-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
1/17
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
2/17
18
Journal o Orthomolecular Medicine Vol. 21, No. 1, 2006
o oroacial dyskinesia in patients previ-ously treated with
haloperidol.2 However,when risperidone is used at higher doses,
it has resulted in levels o EPS similar tothe typical APDs.4
HyperprolactinemiaAntipsychotic drugs, through their
mechanism o dopamine antagonism,cause elevated serum prolactin
levels.Elevated prolactin levels have direct andindirect roles in
the development o breastcancer, osteoporosis, cardiovascular
disease, and sexual dysunction.5 Morespecically, sustained
hyperprolactinemiainduces hypogonadism, causing estrogendeiciency
in women and testosteronedeciency in men. In women, the mostcommon
consequences o elevated pro-lactin levels include amenorrhea,
dyspa-reunia (dicult or painul intercourse),galactorrhea,
gynecomastia, and impaired
mental unctioning. In men, the problemswith elevated prolactin
levels tend toprimarily aect sexual unction and er-tility.6 With
the exception o risperidone,hyperprolactinemia is more o a
concernwith the typical APDs than with the neweratypical ones.
In women on typical APDs, the ensu-ing side eects o menstrual
irregularitiesrange rom 15-91% and galactorrhea rom
10-50%. Hyperprolactinemia-induced hy-pogonadism leads to low
estrogen levelsand possibly a worsening o the psycho-pathology in
emale patients becauseestrogen is believed to have
antipsychoticproperties. The estrogen deciency alsoleads to
symptoms such as vaginal dry-ness during intercourse and loss o
li-bido. Long-term, it can cause decreased
bone mineral density and osteoporosis.Compared to healthy men,
male schizo-phrenics on conventional APDs reportgalactorrhea.6
Haloperidol can raise serum prolactinlevels as early as 72 hours
ater initiatingtreatment, the rise continuing or 6-9 days
then reaching a plateau. Haloperidol at15 mg/day is associated
with sustainedhyperprolactinemia.6 The atypical APDs
are weaker dopamine-type 2 receptor(D2) antagonists than the
typical classo drugs, and thus do not aect prolactinlevels to the
same degree. In three trials oquetiapine at certain doses, the drug
didnot cause a sustained elevation o serumprolactin levels.7
Risperidone is an excep-tion amongst the atypical APDs,
causingdose-related increases in prolactin levelssimilar to typical
drugs such as haloperi-
dol. The increases are seen in both menand women, with the mean
increases be-ing greater in women than in men. Theearly studies on
risperidone used the drugin high doses, but current clinical
practiceuses lower doses (4 mg/day). It is not clearwhether the
lower doses o atypical APDshave less o an eect on prolactin
levels.6
The conficting results in the literature
may be the result o the ollowing: (1)whether or not tolerance
develops to theprolactin-elevating eects o the atypicaldrugs; and
(2) whether theres a correla-tion between prolactin concentration
andpsychopathology.6 Overall, the side eectscaused by
hyperprolactinemia, such asgalactorrhea and sexual dysunction,
leadto noncompliance among schizophrenicpatients.6
Sexual DysfunctionMost patients on APDs experience
some sort o sexual dysunction, whichmay include loss o interest
(libido), de-creased arousal (poor vaginal lubricationor erectile
dysunction), and anorgasmia(inability to have an orgasm).
Surveyssuggest that as much as 40% o women
and 60% o men on typical APDs reportthese symptoms.8 Because o
its depress-ing eects on quality o lie, patients ratesexual
dysunction as the most distressingside eects o drug therapy.
There are several ways by which thesedrugs aect sexual unction.
One mecha-
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
3/17
19
Orthomolecular and Botanical Treatments or Side Eects o
Antipsychotic Drugs
nism involves inhibition o dopaminerelease due to dopamine
blockage at D2receptors that may impair libido and erec-
tion. Another mechanism has to do withblockage o the
alpha-adrenergic path-way in the periphery, which may lead
topriapism (a painul and sustained penileerection which is a
urologic emergency),galactorrhea, amenorrhea, gynecomastiaand
vaginal dryness (due to estrogen de-ciency). Alterations in
serotonin, whichparticipates in initiating arousal throughits
vasodilatory eects in the periphery,
can negatively aect sexual unction.Finally, non-specic central
nervous sys-tem (CNS) eects, such as sedation, cancause a decrease
in the desire or sexualactivity.
As a whole, the primary mechanismo sexual dysunction induced by
thesedrugs is probably the direct dopamineantagonism with some
additional indirect
eects due to hyperprolactinemia.8
Sexualdysunction is an important problem withthe typical APDs,
and to a lesser extentwith the newer atypical drugs. Nonethe-less,
it remains an under-appreciatedproblem.
Weight Gain and Diabetes Mellitus (DM)A common side eect o APDs,
es-
pecially the atypical APDs, is excessive
weight gain. In act, it is now believed tobe the most prominent
long-term sideeect associated with these newer drugsand should be
highly considered whentreatment plans are designed, becauseo the
obvious medical consequences oobesity.1
The weight gain may be related toincreased appetite (due to drug
interac-
tion with the brain monoaminergic andcholinergic systems), and
to the endocrineeects o hyperprolactinemia.9 Clozapineand
olanzapine both induce glucose dys-regulation and dyslipidemia, the
develop-ment o which may be associated withthe combination o sudden
body weight
gain (BWG), insulin resistance, increasedappetite and related
endocrine changes.9
It is hypothesized that clozapine causes
weight gain by increasing adipose tis-sue, which leads to
insulin insensitivity,glucose intolerance, and when severe,diabetes
mellitus (DM).4 In one report,58% o patients on clozapine gained
atleast 10% over baseline.4 Several cases oclozapine-induced
diabetic ketoacidosishave also been reported.10
One cohort study ound that patientsbeing treated with typical or
atypical APDs
are at greater risk o developing DM thanthe general
population.11 The patients inthe risperidone and haloperidol
cohortsshowed the greatest risk.11 Patients onolanzapine averaged
weight gains o5.4 kg over the rst six to eight monthso treatment
and had a 20% increasedrisk o developing DM than patients
onrisperidone who averaged weight gains
o 3.9 kg.4
Quetiapine has been shownto cause lower levels o weight gain
thanother atypical APDs. However, the typicalAPD, haloperidol,
causes less BWG thanthe other drugs.4 It also appears
thatadolescents experience more BWG com-pared to other populations
when takingatypical APDs.
