Embed Size (px)
Citation preview

On the road to recovery:Gasoline content regulations and child health
Michelle Marcus∗
October 7, 2016
Abstract
Gasoline content regulations are designed to curb pollution and im-prove health, but the impact on health has not been quantified. Byexploiting both the timing of regulation and spatial variation in chil-dren’s exposure to highways, I estimate the effect of gasoline regulationon pollution and child health. Results show that the introduction ofcleaner-burning gasoline in California in 1996 reduced asthma admis-sions by 8 percent in high exposure areas. Reductions are greatest forareas downwind from highways, heavy traffic areas, and children of lowsocio-economic status. Stringent gasoline content regulations can im-prove child health, and may diminish existing health disparities.JEL: I14, I18, L71, Q53, Q58Keywords: asthma; gasoline content regulation; air pollution; traffic;vehicle emissions
∗Marcus: Brown University, Department of Economics, Brown University, 64 WatermanStreet, Providence, RI 02912, michelle [email protected]. For their helpful commentsand feedback, I would like to thank Anna Aizer, Emily Oster, Ken Chay, Andrew Fos-ter, Sriniketh Nagavarapu, Vernon Henderson, Daniela Scida, Joseph Acquah, Tim Squires,David Glancy, Alexandra Effenberger, Desislava Byanova, and participants at Brown Uni-versity’s Microeconomics Lunch Seminar. Fellowship support from Resources for the Futureis gratefully acknowledged. All remaining errors are my own.
1

Asthma affects 1 in 10 children and costs the U.S. over $6 billion everyyear. Motor vehicle exhaust has been identified as an important asthma trig-ger, and evidence from epidemiological research shows a strong correlationbetween traffic pollution and health outcomes for children and infants.1 In aneffort to curb pollution and improve health outcomes, state and federal govern-ments have enacted gasoline content regulations designed to reduce pollutionfrom motor vehicle exhaust. However, gasoline content regulations are associ-ated with significant economic costs. These regulations can increase the priceand price volatility of gasoline, which is costly to consumers (Brown et al.,2008; Muehlegger, 2002).2 The compliance cost to refineries is also quite large,over $1 billion per year in California. Given these high costs, it is importantto identify whether or not gasoline content regulation significantly decreasespollution, improves health, and reduces health expenditures.
Several states, including California, have adopted more stringent gasolineprograms than those imposed by the federal government. In 1996, CaliforniaAir Resources Board (CARB) required the introduction of cleaner-burninggasoline (CBG) throughout the state in order to reduce vehicle emissions ofpollutants that cause or contribute to various health problems.3 The pre-cisely targeted, inflexible regulations of California’s CBG required the removalof particularly harmful compounds from gasoline. CBG is likely to have thelargest impact on people living near highways, given the documented relation-ship between distance from highways and level of traffic-related air pollution(Gilbert et al., 2003). In this paper, I exploit spatial variation in children’sexposure to highways to estimate the effect of gasoline regulation on both pol-lution and child health.4 It is clear that a cross-sectional comparison of peopleliving near and far from highways would be biased by differences in observableand unobservable characteristics, such as income, education and preference forclean air, which are correlated both with choice of residence and susceptibility
1See English et al. (1999); Weiland et al. (1994); Duhme et al. (1996); McConnell et al.(2006); Ryan et al. (2005); van Vliet et al. (1997); Brunekreef et al. (1997); Ciccone et al.(1998); Friedman et al. (2001); Wilhelm and Ritz (2003).
2Brown et al. (2008) estimate that the price to consumers increased by an average of3 cents/gal in metropolitan areas with gasoline content regulations, relative to a controlgroup. The price effect, however, varied by 8 cents/gal across different regulated marketsdepending on geographic isolation.
3Although this paper focuses childhood asthma, cleaner-burning gasoline may improvehealth along many dimensions, such as reductions in heart and lung disease and cancer.
4Recent research has suggested that traffic pollution can travel up to 1km from thehighway (Hu et al., 2009). Throughout this paper I consider the area of exposure to bewithin 1km of a highways. However, the results are robust to smaller areas, such as within300m of highways, as shown in Table 9.
2

to asthma.5 However, my identification strategy requires only that the differ-ences between these neighborhoods near and far from highways remain fairlyconstant or change smoothly over time.6 Using a differences-in-differencesframework I examine the between-location difference in both pollution andasthma incidence before and after the introduction of CBG. These estimatesare unbiased as long as the neighborhood characteristics do not shift discon-tinuously at the time of the CBG regulation in 1996.
Previous literature establishing the link between air pollution and healthhas exploited natural experiments to avoid the inherent endogeneity prob-lems of cross-sectional comparisons (Chay and Greenstone, 2003a,b; Lleras-Muney, 2010; Currie and Walker, 2011; Neidell, 2004; Currie and Neidell,2005; Schlenker and Walker, 2015). For example, Neidell (2004) and Currieand Neidell (2005) exploit seasonal variations in pollution within zip codes toidentify pollution’s impact on child asthma hospitalizations and infant mor-tality. Knittel, Miller and Sanders (2015) go further in trying to understandthe role that automobile congestion plays in impacting pollution and infantmortality. One important way that policy makers can try to reduce the neg-ative impact of automobile congestion on health is through gasoline contentregulations. However, existing research has yet to document whether gasolinecontent regulations can be successful in protecting health. Instead, researchon gasoline content regulations has focused on the production response of re-fineries, the impact on price and price volatility, and the improvements inair quality (Auffhammer and Kellogg, 2011; Brown et al., 2008; Muehlegger,2002). When refiners are granted flexibility in deciding which specific com-pounds to remove from gasoline, they chose to remove the cheapest, ratherthan the most harmful pollutants.7 Auffhammer and Kellogg (2011) find that
5In fact, Table B1 in the appendix shows that census tracts near the highway have alarger percentage of non-white residents, a larger percentage of Hispanics, a larger percent-age of single female households with young children, lower levels of educational attainment,a larger percentage of foreign born and non-citizens, higher unemployment, a larger per-centage of blue collar workers, and a greater percentage below the poverty level. Clearly,a cross-sectional comparison would be biased by the differences in underlying populationcharacteristics that are known to be related to health outcomes as well.
6Neighborhood characteristics are somewhat stable over time since people are not per-fectly mobile and the housing market is not perfectly fluid. In fact, according to census2000 estimates, about 80% of residents lived in the same county for the previous 5 years,and 50% remained in the same house. Table B1 in the appendix provides some evidencethat the difference-in-difference estimates of demographic characteristics remain fairly stablebetween areas near and far from highways before and after the policy of interest.
7Pollution abatement policies are often met with unintended consequences that reduceeffectiveness (Henderson, 1996). For example, driving restrictions based on the last digit ofthe vehicle’s license plate in Mexico City failed to improve air quality as drivers responded
3

only the precisely targeted, inflexible CBG regulations improved air quality.However, the health impacts of gasoline content regulations have not yet beenquantified.
This paper asks whether or not CBG improved health outcomes, mea-sured by childhood asthma, by reducing pollution. Identifying the pollutionreduction and associated health benefits from CBG is especially importantgiven that the U.S. EPA has been moving from less restrictive federal gasolineregulations to regulations that bring the nation closer to stringent Californiastandards (CARB, 2008b). I contribute to the literature in several ways.
First, I quantify the impact of CBG on three criteria pollutants: NO2,CO, and SO2. Whereas Auffhammer and Kellogg (2011) estimate air qualityimprovements off of the county-level ozone reductions in California relativeto ozone levels in the rest of the U.S., the results presented in this paperexploit within state, zip code level variation in exposure to highway pollutionto identify the impact of CBG on pollution in California. Estimates show adecline of about 2 percent, 6 percent, and 10 percent in high exposure areasfor NO2, CO, and SO2, respectively.
Second, I quantify the impact of CBG on childhood asthma hospitaliza-tions. Although cleaner-burning gasoline may impact health along severaldimensions, I focus on childhood asthma because it is prevalent, the cost ofhospitalization is high, and children are especially vulnerable to air pollution.Zip code level estimates indicate that CBG caused an 8 percent decline inchildhood asthma hospitalizations in high exposure areas. Using confidentialdata containing a unique patient identifier, I am able to link patients over timeand estimate the change in an individual’s probability of hospital admission forasthma and the length of stay after the policy. The individual level estimatessuggest that CBG reduced the probability of asthma hospitalization by about3 percent and decreased length of stay by about 6 percent.
Third, I examine the impact of cleaner-burning gasoline on a proxy forinfant death to show suggestive evidence infant deaths declined by about 10percent in high exposure areas, which translates into large value-of-life costsavings for gasoline content regulation.8 Fourth, I present a cohort level anal-ysis to estimate the cumulative effect of exposure to CBG and show that thehealth benefits of regulation grow over time as pollution effects accumulate.Finally, I explore heterogeneous effects for the impact on both pollution and
by purchasing more vehicles (Davis, 2008).8According to the CDC, the top two causes of infant death are congenital abnormalities
and disorders related to short gestation and low birth weight, accounting for about 38 percentof infant deaths. Air pollution has been shown to impact fetal growth and development inutero and to increase the chance of congenital abnormalities.
4

asthma. I exploit data on the prevailing wind direction to explore differen-tial effects of CBG on downwind, crosswind, and upwind zip codes. Resultssuggest that downwind zip codes experience the greatest declines in pollutionand asthma. I also make use of traffic data to look for heterogeneous effectsby level of highway usage. Findings suggest that high traffic highways exhibitgreater reductions in pollution and asthma. Additionally, I explore differentialeffects by race, age, and gender. I show that the improvement in asthma wasstrongest for black children. Since families living near highways are more likelyto be lower in socio-economic status, reductions in highway pollution benefita disadvantaged population that already suffers disproportionately adversehealth outcomes, including asthma.
The paper is organized as follows. Section 1 motivates the paper andprovides background on asthma, pollution, and the CBG regulations. Section 2describes the data and defines key variables. Section 3 describes the empiricalstrategy for estimating the impact of regulation on both pollution and asthma.Section 4 shows the results, and Section 5 tests the robustness of the mainresults. Section 6 provides some discussion and a cost-benefit analysis, andSection 7 concludes.
1 Motivation and Background
1.1 Asthma and Pollution
Childhood asthma is a prevalent and costly condition affecting millions of chil-dren in the United States. Over 10 million U.S. children under the age of 18(14%) have at one time been diagnosed with asthma, 7 million (10%) stillhave asthma, and 4 million (55%) of those with asthma experience asthma at-tacks (CDC, 2012). Asthma is more likely among non-Hispanic black children,children in poor families, and children in fair or poor health (Bloom, Jonesand Freeman, 2013). According to the California Environmental ProtectionAgency, nearly 667,000 school-aged children in California have experiencedasthma symptoms during the past year (CARB, 2013). One important asthmatrigger is outdoor air pollution.
Children are especially vulnerable to air pollution for several reasons. First,early exposure to pollution can alter lung development and function. Second,children spend a considerable amount of time engaging in physical activitiesoutdoors. Increases in breathing rate lead to larger levels of environmentalpollutants in the respiratory tract. Finally, children are predominantly oralbreathers, meaning that air by-passes the nasal filter and more particles may
5

enter lower airways (Esposito et al., 2014).Air pollution is associated with an increased risk of asthma exacerbation
and acute respiratory infections. In general, existing evidence of the relation-ship between specific pollutants and asthma is unclear and sometimes conflict-ing (Barnes, 1995; Esposito et al., 2014). It is thought that SO2 particles mayact as irritants, stimulating sensory nerves in the airways to induce cough,bronchoconstriction, and increased mucus secretion. NO2 may induce air-way inflammatory changes, but the mechanisms through which this occurs arenot well understood. Although there is no consensus on the exact biologicalmechanisms through which criteria pollutants impact asthma, epidemiologicalstudies have found that patients with asthma are affected by NO2, CO, andSO2 (Sheppard et al., 1980; Huang, Wang and Hsieh, 1991; Orehek et al.,1976; Kleinman et al., 1983; Bauer et al., 1986; Koenig, Pierson and Horike,1983; Leikauf, 2002).9
The prevalence of asthma imposes a great financial burden across the U.S.health care system. Direct costs include payments for ambulatory care visits,hospital outpatient services, hospital inpatient stays, emergency departmentvisits, physician and facility payments, and prescribed medications. Indirectcosts can also result from missed work or school, and days with restricted workactivity. Smith et al. (1997) estimate that the total costs of asthma (directand indirect) were $5.8 billion in 1994. Hospital expenditures accounted forover half of all expenditures for asthma. Total costs for childhood asthma werealmost $2 billion in 1996 (Wang, Zhong and Wheeler, 2005).10
1.2 Gasoline Content Regulation
Prior to cleaner-burning gasoline regulations, gasoline powered vehicles pro-duced about half of all air pollution in California, according to the Cali-fornia Environmental Protection Agency. California’s reformulated gasoline
9Furthermore, certain Hazardous Air Pollutants (HAPs) may exacerbate asthma be-cause, once sensitized, individuals can respond to remarkably low concentrations, and theseirritants can lower the bronchoconstrictive threshold to respiratory antigens. Benzene and1,3-Butadiene, both restricted by CBG regulations, appear on a list of the 19 compoundswith the highest potential impact on the induction or exacerbation of asthma (Leikauf,2002). Unfortunately, data on these HAPs are sparse and I will not be able to show a firststage for these pollutants. Although it is not possible to estimate the impact of the CBGrestriction on HAPs, reduced form results estimate the impact of CBG on asthma and willinclude the impact of both the reduction in criteria pollutants and the reduction in HAPs.
10Direct medical expenditure was estimated at $1 billion, parents’ loss of productivityfrom asthma-related school absence days was $719.1 million, and lifetime earnings lost fromasthma-related death of children was $264.7 million.
6

