Embed Size (px)
Citation preview

Opportunities for TB Prevention
in College Students
Jennifer Flood MD, MPH
Tuberculosis Control Branch
California Department of Public Health
June 3, 2016

Young adults with TB in U.S.
• 18 year old who
arrived from
Guatemala 3 years
previously
• Presents with fever
and cough to ER
• Bronchitis diagnosed
• Returned to ER with
massive hemoptysis
• 22 year old in U.S.
since college entry
• TB in lymph nodes
around his airway
• With treatment lymph
nodes may get larger
before resolving
Q. “Is there anything I
could have done to
prevent this from
happening?”2

Natural History of TB
Latent TB infection
(LTBI)
5%
Progression to
active TB
disease
“Reactivation”
Exposure to
infectious
TB
90%
Remain latently infected
5%
Develop “primary”
active TB disease
3
Not infected

Failure to Prevent TB
• 1 in 10 individuals who develop TB die
• TB disease is costly ($40K- $1 million)
• TB spreads through the air
4

Questions
• What is the frequency of TB disease and
latent TB infection in young adults?
• What strategies are most effective to
detect and treat TB infection?
• How can TB disease be rapidly identified
when it occurs in college settings?
5

What is the frequency of TB
disease and infection?
6

TB Cases in the United States
1982–2015
CDC, Annual Report, 2015
Salinas, et al. MMWR, 2016
First increase in 23 yrs
7

Trends in TB Cases in Foreign-born Persons,
United States, 1993–2014
8
No. of Cases Percentage

How do TB Cases Occur in California?
9
13%Recent
Transmission
79.5%Reactivation
of remote infection
7.5%Importation
~2,000 TB Cases
Per Year

International Students at U.S.
Colleges and Universities
10

Top 10 States with
International Students
11
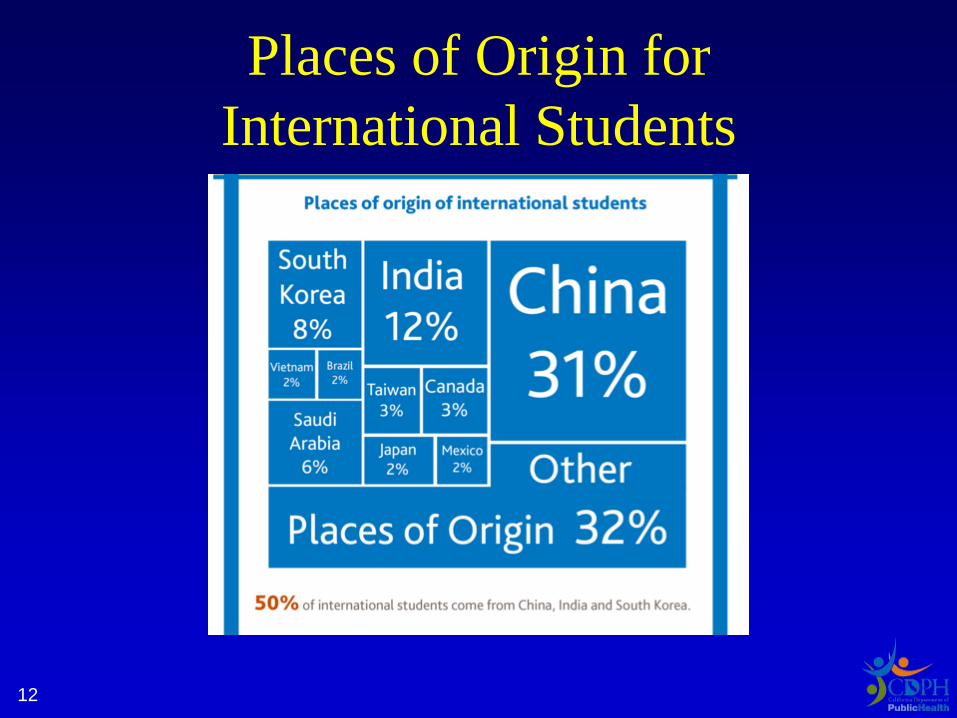
Places of Origin for
International Students
12

WHO 22 High Burden
TB Countries
13

Overseas Screening Requirement
NO TB screening is required for the following groups:
Visitor/tourist
Student Work
Unauthorized (undocumented)
Required for:
Immigrant
Refugees
Permanent resident applicants
Asylees
Status adjusters

TB Disease in Persons
Ages 18-24 in United States, 2011
15
Cases Incidence
Total 878 2.8/100,000
US born 629 0.9/100,000
Foreign-born 249 19/100,000

