 388 respondents gave no response to the question.

49 or 13% of the respondents strongly disagreed to the above question while 106
respondents only disagreed. Other respondents, 10% strongly agreed to being exposed to
breast cancer campaign risk factor while 18% only agreed being exposed to breast cancer
campaign risk factors.
Question 14: The breast cancer campaign is also on the symptoms of breast cancer (that is
how you can detect it)
Table 16: Level of respondents’ exposure to breast cancer symptoms
Response Frequency Percentage
Strongly agree
Agree
Strongly disagree
Disagree
No response
77
84
46
71
110
20
22
12
18
28
Total 388 100

Bar graph and Pie chart showing Level of respondents’ exposure to breast cancer
symptoms
Table 16 displays the distribution of the responses of the respondents on the level of
their media exposure to breast cancer symptoms. From all indications, 20% or 77 out of 388
respondents strongly agreed to the above question while 22% only agreed to having been
exposed to breast cancer symptoms in breast cancer programmes. But 12% strongly
disagreed while 18% of the respondents only disagreed. But 110 out of 388 respondents
representing 28% could not respond to the question.
Question 15: Do you know about breast self examination (BSE) and clinical breast
examination (CBE)?
Table 17: Respondents distribution according to knowledge of breast self examination
(BSE) and clinical breast examination (CBE)
Response Frequency Percentage
Yes
No
242
146
62
38
Total 388 100

Bar graph and Pie chart showing respondents distribution according to knowledge of
breast self examination (BSE) and clinical breast examination (CBE)
The table above displays the respondents knowledge of breast self examination and
clinical breast examination. The result shows that more than half of the respondents
representing 62% or 242 out of 388, had knowledge of BSE and CBE while the remaining
38% or 146 respondents answered in the negative.
Question 16: The campaign programmes on BSE and CBE are educative
Table 18: Responses of respondents to education of BSE and CBE
Response Frequency Percentage
Strongly agree
Agree
Strongly disagree
Disagree
No response
51
67
62
90
145
13
18
16
23
38
Total 388 100

Bar graph and Pie chart showing responses of respondents to education of BSE and
CBE
Table 18 shows the responses of the respondents according to education of BSE and
CBE. From all indications, 13% or 51 respondents strongly agreed to the above question
while 67 respondents only agreed that breast cancer campaign programmes on BSE and
CBE were educative. However about 90 respondents disagreed while 62 respondents
strongly disagreed that the BSE and CBE were educative. The remaining large number of
146 respondents gave no response.
Question 17: Do you practice the BSE to detect breast lump?
Table 19: Distribution of respondents according to practice of BSE

Response Frequency Percentage
Yes
No
182
206
47
53
Total 388 100
Bar graph and Pie chart showing distribution of respondents according to practice of
BSE
The table above displays the distribution of respondents according to practice of BSE
to detect breast lump. The result shows that only 182 out of 388 or 47% of the respondents
practiced BSE while more than half of the respondents (206 or 53%) were not practicing
BSE to detect breast lump.

Question 18: Do you practice the CBE?
Table 20: Practice of CBE by respondents
Response Frequency Percentage
Yes
No
50
338
13
87
Total 388 100
Bar graph and Pie chart showing practice of CBE by respondents
Table 20 shows the distribution of respondents according to the practice of CBE. The
result indicates that more than half of the respondents were not practicing CBE as 338 out

of 388 respondents or 87% gave a negative response to the practice of CBE while 13% or
50 respondents agreed to practice CBE.
Question 19: If the question 17 is yes, how often do you do BSE?
Table 21: Level of respondent practice of BSE
Response Frequency Percentage
Daily
Every two days
Once a week
Once a month
Once in two months
Once in six months
Once a year
No response
24
11
14
21
28
54
30
206
6
3
4
5
7
14
8
53
Total 388 100

Bar graph and Pie chart showing level of respondents practice of BSE
The above table shows the distribution of the respondents according to the level of
performance of BSE. The result indicates that a greater number of respondents (206 or 53%)
still were not practicing BSE. 24 respondents agreed practicing BSE daily, while 11
respondents practiced every two weeks. Moreso, 14 or 4% of respondents practiced BSE on
a weekly basis, 21 respondents practiced on a monthly basis, 28 of them practiced bi-
monthly while 54 and 30 respondents practiced once every 6 months and once a year
respectively.
Question 20: If question 18 is yes, how often do you visit the hospital for CBE?
Table 22: Distribution of respondents according to the level of practice of CBE
Response Frequency Percentage
Once in a month
Once in two months
Once in six months
Once in a year
No response
14
10
16
10
338
5
3
4
3
87
Total 388 100

