Embed Size (px)
Citation preview

INTRODUCTION
Medial knee osteoarthritis is not uncommon and hightibial osteotomy (HTO) was described for the first time,more than 50 years ago [1-3]. Nowadays, it remains agood option [4-13] despite the large expansion of totalknee replacement (TKR) or the revival of unicompart-mental knee prosthesis boosted by the less-invasivesurgery concept. It is well indicated for “young” andactive people (less than 65 years of age) with moderatearthritis (narrowing joint line up to 100% without anybone wear or instability).
Nevertheless, it is a demanding surgery, exposing toexcessive over or under correction leading to earlier fail-ure [12] or oblique joint line (Fig. 1) being the cause ofdifficulties when performing later TKR. This obliquejoint line corresponds to an excessive valgus of the tibialmechanical axis [14]. It is all the more frequent whenvarus is important because of a femoral or a femoral andtibial deformity. The desirable over correction (3° to 6°)to achieve a good clinical result increases even more thisoblique joint line.
One can consider combined femoral and tibial osteo-
tomy as a solution to avoid excessive joint line obliquity.However, prior to the advent of computer navigation thiswas only performed on a limited basis because of the dif-ficulty in obtaining an accurate lower leg axis withoutany reproducible assistance.
Lebanese Medical Journal 2017 • Volume 65 (3) 133
OORRTTHHOOPPAAEEDDIICCSSCOMPUTER-ASSISTED OSTEOTOMIES FOR GENU VARUM DEFORMITYRationale, Surgical Technique, Outcome and Return to Sportshttp://www.lebanesemedicaljournal.org/articles/65-3/original2.pdfDominique SARAGAGLIA1*, René-Christopher ROUCHY1, Jérémy COGNAULT1, Roch MADER1
Brice RUBENS-DUVAL1, Régis PAILHÉ1
Saragaglia D, Rouchy RC, Cognault J, Mader R, Rubens-Duval B, Pailhé R. Computer-assisted osteotomies for genuvarum deformity: rationale, surgical technique, outcome andreturn to sports. J Med Liban 2017 ; 65 (3) : 133-138.
Saragaglia D, Rouchy RC, Cognault J, Mader R, Rubens-Duval B, Pailhé R. Les ostéotomies de valgisation assistées parordinateur dans le genu varum: raisons, techniques opératoires,résultats et reprise du sport. J Med Liban 2017; 65 (3): 133-138.
ABSTRACT•High tibial osteotomy (HTO) is commonly usedfor genu varum deformity in young and active patients.Corrective valgus osteotomy may however lead to an obliquejoint line in cases of associated femur varum or absence oftibia vara. To avoid this drawback, we use an accurate andreproducible radiological protocol allowing to choose the bestindication between HTO, double level osteotomy (DLO) anddistal femoral osteotomy (DFO). Computer-navigation of theosteotomies is the best choice to achieve the preoperativegoal, above all to avoid too much overcorrection, whichcould be detrimental to resume sports. In this article, therationale of this choice, the operative procedures, theirresults as well as the possibilities to resume sports will bepresented
Keywords : genu varum; navigation; computer; osteotomy;sport
RÉSUMÉ • L’ostéotomie tibiale de valgisation est couram-ment utilisée chez les patients jeunes et actifs pour traiter legenu varum. Cependant, l’ostéotomie de correction peut con-duire à un interligne oblique en cas de varus fémoral associéou en l’absence de tibia vara. Afin d’éviter cette situation,nous utilisons un protocole radiologique reproductible qui per-met de choisir la meilleure indication entre ostéotomie tibialede valgisation (OTV), double ostéotomie et ostéotomie fémo-rale distale. La navigation informatisée des ostéotomies est lemeilleur choix pour atteindre l’objectif préopératoire, et toutparticulièrement, pour éviter une trop grande hypercorrectionqui pourrait compromettre la reprise sportive. Dans cet article,seront présentés les raisons de ce choix, les techniques opé-ratoires et leurs résultats ainsi que les possibilités de reprisedu sport.
1Department of Orthopaedic Surgery and Sport Traumatology,Grenoble South Teaching Hospital, 38130, Échirolles, France.
*Corresponding author: Dominique Saragaglia, MD. e-mail: [email protected]
FIGURE 1. Severe oblique joint line (right knee) after high tibial osteotomy. Notice the extreme tibial valgus.
