Embed Size (px)
Citation preview

Oriental Cholangitis
Richard H. Carmona, MD, San Francisco, California
Richard A. Crass, MD, San Francisco, California
Robert C. Lim, Jr., MD, San Francisco, California
Donald D. Trunkey, MD, San Francisco, California
The syndrome of oriental cholangitis, which is also known as recurrent pyogenic cholangitis, oriental biliary obstruction syndrome and oriental cholan- giohepatitis, is character&d by intrahepatic pigment stone formation with recurrent exacerbations and remissions of abdominal pain frequently associated with jaundice, chills, and fever. This syndrome is endemic to and has been recognized for over half a century in asian societies, but it’s pathophysiologic characteristics are still poorly understood [I ,.2]. This unusual biliary tract syndrome is now being en- countered with increased frequency in western so- cieties, especially in the United States, largely as a result of the increased immigration of refugees from Asia during and after the Vietnam War. Western physicians are used to caring for a very dissimilar biliary tract disease and it’s complications (Table I). Cholelithiasis is largely a result of liver secretion of bile supersaturated with cholesterol that precipitates and forms stones in the gallbladder [3]. Approxi- mately 75 percent of patients in western societies have cholesterol stones, whereas patients with or- iental cholangitis uniformly have intrahepatic and extrahepatic pigment stones that are associated with bacterial colonization of the biliary tract [4,5]. In addition, several reports [2,6,7] have noted the fre- quent association of oriental cholangitis with par- asitic infestation, usually Clonorchis sinensis, the Chinese liver fluke. This relationship is still disputed
From the Department of Surgery, lJnive~r5lty of California, San Francisco and the San Francisco General Hospital, San Francisco, California. Sup- ported in part by National Institutes of Health Trauma Qrant GM 07032.
l?eqUBUts for [email protected] should be addressed to Rkhard A. Crass, MD, De- partment of Surgery, Ward 3A. San Francisco General Hospital, San Fran- cisco, California 94110.
Presented at the 55th Annual Meeting of the Pacific Coast Surgical As- sociation, Newport Beach, California, February 19-22, 1984.
since large populations of people in endemic areas are infected with liver flukes without ever having the development of oriental cholangitis [6,&S]. Due to the previously restricted geographic and ethnic in- cidence of this disease, most western physicians are unfamiliar with its presentation and management, and therefore the potential exists for errors in diag- nosis and management.
This study reviews our experience with 21 patients with oriental cholangitis and provides recommen- dations for diagnosis and surgical management.
Material and Methods
Twenty-one patients, (9 men and 12 women) 19 to 84 years of age with oriental cholangitis, were treated at San Francisco General Hospital between 1970 and 1933. All had immigrated from Asia, and 20 had a history of previous episodic abdominal pain with 15 having had previous epi- sodes of jaundice, chills, or fever. The most common pre- senting signs and symptoms were pain in the right upper quadrant, jaundice, fever, and chills. Patients had been symptomatic from 1 year to a maximum of 30 years (one patient). Four patients had a previous history of docu- mented parasitic infection. Laboratory values varied hut frequently indicated hyperbiibinemia, leukocytosis, or both (18 patients). The preoperative radiologic workup also varied in each patient and was dependent on studies available at the time the patient was initially seen. Patients examined earlier in the study frequently had liver scans and intravenous cholangiograms, whereas those seen more recently had abdominal sonograms and computed tomo- grams as these newer modalities became available. Transhepatic cholangiography and endoeco ic retrograde cholangiography were used only in selecte J patients. All patients had operations, 12 initially in their country of origin or at a referring hospital and 9 initially at San Francisco General Hospital. In addition, 10 patients un- derwent second operations at San Francisco General Hospital. Intraoperative biliary tract specimens were ob-
vohmle 148, July 1994 117

Carmona et al
TABLE I Comparison of a Pigment and Nonpigment Stone Disease
Oriental Cholangitis
Age Varied Sex Equal number of males and females Endemic area Coastal Asia Population Lower socioeconomic group Stones Pigment (calcium bilirubinate) Stone location lntrahepatic and extrahepatic ducts Gallbladder Usually normal Biliary cultures Frequently E. coli with or without other
pathogens Laboratory findings Frequently leukocytosis and hyperbilirubinemia Radiology lntrahepatic stones and duct dilation, strictures
occasionally Treatment Always surgical Prognosis Previously poor to fair but potentially improving
Cholelithiasis
Increasing with age More females than males West General Cholesterol Gallbladder, sometimes extrahepatic ducts lnflammed Frequently negative findings
Usually normal Stones in gallbladder, extrahepatic ducts, or
both Usually surgical Excellent with surgery
tained for culture from all patients. Duration of follow-up ranged from 2 months to 8 years.
