Embed Size (px)
Citation preview

Jill Cowper, Pharm.D.Division Infectious Diseases Pharmacist
Parallon Supply Chain SolutionsRichmond, VAP: 607‐221‐5101
Optimize Durations of Antimicrobial Therapy
Evidence & Application
Disclosure
I have no relevant finances to disclose.
Objectives
Explain the importance of optimizing durations of antibiotic therapy Describe evidence supporting shorter durations of therapy for infectious indications Discuss an initiative to optimize durations of antibiotic therapy Demonstrate improvements in durations of antibiotic therapy
Audience Question
Who has implemented a process that requires indications and durations for
every antibiotic order?
Optimizing Antimicrobial Therapy
Optimal efficacy & safety of antimicrobials depends on the following: Avoiding them when they’re not indicated The 4 “Ds” of optimal therapy
1. Right Drug2. Right Dose3. De‐escalation to pathogen‐directed therapy4. Right Duration
File TM. J Hosp Med 2012.

Durations of Antimicrobials – The Problem
False perception that more is better Durations ordered per indication at a 506‐bed HCA facility:
Average Min Max Recommended or data supporting DOT
C. difficile 10 7 28 10‐14CAP 8 3 21 5HAP 8 5 14 7COPD exacerbation 7 3 20 ≤ 5Intra‐abdominal 9 3 15 4Skin and soft tissue 8 3 28 5‐6Upper respiratory infection 7 3 42 5UTI 7 3 28 3‐uncomplicated
7‐14 ‐ complicatedSpellberg B. JAMA Intern Med 2016.
Why is this Important?

Importance of Durations of Antimicrobials
Longer courses of antibiotic therapy lead to moreresistance development
Short‐course Long‐course P‐valueSingh et al. 5/37 (15%) 14/37 (35%) 0.017
Chastre et al. 24/57(42.1%) 33/53 (62.3%) 0.04
Singh, et al. Am J Respir Crit Care Med 2000; Chastre, et al. JAMA 2003.
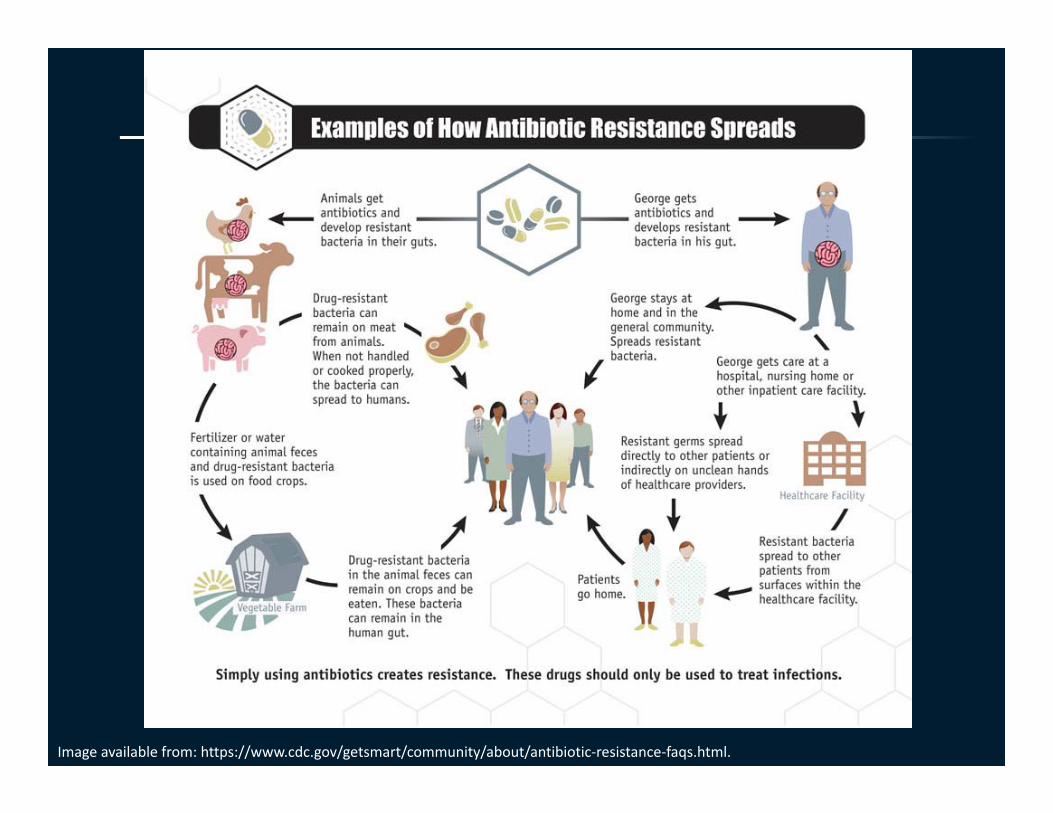
Image available from: https://www.cdc.gov/getsmart/community/about/antibiotic‐resistance‐faqs.html.
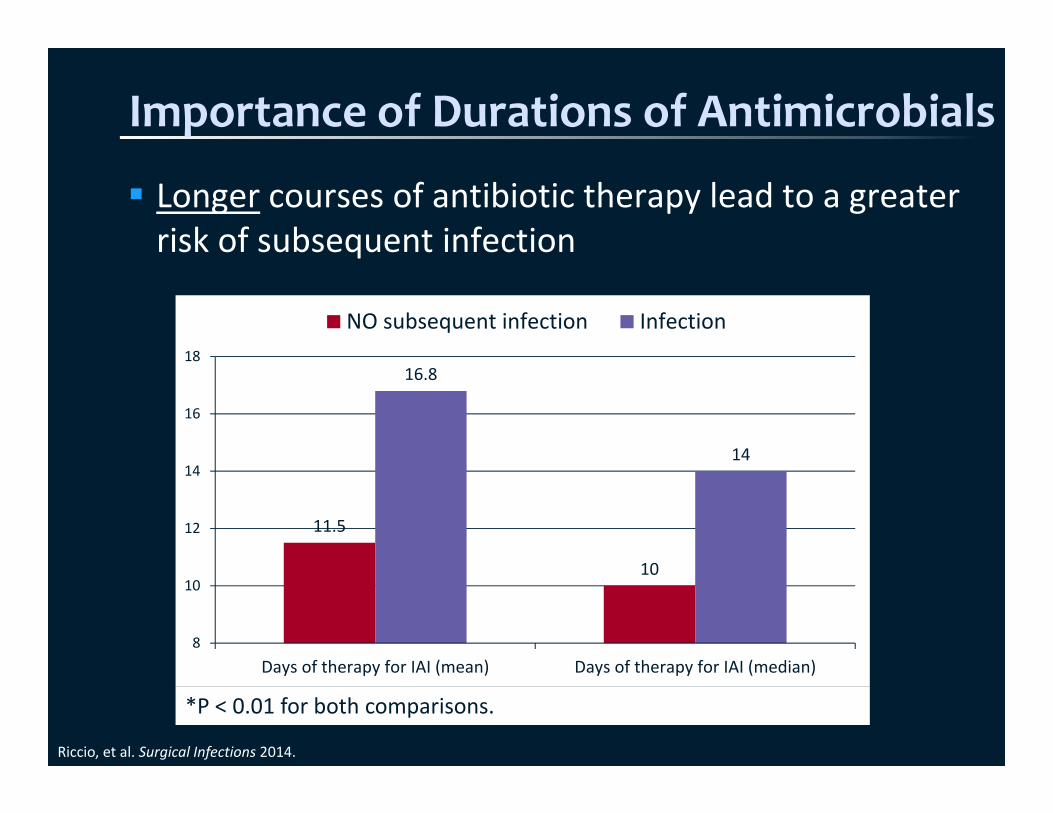
Importance of Durations of Antimicrobials
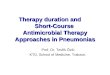
Longer courses of antibiotic therapy lead to a greater risk of subsequent infection
Riccio, et al. Surgical Infections 2014.
11.5
10
16.8
14
8
10
12
14
16
18
Days of therapy for IAI (mean) Days of therapy for IAI (median)
NO subsequent infection Infection
*P < 0.01 for both comparisons.
Importance of Durations of Antimicrobials
Longer courses of antibiotic therapy lead to a greater risk of side effects
Image available from: https://www.cdc.gov/drugresistance/protecting_yourself_family.html.

Importance of Durations of Antimicrobials
C. difficile risk increases with increasing duration of antibiotic therapy
Stevens, et al. Clin Infect Dis 2011.
Audience Question
Why is it important to optimize durations of antimicrobial therapy?A. Excessive durations of therapy lead to more
resistance developmentB. Longer durations of therapy have been associated
with a greater risk of subsequent infectionC. Longer durations of therapy increase the risk of
antimicrobial‐related side effectsD. There is a dose‐response relationship between
antibiotic days of therapy and risk of C. difficileE. All of the above
Is There Evidence for Shorter Durations?
CAP – 5 vs 10 days Multicenter, randomized trial evaluating whether duration of antibiotics based on IDSA guideline criteria was just as effective as conventional therapy Intervention ‐ IDSA guideline criteria
• Minimum of 5 days• Antibiotics discontinued if afebrile for 48 hrs and had no
more than 1 CAP‐associated sign of clinical instability (SBP < 90 mm Hg, HR > 100/min, RR > 24/min, arterial O2 saturation < 90%, or PaO2 less than 60 mm Hg in room air)
Conventional therapy duration determined by treating physician
Uranga, et al. JAMA Intern Med 2016.
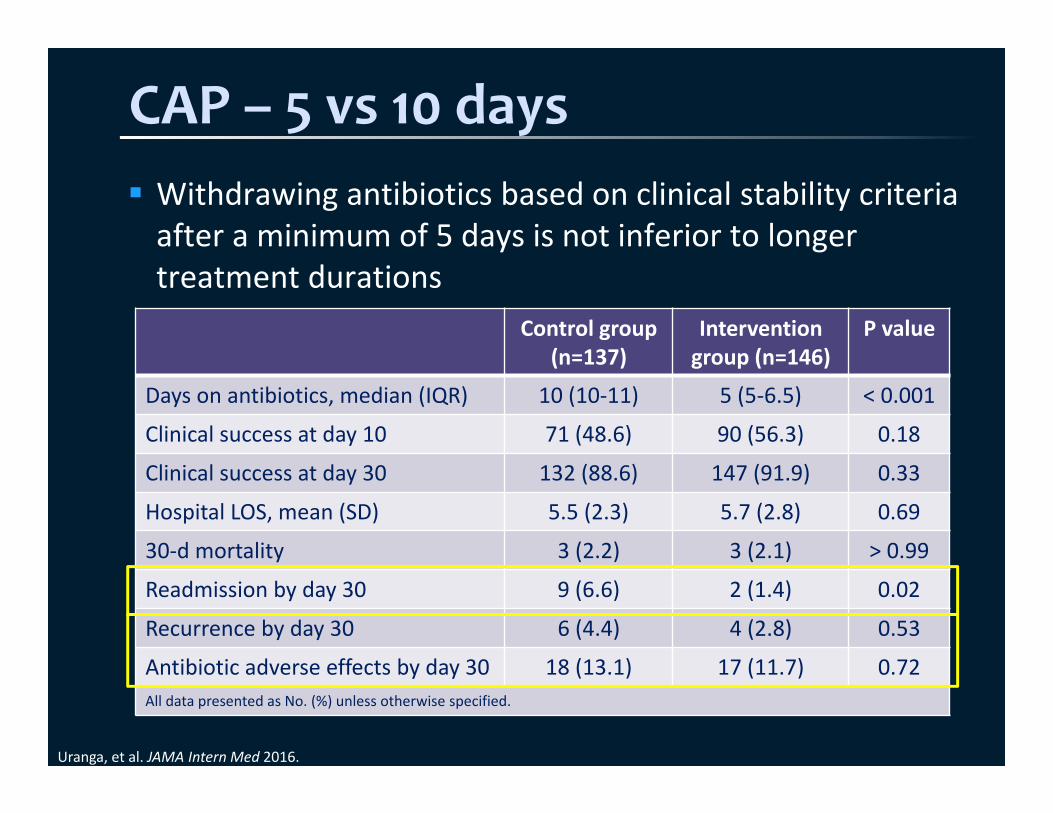
CAP – 5 vs 10 days Withdrawing antibiotics based on clinical stability criteria after a minimum of 5 days is not inferior to longer treatment durations
Uranga, et al. JAMA Intern Med 2016.
