Embed Size (px)
Citation preview
Ontario’s Maternity Care Expert Panel Recommendations and Next Steps
Best Start Annual ConferenceJanuary 17, 2006
For Discussion Only
2
Background
• Created by the Ontario Women’s Health Council in October 2004 to address concerns about the quality and sustainability of maternity care in Ontario.
• Multi-disciplinary 15-member panel of professionals and a consumer
• Report to identify the status of maternity care in the various regions across the province and to provide recommendations for access and accountability in maternity care.
3
OMCEP Vision and Scope
OMCEP Vision
Every woman in Ontario has access to high quality, woman and family-centred maternity care as close to home as possible.
Scope
The panel is developing recommendations for a coordinated province-wide system of essential maternity-care services.
Continuum of Maternity Care
Maternity care begins with pre-conception counseling, continues with prenatal, labour and birth care, and concludes with services to mother and newborn until approximately 6-weeks/2-months after birth.
4
OMCEP Research
Hospital Demographics Survey – 109 Hospitals in Ontario that provide or recently ceased providing maternity care
• Literature Reviews and Environmental Scans:• Women’s Input into Maternity Care
• Human Resources Planning
• Models of Maternity Care
• Legislation/Regulation of Maternity Care
• Remuneration and Funding Schemes
• Liability Insurance
• Data and Evaluation Systems
• Focus Groups – consumer, provider, hospital staff, shared research findings
• Stakeholder Input
5OMCEP Interim RecommendationsGuiding Principles
• Pregnancy and Birth as a Normal Physiological Process • Equitable Access/Close to Home • Co-ordinated Access to High-risk Care, when needed • Woman and Family Centred Care - Empowerment and Participation• Informed Choice• Choice of Birthplace• Care Across the Continuum of Maternity and Newborn Care• Valuing Maternity Care Providers• Continuity of Care• Collaboration – inter-professional, respectful and seamless• Quality Care including to Diverse Populations• Effective Coordination of Services• Provider Preparation, Competence and Confidence• Continuous Evaluation and Improvement• Maternity Care as Essential Component of Primary Care • Alignment of System with Nat. and Internat. Determinants of Health• Financial Responsibility and Accountability

6
Collaboration
Care and services across the maternity care continuum are, by their very nature, collaborative. Quality care depends upon:
• Sequential and concurrent communication and participation • across continuum