Drawing on our experience with TKR and HTO navi-gation [15-19] we used the principles of computer-assistedsurgery for double level osteotomy (DLO) hoping to in-crease the accuracy of this difficult procedure.
The preoperative radiological assessment will be pre-sented as well as the computer-assisted operative proce-dure, the indications of HTO, DLO and distal femoralosteotomy (DFO). And the rationale behind this line ofthought will be discussed. Moreover, return to sportingactivity will be discussed knowing that only a few papershave been published about this topic [20-25].
RADIOLOGICAL ASSESSMENT
Preoperatively standing AP, lateral, and 45° PA weight-bearing views are obtained. In addition, it is essential toobtain AP long leg standing X-rays to assess the hip kneeankle (HKA) angle for preoperative planning.
Ramadier’s protocol [26] allows these measurementsto be reproducible pre- and postoperatively. This proto-col can be described as follows: first, to determine accu-rately the frontal plane by looking for a true lateral viewof the knee which is obtained when the posterior mar-gins of the condyles are superimposed; secondly, to turn90° around the knee the image intensifier to obtain an
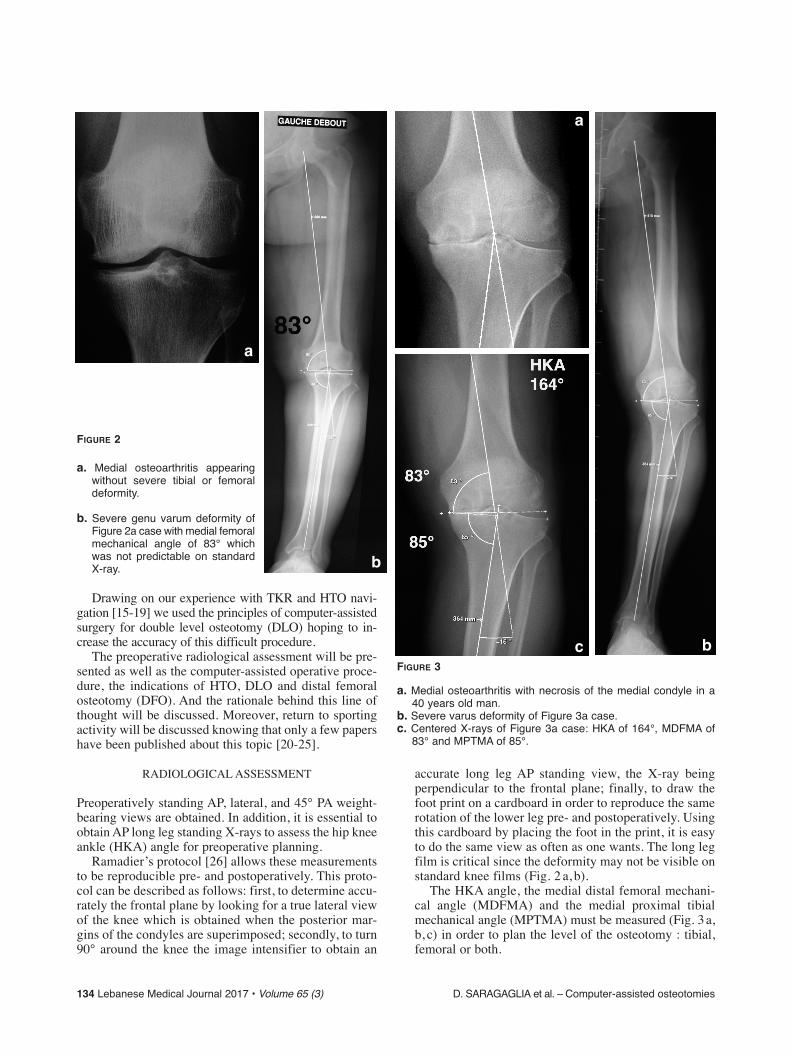
accurate long leg AP standing view, the X-ray beingperpendicular to the frontal plane; finally, to draw thefoot print on a cardboard in order to reproduce the samerotation of the lower leg pre- and postoperatively. Usingthis cardboard by placing the foot in the print, it is easyto do the same view as often as one wants. The long legfilm is critical since the deformity may not be visible onstandard knee films (Fig. 2 a, b).
