Embed Size (px)
Citation preview
3/6/2018
1
Oncologic Emergencies
Ellen Alberts MSN, ARNP-CNS, AGCNS-BC, AOCNS
PSONS Fundamentals of Oncology
Spring 201
Overview
The Basics Oncologic emergencies are life-threatening medical
emergencies and must be treated as such!
Why do they occur?
• Malignancy
• Treatment of malignancy
When do they occur?
• Early in disease process (initial manifestation of malignancy itself)
• Late in disease process (manifestation of treatment of malignancy)
Structural Emergencies
• Spinal Cord Compression
• Superior Vena Cava (SVC) Syndrome
• Increased Intracranial Pressure (ICP)
• Cardiac Tamponade
Metabolic Emergencies
• Tumor Lysis Syndrome (TLS)
• SIRS/Sepsis/Septic Shock
• Disseminated Intravascular Coagulation (DIC)
• Thrombotic Thrombocytopenia (TTP)
• Hypercalcemia
• Inappropriate Antidiuretic Hormone Secretion (SIADH)
• Anaphylaxis
• Hypersensitivity
(Maloney, 2016; Vogel 2016)
The Basics
3/6/2018
2
Structural Emergencies
• Spinal Cord Compression
• Superior Vena Cava (SVC) Syndrome
• Increased Intracranial Pressure (ICP)
• Cardiac Tamponade
Metabolic Emergencies
• Tumor Lysis Syndrome (TLS)
• SIRS/Sepsis/Septic Shock
• Disseminated Intravascular Coagulation (DIC)
• Thrombotic Thrombocytopenia (TTP)
• Hypercalcemia
• Inappropriate Antidiuretic Hormone Secretion (SIADH)
• Anaphylaxis
• Hypersensitivity
(Maloney, 2016; Vogel 2016)
The Basics
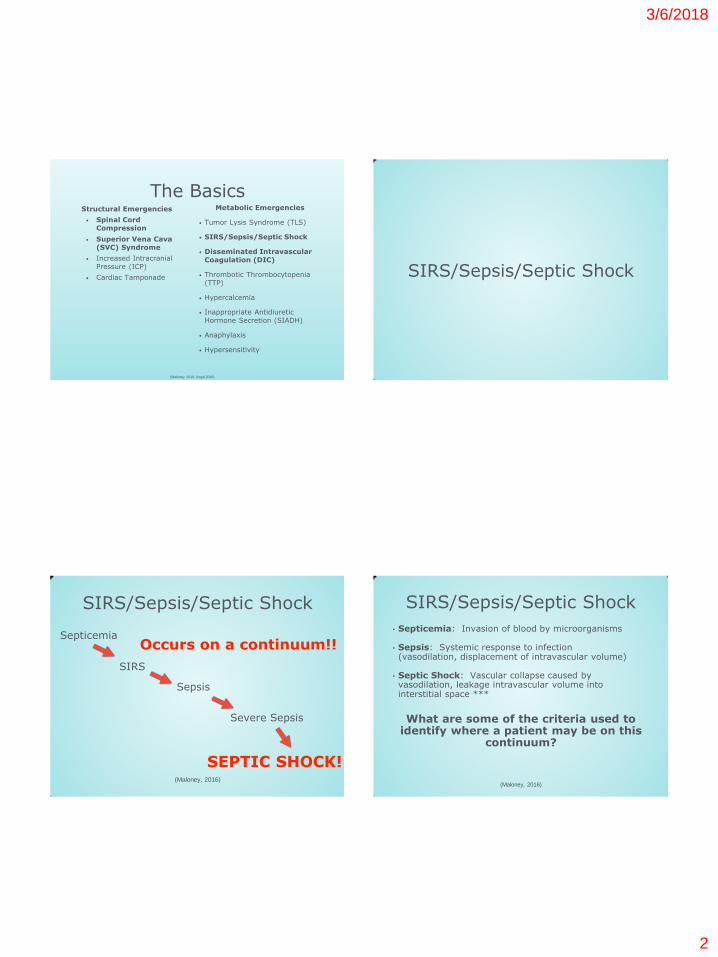
SIRS/Sepsis/Septic Shock
Occurs on a continuum!! Septicemia
SIRS
Sepsis
Severe Sepsis
SEPTIC SHOCK! (Maloney, 2016)
SIRS/Sepsis/Septic Shock
• Septicemia: Invasion of blood by microorganisms
• Sepsis: Systemic response to infection (vasodilation, displacement of intravascular volume)
• Septic Shock: Vascular collapse caused by vasodilation, leakage intravascular volume into interstitial space ***
What are some of the criteria used to identify where a patient may be on this
continuum?