Cardiovascular Side Effects
Clozapine poses a risk o myocar-ditis, especially during the rst
montho therapy. A 2002 advisory by HealthCanada reported an
association betweenclozapine use and pericarditis, myo-cardial
inarction, pericardial eusion,cardiomyopathy, heart ailure, and
mitralinsuciency.4 In addition, antipsychoticdrugs, including some
atypical APDs, may
cause electrocardiogram (ECG) changesthat can lead to
drug-induced arrhythmiaand, rarely, sudden unexplained death.7
In one study, risperidone showed a sig-nicant increase in QT
interval durationcompared to placebo,12 yet in anotherstudy (albeit
conducted by the company
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
4/17
20
Journal o Orthomolecular Medicine Vol. 21, No. 1, 2006
who manuactures the drugs), none o theatypical drugs were ound
to cause QTelevations that were considered clinically
signicant.7
Implications of Use During Pregnancyand Lactation
A study involving lactating womentaking clozapine ound the level
in theiroremilk to be 2.8 to 4.3 times the level oclozapine in the
maternal plasma, but nostudies have been done to accurately as-sess
the direct implication o these levels
on the breasteeding neonate.13Clozapine and olanzapine
increase
the risk o signicant weight gain, andDM puts the inant at
greater risk orperinatal mortality, prematurity, con-genital
abnormalities (e.g., neural tubedeects), macrosomia and, as
previouslystated, increases the chances o develop-ing DM in the
uture. Physicians should
also be aware that stopping antipsychoticmedication when
pregnant or post-par-tum, especially abruptly, could have
thepotential consequence o causing a psy-chotic relapse in the
patient, which maybe severe and include maternal suicideand
inanticide.
Avoidance o phenothiazines are rec-ommended because o their
associationwith signicant increases in congenital
abnormalities. As well, clozapine, orcombinations o typical
APDs, with dos-ages within their upper ranges should beavoided
during pregnancy and lactation,until urther evidence determines
themto be sae.13
Blood DyscrasiasClozapine has a well known, albeit,
minimal risk, o lie-threatening blooddyscrasias
(agranulocytosis). This is oneo the major reasons why the drug is
usedprimarily or patients reractory to otherAPDs and is not
rst-line therapy. Pa-tients on clozapine require regular
bloodmonitoring and surveillance every 1 to 2
weeks, which makes this drug problematicas it disrupts a
patients quality o lie.4
Additional Side EffectsPatients on quetiapine are recom-mended
to have regular ollow-up eyeexaminations every six months, due
tospeculation that the drug may be linkedto lens abnormalities such
as cataracts.4, 7
Thyroid unction may also be eected byquetiapine, since higher
end doses wereshown to cause a 20% decrease in totaland ree
thyroxine.7 This may be one o the
reasons why olanzapine and quetiapineare associated with a airly
high incidenceo drowsiness. Unlike some o the otheratypical APDs,
insomnia is a commonadverse eect caused by risperidonetherapy.4
Additionally, risperidone shouldbe used with caution in patients
also tak-ing indinavir and ritonavir because such acombination can
induce reversible coma.14
Another atypical APD, clozapine, caninduce dose-dependent
seizures.15
One o the newer atypical drugs onthe market is aripiprazole,
which is sup-posed to have ewer side eects comparedto the other
atypical APDs. It still hasbeen shown to cause headaches,
nausea,vomiting, constipation, dyspepsia, ortho-static hypotension,
tachycardia, insomnia,somnolence, and tremors.12Table 1 (p.21)
summarizes the main side eects causedby selected atypical and
typical APDs.
Worsening the Long-term OutcomeContinuous use o APDs has
actually
been shown to worsen the long-term out-come in schizophrenic
patients. Althoughthese drugs are eective in treating
acutepsychotic symptoms, they do not improve
patients lives in the long run.
16
The rstpivotal study to show this was the 1960National Institute
o Mental Health studythat ound the drugs to have short-termbeneit
but higher relapse rates i usedlong-term.16 The World Health
Organiza-tion later conducted a study on conven-
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
5/17
21
Orthomolecular and Botanical Treatments or Side Eects o
Antipsychotic Drugs
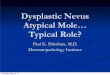
Table 1. Summary o the main side eects caused by selected
atypical andtypical APDs
Anti-psychotic EPS&TD Hyperpro- WeightGain Sexual Other
Agent lactinemia Risperidone Yes Yes Lesser extent(atypical
agent)
Clozapine Lesser extent Lesser extent(atypical agent)
Olanzapine Lesser extent Lesser extent(atypical agent)
Quetiapine Lesser extent Lesser extent Lesser extent(atypical
agent)
Aripiprazole Lesser extent Lesser extent Lesser extent Lesser
extent(atypical agent)
Haloperidol Yes Yes Lesser extent Yes(typical agent)
Minimal risk of life-threatening blood dys-crasias
(agranulocytosis),cardiovascular toxicity,drowsiness, and
dosedependent seizures
Dose-dependentincreases in EPS.At high doses,incidence of EPS
issimilar to that seenwith Haloperidol
Insomnia, increased QTinterval, and interac-tion with indinavir
andritonavir
Orthostatic hypotensionand lens abnormalities
GI symptoms, insomnia,tremors, and tachycardia
Higher risk for adult-onset DM, especially with
increasing age
Yes, and increasedrisk of developingadult-onset DM
Dose-dependentincreases in EPS
Orthostatic hypotensionand drowsiness
Low incidence ofEPS across all doses
Dose-dependantincreases in EPS
Yes, and increasedrisk of developing
adult-onset DM
tional neuroleptics, which showed that inthe developing world,
where patients arekept on the drugs or a short period otime,
patients had exceptionally good socialoutcome compared to the poor
long-termoutcome o patients in the developed worldwho are kept on
the drugs chronically.16
In the late 1970s, Canadian investiga-tors at McGill University
reported thatthe brains o patients treated with APDsdeveloped an
increased density o D2 re-ceptors by 30% or more in an attempt
tocompensate or the dopamine antagonistic
eects o the drugs. Patients can becomesuper-sensitized to
dopamine (thoughtto be the mediator o psychosis), so thatwhen they
abruptly stop the drugs, theyhave a higher tendency towards
psycho-sis.16 This mechanism makes medicatedpatients more
biologically vulnerable to
psychosis. The need or continued anti-psychotic treatment may
itsel be druginduced.16
Atypical APDs have established det-rimental eects on metabolic
unction,similar to the older, typical APDs. They
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
6/17
22
Journal o Orthomolecular Medicine Vol. 21, No. 1, 2006
also increase the density o D2 recep-tors, making patients more
vulnerable topsychosis, and probably reduce liespan
when used long term. Ironically, modernpsychiatry seems to be
prescribing themto an increasing number o patients,including those
at risk o developingschizophrenia. The real goal should be
tominimize their use and to wean patientso o them very slowly.