Table 22 shows the responses of respondents according to the level of practice of
CBE. The results shows that apart from a large number of respondents totaling 338 or 87%,
who were not practicing CBE, 14 respondents practiced CBE on a monthly basis while 10
of them practiced CBE bimonthly. The remaining 16 and 10 respondents practiced CBE
every six months and every year respectively.
Question 21: But if your answer to question 17 is No, please state your reason(s).
The result from question 21 indicates that out of 388 respondents, 206 respondents
were not practicing BSE. Various reasons were given by different number of respondents.
146 respondents had no knowledge of BSE at all. While 20 out of the remaining 60
respondents specified having inadequate information on BSE from the media, with little or
no time to practice BSE and not being aware of the need of BSE.
Question 22: And if your answer to question 18 is also no, please state your reason(s).

Question 22 result, indicates that large number of respondents representing 338 out
of 388 respondents were not practicing CBE due to the following reasons: 146 respondents
indicated having no knowledge of CBE, 97 acknowledged having inadequate information
on CBE while the remaining 95 did not have ample time to practice CBE, but 100
respondents acknowledged not being aware of the need of CBE.
Question 23: The general response of women towards the media campaign on breast cancer
is rated very high and positive.
Table 23: Distribution of respondents’ general attitude to breast cancer campaigns
considered very high and positive
Response Frequency Percentage
Strongly agree
Agree
Strongly disagree
Disagree
No response
36
47
90
97
118
9
12
23
25
31
Total 388 100

Bar graph and Pie chart showing distribution of respondents’ general attitude to
breast cancer campaigns considered very high and positive
Table 23 shows the distribution of responses of respondents according to the
women’s general attitude to breast cancer campaigns rated very high and positive. The
result indicates that 47 out of 388 respondents agreed that general responses of women
towards breast cancer messages were high and positive while 9% of respondents only
strongly agreed to the above statement. 97 respondents, in the other hand disagreed likewise
90 of them who strongly disagreed that women’s general attitude to breast cancer campaign
were high and positive. The remaining 118 out of 388 or 31% of the respondent did not
respond to the above statement.
Question 24: Which of the media do you think is most effective for breast cancer
campaigns?
Table 24: The medium that is most effective for breast cancer campaigns
Response Frequency Percentage
Radio
Television
Newspaper
Magazine
Leaflets
Billboards/posters
No response
190
120
12
0
4
8
54
49
31
3
0
1
2
14
Total 388 100

Bar graph and Pie chart showing the medium that is most effective for breast cancer
campaigns.
Table 24 shows the distribution of the respondents according to the medium most
effective for breast cancer campaigns. The result indicates that largest number of
respondents (190 or 49%) chose radio as the most effective medium for breast cancer
campaigns while 120 or 31% of the respondents opted for television. About 3% of the
respondents went for newspaper and 2% for billboards/posters, with 1% for leaflet. None
went for magazine while the remaining 54 or 14% respondents gave no answer to the above
question.
Findings:
1. The study found infrequent and incomprehensive media campaigns on breast cancer
that can cause a positive behaviour change of Edo women.
2. The findings indicated low exposure and poor knowledge of Edo women to detailed
information on breast cancer
3. It was found that media campaign programmes exposed to Edo women excluded
drama, internet radio jingles and television commercials.
4. The study revealed radio as the women’s major source of information on breast
cancer.
5. The findings showed that the women were more exposed to radio
6. It also showed that greater number of the women were illiterates, semi-literate, low-
earned-rural and semi-rural dwellers, who could not read printed media.
7. The study found negative attitude of the women in performing their BSE and CBE.
8. Radio was considered the most effective medium for breast cancer Campaigns.
4.3 Discussion of Findings.
The result obtained from the analysis of this study indicated that the media
campaigns on breast cancer have not been adequate to engender a prompt and quick
compliance of Edo women to early presentation of breast cancer and equally prevent the
increase of its mortality rates. The study revealed how weak the media campaigns on breast
cancer have been. Findings from Tables 8 and 9, and question 5 showed that breast cancer
programmes did not feature frequently but in most cases featured monthly except for
Silverbird radio and Television that carry their breast cancer messages after most news
casting. This is evident in Table 9 where majority of the women (212) were monthly
exposed to breast cancer messages while greater number of the women (214) in Table 8
who have heard about breast cancer for 3 years could still not identify breast cancer risk
factors and symptoms let alone having a good understanding of the whole campaign
messages.

