Embed Size (px)
Citation preview
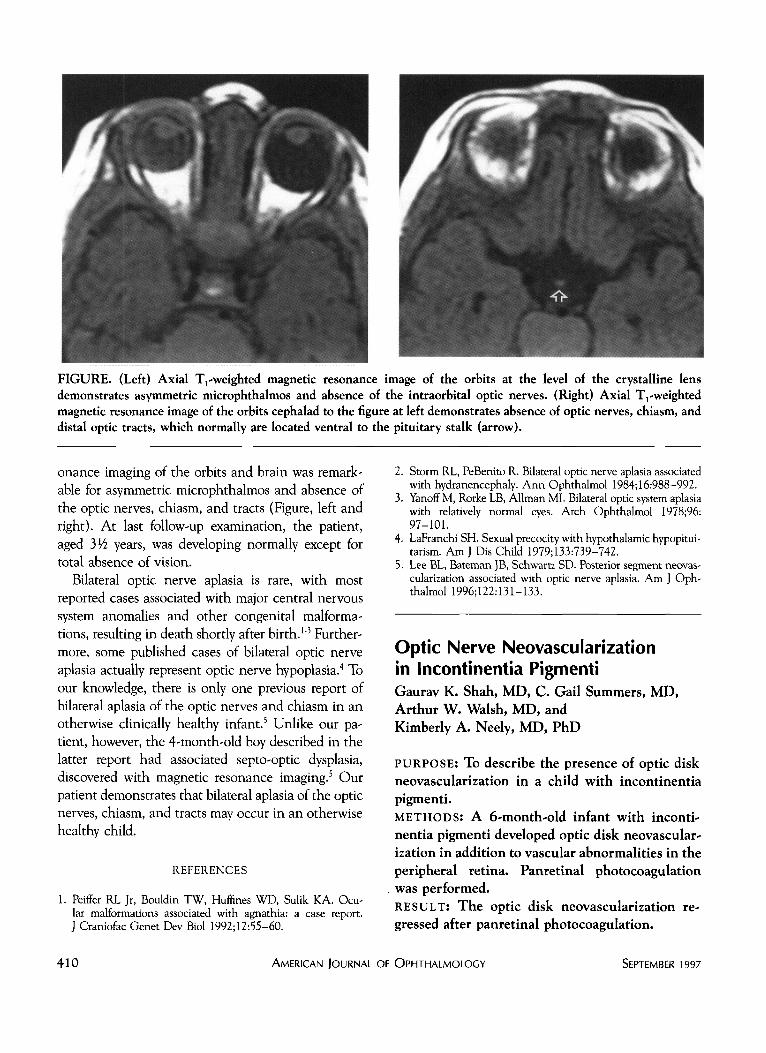
FIGURE. (Left) Axial ^-weighted magnetic resonance image of the orbits at the level of the crystalline lens demonstrates asymmetric microphthalmos and absence of the intraorbital optic nerves. (Right) Axial Tj-weighted magnetic resonance image of the orbits cephalad to the figure at left demonstrates absence of optic nerves, chiasm, and distal optic tracts, which normally are located ventral to the pituitary stalk (arrow).
onance imaging of the orbits and brain was remarkable for asymmetric microphthalmos and absence of the optic nerves, chiasm, and tracts (Figure, left and right). At last follow-up examination, the patient, aged 3lA years, was developing normally except for total absence of vision.
Bilateral optic nerve aplasia is rare, with most reported cases associated with major central nervous system anomalies and other congenital malformations, resulting in death shortly after birth.1'3 Furthermore, some published cases of bilateral optic nerve aplasia actually represent optic nerve hypoplasia.4 To our knowledge, there is only one previous report of bilateral aplasia of the optic nerves and chiasm in an otherwise clinically healthy infant.5 Unlike our patient, however, the 4-month-old boy described in the latter report had associated septo-optic dysplasia, discovered with magnetic resonance imaging.5 Our patient demonstrates that bilateral aplasia of the optic nerves, chiasm, and tracts may occur in an otherwise healthy child.
REFERENCES
1. Peiffer RL Jr, Bouldin TW, Huffines WD, Sulik KA. Ocular malformations associated with agnathia: a case report. J Craniofac Genet Dev Biol 1992;12:55-60.
2. Storm RL, PeBenito R. Bilateral optic nerve aplasia associated with hydranencephaly. Ann Ophthalmol 1984;16:988-992.
3. Yanoff M, Rorke LB, Allman MI. Bilateral optic system aplasia with relatively normal eyes. Arch Ophthalmol 1978;96: 97-101.
