Embed Size (px)
Citation preview

CroniconO P E N A C C E S S EC PAEDIATRICS
Case Report
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Dimitrios Panagopoulos*Neurosurgical Department, University Hospital of Alexandroupoli, Medical School, Greece
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
*Corresponding Author: Dimitrios Panagopoulos, Assistant Professor, Neurosurgical Department, University Hospital of Alexandrou-poli, Medical School, Greece.
Received: March 12, 2018; Published: March 27, 2018
AbstractBackground: Despite major advances in antimicrobial therapy, imaging technology and neurosurgical techniques, brain abscesses are an ongoing treatment issue. Although mortality has declined in the past decades, long-term sequelae occur in about one-third of patients and include mental retardation, seizures and focal neurologic deficits. Our objective is to illustrate two cases with unusual clinical and imaging characteristics, as their treatment was challenging, because of them.
Case Presentation: We present the case of an 11 year old boy, who suffered at least three pyogenic abscesses of the posterior fossa with resultant ongoing obstructive hydrocephalus, in the field of a previous purulent otitis media. Also, we report the case of an 11 year old girl, who suffered from concomitant maxillary, frontal and ethmoid sinusitis, and frontal lobe abscess with concomitant pus extension into the soft tissues of the forehead and erosion of the frontal bone. Both patients were operated on, treated completely and were discharged without any neurological sequelae.
Conclusions: Despite these cases were fulfilling a lot of criteria mandating a dismal prognosis, as delayed clinical presentation with hydrocephalus, the ultimate functional and neurosurgical outcome was excellent, with complete removal of the abscesses. The clini-cal, imaging and surgical details of both cases as well as a brief review of the literature follow.
Keywords: Multiple Abscesses; Obstructive Hydrocephalus; Delayed Presentation
Introduction Brain abscess is a focal suppurative process of the brain parenchyma. The most frequent intracranial locations of brain abscesses are:
frontal, temporal, frontal-parietal, partial, cerebellar, and occipital lobes. The diagnosis and management of have changed over the past decades because of the availability of noninvasive radiographic diagnostic techniques, antimicrobials that penetrate the blood–brain barrier and into abscesses, and minimally invasive surgical procedures. Successful treatment of a brain abscess requires a high index of suspicion, and often a combination of drainage and antimicrobial therapy.
351
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
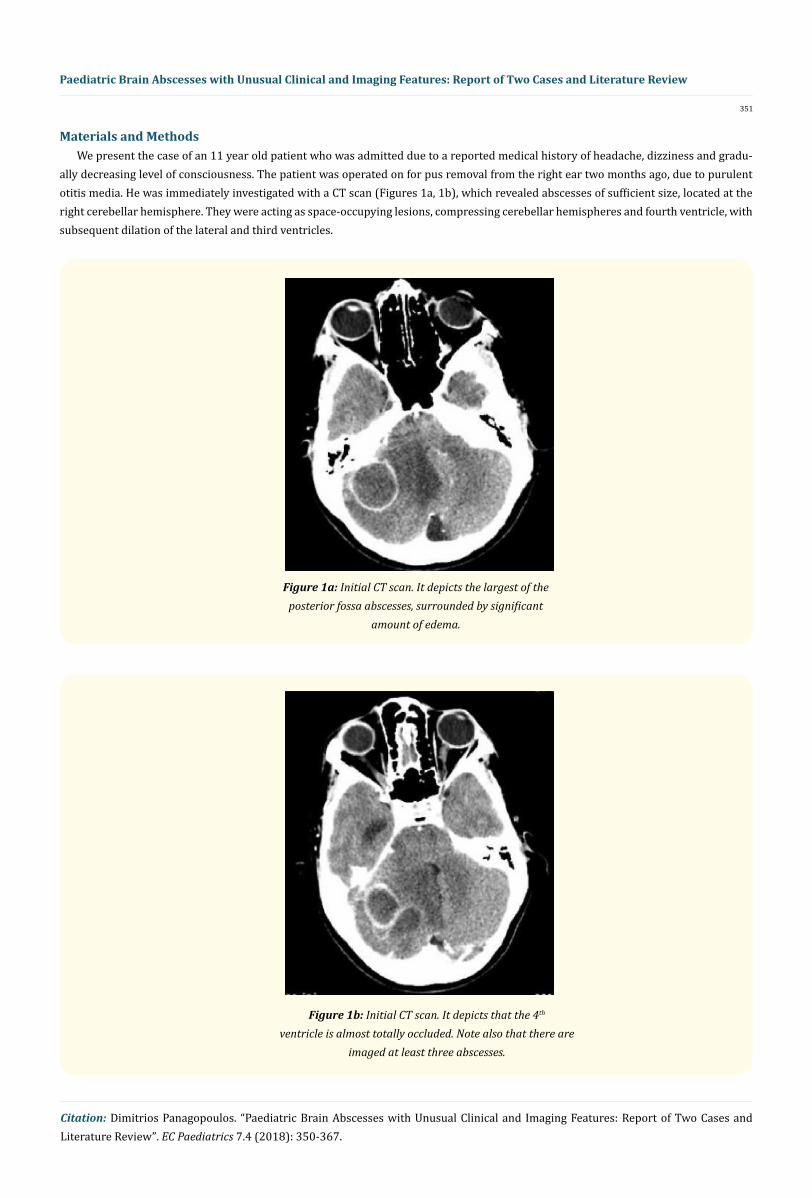
Materials and MethodsWe present the case of an 11 year old patient who was admitted due to a reported medical history of headache, dizziness and gradu-
ally decreasing level of consciousness. The patient was operated on for pus removal from the right ear two months ago, due to purulent otitis media. He was immediately investigated with a CT scan (Figures 1a, 1b), which revealed abscesses of sufficient size, located at the right cerebellar hemisphere. They were acting as space-occupying lesions, compressing cerebellar hemispheres and fourth ventricle, with subsequent dilation of the lateral and third ventricles.
Figure 1a: Initial CT scan. It depicts the largest of the posterior fossa abscesses, surrounded by significant
amount of edema.
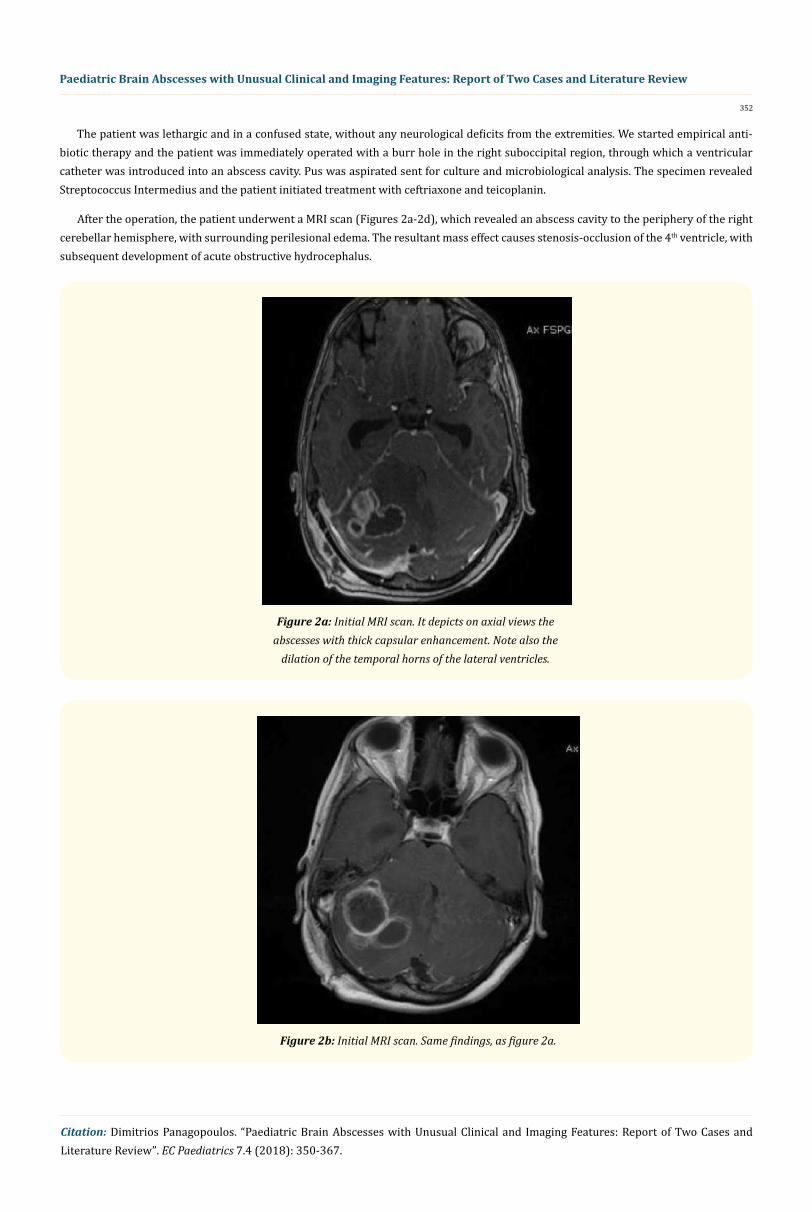
Figure 1b: Initial CT scan. It depicts that the 4th ventricle is almost totally occluded. Note also that there are
imaged at least three abscesses.
