Embed Size (px)
Citation preview

Operative Management of Spinal Disorders

CLASSIFICATIONS of SPINE INJURIES
• Cervical spine• Upper cervical spine
• Lesions of the craniovertebral junction• Atlas fractures• Rotary atlantoaxial dislocation• Odontoid fractures• Hangman’s fractures
• Lower cervical spine
• Thoracolumbar spine• The Denis classification• The AO classification (Magerl)

CLASSIFICATIONS of SPINE INJURIES

SURGICAL METHODS: Upper cervical spine
• Atlanto-occipital and atlas fractures• Traction has been demonstrated to be potentially harmful at this
level. • Occipitocervical fusion induces ankylosis, decreasing the patient’s
mobility by at least 50% especially in rotation. • These consequences must be taken into account in the indications
for this technique. However, this is a vital zone and no instability can be tolerated.
• Bone grafts are recommended but may have limited efficacy, as re-operations usually reveal bony masses that may or may not have a stabilizing role.

SURGICAL METHODS: Upper cervical spine
• Rotary atlantoaxial dislocation• These dislocations are reduced by progressive transcranial traction. • After reduction, C1–C2 screw fixation is performed by means of a
simple technique but which can be dangerous due to the variable proximity of the vertebral artery.
• Fluoroscopic navigation is very useful in this setting. • The key to the technique is to penetrate the caudal part of the C2
articular processes and direct the screw towards the anterior arch of the atlas.

SURGICAL METHODS: Upper cervical spine
• C2 fractures: Odontoid fractures• Displaced fractures are reduced by progressive
traction (tongs).• Anatomical reduction is essential prior to anterior
screw fixation.• The classifications are very useful to select the
most appropriate technique:• Posterior displacement (posterior oblique fracture)
requires fixation by anterior screw fixation according to a standardized technique: the entry point of the screw, visualized by image intensifier (fluoroscopy) on AP and lateral views, is situated at the anterior aspect of the inferior endplate of C2. Advancement of the K wire and guide tube used to insert the perforated system (drill then screws) is monitored. Correct screw length reaches the apex of the dens. Self-tapping screws that are only threaded in their distal part are used to apply compression on the fracture site. The subject’s morphology may make this technique difficult or even impossible in the case of barrel chest, preventing screw fixation of the axis.

SURGICAL METHODS: Upper cervical spine
• C2 fractures: Odontoid fractures• Anterior oblique fractures require a posterior approach with C1–C2
fusion between the posterior arch of the atlas and the laminae of C2. Regardless of the instrumentation used (wiring deserves its bad reputation), fixation must ensure compression and a bone graft is usually performed between the posterior arch of C1 and the cranial aspect of the previously roughened lamina of C2. This also avoids overcorrection in lordosis. Horizontal fractures are preferably treated by anterior screw fixation.

SURGICAL METHODS: Upper cervical spine
• C2 fractures: Hangman’s fractures:• The lesion of the C2–C3 disc determines the instability of this
fracture, which must be reduced by tongs. An anterior or posterior approach is used depending on the site of the fracture line.
• The anterior approach consists of C2–C3 intervertebral arthrodesis with a screw plate.
• The posterior approach consists of bipedicular screw fixation, which is a simple technique when the screw is inserted into the superomedial quadrant of the articular process of C2 and when the C1–C2 interspace is widened by removing an equivalent amount of ligamentum flavum. Initial progression of the screw in the pedicle is monitored under direct vision.

SURGICAL METHODS: Lower cervical spine
• The lesion involving one or only a few segments is reduced preoperatively• An anterior approach should be used, as this easy technique is
better supported by a supine patient. • For lesions involving one segment (bilateral dislocation of the
facet joints for example), the anterior sternocleidomastoid approach is easy and anatomical, as it only sections one omohyoid muscle or one superior thyroid artery and only very occasionally.
• This is a noninvasive approach. The blood vessels are situated laterally, the viscera are medial and, after dissection of the midline fascia of the neck, the finger is in contact with the spine.
• Discectomy is systematically performed. • Abrasion of the endplates must not destroy them. The
autologous bone graft or bone substitute, which is very useful in this situation, is inserted and maintained by a 4-screw plate.
• The length of the screws must not exceed 16 mm and bicortical screw fixation is unnecessary and can be dangerous.