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
3/6/2018
3
Pathophysiology:
1. Infection (can be bacterial, viral, or fungal)
2. Endotoxins and other cellular components released
3. Vasodilation
4. Increased vascular permeability
5. Decreased arterial/venous tone
6. Clot formation
7. End-organ damage
8. Cell death
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
• Neutropenia
• Infection
• Medical devices
• Mucositis
• Hospitalization
• Corticosteroids or other immunosuppressants
Risk Factors:
• Splenectomy
• Age
• Poor nutritional
status
• Concurrent
immunosuppressive disease
• Type of malignancy
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
Mr. J.: Seven days post-3rd cycle R-CHOP
•Wife calls outpatient clinic at 5 pm on Friday and reports husband has:
–Fever –Dry cough –Discomfort with swallowing
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
3/6/2018
4
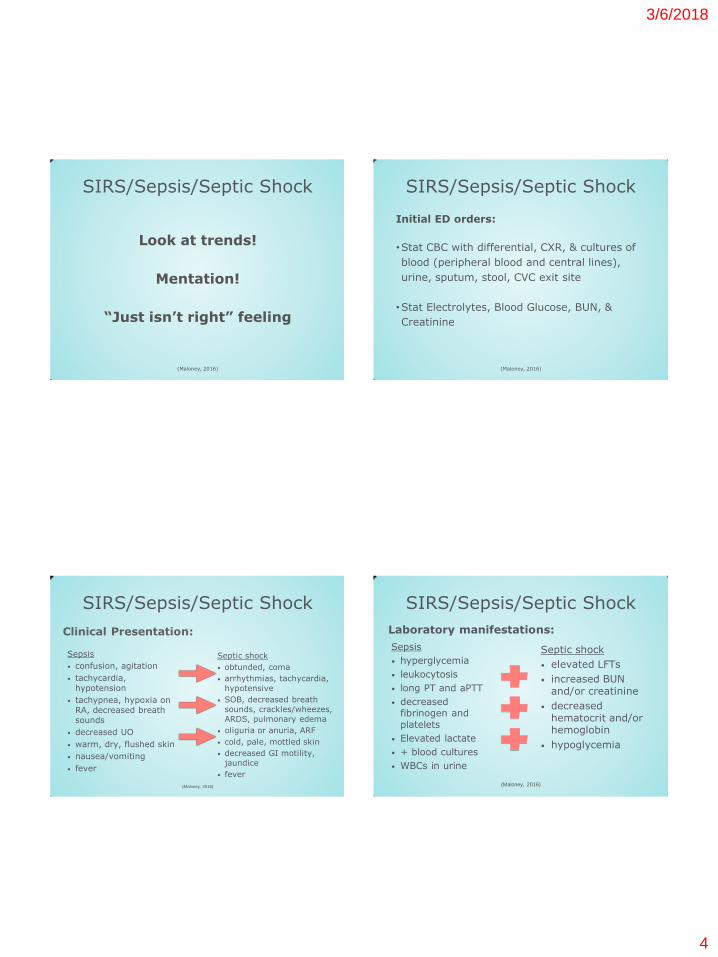
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
•Stat CBC with differential, CXR, & cultures of
blood (peripheral blood and central lines),
urine, sputum, stool, CVC exit site
•Stat Electrolytes, Blood Glucose, BUN, &
Creatinine
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
Sepsis
• confusion, agitation
• tachycardia, hypotension
• tachypnea, hypoxia on RA, decreased breath sounds
• decreased UO
• warm, dry, flushed skin
• nausea/vomiting
• fever
Clinical Presentation:
Septic shock
• obtunded, coma
• arrhythmias, tachycardia,
hypotensive
• SOB, decreased breath
sounds, crackles/wheezes,
ARDS, pulmonary edema
• oliguria or anuria, ARF
• cold, pale, mottled skin
• decreased GI motility,
jaundice
• fever
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
Septic shock
• elevated LFTs
• increased BUN and/or creatinine
• decreased hematocrit and/or hemoglobin
• hypoglycemia
Laboratory manifestations:
Sepsis
• hyperglycemia
• leukocytosis
• long PT and aPTT
• decreased fibrinogen and
platelets
• Elevated lactate
• + blood cultures
• WBCs in urine
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
3/6/2018
5
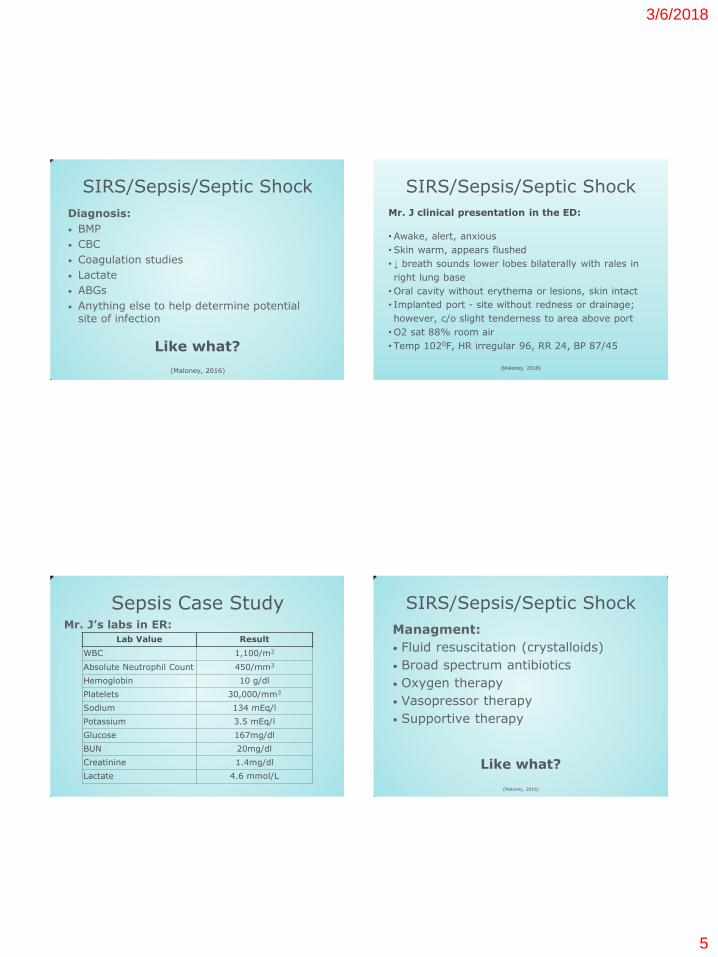
Diagnosis:
• BMP
• CBC
• Coagulation studies
• Lactate
• ABGs
• Anything else to help determine potential site of infection
(Maloney, 2016)
Like what?
