Embed Size (px)
Citation preview
Outcomes of Treatment for Pain and Disability Associated with Complex Regional Pain
SyndromeRIC Center for Pain Management
Randy Calisoff, MD1
Zachary McCormick, MD2
Jaymin Patel, MD3
Mary Caldwell, DO1
George C. Chang-Chien, DO4
James Atchison, DO1
Christine Gagnon, Ph.D1
Steven Stanos, DO5
R. Norman Harden, MD6
1. Rehabilitation Institute of Chicago, Northwestern McGaw Medical Center. Department of Physical Medicine and Rehabilitation. Chicago, IL.
2. Pain Fellow, PGY5, Northwestern University Medical Center, Department of Anesthesiology, Northwestern University, Chicago, IL.
3. Pain Fellow, PGY5, University of Pittsburgh Medical Center, Pittsburgh, PA.4. Medical Director, Ventura County Medical Center, Ventura, CA.5. Medical Director, Swedish Pain Services, Swedish Health Systems, Seattle, WA.6. Professor Emeritus, Northwestern University; Director, Analgesic Research Consultants, LLC, Athens, GA.
Disclosures:None
Background: CRPS
• CRPS: Difficult to treat• A more comprehensive approach• Interdisciplinary care
Treatments for CRPSMirror TherapyContrast BathsExposure TherapyEdema ControlIsometric Strengthening ExercisesMaintaining FlexibilityIsotonic StrengtheningDesensitizationErgonomicsInjections
(Stanton-Hicks, et al.)
Background: CRPS• One cohort study of 12 patients with CRPS who underwent an intensive interdisciplinary pain management program (Singh, 2004)
• Study Design:• 12 patients, 4 weeks of interdisciplinary rehabilitation• PT/OT/Pool Therapy/Group Psychology/Med Management• Weight Bearing• Pressure Tolerance• Upper Extremity Isometric Endurance• Fine Motor Skills
Background: CRPS•Study Findings:•Improved:• Weight Bearing, • Pressure Tolerance, • Upper Extremity Isometric Endurance,• Fine Motor Skills