352
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
The patient was lethargic and in a confused state, without any neurological deficits from the extremities. We started empirical anti-biotic therapy and the patient was immediately operated with a burr hole in the right suboccipital region, through which a ventricular catheter was introduced into an abscess cavity. Pus was aspirated sent for culture and microbiological analysis. The specimen revealed Streptococcus Intermedius and the patient initiated treatment with ceftriaxone and teicoplanin.
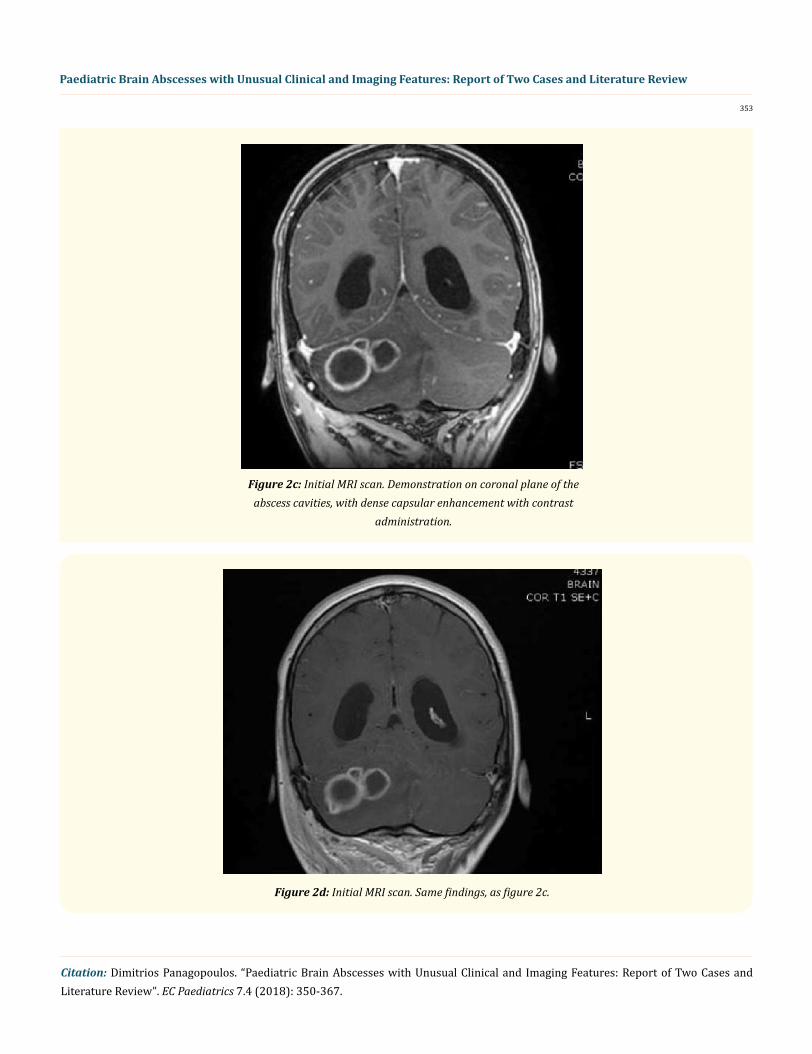
After the operation, the patient underwent a MRI scan (Figures 2a-2d), which revealed an abscess cavity to the periphery of the right cerebellar hemisphere, with surrounding perilesional edema. The resultant mass effect causes stenosis-occlusion of the 4th ventricle, with subsequent development of acute obstructive hydrocephalus.
Figure 2a: Initial MRI scan. It depicts on axial views the abscesses with thick capsular enhancement. Note also the
dilation of the temporal horns of the lateral ventricles.
Figure 2a: Initial MRI scan. It depicts on axial views the abscesses with thick capsular enhancement. Note also the
dilation of the temporal horns of the lateral ventricles.
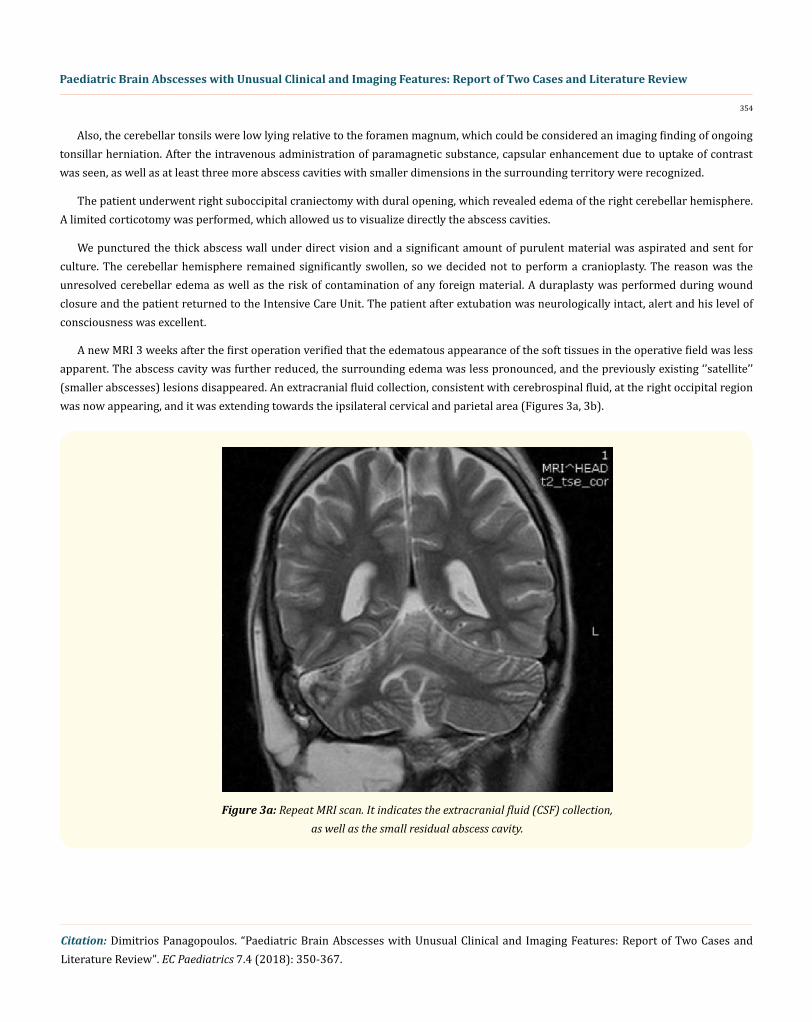
Figure 2b: Initial MRI scan. Same findings, as figure 2a.