All patients underwent cholecystectomy, and three pa- tients also had common duct exploration. Nine patients had their initial operation at San Francisco General Hos- pital. All had a cholecystectomy, and five also underwent a choledochojejunostomy; (one with hepatic lobectomy, three with a choledochoduodenostomy, and one with a hepaticojejunostomy). Ten patients had their second op- eration at San Francisco General Hospital. Six patients had a choledochojejunostomy (1 with a left hepatic lobe&my), three had a choledochoduodenostomy and one patient had a liver abscess drained and common duct exploration.
Results
Intraoperative findings revealed that all patients had intrahepatic and extrahepatic pigment stones. Intrahepatic and extrahepatic ductal systems were
dilated in all patients, and two patients also had in- trahepatic strictures. Five patients were also found to have cholelithiasis, and four patients had intra- ductal parasites. One of the four had Clonorchis si- nensis only, two had multiple parasites including Clonorchis sinensis, and one patient had Ascaris lumbricoides and Trichuris trichiura. All patients had positive findings on biliary tract culture. Eight had Escherichia coli alone, and 13 had E. coli and at least one other organism. In the group of 12 patients that initially underwent only cholecystectomy, with or without common duct exploration, all eventually became symptomatic again (Table II). Eight of these patients underwent reoperation (three had choledochoduodenostomies and five had choledo- chojejunostomies, one with left hepatic lobectomy). Three patients refused a second operation and one
TABLE II Follow-Up of lnltlal Nondralnage Blllary Tract Operations
Patient Initial Operation Second Operation*
Year Type Year Type Follow-Up
2 1968 C 1976 3 1974 C, CDE
5 1972 6 1970 : 8 1969 : 1981 9 1967 1975
1979 11 1980 C, CDE
CDJ LTF LTF LTF CDD CDJ TS LTF
2 yr, asymptomatic 2 mo, recurrent symptoms 2 mo, recurrent symptoms 1 yr, recurrent symptoms 1 yr, asymptomatic 4 yr, asymptomatic recurrent stones,
refused reoperation 2mo
14 1970 C 1972 CDD 8 yr, asymptomatic 17 1967 C, CDE 1983 CDJ 6 mo, asymptomatic 18 1979 C 1983 CDD 6 mo, 19 1972
asymptomatic C 1983 CDJ, LHL 1
21 yr, asymptomatic
1979 C 1980 CDD 1983 CDJ 2 mo, asymptomatic
l Patients 3, 5, and 8 refused a second operation. C = ChOleCYSteCtOtTIY; CDD = choledochoduodenostomy; CDE = common duct exploration; CDJ = choledochojejunostomy; HJ = hep
aticojejunostomy; LHL = left hepatic lobectomy; LTF = lost to follow-up; TS = transhepatic stent.