The HKA angle, the medial distal femoral mechani-cal angle (MDFMA) and the medial proximal tibialmechanical angle (MPTMA) must be measured (Fig. 3a,b, c) in order to plan the level of the osteotomy : tibial,femoral or both.
134 Lebanese Medical Journal 2017 • Volume 65 (3) D. SARAGAGLIA et al. – Computer-assisted osteotomies
FIGURE 2
a. Medial osteoarthritis appearingwithout severe tibial or femoraldeformity.
b. Severe genu varum deformity ofFigure 2a case with medial femoralmechanical angle of 83° whichwas not predictable on standardX-ray.
FIGURE 3
a. Medial osteoarthritis with necrosis of the medial condyle in a40 years old man.
b. Severe varus deformity of Figure 3a case.c. Centered X-rays of Figure 3a case: HKA of 164°, MDFMA of
83° and MPTMA of 85°.
a
b
a
bc

D. SARAGAGLIA et al. – Compuer-assisted osteotomies Lebanese Medical Journal 2017 • Volume 65 (3) 135
Grading of osteoarthritis is performed typically usingthe modified Ahlbäck classification [18]. (Table I)
SURGICAL TECHNIQUES
Opening wedge computer-navigated HTOThe software is a derivative of the one used for TKAwhich has been fully described in previous articles [15-17] (Orthopilot® Navigation System, B-Braun-Aesculap,Tuttlingen, Germany). The same principals of real timeacquisition of the rotation center of the hip, knee andankle centers and of the anatomical landmarks at the levelof the knee joint line and ankle is applied. This allows themechanical axis of the lower limb to be shown dynami-cally on the computer screen, i.e. the axis of the lowerlimb to be seen both pre- and postosteotomy and to checkif the preplanned correction has been established.
A tourniquet is placed at the root of the thigh and theprocedure follows this sequence: The rigid body markersare fixed at the level of the distal femur and proximaltibia allowing acquisition of the centers of the hip, kneeand ankle (Fig. 4). The lower limb mechanical axis thenappears on the screen and can be compared with the pre-operative radiological goniometry.
A five to six centimeters long incision is made on themedial upper end of the tibia just at the level of the ante-rior tuberosity of the tibia. The pes anserinus is incisedjust above the gracilis tendon and a retractor is placedagainst the posteromedial corner of the tibia. Then, thesuperficial medial collateral ligament is released fromits tibial insertion to allow an adequate opening of theosteotomy. The HTO is performed three centimetersbelow the level of the medial joint line, the level con-firmed by placing an intra-articular needle. The osteo-tomy is directed at the fibula head, keeping the saw ashorizontal as possible to avoid fracturing the lateral tibialplateau.
With the aid of two osteotomes inserted along thetrack of the saw cut, the tibia is placed into valgus. Theseare then replaced by a metal spacer, which is inherently
stable and allows the amount of correction to be calmlychecked. If there is 8° of varus, we will try a 10-11 mmspacer and make sure that an appropriate hypercorrec-tion is produced real time on the computer screen. If thisis insufficient, a thicker spacer may be trialed, and thereverse if the correction is too great. The metallic spaceris then replaced with a bio-absorbable tricalcium phos-phate wedge (Biosorb®, SBM Company, Lourdes, France)of the desired thickness, and the intervention completedby plating the proximal tibia with a locking screw plate.Then the accuracy of the osteosynthesis is checked withthe image intensifier (Fig. 5) and the wound is closed.
Computer-assisted double level osteotomyA tourniquet is placed at the root of the thigh and the firststage is essentially the same as for an HTO: insertion ofthe rigid body markers (high enough not to hamper thefemoral osteotomy and low enough on the other level toavoid interfering with the tibial osteotomy), followed bykinematic acquisition of the hip center, middle of theknee and tibio-tarsal joints in order to find the mechani-cal axis of the lower limb.
TABLE IMODIFIED AHLBACK CRITERIA ACCORDING TO SARAGAGLIA & ROBERTS
Grade 1 < 50% joint space narrowingGrade 2 50-100% joint space narrowingGrade 3 100% narrowing whithout any bone wearGrade 4 Bone wear but no lateral instability
Grade 5 Bone wear with lateral compartmentdecoaptation ± posterolateral subluxation
FIGURE 4. Left lower leg with rigid bodies at the levelof the femur and the tibia. FIGURE 5. Radiological result of an HTO (3 months follow-up).