353
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Figure 2c: Initial MRI scan. Demonstration on coronal plane of the abscess cavities, with dense capsular enhancement with contrast
administration.
Figure 2d: Initial MRI scan. Same findings, as figure 2c.
354
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Also, the cerebellar tonsils were low lying relative to the foramen magnum, which could be considered an imaging finding of ongoing tonsillar herniation. After the intravenous administration of paramagnetic substance, capsular enhancement due to uptake of contrast was seen, as well as at least three more abscess cavities with smaller dimensions in the surrounding territory were recognized.
The patient underwent right suboccipital craniectomy with dural opening, which revealed edema of the right cerebellar hemisphere. A limited corticotomy was performed, which allowed us to visualize directly the abscess cavities.
We punctured the thick abscess wall under direct vision and a significant amount of purulent material was aspirated and sent for culture. The cerebellar hemisphere remained significantly swollen, so we decided not to perform a cranioplasty. The reason was the unresolved cerebellar edema as well as the risk of contamination of any foreign material. A duraplasty was performed during wound closure and the patient returned to the Intensive Care Unit. The patient after extubation was neurologically intact, alert and his level of consciousness was excellent.
A new MRI 3 weeks after the first operation verified that the edematous appearance of the soft tissues in the operative field was less apparent. The abscess cavity was further reduced, the surrounding edema was less pronounced, and the previously existing ‘’satellite’’ (smaller abscesses) lesions disappeared. An extracranial fluid collection, consistent with cerebrospinal fluid, at the right occipital region was now appearing, and it was extending towards the ipsilateral cervical and parietal area (Figures 3a, 3b).
Figure 3a: Repeat MRI scan. It indicates the extracranial fluid (CSF) collection, as well as the small residual abscess cavity.
355
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
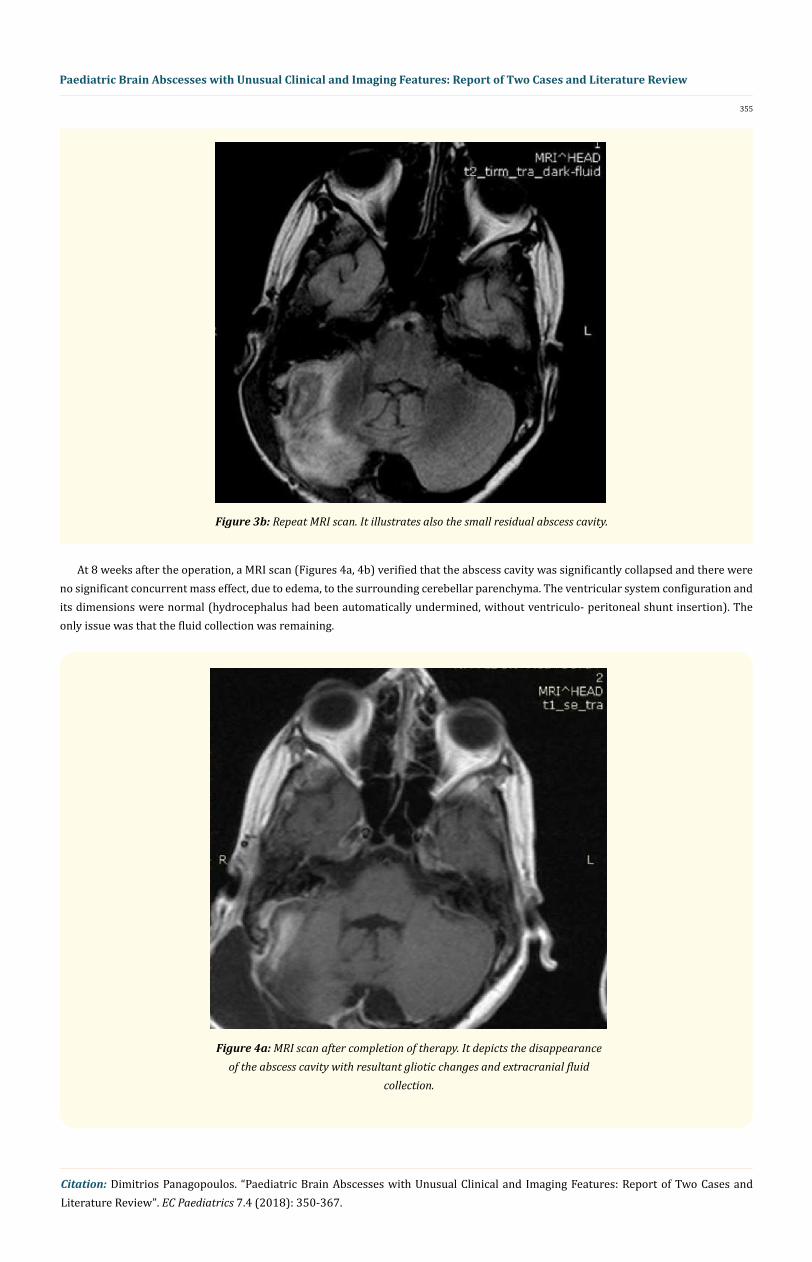
Figure 3b: Repeat MRI scan. It illustrates also the small residual abscess cavity.
At 8 weeks after the operation, a MRI scan (Figures 4a, 4b) verified that the abscess cavity was significantly collapsed and there were no significant concurrent mass effect, due to edema, to the surrounding cerebellar parenchyma. The ventricular system configuration and its dimensions were normal (hydrocephalus had been automatically undermined, without ventriculo- peritoneal shunt insertion). The only issue was that the fluid collection was remaining.
Figure 4a: MRI scan after completion of therapy. It depicts the disappearance of the abscess cavity with resultant gliotic changes and extracranial fluid
collection.
356
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
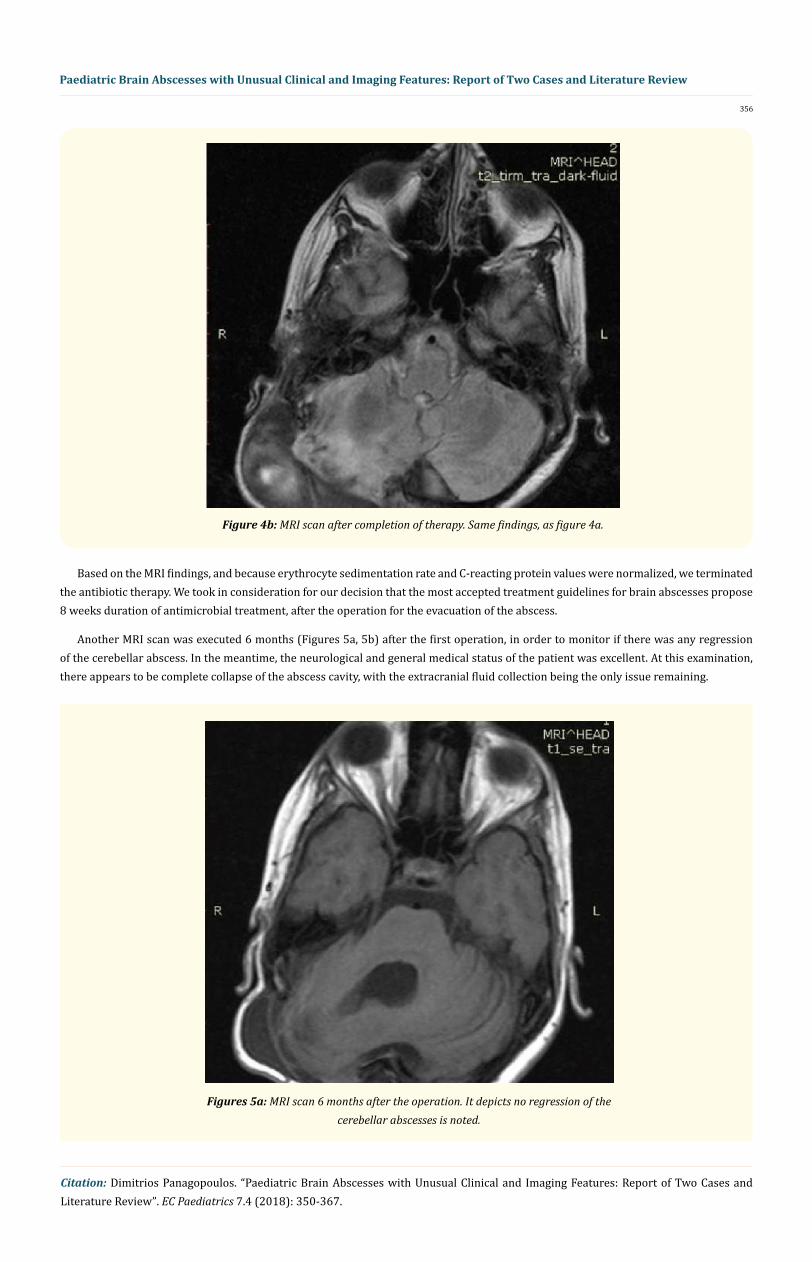
Figure 4b: MRI scan after completion of therapy. Same findings, as figure 4a.