118 The American Journal of Surgery

Oriental Cholangitis
TABLE III Follow-Up of Initial Blllary tract Dralnage Operations
Patient Initial Operation Second Operation
Year Type Year Type Follow-Up
1 1978 C, CDD 3 mo, asymptomatic 4 1967 c, CDJ 1973 Revision CDJ 3 yr, asymptomatic 7 1981 c, CDJ 1 yr, asymptomatic
10 1976 C, CDJ, LHL 2 yr, asymptomatic 12 1982 C, CDD 2 mo, asymptomatic 13 1980 C, MJ 1 yr. asymptomatic 15 1976 C, CDD 2 yr, asymptomatic 16 1982 C, CDJ 1 yr, asymptomatic 20 1973 C, CDJ 1983 Drain liver abscess T tube 6 mo, asymptomatic
C = chokystectomy; CDD = choledochoduodenostomy: CDJ = choledochojejunostomy; HJ = hepaticojejunostomy; LHL = left hepatic
was lost to follow-up. In the nine patients who ini- tially underwent biliary enteric anastomoses, all were asymptomatic at follow-up which ranged from 3 months to 2 years postoperatively (Table III). However, one patient required revision of the chol- edochojejunostomy after 6 years and one patient underwent drainage of a liver abscess 10 years after the initial operation. In the group of 10 patients who had their second operation at San Francisco General Hospital (consisting of the previously described biliary enteric drainage operations), 1 patient refused reoperation and is doing well at the present time with a percutaneous biliary stent. Another of these pa- tients deserves special note since he presented in septic shock with pyopericardium and tamponade secondary to transdiaphragmatic erosion of a hepatic abscess. This patient required thoracotomy in ad- dition to laparotomy and a biliary enteric anasto- mosis. He is now doing well and is asymptomatic. There was no operative death in this series.
Comments
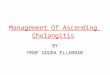
Oriental cholangitis is a well described but poorly understood clinical syndrome. Associations with a specific endemic area (Figure 1) and socioeconomic class, parasitic infections, and biliary tract bacterial colonization have been well documented [2,5,7,8]. However the common pathway to intrahepatic pig- ment stone formation remains speculative [8]. Biliary tract stasis that may be caused by parasites or have other causes, along with the very high incidence of biliary tract bacterial colonization, especially with E. coli or other bacteria that produce /3-glucuron- idase, seem to be necessary for the propagation of this syndrome of intrahepatic and extrahepatic pigment stones [5]. Men and women seem to be affected al- most equally, and there is a strong association with lower socioeconomic class (Table I). The natural history of the disease is one of chronic recurring bouts of cholangitis. Some patients have been reported to be symptomatic for more than 25 years. If hepato-
biliary infestation with Clonorchis sinensis or other parasites is truly the inciting agent of stasis and in- flammation with subsequent bacterial colonization, this is indeed a problem since there is no satisfactory therapy for clonorchiasis, and efforts would have to be directed toward preventive medical aspects in order to break the cycle of people ingesting the par- asites from certain fresh water fish [2]. In addition, it is known that Clonorchis sinensis may survive for 25 years of more in its host [2]. In some cases, biliary tract parasitic infestation may predispose to oriental cholangitis; however, several studies have demon-
Flgun, 1. Endemk area for orkntai chelangMs.
Volume 140,JuIy1984 119

Carmona et al
strated that oriental persons in the endemic areas have a high incidence of parasitic infection, including biliary tract infestation but never have development of oriental cholangitis [JO]. A more consistent ex- planation from the same endemic area may be asso- ciated with the fact that all of these patients have intrahepatic pigment stones or sludge and usually subsist on a low protein diet. The relationship may be that, as a result of the low protein diet, a deficiency of glucaro-1:4-lactone in the bile exists. This sub- stance normally inhibits endogenous p glucuronidase and also that produced by accumulating E. coli and other potential biliary tract pathogens. It is known that p glucuronidase catalyzes the reaction of bili- rubin glucuronide to bilirubin and glucuronic acid. The free bilirubin may then combine with calcium to form calcium bilirubinate pigment stones [IO]. This hypothesis has been substantiated in animal experiments [11]. In addition, animal and human studies suggest that the source of bacteria may be the portal system and not hematogenous spread or as- cending progression as is seen in ascending cholan- gitis [IO]. Although possibly multifactorial in nature, the evidence that has been accumulated thus far in this and other studies supports a probable cause (Figure 2).