The infrequencies inherent in the presentation of these breast cancer programmes
could probably explain why the breast cancer campaigns have not produced positive
changes in Edo women as shown clearly in Tables 19 and 20. In Table 19, more than half of
the respondents (206 or 53%) did not practice BSE, while only 50 women practiced CBE,
although Table 17 confirmed the BSE and CBE awareness of 242 out of 388 surveyed
women, as screening tools for early detection of breast cancer lump. This according to
Blugs, Cummings, Spencer and Palladino (2009), Okobia, Bunker, Okonofua and Osime
(2006) have been found to reduce risk of breast cancer mortality when performed by the
women themselves. The apparent low practice of BSE and CBE explained the late
presentation of breast cancer and increase in its mortality rate as confirmed by the
testimonies of the surveyed women who became ‘breast cancer aware’ because of their
deceased family members and friends who were victims of the disease.
Table 5 showed that the majority of the women (364 or 94%) had knowledge of
breast cancer. But table 6 revealed a complete level of ignorance of 24 surveyed women
who were not exposed to breast cancer campaigns from both people (interpersonal
communication) and the media. Highest proportion of the women (290) obtained
information about breast cancer from both people and the media, 34 of them, obtained
solely from the media while 40 of them had knowledge of breast cancer from people
(interpersonal communication).
However the 40 respondents who obtained breast cancer information from people
became ‘breast cancer aware’ due to deaths of their loved ones, family members and friends
while more than half of the 290 study women also testified of obtaining their first
information on breast cancer from the deaths of their loved ones before their exposure to
media messages on breast cancer. But among these women (290 and 40 respondents) some
were equally informed of breast cancer through women fora, people in the community,
friends, relations, and ante-natal and post-natal check-ups, where they were taught about
breast cancer risk factors, common symptoms and methods of early detection.
The findings therefore indicated low exposure and poor knowledge of women to
detailed information on breast cancer’s risk factors, symptoms and method of early
diagnosis from the media without individual exposure from interpersonal communication.

That is why highest proportion of the surveyed women in Table 13 (160 or 41% and 106 or
27%) respectively disagreed that media campaigns on breast cancer were educative.
Moreover, findings from Table 12 revealed that media campaign programmes on
breast cancer that Edo women were exposed to excluded drama, Internet, Radio jingles and
television commercials but included the Newspaper health stories / interview, radio news
bits, radio interview / health talks, television news bits, television interview / health talks,
leaflets breast cancer messages, billboard breast cancer messages and magazine health
stories / interview. But it was found that women’s knowledge of the above breast cancer
programmes were not deep-rooted as majority of them in Tables 10, 15 and 16, had little
understanding of the programmes, lack comprehensive information on the programme’s risk
factors and common symptoms
However, Table 13, buttressed by Table 14 bared the abysmal level of inadequacies
of the above breast cancer campaigns programmes as it pertains to the comprehensive
nature of their educative roles. The study revealed the inexhaustive breast cancer messages
carried in the various media as majority of the women (79 and 84) totally disagreed that
education on breast cancer programme are comprehensive while 148 respondents who were
not able to respond could not remember whether breast cancer messages they received from
the various media are thorough or not.
Additionally, Table 10, substantially affirmed the women’s poor knowledge to breast
cancer campaign messages, when more than half of them (144 and 80 respectively) agreed
having little and very little understanding of the campaign programmes from the mass
media. Tables 15 and 16 disclosed the low level of women’s exposure to breast cancer risk
factors and symptoms. It was found that breast cancer risk factors and common symptoms
embedded in the various campaign programmes were seriously inadequate and poor. Table
15 indicated that the highest proportion of respondents comprising 49 and 106 respectively,
disagreed that media campaigns on breast cancer educate the women on these risk factors.
Results from table 16, similarly indicated that media campaigns on breast cancer
symptoms, exposed to respondents remained inadequate to elicit women’s quick and prompt
compliance to the prevention of late presentation of the disease and its (deaths) mortality
rates. Thus greater number of study women, totaling 46 and 71 did not agree that media
campaigns on breast cancer educate them on the symptoms of the disease while some of the