Managing the Side Effects of Drowsiness,Exhaustion, Fatigue, and
Somnolence
All the atypical APDs cause somecombination o drowsiness,
exhaustion,atigue, and somnolence. One o the bestorthomolecular
methods to combat theseside eects is injectable vitamin B12
(hy-droxocobalamin). Newbold has writtenabout the therapeutic uses
o injectablevitamin B12 as an antidote or over-se-dation.17 In
Newbolds report, he recalled
a case involving one o his clients, anactress, who was dealing
bootleg Quaalu-des as a source o income. She apparentlytreated her
clients with 6000 mcg (micro-grams) o injectable
hydroxocobalaminwhen they would become over-sedatedrom these pills
and would be unable toleave her premises. From giving them
highdoses o injectable hydroxocobalamin,she was able to reverse
their sedation
enabling them to leave her apartment. Inthe same report, Newbold
also discussedanother case involving a comatose patientwith marked
symptoms o over-sedationinduced by bootleg Quaaludes and ex-cessive
amounts o vodka. This patientalso responded to injectable
hydroxo-cobalamin, but required 9000 mcg o itin order to regain
consciousness and be
alert. From these experiences, Newboldsuggested that all
patients with symp-toms o over-sedation rom overdoses osedatives,
tranquilizers, and/or alcohol begiven a therapeutic trial o 9000
mcg ohydroxocobalamin.
I (Prousky) have treated several pa-
tients on atypical APDs with injectablehydroxocobalamin due to
symptoms oover-sedation. I am impressed with the
vitamins ability to perk these patientsup and help them make it
through the day.It is not a cure-all, but it does improvequality o
lie. The recommended dose tostart with is 5000 mcg once or twice
eachweek. Generally patients respond avor-ably within 24 to 48
hours ater their rstinjection. Instead o eeling excessivelysleepy,
many o these patients reportmore energy and an increased
alertness.
Patients who do not respond to the inject-able vitamin B12
should be provided withsupplemental calcium and magnesiumsince
these minerals help vitamin B12 gainentrance into the cells.17
Managing the Side Effects of EPSOther symptoms that are
believed
to occur less requently with the atypical
APDs are the EPS. However, I (Prousky)have seen several patients
with some de-gree o EPS while on the atypical APDs,and most o these
patients have beenprescribed benztropine mesylate to dealwith them.
Unortunately, the addition obenztropine mesylate merely adds
moremental symptoms to patients alreadystruggling with their
psychiatric condi-tion (e.g., conusion, disorientation, and
memory impairment). The botanical med-icine, ginkgo biloba
extract (GBE) mightbe helpul. In a study involving treat-ment
resistant schizophrenic patients,the addition o 360 mg per day o
GBEwith haloperidol was shown to decreaseEPS and enhance
eectiveness o thedrug.18 Even though this study assessedthe
combination o GBE with a typical
APD, similar positive results might alsooccur when combining GBE
with atypicalAPDs. This drug-botanical combinationmight reduce EPS
and enhance atypicalAPD eectiveness, possibly preventingurther
increases in medication dosage.The ability o GBE to enhance
medication
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
7/17
23
Orthomolecular and Botanical Treatments or Side Eects o
Antipsychotic Drugs
eectiveness might also allow patients toreduce their dosages and
experience ewerside eects rom their medications.19
In addition to GBE, there are a numbero nutritional treatments
that would helpreduce and/or prevent EPS that includeascorbic acid,
manganese, phosphatidyl-choline, pyridoxine hydrochloride,
andvitamin E (d-alpha tocopheryl acetate).Werbach has summarized
various studiesdemonstrating the eectiveness o thesenutrients to
reduce and/or eliminate TDamong patients taking typical APDs.20
Although none o these nutritional agentshave been subjected to
clinical trials involv-ing patients on atypical APDs, they
prob-ably have a similar spectrum o ecacywhen used in combination
with this classo antipsychotic medications. Table 2 (be-low) lists
these orthomolecular agents andtheir corresponding dose ranges.
Managing Sexual DysfunctionIn male schizophrenic patients,
anumber o viable orthomolecular and/orbotanical options exist that
should helpreverse some o the sexual dysunction as-sociated with
the use o atypical APDs.
L-arginine. One o the rst agents tobe considered is L-arginine.
This aminoacid is a biologic precursor to nitric oxide,which plays
an important role in endothe-
lium-dependent processes.21 In act, prob-
lems with penile endothelial L-arginineare thought to be
responsible or part othe pathogenesis o erectile dysunction
(ED).22
In a small clinical trial involvingmen with ED, 40% o the
treatment groupon 2.8 g o L-arginine daily or two weeksdemonstrated
improvements comparedto no improvements among men in theplacebo
group.23 In a larger trial, 50 menwith ED were given 5 g o
L-arginine perday or a matching placebo or six weeks.There was a
subjective improvementamong 31% o the men in the L-arginine
group.24 Another study combined 1.7 g oL-arginine with
increasing doses o pyc-nogenol in a three-month trial involving40
men with ED.25 All the men took 1.7 go L-arginine during the rst
month, andthen during the second month were given40 mg o pycnogenol
twice daily withthe same dose o L-arginine. During thethird month,
the dose o the pycnogenol
was increased to 40 mg three times dailywith the same dose o
L-arginine. At theend o the second month, 80% reporteda normal
erection, and by the end o thethird month this therapeutic
responseincreased to 92.5%. Other benets thatwere noted included a
quicker erection inresponse to stimulation, and an
increasedduration o erection.