Based on the MRI findings, and because erythrocyte sedimentation rate and C-reacting protein values were normalized, we terminated the antibiotic therapy. We took in consideration for our decision that the most accepted treatment guidelines for brain abscesses propose 8 weeks duration of antimicrobial treatment, after the operation for the evacuation of the abscess.
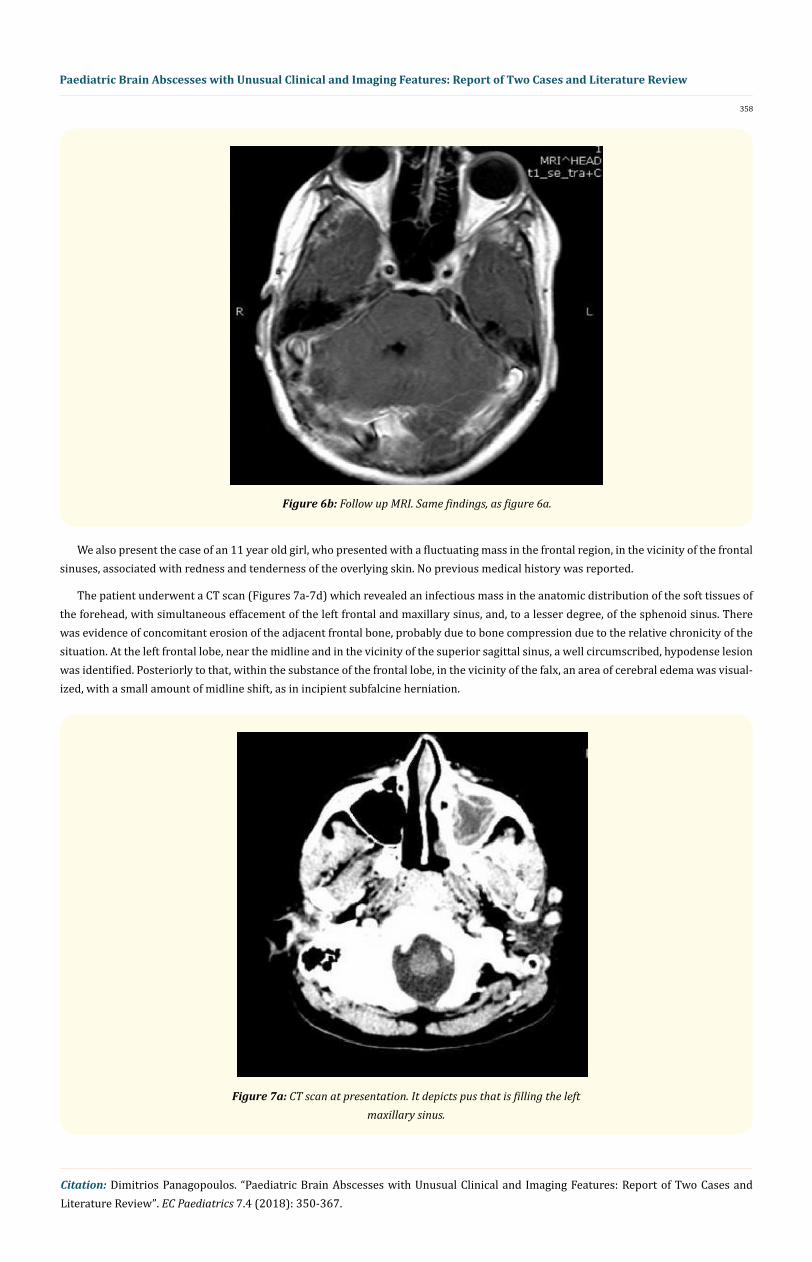
Another MRI scan was executed 6 months (Figures 5a, 5b) after the first operation, in order to monitor if there was any regression of the cerebellar abscess. In the meantime, the neurological and general medical status of the patient was excellent. At this examination, there appears to be complete collapse of the abscess cavity, with the extracranial fluid collection being the only issue remaining.
Figures 5a: MRI scan 6 months after the operation. It depicts no regression of the cerebellar abscesses is noted.

357
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Figure 5b: MRI scan 6 months after the operation. Same findings, as figure 5a.
Approximately 7 months after the initial operation of abscess excision, a revision duraplasty was performed and the extracranial fluid collection was evacuated. Simultaneously, a cranioplasty was executed, with an implant of polymethylmethacrylate, customized for the specific patient via 3Dimensional CT scan.
A MRI scan one year after the initial operation did not reveal any active residual abscess activity, there was no bony defect and there was no extraparenchymal cerebrospinal fluid collection (Figures 6a, 6b).
Figure 6a: Follow up MRI. Approximately after one year from the first operation and the performance of duraplasty and cranioplasty, no CSF
collection is noted and no signs of abscess recurrence.
358
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Figure 6b: Follow up MRI. Same findings, as figure 6a.