124 and 110 women in both table 15 and 16 could not answer to the question, because of
their inability to remember if the information received from the mass media on breast
cancer deal on their risk factors and common symptoms or not.
Moreover, the women that were informed by both mass media and people, indicated
radio in Table 7 as their major source of information as greater number (180 or 46%)
obtained information from mainly silverbird radio, ITV radio and EBS radio followed by
ITV, EBS and STV television (128 or 33%) and The Nation and Guardian newspaper (16 or
4%). The greater number of radio audience in this study is in keeping with the findings of
other researchers. For instance, in a survey of HIV/AIDS campaigns on audience
behavioural changes, Anyaegbudike (2005) found that radio was the most widely used
medium among his Enugu respondents in Nigeria.
However the surveyed women were found to be more exposed to radio as a result of
the epileptic power supply predominant in most areas of the state and coupled with the busy
nature of their businesses as most of them are market women, hence no time for television
viewership. Most importantly, high level radio exposure was found to be related to the fact
that greater number of the surveyed women are illiterate and semi-literate, low-earned rural
and semi-urban dwellers. But the issue of breast cancer billboards, Tell, Newswatch,
Thisweek,Thenews, Insider, South South and Source magazines, breast cancer leaflets and
Internet, not constituting a major source of information to the women, more so, revealed the
incompetence of the printed media to communicate effectively with indigenous (local)
languages in the campaign messages and it also revealed the low level of educational status
of the women, as more than half of them (104 and 108) have only primary six and
WAEC/GCE education respectively, with 24 women who have no education. For instance,
it was found that these women could not read or understand the limited numbers of
MWAN’S leaflets on Breast self examination shared to them, let alone availing themselves
of other printed media.
Results obtained from table 23 indicated negative attitude of women in complying to
the campaign messages of early presentation of breast cancer. This is seen in the responses
of the majority of the women (90 and 97 women respectively) that answered in the negative.
It was therefore found that the negative attitude was mainly consequent among other things
on the infrequencies of breast cancer programmes presented in the aforementioned media.

Finally, in responding to the question of the medium considered the most effective
for breast cancer campaigns, large number of women (120 or 31 %) identified television
because of its added advantage of sight and sound over other media while a larger number
(190 or 49%) identified radio. Most of the respondents believed radio is most effective
medium for dissemination of breast cancer campaigns consequent on its affordability,
mobility, portability, complementary nature of its battery usage, and most importantly its
widest reach and the efficiency with which it transcends literacy level of the audience.

CHAPTER FIVE
SUMMARY, CONCLUSION AND RECOMMENDATIONS
5.1 Summary
The study reviewed foreign and local literatures that related and bordered on evaluation of
media campaigns on breast cancer in Edo state. This is coupled with examining of relevant
theories that constituted the fundamental framework of the study.
The study designed to appraise the effectiveness of the various media campaigns on
breast cancer and the women’s level of exposure and compliance to the campaign messages,
generated results from the responses of 400 women randomly and systematically selected
from 12 wards, of Oredo local government area of Edo state.
However, the results obtained from a 28-item questionnaire that comprised but
demographic and psychographic data of Edo women, were analyzed and presented in
appropriate tables and percentages, pie charts and bar charts. The study emphatically
revealed that the breast cancer programmes inherent in the media campaigns were grossly
infrequent, inadequate and poor in themselves to elicit prompt and quick adherence of
women to early presentation of breast cancer through the practice of BSE and CBE.
Therefore, results of the study have shown that the media campaigns on breast cancer have
little effect on the Edo women.
5.2 Conclusion
In conclusion of this study, major findings revealed that media campaigns on breast cancer
have not been adequate to produce sustainable changes in Edo women in screening their
breast by themselves and by visiting the hospitals for early detection of breast cancer.
Results obtained from the study revealed that media campaign messages on breast cancer’s
risk factors, common symptoms and methods of early diagnosis, exposed to the women
were abysmally incomprehensive and poor. This was evident in the greater number of the
research questions that received negative responses from the surveyed women.
Confirming the above, it was found that the frequencies of these media exposure,
their contents and the level of the women’s understanding of the entire campaign
programmes were altogether inconsistent and low. It was equally discovered that more than
half of the women were not opportuned to have an adequate exposure and a better

