Embed Size (px)
Citation preview

J Med Dent Sci 2011; 58: 49-59
Corresponding Author: Mihoko AkiyoshiTokyo Medical and Dental University, Graduate School of Health Care Sciences Biomedical Laboratory Sciences, Anatomy & Physiological Sciences, 1-5-45 Yushima Bunkyo-ku, Tokyo 113-8519 JAPANTel: 03-5803-5322 Fax: 03-5803-0295E-mail: [email protected] January 7;Accepted March 11, 2011
Original Article
Relationship between estrogen, vasomotor symptoms, and heart rate variability in climacteric women
Mihoko Akiyoshi1), Kiyoko Kato2), Yoko Owa2), Michiko Sugiyama3), Naoyuki Miyasaka2), Satoshi Obayashi2), Toshiro Kubota2), Takeshi Aso2), Tetsuya Kimura4), Toshio Moritani5) and Kenji Sato1)
1) Tokyo Medical and Dental University, Graduate School of Health Care Sciences, Anatomy and Physiological Sciences2) Tokyo Medical and Dental University, Graduate School of Medical and Dental Sciences, Comprehensive Reproductive Medicine3) Kanagawa University of Human Services4) Ritsumeikan University5) Kyoto University
The present study investigated resting cardiac autonomic function in Japanese climacteric women using heart rate variability (HRV) power spectral analysis to evaluate the relationship between HRV indices and estrogen, as well as the ability of each HRV index to predict vasomotor symptoms. Forty-five peri- and postmenopausal women completed a questionnaire about the presence of vasomotor symptoms (hot flashes, sweating). To analyze the relationship between HRV and hot flashes or sweating, we classified subjects into groups based on symptoms and combinations of symptoms: no hot flashes (H1), hot flashes (H2), non-sweating (S1), sweating (S2), neither hot flashes nor sweating (V1), either hot flashes or sweating (V2), and both hot flashes and sweating (V3). Values for total power and the low-frequency component of HRV were significantly lower in the H2 group than in H1 ( p < 0.05); values for total power and the high-frequency and low-frequency components of HRV were significantly lower in group S2 than S1 ( p < 0.05); and values for total power and the
high-frequency and low-frequency component of HRV were significantly lower in groups V2 and V3 compared to V1 ( p < 0.05). Clinical diagnosis of climacterium relies upon subjective complaints of patients. Our findings suggest that HRV indices may help to evaluate vasomotor symptoms.
Key words: Climacteric, estrogen, vasomotor symptoms, autonomic nervous system, heart rate variability
Introduction
Cl imacter ium signif ies a transit ion from the reproductive to non-reproductive period1 in a woman’s life, corresponding to the time around menopause, which is the permanent cessation of menstruation due to loss of ovarian function.2 Menopause typically occurs between the ages of 45 and 56 years (median age, 50.5 years) in Japanese women.3 During climacterium, a myriad of vague symptoms centered around vasomotor symptoms arise (e.g., hot flashes and sweating), as well as emotional symptoms (e.g., depression and anxiety), shoulder stiffness, and fatigability. These climacteric symptoms can greatly detract from health and quality of life. 4 Hot flashes and sweating are the most common symptoms, experienced by 65% to 76% of menopausal women.5 Hot flashes, expressed as a “burning feeling in the face,” is a symptom of climacterium generally used in clinical practice. It is thought to be a sensation

50 J Med Dent SciM. Akiyoshi et al.
of heat that suddenly occurs around the chest, neck, face and head,6 but the underlying mechanisms of pathogenesis have yet to be explained. Although the rapid decline in estrogen is considered a contributing factor in hot flashes and sweating, symptoms vary even among women with similar levels of estrogen. The relationship between estrogen and the autonomic nervous system is also unclear. The diagnosis of climacterium is currently based on the patient’s subjective complaints, and is therefore not objective. The autonomic nervous system is divided into sympathetic and parasympathetic nervous systems. These two systems cooperatively regulate functions such as respiration, digestion, endocrine system, body temperature maintenance, and reproduction, while exerting reciprocal or antagonistic control over various internal organs. In this way, they play an important role in maintaining homeostasis. Various methods have been developed to test autonomic function, including one reported by Akselrod et al., 7 which is a popular noninvasive and objective quantitative technique based on heart rate variability (HRV). 8-14 Although the heart appears to beat with a regular sinus rhythm, periodic fluctuations are caused by autonomic activities such as respiration and circulation. Sands et al. 15 reported that these fluctuations disappear in a transplanted heart with completely severed autonomic nerves, resulting in a regular metronome-like rhythm. These fluctuations in the autonomic nervous system input to the sinus node and are widely used to evaluate autonomic function and make prognostic predictions for heart disease. Park et al. 16 assessed HRV in 637 healthy men and women to establish standard values for HRV indices. Kleiger et al. 17 found that reductions in HRV indices in patients with acute myocardial infarction were strongly associated with mortality during the follow-up period. Here we assessed autonomic function in climacteric women by analyz ing HRV, and evaluated the association between HRV indices and estrogen. Furthermore, we used each of these indices to evaluate vasomotor symptoms (hot flashes, sweating) from the perspective of cardiac sympathetic/parasympathetic nerves.