• low to high-risk care
• Multiple provider groups, learners and others
• Integrated services by transport, laboratory, imaging and pharmacy
• Institutional and community agency services and support by hospital staff, public health, child welfare, educators, lactation, others
• Emerging IT initiatives – telecare and consultation, info systems
• Services delivered within models that are considered ‘uni-professional’ and ‘inter-professional’ (most responsible person, MRP)
• Supported by coordinated, integrated funding, regulatory and insurance schemes at the ministry/provincial level
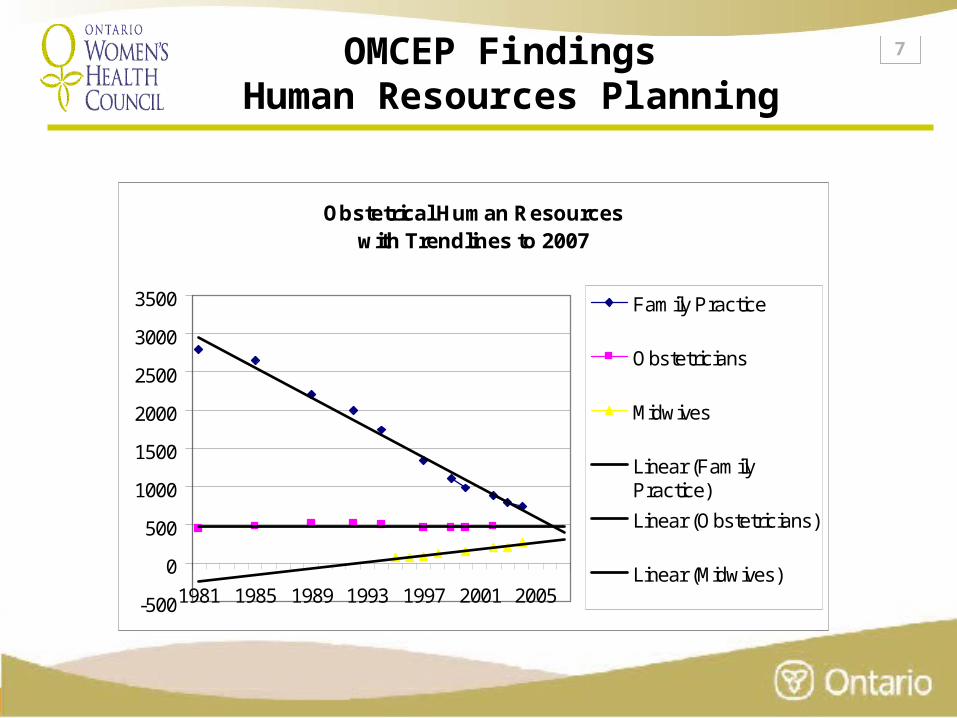
7OMCEP Findings Human Resources Planning
Obstetrical Human Resourceswith Trendlines to 2007
-500
0
500
1000
1500
2000
2500
3000
3500
1981 1985 1989 1993 1997 2001 2005
Family Practice
Obstetricians
Midwives
Linear (FamilyPractice)
Linear (Obstetricians)
Linear (Midwives)
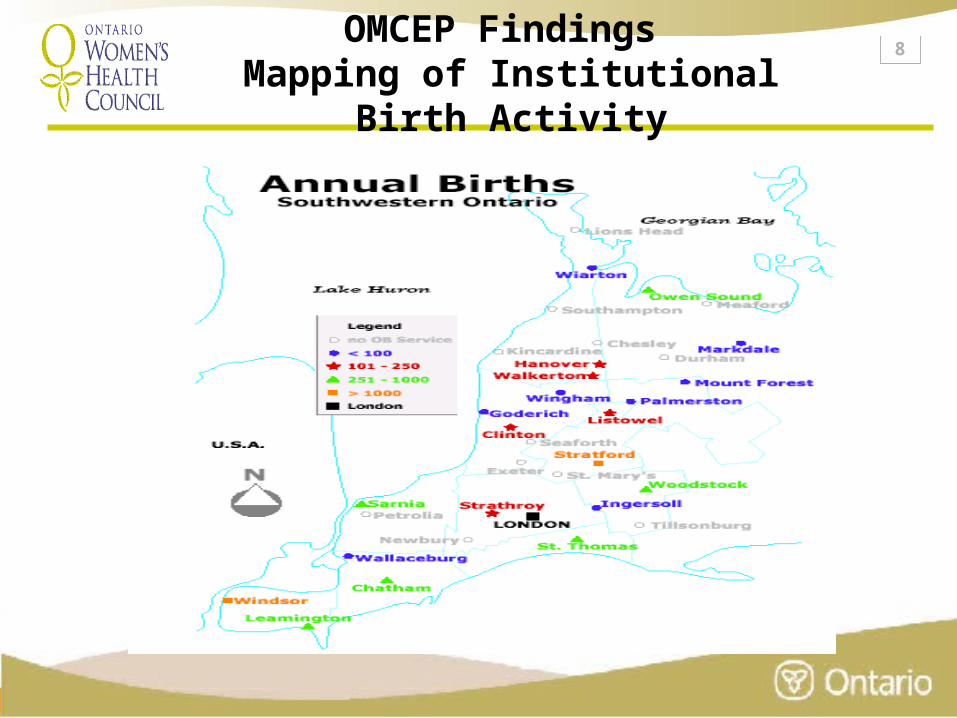
8OMCEP Findings Mapping of Institutional Birth Activity
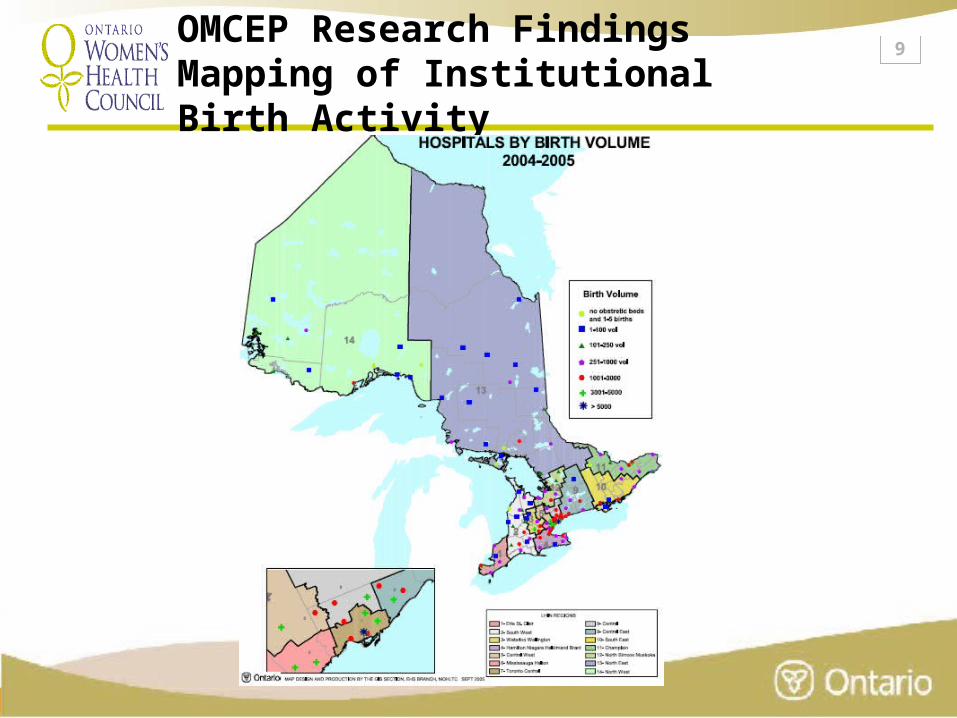
9OMCEP Research Findings Mapping of Institutional Birth Activity
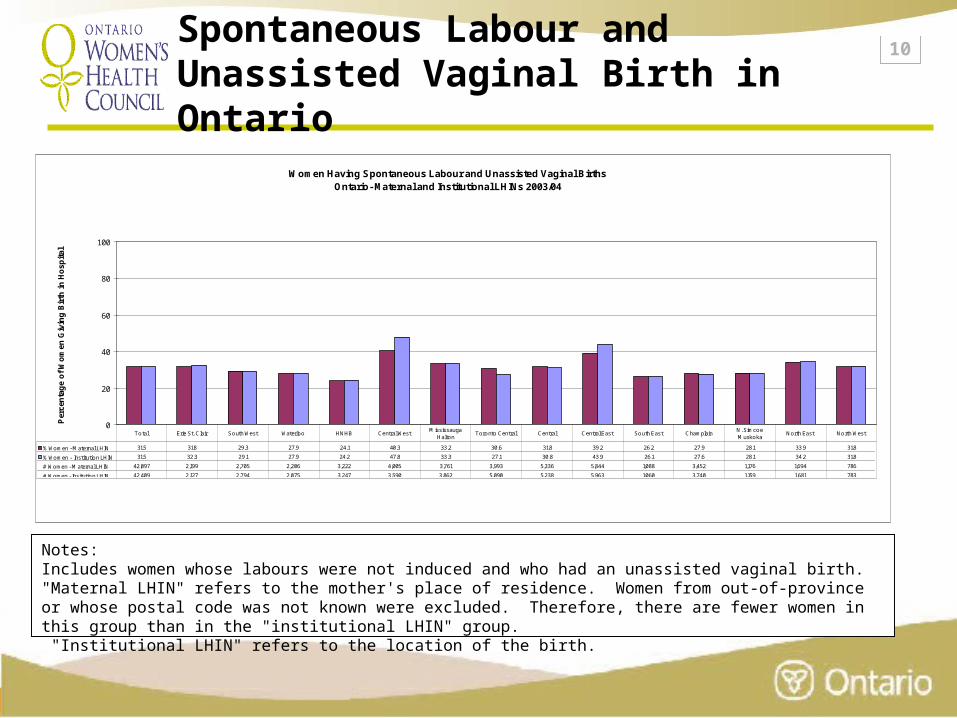
10Spontaneous Labour and Unassisted Vaginal Birth in Ontario
Women Having Spontaneous Labour and Unassisted Vaginal BirthsOntario- Maternal and Institutional LHINs 2003/04