Control group (n=137)
Intervention group (n=146)
P value
Days on antibiotics, median (IQR) 10 (10‐11) 5 (5‐6.5) < 0.001
Clinical success at day 10 71 (48.6) 90 (56.3) 0.18
Clinical success at day 30 132 (88.6) 147 (91.9) 0.33
Hospital LOS, mean (SD) 5.5 (2.3) 5.7 (2.8) 0.69
30‐d mortality 3 (2.2) 3 (2.1) > 0.99
Readmission by day 30 9 (6.6) 2 (1.4) 0.02
Recurrence by day 30 6 (4.4) 4 (2.8) 0.53
Antibiotic adverse effects by day 30 18 (13.1) 17 (11.7) 0.72All data presented as No. (%) unless otherwise specified.

HAP/VAP – 7 vs 10‐15 daysPugh et al. Dimopoulos et al.
Antibiotic‐free days, mean difference (95% CI)
4.02 (2.26, 5.78) 3.40 (1.43, 5.37)
Mortality, OR (95% CI) 1.18 (0.77, 1.8) 1.20 (0.84, 1.72)
Mortality; NF‐GNB, OR (95% CI)
0.95 (0.39, 2.27) 1.33 (0.33, 5.26)
Recurrence, OR (95% CI) 1.41 (0.94, 2.12) 1.67 (0.99, 2.83)
Recurrence; NF‐GNB, OR (95% CI)
2.18 (1.14, 4.16) NA
Superinfection, OR (95% CI) 0.44 (0.21, 0.95) NA
ICU LOS, mean difference (95% CI)
0.15 (‐1.00, 1.29) 0.16 (‐0.99, 1.31)
Hospital LOS, mean difference (95% CI)
‐1.0 (‐4.11, 2.11) NA
CI, confidence interval; LOS, length of stay; NF‐GNB, non‐fermenting gram‐negative bacilli; OR, odds ratio.
Pugh R, et al. Cochrane Database Syst Rev 2015; Dimopoulos G, et al. Chest 2013.
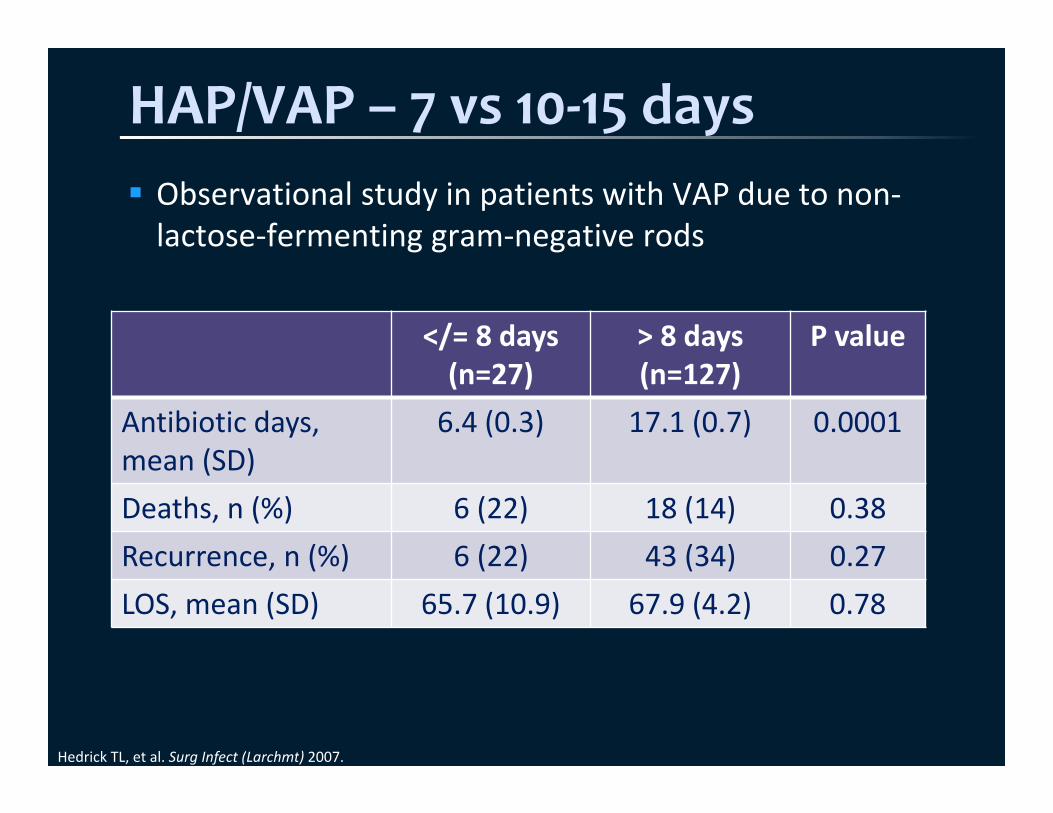
HAP/VAP – 7 vs 10‐15 days
</= 8 days(n=27)
> 8 days (n=127)
P value
Antibiotic days, mean (SD)
6.4 (0.3) 17.1 (0.7) 0.0001
Deaths, n (%) 6 (22) 18 (14) 0.38Recurrence, n (%) 6 (22) 43 (34) 0.27LOS, mean (SD) 65.7 (10.9) 67.9 (4.2) 0.78
Hedrick TL, et al. Surg Infect (Larchmt) 2007.
Observational study in patients with VAP due to non‐lactose‐fermenting gram‐negative rods
HAP/VAP – 7 vs 10‐15 days IDSA guidelines published in 2016:
• “For patients with HAP, we recommend a 7‐day course of antimicrobial therapy.”
Meta‐analysis conducted by guideline authors:• No difference between short‐ (7‐8 days) and long‐course regimens (10‐15 days)
• Non‐lactose‐fermenting gram‐negative rods: No difference in pneumonia recurrence (OR, 1.42; 95% CI, 0.66‐3.04)
No difference in mortality (OR, 0.94; 95% CI, 0.56‐1.59)
7‐day duration, regardless of pathogen
Kalil AC, et al. Clin Infect Dis 2016.
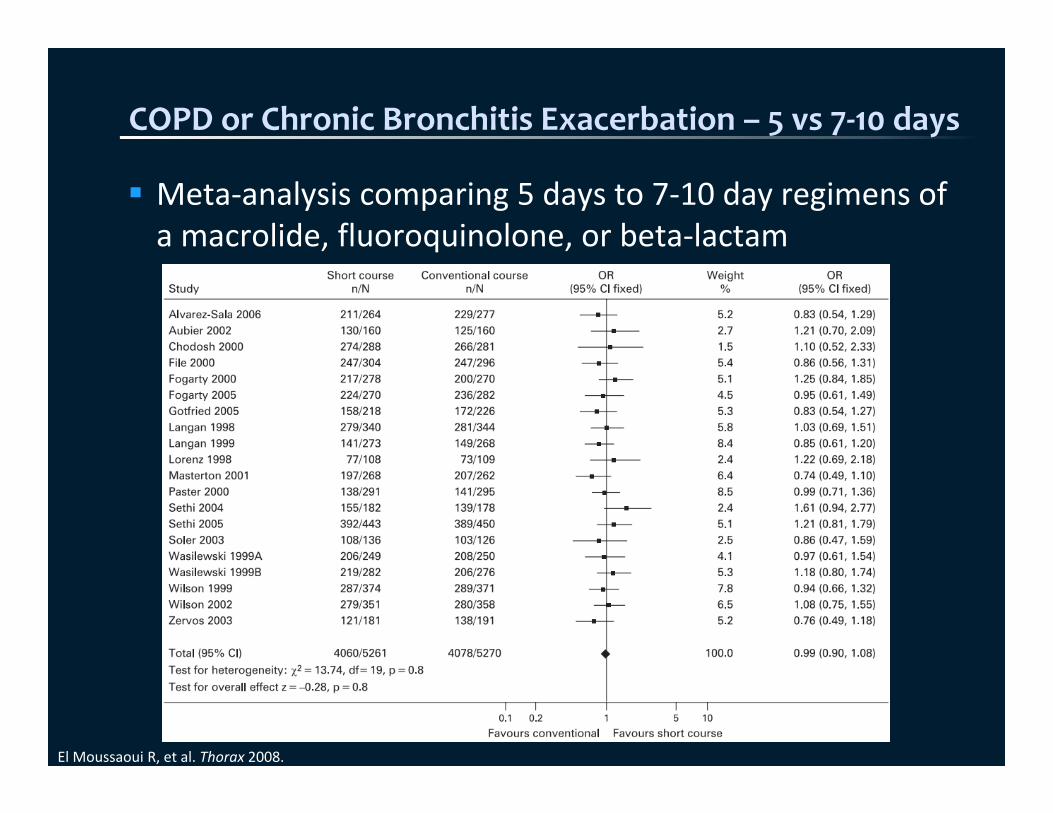
COPD or Chronic Bronchitis Exacerbation – 5 vs 7‐10 days
Meta‐analysis comparing 5 days to 7‐10 day regimens of a macrolide, fluoroquinolone, or beta‐lactam
El Moussaoui R, et al. Thorax 2008.
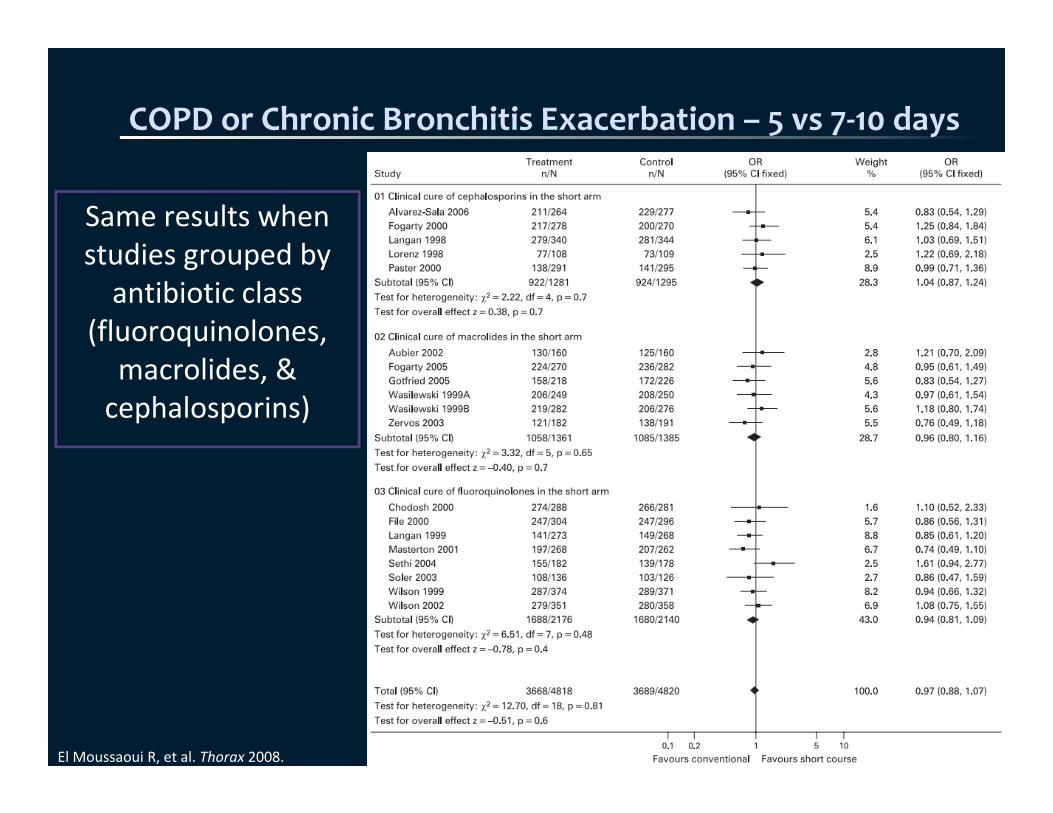
COPD or Chronic Bronchitis Exacerbation – 5 vs 7‐10 days
Same results when studies grouped by antibiotic class
(fluoroquinolones, macrolides, & cephalosporins)
El Moussaoui R, et al. Thorax 2008.