Materials and Methods
Subjects Subjects were 133 women (mean age±SE, 50.9±0.5 years) who had undergone a climacteric outpatient examination at the Department of Maternal and Woman’s Clinic in the University Hospital of Medicine at
Tokyo Medical and Dental University, for the purpose of improving climacteric symptoms or health maintenance. The study protocol was approved by the medical ethics committee of Tokyo Medical and Dental University and carried out in accordance with the Declaration of Helsinki. The study purpose and procedures were explained in detail to all subjects in advance, and their intent to participate in the study was obtained by written consent. All subjects underwent physical measurements and completed a questionnaire that included items about the presence/absence of vasomotor symptoms (hot flashes, sweating), clinical history, medications, presence/absence of menstruation, age at menopause, form of menopause, smoking status, alcohol intake, and exercise habits. Exclusion criteria were diabetes, hypertension, cardiac disease, thyroid disease, current use of hormone replacement therapy, and surgical removal of uterus or ovaries. We also excluded women who exercised regularly, smoked, or drank heavily. Of the 133 subjects, the relationship between vasomotor symptoms and HRV were evaluated in 45 perimenopausal and menopausal women (blood estradiol [E2] ≤50 pg/mL, follicle-stimulating hormone (FSH) levels ≥40 mIU/mL, and 6 months to 5 years without menstruation). To eliminate the effects of food intake on test results, we confirmed that at least 3 h had elapsed after eating before beginning the tests. To determine the relationship between HRV and hot flashes or sweating, subjects were classified into groups based on symptoms and combinations of symptoms: no hot flashes (H1), hot flashes (H2), non-sweating (S1), sweating (S2), neither hot flashes nor sweating (V1), either hot flashes or sweating (V2), and both hot flashes and sweating (V3).
Research protocol We measured each subject’s height and weight and calculated the body mass index (BMI). Subjects rested for 20 min, and then electrodes were attached after lowering skin resistance with alcohol. The thoracic electrocardiogram (CM5) was measured continuously for 5 min while the subjects were in a supine position. Measurements were obtained at a respiratory rate of 0.25 Hz (15 times/min) using a digital metronome. All measurements were performed between 9 AM and 3 PM in a quiet room maintained at 25°C.
HRV power spectral analysis We performed HRV power spectral analysis, in which Fourier transformation is used for frequency

51HRV in climacteric women
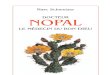
domain analysis of RR interval data obtained from electrocardiograms, and frequency components are expressed as a power spectrum. The power spectral analysis method used in the present study is summarized in Figure 1. We first amplified the CM5 electrocardiogram with a multi-channel amplifier (AB-622M, Nihon Kohden, Tokyo, Japan) and performed analog-to-digital conversion (Model PS-2032 GP, TEAC, Tokyo, Japan) at 1000 Hz. Using a computer algorithm created in HTBasic (Trans Era, Utah, USA), we then obtained the RR interval with a precision of 1 ms and calculated the interval time-series data. In accordance with previous studies,18 we converted the data into 2-Hz equidistant sampling (Fig. 1b). We removed the DC component and trends from the RR interval time-series data using a numerical filter, performed a high-speed Fourier transform on 512 consecutive data points through a Hamming-type data window, and calculated the power of each frequency component of HRV (Fig. 1c). From this power spectrum (curve expressing the relationship between frequency and power), the HF component reflecting cardiac parasympathetic function (0.15–0.5 Hz) and LF component reflecting cardiac sympathetic and parasympathetic functions (0.03–0.15 Hz) were quantified (Fig. 1c). The HF and LF components were added to calculate the total power (TP; 0.03–0.5 Hz) to
evaluate total autonomic function11-14. We did not assess LF/HF because it could not reflect interindividual differences. While there are some reports that use LF/HF as an indicator of sympathetic activity 19, one study has reported that these indicators did not adequately reflect differences at the interindividual level of sympathetic activity. 20 Furthermore, it has been reported that LF/HF and properties inversely proportional to the size of the HF component, and it was possible that changes in LF/HF were at least partially due to inverse changes in cardiac parasympathetic function by definition20. These values were expressed as natural logarithms (ln) in accordance with previous studies. 21
Blood sample collection and analysis Blood samples were collected after electrocardiography was performed. E2 levels were determined with an electrochemiluminescence immunoassay (ECLIA) (Roche Diagnostics), and FSH levels were determined with a fluorometric enzyme immunoassay (Tosoh). These values were converted to natural logarithms.