SIRS/Sepsis/Septic Shock
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
Mr. J clinical presentation in the ED:
• Awake, alert, anxious
• Skin warm, appears flushed
• ↓ breath sounds lower lobes bilaterally with rales in
right lung base
•Oral cavity without erythema or lesions, skin intact
• Implanted port - site without redness or drainage;
however, c/o slight tenderness to area above port
•O2 sat 88% room air
• Temp 1020F, HR irregular 96, RR 24, BP 87/45
Mr. J’s labs in ER:
Lab Value Result
WBC 1,100/m2
Absolute Neutrophil Count 450/mm3
Hemoglobin 10 g/dl
Platelets 30,000/mm3
Sodium 134 mEq/l
Potassium 3.5 mEq/l
Glucose 167mg/dl
BUN 20mg/dl
Creatinine 1.4mg/dl
Lactate 4.6 mmol/L
Sepsis Case Study
Managment:
• Fluid resuscitation (crystalloids)
• Broad spectrum antibiotics
• Oxygen therapy
• Vasopressor therapy
• Supportive therapy
Like what?
(Maloney, 2016)
SIRS/Sepsis/Septic Shock

3/6/2018
6
SIRS/Sepsis/Septic Shock
Start Immediately Complete Within 3
Hours
Complete Within 6 Hours
• Measure lactate level • Administer 30 mg/kg
crystalloid over 10-15 minutes
• Obtain blood cultures • Administer broad-
spectrum antibiotics following blood cultures
• Administer vasopressors for hypotension unrelieved by crystalloids
• Measure central venous pressure and venous oxygen saturation
• Re-measure lactate
Dellinger, RP et al (2013). Surviving sepsis campaign: International guidelines
for management of severe sepsis and septic shock, 2012. Intensive Care
Medicine, 39, 165-228.
SIRS/Sepsis/Septic Shock
Complete Within 24
Hours
Additional Supportive
Measures
• Administer low-dose corticosteroids if hypotensive despite vasopressors
• Maintain glucose between lower limit of normal and 150 mg/dl
• Maintain inspiratory plateau pressure <30 cm H2O for mechanically ventilated
• Maintain adequate nutrition
• Prevent deep vein thrombosis
• Prevent stress and pressure ulcers
• Prevent additional infection
Dellinger, RP et al (2013). Surviving sepsis campaign: International guidelines for management
of severe sepsis and septic shock, 2012. Intensive Care Medicine, 39, 165-228.
Sepsis Case Study Admission orders for Mr. J:
•Meropenem 1 gm IV stat & Q8h
•Vancomycin 1000 mg IV stat & Q12h
•Supplemental O2 to keep saturations > 92%
•Vital signs Q_ hours
•Blood glucose checks Q_ hours
•CBC, CMP Qam
• Immunocompromised diet
•Admit to medical oncology unit
•Neutropenic precautions
Sepsis Case Study Nursing Assessment of Mr. J upon inpatient admission: •Extreme restlessness & anxiety
•Shaking chills
•Skin warm, flushed
•Temp 102.40F
•HR 120 irregular, bounding
•RR 26, oxygen saturation 89% 2 lpm via nc
•BP 74/40
•No urine output since early am
•Blood glucose 61 mg/dl
3/6/2018
7
Sepsis Case Study
RRT
Transfer to higher level of care
Nursing Management:
• Prevention and early recognition!!!!
• Frequent vitals and assessments
• Maintain adequate oxygenation
• Administer fluids and antibiotics on time
• Educate!
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
Test your knowledge!
You have just started your shift and received bedside report. Which patient should you go to see first?
A. The independent patient receiving EPOCH and is
starting to have frequent diarrhea
B. The patient who is receiving their second bag of
PRBCs, which they are tolerating well
C. The independent, neutropenic patient, who is
having frequent diarrhea
D. The patient with a central line and a peripheral IV,
both of which are being used
SIRS/Sepsis/Septic Shock
Test your knowledge!