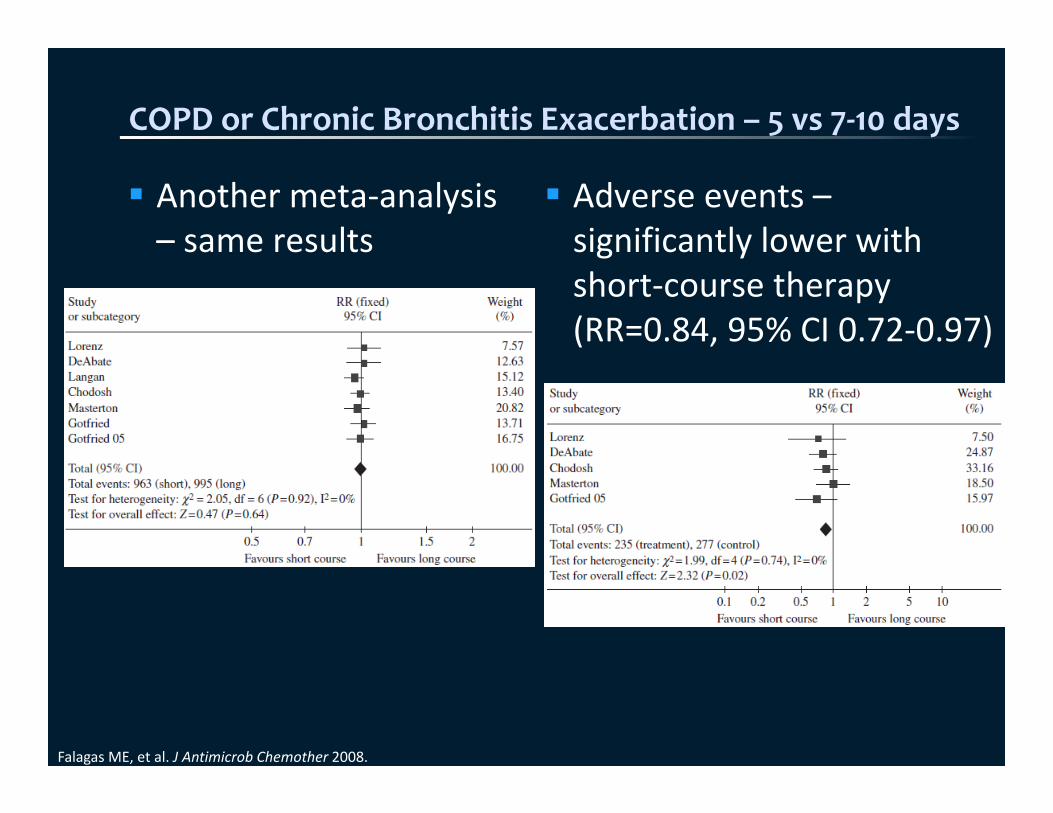
COPD or Chronic Bronchitis Exacerbation – 5 vs 7‐10 days
Falagas ME, et al. J Antimicrob Chemother 2008.
Another meta‐analysis – same results
Adverse events –significantly lower with short‐course therapy (RR=0.84, 95% CI 0.72‐0.97)

Sinusitis – 5 vs 10 days Meta‐analysis evaluating 3‐7 vs 6‐10 days
Falagas ME, et al. Br J Clin Pharmacol 2009.
Outcome (N of studies) Pooled OR (95% CI)Clinical Success3‐7 days vs 6‐10 days (N=12) 0.95 (0.81, 1.12)
Clinical Success5 days vs 10 days (N=7) 0.98 (0.79, 1.22)
Clinical SuccessBeta‐lactams (N=6) 0.95 (0.76, 1.20)
Adverse Events3‐7 days vs 6‐10 days (N=10) 0.88 (0.71, 1.09)
Adverse Events5 days vs 10 days (N=5) 0.79 (0.63, 0.98)
Intra‐Abdominal – 4 vs 10 days Multicenter, randomized, open‐label trial evaluating whether a 4‐day duration of antibiotics would lead to similar outcomes as traditional therapy Intervention – antibiotics x 4 days after source control Traditional therapy – continuing antibiotics until 2 days after resolution of SIRS‐related physiologic abnormalities (max of 10 days)• Afebrile x 1 day• WBC < 11• Ability to consume more than half of regular diet
without adverse effects
Sawyer RG, et al. N Engl J Med 2015.

Intra‐Abdominal – 4 vs 10 days No difference in primary composite outcome (surgical site infection, recurrent intraabdominal infection, or death), P=0.92• Control group – 58/260 (22.3%)• Intervention group – 56/257 (21.8%)
No difference in time to event:
Sawyer RG, et al. N Engl J Med 2015.
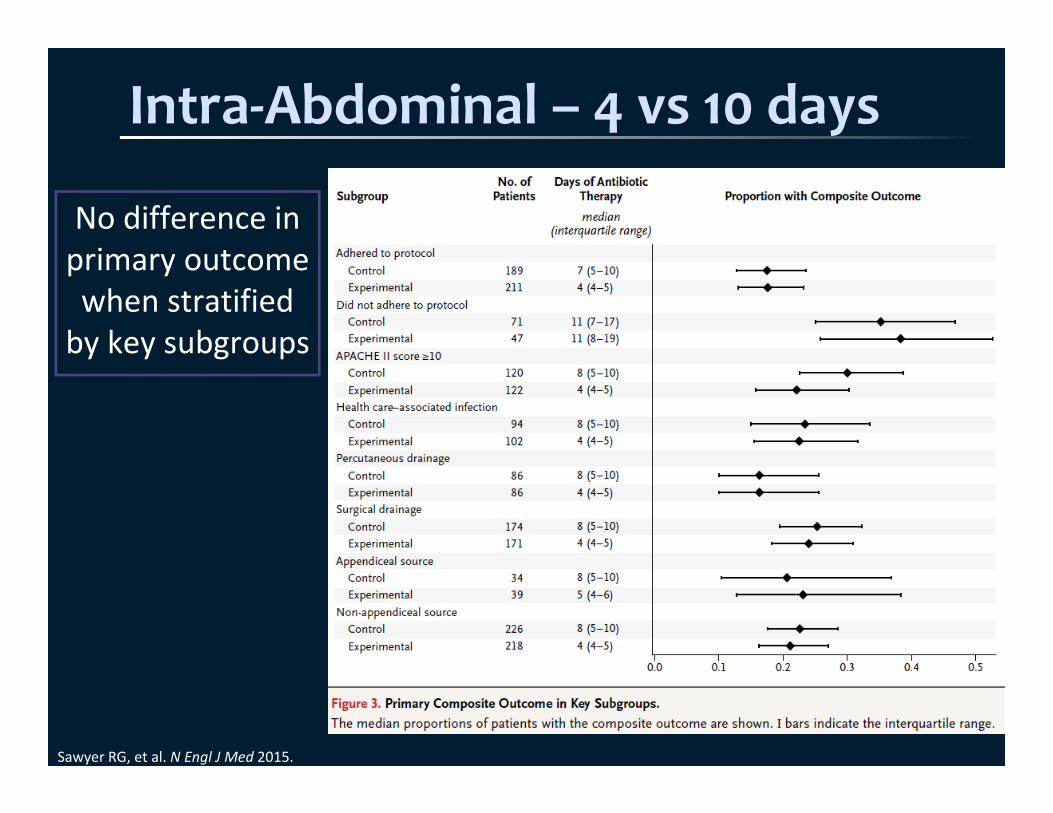
Intra‐Abdominal – 4 vs 10 days
Sawyer RG, et al. N Engl J Med 2015.
No difference in primary outcome when stratified by key subgroups
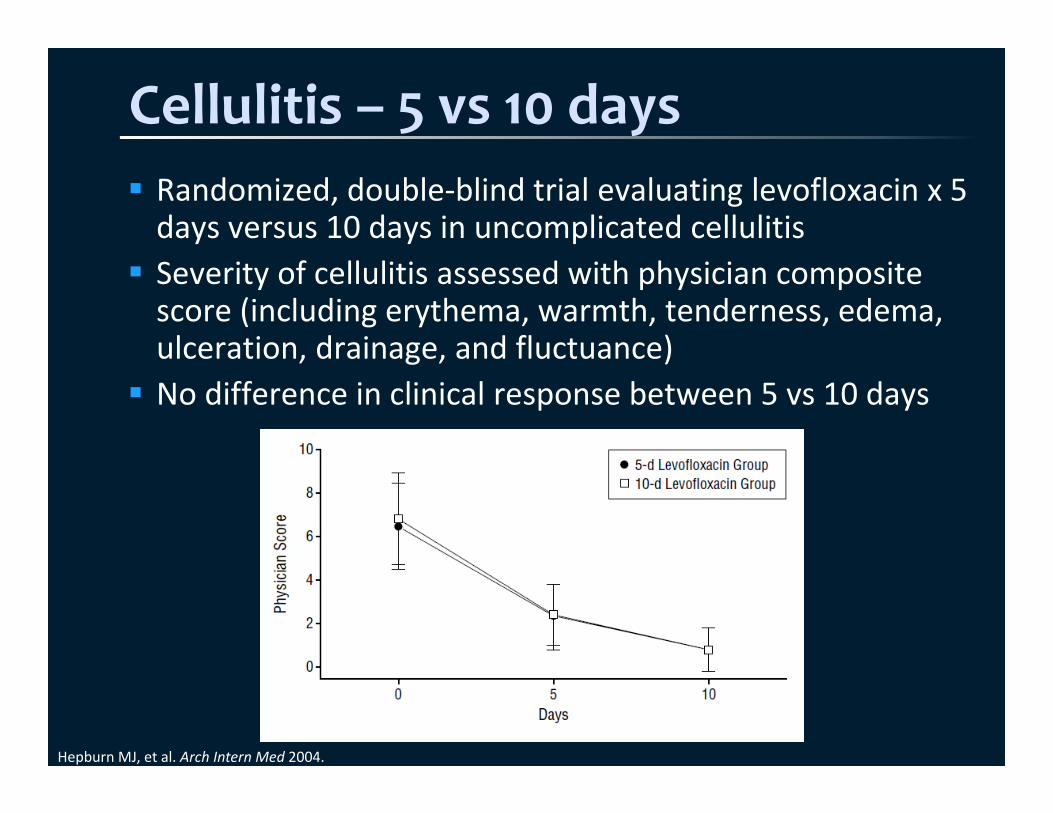
Cellulitis – 5 vs 10 days Randomized, double‐blind trial evaluating levofloxacin x 5 days versus 10 days in uncomplicated cellulitis Severity of cellulitis assessed with physician composite score (including erythema, warmth, tenderness, edema, ulceration, drainage, and fluctuance) No difference in clinical response between 5 vs 10 days
Hepburn MJ, et al. Arch Intern Med 2004.