understanding of the few leaflets shared to them by Medical Women Association of Nigeria,
(MWAN) Edo State chapter, mainly due to their low educational status. This was similar to
the standard billboard on breast cancer displayed at the king square (Oredo local
government), irrespective of two others, equally displayed at Uselu market (Egor local
government) and Oregbeni park (Ikpoba okha local government) by MWAN, Edo state
chapter.
It therefore showed that the media campaigns on breast cancer received very low
women exposure even though there was a high women exposure to silverbird radio and ITV
radio as a medium identified as their major source of breast cancer knowledge. Generally,
radio was additionally identified as the most effective medium in breast cancer campaigns
due to its far reaching capabilities to the remotest parts of a community.
These facts obtained from the surveyed women as they pertain to their inadequate
media exposure and poor knowledge, however explained why the practice of BSE and CBE
was very low among them. Other reasons for nor performing BSE and CBE, apart from not
having enough information, include not having enough time and not being aware of the
need for BSE and CBE. Meanwhile, studies have proved that adherence to BSE and CBE
are fundamental to facilitating early diagnosis and treatment of breast cancer.
However, findings also showed that the surveyed women who were informed by
people (interpersonal communication) and not by mass media were better exposed to breast
cancer messages than the women who were informed by mass media. This affirms the
importance of interpersonal communication or social interaction to media campaigns in
producing positive results. As stated by Hornik and Yanavitzky (2003), that one of the three
ways media campaigns affects behavior change is through social interaction with family
members, friends and other people in the community.
As studies, reports, public opinion experts and social scientists have established, that
media campaigns cannot therefore produce desired positive changes or prevent negative
ones without a support of face- to- face campaigns or interpersonal communication (social
interaction)
5.3 Recommendations
Based on the above findings, the study recommends that:
1. Breast cancer campaigns should be made elaborate, well spelt out, comprehensive
and strategic like that of HIV/AIDS campaigns in educating the women on the risk

factors, common symptoms and early diagnosis and treatment of breast cancer. There
should be breast cancer dramas, clear cut jingles and commercials, intensive and
consistent health talks repeatedly carried in every media to ensure a holistic, change-
oriented campaign piece.
2. The analysis, planning, execution and evaluation of these breast cancer campaign
programmes should be thoroughly researched and packaged to change Edo women
from low performance of BSE and CBE to achieving a quick and prompt compliance
of early presentation of breast cancer and to prevent untimely deaths. These
researches should comprise audience, media message and source researches.
3. Employment of different native languages, including ‘Pidgin English’ and persuasive
breast cancer messages should be used in communicating to the women to ensure
utter comprehension of the programmes which will in turn influence their voluntary
behaviour to achieving positive results.
4. Apart from employment of posters, billboards, leaflets, magazines and newspapers
for the literate and elite class, radio and television should mainly be utilized to
disseminate persuasive, educative and comprehensive breast cancer messages to the
semi-literate and illiterates groups in their widest semi-urban and rural areas.
5. Religious fora, women fora and others should be intensified and deliberate in
furthering the breast cancer education of the women.
6. Apart from the federal government involvement, local and state government should
totally take up the sponsorship and be involved in the fight against breast cancer
pandemic and should not be left for few individuals and group organizations NGOs
or the media.
7. To actualize the behavioural change of Edo women in adhering to an early
presentation of breast cancer lump, believed to be the cure, the media campaigns
need to be featured on a frequent basis according to the dictates of a true campaign to
ensure clarity and total comprehension of breast cancer messages
8. Most importantly, supportive programmes in the case of mixed communication
strategy should be employed in carrying out extensive, massive and organized
community campaigns throughout the length and breathe of Edo state. That is, the
use of face-to-face (interpersonal) campaign and that of the media campaign. This
mixed communication campaign strategy should be carried to every community,

market places, women fora, social gatherings, religious gatherings and tertiary
institutions to reinforce reinvigorate and ensure credibility of breast cancer source
and clarity of breast cancer messages. This definitely will mobilize the women’s
actions for a positive change to take place. In other words, media campaigns on
breast cancer singnificantly need a complementary support of face-to-face
communication campaign to be adequate and effective to produce positive changes in
the performance of BSE and CBE by Edo women which will advertently prevent late
diagnosis of the disease with its attendant mortality rates.