You have just started your shift and received bedside report. Which patient should you go to see first?
A. The independent patient receiving EPOCH and is
starting to have frequent diarrhea
B. The patient who is receiving their second bag of
PRBCs, which they are tolerating well
C. The independent, neutropenic patient, who is
having frequent diarrhea
D. The patient with a central line and a peripheral IV,
both of which are being used
SIRS/Sepsis/Septic Shock
3/6/2018
8
Test your knowledge!
Which of the following oncologic emergencies is a potential
complication of septic shock?
A. Increased intracranial pressure
B. Disseminated intravascular coagulation
C. Tumor lysis syndrome
D. Anaphylaxis/hypersensitivity
SIRS/Sepsis/Septic Shock
Test your knowledge!
Which of the following oncologic emergencies is a potential
complication of septic shock?
A. Increased intracranial pressure
B. Disseminated intravascular coagulation
C. Tumor lysis syndrome
D. Anaphylaxis/hypersensitivity
SIRS/Sepsis/Septic Shock
Disseminated Intravascular Coagulation
(DIC)
Disseminated Intravascular Coagulation
Definition: Generalized activation of the hemostatic system, which results in widespread
intravascular deposition of fibrin in the microvasculature and the simultaneous consumption of coagulation factors and
platelets. DIC is never a primary diagnosis. It ALWAYS is
a symptom of an underlying disease.
(Maloney, 2016; Viele, 2008)
3/6/2018
9
Causes:
• Sepsis
• Severe infection
• Vascular abnormalities
• Severe allergic reactions
• Severe immunologic reactions
• Malignancy (both solid and liquid)
(Maloney, 2016; Viele, 2008)
Disseminated Intravascular Coagulation
Disseminated Intravascular Coagulation
Basic pathophysiology:
• Overactivation of coagulation cascade from certain proteins
• can be intrinsic (blood vessel damage)
• can be extrinsic (tissue damage)
• Clots begin to form and are deposited throughout the body’s vasculature
• Because of excessive clotting, clotting factors and platelets are all used up!
• This means there is no more clotting factors and platelets for normal clotting anymore, which allows for abnormal bleeding!
(Maloney, 2016; Viele, 2008)
Disseminated Intravascular Coagulation
Clinical Presentation:
• Skin: pallor, petechiae, jaundice, ecchymosis,
hematomas, acrocyanosis
• EENT: visual disturbances, scleral injection, periorbital edema, subconjunctival hemorrhage, eye and ear pain,
petechiae on nasal and/or oral mucosa, epistaxis, tender and bleeding gums
• Cardiac: tachycardia, hypotension, weak
peripheral pulses, color and temperature changes to extremities
• Respiratory: dyspnea, tachypnea, hypoxia, hemoptysis, cyanosis, SOB
(Maloney, 2016; Viele, 2008)
Disseminated Intravascular Coagulation
Clinical Presentation (continued):
• GI: tarry stools, hematemesis, abdominal pain, abdomina distension, guiac positive stools
• GU: hematuria, decreased UO
• Musculoskeletal: joint pain and stiffness
• Neuro: headache, restlessness, confusion, lethargy, altered LOC, obtundation,
seizures, coma
(Maloney, 2016; Viele, 2008)
Disseminated Intravascular Coagulation
3/6/2018
10