Statistical analysis Statistical analysis was performed with StatView v. 5.0 (StatView for Windows, SAS Institute Inc, Cary, NC, USA). Relationships between age, sex hormone levels,
High Frequency Power (HF) Low Frequency
Power (LF)
Total Power(TP) = LF+HF
Figure 1 : Representative heart rate variability power spectral analysis.a) Electrocardiogram (ECG); b) ECG R-R interval changes; c) heart rate variability (HRV) power spectra. The HRV power spectral analysis identified two separate frequency components, high (0.15-0.5Hz) and low (0.03-0.15 Hz), which are represented by white and black areas, respectively.

52 J Med Dent SciM. Akiyoshi et al.
and each HRV index were evaluated using Pearson’s correlation coefficient, followed by stepwise multiple regression. Groups based on presence/absence of vasomotor symptoms were compared by unpaired t-test and one-way analysis of variance. Results are expressed as mean ± standard error; p<0.05 was considered significant.
Results
Anthropometric and clinical characteristics of the 133 subjects are shown in Table Ⅰ. As shown in Figure 2, TP and the HF and LF components of HRV decreased with increasing age (HF component: r = -0.285, p < 0.01; LF component: r = -0.273, p < 0.01; TP: r = -0.305, p < 0.01). E2 levels were positively correlated with the HRV indices (HF component: r = 0.307, p < 0.001; LF component: r = 0.283, p < 0.001; TP: r = 0.344, p < 0.001), whereas FSH levels were negatively correlated with HRV indices (HF component: r = -0.219,
Variables n = 133
Age (years) 50.9 ± 0.5Height (cm) 157.4 ± 0.5Weight (kg) 54.6 ± 0.9Body mass index (kg/m2) 22.0 ± 0.3Heart rate (beats/minutes) 67.2 ± 0.8Systolic pressure (mm Hg) 125.1 ± 1.5Diastolic pressure (mm Hg) 76.2 ± 0.9Estradiol (pg/mL) 85.6 ± 7.5FSH (mIU/mL) 59.1 ± 3.9LDL-C (mg/dL) 122.9 ± 3.2HDL-C (mg/dL) 74.5 ± 1.5Triglycerides (mg/dL) 107.3 ± 8.0Blood glucose (mg/dL) 96.8 ± 1.1Menarche (years) 12.9 ± 0.1Pregnancies (n) 2.0 ± 0.1Childbirths (n) 1.5 ± 0.1
FSH, follicle-stimulating hormone; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density cholesterol.
� � � � � �
Figure 2 : Correlations between age or sex hormone levels and heart rate variability (HRV).a) Age and HRV are negatively correlated (high-frequency [HF] component: r=-0.285; low-frequency [LF] component: r=-0.273; total power [TP]: r=-0.305; p<0.05). b) Estradiol (E2) and HRV are positively correlated (HF component: r=0.307; LF component: r=0.283; TP: r=0.344; p<0.05). c) FSH and HRV are negatively correlated (HF component: r=-0.219; LF component: r=-0.242; TP: r=-0.258; p<0.05).
Table Ⅰ. Anthropometric and clinical characteristics of subjects.

53HRV in climacteric women
p < 0.05; LF component: r = -0.242, p < 0.01; TP: r = -0.258, p < 0.01). Stepwise multiple regression analysis was performed to determine the significance of age and sex hormone levels on HRV (Table Ⅱ). E2 levels were found to predict the HF component, with a standardized regression coefficient of 0.307. E 2 levels also predicted the LF component, with a standardized regression coefficient of 0.283. For TP, E2 levels were selected first, followed by age with standardized regression coefficients of 0.257 and -0.185, respectively.
Relationship between vasomotor symptoms and HRV Demographic and clinical data for subjects are shown according to presence/absence of vasomotor symptoms (hot flashes, sweating) in Table Ⅲ. The women in groups H1 (no hot flashes) and H2 (experiencing hot flashes) did not differ by age, years after menopause, E2 levels, or FSH levels. However, the mean heart rate of group H2 (70.4 ± 1.6 beats/min) was significantly higher than that of H1 (65.2 ± 2.2 beats/min; p < 0.05). In addition, values for lnTP and the lnLF component of HRV were
Standardized regressioncoefficient
Partial correlationcoefficient F-value P-value
HF(R2 = 0.088)
Age0.307
-0.168 3.7670.001Estradiol 13.676
FSH -0.016 0.032
LF(R2 = 0.073)
Age0.283
-0.166 3.6990.01Estradiol 11.412
FSH -0.072 0.672
TP(R2 = 0.132)
Age -0.185 4.0580.001Estradiol 0.257 7.861
FSH 0.024 0.075
FSH = Follicle-stimulating hormone; HF = high frequency component of HRV; LF = low frequency component of HRV; TP = total power of HRV.