0
20
40
60
80
100
Per
cen
tag
e o
f W
om
en G
ivin
g B
irth
in
Ho
spit
al
% Women - Maternal LHIN 31.5 31.8 29.3 27.9 24.1 40.3 33.2 30.6 31.8 39.2 26.2 27.9 28.1 33.9 31.8
% Women - Institution LHIN 31.5 32.3 29.1 27.9 24.2 47.8 33.3 27.1 30.8 43.9 26.1 27.6 28.1 34.2 31.8
# Women - Maternal LHIN 42,097 2,199 2,705 2,206 3,222 4,005 3,761 3,993 5,336 5,844 1,088 3,452 1,176 1,694 786
# Women - Insitution LHIN 42,409 2,127 2,794 2,075 3,247 3,590 3,862 5,090 5,238 5,963 1,060 3,740 1,159 1,681 783
Total Erie St. Clair South West Waterloo HNHB Central WestMississauga
HaltonToronto Central Central Central East South East Champlain
N. Simcoe Muskoka
North East North West
Notes:Includes women whose labours were not induced and who had an unassisted vaginal birth."Maternal LHIN" refers to the mother's place of residence. Women from out-of-province or whose postal code was not known were excluded. Therefore, there are fewer women in this group than in the "institutional LHIN" group. "Institutional LHIN" refers to the location of the birth.
11
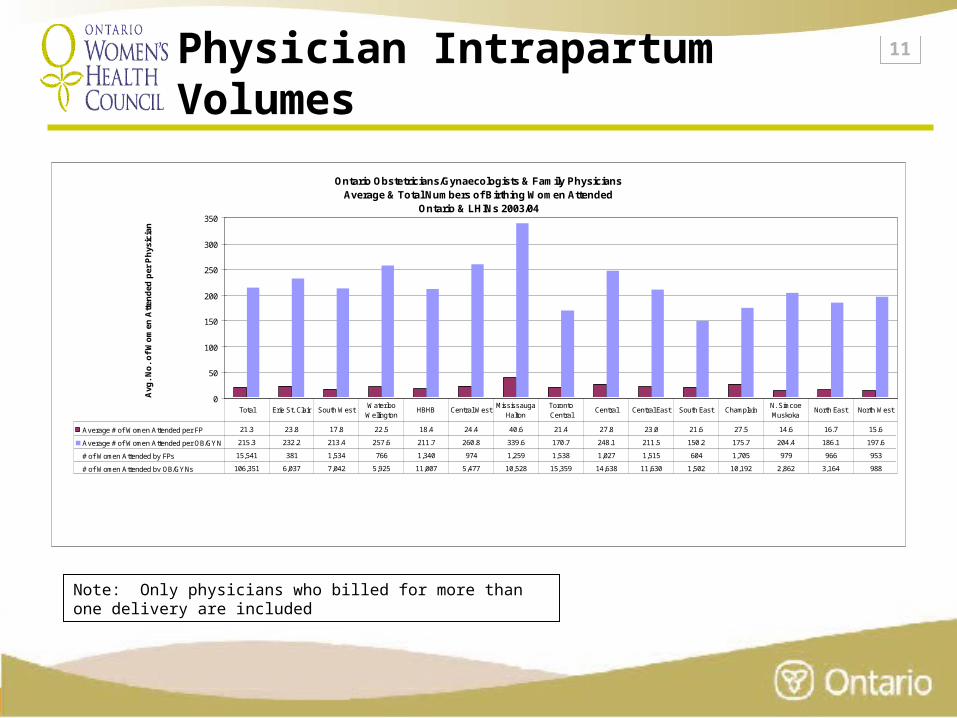
Physician Intrapartum Volumes
Ontario Obstetricians/Gynaecologists & Family Physicians Average & Total Numbers of Birthing Women Attended
Ontario & LHINs 2003/04
0
50
100
150
200
250
300
350
Avg
. N
o.