The spectrum of clinical presentation is varied. In our study, 21 patients presented with abdominal pain, 15 patients presented with jaundice, 17 patients presented with chills, and 17 patients presented with fever. Leukocytosis and hyperbilirubinemia were also frequently present (13 and 18 patients, respectively). Other very important but often overlooked historical points are whether the patient lives in an endemic area and a history of abdominal pain with or without fever, chills, or jaundice. In our study, all 21 patients immigrated from an endemic area. Twenty had a history of abdominal pain, 12 had a history of jaun-
dice, 13 chills, 15 fever, and 4 parasite infection. All of our patients except possibly one had this history, and he may have also but his history was incom- plete.
After the clinicians index of suspicion has been raised, the diagnosis must be pursued in the most expedient, cost-effective manner. Earlier in this pa- tient group before the widespread availability and use of computerized tomography and sonography, patients usually underwent upper gastrointestinal series and some form of contrast visualization of the biliary tract or liver scans or both. All had their use- fulness, but often the diagnosis or complete assess- ment of the disease process could not be accom- plished because of failure of dye to bypass stones or strictured ducts. Transhepatic cholangiography and endoscopic retrograde cholangiography, when used after appropriate antibiotic preparation, offer a safe method to study the intrahepatic and extrahepatic biliary tract anatomy, but as was sometimes the case in our series, that may fail to fully document the ex- tent of disease because strictures may prevent filling of the proximal or distal areas of disease. More re- cently, ultrasonography and computerized tomog- raphy have been used successfully although ultra- sonography was inconsistent in demonstrating ductal disease and the soft pigment stones in some of our patients. However, in all patients in whom comput- erized tomography was used, the extent of intrahe- patic and extrahepatic disease was clearly defined with no associated morbidity. In addition, comput- erized tomography proved to be a useful screening tool in suspected cases and an excellent means for following patients postoperatively with this chronic relapsing disease [12].
The importance of quickly and correctly deter- mining the diagnosis is underscored in this series where nearly all patients who initially were treated with nondrainage biliary tract operations eventually needed reoperation consisting of some form of per- manent biliary tract decompression (Table II). These patients all continued to experience recurrences of their signs and symptoms in the interim period but had remarkable improvement after the second op- eration. Oriental cholangitis cannot be managed as we usually manage ascending cholangitis, that is, with cholecystectomy, common duct exploration, and T-tube drainage. Initial permanent biliary tract de- compressive or drainage procedures, such as chole- dochoduodenostomy, choledochojejunostomy, or in some cases, hepaticojejunostomy are necessary. In the 9 patients who initially underwent a bilioenteric anastomosis, their outcome was exceptionally good (Table III) in contrast with the 12 patients who ini- tially underwent nondrainage biliary operations (Table II).
We found no evidence to favor choledochoduode- nostomy over choledochojejunostomy other than
120 lM American Journal ol Surgery

Oriental Cholangitis
intraoperative anatomic findings that would preclude one or the other. Hepaticojejunostomy was used in one patient who was also found to have a choledochal cyst. Although infrequent, it’s use may also be war- ranted in those patients who present late and have common duct strictures in addition to the other findings consistent with oriental cholangitis. In pa- tients with unresectable strictures of the intrahepatic ducts or with a failed previous bilioenteric anasto- mosis, we favor a Roux-Y choledochojejunostomy with the end of the loop left in the subcutaneous tissue of the abdominal wall to allow later access for endoscopic or invasive radiologic manipulations, such as extracting stones or dilating strictures. As with other published reports [2,13], we found a predelic- tion for disease in the left hepatic lobe. All patients had some left lobe involvement, alone or in addition to other findings. When significant intrahepatic strictures or an abscess are present, we favor lobec- tomy whenever possible since this disease is of a chronic relapsing nature, and initial aggressive at- tempts to eradicate any future potential for increased morbidity are justified.
When available and carried out appropriately, the preoperative radiologic workup (especially com- puterized tomography) will help the surgeon deter- mine and plan the extent of surgery since frequently even intraoperative examination will not reveal the full extent of intrahepatic disease. As has been doc- umented in this study, incomplete assessment or operation almost ensures continued symptoms and reoperation.