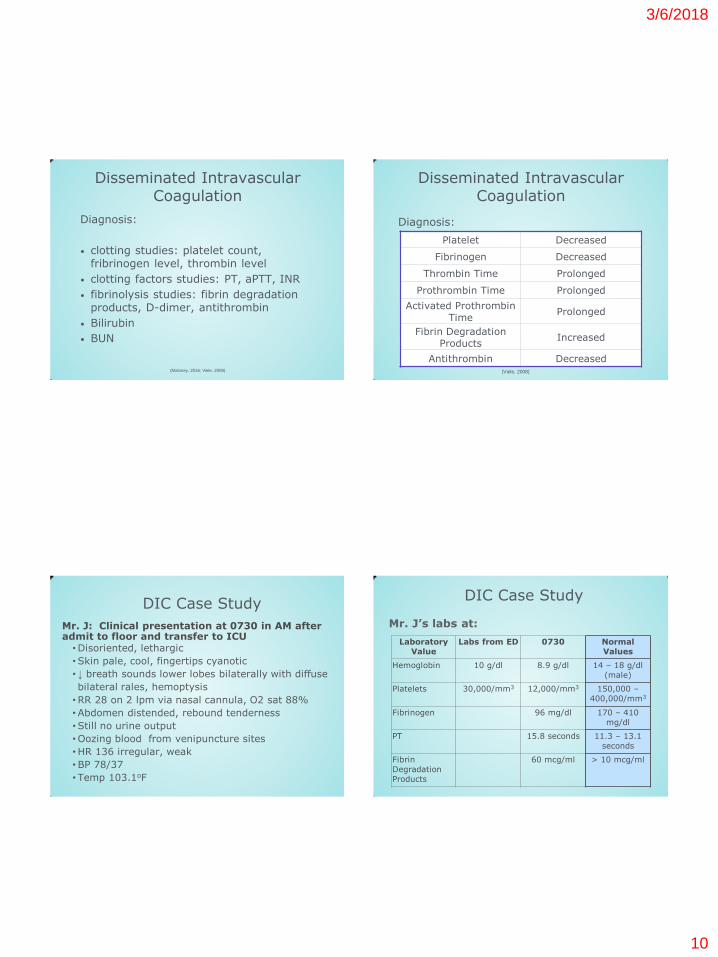
Diagnosis:
• clotting studies: platelet count, fribrinogen level, thrombin level
• clotting factors studies: PT, aPTT, INR
• fibrinolysis studies: fibrin degradation products, D-dimer, antithrombin
• Bilirubin
• BUN
(Maloney, 2016; Viele, 2008)
Disseminated Intravascular Coagulation
Diagnosis:
Platelet Decreased
Fibrinogen Decreased
Thrombin Time Prolonged
Prothrombin Time Prolonged
Activated Prothrombin
Time Prolonged
Fibrin Degradation Products
Increased
Antithrombin Decreased (Viele, 2008)
Disseminated Intravascular Coagulation
DIC Case Study
Mr. J: Clinical presentation at 0730 in AM after admit to floor and transfer to ICU
•Disoriented, lethargic
•Skin pale, cool, fingertips cyanotic
• ↓ breath sounds lower lobes bilaterally with diffuse
bilateral rales, hemoptysis
•RR 28 on 2 lpm via nasal cannula, O2 sat 88%
•Abdomen distended, rebound tenderness
•Still no urine output
•Oozing blood from venipuncture sites
•HR 136 irregular, weak
•BP 78/37
• Temp 103.1oF
DIC Case Study
Laboratory
Value
Labs from ED 0730 Normal
Values
Hemoglobin 10 g/dl 8.9 g/dl 14 – 18 g/dl
(male)
Platelets 30,000/mm3 12,000/mm3 150,000 –
400,000/mm3
Fibrinogen 96 mg/dl 170 – 410
mg/dl
PT 15.8 seconds 11.3 – 13.1
seconds
Fibrin
Degradation
Products
60 mcg/ml > 10 mcg/ml
Mr. J’s labs at:
3/6/2018
11
Managment:
1. Treat underlying cause!!
May include:
✴ Transfusions (platelets, FFP,
cryopreciptate)
✴ Anticoagulants
✴ Fibrinolytic agents
✴ Anticoagulant factor concentrates
(Maloney, 2016; Viele, 2008)
Disseminated Intravascular Coagulation
Nursing Management
(Vogel, 2016)
• Early recognition!
• Good assessments
• VS
• Hemodynamics
• Oxygenation
• Fluid status
• Ensure patient safety
• Manage active bleeding
• Administration of anticoag therapy,
other meds, fluids, blood products
• Assist in patient coping
Disseminated Intravascular Coagulation
DIC Case Study
Orders for Mr. J:
• IV Heparin per hospital protocol
• 2 units PRBCs
• Strict I/O
• VS Q_ hours
• Supplemental O2 titrate to O2sat >92%
Spinal Cord Compression

3/6/2018
12
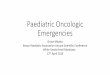
Spinal Cord Compression
Definition:
A neurological
emergency where the
spinal cord or cauda
equina is compromised by direct pressure,
vertebral collapse, or
both caused by direct
extension or
metastatic spread of
malignancy.
(Schulmeister & Gatlin, 2008; Vogel, 2016)
http://www.medscape.com/viewarticle/442735
Spinal Level % Involvement Associated Cancers
Cervical 10 Lung, breast, kidney,
lymphoma, myeloma,
melanoma
Thoracic 70 Lung, breast, kidney,
lymphoma, myeloma,
prostate
Lumbosacral 20 Lung, breast, kidney,
lymphoma, myeloma,
melanoma, prostate, GI
Cancers associated with spinal cord compression:
(Schulmeister & Gatlin, 2008)
Spinal Cord Compression
Risk Factors:
• Cancers that have a natural history of spreading to the bone
• Cancers that have a natural history of spreading to the brain and spinal cord
• Primary cancers of the spinal cord
• History of vertebral compression fractures
(Vogel, 2016)
Spinal Cord Compression
Pathophysiology: • Compression of spinal cord ✴Direct tumor pressure on cord ✴Tumor invasion of the vertebral column causing collapse & pressure on cord