4. LaFranchi SH. Sexual precocity with hypothalamic hypopitui-tarism. AmJ Dis Child 1979;133:739-742.
5. Lee BL, Bateman JB, Schwartz SD. Posterior segment neovas-cularization associated with optic nerve aplasia. Am J Ophthalmol 1996;122:131-133.
Optic Nerve Neovascularization in Incontinentia Pigmenti Gaurav K. Shah, MD, C. Gail Summers, MD, Arthur W. Walsh, MD, and Kimberly A. Neely, MD, PhD
PURPOSE: To describe the presence of optic disk neovascularization in a child with incontinentia pigmenti. METHODS: A 6-month-old infant with incontinentia pigmenti developed optic disk neovascularization in addition to vascular abnormalities in the peripheral retina. Panretinal photocoagulation was performed. RESULT: The optic disk neovascularization regressed after panretinal photocoagulation.
410 AMERICAN JOURNAL OF OPHTHALMOLOGY SEPTEMBER 1997
CONCLUSIONS: Optic disk neovascularization is another notable retinal manifestation of incon-tinentia pigmenti. When optic disk neovascularization is detected, retinal ablation should be considered as treatment.
OPTIC DISK NEOVASCULARIZATION HAS RECEIVED minimal attention in previous descriptions of
posterior segment findings in incontinentia pigmenti. The findings in our patient show that optic disk neovascularization can occur in patients with incontinentia pigmenti.
A 6-month-old infant was referred to us for evaluation of an alternating esotropia. Born full term, the patient had blisters on her fingers and toes. Two days after birth, she developed a rash that later became verrucous. Her mother had incontinentia pigmenti and had previously spontaneously aborted a male fetus.
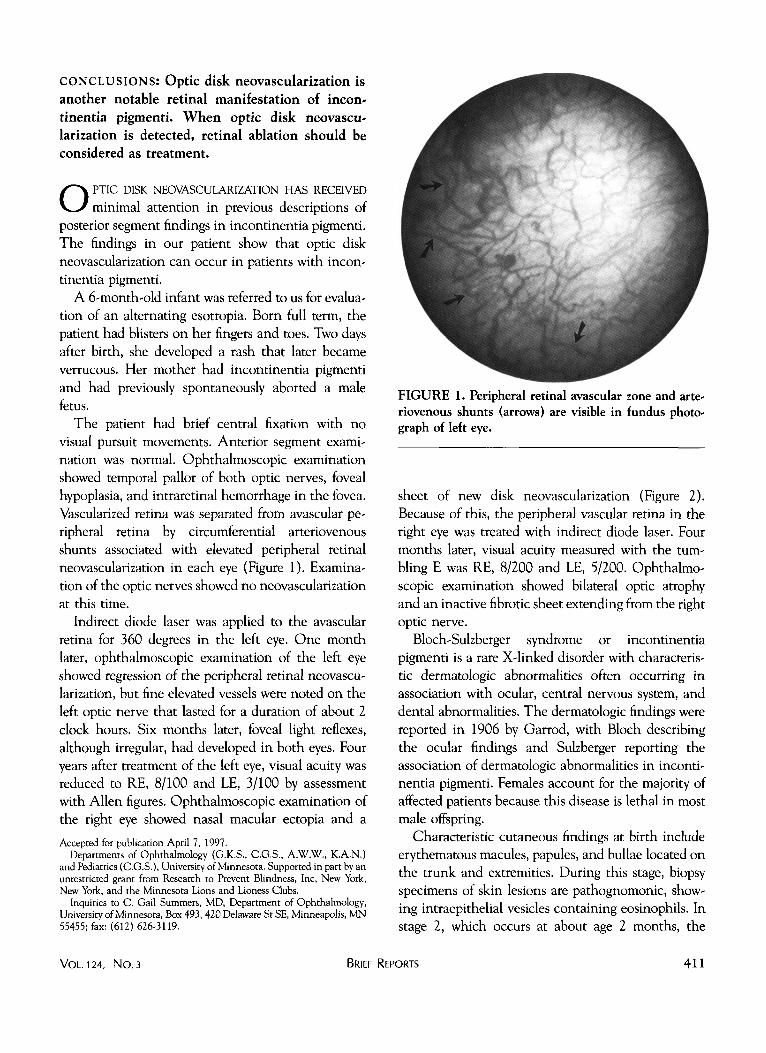
The patient had brief central fixation with no visual pursuit movements. Anterior segment examination was normal. Ophthalmoscopic examination showed temporal pallor of both optic nerves, foveal hypoplasia, and intraretinal hemorrhage in the fovea. Vascularized retina was separated from avascular peripheral retina by circumferential arteriovenous shunts associated with elevated peripheral retinal neovascularization in each eye (Figure 1). Examination of the optic nerves showed no neovascularization at this time.