Morbidity in this group of patients is difficult to characterize since most present with sepsis and some with other or associated conditions. However, all patients recovered to their premorbid condition, and there were no intraoperative or perioperative deaths.
The most important part of recognition of this increasingly encountered disorder is physician awareness. Although this disorder may appear as routine “western” cholelithiasis and ascending cholangitis, it is a different syndrome that requires a more comprehensive workup and different surgical intervention. A history of having lived in an endemic area, especially amdng the lower socioeconomic groups, along with previous episodes of abdominal pain, usually with jaundice, fever, and chills, should alert the astute clinician to entertain the diagnosis of oriental cholangitis and therefore pursue a more in depth preoperative workup of the hepatobiliary tree, including computerized tomography. Once the diagnosis of this chronically recurring disease is made and confirmed intraoperativels, a Dermanent biliarv tract drainage procedure is r&ndatory in order tb avoid unnecessary morbidity and reoperation. When encountered, intrahepatic strictures and abscesses are best managed by hepatic resection, hepaticoen-
terostomy if possible, or both. The syndrome of or- iental cholangitis has become more prevalent in western society over the past decade. However, if our clinical experience is typical, then there are un- doubtedly still many cases going unrecognized, misdiagnosed, and therefore, are not being treated properly.
Summary
Oriental cholangitis is a poorly understood syn- drome consisting of intrabepatic pigment stone for- mation with chronically recurrent exacerbations and remissions. Endemic to Asia, it is being encountered more frequently in the United States due to in- creased immigration of asians. Twenty-one patients with oriental cholangitis (9 men and 12 women), 19 to 84 years of age, all of whom immigrated from asian countries, were treated between 1970 and 1983. All had histories of episodic abdominal pain, most with jaundice, chills, and fever. Laboratory results were nonspecific but frequently included leukocytosis and hyperbilirubinemia. All patients were operated on with 15 having cholecystectomy, common duct ex- ploration, and a bilioenteric anatomosis. E. coli was cultured from specimens obtained from the biliary tracts of all patients, and 13 patients had more than one organism. Four patients had a previous history of parasitic infection, and four different patienta had parasites identified in the biliary tract intraopera- tively. Early recognition and appropriate operation will decrease morbidity and mortality.
References
1. Digby KH. Common duct stones of liver origin. Br J Surg 1930;17:578-91.
2. Yellin AE, Donovan AJ. Biliary lithiasis and helminthiasis. Am J Surg 1981;142:128-36.
3. Way LW. Current surgical diagnosis and treatment. Los Altos: Lange Medical, 198350%35.
4. ChoiTK,WongJ,DngGB.ThesurgkximaqemeMofprimary intrahepatic stones. Br J Surg 1982;89:88-90.
5. Tabata M, Nakayama F. Bacteria and gallstones: etiological significance. Dig Dis Sci 1981;26:218-24.
6. Sullivan WG, Koep LJ. Common bile duct obstruction and cholangiohepatitis in clonorchiasis. JAMA 1980;243: 2060- 1.
7. Stock FE, Fung JHY. Oriental cholangiohepatitis. Arch Surg 1962;84:409-12.
8. Stock FE. Drii cholangiohepetitii. In: abdomii qwa6ons. Maingot, ed, 7th ed. New York: Appleton-Century-Crofts. 1980;1268-74.
9. Ameres JP, Levine MP, Da Blasi HP. Acalculous clcnorchiasis obstructing the common bile duct. Am Surg 197642: 170-2.
IO. Chou ST, Ghan CW. Recwrent pyogsnic cholangiiis: a necropsy study. Pathology 1980;12:415-28.
11. Matsushiro T. Susuki N, Sato T, et al. Effects of diet on glucaric ackf concentration in bile and the formation of cai&m bil- irubinate gallstones. Gastroenterdogy 1977;72:630-3.
12. Federle MP, Cello JP, Laing FC, Jeffrey BFt Jr. Recurrent py- ogenic cholangitis in asian immigrants. Radiology 1982; 143:151-6.