Ginseng. Another agent that might
beneit male schizophrenic patients is
Table 2. Orthomolecular and botanical agents to reduce and/or
eliminate EPSand TD associated with atypical APDs.
Supplement RecommendedDailyDosageAscorbic Acid 1300-4000
mgGinkgo biloba extract 360 mg
Manganese 15-60 mgPhosphatidylcholine Dose equivalent to
2400-6400 mg of cholinePyridoxine hydrochloride 250-800 mgVitamin E
250-800 mg of d-alpha tocopheryl acetate
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
8/17
24
Journal o Orthomolecular Medicine Vol. 21, No. 1, 2006
panax ginseng. The active compounds inpanax ginseng, the
ginsenosides, inducerelaxation o the smooth muscle o the
corpus cavernosum in rabbits by augment-ing the release o nitric
oxide.26-27 Clinicaltrials involving human subjects have
dem-onstrated that panax ginseng can improveerectile unction and
sexual satisaction.In one trial, 90 patients were divided intothree
groups: the panax ginseng group, theplacebo, and the trazodone
group.28 Eventhough parameters such as intercourserequency,
premature ejaculation, and
morning erection ater treatment were thesame in all three
groups, the panax ginsenggroup did have a signicant improvementin
penile rigidity, girth, duration o erec-tion, libido, and patient
satisaction. Theoverall ecacy o panax ginseng on EDwas 60% compared
to only 30% among theplacebo and trazodone groups.
A more recent randomized, double-
blind, placebo-controlled, crossover studyassessed the ecacy o
panax ginsengamong 45 men with ED.29 One group omen were given 900
mg o panax ginsengthree times daily or eight weeks. Theother group
was given an identical lookingplacebo three times daily or eight
weeks.Ater the eight weeks, each group was sub-jected to a two week
washout period andthen received crossover treatment with
placebo or panax ginseng or an additionaleight weeks. The men on
panax ginsengscored signicantly higher on the Inter-national Index
o Erectile Function (IIEF)compared to men on placebo. The
panaxginseng group also had better penile tiprigidity as measured
by a device called theRigiScan, compared to the placebo group.The
authors o this study were unable to
explain the benets o panax ginseng interms o its hemodynamic and
hormonalactions. Instead, it was purported thatpanax ginseng
beneted ED due to itseects upon multiple mechanisms.
Gingko Biloba. Another botanicalmedicine, GBE, ought to be tried
when
helping both male and emale schizo-phrenic patients suering rom
sexualdysunction. Although the reports on
GBE assessed its value in treating sexualdysunction induced by
antidepressantmedications, it might oer some benetto schizophrenic
patients on atypicalAPDs. The rst report o GBEs abilityto improve
ED involved male geriatricpatients taking antidepressant
medica-tions.30 While these patients were takingGBE to improve
their memory, many othem noticed an improvement with their
erections. The dosages used in this trialwere 40-60 mg capsules
taken twice daily,and was increased to 120 mg twice daily.The
average dose during the trial was207 mg/day. Around 76% o the
patientsound GBE to be eective at restoring allaspects o their
sexual response, includ-ing erectile unction. The
mechanismresponsible or GBEs positive eects upon
sexual unction had to do with its abilityto augment nitric oxide
synthase (e.g.,increase nitric oxide availability). Thesepositive
eects occurred in the presenceo serotonin, which can impede
nitricoxide production.31
Another trial evaluated the eective-ness o GBE or
antidepressant-inducedsexual dysunction.32 Twenty-our pa-tients
participated in the trial, with an
equal number o men and women. Therewas a signicant improvement
in sexualresponse ater three and six weeks ouse. However, the data
was inconclusivesince the therapeutic response to GBEwas so
variable among the patients. Ina smaller trial involving both male
andemale patients, GBE was not successulat helping any o the nine
male patients,
and was only helpul among three o the13 emale patients tested.33
In a placebo-controlled, double-blind trial or
antide-pressant-induced sexual dysunction,37patients were
randomized to receive GBEor a placebo.34 The participants on
GBEreceived 120 mg or the rst two weeks,
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
9/17
25
Orthomolecular and Botanical Treatments or Side Eects o
Antipsychotic Drugs
160 mg or the next two weeks, and 240mg or the remaining our
weeks o the trial.All participants were given a questionnaire
beore taking either GBE or placebo, andater the second, orth,
and eighth weeks.Unortunately, no statistical signicance
wasachieved or patients on GBE compared tothose on placebo.
Nonetheless, GBE mightbe helpul. It should be prescribed to maleand
emale schizophrenic patients sueringrom sexual dysunction induced
by theatypical APDs. Table 3, (below) lists theorthomolecular and
botanical agents that
might reduce the sexual dysunction associ-ated with atypical
APDs.
Managing HyperprolactinemiaThe most well known botanical
agent
that lowers prolactin levels is vitex agnuscastus. In a review o
its prolactin-reducingeects, Brown reported: (1) that vitex invitro
inhibited the basal and the thyrotro-
pin-releasing hormone (TRH) stimulationo prolactin levels; and
(2) that it containsconstituents that directly bind to the
dopa-mine receptors o the anterior pituitary.35For these reasons,
it is inadvisable or anyschizophrenic patient currently taking anyo
the atypical APDs to concomitantly usevitex as a means to lower
prolactin levels.Atypical APDs are dopamine-receptor block-ing
agents, and taking vitex would reduce
their eectiveness.The orthomolecular agent, gamma-
aminobutyric acid (GABA), should also be
avoided. GABA is an inhibitory neurotrans-mitter with anxiolytic
properties similar toclonazepam and other benzodiazepines.36
Like vitex, GABA has the ability to aug-ment dopamine release
and reduce pro-lactin secretion. GABAs exact biochemicalmechanisms
are not well understood, butstudies using animal models have
beenhelpul in elucidating some o them. Inone in vitro study, the
GABA (B) receptoragonist, bacloen, was shown to inhibit thebasal
and thyrotropic releasing hormone-stimulated prolactin secretion in
anterior
pituitary cells.37 In another rat experiment,it was concluded
that endogenous GABA,by acting through GABA (A) receptors,infuences
the basal and diurnal changeso tuberoinundibular dopaminergic
neu-ronal activity, and consequently prolactinsecretion.38 Since
there are GABA receptors(A and B types) located in the
anteriorpituitary, orally administered GABA might
stimulate these pituitary receptors caus-ing a release o
dopamine and a drop inprolactin secretion. Although it is uncleari
orally administered GABA can eectivelygain entrance into the CNS,
the use o thisagent should be avoided due to its potentialeects
upon dopamine, and its potentialantagonistic eects upon atypical
APDs.At present, the authors o this report areunaware o any
orthomolecular and/or
botanical agents that can lower prolactinlevels without possibly
compromising theeectiveness o the atypical APDs.
