Embed Size (px)
Citation preview

Oral Pathology Exam I Review Slides

Physical/Chemical Injury

Items covered:• Physical/Chemical injury
– Traumatic bone cyst– Osteoporotic (Hematopoietic) bone marrow defect– Surgical ciliated cyst of maxilla (aka traumatic ciliated cyst or
postoperative maxillary cyst)– Pulse granuloma– Lipid granuloma– Cotton roll injury– Saliva ejector injury– Air emphysema– Injection hematoma– Amalgam tattoo– Cheek biting (morsicatio buccarum)– Tongue biting (morsicatio linguarum)– Traumatic (eosinophilic) granuloma– Pizza burn (thermal food injury)– Palatal petechiae– Riga-fede disease– Keratotic lesions
• Nicotine stomatitis• Snuff dipper’s keratosis
– Mass Lesions• Mucocele• Ranula• Pyogenic granuloma• Fibroma• Linea alba• Peripheral ossifying fibroma• Peripherial giant cell granuloma
Traumatic (amputation) neuromaAspirin Burn
• Mecication reactions Gingival fibromatosis Tetracycline/minocycline stain Stomatitis medicamentosa Stomatitis veneata cinnamon reaction Angioedema
• Lesions affected by prosthesis Denture sore mouth Denture base allergy Papillary hyperplasia Epulis Fissuratum Angular Cheilits Osseous and chondromatous metaplasia Subpontic osseous hyperplasiaFlorid osseous dysplasia
Occurs primarily in the mandible, medullary hemorrhage leaves clot which dissolves, leaving empty cavity. Radiographic: small to large well-defined radiolucency with sclerotic borders, upper margin scalloped between roots, typically above mandibular canal, can be multilolulcar/expansile. Does NOT displace teeth, usually located in anterior, does not go beyond 3rd molar, teeth are vital, no epithelial lining.
Traumatic Bone Cyst
Located in posterior mandible, usually in the 3rd molar site, red marrow fills socket instead of bone, Female predilection, asymptomatic, Radiographic: ill defined radiolucency, Histologic: normal red bone marrow (adipose and megakaryocytes
Osteoporotic (Hematopoietic) Bone
Marrow Defect

Maxilla only, sequella of antral sinus surgery or sinus perforation, fragment of sinus epithelium is pushed and entrapped in maxilla and proliferates into a cyst, Radiographic: well defined radiolucency in posterior maxillaHistologic: Cyst with sinus lining (pseudostratified ciliated columnar epithelium)
Surgical Ciliated Cyst of the
Maxilla

Vegetable (often leguminous) material lodged into mandibular 3rd molar extraction site, evokes foreign body inflammatory reactionRadiographic: ill defined lytic lesionHistologic: Spherical bodies surrounded by a foreign body giant cell reaction
Pulse Granuloma

Petroleum jelly containing substance is squeezed into third molar extraction site, lipid evokes a foreign body giant cell response, causes deep gnawing pain approximately 3 months or so laterHistologic: Clear lipid vacuoles surrounded by a foreign body giant cell reaction
Lipid Granuloma

Cotton absorbs moisture from mucosa and sticks-removal of cotton rips off part of the mucosa
Cotton Roll Injury

Mucosa gets caught in saliva ejector and is ripped out
Saliva Ejector Injury

Instant swelling associated with air blown into laceration where bone is exposed, palpation of the area will have crepitus (little bubbles of air), usually resolves itself, but can cause respiratory distress and is an emergency
Air Emphysema

Usually a PSA, anesthetic solution gets into the pterygoid plexus of veins in the area of the buccal fat pad and cause pain.
Injection Hematoma

Implantation of amalgam fragments into the connective tissue, slate gray in appearance, looks similar to melanoma, occurs with: flossing vigorously soon after proximal amalgam placement, fractured amalgam during surgical extraction, apicoectomy with retrofillHistology: Fine to coarse black/brown/green pigment granules in connective tissue, distributed along reticulin/elastin fibers appearing as tobacco strands, no inflammatory reaction
Amalgam Tattoo

Necrosis of localized mucosa due to injection of anesthetic containing epinephrine, local blood supply is cut off, resulting in ischemia and necrosis
Anesthetic Necrosis