•Limitations:• 12 patients• No psychological indices were used, only function• No medication usage was determined• Pain scores were not included
RIC Clinical ReviewPurpose: Determine if CRPS can be effectively treated in a comprehensive interdisciplinary pain management program • Larger cohort of patients• Changes in function• Changes in pain• Changes in pain medication usage•Changes in mood•Changes in coping
Methods
• Retrospective cohort study
• Rehabilitation Institute of Chicago Center for Pain Management
RIC InterventionFull Day 4-Week, Monday through Friday8am to 4pm x 4 weeks totalInterdisciplinary Pain Management Program• Physical Therapy• Occupational Therapy• Pain Psychology• Relaxation Training• Pool Therapy, Aerobic Conditioning• Weekly Physician Visits• Nursing Education
Inclusion Criteria Exclusion Criteria• 18-89 years of age
• 4 week full day Interdisciplinary Pain Management Program
• Fulfilled Budapest Criteria (Harden, et al. 2010)
• Patients missing at least 2 of the following:
-NRS Pain Scores
-Functional Measurements
-Medication usage
Budapest Clinical Diagnostic Criteria for CRPS(Harden, et al. 2010)
A. Pain disproportionate to inciting eventB. Report 1 symptom in 3 of the 4 categories C. Display 1 sign in 2 or more of 4 categories
I. Hyperesthesia; AllodyniaII. Temperature asymmetry; Skin color changes; Skin color asymmetryIII. Edema; Sweating changes; Sweating asymmetryIV. Decreased range of motion; Motor dysfunction; Trophic changes
(D) There is no other diagnosis
Time Points of Data Collection
• Start of 4 week RIC Interdisciplinary Program
• End of 4 week RIC Interdisciplinary Program
Patient Characteristics: RIC Study
Total: 49 patients
- Female: 67%
- Average age: 39.6 years
- Workers Compensation: 33%
RIC Outcome Measures
Mood• Center for Epidemiologic Studies Depression Scale (CESD-10)• Pain Anxiety Symptoms Scale (PASS-20)