Table 3. Orthomolecular and botanical agents to reduce and/or
eliminatesexual dysunction associated with atypical APDs
Supplement RecommendedDailyDosageL-Arginine (male patients only)
1.7-2.8 gPycnogenol (male patients only) 120 mgPanax Ginseng (male
patients only) 2700 mgGinkgo Biloba Extract (male & female
patients) 240 mg
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
10/17
26
Journal o Orthomolecular Medicine Vol. 21, No. 1, 2006
Managing Weight GainBesides the well known liestyle
measures that are time-tested in terms
o losing weight (e.g., diet and exercise),supplementation with
green tea extractshould help to control some o the weightgain
produced by the atypical APDs. Inone human trial involving ten
healthymen, the administration o green teaextract containing 50 mg
o caeine and90 mg o epigallocatechin gallate (EGCG)given three
times daily with meals pro-duced statistically signicant
results.39
Specically, green tea extract increasedthe 24-hour energy
expenditure, reducedthe 24-hour respiratory quotient, andincreased
the 24-hour urinary excretiono norepinephrine (NE). The
investigatorsconcluded that green tea extract, apartrom caeines
thermogenic properties,controlled body composition through
itssympathetic activation o thermogenesis,
at oxidation, or rom a combination othese two actors.In another
study, the catechin-poly-
phenols and caeine ound in green teaextract stimulate
thermogenesis by sym-pathetically releasing norepinephrine.40The
catechin-polyphenols rom green teaextract increases norepinephrine
via theirinhibition o catechol-O-methyl-transer-ase (the enzyme
that degrades NE), and
the caeine content inhibits transcel-lular phosphodiesterases
(enzymes thatbreakdown NE-induced cyclic adenosinemonophosphate).
The possible net eectsare sympathetic stimulation o thermo-genesis
and improved weight control. Thebenecial eects o green tea extract
havebeen more ormally studied in an opentrial o moderately obese
patients.41 An
80% ethanolic dry extract o green teastandardized to 25%
catechins (expressedas EGCG), was ound to decrease bothbody weight
and waist circumerenceater three months o use. The authorso this
study suggested that green teaextract might avorably infuence
body
composition by inhibition o gastric andpancreatic lipases and
rom the stimula-tion o thermogenesis.
These studies demonstrate that greentea extract can have a
avorable eectupon body composition. However, theuse o green tea
extract also increasesthe production o NE and should be usedwith
caution in all schizophrenic patients.The oxidized derivative o
norepinephrine,noradrenochrome, likely contributesto the psychosis
o schizophrenia. Anyincrease in norepinephrine, thereore,
could be detrimental. To oset this prob-lem, make sure that
green tea extract isgiven with a complement o
antioxidants.Caeine-ree green tea extracts wouldproduce less NE
since it would not havethe same type o sympathetic stimulationwhen
compared to extracts containingcaeine. The optimal dose o green
teaextract appears to be 270 mg daily that is
standardized to 25% catechins (expressedas EGCG).
Managing DiabetesPatients on atypical APDs can devel-
op drug-induced glucose intolerance andhave a syndrome that
mimics adult-onsetdiabetes. In terms o diabetes control
andprevention, the most important orthomo-lecular agent appears to
be chromium. For
many years, chromium was thought to beinvolved in the
glucose-tolerance actor(GTF) molecule that presumably
increasesinsulin sensitivity. The composition oGTF, as isolated rom
yeast, is made ochromic ion, nicotinic acid, and the aminoacids
glycine, glutamic acid, and cyste-ine.42 However, GTF o any type
has neverbeen ound in human tissues. More re-
cently, a naturally occurring oligopeptidelow-molecular weight
chromium-bindingsubstance (LMWCr) has been proposedto be the
biologically active orm o chro-mium.43 This compound has been
oundin many dierent types o mammals, andis widely distributed in
numerous tis-
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
11/17
27
Orthomolecular and Botanical Treatments or Side Eects o
Antipsychotic Drugs
sues (e.g., liver, kidney, spleen, intestine,testicles, and
brain). This oligopeptide isalso comprised o the amino acids
glycine,
cysteine, glutamic acid, aspartic acid, andhas a multinuclear
chromic assembly inwhich the chromic centers are bridgedby the
anionic ligands, oxide and/or hy-droxide.43 This LMWCr compound is
parto an insulin amplication system thatregulates glucose
homeostasis through acomplex series o biochemical
reactionsoccurring at the insulin receptor.44,45 In astudy
involving 185 adult-onset diabetic
patients, there were signicant decreasesin the concentration o
asting and two-hour glucose levels, insulin, hemoglobinA1C, and
total cholesterol among patientssupplemented with 1000 mcg o
chromi-um picolinate compared to those on 200mcg o chromium
picolinate or placebo.46Thus, chromium as part o the LMWCr,should
have the ability to improve glucose
tolerance and increase insulin sensitiv-ity in schizophrenic
patients with poorglucose control.
In terms o toxicity, Lamson and Pla-za have summarized the
chromium litera-ture, and have evaluated its mechanismso action and
exceptional saety prole.According to these investigators, thereis
no demonstration o general chromiumtoxicity in animals at a dose
that would
extrapolate to humans as 1050 mg daily.47One o these
investigators has even used3000-4000 mcg o chromium as
nicotinategiven twice daily to adult-onset diabeticpatients or
months to years resulting intremendous reductions o glucose
andlipid levels without any increases in bloodurea nitrogen, liver
enzymes, or otherlaboratory abnormalities. It is interesting
to note that high supplemental doses ochromium would never come
even closeto 1050 mg per day.