BIBLIOGRAPHY
Books
America Cancer Society (2007) Breast cancer facts and figures. Atlanta: ACS, Inc.
Becker, M.H. (ed) (1974) The health belief model and personal health behaviour.
Thorofare, NJ: Charles B. Slack.
Blugs, W.S., Cummungs, M.r., Spencer, C.A. and Palladino, M.A. (2009). Concepts of
genetics. America: Pearson Prentice Hall.
Commonwealth Africa communication (2006).Landmark achievements of Oredo local
government council under the leadership of Victor Edos Ebomoyi(May 2004-December
2006)Benin-city: Commonwealth Africa Communication
Igbare, E. (2009) social Development, Television and politics in Nigeria. Ibadan: Kraft
Books limited.
King, S., (2006). Pink Ribbons Inc: breast cancer and the politics of philanthropy.
Minneapolis?: University of Minnesota Press.
Kotter, P. and Armstrong, G., (2009) principles of marketing, (13th
ed) Upper Saddle, River,
NJ: Prentice Hall.
Ogbuoshi, L.I (2006). Understanding research methods and thesis
writing. Enugu: Linco Publishers.
Ohaja, E.U (2003). Mass communication research project report writing.
Lagos: John Letterman Ltd.
Olson, J.S. (2002). Bathsheba’s breast: Women, Cancer and History. Baltimore: The John
Hopkins University Press.
Shaibu, R. (2008 February). Tiny RNA molecules control breast cancer’s spread. Tell
magazine, p 13.
Sulik, G. (2010). Pink Ribbon Blues: How breast cancer culture undermine women’s
health. New York Oxford University press.
WHO/UICC (2005) Global action against cancer. New Switzerland: WHO/UICC.
Wakefield, M.A., Loken, B. and Hornik, R.C. (2010). Use of mass media campaigns to
change health behavior. Retrieved on 26 Feb., 2011.
Wikipedia (2011) Breast cancer awareness www.wikipedia.com.

Magazine
Adebayo, F. (2010 April). Cancer goes commercial. Tell magazine, pp 12.
Adebayo, F. (2010 February). Between early menstruation and cancer. Tell magazine,pp
13.
Oyetayo, A. (2010 April). Prevention is better than cancer. Tell magazine, pp 12.
Shaibu, R. (2008 February). Tiny RNA molecules control breast cancer’s spread. Tell
magazine, p 13.
The scourge of cancer (2011,Febuary 7). Tell magazine pp 5.
Journals
Bottoff, J., Mckcown, S.B., Grey, J., Haines, R., Okoli, C., Johnson, K.C., Easley, J.,
Ferrence., B., Baillie, L., and Ptolemy E. (2010) Young women’s response to smoking
and breast cancer risk information. Oxford Journal Medicine, 25, 668 677.
Buffetla, P. Hashibe, M., La Vecchia C., Zatonski, W. and Rehm, J. (2006) The burden of
cancer attributes to alcohol drinking. International Journal of cancer, 119(4) 884-7.
Dumitrescu, G. and Cotaria, I (2004) Understanding breast cancer risk: Where do we stand?
Journal of cell molecular medicine, 9(11), 208-11.
Grunfeld, E.A., Ramirez, A.J., Hunter M.S. and Richards, M.A. (2002). Women’s
knowledge and beliefs regarding breast cancer. Breast Cancer Journal 86: 1373-1378.
Kahneman, D and Tversky, A. (1979)prospect theory: an analysis of decision under risk.
Econometrica, 47,263-291.
Kamangar, F. Dores, G.M. and Anderson, W.F. 92006 patterns of cancer incidence,
mortality and prevalence across five continents: defining priorities to reduce cancer
disparities in different geographic regions of the world. Journal of clinical Oncology.
24:2137-50
Kayoed, F.O., Akande, T.M. and Osagbemi, G.k. (2005). Knowledge, attitude and practice
of breast self examination among female secondary school teachers in Ilorin, Nigeria.
European Journal of Scientific Research, PP 42.
McCombs and Shaw, D.L (1973) The agenda-setting function of the mass media. Public
opinion Quarterly, 37,63-75.
Okobia, M.N., Bunker C.H., and Osime, U. (2006) Knowledge, attitude and practice of
Nigeria women towards breast cancer, a cross sectional study. Retrieved from
http://creativecommons.org/licenses/by/120
Parkin, D.M., Bray, F., Ferlay, J. and Pisani, P. (2005) Global Cancer Statistics. 2005. CA:
A Cancer Journal for Clinicians, 55(2), 74-108.
Prochaska, J.O., Diclemente, C.C., and Norcross, J.C. (1992) In search of how people
change: Applications to addictive behaviour. American psychologist, 47, 1102-1114.