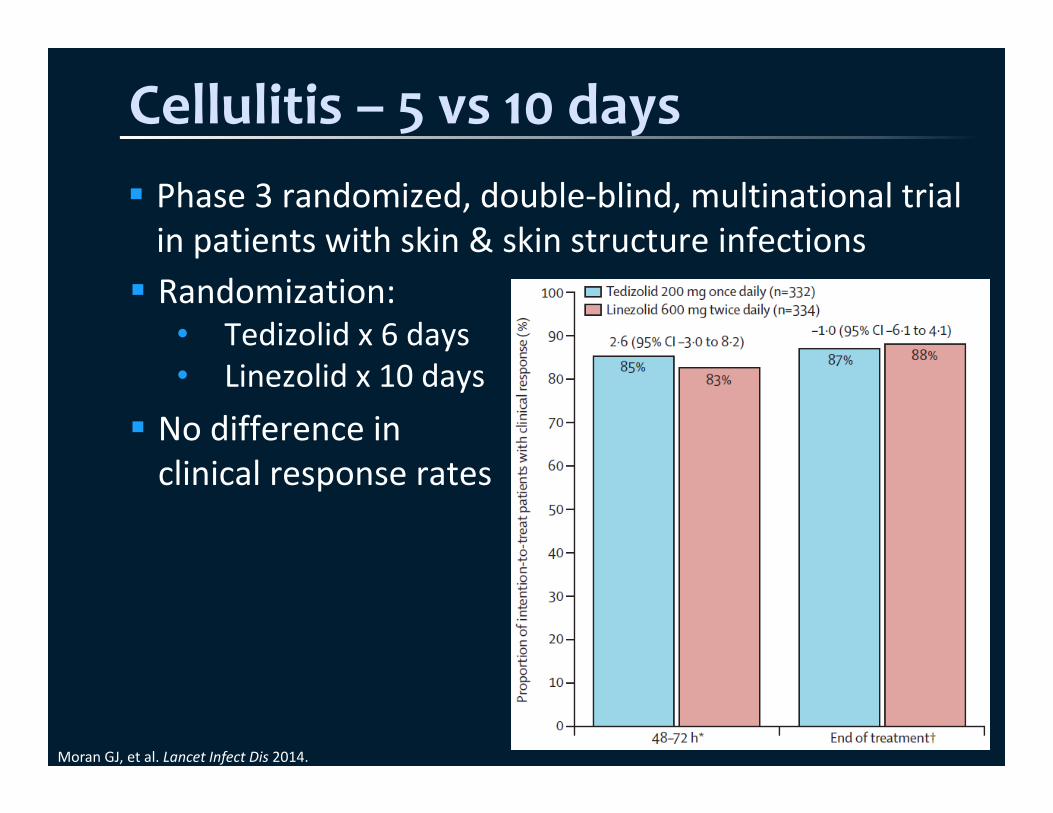
Cellulitis – 5 vs 10 days Phase 3 randomized, double‐blind, multinational trial in patients with skin & skin structure infections
Moran GJ, et al. Lancet Infect Dis 2014.
Randomization:• Tedizolid x 6 days• Linezolid x 10 days
No difference in clinical response rates
UTIs & Pyelonephritis – 5‐7 vs 10‐14 days
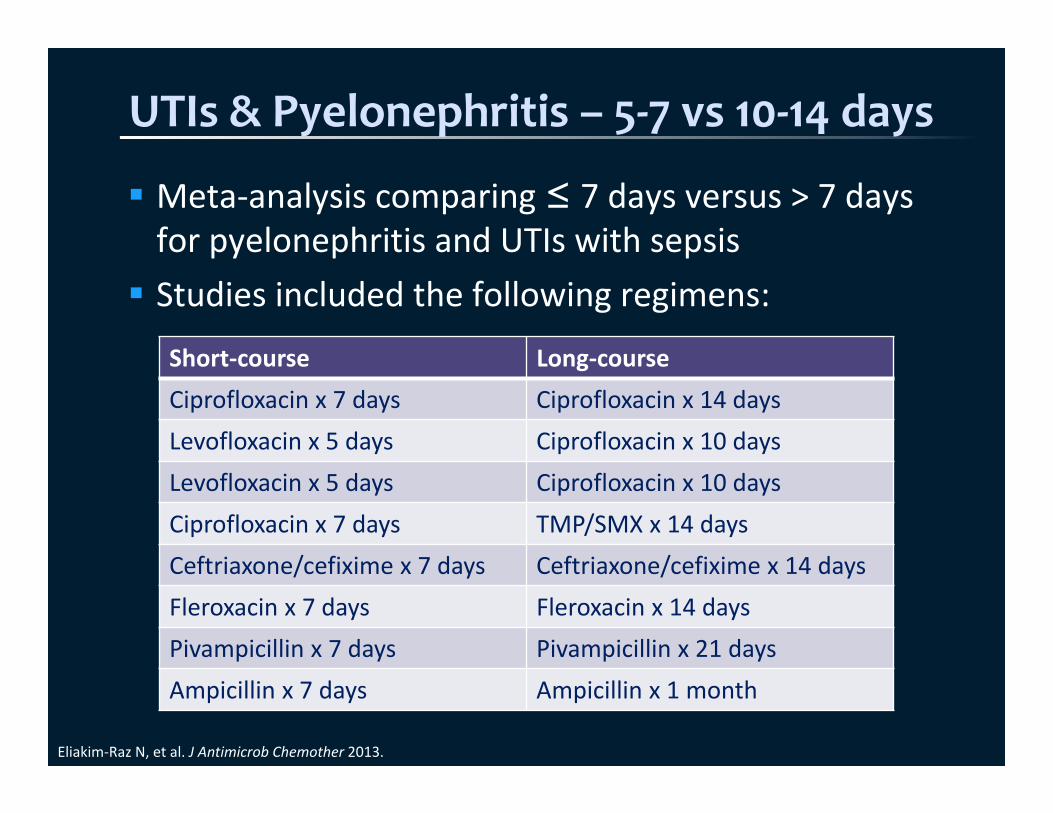
Meta‐analysis comparing ≤ 7 days versus > 7 days for pyelonephritis and UTIs with sepsis Studies included the following regimens:
Eliakim‐Raz N, et al. J Antimicrob Chemother 2013.
Short‐course Long‐courseCiprofloxacin x 7 days Ciprofloxacin x 14 daysLevofloxacin x 5 days Ciprofloxacin x 10 daysLevofloxacin x 5 days Ciprofloxacin x 10 daysCiprofloxacin x 7 days TMP/SMX x 14 daysCeftriaxone/cefixime x 7 days Ceftriaxone/cefixime x 14 daysFleroxacin x 7 days Fleroxacin x 14 daysPivampicillin x 7 days Pivampicillin x 21 daysAmpicillin x 7 days Ampicillin x 1 month
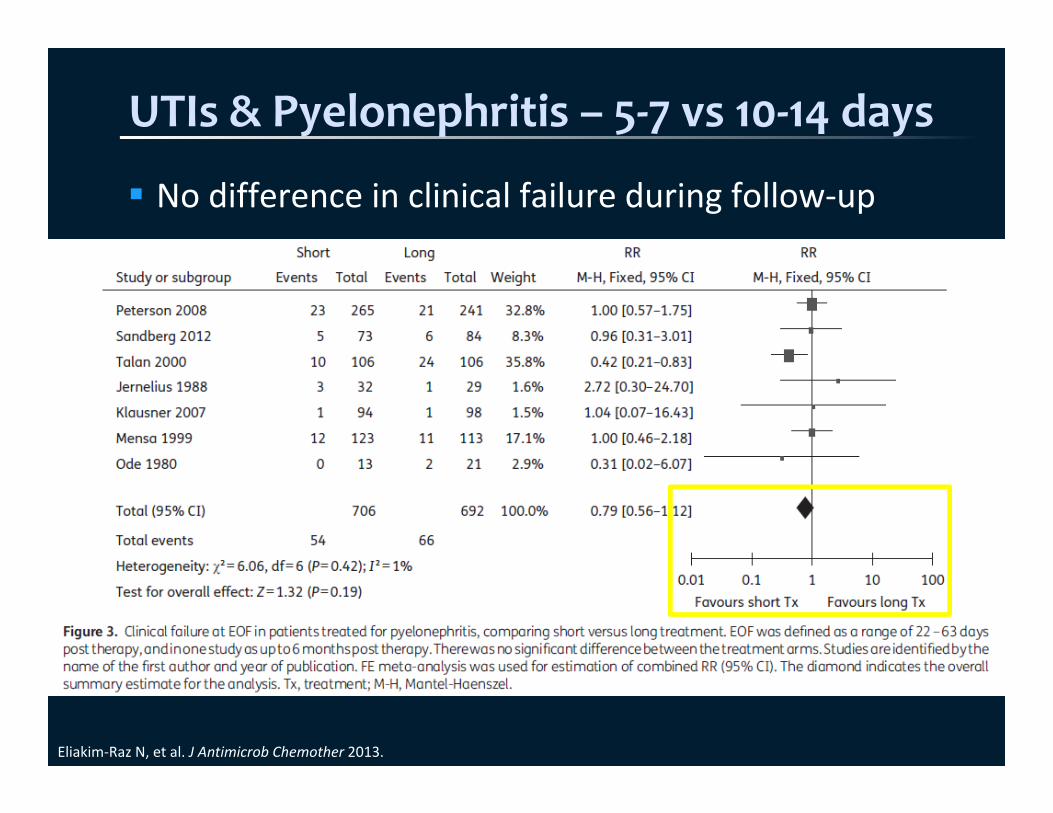
UTIs & Pyelonephritis – 5‐7 vs 10‐14 days
No difference in clinical failure during follow‐up
Eliakim‐Raz N, et al. J Antimicrob Chemother 2013.
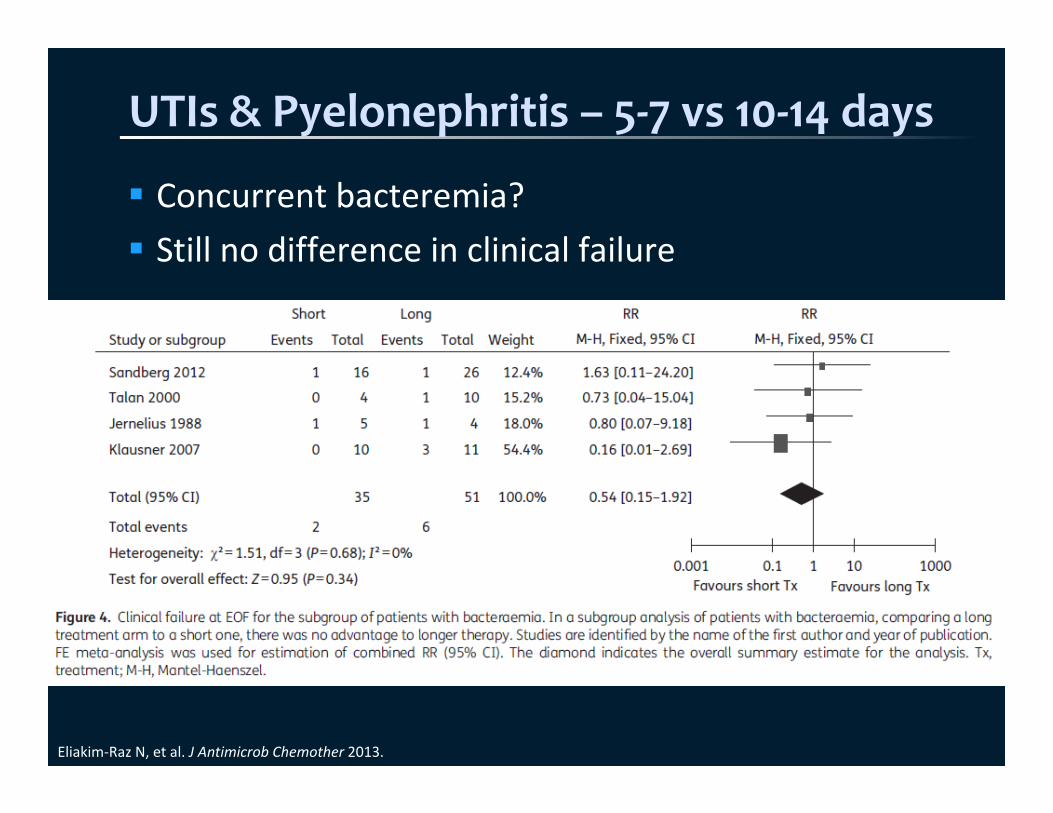
UTIs & Pyelonephritis – 5‐7 vs 10‐14 days
Concurrent bacteremia? Still no difference in clinical failure
Eliakim‐Raz N, et al. J Antimicrob Chemother 2013.