TB Exposures on College
Campuses in U.S.
• ~ 900 TB cases in 18-24 year olds
Potential for ~1 TB exposure every day on a
college campus in US

Reason for presentation: TB Cases among Adults 18-24 years old in United States, 2011
Reason for TB evaluation
n (%)
TOTAL 878
TB Symptoms 671 (76%)
Contact investigation 57 (7%)
Targeted testing 48 (5%)
Occupational screen 23 (3%)
Immigrant medical exam 27 (3%)
Other (HCW, incidental lab result,
unknown)52 (6%)

TB Case Characteristics in Foreign-born Adults 18-24 years old, U.S., 2011
CharacteristicForeign-born
n %
Years in US at TB diagnosis
<2 years 288 45.8%
2 – 5 years 231 36.7%
> 5 years 110 17.5%
Location of Birth
Mexico 125 19.9
Guatemala 46 7.3
India 43 6.8
China 40 6.4
Philippines** 40 6.4
Vietnam 36 5.7
Other 299 47.5

Clinical Characteristics TB Case: Adults 18-24 years old, U.S., 2011
Characteristic N %
Infectiousness
Smear positive, culture positive 346 39%
Smear negative, culture positive 193 22%
Site of Disease
Extrapulmonary only 165 19%
Pulmonary only 616 70%
Both extrapulmonary and pulmonary95 11%
Abnormal chest radiograph 694 79%
Cavitary chest radiograph 278 32%

Latent TB Infection in
18-24 year olds, U.S. 2011
IGRA positive
US-born 1.3%
Foreign-born 8.7%
________________________________
Total 2.5%
~ 800,000 young adults
Source:
Estimated using NHANES and 2011 census data20

Most are unaware of their TB
infection and untreated!
21

American College Health Association
• All incoming students should be screened for risk factors
for TB through a screening questionnaire
• Students with identifiable risks factors should be tested
• Treatment for LTBI should be recommended and
completion should be a high priority
ACHA Guidelines: Tuberculosis Screening and Targeted Testing of College and University Students,
April 2014

Barriers to TB Prevention
Patient
• Patient feels well
• Perception of risk: uncertain and not urgent
• Worried about medicine side effects
Provider
• Not considered important clinical problem
• Unclear who to test/treat
• Suboptimal tests/treatment options
23

Opportunities for TB Prevention
in College Setting
• Young healthy adults
• Student enrollment procedures may
facilitate screening
• Recent testing and treatment advances
(specific test, shorter treatment)
• Can be monitored through treatment
• Risk of TB spread in dorm and classroom
setting is a motivating factor
24

Part 1: Key Points
• Most TB cases in the U.S. are due to
reactivation of LTBI and are preventable
• TB disease continues to cause death
• TB disease disproportionately affects the
foreign-born
• Latent TB infection is nearly 10 X higher in
foreign-born
• Historical barriers have impeded LTBI treatment
adoption in many practice settings
25

What are the effective strategies
for detection and treatment?
26

What is Risk-based Testing?
• Only test patients who have “TB risk
factors”
• Treatment decisions routine:
“A decision to test is a decision to
treat”
CDC, MMWR, 2000 27

Why not Test Everyone?
• Testing populations with low prevalence
will result in many false-positive results
• Among low-risk U.S.-born patients:
Miramontes, PLOS One, 2015
Pai, Clin Micro Rev, 2014
Prevalence of
latent TB
infection
False-positive
rate
2.8% 46%
28

U.S. Preventive Services Task Force
Population
Adults who are at increased risk for tuberculosis:
• persons born in, or former residents of, countries with
increased tuberculosis prevalence
• persons who live in, or have lived in, high-risk congregate
settings (such as homeless shelters and correctional
facilities)March 2016. http://www.uspreventiveservicestaskforce.org/Page/Document/draft-recommendation-
statement144/latent-tuberculosis-infection-screening
Recommendation Grade
The USPSTF recommends screening for
latent tuberculosis infection (LTBI) in
populations that are at increased risk.
29