• Compression leads to: ✴Edema ✴Inflammation
• Resulting in: ✴Direct neural injury to cord ✴Vascular damage
(Kaplan, 2013)
Spinal Cord Compression
3/6/2018
13
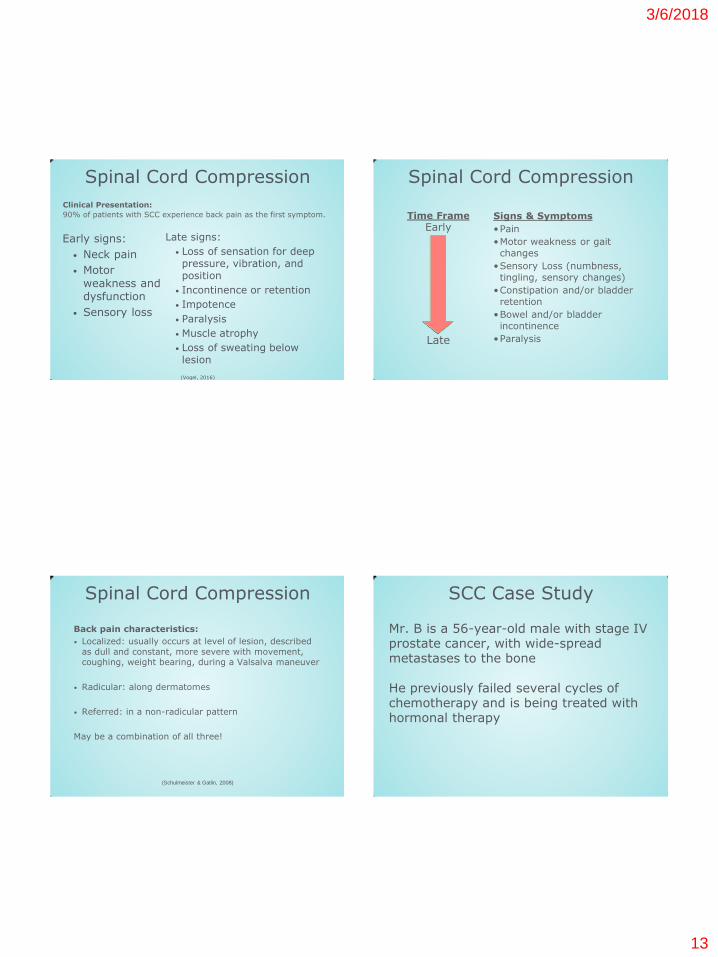
Early signs:
• Neck pain
• Motor
weakness and dysfunction
• Sensory loss
Clinical Presentation:
90% of patients with SCC experience back pain as the first symptom.
Late signs:
• Loss of sensation for deep pressure, vibration, and position
• Incontinence or retention
• Impotence
• Paralysis
• Muscle atrophy
• Loss of sweating below lesion
(Vogel, 2016)
Spinal Cord Compression Spinal Cord Compression
Signs & Symptoms
•Pain
•Motor weakness or gait
changes
•Sensory Loss (numbness,
tingling, sensory changes)
•Constipation and/or bladder
retention
•Bowel and/or bladder
incontinence
•Paralysis
Time Frame
Early
Late
Back pain characteristics:
• Localized: usually occurs at level of lesion, described as dull and constant, more severe with movement, coughing, weight bearing, during a Valsalva maneuver
• Radicular: along dermatomes
• Referred: in a non-radicular pattern
May be a combination of all three!
(Schulmeister & Gatlin, 2008)
Spinal Cord Compression SCC Case Study
Mr. B is a 56-year-old male with stage IV prostate cancer, with wide-spread metastases to the bone He previously failed several cycles of chemotherapy and is being treated with hormonal therapy

3/6/2018
14
Mr. B presents to Emergency Department with:
–Bi-lateral weakness in lower extremities
•Initial onset 5 days ago
•Difficulty ambulating, reports falling this
morning
–Numbness in the lower extremities
•Began earlier in the day
–Increasing back pain
•Has been taking oxycodone every 4 hours
which controlled his pain well until 4-5 days ago
•Currently rates his pain as 7 out of 10
SCC Case Study
Diagnosis: • MRI
– Gold standard for diagnosis – Accurate, sensitive, and specific diagnostic for malignant spinal cord compression
• Other diagnostic tests – Spinal x-rays
– CT scan – Bone scan and/or PET scan
(Vogel, 2016)
Spinal Cord Compression
Nonpharmacologic:
• Radiation
• Surgery
• Surgery followed by radiation
Treatment:
Immediate and aggressive!
Pharmacologic:
• Corticosteroids
• Chemotherapy
• Analgesics
• Bone remodeling
agents
(Vogel, 2016)
Spinal Cord Compression
Nursing Management:
(Vogel, 2016)
Spinal Cord Compression
• Manage pain and increase comfort • Promote physical mobility
• Improve or maintain neurologic function • Improve or maintain skin integrity • Increase knowledge of disease process
and therapeutic interventions • Preserve self-image and role performance
• Administer treatment as ordered!
3/6/2018
15
(Vogel, 2016)
•Mr. B received a loading dose of dexamethasone
10 mg, followed by tapering doses.
•He was admitted to the inpatient oncology unit
with initial activity orders for bed rest with only
log-rolling
•Surgical & radiation therapy consults were
ordered
SCC Case Study
•Three days after initiating radiation therapy, Mr.
B. developed urinary retention
•The following day he developed paraplegia,
urinary & bowel incontinence.