Audience Question
For each indication, what is the evidence‐based duration of therapy?a) CAPb) HAP/VAPc) COPD exacerbationd) Sinusitise) Intra‐abdominal infectionf) Skin and soft tissue infectiong) Pyelonephritis
What is the Solution?
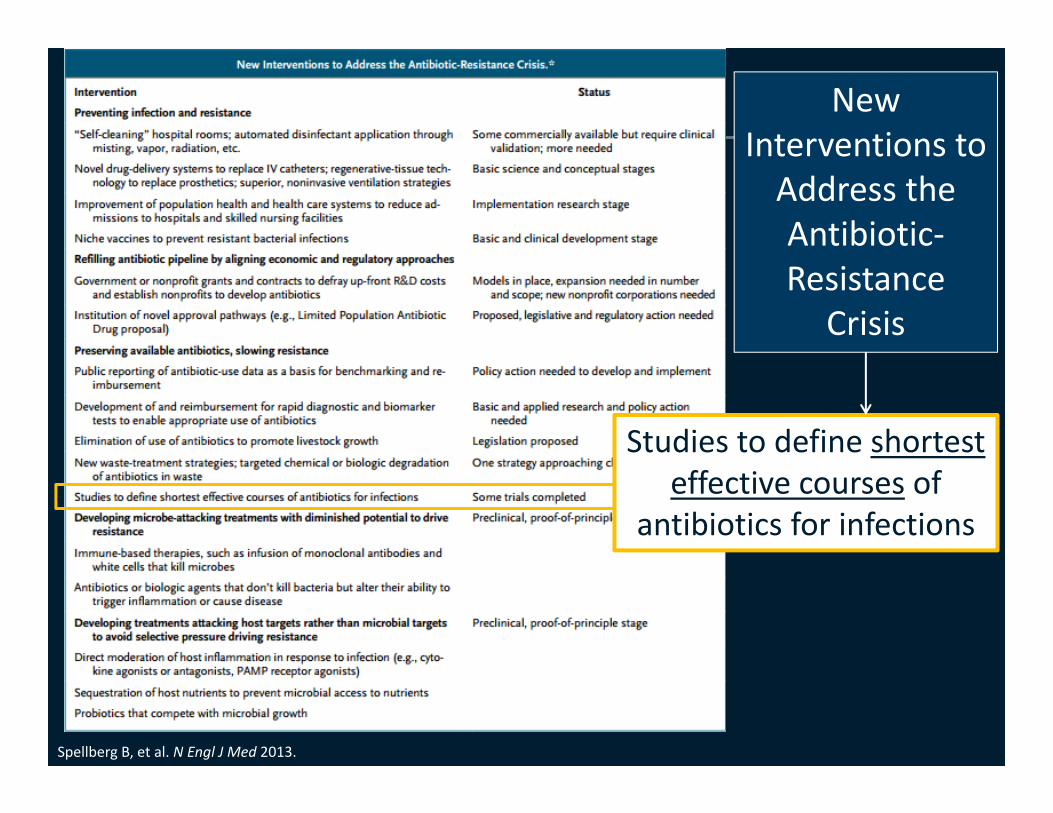
Spellberg B, et al. N Engl J Med 2013.
Studies to define shortest effective courses of
antibiotics for infections
New Interventions to Address the Antibiotic‐Resistance
Crisis

Duration for every Antibiotic Order

Recommended Durations by Source
FDA‐approved Guidelines LiteratureCAP 5 5 5
HAP/VAP 7 7 7
COPD exacerbation 7 5‐7 5
Sinusitis 5 5‐7 5
C. difficile 10 10‐14 10‐14
Intra‐abdominal infection
4‐14 4‐7 4
Skin and soft tissue infection
5‐14 5 5
UTI, complicated 75 (levofloxacin)
75 (levofloxacin)
5‐7
Pyelonephritis 75 (levofloxacin)
10‐145 (levofloxacin)7 (ciprofloxacin)
5‐7
How do I Implement This?
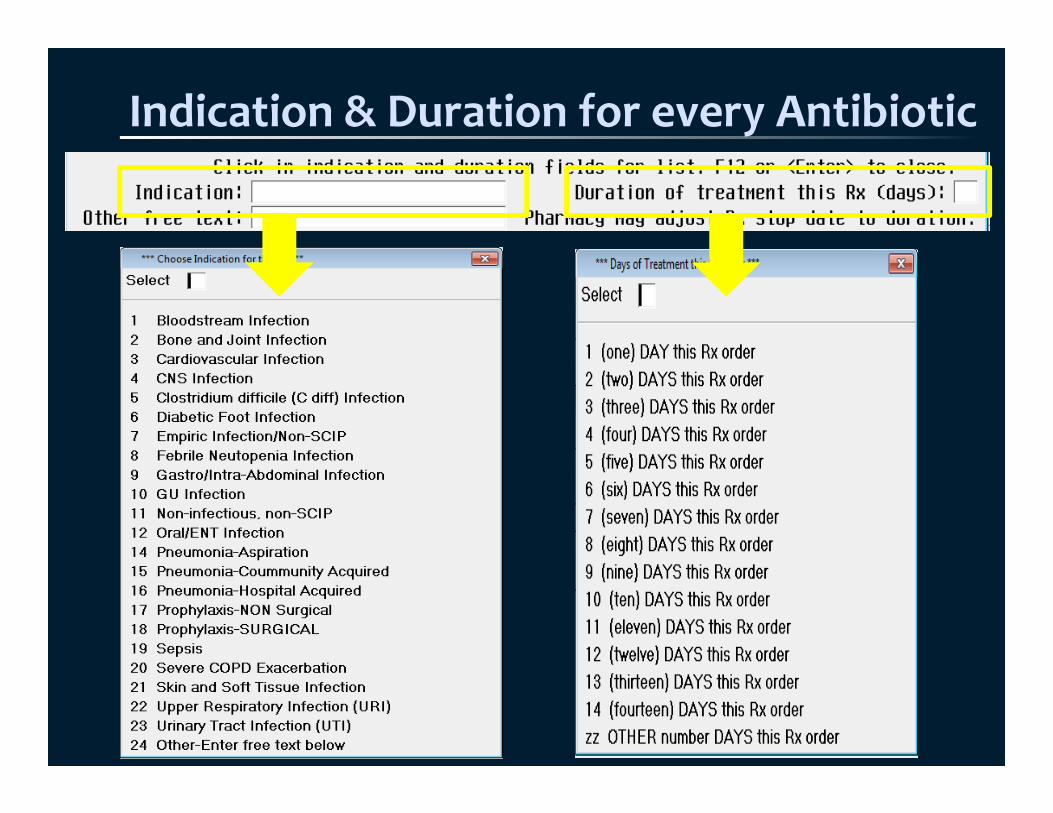
Indication & Duration for every Antibiotic
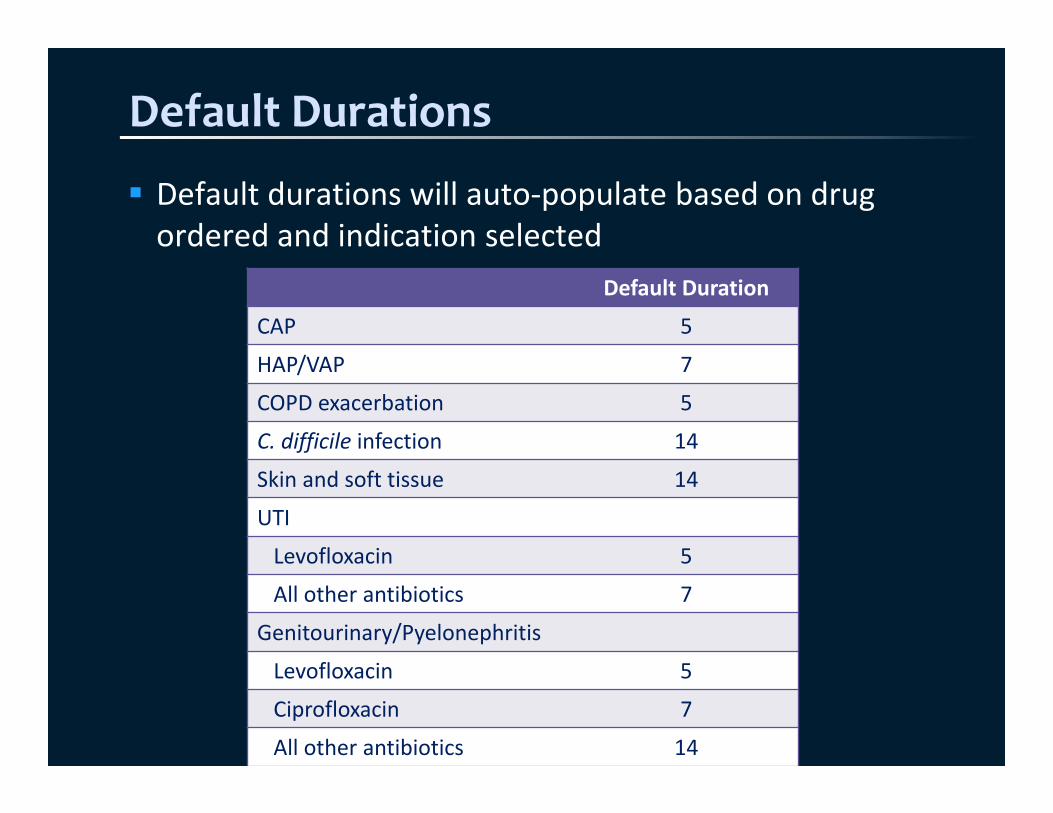
Default Durations
Default durations will auto‐populate based on drug ordered and indication selected
