Embed Size (px)
Citation preview

Our Workforce and Organisational
Development Approach
@ATBDudley


MCP connected to
the community.
Locality approach
provides resilience
and a basis for
services at
appropriate scale.

Teams without walls
Maximising their potential to work efficiently and effectively together – to take a shared responsibility for achieving shared outcomes
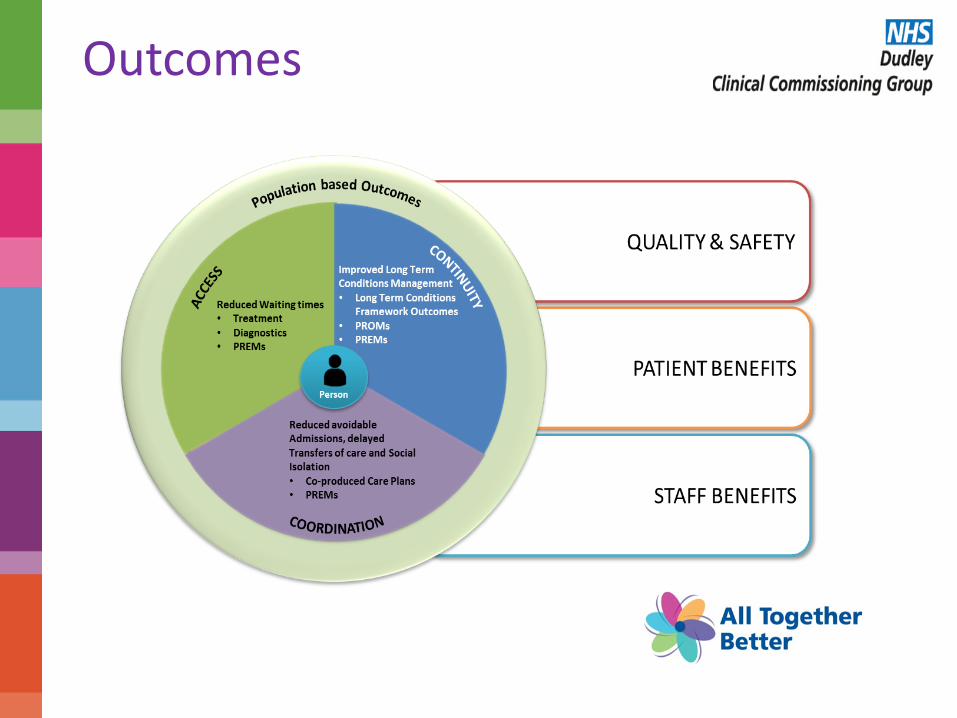
Outcomes

Creating an empowerment culture
Provide clarity of purpose
Empower delivery and improvement
Unblock barriers and encourage learning
Deliver care
Locus for improvement and learning
Identify faults and highlight barriers
Leaders
Staff

• Shared purpose
• Shared accountability
• Shared outcomes
• Understanding and respecting different organisational cultures
• Taking responsibility
• Developing talent
• Managing change
• Empowered and autonomous
• Develop distributed leadership
• Give people permission
• Cross professional boundaries
• Manage and develop relationships
Teams without Walls People make or break the difference……

• Team Development Management of change (with particular focus on changing the culture by enabling “teams without walls” )
– Practice MDTs
– Locality MDTs
– System Wide Teams
– Talent Management (ambassadors of change)
– System approach to staff engagement
• Leadership MCP strategic system wide development
– Partnership Board
– Clinical Strategy Board
– Development of Locality MCP Integration GP lead roles
– Consultants working out in the community setting
– Relationship management
– Negotiation and influencing skills
• Development of Professional Teams – Spreading the vision
– Breaking down the walls
– Effective use of skill mix
Teams without Walls People make or break the difference……

• Workforce Development – Integrated Plus
– MDT Care Co-Ordinators
– Extended role of Pharmacy
– Community Paramedics
– Place-based System Workforce Development Plan (particularly linked to STP)
– EPIC - Enabling Practices to Improve and Change
• Patient Engagement – Real patient stories
– Practice Patient Participation Groups
– Task and Finish Groups for New Care Model
– Listening events
– Public consultation
– Patient representation on Procurement Board
• Communications & HR working together – Multi-organisational with consistent language and messages
– Staff engagement
– Statement of Intent
Teams without Walls People make or break the difference……

Transformation: • Potentially the biggest change that the NHS has ever seen • A real feeling of exhilaration and trepidation • OD approach before a contracting approach – winning hearts and minds • Makes the contract an enabler of the model • Drive to make this happen Leadership: • Organisational and leadership conflict • The challenge of leaving your organisation at the door • Good leaders are nothing without their followers Staff engagement and workforce: • Inherent since before day one • New workforce solutions • Support from the new care models team • All organisations committed to joint messages and engagement • Future commissioning arrangements – the new CCG
Teams without Walls People make or break the difference……