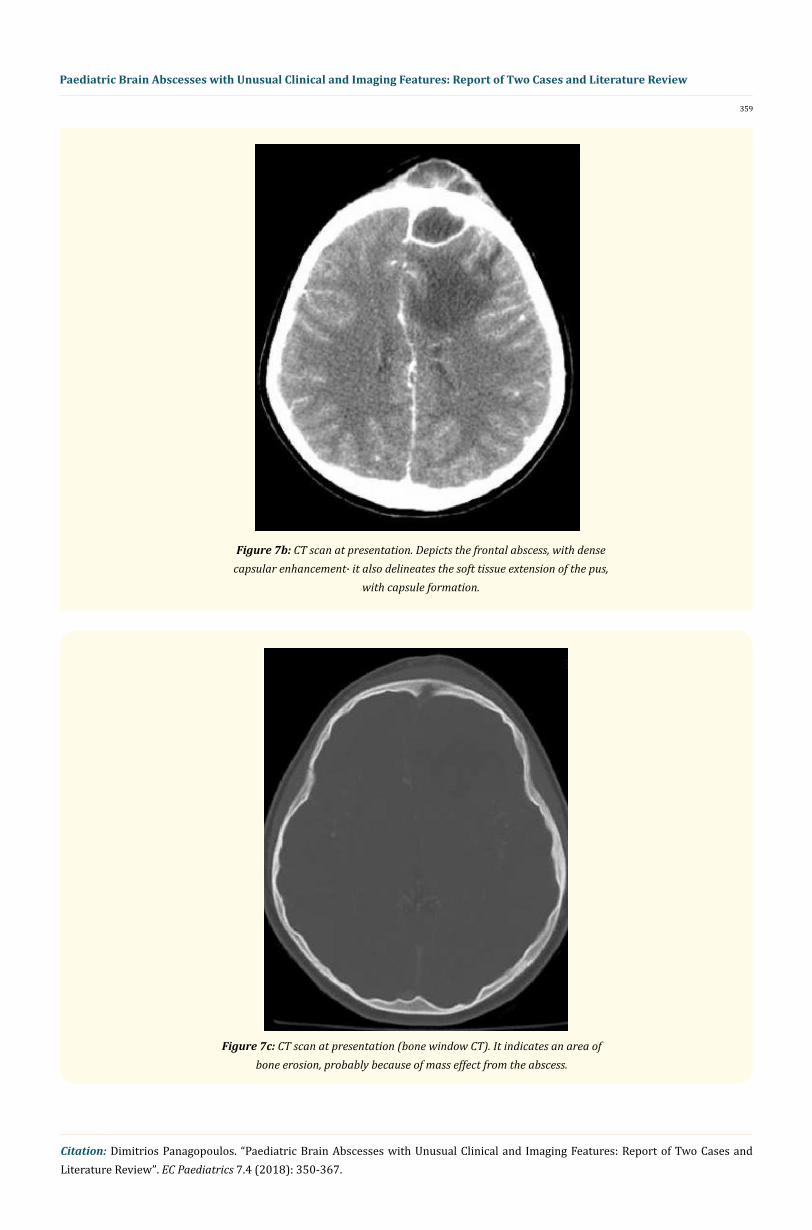
We also present the case of an 11 year old girl, who presented with a fluctuating mass in the frontal region, in the vicinity of the frontal sinuses, associated with redness and tenderness of the overlying skin. No previous medical history was reported.
The patient underwent a CT scan (Figures 7a-7d) which revealed an infectious mass in the anatomic distribution of the soft tissues of the forehead, with simultaneous effacement of the left frontal and maxillary sinus, and, to a lesser degree, of the sphenoid sinus. There was evidence of concomitant erosion of the adjacent frontal bone, probably due to bone compression due to the relative chronicity of the situation. At the left frontal lobe, near the midline and in the vicinity of the superior sagittal sinus, a well circumscribed, hypodense lesion was identified. Posteriorly to that, within the substance of the frontal lobe, in the vicinity of the falx, an area of cerebral edema was visual-ized, with a small amount of midline shift, as in incipient subfalcine herniation.
Figure 7a: CT scan at presentation. It depicts pus that is filling the left maxillary sinus.
359
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Figure 7b: CT scan at presentation. Depicts the frontal abscess, with dense capsular enhancement∙ it also delineates the soft tissue extension of the pus,
with capsule formation.
Figure 7c: CT scan at presentation (bone window CT). It indicates an area of bone erosion, probably because of mass effect from the abscess.

360
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Figure 7d: CT scan at presentation (bone window CT). It delineates the extent of involvement of the ethmoid sinuses.
After the administration of contrast material, the lesion in the frontal lobe appeared a dense peripheral ring contrast enhancement, simulating brain abscess with thick, organized, peripheral capsule. The patient was immediately placed on empirical antimicrobial treat-ment (vancomycin, metronidazole and cefepime).
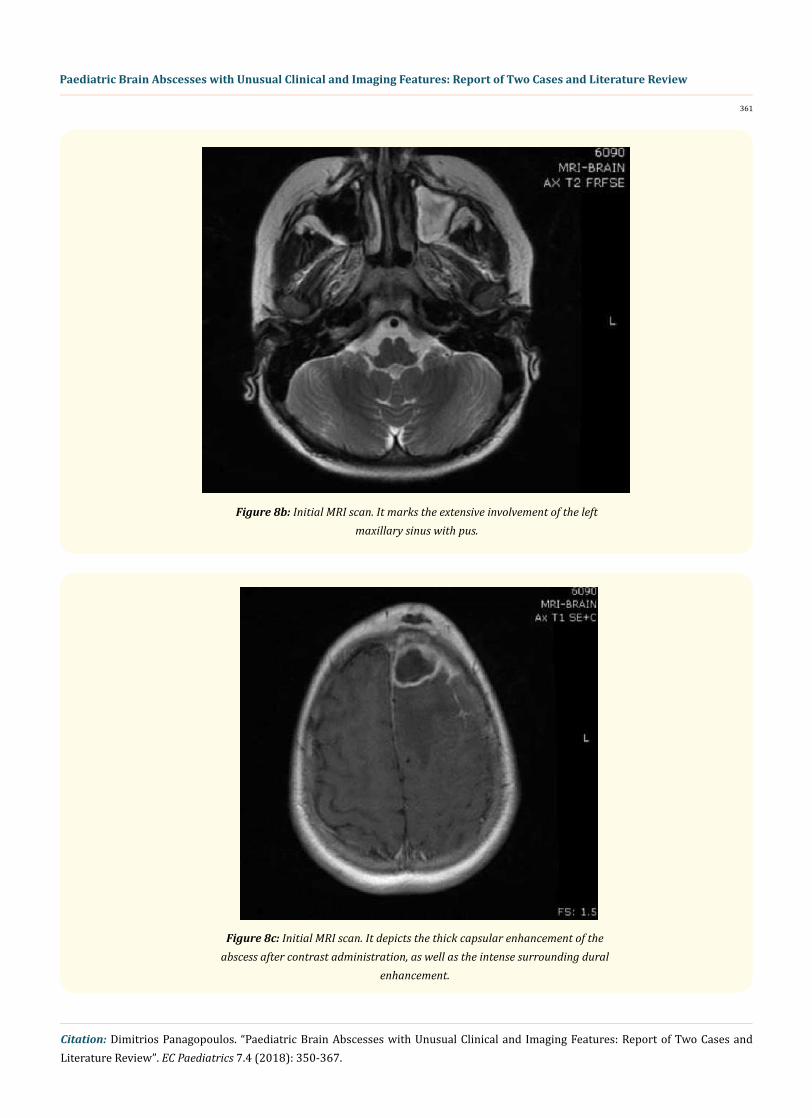
The patient was immediately treated by the otolaryngologists, who evacuated the pus collection of the maxillary and part of the frontal sinus and specimen of pus was sent for microbiologic analysis. Streptococcus Intermedius was the causative factor∙ it appeared no antibi-otic resistance and the antibiotic scheme was continued. He underwent a MRI scan (Figures 8a-8d) of the head, which revealed a frontal brain abscess 3, 2 cm x 3 cm x 2, 2 cm. There was concomitant angiogenic edema and meningeal enhancement after contrast administra-tion and a small amount of midline shift to the right. The abscess seems to be contingent with the posterior wall of the left frontal sinus, while there seems that the cranial vault is eroded in this region, and extension of the pathological findings to the soft tissues of the frontal region.
Figure 8a: Initial MRI scan. It indicates the location of the frontal lobe abscess, with significant amount of surrounding edema. Also, the extension of the
abscess to the frontal soft tissues is illustrated.
361
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Figure 8b: Initial MRI scan. It marks the extensive involvement of the left maxillary sinus with pus.