SURGICAL METHODS: Lower cervical spine
• A teardrop fracture does not require reduction, which is only rarely obtained and which is dangerous in view of the associated ligament damage, with a risk of overcorrection with traction of the spinal cord.
• This lesion resembles a burst fracture of the lumbar vertebrae but comprises very severe ligamentous lesions.
• Corpectomy is generally required, and is filled by a tricortical graft maintained by a screwed plate.
• The lesion is not reduced• This is often the case in unilateral dislocations. • A posterior approach is required allowing fusion by articular screw
fixation and plates or rods or by interlaminar clamps with rods.
• Lesions at multiple levels• They should be treated via a posterior approach.
• Dual approach• A dual approach is only indicated for lesions with vertebral defects

SURGICAL METHODS: Thoracolumbar spine
• A posterior approach which is the approach most often used. • This single approach is simple and the failures leading to malunions
following this technique are rare. • Reduction of the lesions, apart from dislocations which require
difficult reduction manoeuvres especially in the thoracic spine, is generally achieved by placing the patient on the operating table.
• The length of the plate, classically estimated at two levels on either side of the fractured vertebra, depends on the severity of the lesions.
• Short plates have the advantage of a shorter incision and a more limited future restriction of movement, but should be reserved to cases in which screw fixation in the fractured vertebra is possible (depending on the state of the pedicles).
• Techniques are otherwise simple and essentially involve the pedicle.

SURGICAL METHODS: Thoracolumbar spine
• Pedicle screw fixationThoracic spine: • Pedicle screw fi xation is performed below the interspace, at the level of
the transverse process which is the main landmark of the pedicle.• The angle of the screw is guided by CT views of the direction of the
pedicles.• Screws must not be larger than 5 mm in diameter and are connected by
plates or rods adapted to the patient’s kyphosis.Lumbar and lower thoracic spine: • the diameter of the pedicles allows the use of screws 6.5 mm in
diameter, but barely longer than 45 mm due to the vascular risks. • Pedicle screw fixation is performed at the junction of the articular
process and the transverse process and is convergent, as lumbar pedicles are also often convergent.

SURGICAL METHODS: Thoracolumbar spine
• Anterior approaches• The use anterior fusion as a second-line
procedure when there is a large anterior defect or in the case of non-union which is rare (about 2% of our patients).
• The surgical approach is simple: short right thoracotomy, flank incision.
• Thoracolaparotomy is gradually being replaced by minimally invasive techniques.
• Anterior fusion consists of corpectomy or discectomies filled by autologous bone grafts and maintained by fixation of the vertebral bodies.
• Bone grafts• Bone grafts are used systematically in all
anterior fusion procedures. • Synthetic grafts are used for lesions involving a
single vertebra and autologous bone grafts are used after corpectomy.
• Posterolateral bone grafts are used in posterior approaches to the thoracolumbar spine only in the rare case of pure ligamentous lesions.

Timing
• Timing is the key to optimal axonal preservation. • The six-hour rule must be used as a guide

Trauma in children
• Different traumatic lesions are observed in children. • Apart from SCIWORA, described above, fixation must be
performed very cautiously as it corresponds to arthrodesis at this age.
• The resulting growth disorders very often have a pejorative functional course.
• Orthopaedic techniques should be preferred in children and surgery should be reserved for the fortunately rare cases of extreme instability.

HOW TO AVOID COMPLICATIONS
• The best way to avoid complications of surgery is a rigorous surgical technique.
• There is now a sufficient number of workshops to acquire these techniques on cadavres.
• To prevent neurological impairment, handling of patients prior to surgery must be clearly understood and rigorously applied by all teams involved from the site of the accident to the operating room.
• Bladder catheterization is performed as an emergency to preserve future bladder contractions.
• Skin capital must be preserved by protecting exposed areas and preventing pressure ulcers.
• Ventilatory assistance with careful intubation must be used in the early stages, specially for tetraplegic patients, followed by tracheotomy, when necessary, to prevent dramatic atelectasis.