Chronic Pain Acceptance• Chronic Pain Acceptance Questionnaire (CPAQ)
Coping with Pain• Coping Strategies Questionnaire-Revised (CSQ-R)
Pain Ratings• NRS Pain scores (Best, Worst, Current)
RIC Outcome Measures (continued)
Physical Functioning• 6 Minute Walk Test• 2 Minute Sit to Stand Test
Perceived Disability• Pain Disability Index (PDI)
RIC Outcome Measures (continued)
Medication Usage• Medication Quantification Scale III (MQS III) Score•Assigns detriment weights to each medication•Overall risk of medication usage
(Gallizzi, et al. 2008)
RIC Outcome Measures (continued)RIC Multidimensional Patient Impression of Change (RIC-MDPIC)•Overall Status• Overall Pain• Sleep• Mood• Physical Functioning • Effectiveness of Medication• Ability to Cope with Pain, Flare-ups
Results of RIC Study
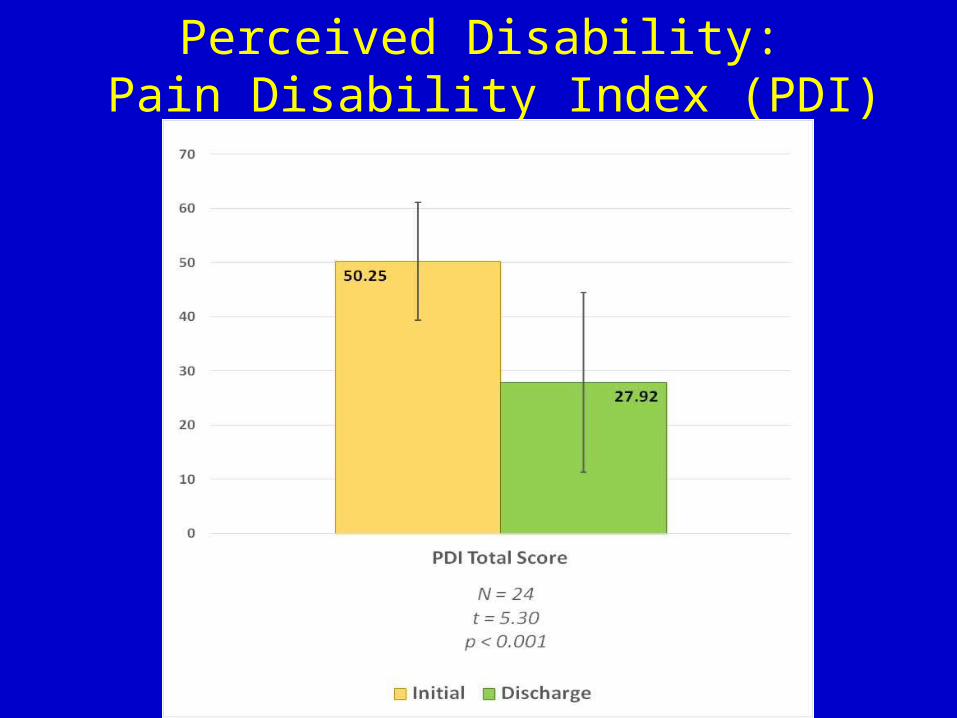
Perceived Disability: Pain Disability Index (PDI)