Voluma 149, July 1994 121

Carmona et al
13. Choi TK, Wong J, Ong G8. The swgical management of primary intrahepatic stones. Sr J Surg 1982;89:88-90.
Discussion
Ronald K. Tompkins (Los Angeles, CA): Dr. Carmona and his coauthors have presented a nice analysis of this perplexing biliary problem. Their manuscript contains much important information regarding the theories of etiology and other methods of diagnosing and treating oriental cholangitis. I have little to add to their discussion except to emphasiie several key points. First, the diagnosis is often made by cholangiogram, but the extent of the disease is often not appreciated due to incomplete filling of the ductal system. Second, cholecystectomy alone is inadequate treatment as the gallbladder is very often not involved with stones but reflects secondary inflammation. The intrahepatic ductal strictures can often be dilated, and removal of stones in the proximal ducts can be effected. In this regard, the operative cholangioscope is indispensable. It is not uncommon for the surgeon to require several hours of diligent removal of stones to effect clearing of the in- trahepatic ducts. A word of caution-it should not be as- sumed that stone fragments in these proximal ducts will pass through the strictured areas and through the bi- lioenteric anastomosis. Often, they are of such size and shape (angled) that they are certain not to pass. The technique of crushing is most frequently required to reduce the size of these calcified masses and to remove them. Since stasis seems to play a prominent role in formation of pig- ment stones, it is important to perform a high bilioenteric anastomosis. We favor the Roux-Y hepaticojejunostomy or choledochojejunostomy for drainage. The transhepatic U tube has worked well in our experience and is used to provide a route for daily irrigation with saline solution which helps in flushing cholangitic mucus and stone debris from the ductal system.
I agree with the authors’statement that dietary factors play an important role in the cause. This was brought home to me by a patient with oriental cholangitis treated in the recent past. Although born in Japan, he moved to the United States as a young child and became Americanized in almost every way. He married a woman from South America, learned Spanish as a third language, and taught in high school. The one link to his homeland was his steadfast adherence to a Japanese rural diet of fish, rice, and vegetables. His presentation with oriental cholangitis was 28 years after moving to the United States and was typical of those patients who have immigrated recently. I side with those who theorize that this disease is acquired and not genetic.
Charles F. Frey (Sacramento, CA): We have had ex- perience with nine patients with oriental cholangitis at the University of California, Davis. Our experience supports the observations and recommendations of Dr. Carmona and his associates. There were two points made by Dr. Carmona and his coauthors that I would like to emphasize. First, there is difficulty in assessing the presence or absence of pigment stones in the intrahepatic radicals of the biliary tree by cholangiography alone whether it is endoscopic retrograde cholangiopancreatography, transhepatic chongiography, or T-tube cholangiography. Second, the necessity of resecting the portions of the liver, be it a seg-
ment or lobe, not adequately drained as a result of stric- tures of the corresponding bile duct must be accomplished if infection is to be eliminated from the biliary tree. Ra- diographs from a 29 year old Laotian man who entered our hospital in septic shock and underwent emergency chole- cystectomy and T-tube drainage of the common bile duct for suppurative cholangitis illustrate these points. The postoperative cholangiogram showed incomplete filling of the left hepatic duct and did not show any of the duct to the lateral segment. It was only after basketing a large number of stones that we began to recognize the extent of the disease involving the left hepatic duct. We found that we were unable to dilate or to crush the stones in the lateral segment of the left lobe of the liver, and at that point, we proceeded to resect the lateral segment which was mark- edly diseased and atrophic. We removed a large cast from the lateral segment. Bile cultures were positive for E. coli. Without resection we would never have dealt adequately with the disease.
Dr. Trunkey, what is your definition of a significant stricture of the intrahepatic ducts requiring resection? If you can dilate the stricture, is that going to be a permanent solution? With your large series, there is an opportunity to learn something of the natural history of oriental chol- angitis. Do you have any information as to what happens to the dilated abnormal external intrahepatic ducts after choledochojejunostomy or choledochoduodenostomy 2 to 5 years postoperatively? Do the ducts return to a more normal configuration? You did not employ sphincterop- lasty. Do you have any theoretic or actual observations that would discourage its use compared with choledochojeju- nostomy or choledochoduodenostomy.