Rimal, R.N. (2000). Closing the knowledge-behaviour gap in health promotion: The
mediating roles of self-efficacy. Health Communication, 12(3), 219-237.
Siahpush, M. and Singhm, G.K. (2002). Sociodemagraphic predictors of pap test receipt,
currency and knowledge among Australian women. 35:362-368.
Soola, E.O. (2009). Communication and educational approaches and strategies for effective
environmental awareness. European Journal of Social Sciences, 9(1), 15-28.
Udoudo, A.J, (2008) Rising cases of cancer and media social responsibility. International
journal of communication. Vol. 2 pp 364 – 373.
Research Project
Anyaegbudike, V. (2005) The impact of HIV/AIDS campaigns on audience behavioural
changes. An unpublished project work of the department of mass communication.
University of Nigeria Nsukka.
Coffman, J. (2002) public communications campaign evaluation: An environment scan
challenges, criticism, practice and opportunities. Cambridge, M.A family Research
project. Retrieved from www.thelancet.com.
Osemeke, I.T., (2011) Role of radio in the creation of awareness on breast cancer: A study
of Rhythm 93.7 fm. Benin-City. An unpublished project work of the department of mass
communication. Benson Idahosa University, Benin-City Ed. State.
Leaflet
Medical Women Association of Nigeria, Edo State. (2011) Breast self examination. Edo
state: medical women association of Nigeria.
Television
Nigeria Television Authority (2011,February 4)7am Network News.
Stober, C., (Newscaster). (2011 Feb., 4). 9pm Network news. Abuja: Nigeria.
Newspaper
Ogbodo, P. (2010, November 11). Nigeria: Bauchi Awol begins breast cancer awareness
campaign. Daily Independent, P.
Personal Interview
Iyasere, K.E., (2011,June 18) {personal interview}.

Internet materials
Azenha, G., Bass, L.p., Caleffi, M., Smith, R., Pretorius, L., Durstine, A. and C.P.
(2011) The role of breast cancer civil society in different resources settings.
Breast Without Spot Initiative (BWS)
http://www.internationalcancerweekinitiative.com/index.php?
Cadbury Bournvita pushes the envelop against breast cancer
http://businessworldng.com/web/articles/238/1/CRS
Gallagher, K.M., Updegraff, J.A., Rothman, A.J, and Sims L. (2011) perceived
susceptibility moderates framed messages. Retrieved 26 Feb. 2011.
Hormik, R.C., and Yanovitzky, I. (2003) Using theory to design evaluations of
communication campaigns: the case of the national youth anti-drug media campaign.
From http://repository.upenn.edu/asc.papers/a8.
Humphrey, L.L., Helfand, M., Chan, B.K.S and Woolf S.H. (2002) breast cancer
Joanneum Research, Nielsen media Research, University of Shelfield, Ontotext lab.
University of Twente, HS-ART Softeco Sismat and TNO Netherlands (2009) Media
Campaign.http://blog.thoughpick.com/2009/06/10-social-campaigns-that-rock-learn-
how-to-do-the-game.html//more877
Kingston, A. (2010) A nice rack of slogan. Maclean’s 123(41) 73
http://www.worldcat.org/issn/0024-9262.
Nazrul, M.O. (2010). Awareness on breast cancer among the women of reproductive age in
Bangladesh. Retrieved on 26 Feb., 2011.
ORCMacro and APCO (2004). Theoretical framework multi-year mass media campaign
plan. Retrieved on 26 Feb., 2011.
Pielle, (2005). Public Service: breast cancer awareness campaigns – Pakistan. Retrieved 26
Feb., 2011. Retrieved from http://creativecommons.org/licenses/by/20.
Russell, M. (2007) Understanding Diseases. http://EzineArticle.com/?expert=micheal
http://www.answers.com/topic/massmediaAPPENDIX
APPENDIX
Department of Mass Communication
Faculty of Arts.
University of Nigeria, Nsukka
Enugu State.
Dear Respondent,

This questionnaire being presented for your completion is purely for academic
research purpose in partial fulfillment for the award of M.A degree in the above department
and university.
It is designed to gather information on the topic: evaluation of media campaign on
breast cancer, a study of women in Edo state.
It is my request, therefore, that you supply sincere answers, for the information
provided will be handled as confidential.
Thanks for your anticipated co-operation.
Okeibunor Ngozi B.