136 Lebanese Medical Journal 2017 • Volume 65 (3) D. SARAGAGLIA et al. – Computer-assisted osteotomies
The second stage consists of making the femoral closingosteotomy in the distal femur (in general a 5 to 6° alterationis made, although sometimes more in congenital femoralvarus) and fixing it in position with a locking screw plate.A lateral approach with elevation of the vastus lateralis ischosen, the lateral arthrotomy allowing to locate the tip ofthe trochlea. The track of the osteotomy lies above thetrochlea and is directed obliquely from above laterally tobelow on the medial femoral cortex. A wedge of bone isthen excised from the distal femur with a 4-5 mm lateralbase, corresponding to a 5-6° correction. The osteotomy isfixed with the plate after placing the femur into valgusmanually. Once this stage is reached the mechanical axis isrechecked so that the required correction at the level of thetibia can be calculated in order to achieve the preoperativeobjectives. Then the wound is closed on a drain.
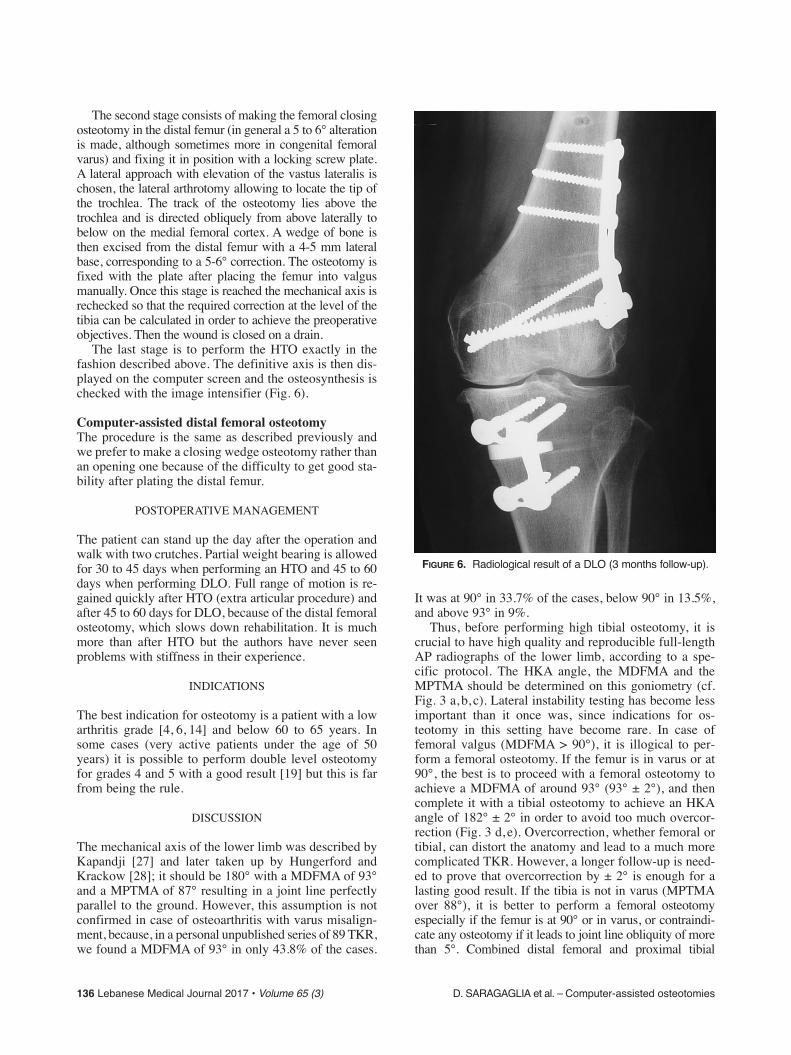
The last stage is to perform the HTO exactly in thefashion described above. The definitive axis is then dis-played on the computer screen and the osteosynthesis ischecked with the image intensifier (Fig. 6).
Computer-assisted distal femoral osteotomyThe procedure is the same as described previously andwe prefer to make a closing wedge osteotomy rather thanan opening one because of the difficulty to get good sta-bility after plating the distal femur.
POSTOPERATIVE MANAGEMENT
The patient can stand up the day after the operation andwalk with two crutches. Partial weight bearing is allowedfor 30 to 45 days when performing an HTO and 45 to 60days when performing DLO. Full range of motion is re-gained quickly after HTO (extra articular procedure) andafter 45 to 60 days for DLO, because of the distal femoralosteotomy, which slows down rehabilitation. It is muchmore than after HTO but the authors have never seenproblems with stiffness in their experience.