California Tuberculosis Risk Assessment
A tuberculosis (TB) screening tool for College and University Students
Check appropriate risk factor boxes below. LTBI testing is recommended if any of the 5 boxes below are checked.
o Foreign-born person from a country with an elevated TB prevalence All countries within Africa, Asia/Pacific, Eastern Europe (including Russia), Latin America (including Mexico)
Interferon Gamma Release Assay (IGRA) is preferred over Tuberculin Skin Test (TST) for foreign-born persons.
o Current or planned immunosuppressionHIV infection, organ transplant recipient, treated with TNF-alpha antagonist (e.g., infliximab, etanercept, others), steroids (equivalent of
prednisone ≥15 mg/day for ≥1 month) or other immunosuppressive medication
o Close contact to someone with infectious active TB disease at any time
o Volunteered, worked or lived in a healthcare, homeless or correctional facility
o Travel or residence of > 1 month in a country with an elevated TB prevalence All countries within Africa, Asia/Pacific, Eastern Europe (including Russia), Latin America (including Mexico)
If LTBI test result is positive and active TB disease is ruled out, LTBI treatment is recommended.
DRAFT

Tuberculin Skin Test (TST)
• Delayed-type hypersensitivity reaction
• How to read: – Measure induration (not
erythema) at 48-72 hrs
– Record millimeters
• Positive test:– ≥ 5mm for immunosuppressed
including HIV, recent contacts
– ≥ 10mm for all others with TB risk
31

Interferon-Gamma Release Assays
(IGRAs)• QuantiFERON®-TB Gold (QFT)
– Reported as positive, negative, or
indeterminate
• T-SPOT.TB (T-Spot)
– Reported as positive, borderline, negative, or
indeterminate
32

IGRA advantages
• Advantages over TST
– Not affected by BCG vaccination
– Not affected by most non-tuberculous
mycobacteria
– Interpretation is more objective
– No return visit needed for test interpretation
– Patients and providers may lack confidence in
TST results
CDC, MMWR, 2010 | Pai, Clin Micro Rev, 2014 33

TST and QFT Specificity
Specificity95%
confidence
interval
TST without
BCG97 95–99
TST with BCG 59 46–73
QFT 96 94–98
Menzies, Ann Intern Med, 2007
Pai, Ann Intern Med, 2008 34

Testing Foreign-Born Patients
• Using a test with poor specificity will result in
many false-positive results
• Among foreign-born patients with prevalence 16%:
Pai, Clin Micro Rev, 2014
Miramontes, PLOS One, 2015
Test False-positive
rate
QFT 12%
TST 73%
35

Diagnosing Latent TB Infection
• TSTs and IGRAs cannot distinguish between
latent TB infection and active TB disease
• Active TB disease must be evaluated if
IGRA or TST is positive
Positive
TST or IGRA
Latent TB
infection
Active TB
disease
? ?
36

Rule out Active Disease Before
Starting LTBI Treatment!
• Symptom screen + chest radiograph
• If abnormal collect sputum:
1.AFB smear and culture
2.TB PCR/NAAT
• If sputum collected:
– Either start empiric treatment for active
disease
– Or await final culture results before starting
LTBI Rx 37

Part 2: Key Points
• Either IGRA or TST can aid in the
diagnosis of latent TB infection
• Neither test can distinguish between latent
TB infection and active TB disease
• IGRAs have advantages over TST in
foreign-born (BCG vaccinated)
38