Rough, masserated, white, torn lesion (usually bilateral), with or without red areas, in area easily accessible by the teethHistology: Macerated hyperparakeratosis, acanthosis, with vacuolated cells.
Cheek Biting (Morsicatio Buccarum)
Tongue biting (Morsicato Linguarum)

Lateral tongue lesion with central deep ulcer that normally goes to the muscle layer and has firm elevated borders, caused by chronic local (sharp edges on teeth) and non-local (tardive dyskinesia) factors, resembles SCC clinicallyHistology: Surface ulcer with fibrin coating, deep inflammation into muscle with histiocytes and eosinophils
Traumatic (eosinophilic)
granuloma

Injury caused by hot food contacting the hard palate, occurs in the region of the incisive papilla (turns red and mucosa sloughs off)
Pizza Burn

Clinically descriptive term for small, focals areas of submucosal hemorrhage, caused by: forcible retching, forcible fellatio, influenza, measles, scarlet fever, mononucleosis, clotting disorders, thrombocytopenias
Palatal petechiae

Laceration in the lingual frenum area in the midline of the floor of the mouth in infants due to tongue thrust during feeding against premature tooth or teeth
Riga-fede disease

Seen on the hard palate of pipe smokers, heat of the pipe causes reactive hyperkeratosis, white fissured palate with multiple papules having central red spots representing inflamed salivary ducts, resolves within 2 weeks of cessation of pipe smoking
Nicotine Stomatitis

White fissured lesions (dry river bottom) in the area where the tobacco is held, usually in the vestibule area extending onto alveolar mucosa and the lip, may transform after many years, associated with gingival recession, periodontal bone loss, tooth abrasion and stains, resolves 2-6 weeks after cessationHistology: Chevron shaped hyperparakeratosis and acanthosis.
Snuff dipper’s keratosis

Occurs only where salivary tissue is located, primarily on the lower lip, mostly in children, laceration of lower lip tears a salivary duct, saliva pumps into CT and is walled off by granulation tissue, blows up like a balloon and is encapsulated. Soft, fluctuant, pink or blue submucosal massHistology: mucous sac lined by thin layer of granulation tissue, will eventually becom a fibrous lump and needs to be removed and submitted for biopsy
Mucocele
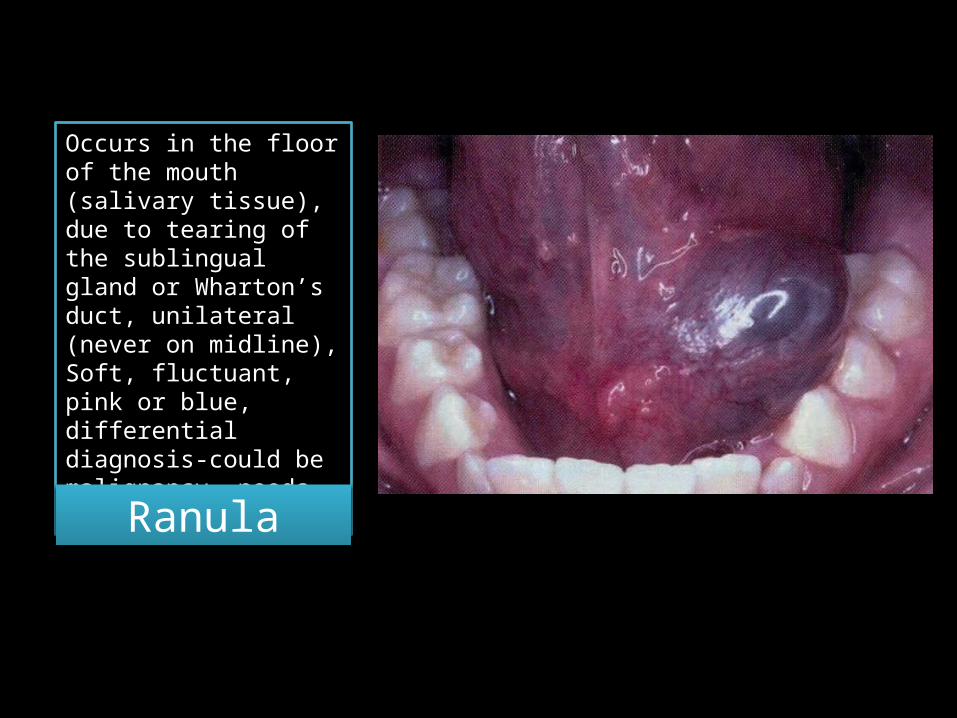
Occurs in the floor of the mouth (salivary tissue), due to tearing of the sublingual gland or Wharton’s duct, unilateral (never on midline), Soft, fluctuant, pink or blue, differential diagnosis-could be malignancy, needs to be biopsied
Ranula