INDICATIONS
The best indication for osteotomy is a patient with a lowarthritis grade [4, 6, 14] and below 60 to 65 years. Insome cases (very active patients under the age of 50years) it is possible to perform double level osteotomyfor grades 4 and 5 with a good result [19] but this is farfrom being the rule.
DISCUSSION
The mechanical axis of the lower limb was described byKapandji [27] and later taken up by Hungerford andKrackow [28]; it should be 180° with a MDFMA of 93°and a MPTMA of 87° resulting in a joint line perfectlyparallel to the ground. However, this assumption is notconfirmed in case of osteoarthritis with varus misalign-ment, because, in a personal unpublished series of 89 TKR,we found a MDFMA of 93° in only 43.8% of the cases.
It was at 90° in 33.7% of the cases, below 90° in 13.5%,and above 93° in 9%.
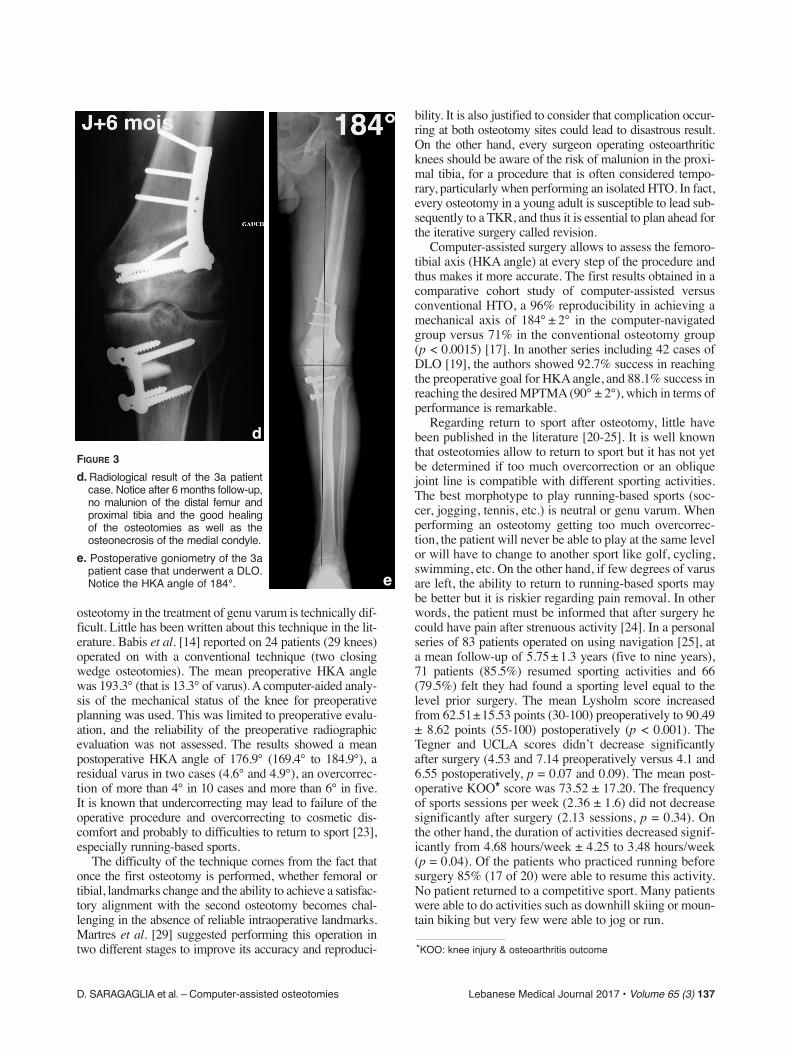
Thus, before performing high tibial osteotomy, it iscrucial to have high quality and reproducible full-lengthAP radiographs of the lower limb, according to a spe-cific protocol. The HKA angle, the MDFMA and theMPTMA should be determined on this goniometry (cf.Fig. 3 a, b, c). Lateral instability testing has become lessimportant than it once was, since indications for os-teotomy in this setting have become rare. In case offemoral valgus (MDFMA > 90°), it is illogical to per-form a femoral osteotomy. If the femur is in varus or at90°, the best is to proceed with a femoral osteotomy toachieve a MDFMA of around 93° (93° ± 2°), and thencomplete it with a tibial osteotomy to achieve an HKAangle of 182° ± 2° in order to avoid too much overcor-rection (Fig. 3 d, e). Overcorrection, whether femoral ortibial, can distort the anatomy and lead to a much morecomplicated TKR. However, a longer follow-up is need-ed to prove that overcorrection by ± 2° is enough for alasting good result. If the tibia is not in varus (MPTMAover 88°), it is better to perform a femoral osteotomyespecially if the femur is at 90° or in varus, or contraindi-cate any osteotomy if it leads to joint line obliquity of morethan 5°. Combined distal femoral and proximal tibial
FIGURE 6. Radiological result of a DLO (3 months follow-up).