•Surgical consult re-evaluated Mr. B for emergent
decompression of spinal cord
•After family conference, Mr. B and his family
decided against surgical intervention and decided
on palliative care
SCC Case Study
Spinal Cord Compression
Nursing Interventions Early recognition:
• Thorough assessment of neck & back pain in high risk patients
Neurological assessments Assess effectiveness pain control Monitor bowel & bladder function PT, OT referrals, as appropriate
• Assess need for home care referrals and supportive medical equipment
Promote physical mobility Protect and/or improve skin integrity
•Mr. B completed his course of radiation
therapy while inpatient
•A hospice consult was obtained. Mr. B was
discharged from inpatient care to a hospice
facility
•Mr. B passed away 23 days later
SCC Case Study
3/6/2018
16
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Definition: Describes a pattern of physical findings that results from the obstruction of
blood flow through the superior vena cava, due to tumor or thrombus, compromising venous drainage from the head, neck, upper
extremities, and thorax.
(Mack & Becker, 2008; Vogel, 2016)
Risk Factors:
• Mediastinal malignancy
• Presence of a CVC and/or pacemaker
• History of radiation to the mediastinum
• Other associated conditions
• mediastinal fibrosis
• fungal infection
• aortic aneurysm
• benign mass
(Mack & Becker, 2008; Vogel, 2016)
Superior Vena Cava Syndrome
Pathophysiology:
1. Obstruction of the SVC occurs (depending on cause)
2. Venous pressure and congestion in the head, neck, thorax, upper extremities, and throat increases
3. Decreased cardiac filling and output occurs
4. Blood flow is diverted to smaller collateral vessels
(Mack & Becker, 2008; Vogel, 2016)
Superior Vena Cava Syndrome
3/6/2018
17
• Redness and edema in conjunctiva and around eyes and face
• Swelling of neck, arms, and hands
• Neck and thoracic vein distention
• Dyspnea
Early Clinical Presentation: Symptoms are more pronounced in AM or when bending over.
• Nonproductive cough
• Hoarseness, occasionally dysphagia
• Cyanosis of upper torso
• Nasal stuffiness and head fullness
• Breast swelling
(Vogel, 2016)
Superior Vena Cava Syndrome
• Symptoms of ICP
• Irritiability, altered mental status
• Stridor, signs of CHF
• Tachcardia, tachypnea, orthopnea
Late Clinical Presentation:
• Hypotension, no peripheral pulses
• Dysphagia,
hoarseness, hemoptysis
• Progressive cyanosis, facial edema
• Horner syndrome
(Vogel, 2016)
Superior Vena Cava Syndrome
SVC Case Study
• Mr. A is a 67 yo male referred to pulmonologist after a right upper lobe lung
mass was found on X-ray.
• After bronchoscopy with biopsy, he was diagnosed with stage 3 small cell lung
cancer, and sent to an oncologist.
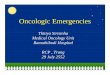
SVC Case Study At his first oncologist visit, he c/o SOB when bending over, dizziness and head pain.
Review of systems and physical exam:
• AM neck swelling
• Hoarseness
• Purple discoloration to check and neck
• Dyspnea
• Difficulty swallowing
• Dry cough • Engorged chest veins and under tongue
• Left arm/hand edema
3/6/2018
18
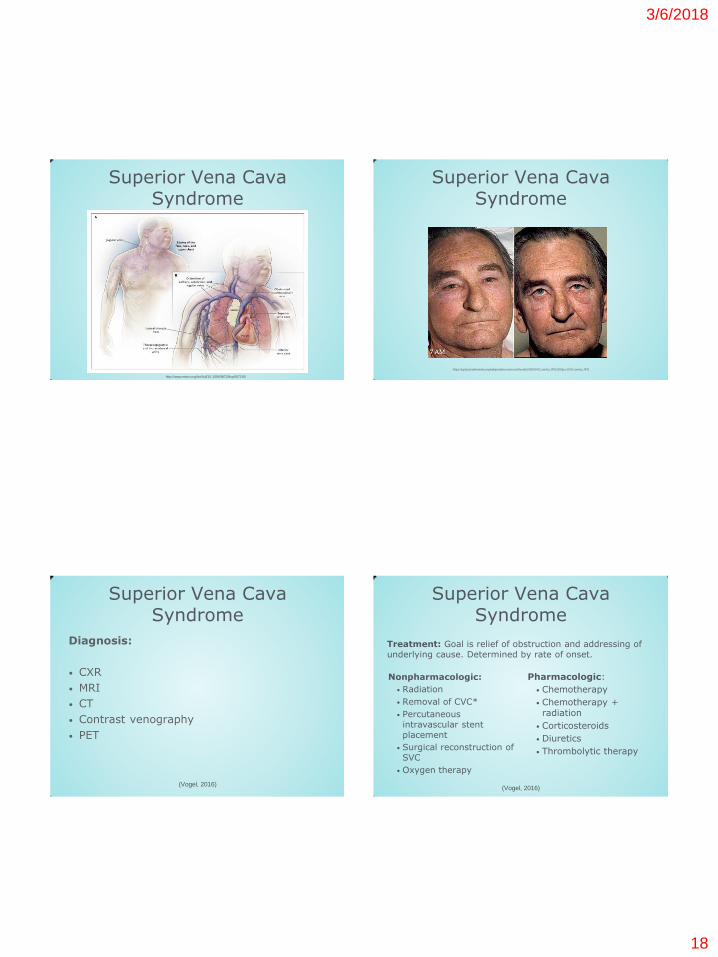
Superior Vena Cava Syndrome
http://www.nejm.org/doi/full/10.1056/NEJMcp067190
Superior Vena Cava Syndrome
https://upload.wikimedia.org/wikipedia/commons/thumb/2/28/SVCcombo.JPG/300px-SVCcombo.JPG
Diagnosis:
• CXR
• MRI
• CT
• Contrast venography
• PET
(Vogel, 2016)
Superior Vena Cava Syndrome
Nonpharmacologic:
• Radiation
• Removal of CVC*
• Percutaneous intravascular stent placement
• Surgical reconstruction of SVC
• Oxygen therapy
Treatment: Goal is relief of obstruction and addressing of underlying cause. Determined by rate of onset.