While on atypical APDs, many schizo-phrenic patients develop
insulin resis-tance, increased appetite, and relatedendocrine
changes. I (Prousky) speculate
that the glucose intolerance resultingrom atypical APDs disrupts
chromiumhomeostasis and creates an increased
metabolic need that can be met onlythrough high-dose
supplementation. Ican recall one patient who had positivebody
composition changes, such as weightloss, ollowing a ew months o
taking3000 mcg o chromium rom yeast eachday. Although asting
glucose measure-ments were not done prior to and aterthe chromium
intervention, the bodycomposition changes in this one patient
were probably a refection o improvedglucose homeostasis. The
dose ranges thatare likely o value among schizophrenicpatients on
atypical APDs are 1000-4000mcg o chromium given twice daily.
Managing Cardiovascular Side EffectsThe most worrisome
cardiovascular
side eects are the cardiac arrhythmias
that in rare cases can lead to unexplaineddeath. The best way to
manage and/orprevent cardiac arrhythmias is throughdaily
supplementation with sh oil. Ina randomized, double-blind,
placebo-controlled trial, 65 patients with cardiacarrhythmias
(without coronary heart dis-ease or heart ailure) were ollowed
orsix months, and were divided into twogroups.48 One group was
given 3 g daily
o encapsulated sh oil (equivalent to 1g daily o omega-3 PUFA),
whereas theother group was given 3 g daily o oliveoil as placebo.
In the sh oil group therewere considerable lipid-modiying ben-ets
that included a decrease o serumtriglycerides, total cholesterol,
low-den-sity lipoprotein cholesterol, plasma reeatty acids, and
thromboxane B2, and
an increase in high-density lipoproteincholesterol. The subjects
in the sh oilgroup also had 46.9%, 67.8%, 71.8%, and100% ewer
incidences o the our typeso arrhythmia monitored in this
study(atrial premature complexes, ventricularpremature complexes,
couplets, and trip-
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
12/17
28
Journal o Orthomolecular Medicine Vol. 21, No. 1, 2006
lets). Unlike the sh oil group, no positivechanges occurred in
the placebo group.The results o this study demonstrated
that sh oil supplementation has anti-arrhythmic eects, and can
reduce theincidence o atal myocardial inarctionand sudden cardiac
death. For the reasonscited in this study, and rom the conclu-sions
o other investigators,49,50 its seemsprudent that all schizophrenic
patientstaking atypical APDs are supplementedwith sh oils due to
their anti-arrhyth-mic and lipid-modiying eects. In terms
o the optimum dosage, schizophrenicpatients should consume a
daily amounto sh oil that is recommended or pa-tients with and
without coronary heartdisease (CHD). For cardioprotection, thedaily
dose should contain 450-1000 mg oeicosapentaenoic acid (EPA) and
docosa-hexaenoic acid (DHA).51
Case ReportThe ollowing case report is an excel-lent example o
the eectiveness o theorthomolecular and botanical approach.The
patient was eventually able to discon-tinue most o his mainstream
treatments(except or risperidone), and signicantlyrecover rom his
diagnosis o schizoaec-tive disorder.
The patient, a 24-year-old Hispanic
male, rst presented to Dr. Prouskys pri-vate naturopathic
practice on November13, 2004, or chie complaints o schizoa-
ective disorder and obesity. He describeda history o being
unwell emotionally romthe age o 15 onwards. His symptoms
became more severe at the age o 16when he started hearing
messages rombillboards, would spend countless hourssurng the
Internet, was emotionally veryfat, had a belie that 100% o the
biblewas true, and that the devil was orcinghim to do things. He
would read exces-sively and did report some occasionalthoughts o
violence. Due to his moods, heparticipated in a hospital-based
program
or depression that helped very much. Hispast medical history did
include a suicideattempt at the age o 21, or which he
washospitalized and released shortly therea-ter. Review o systems
illuminated otherproblems that consisted o glaucoma,
mildmusculoskeletal complaints, obesity, andshortness o breath. His
weight was about200 pounds in the year 2000. Since being
prescribed risperidone in 2001, his weightincreased to 260
pounds. His current pre-scription medications were risperidone (3mg
daily), olanzapine (20 mg daily), andbupropion hydrochloride (150
mg daily).The patients amily history revealed somegenetic
predisposition to schizophrenia,as his paternal grandmother was
diag-nosed with this disorder at 60 years old.On physical
examination, the patient
was well nourished, clinically obese, hadhigh to normal blood
pressure, and mildtachycardia. All o his main systems were
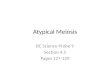
Table 4. Patients First Set o HOD Results.
HODTestItems December2004ResultsTotal Score (TS) 40Perceptual
Score (PerS) 4Paranoid Score (PS) 2Depression Score (DS) 10Ratio
Score (RS) 4Short Form (SF) 1
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
13/17
29
Orthomolecular and Botanical Treatments or Side Eects o
Antipsychotic Drugs
within normal limits. He was prescribedvitamin B6 (250 mg
daily), niacinamide(1000 mg three times daily), vitamin C
(1000 mg three times daily), chromium(1000 mcg three times
daily), liquid shoil (1 teaspoon twice daily) providing closeto 2 g
o EPA, zinc (50 mg daily), and wastold to discontinue all dairy and
milkproducts. Regular use o dairy and milkproducts can be
associated with psychosisand depression.52
On December 13, 2004, the patientreturned or a ollow-up. He
reported an
increased sense o alertness and vigorrom the treatments. He also
describedsymptoms o social anxiety where hewould eel scared to talk
to people, andwould even avoid teachers and classmateswhile
completing his auto mechanic pro-gram. He did have some depression
sincethe last visit, and experienced suicidalideation on three
separate occasions since
the initial visit. His vitals were withinnormal limits. The
patient was giventhe Beck Anxiety Inventory (BAI) andthe Beck
Depression Inventory (BDI) toll-out. His BAI score was 33,
indicatingmoderate anxiety. His BDI score was 26,indicating
moderate depression. Labora-tory tests showed a normal CBC,
normalasting plasma glucose, and an abnormallipid prole showing the
patient to be at
an above average risk or coronary heartdisease. The patient was
switched romthe niacinamide to niacin at a dose o1500 mg three
times daily to help controlhis psychiatric symptoms and to
avorablyimpact his lipid prole. He was also givenL-glycine or his
symptoms o panic, at adose o 2000 mg sublingually as needed.An
intramuscular injection o vitamin B12
(1500 mcg) was also provided. The patientwas given the
Hoer-Osmond Diagnostic(HOD) test to determine the severity ohis
schizoaective disorder.