D. SARAGAGLIA et al. – Computer-assisted osteotomies Lebanese Medical Journal 2017 • Volume 65 (3) 137
osteotomy in the treatment of genu varum is technically dif-ficult. Little has been written about this technique in the lit-erature. Babis et al. [14] reported on 24 patients (29 knees)operated on with a conventional technique (two closingwedge osteotomies). The mean preoperative HKA anglewas 193.3° (that is 13.3° of varus). A computer-aided analy-sis of the mechanical status of the knee for preoperativeplanning was used. This was limited to preoperative evalu-ation, and the reliability of the preoperative radiographicevaluation was not assessed. The results showed a meanpostoperative HKA angle of 176.9° (169.4° to 184.9°), aresidual varus in two cases (4.6° and 4.9°), an overcorrec-tion of more than 4° in 10 cases and more than 6° in five.It is known that undercorrecting may lead to failure of theoperative procedure and overcorrecting to cosmetic dis-comfort and probably to difficulties to return to sport [23],especially running-based sports.
The difficulty of the technique comes from the fact thatonce the first osteotomy is performed, whether femoral ortibial, landmarks change and the ability to achieve a satisfac-tory alignment with the second osteotomy becomes chal-lenging in the absence of reliable intraoperative landmarks.Martres et al. [29] suggested performing this operation intwo different stages to improve its accuracy and reproduci-
bility. It is also justified to consider that complication occur-ring at both osteotomy sites could lead to disastrous result.On the other hand, every surgeon operating osteoarthriticknees should be aware of the risk of malunion in the proxi-mal tibia, for a procedure that is often considered tempo-rary, particularly when performing an isolated HTO. In fact,every osteotomy in a young adult is susceptible to lead sub-sequently to a TKR, and thus it is essential to plan ahead forthe iterative surgery called revision.
Computer-assisted surgery allows to assess the femoro-tibial axis (HKA angle) at every step of the procedure andthus makes it more accurate. The first results obtained in acomparative cohort study of computer-assisted versusconventional HTO, a 96% reproducibility in achieving amechanical axis of 184° ± 2° in the computer-navigatedgroup versus 71% in the conventional osteotomy group(p < 0.0015) [17]. In another series including 42 cases ofDLO [19], the authors showed 92.7% success in reachingthe preoperative goal for HKA angle, and 88.1% success inreaching the desired MPTMA (90° ± 2°), which in terms ofperformance is remarkable.
Regarding return to sport after osteotomy, little havebeen published in the literature [20-25]. It is well knownthat osteotomies allow to return to sport but it has not yetbe determined if too much overcorrection or an obliquejoint line is compatible with different sporting activities.The best morphotype to play running-based sports (soc-cer, jogging, tennis, etc.) is neutral or genu varum. Whenperforming an osteotomy getting too much overcorrec-tion, the patient will never be able to play at the same levelor will have to change to another sport like golf, cycling,swimming, etc. On the other hand, if few degrees of varusare left, the ability to return to running-based sports maybe better but it is riskier regarding pain removal. In otherwords, the patient must be informed that after surgery hecould have pain after strenuous activity [24]. In a personalseries of 83 patients operated on using navigation [25], ata mean follow-up of 5.75 ± 1.3 years (five to nine years),71 patients (85.5%) resumed sporting activities and 66(79.5%) felt they had found a sporting level equal to thelevel prior surgery. The mean Lysholm score increasedfrom 62.51±15.53 points (30-100) preoperatively to 90.49± 8.62 points (55-100) postoperatively (p < 0.001). TheTegner and UCLA scores didn’t decrease significantlyafter surgery (4.53 and 7.14 preoperatively versus 4.1 and6.55 postoperatively, p = 0.07 and 0.09). The mean post-operative KOO* score was 73.52 ± 17.20. The frequencyof sports sessions per week (2.36 ± 1.6) did not decreasesignificantly after surgery (2.13 sessions, p = 0.34). Onthe other hand, the duration of activities decreased signif-icantly from 4.68 hours/week ± 4.25 to 3.48 hours/week(p = 0.04). Of the patients who practiced running beforesurgery 85% (17 of 20) were able to resume this activity.No patient returned to a competitive sport. Many patientswere able to do activities such as downhill skiing or moun-tain biking but very few were able to jog or run.