Pharmacologic:
• Chemotherapy
• Chemotherapy + radiation
• Corticosteroids
• Diuretics
• Thrombolytic therapy
(Vogel, 2016)
Superior Vena Cava Syndrome
3/6/2018
19
SVC Case Study
Mr. A started chemotherapy immediately.
Additional orders included:
• VS Q_hours
• Maintain O2 saturation > __%
• Elevate head of bed
• Scheduled lasix and methylprednisolone
He responded quickly and was able to breath
easily when he was eventually discharged home.
Nursing Management:
(Vogel, 2016)
Superior Vena Cava Syndrome
• Maintain adequate gas exchange • Maintain adequate cardiac output
• Decrease anxiety • Increase knowledge of disease process and
therapeutic interventions
• Prevent injury • Administer treatment as ordered
Clinical Pearls Know your patient! Know the risk factors! Know how to complete a good physical assessment! Early recognition may save a life!
References Brashers, V. L. (2014). Alterations in Cardiovascular Function. In K. L. McCance & S. E. Huether (Authors) & V. L.
Brashers & N. S. Rote (Eds.), Pathophysiology: The Biologic Basis for Disease in Adults and Children (7th ed., pp. 1129-1193). St. Louis, MO: Elsevier.
Camp-Sorrell, D. (2008). Cardiac Tamponade. In R. A. Gates (Author) & R. M. Fink (Ed.), Oncology Nursing Secrets (3rd ed., Nursing Secrets Series, pp. 513-517). St. Louis, MO: Mosby Elsevier.
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies: A resource for nurses. (2nd ed., pp. 433-459). Pittsburgh, PA. Oncology Nursing Society.
Jensen, G. (2008). Hypercalcemia of Malignancy (HCM). In R. A. Gates (Author) & R. M. Fink (Ed.), Oncology Nursing Secrets (3rd ed., Nursing Secrets Series, pp. 523-527). St. Louis, MO: Mosby Elsevier.
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic emergencies: A resource for nurses. (2nd ed., pp. 337-383). Pittsburgh, PA. Oncology Nursing Society.
Mack, K. C., & Becker, C. (2008). Superior Vena Cava Syndrome. In R. A. Gates (Author) & R. M. Fink (Ed.), Oncology Nursing Secrets (3rd ed., Nursing Secrets Series, pp. 551-556). St. Louis, MO: Mosby Elsevier.
Maloney, K. W. (2016). Metabolic Emergencies (J. M. Brant, F. A. Conde, & M. G. Saria, Eds.). In J. K. Itano (Ed.), Core Curriculum for Oncology Nursing (5th ed., pp. 478-494). St. Louis, MO: Elsevier.
National Comprehensive Cancer Network (2016). Non-Hodgkin’s Lymphomas, Version 3.2016. Retrieved from https://www.nccn.org/professionals/physician_gls/pdf/nhl.pdf
Sanofi-Aventis US (2016). Elitek Package Insert. Retrieved from http://products.sanofi.us/elitek/elitek.html#section-4.1
Schulmeister, L., & Gatlin, C. G. (2008). Spinal Cord Compression. In R. A. Gates (Author) & R. M. Fink (Ed.), Oncology Nursing Secrets (3rd ed., Nursing Secrets Series, pp. 546-550). St. Louis, MO: Mosby Elsevier.
Viele, C. S. (2008). Disseminated Intravascular Coagulation (DIC). In R. A. Gates (Author) & R. M. Fink (Ed.), Oncology Nursing Secrets (3rd ed., Nursing Secrets Series, pp. 518-522). St. Louis, MO: Mosby Elsevier.
Vogel, W. H. (2016). Structural Emergencies (J. M. Brant, F. A. Conde, & M. G. Saria, Eds.). In J. K. Itano (Ed.), Core Curriculum for Oncology Nursing (5th ed., pp. 495-508). St. Louis, MO: Elsevier.
Zobec, A. (2008). Tumor Lysis Syndrome (TLS). In R. A. Gates (Author) & R. M. Fink (Ed.), Oncology Nursing Secrets (3rd ed., Nursing Secrets Series, pp. 557-560). St. Louis, MO: Mosby Elsevier.