The new integrated way of working has
helped me: better integrate with teams,
understand what services can offer...
pulling this all together in a regular meeting
has given me greater autonomy this has
directly improved patient pathways of care
and reduced unplanned admissions to
hospital.
It’s more holistic and
person centred. A
good idea that could
get much better.
It is rewarding seeing how
integration has re-energised team
members and the enthusiasm of
key professionals in the service has
encouraged more staff to want to
become involved...
Describing success: What staff are saying

“Due to this disability I have had to give up
work and I am now virtually housebound.
…[this] has opened up a lot of possibilities
for me by encouraging me to become
involved with a number of activities which
has been a massive help to me… it has
made a huge difference to my life.”
“I could have just stayed at home and
given up. I wished I would have known
about this five years ago. I’ve got what I
really want, it’s lifted me and I have a
laugh. I can feel a change in myself – I feel
more alive to be honest.”.
Describing success: What patients are saying

Focus on the Pharmaceutical Public Health Team
Clair Huckerby & Dr Duncan Jenkins
Pharmaceutical Public Health Team,
Dudley CCG and Dudley Office of Public Health

We will cover
• Our mission • How Dudley CCG uses the pharmacy workforce • History of the Practice Based Pharmacist (PBP)
team • Expansion of the team to meet workforce
pressures • An outcome based approach with a population
focus • Clinical and systems leadership – driving strategy
through to patient care

Our mission
• To improve the health and wellbeing of the population of Dudley through the safe and effective use of medicines and pharmacy services.
• To make Dudley the safest place to take medicines in the UK.
• To reduce the gap in health inequality and increase healthy life expectancy by taking a population approach to managing medicines

Pharmaceutical Public Health Agenda
Prescribing
Medicines Optimisation
Community pharmacy
development
Population level pharmaceutical needs
Governance
Clinical and systems leadership

Pharmacy in Dudley

Goals
Product
Patient
Pathway Programme
Population
5Ps value model

Meeting workforce pressures

Team history
• Dudley CCG has an established medicines management service
– Developed over last 14 years
– Led by Pharmaceutical Public Health Team
– Focussing on population health, year on year results- quality and cost focussed outcomes
– Excellent reputation
– Contribution to QIPP in excess of £1.6M / year
SHORTLISTED 2011/12
AWARDS 2016 – HIGHLY COMMENDED
WINNERS: Dudley Pharmaceutical Public Health Team Prescribing and medicines management – a Medicines Optimisation Framework for the Future.

Population focus
• MCP: population based commissioning
• Fundamental need to take a population view:
– Health economics - segmentation and targeting
– Systematic approach to care - quality and consistency
– Outcomes vs activity
• IT capabilities
• Need to deliver primary care at scale

Recent Developments…
• Extending the Role of Primary Care Practice Based Pharmacists
• Developing a Repeat Prescription Ordering Direct system (POD)
• Systematising the approach to medicines management

Outcome based
• Pharmoutcomes used to collect activity data
• Standardises data sets
• Integrated into practice
• Simplifies evaluation
• Demonstrates value
• Align to MCP outcomes framework

Primary Care Pharmacy- What does success look like?
• Skills escalator in line with tiers of service and development of specialist roles
• Accelerated learning within team-clinical skills
• PBP input into every GP practice MDT
• In excess of 8000 medication reviews
• In excess of 32,000 quality medicines interventions accepted by general practice (21K EPIC)
• In excess of £1.6M saved (over performance of QIPP by £500K)
• EPIC:
– 1131 GP appointments saved
– 530 GP hours saved
– £458K saved in 9 EPIC practices- resource costs £97K
– 217 admissions / outpatient appointments avoided
• Integration with community and hospital pharmacy
• Impact on longer term outcomes such as CVD mortality rate through managing hypertension
• Development of the HARMs project – systematising the approach to medicines management
• ROI 4:1


Clinical and systems leadership
• Systematic approach to medicines safety
• Hospital Admissions Related to Medicines
• Boundaries of clinical practice statements
• Clinical supervision
• Skills escalator


HARMs

Acute kidney injury
• Around 600 admissions AKI – HES data
• Med review and RCA to establish if a HARM – And gain learning
• Approx 47,000 on ACEIs, ARBs, diuretics
• Approx 16,000 > 75 years
• Design interventions
• Use sensitivity analyses to establish likely benefit vs cost of intervention.
• Implement through PBP team


Future plans and development
• Team expansion- 300 hours per week (Sept 2016- by Jan 2016 full capacity) continue in 2017/18
• Multispecialty Care Provider Model
• Extending competencies of individual PBPs
• Team leader role – management vs. clinical
• Sharing our learning- HSCNI, PDA, Scotland
• Further collaborations with HEIs
• Further develop population MO model
• Publications due in IJPP and Pharmaceutical Journal early 2017
• Expansion of POD
• Making an already great team better
Conclusions
• Mature approach to workforce development
• Strategy drives down into clinical practice
• Skills escalator and focus on competency
• Clinical and systems leadership essential component
• Fit for purpose for a future population based / accountable care model.

Thank You Any Questions?






