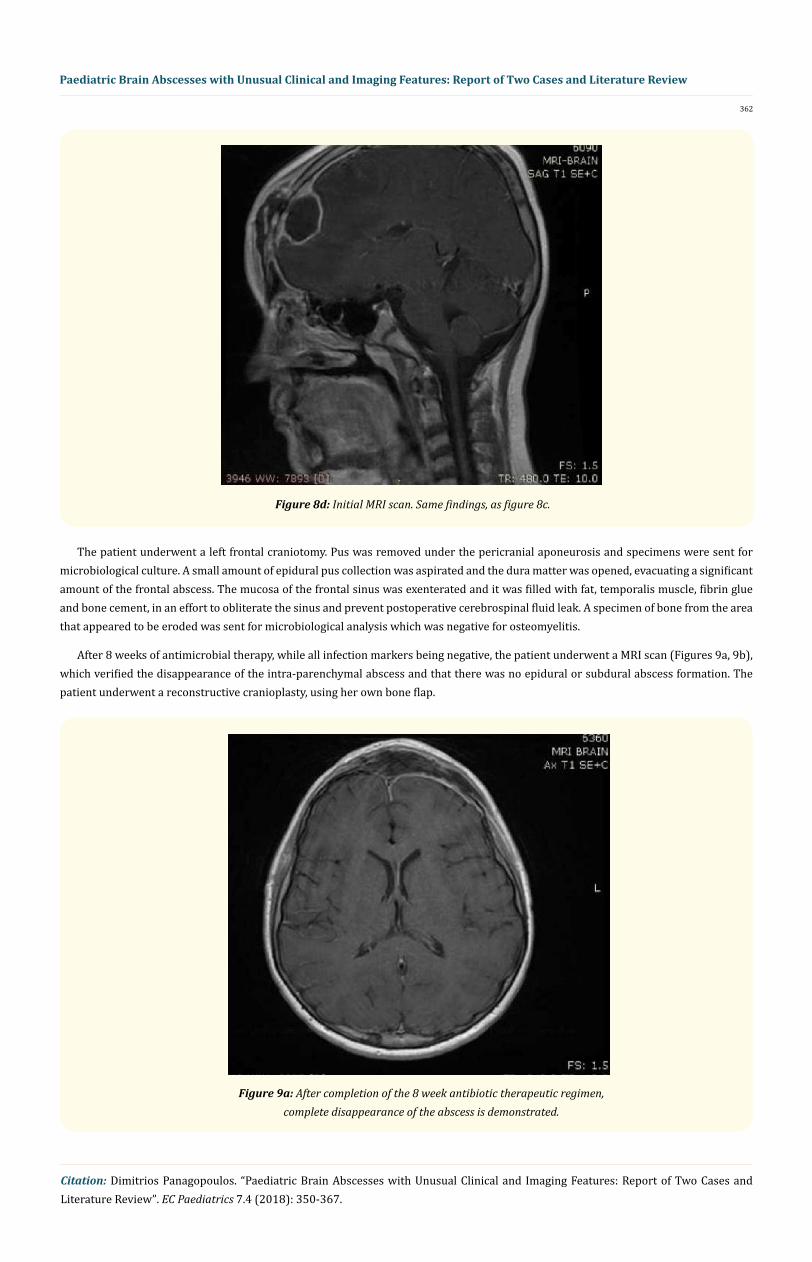
Figure 8c: Initial MRI scan. It depicts the thick capsular enhancement of the abscess after contrast administration, as well as the intense surrounding dural
enhancement.
362
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
The patient underwent a left frontal craniotomy. Pus was removed under the pericranial aponeurosis and specimens were sent for microbiological culture. A small amount of epidural pus collection was aspirated and the dura matter was opened, evacuating a significant amount of the frontal abscess. The mucosa of the frontal sinus was exenterated and it was filled with fat, temporalis muscle, fibrin glue and bone cement, in an effort to obliterate the sinus and prevent postoperative cerebrospinal fluid leak. A specimen of bone from the area that appeared to be eroded was sent for microbiological analysis which was negative for osteomyelitis.
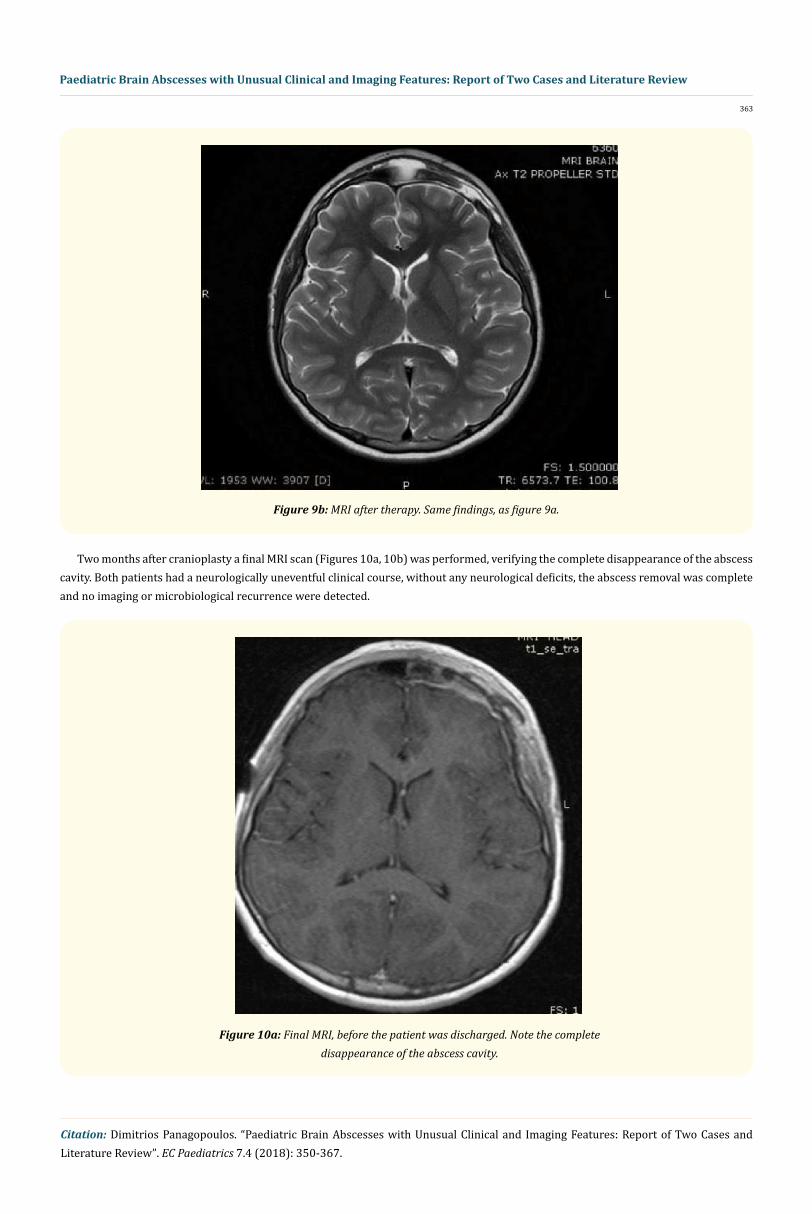
After 8 weeks of antimicrobial therapy, while all infection markers being negative, the patient underwent a MRI scan (Figures 9a, 9b), which verified the disappearance of the intra-parenchymal abscess and that there was no epidural or subdural abscess formation. The patient underwent a reconstructive cranioplasty, using her own bone flap.
Figure 8d: Initial MRI scan. Same findings, as figure 8c.
Figure 9a: After completion of the 8 week antibiotic therapeutic regimen, complete disappearance of the abscess is demonstrated.
363
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Figure 9b: MRI after therapy. Same findings, as figure 9a.