Low grade, persistent irritation that stimulates the healing reaction to produce excessive granulation tissue, common reactive lesion of the gingiva (75%) , lips and tongue, pregnant women are more prone (top left shows pyogenic granuloma during pregnancy [top] and 3 months after [bottom], can resemble cancer, soft, bleed easily, red and never hyperkeratinized
Pyogenic Granuloma

Granulation tissue that wells up in a recent extraction site due to irritant.
Epulis Granulomatosum

Reactive smooth fibrous hyperplasia to a low grade chronic irritant (cheek biting, resolution of a pyogenic granuloma, resolution of mucocele, rough margin/defective restoration, irritating RPD clasp, irritating ortho band
Fibroma

Band of white tissue (hyperkeratosis/fibrosis) that goes across the entire occlusal line on the buccal mucosa, due to cheek sucking
Linea Alba

Firm, pink,fibroma which is initiated by an irritant, then enlarges independently, occurs only on gingiva, mostly tooth bearing, derived from the PDL and sometimes the periosteum, will displace teethRadiographic: Triangulation of radiolucency along root surface with some radiopacity Histologic: Spindly cellular fibrous stroma forming bone and/or cementum
Peripherial Ossifying Fibroma

Soft, red, painless mass caused by low grade trauma to gingiva, PDL or periosteum, bleeds easily, seen only on gingiva (usually anterior) Radiographic: Can show cupping of underlying boneHistologic: Cellular spindly stroma containing clusters of foreign body multinucleated giant cells and vessels with hemorrhage
Peripheral giant cell granuloma

Tearing or crushing a peripheral nerve, nerve twigs attempt to re-establish path but become blocked by fibrous scar and proliferate in a hyperplastic twisted, tangled mass lesion which is painful. Seen on tongue after bite injury, 3rd molar area or mandibular canal after extraction, mental nerve area after ill fitting denture or atrophic ridge. Looks just like a fibroma but is painful.Histologic: Dense fibrous tissue like a fibroma but contains many hyperplastic nerve endings
Traumatic (amputation) neuroma

Chemical cautery (protein denaturation) of mucosa due to placing aspirin directly on source of tooth pain. Similar reactions occur with: nitroglycerine, bisphosphonates, chlorpromazine, eugenol, phenol, hydrogen peroxide, formocreosol, listerineHistology: necrosis and sloughing of epithelium
Aspirin Burn

Generalized firm and fibrous non-hemorrhagic growth of the gingiva, 3 drugs involved-anticonvulsants (dilantin), Calcium Channel Blockers (nifidipine), Cyclosporine. Hyperplasia is increased with poor oral hygiene and increased dose of offending drug
Gingival Fibromatosis

Tetracycline uptake in growing calcifying tissues (bone, dentin, enamel) causes a yellow, grey or brown intrinsic stain, severity is dependent on length of usage and dose (note: Minocycline will stain teeth in a similar manner, except that it can stain formed teeth as well)
Tetracycline Stain

Oral hypersensitivity and lesion reaction to a systemic drug, similar to stevens-johnson syndrome, slough of oral cavity
Stomatitis Medicamentosa

Oral hypersensitivity to a topical agent (contact allergy), presents as white and/or red lesions adjacent to contacting material, occurs commonly with corroded amalgam, can occur years after placement of amalgams
Stomatitis Venenata

Unilateral, burning white or red lesion on buccal mucosa and lateral tongue due to cinnamonHistologic: perivascular inflammation in the submucosal tissue, lichenoid reaction
Cinnamon Reaction

Type 1 hypersensitivity due to multiplecauses (non-hereditary form, hereditary form, ACE inhibitors) which causes rapid, painless swelling of lips, face, eyelid, tongue, floor of mouth, larynx. Lasts 24-36 hours before it completely dissipates
Angioedema