HOW TO AVOID COMPLICATIONS
• The patient’s positions in bed must be defined and observed daily to avoid abnormal positions of paralysed joints, especially the ankles.
• Spasticity must be rapidly treated by drugs. • Overactive bladder must be treated early to prevent
damage to the upper urinary tract.• Good realignment of the spine constitutes the best
prevention of the very high rate of posttraumatic syringomyelia (about 28% of paraplegic and quadriplegic patients).
• However, the essential guideline is that all spinal cord injury patients, until radiological proof to the contrary, must be considered to be unstable, from the time of the accident until installation on the operating table.


OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH1.1 The surgical technique
The surgical technique is detailed step-by-step, for degenerative disc pathology in subaxial spine
• Anaesthesia• Standard intubation for the standard case: tube protection (spiral) avoids
kinking• High volume, low pressure cuffs: reduce trauma to tracheal mucosa and
innervation• Alternative: naso-tracheal intubation with extension tube fixed to forehead• Endoscopic intubation: cervical instability, severe stenosis with myelopathy,
any foreseen difficult intubation (anatomical factors)• Positioning
• Flat on the back, neck slightly extended for a horizontal approach• No head fixation except in instability (Mayfield)• Lateral fluoroscopy (antero-posterior only for disc prosthesis or dens
screwing)• Shoulders caudally fixed in case of short neck, or C6 to T1 approach, elbows
protected• Check-up of tracheal tubing to respirator• Neuromonitoring if requested by pathology (severe myelopathy)


OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH
• Side of approach• Right side for right handed surgeon
• Left side from C6-T1 reduces recurrent laryngeal nerve irritation or lesion
• Some difficult reoperations may be easier handled from the other side (or by a posterior approach)
• Globally, view is better to the opposite foramen and especially in anterolateral approach
• Skin incision• Transverse centered on disc space is cosmetically best, 3–6 cm for
1–3 levels, reaching or crossing midline 1 cm (prosthesis)
• Transverse cutting of platysma, upper and lower mobilisation to transform wound to a more vertical approach by small Gelpi retractor
• Dissection of superficial fascia followed by atraumatic finger dissection along anterior border of sternocleidomastoid muscle, feeling common carotid artery pulsations

OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH
• Prevertebral space• Using smooth retractors, the visceral content is mobilised medially
and the vascular package laterally down to deep fascia, opened near midline to expose prevertebral space (thyroid vessels mostly preserved)
• Attention: recurrent laryngeal nerve!• Lateral fluoroscopy to localise disc space with a needle• Dissect and elevate longus colli insertions (diffi cult with large
osteophytes) avoiding venous bleeding (only bipolar coagulation)• Attention: vertebral artery (VA) if dissection too lateral!
• Retraction• Only centered incision and correct dissection allow atraumatic
retraction• Teethed Caspar retractor blades are inserted under longus colli
muscle to avoid vascular or visceral lesion, with reasonable opening pressure to visualise the whole anterior disc space
• Retainer pins midline insertion near the center of vertebral body facilitates orientation during decompression, essential in case of prosthesis or further plating

OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH• Discectomy
• Microscope gives light, precision, security• Annulus incision, clearing of disc space with curettes, small rongeurs
and disc pounches avoiding cartilage penetration• Only large anterior osteophytes should be removed to avoid anterior
vertebral rim weakening promoting cage or prosthesis subsidence• Complete discectomy down to posterior longitudinal ligament (PLL )
and medial to remaining lateral annulus (PLL is preserved only if soft DH and no subligamentous extrusion)
• Decompression• Really begins in posterior 1/3 of disc space under magnification, aided
by progressive intervertebral distraction• Removal of osteophytes and uncus with microdrill, 1-2 mm Kerrison
rongeurs, internal foraminotomy to visualise emerging nerve root• Microincision in PLL, elevate with micro nerve hook and resect
completely with posterior rim attachment, from midline to foramina• Attention: venous plexus, VA• Careful haemostasis with bipolar, gelfoam, bone wax (fibrin glue if
heavy bleeding)

OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH
• Implantation• Nothing: avoid too much anterior and lateral decompression
favouring kyphosis• Iliac bone graft: observe tricortical graft with anterior rim
contact limiting subsidence• Cage: same, avoid endplate weakening• Prosthesis: exactly centered midline on spinous process line in
anteroposterior view (malfunction)• Plate: flatten anterior rim and medialise screws for improved
stability
• Wound closure• Last fluoro-check for implants• Review haemostasis: epidural, bony, muscular• Usually no wound drainage required• Only platysma and intradermal suture (small dressing)• No collar unless severe traumatic instability• Awake on table with neurological examination

OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH
• Postoperative care• Analgesics, non steroid antiinfl ammatory drug, 24 h ATB, low
molecular heparin next day• Corticosteroids only in defi cit or abnormal tracheal swelling
requiring laryngoscopic screening• CT or MRI immediately in case of any new defi cit to rule out
bleeding, compression versus contusion• EMG for peripheral nerve lesion (plexus, ulnar)• Get-up next day with X-ray control for implants• Stay 3–6 days with rehabilitation as needed• Next visit 1month (and 3 m, 1y for implants)

OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH
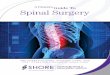
1.2 Corpectomy Indication: degeneration, trauma, tumor with severe myelopathy• More radical, also retrocorporeal dural decompression by
vertebral body resection (1–3 levels) in extended stenosis, including disc above and below
• Impacted graft or better adapted spacer with bone fi lling for improved stability until fusion
• Common risk is graft dismantling typically at the inferior border with recurrent myelopathy
• Plating mandatory to avoid fracture and pseudarthrosis of long grafts
• Intermediate fixation technique (Benzel) increases stability with 3-point fixation
• Dynamic plating adapts natural graft settling and avoids screw displacement (kyphosis)
• Drain the wound as haematoma, air way obstruction more frequent

Corpectomy C3C5 for metastatic cancer with spacer and plate fixation for lordoticstabilisation. Note osteolytic tumor compressing spinal cord with marked kyphosis on preoperativeMRI


OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH1.3 Anterolateral approach
• Unilateral corporo-transverse approach for oblique decompression• Anterior microforaminotomy• Surgical principle is freeing and protecting vertebral artery (VA) for a more
lateral approach to the anterior offending lesion in radiculopathy, with bilateral anterior decompression from the most pathological side in myelopathy
• Total or subtotal uncus resection respecting as much as possible the intervertebral disc to avoid instability, no instrumentation required claimed by pioneers
• Risk: • Vertebral artery (VA) (bleeding, AV fistula, vertebro-basilar stroke) and
sympathic chain (Horner)• Spinal accessory nerve above C3, lymphatic chain below C6
• Technically demanding more in myelopathy than in radiculopathy (for specialists)
• Most useful when control of VA required: foraminal tumors or vascular lesions

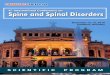
OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH1.4 Direct anterior dens screwing
Indication: odontoid type II fracture• Double fluoroscopy: lateral L + anteroposterior AP: visualise dens in
open mouth view (cotton roll packed between teeth)• Maximum neck extension under fluoro-control in Mayfield clamp or in
slight submandibular traction: fracture reducible suitable for anterior approach otherwise posterior fixation
• Simulate ideal screw trajectory (L view) by metal bar along neck from odontoid tip to thoracic wall: limited neck extension and thoracic kyphosis are contraindications
• Transverse skin incision at C5 with upward transmuscular finger dissection to palpate and mark C2C3 disc at midline with a pointer under AP + L view (entry point)
• Resect some bone around entry point on midline C3 anterior rim (logging also further screw head) to improve instrument inclination for virtual screw axis created by pointer a few mm behind anterior rim of C2 and a few mm in the endplate

OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH
1.4 Direct anterior dens screwingIndication: odontoid type II fracture• Introduce an adapted guide wire in the hole with fluoro-control,
then the tubular guide for instrument passing and protection of soft tissues for next steps avoiding vascular and visceral lesions
• Drill guide wire (easier to correct trajectory) under AP + L view through middle of fracture line up to the cortex of odontoid tip followed by canulated drill and tap on same wire
Direct anterior screw fixation for displaced reducible odontoid type II fracture. Note entry point, direction and tip of canulated lag screw

OPERATIVE TECHNIQUE FOR ANTERIOR APPROACH
1.4 Direct anterior dens screwingIndication: odontoid type II fracture• Evaluate screw length on scale and position canulated lag screw
under compression of distal fragment (screw passing fracture line in L view) in/ or better slightly through odontoid tip cortex for improved stability • Retract tubular guide, palpate and inspect screw head logging in bone cavity
• Last fluoro-check for screw position in AP + L• Review haemostasis and close wound in 2 layers usually without
drainage• Immediate mobilisation without collar, very useful in elderly
patients• Technical failures: instability, pain and rarely neurological deficit,
non union or pseudarthrosis in evolution indicating reoperation by anterior or posterior approach:
• Insufficient fracture reduction by positioning or fracture distraction by a too short screw
• AP or L screw deviation mostly by incorrect C2 approach, prominent thorax, poor dens visualisation in osteoporosis