(CaRFG) program set stringent standards for gasoline to reduce emissions fromgasoline-powered vehicles.11 The program was implemented in three phases.12
The most significant changes occurred with the introduction of cleaner-burninggasoline (CBG) in Phase 2, which set specifications for sulfur, aromatics, oxy-gen, benzene, T50, T90, olefins, and RVP. Specifically, CBG requires an 80percent reduction in the sulfur content of gasoline to reduce the emission ofSO2 and NOx. It also calls for added oxygen, which is intended to reduceCO.13
California’s EPA estimated that CBG would cause a reduction in theamount of on-road pollution from NOx (11%), CO (11%), and SO2 (80%).14
Given that on-road pollution accounts for about 53 percent, 79 percent, and7 percent of total NOx, CO, and SO2 emissions, one would expect to see anoverall decline of about 5.8 percent, 8.7 percent, and 5.6 percent, respectively,based on the projections (CARB, 2008a; EPA, 2000). This paper finds ev-idence to support the expected reduction in air pollution following CBG inareas near highways. Estimates show a decline of about 2, 6, and 10 percentin high exposure areas for NO2, CO, and SO2, respectively.15 It is not sur-prising that the findings are slightly smaller than projected estimates, becausethe control group (low exposure to highways) may also experience a small re-duction in pollution. Therefore, estimates of total pollution reduction will beunderstated.
11The new stringent state-wide gasoline standard affected all cars simultaneously, unlikerestrictions made to engines and vehicles, such as low-emission vehicle standards, which areimplemented only through vehicle turnover.
12Phase 1 eliminated lead from gasoline and set regulations for deposit control additivesand reid vapor pressure (RVP) in 1992. However, lead limits had already been decreasedsignificantly by this time to a limit of 0.8 g/gal and the lead phase-down efforts had alreadydecreased lead usage in gasoline by 99 percent between 1977 and 1989 (from 16,500 to 194tons). Several major oil companies had already phased out leaded gasoline and ambientconcentrations had already fallen so low that the official elimination of lead from gasolinewas unlikely to have a dramatic impact. Phase 3 eliminated methyl-tertiary-butyl-ether(MTBE) from California gasoline in January of 2003, which is after the sample periodstudied in this analysis.
13CBG places a cap on the benzene content of gasoline at 1 percent by volume, andapplies a 7.0 psi RVP limit. There is also a limit on the concentrations of two other classesof VOCs that are highly reactive: olefins (6 percent by volume) and aromatic hydrocarbons(25 percent by volume).
14California’s EPA also estimated a reduction in smog-forming gases, volatile organiccompounds (17%), benzene, and 1,3-butadiene.
15One might be concerned that trading markets for SO2 and NOx were responsible forthis decrease in pollution, but this is unlikely to be the case. Section 5.3 addresses theseprograms in detail.
7

2 Data
Patient Discharge DataThe California Patient Discharge Data is an extensive source of individualhealth outcomes. This dataset is comprised of a record for each inpatient dis-charged from a licensed acute care hospital in the state of California. Dataare available from 1992 to 2000, and each year contains information on theprincipal diagnosis of the patient upon release from the hospital, zip code ofthe patient’s residence, age, sex, race, ethnicity, and the expected principalsource of payment. Although hospital data does not include information onall asthma attacks that occur in a given period, hospital discharges are a moreobjective measure than self-reported surveys which could be subject to report-ing biases.16 Furthermore, this dataset provides a large number of observationsat a fine geographic scale across the entire state of California, whereas manysurveys are only representative of select MSAs and large counties.
The primary outcome variable of interest, Asthma, is defined using the In-ternational Classification of Diseases, Ninth Revision, (ICD-9) codes to identifypatients admitted to the hospital for asthma related conditions (code 493).17,18
The population of interest in this paper will be children under 10 years of age,since this is an especially vulnerable population. Therefore, Asthma is definedas the number of childhood discharges for asthma, per 10,000 children underage 10, for each zip code.19
Asthmax =
∑i 1{PrimaryDiagnosisix = Asthma}
Populationx
(1)
for each x ∈ X, where X is the set of all zip code-year combinations and iindexes individuals. The preferred specification also includes all respiratory
16According to the CDC, asthma hospitalizations occur at the rate of about 2 per 100persons with asthma.
17The International Classification of Diseases (ICD) is maintained by the World HealthOrganization and is designed as the international standard health care classification system.It provides a system of diagnostic codes for classifying diseases, including generic categoriestogether with specific variations.
18The results are very similar when DRG codes (DRG code 98 for bronchitis and asthma)are used to identify asthma hospitalizations rather than ICD-9 codes. Diagnosis-relatedgroup (DRG) is a system used to classify hospital cases into different groups. Becausepatients within each classification are clinically similar, DRGs have been used in the U.S.since 1982 in order to determine Medicare reimbursement to hospitals.
19The 1990 and 2000 U.S. Census data will provide population counts by age, race, andgender for each zip code. I use linear interpolations of population to calculate the numberof children in each zip code for each year between 1990 and 2000.
8

related discharges for children less than one year old, since diagnosis of asthmaamong infants is especially difficult (Martinez et al., 1995).20
Another outcome variable, InfantDeaths, is defined using the diagnosisrelated group (DRG) code 385 for “neonate, died or transferred to anotheracute care facility.”21 Similar to the asthma measure, it is defined as the num-ber of patients with DRG code 385 per 10,000 infants for each zip code, whereinfant is defined as less than one year old. Although this is not a perfect mea-sure of infant deaths, since it contains some transfers, it is a good proxy forinfant deaths.
Highways and Traffic DataInformation on the location of highways comes from combining data on U.S.and State Highways from the U.S. Census Bureau’s 2000 TIGER/Line geo-graphical information systems (GIS) shapefiles, available through the Cali-fornian Spatial Information Library. The highway data is spatially linked toCartographic Boundary files for census tracts and zip codes using ArcMap10.1. For the purposes of this paper, a highway refers to either a U.S. or Statehighway, as defined by the U.S. Census Bureau (see Appendix A).
Traffic volume data comes from California’s Department of Transporta-tion, Division of Traffic Operations for 2011. Although traffic volume data isnot available for the study period, 1992-2000, traffic volumes from 2011 arestrongly correlated with past volumes.22 Annual average daily traffic (AADT)is recorded for 6,926 count locations on Californian highways. Using ArcMap10.1 to determine zip code proximity to highways and AADT count locations,I calculated the average AADT level for each zip code. For the purposes ofthis paper, I consider high traffic roads to have an average AADT of at least60,000 vehicles per day, which is consistent with the literature.
Air Pollution DataDaily data on air pollution comes from the EPA’s Air Quality System (AQS)
20The results have been estimated for an outcome variable that restricted the under 1age category to only those with asthma diagnoses, excluding infants with a diagnosis of anyother respiratory condition. These results are similar, although less well identified for theyoungest age group for whom it is difficult to diagnose asthma.
21Ideally, California Department of Public Health Birth Cohort files would provide linkedbirth and death files for infants. Unfortunately, geographic information is not available forthe Birth Cohort files prior to 2002.
22Using information on the highway post mile traffic recording location, I link 1901 record-ing locations between 2011 and 2001. The correlation between traffic volumes (Back AADT)in 2011 and 2001 is 98.5%. Since the correlation is so high, I utilize the more precise geo-graphic information from the geocoded 2011 data.
9

Data Mart through AirData. Daily air quality summary statistics are availablefor the criteria pollutants NO2, CO, and SO2 by monitor for the state ofCalifornia.23 There are 275 monitors throughout California that have readingsduring the sample period of 1992 to 2000. There may be some concern aboutendogenous placement of monitors during the sample period if the placementof new monitors coincides with locations that experience an unusually largechange in pollution. Therefore, the main specifications limit the sample toconsistently observed monitors, which are monitors observed for at least 3months in every year of the sample period. Pollution monitors record differenttypes of criteria pollutants. For the sample of consistently observed monitors,90 record NO2, 74 record CO, and 30 record SO2. Results are similar for thefull sample of monitors.
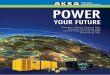
Air quality monitors are located throughout California, as shown in Fig-ure 1. Generally, monitors are more likely to be located in areas with higherpopulation density. Although there are many monitors recording NO2 andCO levels, a sparsity of monitors for SO2 will cause more noise in estimatesfor this pollutant.
To link Californian air quality monitors with zip codes, I follow the method-ology used in Neidell (2004) and Currie and Neidell (2005). First, I calculatethe monthly average measure of pollution for each air quality monitor. I findthe centroid of each zip code and create a weighted average of all monitorswithin 20 miles of the centroid, using the inverse of distance to the centroidas the weight.24
Another option is to use Kriging, which is a popular method of interpola-tion based on estimating the parameters that describe the spatial correlationbetween observed data points and then using these estimates to find predic-tions that minimize the sum of squared errors.25 Some research has suggestedthat Kriging methods provide superior predictions over deterministic interpo-lation (Lleras-Muney, 2010; Anselin and Le Gallo, 2006; Zimmerman et al.,1999). Although the main results are based on inverse distance weighting,I also estimate results in Appendix Table C4 based on the Kriging method-
23NO2 and SO2 are measured as the mean daily maximum 1-hour concentration, whileCO is measured as the mean daily maximum 8-hour concentration, following EPA standards.
24The results were estimated using a weighted average of all monitors within alternativedistances from the centroid with similar results. Neidell (2004) and Currie and Neidell (2005)also test the validity of these weighted averages by comparing the actual level of pollution ateach monitor location in California with the level of pollution that would be assigned usingtheir method if the monitor in question was not located there. These correlations betweenactual and predicted levels of pollution were very high (0.77-0.92).
25See Cressie (1993) for methodological details.
10

Figure 1: Air quality monitors
Legend
NO2 monitors
CO monitors
SO2 monitors
ZCTA 0 80 16040 Miles
Los Angeles
Notes: Air quality monitors are shown for all monitors consistently observed from 1992 to2000 with measurements for pollution recorded for at least 3 months in every year of thestudy period.
11

ology.26 One additional benefit is that the Kriging methodology provides ameasure of the accuracy of the predictions. Results weighted by the inverseof the prediction error are also shown in the appendix and remain of similarmagnitude.
Wind and Weather DataWeather data were obtained from the National Climatic Data Center’s (NCDC)Global Summary of the Day files. Available weather elements include meanvalues of: average temperature, minimum and maximum temperature, dewpoint temperature, wind speed, maximum sustained wind speed and maxi-mum gust, and precipitation amount. These data comprise daily averagescomputed from global hourly station data. Daily mean dew point and tem-peratures were reported in degrees Fahrenheit. Daily absolute humidity, inpounds mass per cubic foot (lbm/ft3), was calculated from daily dew pointand temperature, following standard meteorologic formulas (Parish and Put-nam, 1977). Zip code specific weather measures were calculated using the sameinverse distance weighting methodology as the pollution measures describedabove.
Wind direction comes from the GHCN (Global Historical ClimatologyNetwork)-Daily database obtained from NOAA’s National Climatic Data Cen-ter. GHCN-Daily is an integrated database of daily climate summaries fromland surface stations across the globe. Average wind directions are calculatedfor the 79 stations in California recording wind direction during the study pe-riod. Using ArcMap 10.1, the prevailing wind direction is interpolated acrossCalifornia using inverse distance weighting (see Figure A2 in the appendix fora map of prevailing wind direction and station locations).
I designate zip codes into one of three groups: downwind, crosswind, orupwind from the highway. Groups are based on the difference between theangle from which the prevailing wind originates and the angle from the zipcode centroid to the nearest highway. If these two angles are very similar,the zip code is most likely downwind from the highway. As seen in Figure 2,downwind, crosswind, and upwind zip codes are those with an absolute valueangle difference less than 45, 45 to 135, and over 135 degrees, respectively (seeFigure A3 in the appendix for a map of zip code classifications). Zip codeslocated downwind (upwind) from the highway are likely to experience thegreatest (lowest) levels of traffic-related air pollution. The prevailing wind di-rection is fairly consistent across time in this region. When considering yearly
26Details of the models that were used to generate Kriging predictions are available fromthe author on request.
12

Figure 2: Wind and highway direction degree difference
-165-15
0-13
5
-120
-105-90
-75
-60
-45-30
-15 0 1530
45
6075
90
105
120
135
150165180
Downwind
Crosswind
Upwind
Crosswind
variation in wind direction, zip codes I classify as downwind are downwind 76percent of the time.
3 Empirical strategy
3.1 Treatment Designation
Research has shown that traffic pollution can travel up to 1km from high-ways in California (Hu et al., 2009). Ideally, patient addresses would identifywhether or not an individual lived within 1km of a highway. However, due topatient confidentiality constraints, only zip code of residence is available in thedata.27 Using data on the location of highways in California and census tract
27I have made some assumptions about where people spend the majority of their time. Forchildren, school location may matter, since school attendance may encompass a significantportion of their time. Epidemiological research suggests that asthma risk increases withtraffic-related pollution exposure near both homes and near schools, and that a dispropor-tionate number of economically disadvantaged and nonwhite children attend high-exposureschools in California (McConnell et al., 2010; Green et al., 2004). However, given the currentassumptions, as long as children are likely to attend school within their own residential zipcode, the results should be unaffected by this distinction.
13

population data from the 2000 Census to determine within zip code densityof population, I calculate the percentage of the population of a zip code thatis living within 1km of a highway, τ .28 I present results using this continuousmeasure of τ , but for ease of interpretation I also create a binary treatmentindicator using the median value as a cut point.29
Figure 3 shows the location of treatment and control zip codes in California,based on this definition. Treated zip codes are dispersed across the entire stateand do not represent any specific region. Even within Los Angeles, a denselypopulated area, there are zip codes assigned to both the treatment and controlgroups.
3.2 First Stage Strategy: Pollution
Summary statistics for the criteria pollutants and raw difference-in-differenceestimates are shown in Table 1. All three pollutant levels are higher in thetreatment zip codes relative to the control, which is to be expected. The finalcolumn shows that the gap in pollution level between treatment and control zipcodes is narrowing after the policy. This raw difference-in-difference estimateis significant for each pollutant.
With pollution measures linked to zip codes, I can calculate the difference-in-difference estimates of the implicit first stage effects of CBG regulation onpollution. The preferred specification will be as follows:
Pollutionzt = B0 +B1Treat∗Afterzt + Zz + Θy +Qq +B2timet + ε1zt (2)
where z indexes zip codes and t indexes time, in months. Treat is equal toone if the zip code is considered treated. After is equal to one after CBG takeseffect. The results are estimated with zip code fixed effects, Zz, year dummies,Θy, quarter dummies, Qq, and a linear time trend, timet. Standard errors areclustered at the zip code level. The parameter of interest, B1, estimates thechange in pollution concentration in treatment relative to control zip codesfollowing the implementation of CBG. The results presented in the next sectionprovide further evidence that pollution dropped significantly in zip codes withmany people living close to the highway after the CBG regulations.
28Figure A4 in Appendix A shows the map of U.S. and state highways in California.Figure A1 in Appendix A shows the distribution of τ across zip codes in CA.
29The choice of a cutoff value is somewhat arbitrary, but the results are robust to alter-native choices of a cutoff value. These results are shown in Table C2 of the Appendix C.
14

Figure 3: Treatment and control zip codes
Los Angeles
Legend
US & State Highways
Control Zipcodes (median)
Treat Zipcodes (median) 0 80 16040 Miles
Notes: Treated (control) zip codes are those with at least (less than) the median percentage,42.5%, of the zip code population living within 1km of a highway. Some areas of Californiaare not covered by zip codes and these areas are left blank.
15