The patients HOD test was re-ceived and scored on December 17,
2004(Table 4,p.28). The higher the total score,
the greater the probability o that patienthaving schizophrenia.
For a patient witha pre-established diagnosis, the HOD test
can also be used to evaluate the severity omental disturbances
and assess a patientsresponse to treatment. In this patientscase,
his total score did indicate thathe was symptomatic. I his total
scoreswere to decline over time, it would be anindication o
improvement.
About six weeks later, on January 26,2005, the patient returned
or another ap-pointment. He elt that he was no longer
symptomatic in terms o his diagnosiso schizoaective disorder.
The niacincaused the patient to vomit, so he reducedthe dose to
1000 mg three times daily. Hedid not like the taste o L-glycine so
henever really tried the treatment. He dideel that his anxiety had
improved about10%. The patient was given another in-tramuscular
injection, but the dose was
dierent as it now contained olic acid (0.5mL or 2.5 mg) and had
a greater concen-tration o vitamin B12 (1 mL or 5000 mcg).He was
asked to retry the L-glycine andreturn in another 5 to 6 weeks.
On March 7, 2005, the patient eltthat his diagnosis was better
describedas social anxiety disorder with somesymptoms o
schizoaective disorder.He did not try the L-glycine as he was
instructed to do. In terms o his anxiety,he elt about 20-30%
better than the lastvisit. He was given another
intramuscularinjection o olic acid (2.5 mg) and vitaminB12 (5000
mcg).
The patient returned or another ap-pointment on April 20, 2005.
He had seena new psychiatrist who recommended thatthe patient
complete a series o cognitive
behavior therapy or his social anxietydisorder. The patient was
also attendinga weekly group or patients with socialanxiety
disorder. The psychiatrist pre-scribed 20 mg o citalopram, and took
himo the olanzapine. He was sleeping lesssince discontinuing the
olanzapine. The
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
14/17
30
Journal o Orthomolecular Medicine Vol. 21, No. 1, 2006
psychiatrist also instructed the patientto continue with
risperidone (4 mg atbedtime), and bupropion hydrochloride
(150 mg daily). The patient did report abetter sense o well
being, even though heelt more depressed during the previousweek.
His only problem was ear. He wasunable to look at people when
riding thesubway because o the way people lookedback at him. He
also thought that peoplewere judging him. For his anxiety,
thepatient was prescribed L-taurine at adose o 1500 mg twice daily
to be taken
away rom ood. He was also prescribedginkgo biloba extract (180
mg daily) tohelp with depression, the side eects orisperidone, and
or erectile dysunction.Another intramuscular injection o olicacid
(2.5 mg) and vitamin B12 (5000 mcg)was given to the patient.
The patient had one more ollow-upon June 27, 2005. He reduced
the risperi-
done to 2 mg daily on his own. He alsodiscontinued the
citalopram and bupro-pion hydrochloride. He did not eel worsethan
beore and, in act, indicated that hewas more alert and required
less sleep.He did not complain o any withdrawalsymptoms rom
discontinuing the medi-cations. His social anxiety seemed
muchimproved. He was able to cover or his a-ther as a courier and
interact with people.
This would not have been possible just aew months previously.
The patient justcompleted his auto mechanic program,
and was excited about going to college inthe all or accounting.
He also remarkedthat his paranoid thoughts were gone, and
were much better since stopping the twomedications. The patient
was instructedto stay on the orthomolecular and bo-tanical
treatments. He was also advisedto continue avoiding all milk and
dairyproducts. I assured him that as long as heremained consistent
with the program, hehad very little chance o a relapse.
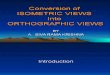
I received the patients nal set oHOD results on June 30, 2005.
As evident,
the patients scores dramatically improveddemonstrating the
eectiveness o theorthomolecular and botanical approach.(See Table
5, below).
DiscussionThe goals o this report were to review
the known side eects o the atypicalAPDs, and clariy some o the
best ortho-
molecular and botanical strategies thatmight have value in terms
o side eectprevention and/or reduction. Even withthis knowledge,
schizophrenic patientsnd themselves in an unortunate pre-dicament.
Should they stay on the atypi-cal APDs and suer extreme
metabolicconsequences despite using adjunctiveorthomolecular and
botanical treatments?Hoer has written about the tranquilizer
psychosis, and how the atypical APDsmake chronic schizophrenic
patientssick.53 In that same report, he mentions
Table 5. Patients nal set o HOD results
HODTestItems June2005ResultsTotal Score (TS) 5Perceptual Score
(PerS) 0Paranoid Score (PS) 0Depression Score (DS) 1Ratio Score
(RS) 5Short Form (SF) 0
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
15/17
31
Orthomolecular and Botanical Treatments or Side Eects o
Antipsychotic Drugs
how these drugs damage the brain anddecrease the odds these
patients can everrecover. Even with adjunctive orthomo-
lecular and botanical treatments, it is ex-tremely dicult or
schizophrenic patientsto ully recover or considerably improvewhile
remaining on atypical APDs.
Another option is or schizophrenicpatients to go o o their
atypical APDsand suer the consequences o havingterrible withdrawal
symptoms and a re-currence o their psychoses. This choiceis also
inadequate. We propose a third
and more reasonable solution, which is tovery slowly (over
months and sometimesyears) withdraw rom the atypical APDsand
include the components o an idealtreatment program. The components
osuch an ideal treatment, as reported byHoer, include: (1) shelter;
(2) decency,understanding, support, saety, and pri-vacy; (3)
psychiatric treatment; and (4)
orthomolecular treatment.53
All o thesecomponents are equally important. Mucho the success o
this ideal treatment pro-gram depends on the skill o the
treatingclinician and the compliance and patienceo the patient.