of
Wo
men
Att
end
ed p
er P
hys
icia
n
Average # of Women Attended per FP 21.3 23.8 17.8 22.5 18.4 24.4 40.6 21.4 27.8 23.0 21.6 27.5 14.6 16.7 15.6
Average # of Women Attended per OB/GYN 215.3 232.2 213.4 257.6 211.7 260.8 339.6 170.7 248.1 211.5 150.2 175.7 204.4 186.1 197.6
# of Women Attended by FPs 15,541 381 1,534 766 1,340 974 1,259 1,538 1,027 1,515 604 1,705 979 966 953
# of Women Attended by OB/GYNs 106,351 6,037 7,042 5,925 11,007 5,477 10,528 15,359 14,638 11,630 1,502 10,192 2,862 3,164 988
Total Erie St. Clair South WestWaterloo Wellington
HBHB Central WestMississauga
HaltonToronto Central
Central Central East South East ChamplainN. Simcoe Muskoka
North East North West
Note: Only physicians who billed for more than one delivery are included
12Services to Diverse PopulationsBarriers
•Rural and Remote – • Human resources shortages
• Some hospitals at risk of closure, maternity care programs under pressure
• Access issues pervasive
• Reduced services – primary health care and primary maternity care, paediatrics, anaesthesia, well woman and newborn care
• Evacuation and associated risks
13Services to Diverse PopulationsBarriers – cont’d
•Aboriginal• Above plus disconnected services between Aboriginal
and non-Aboriginal programs, federal and provincial Aboriginal programs
• Urban Aboriginal populations
•Diverse populations• Interpretation
• Antenatal, sexual and public health education
• Socio-economic disadvantage
• Transportation
14
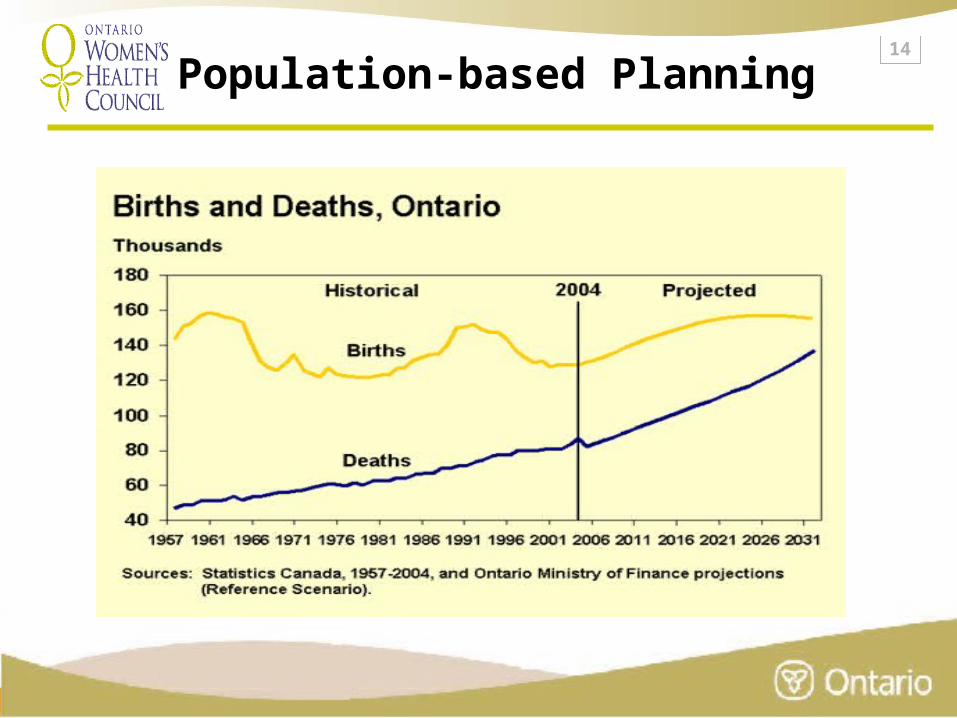
Population-based Planning
15
Population-based Planning cont’d
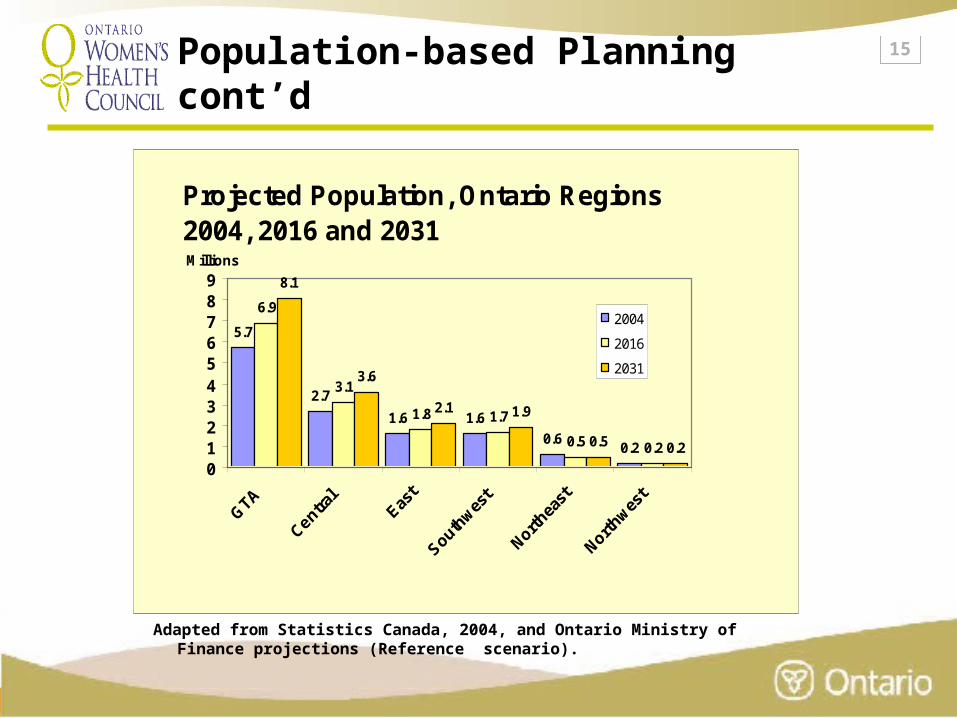
Projected Population, Ontario Regions 2004, 2016 and 2031
5.7
2.7
1.6 1.6
0.60.2
6.9
3.1
1.8 1.7
0.5 0.2
8.1
3.6
2.1 1.9
0.5 0.2
0123456789
Millions
2004
2016
2031
Adapted from Statistics Canada, 2004, and Ontario Ministry of Finance projections (Reference scenario).
16OMCEP Interim RecommendationsHuman Resources Planning
• to monitor and anticipate the health needs of Ontarians and make recommendations on the appropriate supply, mix and distribution of health human resources to meet those needs.
• broad education/promotion campaign to promote birth as a normal physiological process for women and timely access to high risk services, when needed
• intrapartum care as a positive career choice for providers
• coordination between provincial maternity care human resources planning and regional/local institutional, community and provider programs across the continuum