Table 1: Summary statistics and raw diff-in-diff: pollution and asthmaBefore After Diff-in-diff
Control Treat Diff Control Treat DiffPollution
NO2 (ppb) 41.80 46.02 -4.220*** 37.01 40.70 -3.688*** -0.679***CO (ppm) 1.57 1.86 -0.285*** 1.19 1.43 -0.237*** -0.064***SO2 (ppb) 4.79 5.62 -0.829*** 4.61 4.93 -0.319*** -0.533***
Asthma 44.98 56.53 -11.544*** 42.08 49.18 -7.105*** -3.799**
Notes: Treated (control) zip codes are those with at least (less than) the median percentage, 42.5%, of thezip code population living within 1km of a highway. NO2 and SO2 are measured as the mean daily maximum1-hour concentration. CO is measured as the mean daily maximum 8-hour concentration, following EPAstandards. Asthma is the number of asthma admissions per 10,000 children, as defined in section 2.
3.3 Reduced Form Strategy: Asthma
Table 1 shows the overall level of asthma admissions in both treatment andcontrol zip codes before and after the policy. The raw difference-in-differenceestimate suggests a reduction in hospitalizations following CBG of about 3.8per 10,000 children.
The reduced form effect of CBG on child health at the zip code level isestimated with the following specification:
Outcomezy = δ0 + δ1Treat∗Afterzy + Zz + Θy + ε2zy (3)
where z indexes zip code and y indexes time, in years. The main outcomevariable, Asthmazy, is the number of childhood asthma admissions per 10,000children. InfantDeathszy is a secondary outcome variable of interest (seesection 2 for definitions). Treat is equal to one if the zip code is consideredtreated. After is equal to one after CBG takes effect in 1996. The results areestimated with zip code fixed effects, Zz, and year dummies, Θy. Standarderrors are clustered at the zip code level. The parameter of interest is δ1,which estimates the outcome change in treatment relative to control zip codesfollowing the implementation of CBG.
Using confidential data containing a record linkage number that is uniqueto patients, I am able to link the same patient across multiple admissionsover time and limit the sample to non-movers. I estimate the change in anindividual’s probability of being admitted to the hospital for asthma after thepolicy, as well as any change in the length of stay. The probability of admissionrepresents the extensive margin, while the length of stay corresponds to theintensive margin.30 The individual level analysis is estimated in the following
30Since the length of stay can be zero days, this estimation actually reveals changes inboth the intensive and extensive margins.
16

linear probability model:
BinaryAsthmaiy = ω0 + ω1Treat∗Afteriy + Ii + Θy + ε3iy (4)
where i indexes individuals and y indexes time, in years. The first outcomevariable, BinaryAsthmaiy is equal to one if a child has been admitted tothe hospital for asthma at least once during that year, and zero otherwise.Secondly, I utilize a Poisson model to estimate the impact on StayLengthiy(in days) as a proxy for severity, to see if there are any changes in the intensivemargin following the policy:
StayLengthiy = ν0 + ν1Treat∗Afteriy + Ii + Θy + ε4iy (5)
Individual fixed effects, Ii, and year dummies, Θy are included.31 These indi-vidual level estimates are based only on individuals who have been admittedto the hospital for asthma at least once during the study period and thereforemay not be representative for the general population. However, children whohave been admitted to the hospital are an important and expensive patientgroup. Any change in the probability of asthma admission or length of stayfor this group would be important for policy considerations.
4 Results
4.1 First Stage Results: Pollution
Graphical evidence of the reduction in pollution following CBG is shown inFigure 4, which shows the relationship between the change in pollution afterthe policy and the percent of the population living within 1km of a highway, τ .The change in pollution following the policy was calculated for each zip codeand local mean smoothing over exposure to highways shows that the decreasein pollution is largest for zip codes with the highest values of τ , as expected.
Table 2 shows the results from the estimation of equation (2) for each ofthe criteria pollutants, NO2, CO, and SO2. Panel A shows estimates based onthe binary treatment status indicator and Panel B shows estimates based onthe continuous measure of treatment status, τ . The regression results supportthe graphical evidence that pollution decreased after the implementation of
31Individual level regressions are limited to individuals who do not move during the studyperiod. Ages are restricted to be between 0 and 18 years old, and regressions are weightedby the number of observations during the study period. Length of stay is set to 1 day forindividuals who were admitted for asthma but stayed less than one day.
17

Figure 4: Change in pollution following CBG−
6−
5.5
−5
−4.
5−
4N
O2
0 .2 .4 .6 .8 1
95% CI ∆ NO2
NO2
−.5
5−
.5−
.45
−.4
−.3
5C
O
0 .2 .4 .6 .8 1
95% CI ∆ CO
CO
−1
−.5
0.5
SO
2
0 .2 .4 .6 .8 1
95% CI ∆ SO2
SO2
% population within 1km of highway
Notes: Shows the change in pollution levels from before to after the policy. The levelchange is calculated by zip code for NO2, CO, and SO2. Figures show the local meansmoothed relationship between the change in pollution and the percentage of the populationliving within 1km of a highway, τ . Zip codes nearer to the highway (i.e. values of τ near1) experienced the largest decreases in pollution after the policy. Lines show local meansmoothing using “lpoly,” with degree zero and a 0.1 bandwidth.
the CBG regulation in zip codes with a large percentage of the populationliving near a highway. Estimates indicate that NO2 pollution decreased byabout 2 percent from the pre-policy, treated zip code level. Similarly, CO pol-lution decreased by about 6 percent, and SO2 pollution decreased by about 10percent. These estimates are in line with the expected reductions in pollutionpredicted by California’s EPA, although their estimates were slightly largerfor NO2 and CO, and slightly smaller for SO2.
32
4.2 Reduced Form Results: Asthma
Graphical evidence of the reduction in asthma near highways after CBG canbe seen in Figure 5. One can see the smoothed relationship between asthmahospitalizations and the percentage of the zip code population living within1km of a highway, τ , over time. Solid and dashed lines indicate years beforeand after gasoline content regulation, respectively. After the implementationof CBG in 1996, the gradient shifts downward for zip codes with the largest τvalues. For lower values of τ , the gradient remains fairly consistent over time.As expected, the reduction in asthma after CBG is concentrated in zip codeswith a large percentage of the population living near the highway.
32Projected reductions for NOx, CO, and SO2 emissions were 5.8 percent, 8.7 percent,and 5.6 percent, respectively, as calculated in section 1.
18

Table 2: First stage: difference-in-difference estimates
NO2 CO SO2(1) (2) (3)
Panel A.Treat*After -0.870*** -0.104*** -0.597***
(0.160) (0.0101) (0.0835)
%∆ from pre-treat -1.9 -5.5 -10.7%∆ in gap -20.4 -35.9 -72.9%∆ of std dev -4.8 -9.9 -16.2
Panel B.%Close*After -1.510*** -0.214*** -1.215***
(0.247) (0.0157) (0.126)
Observations 112,055 114,387 73,625R-squared 0.797 0.733 0.521Zipcode FE yes yes yesYear dummies yes yes yesQuarter dummies yes yes yesTime trend yes yes yes
Notes: Panel A shows regression results based on the binary treat-ment status indicator. Panel B shows regression results based on thecontinuous measure of treatment status. Estimates are based on aconsistently observed set of monitors, as defined in section 2. Stan-dard errors clustered at the zip code level are in parentheses. ***p<0.01, ** p<0.05, * p<0.1
19

Further graphical evidence of the decrease in childhood asthma can be seenin Figure 6. The left panel shows the raw means by year for treatment andcontrol zip code groups. As expected, there is a level difference between thetwo groups, with asthma hospitalizations higher in the treatment group. Priorto the policy, these two lines follow similar yearly patterns with shocks affectingboth treatment and control groups in the same way. After the policy, the gapbetween the treatment and control groups decreases as the level of asthma inthe treatment group becomes more similar to that of the control group, asexpected. The right panel plots the difference between treatment and controlgroups by year. The difference is fairly constant at around 12 hospitalizationsper 10,000 children prior to the policy. This difference between treatment andcontrol group drops in 1996 and continues in a downward trend.
Figure 5: Asthma hospitalizations by exposure to pollution
3040
5060
70A
sthm
a
0 .2 .4 .6 .8 1% pop within 1km of highway
92−93 94−95 96 97−98 99−00
Notes: Figure shows the smoothed relationship between asthma hos-pitalizations (per 10,000 children under age 10) and the percentage ofthe population living within 1km of a highway, τ , in different years.Dashed and solid lines indicate years after and before the policy,respectively. Lines show local mean smoothing using “lpoly,” withdegree zero and a 0.07 bandwidth.
Regression results showing estimates of equation 3 support the graphicalevidence. Table 3 shows the difference-in-difference estimates of the effectof CBG on asthma. Panel A shows estimates based on the binary treatmentstatus indicator and Panel B shows estimates based on the continuous measure
20

Figure 6: Mean asthma hospitalizations over time35
4045
5055
60A
sthm
a
1992 1994 1996 1998 2000Year
Treat Control
24
68
1012
Ast
hma
1992 1994 1996 1998 2000Year
Difference (Treat − Conrol)
Notes: The left panel shows raw mean childhood asthma hospitalizations (per 10,000 chil-dren under age 10) by year for the treatment and control groups, separately. The right panelplots the difference in the average yearly asthma hospitalization level between treatment andcontrol groups.
of treatment status, τ .33 Columns (1)-(7) present the zip code level estimates.Column (1) includes zip code fixed effects and a dummy indicating the post-policy period. Columns (2)-(7) weight the regression results by zip code childpopulation to give greater weight to the more precisely estimated zip codes.Column (3) includes year dummies to account for any widespread yearly shocksto asthma affecting all zip codes.
One might be concerned that treated zip codes are more likely urban andthat differential changes in certain urban centers throughout this period maydifferentially impact health. To address this concern, column (4) includes CoreBased Statistical Area (CBSA)-year specific dummies to control flexibly fordifferential trends or shocks in each CBSA. In addition, column (5) includeszip code specific linear time trends to account for any differential long-runchanges that occur over time for each zip code. The estimates in columns(4)-(5) remain significant and of similar magnitude. Finally, column (6) usesan age-adjusted outcome measure for the asthma rate to account for differ-ent prevalence rates among age groups. The results remain consistent acrossthese specifications, suggesting a statistically significant reduction of about4.5 asthma hospitalizations per 10,000 children following CBG implementa-tion. This is a reduction of about 8 percent from the pre-policy treatment zipcode level, or a reduction in the treatment-control asthma gap of 40 percent.
33Figure C5 in the appendix shows results from a non-parametric specification based onbinned values of τ .
21

Column (7) presents estimates of the impact on infant deaths, indicatingthat CBG reduced infant deaths by about 24 per 10,000 children under age1. This is a reduction of about 10 percent from the pre-policy treatment zipcode level. However, it is important to remember that the outcome variablealso contains neonatal transfers, so although it appears that infant deaths aredecreasing by 10 percent, some of this may be due to decreases in transfers.
The last two columns show individual level estimates. Column (8) presentsthe individual level estimate of the linear probability model in equation 4.After including individual level fixed effects and year dummies, the resultssuggest CBG reduced the probability of asthma hospitalization by about 0.8percentage points, or 3 percent from pre-policy treatment levels. Not only didCBG reduce the probability of an asthma hospitalization, but it decreased theseverity of hospitalizations, as proxied by length of stay. The final columnestimates the Poisson model from equation 5 where the outcome variable islength of stay in days per hospital visit. The coefficient implies that days inthe hospital declined significantly, by about 6 percent.34
34100× [exp(−0.0638)− 1] ≈ −6.18%
22

Tab
le3:
Red
uce
d-f
orm
impac
ton
asth
ma
Zip
code
leve
lan
alysi
sIn
div
idual
leve
lan
alysi
sA
sthm
aA
sthm
aA
sthm
aA
sthm
aA
sthm
aA
sthm
aIn
fant
Dea
thA
sthm
aL
engt
h(b
inar
y)
ofSta
y(1
)(2
)(3
)(4
)(5
)(6
)(7
)(8
)(9
)Pan
elA.
Tre
at*A
fter
-4.0
74**
*-4
.514
***
-4.5
05**
*-4
.113
***
-4.0
20**
*-4
.587
***
-24.
84**
*-0
.008
07**
*-0
.063
8***
(1.3
12)
(1.1
56)
(1.1
57)
(1.2
06)
(0.9
19)
(1.4
38)
(8.1
66)
(0.0
0252
)(0
.007
40)
%∆
from
pre
-tre
at-7
.21
-7.9
9-7
.97
-7.2
8-7
.11
-6.7
0-1
0.2
-3.2
%∆
inga
p-3
5.3
-39.
1-3
9.0
-35.
6-3
4.8
-51.
4-4
42.8
-82.
3%
∆of
std
dev
-9.7
8-1
0.8
-10.
8-9
.88
-9.6
5-9
.30
-11.
9-1
.8Pan
elB.
%C
lose
*Aft
er-7
.603
***
-7.8
89**
*-7
.865
***
-6.9
13**
*-6
.192
***
-7.7
11**
*-4
2.08
***
-0.0
133*
**-0
.092
3***
(2.3
51)
(2.0
71)
(2.0
71)
(2.2
67)
(1.3
11)
(2.5
60)
(15.
53)
(0.0
0490
)(0
.014
2)
Obse
rvat
ions
11,5
6811
,568
11,5
6811
,568
11,5
6810
,449
11,4
2560
0,85
850
9,88
8R
-squar
ed0.
615
0.80
80.
823
0.84
30.
854
0.81
10.
514
0.22
7-
Indiv
idual
FE
--
--
--
-ye
sye
sZ
ipC
ode
FE
yes
yes
yes
yes
yes
yes
yes
--
Pop
Wei
ghts
no
yes
yes
yes
yes
yes
yes
--
Yea
rdum
mie
sno
no
yes
no
no
yes
yes
yes
yes
CB
SA
-yea
rdum
mie
sno
no
no
yes
no
no
no
--
Zip
tren
ds
no
no
no
no
yes
no
no
--
Age
-adju
sted
no
no
no
no
no
yes
--
-
Not
es:
Pan
elA
show
sre
gre
ssio
nre
sult
sb
ased
on
the
bin
ary
trea
tmen
tst
atu
sin
dic
ato
r.P
anel
Bsh
ows
regre
ssio
nre
sult
sb
ased
on
the
conti
nuou
sm
easu
reof
trea
tmen
tst
atu
s.T
he
ou
tcom
eva
riab
lefo
rco
lum
ns
1-6
isth
enu
mb
erof
chil
dh
ood
ast
hm
aad
mis
sion
sp
er10,0
00
chil
dre
n,
as
defi
ned
inse
ctio
n2.
Colu
mn
4in
clu
des
CB
SA
-yea
rd
um
mie
san
dco
lum
n5
incl
ud
eszi
pco
de
spec
ific
lin
ear
tren
ds.
Th
eou
tcom
eva
riab
lefo
rco
lum
n7
isth
enu
mb
erof
“neo
nate
s,d
ied
or
tran
sfer
red
”(D
RG
cod
e385
)p
er10,0
00
infa
nts
,as
defi
ned
inse
ctio
n2.
Colu
mn
8is
aL
inea
rP
rob
abil
ity
Mod
elw
her
eth
eoutc
om
eis
ab
inary
vari
able
equ
alto
on
eif
anin
div
idu
alw
asad
mit
ted
toth
eh
osp
ital
for
ast
hm
ain
each
year.
Colu
mn
9is
aP
ois
son
mod
elw
her
eth
eou
tcom
eva
riab
leis
the
len
gth
of
stay
per
vis
itin
day
s.C
olu
mn
s8-9
are
rest
rict
edto
non
-mov
ers
bet
wee
n0
an
d18
years
old
an
dare
wei
ghte
dby
the
nu
mb
erye
ars
ob
serv
edp
erp
erso
n.
Sta
nd
ard
erro
rsare
clu
ster
edat
the
zip
cod
ele
vel
for
colu
mn
s1-7
an
dat
the
ind
ivid
ual
level
for
colu
mn
s8.
***
p<
0.0
1,
**
p<
0.0
5,
*p<
0.1
23