Henry A. Pitt (Los Angeles, CA): I have one question relating to the pathogenesis and another regarding the management of patients with oriental cholangitis. With respect to pathogenesis, we know that these patients take in a diet high in carbohydrate, pigment stones form, they all have bactibilia, usually with E. coli, and some have parasites in their liver and bile. How these various factors result in stones throughout the biliary system, however, remains unclear.
As you know, our laboratory and clinical studies have strongly suggested that gallbladder stasis plays a key role in the pathogenesis of cholesterol gallstones and in the formation of pigment stones that develop in the gallbladder of patients receiving long-term total parenteral nutrition. Stasis in the gallbladder, however, is not sufficient to ex- plain the extensive stone disease that is seen in patients with oriental cholangitis. I wonder, therefore, whether stasis at the sphincter of Oddi could be a contributing pathogenic factor in oriental cholangitis. Dr. Trunkey, do you have any data on cholescintographic or manometric function or the endoscopic or pathologic appearance of the sphincter of Oddi in your patients with oriental cholangi- tis? Another question relates to the antibiotic management of these patients when they present with cholangitis. In recent years, four investigators have reported that anaer- obes can be isolated from the bile in 20 to 40 percent of patients undergoing biliary surgery and Bacteroides fragilis can be isolated in 10 to 20 percent of such patients. Further analysis of these studies, however, suggests that anaerobes are most likely to be recovered in elderly pa- tients, those who present with cholangitis, and those with
122 The Amerkan Journal of Surgery

Oriental Cholangitis
complex biliary problems. Since patients with oriental cholangitis have the last two of these criteria, I imagine that they would have a high incidence of anaerobes in their bile. Dr. Trunkey, how often were anaerobes found in your pa- tients, and when these patients present with cholangitis, should they receive antibiotics with specific coverage for anaerobic bacteria?
Leon Morgenstern (Los Angeles, CA): It should be stressed that one must know whether or not there is a stricture proximal to the enterohepatic stones or a bi- lioenteric anastomosis won’t work. We were forced to resect a segment of liver in a 43 year old Filipino man who had a sphincteroplasty followed by biliary sepsis and abscess formation. There were many dilated ducts. The liver, with marked dilated ducts, had a single pigment stone, although there were previously many others.
Dr. Tompkins mentioned the importance of choledo- choscopy or cholangioscopy. The routine cholangioscope is usually too large to get up past the secondary and tertiary ducts. We are now working with a prototype of a 1.5 mm endoscope which can go up into the very proximal ducts. If it fulfills its promise, I will perhaps show it next year.
Albert E. Yellin (Los Angeles, CA): Biliary tract hel- minthiasis occurs worldwide. Many parasites in addition to Clonorchis sinensis commonly invade the biliary tract. Being close to the Mexican border, we often see patients in whom Ascaris lumbricoides is the etiologic parasite. This parasite is often incorporated into the common duct stone. We reported our series of oriental cholangitis 3 years ago at this meeting.
The classic findings originally described by Digby in 1930 were a normal gallbladder, primary stones filling the common bile duct, stricture of the left hepatic duct with multiple stones, and distal abscess formation. We continue to see one or two such patients annually, and have had to perform four left hepatic lobectomies in patients with ad- vanced disease. In markedly dilated and thickened hepatic ducts filled with large, black friable stones, the hepatic parenchyma is almost totally replaced by fibrous tissue. It is unlikely that these strictures could be effectively di- lated. We also concluded that, for patients with Clonorchis sinensis related oriental cholangitis, cholecystectomy, common bile duct exploration, and biliary enteric anas- tomosis are essential to provide a drainage mechanism for the stones that continue to form as a result of the ongoing irritation caused by the parasite. Clonorchis sinensis re- mains viable in the biliary tree for 20 or more years, and there has been no drug capable of eradicating the parasite. In patients with Ascaris, lumbricoides can be eradicated. Therefore, there is no further stone formation and biliary enterostomy is unnecessary.