d
e
FIGURE 3d. Radiological result of the 3a patient
case. Notice after 6 months follow-up,no malunion of the distal femur andproximal tibia and the good healing of the osteotomies as well as theosteonecrosis of the medial condyle.
e. Postoperative goniometry of the 3apatient case that underwent a DLO.Notice the HKA angle of 184°.
*KOO: knee injury & osteoarthritis outcome

138 Lebanese Medical Journal 2017 • Volume 65 (3) D. SARAGAGLIA et al. – Computer-assisted osteotomies
CONCLUSION
“Young” patient genu varum deformity can be corrected byhigh tibial valgus osteotomy, but it is not the sole option. Theindication is based on an accurate and reproducible radio-logical protocol including at least standing AP long legX-ray. It is useful to measure not only the HKA angle butalso the medial distal femoral mechanical (MDFMA) andmedial proximal tibial mechanical (MPTMA) angles. Thesemeasures will guide the surgeon to choose the best indica-tion. When the MDFMA is in valgus (≥ 93°) and the MP-TMA in varus (< 88°) the best one is HTO. When the MD-FMA is in varus (≤ 90°) and the MPTMA in varus (< 88°)the best indication is DLO. Finally, when the MDFMA is invarus and the MPTMA > 88° the best indication is DFO.This way of thinking should avoid a too much oblique jointline, which is a difficult condition when performing revi-sion to TKA. Regarding return to sport activity, HTO andDLO allow it, but the patient must be informed that residualpain during strenuous sports is not exceptional especially ifthe osteotomy leaves some undercorrection.
REFERENCES
1. Jackson JP, Waugh W. Tibial osteotomy for osteoarthritisof the knee. J Bone Joint Surg Br 1961; 43: 746-51.
2. Merle d’Aubigné R, Ramadier JO. Arthrose du genou etsurcharge articulaire. Acta Orthop Belg 1961; 27: 365-75.
3. Judet R, Dupuis JF, Honnard F et al. Désaxations et ar-throses du genou. Le genu varum de l’adulte. Indicationsthérapeutiques, résultats. Rev Chir Orthop 1964; 13: 1-28.
4. Hernigou Ph, Medevielle D, Debeyre J et al. Proximaltibial osteotomy for osteoarthritis with varus deformity: aten to thirteen-year follow-up study. J Bone Joint SurgAm 1987; 69: 332-54.
5. Yasuda K, Majima T, Tsuchida T et al. A ten to 15-yearfollow-up observation of high tibial osteotomy in medialcompartment osteoarthrosis. Clin Orthop Relat Res 1992;282: 186-95.
6. Coventry MB, Ilstrup DM, Wallrichs SL. Proximal tibialosteotomy : a critical long-term study of eighty-sevencases. J Bone Joint Surg Am 1993; 75: 196-201.
7. Lootvoet L, Massinon A, Rossillon R et al. Ostéotomietibiale haute de valgisation pour gonarthrose sur genu va-rum : à propos d’une série de 193 cas revus après 6 à 10ans de recul. Rev Chir Orthop 1993; 79: 375-84.
8. Jenny JY, Tavan A, Jenny G et al. Taux de survie à longterme des ostéotomies tibiales de valgisation pour gonar-throse. Rev Chir Orthop 1998; 84: 350-7.
9. Rinonapoli E, Mancini GB, Corvaglia A et al. Tibial os-teotomy for varus gonarthrosis. A 0 to 21-year follow-upstudy. Clin Orthop Relat Res 1998; 353: 185-93.
10. Lerat JL. Ostéotomies dans la gonarthrose. Cahiers d’en-seignement de la SOFCOT 2000, Elsevier (ed.), Paris,pp 165-201.