Default Duration
CAP 5
HAP/VAP 7
COPD exacerbation 5
C. difficile infection 14
Skin and soft tissue 14
UTI
Levofloxacin 5
All other antibiotics 7
Genitourinary/Pyelonephritis
Levofloxacin 5
Ciprofloxacin 7
All other antibiotics 14
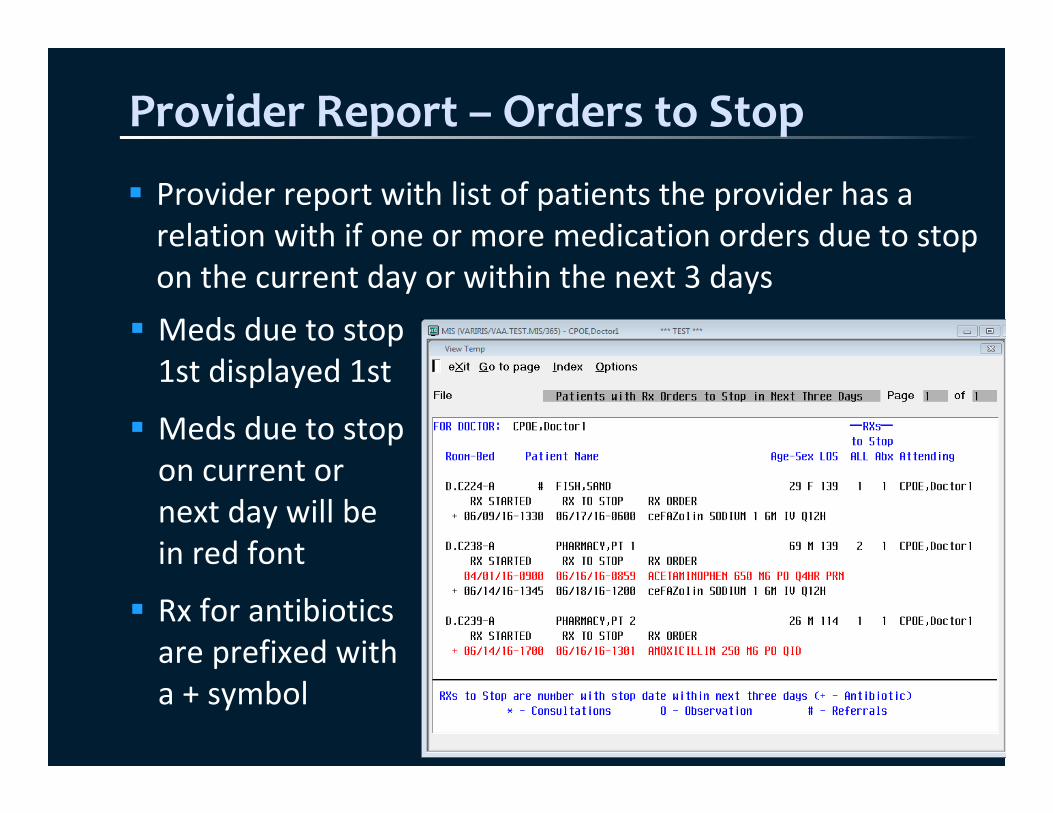
Provider Report – Orders to Stop
Provider report with list of patients the provider has a relation with if one or more medication orders due to stop on the current day or within the next 3 days Meds due to stop 1st displayed 1st
Meds due to stop on current or next day will be in red font
Rx for antibiotics are prefixed with a + symbol
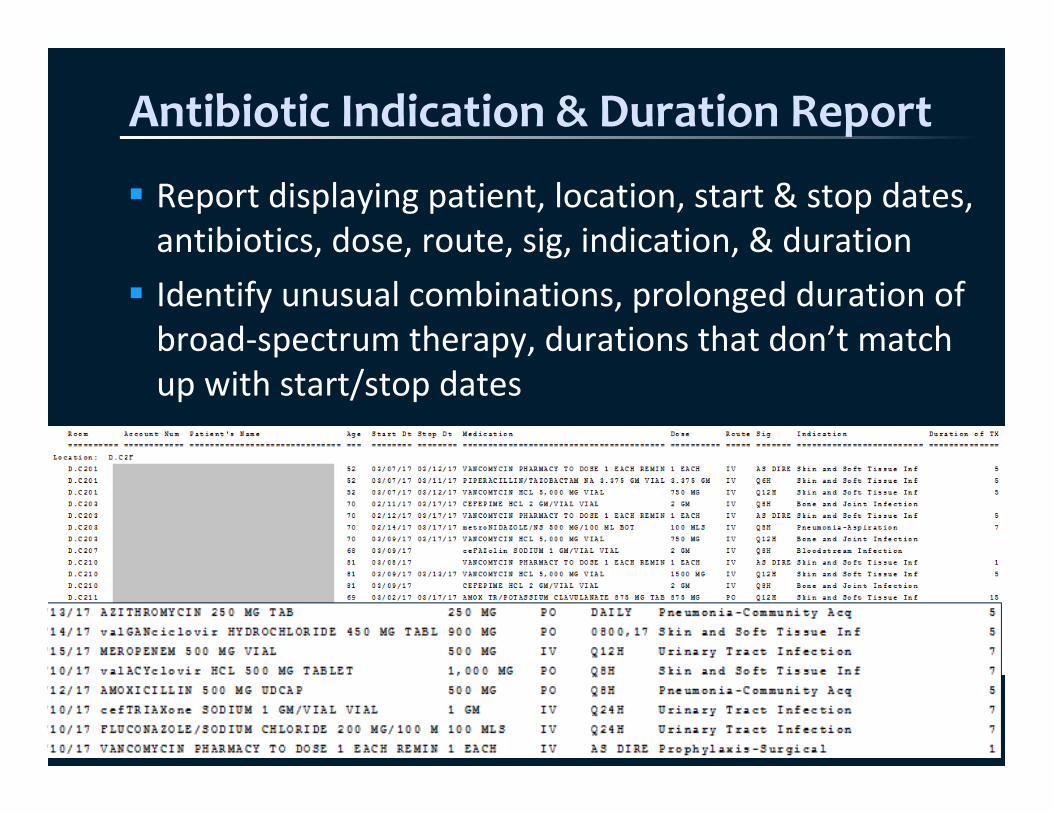
Antibiotic Indication & Duration Report
Report displaying patient, location, start & stop dates, antibiotics, dose, route, sig, indication, & duration Identify unusual combinations, prolonged duration of broad‐spectrum therapy, durations that don’t match up with start/stop dates
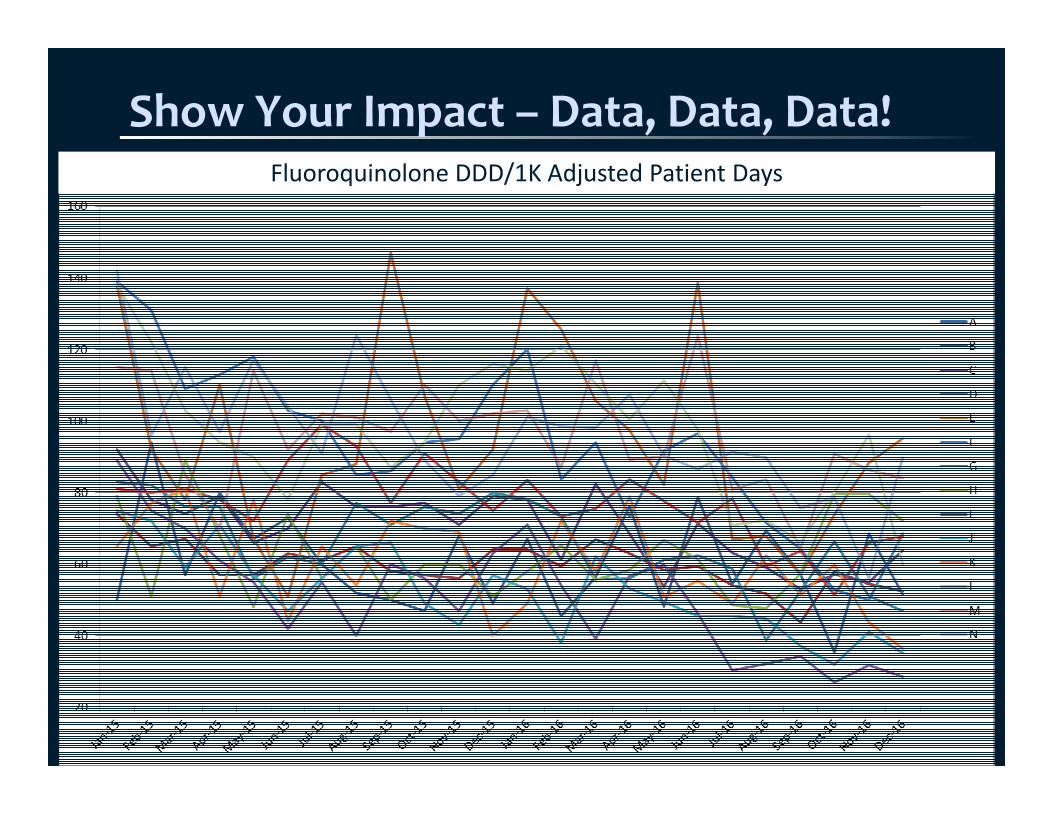
Show Your Impact – Data, Data, Data!Fluoroquinolone DDD/1K Adjusted Patient Days
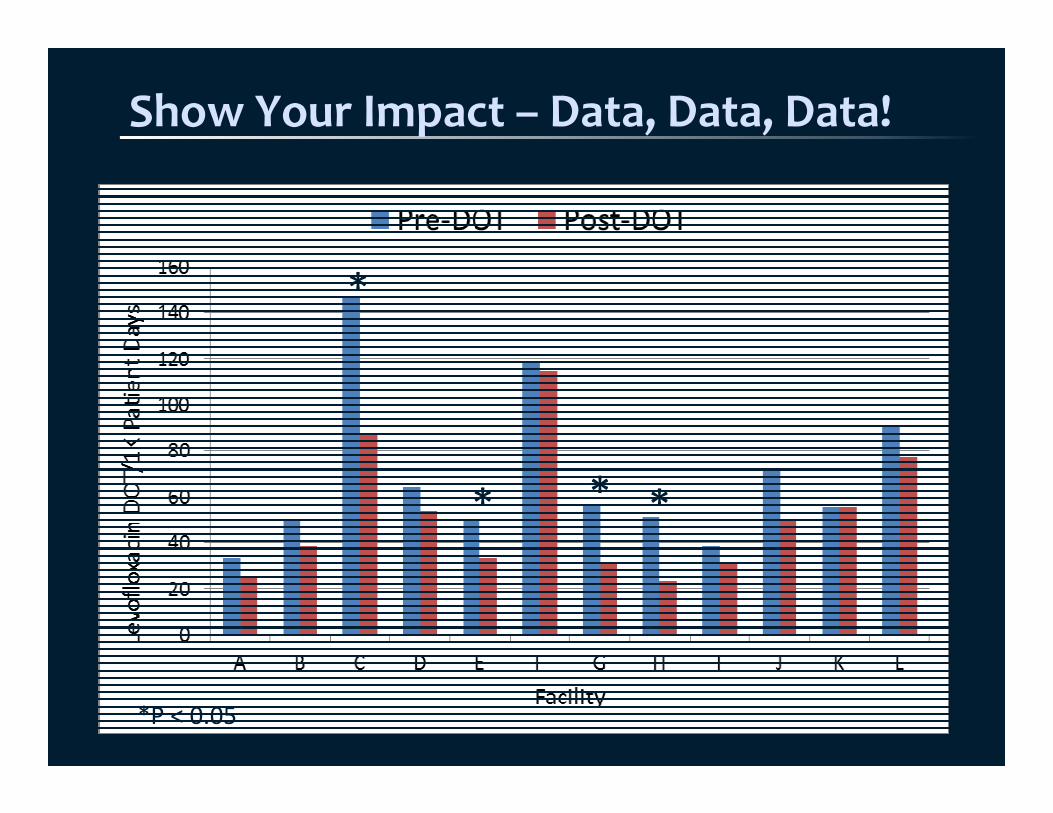
Show Your Impact – Data, Data, Data!