Indirect diode laser was applied to the avascular retina for 360 degrees in the left eye. One month later, ophthalmoscopic examination of the left eye showed regression of the peripheral retinal neovascularization, but fine elevated vessels were noted on the left optic nerve that lasted for a duration of about 2 clock hours. Six months later, foveal light reflexes, although irregular, had developed in both eyes. Four years after treatment of the left eye, visual acuity was reduced to RE, 8/100 and LE, 3/100 by assessment with Allen figures. Ophthalmoscopic examination of the right eye showed nasal macular ectopia and a
Accepted for publication April 7, 1997. Departments of Ophthalmology (G.K.S., C O S . , A.W.W., K.A.N.)
and Pediatrics (COS.), University of Minnesota. Supported in part by an unrestricted grant from Research to Prevent Blindness, Inc, New York, New York, and the Minnesota Lions and Lioness Clubs.
Inquities to C. Gail Summers, MD, Department of Ophthalmology, University of Minnesota, Box 493, 420 Delaware St SE, Minneapolis, MN 55455; fax: (612) 626-3119.
VOL.124, No. 3 BRIEF
FIGURE 1. Peripheral retinal avascular zone and arteriovenous shunts (arrows) are visible in fundus photograph of left eye.
sheet of new disk neovascularization (Figure 2). Because of this, the peripheral vascular retina in the right eye was treated with indirect diode laser. Four months later, visual acuity measured with the tumbling E was RE, 8/200 and LE, 5/200. Ophthalmoscopic examination showed bilateral optic atrophy and an inactive fibrotic sheet extending from the right optic nerve.
Bloch-Sulzberger syndrome or incontinentia pigmenti is a rare X-linked disorder with characteristic dermatologic abnormalities often occurring in association with ocular, central nervous system, and dental abnormalities. The dermatologic findings were reported in 1906 by Garrod, with Bloch describing the ocular findings and Sulzberger reporting the association of dermatologic abnormalities in incontinentia pigmenti. Females account for the majority of affected patients because this disease is lethal in most male offspring.
Characteristic cutaneous findings at birth include erythematous macules, papules, and bullae located on the trunk and extremities. During this stage, biopsy specimens of skin lesions are pathognomonic, showing intraepithelial vesicles containing eosinophils. In stage 2, which occurs at about age 2 months, the
REPORTS 411
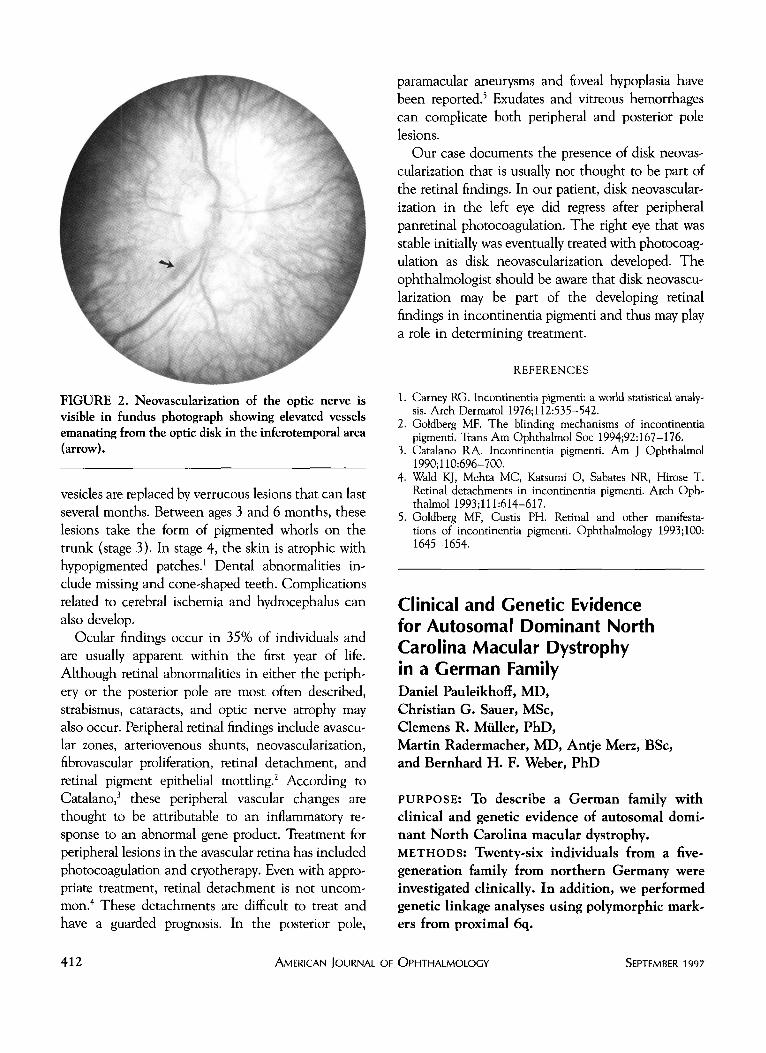
FIGURE 2. Neovascularization of the optic nerve is visible in fundus photograph showing elevated vessels emanating from the optic disk in the inferotemporal area (arrow).