LTBI Treatment Regimens
39

Treatment Regimens for
Latent TB Infection
Medication(s) Frequency Duration Doses
Isonizaid (INH) Daily6–9
months180 - 270
Rifampin Daily 4 months(vs 3months)
120
Rifapentine
(RPT) + INHWeekly 3 months 12
40
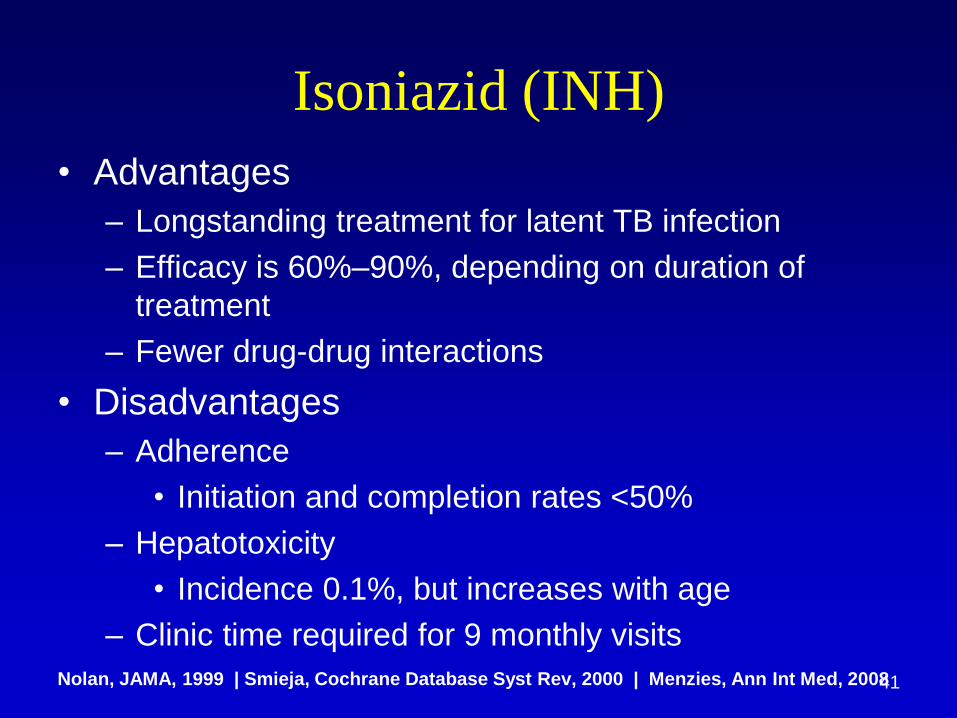
Isoniazid (INH)
• Advantages
– Longstanding treatment for latent TB infection
– Efficacy is 60%–90%, depending on duration of
treatment
– Fewer drug-drug interactions
• Disadvantages
– Adherence
• Initiation and completion rates <50%
– Hepatotoxicity
• Incidence 0.1%, but increases with age
– Clinic time required for 9 monthly visits
Nolan, JAMA, 1999 | Smieja, Cochrane Database Syst Rev, 2000 | Menzies, Ann Int Med, 200841

Rifampin
• Advantages:
– Less hepatotoxicity (~5x less than INH)
– Greater adherence (78% RIF vs. 60% INH)
• Disadvantages:
– Less evidence of efficacy
– Multiple drug interactions
• Warfarin, oral contraceptives, methadone,
protease inhibitors
Hong Kong Chest Service/Tuberculosis Research Centre, Am Rev Respir Dis, 1992
Villarino, Am J Respir Crit Care Med, 1997 | Menzies, Ann Intern Med, 2008 42

Sterling, NEJM, 2011
INH-RPT INH
No. of
patients3,986 3,745
Frequency Weekly Daily
Duration 3 months 9 months
Administrati
onDirectly-observed Self-administered
43

Prevent TB Study Results
INH-RPT INH P-value
Effectiveness 1.9 per 1,000 4.3 per 1,000Non-
inferior
Completion 82.1% 69.0% P<0.001
Hepatotoxicity 0.4% 2.7% P<0.001
Sterling, NEJM, 2011 44
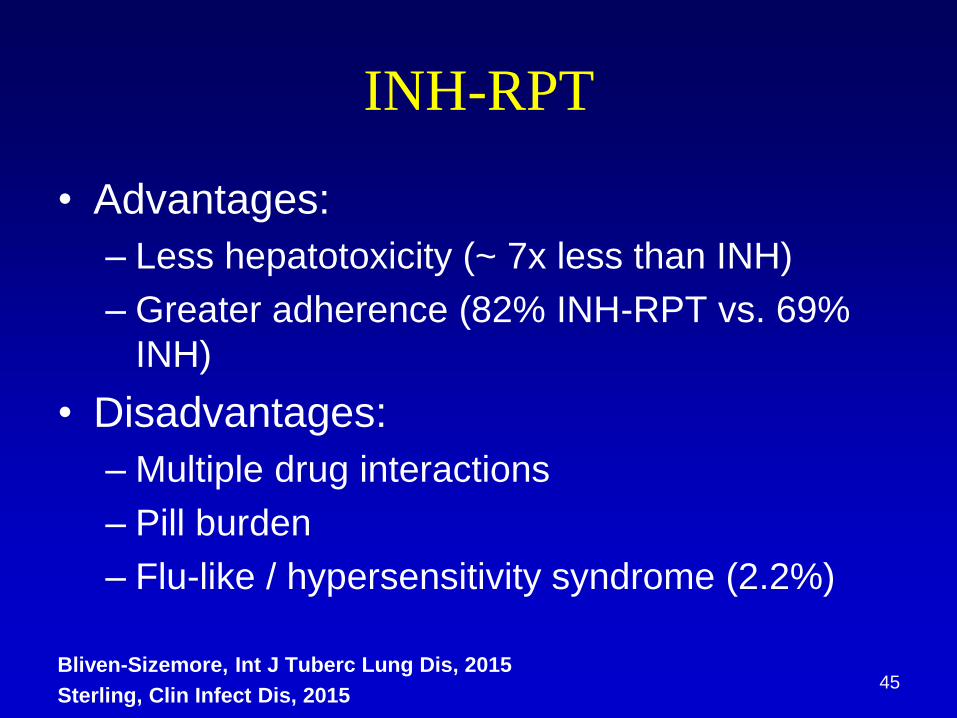
INH-RPT
• Advantages:
– Less hepatotoxicity (~ 7x less than INH)
– Greater adherence (82% INH-RPT vs. 69%
INH)
• Disadvantages:
– Multiple drug interactions
– Pill burden
– Flu-like / hypersensitivity syndrome (2.2%)
Bliven-Sizemore, Int J Tuberc Lung Dis, 2015
Sterling, Clin Infect Dis, 201545