4.3 Heterogeneous & Cumulative Effects
Heterogeneous Effects: Wind DirectionThe results presented above show that CBG did indeed reduce childhoodasthma in zip codes with a large portion of residents living near highwaypollution. However, this analysis does not consider how wind direction mightinfluence pollution dispersion from highways. It is likely that residents down-wind from a highway experience higher levels of highway pollution and mayhave benefited even more from cleaner-burning gasoline than residents upwindfrom a highway. In this analysis I use data on the prevailing wind directionduring the study period, as described in section 2, to estimate the impact ofCBG in downwind, crosswind, and upwind zip codes.
Figure 7 shows the smoothed relationship between asthma and the percentof the population living near the highway, τ , by year for downwind and upwindzip codes, separately. Clearly, for downwind zip codes, there is a strong positiverelationship between asthma and the percent of the population living near ahighway. Asthma rates are especially high for zip codes where over 80% ofthe population lives near a highway. For upwind zip codes, there is an almostflat relationship between asthma rates and percent of the population near thehighway. As one might expect, this suggests that living near the highway in adownwind zip code is much more detrimental to health than living upwind.
Figure 8 is analogous to Figure 6 but for only downwind zip codes. The leftpanel shows the yearly means for treatment and control zip codes. As before,there is a level difference between the two groups, with asthma hospitaliza-tions higher in the treatment group, where more of the residents live within1km of the highway. After the policy, the level of asthma in the treatmentgroup becomes more similar to that of the control group, and the gap narrows.The right panel plots the difference between treatment and control groups byyear for downwind zip codes. Compared to the full sample in Figure 6, thedownwind sample in Figure 8 shows an even more distinct drop in asthma atthe time of the policy. The right panel shows that the gap between treatmentand control downwind zip codes was increasing prior to the policy. It droppeddramatically in 1996 and then continued in a downward trend.
Regression results support this graphical evidence. Table 4 shows estima-tion of the following equations for pollution and asthma:
24

Figure 7: Asthma Gradient Over Time: Upwind vs. Downwind30
3540
4550
5560
6570
75A
sthm
a
0 .2 .4 .6 .8 1% pop within 1km of highway
Downwind
3035
4045
5055
6065
7075
Ast
hma
0 .2 .4 .6 .8 1% pop within 1km of highway
Upwind
92-93 94-95 96 97-98 99-00
Notes: Figures show the smoothed relationship between asthma hospitalizations and thepercentage of the population living within 1km of a highway, τ , in different years. Dashedand solid lines indicate years after and before the policy, respectively. Lines are smoothedusing “lpoly,” with degree zero and a 0.1 bandwidth. Downwind (upwind) zip codes aredefined as zip codes where the difference between the wind source angle and the anglefrom the zip code centroid to the nearest highway is less than 45 degrees (greater than 135degrees).
Figure 8: Mean Asthma Hospitalizations Over Time: Downwind
3035
4045
5055
Ast
hma
1992 1994 1996 1998 2000Year
Treat Control
810
1214
16A
sthm
a
1992 1994 1996 1998 2000Year
Difference (Treat − Conrol)
Notes: Sample is limited to downwind zip codes, where the difference between the windsource angle and the angle from the zip code centroid to the nearest highway is less than45 degrees. The left panel shows raw mean childhood asthma hospitalizations by year forthe treatment and control groups, separately. The right panel plots the difference in theaverage yearly asthma hospitalization level between treatment and control groups.
25

Pollutionzt =λ0 + λ1DD∗Downzt + λ2DD
∗Crosszt + λ3DD∗Upzt+ (6)
Zz + Θy +Qq +Down∗zΘyκ+ Up∗zΘyχ+ ε5zt
Asthmazy =ϕ0 + ϕ1DD∗Downzt + ϕ2DD
∗Crosszt + ϕ3DD∗Upzt (7)
+ Zz + Θy +Down∗zΘyη + Up∗zΘyψ + ε6zy
where Down, Up, and Cross are indicators equal to one if the zip codeis downwind, upwind, or crosswind from a highway, respectively. DD is thedifference-in-difference estimator which is equal to one in treatment zip codesafter the policy. The remaining variables include zip code, year, and quarterdummies, as well as downwind-year and upwind-year dummies which con-trol flexibly for differential shocks or trends among upwind and downwind zipcodes. Table 4 shows the regression estimates for both the first stage andreduced form.
Column (1) presents the reduced form results on asthma. Both downwindand crosswind zip codes show a statistically significant decline after the policy,while the decrease in asthma in upwind zip codes is not different from zero. Itis not surprising that crosswind zip codes show a large and significant declinein asthma since this is the largest group and contains about half of all zipcodes. However, measurement error in the construction of wind measuresprevents any statistical distinction between these three coefficients, as can beseen though the coefficient equality tests.35 Nevertheless, point estimates andgraphical evidence indicate that asthma declined by the greatest amount indownwind zip codes.
Columns (2)-(4) show the first stage results on pollution. For each pollu-tant, there is a significant decline for downwind, crosswind, and upwind zipcodes. As before, these coefficients are generally not statistically different fromone another due to measurement error in both the interpolation of pollutionand wind. However, point estimates for CO and NO2 are largest for the down-wind zip codes, as expected.36
35Measurement error arises from the fact that wind is measured with error, from theinterpolation of wind direction across space, and from using wind and highway directionangles with reference to the zip code centroid rather than at all points within the zip code.
36In the case of SO2, the point estimate is slightly higher for upwind zip codes, but thisis likely due to the sparsity of monitors recording SO2 and the fact that traffic pollutionaccounts for a much smaller percentage of overall ambient SO2 levels. Therefore, it is notsurprising that SO2 results are not as consistent.
26

Table 4: Wind Direction Results
PollutionAsthma CO NO2 SO2
(1) (2) (3) (4)
DD*Downwind -5.773** -0.118*** -1.138*** -0.734***(2.579) (0.0188) (0.213) (0.164)
DD*Crosswind -4.866*** -0.103*** -0.815*** -0.405***(1.437) (0.0144) (0.226) (0.115)
DD*Upwind -2.401 -0.089*** -0.885*** -0.850***(2.720) (0.0214) (0.319) (0.172)
Equality tests:DD*Down = DD*Up 0.3685 0.3125 0.5680 0.6228DD*Down = DD*Cross 0.7588 0.5375 0.3983 0.0997DD*Up = DD*Cross 0.4232 0.5814 0.8577 0.0312
Observations 11,568 114,387 112,055 73,625R-squared 0.823 0.733 0.797 0.522Zip Code FE yes yes yes yesYear dummies yes yes yes yesDownwind-year dummies yes yes yes yesUpwind-year dummies yes yes yes yesQuarter dummies - yes yes yes
Notes: Asthma regression weighted by zip code population. Standard errors clusteredat the zip code level are in parentheses. *** p<0.01, ** p<0.05, * p<0.1
27

Heterogeneous Effects: TrafficIn addition to the distance one lives from a highway, the type of traffic condi-tions on the highway might also cause a differential impact on asthma rates.Data on the annual average daily traffic (AADT) of Californian highways pro-vides a measure of the average number of vehicles using a highway each day.Highways with high traffic should produce more pollution than low traffichighways and might experience a greater reduction in pollution from the im-plementation of CBG.37 However, human exposure depends on both residentialdistance to a highway and the traffic intensity on that highway.
Figure 9 shows the smoothed relationship between the percent of the pop-ulation living near the highway, τ , and asthma by year for zip codes with hightraffic and low traffic, separately. First, it is clear that the positive relationshipbetween the percent of the population living near the highway and asthma isstronger for high traffic zip codes. Especially for values of τ above 80 percent,the level of asthma is much higher in high traffic zip codes. For high trafficzip codes, there is a large drop in asthma after the policy across almost alllevels of τ . Whereas, low traffic zip codes exhibit a decline in the gradientthat leads to lower asthma for only zip codes with a large percent of the pop-ulation living near highways. As one might expect, it seems that CBG causeda reduction in asthma for almost all high traffic zip codes, regardless of thepercent of the population living close to the highway. Even among zip codeswhere a smaller portion of the population lives near the high traffic highways,pollution and asthma rates may be so high for those exposed residents thatcleaner-burning gasoline still has a large impact on asthma. On the otherhand, for low traffic zip codes, CBG was only effective in reducing asthma inzip codes where a large portion of residents lived close to highways. Therefore,the natural comparison or control group should be zip codes with low trafficand most residents living far from highways, “Far & Low Traffic.” Then, thethree potentially treated groups include “Close & High Traffic,” “Far & HighTraffic,” and “Close & Low Traffic,” where zip codes are close (far) if τ isgreater than (less than or equal to) the median.
Figure 10 plots the difference in asthma rates for each treated group relativeto the control group. Unsurprisingly, the largest relative asthma level is among“Close & High Traffic” zip codes, where many residents live near high traffichighways. It is clear that asthma rates were increasing in each of the threegroups relative to the control group before 1996. With the implementation of
37Previous research has shown that traffic jams and highway idling have a large impacton pollution levels as well (Currie and Walker, 2011; Friedman et al., 2001). I focus only onthe AADT measure due to data availability constraints.
28

CBG in 1996, there was a sharp initial drop in relative asthma rates whichcontinued on a new downward path after CBG. The impact of the policy isclear across all three treatment groups.
Figure 9: Asthma hospitalizations by exposure and traffic density
3540
4550
5560
6570
Ast
hma
0 .2 .4 .6 .8 1% pop within 1km of highway
Low Traffic
3540
4550
5560
6570
Ast
hma
0 .2 .4 .6 .8 1% pop within 1km of highway
High Traffic
92−93 94−95 96 97−98 99−00
Notes: Shows the smoothed relationship between asthma hospitalizations and the percentageof the population living within 1km of a highway, τ , in different years. Dashed and solid linesindicate years after and before the policy, respectively. Lines are smoothed using “lpoly,”with degree zero and a 0.1 bandwidth. High (low) traffic zip codes zip codes with an averageAADT of at least (less than) 60,000 vehicles per day.
Regression results support this graphical evidence. Table 5 shows estima-tion of the following equations for pollution and asthma:
Pollutionzt =γ0 + γ1Close∗High∗Afterzt + γ2Close
∗Low∗Afterzt (8)
+ γ3Far∗High∗Afterzt + Zz + Θy +Qq + ε7zt
Asthmazy =ρ0 + ρ1Close∗High∗Afterzt + ρ2Close
∗Low∗Afterzt (9)
+ ρ3Far∗High∗Afterzt + Zz + Θy + ε8zy
where Close (Far) is an indicator equal to one if the zip code has greaterthan (less than or equal to) the median value of τ , the percent of the zip codepopulation near a highway. High is an indicator for high traffic zip codes,Low is an indicator for low traffic zip codes, After is an indicator equal toone after CBG is required and the remaining variables include zip code, year,and quarter dummies, as defined previously. The reference group includes zipcodes where people live far from highways with low traffic levels. Table 5 showsthe regression estimates for both the first stage and reduced form.
29

Figure 10: Relative difference in asthma by distance to highways and traffic
05
1015
20A
sthm
a
1992 1994 1996 1998 2000Year
Close High − Far Low Close Low − Far LowFar High − Far Low
Notes: Plots the difference in the average yearly asthma hospitalization level betweeneach possible treatment group and control zip codes (“Far-Low”). High (low) traffic zipcodes are zip codes with an average AADT of at least (less than) 60,000 vehicles perday. Close (far) zip codes have greater than (less than or equal to) the median value ofτ .
30

Table 5: Impact of CBG by level of traffic
PollutionAsthma CO NO2 SO2
(1) (2) (3) (4)
Close*High*After -7.399*** -0.204*** -2.001*** -0.592***(1.441) (0.0110) (0.179) (0.0982)
Close*Low*After -6.401*** -0.062*** -0.318 -0.064***(1.785) (.0161) (0.226) (0.136)
Far*High*After -4.545*** -0.180*** -1.699*** -0.073(1.728) (0.0134) (0.228) (0.123)
Equality tests:Close*High*After = Close*Low*After 0.5175 0.0000 0.0000 0.7178Close*High*After = Far*High*After 0.0531 0.0367 0.1812 0.0000Close*Low*After = Far*High*After 0.3061 0.0000 0.0000 0.0001
Observations 11,856 119,632 116,907 76,524R-squared 0.823 0.736 0.798 0.516Zip Code FE yes yes yes yesYear dummies yes yes yes yesQuarter dummies - yes yes yes
Notes: Reference group includes zip codes with low traffic and far from highways. Asthma regressionweighted by zip code population. Standard errors clustered at the zip code level are in parentheses.*** p<0.01, ** p<0.05, * p<0.1
31

Reduced form results on asthma show large significant reductions acrossall three treatment groups relative to the “Far & Low Traffic” group. Thepoint estimate is highest for the “Close & High Traffic” group, followed bythe “Close & Low Traffic” group, but a test of equality shows that these pointestimates are not statistically different. Only the point estimate for the “Close& High Traffic” group is significantly larger at the 10 percent level from the“Far & High Traffic” group. Unlike asthma that depends both on residentiallocation and traffic, the pollution results reveal, not surprisingly, that pollu-tion depends most strongly on traffic. Focusing on CO and NO2, the decreasein pollution is much larger for both high traffic groups. For both the “Close &High Traffic” and the “Far & High Traffic” groups, the decrease in pollution isstatistically different from the “Close & Low Traffic” and “Far & Low Traffic”groups. Results for SO2 follow a different pattern, but this is likely due to thescarcity of monitors and increased measurement error for this pollutant. Soalthough pollution declined by the greatest amount in high traffic zip codes,subsequent declines in asthma were significant for all high traffic zip codes, aswell as low traffic zip codes where a large portion of residents live very nearto a highway.
Heterogeneous Effects: Age, Gender, & RaceFurthermore, I explore heterogeneous effects of the policy by exploiting de-mographic information in the hospital data. Table 6 shows the difference-in-difference estimates for different sub-samples of the population by age, gender,and race. While results appear similar for males and females, it does appearthat the results are stronger for black children and younger children. From thesummary statistics presented in Appendix Table B1, one can see that blacksare more likely to live in census tracts with close proximity to highways, whilewhites are far less likely to live very near highways. Given this stylized fact,but only having zip code level residential information, one might expect to finda stronger effect for black patients since they are more likely to be impacted byCBG. As expected, the effect of CBG on asthma is only statistically significantfor black children. Within a zip code, black children are more likely to livevery close to highways, and therefore more likely to benefit from a reduction intraffic pollution.38 This suggests that gasoline content regulation could reducehealth disparities for children of low socio-economic status who are more likelyto live near highways.
38Because I cannot identify exact residential location, it is unclear whether the largerimpact on black children is driven by sorting of families such that black children are morelikely to live near highways within a zip code, or because, conditional on location, blackchildren are more susceptible to asthma.
32