*
*P < 0.05
* * *
Show Your Impact – Data, Data, Data!
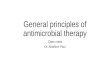
4
6
8
10
12
14
CAP ‐levofloxacin
UTI ‐levofloxacin
CAP ‐ceftriaxone
UTI ‐ceftriaxone
C. difficile ‐oral vanco
Average Du
ratio
n Ordered
(Days)
Pre‐Default Post‐Default
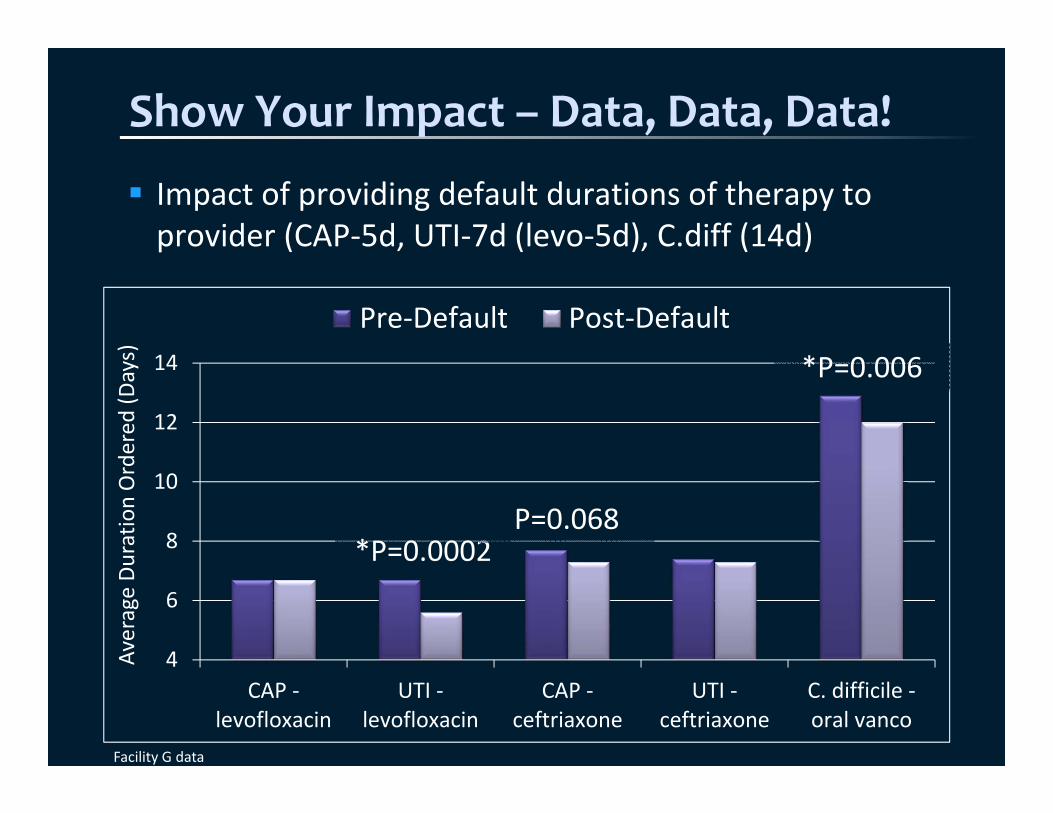
Impact of providing default durations of therapy to provider (CAP‐5d, UTI‐7d (levo‐5d), C.diff (14d)
*P=0.0002P=0.068
*P=0.006
Facility G data
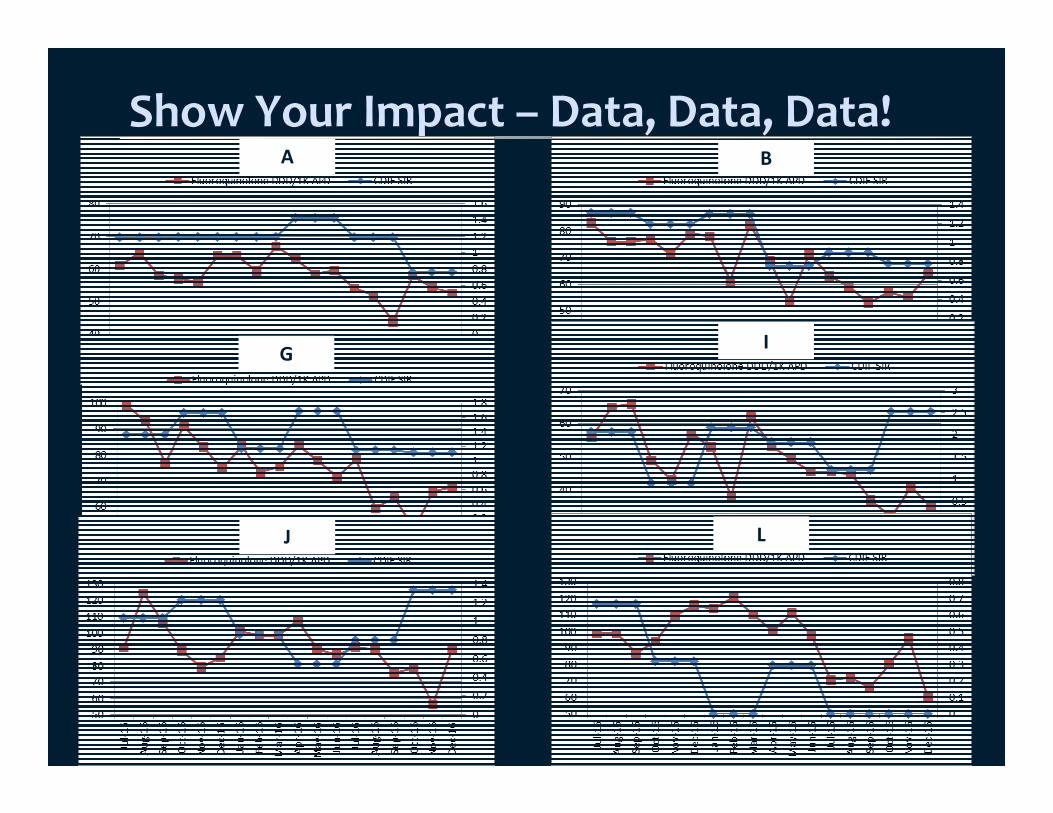
Show Your Impact – Data, Data, Data!A B
G I
J L
Keep Adding Enhancements
Antifungal Indications & DurationsHAP/VAP duration of 7 days Fluoroquinolone FDA Advisory for uncomplicated infections
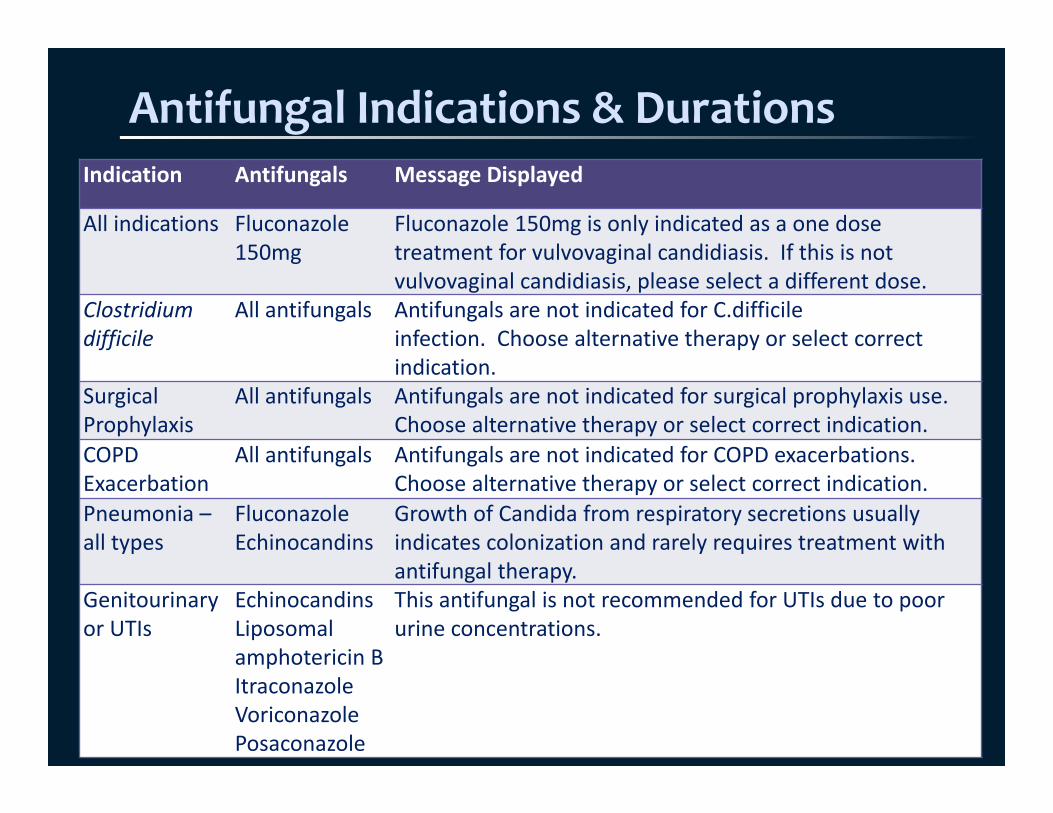
Antifungal Indications & DurationsIndication Antifungals Message Displayed
All indications Fluconazole 150mg
Fluconazole 150mg is only indicated as a one dose treatment for vulvovaginal candidiasis. If this is not vulvovaginal candidiasis, please select a different dose.
Clostridium difficile
All antifungals Antifungals are not indicated for C.difficile infection. Choose alternative therapy or select correct indication.
Surgical Prophylaxis
All antifungals Antifungals are not indicated for surgical prophylaxis use. Choose alternative therapy or select correct indication.
COPD Exacerbation
All antifungals Antifungals are not indicated for COPD exacerbations. Choose alternative therapy or select correct indication.
Pneumonia –all types
FluconazoleEchinocandins
Growth of Candida from respiratory secretions usually indicates colonization and rarely requires treatment with antifungal therapy.
Genitourinary or UTIs
EchinocandinsLiposomal amphotericin BItraconazoleVoriconazolePosaconazole
This antifungal is not recommended for UTIs due to poor urine concentrations.