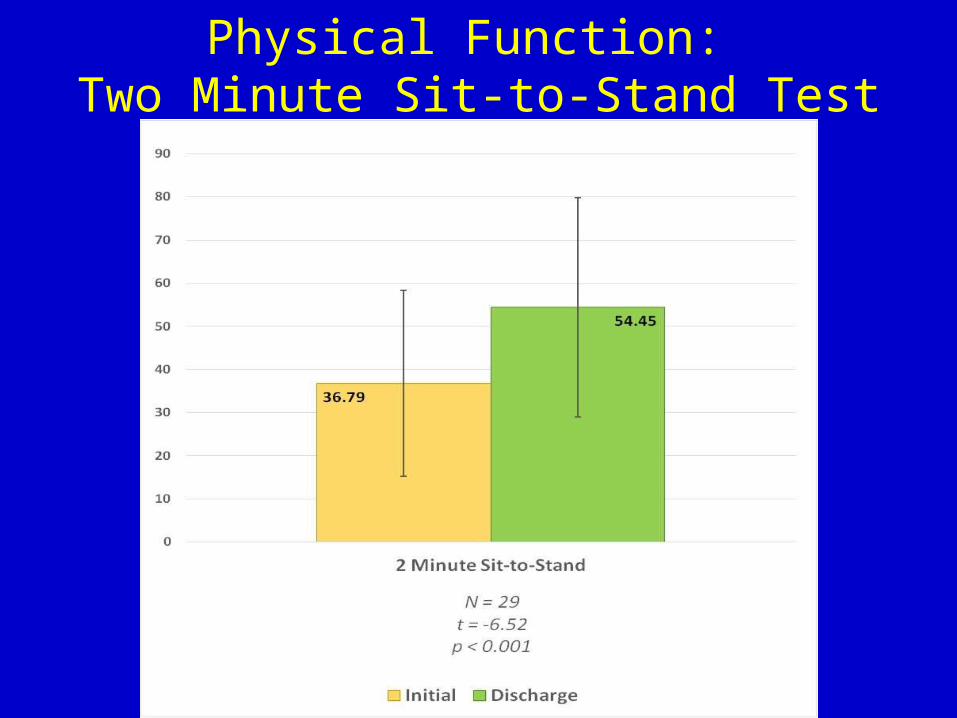
Physical Function: Two Minute Sit-to-Stand Test
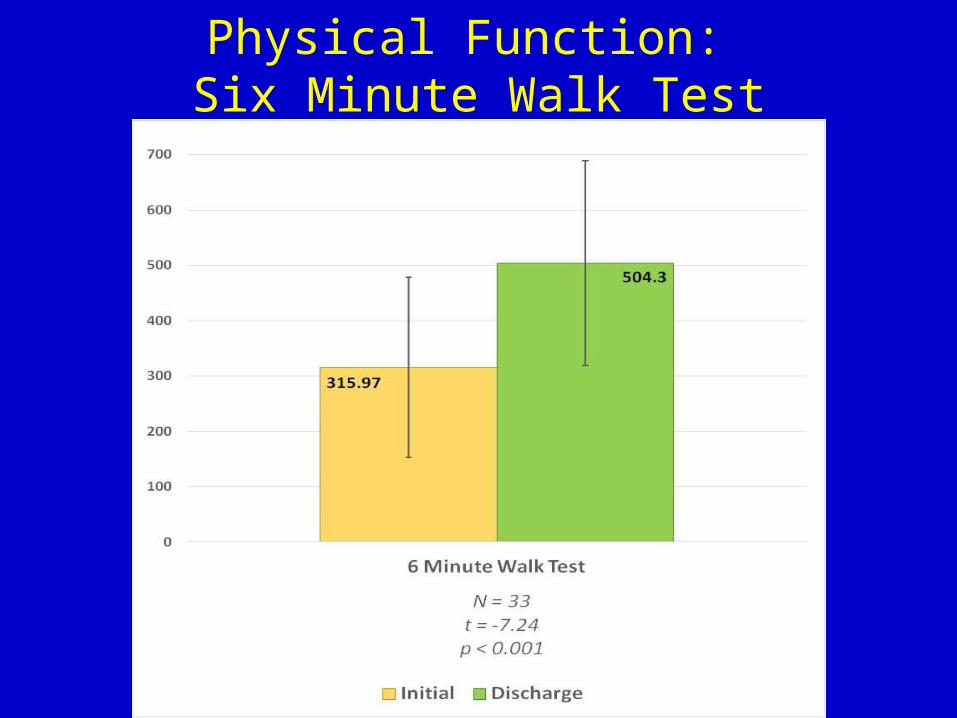
Physical Function: Six Minute Walk Test
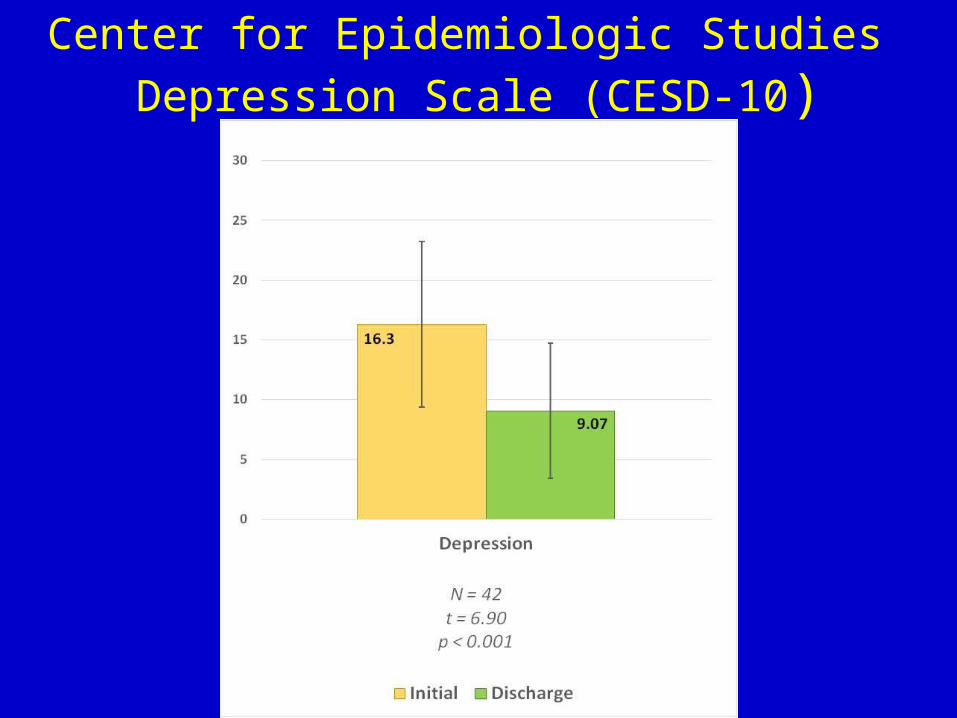
Center for Epidemiologic Studies Depression Scale (CESD-10)
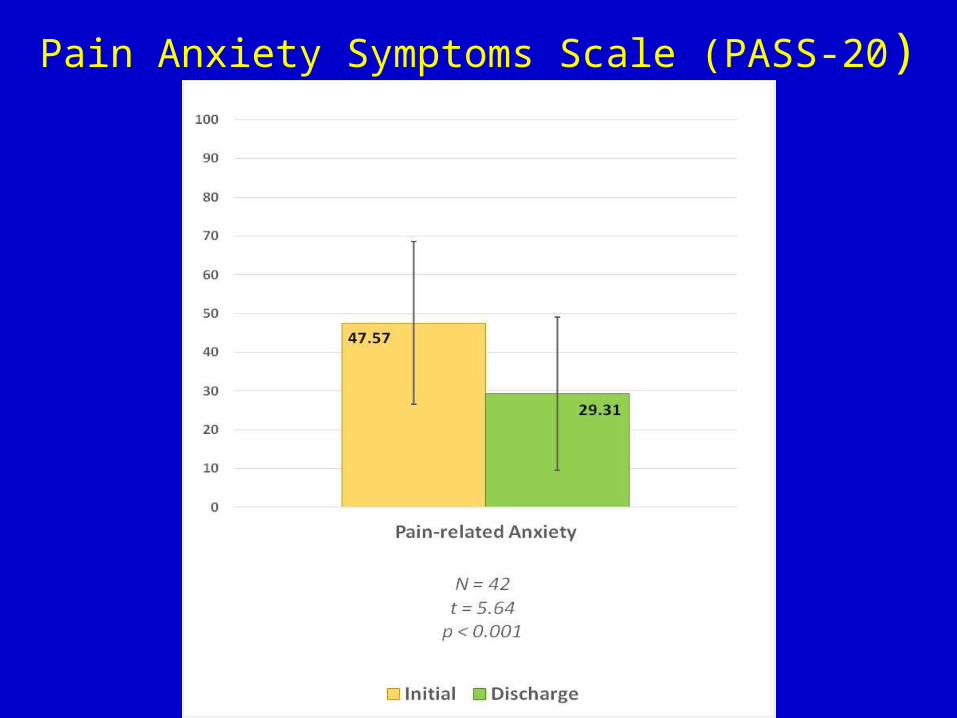
Pain Anxiety Symptoms Scale (PASS-20)
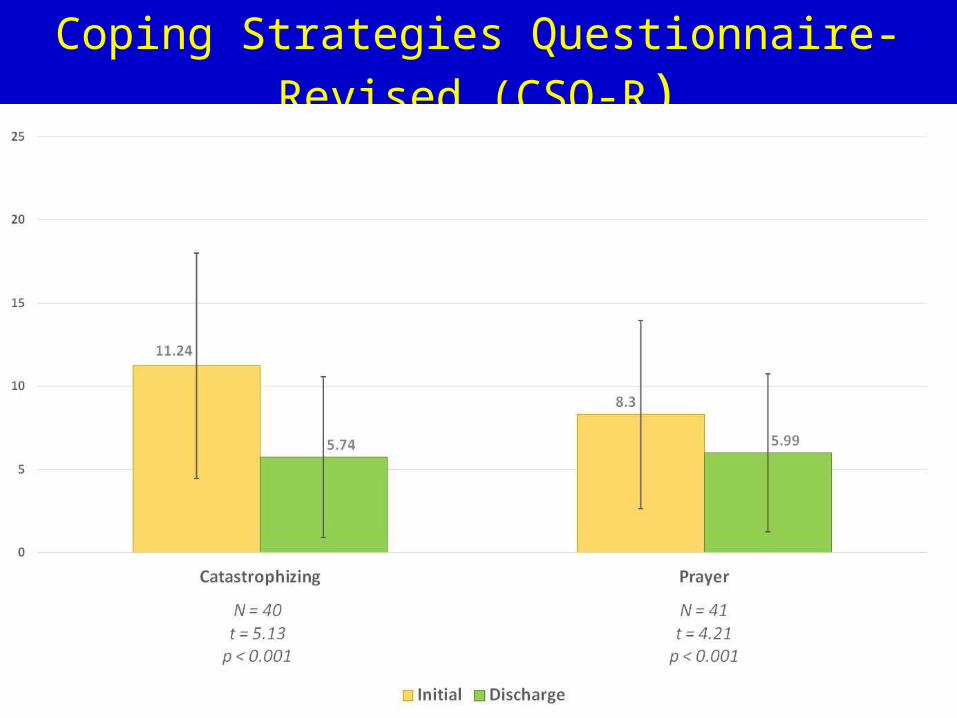
Coping Strategies Questionnaire-Revised (CSQ-R)
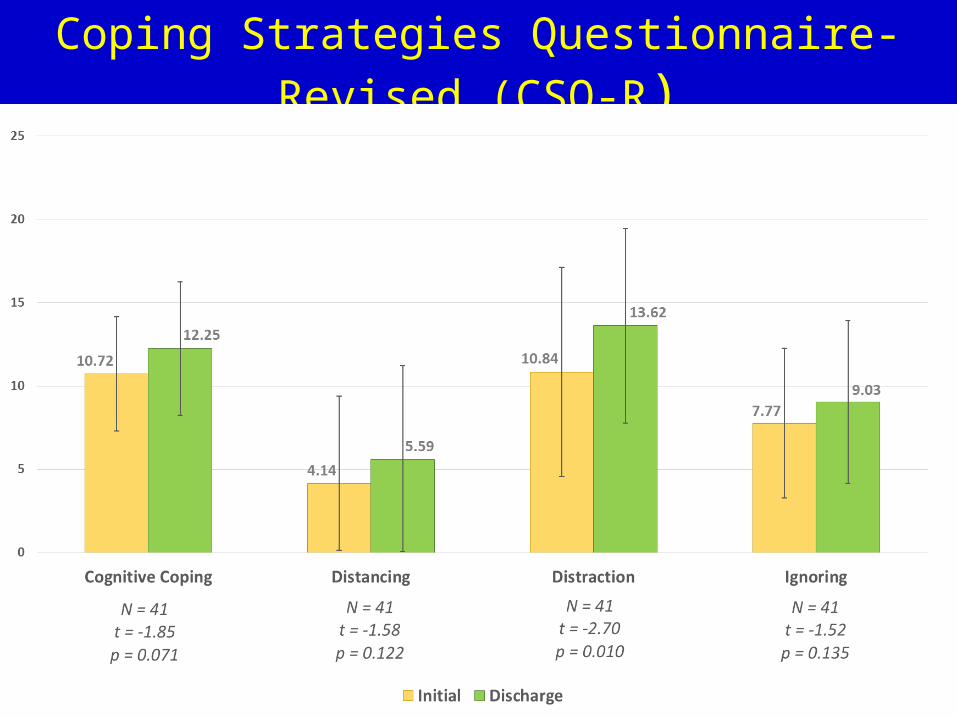
Coping Strategies Questionnaire-Revised (CSQ-R)
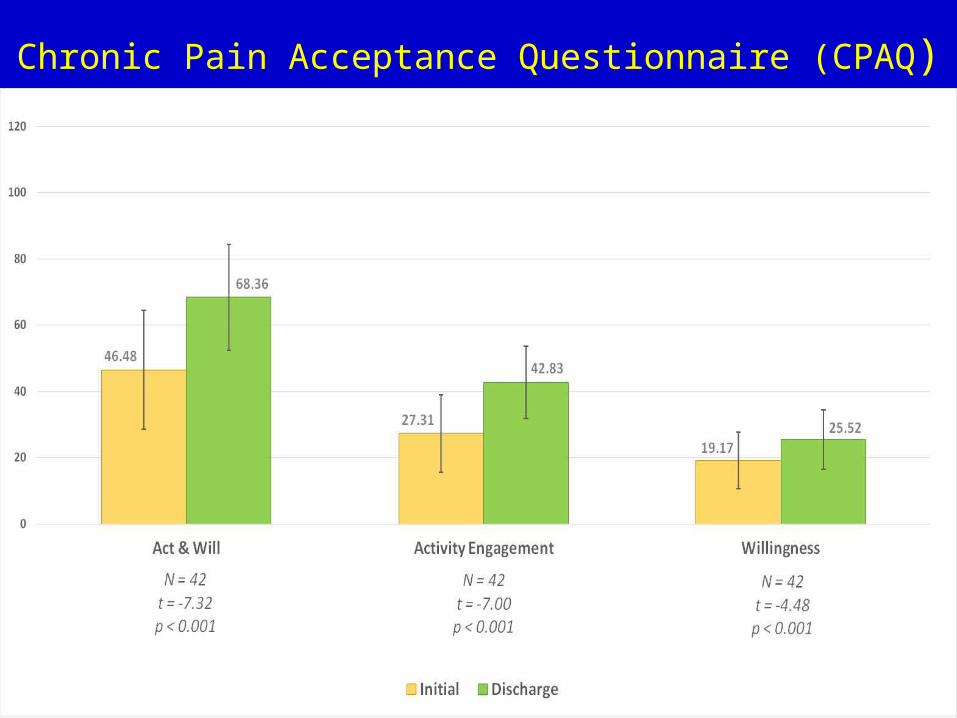
Chronic Pain Acceptance Questionnaire (CPAQ)
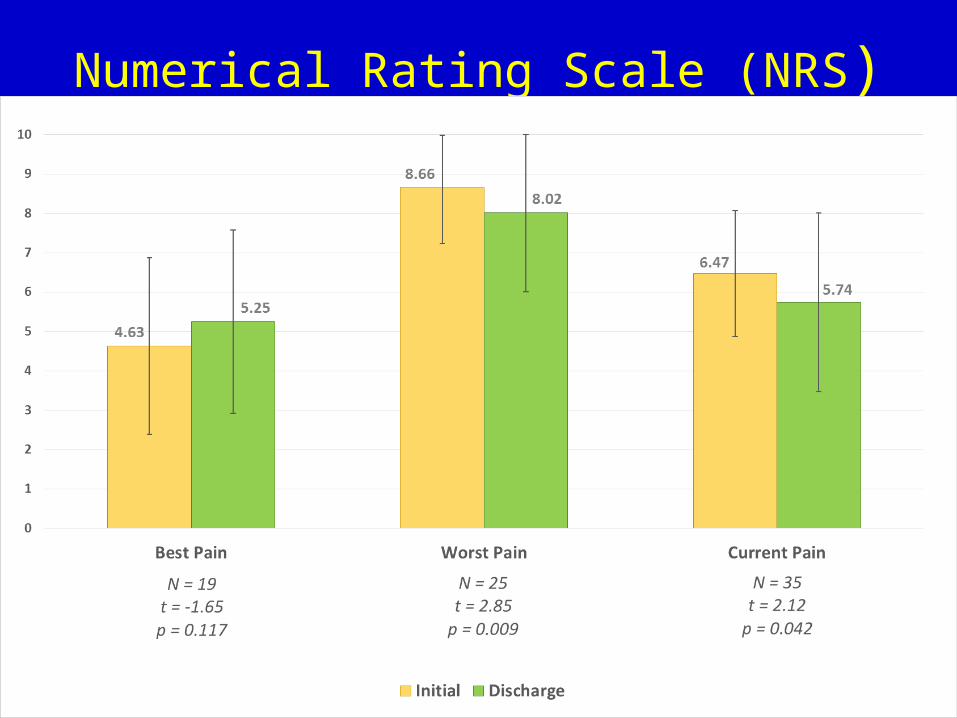
Numerical Rating Scale (NRS)
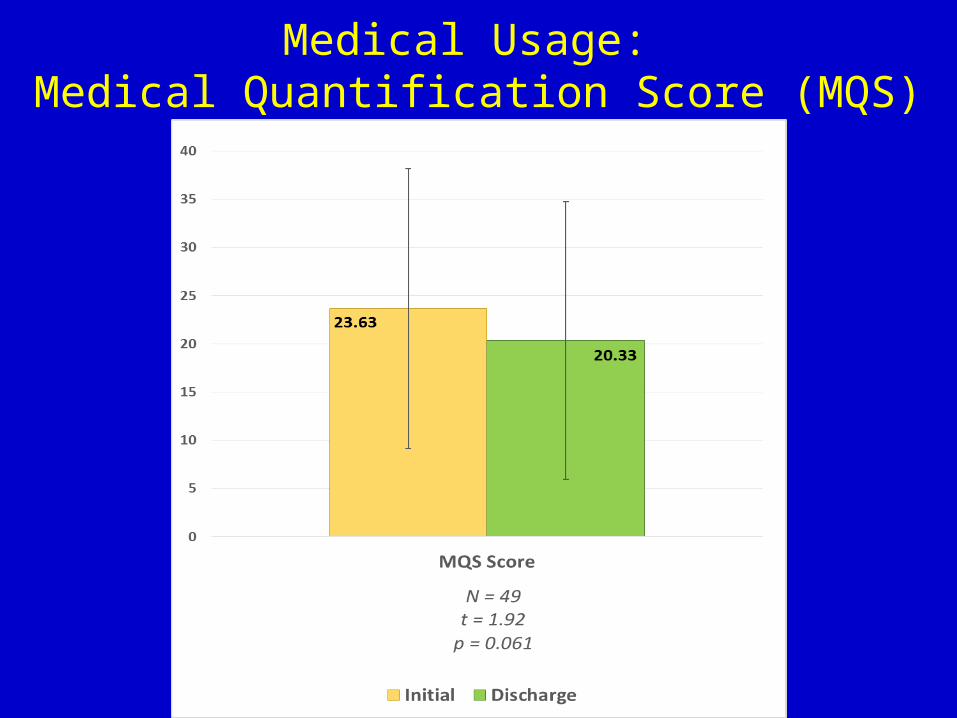
Medical Usage: Medical Quantification Score (MQS)
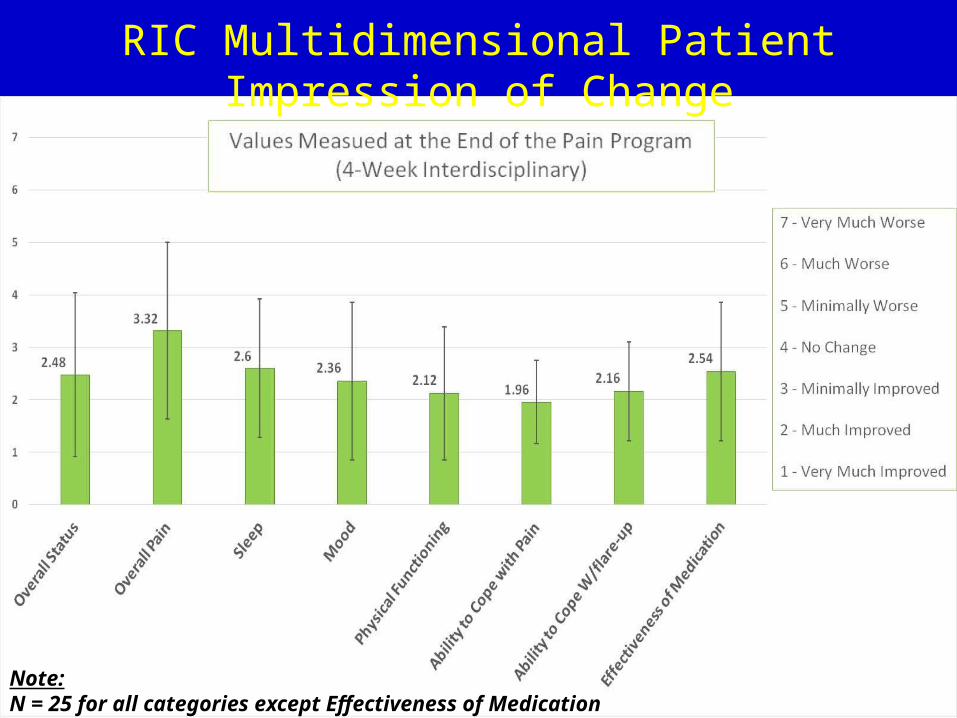
RIC Multidimensional Patient Impression of Change
Note:N = 25 for all categories except Effectiveness of Medication (N=24)
Conclusions: RIC Study
Patients’ improved with regards to:• Function• Psychometrics• Pain
Conclusions: RIC Study
Function:- Walking - Lower Extremity Transfers- Overall Activity- Perceived Disability
Conclusions: RIC Study
Psychometrics:- Depression- Pain Related Anxiety- Catastrophizing- Acceptance of pain
Conclusions: RIC Study
Pain:- Worst pain is significantly less-Current pain is significantly less-Best pain is worse at end of program, but not significantly worse
Conclusions: RIC Study Medication Use:
-Use is lower, but not significantly lower, trending
Conclusions: RIC Study
Interdisciplinary Approaches:-Benefits-Chronic Pain Conditions
Future Research at RIC• Larger Sample Size• Longer Term Outcomes•Adding a Prospective Component •Phone Call Follow Up
1. Andresen EA, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: Evaluation of a short form of the CES-D. Am JPrev 1994; 10: 77-84.