Table 6 also shows that CBG has the largest impact for children under oneyear old and that the effect diminishes with age. This may be due to the factthat younger children are more sensitive to pollution. Additionally, pollutionmay have a cumulative impact on health, such that exposure to pollution ata young age may impact health in later years.
Table 6: Heterogeneous effects by age, gender, and raceAge Gender Race
<1 yr 1-4 yrs 5-9 yrs Male Female White Black(1) (2) (3) (4) (5) (6) (7)
Panel A.Treat*After -30.57** -2.004* -1.114* -4.856*** -4.536*** 5.215 -9.582*
(11.90) (1.028) (0.623) (1.758) (1.249) (3.536) (4.930)
%∆ from pre-treat -6.7 -5.1 -6.2 -6.0 -8.6 10.7 -7.9%∆ in gap -113.4 -19.9 -21.7 -38.3 -55.8 176.4 -52.9%∆ of std dev -7.9 -5.2 -5.7 -6.3 -7.3 9.5 -5.8
Panel B.%Close*After -51.18** -3.657* -1.763 -9.818*** -6.770** 15.20** -4.149
(20.19) (1.917) (1.147) (3.151) (2.264) (7.242) (8.282)
Observations 10,637 10,846 10,696 12,006 11,968 11,028 8,275R-squared 0.778 0.650 0.615 0.752 0.685 0.636 0.473Zip Code FE yes yes yes yes yes yes yesYear dummies yes yes yes yes yes yes yes
Notes: Panel A shows regression results based on the binary treatment status indicator. Panel B shows regressionresults based on the continuous measure of treatment status. Each column shows the difference-in-differenceestimate based on a subset of the population. The outcome variables are asthma hospitalization rates based ongroup-specific population levels. Regressions are weighted by zip code population. Standard errors clustered atthe zip code level are in parentheses. *** p<0.01, ** p<0.05, * p<0.1
Cumulative EffectsThe following cohort analysis explores the possible cumulative impact of pol-lution. First, Exp is defined as the number of years each cohort has beenexposed to CBG.39,40 Table 7 shows results from the estimation of the follow-ing equations.
39Exp is defined using age group and year data such that Exp = min(max(year −1996, 0), age). Data on population estimates by zip code for the 1990 census are limited toage groups, rather than individual years. This prevents the analysis from being conductedat the individual age-year-zip code level. Instead, I use the following age groups: under 1,1-2, 3-4, 5, 6, and 7-9 years old.
40Note that there is some inherent measurement error associated with this definition. Icannot determine exact duration of exposure since I cannot identify how long each child haslived in the zip code of current residence.
33

Asthmazay = α0 + α1τ∗Expzay + Eay + Aa + Zz + Θy + ε9zay (10)
Asthmazay = π0 +4∑
i=1
[πiτ∗1{Exp = i}zay] + Eay + Aa + Zz + Θy + ε10zy
(11)
where τ is the percent of the zip code’s population that lives within 1kmof a highway, and both equations include zip code fixed effects, Zz, age groupdummies, Aa, cohort exposure dummies, Eay, and year dummies, Θy. If thereis a cumulative impact of CBG, one would expect to see that years of expo-sure to CBG is negatively related to asthma for zip codes with high τ values.Column (1) of Table 7 shows that this is the case. Column (2) shows that asthe years of exposure increase, the negative coefficient becomes monotonicallylarger in magnitude and more significant. These results suggest that there isindeed a cumulative impact of the policy.41
5 Robustness & Measurement Error
5.1 Pollution Robustness
Table 8 tests the robustness of the pollution estimates and addresses somemeasurement concerns. First, one may be concerned that treated zip codesmay have different long-run trends from control zip codes. Column (2) includeszip code specific linear time trends to account for any zip code specific long-run trends. The results remain significant for all three pollutants. In fact,results become larger for both NO2 and CO, but become smaller in magnitudefor SO2. This is not surprising given there are only half as many monitorsrecording SO2 as the other criteria pollutants.
Secondly, due to the method of inverse distance weighted interpolationof pollution measures for each zip code, measurement error is an inherentproblem for these results. In order to address this concern, Columns (3)-(5)present estimates designed to reduce measurement error. Column (3) weightsthe results by the number of air quality monitors within 20 miles of the zipcode’s centroid that were used to calculate the zip code level of pollution.Column (4) weights the results by the inverse of the average air quality monitor
41The cumulative effect is qualitatively similar when estimated at the individual levelusing data linked across time by the confidential patient record linkage number.
34

Table 7: Cumulative effects by exposure to CBG
Asthma(1) (2)
τ * Exp -2.974**(1.389)
τ * 1{Exp = 1} -2.327(7.426)
τ * 1{Exp = 2} -5.327(4.229)
τ * 1{Exp = 3} -9.734**(4.545)
τ * 1{Exp = 4} -11.72**(4.609)
Observations 68,517 68,517R-squared 0.684 0.684Zip Code FE yes yesYear dummies yes yesAge dummies yes yesExposure dummies yes yes
Notes: Exp is the number of years each cohort has beenexposed to CARB gasoline, and τ is the percent of the zipcode’s population that lives within 1km of a highway. Re-sults weighted by zip code-cohort population. Standard er-rors clustered at the zip code level are in parentheses. ***p<0.01, ** p<0.05, * p<0.1
35

distance from the centroid. Column (5) limits the analysis to only zip codeswith at least 3 monitors within the 20 mile radius of the zip code centroid.The results remain significant and of similar magnitude to the baseline results.Finally, results based on the Kriging methodology to interpolate pollution dataare presented in Appendix Table C4. The Kriging methodology convenientlyprovides a measure of the accuracy of the predictions. Results weighted bythe inverse of the prediction error are also shown in the appendix and remainof similar magnitude.
Table 8: Pollution robustness
Zip time Weight: Weight: ≥ 3Baseline trends # Mon. Mon. dist. Mon.
(1) (2) (3) (4) (5)
NO2 -0.870*** -1.516*** -0.979*** -0.638*** -0.658***(0.160) (0.140) (0.198) (0.175) (0.205)
CO -0.104*** -0.166*** -0.107*** -0.0992*** -0.0777***(0.0101) (0.00741) (0.0122) (0.0146) (0.0102)
SO2 -0.597*** -0.247*** -0.510*** -0.561*** -0.315***(0.0835) (0.0768) (0.0804) (0.0956) (0.0818)
Zip FE yes yes yes yes yesYear dummies yes yes yes yes yesQuarter dummies yes yes yes yes yesTime trend yes yes yes yes yes
Notes: Each coefficient represents a separate regression. Column 1 reproduces the main resultsfrom Table 2. Column 2 includes zip code specific linear time trends. Column 3 weights theestimates by the number of air quality monitors within 20 miles. Column 4 weights the estimatesby the inverse of the average monitor distance from the zip code centroid. Column 5 limits theanalysis to zip codes with at least 3 monitors within 20 miles. Standard errors clustered at thezip code level are in parentheses. *** p<0.01, ** p<0.05, * p<0.1
5.2 Asthma Robustness
The reduced-form asthma results are robust to alternate specifications, asseen in columns (2)-(6) of Table 9. First, column (2) tests the robustness ofthe results to an alternate choice of the relevant distance that pollution maytravel from the highway. It is likely that this distance depends on many factorsincluding the direction of the wind, temperature, and surrounding geographies.Some epidemiological literature has suggested that distances smaller than 1kmmay be more relevant, such as 300m. Results based on the percent of residentsliving within 300m of a highway, shown in column (2), are significant and
36

similar in magnitude to the baseline. This gives confidence that the resultsare not driven by the cutoff choice for pollution dispersion from a highway.
Another concern is that the inclusion of rural zip codes with large areasand few residents may bias the results and introduce unnecessary measurementerror. Column (3) presents results based on a sample of zip codes that excludesthe 10 percent of the zip codes with the largest areas. The results remainsignificant. Therefore, it seems that the results are not driven by the inclusionof these large zip codes. Though it is not necessary for the control groupto look identical to the treated group, using control zip codes that are moresimilar to treated zip codes may help reduce any concern that the results aredriven by differential changes over time between these groups. Column (4)uses only control zip codes that share a border with a treated zip code, andthe results remain significant.
Both asthma and traffic pollution levels are influenced by weather condi-tions. In order to control for any differential changes in weather that maybe driving the results, Column (5) shows the coefficient remains of similarmagnitude even after adding zip code-year specific weather variables, includ-ing minimum and maximum temperatures, wind speed, absolute humidity,and precipitation. Zip code specific weather variables are calculated using thesame inverse distance weighting methodology as for pollution measures.
It is also important to note that the asthma outcome variable exhibits aprobability mass at zero. It is not possible for any zip code to attain an asthmarate that is below zero, but there are certainly zip codes that are much closerto crossing the margin to attain a positive value than others. Therefore, Iestimate the results using a corner solution model. Column (6) presents theaverage partial effects from a Tobit model. The effects maintain significanceand are of similar magnitude to the baseline. This suggests that the mainresults are not biased by the probability mass at zero for asthma.
37

Tab
le9:
Ast
hm
aro
bust
nes
s
Rob
ust
nes
sT
ests
Pla
ceb
oT
ests
300m
Dro
pla
rge
Con
trol
Wea
ther
Inju
ries
Ner
vou
sB
asel
ine
cuto
ffzi
pco
des
bor
der
str
eat
contr
ols
Tob
it&
bu
rns
syst
em(1
)(2
)(3
)(4
)(5
)(6
)(7
)(8
)Pan
elA.
Tre
at*A
fter
-4.5
05**
*-3
.650
***
-3.9
72**
*-4
.238
***
-3.5
47**
*-4
.461
***
-0.0
686
-0.0
253
(1.1
57)
(1.1
88)
(1.2
17)
(1.1
93)
(1.2
48)
(1.0
98)
(0.6
27)
(0.2
91)
Pan
elB.
%C
lose
*Aft
er-7
.865
***
-11.
07**
*-6
.786
***
-7.4
84**
*-6
.145
***
-7.8
43**
*-0
.814
-0.8
37(2
.071
)(4
.156
)(2
.125
)(2
.115
)(2
.152
)(1
.965
)(1
.161
)(0
.548
)
Ob
serv
atio
ns
11,5
6811
,160
10,3
5410
,535
9,15
311
,568
10,8
6510
,865
R-s
qu
ared
0.82
30.
824
0.82
70.
827
0.82
90.
465
0.39
5Z
ipC
od
eF
Eye
sye
sye
sye
sye
sye
sye
sye
sY
ear
du
mm
ies
yes
yes
yes
yes
yes
yes
yes
yes
Clu
ster
edS
Eye
sye
sye
sye
sye
s-
yes
yes
Pop
wei
ghts
yes
yes
yes
yes
yes
yes
yes
yes
Not
es:
Pan
elA
show
sre
gres
sion
resu
lts
bas
edon
the
bin
ary
trea
tmen
tst
atu
sin
dic
ator
.P
anel
Bsh
ows
regre
ssio
nre
sult
sb
ase
don
the
conti
nu
ous
mea
sure
of
trea
tmen
tst
atu
s.C
olu
mn
1re
pro
du
ces
the
mai
nre
sult
sfr
om
Tab
le3.
Col
um
n2
alt
ers
the
trea
tmen
tst
atu
sto
be
defi
ned
bas
edon
a30
0m
dis
tan
cefr
omth
eh
ighw
ay,
rath
erth
an1km
.C
olu
mn
3ex
clud
esth
e10
per
cent
of
zip
cod
esw
ith
the
larg
est
area
s.C
olu
mn
4d
rop
sco
ntr
ol
zip
cod
esth
atd
on
otsh
are
ab
ord
erw
ith
atr
eate
dzi
pco
de.
Colu
mn
5in
clu
des
zip
cod
e-ye
ar
spec
ific
contr
ols
for
min
imu
man
dm
axim
um
tem
per
atu
re,
win
dsp
eed
,ab
solu
tehum
idit
y,an
dp
reci
pit
ati
on
.C
olu
mn
6p
rese
nts
aver
age
part
ial
effec
tsfr
om
aT
obit
mod
el,
cen
sore
dat
zero
.C
olu
mn
s7
and
8p
rese
nt
pla
ceb
ote
sts
base
don
hosp
ital
ad
mis
sion
sfo
rd
iagn
ose
su
naff
ecte
dby
the
pol
icy
(see
text
for
crit
eria
).T
he
outc
ome
vari
able
for
colu
mn
7is
the
nu
mb
erof
chil
dre
nad
mit
ted
for
“d
isea
ses
an
dd
isor
der
sof
the
ner
vou
ssy
stem
”(M
ajo
rD
iagn
osi
sC
ate
gory
1)p
er10
,000
chil
dre
n.
Th
eou
tcom
eva
riab
lefo
rco
lum
n8
isth
enu
mb
erof
chil
dre
nad
mit
ted
for
“in
juri
es,
pois
on
ings
and
toxic
effec
tsof
dru
gs”
and
“bu
rns”
(Majo
rD
iagn
osis
Cate
gori
es21
&22)
per
10,0
00
chil
dre
n.
Sta
nd
ard
erro
rsin
pare
nth
eses
.**
*p<
0.0
1,**
p<
0.05
,*
p<
0.1
38