17OMCEP Interim Recommendations Education and Training
• Maximize capacity of maternity care provider program entrant class sizes, residency positions and clinical placements for midwifery, family med, nursing and OB
• Maternity care (incl. normal intrapartum) as a core part of curriculum
• Central provider and teaching registry
• Funded continuing education for providers in low-volume communities
• Inter-professional preparatory, post grad and continuing education opportunities
• Inter-professional modeling in clinical education placements
18OMCEP Interim Recommendations Recruitment and Retention
• Incorporate best practice re: retention and recruitment incentives into maternity care system
• Value maternity care providers - social, professional and compensation
• Under-serviced area support and recruitment
• Support confidence and competence through evidence-based continuing education, especially in low-volume situations
• Incorporate discourses and research on understanding risk and risk tolerance/management into provincial strategy to reduce provider stress
19OMCEP Interim Recommendations Models of Maternity Care
• Models are evolving in communities in response to access to care issues
• Model’S’- We confirmed that one model does not fit all Ontario situations
• Local model solutions, as identified by communities, are needed• Approximately 8 existing models of maternity care currently being
delivered in Ontario – current barriers present to using providers to full extent of scope
• An additional 15 models surveyed from existing proposals and other provinces will be recommended in ‘menu’-style inventory
• Inter-professional models are seen as positive option (not single solution)
• Model development and implementation to become part of regional maternity care planning (with regions/LHINs)
20OMCEP Interim Recommendations Maternity Care System Structure
• Provincial Coordination and LHINs
• Legislation and Regulation
• Funding
• Risk Management and Liability Insurance
21Maternity Care System StructureProvincial Coordination and LHINs
OMCEP’s premise:
Ontario must establish and maintain a coordinated Ministry-mandated provincial plan for maternity care to provide the foundation for a sustainable system. The proposed system will be monitored and coordinated at the provincial level and be dynamically adaptable to the needs of local communities in consultation with Local Health Integration Networks, local/regional stakeholders and service recipients.