11. Papachristou G, Plessas S, Sourlas J et al. Deterioration oflong-term results following high tibial osteotomy in pa-tients under 60 years of age. Int Orthop 2006; 30: 406-8.
12. Saragaglia D, Blaysat M, Inman D et al. Outcome ofopening-wedge high tibial osteotomy augmented with a
Biosorb® wedge and fixed with a plate and screws in 124patients with a mean of ten years follow-up. Inter Orthop2011; 35: 1151-6.
13. LaPrade RF, Spiridonov SI, Nystrom LM et al. Prospec-tive outcomes of young and middle-aged adults withmedial compartment osteoarthritis treated with a proxi-mal tibial opening wedge osteotomy. Arthroscopy 2012;28: 354-64.
14. Babis GC, An KN, Chao E.YS et al. Double level osteo-tomy of the knee: a method to retain joint-line obliquity.J Bone J Surg Am 2002; 84: 1380-8.
15. Picard F, Leitner F, Raoult A et al. Computer assistedknee arthroplasty. In “Reschnergestützte Verfahren inOrthopädie und Unfallchirurgie”. Steinkopff Darmstadt,PA: Jerosch, Nichol and Peikenkam, 1999: 461-71.
16. Saragaglia D, Picard F, Chaussard C et al. Mise en placedes prothèses totales du genou assistée par ordinateur :comparaison avec la technique conventionnelle. Résul-tats d’une étude prospective randomisée de 50 cas. RevChir Orthop 2001; 87: 18-28.
17. Saragaglia D, Pradel Ph, Picard F. L’ostéotomie de valgi-sation assistée par ordinateur dans le genu varum arthro-sique: résultats radiologiques d’une étude cas-témoin de 56cas. E-mémoires de l’Académie Nationale de Chirurgie2004; 3: 21-25. Available at: http://www.bium.univ-paris5.fr/acad-chirurgie
18. Saragaglia D, Roberts J. Navigated osteotomies around theknee in 170 patients with osteoarthritis secondary to genuvarum. Orthopaedics 2005; 28 (Suppl 10): S1269-S1274.
19. Saragaglia D, Blaysat M, Mercier N et al. Results of forty-two computer-assisted double level osteotomies for severegenu varum deformity. Inter Orthop 2012; 36: 999-1003.
20. Odenbring S, Tjornstrand B, Egund N et al. Functionafter tibial osteotomy for medial gonarthrosis below age50 years. Acta Orthop Scand 1989; 60: 527-31.
21. Gougoulias N, Khanna A, Maffulli N. Sports activitiesafter lower limb osteotomy. British Medical Bulletin2009; 91: 111-21.
22. Salzmann GM, Ahrens P, Naal FD et al. Sporting activi-ty after high tibial osteotomy for the treatment of medialcompartment knee osteoarthritis. Am J Sports Med 2009;37: 312-18.
23. Warme BA, Aalderink K, Amendola A. Is there a role forhigh tibial osteotomies in the athlete? Sports Health2011; 3: 59-69.
24. Bonnin MP, Laurent JR, Zadegan F et al. Can patientsreally participate in sport after high tibial osteotomy?Knee Surg Sports Traumatol Arthrosc 2013; 21: 64-73.
25. Saragaglia D, Rouchy RC, Krayan A, Refaie R. Return tosports after valgus osteotomy of the knee joint in patientswith medial unicompartmental osteoarthritis. Inter Orthop2014; 38: 2109-114.
26. Ramadier JO, Buard JE, Lortat-Jacob A et al. Mesureradiologique des déformations frontales du genou. Pro-cédé du profil vrai radiologique. Rev Chir Orthop 1982;68: 75-8.
27. Kapandji IA. Physiologie articulaire. Fascicule II 4e éd. :membre inférieur. Paris: Maloine SA (ed), 1974: p104.
28. Hungerford DS, Krackow KA. Total joint arthroplasty ofthe knee. Clin Orthop Relat Res 1985; 192: 23-30.
29. Martres S, Servien E, Aït Si Selmi T et al. Double ostéo-tomie: indication dans la gonarthrose. Rev Chir Orthop2004; 90 (Suppl n°6 ): 2S137-2S138.





