VariablesHot flashes Sweating
no hot flashes(H1, n=11)
hot flashes(H2, n=34)
non-sweating(S1, n=5)
sweating(S2, n=40)
Age (years) 51.7 ± 1.2 51.8 ± 0.6 50.8 ± 1.4 51.9 ± 0.6Years after menopause (years) 1.4 ± 0.5 1.4 ± 0.2 1.4 ± 0.6 1.4 ± 0.2Height (cm) 159.2 ± 1.9 157.1 ± 0.8 160.4 ± 1.4 157.2 ± 0.8Weight (kg) 56.3 ± 2.3 54.8 ± 1.4 53.4 ± 1.2 55.4 ± 1.3Body mass index (kg/m2) 22.3 ± 1.2 22.3 ± 0.6 20.8 ± 0.6 22.5 ± 0.6Heart rate (beats/minutes) 65.2 ± 2.2 70.4 ± 1.6* 60.3 ± 2.9 70.3 ± 1.4*Systolic pressure (mm Hg) 128.0 ± 4.7 130.5 ± 3.1 117.0 ± 6.4 131.5 ± 2.7*Diastolic pressure (mm Hg) 78.4 ± 3.2 78.8 ± 2.0 70.0 ± 3.9 79.8 ± 1.8*Estradiol (pg/mL) 24.5 ± 3.8 23.4 ± 2.2 27.8 ± 7.0 23.1 ± 2.0FSH (mIU/mL) 90.8 ± 6.9 94.9 ± 5.9 98.3 ± 11.6 93.4 ± 5.1LDL-C (mg/dL) 138.2 ± 12.0 135.0 ± 5.6 127.6 ± 16.5 137.0 ± 5.4HDL-C (mg/dL) 71.4 ± 5.9 74.1 ± 3.3 81.0 ± 10.3 72.4 ± 2.9Triglycerides (mg/dL) 102.5 ± 15.4 125.7 ± 15.9 75.8 ± 6.9 125.5 ± 13.9Blood glucose (mg/dL) 96.6 ± 2.3 98.8 ± 1.5 92.2 ± 2.6 99.0 1.3*
FSH, follicle-stimulating hormone; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density cholesterol.Results are expressed as mean±SE; P<0.05.
Table Ⅱ. Stepwise multiple regression analysis of heart rate variability (HRV) indices with age and sex hormones as predictive variables (n=133).
Table Ⅲ. Anthropometric and clinical characteristics of subjects (n=45).

54 J Med Dent SciM. Akiyoshi et al.
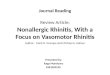
significantly lower in the H2 group than in H1 (group H1 vs. H2; lnLF, 4.9 ± 0.3 vs. 4.4 ± 0.1 ms2, p < 0.05; lnTP, 5.6 ± 0.3 vs. 5.2 ± 0.1 ms2, p < 0.05) (Fig. 3a). Similarly, no differences were observed between group S1 (no sweating) and S2 (experiencing sweating) in age, years after menopause, E2 levels, or FSH levels (Table Ⅲ). However, heart rate, systolic blood pressure, diastolic blood pressure, and blood glucose levels were significantly higher in group S2 than in S1 (group S1 vs. S2; heart rate, 60.3 ± 2.9 vs. 70.3 ± 1.4 beats/min; systolic blood pressure, 117.0 ± 6.4 vs. 131.5 ± 2.7 mmHg; diastolic blood pressure, 70.0 ± 3.9 vs. 79.8 ± 1.8 mmHg; blood glucose levels, 92.2 ± 2.6 vs. 99.0 ± 1.3 mg/dL; p < 0.05). In addition, as shown in Fig. 3b, values for lnTP and the lnHF and lnLF components of HRV were significantly lower in group S2 than S1 (group S1 vs. S2; lnHF, 5.5 ± 0.4 vs. 4.4 ± 0.2 ms2, p < 0.01; lnLF, 5.8 ± 0.3 vs. 4.4 ± 0.1 ms 2, p < 0.001; lnTP, 6.4 ± 0.3 vs. 5.1 ± 0.1 ms2, p < 0.001). Representative electrocardiogram RR intervals and their corresponding power spectral data are shown for women who experienced neither hot flashes nor sweating (V1) and women who experienced both hot flashes and sweating (V3) (Fig. 4). Table Ⅳ shows demographic and clinical characteristics according to group: V1, V2 (women who experienced either hot flashes or sweating), and V3. The groups did not differ by age, years after menopause, E 2 levels, or FSH
levels. However, heart rate, systolic blood pressure, diastolic blood pressure, and blood glucose levels were significantly higher in group V2 than in V1 (group V1 vs. V2; heart rate, 60.3 ± 2.9 vs. 69.3 ± 2.3 beats/min; systolic blood pressure, 117.0 ± 6.4 vs. 137.2 ± 4.0 mmHg; diastolic blood pressure, 70.0 ± 3.9 vs. 85.3 ± 2.4 mmHg; blood glucose level, 92.2 ± 2.6 vs. 100.3 ± 3.1 mg/dL; p < 0.05). In addition, mean heart rate in group V3 (70.4 ± 1.6 beats/min) was significantly higher than that of V1 (60.3 ± 2.9 beats/min; p < 0.05). Furthermore, as shown in Fig. 5, values for lnTP and the lnHF and lnLF components of HRV were significantly lower in groups V2 and V3 than in V1 (group V1 vs. V2 vs. V3; lnHF, 5.5 ± 0.4 vs. 4.2 ± 0.3 vs. 4.4 ± 0.2 ms2, p < 0.05; lnLF, 5.8 ± 0.3 vs. 4.2 ± 0.3 vs. 4.4 ± 0.1 ms2, p < 0.05; lnTP, 6.4 ± 0.3 vs. 5.0 ± 0.2 vs. 5.2 ± 0.1 ms2, p < 0.05).