22Maternity Care System StructureProvincial Coordination and LHINs
• Provincial unit, Maternity Care Ontario• Supported by steering committee and 6-region structure
with complementary permeable boundaries to LHINs• Boundaries support regional referral patterns and sharing
of resources • Build capacity in all 6 regions to plan for continuum of
maternity and newborn services – maximise complementary contributions by existing Regional Perinatal Programs
• Stakeholder and consumer input across the continuum of programs that contribute to maternity care
23Maternity Care System StructureLegislation and Regulation
• Barriers re: scopes of practice and institutional governance that are interrupting access and decreasing quality
• OMCEP Recos focus on Ministry-mandated omnibus approach to leg/reg maintenance across maternity care sector
• Increased scope (in selected authorized acts) for midwives and nurses in remote areas
24Maternity Care System StructureFunding and Remuneration
• Total sector expenditures over $1B
• No provincial envelope, standard reporting or accountability for maternity services sector, most expenditures blended into larger budgets
• Barriers re: disconnected funding schemes for FFS, Alternate payment, Midwifery, Nurse Practitioners, Hospitals
• Lack of equity between providers, groups and programs resulting in decrease in quality, access and provincial uptake of services
• OMCEP Recos focus on improved accountability, equity, coordination and efficiency through planning
• Maternity Care Ontario would coordinate funding streams in Ministry and work with LHINs to improve accountability at regional/local levels
25Maternity Care System StructureRisk Management and Liability Insurance
• Current expenditures on provider liability insurance over $60M (reimbursements for obstetricians, family physicians and midwives only)
• Competition between insurers and risk averse practice (vs. EBP) driving care and recruitment and retention pressures
• OMCEP recommendations focus on risk tolerance/management strategy at provincial level in coordination with regional maternity care plans
26
Women’s Input/Access to Care
•OMCEP approach is to recommend women’s input at all levels of maternity care system
• Provincial, regional, community, institutional and provider levels
•Maternity Experience Survey – to be developed
•LHIN linkages with women’s organizations
27
Data and Evaluation
• OMCEP Logic Model
• Survey of Maternity Care Indicators
• Linking of Niday with Midwifery Data providing province’s first complete set of perinatal data
• Evaluation Plan to continue to bridge data sources for ongoing monitoring:
• Ontario Hospital Reports Collaborative
• Hospital Costing
• Public Health
• Women’s Experience of Maternity Care
• Management Information System to support Maternity Care Ontario
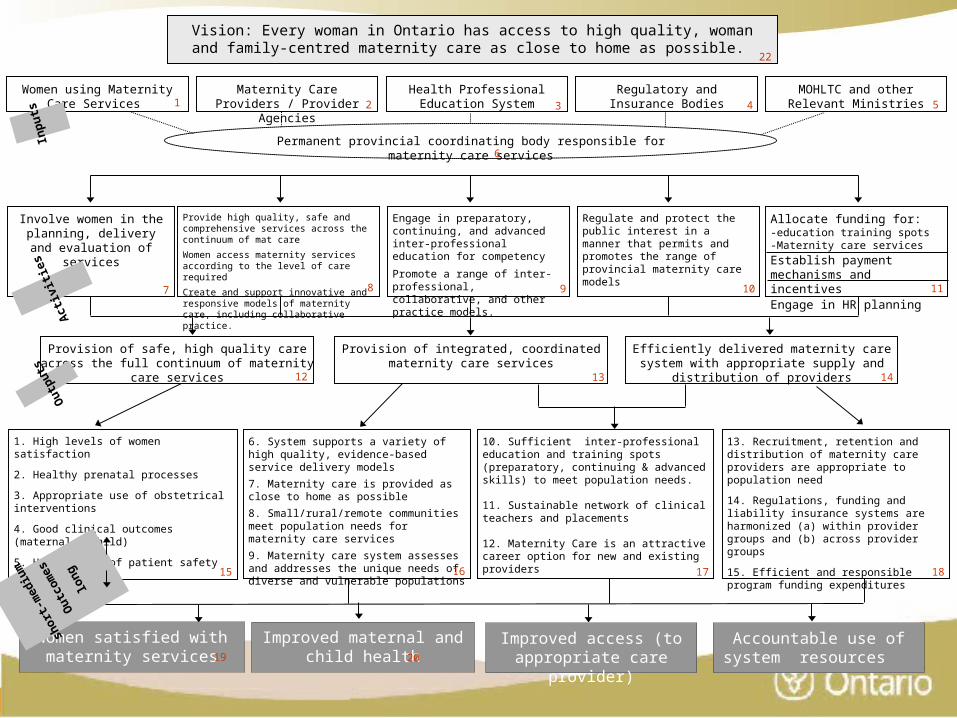