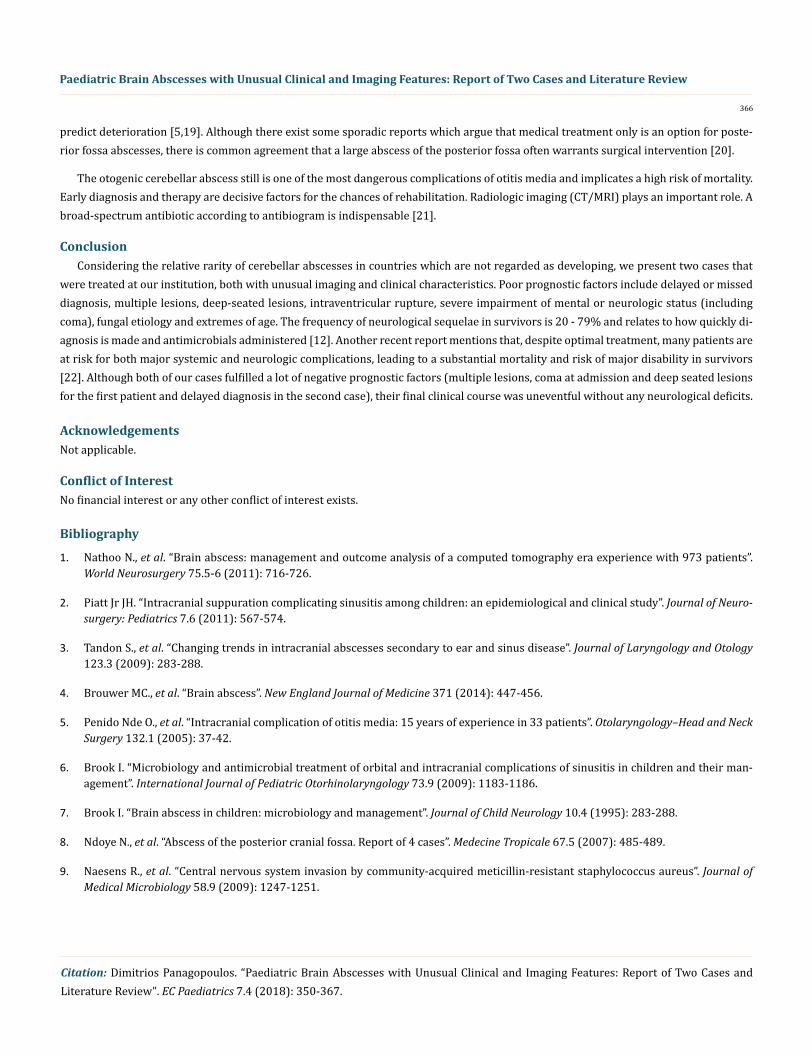
Two months after cranioplasty a final MRI scan (Figures 10a, 10b) was performed, verifying the complete disappearance of the abscess cavity. Both patients had a neurologically uneventful clinical course, without any neurological deficits, the abscess removal was complete and no imaging or microbiological recurrence were detected.
Figure 10a: Final MRI, before the patient was discharged. Note the complete disappearance of the abscess cavity.

364
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
Figure 10b: Final imaging with MRI, before the patient was discharged. Same findings, as figure 10a.
Results and Discussion
A bacterial brain abscess is an intraparenchymal infection that starts as an area of cerebritis and matures into a well-circumscribed walled-off area of purulence. Bacterial pathogens gain access to the central nervous system through a variety of pathways, including direct extension, iatrogenic causes, traumatic injury and by hematogenous dissemination. Direct extension from the sinuses, mastoid and mid-dle ear generally produce a localized abscess near the site of the original infection. In children, cerebellar abscesses occur more com-monly than temporal lobe abscesses. The predisposing factors are age dependent: otitis media is common among young children and older adults; paranasal sinusitis is frequent among older children and young adults [1-3]. The major predisposing conditions are: an as-sociated contiguous focus of infection (e.g. sinusitis, subacute or chronic otitis media and mastoiditis); (40 - 50% of cases) trauma (e.g. penetrating head injury, post-neurosurgery) (10% of cases); hematogenous spread from a distant focus (e.g. in association with pulmo-nary, skin, abdominal and pelvic infections, endocarditis, injected drug use, neutropenia, transplantation, cyanotic heart disease, intrapul-monary right-to-left shunting and esophageal dilation or sclerosis of varices (25%), cryptogenic (no recognized focus) (15%). Acute otitis media can lead to vital complications due to spread of infection. Streptococci and Haemophilus are the most frequent germs for acute otitis media∙ Streptococcus was also the offending organism to our patient [4,5]. Depending on their extension the result can be labyrinthitis, meningitis, a subdural abscess, an epidural abscess, a sinus thrombosis, a brain abscess and/or facial paresis. The otogenic brain abscess can be located in the temporal lobe or in the cerebellum. It is the most dangerous otogenic endocranial complication, which still today results in high mortality. Brain abscesses associated with a contiguous focus of infection generally cause a single abscess. This is in con-tradistinction with one of our presenting cases, which presented with multiple abscesses of the posterior fossa. The commonest

365
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
underlying conditions in developed countries are subacute and chronic otitis media, mastoiditis and congenital heart disease [2,4]. How-ever, their role has declined with introduction of pneumococcal vaccination and administration of antimicrobial therapy for ear infections [3]. However, BA associated with sinus infection remains an important predisposing cause in all ages [3,7,8]. Brain abscesses associated with otitis media and mastoiditis are most common in the inferior temporal lobe and cerebellum, whereas those associated with sinusitis occur primarily in the frontal or the temporal lobes. The posterior cerebral fossa is an uncommon location for cerebral abscess. In most cases diagnosis is made at the encapsulation stage with the risk of life-threatening tonsillar herniation [1,8], something that was the case in one of our patients. The largest documented series of brain abscess include 973 patients treated over a 20-year period (1983 - 2002) [1]. The majority of brain abscesses were supratentorial (n = 872, 89.6%). The causes were of BAs were supratentorial (n = 872, 89.6%). The causes were otorhinogenic (38.6%), traumatic (32.8%), pulmonary (7%), cryptogenic (4.6%), postsurgical (3.2%), meningitis (2.8%), cardiac (2.7%) and ‘‘other” (8.6%). The microbial etiology depends on the site of primary infection; the patient’s age, underlying condition and immune status, and the geography. The organisms most commonly isolated are anaerobes, Streptococci, Enterobacteriaceae, S. aureus (including increasing numbers of methicillin- resistant) [9,10] and fungi; 30 - 60% are polymicrobial. The predominate anaerobes are members of the oropharyngeal flora associated with otorhinolaryngological infections. Specimens obtained during surgery or stereotac-tic computerized axial tomography (CT) – guided aspiration should be sent for aerobic, anaerobic, mycobacterial and fungal cultures and, when indicated, for protozoa. In one study, the Gram stain revealed organisms in 82% of cases and culture was positive in 88% [11]. Be-fore abscess encapsulation and localization, antimicrobials, accompanied by measures to control increasing intracranial pressure, are essential [12]. Once an abscess has formed, surgical excision or drainage combined with prolonged antimicrobial therapy (usually 4 - 8 weeks) remains the treatment of choice. Some advocate complete evacuation of the abscess, while others advocate repeated aspirations as indicated [13]. The procedures used are aspiration through a burr hole and complete excision after craniotomy. Drainage permits mi-crobiologic evaluation of abscess material, which can guides antimicrobial therapy. Since aspiration is generally as effective as excision and is less invasive, it became the procedure of choice. Stereotactic CT – guided aspiration permits accurate access even to areas that had been difficult to reach, such as the brainstem, cerebellum and thalamus, and multiple abscesses [14]. Emergency intervention should be performed for a single abscess. Abscesses > 2.5 cm are excised or aspirated, while those < 2.5 cm or are at the cerebritis stage are aspi-rated for diagnostic purposes only. In cases of multiple abscesses or in abscesses in essential areas, repeated aspirations are preferred [15]. Instead, we preferred surgical drainage of all three abscesses of the posterior fossa at once. Patients with cerebritis can be treated with a shorter course (4 - 6 weeks). However those with an encapsulated abscess, tissue necrosis, undrained abscess(s), multiloculated abscess(s), lesions in vital locations, and the immunocompromised, need 6 - 8 weeks or longer, depending on initial size, causative pathogen(s), and treatment response [15]. The long course is needed for brain tissue to repair and close the abscess space. The initial course is intravenously, often followed by a 2 - 6 months of oral therapy. A shorter course (3 - 4 weeks) may be adequate in patients who had surgical drainage. Prognosis has improved considerably, since the introduction of CT scanning. Mortality has declined in the past two decades and is now 5 - 15% [16]. Long-term sequelae occur in about one-third of patients and include mental retardation, seizures and focal neurologic deficits. Poor prognostic factors include delayed or missed diagnosis, multiple lesions, deep-seated lesions, intraventricu-lar rupture, severe impairment of mental or neurologic status (including coma), fungal etiology and extremes of age. The frequency of neurological sequelae in survivors is 20 - 79% and relates to how quickly diagnosis is made and antimicrobials administered [17]. Be-cause of the small size of the posterior cerebral fossa, abscess in that location requires emergency treatment. Delay can be life-threatening due to the risk of obstructive hydrocephalus and tonsillar herniation. Although they may be clinically silent at times or present with minimal symptoms, they can be fatal if not treated immediately. These lesions often tend to have an unpredictable course depending on the patient’s level of consciousness at presentation, and the timing and aggressiveness of the intervention chosen. The overall rate of complications and death due to brain abscesses has progressively fallen because of the availability of antibiotic medications, the advent of better imaging modalities such as CT scanning, and improved surgical and anesthetic management of the patients. However, even in this modern neurosurgical era, the mortality rate due to cerebellar abscesses remains distressingly high at around 10 to 15% in various large series [17,18]. Cerebellar abscesses can suddenly totally occlude the cerebrospinal fluid pathway, leading to acute hydrocephalus, coma, and death. Cerebrospinal fluid obstruction can be more acute and dangerous in children, in whom it is more difficult to recognize and
366
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
predict deterioration [5,19]. Although there exist some sporadic reports which argue that medical treatment only is an option for poste-rior fossa abscesses, there is common agreement that a large abscess of the posterior fossa often warrants surgical intervention [20].