Discussion
Hot flashes and sweating are the most common vasomotor symptoms of climacterium.22,23 At our climacteric outpatient clinic, approximately 70% of patients report both symptoms, which like depression and insomnia, affect physical and mental functioning and quality of life. 4 Although the estrogen reduction associated with menopause is considered the main cause of vasomotor symptoms, the pathophysiology
Figure 3 : Relationship between vasomotor symptoms (hot flashes, sweating) and heart rate variability (HRV).a) The low-frequency (LF) component and total power (TP) of HRV of Group H2 were significantly lower than those of H1. b) The HF component, LF component, and TP of HRV in Group S2 were significantly lower than those in S1. *p<0.05 vs. group without vasomotor symptoms (vs); **p<0.01 vs. group without vs; ***p<0.001 vs. group without vs.

55HRV in climacteric women
is not completely understood. 5,23,24 Furthermore, although vasomotor symptoms are mediated by the sympathetic nervous system and HRV changes appear to be associated with estrogen fluctuations, 25,26 the relationship between estrogen and the autonomic nervous system is not c lear . 27-29 Reports of a relationship between estrogen and HRV have focused
on the effects of hormone replacement therapy in postmenopausal women25,29,30 or on HRV during the menstrual cycle in premenopausal women,31-33 but few studies have reported the relationship between estrogen and HRV during the perimenopausal period. Further, we are not aware of studies that have investigated the relationship between HRV, estrogen,
Variables No hot flashes or sweating(V1, n=5)
Either hot flashes or sweating(V2, n=6)
Both hot flashes and sweating(V3, n=34)
Age (years) 50.8 ± 1.4 52.5 ± 1.9 51.8 ± 0.6Years after menopause (years) 1.4 ± 0.6 1.3 ± 0.7 1.4 ± 0.2Height (cm) 160.4 ± 1.4 158.1 ± 3.3 157.1 ± 0.8Weight (kg) 53.4 ± 1.2 58.6 ± 3.9 54.8 ± 1.4Body mass index (kg/m2) 20.8 ± 0.6 23.6 ± 2.0 22.3 ± 0.6Heart rate (beats/minutes) 60.3 ± 2.9 69.3 ± 2.3* 70.4 ± 1.6*Systolic pressure (mm Hg) 117.0 ± 6.4 137.2 ± 4.0* 130.5 ± 3.1Diastolic pressure (mm Hg) 70.0 ± 3.9 85.3 ± 2.4** 78.8 ± 2.0Estradiol (pg/mL) 27.8 ± 70 21.8 ± 4.2 23.4 ± 2.2FSH (mIU/mL) 98.3 ± 11.6 84.6 ± 8.3 94.9 ± 5.9LDL-C (mg/dL) 127.6 ± 16.5 147.0 ± 17.6 135.0 ± 5.6HDL-C (mg/dL) 81.0 ± 10.3 63.3 ± 5.2 74.1 ± 3.3Triglycerides (mg/dL) 75.8 ± 6.9 124.7 ± 25.0 125.7 ± 15.9Blood glucose (mg/dL) 92.2 ± 2.6 100.3 ± 3.1* 98.8 ± 1.5
FSH, follicle-stimulating hormone; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density cholesterol.Results are expressed as mean±SE. *P<0.05; **P<0.01.
a) b)
Table Ⅳ. Anthropometric and clinical characteristics of subjects according to combination of symptoms (n=45).
Figure 4 : Representative electrocardiogram R-R interval changes and corresponding power spectra for resting women a) without vasomotor symptoms (hot flashes, sweating) or b) with vasomotor symptoms (both hot flashes and sweating).