Diffuse red velvety area that outlines the denture base and does not extend beyond, caused by ill-fitting dentures or a dirty denture that a patient does not remove at night, predisposes to candida infection
Denture Sore Mouth
Velvety red area outlining the denture base of a recently repaired denture. Due to allergy of excess monomer present in recently repaired denture.
Denture Base Allergy

Pyogenic granulomas that mature and become tiny fibromas, occurs in longstanding DSM where granulation tissue develops and matures into fibrous papules with a cobblestone appearance. Seen exclusively on hard palate. Candida is almost always involved. Patients with high palatal vaults are more prone to thisHistology: Inflammatory fibrous hyperplasia, each papillary nodule is a fibroma, inflamed salivary gland ducts show reactive squamous metaplasia resulting in pseudoepitheliomatous hyperplasia
Papillary Hyperplasia

Inflammatory fibrous hyperplasia (similar to fibroma) under an overextended denture, parallel fibrous folds grow on each side of the flange separated by a longitudinal fissure where the flange sits, the central fissure is usually ulcerated, rarely transform
Epulis Fissuratum

Bilateral inflammation of commissures of the lips, caused by candida (perleche), B-vitamin deficiency, overclosed VDO
Angular cheilitis

Chronic irritation of periosteum causes painful spurs of bone or cartilage to form arising clinically as bumps in the vestibule, occurs when unstable denture rocks anteriorly on a thin, atrophic anterior ridge, presses on the periosteum and causes spurs of bone or cartilage to form, primarily occurs in the anterior
Osseus and chondromatous
metaplasia
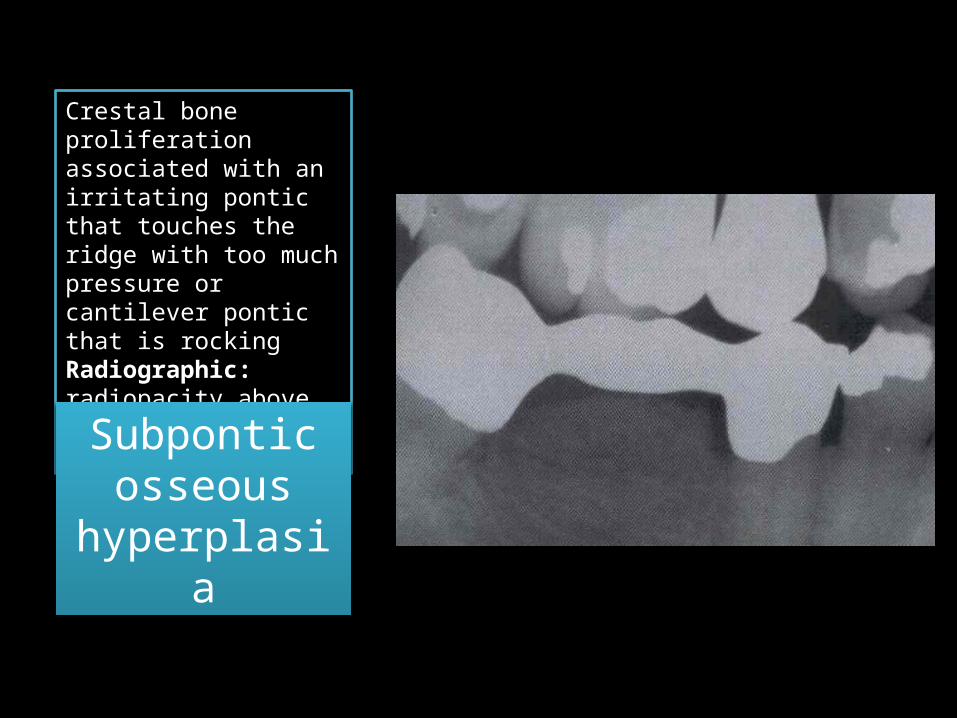
Crestal bone proliferation associated with an irritating pontic that touches the ridge with too much pressure or cantilever pontic that is rockingRadiographic: radiopacity above edentulous restal bone under a pontic
Subpontic osseous
hyperplasia

Dense masses of sclerotic bone and cementum form in the mandible for unknown reasons, remains stable until a denture is made, the normal bone resorption that accompanies dentures exposes the sclerotic bone which becomes infected and sloughs
Florid (Cemento)
Osseous Dysplasia