2. Bendix AF, Bendix T, Ostenfeld S, Bush E, Andersen. Active treatment programs for patients with chronic low back pain: A prospective,randomized, observer-blinded study. Eur Spine J. 1995; 4(3):148-52.
3. Bombardier C. Outcome assessments in the evaluation of treatment of spinal disorders: summary and general recommendations. Spine (Phila PA 1976) 2000; 25: 3100-3 4. Gagnon CM, Stanos SP, van der Ende G, Rader LR, Harden RN. Treatment outcomes for workers compensation patients in a U.S.-based interdisciplinary pain management program. Pain Pract 2013 Apr; 13(4):282-8.
5. Gallizzi M, Gagnon C, Harden RN, Stanos S, Khan A. Medication Quantification Scale Version III: Internal Validation of Detriment Weights Using a Chronic Pain Population. Pain Practice, Volume 8, Issue 1, 2008 1–4
6. Gatchel RJ, McGeary DD, Peterson A, Moore M, LeRoy K, Isler WC, Hryshko-Mullen AS, Edell T. Preliminary findings of a randomized controlled trial of an interdisciplinary military pain program. Mil Med 2009 Mar; 174(3):270-7. 7. Harden RN, Bruehl S, Perez RS, Birklein F, Marinus J, Maihofner C, Lubenow T, Buvanendran A, Mackey S, Graciosa J, Mogilevski M, Ramsden C, Chont M, Vatine JJ. Validation of proposed diagnostic criteria (the "Budapest Criteria") for Complex Regional Pain Syndrome. Pain 2010 Aug; 150(2):268-74.
8. Harden RN, Oaklander AL, Burton AW, Perez R, Richardson K, Swan M, Barthel J, Costa B, Graciosa J, Bruehl S. Complex Regional Pain Syndrome: Practical Diagnostic and Treatment Guidelines, 4 th Edition. Pain Medicine 2013; 14: 180-229.
9. Lang E, Liebig K, Kastner S, Neundörfer B, Heuschmann P. Multidisciplinary rehabilitation versus usual care for chronic low back pain in the community: effects on quality of life. Spine J 2003 Jul-Aug; 3(4):270-6.
References
10. McCracken LM, Dhingra L. A short version of the Pain Anxiety Symptoms Scale (PASS-20): Preliminary development and validity. Pain Res Manage 2002;7:45-50.
11. Moradi B, Hagmann S, Zahlten-Hinguranage A, Caldeira F, Putz C, Rosshirt N, Schönit E, Mesrian A, Schiltenwolf M, Neubauer E. Efficacy of multidisciplinary treatment for patients with chronic low back pain: a prospective clinical study in 395 patients. J Clin Rheumatol. 2012 Mar; 18(2):76-82.
12. Ohnmeiss DD. Repeatability of pain drawings in a low back pain population. Spine (Phila Pa 1976). 2000 Apr 15;25(8):980-8.
13. Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Pain 2004; 8: 283-91
14. Singh G, Willen SN, Boswell MV, Janata JW, Chelimsky TC. The value of interdisciplinary pain management in complex regional pain syndrome type I: A prospective outcome study. Pain Physician. 2004 Apr; 7(2):203-9. 15. Staal JB, de Bie R, de Vet HC, Hildebrandt J, Nelemans P. Injection therapy for subacute and chronic low-back pain. Cochrane Database Syst Rev 2008: CD001824
16. Stanton-Hicks M, Baron R, Boas R. Complex Regional Pain Syndrome: Guidelines for Therapy. Clin J Pain 1998; 14: 155-66.
17. Turk DC, Okifuji A, Sinclair JD, Starz TW. Differential responses by psychosocial subgroups of fibromyalgia syndrome patients to an interdisciplinary treatment. Arthritis Care Res. 1998 Oct; 11(5):397-404.
18. Worrel LM, Krahn LE, Sletten CD, Pond GR. Treating fibromyalgia with a brief interdisciplinary program: initial outcomes and predictors of response. Mayo Clin Proc 2001 Apr; 76(4):384-90.
19. Zunin ID, Orenstein S, Chang M, Cho S. Comprehensive Pain Program outcomes evaluation: A preliminary study in Hawaii. Hawaii Med J. 2009 Aug; 68(7):158-61.
References

Thank You





