Orthomolecular interven-tions do not work immediately, and
manymonths might go by beore therapeutic e-ects are noticed. We do
recommend thatduring the lengthy process o recovery, cli-
nicians utilize many o the orthomolecularand botanical
approaches to minimize thedamaging metabolic eects o these
drugs.Patients need to know that they cannotbegin the process o
drug withdrawal untilthey begin to eel better. Once this hap-pens,
the atypical APD can be slowly re-duced over many months and even
years.I the drug is withdrawn too rapidly, very
unpleasant withdrawal symptoms occur,in addition to an increased
likelihood opsychosis. For more inormation on thecomponents o an
ideal treatment plan,please reer to Hoers latest book
onschizophrenia.54Conclusion
The atypical APDs cause numerousside eects such as EPS,
hyperprolac-tinemia, weight gain, diabetes, atigue, and
cardiac arrhythmias. Some o these sideeects might be reduced
and/or preventedby using speciic orthomolecular andbotanical
treatments. Controlled clinicaltrials are needed to properly
evaluate theeectiveness that orthomolecular andbotanical agents
have upon mitigatingthe side eects o atypical APDs. At pres-ent,
Hoers ideal treatment plan appearsto be the only eective approach
that
enables chronic schizophrenic patientsthe opportunity to ully
recover withoutmetabolic dysunction and long-termbrain damage.
AcknowledgementsWritten consent was obtained rom
the patient or publication o this report.Special thanks goes to
Mrs. Erynn Marcus
or her editing and review o this report.
References1. Tandon R, Halbreich U: The second generation
atypical antipsychotics: similar improved e-cacy but dierent
neuroendocrine side eects.
Psychoneuroendocrinology, 2003; 28: 1-7.2. Carvalho RC, Silva
RH, Ablio PN, et al: An-
tidyskinetic eects o risperidone on animalmodels o tardive
dyskinesia in mice. Brain
Res Bull, 2003; 60: 115-124.
3. Schulz SC, Thomson R, Brecher M: The ecacyo quetiapine vs
haloperidol and placebo: ameta-analytic study o ecacy. Schizophr
Res,2003; 62(1-2): 1-12.
4. Lalonde P: Evaluating Antipsychotic Medica-tions: Predictors
o Clinical Eectiveness.Can
J Psychiatry, 2003; 48(suppl 1): 3S-12S.5. Halbreich U, Kinon
BJ, Gilmore JA, et al: El-
evated prolactin in patients with schizophre-nia: mechanisms and
related adverse eects.
Psychoneuroendocrinology, 2003; 28: 53-67.6. Hammer M: The Eects
o atypical antipsy-
chotics on serum prolactin levels. Ann ClinPsychiatry, 2002;14
(3):163-173.
7. Nasrallah HA, Tandon R: Ecacy, saety andtolerability o
quetiapine in patients withschizophrenia. J Clin Psychiatry, 2002;
63(suppl 13): 12-20.
8. Cutler AJ: Sexual dysunction and antipsy-
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
16/17
-
7/27/2019 Ortho and Botanical Treatments to Alleviate Side
Effects of Atypical Antipshy Drugs
17/17
Orthomolecular and Botanical Treatments or Side Eects o
Antipsychotic Drugs
cells. Mechanism o action coupled to endo-crine eects.
Neuroendocrinology, 2001; 73:334-343.
38. Lee TY, Pan JT: Involvement o central GAB-
Aergic neurons in basal and diurnal changeso tuberoinundibular
dopaminergic neuronalactivity and prolactin secretion.Lie Sci,
2001;68: 1965-1975.
39. Dulloo AG, Duret C, Rohrer D, et al: Ecacy oa green tea
extract rich in catechin polyphe-nols and caeine in increasing 24-h
energyexpenditure and at oxidation in humans.Am
J Clin Nutr, 1999; 70: 1040-1045.40. Dulloo AG, Seydoux J,
Girardier L, et al: Green
tea and thermogenesis: interactions between
catechin-polyphenols, caeine and sympa-thetic activity.Int J
Obes Relat Metab Disord,2000; 24: 252-258.
41. Chantre P, Lairon D: Recent ndings o greentea extract AR25
(Exolise) and its activityor the treatment o obesity.
Phytomedicine,2002;9:3-8.
42. Toeper EW, Mertz W, Polansky MM, et al:Preparation o
chromium-containing mate-rial o glucose tolerance actor activity
romBrewers yeast extracts and by synthesis. J
Agric Food Chem, 1977; 25: 162-166.43. Vincent JB: Quest or the
molecular mecha-nism o chromium action and its relationshipto
diabetes.Nutr Rev, 2000; 58: 67-72.
44. Davis CM, Vincent JB: Chromium in carbohy-drate and lipid
metabolism.J Biol Inorg Chem,1997; 2: 675-679.
45. Vincent JB: Mechanisms o chromium
action:low-molecular-weight, chromium-bindingsubstance.J Am Coll
Nutr, 1999; 18: 6-12.
46. Anderson RA, Cheng N, Bryden NE, et al:Elevated intakes o
supplemental chromiumimprove glucose and insulin variables in
indi-viduals with type II diabetes.Diabetes, 1997;46:
1786-1791.
47. Lamson DW, Plaza SM: The saety and ecacyo high-dose
chromium.Altern Med Rev, 2002;7: 218-235.
48. Singer P, Wirth M: Can n-3 PUFA reduce car-diac arrhythmias?
Results o a clinical trial.
Prostaglandins Leukot Essent Fatty Acids,2004; 71: 153-159.
49. Xiao YF, Ke Q, Chen Y, et al: Inhibitory eect
o n-3 sh oil atty acids on cardiac Na+/Ca2+exchange currents in
HEK293t cells.Biochem
Biophys Res Commun, 2004; 321: 116-123.50. Lee KW, Hamaad A,
MacFadyen RJ, et al:
Eects o dietary at intake in sudden death:reduction o death with
omega-3 atty acids.Curr Cardiol Rep, 2004; 6: 371-378.
51. Harris WS: Are omega-3 atty acids the mostimportant
nutritional modulators o coronaryheart disease risk? Curr
Atheroscler Rep, 2004;6: 447-452.
52. Hoer A: Treatment o schizophrenia. In. eds.Williams RJ,
Kalita DK.A Physicians Handbookon Orthomolecular Medicine. New
Canaan, CT,Keats Publishing, Inc. 1977; 83-89.
53. Hoer A: Treating chronic schizophrenicpatients.J Orthomol
Med, 2002; 17: 25-41.
54. Hoer A: Healing Schizophrenia. Toronto,
Ontario. CCNM Press Inc. 2004.