OPERATIVE TECHNIQUE FOR POSTERIOR APPROACH
• Prone position of patient with careful padding on table, arms fixed along the body
• Head fixation in a Mayfield clamp avoids ocular and throat compression
• Slight flexed neck to enhance exposure by opening space between posterior arches
• Slight reverse Trendelburg position to empty cervical draining veins avoiding head about heart: risk of air embolism (main reason against sitting position)
• Operative level is checked on fluoroscopy and marked with a drop of methyl blue at the facet junction of corresponding disc (more precise than spinous process in limited approach)
• In case of any foreseen instrumentation, fluoroscopy is draped in the operative field
• Actually the author does not use navigation proposed by some investigators for C1C2 transarticular screwing because of cumbersome handling and lack of mm precision in a moving procedure

OPERATIVE TECHNIQUE FOR POSTERIOR APPROACH
2.1 MicroforaminotomyIdeal case: Lateralised DH (soft) mainly at cervico-thoracic junction.• Small midline incision sufficient for subperiostal unilateral muscle
stripping over the corresponding facets allowing introduction of a tubular retractor centered on lamino-articular junction
• Introduction of microscope for light, precision and security• Key-hole lamino-arthrotomy with microdrill and/or small 2 mm Kerrison:
medial facet resection is mandatory to avoid dural retraction• Following careful flavum resection, the epidural veins are compressed by
small cotton at upper and lower corner (the only permanent retactors)• Micro-hook palpates disc fragment or protrusion under the displaced
nerve root near axilla

OPERATIVE TECHNIQUE FOR POSTERIOR APPROACH
2.1 MicroforaminotomyIdeal case: Lateralised DH (soft) mainly at cervico-thoracic
junction.• Gentle elevation of nerve root allows disc fragment removal
and limited curettage• Careful hemostasis with bone wax and micro-bipolar is required
to avoid an epidural or wound haematoma (always drain in dubious case)
• No need for a collar in absence of instability except for initial muscle pain
Posterior foraminotomy approach with key-hole lamino-arthrotomy exposing lateraldura and compressed nerve root by underlying disc herniation. Note dilated epidural veinscompressed by micro-cottons

OPERATIVE TECHNIQUE FOR POSTERIOR APPROACH
2.2 LaminectomyClassical posterior decompression for stenosis is mostly sufficient in
elderly patients with rigid spine. Additional instrumentation for instability is required according to preoperative sagittal imbalance and degree of facet undermining during operation.
• Laminectomy should be sufficiently high and large • Pay attention: facets, C2 spinous process muscle insertions (rotatory
muscles)• Careful lamina resection with small instruments: risk of dural laceration or
cord contusion in severe stenosis, easier handling on microscope • Sufficient foraminal nerve decompression: foraminotomy • Limited attempt at disc exploration (only laterally allowed): risk of
neurological deficit• Meticulous epidural, bone and muscle haemostasis with drainage: risk of
haematoma

OPERATIVE TECHNIQUE FOR POSTERIOR APPROACH
2.2 Laminectomy• In case of dural tear or defect (trauma, tumor): primary closure with
microsuture/graft if accessible otherwise sandwich packing with fat/ muscle reinforced with fibrin glue, more meticulous closure of muscle (eventually flap rotation according to plastic surgery techniques), fascial, subcutaneous plan with separate stitches on skin
• Common risk: kyphosis, instability with axial neck and shoulder pain, C5 paresis (spinal cord posterior migration following decompression) mostly regressive
• Contraindication: loss of lordosis indicating posterolateral fusion and collar
• Or more stable: transarticular arthrodesis according to Roy-Camille (short screw straight ahead avoiding neuroforamen) or to Magerl (longer screw superolaterally orientated avoiding VA)
• Alternative: translaminar screw fixation at cervico- thoracic junction Instrumented laminectomy (or/and double approach) are mandatory
in case of osteoporotic, traumatic and tumor involvement of anterior column.