Part 3: Key Points
• INH has been front line drug, but has low
treatment initiation and completion rates
• Short course regimens now preferred
given higher completion rates and lower
hepatotoxity
• INH-RPT (12 doses) is as efficacious as
INH (9 months)
46

TB Diagnosis
47

Clinical Presentation:
Signs and Symptoms
Cough (dry/productive sputum) 75-80%
Weight loss 45-75%
Fatigue 60-70%
Fever 50-60%
Night sweats 50-55%
Hemoptysis 25-35%
Pleuritic chest pain
No symptoms 10-20%
Barnes 1988, Miller 2000
48

Radiographic Patterns of
Pulmonary TB
Pattern
Infiltrate Majority of Cases (80%)
85% upper
Cavitation Minority of Cases (20%)Rare in children and
primary TB
Adenopathy Uncommon
More common in children
and primary TB
Effusion May be present
49

Sputum AFB smear
• Smear positive ≥ 104 bacilli per ml
• Smear AFB amount correlates with infectiousness
• 40-60% of culture positive cases will be smear negative
Three smear negative specimens
does not “rule out” TB!
50

What is the Added Value of NAAT?
• For AFB smear (–):
– 50-70% of smear –/culture + cases will be + by
NAAT start treatment (earlier)
– If NAAT (–), the likelihood of TB lower• Release from isolation earlier (2 Xpert results finds all smear +)
• Still start treatment if suspicion is high
• For AFB smear (+):
– NAAT can confirm TB quickly
– If NAAT negative, prevent falsely diagnosing TB(likely NTM if inhibitors are ruled out and result repeated)
Luetkemeyer Clin Infect Dis 2016 51

Xpert MTB/RIF Test Performance
Compared with Culture, U.S. Patients
Sensitivity Specificity
1 Xpert 2 Xperts
Smear (+) 96.7%(59/61)
100%(62/62)
99.2%Smear (–) 59.3%
(16/27)
71.4%(20/28)
Luetkemeyer Clin Infect Dis 2016 52

Use of NAATs!
• NAAT should be used unless results
would not impact clinical or public health
management
• Xpert results showing Rif resistance
should:
– Be confirmed using sequencing and/or culture
– Trigger suspicion for MDR TB (not Rif
monoR)
CDC MMWR October 18, 2013 / 62(41);821-82453
Part 4: Key Points
• Most but not all patients have TB
symptoms
• Most patients do not have a cavity on CXR
• Use NAATs
• Clinical suspicion is crucial don’t be
afraid of empiric TB treatment
• Discuss with state/local TB control
program
54

Summary
• Most TB cases in the U.S. are preventable
• TB disease persists as a cause of
preventable morbidity and mortality
• College students should have risk-base
testing and treated if positive
• Foreign birth/travel, immunosuppressed,
TB contact are the main risks for TB
55

Summary
• Both IGRAs or TSTs can be used to
support the diagnosis of latent TB infection
• Neither test can distinguish between latent
TB infection and active TB disease
• IGRAs have advantages over TST in
foreign-born (BCG vaccinated)
56

Summary: How to treat?
• Short course regimens have higher
completion rates and are less hepatotoxic
• INH has very low treatment completion
rates
• INH-RPT (3 months) is as efficacious as
INH (9 months)
57

TB Elimination is achievable
• New tools can help simplify and improve
management of latent TB infection
1. Simple TB risk assessment
2. IGRAs
3. Short course regimens
58

59

Thank you!
60

Acknowledgements
• Pennan Barry
• Joanna Lu
• Neha Shah
• Jim Scott
61
Resources to look forward to:
• ATS/IDSA/CDC LTBI guidelines
• NTCA companion document
• ATS diagnostic standards
• Up to Date revisions
62