SECTION A
Demographic Data
Please tick as it applies to you
1. Age Range
a) 18-25
b) 26-35
c) 36-45
d) 46 and above
2. Marital Status
a). Single
b) Married
c) Divorced
d) Widowed
3. Educational Status
a) Primary six
b) WAEC/GCE
c) OND/NCE
d) HND/BSC/BA
e) MSC/MA
f) PHD and above
g) No education
4. Occupation
a) Trader
b) Farmer
c) Business Woman
d) Civil / Public Servant
e) Professional

Psychographic Data
1. Have you heard about breast cancer before?
a) Yes
b) No
2. From where did you hear about breast cancer?
a) Mass Media
b) People
c) All of the above
d) None of the above
3. If the answer to number 2 is mass media, then which of the media is your major source of
information on breast cancer?
a) Radio Nigeria Benin, ITV, EBS, Ray Power or Silverbird Radio
b) NTA Benin, ITV, EBS, STV or AIT Television
c) Observer, Vanguard, Punch, Guardian, Tribune or The Nation Newspaper
d) Tell, Newswatch, ThisWk, Insider, South South, TheNews, Source Mag
e) Breast Cancer Billboard/Posters
f) Breast Cancer Leaf lets
g) Internet
h) None of the above
i) No response
4. For how long have you received breast cancer information from the mass media?
a) 6 months
b) One years
c) Two years
d) Three years
e) Above 3 years
f) No response

5. How often does the medium of your major source of information feature breast cancer
programmes ?
a) Daily
b) Weekly
c) Every two weeks
d) Monthly
e) No response
6. How often do you listen, read or watch breast cancer programmes from the medium?
a) Daily
b) Weekly
c) Every two weeks
d) Monthly
e) No response
7. What is the level of your understanding of breast cancer campaign programmes?
a) Very well
b) Well
c) Very little
d) Little
e) No response
8. The various campaign programmes on breast cancer that are exposed to you fall within
the following: Drama, newspaper health stories / interviews, magazine health stories /
interviews, radio newsbits, TV newsbits, radio interviews /health talks, TV interviews /
health talks, billboard breast cancer messages, leaflet breast cancer messages, jingles (Radio
adverts) and commercials (television adverts) and Internet breast cancer stories.
a) Yes
b) No
9. If your answer to question 8 is yes, indicate the one (s)
a) Drama
b) Newspaper health stories / interviews
c) Magazine health stories / interviews
d) Radio newsbits
e) Radio Jingles
f) Radio interviews / health talks
g) TV newsbits
h) TV commencials
i) TV interviews / health talks

j) Billboard breast cancer messages
k) Leaflet breast cancer messages
l) Internet breast cancer messages
m) None of the above
n) No response
10. If no specify the exact campaign programme (s) you are exposed to?
11. The breast cancer programmes are educative.
a) Strongly agree
b) Agree
c) Strongly disagree
d) Disagree
e) No response
12. The education is a comprehensive one.
a) Strongly agree
b) Agree
c) Strongly disagree
d) Disagree
e) No response
13. The breast cancer campaign is on the risk factors (factors likely to cause breast cancer)
a) Strongly agree
b) Agree
c) Strongly disagree
d) Disagree
e) No response
14. The breast cancer campaign is also on the symptoms (i.e the signs of breast cancer).
a) Strongly agree
b) Agree
c) Strongly disagree
d) Disagree
e) No response

15. Do you know about Breast Self Examination (BSE) and Clinical Breast Examination
CBE)?
a) Yes
b) No
16. The campaign programmes on BSE and CBE are educative
a) Strongly agree
b) Agree
c) Strongly disagree
d) Disagree
e) No response
17. Do you practice BSE to detect early breast lump?
a) Yes
b) No
18. Do you practice CBE?
a) Yes
b) No
19. If question 17 is yes, how often do you do BSE?
a) Daily
b) Every two days
c) Once in week
d) Once every two weeks
e) Once in a month
f) Once in two months
g) Once in six months
h) Once in year
i) No response
20. If question 18 is yes, how often do you visit the hospital for CBE?
a) Once in a month
b) Once in two weeks
c) Once in six months
d) Once in a year
e) No response

21. But if your answer to question 17 is no, please state your reason (s)
22. If your answer to question 18 is no, please state your reason (s)
23. The general response of women towards the media campaign on breast cancer is rated
very high and positive?
a) Strongly agree
b) Agree
c) Strongly disagree
d) Disagree
e) No response
24. Which of the mass media, do you think is most effective for breast cancer messages?
a) Radio
b) Television
c) Newspaper
d) Magazine
e) Leaflets
f) Billboards/ Posters
g) No response
Thank You

![A [3+3] cyclization strategy for asymmetric synthesis of ...download.xuebalib.com/xuebalib.com.50934.pdfused as electrophiles.5 In the case of cyclic ... sulfamidates as synthetically](https://img.pdfslide.net/doc/110x75/5ae1e23b7f8b9a90138ba9e2/a-33-cyclization-strategy-for-asymmetric-synthesis-of-as-electrophiles5.jpg)



