OPERATIVE TECHNIQUE FOR POSTERIOR APPROACH2.3 Laminoplasty
• Multiples techniques mainly developed in Japan (where OPLL is frequent), but increasing interest outside because impressive enlargement of spinal canal at multilevel stenosis much like laminectomy with less destabilisation (unless using long posterior fi xation) avoiding also extended anterior approaches with graft related problems (now better controlled with intervertebral spacers and dynamic platting):
• Z-laminoplasty (Hattori)• Open-door technique (Hirabayashi)• En bloc laminoplasty (Kurokawa)• Instrumented laminoplasty
• The surgical principle is to open the canal on one side (open-door) for bilateral decompression much as in laminectomy and to maintain enlargement by fi xation of lamina (wire, screw, spacer) in a higher position.
• Sagittal imbalance and preoperative instabilities are also relative contraindications.• Complications are about the same as for laminectomy (neck/shoulder pain, C5
paresis). • Laminoplasty is probably underused in degenerative pathology, but also in spinal cord
tumors mainly in children to replace posterior arches avoiding long term deformity

Indications for tracheal intubation in spinal injury
• Insecure airway or inadequate arterial oxygen saturation (i.e. less than 90%) despite the administration of high concentrations of oxygen.
• Orotracheal intubation is rendered more safe if an assistant holds the head and minimises neck movement and the procedure may be facilitated by using an intubation bougie.
• Flexible fibreoptic instruments may provide the ideal solution to the intubation of patients with cervical fractures or dislocations.

Indications for tracheal intubation in spinal injury
• If possible, suction should be avoided in tetraplegic patients as it may stimulate the vagal reflex, aggravate preexisting bradycardia, and occasionally precipitate cardiac arrest
• The risk of unwanted vagal effects can be minimised if atropine and oxygen are administered beforehand.

Hypotension
• In uncomplicated cases of high spinal cord injury (cervical and upper thoracic), patients may be hypotensive due to sympathetic paralysis and may easily be overinfused.

Nursing management
In the emergency departmentIn the acute and rehabilitation care setting

Nursing intervention
• Internal environment• Pain management• Skin hygiene and care• Nutrition• Bladder management• Bowel care• Sexuality

Nursing intervention: Internal environment
• Patients with high thoracic and cervical lesions are susceptible to respiratory complications: long-term goal of reducing the risk of chest infections
• Monitoring in the acute phase should include • skin colour, level of orientation, respiratory rate and
depth, chest wall and diaphragmatic movement, • oxygen saturation, chest auscultation, and vital
capacity.
• Some patients will require additional oxygen therapy and possibly non-invasive pressure support.

Nursing intervention: Internal environment
• A 24-hour physiotherapy with assisted coughing and bronchial and oral hygiene.
• Cardiovascular monitoring will include patient’s blood pressure and pulse (high lesion patients may be hypotensive and bradycardic),
• Observing for evidence of deep vein thrombosis (circumference of the calves and thighs, the patient’s temperature must be monitored), as a low grade pyrexia is sometimes the only indication that thromboembolic complications are developing.
• Appropriately measured and fitted thigh-length anti embolism stockings should be applied.

Nursing intervention: Internal environment
• Patients with high thoracic and cervical lesions are susceptible to respiratory complications: long-term goal of reducing the risk of chest infections
• Monitoring in the acute phase should include • skin colour, level of orientation, respiratory rate and
depth, chest wall and diaphragmatic movement, • oxygen saturation, chest auscultation, and vital
capacity.
• Some patients will require additional oxygen therapy and possibly non-invasive pressure support.

Tracheostomy
• High spinal cord injury (above C5) produces partial or total diaphragmatic impairment and ventilatory failure.
• Injury below C5 decreases expiratory muscle function resulting in decreased cough, mucous impaction and atelectasis

Hypotension in Spinal cord Injury
• Neurogenic shock refers to a pattern of decreased heart rate, blood pressure, and systemic vascular resistance that develops secondary to high thoracic or cervical spinal cord injury
• Underlying mechanism is sympathetic denervation to the heart and peripheral vasculature.
• Management includes intravascular fluid resuscitation and enhancing inotropy and peripheral vasoconstriction; dopamine may be a useful first-line agent

Thank You