-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
1/28
Oropharyngeal Candidiasis inPatients with AIDS
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
2/28
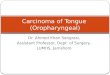
Case
29-year-old male with AIDS CD4 198 Complaining of painful cracks
at the
corners of the mouth
What is your diagnosis?
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
3/28
Oropharyngeal Candidiasis: Angular Cheilitis
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
4/28
Learning Objectives
Upon completion of this activity,participants should be able
to:
Describe symptoms of oropharyngeal
candidiasis Discuss methods for diagnosing
oropharyngeal candidiasis Review treatments for
oropharyngeal
candidiasis
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
5/28
Overview on Oropharyngeal Candidiasis
Candida albicans is the most commoncause of oropharyngeal
candidiasis
Oral candidiasis is broadly known as
thrush Candida albicans is a mouth commensal
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
6/28
Overview
Common risk factors include CD4
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
7/28
Clinical Presentation
Discovered on routine examination Often asymptomatic but
patients may
experience: Burning sensation in mouth Taste alteration Pain
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
8/28
Clinical Presentations ofOropharyngeal Candidiasis
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
9/28
Pseudomembranous Candidiasis
White/Grey Plaqueson the Hard
Palate(Pseudomembranouscandidiasis)
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
10/28
Erythematous Candidiasis
ErythematousCandidiaisis Affectingthe Hard Palate
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
11/28
Corners of theMouth AngularCheilitis
Angular Cheilitis
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
12/28
Diagnosis
Diagnosis usually clinical Easily removable white/grey plaques
with
erythematous base Scraping away these plaques reveals raw
ulcerated area Can also present atypically as
erythematous patches and angularcheilitis
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
13/28
Diagnosis
Fungal culture of mouth lesions not usefulfor diagnostic
purposes since positiveresults may be due to high rates of
mouth
colonization Fungal culture of mouth lesions used for
identification of Candida species and
resistance testing
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
14/28
Diagnosis
If laboratoryconfirmation needed,exudates of epithelialscrapings
may beexaminedmicroscopically foryeast and/orpseudohyphae by 10%KOH
(potassiumhydroxide) wet mountpreparation
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
15/28
Treatment
Use oral topical treatments as initialtherapy Systemic therapy
seldom required and
only use if absolutely necessary Relapse common, therefore
prescribe
intermittent treatment rather than
continuous
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
16/28
Treatment
Preferred First Line Therapy Topical nystatin or
clotrimazole
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
17/28
Second Line Therapy for Refractory Cases
Fluconazole 100 mg po daily for 7 14 daysafter clinical
improvement (preferred) Itraconazole 200 mg po daily for 7 14
days after clinical improvement
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
18/28
Second Line Therapy for Refractory Cases
Topical amphotericin B OR Amphotericin B 0.3 mg/kg per day IV
for
7 14 days after clinical improvement
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
19/28
Treatment
If no Response to Alternative Therapy Check adherence Reconsider
diagnosis Consider resistance to azole and/or
amphotericin
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
20/28
Drug Interactions
Azoles are prone to drug interactions throughthe cytochrome P450
(CYP450) enzymes The CYP450 pathway is involved in the
metabolism of commonly prescribed drugs Check package insert for
drug interactions
when prescribing azoles concurrently with otherdrugs
Azoles can be associated with hepatotoxicityand gastrointestinal
intolerance
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
21/28
Drug Interactions: Absorption
Itraconazole capsules require gastric acidfor absorption.
Absorption affected byBuffered didanosine, proton pump
inhibitors, H2 blockers and antacids Itraconazole liquid is
better absorbed and
should be taken on an empty stomach
Fluconazole absorption is not affected byfood or gastric pH
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
22/28
Treatment Side Effects
Clotrimazole Generally well tolerated Occasionally can cause
gastrointestinal
toxicity Nystatin
Bitter taste
Can be associated with gastrointestinaltoxicity
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
23/28
Maintenance Therapy
Generally not recommended Occasionally needed if recurrence
frequent Topical therapy preferred
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
24/28
Maintenance Therapy
If refractory to topical therapy considerazoles Fluconazole or
itraconazole 100 mg po daily
Chronic use of azoles can lead toresistance Optimal prevention
is immune
reconstitution with ART
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
25/28
Additional Considerations
Reinforce importance of maintainingadequate nutrition Educate
the patient on good mouth
hygiene Counsel the patient on which foods may
be difficult to chew as they can
exacerbate mouth discomfort
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
26/28
Summary
Common in patients with AIDS Diagnosis usually clinical Treat
with topical agents Preserve systemic treatment and only use
if absolutely necessary Relapse common
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
27/28
Summary
Maintenance generally notrecommended Reinforce the importance of
good oral
hygiene Optimal prevention is immune
reconstitution with ART
-
8/2/2019 Oropharyngeal Candidiasis in Patients With AIDS
28/28
References
Bartlett, J and Gallant, J. 2007. Medical Management of HIV
Infection. Johns Hopkins University. Baltimore, MD.
Boon, NA et al. 2006. Davidsons Principles and Practice of
Medicine. Elsevier Science Health Science div. 20th Edition. pg
373-375.
The Hopkins HIV Guide: http://www.hopkins-hivguide.org
Ramrez-Amador, V. et al. 2003. The Changing Clinical Spectrum of
Human Immunodeficiency Virus (HIV)-Related Oral Lesions in 1,000
Consecutive Patients: A 12-Year Study in a Referral Center in
Mexico. Medicine . 82: 39-50.
Vazquez, JA. 2000. Therapeutic options for the management of
oropharyngeal and esophageal candidiasis in HIV/AIDS patients. HIV
Clin Trials . Jul-Aug; (1): 47-59.