In the final two columns, I perform placebo tests using data on hospitaladmissions for other primary diagnoses. The choice of a placebo hospital ad-mission must meet two criteria. First, there should be no pathway throughwhich traffic pollution might impact the prevalence of the condition. Second,the condition should occur with sufficient frequency among children under 10years old. Given these criteria, I estimate the impact of CBG on hospital ad-missions for “diseases and disorders of the nervous system” (Major DiagnosisCategory 1) and “injuries, poisonings and toxic effects of drugs” and “burns”(Major Diagnosis Categories 21 & 22). One would not expect to find a signifi-cant effect of CBG legislation on the amount of discharges for these conditions.If one were to see an impact, it would call into question the validity of theresults presented above. As expected, the estimates shown in columns (7)and (8) are insignificant and the confidence intervals do not overlap with thebaseline results, which provides greater confidence that the decrease in asthmahospitalizations is a result of cleaner-burning gasoline rather than an overalltrend across all types of hospitalizations.
Finally, given the spatial nature of the zip code level data, it is possible forneighboring zip codes to have correlated error terms. There are three types ofspatial models that might not be captured by clustered standard errors: spatiallag of the dependent variable, spatial lag in the error term, or a combination ofboth a spatial lag in the dependent variable and error term (SARMA model).In order to test for spatial autocorrelation, I create a queen weights matrix todefine the relationship of each zip code to its neighboring zip codes.42 Withthis information, I perform Lagrange Multiplier tests for spatial lag, spatialerror, and SARMA models. For each model, I fail to reject the null hypothesisof no spatial dependence among zip codes. This suggests that a spatial modelwould not be appropriate for this process.43
5.3 Potential confounding policies
It is important to consider the impact of several other policies which occurredduring our sample period. First, one might be concerned that trading marketsfor SO2 and NOx were responsible for the decrease in pollution shown pre-viously. Title IV of the 1990 Clean Air Act (CAA) Amendments establishedthe SO2 emissions allowance trading program for electric generating units.The first phase began in 1995, but virtually all of the affected electricity-generating facilities were located east of the Mississippi River, suggesting that
42A queen weights matrix defines a zip code’s neighbors as those with either a sharedborder or vertex (in contrast to a rook weights matrix, which only includes shared borders).
43The test statistics and associated P-values are shown in Appendix C.
39

facilities in California were likely unaffected (Burtraw and Szambelan, 2009).The CAA Amendments also addressed the problem of acid rain by regulatingNOx emissions from coal-fired electric generators.44 In California, the SouthCoast Air Quality Management District was the first to start a large urbancap-and-trade program for NOx in 1994, known as Regional Clean Air Incen-tives Market (RECLAIM). One might be concerned that this cap-and-tradeprogram caused a general downward trend in pollution in areas near highwaysthat was unrelated to CBG if coal-fired electric generator plants were morelikely to locate near highways as well. However, this should not be a largeconcern for the following reason. Firms could choose a baseline year between1989 and 1992 upon which their initial emissions allocation was determined.This period was characterized by high levels of economic activity, providing ahigh baseline. Because of a regional decline in economic activity during thefirst years of the RECLAIM program and the inability to bank allowances,there was a large surplus of emissions allowances that expired unused. Therewere few real emissions reductions, low allowance prices, and little trading inthe early years of the program (Klier, Mattoon and Prager, 1997). Meaningfultrades in the NOx market did not begin to take place until the beginning of2000, after my sample period (Burtraw and Szambelan, 2009).
Second, federal reformulated gasoline (RFG) was required in certain partsof California in 1995, one year prior to the implementation of CBG. However,existing evidence in Auffhammer and Kellogg (2011) suggests that RFG hadlittle impact on pollution, as opposed to the stricter CBG regulations. Resultsin Appendix D confirm that RFG also had little impact on asthma and thatthe results presented above are driven by the introduction of CBG. Third is thepassage of the Personal Responsibility and Work Opportunity ReconciliationAct in 1996 (PRWORA). As a result of changes to welfare and Medicaideligibility rules, monthly Medicaid enrollment declined 12 percent in Californiafrom 1995 to 1998 (Ellwood 1999). This would be problematic if patientseligible for Medicaid were more likely to live in the treatment zip codes, andthey were less likely to show up in the hospital data due to enrollment issuesrather than an asthma decline. Evidence presented in Appendix D suggestthat this is not driving the results. Barriers to Medicaid enrollment are morelikely to impact access to and use of asthma prescription drugs than hospitaladmissions. State utilization data from the Medicaid Drug Rebate Programshow that the total amount reimbursed for asthma prescription drugs declinedduring this period in both California and the nation. This decline may be
44Coal-fired electric generators are the primary stationary source of NOx, but the elec-tricity sector contributes only 22 percent of total US NOx emissions.
40

attributed both to the reduction in asthma from cleaner-burning gasoline andthe reduction in access to prescription drugs through Medicaid. It is difficultto distinguish between these two factors since they occur contemporaneously.However, the reduction in access to asthma control medications would likelyincrease the number of hospitalizations for asthma. Therefore, if anything, theresults here will be understated.
6 Economic Impact
Gasoline content regulations are associated with numerous costs, includingcompliance costs, enforcement costs and increased prices for consumers. Onthe other hand, the main findings in this paper indicate that gasoline contentregulation can also improve health outcomes, leading to a reduction in costlymedical expenditures. Given the health benefit estimates shown previously,one can make a back-of-the-envelope calculation of the costs and benefits fromthe CBG legislation.
Auffhammer and Kellogg (2011) suggest a compliance cost of about 8-11cents per gallon for refineries.45 Data from the U.S. Department of Trans-portation estimates that gasoline consumption in California in 2006 was 15.8billion gallons, which implies a yearly cost of about $1.2-$1.7 billion.
I estimate that CBG reduced asthma hospitalizations by about 4 per 10,000children in areas near highways relative to far from highways. According tothese estimates, CBG reduced childhood asthma hospitalizations by about1,449 in California in 2006 alone. Hospital expenditures accounted for over halfof all expenditures for asthma. In fact, Stranges, Merrill and Steiner (2008)estimates that hospitalizations cost about $9,100 per child in 2006, whichmeans that CBG reduced medical expenditures from asthma hospitalizationsby about $13 million per year in California.
Without considering any other benefits, the compliance cost to refineriesgreatly outweighs the cost savings from reduced childhood asthma hospital-izations. However, this calculation does not take into account other benefitsfrom cleaner-burning gasoline, such as a reduction in infant mortality and areduction in cardiovascular disease (CVD).
In terms of infant mortality, estimates suggest that CBG may have reducedinfant deaths by up to 24 per 10,000 infants each year in high exposure areas,
45Interestingly, Brown et al. (2008) estimate that the price to consumers increased by anaverage of 3 cents/gal in metropolitan areas with gasoline content regulations, relative toa control group. This price effect, however, varied by 8 cents/gal across different regulatedmarkets depending on geographic isolation.
41

which equates to about 873 saved lives in 2006.46 Given that the EPA’s officialvalue of a statistical life is $6.45 million, this implies a savings of over $5.5billion.47
In terms of cardiovascular disease, previous research has established a linkbetween air pollution and hospital admissions for cardiovascular disease. Es-timates from Schwartz (1997) translate into a 1.68 percent decrease in CVDadmissions per 1 ppm decrease in CO. Using California’s data on the totalnumber and average cost of CVD admissions in 2006, along with my estimatethat CBG decreased CO by about 0.1 ppm, the savings amount to about $630million.48
Accounting for the reduced childhood asthma, infant mortality, and CVD,the benefits from CBG are about $6.3 billion per year, which is well above theestimated compliance costs of $1.2-$1.7 billion. A comprehensive accountingfor all health and environmental benefits would likely increase the cost savingsof CBG even further. Other potentially important benefits include benefits tothe environment, a reduction in poor birth outcomes (low birthweight, pre-maturity, etc.), a reduction in respiratory conditions among adults and theelderly, a reduction in cancer, and a decrease in health inequality among lowsocio-economic families living near highways.
7 Conclusion
This paper provides an estimate of the effect of the 1996 cleaner-burning gaso-line content regulation on asthma hospitalizations among children in Califor-nia. This paper exploits variation in residential exposure to highways in orderto, first, support existing evidence that CBG reduced air pollution, and sec-ond, to show that the reduction in pollution was associated with a declinein asthma hospitalizations for children. As hypothesized, the strict gasolinecontent regulations caused a greater reduction in childhood asthma in areasclose to major highways, as compared to areas further away, after the regula-tions were introduced. The results indicate that the CBG regulations caused
46Again, this estimate is possibly overstated due to the fact that infant deaths cannotbe separated from infant transfers in the data. Nevertheless, it is likely that infant deathsdropped significantly after the policy and this measure can be used as a proxy.
47Note that this will be an overstatement if our proxy for infant deaths is biased bychanges in infant transfers over this period.
48CVD admissions include all admissions for ICD-9 codes 390-429. OSHPD Patient Dis-charge Data reports 3,508,221 discharges for CVD in 2006. The average cost of heart attackhospitalizations was $106,845, which was calculated across all payer categories for 2006(OSHPD, 2011).
42

a significant and large reduction in childhood asthma admissions of about 8percent in California, or 4.5 per 10,000 children. These results are robust tonumerous alternative specifications.
Exploration of heterogeneous effects indicate that downwind and high traf-fic zip codes experience the greatest declines in pollution and asthma. More-over, a cohort-level analysis reveals that the reduction in asthma is larger forcohorts which have been exposed to the cleaner-burning gasoline for longer pe-riods of time, suggesting a cumulative impact. Finally, we know that familiesliving near major highways are of lower socio-economic status and the re-sults confirm that the largest health improvements occurred among low socio-economic status patients. Evidence from this policy suggests that gasolinecontent restricts may reduce disparities in asthma-related health outcomes.More stringent regulation of gasoline content could have significant impactson child health and quality of life, as well as reduce medical expenditures forthe treatment of asthma.
References
Anselin, Luc, and Julie Le Gallo. 2006. “Interpolation of air quality mea-sures in hedonic house price models: spatial aspects.” Spatial EconomicAnalysis, 1(1): 31–52.
Auffhammer, Maximilian, and Ryan Kellogg. 2011. “Clearing the air?the effects of gasoline content regulation on air quality.” The American Eco-nomic Review, 101(6): 2687–2722.
Barnes, Peter J. 1995. “Air pollutionand asthma: molecular mechanisms.”Molecular medicine today, 1(3): 149–155.
Bauer, MA, MJ Utell, PE Morrow, DM Speers, and FR Gibb.1986. “Inhalation of 0.30 ppm nitrogen dioxide potentiates exercise-inducedbronchospasm in asthmatics.” The American review of respiratory disease,134(6): 1203.
Bloom, B, LI Jones, and G Freeman. 2013. “Summary health statisticsfor U.S. children: National Health Interview Survey, 2012.” National Centerfor Health Statistics. Vital Health Stat 10(258).
Brown, Jennifer, Justine Hastings, Erin T Mansur, and Sofia BVillas-Boas. 2008. “Reformulating competition? Gasoline content regu-
43

lation and wholesale gasoline prices.” Journal of Environmental economicsand management, 55(1): 1–19.
Brunekreef, Bert, Nicole AH Janssen, Jeroen de Hartog, HendrikHarssema, Mirjam Knape, and Patricia van Vliet. 1997. “Air pollu-tion from truck traffic and lung function in children living near motorways.”Epidemiology, 298–303.
Burtraw, Dallas, and Sarah Jo Fueyo Szambelan. 2009. “US emissionstrading markets for SO2 and NOx.” Resources for the Future DiscussionPaper, , (09-40).
CARB. 2008a. “Clean Air Benefits.” California Environmental ProtectionAgency.
CARB. 2008b. “Cleaner-Burning Gasoline: An Update.” California Environ-mental Protection Agency.
CARB. 2013. “Asthma and Air Pollution.” California Environmental Protec-tion Agency.
CDC. 2012. “National Health Interview Survey (NHIS) data: 2011 lifetimeasthma, current asthma, asthma attacks among those with current asthma.”US Department of Health and Human Services, CDC.
Chay, Kenneth Y, and Michael Greenstone. 2003a. “Air quality, infantmortality, and the Clean Air Act of 1970.” National Bureau of EconomicResearch.
Chay, Kenneth Y, and Michael Greenstone. 2003b. “The Impact of AirPollution on Infant Mortality: Evidence from Geographic Variation in Pollu-tion Shocks Induced by a Recession.” The Quarterly Journal of Economics,118(3): 1121–1167.
Ciccone, Giovannino, Francesco Forastiere, Nera Agabiti, AnnibaleBiggeri, Luigi Bisanti, Elisabetta Chellini, Giuseppe Corbo, Vale-rio Dell’Orco, Paola Dalmasso, Tadeja Fatur Volante, et al. 1998.“Road traffic and adverse respiratory effects in children. SIDRIA Collabo-rative Group.” Occupational and environmental medicine, 55(11): 771–778.
Cressie, N. 1993. Statistics for Spatial Data: Wiley Series in Probability andStatistics. Wiley: New York, NY, USA.
44

Currie, Janet, and Matthew Neidell. 2005. “Air Pollution and InfantHealth: What Can We Learn from California’s Recent Experience?” TheQuarterly Journal of Economics, 120(3): 1003–1030.
Currie, Janet, and Reed Walker. 2011. “Traffic Congestion and InfantHealth: Evidence from E-ZPass.” American Economic Journal: AppliedEconomics, 3(1): 65–90.
Davis, Lucas W. 2008. “The effect of driving restrictions on air quality inMexico City.” Journal of Political Economy, 116(1): 38–81.
Duhme, Heinrich, Stephan K Weiland, Ulrich Keil, Barbara Krae-mer, Manfred Schmid, Monika Stender, and Lloyd Chambless.1996. “The association between self-reported symptoms of asthma and al-lergic rhinitis and self-reported traffic density on street of residence in ado-lescents.” Epidemiology, 7(6): 578–582.
Ellwood, Marilyn R, et al. 1999. “The Medicaid eligibility maze: Coverageexpands, but enrollment problems persist.” The Urban Institute.
English, Paul, Raymond Neutra, Russell Scalf, Moira Sullivan,Lance Waller, and Li Zhu. 1999. “Examining associations between child-hood asthma and traffic flow using a geographic information system.” En-vironmental health perspectives, 107(9): 761.
EPA. 2000. “National Air Pollutant Emission Trends, 1900-1998.” Office ofAir Quality Planning and Standards.
Esposito, Susanna, Rossana Tenconi, Mara Lelii, Valentina Preti,Erica Nazzari, Silvia Consolo, and Maria F Patria. 2014. “Possiblemolecular mechanisms linking air pollution and asthma in children.” BMCpulmonary medicine, 14(1): 31.
Friedman, Michael S, Kenneth E Powell, Lori Hutwagner, LeRoy MGraham, and W Gerald Teague. 2001. “Impact of changes in trans-portation and commuting behaviors during the 1996 Summer OlympicGames in Atlanta on air quality and childhood asthma.” JAMA: the journalof the American Medical Association, 285(7): 897–905.
Gilbert, Nicolas L, Sandy Woodhouse, David M Stieb, and Jeffrey RBrook. 2003. “Ambient nitrogen dioxide and distance from a major high-way.” Science of the Total Environment, 312(1): 43–46.
45

Green, Rochelle S, Svetlana Smorodinsky, Janice J Kim, RobertMcLaughlin, and Bart Ostro. 2004. “Proximity of California publicschools to busy roads.” Environmental Health Perspectives, 112(1): 61.
Henderson, J. Vernon. 1996. “Effects of Air Quality Regulation.” AmericanEconomic Review, 86(4): 789 – 813.
Huang, Jing-Long, Shih-Yue Wang, and Kue-Hsiung Hsieh. 1991.“Effect of short-term exposure to low levels of SO2 and NO X on pul-monary function and methacholine and allergen bronchial sensitivities inasthmatic children.” Archives of Environmental Health: An InternationalJournal, 46(5): 296–299.
Hu, Shishan, Scott Fruin, Kathleen Kozawa, Steve Mara, Suzanne EPaulson, and Arthur M Winer. 2009. “A wide area of air pollutant im-pact downwind of a freeway during pre-sunrise hours.” Atmospheric Envi-ronment, 43(16): 2541–2549.
Kleinman, MT, RM Bailey, WS Linn, KR Anderson, JD Whynot,DA Shamoo, and JD Hackney. 1983. “Effects of 0.2 ppm nitrogen diox-ide on pulmonary function and response to bronchoprovocation in asth-matics.” Journal of Toxicology and Environmental Health, Part A CurrentIssues, 12(4-6): 815–826.
Klier, Thomas H, Richard H Mattoon, and Michael A Prager. 1997.“A Mixed Bag: Assessmentof Market Performance and Firm Trading Be-haviour in the NOx Reclaim Programme.” Journal of Environmental Plan-ning and Management, 40(6): 751–774.
Knittel, Christopher R, Douglas L Miller, and Nicholas J Sanders.2015. “Caution, drivers! Children present: Traffic, pollution, and infanthealth.” Review of Economics and Statistics, Forthcoming.
Koenig, JQ, WE Pierson, and M Horike. 1983. “The effects of inhaledsulfuric acid on pulmonary function in adolescent asthmatics.” The Ameri-can review of respiratory disease, 128(2): 221–225.
Ku, Leighton, and Teresa A. Coughlin. 1997. “How the new welfarereform law affects Medicaid.” The Urban Institute.
Leikauf, George D. 2002. “Hazardous air pollutants and asthma.” Environ-mental Health Perspectives, 110(Suppl 4): 505.
46