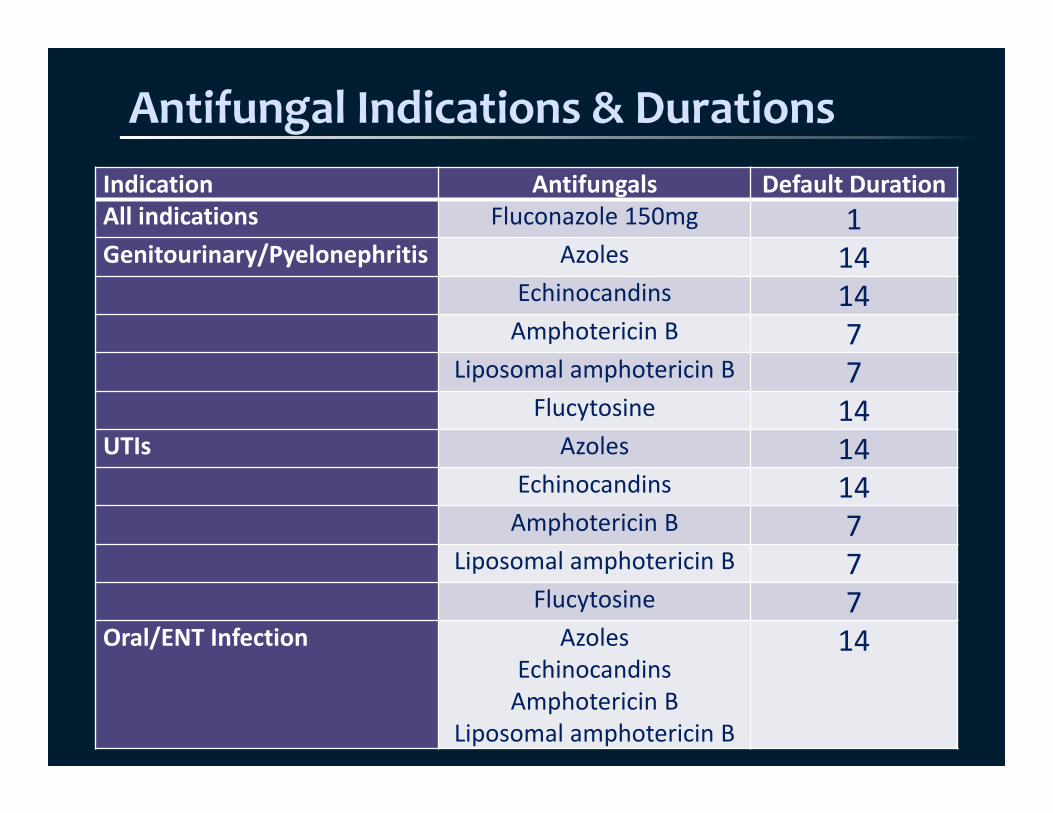
Antifungal Indications & DurationsIndication Antifungals Default DurationAll indications Fluconazole 150mg 1Genitourinary/Pyelonephritis Azoles 14
Echinocandins 14Amphotericin B 7
Liposomal amphotericin B 7Flucytosine 14
UTIs Azoles 14Echinocandins 14Amphotericin B 7
Liposomal amphotericin B 7Flucytosine 7
Oral/ENT Infection AzolesEchinocandinsAmphotericin B
Liposomal amphotericin B
14
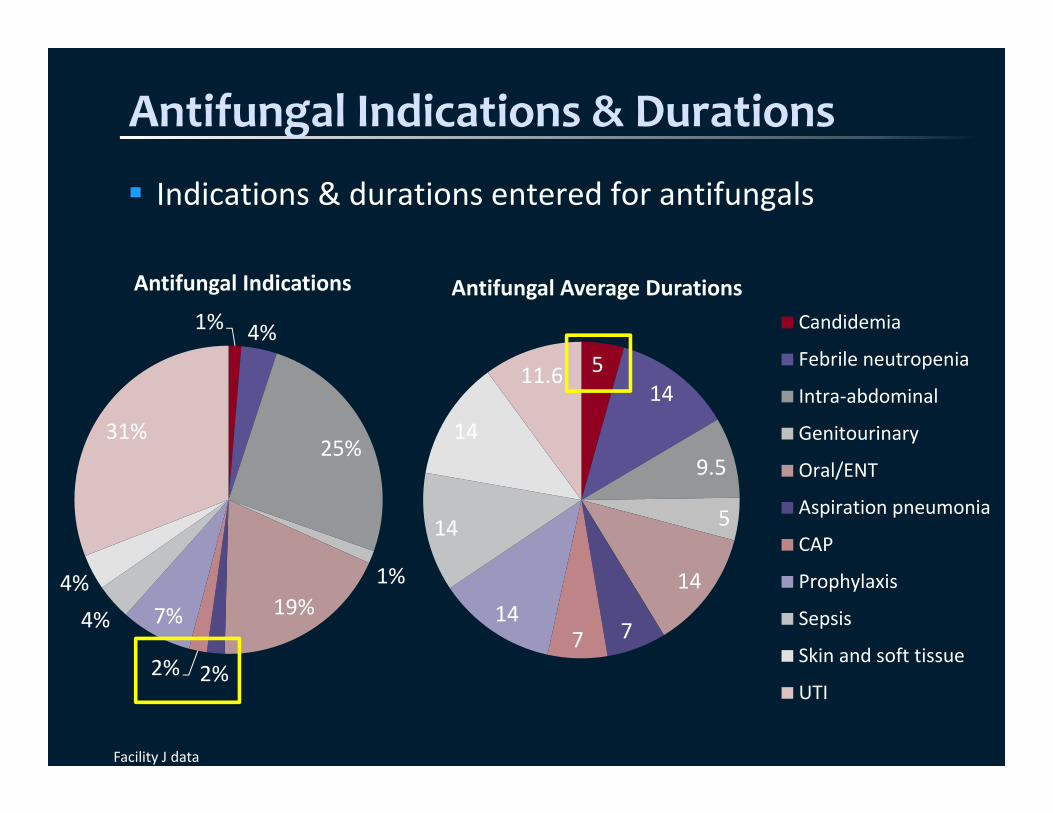
Antifungal Indications & Durations
Indications & durations entered for antifungals
Facility J data
1% 4%
25%
1%19%
2%2%
7%4%4%
31%
Antifungal Indications
514
9.5
5
14
7714
14
14
11.6
Antifungal Average DurationsCandidemia
Febrile neutropenia
Intra‐abdominal
Genitourinary
Oral/ENT
Aspiration pneumonia
CAP
Prophylaxis
Sepsis
Skin and soft tissue
UTI
Keep Adding Enhancements
Antifungal Indications & DurationsHAP/VAP duration of 7 days Fluoroquinolone FDA Advisory for uncomplicated infections
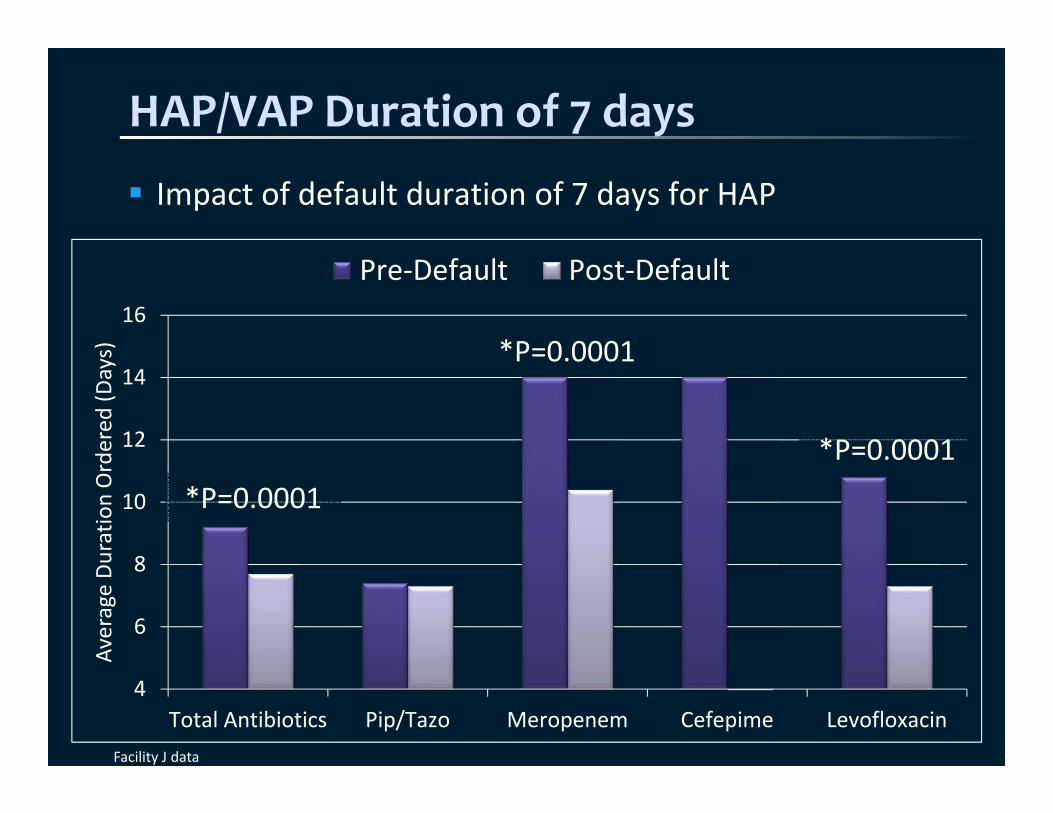
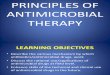
HAP/VAP Duration of 7 days
Impact of default duration of 7 days for HAP
4
6
8
10
12
14
16
Total Antibiotics Pip/Tazo Meropenem Cefepime Levofloxacin
Average Du
ratio
n Ordered
(Days)
Pre‐Default Post‐Default
Facility J data
*P=0.0001
*P=0.0001
*P=0.0001
Keep Adding Enhancements
Antifungal Indications & DurationsHAP/VAP duration of 7 days Fluoroquinolone FDA Advisory for uncomplicated infections

Fluoroquinolone FDA Advisory
In 2015, fluoroquinolones accounted for the most reports of persistent adverse effects that became long‐term health issues (e.g. painful joint, muscle, & tendon disorders) FDA has stated that these adverse effects outweigh their benefits for uncomplicated infections and alternatives should be used When an uncomplicated infection is chosen for a fluoroquinolone, a warning message is presented with alternative first‐line options Genitourinary Infections Upper Respiratory Infections Urinary Tract Infections

Fluoroquinolone FDA Advisory
Number of fluoroquinolone orders for each indication before & after fluoroquinolone FDA advisory message:
Facility H Facility IBefore (n=238)
After (n=200)
P‐value Before (n=166)
After (n=223)
P‐value
GenitourinaryInfection
11 (19.6%) 4 (7.5%) 0.095 16 (23.5%) 8 (12.9%) 0.174
Upperrespiratory infection
10 (34.5%) 4 (11.1%) 0.034 9 (40.9%) 2 (7.1%) 0.006
UTI 54 (35.3%) 18 (16.2%) 0.0007 26 (34.2%) 25 (18.8%) 0.019
Total 75 (31.5%) 26 (13.0%) 0.0001 51 (30.7%) 35 (15.7%) 0.0005
Conclusion
Optimal antimicrobial use includes avoiding them when they’re not indicated and giving the right drug, right dose, de‐escalating to pathogen‐directed therapy, and treating for the right duration. Excessive durations of therapy leads to more resistance development, greater risk of other infections, and a greater risk of side effects, including C. difficile. Shorter durations of therapy have been shown to be just as effective as longer durations for several infectious indications, including CAP, HAP/VAP, COPD exacerbations, sinusitis, intra‐abdominal infections, skin and soft tissue infections, & pyelonephritis.
Post‐Test Question 1
Excessive durations of antibiotic therapy have been found to:
A. Improve clinical cure ratesB. Increase the risk of a subsequent infectionC. Result in similar efficacy and safetyD. Decrease rates of C. difficile
Post‐Test Question 2
How many days of antibiotics do patients with hospital‐acquired or ventilator‐associated pneumonia need based on recent evidence?
A. 5B. 7C. 7‐8 for most organisms; 15 for non‐lactose
fermenting gram‐negative rodsD. 10 for most organisms; 15 for non‐lactose
fermenting gram‐negative rods
Questions?
Jill Cowper, Pharm.D.Division Infectious Diseases Pharmacist
Parallon Supply Chain SolutionsRichmond, VAP: 607‐221‐5101
Optimize Durations of Antimicrobial Therapy
Evidence & Application








![Antimicrobial Salvage Therapy for Persistent ...nizetlab.ucsd.edu/Publications/Dapto-Ceftaroline.pdf · Clinical Therapeutics/Volume ], Number ], 2014 Antimicrobial Salvage Therapy](https://img.pdfslide.net/doc/110x75/5e1833d08b13d527220aeb61/antimicrobial-salvage-therapy-for-persistent-clinical-therapeuticsvolume-.jpg)