vesicles are replaced by verrucous lesions that can last several months. Between ages 3 and 6 months, these lesions take the form of pigmented whorls on the trunk (stage 3). In stage 4, the skin is atrophic with hypopigmented patches.1 Dental abnormalities include missing and cone-shaped teeth. Complications related to cerebral ischemia and hydrocephalus can also develop.
Ocular findings occur in 35% of individuals and are usually apparent within the first year of life. Although retinal abnormalities in either the periphery or the posterior pole are most often described, strabismus, cataracts, and optic nerve atrophy may also occur. Peripheral retinal findings include avascu-lar zones, arteriovenous shunts, neovascularization, fibrovascular proliferation, retinal detachment, and retinal pigment epithelial mottling.2 According to Catalano,3 these peripheral vascular changes are thought to be attributable to an inflammatory response to an abnormal gene product. Treatment for peripheral lesions in the avascular retina has included photocoagulation and cryotherapy. Even with appropriate treatment, retinal detachment is not uncommon.4 These detachments are difficult to treat and have a guarded prognosis. In the posterior pole,
412 AMERICAN JOURNAL
paramacular aneurysms and foveal hypoplasia have been reported.5 Exudates and vitreous hemorrhages can complicate both peripheral and posterior pole lesions.
Our case documents the presence of disk neovascularization that is usually not thought to be part of the retinal findings. In our patient, disk neovascularization in the left eye did regress after peripheral panretinal photocoagulation. The right eye that was stable initially was eventually treated with photocoagulation as disk neovascularization developed. The ophthalmologist should be aware that disk neovascularization may be part of the developing retinal findings in incontinentia pigmenti and thus may play a role in determining treatment.
REFERENCES
1. Carney RG. Incontinentia pigmenti: a world statistical analysis. Arch Dermatol 1976;112:535-542.
2. Goldberg ME The blinding mechanisms of incontinentia pigmenti. Trans Am Ophthalmol Soc 1994;92:167-176.
3. Catalano RA. Incontinentia pigmenti. Am J Ophthalmol 1990;110:696-700.
4. Wald KJ, Mehta MC, Katsumi O, Sabates NR, Hirose T. Retinal detachments in incontinentia pigmenti. Arch Ophthalmol 1993;111:614-617.
5. Goldberg MF, Custis PH. Retinal and other manifestations of incontinentia pigmenti. Ophthalmology 1993;100: 1645-1654-
Clinical and Genetic Evidence for Autosomal Dominant North Carolina Macular Dystrophy in a German Family Daniel Pauleikhoff, MD, Christian G. Sauer, MSc, Clemens R. Miiller, PhD, Martin Radermacher, MD, Antje Merz, BSc, and Bernhard H. F. Weber, PhD
PURPOSE: To describe a German family with clinical and genetic evidence of autosomal dominant North Carolina macular dystrophy. METHODS: Twenty-six individuals from a five-generation family from northern Germany were investigated clinically. In addition, we performed genetic linkage analyses using polymorphic markers from proximal 6q.
OPHTHALMOLOGY SEPTEMBER 1997





