56 J Med Dent SciM. Akiyoshi et al.
and vasomotor symptoms in perimenopausal Japanese women. Therefore, we evaluated resting cardiac autonomic function in climacteric women using HRV power spectral analysis. We evaluated the relationships between HRV indices and estrogen, as well as the ability of each HRV index to predict vasomotor symptoms. HRV is separated by power spectral analysis into frequency components of the cardiac sympathetic and parasympathetic nerves, and is used to assess autonomic function under a variety of physiologic or clinical conditions. 9-14,16,17,25,27,31-33
HRV power spectral analyses are carried out considering RR time series data as a set of continuous waves. RR interval time-series data generally show bimodal peaks for resting healthy subjects, with a high-frequency (HF) component centered around 0.25 Hz and a low-frequency (LF) component centered around 0.1 Hz. 7,19,34 The origin of the HF component is the heartbeat fluctuation caused by breathing (e.g., 15 breaths/60 sec=0.25 Hz), whereas the LF component is thought to arise from blood pressure variability at Mayer wave frequencies (10-sec cycle=0.1 Hz) resulting from the baroreceptor reflex. Due to different signal transduction pathways of sympathetic nerve β- receptors and parasympathetic nerve acetylcholine receptors, human cardiac sympathetic nerve activity is
lower than 0.15 Hz, whereas cardiac parasympathetic nerve activity reaches 1 Hz. 35 HF and LF components of HRV are almost eliminated when atropine (0.04 mg/kg) is administered, whereas intravenous administration of propranolol (0.2 mg/kg) decreases the standing LF component with little effect on the resting LF component. The origin of each component and experimental results indicate that the HF component is mediated solely by the cardiac parasympathetic nerve, whereas the LF component is mediated by both sympathetic and parasympathetic nerves. 7,34 Therefore, we used the HF component as an indicator of cardiac parasympathetic nerve activity and the LF component as an indicator of both cardiac sympathetic and parasympathetic nerve activities. In the present s tudy , we per formed 5 -m in electrocardiography, which is a simple, non-invasive measurement that is practical and effective as a test for climacteric women with numerous unidentified complaints. Electrocardiography is frequently performed during ordinary physical examinations and is well accepted by patients. There are few contraindications for this test; therefore, it was thought to be suited for application in climacteric outpatient clinics. In the present study of resting cardiac autonomic function in climacteric women, we observed that TP and the HF and LF components of HRV decrease with
Figure 5 : Relationship between vasomotor symptoms (hot flashes, sweating) and heart rate variability (HRV).The HF component, LF component, and TP of HRV of Groups V2 and V3 were significantly lower than those of V1. *p<0.05 vs. V1; **p<0.01 vs. V1; ***p<0.001 vs. V1.

57HRV in climacteric women
age. These results are consistent to results of previous studies. 26,31,36,37 We also found that the decrease in cardiac parasympathetic system function was dependent on sex hormones; TP and the HF and LF components decreased with the reduction in estrogen and increase in FSH. Multiple regression analysis revealed that estrogen exerted a stronger influence than age on HRV. TP and the HF and LF components of HRV were lower in women who experienced vasomotor symptoms than in women without these symptoms, suggesting that cardiac parasympathetic function had decreased. Given that blood pressure and heart rate were significantly higher in women with vasomotor symptoms as well, the sympathetic system was presumed to be compensating. Cardiac parasympathetic function decreases in climacteric women due to the physiologic changes of aging itself and changes in endocrine physiology ( i .e. , estrogen reduction accompanying natural menopause). Many issues are unclear with respect to the significance of menopause in aging for climacteric women.38 Our results demonstrated that the impact of estrogen decrease unique to women is stronger than the effect of age on cardiac parasympathetic function. The decline in cardiac parasympathetic function with respect to aging is thought to be due to lower cardiac parasympathetic activity, changes in the heart, or both. Mechanisms by which estrogen may control autonomic nerves include: 1) changes in hypothalamic–pituitary system activity mediated by the negative feedback of estrogen, 2) control of hypothalamic estrogen receptor-positive neurons that project to medullary autonomic centers, and 3) actions in peripheral organs. 39
Even under the similar hormonal environment of rapid estrogen reduction caused by natural menopause, women with vasomotor symptoms showed lower cardiac parasympathetic function and a greater compensation of the cardiac sympathetic system than women without those symptoms. Thus, some factor other than aging or menopause appears to increase the risk of developing these symptoms. Potential factors that may affect the autonomic nervous system in this way include lack of exercise, 12,40 poor eating habits, 41 and mental stress. 42
Although few studies have examined the relationship between vasomotor symptoms and HRV, Rebbeca et al. evaluated 24-h electrocardiograms of perimenopausal women and reported that the HF component of HRV decreases during hot flashes. 43 Hoikkala et al. performed similar studies and suggested that changes in cardiac autonomic control may be involved in the mechanism of hot flashes. 44 Our findings do not reveal
the precise mechanism by which vasomotor symptoms occur in climacteric women; however, decreased rest ing cardiac parasympathet ic funct ion and compensation of sympathetic nerves appear to play a role. Clinical diagnosis of climacterium relies upon the subjective complaints of patients; therefore, an objective method is needed. In this study, we observed a relationship between vasomotor symptoms and HRV, suggesting that HRV indices may be useful to evaluate symptoms. Future studies will investigate the relationship of climacteric symptoms to the autonomic nervous system and further investigate whether HRV could be used as an objective quantitative assessment to diagnose climacteric syndrome or assess treatments such as hormone replacement therapy. A limitation of this study was the assessment of resting HRV only; we did not perform electrocardiography during the occurrence of vasomotor symptoms. To capture the effects of transient vasomotor symptoms that occur suddenly and determine their relationship to HRV, studies such as those using a Holter monitor should be considered.