Within the past month the Food and Drug Adminis- tration has approved the use of a new drug, praziquantel, for Clonorchis sinensis. A single day of therapy clears the parasite in 99 percent of cases. Now, for the first time, the inciting mechanism can be eradicated, and hopefully, the problem of strictures, recurrent stones, and the need for biliary enterostomy will be avoided. Incidentally, this drug also eliminates schistosomiasis which has caused even greater worldwide morbidity from periportal fibrosis and portal hypertension. Assuming that we now can eradicate
the Clonorchis sinensis, Dr. Trunkey, would you care to speculate on whether routine bilioenteric anastomoses could be avoided, and should symptomatic strictures later develop, could we dilate them percutaneously or with peroral retrograde cholangioscopy?
Nicholas A. Halasz (San Diego, CA): I would like to add two points. One is that the importance of strictures cannot be overestimated. We have found these to be present in over three quarters of our patients. Dr. Ong, who probably has the largest experience in the world with this condition, routinely dilates and does few resections. On the other hand, if one looks at the thick, fibrous capsule around the duct, it is difficult to visualize how it could be dilated. Maybe Dr. Ong treats an earlier phase of the disease than we see. Much as Dr. Tompkins described, we have used U tubes in most of these patients. Since the ducts are tightly packed with material that has the consistency of hard plasticine, it is often very difficult to get every last bit of foreign material out. Therefore, after working on a duct for an hour or two, one decides to put in a U tube and let the interventive radiologist continue with the procedure during the following weeks. This is particularly true when much granulation tissue is present, and the ductal system bleeds. My other comment has to do with antibiotics. Since most of these patients do not have complete obstruction, a drug secreted into the biliary tree is excellent for protecting patients during their postoperative period of ductal ma- nipulation. Two drugs of this type with a good antibacter- ial spectrum exist: cefoperazone and doxycycline. We have maintained our patients with suppressive doses of these drugs, and have had minimal problems with cholan- gitis.
Donald D. Trunkey (closing): Dr. Frey, concerning what type of pathologic condition that would persuade us to do a resection; if the left lobe was atrophied, that would be the one hallmark for doing a resection, but another is the one that you outlined. If you do not believe that you can dilate the ducts on the left side, then resection probably would be appropriate. You also asked what happens to these dilated ducts. They stay dilated, and in our experi- ence, they do not reduce in size over time. In fact, they have almost a hard cast around them. In our opinion, sphinc- teroplasty is not beneficial in this advanced group of pa- tients. The reason is that I don’t think it is where the pa- thology is. I think the abnormality is primarily in the common and intrahepatic ducts. I don’t think the sphincter plays a role in stasis either. Dr. John Cello, our gastroen- terologist, has done two endoscopic retrograde cholan- giopancreatographic studies on these patients, and in both instances, the sphincter appeared normal, and the distal duct did not appear to be involved in the disease process. Dr. Pitt, I don’t know that stasis doesn’t play a role, but I am convinced that this is a metabolic disease and that it involves the entire duct. In our series, 30 percent of the patients had anaerobic organisms within the ducts, and for that reason, I recommend something like metranidazole concomitant with other antibiotics. We agree with Dr. Morgenstern that cholangiograms cannot specify the di- agnosis all the time. They do not show all the diseased areas, but computerized tomographic scans have been very helpful, and we believe this is a better diagnostic tool than
Volume148,July1984 123

Carmona et al
the cholangiogram. We have an unwritten rule at the San Francisco General Hospital that when someone comes to the emergency room with jaundice and fever, that they receive an ultrasonographic examination. If the ducts are dilated, they go to surgery, and if the ducts are not dilated, they go to the medical floor.
Dr. Yellin, we don’t think parasites are the primary cause of disease because only four of our patients had demon-
strated parasites. Some of them may have had parasites at previous times. They may contribute to the disease pro- cess but they probably are not the primary cause. I don’t think that praxiquantel would alter the disease process be- cause parasites probably are not the primary cause of the problem. We still recommend that these patients have a drainage procedure, primarily a choledochoenter- ostomy.
124 The Amerlcnn Journal of Surgery