Lleras-Muney, Adriana. 2010. “The needs of the army using compulsoryrelocation in the military to estimate the effect of air pollutants on childrenshealth.” Journal of Human Resources, 45(3): 549–590.
Martinez, Fernando D, Anne L Wright, Lynn M Taussig, Catharine JHolberg, Marilyn Halonen, and Wayne J Morgan. 1995. “Asthmaand wheezing in the first six years of life.” New England Journal of Medicine,332(3): 133–138.
McConnell, Rob, Kiros Berhane, Ling Yao, Michael Jerrett, FredLurmann, Frank Gilliland, Nino Kunzli, Jim Gauderman, et al.2006. “Traffic, susceptibility, and childhood asthma.” Environmental HealthPerspectives, 114(5): 766.
McConnell, Rob, Talat Islam, Ketan Shankardass, Michael Jerrett,Fred Lurmann, Frank Gilliland, Jim Gauderman, et al. 2010. “Child-hood incident asthma and traffic-related air pollution at home and school.”Environmental Health Perspectives, 118(7): 1021.
Muehlegger, Erich J. 2002. “The role of content regulation on pricing andmarket power in regional retail and wholesale gasoline markets.” WorkingPaper.
Neidell, Matthew J. 2004. “Air pollution, health, and socio-economic status:the effect of outdoor air quality on childhood asthma.” Journal of healtheconomics, 23(6): 1209–1236.
Orehek, J, JP Massari, P Gayrard, C Grimaud, and J Charpin. 1976.“Effect of short-term, low-level nitrogen dioxide exposure on bronchial sen-sitivity of asthmatic patients.” Journal of clinical investigation, 57(2): 301.
OSHPD. 2011. “Trends in Cardiac Car in California, 1988 to 2008.” HealthFacts.
Parish, O Owen, and Terrill W Putnam. 1977. “Equations for the de-termination of humidity from dewpoint and psychrometric data.” NationalAeronautics and Space Administration (NASA).
Ryan, Patrick H, Grace LeMasters, Jocelyn Biagini, David Bern-stein, Sergey A Grinshpun, Rakesh Shukla, Kimberly Wilson,Manuel Villareal, Jeff Burkle, and James Lockey. 2005. “Is it traffictype, volume, or distance? Wheezing in infants living near truck and bustraffic.” Journal of allergy and clinical immunology, 116(2): 279–284.
47

Schlenker, Wolfram, and W Reed Walker. 2015. “Airports, air pollution,and contemporaneous health.” The Review of Economic Studies, rdv043.
Schwartz, Joel. 1997. “Air pollution and hospital admissions for cardiovas-cular disease in Tucson.” Epidemiology, 371–377.
Sheppard, Dean, W Scott Wong, Ch F Uehara, Jay A Nadel, andHomer A Boushey. 1980. “Lower threshold and greater bronchomotorresponsiveness of asthmatic subjects to sulfur dioxide.” The American reviewof respiratory disease, 122(6): 873–878.
Smith, David H, Daniel C Malone, Kenneth A Lawson, Lynn JOkamoto, Carmelina Battista, and William B Saunders. 1997. “Anational estimate of the economic costs of asthma.” American Journal ofRespiratory and Critical Care Medicine, 156(3): 787–793.
Stranges, Elizabeth, Chaya T Merrill, and Claudia A Steiner. 2008.“Hospital Stays Related to Asthma for Children, 2006.” Agency for HealthCare Policy and Research.
van Vliet, Patricia, Mirjam Knape, Jeroen de Hartog, NicoleJanssen, Hendrik Harssema, and Bert Brunekreef. 1997. “Motorvehicle exhaust and chronic respiratory symptoms in children living nearfreeways.” Environmental research, 74(2): 122–132.
Wang, Li Yan, Yuna Zhong, and Lani Wheeler. 2005. “Direct and In-direct Costs of Asthma in School-age Children.” Preventing chronic disease[electronic resource]., 2(1).
Weiland, Stephan K, Kenneth A Mundt, Anja Ruckmann, and Ul-rich Keil. 1994. “Self-reported wheezing and allergic rhinitis in children andtraffic density on street of residence.” Annals of epidemiology, 4(3): 243–247.
Wilhelm, Michelle, and Beate Ritz. 2003. “Residential proximity to trafficand adverse birth outcomes in Los Angeles county, California, 1994-1996.”Environmental Health Perspectives, 111(2): 207.
Zimmerman, Dale, Claire Pavlik, Amy Ruggles, and Marc P Arm-strong. 1999. “An experimental comparison of ordinary and universal krig-ing and inverse distance weighting.” Mathematical Geology, 31(4): 375–390.
48

A Data Appendix
A.1 Key Variables
Figure A1: Distribution of τ across zip codes0
.51
1.5
22.
5D
ensi
ty
0 .2 .4 .6 .8 1Percent of population living near highway
49

A.2 Wind
Figure A2: Prevailing Wind Direction
P
P
P P
P
P
P
PP P
P
P
P
P
P
PP P
P
P
P
P
P
PP
P
P
P
P
P
P
P
P
P
PP
P
P
P
P
P
P
P
P
P
P
P
P
P
P
P
P
PP
P
P
P
PP
P
P
P
P
PP
P
P
P
P
P
P
P
P
P
P
P
P
P
P
¶
¶¶¶
¶
¶¶
¶
¶
¶
¶
¶¶
¶ ¶
¶
¶
¶
¶¶
¶¶
¶
¶ ¶
¶
¶
¶¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶¶
¶¶
¶
¶
¶ ¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶¶
¶
¶
¶¶
¶
¶
¶
¶¶
¶
¶ ¶
¶
¶
¶
¶
¶
¶
¶¶¶
¶
¶
¶ ¶
¶
¶ ¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶¶
¶¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶¶
¶¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶¶
¶
¶¶
¶
¶
¶
¶
¶
¶¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶¶ ¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶¶
¶
¶
¶¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶
¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶ ¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶
¶ ¶ ¶ ¶ ¶ ¶ ¶ ¶ ¶ ¶ ¶ ¶ ¶ ¶
LegendWind Direction & Strength
¶ 0.000 - 0.207
¶ 0.208 - 0.367
¶ 0.368 - 0.496
¶ 0.497 - 0.625
¶ 0.626 - 0.809P Weather Stations
ZCTA0 80 16040 Miles
±
Notes: Average wind directions are calculated for the 79 stations in California recordingwind direction during the study period. Using ArcMap 10.1, the prevailing wind directionis interpolated across California using inverse distance weighting.
50

Figure A3: Prevailing Wind Direction Classifications
LegendUS & State HighwaysDownwindCrosswindUpwind
0 80 16040 Miles
±
Notes: Groups are based on the difference between the angle from which the prevailing windoriginates and the angle from the zip code centroid to the nearest highway. Downwind,crosswind, and upwind zip codes are those with an angle difference less than 45, 45 to 135,and over 135 degrees, respectively.
51

A.3 Highways
Figure A4: U.S. and state highways in California
Notes: Information on the location of highways comes from combining data on U.S. andState Highways from the U.S. Census Bureau’s 2000 TIGER/Line geographical informationsystems (GIS) shapefiles available through the Californian Spatial Information Library. Thehighway data is spatially linked to Cartographic Boundary files for census tracts and zipcodes using ArcMap 10.1. I define a highway as either a U.S. or State highway, as definedby the U.S. Census Bureau.
52

The U.S. Census Bureau classifies U.S. and State highways in the follow-ing way. U.S. highways fall under one of two categories: “Primary highwaywith limited access” (A1) and “primary road without limited access” (A2).Interstate highways and some toll highways are in the A1 category and aredistinguished by the presence of interchanges. These highways are accessed byway of ramps and have multiple lanes of traffic. The A2 category includes na-tionally and regionally important highways that do not have limited access asrequired by category A1. It consists mainly of U.S. highways, but may includesome state and county highways that connect cities and larger towns. Statehighways are defined by the U.S. Census Bureau as category A3, “secondaryand connecting roads”, which include mostly state highways and some countyhighways that connect smaller towns, subdivisions, and neighborhoods. Forthe purposes of this project I will consider highways to be all roadways thatfall into categories A1, A2, or A3.
B Neighborhood Characteristics
CBG is likely to have the largest impact on people living near highways,given the documented relationship between distance from highways and levelof traffic-related air pollution (Gilbert et al., 2003). However, a cross-sectionalcomparison of people living near and far from highways will be biased by dif-ferences in observable and unobservable characteristics which are correlatedboth with choice of residence and susceptibility to asthma. Table B1 showssummary statistics from the 1990 and 2000 Censuses for census tracts based onproximity to highway traffic.49 Looking at the average characteristics of tractsfar and near highways in 1990 (columns 2 and 3), tracts near the highway aregenerally more disadvantaged. They are more likely to have a larger percent-age of non-white residents, a larger percentage of Hispanics, a larger percent-age of single female households with young children, lower levels of educationalattainment, a larger percentage of foreign born and non-citizens, higher unem-ployment, a larger percentage of blue collar workers, and a greater percentagebelow the poverty level. Clearly, a cross-sectional comparison would be biasedby the differences in underlying population characteristics that are known tobe related to health outcomes as well.
Table B1 also shows the change in demographic characteristics from the1990 to 2000 Censuses for tracts that are both near and far from highways.
49The “near” group contains all census tracts with over 99.9 percent of the area within 1kmof a highway and the “far” group contains all other tracts. Recent research has suggestedthat traffic pollution can travel up to 1km from the highway (Hu et al., 2009).
53

Columns (10) and (11) show the 2000-1990 difference in characteristics fortracts far and near to highways, respectively. For example, the percentagewhite decreased by about 10.3 percent and 9.9 percent for far and near tracts,respectively, from 1990 to 2000. The relative change in characteristics from1990 to 2000 between far and near tracts is shown in the final column. As youcan see, there are statistically significant differences in characteristics betweennear and far tracts in both 1990 and 2000 (columns 4 and 8), but column(12) shows that the relative change in characteristics over time is much lessoften significant. Although some characteristics remain significant, such as thepercentage black, the magnitude of the difference-in-difference is very small,less than 1 percent, and it is unlikely that these demographic characteristicsshifted discontinuously at the time of the policy.
54

Tab
leB
1:C
ensu
str
act
dem
ogra
phic
char
acte
rist
ics
(%)
1990
2000
2000
-199
0D
iffer
ence
Diff
-in-d
iffT
otal
Far
Nea
rD
iffT
otal
Far
Nea
rD
iffT
otal
Far
Nea
r(1
)(2
)(3
)(4
)(5
)(6
)(7
)(8
)(9
)(1
0)(1
1)(1
2)
Whit
e0.
588
0.62
50.
473
0.15
1***
0.48
60.
521
0.37
50.
146*
**-0
.102
***
-0.1
03-0
.099
-0.0
05B
lack
0.06
70.
058
0.09
4-0
.036
***
0.06
20.
056
0.08
3-0
.027
***
-0.0
05*
-0.0
03-0
.011
0.00
9***
Am
eric
anIn
dia
n0.
007
0.00
70.
005
0.00
3***
0.00
60.
007
0.00
40.
003*
**-0
.001
**-0
.001
-0.0
010.
000
Asi
an0.
087
0.08
20.
104
-0.0
22**
*0.
107
0.10
20.
124
-0.0
22**
*0.
020*
**0.
020
0.01
90.
001
Oth
er0.
002
0.00
20.
002
-0.0
00**
*0.
029
0.02
90.
029
0.00
00.
027*
**0.
027
0.02
70.
001
His
pan
ic0.
249
0.22
70.
322
-0.0
95**
*0.
310
0.28
60.
386
-0.1
00**
*0.
060*
**0.
059
0.06
4-0
.005
*
Fem
ale
hou
sehol
d0.
117
0.11
00.
136
-0.0
25**
*0.
129
0.12
40.
148
-0.0
24**
*0.
013*
**0.
013
0.01
20.
002
Sin
gle
Mot
her
0.07
70.
074
0.09
-0.0
16**
*0.
088
0.08
40.
101
-0.0
17**
*0.
011*
**0.
011
0.01
1-0
.001
Les
sth
an9t
hgr
ade
0.11
90.
108
0.15
6-0
.049
***
0.12
20.
110
0.16
1-0
.051
***
0.00
30.
002
0.00
5-0
.002
9th
to12
thgr
ade
0.13
10.
126
0.14
4-0
.017
***
0.12
10.
116
0.13
7-0
.021
***
-0.0
09**
*-0
.010
-0.0
06-0
.004
**H
igh
school
grad
uat
e0.
223
0.22
70.
210.
017*
**0.
202
0.20
60.
191
0.01
5***
-0.0
21**
*-0
.021
-0.0
19-0
.002
Som
eco
lleg
e0.
301
0.31
00.
275
0.03
5***
0.29
60.
306
0.26
40.
041*
**-0
.006
***
-0.0
04-0
.011
0.00
7***
Bac
hel
ors
deg
ree
0.14
80.
150
0.14
0.00
9***
0.16
50.
167
0.15
80.
009*
*0.
017*
**0.
017
0.01
70.
000
Gra
duat
edeg
ree
0.07
80.
079
0.07
40.
005*
0.09
40.
095
0.08
90.
007*
0.01
6***
0.01
60.
015
0.00
2
Nat
ive
0.79
10.
814
0.71
90.
095*
**0.
747
0.77
10.
672
0.09
9***
-0.0
44**
*-0
.044
-0.0
470.
003
Bor
nin
CA
0.46
60.
481
0.41
80.
062*
**0.
502
0.51
70.
453
0.06
4***
0.03
6***
0.03
60.
034
0.00
1B
orn
inot
her
stat
e0.
312
0.32
00.
287
0.03
3***
0.23
40.
243
0.20
80.
035*
**-0
.078
***
-0.0
77-0
.079
0.00
2F
orei
gnB
orn
0.20
90.
186
0.28
1-0
.095
***
0.25
30.
229
0.32
8-0
.099
***
0.04
4***
0.04
40.
047
-0.0
03N
on-c
itiz
en0.
142
0.12
30.
202
-0.0
79**
*0.
152
0.13
40.
209
-0.0
75**
*0.
010*
**0.
011
0.00
70.
005*
Unem
plo
yed
0.04
40.
043
0.04
9-0
.006
***
0.04
40.
043
0.04
7-0
.004
***
-0.0
000.
001
-0.0
020.
003*
**B
lue
Col
lar
0.41
00.
404
0.42
9-0
.026
***
0.39
30.
386
0.41
4-0
.028
***
-0.0
17**
*-0
.018
-0.0
15-0
.002
Bel
owp
over
tyle
vel
0.09
80.
090
0.12
5-0
.036
***
0.11
20.
103
0.14
3-0
.041
***
0.01
4***
0.01
30.
018
-0.0
05**
Fem
ale
hh
bel
owp
over
ty0.
044
0.04
00.
058
-0.0
18**
*0.
047
0.04
20.
061
-0.0
19**
*0.
002*
*0.
002
0.00
4-0
.002
Not
es:
Nea
rdes
ignate
sce
nsu
str
acts
that
are
wit
hin
1km
of
ahig
hw
ay(o
ver
99.9
%of
the
tract
are
a).
Far
des
ignat
esall
oth
erce
nsu
str
act
s.C
olum
ns
(1)
and
(5)
show
aver
age
censu
sdem
ogra
phic
chara
cter
isti
csin
1990
and
2000
for
all
censu
str
act
s,re
spec
tive
ly,
and
colu
mn
(9)
show
sth
eov
eral
ldiff
eren
cein
chara
cter
isti
csac
ross
all
trac
tsfr
om19
90to
2000.
Colu
mns
(2)
and
(3)
show
the
1990
aver
age
chara
cter
isti
csof
tract
sfa
rand
nea
rhig
hw
ays,
resp
ecti
vely
,an
dco
lum
n(4
)sh
ows
the
far-
nea
rdiff
eren
cein
1990
.C
olu
mns
(6)
and
(7)
show
the
2000
aver
age
chara
cter
isti
csof
tract
sfa
rand
nea
rhig
hw
ays,
resp
ecti
vel
y,an
dco
lum
n(8
)sh
ows
the
far-
nea
rdiff
eren
cein
2000
.C
olum
ns
(10)
and
(11)
show
the
diff
eren
cein
aver
age
chara
cter
isti
csfr
om
1990
to2000
for
trac
tsfa
ran
dnea
rhig
hw
ays,
resp
ecti
vely
.F
inal
ly,
and
ofm
ost
inte
rest
,co
lum
n(1
2)
esti
mat
esth
ediff
eren
ce-i
n-d
iffer
ence
,w
hic
his
the
200
0-1
990
far
diff
eren
ce(c
olum
n10)
min
us
the
2000
-1990
nea
rdiff
eren
ce(c
olum
n11
).***
p<
0.0
1,**
p<
0.05
,*
p<
0.1
55