Acknowledgements
We wish to express our appreciation to Dr. Tokuhiro Kawara, Department of Biofunctional Informatics, Graduate School of Health Care Sciences, Tokyo Medical and Dental University, for his constructive suggestions and cooperation.
References1. Utian WH, Serr D. The climacteric syndrome/ van
Keep PA, Greenblatt RB, Fernet A, et al. Consensus on menopause research. MTP Press, Lancaster. 1976; 1-4.
2. Utian WH. Editorial, menopause - A proposed new functional definition. Maturitas. 1991; 14 (1).
3. Japan Society of Obsterics and Gynecology Education/Terminology Committee Report. Reasons for committee proposal regarding “Menopause age among Japanese women.” The Journal of Obsterics and Gynaecology Research(in Japanese). 1995; 47: 449-451.
4. Avis NE, Ory M, Matthews KA, et al. Health- related quality of l ife in a multiethnic sample of middle- aged women. Study of Women’s Health across the Nation(SWAN). Med Care. 2003; 41: 1262-76.
5. Randolph JF Jr., Sowers M, Bondarenko I, et al. The relationship of longitudinal change in reproductive hormones and vasomotor symptoms dur ing the menopausal transition. J Clin Endocrinol Metab. 2005; 90: 6106-12.

58 J Med Dent SciM. Akiyoshi et al.
6. Aso T, ed. General outpatient treatment of women- fundamentals and practice (in Japanese).Bunkodo. Tokyo. 2007: 68.
7. Akselrod S, Gordon D, Ubel FA, et al. Power spectrum analysis of heart rate fluctuation: a quantitative probe of beat-to-beat cardiovascular control. Science. 1981; 213: 220-222.
8. Task force of the European Society of Cardiology and the North American Society of Pacing and Electro-physiology. Heart rate variability. Standard of measurements, physiological interpretation and clinical use. Circulation. 1996; 93: 1043-1065.
9. Moritani T, Kimura T, Hamada T, et al. Electro-physiology and kinesiology for health and disease. J Electromyogr Kinesiol. 2005; 15: 240-255.
10. Kimura T, Matsumoto T, Akiyoshi M, et al. Body fat and blood lipids in postmenopausal women are related to resting autonomic nervous system activity. Eur L Appl Physiol. 2006; 97: 542-547.
11. Hayashi T, Masuda I, Moritani T, et al. Autonomic nervous activity during physical exercise and postural change: investigations by power spectral analysis of heart rate variability. Jpn J Biochem Exerc. 1994; 6: 30-7.
12. Amano M, Kanda T, Moritani T, et al. Effects of exercise training on autonomic nervous system activity in obese middle aged individuals. Med Sci Sport Exerc. 2001; 33: 1287-91.
13. Moritani T, Hayashi T, Shinohara M, et al. Sympatho-vagal activities of NIDDM patients during exercise as determined by heart rate spectral analysis. In: Kawamori R, Vranic M, Horton ES, et al. Glucose fluxes, exercise and diabetes. Smith-Gordon: Great Britain. 1995: 91-6.
14. Nagai N, Moritani T. Effect of physical activity on autonomic nervous system function in lean and obese children. Int J Obes Relat Metab Disord. 2004; 28: 27-33.
15. Sands KEF, Appel ML, Lilly LS, et al. Power spectrum analysis of heart rate variability in human cardiac transplant recipients. Circulation. 1989; 79: 76-82.
16. Park SB, Lee BC, Jeong KS. Standardized tests of heart rate variability for autonomic function tests in healthy Koreans. Int J Neurosci. 2007 Dec; 117(12): 1707-17.
17. Kleiger RE, Miller JP, Bigger JT Jr, et al. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol. 1987; 59: 256-62.
18. Rompelman O, Coenen AJR, Kitny RI. Measurement of heart-rate variability: part 1 – comparative study of heart-rate variability analysis methods. Med Biol Eng Comput. 1977; 15: 233-239.
19. Pagani M, Lombardi F, Guzzetti S, et al. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ Res. 1986; 59: 178-193.