The otogenic cerebellar abscess still is one of the most dangerous complications of otitis media and implicates a high risk of mortality. Early diagnosis and therapy are decisive factors for the chances of rehabilitation. Radiologic imaging (CT/MRI) plays an important role. A broad-spectrum antibiotic according to antibiogram is indispensable [21].
ConclusionConsidering the relative rarity of cerebellar abscesses in countries which are not regarded as developing, we present two cases that
were treated at our institution, both with unusual imaging and clinical characteristics. Poor prognostic factors include delayed or missed diagnosis, multiple lesions, deep-seated lesions, intraventricular rupture, severe impairment of mental or neurologic status (including coma), fungal etiology and extremes of age. The frequency of neurological sequelae in survivors is 20 - 79% and relates to how quickly di-agnosis is made and antimicrobials administered [12]. Another recent report mentions that, despite optimal treatment, many patients are at risk for both major systemic and neurologic complications, leading to a substantial mortality and risk of major disability in survivors [22]. Although both of our cases fulfilled a lot of negative prognostic factors (multiple lesions, coma at admission and deep seated lesions for the first patient and delayed diagnosis in the second case), their final clinical course was uneventful without any neurological deficits.
AcknowledgementsNot applicable.
Conflict of InterestNo financial interest or any other conflict of interest exists.
Bibliography
1. Nathoo N., et al. “Brain abscess: management and outcome analysis of a computed tomography era experience with 973 patients”. World Neurosurgery 75.5-6 (2011): 716-726.
2. Piatt Jr JH. “Intracranial suppuration complicating sinusitis among children: an epidemiological and clinical study”. Journal of Neuro-surgery: Pediatrics 7.6 (2011): 567-574.
3. Tandon S., et al. “Changing trends in intracranial abscesses secondary to ear and sinus disease”. Journal of Laryngology and Otology 123.3 (2009): 283-288.
4. Brouwer MC., et al. “Brain abscess”. New England Journal of Medicine 371 (2014): 447-456.
5. Penido Nde O., et al. “Intracranial complication of otitis media: 15 years of experience in 33 patients”. Otolaryngology–Head and Neck Surgery 132.1 (2005): 37-42.
6. Brook I. “Microbiology and antimicrobial treatment of orbital and intracranial complications of sinusitis in children and their man-agement”. International Journal of Pediatric Otorhinolaryngology 73.9 (2009): 1183-1186.
7. Brook I. “Brain abscess in children: microbiology and management”. Journal of Child Neurology 10.4 (1995): 283-288.
8. Ndoye N., et al. “Abscess of the posterior cranial fossa. Report of 4 cases”. Medecine Tropicale 67.5 (2007): 485-489.
9. Naesens R., et al. “Central nervous system invasion by community-acquired meticillin-resistant staphylococcus aureus”. Journal of Medical Microbiology 58.9 (2009): 1247-1251.
367
Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review
Citation: Dimitrios Panagopoulos. “Paediatric Brain Abscesses with Unusual Clinical and Imaging Features: Report of Two Cases and Literature Review”. EC Paediatrics 7.4 (2018): 350-367.
10. Roche M., et al. “A twelve-year review of central nervous system bacterial abscesses; presentation and aetiology”. Clinical Microbiol-ogy and Infection 9.8 (2003): 803-809.
11. Rath TJ., et al. “Imaging of cerebritis, encephalitis, and brain abscess”. Neuroimaging Clinics of North America 22.4 (2012): 585-607.
12. Yogev R and Bar-Meir M. “Management of brain abscesses in children”. Pediatric Infectious Disease Journal 23.2 (2004): 157-159.
13. Ratnaike TE., et al. “A review of brain abscess surgical treatment- 78 years: aspiration versus excision”. World Neurosurgery 76.5 (2011): 431-436.
14. Kocherry XG., et al. “Efficacy of stereotactic aspiration in deep- seated and eloquent-region intracranial pyogenic abscesses”. Neuro-surgical Focus 24.6 (2008): E13.
15. Brook I. “Microbiology and treatment of brain abscess”. Journal of Clinical Neuroscience 38 (2017): 8-12.
16. Tattevin P., et al. “Bacterial brain abscesses: a retrospective study of 94 patients admitted to an intensive care unit (1980 to 1999)”. American Journal of Medicine 115.2 (2003): 143-146.
17. Brydon HL and Hardwidge C. “The management of cerebellar abscess since the introduction of CT scanning”. British Journal of Neu-rosurgery 8.4 (1994): 447-455.
18. Nadvi SS., et al. “Cerebellar abscess: the significance of cerebrospinal fluid diversion”. Neurosurgery 41.1 (1997): 61-67.
19. Pandey P., et al. “Cerebellar abscesses in children: excision or aspiration?” Journal of Neurosurgery: Pediatrics 1.1 (2008): 31-34.
20. Turner RC., et al. “Medical management of cerebellar abscess: a case report and review of the literature”. West Virginia Medical Journal 107.2 (2011): 21-23.
21. Durisin M., et al. “Otogenic cerebellar abscess due to purulent labyrinthitis and defect of the superior semicircular canal and its propagation through the endolymphatic sac”. European Archives of Oto-Rhino-Laryngology 264.8 (2007): 955-958.
22. Brouwer MC and van de Beek D. “Management of bacterial central nervous system infections”. Handbook of Clinical Neurology 140 (2017): 349-364.
Volume 7 Issue 4 April 2018©All rights reserved by Dimitrios Panagopoulos.





