C Robustness
Table C2: Robustness to variation in treatment definition
Asthma hospitalizations per 10,000 childrenMedian 50% Tercile Quartile %Close
(1) (2) (3) (4) (5)
Treat*After -4.248*** -3.602*** -4.468*** -5.445** -7.652***(1.365) (1.289) (1.723) (2.110) (2.461)
%∆ from pre-treat -8.3 -7.0 -8.7 -10.6 -14.9Observations 11,787 11,787 7,707 5,740 11,787R-squared 0.594 0.593 0.586 0.564 0.594Zip Code FE yes yes yes yes yesYear dummies yes yes yes yes yes
Notes: The first column is based on treated (control) zip codes with at least (less than) themedian percentage (42.5 percent) of τ . Column 2 is based on treated (control) zip codeswith at least (less than) 50 percent of τ . Column 3 is based on treated (control) zip codesthat are in the highest (lowest) tercile of τ . Column 4 is based on treated (control) zip codesthat are in the highest (lowest) quartile of τ . Standard errors clustered at the zip code levelare in parentheses. *** p<0.01, ** p<0.05, * p<0.1
Table C3: Diagnostics for spatial dependence
Test Value ProbLagrange Multiplier (lag) 0.039 0.8438Robust LM (lag) 0.030 0.8626
Lagrange Multiplier (error) 0.014 0.9062Robust LM (error) 0.005 0.9436
Lagrange Multiplier (SARMA) 0.044 0.9783
Notes: Test statistics and P-values for Lagrange Multiplier tests forspatial lag, spatial error, and SARMA models. The null hypothesisis no spatial dependence. Neighboring zip codes are defined using aqueen weights matrix.
56

C.1 Non-parametric results
Asthmazy = B0 +10∑x=2
[BxAfter∗τx] + Zz + Θy + ε11zy (12)
where τx is a set of 10 binned dummy variables, one for each 10 percentagepoint range of τ .
Figure C5: Non-parametric results
−15
−10
−5
05
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Notes: Coefficients and 90% confidence intervals are shown for each of the After∗τx variablesfrom equation 12. The largest and most significant declines in asthma occur in zip codeswith the largest portion of the population living within 1km from a highway, as expected.
57

C.2 Pollution Interpolation: Kriging
Figure C6: Change in pollution following CBG: interpolation by Kriging
-3.5
-3-2
.5-2
-1.5
no2
0 .2 .4 .6 .8 1
95% CI D no2
no2
-.4
-.35
-.3
-.25
-.2
-.15
co
0 .2 .4 .6 .8 1
95% CI D co
co
-1-.
8-.
6-.
4-.
2so
2
0 .2 .4 .6 .8 1
95% CI D so2
so2
% population within 1km of highway
Notes: Shows the change in pollution levels from before to after the policy. The levelchange is calculated by zip code for NO2, CO, and SO2. Figures show the local meansmoothed relationship between the change in pollution and the percentage of the populationliving within 1km of a highway, τ . Zip codes nearer to the highway (i.e. values of τ near1) experienced the largest decreases in pollution after the policy. Lines show local meansmoothing using “lpoly,” with degree zero and a 0.1 bandwidth.
Table C4: First stage: interpolation by KrigingNO2 CO SO2 NO2 CO SO2(1) (2) (3) (4) (5) (6)
Panel A.Treat*After -0.750*** -0.098*** -0.228*** -0.546*** -0.094*** -0.204***
(0.141) (0.0101) (0.0431) (0.150) (0.0109) (0.0374)
Panel B.%Close*After -1.381*** -0.195*** -0.532*** -0.977*** -0.188*** -0.450***
(0.244) (0.0182) (0.0801) (0.258) (0.0195) (0.0677)
Observations 13,434 13,471 10,610 13,434 13,471 10,610R-squared 0.980 0.971 0.716 0.979 0.969 0.740Zipcode FE yes yes yes yes yes yesYear dummies yes yes yes yes yes yesWeighted no no no yes yes yes
Notes: Panel A shows regression results based on the binary treatment status indicator. Panel B showsregression results based on the continuous measure of treatment status. Columns (4)-(6) show resultsweighted by the inverse of the interpolation prediction error. Standard errors clustered at the zip codelevel are in parentheses. *** p<0.01, ** p<0.05, * p<0.1
58

D Potential Confounders
D.1 RFG
As part of the Clean Air Act Amendment of 1990, the federal governmentmandated specific requirements for gasoline, such as limitation on lead-basedantiknock agents, mandated detergent additives, limitations on Reid VaporPressure, mandated oxygen content, and reformulated gasoline (RFG). RFGtargets both NOx and CO emissions. Severe ozone non-attainment areas ofthe U.S., including parts of California, were required to implement Phase Iof RFG gasoline in January of 1995. However, in 1996 the entire state ofCalifornia, both RFG and non-RFG areas, became subject to more stringentCBG standards. Therefore, there may be some downward trend in pollutionthat begins in 1995, rather than 1996 for RFG areas in California. However,research by Auffhammer and Kellogg (2011) finds that RFG gasoline has littleimpact on pollution. In fact, they find that the only significant impacts onpollution come from the more stringent CBG regulations.
With data indicating which areas of California were subject to RFG gaso-line, I can examine whether the decrease in asthma originates from RFG orCalifornia’s CBG. Table D5 shows the baseline estimates in column (1). Col-umn (2) limits the sample to non-RFG zip codes, showing that there is still asignificant decrease in asthma for areas that only experienced CBG in 1996.Even though the sample size is smaller, the results remain significant, whichprovides some confidence that CBG does impact asthma. Column (3) testswhether the RFG zip codes have a significant difference from non-RFG zipcodes following RFG implementation in 1995. The estimate is negative but notsignificant, suggesting that there is not much difference in asthma after 1995for RFG zip codes. Column (4) exploits zip code level variation in exposureto highways to test whether zip codes close to highways and in RFG areas hadfewer asthma hospitalizations following RFG implementation in 1995. Again,the coefficient is negative and slightly larger, but still not significant. Whenthis variable is included along with the primary CBG difference-in-differenceestimator in column (5), the CBG estimator is strongly significant and theRFG estimator is insignificant. This supports the claim that the more strin-gent CBG regulations had a strong impact on asthma hospitalizations and thisimpact was not driven by federal RFG gasoline.
59

Table D5: Control for Federal RFG gasoline regulation in 1995
Asthma hospitalizations per 10,000 childrenBaseline Non-RFG
(1) (2) (3) (4) (5)
Treat*After96 -4.248*** -4.419** -4.422***(1.365) (2.097) (1.498)
RFG*After95 -0.0377(1.520)
Treat RFG*After95 -2.184 0.376(1.423) (1.545)
Observations 11,787 5,310 11,787 11,787 11,787R-squared 0.594 0.538 0.593 0.593 0.594Zip Code FE yes yes yes yes yesYear dummies yes yes yes yes yes
Notes: Standard errors clustered at the zip code level are in parentheses. *** p<0.01, **p<0.05, * p<0.1
D.2 PRWORA
The Personal Responsibility and Work Opportunity Reconciliation Act waspassed in 1996 (PRWORA). This welfare reform legislation replaced the Aidto Families with Dependent Children (AFDC) with Temporary Assistance forNeedy Families (TANF), a new federal block grant to states. Before TANF,eligibility for Medicaid and AFDC were closely linked. In fact, a person whoreceived an AFDC check was automatically entitled to Medicaid. Policymakersunlinked TANF from Medicaid eligibility amidst concerns that tighter welfareeligibility criteria in TANF might unintentionally cause many people to losehealth insurance coverage. The new law required states to use the AFDC eli-gibility criteria from before the law change in determining Medicaid eligibilityfor families with children, regardless of TANF eligibility (Ku and Coughlin,1997).
However, research has suggested that enrollment problems arose followingthe PRWORA changes. Medicaid policies and eligibility requirements are com-plex, especially for the poorest families, and welfare staff are not adequatelytrained in Medicaid policies to assist families who may not qualify for wel-fare, but could qualify for Medicaid. From 1995 to 1998, monthly Medicaidenrollment declined 12 percent in California (Ellwood et al., 1999).
60

Although this affects everyone in the state of California, it could be prob-lematic if patients eligible for Medicaid are more likely to live in the treatmentzip codes, and they are less likely to show up in the hospital data due toenrollment issues rather than an asthma decline.
However, this is probably not driving the results for the following reasons.First, consider only patients with private insurance. If enrollment issues weredriving the main results, then we should not see a decline in asthma among theprivate insurance patients. Medicaid enrollment issues should only impact theprivate insurance group if former Medicaid patients switch to private insurancefollowing PRWORA. If anything, these switchers might drive the asthma rateup for the private insurance group since they are likely to be of lower SES.However, in Table D6 we see a decline in asthma for private insurance patientsin treatment relative to control zip codes following CBG implementation. Thissuggests that Medicaid enrollment issues are not driving the results.
Second, the Emergency Medical Treatment and Active Labor Act (EM-TALA) of 1986 required hospitals to provide care to anyone needing emergencyhealth care treatment regardless of citizenship, legal status, or ability to pay.Given that the uninsured are often forced to use the emergency room as theirprimary source of care, PRWORA should not have an impact on emergencyhospitalizations for asthma. We can test this more clearly in two ways: limit-ing our sample of asthma patients to those whose hospital admission originatedin the ER (column 5), and using the sample of asthma patients whose visitwas unscheduled (column 6).
The reduction in asthma admissions remains significant. Furthermore, bar-riers to Medicaid enrollment from the PRWORA are more likely to impactaccess to and use of prescription drugs used to treat asthma. In Figure D7,state utilization data from the Medicaid Drug Rebate Program show thatthe total amount reimbursed for prescription drugs used to treat asthma de-clined sharply during this period in both California and the entire US. Fig-ure D8 shows that the drop can be attributed almost entirely to quick-reliefmedicines, or “rescue drugs”, used to control asthma symptoms or during anasthma attack. The drop in prescription drug use can be attributed both toMedicaid enrollment issues and a reduction in pollution levels following CBG.It is difficult to distinguish between these two factors since they occurredcontemporaneously. However, the reduction in access to asthma control med-ications from PRWORA would likely increase the number of hospitalizationsfor asthma. Therefore, if anything, the asthma hospitalization results here willbe understated.
61

Table D6: Heterogeneous effects: Insurance type, ER, and unscheduled hospi-talizations
Insurance TypeMedicare or
Medi-Cal Private Self-Pay Other ER Unscheduled(1) (2) (3) (4) (5) (6)
Panel A.Treat*After -3.748*** -2.300*** 0.480* -0.185 -3.163*** -5.292***
(1.122) (0.743) (0.267) (0.204) (1.113) (1.407)
%∆ from pre-treat -9.6 -9.5 19.8 -16.4 -8.4 -9.8%∆ in gap -52.12 -36.4 -95.8 -70.3 -35.4 -46.4%∆ of std dev -9.0 -15.1 11.1 -4.8 -9.8 -12.9
Panel B.%Close*After -8.104*** -3.496*** 1.113** -0.422 -5.641*** -10.05***
(2.043) (1.278) (0.478) (0.370) (2.119) (2.492)
Observations 10,799 10,799 10,799 10,799 11,850 11,850R-squared 0.701 0.376 0.197 0.259 0.572 0.583Zip Code FE yes yes yes yes yes yesYear dummies yes yes yes yes yes yes
Notes: The insurance variable recorded in the data was modified in 1995 and 1999. The categories presented herewere consistently queried over time, but the composition of each may have been affected by changes in the othercategories surveyed. The majority of patients fell into either Medicare/Medi-Cal or private insurance. Standarderrors clustered at the zip code level are in parentheses. *** p<0.01, ** p<0.05, * p<0.1
Figure D7: Medicaid reimbursement for asthma pre-scription drugs
1516
1718
19Lo
g(T
otal
Am
ount
Rei
mbu
rsed
)
1992q3 1994q3 1996q3 1998q3 2000q3
National CA
Notes: Asthma prescription drugs include antiasthmatic com-binations, inhaled corticosteroids, leukotriene modifiers, long-acting inhaled beta-2 agonists, mast cell stablizers, methylxan-thines, and short-acting inhaled beta-2 agonists.
62

Figure D8: Medicaid reimbursement for asthma pre-scription drugs: quick-relief and long-term control
1415
1617
1819
Log(
Tot
al A
mou
nt R
eim
burs
ed)
1992q3 1994q3 1996q3 1998q3 2000q3
quick−relief CA quick−relief USlong−term control CA long−term control US
Notes: Asthma drugs that provide quick-relief from asthmasymptoms are the short-acting inhaled beta-2 agonists. Long-term control medications include inhaled corticosteroids,leukotriene modifiers, long-acting inhaled beta-2 agonists, mastcell stablizers, and methylxanthines.
63