20. Hopf H-B, Skyschally A, Heusch G, et al. Low- frequency spectral power of heart rate variability is not a specific marker of cardiac sympathetic modulation. Anesthesiol. 1995; 82: 609-16.
21. Nagai N, Hamada T, Moritani T, et al. Moderate physical exercise increase cardiac autonomic nervous system activity in children with low heart rate variability. Childs Nerv Syst. 2004; Apr. 20(4): 209-14.
22. Gold E, Colvin A, Avis N, et al. Longitudinal analysis of vasomotor symptoms and race/ethnicity across the menopausal transition: Study of Women’s Health across the Nation(SWAN). Am J Public Health. 2006; 96: 1226-35.
23. Thurston RC, Christie IC, Matthews KA. Hot flashes and cardiac vagal control: a link to cardiovascular risk? Menopause. 2010; 17(3): 456-61.
24. Freedman RR. Pathophysiology and treatment of menopausal hot flashes. Semin Reprod Med. 2005; 23: 117-25.
25. Rosano GM, Patrizi R, Leonard F, et al. Effect of estrogen replacement therapy on heart rate variability and heart rate in healthy postmenopausal women. Am J Cardiol. 1997; 80(6): 815-7.
26. Stein PK, Kleiger RE, Rottman JN. Differing effects of age on heart rate variability in men and women. Am J Cardiol. 1997; 80(3): 302-5.
27. Yildirir A, Kabakci G, Yarali H, et al. Effects of hormone replacement therapy on heart rate variabil ity in postmenopausal women. Ann Noninvasive Electrocardiol. 2001; 6(4): 280-4.
28. Schwartz J , Freeman R, Fr ischman W. Cl in ica l pharmacology of estrogens: cardiovascular actions and cardioprotective benefits of replacement therapy in postmenopausal women. J Clin Pharmacol. 1995; 35(3): 314-29.
29. Niskanen L, Laitinen T, Tuppurainen M, et al. Does postmenopausal hormone replacement therapy affect cardiac autonomic regulation in osteoporotic women? Menopause. 2002; 9(1): 52-7.
30. Virtanen I, Polo-Kantola P, Erkkola R, et al. Climacteric vasomotor symptoms do not imply autonomic dysfunction. Br J Obstet Gynaecol. 1999; 106(2): 155-64.
31. Ryan SM, Goldberger AL, Pincus SM, et al. Gender- and age-related differences in heart rate dynamics: are women more complex than men? J Am Coll Cardiol. 1994; 24(7): 1700-7.
32. Princi T, Parco S, Accardo A, et al. Parametric evaluation of heart rate variability during the menstrual cycle in young women. Biomed Sci Instrum. 2005; 41: 340-5.
33. Bai X, Li J, Zhou L, et al. Influence of the menstrual cycle on nonlinear properties of heart rate variability in young women. Am J Physiol Heart Circ Physiol. 2009; 297(2): 765-74.
34. Pomeranz B, Macaulay RJB, Caudi l l MA, et a l . Assessment of autonomic function in humans by heart rate spectral analysis. Am J Physiol. 1985; 248: H151-3.
35. Berger RD, Saul JP, Cohen RJ. Transfer function analysis of autonomic regulation, I: canine atrial rate response. Am J Physiol. 1989; 2565: H142-52.
36. Kuo TB, Lin T, Tang CC, et al. Effect of aging on gender differences in neural control heart rate. Am J Physiol.

59HRV in climacteric women
1999; 277(6Pt2): H2233-9.37. Liu CC, Kuo TB, Yang CC. Effects of estrogen on gender-
related autonomic differences in humans. Am J Physiol Heart Circ Physiol. 2003; 285: H2188-93.
38. The Japan Menopause Society, ed. The Guidebook on Menopause Health Care(in Japanese). 2008.
39. Sakuma Y. Modification of autonomic function caused by sex hormones. Clinical Neuroscience(in Japanese). 2003; 21(12): 1377-80.
40. Mandigout S, Melin A, Fauchier L, et al. Physical training increase heart rate variability in healthy prepuberal children. Eur J Clin Invest. 2002; 32: 479-87.
41. Kohashi R. Impact of dieting experience on autonomic
activit ies in young women. Obesity Research(in Japanese). 2009; 15(2): 179-84.
42. Kim CK, McGorray SP, Bartholomew BA, et al. Depressive symptoms and heart rate variability in postmenopausal women. Arch Intern Med. 2005; 165: 1269-44.
43. Rebbeca C. T. et al. Hot flashes and cardiac vagal control: a link to cardiovascular risk? Menopause. 2010; 17(3): 456-61.
44. Hoikkala H, Haapalahti P, Viitasalo M, et al. Association between vasomotor hot flashes and heart rate variability in recently postmenopausal women. Menopause. 2010; 17(2): 315-20.