Vision: Every woman in Ontario has access to high quality, woman and family-centred maternity care as close to home as possible.
Maternity Care Providers / Provider Agencies
Regulatory and Insurance Bodies
Health Professional Education System
Involve women in the planning, delivery and evaluation of services
1. High levels of women satisfaction
2. Healthy prenatal processes
3. Appropriate use of obstetrical interventions
4. Good clinical outcomes (maternal & child)
5. High levels of patient safety
Provide high quality, safe and comprehensive services across the continuum of mat care
Women access maternity services according to the level of care required
Create and support innovative and responsive models of maternity care, including collaborative practice.
Engage in preparatory, continuing, and advanced inter-professional education for competency
Promote a range of inter-professional, collaborative, and other practice models.
Regulate and protect the public interest in a manner that permits and promotes the range of provincial maternity care models
Permanent provincial coordinating body responsible for maternity care services
MOHLTC and other Relevant Ministries
Women using Maternity Care Services
Provision of safe, high quality care across the full continuum of maternity care services
Provision of integrated, coordinated maternity care services
Efficiently delivered maternity care system with appropriate supply and distribution of providers
Allocate funding for:-education training spots-Maternity care services
Establish payment mechanisms and incentivesEngage in HR planning
Out
puts
Improved maternal and child health
6. System supports a variety of high quality, evidence-based service delivery models
7. Maternity care is provided as close to home as possible
8. Small/rural/remote communities meet population needs for maternity care services
9. Maternity care system assesses and addresses the unique needs of diverse and vulnerable populations
10. Sufficient inter-professional education and training spots (preparatory, continuing & advanced skills) to meet population needs.
11. Sustainable network of clinical teachers and placements
12. Maternity Care is an attractive career option for new and existing providers
13. Recruitment, retention and distribution of maternity care providers are appropriate to population need
14. Regulations, funding and liability insurance systems are harmonized (a) within provider groups and (b) across provider groups
15. Efficient and responsible program funding expenditures
Women satisfied with maternity services
Improved access (to appropriate care provider)
Inp
uts
Act
ivit
ies
shor
t-m
ediu
m
Out
com
es
long
1 2 543
6
7 8 9 10 11
12 13 14
18171615
19 2021
22
Accountable use of system resources
29
Next Steps
• Stakeholder outreach and consultation
• Ministry briefing
• Finalize Draft Report
• Presentation of Final Report to OWHC





























